Submitted:
09 May 2025
Posted:
12 May 2025
You are already at the latest version
Abstract
Low respiratory tract infections remain a leading cause of morbidity and mortality among Intensive Care Unit patients, with severe cases often progressing to acute respiratory distress syndrome (ARDS). This life-threatening condition results from damage to the alveolar-capillary membrane, causing refractory hypoxemia and respiratory failure. Early detection and management are critical to treat the underlying cause, provide protective lung ventilation and, eventually, improve patients’ outcome. The Berlin definition, introduced in 2012, standardized ARDS diagnosis but excluded patients managed with non-invasive ventilation (NIV) or high-flow nasal cannula (HFNC) modalities, which are increasingly used, especially after the COVID-19 pandemic. This exclusion may delay diagnosis and treatment in patients who worsen despite non-invasive ventilatory support. Recent efforts aimed to broaden ARDS criteria by incorporating NIV and HFNC use, alongside alternative diagnostic tools like lung ultrasound and the SpO₂/FiO₂ ratio. These proposed modifications attempted to enhance the diagnosis of ARDS in resource-limited settings where access to arterial blood gas analysis or advanced imaging modalities may be restricted, thereby increasing the global applicability of ARDS classification. However, broadening the diagnostic criteria introduces several challenges, including the risk of overdiagnosis and the difficulty in differentiating ARDS from other causes of acute hypoxemic respiratory failure. Furthermore, inter-observer variability in imaging interpretation and inconsistencies in oxygenation assessment, particularly when relying on non-invasive measurements, may compromise diagnostic reliability. To address these limitations, a more nuanced diagnostic framework is needed, one that incorporates individualized therapeutic strategies, emphasizes lung-protective ventilation, and integrates advanced physiological or biomarker-based indicators. Such an approach has the potential to improve patient stratification, enable more targeted interventions, and ultimately enhance conduction of interventional trials.
Keywords:
ARDS
; invasive and non-invasive mechanical ventilation
; high-flow nasal cannula (HFNC)
; pneumonia
1. Introduction
Respiratory complications are among the most significant clinical challenges in critically ill patients admitted to Intensive Care Units (ICUs). Among these, low respiratory tract infections (LRTI), in particular pneumonia, play a major role as it frequently coexists with other critical conditions and contributes to worse outcomes [1,2]. The need for respiratory support is one of the primary reasons for ICU admission in patients with LRTI or pneumonia, with treatment options ranging from low- and high-flow oxygen therapy to non-invasive ventilation (NIV) and invasive mechanical ventilation [3]. The COVID-19 pandemic notably increased the adoption of HFNC and NIV, driven in part by the limited availability of invasive mechanical ventilation [4]. Given the potential severity of pneumonia, timely diagnosis and appropriate treatment are crucial for improving clinical outcomes. For this reason, these patients require close monitoring through imaging techniques, such as lung ultrasonography, chest X-rays and CT-scans. Microbiological sputum samples should be collected to ensure targeted antibiotic therapy against the responsible pathogen, and respiratory function must be assessed using parameters such blood gas analyses and the PaO₂/FiO₂ ratio via frequent arterial blood gas analysis [5].
In some cases, LRTI and pneumonia can progress to Acute Respiratory Distress Syndrome (ARDS), a severe inflammatory condition leading to hypoxemia and respiratory failure, often necessitating orotracheal intubation and mechanical ventilation [6]. The Berlin ARDS criteria, which are actually used to define ARDS, serve as a key diagnostic tool assisting clinicians in defining this syndrome [7]; however, many patients with diffuse acute lung injury who receive HFNC or NIV do not meet the Berlin definition for ARDS, suggesting that its incidence may be underdiagnosed. Indeed, one recent international observational study involving several intensive care units across 50 countries indicate that ARDS remains underrecognized, with clinician recognition rates as low as 60%, particularly for mild cases; this phenomenon is associated with insufficient application of recommended therapeutic measures, which contribute to persistently high mortality rates (approximately 40%) [8]. Therefore, a revised definition of ARDS has been proposed, potentially including patients treated with non-invasive ventilation, which could facilitate earlier diagnosis and more effective therapeutic interventions, improving overall patient outcomes [9].
In this brief clinical review, we aimed to examine the recent literature to provide an updated overview of the ARDS definition and explore potential approaches for refining both its classification and management.
2. Definition Of ARDS
First defined in 1967 [10] and diagnostic criteria being revised in 1988 [11], ARDS is a syndrome of respiratory failure with multiple etiologies that share common clinical-pathological characteristics including: (a) increased permeability of the alveolo-capillary membrane, leading to inflammatory edema; (b) increased non-aerated lung tissue resulting in higher lung elastance (lower compliance); and (c) increased venous admixture and dead space, which cause hypoxemia and hypercapnia [12]. The first clinical definition of ARDS has evolved significantly over the decades, with the American-European Consensus Conference (AECC) in 1994 formalizing diagnostic criteria [13]. Given the significant variability in clinical practice and research the AECC sought to refine and unify the prevailing definitions of ARDS and Acute Lung Injury (ALI). AECC established diagnostic criteria for ALI as a syndrome with acute onset, bilateral infiltrates on chest X-rays, arterial oxygenation (PaO₂/FiO₂ ≤ 300 mmHg), and no evidence of left atrial hypertension (wedge pressure ≤ 18 mmHg) and ARDS as a more severe form of ALI with PaO₂/FiO₂ ≤ 200 mmHg [14]. Despite its utility, the AECC criteria faced criticism for lacking precision and clarity in several areas, such as variability in interpreting chest X-rays and the absence of severity stratification [15]. These limitations prompted the development of the Berlin definition in 2012 [7]. The key critical elements for diagnosis now include an acute onset within one week of a recognized clinical event or a significant worsening of respiratory symptoms; the presence of bilateral opacities on chest imaging (X-ray or CT) not fully attributable to other causes such as fluid overload, effusions or lung collapse. Additionally, the diagnosis requires the exclusion of cardiogenic or hydrostatic pulmonary edema as the primary cause of respiratory failure and a PaO₂/FiO₂ ratio below 300 mmHg, with a minimum PEEP of 5 cm H₂O or more [7,16]. In 2016 Riviello et al. conducted a study at the referral hospital of Kigali, Rwandan, using a modified version of the Berlin Definition, adapted for resource-limited settings [17]. The “Kigali modification” replaced the PEEP requirement with SpO₂/FiO₂ ≤ 315 and allowed lung ultrasound instead of chest X-ray to detect bilateral opacities. The study demonstrated that the Berlin criteria underestimate ARDS cases in low-resource settings, highlighting the need for context-appropriate diagnostic tools to better understand and address the global burden of ARDS [17]. However, the Kigali modification has not been formally incorporated into the current ARDS definition, due to lack of large and rigorous study comparing the original Berlin definition to this modified proposal [17]. In 2023, the European Society of Intensive Care Medicine (ESICM) updated its guidelines on ARDS, revising key aspects related to its definition, phenotyping, and respiratory support strategies (Table 1 and Table 2, Figure 1) [12]. Notably, these new recommendations acknowledge the evolving role of non-invasive respiratory support, such as HFNC and NIV, and discuss their potential inclusion in ARDS definitions. Additionally, the guidelines emphasize a more personalized approach to mechanical ventilation, considering lung-protective strategies, driving pressure, and patient self-inflicted lung injury (P-SILI) to optimize clinical outcomes. These updates reflect the latest evidence and clinical insights aimed at improving the diagnosis and management of ARDS patients [12].

Table 1.
Different definitions of ARDS for diagnosis.
| DIAGNOSIS | ||||
|---|---|---|---|---|
| Criteria | Ashbaught (1967) | AECC (1994) | Berlin (2012) | Kigali (2016) |
| Onset | RF with tachypnea, lung stiffness | RF with tachypnea, lung stiffness | RF within 1 week not fully explained by cardiac function or volume overload | RF within 1 week not fully explained by cardiac function or volume overload |
| Imaging | Bilateral opacities on CRX | Bilateral opacities on CRX | Bilateral opacities on CRX or CT not fully explained by effusion, collapse or nodules | Bilateral opacities on CRX or US not fully explained by effusion, collapse or nodules |
| Oxygenation | Oxygenation impairment | Oxygenation impairment: ALI (P/F ≤ 300 mmHg) ARDS (P/F ≤ 200 mmHg) |
Oxygenation impairment: Mild 200 < P/F ≤ 300 mmHg with PEEP ≥ 5 cmH2O Moderate 100 < P/F ≤ 200 mmHg with PEEP ≥ 5 cmH2O Severe P/F < 100 mmHg with PEEP ≥ 5 cmH2O |
Oxygenation impairment: SpO2/FiO2 <315; no PEEP requirement |
RF: Respiratory Failure; CRX chest radiography; US ultrasound scan, CT: computed tomography scan; ALI: acute lung injury; PEEP: positive end expiratory pressure; PaO2: partial pressure of arterial oxygen; FiO2: fraction of inspired oxygen; SpO2: oxygen saturation; P/F: PaO2/FiO2 ratio.
Table 2.
Most important component of ARDS management, according to ESICM 2023 [11].
Table 2.
Most important component of ARDS management, according to ESICM 2023 [11].
| MANAGEMENT ESICM 2023 |
|---|
| Low Tv ≤ 4-8 mL/kg PBW |
| Pplat ≤ 30 cmH2O, DP ≤ 15 cmH2O, Reduction Mechanical Power |
| Individualized PEEP titration, avoid lung recruitment maneuvers |
| Use of NIV or HFNC to reduce risk of intubation |
| Prone Position (PaO2/FiO2 < 150, PEEP ≥ 5 cmH2O) and awake prone position |
| Use of ECMO VV in severe ARDS, avoid ECCO2R |
| Avoid continuous infusion of NMBA |
Tv: Tidal volume; PBW: Predicted Body Weight; Pplat: plateau pressure; DP: driving Pressure; PEEP: positive end expiratory pressure; PaO2: partial pressure of arterial oxygen; FiO2: fraction of inspired oxygen; NIV: non-invasive ventilation; HFNC: high flow nasal cannula; ECMO VV: venovenous extracorporeal membrane oxygenation; ECCO2R: extracorporeal carbon dioxide removal; NMBA: neuro-muscolar blocking agents.
Figure 1.
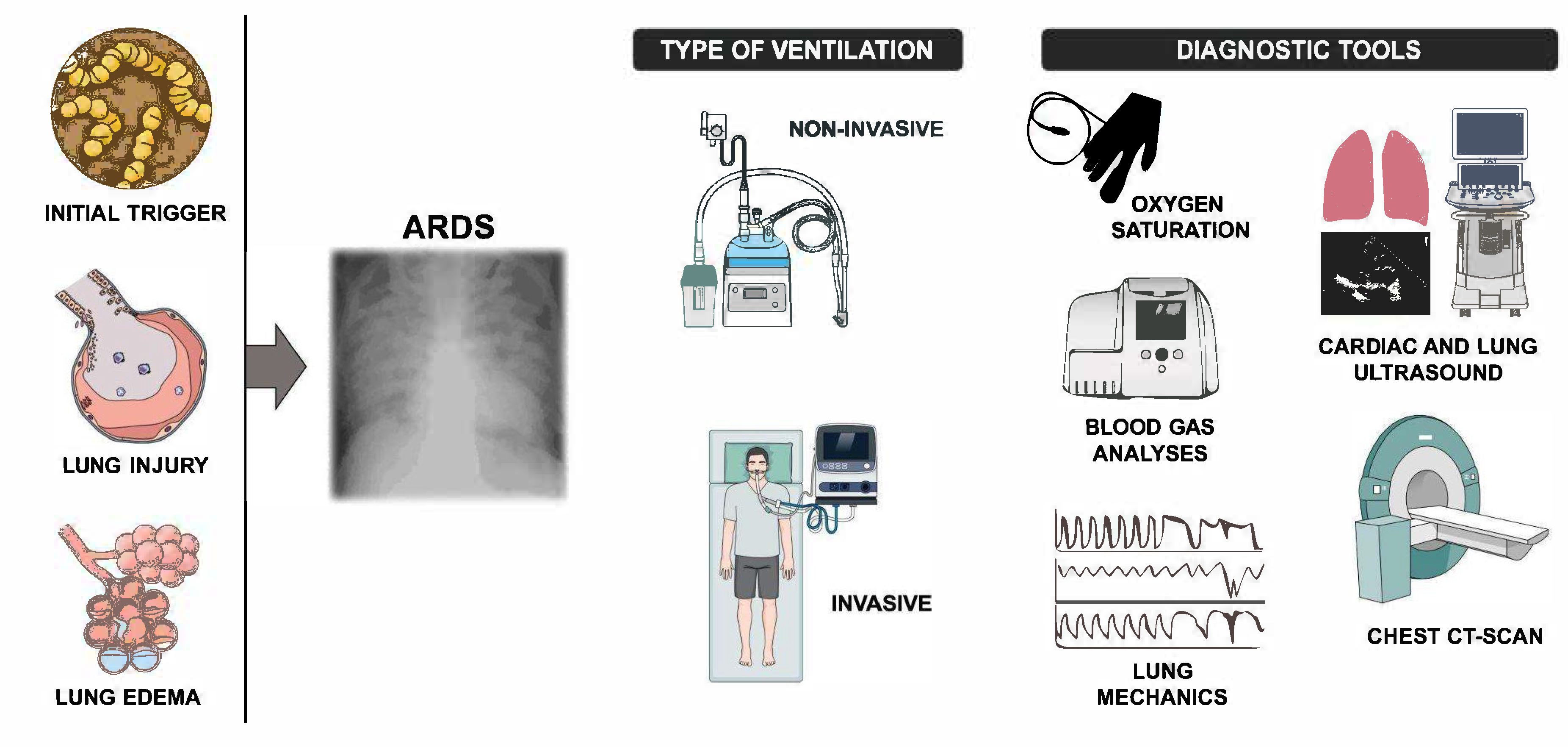
The figure shows the main steps leading to ARDS, the typical chest X-ray of the injured lungs, the ventilatory strategies (non-invasive and invasive), and the pivotal diagnostic tools used in daily clinical practice to assess the severity of th e illness.2. Management Of ARDS.
Figure 1.
The figure shows the main steps leading to ARDS, the typical chest X-ray of the injured lungs, the ventilatory strategies (non-invasive and invasive), and the pivotal diagnostic tools used in daily clinical practice to assess the severity of th e illness.2. Management Of ARDS.
2. Management Of ARDS
The management of ARDS has advanced significantly in recent years. The cornerstone of ARDS treatment is supportive care, with a focus on lung-protective ventilation strategies, adjunctive therapies, and individualized approaches tailored to the patient’s clinical condition. The use of low tidal volumes (e.g. 6 mL/kg of predicted body weight) reduces the risk of ventilator-induced lung injury. Moreover, maintaining a plateau pressure below 30 cm H₂O and a driving pressure below 15 cm H₂O is equally important to prevent alveolar overdistension [18,19]. Positive end-expiratory pressure (PEEP) prevents alveolar collapse and improves oxygenation [9]. Furthermore, prone positioning, enhancing ventilation/perfusion matching, and reducing alveolar collapse in dorsal regions, has proven to be one of the most effective strategies for managing severe ARDS and reduce mortality in most severe cases (e.g. PaO2/FiO2 < 150) [6,20,21] [22]. In selected refractory ARDS patients, the insertion of veno-venous extracorporeal membrane oxygenation (V-V ECMO) could improve gas exchange and enhance survival by enabling ultraprotective lung ventilation or lung rest [6]. The use of V-V ECMO was long considered only a rescue therapy for patients with severe ARDS. However, according to the latest ARDS guidelines from the European Society of Intensive Care Medicine (ESICM) of 2023, V-V ECMO is now recommended for selected patients with severe ARDS meeting specific eligibility criteria described by the EOLIA trial (2018): PaO2/FiO2 <50 mmHg for over 3 hours, <80 mmHg for over 6 hours, or arterial pH <7.25 with PaCO2 >60 mmHg for over 6 hours [23,24]. While the EOLIA trial did not demonstrate a significant reduction in 60-day mortality in ECMO-treated patients compared to those receiving only invasive mechanical ventilation, it highlighted an increased risk of bleeding or ischemic stroke. However, a more recent meta-analysis that examined two randomized trials demonstrated a decrease in mortality at 60 days in patients treated with V-V ECMO [23,25,26].
3. NIV and HFNC
NIV and HFNC recently have emerged as valuable tools in managing ARDS, particularly in patients with mild-to-moderate hypoxemia, such as those in the early stages of respiratory failure or in resource-limited settings where invasive MV may not be immediately available. In particular, HFNC emerged as a critical non-invasive respiratory support tool during COVID-19 pandemic due to its ability to deliver heated, humidified oxygen at high flow rates, reducing respiratory effort and improving oxygenation [23,26,27,28] . These strategies, moreover, aim to reduce the need for invasive MV, avoiding associated complications, such as ventilator-induced lung injury (VILI), sedation-related risks, and ventilator-associated pneumonia [29]. Clinical trials have demonstrated that HFNC can reduce tracheal intubation rates and improve survival compared to conventional oxygen therapy [30]. Despite their advantages, NIV and HFNC have limitations in ARDS management. Vigorous respiratory efforts can exacerbate lung injury through patient-self inflicted lung injury (P-SILI), particularly in patients with severe ARDS or high inspiratory efforts [31]. Furthermore, delayed intubation in patients failing NIV or HFNC has been associated with higher mortality, emphasizing the importance of close respiratory monitoring and timely escalation to invasive MV when necessary [32]. ESICM guidelines emphasize personalized treatment approaches based on ARDS phenotypes and suggest lung-protective ventilation strategies, such as low tidal volume, appropriate PEEP titration, and prone positioning. Additionally, they discuss the role of NIV and HFNC, acknowledging their benefits but also cautioning against delayed tracheal intubation. These recommendations aim to optimize patient outcomes by integrating the latest evidence on MV, respiratory mechanics and individualized treatment strategies [12].
3. New Criteria Of ARDS
The increasing use of NIV and HFNC in managing acute hypoxemic respiratory failure has contributed to the ongoing evolution of ARDS definitions, reflecting efforts to enhance diagnostic accuracy, improve clinical utility, and facilitate early intervention [15,31]. In 2023 a global consensus conference [9] with broad international representation suggested recommendations for updating the ARDS definition, identifying criteria that could be applied to all ARDS categories (risk factors and origin of edema, timing, chest imaging) and criteria that could be applied to specific ARDS categories [18].
3.1. Rationale and Evidence
The Berlin definition, while a significant advancement in the diagnosis and classification of ARDS, has notable limitations. One critical point is the exclusion of patients receiving NIV respiratory support [33]. By requiring MV with a minimum PEEP of 5 cm H₂O, the Berlin criteria leave out patients on HFNC or NIV. These patients often show similar clinical and pathophysiological features to those who are intubated but are not included under the current ARDS definition. This gap may result in a failure to identify ARDS in its early stages for patients who do not require intubation, leading to delayed interventions and possibly worsening outcomes [34]. Additionally, the imaging criteria in the Berlin definition introduce significant subjectivity, as differences in interpretation between clinicians and imaging modalities - such as chest X-rays versus CT scans - can lead to inconsistencies in diagnosis. This variability affects the reproducibility and reliability of ARDS diagnosis, making its application in routine practice more challenging [35]. Another issue is the reliance on oxygenation thresholds, specifically the PaO₂/FiO₂ ratio, for identifying ARDS. This approach can lead to delayed diagnoses, as significant hypoxemia may not emerge until later in disease progression [9,36]. Moreover, recent evidence suggests that the PaO₂/FiO₂ ratio alone insufficiently captures the complexity of ARDS, particularly concerning ventilator-induced lung injury (VILI) [37]. Incorporating metrics such as the Oxygenation Factor (OF), which combines oxygenation data with mechanical variables like mean airway pressure (Paw) and positive end-expiratory pressure (PEEP), may offer a more comprehensive evaluation [38]. Finally, the Berlin definition’s dependence on arterial blood gas measurements and specific MV parameters limits its global applicability. In resource-limited settings, with limited access to advanced diagnostic tools, applying the current criteria is often not feasible [31]. The diagnostic criteria of ARDS and new definitions are reported in Table 3.
Table 3.
Diagnostic criteria of ARDS in the new definition and differences from the Berlin criteria.
Table 3.
Diagnostic criteria of ARDS in the new definition and differences from the Berlin criteria.
| NEW ARDS DEFINITION | BERLIN DEFINITION |
|---|---|
| Criteria for ALL ARDS categories | |
| |
|
Criteria for SPECIFIC ARDS categories NEW ARDS DEFINITION |
Criteria for SPECIFIC ARDS categories BERLIN DEFINITION |
|
|
PaO2: partial pressure of arterial oxygen; FiO2: fraction of inspired oxygen; SpO2: saturation of oxygen; P/F: PaO2/FiO2 ratio; PEEP: positive end expiratory pressure; NIV: non-invasive ventilation; HFNC: high flow nasal cannula; CPAP: continuous positive airway pressure.
4. Advantages and Limits
4.1. Advantages
The new definition expands ARDS to include patients treated with HFNC or NIV. This change acknowledges that many patients treated with non-invasive support referred to as "non-intubated ARDS” exhibit similar pathophysiological and clinical characteristics to those who are intubated [34]. Moreover, inclusion of alternative oxygenation metrics, such as the SpO₂/FiO₂ ratio, facilitates earlier recognition of ARDSb[39]. This equivalence between SpO₂/FiO₂ and PaO₂/FiO₂ ratios was established through large-scale clinical validation studies demonstrating a strong linear correlation, leading to defined threshold values that reliably correspond to established PaO₂/FiO₂ diagnostic thresholds of 200 (SpO₂/FiO₂ ratio of 235) and 300 (SpO₂/FiO₂ ratio of 315) for ARDS and Acute Lung Injury (ALI), respectively [40,41]. These metrics are particularly useful in settings where arterial blood gas analysis may not be feasible, making the definition more accessible and practical for resource-limited environments [31]. A notable enhancement in the revised definition is its ability to stratify ARDS severity with greater accuracy. Adjustments to oxygenation thresholds and the introduction of PEEP-equivalent metrics for HFNC users enable a more accurate classification of severity in both intubated and non-intubated patients, allowing clinicians to personalize therapeutic strategies to meet individual patient needs and improve treatment effectiveness [9]. With the Kigali modification, bilateral B-lines or consolidations on lung-ultrasound (LUS) were allowed to fulfil the imaging criteria for ARDS. In comparison to the gold standard computed tomography (CT) in high-resource settings, these criteria proved to be highly sensitive but with low to moderate specificity [42]. Recent international guidelines have increasingly recognized the potential value of lung ultrasound (LUS), as introduced by the Kigali modification, although it has not yet been formally incorporated into the standard global definition of ARDS [12]. A useful development is the LUS-ARDS score, a data driven and externally validated method based on LUS-scores from both the left and right lungs, combined with the identification of an abnormal pleural line in the antero-lateral regions [43]. This method involves more complexity than the Kigali modification but exhibits higher accuracy in diagnosing and excluding ARDS [44]. Another critical advantage of the new definition is its improved global applicability, including in resources-limited settings. This adaptability ensures that ARDS can be diagnosed and effectively managed even in low-income countries where access to advanced diagnostics and MV is often restricted [31,45] (Table 4).
Table 4.
Practical advantages and limitations of new ARDS definition.
| NEW ARDS DEFINITION | |||
|---|---|---|---|
| New Definition | Advantages | Limitations | Clinical implications |
| Inclusion of HFNC/NIV | Expands recognition of “non intubated ARDS” | Potential for overdiagnosis | Closer monitoring needed to avoid delayed intubation |
| SpO₂/FiO₂ for diagnosis | Useful in low resource settings | Affected by perfusion, skin pigmentation, device accuracy | May require arterial blood gas confirmation |
| Use of lung ultrasound | Portable, bedside diagnostic tool | Operator-dependent, lacks standardized criteria | Training and standardization are essential |
| Applicability in resource-limited settings | Does not require PEEP for diagnosis | Excludes ECMO patients | May help early diagnosis but could overdiagnose ARDS |
HFNC: High flow nasal cannula, NIV: non-invasive ventilation, SpO2/FiO2: saturation of oxygen/fraction of inspired oxygen.
4.2. Limitations
The revised ARDS definition, while offering significant advancements, has several limitations that should be acknowledged. One prominent concern is the potential for overdiagnosis. By broadening the criteria to include non-intubated patients on HFNC or NIV, there is a risk of misclassifying other causes of acute hypoxemic respiratory failure as ARDS. This could lead to unnecessary treatments and resource utilization, potentially overburdening healthcare systems and diluting the specificity of ARDS as a distinct clinical entity [34]. The application of the new definition is also problematic in certain specific patient populations, such as those receiving V-V ECMO. Many V-V ECMO patients are awake and spontaneously breathing. Since in these patients oxygenation-based criteria, such as PaO₂/FiO₂ or SpO₂/FiO₂ ratios, could be normal they’ll be automatically excluded from ARDS diagnosis. As a result, the revised criteria may not fully address the diagnostic needs of ECMO-supported ARDS patients, leading to inconsistent classification [9]. The use of alternative oxygenation metrics, such as the SpO₂/FiO₂ ratio is practical in resource-limited settings; however, they are inherently less accurate than arterial blood gas measurements. Additionally, recent studies highlight significant limitations of the SpO₂/FiO₂ ratio for ARDS severity classification, showing misclassification in about one-third of cases due to measurement inaccuracies and a high dependency on FiO₂ settings [46] . Factors such as poor perfusion, skin pigmentation, patient movement, and device variability further limit the accuracy of SpO₂-based measurements, emphasizing the need for careful interpretation and potential additional validation in clinical practice. These inaccuracies may result in overestimation or underestimation of ARDS severity, particularly in cases with borderline oxygenation status [31]. Additionally, the incorporation of LUS into ARDS diagnostics is valuable for bedside assessments, but on the other hand has some limitations, as its accuracy depends heavily on the clinician’s skill and experience and may be less effective in differentiating ARDS from other conditions with similar findings. Finally, the lack of standardization in LUS protocols and interpretation criteria poses challenges for ARDS diagnosis [35,47] (Table 4).
5. Future Perspectives
The ongoing evolution of ARDS diagnostic criteria reflects the need for greater precision in identifying and managing this complex syndrome. Various authors have proposed refinements to improve diagnostic accuracy and to adapt the criteria more effectively for both clinical practice and research purposes [48].
One promising approach involves the use of PEEP-adjusted PaO₂/FiO₂ ratio: (P/FP) or SpO₂/FiO₂ (S/FP) ratios. These indices account for the level of positive end-expiratory pressure (PEEP) applied during ventilation, which plays a critical role in maintaining alveolar recruitment and optimizing oxygenation. P/FP is calculated by dividing the traditional PaO₂/FiO₂ ratio by the applied PEEP and then multiplying the result by a correction factor of 10. The same concept can be used for S/FP calculation. This formula adjusts for the contribution of PEEP to oxygenation, reflecting the interaction between alveolar recruitment and gas exchange efficiency [49]. Some authors used the ROX index calculated as SpO₂/FiO₂ ratio/respiratory rate as an indicator of the severity of respiratory failure in patients with ARDS receiving non invasive ventilation. Given its ease of bedside calculation, the ROX index represents a promising area of research for future ARDS definitions, potentially complementing current criteria [50,51].
For research purposes, several authors have emphasized the importance of integrating advanced physiological and imaging-based parameters into ARDS definitions [52,53]. These include measures of pulmonary vascular permeability, lung weight, and aeration. Pulmonary vascular permeability, which quantifies endothelial injury and capillary leak, is a direct indicator of the inflammatory and edematous processes underlying ARDS [54]. Ranieri and colleagues have argued that incorporating such measures could help distinguish ARDS from other causes of hypoxemic respiratory failure and offer a more refined characterization of disease severity [35]. Similarly, the assessment of lung weight and aeration through advanced imaging techniques, such as computed tomography (CT) or magnetic resonance imaging (MRI), provides valuable insights into the extent of alveolar flooding and consolidation. These parameters not only improve the reliability of severity stratification but also enable clinicians to assess therapeutic responses with greater accuracy [44].
6. Conclusions
In summary, the development of ARDS diagnostic criteria and management strategies represent a significant effort to improve patient outcomes by adapting approaches to individual and contextual needs. The inclusion of non-invasive respiratory support tools, such as HFNC and NIV, in the broader definition of ARDS acknowledge their crucial role in modern clinical practice, particularly in resource-limited settings and during global health crises, like occurred for the COVID-19 pandemic. While these advancements improve diagnostic inclusivity and accessibility, they also bring challenges, such as potential overdiagnosis and variability in diagnostic tools like SpO₂/FiO₂ ratios and lung ultrasound. Future perspectives in ARDS research and management point towards integrating advanced physiological indices, imaging modalities, and personalized approaches to refine diagnosis and stratify disease severity.
Author Contributions
Cesare Biuzzi and Elena Modica contributed equally to this study. Cesare Biuzzi and Elena Modica have given substantial contributions to the conception, writing of the manuscript, acquisition, analysis, and interpretation of the data. Noemi De Filippis contributed to drafting the introduction section. Cesare Biuzzi and Elena Modica realized the tables. Fabio Silvio Taccone and Sabino Scolletta created the figure. Agnese Di Chiaro, Daria Pizzirani, Benedetta Galgani and Daniele Marianello revised it critically. Sabino Scolletta, Federico Franchi and Fabio Silvio Taccone supervised and revised it critically. All authors read and approved the final version of the manuscript.
Funding
This research received no external funding.
Acknowledgments
The authors have reviewed and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Cillóniz, C.; Torres, A.; Niederman, M.S. Management of Pneumonia in Critically Ill Patients. BMJ 2021, e065871. [Google Scholar] [CrossRef]
- Niederman, M.S. Pneumonia: Considerations for the Critically Ill Patient. In Critical Care Medicine; Elsevier, 2008; pp. 867–883, ISBN 978-0-323-04841-5.
- Morris, A.C. Management of Pneumonia in Intensive Care. J Emerg Crit Care Med 2018, 2, 101–101. [Google Scholar] [CrossRef]
- Grieco, D.L.; Menga, L.S.; Cesarano, M.; Rosà, T.; Spadaro, S.; Bitondo, M.M.; Montomoli, J.; Falò, G.; Tonetti, T.; Cutuli, S.L.; et al. Effect of Helmet Noninvasive Ventilation vs High-Flow Nasal Oxygen on Days Free of Respiratory Support in Patients With COVID-19 and Moderate to Severe Hypoxemic Respiratory Failure: The HENIVOT Randomized Clinical Trial. JAMA 2021, 325, 1731. [Google Scholar] [CrossRef] [PubMed]
- Metlay, J.P.; Waterer, G.W.; Long, A.C.; Anzueto, A.; Brozek, J.; Crothers, K.; Cooley, L.A.; Dean, N.C.; Fine, M.J.; Flanders, S.A.; et al. Diagnosis and Treatment of Adults with Community-Acquired Pneumonia. An Official Clinical Practice Guideline of the American Thoracic Society and Infectious Diseases Society of America. Am J Respir Crit Care Med 2019, 200, e45–e67. [Google Scholar] [CrossRef]
- Grotberg, J.C.; Reynolds, D.; Kraft, B.D. Management of Severe Acute Respiratory Distress Syndrome: A Primer. Crit Care 2023, 27, 289. [Google Scholar] [CrossRef]
- ARDS Definition Task Force; V Marco Ranieri Acute Respiratory Distress Syndrome: The Berlin Definition. JAMA 2012, 307. [CrossRef]
- Bellani, G.; Laffey, J.G.; Pham, T.; Fan, E.; Brochard, L.; Esteban, A.; Gattinoni, L.; Van Haren, F.; Larsson, A.; McAuley, D.F.; et al. Epidemiology, Patterns of Care, and Mortality for Patients With Acute Respiratory Distress Syndrome in Intensive Care Units in 50 Countries. JAMA 2016, 315, 788. [Google Scholar] [CrossRef]
- Matthay, M.A.; Arabi, Y.; Arroliga, A.C.; Bernard, G.; Bersten, A.D.; Brochard, L.J.; Calfee, C.S.; Combes, A.; Daniel, B.M.; Ferguson, N.D.; et al. A New Global Definition of Acute Respiratory Distress Syndrome. Am J Respir Crit Care Med 2024, 209, 37–47. [Google Scholar] [CrossRef]
- Ashbaugh, DavidG. ; Boyd Bigelow, D.; Petty, ThomasL.; Levine, BernardE. ACUTE RESPIRATORY DISTRESS IN ADULTS. The Lancet 1967, 290, 319–323. [Google Scholar] [CrossRef]
- Murray, J.F.; Matthay, M.A.; Luce, J.M.; Flick, M.R. An Expanded Definition of the Adult Respiratory Distress Syndrome. Am Rev Respir Dis 1988, 138, 720–723. [Google Scholar] [CrossRef]
- Grasselli, G.; Calfee, C.S.; Camporota, L.; Poole, D.; Amato, M.B.P.; Antonelli, M.; Arabi, Y.M.; Baroncelli, F.; Beitler, J.R.; Bellani, G.; et al. ESICM Guidelines on Acute Respiratory Distress Syndrome: Definition, Phenotyping and Respiratory Support Strategies. Intensive Care Med 2023, 49, 727–759. [Google Scholar] [CrossRef] [PubMed]
- Petty, T.L.; Ashbaugh, D.G. The Adult Respiratory Distress Syndrome. Chest 1971, 60, 233–239. [Google Scholar] [CrossRef]
- Bernard, G.R.; Artigas, A.; Brigham, K.L.; Carlet, J.; Falke, K.; Hudson, L.; Lamy, M.; Legall, J.R.; Morris, A.; Spragg, R. The American-European Consensus Conference on ARDS. Definitions, Mechanisms, Relevant Outcomes, and Clinical Trial Coordination. Am J Respir Crit Care Med 1994, 149, 818–824. [Google Scholar] [CrossRef]
- Griffiths, M.J.D.; McAuley, D.F.; Perkins, G.D.; Barrett, N.; Blackwood, B.; Boyle, A.; Chee, N.; Connolly, B.; Dark, P.; Finney, S.; et al. Guidelines on the Management of Acute Respiratory Distress Syndrome. BMJ Open Resp Res 2019, 6, e000420. [Google Scholar] [CrossRef]
- Matthay, M.A.; Zemans, R.L.; Zimmerman, G.A.; Arabi, Y.M.; Beitler, J.R.; Mercat, A.; Herridge, M.; Randolph, A.G.; Calfee, C.S. Acute Respiratory Distress Syndrome. Nat Rev Dis Primers 2019, 5, 18. [Google Scholar] [CrossRef]
- Riviello, E.D.; Kiviri, W.; Twagirumugabe, T.; Mueller, A.; Banner-Goodspeed, V.M.; Officer, L.; Novack, V.; Mutumwinka, M.; Talmor, D.S.; Fowler, R.A. Hospital Incidence and Outcomes of the Acute Respiratory Distress Syndrome Using the Kigali Modification of the Berlin Definition. Am J Respir Crit Care Med 2016, 193, 52–59. [Google Scholar] [CrossRef]
- Matthay, M.A.; Thompson, B.T.; Ware, L.B. The Berlin Definition of Acute Respiratory Distress Syndrome: Should Patients Receiving High-Flow Nasal Oxygen Be Included? The Lancet Respiratory Medicine 2021, 9, 933–936. [Google Scholar] [CrossRef]
- Papazian, L.; Aubron, C.; Brochard, L.; Chiche, J.-D.; Combes, A.; Dreyfuss, D.; Forel, J.-M.; Guérin, C.; Jaber, S.; Mekontso-Dessap, A.; et al. Formal Guidelines: Management of Acute Respiratory Distress Syndrome. Ann. Intensive Care 2019, 9, 69. [Google Scholar] [CrossRef]
- Guérin, C.; Albert, R.K.; Beitler, J.; Gattinoni, L.; Jaber, S.; Marini, J.J.; Munshi, L.; Papazian, L.; Pesenti, A.; Vieillard-Baron, A.; et al. Prone Position in ARDS Patients: Why, When, How and for Whom. Intensive Care Med 2020, 46, 2385–2396. [Google Scholar] [CrossRef]
- Ramji, H.F.; Hafiz, M.; Altaq, H.H.; Hussain, S.T.; Chaudry, F. Acute Respiratory Distress Syndrome; A Review of Recent Updates and a Glance into the Future. Diagnostics 2023, 13, 1528. [Google Scholar] [CrossRef]
- Qadir, N.; Sahetya, S.; Munshi, L.; Summers, C.; Abrams, D.; Beitler, J.; Bellani, G.; Brower, R.G.; Burry, L.; Chen, J.-T.; et al. An Update on Management of Adult Patients with Acute Respiratory Distress Syndrome: An Official American Thoracic Society Clinical Practice Guideline. Am J Respir Crit Care Med 2024, 209, 24–36. [Google Scholar] [CrossRef] [PubMed]
- Combes, A.; Hajage, D.; Capellier, G.; Demoule, A.; Lavoué, S.; Guervilly, C.; Da Silva, D.; Zafrani, L.; Tirot, P.; Veber, B.; et al. Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Distress Syndrome. N Engl J Med 2018, 378, 1965–1975. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Su, F.; Zhang, N.; Wu, H.; Shen, Y.; Liu, H.; Li, X.; Li, Y.; Xie, K. The Impact of the New Acute Respiratory Distress Syndrome (ARDS) Criteria on Berlin Criteria ARDS Patients: A Multicenter Cohort Study. BMC Med 2023, 21, 456. [Google Scholar] [CrossRef]
- Rizzo, A.N.; Aggarwal, N.R.; Thompson, B.T.; Schmidt, E.P. Advancing Precision Medicine for the Diagnosis and Treatment of Acute Respiratory Distress Syndrome. JCM 2023, 12, 1563. [Google Scholar] [CrossRef]
- Peek, G.J.; Clemens, F.; Elbourne, D.; Firmin, R.; Hardy, P.; Hibbert, C.; Killer, H.; Mugford, M.; Thalanany, M.; Tiruvoipati, R.; et al. CESAR: Conventional Ventilatory Support vs Extracorporeal Membrane Oxygenation for Severe Adult Respiratory Failure. BMC Health Serv Res 2006, 6, 163. [Google Scholar] [CrossRef]
- Abdelbaky, A.M.; Elmasry, W.G.; Awad, A.H.; Khan, S.; Jarrahi, M. The Impact of High-Flow Nasal Cannula Therapy on Acute Respiratory Distress Syndrome Patients: A Systematic Review. Cureus 2023. [CrossRef]
- Gershengorn, H.B.; Hu, Y.; Chen, J.-T.; Hsieh, S.J.; Dong, J.; Gong, M.N.; Chan, C.W. The Impact of High-Flow Nasal Cannula Use on Patient Mortality and the Availability of Mechanical Ventilators in COVID-19. Annals ATS 2021, 18, 623–631. [Google Scholar] [CrossRef]
- Grieco, D.L.; Chen, L.; Brochard, L. Transpulmonary Pressure: Importance and Limits. Ann Transl Med 2017, 5, 285. [Google Scholar] [CrossRef] [PubMed]
- Frat, J.-P.; Thille, A.W.; Mercat, A.; Girault, C.; Ragot, S.; Perbet, S.; Prat, G.; Boulain, T.; Morawiec, E.; Cottereau, A.; et al. High-Flow Oxygen through Nasal Cannula in Acute Hypoxemic Respiratory Failure. N Engl J Med 2015, 372, 2185–2196. [Google Scholar] [CrossRef]
- Oczkowski, S.; Ergan, B.; Bos, L.; Chatwin, M.; Ferrer, M.; Gregoretti, C.; Heunks, L.; Frat, J.-P.; Longhini, F.; Nava, S.; et al. ERS Clinical Practice Guidelines: High-Flow Nasal Cannula in Acute Respiratory Failure. Eur Respir J 2022, 59, 2101574. [Google Scholar] [CrossRef]
- Nava, S.; Navalesi, P.; Conti, G. Time of Non-Invasive Ventilation. Intensive Care Med 2006, 32, 361–370. [Google Scholar] [CrossRef]
- Hultström, M.; Hellkvist, O.; Covaciu, L.; Fredén, F.; Frithiof, R.; Lipcsey, M.; Perchiazzi, G.; Pellegrini, M. Limitations of the ARDS Criteria during High-Flow Oxygen or Non-Invasive Ventilation: Evidence from Critically Ill COVID-19 Patients. Crit Care 2022, 26, 55. [Google Scholar] [CrossRef]
- Van Der Ven, F.-S.L.I.M.; Valk, C.M.A.; Blok, S.; Brouwer, M.G.; Go, D.M.; Lokhorst, A.; Swart, P.; Van Meenen, D.M.P.; Paulus, F.; Schultz, M.J.; et al. Broadening the Berlin Definition of ARDS to Patients Receiving High-Flow Nasal Oxygen: An Observational Study in Patients with Acute Hypoxemic Respiratory Failure Due to COVID-19. Ann. Intensive Care 2023, 13, 64. [Google Scholar] [CrossRef]
- Ranieri, V.M.; Rubenfeld, G.; Slutsky, A.S. Rethinking Acute Respiratory Distress Syndrome after COVID-19: If a “Better” Definition Is the Answer, What Is the Question? Am J Respir Crit Care Med 2023, 207, 255–260. [Google Scholar] [CrossRef]
- Del Sorbo, L.; Nava, S.; Rubenfeld, G.; Thompson, T.; Ranieri, V.M. Assessing Risk and Treatment Responsiveness in ARDS. Beyond Physiology. Am J Respir Crit Care Med 2018, 197, 1516–1518. [Google Scholar] [CrossRef]
- El-Khatib, M.F.; Karam, C.J.; Zeeni, C.A.; Husari, A.W.; Bou-Khalil, P.K. Oxygenation Indexes for Classification of Severity of ARDS. Intensive Care Med 2025. [Google Scholar] [CrossRef]
- Catozzi, G.; Pozzi, T.; Nocera, D.; Camporota, L. Oxygenation Indexes for Classification of Severity of ARDS. Authors’ Reply. Intensive Care Med 2025. [Google Scholar] [CrossRef]
- Matthay, M.A.; Ware, L.B.; Riviello, E.D.; Wick, K.D.; Thompson, T.; Martin, T.R. Reply to Liufu et al. and to Palanidurai et Al. Am J Respir Crit Care Med 2024, 209, 1280–1280. [Google Scholar] [CrossRef]
- Brown, S.M.; Grissom, C.K.; Moss, M.; Rice, T.W.; Schoenfeld, D.; Hou, P.C.; Thompson, B.T.; Brower, R.G. Nonlinear Imputation of Pao2/Fio2 From Spo2/Fio2 Among Patients With Acute Respiratory Distress Syndrome. CHEST 2016, 150, 307–313. [Google Scholar] [CrossRef]
- Rice, T.W.; Wheeler, A.P.; Bernard, G.R.; Hayden, D.L.; Schoenfeld, D.A.; Ware, L.B. Comparison of the Sp o 2 /F Io 2 Ratio and the Pa o 2 /F Io 2 Ratio in Patients With Acute Lung Injury or ARDS. Chest 2007, 132, 410–417. [Google Scholar] [CrossRef]
- Costamagna, A.; Pivetta, E.; Goffi, A.; Steinberg, I.; Arina, P.; Mazzeo, A.T.; Del Sorbo, L.; Veglia, S.; Davini, O.; Brazzi, L.; et al. Clinical Performance of Lung Ultrasound in Predicting ARDS Morphology. Ann. Intensive Care 2021, 11, 51. [Google Scholar] [CrossRef] [PubMed]
- Mongodi, S.; Chiumello, D.; Mojoli, F. Lung Ultrasound Score for the Assessment of Lung Aeration in ARDS Patients: Comparison of Two Approaches. Ultrasound Int Open 2024, 10, a–2421. [Google Scholar] [CrossRef] [PubMed]
- Smit, M.R.; Brower, R.G.; Parsons, P.E.; Phua, J.; Bos, L.D.J. The Global Definition of Acute Respiratory Distress Syndrome: Ready for Prime Time? Am J Respir Crit Care Med 2024, 209, 14–16. [Google Scholar] [CrossRef]
- Riviello, E.D.; Pisani, L.; Schultz, M.J. What’s New in ARDS: ARDS Also Exists in Resource-Constrained Settings. Intensive Care Med 2016, 42, 794–796. [Google Scholar] [CrossRef]
- Erlebach, R.; Pale, U.; Beck, T.; Markovic, S.; Seric, M.; David, S.; Keller, E. Limitations of SpO2 / FiO2-Ratio for Classification and Monitoring of Acute Respiratory Distress Syndrome—an Observational Cohort Study. Crit Care 2025, 29, 82. [Google Scholar] [CrossRef]
- Pham, T.; Pesenti, A.; Bellani, G.; Rubenfeld, G.; Fan, E.; Bugedo, G.; Lorente, J.A.; Fernandes, A.D.V.; Van Haren, F.; Bruhn, A.; et al. Outcome of Acute Hypoxaemic Respiratory Failure: Insights from the LUNG SAFE Study. Eur Respir J 2021, 57, 2003317. [Google Scholar] [CrossRef]
- Alipanah-Lechner, N.; Cavalcanti, A.B.; Diaz, J.; Ferguson, N.D.; Myatra, S.N.; Calfee, C.S. From Berlin to Global: The Need for Syndromic Definitions of Acute Respiratory Distress Syndrome. Am J Respir Crit Care Med 2024, 209, 21–23. [Google Scholar] [CrossRef]
- Palanidurai, S.; Chan, Y.H.; Mukhopadhyay, A. “PEEP-Adjusted P/F Ratio” in Acute Respiratory Distress Syndrome: A Call for Further Enhancement of Global Definition. Am J Respir Crit Care Med 2024, 209, 1279–1280. [Google Scholar] [CrossRef]
- Nishiyama, K.; Ichikado, K.; Anan, K.; Nakamura, K.; Kawamura, K.; Suga, M.; Sakagami, T. The ROX Index (Index Combining the Respiratory Rate with Oxygenation) Is a Prognostic Factor for Acute Respiratory Distress Syndrome. PLoS ONE 2023, 18, e0282241. [Google Scholar] [CrossRef]
- Roca, O.; Messika, J.; Caralt, B.; García-de-Acilu, M.; Sztrymf, B.; Ricard, J.-D.; Masclans, J.R. Predicting Success of High-Flow Nasal Cannula in Pneumonia Patients with Hypoxemic Respiratory Failure: The Utility of the ROX Index. Journal of Critical Care 2016, 35, 200–205. [Google Scholar] [CrossRef]
- Bos, L.D.J.; Laffey, J.G.; Ware, L.B.; Heijnen, N.F.L.; Sinha, P.; Patel, B.; Jabaudon, M.; Bastarache, J.A.; McAuley, D.F.; Summers, C.; et al. Towards a Biological Definition of ARDS: Are Treatable Traits the Solution? ICMx 2022, 10, 8. [Google Scholar] [CrossRef] [PubMed]
- Beitler, J.R.; Goligher, E.C.; Schmidt, M.; Spieth, P.M.; Zanella, A.; Martin-Loeches, I.; Calfee, C.S.; Cavalcanti, A.B. ; The ARDSne(x)t Investigators Personalized Medicine for ARDS: The 2035 Research Agenda. Intensive Care Med 2016, 42, 756–767. [Google Scholar] [CrossRef] [PubMed]
- Al-Husinat, L.; Azzam, S.; Al Sharie, S.; Araydah, M.; Battaglini, D.; Abushehab, S.; Cortes-Puentes, G.A.; Schultz, M.J.; Rocco, P.R.M. A Narrative Review on the Future of ARDS: Evolving Definitions, Pathophysiology, and Tailored Management. Crit Care 2025, 29, 88. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



