Submitted:
20 May 2025
Posted:
21 May 2025
You are already at the latest version
Abstract
Background: Telemedicine home monitoring of physical rehabilitation in cardiovascular patients, which may substantially improve adherence and, thus, prognosis and quality of life, is an underused practice. Indeed, the Apps and websites available are generic and cannot be easily adapted to each specific rehabilitation protocol. We thus aimed at developing a flexible, low-cost, and open-source telemedicine tool that can be customized and operated by any healthcare professional with just user-level internet knowledge. Methods: The website was co-designed by an interdisciplinary team, including website developers and clinical experts in physical rehabilitation programs for patients with cardiovascular diseases. The operability and robustness of the website were tested on simulated patients and health professionals, and the suitability of the tutorial for website customization was assessed. Results: The website asks the patient to complete a periodic diary of physical activities (e.g., intensity, type, duration, warm-up, cool-down, subjective effort). At any time, the patient can see graphs of the different types of exercise performed during a selected period. The website allows healthcare professionals to browse patients' data, send feedback messages, and export data in a conventional spreadsheet format. The tutorial for website customization was prepared as a learning by doing tool. Conclusions: The website developed can interest cardiovascular physical rehabilitation professionals aiming at quickly and cheaply setting up an approach for home monitoring programs. This telemedicine tool can also be customized to different clinical applications and is particularly well suited for low-resource settings.
Keywords:
cardiac rehabilitation
; home monitoring
; open-source website
; healthcare follow-up
; telemedicine
; low-cost
1. Introduction
Physical exercise is good for health in general and especially as a tool in rehabilitation programs for patients with different diseases (e.g., cancer [2], respiratory disease [3], and pain [4]). In patients with atherosclerotic cardiovascular disease and heart failure, exercise training is associated with a reduction in hospitalization, adverse cardiovascular events, and mortality rates [5,6,7]. Therefore, the European and American Guidelines recommend patients with cardiovascular disease enroll in cardiac exercise rehabilitation [6,7].
Physical rehabilitation programs can be carried out at hospitals or other healthcare facilities. This clinical practice is excellent because healthcare professionals monitor the patient in person. However, the applicability and extension of rehabilitation programs for most patients who could benefit is limited. Indeed, the development of physical rehabilitation programs at healthcare premises is very expensive in terms of material infrastructure and labor requirements. It is also a problem for patients with time/work constraints or not living near such premises thus requiring expensive and bothering patient displacements. This problem is particularly relevant in rural areas with low-density populations and in underfinanced regions such as low- and medium-income countries [8]. Fortunately, developing rehabilitation programs at the patient’s home overcomes these limitations and has shown effectiveness in a variety of pathologies, particularly in cardiovascular diseases [9]. However, to be effective in terms of patient adherence, a home rehabilitation program requires as much frequent follow-up as possible by health care staff. Whereas such follow-up is difficult to apply through in-person home care visits, it is feasible and effective to use telemedicine tools to facilitate patient-professional interaction [8]. Unfortunately, the few applications (Apps) and websites available for home monitoring are proprietary and generic and thus cannot be easily adapted to each specific rehabilitation protocol. The only conventional option would require high development costs entrusted to professional website designers. Therefore, to solve this problem, our work focused on designing and testing a website for the home follow-up of physical rehabilitation for patients with cardiovascular diseases. This telemedicine tool should be characterized by its simplicity for patients and staff, safety by ensuring patient anonymity, open-source availability for any user, and negligible exploitation costs. Our specific twofold aims were first to develop a website that any healthcare professional can download and use as it is. A second and more outreaching objective was to provide a user-friendly Tutorial allowing any healthcare professional without training in website design to customize the pages content to any specific application field.
2. Materials and Methods
2.1. Website design
We developed a website that can be directly and straightforwardly used by any professional aiming to set up a home cardiovascular rehabilitation follow-up. To this end we followed the innovative approach shown in Figure 1.
The website template, which includes separate areas for patients and healthcare staff, was co-designed by an interdisciplinary team, including website developers and clinical experts in physical rehabilitation programs for patients with cardiovascular diseases. The part of the webpage for the patients is aimed at asking them to complete a periodic diary of different possible physical activities, including the date, type, and time, as well as data on the performance of a warm-up and cool-down and the Borg scale score during exercise (used for subjective self-monitoring through perception of effort). At any time, the patient should be able to see graphs of the data on the different types of exercise performed during a selectable time window. The part of the webpage for healthcare professionals should allow them to browse and select the patients' diaries, observe their data in plot format, and send them a feedback message. The healthcare staff should also be able to export any required patient’s data in a conventional spreadsheet format for further analysis.
Once the website prototype was implemented, its usability and reliability were tested by using simulated patients and healthcare staff involving more than 3000 transferred data and messages. Each simulated patient used the website to introduce the data on their daily rehab exercises, and the testing process was followed up by professionals playing the role of the healthcare staff in charge of the patient’s rehabilitation program. At the end of the test, all the professionals involved checked whether there were incidents in the process and verified that all the patient’s exercise data downloaded from the webpage for further data analysis were fully accurate and easily usable.
2.2. Website customization
To ensure that the website layout can be easily modified for different variants fitting the aims of potential users, we developed a Tutorial for health professionals with no expertise in website development (Supplementary material). The Tutorial has 3 different sections and is designed as a learning by doing tool [10]. The first section is addressed to healthcare professionals who are not familiar with the physical rehabilitation website. This section explains how this website works since it will be used as the original template for creating websites for other applications. The second section of the Tutorial provides step-by-step instructions on how to install the website, create users and verify its functionality. The third section presents two examples: the first one explains how to carry out minor modifications in the webpage template to adapt it to the user specific interest and application; the second example guides healthcare professionals who aim to use the website template to create a home follow-up application for a completely different application in any field of nursing, physiotherapy, and medicine, by using the example of creating a website for general healthcare follow-up
3. Results
3.1. Website design
3.1.1. Website platform.
The website was created focusing on minimum cost, easy usability, and the possibility to allow straightforward source cloning by any interested user. Among the many different public platforms available for building websites, WebflowTM was chosen to serve as the front-end (the visible part of the website) for its web cloning features. Indeed, this platform offers the possibility to post an entire website, e.g. the one we designed, in their ‘Made in Webflow’ section and to allow other Webflow users to clone this site freely. The XanoTM platform was selected because its ‘Snippets’ function allows the backend to be cloned easily. After cloning the original site, the user can rename the new website with any specific name (xxx) with the format ‘https://xxx.webflow.io’. For instance, our web rehabilitation site was named https://exercise-follow-up-template.webflow.io/. If the user wants to replace the extension “.webflow.io” by a more common one (e.g., “.com”) it is possible, at a very low cost (10-20 US$/year), to buy a website domain (i.e., address) and link it to the generated Webflow site.
The Tutorial in the Supplementary Material shows how any user can freely register on the platforms and clone the website and the backend for their use. Everything required for such cloning can be accessed freely. However, payment is required to achieve the website functionality, specifically to connect the front end to the back end. When following the Tutorial, this payment must be completed before performing any customizations. It involves upgrading the free website plan to a paid plan (see Supplementary Materials). It is interesting to mention that the cost (168 US$/year as of April 2025) is virtually free (<0.5 US$/day).
3.1.2. Patient’s interface
When the patient is included in the rehabilitation program website, the healthcare staff in charge provides them with a username and a password, e.g., randomly generated, thus ensuring full anonymity on the website and the internet. The entry point of the template website is the login page (Figure 2). Through this page, users are authenticated and then redirected to the patient’s interface.
When a patient logs in, they is directed to the patient’s home webpage (Figure 3), where the messages interchanged with the healthcare staff can be seen, and the patient can send messages to the healthcare staff.
Then, using the menu on the top of the page the patient can go to ‘Enter data’, ‘My track’ and ‘Information’ pages, as well as log out. At the ‘Enter data’ page (Figure 4), the patient can complete the physical activity diary. The user can select a date, which is useful in case of reporting data of rehabilitation exercises from previous days. The exercise type can also be selected, and, if the patient has done an exercise type that is not included in the list, the ‘Other’ option can be selected, and a free text field will appear to specify it. Additionally, if a patient has exercised more than once a day, more entries can be made for that same day with the details of each physical activity.
By clicking the ‘My track’ button in the top menu, the patient can see the time evolution of their exercises (Figure 5). Also, they can choose which exercise to see graphically and on which time scale.
At the ‘Information’ page (Figure 6), the patient can download the website user instructions and any written or video information that the rehabilitation program has made available to them.
By clicking at the ‘Log Out’ button on the top-right of any page, the user will be logged out of the website and redirected to the entry point, i.e., the login page.
3.1.3. Healthcare staff’s interface
Users who are part of the healthcare staff will be automatically identified as a program professional (according to their username) and directed to the staff’s home page (Figure 7). There, the most recent messages interchanged with patients can be seen (either all of them or filtered by patients). Also, messages can be sent by filling the ‘Send a message’ box with the patient’s ID and the message.
Through the menu on the top of the page, the staff user can go to ‘My patients’ or ‘Information’ pages, as well as log out. At the ‘My patients’ page (Figure 8), the user can browse and select among all the patients included in the home care program to see a graphical display of the time evolution of the patient’s activities. In addition, the buttons below the graphs allow the professional to send a message to the patient (redirecting to the homepage), to download the data (in ExcelTM format) corresponding to the graphs on the screen in an (‘Download data for these filters’ button), or to download all the data from all the patients (‘Download data of all patients’ button), so that any analysis tool can be used to further process the data. The ExcelTM files data can be accessed by free readers.
The staff interface also has an ‘Information’ page (similar to that of the one in the patient homepage) (Figure 6) where the user can download the website instructions for staff and any other information that has been made available to patients. While being at any page the staff can log out by clicking at the ‘Log Out’ button at the top-right of the page.
The test on the simulated patients and professionals showed that both the patient and healthcare webpages are clear and user friendly, and it was verified that there were no errors in the downloaded data as compared with the ones introduced in the rehabilitation diaries. The designed websites were satisfactorily tested using the most widely used internet browsers (Google Chrome, Safari, Microsoft Edge, Mozilla Firefox, and Opera) [11].
3.2. Website customization
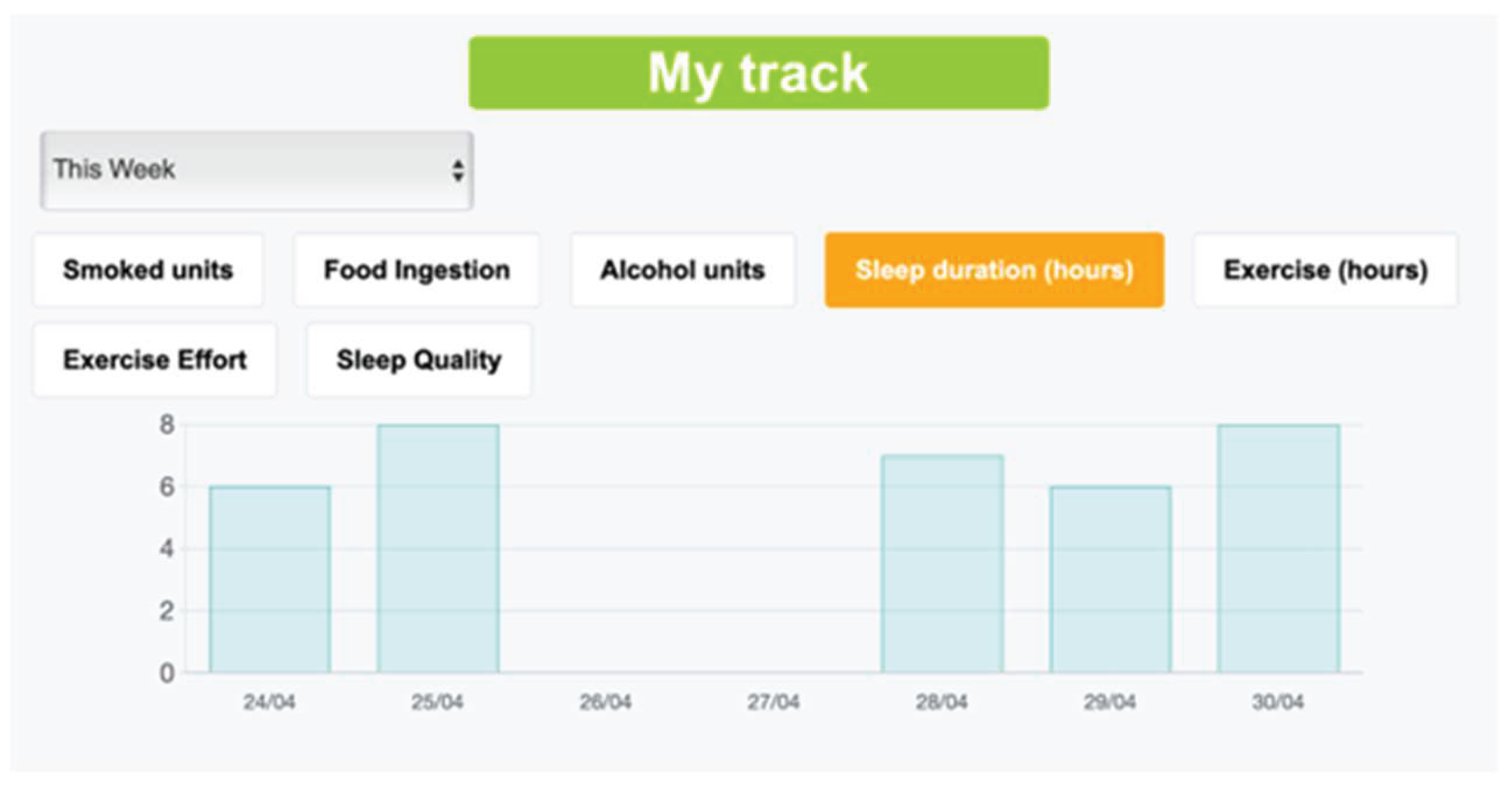
The previously shown website for physical rehabilitation can be used as a template for slightly modifying it or for creating a different website for other applications in homecare follow-up, as explained in detail in the Tutorial (Supplementary Materials). The second example of the Tutorial’s third section focuses on the steps to follow for modifying the questions to ask the patient and for redesigning the webpage appearance. Given that the Tutorial is designed as a learning by doing tool for healthcare users with no previous training in website construction, the reader is asked to create a new website example aimed at following up issues regarding the general health status of the patient. This example is not comprehensive and thus not aimed at immediate use, it is simply intended for illustrating the process for website customization. When the reader fulfils the Tutorial tasks, they is able to create a website for following-up patient objective behaviors (medication compliance, sleep time, exercise duration, smoking, alcohol drinking, and eating) and their subjective perceptions (sleep quality, exercise effort and general wellbeing), as illustrated in Figure 9. The “My track” page then shows the time course of the new variables (Figure 10) after making some modifications. The Tutorial also describes how to modify other webpage details, e.g., to change webpage logo and presentation or modify the files in the ‘Information’ pages.
The estimated time required to perform the different tasks described in the Tutorial by a person who has a user-level knowledge of internet, not trained in webpage construction, were the following: 1) 1.5 -1.75 h to clone and install the website as it is , 2) 0.5-0.75 h to implement a simple variant of the downloaded website, and 3) 1.25-1.5 h to customize it to for a different application in another healthcare application.
4. Discussion
The telemedicine tool we present in this work enables any professional in the field of physical rehabilitation of patients with cardiovascular diseases to immediately and straightforwardly initiate a home care monitoring program by directly using the developed website. Moreover, the Tutorial we propose may allow that, after a minimum training, any healthcare professional without previous experience in website design is able to customize the patient’s and healthcare professional’s pages for home monitoring in any clinical specialty beyond physical rehabilitation.
We based our telemedicine tool on public internet platforms to avoid requiring the use of proprietary information and communication networks (e.g., from hospitals or other institutions). This enables any healthcare professional to use the website in regions with poorly available Information and Communication Technology provisions from specific institutions, as is common in small or rural healthcare centers or in private practices. The two commercial internet platforms we selected provide the highest data security, processing integrity, privacy, and confidentiality according to most rigorous safety standards (SOC 2 Type 2 certification). Moreover, it is noteworthy that the website was designed to ensure full patient’s privacy protection. Indeed, on the one hand, no personal or clinical data related to the patient’s health is introduced into the website (only anonymous data on daily exercise). Furthermore, the patient’s username and password can be randomly generated by the healthcare professional, hence including no information relative to the patient. Interestingly, the code file linking each patient with their username and password can be kept in a private file curated by the healthcare professional and stored in a physical repository outside the internet and even outside any computer.
The webpages we designed were deliberately simple to facilitate usability for most patients and healthcare professionals. For instance, each tab in the patient page is contained in a single screen, the labels and windows to introduce data are great enough to enhance visibility for aged patients or those with visual limitations, and colors belong to a blind color friendly palette [12]. For the sake of simplicity and flexibility, the data processing and viewing in the healthcare professional page was minimized. Alternatively, allowing the data to be downloaded into a conventional data sheet format makes it possible that any healthcare user involved in the program to further define a specific graphical and statistical processing format. Also, for simplicity we avoided including video calls, with the bidirectional patient-healthcare professional communication based on written messages into the website. If deemed necessary, nowadays a video call can always be established by widespread conventional tools. Interestingly, the website is designed for friendly appearance in both computer, tablet or mobile phone screens. The latter can be particularly useful for open-source initiatives for home monitoring in low- and middle-income countries, where mobile phones are progressively ubiquitous [14].
A remarkable feature of our approach in developing this telemedicine tool was its flexibility to be easily customized for a wide range of applications in home monitoring of patients with different health diseases. As illustrated by the customization section in the Tutorial (a simple possible example for general healthcare follow-up), the website questions and pages layout can be easily modified to cover almost all questions that any home came program may need, e.g., in endocrinology, pneumology, sleep disturbances, neurology, psychiatry, postoperative and elder patient care, high-risk pregnancies monitoring, or neonatal follow-up [15-18]. It could be also possible to customize the website for professional team-building purposes or for improving coordination among healthcare staff in places without availability of professional communication networks [19-21]. For instance, following the rationale and structure of the website template we present herein, the role of the patients can be replaced by health community workers or small rural/local centers, and reference hospitals can play the role of the health professionals as network coordinators. Accordingly, instead regarding exercise activity, the data interchanged among them could be on a variety of aspects related to clinical practice (e.g., diseases incidence, treatments application, waiting lists or professional inter-consultation), thus allowing to set up an empowering customized network to improve patient’s healthcare. Most importantly, with the aid of the Tutorial, such website customization can be carried out by health professionals who are not experts in the construction of webpages, and simply requires internet access, with no need for institutional digital networks availability.
5. Conclusions
First, the website developed and presented herein can be of interest for cardiovascular physical rehabilitation professionals aiming at quickly setting up a free tool for home monitoring programs. Second, this telemedicine tool can be customized for different fields of health care applications. Finally, being open-source, very low-cost, and not requiring institutional digital infrastructure, this approach can be of particular interest in low-resource settings.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Funding
This research received no external funding.
Authors Contributions
Conceptualization: A.S., N.F.; Technological design: A.S., R.S. R.F., J.O.; Healthcare design: D.M., A.L., N.F.; Website development: A.S.; original draft preparation: A.S., N.F.; final manuscript edition and project direction: N.F. All authors have read and agreed to the published version of the manuscript.
Institutional Review Board Statement
Not applicable.
Data Availability Statement
This work did not involve data filing. All the methodological information is provided in the main text and in the Supplementary Materials.
Public Involvement Statement
No public involvement in any aspect of this research.
Use of Artificial Intelligence
AI or AI-assisted tools were not used in drafting any aspect of this manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Stamatakis E, Biswas RK, Koemel NA, Sabag A, Pulsford R, Atkin AJ, Stathi A, Cheng S, Thøgersen-Ntoumani C, Blodgett JM, Bauman A, Celis-Morales C, Hamer M, Gill JMR, Ahmadi MN. Dose Response of Incidental Physical Activity Against Cardiovascular Events and Mortality. Circulation. 2025 Apr 15;151(15):1063-1075. [CrossRef]
- Xu SH, Xu H, Xiao KW, Mao SJ. Exercise rehabilitation on patients with non-small cell lung cancer: A meta-analysis of randomized controlled trials. World J Clin Cases. 2025 Apr 16;13(11):100161. [CrossRef]
- Rochester CL, Alison JA, Carlin B, Jenkins AR, Cox NS, Bauldoff G, Bhatt SP, Bourbeau J, Burtin C, Camp PG, Cascino TM, Dorney Koppel GA, Garvey C, Goldstein R, Harris D, Houchen-Wolloff L, Limberg T, Lindenauer PK, Moy ML, Ryerson CJ, Singh SJ, Steiner M, Tappan RS, Yohannes AM, Holland AE. Pulmonary Rehabilitation for Adults with Chronic Respiratory Disease: An Official American Thoracic Society Clinical Practice Guideline. Am J Respir Crit Care Med. 2023 Aug 15;208(4):e7-e26. [CrossRef]
- Du S, Cui Z, Peng S, Wu J, Xu J, Mo W, Ye J. Clinical efficacy of exercise therapy for lumbar disc herniation: a systematic review and meta-analysis of randomized controlled trials. Front Med (Lausanne). 2025 Mar 28;12:1531637. [CrossRef]
- Molloy CD, Long L, Mordi IR, Bridges C, Sagar VA, Davies EJ, Coats AJS, Dalal H, Rees K, Singh SJ, Taylor RS. Exercise-based cardiac rehabilitation for adults with heart failure - 2023 Cochrane systematic review and meta-analysis. Eur J Heart Fail. 2023 Dec;25(12):2263-2273. [CrossRef]
- Byrne RA, Rossello X, Coughlan JJ, Barbato E, Berry C, Chieffo A, Claeys MJ, Dan GA, Dweck MR, Galbraith M, Gilard M, Hinterbuchner L, Jankowska EA, Jüni P, Kimura T, Kunadian V, Leosdottir M, Lorusso R, Pedretti RFE, Rigopoulos AG, Rubini Gimenez M, Thiele H, Vranckx P, Wassmann S, Wenger NK, Ibanez B; ESC Scientific Document Group. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur Heart J. 2023 Oct 12;44(38):3720-3826. doi: 10.1093/eurheartj/ehad191. Erratum in: Eur Heart J. 2024 Apr 1;45(13):1145. [CrossRef]
- Vrints C, Andreotti F, Koskinas KC, Rossello X, Adamo M, Ainslie J, Banning AP, Budaj A, Buechel RR, Chiariello GA, Chieffo A, Christodorescu RM, Deaton C, Doenst T, Jones HW, Kunadian V, Mehilli J, Milojevic M, Piek JJ, Pugliese F, Rubboli A, Semb AG, Senior R, Ten Berg JM, Van Belle E, Van Craenenbroeck EM, Vidal-Perez R, Winther S; ESC Scientific Document Group. 2024 ESC Guidelines for the management of chronic coronary syndromes. Eur Heart J. 2024 Sep 29;45(36):3415-3537. doi: 10.1093/eurheartj/ehae177. Erratum in: Eur Heart J. 2025 Feb 21:ehaf079. [CrossRef]
- Sugiharto F, Nuraeni A, Trisyani Y, Melati Putri A, Aghnia Armansyah N. Barriers to Participation in Cardiac Rehabilitation Among Patients with Coronary Heart Disease After Reperfusion Therapy: A Scoping Review. Vasc Health Risk Manag. 2023;19:557-570. [CrossRef]
- Anderson L, Sharp GA, Norton RJ, Dalal H, Dean SG, Jolly K, Cowie A, Zawada A, Taylor RS. Home-based versus centre-based cardiac rehabilitation. Cochrane Database Syst Rev. 2017 Jun 30;6(6):CD007130. doi: 10.1002/14651858.CD007130.pub4. Update in: Cochrane Database Syst Rev. 2023 Oct 27;10:CD007130. [CrossRef]
- Zhang, X.-S.; Xie H. Learning by Doing Approach in the Internet Environment to Improve the Teaching Efficiency of Information Technology, Physics Procedia, 2012, 24C, 2231-2236. [CrossRef]
- Browser Market Share Worldwide, StatCounter. Available online: https://gs.statcounter.com/ (accessed on 2025, April 11th).
- Frane A. A Call for Considering Color Vision Deficiency When Creating Graphics for Psychology Reports. J Gen Psychol. 2015;142(3):194-211. [CrossRef]
- Open-source medical devices for low- and middle-income countries. Available online: https://open-sourc-medical-devices.com (accessed on 2025, April 11th).
- The-State-of-Mobile-Internet-Connectivity-Report-2024.pdf. GSMA. Available online: https://www.gsma.com/r/wp-content/uploads/2024/10/The-State-of-Mobile-Internet-Connectivity-Report-2024.pdf?utm_source=website&utm_medium=button&utm_campaign=somic24 (accessed on 2025, April 11th).
- Farias FAC, Dagostini CM, Bicca YA, Falavigna VF, Falavigna A. Remote Patient Monitoring: A Systematic Review. Telemed J E Health. 2020 May;26(5):576-583. [CrossRef]
- Suemitsu T, Kadooka M, Mitani T, Matsui H, Suzuki M. Telemedicine for home care of fetal growth restriction with mobile cardiotocography: A case series. Int J Gynaecol Obstet. 2023 Jun;161(3):949-955. [CrossRef]
- Isetta V, Negrín MA, Monasterio C, Masa JF, Feu N, Álvarez A, Campos-Rodriguez F, Ruiz C, Abad J, Vázquez-Polo FJ, Farré R, Galdeano M, Lloberes P, Embid C, de la Peña M, Puertas J, Dalmases M, Salord N, Corral J, Jurado B, León C, Egea C, Muñoz A, Parra O, Cambrodi R, Martel-Escobar M, Arqué M, Montserrat JM; SPANISH SLEEP NETWORK. A Bayesian cost-effectiveness analysis of a telemedicine-based strategy for the management of sleep apnoea: a multicentre randomised controlled trial. Thorax. 2015 Nov;70(11):1054-61. [CrossRef]
- Isetta V, Lopez-Agustina C, Lopez-Bernal E, Amat M, Vila M, Valls C, Navajas D, Farre R. Cost-effectiveness of a new internet-based monitoring tool for neonatal post-discharge home care. J Med Internet Res. 2013 Feb 18;15(2):e38. [CrossRef]
- Surka S, Edirippulige S, Steyn K, Gaziano T, Puoane T, Levitt N. Evaluating the use of mobile phone technology to enhance cardiovascular disease screening by community health workers. Int J Med Inform. 2014 Sep;83(9):648-54. [CrossRef]
- Misra V, Sedig K, Dixon DR, Sibbald SL. Prioritizing coordination of primary health care. Can Fam Physician. 2020 Jun;66(6):399-403. Erratum in: Can Fam Physician. 2020 Aug;66(8):554. Erratum in: Can Fam Physician. 2020 Aug;66(8):554.
- Wilson MM, Devasahayam AJ, Pollock NJ, Dubrowski A, Renouf T. Rural family physician perspectives on communication with urban specialists: a qualitative study. BMJ Open. 2021 May 13;11(5):e043470. [CrossRef]
Figure 1.
Diagram of the website to follow-up physical rehabilitation of cardiovascular patients at home. Any interested professional can download the website freely (1) and maintain its original format or customize it using the downloaded Tutorial (2). The website is ready for home monitoring patient rehabilitation (3).
Figure 1.
Diagram of the website to follow-up physical rehabilitation of cardiovascular patients at home. Any interested professional can download the website freely (1) and maintain its original format or customize it using the downloaded Tutorial (2). The website is ready for home monitoring patient rehabilitation (3).
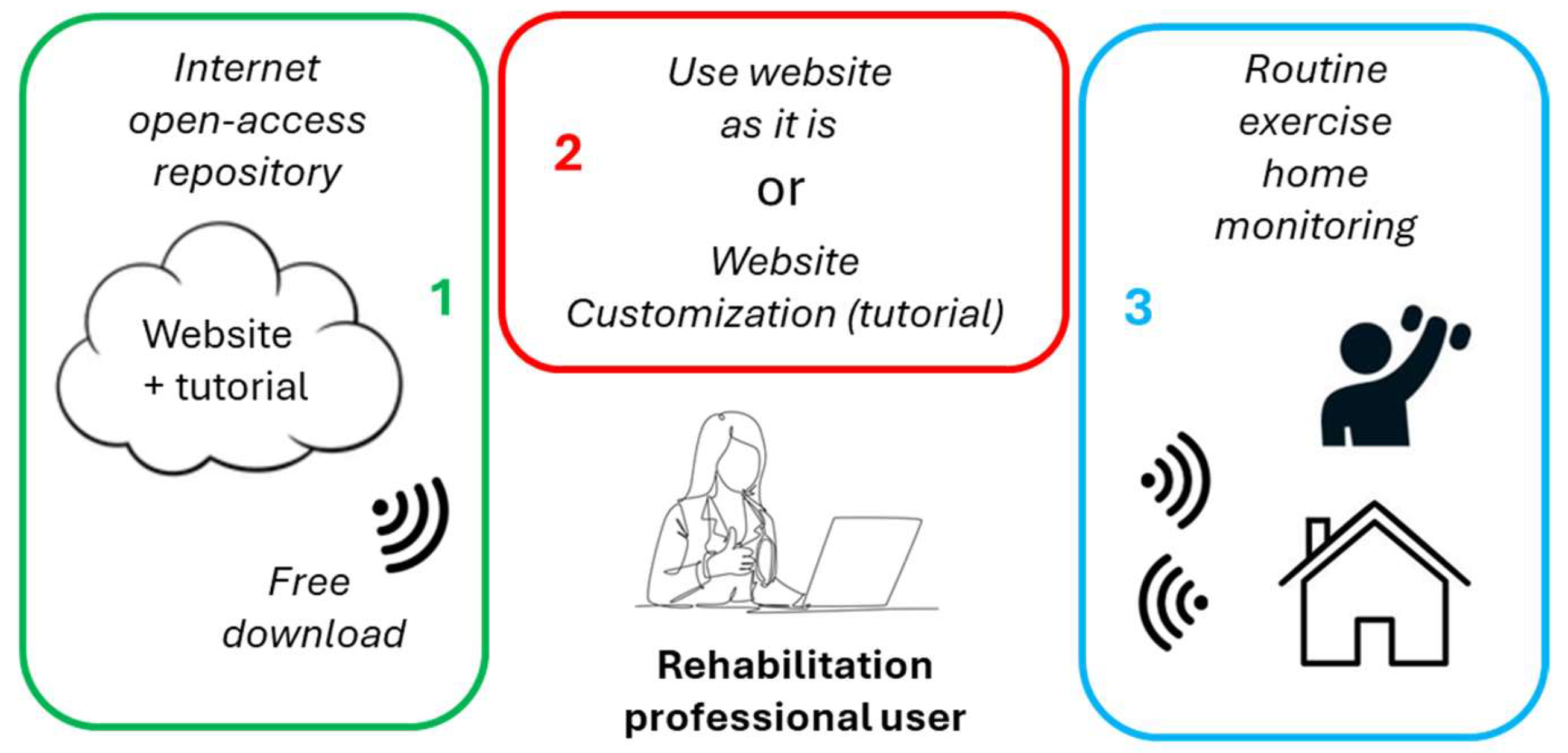
Figure 2.
Figure 2. Login page.
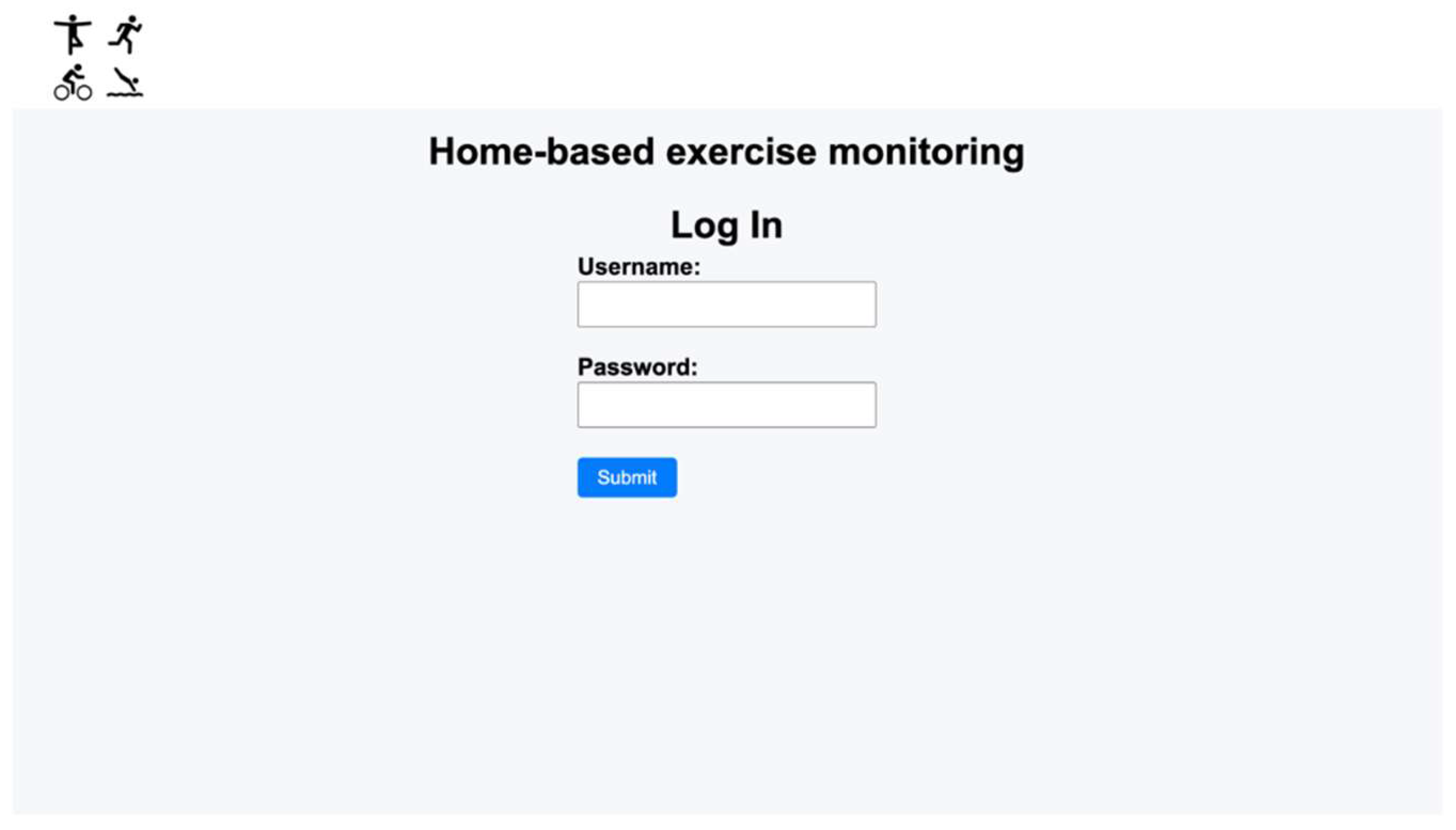
Figure 3.
Patient’s home page.
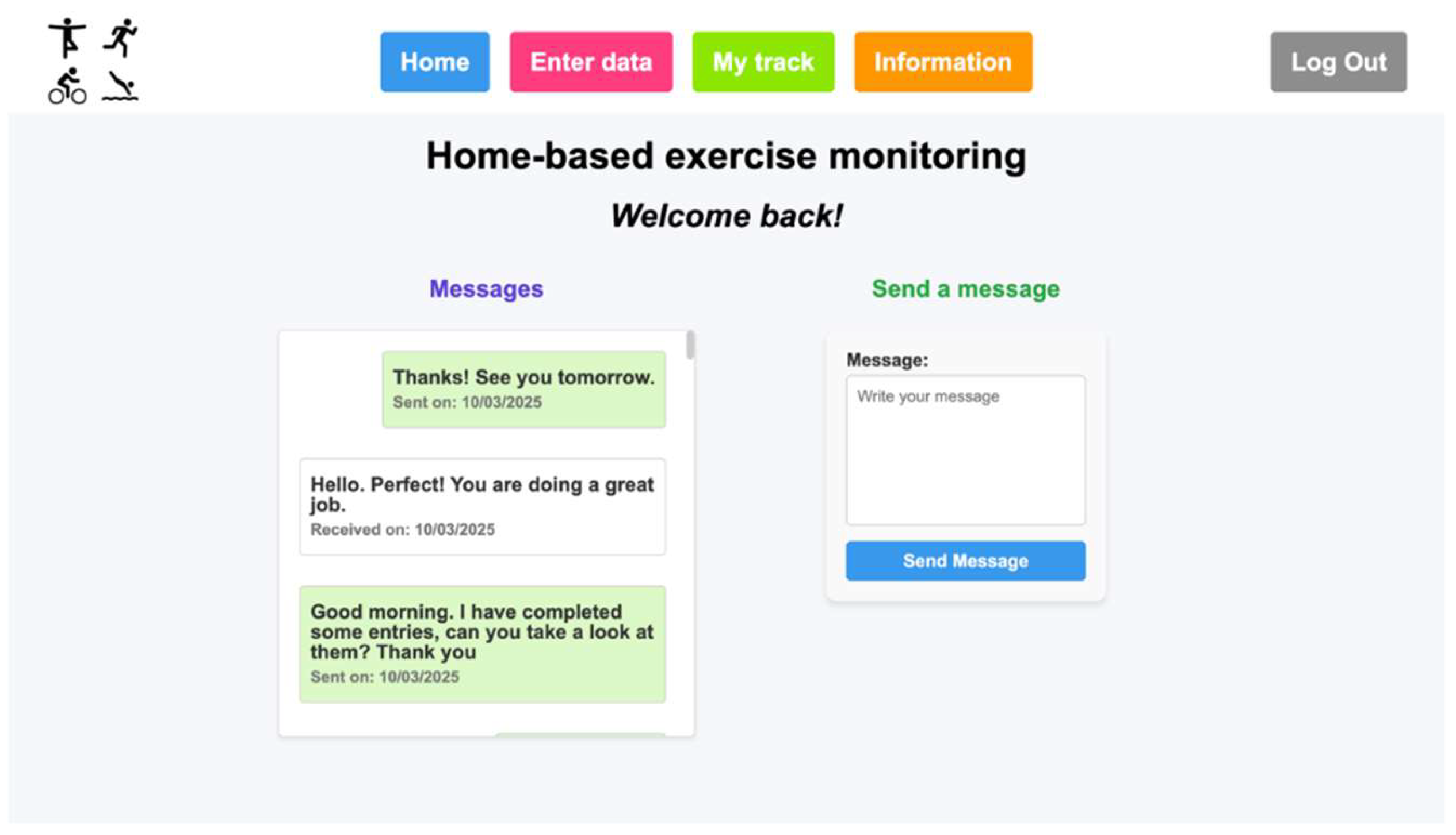
Figure 4.
Patient’s ‘Enter data’ page.
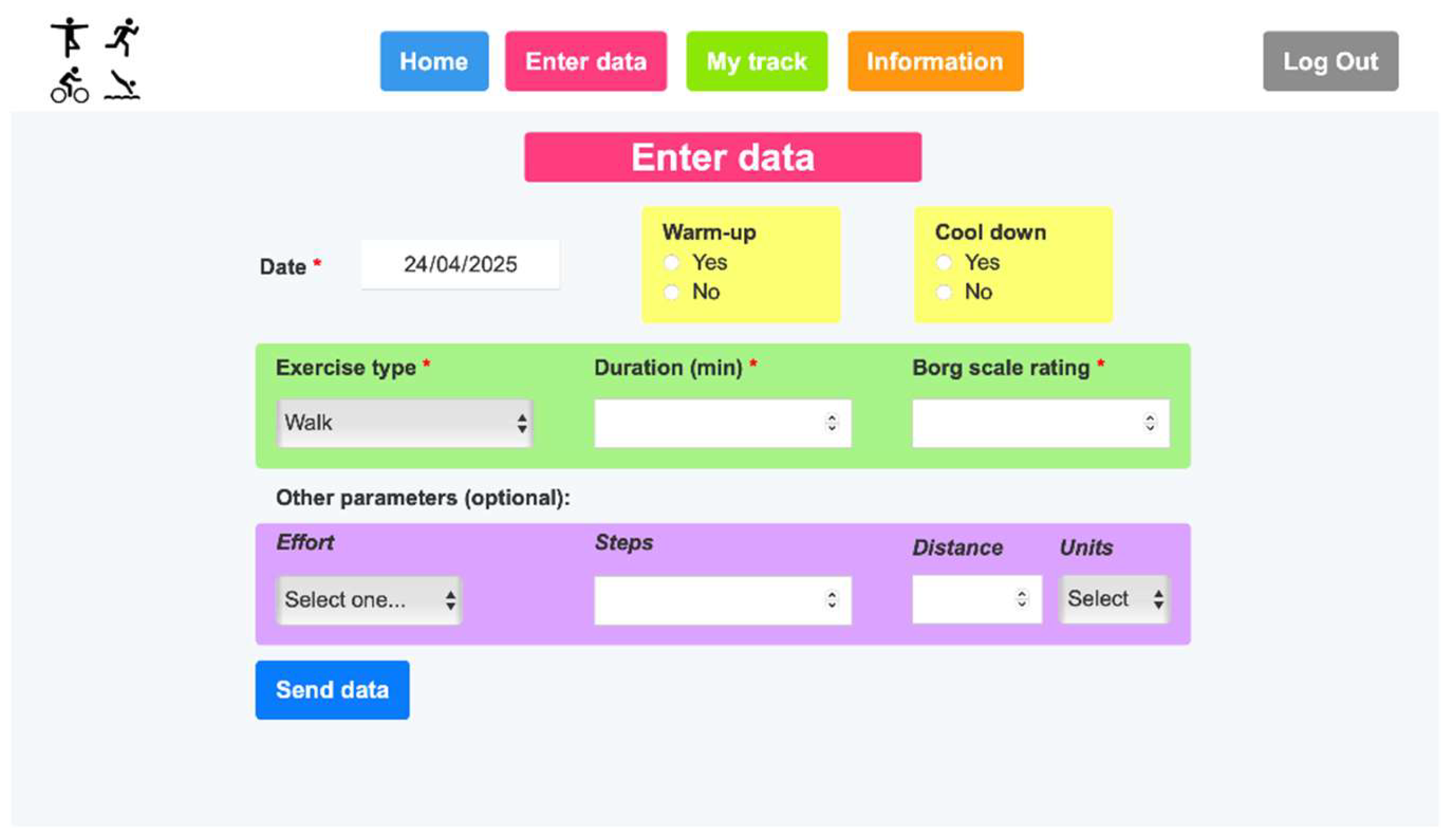
Figure 5.
Patient’s ‘My track’ page.
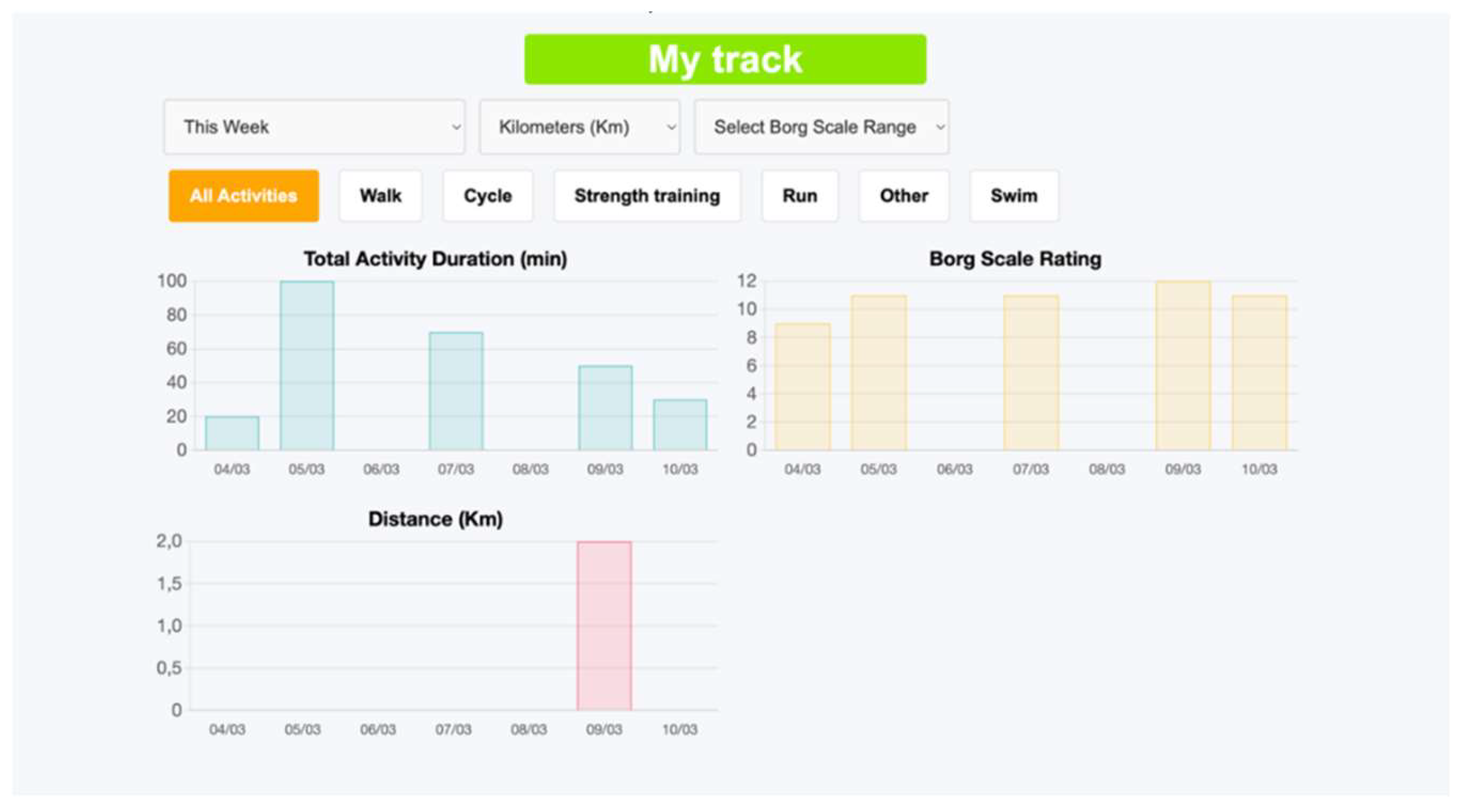
Figure 6.
Patient’s ‘Information’ page.
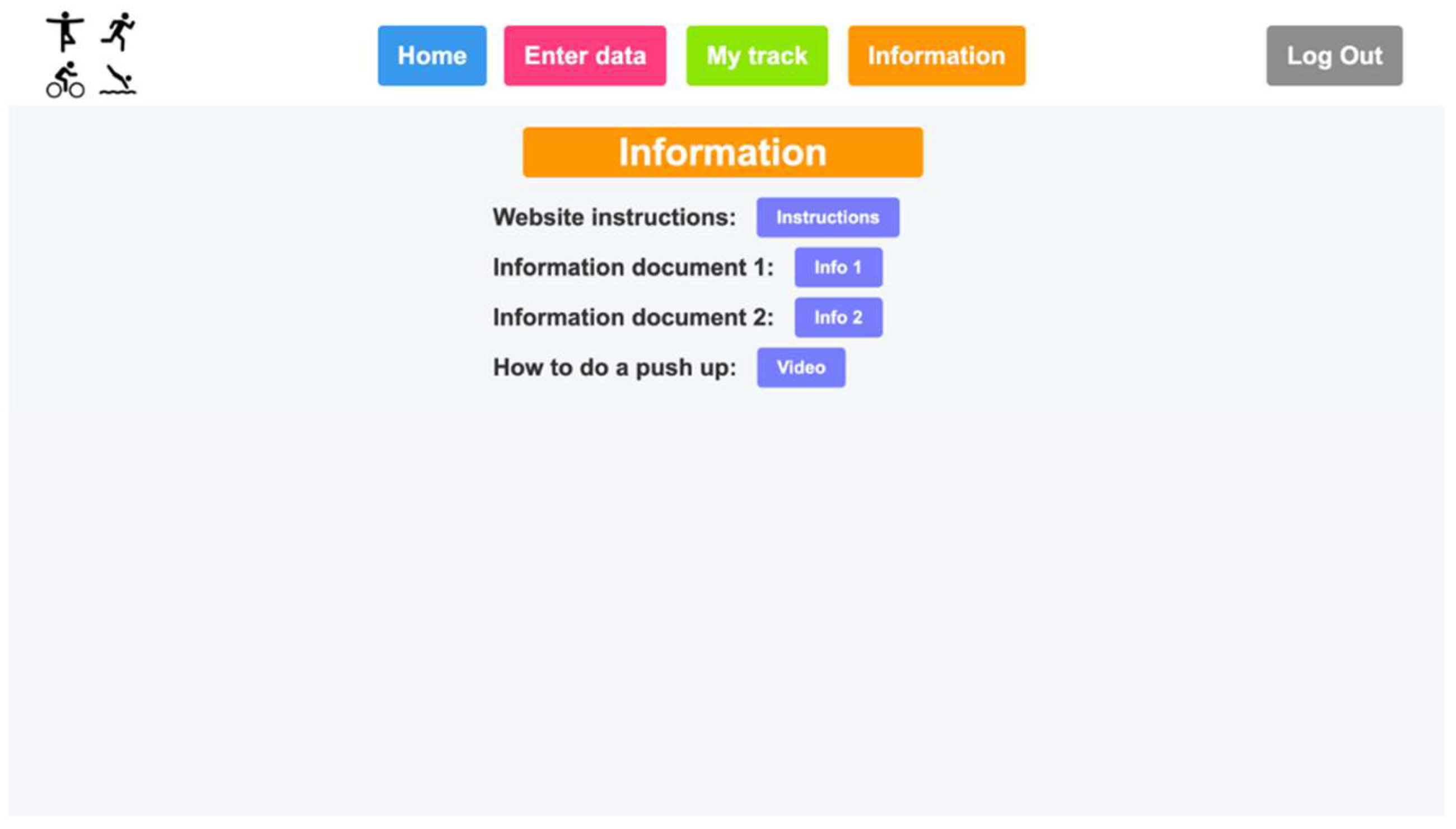
Figure 7.
Healthcare staff’s home page.
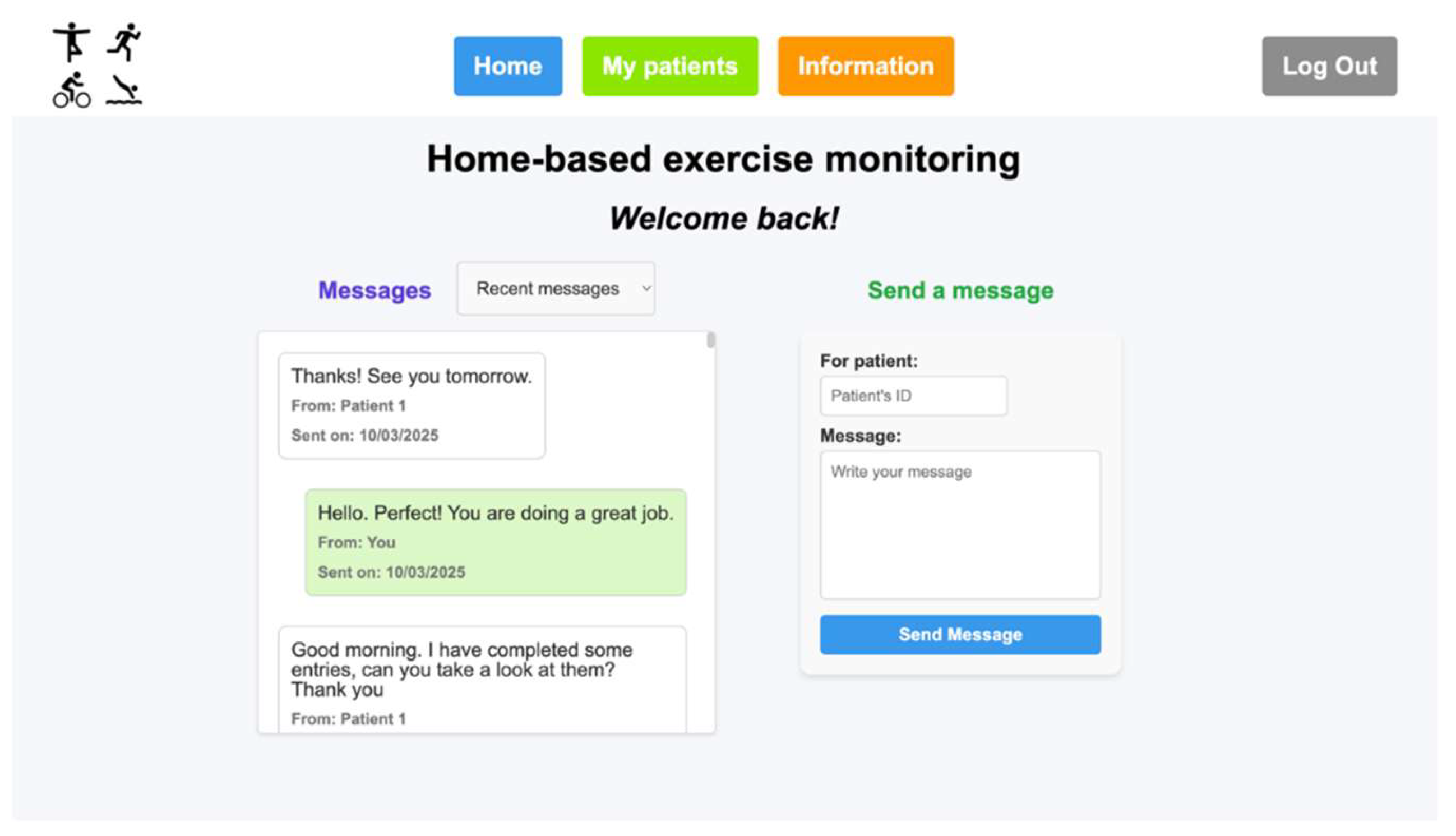
Figure 8.
Healthcare staff’s ‘My patients’ page.
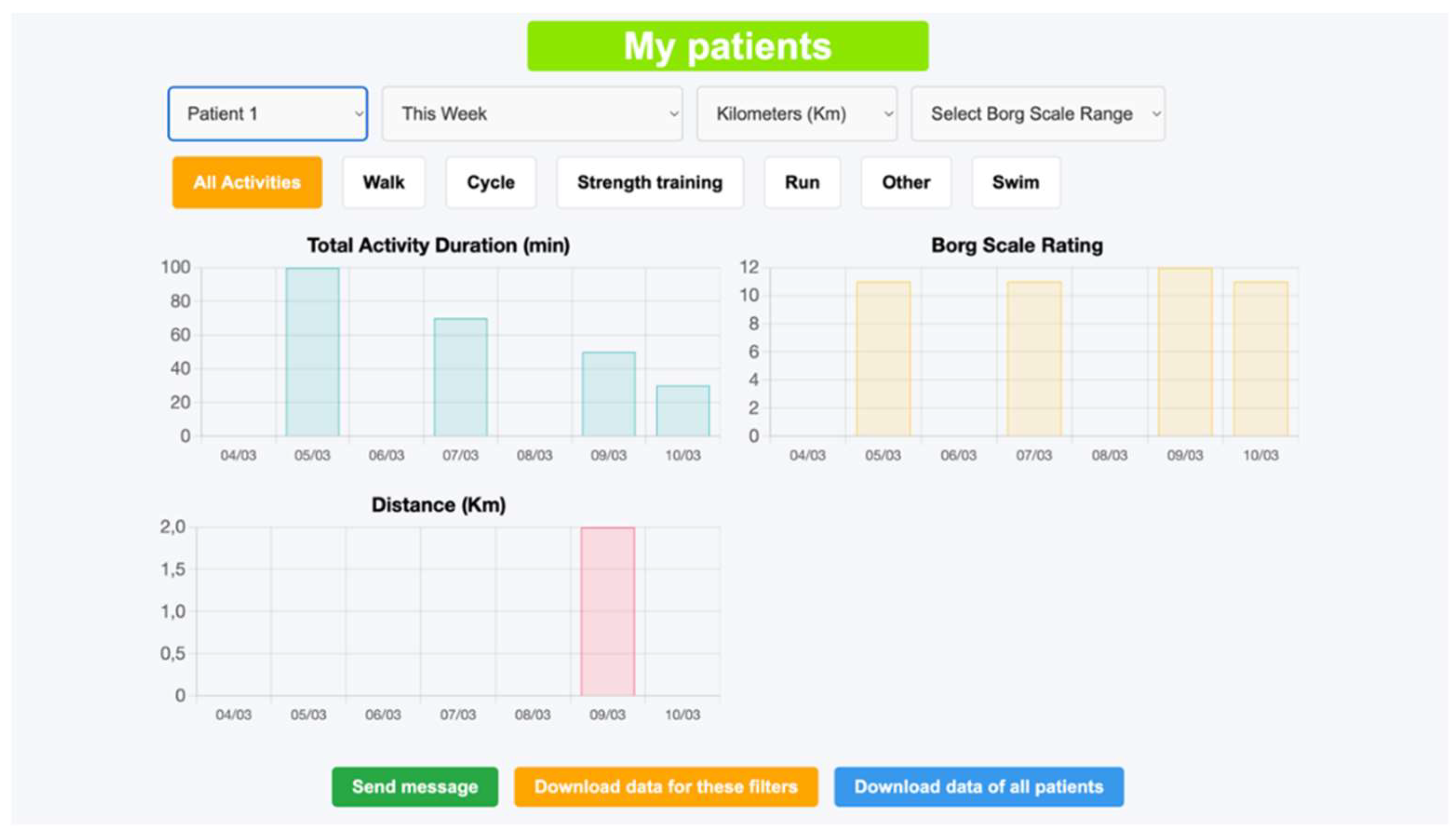
Figure 9.
Patient’s ‘Enter data’ page in the new customized webpage following the Tutorial (Supplementary Materials)
Figure 9.
Patient’s ‘Enter data’ page in the new customized webpage following the Tutorial (Supplementary Materials)
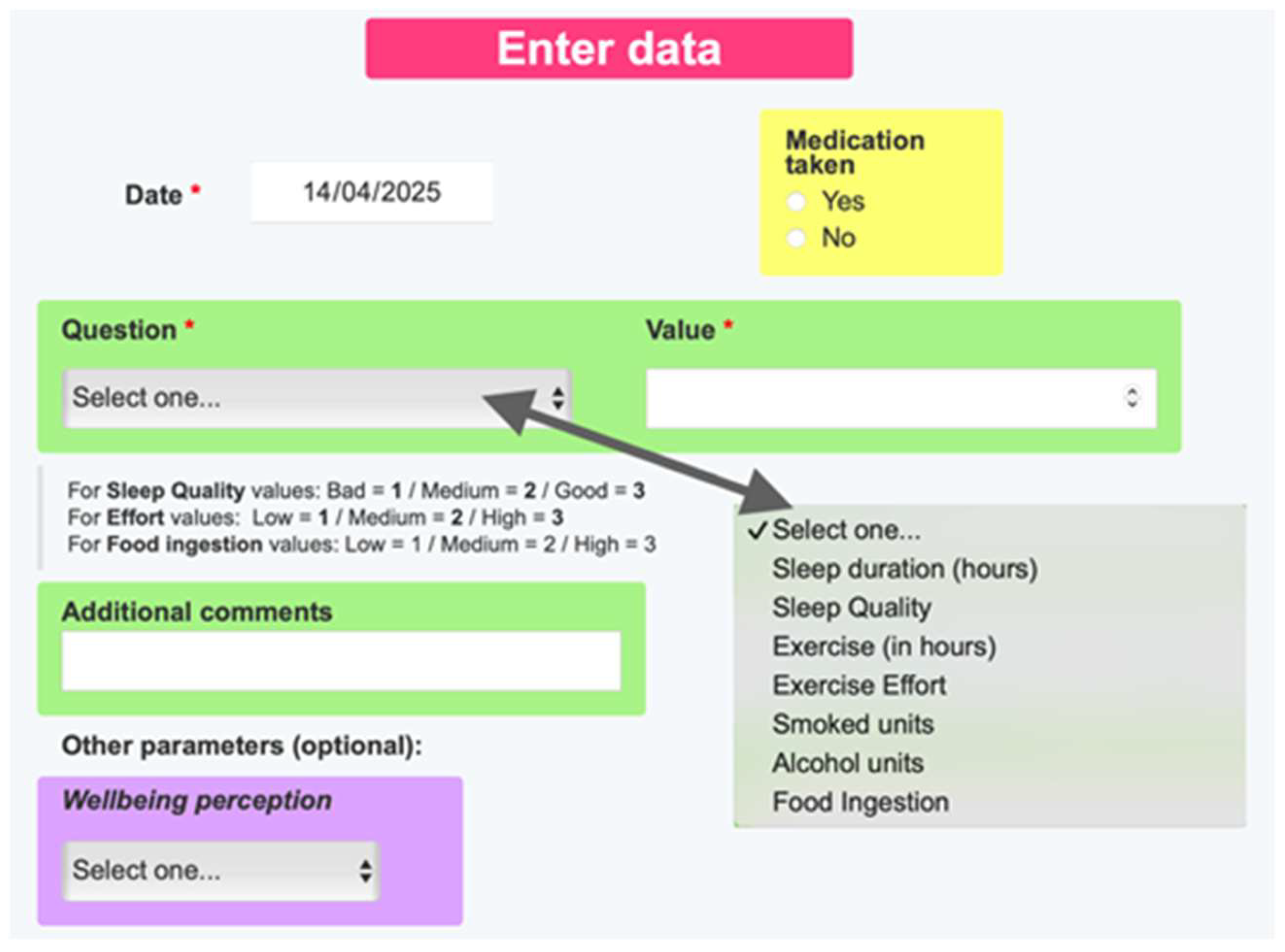
Figure 10.
Patient’s ‘My track’ page in the new customized webpage following the Tutorial (Supplementary Materials)
Figure 10.
Patient’s ‘My track’ page in the new customized webpage following the Tutorial (Supplementary Materials)
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



