Submitted:
20 May 2025
Posted:
20 May 2025
You are already at the latest version
Abstract
Recent documents from leading international pediatric respiratory societies have strongly encouraged the use of lung function tests in clinical practice and research. These tests can explore ventilatory function across its volumetric and temporal domains, providing information on the intrapulmonary location and extent of damage caused by respiratory diseases. The choice of which test to use in each case to investigate presenting respiratory symptoms depends on the patient's symptoms and the diagnostic-therapeutic phase being addressed.
In the most common and representative chronic pediatric condition—bronchial asthma—lung function tests play an especially important role due to the disease’s complexity and the fluctuating nature of airway obstruction. This review aims to examine the potential of various lung function tests in asthma, helping clinicians and researchers optimize diagnosis and follow-up with the most appropriate methodology.
Keywords:
spirometry
; forced oscillation technique
; interrupter technique
; bronchodilator and bronchoconstrictor challenges
; topographical and temporal ventilation heterogeneities
; vocal cord dysfunction
; dyspn
Introduction
Over the past decades, pediatric respiratory medicine has placed growing importance on lung function testing. Major international respiratory medicine societies [1,2,3,4,5] have published guidelines for evaluating the functional damage of respiratory diseases, standardizing and structuring tests for shared interpretation. This progress was made possible by the development of reference normative values for parameters by age, height, and sex [6,7,8,9,10].
As in adults, pediatric tests indicate the presence and extent of functional damage to the lungs, but not necessarily the underlying mechanisms [11]. For instance, a reduction in FEV₁ in an asthmatic child indicates airway obstruction, whereas in cystic fibrosis, the same reduction reflects compression of ectatic airways during forced expiration. In neuromuscular disorders, it represents the loss of respiratory muscle strength and endurance. As noted in guidelines, combining different tests helps to detect typical functional patterns of various pediatric respiratory diseases and to guide appropriate therapy [1,2,3,4,5].
Starting from the concept that respiratory diseases are inherently complex and characterized by varied functional patterns, this review aims to assess the ability of currently available lung function tests to explore and identify the structural and dynamic components of the most common pediatric disease: bronchial asthma [12,13]. A deeper understanding of the mechanisms and their in vivo interaction causing bronchospasm, through lung function testing, is crucial for both clinical care and research.
Clinical Applications and Discussion
Lung Function Evaluation
The most frequently used tests in pediatric clinics or pulmonary function labs for the initial evaluation of suspected bronchial asthma are spirometry, flow resistance measurement using the interrupter technique, and resistance estimation through respiratory impedance [1]. This first diagnostic step is crucial to confirm or exclude airway obstruction under baseline conditions. For instance, detecting an obstructive ventilatory pattern can immediately support the hypothesis of asthma based on clinical history and symptoms, thus allowing for prompt initiation of appropriate pharmacological treatment [14]. On the other hand, if airways appear normally patent, the next step is to select further diagnostic approaches to determine whether the patient’s or parents' reported symptoms are consistent with asthma.
Spirometry is traditionally the test that best identifies either normal patterns or obstructive functional damage [11]. Based on fluid dynamics principles [15], it can reveal deviations from expected ventilatory patterns [11]. However, the test requires considerable patient cooperation during forced expiratory maneuvers from full lung capacity, which often makes results unreliable and poorly repeatable, especially in preschool or early school-age children [16,17].
In some labs, the interrupter technique is used instead, which can assess function during quiet breathing with good accuracy [1,18,19], although day-to-day variability tends to be high [20]. The use of forced oscillation technique (FOT) [21,22,23,24] has opened new avenues in this field due to its high acceptability, minimal cooperation requirement, and its ability to evaluate lung function during quiet breathing. In pediatric practice, a single low-frequency oscillatory signal (5–8 Hz) is used to facilitate the measurement of resistance (R) and reactance (X) components of respiratory impedance (I) [22,23,24]. R reflects airway patency—an increase suggests airway obstruction. Conversely, X represents the system’s ability to absorb and transmit the oscillatory signal to the peripheral airways and lung parenchyma. A negative X at low frequency in asthma is consistent with ventilation heterogeneity as a result of some airways being so obstructed that oscillatory flow is redirected to better-ventilated regions [22,23,24]. Predicted normal values for FOT exist across pediatric age ranges, allowing the test to be broadly applied in both clinical and research settings [25,26].
Another technique that assesses ventilation heterogeneity in asthma is the multiple breath nitrogen washout (MBNW) [1,4,27,28,29]. This test measures the slope of nitrogen’s phase III during quiet breathing in 100% oxygen. In asthma, this slope increases due to uneven ventilation distribution. The Lung Clearance Index (LCI) quantifies the number of breaths required to reduce nitrogen concentration below a specific threshold. High LCI values indicate ventilation heterogeneity, mainly within the convective-dependent regions of the airways. The test is non-invasive and generally well tolerated by children.
Bronchodilator Response and Hyperresponsiveness
Historically, and in line with international guidelines [1,2,3,6,14], the bronchodilator response test is the most widely used in diagnosing bronchial asthma. This is based on the principle that responses exceeding the natural variability limits are consistent with the presence of disease. This test is also preferred due to its feasibility in any clinical setting and the excellent safety profile of the challenge. Bronchodilator reversibility can be assessed using spirometry or respiratory impedance (as mentioned above), with the known limitations of acceptability and data quality—especially for spirometry.
However, what remains uncertain and not fully standardized is the statistical threshold above which a positive response is considered diagnostic of asthma [6,11]. Clearly, a very large response is highly suggestive of asthma and supports the need for appropriate drug treatment. Borderline or just-above-threshold responses may reflect the effect of the drug on the airways but not necessarily indicate the presence of asthma—additional confirmatory tests may be required.
When it comes to bronchoconstrictor challenges in children, the tests are typically limited to spirometry and FOT. While spirometry presents challenges in ensuring data quality due to the level of cooperation required from the child, FOT is far less affected by this issue, as it analyzes respiratory function during tidal (quiet) breathing.
As mentioned earlier, FOT can assess two different and independent components of respiratory impedance: resistance and reactance, which can reveal different and not necessarily synchronous patterns during bronchoconstrictor response. A drop in reactance (X) during bronchoconstrictor challenge suggests the onset of ventilation heterogeneity—a shift of airflow from obstructed regions to better-ventilated ones [22,23,24].
Recent observations from our center show that in some cases, while airway resistance increases (indicating airway narrowing), the fall in reactance dominates the functional response, especially in the later phases of the test. For example, in the two cases shown in Figure 1, the drop in X due to increased resistance is much greater in panel B than in panel A. Literature data confirm that ventilation heterogeneity is a hallmark of asthma [30,31,32,33], and is associated with disease severity, clinical instability [28], and dyspnea [34]. Therefore, measuring FOT during bronchial hyperresponsiveness testing plays an important role not only in confirming the presence or absence of airway hyperresponsiveness but also in identifying patients prone to developing ventilation heterogeneity, and thus at greater risk of unstable disease.
Two additional aspects strongly support the use of FOT in assessing pediatric asthma.
In Figure 2, we describe a case of inspiratory dyspnea in a 12-year-old boy during a methacholine (MCh) challenge for suspected asthma. He had a persistent cough for over a year. At baseline, the boy showed no dyspnea, and inspiratory R and X were within normal Z-score limits [25] (Figure 2A). MCh inhalation from 20 mcg to 160 mcg during tidal breathing caused no symptom or mechanical changes. However, the next dose triggered sudden, acute cough followed by dyspnea, stridor, and jugular retraction during inspiration. At that point, inspiratory R significantly increased and X dropped well below normal limits (Figure 2B), peaking during mid-tidal inspiration. In the expiratory phase, R returned to normal and X increased. This pattern was consistent with vocal cord dysfunction. Laryngologic evaluation confirmed normal anatomy and motion, but videolaryngostroboscopy revealed paradoxical vocal fold movement—an adductory tendency during inspiration (Figure 2C). No other test could have so clearly and confidently identified this laryngeal reaction (rather than bronchospasm) as the cause of the acute dyspnea during the methacholine challenge.
Another unique advantage of FOT is its potential to noninvasively estimate the velocity of airway narrowing in asthma. In healthy individuals, after a deep breath, resistance decreases and gradually returns to baseline within 1–2 minutes. In asthma, this bronchodilatory effect is reduced, and airway re-narrowing occurs more rapidly [35,36]. If airway constriction is driven primarily by airway smooth muscle (ASM) shortening, modulated by external and internal loads, then a faster reconstriction rate reflects increased ASM contraction velocity—a key pathophysiological feature of asthma [37]. In research, this measurement could be critical for testing the efficacy of asthma medications and for monitoring disease progression.
Temporal Variability of Asthma
According to the current GINA 2025 guidelines [14], home monitoring of lung function in asthma can be performed using peak expiratory flow (PEF) measurements in the morning and evening. This test is based on the assumption that PEF is a functional marker of asthma, and that measuring it twice daily over a couple of weeks can reveal one of the most characteristic features of asthma—daily variability.
Although there is full agreement in the scientific community that temporal variability is a hallmark of asthma and can be very helpful diagnostically, the test is rarely used in clinical practice, despite the low cost of the equipment. This is mainly due to the difficulty in obtaining reliable and repeatable results and the uncertainty surrounding its physiological interpretation [11].
In contrast, using the Forced Oscillation Technique (FOT) to measure variability in lung function in asthma appears much more promising, as recently demonstrated [38,39,40]. This is due to its ease of execution, patient acceptability, result accuracy, and its statistical superiority compared to PEF. In healthy adults, the normal variation coefficient for resistance (R) is around 0.10. Preliminary data in children appear similar, although further confirmation is needed.
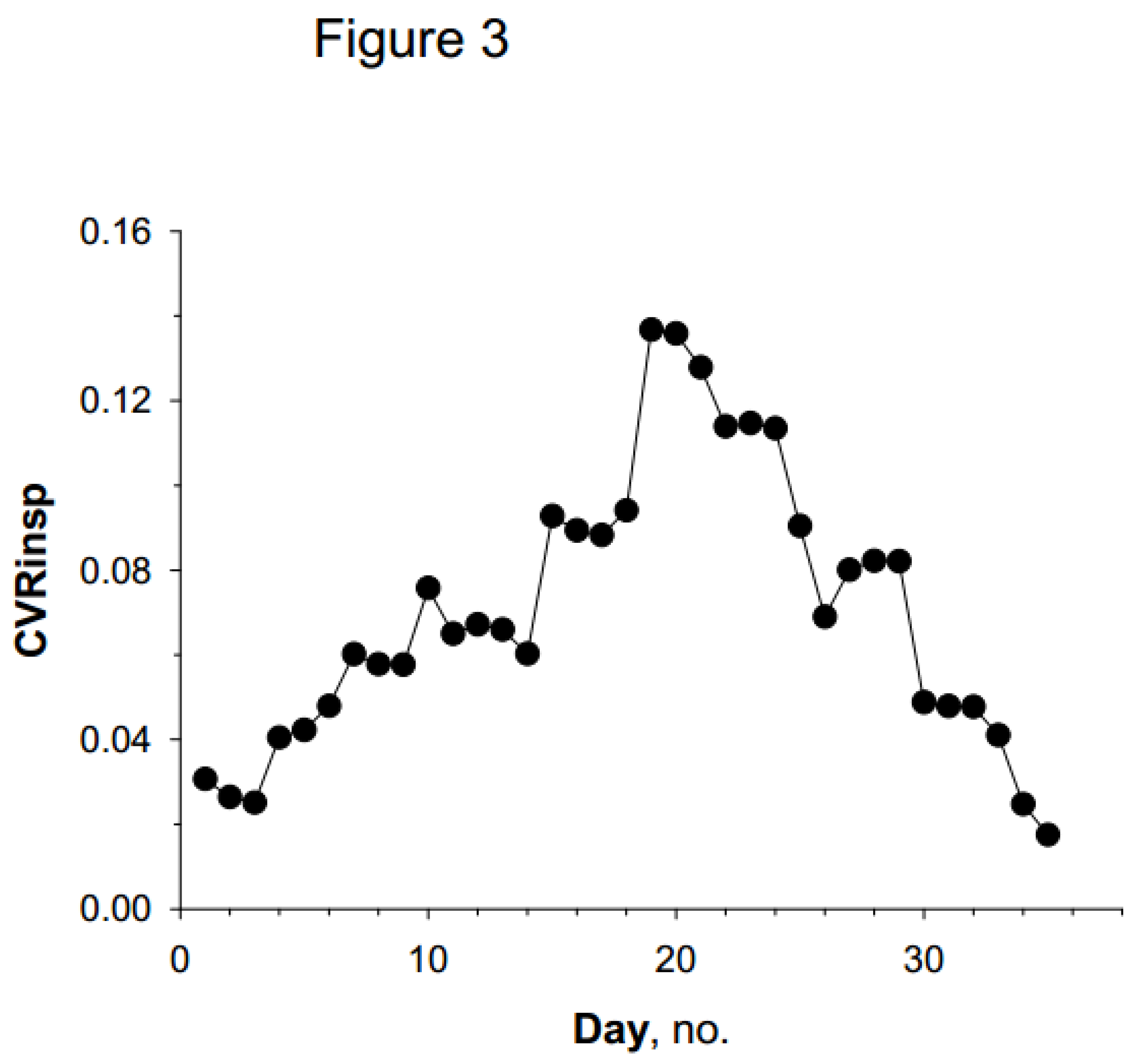
In the example shown in Figure 3, values of coefficient of variation of inspiratory resistance (CVRinsp) gradually increase beyond the expected normal range, thus suggesting significant instability of bronchial tone. Definitive reference values for the variability coefficient of R in children will be available soon. In such cases, asthma treatment is considered effective if R returns to within normal limits, both in terms of absolute values and in their temporal variability.
Conclusions and Future Directions
The content presented above demonstrates the immense potential of lung function tests in evaluating asthma, and underscores the importance of using these tools to effectively answer the clinician’s or researcher’s specific questions regarding the severity and nature of the disease in each individual case. However, not all tests are created equal, as each explores different aspects of lung function.
Given the anatomical, topographical, and temporal complexity of asthma, it is essential to evaluate airway function either comprehensively or selectively, depending on the clinical or research question being addressed. Spirometry, for example, is grounded in the principles of fluid dynamics, which gives it strong and robust overall results. However, this test cannot decompose the individual mechanisms contributing to airflow limitation—such as lung elastic recoil, upstream resistance before the choke point, and downstream airway collapsibility—since these are deeply interconnected. Additionally, poor cooperation from pediatric patients may reduce data quality and hinder accurate interpretation.
Looking ahead, there are exciting opportunities to evaluate lung function in asthmatic children using innovative techniques like MBNW and especially FOT, both in research and in routine clinical practice when a near-definitive diagnosis is required or when the goal is to identify and quantify the many mechanisms causing airflow limitation in the pediatric asthmatic airway.
References
- Beydon, N. , Davis, S.D.; Lombardi, E.; Allen, J.L.; Arets, H.G.M.; Aurora, P.; Bisgaard, H.; Davis, G.M.; FM; Eigen, H.; Gappa, M.; et al.; American Thoracic Society/European Respiratory Society Working Group on Infant and Young Children Pulmonary Function Testing. (2007). An official American Thoracic Society/European Respiratory Society statement: pulmonary function testing in preschool children. Am. J. Respir. Crit. Care Med. 2007, 175, 1304–1345. [Google Scholar] [CrossRef] [PubMed]
- Gaillard, E.A.; Kuehni, C.E.; Turner, S.; Goutaki, M.; Holden, K.A.; de Jong, C.C.M.; Lex, C.; Lo, D.K.H.; Lucas, J.S.; Midulla, F.; et al. European Respiratory Society clinical practice guidelines for the diagnosis of asthma in children aged 5-16 years. Eur. Respir. J. 2021, 58, 2004173. [Google Scholar] [CrossRef] [PubMed]
- Elenius, V.; Chawes, B.; Malmberg, P.L.; Adamiec, A.; Ruszczyński, M.; Feleszko, W.; Jartti, T. Lung function testing and inflammation markers for wheezing preschool children: A systematic review for the EAACI Clinical Practice Recommendations on Diagnostics of Preschool Wheeze. EAACI Preschool Wheeze Task Force for Diagnostics of Preschool Wheeze. Pediatr. Allergy Immunol. 2021, 32, 501–513. [Google Scholar] [CrossRef] [PubMed]
- Robinson, D.; Latzin, P.; Verbanck, S.; Hall, G.H.; Horsley, A.; Gappa, M.; Thamrin, C.; Arets, H.G.M.; Aurora, P.; I. Fuchs, S.I.; et al. Consensus statement for inert gas washout measurement using multiple- and singlebreath tests. Eur. Respir. J. 2013, 41, 507–522. [Google Scholar] [CrossRef]
- Hedlin, G. , Eber, E.; Aurora, P.; Lødrup Carlsen, K.C.L.; Ratjen, F.; Dankert-Roelsee, J.E.; Ross-Russell,R.I.; Turner, S.; F. Midulla, F.; Baraldi, E.; et al. Paediatric respiratory disease: past, present and future. Paediatric Assembly contribution to the celebration of 20 years of the ERS. Eur. Respir. J. 2010, 36, 225–228. [Google Scholar] [CrossRef]
- Stanojevic, S.; Kaminsky, D.A.; Miller, M.R.; Thompson, B.; Aliverti, A; Barjaktarevic, I.; Cooper, B.G.; Culver, B.; Derom, E.; Hall, G.L.; et al. ERS/ATS technical standard on interpretive strategies for routine lung function tests. Eur. Respir. J. 2022, 60: 2101499.
- Merkus, P.J.F.M.; Stocks, J.; Beydon, N.; Lombardi, E.; Jones, M.; McKenzie, S.A.; Kivastik, J.; Arets, B.G.M.; Stanojevic, S. Reference ranges for interrupter resistance technique: the Asthma UK Initiative. Eur. Respir. J. 2010, 36, 157–163. [Google Scholar] [CrossRef]
- Calogero, C.; Simpson, S.J.; Lombardi, E.; Parri, N.; Cuomo, B.; Palumbo, M.; Maurizio de Martino, M.; Shackleton, C.; Verheggen, M.; Tania Gavidia MIH, T.; et al. Respiratory impedance and bronchodilator responsiveness in healthy children aged 2–13 years. Pediatr. Pulmonol. 2013, 48, 707–715. [Google Scholar] [CrossRef]
- Kirkby, J.; Stanojevic, S.; Welsh, L.; Lum, S.; Badier, M.; Beardsmore,C.; Custovic, A.; Nielsen, K.; Paton, J.; Tomalak, W.; et al. Reference equations for specific airway resistance in children: the Asthma UK initiative. Eur. Respir. J. 2010 36, 622–629. [CrossRef]
- Ramsey, K.A.; Stanojevic, S.; Chavez, L.; Johnson, N.; Bowerman, C.; Hall, G.L.; Latzin, P.; O’Neill, K.; Robinson, P.D.; Stahl. , M.; et al. on behalf of the contributing GLI MBW task force members. Global Lung Function Initiative reference values for multiple breath washout indices. Eur. Respir. J. 2024, 64, 2400524. [Google Scholar] [CrossRef]
- Pellegrino, R.; Viegi, G.; Brusasco, V.; Crapo, R.O.; Burgos, F.; Casaburi, R.; Coates, A.; van der Grinten, C.P.M.; Gustafsson, P.; Hankinson, J.; et al. Interpretative strategies for lung function tests. Eur. Respir. J. 2005, 26, 948–968. [Google Scholar] [CrossRef]
- Zar, H.J.; Ferkol, T.W. The global burden of respiratory disease-impact on child health. Pediatr. Pulmonol. 2014, 49, 430–434. [Google Scholar] [CrossRef]
- Martin, J.; Townshend, J.; Brodlie, M. Diagnosis and management of asthma in children. BMJ Paediatrics Open 2022, 6, e001277. [Google Scholar] [CrossRef] [PubMed]
- https://ginasthma.org/wp-content/uploads/2024/05/GINA-2024-Strategy-Report-24_05_22_WMS.pdf.
- Hyatt, R.E. Forced expiration. In: Macklem PT, Mead J (eds). Handbook of Physiology. Section 3, vol. III, part 1. The respiratory system. Mechan ics of breathing. American Physio logical Society, Bethesda 1986; 295-314.
- Perrem, L.; Wilson, D.; Dell, S.D.; and Ratjen, F. Development and Validation of an Algorithm for Quality Grading of Pediatric Spirometry: A Quality Improvement Initiative. Ann. Am. Thorac. Soc. 2022, 19, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Gochicoa-Rangel, L.; Vargas, C.; García-Mujica, M.; Bautista-Bernal, A.; Salas-Escamilla, I.; Perez Padilla, R.; Torre-Bouscoulet, L. Quality of Spirometry in 5-to-8-Year-Old Children. Pediatr. Pulmonol. 2013, 48, 1231–1236. [Google Scholar] [CrossRef]
- van der Plas, K.; P Vooren, P. The "opening" interruptor. A new variant of a technique for measuring respiratory resistance. Eur. J. Respir. Dis. 1982, 63, 449–548. [Google Scholar]
- Bates, J.H.; Baconnier, P.; Milic-Emili, J. A theoretical analysis of interrupter technique for measuring respiratory mechanics. J. Appl. Physiol. 1988, 64, 2204–2214. [Google Scholar] [CrossRef]
- Chan, E.Y.; Bridge, P.D.; Dundas, I.; Pao, C.S.; Healy, M.I.R.; McKenzie, S.A. Repeatability of airway resistance measurements made using the interrupter technique Thorax 2003, 58, 344–347. [CrossRef]
- Peslin, R.; Fredberg, J.J. Oscillation Mechanics of the Respiratory System. Supplement 12. Handbook of Physiology, The Respiratory System, Mechanics of Breathing, 2011. [CrossRef]
- Oostveen, E.; MacLeod, D.; Lorino, H.; Farré, R.; Hantos, Z.; Desager, K.; Marchal, F.; ERS Task Force on Respiratory Impedance Measurements-. The forced oscillation technique in clinical practice: methodology, recommendations and future developments. Eur. Respir. J. 2003, 22, 1026–1241. [Google Scholar] [CrossRef]
- King, G.G.; Bates, J.; Berger, K.I.; Calverley, P.; de Melo, P.L.; Dellacà, R.L.; Farré, R.; Hall, G.L.; Ioan, I.; Irvin, C.G.; et. al. Technical standards for respiratory oscillometry. Eur. Respir. J. 2020, 55, 1900753. [Google Scholar] [CrossRef]
- Goldman, M.G. Clinical application of forced oscillation. Pulm. Pharmacol. Ther. 2001, 14, 341–350. [Google Scholar] [CrossRef]
- Ducharme, F.M.; Davis, G.M.; Ducharme, G.R. Pediatric reference values for respiratory resistance measured by forced oscillation. Chest 1998, 113, 1322–1328. [Google Scholar] [CrossRef]
- Calogero, C.; Simpson, S.J.; Lombardi, E.; Parri, N.; Cuomo, B.; Palumbo, M.; de Martino, M.; Shackleton, C.; Verheggen, M.; Gavidia, T.; et al. Respiratory impedance and bronchodilator responsiveness in healthy children aged 2–13 years. Pediatr. Pulmonol. 2013, 48, 707–715. [Google Scholar] [CrossRef]
- Verbanck, S.; Schuermans, D.; Van Muylem, A.; Paiva, M.; Noppen, M.; Vincken, W. Ventilation distribution during histamine provocation. J. Appl. Physiol. 1997, 83, 1907–1916. [Google Scholar] [CrossRef] [PubMed]
- Downie, S.R.; Salome, C.M.; Verbanck, S.; Thompson, B.; Berend, N.; King, G.G. Ventilation heterogeneity is a major determinant of airway hyperresponsiveness in asthma, independent of airway inflammation. Thorax 2007, 62, 684–689. [Google Scholar] [CrossRef] [PubMed]
- Jensen, R.; Stanojevic, S.; Klingel, M.; Pizarro, M.E.; Hall, G.L.; Ramsey, K.; Foong, R.; Saunders, C.; Robinson, P.D.; Webster, H.; et al. A Systematic Approach to Multiple Breath Nitrogen Washout Test Quality. PLoS ONE 2016, 11, e0157523. [Google Scholar] [CrossRef]
- Venegas, J.G.; Winkler, T.; Musch, G; Vidal Melo, M. F.; Layfield, D.; Tgavalekos, N.; Fischman, A.J.; Callahan, R.J.; Bellani, G.; Harris, R.S. Self-organized patchiness in asthma as a prelude to catastrophic shifts. Nature 2005, 434, 777–782. [Google Scholar] [CrossRef]
- Winkler, T.; Venegas, J.G. Complex airway behavior and paradoxical responses to bronchoprovocation. J. Appl. Physiol. 2007, 103, 655–663. [Google Scholar] [CrossRef]
- Tgavalekos, N.T.; Venegas, J.G.; Suki, B.; Lutchen, K.R. Relation between structure, function, and imaging in a three-dimensional model of the lung. Ann. Biomed. Eng. 2003, 31, 363–373. [Google Scholar] [CrossRef]
- Rutting, S.; Chapman, D.G.; Farah, C.S.; Thamrin, C. Lung heterogeneity as a predictor for disease severity and response to therapy. Current Opinion in Physiology 2021, 22.
- Antonelli, A.; Crimi, E.; Gobbi, A.; Torchio, R.; Gulotta, C.; Dellaca, R.; Scano, G.; Brusasco, V.; Pellegrino, R. Mechanical correlates of dyspnea in bronchial asthma. Physiol. Rep. 2013, 1, e00166. [Google Scholar] [CrossRef]
- Pellegrino, R.; Wilson, O.; Jenouri, G.; Rodarte, J.R. Lung mechanics during induced bronchoconstriction. J. Appl. Physiol. 1996, 81, 964–975. [Google Scholar] [CrossRef]
- Salome, C.M.; Thorpe, C.W.; Diba, C.; Brown, N.J.; Berend, N.; King, G.G. Airway re-narrowing following deep inspiration in asthmatic and nonasthmatic subjects. Eur. Respir. J. 2003, 22, 62–68. [Google Scholar] [CrossRef]
- Brusasco, V; Pellegrino, R. Complexity of factors modulating airway narrowing in vivo: relevance to assessment of airway hyperresponsiveness. J. Appl. Physiol. 2003, 95, 4305–4313. [Google Scholar] [CrossRef]
- Que, C.L.; Kenyon, C.M.; Olivenstein, R.; Macklem, P.T.; Maksym, G.N. Homeokinesis and short-term variability of human airway caliber. J. Appl. Physiol. 2001, 91: 1131-1141. [CrossRef]
- Gulotta, C.; Suki, B.; Brusasco, V.; Pellegrino, R.; Gobbi, A.; Pedotti, A.; Dellacà, R.L. Monitoring the Temporal Changes of Respiratory Resistance: A Novel Test for the Management of Asthma. Am. J. Respir. Crit. Care Med. 2012, 185, 1330–1331. [Google Scholar] [CrossRef] [PubMed]
- Gobbi, A.; Gulotta, C.; Suki, B.; Mellano, E.; Pellegrino, R.; Brusasco, V.; Dellacà, R.L. Monitoring of respiratory resistance in the diagnosis of mild intermittent asthma Clin. Exper. Allergy. 2019, 49, 921–923. [Google Scholar] [CrossRef]
Figure 1.
Two typical examples of changes in inspiratory resistance and reactance at 8 Hz (R8 and X8) in two children exposed to methacholine challenge. Dose of the constrictor agent is reported in the horizontal axis. In panel A the decrease in X8 is remarkably less than the increase in R8 whereas the opposite is true for the case shown in panel B. The latter is consistent with large ventilation heterogeneities occurring with airway narrow-ing.
Figure 1.
Two typical examples of changes in inspiratory resistance and reactance at 8 Hz (R8 and X8) in two children exposed to methacholine challenge. Dose of the constrictor agent is reported in the horizontal axis. In panel A the decrease in X8 is remarkably less than the increase in R8 whereas the opposite is true for the case shown in panel B. The latter is consistent with large ventilation heterogeneities occurring with airway narrow-ing.
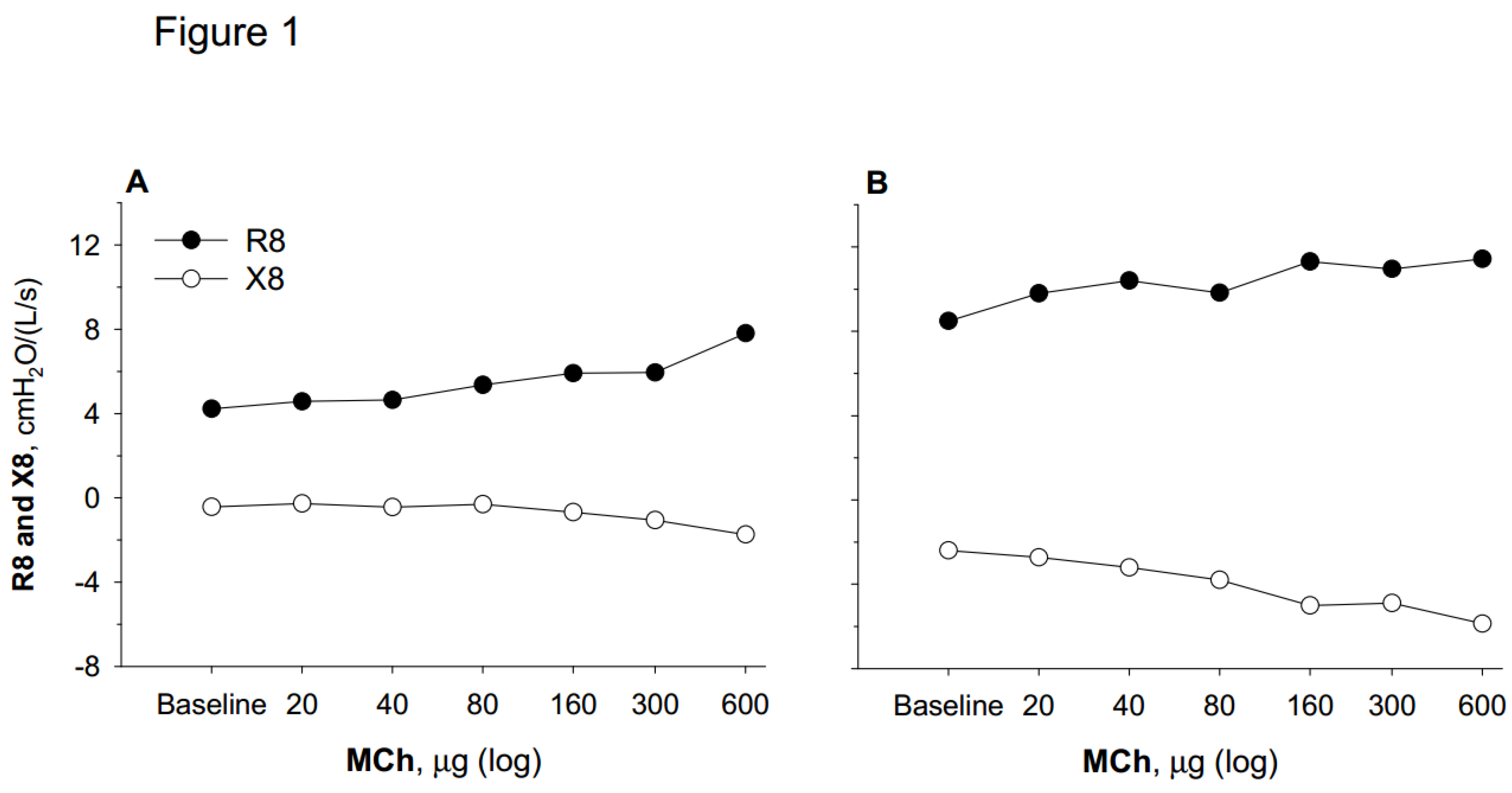
Figure 2.
Panel A: Respiratory impedance (Z) and its resistive (R) and reactance components (X) at 8 Hz during tidal inspiration (Rinsp and Xinsp, respectively) and expiration (Rexp and Xexp, respectively) at baseline conditions. Lower and upper limits of normality for R and X are shown by horizontal continuous and dashed lines, respectively. Panel B: Rinsp and Xinsp on tidal inspiration (Risnp and Xinsp, respectively) and expiration (Rexp and Xexpp, respectively) at the time of inspiratory dypsnea appearance during the bronchial challenge. Note the remarkable increase in Rinsp and decrease in Xinsp well beyond their relevant limits of normality in stark contrast with Rexp and Xexp. Panel C: Laryngologic evaluation: Normally abducted vocal folds (left); vocal cords during phonation (mid); paradoxical adduction during inspiration (right).
Figure 2.
Panel A: Respiratory impedance (Z) and its resistive (R) and reactance components (X) at 8 Hz during tidal inspiration (Rinsp and Xinsp, respectively) and expiration (Rexp and Xexp, respectively) at baseline conditions. Lower and upper limits of normality for R and X are shown by horizontal continuous and dashed lines, respectively. Panel B: Rinsp and Xinsp on tidal inspiration (Risnp and Xinsp, respectively) and expiration (Rexp and Xexpp, respectively) at the time of inspiratory dypsnea appearance during the bronchial challenge. Note the remarkable increase in Rinsp and decrease in Xinsp well beyond their relevant limits of normality in stark contrast with Rexp and Xexp. Panel C: Laryngologic evaluation: Normally abducted vocal folds (left); vocal cords during phonation (mid); paradoxical adduction during inspiration (right).
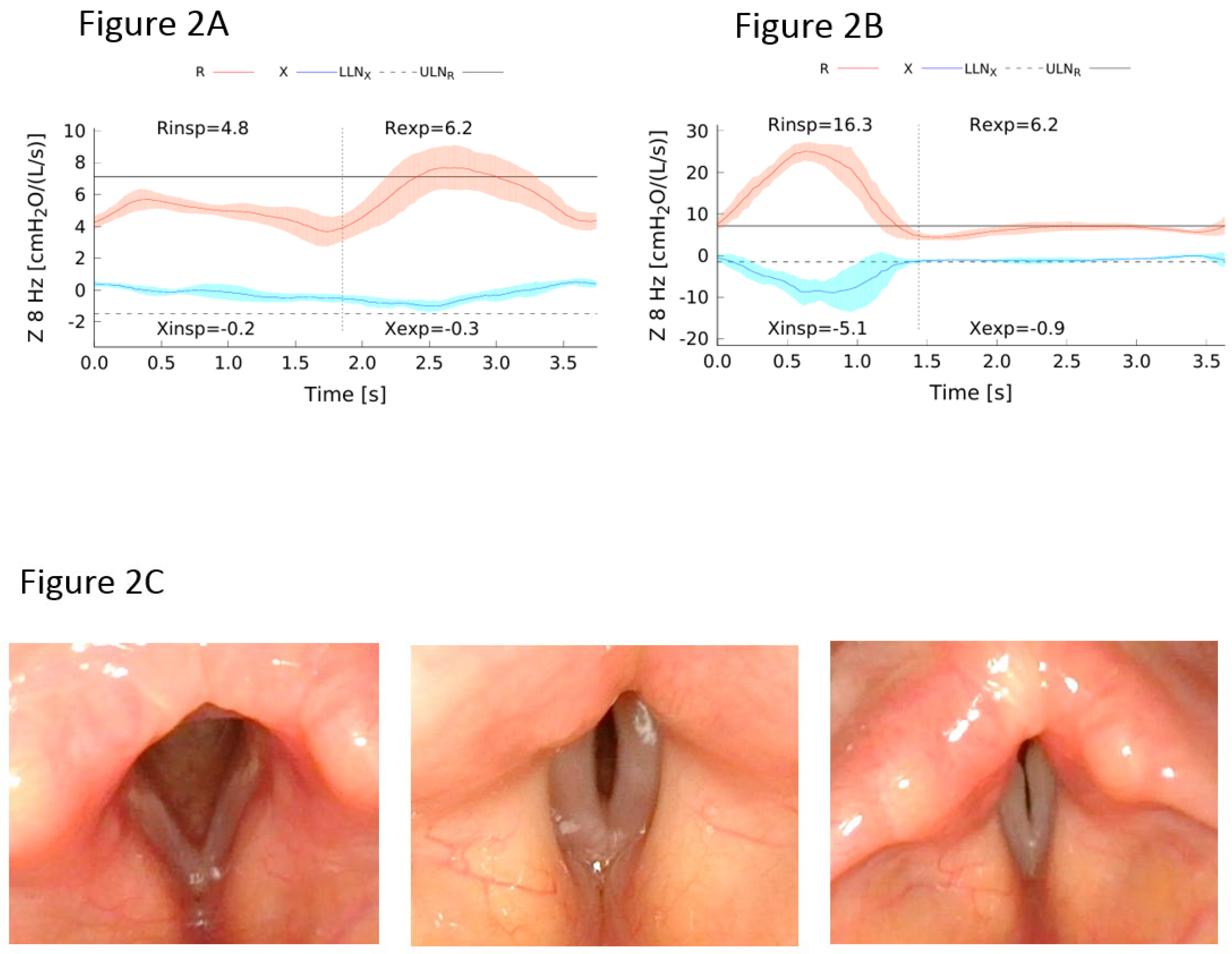
Figure 3.
Coefficient of variation of inspiratory resistance (CVRinsp) at 8 Hz measured in the morning for 32 days in an 8 year old boy. Note a slight initial increase of the CV that well exceeded the expected threshold of 0.10 after about a couple of weeks. This was associated with dyspnea and wheezing. Note the gradual return of CV to normal values after treatment with a combination of inhaled steroid and bronchodilator agent for 1 week.
Figure 3.
Coefficient of variation of inspiratory resistance (CVRinsp) at 8 Hz measured in the morning for 32 days in an 8 year old boy. Note a slight initial increase of the CV that well exceeded the expected threshold of 0.10 after about a couple of weeks. This was associated with dyspnea and wheezing. Note the gradual return of CV to normal values after treatment with a combination of inhaled steroid and bronchodilator agent for 1 week.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



