
Submitted:
19 May 2025
Posted:
19 May 2025
You are already at the latest version
Abstract
Obesity in the pediatric population is a serious public health challenge of this era. Its prevalence has continued to rise throughout the globe and various immediate and long-term consequences of obesity have been observed in children and adolescents. Childhood obesity stays in adulthood and children are prone to develop chronic conditions such as type 2 diabetes mellitus and cardiovascular diseases at an early age which were known to be the diseases of adults in the past. Obesity in childhood has a major impact on the physical and psychological health of a child, therefore, primary prevention is essential in controlling the incidence of obesity in children. This review article will highlight the prevalence, causes, and consequences of childhood obesity and its prevention.
Keywords:
obesity
; overweight
; childhood
; children
; diabetes mellitus
; cardiovascular
Introduction
Definition
World Health Organization (WHO) defines obesity and overweight as excessive accumulation of fat on the body that may impair the health of the individual. Age needs to be considered when classifying overweight and obesity in a child.
According to WHO June 2021 study report, overweight under 5 years is a weight for height more than 2 standard deviations, and obesity is a weight for height greater than 3 standard deviations above the WHO child growth standard median while overweight and obesity between 5 to 19 years are BMI for age more than 1 and 2 standard deviations above the WHO growth reference median, respectively.
Prevalence
Childhood obesity is growing globally both in developed and developing countries [4,5]. The prevalence of obesity almost tripled between 1975 to 2016 in the whole world. Over 60% of overweight children before puberty will be obese in adulthood [6].
Globally 42 million children less than five years are overweight of which 35 million children belong to developing nations according to 2010 global data [5]. Whom 2020 report has shown that 39 million children under the age of five years and 340 million children between the ages of 5 and 19 years in 2016 were obese or overweight.
One out of 3 children is overweight or obese in the World Health Organization (WHO) European region [6]. 2016 data revealed that the European nation has a high prevalence of overweight (30%) and obesity (>10%) in children [7]. Several other nations have seen a rising trend in childhood obesity. For instance, the proportion of overweight or obese children in Israel increased from 5.8% in 1975 to 11.9% in 2016 [7]. In Canada, the proportion of obesity in children remained high with about 25% of children between 4-11 years old and 33% of 12-17 years old classified as overweight or obese [8,9].
According to the Centers for Disease Control and Prevention's (CDC) January 2023 report, childhood obesity has continued to grow over the past 15 years, rising from 17% to 20%, and from 1980, the rate has tripled in children and quadrupled in adolescents. Obesity affects around 15 million children and teens in the United States and CDC data reveals that the rate of gaining weight doubled during the pandemic years of COVID-19 in comparison to pre-pandemic years. The prevalence of obesity in children in the USA [10], Europe [11,12], and Asia [13] is shown in Figure 1, Figure 2 and Figure 3, respectively.
Factors Contributing to Childhood Obesity
Multiple factors are involved in childhood obesity. Energy imbalance between calorie consumption and calorie expenditure is the fundamental cause of weight gain and obesity in children. There has been an increased intake of fat and sugar-containing foods and a sedentary lifestyle throughout the world. There are multiple causes of obesity in children and energy imbalance is one of the various factors [14]. Sometimes in children, there is a discrepancy between energy consumption and expenditure, however, accumulation of excessive fat occurs in children in their early formative years when the energy utilization is less than the caloric intake. Obesity is the complicated interaction of biological, developmental, behavioral, genetic, and environmental factors [15].
Studies revealed that AGOUTI-RELATED PROTEIN (AGRP) which is a mammalian signaling molecule, associated with weight homeostasis, causes adult-onset obesity when overexpressed. It has been identified as a competitive antagonist of melanocortin receptors 3 and 4 (MC3r, MC4r), while MC4r is involved in the hypothalamic control of feeding behavior Figure 4 [16].
Genetic factors: Maternal body mass index (BMI) before pregnancy is the independent risk factor for childhood obesity [17]. When both parents are obese there are increased chances of a child becoming obese [10]. Genetics is one of the big risk factors for childhood obesity. Research reveals that BMI is 25-40% inheritable [18]. Nevertheless, environmental, and behavioral factors coupled with genetics affect weight.
Genetic causes are divided into monogenic and polygenic types. Monogenic obesity is rare and due to mutations in genes in the leptin/melanocortin pathway in the hypothalamus which is crucial for the regulation of food consumption/ fullness, body weight, and metabolism of energy [19]. Leptin modulates eating behaviors, puberty onset, and T-cell immunity. Almost 3% of overweight children have a mutation in leptin and leptin receptors and present with pubertal delay and immune dysregulation [20]. Monogenic type presents with obesity and abnormal eating behaviors in children by 2 years of age [21]. Genetic syndromes associated with obesity in children are Prader-Willi Syndrome (PWS), Bardet-Biedl syndrome, and Alstrom syndrome [22]. Other syndromes are Beckwith-Weideman syndrome and Cohen syndrome. Over 25 syndromic forms of obesity have been identified, and the most common is PWS [23].
Polygenic obesity, a more common form of obesity is the result of gene-environment interaction (GEI) [24]. Variations in genes in obese individuals affect their actions such as their food eating pattern, absence of physical activity, decreased metabolism, and increased predisposition to store body fat [25,26].
New studies reveal epigenetic factors play a role in developing obesity [27]. Maternal nutrition antenatally or in the early postnatal period stimulates these epigenetic changes and increases the risk of long-term diseases i.e., obesity [28].
Endocrine factors: Less than 1 percent of cases of obesity in children are caused by endocrine factors [29]. A child with the underlying endocrine issue presents with mild to moderate obesity, short stature, and hypogonadism. Growth hormone deficiency, hypothyroidism, pseudohypoparathyroidism, precocious puberty, leptin deficiency or resistance to leptin action, prolactin-secreting tumors, polycystic ovary syndrome, and Cushing syndrome are some examples of hormonal conditions associated with obesity.
Lifestyle and dietary practices: A child's eating behavior evolves in the early formative years; they observe their elders and surroundings to develop their eating style [30]. Due to a busy life schedule, parents often present ready-made food to children that is processed and high in calories as shown in Figure 6. Giving formula feeding instead of breastfeeding to the infant, and early introduction of proteins in the infant's diet are reported as contributing factors in weight gain that can persist later in life [31,32]. Moreover, children are encouraged to clean their large meal plates and these practices are seen across various cultures [33]. In daycare or schools, children are exposed to a variety of food options, and they have more independence to eat different foods. Furthermore, limited physical activities at daycare and in schools are also contributing
factors in gaining weight [34] Teenagers have more independence toward calorie-dense foods. Less pricy junk food, their easy availability, and extensive advertisements for different brands of junk food promote high-caloric food in public which is the biggest contributor to obesity [35]. In the United States of America, the price of McDonald's and Coca-Cola decreased (5.44% and 34.89% respectively) from 1990 to 2007 whereas a 17% increase occurred in the cost of fruits and veggies between 1997 to 2003 [36]. In addition to this, playing video games, and sitting in front of the screens for a longer time limit physical activities and impact the mental health in the pubertal age group [37]. Adolescence is the period when they are more anxious about their appearance, and weight and they have other mental health concerns [38]. Hence, a sedentary lifestyle, lack of physical activity, and unhealthy eating behavior i.e., drinking soda/ sweet beverages, and frequent snacking with increased portion size results in high energy consumption and leads to increased incidence of obesity [39,40,41].
Sleep and obesity: Sleep patterns affect the weight of the child [42]. Studies show that 45% of children who get less sleep (<10.5 hours) at age 3 are more prone to obesity at the age of 7 than those children who sleep more than 12 hours at the same age [43,44]. Technology disrupts the sleep and eating patterns in children [45]. The use of electronic devices while in bed decreases the total sleep time, resulting in less physical activity during the daytime which increases weight [46].
Psychological factors: Obesity in the pediatric age group leads to disordered eating behaviors. High body dissatisfaction and low self-esteem may be the contributing factors for both eating disorders and obesity [47]. Early diagnosis of eating disorders such as anorexia nervosa, bulimia nervosa, and binge eating disorders may prevent obesity or help in weight loss in sustained obesity in adolescents [48]. Eating disorders may accompany obesity or they may emerge after getting treatment for obesity in children or adolescents [49]. Binge eating is associated with comorbid obesity followed by bulimia nervosa and around 30% of females with eating disorders had chronic obesity [50]. When emotional dysregulation occurs, it stimulates binge eating episodes which in turn leads to shame and guilt and creates a vicious cycle of losing control of eating [51]. Several socioeconomic factors are considered common risk factors to develop eating disorders and obesity such as frequent criticism, bullying, family/peer, and social pressure [52]. Furthermore, families with binge eating behaviors, parental separation, high parental demands, traumatic life events, and negative experiences in childhood such as physical and sexual abuse, all these are identified as risk factors for eating disorders and obesity [53].
Medications and toxins: Certain medications can cause weight gain and obesity. For example, antidepressants, glucocorticoids, progestins, propranolol, alpha-blockers (terazosin), and insulin. Bisphenol A and dichlorodiphenyltrichloroethane are endocrine-disrupting toxins, and these chemicals can lead to obesity by disrupting the estrogen receptors and metabolic programming [54].
Consequences of Obesity
Obesity profoundly affects children’s physical health and social, and emotional well-being. The majority of them develop low self-esteem, poor academic performance, and lower quality of life.
Chronic diseases: There are various chronic ailments that a child might develop because of obesity. Increased BMI before the age of 5 years is a risk factor for developing obesity in adulthood, obesity-related co-morbidities, and metabolic syndrome [55,56] as demonstrated in Figure 5.
Chronic health conditions related to childhood obesity are cardiovascular conditions such as hypertension, dyslipidemia, coronary artery disease, metabolic issues, for instance, pre-diabetes, type 2 diabetes, hormonal problems i.e., polycystic ovarian syndrome (PCOs), other morbidities are fatty liver disease, early puberty, orthopedic issues i.e., slipped capital femoral epiphysis (SCFE), asthma, sleep apnea, impaired balance [57] and idiopathic intracranial hypertension [58].
Diabetes: Childhood obesity quadruples the risk of developing glucose intolerance and diabetes type 2. Almost 85% of children at the time of diagnosis of non-insulin-dependent diabetes (NIDDM) are either overweight or obese [59] Type 2 diabetes in children presents with aggressive disease and with high treatment failure rates. Children with diabetes may develop co-morbidities and complications early such as fatty liver, nephropathy, dyslipidemia, and polycystic ovarian syndrome, particularly in females [60,61]. In clinical settings, obese children are usually screened for Type 2 diabetes [62].
Hypertension: Obesity is a major risk factor for hypertension in the pediatric population. Around 25% of children with obesity can develop hypertension. The mechanism of developing hypertension in childhood obesity is complex; however, several factors have been recognized such as renin angiotensin aldosterone activation, the activity of the sympathetic nervous system (SNS), disturbed sodium hemostasis, oxidative stress, and dysfunction of the endothelial system. Leptin, resistin, and Interleukin-6, the pro-inflammatory adipokines stimulate the SNS which in turn affects the renal vascular bed [63]. Additionally, hyperinsulinemia increases renal sodium retention, and intracellular calcium and stimulates the SNS [64] which causes high blood pressure.
Hepatic Steatosis: Non-alcoholic fatty liver disease (NAFLD) is an important cause of liver disease in obese children. Clinicians should screen obese children for fatty liver with alanine transaminase (ALT) and ultrasonography. NAFLD is associated with liver fat (steatosis) and with liver inflammation and hepatic injury (NASH- non-alcoholic steatohepatitis) [65]. NAFLD is related to central obesity, insulin resistance, type 2 diabetes, dyslipidemia, and hypertension which are linked to metabolic syndrome [66]. Progression to an end-stage liver disease requiring a liver transplant due to NAFLD is less well-defined in the pediatric population [67] while some studies reveal end-stage liver disease is 14 times more common in children with NAFLD than non-NAFLD.
Gallstones: There are pigment gallstones which are associated with chronic hemolysis and cholesterol gallstones that are linked to environmental and genetic factors and mixed stones. Cholesterol stones account for 70% of overall gallstones. Obese girls are more prone to develop cholelithiasis compared to boys and it is more common during the weight reduction process. Increased synthesis of cholesterol and cholesterol saturation of bile is the cause of gallstone production among obese adolescents [68]. Pediatricians should consult a pediatric gastroenterologist when an overweight child has mysterious stomach ache and or is jaundiced.
Sleep disorders: Children and adolescents with obesity and overweight are at risk of developing obstructive sleep apnea (OSA) [69]. Neurocognitive dysfunction, abnormal behaviors, and increased daytime sleepiness are common in children with OSA [70]. Oxidative systemic stress and inflammation can be caused by OSA in adolescents [71] However, cardiovascular complications are less common in children with OSA compared to adolescents and adults [72,73].
Metabolic syndrome: There is no clear-cut definition of metabolic syndrome in children, however, it is characterized by cardiovascular risk factors such as acanthosis nigricans, dyslipidemia, hypertension, pre-diabetes, and NASH which is caused by insulin resistance due to obesity [74]. Hyperinsulinism [75], poor sleep behaviors, and low vitamin D levels increase the risk of metabolic syndrome. Regular screening and intervention of complications associated with metabolic syndrome in an obese child is vital to save the future of a child’s health.
Asthma: Some studies reveal that asthma and its exacerbations have been found more prevalent and severe in obese and overweight children. Asthma in an obese child is mildly less responsive to inhaled corticosteroids compared to non-obese children. Asthma and childhood obesity are mediated by abnormal obesity-related systemic inflammatory and oxidative stress, airway narrowing, reduced lung volumes, chest restriction, obstructive sleep apnea, and gastroesophageal reflux [76].
Menstrual irregularities and polycystic ovarian syndrome: Obesity in adolescent females puts them at risk of developing irregular menstrual cycles and polycystic ovarian syndrome due to hyperinsulinism and hyperandrogenism. They can have hirsutism, polycystic ovaries, insulin resistance, and distorted body image [77] and they may develop type 2 diabetes and metabolic syndrome.
Growth and puberty: Obesity can affect growth and puberty in children. Excessive weight gain accelerates the linear growth velocity in prepubertal children and advances bone age [78]. Insulin levels can be abnormally high in obese children and leptin resistance can occur in children where higher leptin levels are produced by adipose tissues. Insulin, leptin, and sex hormones impact the maturation of growth plates resulting in advancement in bone age [78,79]. Early puberty can be initiated in overweight children due to hormonal disturbances. They may present with thelarche, adrenarche, and precocious puberty [80]. Research reveals that early pubertal changes are mostly in girls whereas obese boys show delayed puberty and overweight boys may present with early puberty [81]. Premature adrenarche in girls is a risk factor for developing polycystic ovarian syndrome later in life [82]. Moreover, rapid weight gain during infancy is a risk factor for childhood adiposity and early menarche in girls [83]. Obese children are tall and mature early as compared to lean children, but their growth velocity is relatively less in their teen years in comparison to normal-weight adolescents [84].
Social and emotional impacts: Likewise medical concerns, there are emotional and social impacts on children with obesity. Childhood obesity is considered one of the most stigmatizing and least acceptable conditions socially [85]. Obese children are often discriminated against, and they face challenges such as bullying and teasing by peers, negative stereotypes, and social exclusion [86,87]. They are often excluded from competitive physical activities as they tend to be slower than their peers. These negative experiences result in low self-confidence in children which affects their academic performance. Obese children have four times more problems at school and in their academic performances than their normal-weight peers, for instance, missing school more frequently [85].
Socially, obese children are less sociable as they have fewer friends as compared to normal-weight children. They seek places where they can eat comfortably and avoid negative comments, which results in forcing them to spend life in a sedentary way [88].
Similarly, obese adolescents may suffer from depression that results in social isolation, a sedentary lifestyle, and poor eating habits. Moreover, they face peer victimization/bullying and develop body image dissatisfaction, poor self-esteem, and difficult interpersonal relationships. Anxiety disorders and ADHD are associated with childhood and adolescent obesity [89]. They may have decreased resilience to challenging situations [90]. To control their weight and due to negative body image, obese adolescents engage themselves in eating disorders such as anorexia nervosa, binge eating disorders, night eating syndromes, and bulimia nervosa [91].
Persistence of obesity in adulthood: About 55% of obese children will be obese in adolescence almost 80% of adolescents will be obese in adulthood and around 70% will be obese above the age of 30. According to studies,15-30% of adults were obese in their childhood or adolescent period [92].
Preventive Strategies and Management of Childhood Obesity
Prevention is better than cure, this is true for pediatric obesity. The goal in fighting the obesity epidemic in children is to achieve a balance in energy that can be maintained throughout the individual’s life. The treatment of child obesity depends on its cause, and it usually includes lifestyle modifications.
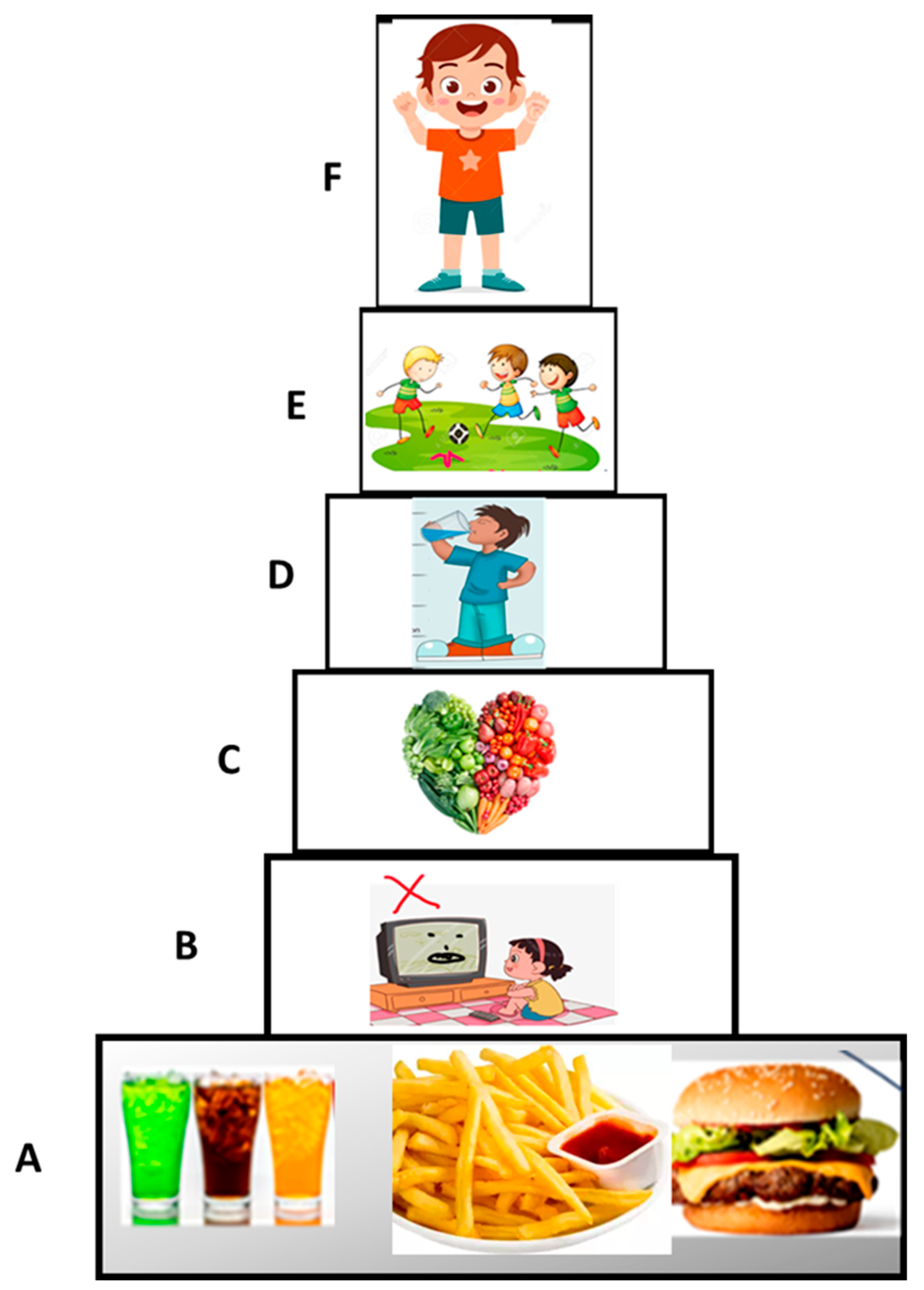
WHO Recommendations: WHO emphasizes largely preventive measures for pediatric obesity with supportive environments and communities that are crucial in shaping people’s choices i.e., choices of healthy food and daily physical activity of 60 minutes which is the most accessible, affordable, available, and easiest choice for children. WHO recommends the increased consumption of fruits, vegetables, legumes, and nuts and less energy intake from sugars and total fats as shown in Figure 6. The food industry can play an essential role in the promotion of a healthy diet e.g., reducing the sugar, salt, and fat content in processed food, restricting the marketing of food that is high in sugar, fat, and salt, particularly that food that is aimed at children and teens, the availability of healthy food choices at school or workplace.
Figure 6.
Prevention of Obesity in Children. A: no/less junk food B: less screen time C: eating more veggies/fruits D: plenty of fluids E: physical activities F: healthy child.
Figure 6.
Prevention of Obesity in Children. A: no/less junk food B: less screen time C: eating more veggies/fruits D: plenty of fluids E: physical activities F: healthy child.
Motivational Interview: Motivational interviewing techniques are useful to encourage positive behaviour change in adolescents and children with obesity because research reveals that language that healthcare providers use sometimes decreases the motivation for weight control which potentially causes the avoidance of preventive care [93] rather it results in binge eating, decrease physical activity, social isolation, avoidance of health care facilities and increased weight gain [94]. Effective provider-patient communication is essential to encourage positive behavior change [95].
Anticipatory guidance: Assisting parents or guardians by a healthcare provider to understand the expected growth and development of the child is anticipatory guidance. It also includes educating parents about healthy and unhealthy eating practices, the importance of physical activity, disadvantages of a sedentary lifestyle e.g., screen time as the lifestyle behavior of children is largely affected by societal factors including family practices [96]. Therefore, family-based multi-component weight loss behavioral treatment is the gold standard for the management of obesity in children, particularly children between 2 and 6 years old [91].
Structured weight management program: A multidisciplinary approach involving physicians, dieticians, and psychologists 1-2 times per week in the structured weight management of children and adolescents is the next step when lifestyle modifications have failed [97,98], however, it is not useful in severe obesity.
Pharmacological treatment: Pharmacological therapy in the management of children and adolescents is limited. However, the Food and Drug Administration (FDA) approved two anti-obesity medications for children and adolescents i.e. Orlistat and phentermine [99].
Orlistat is approved by the FDA for children >12 years of age for the long-term management of obesity. It was not approved for use by FDA in adolescents until 2003 [100]. The dose is 120mg three times a day with meals. The mechanism is the inhibition of pancreatic and gastric lipase, and it decreases the absorption of lipids. Side effects are unpleasant which limits its use i.e., gastric upset, abdominal pain, fecal urgency and incontinence, and fat-soluble vitamin deficiency [101]. Contraindications are malabsorption, pregnancy, and cholestasis [102].
Phentermineis the short-term 12 weeks or less, treatment of obesity in individuals more than 16 years of age. This drug is an amphetamine analog and is FDA-approved. The prescribed dose is 15 mg, 30mg, and 37.5mg daily [100]. Phentermine acts to enhance catecholamine and serotonin activity in the central nervous system which results in the suppression of appetite [100]. Common side effects are increased heart and blood pressure, gastrointestinal side effects, tremors, headaches, mood swings, and dry mouth [103]. Past or uncontrolled cardiovascular disease, glaucoma, hyperthyroidism, and the current use of monoamine oxidase inhibitors are a contraindication to the use of phentermine [104].
Off-label use of drugs such as metformin, exenatide, topiramate or zonisamide, octreotide, and growth hormone (GH) for obesity.
GH is used for the syndromic type of obesity i.e. PWS [105]. It reduces fat mass and increases lean body mass. Octreotide (somatostatin analog) is used for hypothalamic obesity for weight stabilization in adolescents [106] while Lis dexamphetamine which is used for attention deficit hyperactivity disorder (ADHD) is also used for binge eating and severe obesity in adolescents [107]. Metformin has been used in children with insulin resistance and may have some effect on weight, but it is not FDA-approved for obesity in children.
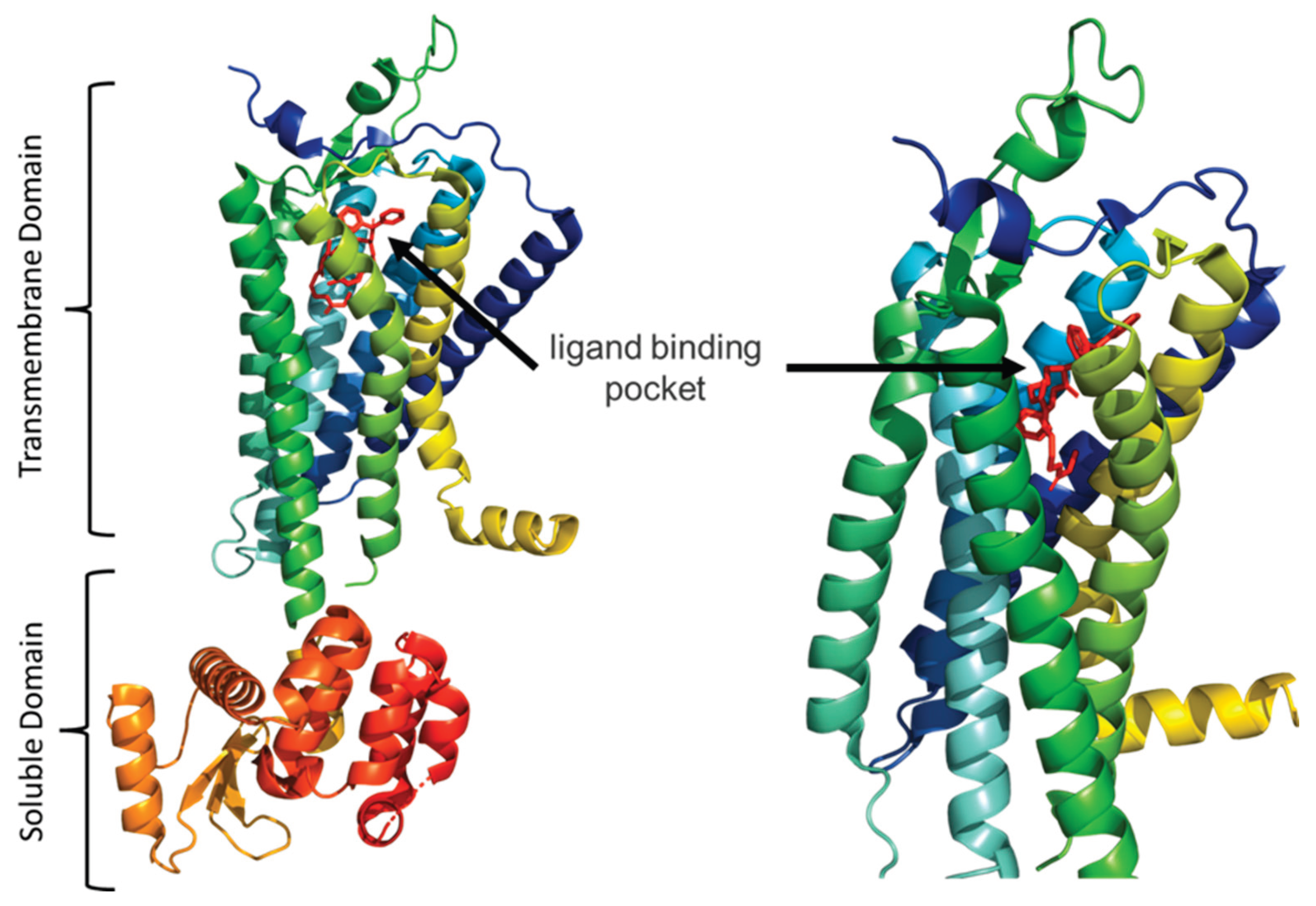
Neuropeptide Y (NPY) is highly abundant in the central nervous system and its receptor belongs to the group of G-protein-coupled receptor superfamily and has crucial roles in food intake, anxiety, and cancer biology. The NPY receptor Y1R is expressed in a variety of tissues and involved in the regulation of many physiological functions, related to obesity and cancer [108] Figure 7.
Bariatric surgery: Indication of weight loss surgery is the age between 14 and 18 years and a body mass index (BMI) of 40 or more or 35 or more with a serious co-morbid condition of obesity such as diabetes type 2. Before considering surgery, patients need to participate in a structured weight-loss program for at least six months with a multidisciplinary team [109]. Roux-en-Y Gastric Bypass (RYGB), laparoscopic Sleeve Gastrectomy (LSG) is currently approved for children under 18 years of age. Gastric banding is not FDA-approved for adolescents. Research reveals weight loss surgery has less severe side effects in adolescents than in adults [110]. The lifetime outcome of surgery in teens is still unknown though five-year data on gastric bypass is promising, however, psychosocial impacts after getting surgery are also challenging and uncertain in adolescents [22].
Conclusions
Obesity in children and adolescents has been growing globally and is known to have a significant impact on physical and psychological health i.e., self-esteem and emotional well-being of children. Obesity is the result of several factors in children such as environmental factors, lifestyle, and cultural preferences play pivotal roles in the rising prevalence of obesity worldwide. In general, overweight and obesity are assumed to be the results of an increase in caloric and fat intake.
Lifestyle intervention is crucial for the prevention of obesity though it has modest effects in severe obesity in children. Parents need to adopt a healthier lifestyle and encourage children to eat more fruits and veggies, less junk food, less screen time, and increased physical activity. A combined dietary modification and physical activity intervention conducted in the community with a school component is more effective at preventing obesity or overweight in the pediatric population, in this way we may lead to a healthier society.
References
- K. M. Flegal, R. Wei, and C. Ogden, "Weight-for-stature compared with body mass index-for-age growth charts for the United States from the Centers for Disease Control and Prevention," Am J Clin Nutr, vol. 75, no. 4, pp. 761-6, Apr 2002. [CrossRef]
- J. H. Himes and W. H. Dietz, "Guidelines for overweight in adolescent preventive services: recommendations from an expert committee. The Expert Committee on Clinical Guidelines for Overweight in Adolescent Preventive Services," Am J Clin Nutr, vol. 59, no. 2, pp. 307-16, Feb 1994. [CrossRef]
- A. Ghosh, "Explaining overweight and obesity in children and adolescents of Asian Indian origin: the Calcutta childhood obesity study," Indian J Public Health, vol. 58, no. 2, pp. 125-8, Apr-Jun 2014. [CrossRef]
- B. M. Popkin and C. M. Doak, "The obesity epidemic is a worldwide phenomenon," Nutr Rev, vol. 56, no. 4 Pt 1, pp. 106-14, Apr 1998. [CrossRef]
- Sahoo, B. Sahoo, A. K. Choudhury, N. Y. Sofi, R. Kumar, and A. S. Bhadoria, "Childhood obesity: causes and consequences," J Family Med Prim Care, vol. 4, no. 2, pp. 187-92, Apr-Jun 2015. [CrossRef]
- G. Nittari, S. Scuri, F. Petrelli, I. Pirillo, N. M. di Luca, and I. Grappasonni, "Fighting obesity in children from European World Health Organization member states. Epidemiological data, medical-social aspects, and prevention programs," Clin Ter, vol. 170, no. 3, pp. e223-e230, May-Jun 2019. [CrossRef]
- S. Scuri, F. Petrelli, M. Tesauro, F. Carrozzo, L. Kracmarova, and I. Grappasonni, "Energy drink consumption: a survey in high school students and associated psychological effects," J Prev Med Hyg, vol. 59, no. 1, pp. E75-E79, Mar 2018. [CrossRef]
- G. D. C. Ball, A. Savu, and P. Kaul, "Changes in the prevalence of overweight, obesity, and severe obesity between 2010 and 2017 in preschoolers: A population-based study," Pediatr Obes, vol. 14, no. 11, p. e12561, Nov 2019. [CrossRef]
- D. P. Rao, E. Kropac, M. T. Do, K. C. Roberts, and G. C. Jayaraman, "Childhood overweight and obesity trends in Canada," Health Promot Chronic Dis Prev Can, vol. 36, no. 9, pp. 194-8, Sep 2016. Tendances en matiere d'embonpoint et d'obesite chez les enfants au Canada. [CrossRef]
- A. Sanyaolu, C. Okorie, X. Qi, J. Locke, and S. Rehman, "Childhood and Adolescent Obesity in the United States: A Public Health Concern," Glob Pediatr Health, vol. 6, p. 2333794X19891305, 2019. [CrossRef]
- O. World Health, "The double burden of malnutrition: policy brief," World Health Organization, Geneva, 2016 2016, issue CC BY-NC-SA 3.0 IGO. [Online]. Available: https://apps.who.int/iris/handle/10665/255413.
- U. W. W. Bank, " joint child malnutrition estimates," 2021 edition interactive dashboard. New York (NY): United Nations Children’s Fund;, report 2021. [Online]. Available: https://data.unicef.org/resources/joint-child-malnutrition-estimates-interactive-dashboard-2021.
- M. Mazidi, M. Banach, A. P. Kengne, Lipid, and G. Blood Pressure Meta-analysis Collaboration, "Prevalence of childhood and adolescent overweight and obesity in Asian countries: a systematic review and meta-analysis," Arch Med Sci, vol. 14, no. 6, pp. 1185-1203, Oct 2018. [CrossRef]
- C. Centers for Disease and Prevention, "CDC grand rounds: childhood obesity in the United States," MMWR Morb Mortal Wkly Rep, vol. 60, no. 2, pp. 42-6, Jan 21 2011. [Online]. Available: https://www.ncbi.nlm.nih.gov/pubmed/21248681.
- A. Qasim et al., "On the origin of obesity: identifying the biological, environmental and cultural drivers of genetic risk among human populations," Obes Rev, vol. 19, no. 2, pp. 121-149, Feb 2018. [CrossRef]
- K. A. Bolin et al., "NMR structure of a minimized human agouti related protein prepared by total chemical synthesis," FEBS Lett, vol. 451, no. 2, pp. 125-31, May 21 1999. [CrossRef]
- P. M. Catalano et al., "Perinatal risk factors for childhood obesity and metabolic dysregulation," Am J Clin Nutr, vol. 90, no. 5, pp. 1303-13, Nov 2009. [CrossRef]
- P. M. Anderson and K. E. Butcher, "Childhood obesity: trends and potential causes," Future Child, vol. 16, no. 1, pp. 19-45, Spring 2006. [CrossRef]
- S. A. Ranadive and C. Vaisse, "Lessons from extreme human obesity: monogenic disorders," Endocrinol Metab Clin North Am, vol. 37, no. 3, pp. 733-51, x, Sep 2008,. [CrossRef]
- S. Farooqi et al., "Clinical and molecular genetic spectrum of congenital deficiency of the leptin receptor," N Engl J Med, vol. 356, no. 3, pp. 237-47, Jan 18 2007. [CrossRef]
- H. Huvenne, B. Dubern, K. Clement, and C. Poitou, "Rare Genetic Forms of Obesity: Clinical Approach and Current Treatments in 2016," Obes Facts, vol. 9, no. 3, pp. 158-73, 2016. [CrossRef]
- A. R. Kansra, S. Lakkunarajah, and M. S. Jay, "Childhood and Adolescent Obesity: A Review," Front Pediatr, vol. 8, p. 581461, 2020. [CrossRef]
- E. Geets, M. E. C. Meuwissen, and W. Van Hul, "Clinical, molecular genetics and therapeutic aspects of syndromic obesity," Clin Genet, vol. 95, no. 1, pp. 23-40, Jan 2019. [CrossRef]
- Y. Heianza and L. Qi, "Gene-Diet Interaction and Precision Nutrition in Obesity," Int J Mol Sci, vol. 18, no. 4, Apr 7 2017. [CrossRef]
- M. Rask-Andersen, T. Karlsson, W. E. Ek, and A. Johansson, "Gene-environment interaction study for BMI reveals interactions between genetic factors and physical activity, alcohol consumption and socioeconomic status," PLoS Genet, vol. 13, no. 9, p. e1006977, Sep 2017. [CrossRef]
- A. Martinez, "Body-weight regulation: causes of obesity," Proc Nutr Soc, vol. 59, no. 3, pp. 337-45, Aug 2000. [CrossRef]
- X. Sun, P. Li, X. Yang, W. Li, X. Qiu, and S. Zhu, "From genetics and epigenetics to the future of precision treatment for obesity," Gastroenterol Rep (Oxf), vol. 5, no. 4, pp. 266-270, Nov 2017. [CrossRef]
- Y. Li, "Epigenetic Mechanisms Link Maternal Diets and Gut Microbiome to Obesity in the Offspring," Front Genet, vol. 9, p. 342, 2018. [CrossRef]
- T. Reinehr, A. Hinney, G. de Sousa, F. Austrup, J. Hebebrand, and W. Andler, "Definable somatic disorders in overweight children and adolescents," J Pediatr, vol. 150, no. 6, pp. 618-22, 622 e1-5, Jun 2007. [CrossRef]
- L. Birch and J. O. Fisher, "Development of eating behaviors among children and adolescents," Pediatrics, vol. 101, no. 3 Pt 2, pp. 539-49, Mar 1998. [Online]. Available: https://www.ncbi.nlm.nih.gov/pubmed/12224660.
- F. Indrio et al., "Epigenetic Matters: The Link between Early Nutrition, Microbiome, and Long-term Health Development," Front Pediatr, vol. 5, p. 178, 2017. [CrossRef]
- B. Koletzko et al., "Prevention of Childhood Obesity: A Position Paper of the Global Federation of International Societies of Paediatric Gastroenterology, Hepatology and Nutrition (FISPGHAN)," J Pediatr Gastroenterol Nutr, vol. 70, no. 5, pp. 702-710, May 2020. [CrossRef]
- S. J. Nielsen and B. M. Popkin, "Patterns and trends in food portion sizes, 1977-1998," JAMA, vol. 289, no. 4, pp. 450-3, Jan 22-29 2003. [CrossRef]
- Institute of Medicine (U.S.). Committee on Food Marketing and the Diets of Children and Youth., J. M. McGinnis, J. A. Gootman, and V. I. Kraak, Food marketing to children and youth : threat or opportunity? Washington, D.C.: National Academies Press, 2006, pp. xx, 516 p.
- R. Benjamin, "Surgeon General's prevention priorities dovetail with health care reform law. Interview by Rebecca Voelker," JAMA, vol. 303, no. 21, pp. 2123-4, Jun 2 2010. [CrossRef]
- S. L. Friedlander, E. K. Larkin, C. L. Rosen, T. M. Palermo, and S. Redline, "Decreased quality of life associated with obesity in school-aged children," Arch Pediatr Adolesc Med, vol. 157, no. 12, pp. 1206-11, Dec 2003. [CrossRef]
- Liu, L. Wu, and S. Yao, "Dose-response association of screen time-based sedentary behaviour in children and adolescents and depression: a meta-analysis of observational studies," Br J Sports Med, vol. 50, no. 20, pp. 1252-1258, Oct 2016. [CrossRef]
- C. J. Lowe, J. B. Morton, and A. C. Reichelt, "Adolescent obesity and dietary decision making-a brain-health perspective," Lancet Child Adolesc Health, vol. 4, no. 5, pp. 388-396, May 2020. [CrossRef]
- F. L. Schiffino et al., "Activation of a lateral hypothalamic-ventral tegmental circuit gates motivation," PLoS One, vol. 14, no. 7, p. e0219522, 2019. [CrossRef]
- J. J. Reilly et al., "Early life risk factors for obesity in childhood: cohort study," BMJ, vol. 330, no. 7504, p. 1357, Jun 11 2005. [CrossRef]
- Di Cesare et al., "The epidemiological burden of obesity in childhood: a worldwide epidemic requiring urgent action," BMC Med, vol. 17, no. 1, p. 212, Nov 25 2019. [CrossRef]
- G. Lissak, "Adverse physiological and psychological effects of screen time on children and adolescents: Literature review and case study," Environ Res, vol. 164, pp. 149-157, Jul 2018. [CrossRef]
- D. A. Dev, B. A. McBride, B. H. Fiese, B. L. Jones, H. Cho, and T. Behalf Of The Strong Kids Research, "Risk factors for overweight/obesity in preschool children: an ecological approach," Child Obes, vol. 9, no. 5, pp. 399-408, Oct 2013. [CrossRef]
- B. Vos and J. Welsh, "Childhood obesity: update on predisposing factors and prevention strategies," Curr Gastroenterol Rep, vol. 12, no. 4, pp. 280-7, Aug 2010. [CrossRef]
- C. Fuller, E. Lehman, S. Hicks, and M. B. Novick, "Bedtime Use of Technology and Associated Sleep Problems in Children," Glob Pediatr Health, vol. 4, p. 2333794X17736972, 2017. [CrossRef]
- H. Chahal, C. Fung, S. Kuhle, and P. J. Veugelers, "Availability and night-time use of electronic entertainment and communication devices are associated with short sleep duration and obesity among Canadian children," Pediatr Obes, vol. 8, no. 1, pp. 42-51, Feb 2013. [CrossRef]
- A. B. Goldschmidt, V. P. Aspen, M. M. Sinton, M. Tanofsky-Kraff, and D. E. Wilfley, "Disordered eating attitudes and behaviors in overweight youth," Obesity (Silver Spring), vol. 16, no. 2, pp. 257-64, Feb 2008. [CrossRef]
- C. Horsager, E. Faerk, A. N. Gearhardt, M. B. Lauritsen, and S. D. Ostergaard, "Food addiction comorbid to mental disorders in adolescents: a nationwide survey and register-based study," Eat Weight Disord, vol. 27, no. 3, pp. 945-959, Apr 2022. [CrossRef]
- S. Stabouli, S. Erdine, L. Suurorg, A. Jankauskiene, and E. Lurbe, "Obesity and Eating Disorders in Children and Adolescents: The Bidirectional Link," Nutrients, vol. 13, no. 12, Nov 29 2021. [CrossRef]
- Z. Aguera, M. Lozano-Madrid, N. Mallorqui-Bague, S. Jimenez-Murcia, J. M. Menchon, and F. Fernandez-Aranda, "A review of binge eating disorder and obesity," Neuropsychiatr, vol. 35, no. 2, pp. 57-67, Jun 2021. [CrossRef]
- R. M. Puhl, M. S. Himmelstein, and R. L. Pearl, "Weight stigma as a psychosocial contributor to obesity," Am Psychol, vol. 75, no. 2, pp. 274-289, Feb-Mar 2020. [CrossRef]
- H. P. Libbey, M. T. Story, D. R. Neumark-Sztainer, and K. N. Boutelle, "Teasing, disordered eating behaviors, and psychological morbidities among overweight adolescents," Obesity (Silver Spring), vol. 16 Suppl 2, pp. S24-9, Nov 2008. [CrossRef]
- R. H. Striegel-Moore, C. G. Fairburn, D. E. Wilfley, K. M. Pike, F. A. Dohm, and H. C. Kraemer, "Toward an understanding of risk factors for binge-eating disorder in black and white women: a community-based case-control study," Psychol Med, vol. 35, no. 6, pp. 907-17, Jun 2005. [CrossRef]
- M. Warner, A. Wesselink, K. G. Harley, A. Bradman, K. Kogut, and B. Eskenazi, "Prenatal exposure to dichlorodiphenyltrichloroethane and obesity at 9 years of age in the CHAMACOS study cohort," Am J Epidemiol, vol. 179, no. 11, pp. 1312-22, Jun 1 2014. [CrossRef]
- R. C. Whitaker, M. S. Pepe, J. A. Wright, K. D. Seidel, and W. H. Dietz, "Early adiposity rebound and the risk of adult obesity," Pediatrics, vol. 101, no. 3, p. E5, Mar 1998. [CrossRef]
- S. B. Jabakhanji, F. Boland, M. Ward, and R. Biesma, "Body Mass Index Changes in Early Childhood," J Pediatr, vol. 202, pp. 106-114, Nov 2018. [CrossRef]
- E. R. Pulgaron, "Childhood obesity: a review of increased risk for physical and psychological comorbidities," Clin Ther, vol. 35, no. 1, pp. A18-32, Jan 2013. [CrossRef]
- S. M. Brara, C. Koebnick, A. H. Porter, and A. Langer-Gould, "Pediatric idiopathic intracranial hypertension and extreme childhood obesity," J Pediatr, vol. 161, no. 4, pp. 602-7, Oct 2012. [CrossRef]
- J. Silverstein et al., "Care of children and adolescents with type 1 diabetes: a statement of the American Diabetes Association," Diabetes Care, vol. 28, no. 1, pp. 186-212, Jan 2005. [CrossRef]
- D. Dabelea et al., "Association of Type 1 Diabetes vs Type 2 Diabetes Diagnosed During Childhood and Adolescence With Complications During Teenage Years and Young Adulthood," JAMA, vol. 317, no. 8, pp. 825-835, Feb 28 2017. [CrossRef]
- M. Cioana et al., "Prevalence of Polycystic Ovary Syndrome in Patients With Pediatric Type 2 Diabetes: A Systematic Review and Meta-analysis," JAMA Netw Open, vol. 5, no. 2, p. e2147454, Feb 1 2022. [CrossRef]
- Zeitler et al., "ISPAD Clinical Practice Consensus Guidelines 2018: Type 2 diabetes mellitus in youth," Pediatr Diabetes, vol. 19 Suppl 27, pp. 28-46, Oct 2018. [CrossRef]
- T. M. Brady, "Obesity-Related Hypertension in Children," Front Pediatr, vol. 5, p. 197, 2017. [CrossRef]
- G. Bonner, "Hyperinsulinemia, insulin resistance, and hypertension," J Cardiovasc Pharmacol, vol. 24 Suppl 2, pp. S39-49, 1994. [Online]. Available: https://www.ncbi.nlm.nih.gov/pubmed/7898093.
- E. L. Anderson, L. D. Howe, H. E. Jones, J. P. Higgins, D. A. Lawlor, and A. Fraser, "The Prevalence of Non-Alcoholic Fatty Liver Disease in Children and Adolescents: A Systematic Review and Meta-Analysis," PLoS One, vol. 10, no. 10, p. e0140908, 2015. [CrossRef]
- J. B. Schwimmer, P. E. Pardee, J. E. Lavine, A. K. Blumkin, and S. Cook, "Cardiovascular risk factors and the metabolic syndrome in pediatric nonalcoholic fatty liver disease," Circulation, vol. 118, no. 3, pp. 277-83, Jul 15 2008. [CrossRef]
- A. E. Feldstein, P. Charatcharoenwitthaya, S. Treeprasertsuk, J. T. Benson, F. B. Enders, and P. Angulo, "The natural history of non-alcoholic fatty liver disease in children: a follow-up study for up to 20 years," Gut, vol. 58, no. 11, pp. 1538-44, Nov 2009. [CrossRef]
- C. Koebnick et al., "Pediatric obesity and gallstone disease," J Pediatr Gastroenterol Nutr, vol. 55, no. 3, pp. 328-33, Sep 2012. [CrossRef]
- S. Jehan et al., "Obstructive Sleep Apnea and Obesity: Implications for Public Health," Sleep Med Disord, vol. 1, no. 4, 2017. [Online]. Available: https://www.ncbi.nlm.nih.gov/pubmed/29517065.
- Narang and J. L. Mathew, "Childhood obesity and obstructive sleep apnea," J Nutr Metab, vol. 2012, p. 134202, 2012. [CrossRef]
- H. J. Eisele, P. Markart, and R. Schulz, "Obstructive Sleep Apnea, Oxidative Stress, and Cardiovascular Disease: Evidence from Human Studies," Oxid Med Cell Longev, vol. 2015, p. 608438. [CrossRef]
- Z. W. Patinkin, R. Feinn, and M. Santos, "Metabolic Consequences of Obstructive Sleep Apnea in Adolescents with Obesity: A Systematic Literature Review and Meta-Analysis," Child Obes, vol. 13, no. 2, pp. 102-110, Apr 2017. [CrossRef]
- A. Kaditis, "From obstructive sleep apnea in childhood to cardiovascular disease in adulthood: what is the evidence?," Sleep, vol. 33, no. 10, pp. 1279-80, Oct 2010. [CrossRef]
- S. N. Magge, E. Goodman, S. C. Armstrong, N. Committee On, E. Section On, and O. Section On, "The Metabolic Syndrome in Children and Adolescents: Shifting the Focus to Cardiometabolic Risk Factor Clustering," Pediatrics, vol. 140, no. 2, Aug 2017. [CrossRef]
- R. Weiss et al., "Obesity and the metabolic syndrome in children and adolescents," N Engl J Med, vol. 350, no. 23, pp. 2362-74, Jun 3 2004. [CrossRef]
- E. Lang, "Obesity, Nutrition, and Asthma in Children," Pediatr Allergy Immunol Pulmonol, vol. 25, no. 2, pp. 64-75, Jun 2012. [CrossRef]
- S. Sadeeqa, T. Mustafa, and S. Latif, "Polycystic Ovarian Syndrome-Related Depression in Adolescent Girls: A Review," J Pharm Bioallied Sci, vol. 10, no. 2, pp. 55-59, Apr-Jun 2018. [CrossRef]
- S. Chung, "Growth and Puberty in Obese Children and Implications of Body Composition," J Obes Metab Syndr, vol. 26, no. 4, pp. 243-250, Dec 30 2017. [CrossRef]
- A. T. Soliman, M. Yasin, and A. Kassem, "Leptin in pediatrics: A hormone from adipocyte that wheels several functions in children," Indian J Endocrinol Metab, vol. 16, no. Suppl 3, pp. S577-87, Dec 2012. [CrossRef]
- C. M. Burt Solorzano and C. R. McCartney, "Obesity and the pubertal transition in girls and boys," Reproduction, vol. 140, no. 3, pp. 399-410, Sep 2010. [CrossRef]
- M. Lee et al., "Timing of Puberty in Overweight Versus Obese Boys," Pediatrics, vol. 137, no. 2, p. e20150164, Feb 2016. [CrossRef]
- S. Franks, "Polycystic ovary syndrome in adolescents," Int J Obes (Lond), vol. 32, no. 7, pp. 1035-41, Jul 2008. [CrossRef]
- K. Ong et al., "Infancy weight gain predicts childhood body fat and age at menarche in girls," J Clin Endocrinol Metab, vol. 94, no. 5, pp. 1527-32, May 2009. [CrossRef]
- S. D. Stovitz, E. W. Demerath, P. J. Hannan, L. A. Lytle, and J. H. Himes, "Growing into obesity: patterns of height growth in those who become normal weight, overweight, or obese as young adults," Am J Hum Biol, vol. 23, no. 5, pp. 635-41, Sep-Oct 2011. [CrossRef]
- J. B. Schwimmer, T. M. Burwinkle, and J. W. Varni, "Health-related quality of life of severely obese children and adolescents," JAMA, vol. 289, no. 14, pp. 1813-9, Apr 9 2003. [CrossRef]
- G. M. Budd and L. L. Hayman, "Addressing the childhood obesity crisis: a call to action," MCN Am J Matern Child Nurs, vol. 33, no. 2, pp. 111-8, quiz 119-20, Mar-Apr 2008. [CrossRef]
- D. Bacchini et al., "Bullying and Victimization in Overweight and Obese Outpatient Children and Adolescents: An Italian Multicentric Study," PLoS One, vol. 10, no. 11, p. e0142715, 2015. [CrossRef]
- V. Niehoff, "Childhood Obesity: A Call to Action," Bariatric Nursing and Surgical Patient Care, vol. 4, no. 1, pp. 17-23, 2009/03/01 2009. [CrossRef]
- J. Rankin et al., "Psychological consequences of childhood obesity: psychiatric comorbidity and prevention," Adolesc Health Med Ther, vol. 7, pp. 125-146. [CrossRef]
- D. Ruiz, M. L. Zuelch, S. M. Dimitratos, and R. E. Scherr, "Adolescent Obesity: Diet Quality, Psychosocial Health, and Cardiometabolic Risk Factors," Nutrients, vol. 12, no. 1, Dec 23 2019. [CrossRef]
- J. F. Hayes, E. E. Fitzsimmons-Craft, A. M. Karam, J. Jakubiak, M. L. Brown, and D. E. Wilfley, "Disordered Eating Attitudes and Behaviors in Youth with Overweight and Obesity: Implications for Treatment," Curr Obes Rep, vol. 7, no. 3, pp. 235-246, Sep 2018. [CrossRef]
- Simmonds, A. Llewellyn, C. G. Owen, and N. Woolacott, "Predicting adult obesity from childhood obesity: a systematic review and meta-analysis," Obes Rev, vol. 17, no. 2, pp. 95-107, Feb 2016. [CrossRef]
- S. J. Pont, R. Puhl, S. R. Cook, W. Slusser, O. Section On, and S. Obesity, "Stigma Experienced by Children and Adolescents With Obesity," Pediatrics, vol. 140, no. 6, Dec 2017. [CrossRef]
- R. Puhl and Y. Suh, "Health Consequences of Weight Stigma: Implications for Obesity Prevention and Treatment," Curr Obes Rep, vol. 4, no. 2, pp. 182-90, Jun 2015. [CrossRef]
- A. I. Carcone, A. J. Jacques-Tiura, K. E. Brogan Hartlieb, T. Albrecht, and T. Martin, "Effective Patient-Provider Communication in Pediatric Obesity," Pediatr Clin North Am, vol. 63, no. 3, pp. 525-38, Jun 2016. [CrossRef]
- C. L. Brown, E. E. Halvorson, G. M. Cohen, S. Lazorick, and J. A. Skelton, "Addressing Childhood Obesity: Opportunities for Prevention," Pediatr Clin North Am, vol. 62, no. 5, pp. 1241-61, Oct 2015. [CrossRef]
- T. Katzmarzyk et al., "An evolving scientific basis for the prevention and treatment of pediatric obesity," Int J Obes (Lond), vol. 38, no. 7, pp. 887-905, Jul 2014. [CrossRef]
- H. F. Skjakodegard et al., "Study Protocol: A randomized controlled trial evaluating the effect of family-based behavioral treatment of childhood and adolescent obesity-The FABO-study," BMC Public Health, vol. 16, no. 1, p. 1106, Oct 21 2016. [CrossRef]
- V. Singhal, A. C. Sella, and S. Malhotra, "Pharmacotherapy in pediatric obesity: current evidence and landscape," Curr Opin Endocrinol Diabetes Obes, vol. 28, no. 1, pp. 55-63, Feb 1 2021. [CrossRef]
- K. Woodard, L. Louque, and D. S. Hsia, "Medications for the treatment of obesity in adolescents," Ther Adv Endocrinol Metab, vol. 11, p. 2042018820918789, 2020. [CrossRef]
- D. Maahs et al., "Randomized, double-blind, placebo-controlled trial of orlistat for weight loss in adolescents," Endocr Pract, vol. 12, no. 1, pp. 18-28, Jan-Feb 2006. [CrossRef]
- J. S. Torgerson, J. Hauptman, M. N. Boldrin, and L. Sjostrom, "XENical in the prevention of diabetes in obese subjects (XENDOS) study: a randomized study of orlistat as an adjunct to lifestyle changes for the prevention of type 2 diabetes in obese patients," Diabetes Care, vol. 27, no. 1, pp. 155-61, Jan 2004. [CrossRef]
- J. R. Ryder, A. Kaizer, K. D. Rudser, A. Gross, A. S. Kelly, and C. K. Fox, "Effect of phentermine on weight reduction in a pediatric weight management clinic," Int J Obes (Lond), vol. 41, no. 1, pp. 90-93, Jan 2017. [CrossRef]
- G. Srivastava and C. M. Apovian, "Current pharmacotherapy for obesity," Nat Rev Endocrinol, vol. 14, no. 1, pp. 12-24, Jan 2018. [CrossRef]
- M. Wolfgram, A. L. Carrel, and D. B. Allen, "Long-term effects of recombinant human growth hormone therapy in children with Prader-Willi syndrome," Curr Opin Pediatr, vol. 25, no. 4, pp. 509-14, Aug 2013. [CrossRef]
- H. Lustig et al., "Octreotide therapy of pediatric hypothalamic obesity: a double-blind, placebo-controlled trial," J Clin Endocrinol Metab, vol. 88, no. 6, pp. 2586-92, Jun 2003. [CrossRef]
- G. Srivastava, V. O'Hara, and N. Browne, "Use of Lisdexamfetamine to Treat Obesity in an Adolescent with Severe Obesity and Binge Eating," Children (Basel), vol. 6, no. 2, Feb 4 2019. [CrossRef]
- C. Park et al., "Structural basis of neuropeptide Y signaling through Y1 receptor," Nat Commun, vol. 13, no. 1, p. 853, Feb 14 2022. [CrossRef]
- A. L. Weiss, A. Mooney, and J. P. Gonzalvo, "Bariatric Surgery: The Future of Obesity Management in Adolescents," Adv Pediatr, vol. 64, no. 1, pp. 269-283, Aug 2017. [CrossRef]
- Lamoshi, A. Chernoguz, C. M. Harmon, and M. Helmrath, "Complications of bariatric surgery in adolescents," Semin Pediatr Surg, vol. 29, no. 1, p. 150888, Feb 2020. [CrossRef]
Figure 1.
Prevalence of children obesity among 2-19 years old in the United States.
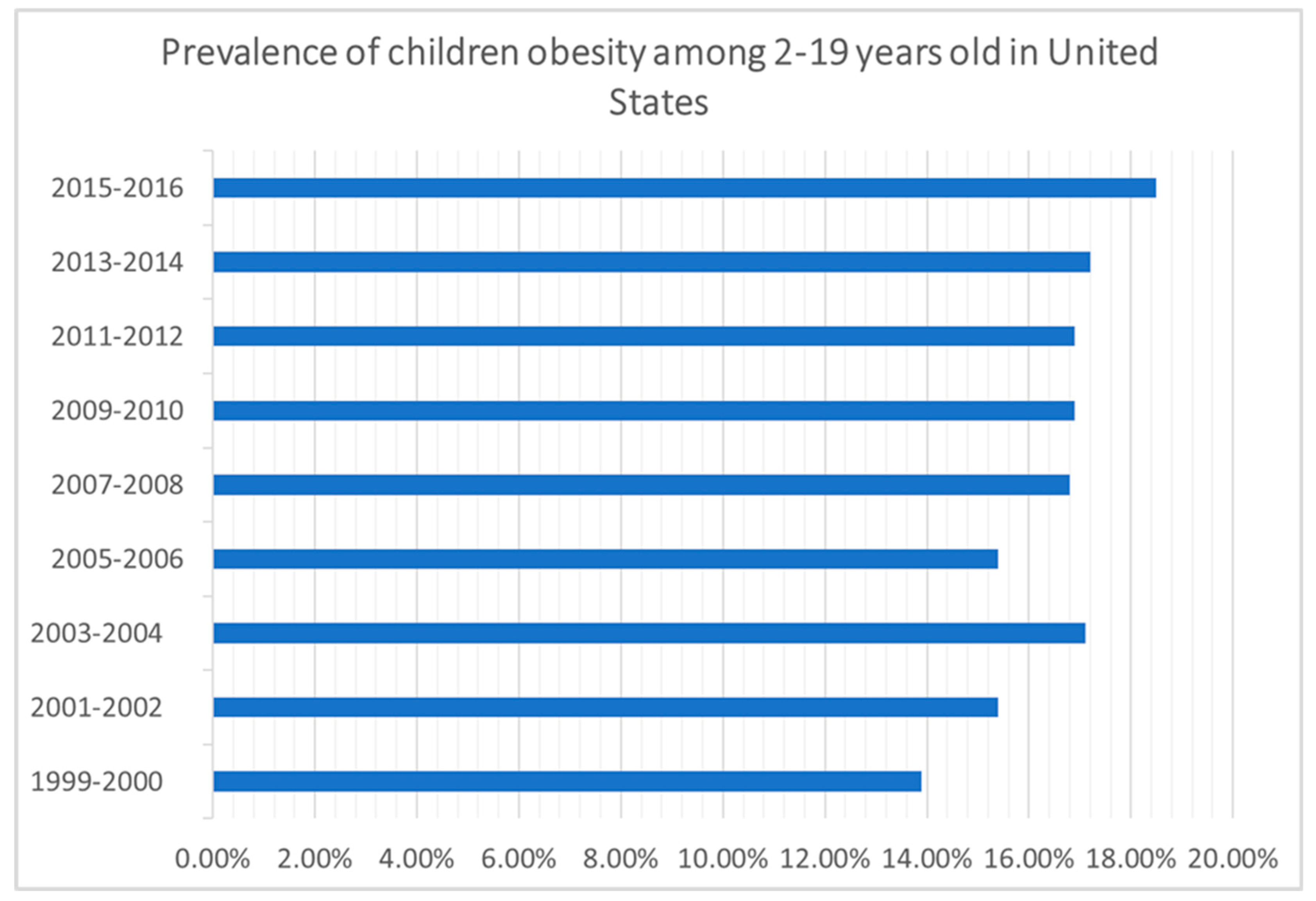
Figure 2.
Prevalence of overweight/obese children under 5 years of age in WHO European region Countries (2020).
Figure 2.
Prevalence of overweight/obese children under 5 years of age in WHO European region Countries (2020).
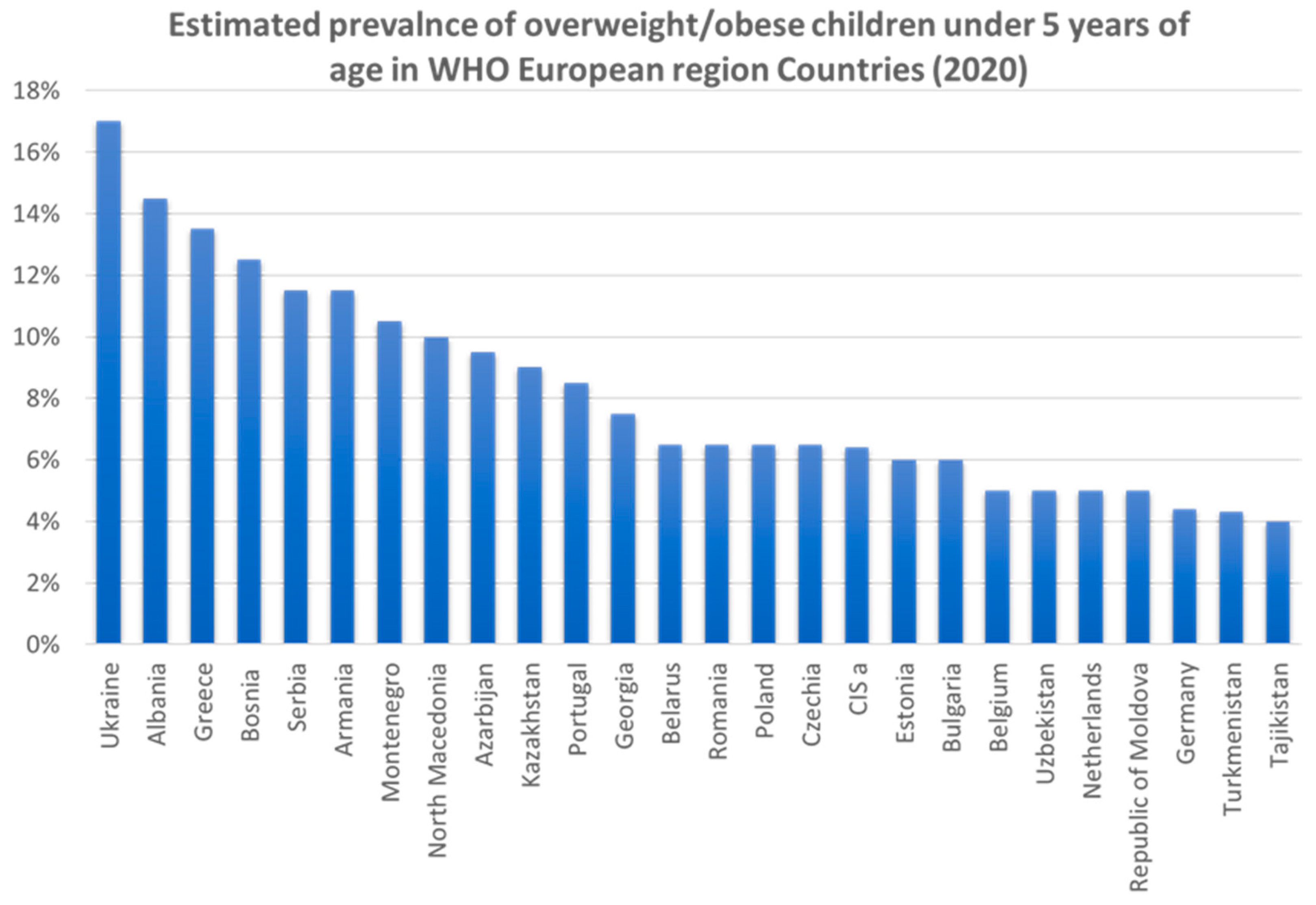
Figure 3.
Proportion of overweight/obese children and adolescents (5-19 years in Asia and Australia (2016).
Figure 3.
Proportion of overweight/obese children and adolescents (5-19 years in Asia and Australia (2016).
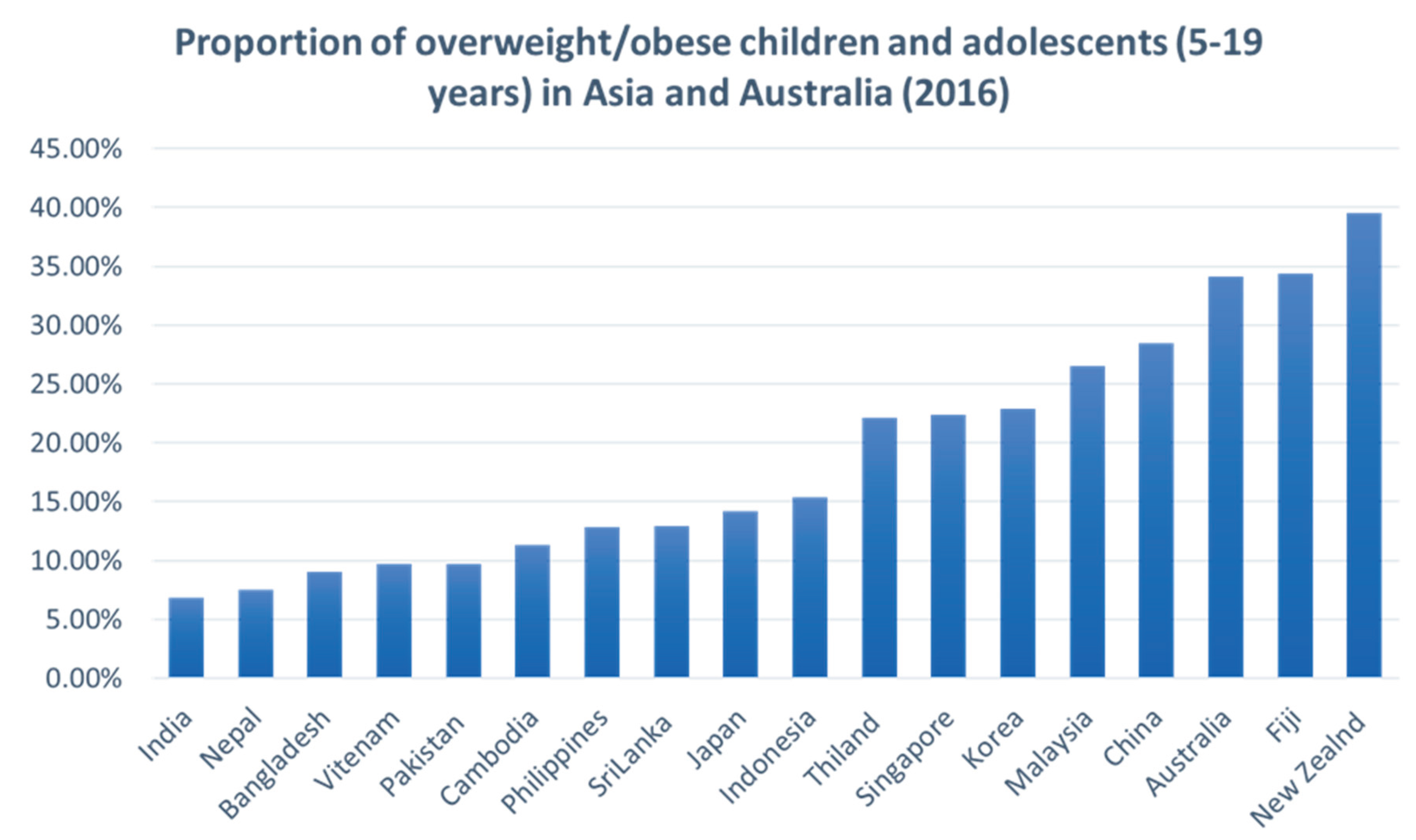
Figure 4.
3D-Stereo view represenation of NMR strucure of minimized AGOUTI-RELATED PROTEIN (AGRP) (87-132) (AC-AGRP(87-132)) PDB ID 1HYK.
Figure 4.
3D-Stereo view represenation of NMR strucure of minimized AGOUTI-RELATED PROTEIN (AGRP) (87-132) (AC-AGRP(87-132)) PDB ID 1HYK.

Figure 5.
Consequences of obesity in children.
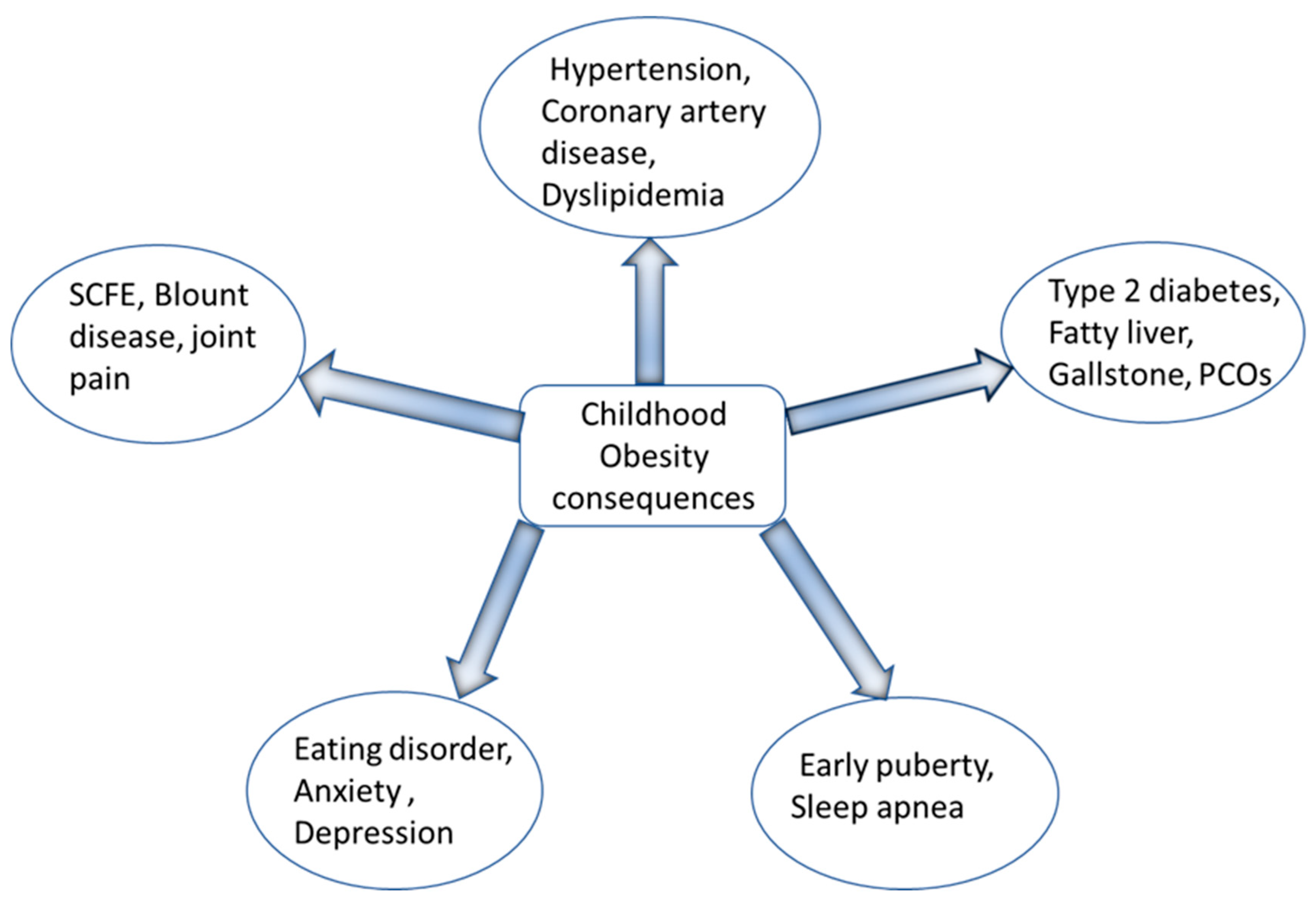
Figure 7.
The Crystal Structure of Human Neuropeptide Y Y1 Receptor with BMS-193885. The receptor is shown in cartoon representation while the ligand is shown as the red stick.
Figure 7.
The Crystal Structure of Human Neuropeptide Y Y1 Receptor with BMS-193885. The receptor is shown in cartoon representation while the ligand is shown as the red stick.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



