Submitted:
07 May 2025
Posted:
08 May 2025
You are already at the latest version
Abstract
Background: Xenotransplantation from genetically modified pigs is emerging as a potential solution to organ shortages, yet, faces religious and cultural barriers, particularly, in the Muslim and Jewish communities whose religions prohibit using pigs for consumption, commerce, and medical treatment. While exceptions exist for life-saving cases, research addressing public perceptions and religious concerns remains limited, obstructing medically informed decisions by these populations. Objectives: The primary research aim was to assess the level of knowledge among Muslim and Jewish individuals regarding religious rulings on the use of porcine organs in medical situations. Additionally, the study evaluated participants’ personal attitudes toward the acceptability of such use. Methods: A cross-sectional survey was conducted using a structured questionnaire completed by 884 Muslim and 916 Jewish participants. The questionnaire examined two main domains: (1) knowledge of religious doctrines concerning the permissibility of pig-derived organ transplantation, and (2) personal attitudes toward the ethical and religious acceptability of such procedures. Results: The results demonstrated a low level of awareness among both Muslim and Jewish participants regarding the religious permissions for medical use of porcine organs. A majority in both groups expressed opposition to pig-derived xenotransplantation. Importantly, the data revealed a strong association between the participants’ knowledge of religious rulings and their attitudes toward such medical interventions. Conclusion: This study reveals a critical gap in public understanding about religious exemptions for life-saving porcine organ transplantation within Muslim and Jewish communities. The findings emphasize the need for better education and culturally sensitive informed consent to support ethically grounded medical decisions regarding xenotransplantation.
Keywords:
religious attitudes
; healthcare decisions
; porcine transplant
1. Introduction
There are some 1.6 billion Muslims in the world, which make up 23% of the world's estimated population of 8.1 billion. The size of the Jewish world population is 15.7 million, which was 0.227% of the world's population in 2023 [1]. Many adherents of these religious faith groups live in Western countries where they constitute an ethnic minority, that must be accommodated by medical treatment in accordance with their beliefs and values. In light of the growing importance of patient-centered care worldwide, this article focuses on the need to adapt medical care for Muslim and Jewish transplant patients when the transplanted organ is derived from pigs, an animal considered ritually impure according to both Islam and Judaism [2,3].
There are still no studies examining the knowledge and attitudes of Muslim and Jewish patients towards the use of organs from the pig. Due to the progress of clinical trials in the past two years using organs derived from pigs and prospects for their use in the future, it is important to examine the theological views of Islam and Judaism on this issue and to explore how the religious rulings of Islamic and Jewish authorities relate to the importance of human health, and the use of pigs for medical purposes [4].
Nearly 37 million adults in the United States are afflicted with chronic kidney disease (CKD), and of these, 786,000 have been diagnosed with end-stage renal disease (ESRD). For individuals with ESRD, the wait for life-saving transplants is a race against time [5]. Xenotransplantation from pigs to humans, an emergent field in medical science to remedy this shortfall, has its roots in extensive research of into pig-to-baboon transplants conducted over the last fifty years [6]. In the 1990s and even earlier, pigs were recognized as favorable candidates for xenotransplantation. This recognition was based on their plentiful population, relative ease of breeding, and a projected higher acceptance among the public when compared to non-human primates. Furthermore, pigs are deemed particularly suited for organ donation given the anatomical and size compatibility of their organs with those of human recipients. This perspective is supported by the research of Mohiuddin [6] and reiterated in the findings of Cooper [7].
For more than a century, xenotransplantation has been seen as a potential way to treat disease. The interest in xenotransplantation was renewed, particularly, by the successful implementation of a heart transplant in a person with heart failure [8]. The world's first human-to-human pig heart transplant was performed at the University of Maryland School of Medicine in the US, where a genetically modified pig heart was successfully transplanted into a 57-year-old man in the final stages of heart disease. The historic operation overcame the biggest possible obstacle caused by hyperacute immune rejection and achieved a good short-term result. But the patient's condition began to deteriorate, and he died two months after the transplant [8,9,10,11].
A few months after the heart transplant, a man in his 50s who agreed to enter an experimental study was declared brain dead and suffering from acute kidney injury superimposed on a history of CKD (stage 2) and hypertension underwent bilateral nephrectomy and termination of dialysis followed by xenotransplantation with 10 genes matched with pig kidneys [12,13,14].
Organs of porcine origin used for medical purposes are regulated as medical use or as a medicinal product [15]. Animal-derived implants are surgical products that are inserted into the body, such as heart transplants, heart valves, kidney, skin, cartilage, meshes used to repair hernias, and spacers used in orthopedic surgeries [16]. The field of xenotransplantation largely developed from experiments using pig tissue and organs, since these cause less immunogenic dangers to human recipients [17]. Transplantation of organs from genetically modified pigs may compensate for the severe shortage of human-donated organs and allow patients to overcome the risks associated with long periods of waiting for a transplant[18,19]. Our article mentions transplantation of pig-derived organs such as, heart, lungs, kidney, pancreas, cartilage and skin, but, there are additional uses, i.e., including common medications using materials derived from pigs.
The pharmaceutical landscape encompasses a broad range of medications and treatments, including anticoagulants like omepradex [20], warfarin sodium for the prevention and management of thrombosis, analgesics for pain relief, anti-thrombotic agents [21,22], digestive aids and supplements, myostatin inhibiting compounds [22], digestive health supplements [23], gelatin-based pharmaceutical capsules, medications with lipid content [24,25], porcine mesh implants utilized in burn treatments, cardiac valve repair, myocardial applications [26,27,28], biological products for knee arthroscopy applications [26,27,28,29], bioprosthetic heart valve (BHV) replacements [30], xenograft treatments employing porcine skin for burn recovery [31], and many others [32,33].
To achieve the gold standard of patient-centered medical care, it is crucial to develop cultural competence by studying religious doctrines that prohibit the use of certain animals for medical treatments. According to a leading medical ethicist, Daniel Rodger [34], the use of medical products derived from animals without obtaining the patients' informed consent violates the principle of respect for their autonomy, hence, the physician's duty to provide full information about the treatment during the informed consent process [20]. However, obtaining consent from each patient is considered controversial, since some physicians and ethicists would argue that it is burdensome and unnecessary. Moreover, in many cases where revealing supplementary ingredients is not required by law, physicians do not have the full information, especially as regards drug treatment [35].
A recent article reports that only 25 percent of the 308 British surgeons who participated in the survey correctly identified the biological derivatives of various surgical products [36]. Not informing a patient about the source of a medical product can be considered a violation of section 9 of the UK Human Rights Act of 1988, which states that "Everyone has the right to express his religion or belief, in worship, teaching, practice, and religious commandment” [37]. Some patients may refuse to use these drugs and medical devices derived from animals because of their religious beliefs, causing non-adherence to medication [24,37,38,39]. However, when xenotransplantation, using porcine material, is the only way to save a life, it is allowed in both Islam and Judaism by almost all religious scholars and according to most interpretations [26,27,28,37].
The ingestion of drugs containing inert ingredients derived from pork products may offend Muslim and Jewish patients [28,35]. Prescribing such medicines and offering vaccines and medical devices to patients with religious prohibitions on the consumption of pork products may undermine the ethical standards both of patients who belong to these religions and of the doctors treating them. The importance of informing patients about prescribed medical treatment and options is reflected in the Montgomery ruling, which shifts the emphasis from what doctors would agree is reasonable disclosure to what a reasonable patient would expect to know. According to this ruling, the patients must be given all the relevant information by their doctor, even if the doctor is aware that by doing so, it may cause the patients to make a decision that does not serve their best interests [35]. However, a significant number of surgeons do not discuss with patients and do not document the use of biological products before surgery with them [40].
The Quran specifically outlines prohibitions against the consumption of specific items, categorizing carrion, blood, and swine flesh as impure (Holy Quran. 5:3, 6:145). It extends these prohibitions to encompass animals that die of natural causes, any meat sacrificially offered to deities apart from Allah, along with the abovementioned categories. The scholarly exploration of these Islamic dietary laws by Easterbrook and Maddern [37] underscore that Islamic doctrine prioritizes the preservation of human life, elevating this principle above other religious mandates, as elaborated by Hedayat and Pirzadeh [41]. Significantly, the Quran recognizes situations where necessities may supersede prohibitions. Thus, while the consumption of pork is generally forbidden, exceptions are considered permissible in specific scenarios lacking lawful alternatives (Holy Quran. 5:3, 2:173, 6:145, 16:115). In medical contexts, engaging a patient’s religious advisor becomes imperative in decision-making processes when faced with no other viable options [42].
Notwithstanding Islamic doctrine, paralleling Judaic principles with the pronounced prohibition against the consumption of porcine products, as well as carrion and blood, the sanctity and inherent value of life holds supreme importance, fostering the conviction that the preservation of life is a fundamental moral obligation [43]. This principle is further reinforced by the Quranic assertion pronounced by Allah that "necessities may override prohibitions." Hence, while the dietary restriction against pork is unequivocally stated, using pork may be considered permissible under certain circumstances where lawful alternatives are absent, demonstrating the flexibility of Islamic law when life is at stake.
The consumption of pork is widely known to be prohibited to Jews and thus, generally avoided. The Hebrew Bible (Tanakh) states that pigs ". . . are unclean. . . . You shall not eat their flesh, and you shall not touch their carrion; they are unclean to you." (Leviticus 11:7-8). In Judaism, it is a divine commandment to save a life, to treat illness, to alleviate suffering, and to ensure that everything possible is done for the sick [44]. Therefore, all medical decisions must be in the best interest of the patient, and the safest and most gentle treatment must always be the preferred option to achieve the higher good of protecting life [45]. However, there is a widespread belief that transplanting porcine products into a patient practicing Judaism is prohibited. Yet, in fact, there is no prohibition that states that it is forbidden to use pigs to cure diseases or to save human life. Therefore, it is legitimate for members of the Jewish faith to do so until science finds a suitable substitute [46].
Some Jews associate taboos with all aspects of the use of pigs and porcine products and fear to use them, despite the lack of a religious law prohibiting its use in medicine. In situations where porcine products are to be used, most Jewish patients will want to know or follow their rabbi's interpretation of the Jewish law [halakha] on the subject. Islamic and Jewish laws prohibit the breeding and consumption of pigs, hence, the erroneous belief that the transplantation of pig organs to practicing Jews and Muslims would be prohibited by their clergy [3,47]. However, the use of xenografts of pig's organs is not considered equivalent to eating a pig, but, rather a significant health benefit derived from pigs and a life saver [26]. It is worth noting that both religions allow exceptions to dietary prohibitions for the ultimate goal of saving lives [3,47].
Muslim law that permits such exceptions invoke the ethical-legal concept of Darūrah to cancel a normative prohibition when there is a danger to life or similar distress, when there is no alternative solution and the harm does not outweigh the benefit [19,26,28,29,48]. An analysis of seventy English-language Sunni e-fatwas (online religious rulings) revealed that pig organs can only be used in emergency and life-saving cases [42].
A well-known Hadith reported that the Prophet stated: "Allah has ordained both illness and its remedy. For every ailment, He has designated a corresponding cure. Therefore, pursue medical treatment, but, refrain from utilizing anything that is deemed unlawful” [49]. The works of Fadel, reference the pronouncement attributed to Prophet Muhammad that asserts: "For every ailment, God has fashioned a cure, with the sole exception of senility [interpreted as 'death']” [50,51,52].
Before using material originating from pigs, it must go through a process of Istihala (transformation and complete conversion of one material into another material to the extent that it becomes a completely new material) when it is no longer considered a pig after which the product or organ can be used [3,26,28,29,53]. However, Istihala is not accepted by all Sunni schools and streams. Some theologians do not agree that the pig is subject to purification through Istihala; others do not believe that pig gelatin undergoes a change that is sufficient to produce permissible vaccines [54,56].
In Jewish law, when pigs are used to save lives, all religious prohibitions are suspended because it is permissible to violate the rules for preserving human life. [45,47,57]. It is important to note that the opinion of one religious leader may differ from that of other leaders of the same religion. It should also be recognized that both Judaism and Islam have subdivisions with certain differences in their positions and interpretations of religious laws [25,58]. This is, perhaps, a reason for the lack of clear advice from professional associations or ethics committees as to guide doctors and surgeons in such situations where the medical need contradicts the patient's religious beliefs [59].
In a review of thirty-five surveys on xenotransplantation, it was found that the majority of respondents who opposed xenotransplantation did so on the basis of religious belief [60]. A survey that included one hundred patients, thirteen of whom were Muslim, indicated that sixty-three patients believed that doctors must inform patients that the medicine they are recommending may contain ingredients that are prohibited by their religion. In addition, 35 percent of these patients believed that other healthcare providers (i.e., pharmacists or nurses) should also provide them with this information [61].
Another survey focusing on xenotransplantation found that most hemodialysis patients preferred to wait for a kidney from a human cadaver instead of receiving a xenotransplant. Two of the patients who strongly objected to receiving a xenograft did so on the grounds of their Muslim faith [62]. Eriksson et al [20] contacted religious leaders and asked their opinion as to the use of substances of animal origin for medical purposes. They found that all participants, including the Muslim and Jewish leaders, accepted the use of all products in life-threatening situations, but, only when there were no alternatives.
In Jewish ethics, the ethical framework is the principle of pikuach nefesh, which posits that the preservation of human life supersedes most religious laws. Consequently, in situations where the use of a porcine medical product is essential for saving life, religious prohibitions are set aside. Consultations with rabbinic authorities confirm that while The consumption of pork is prohibited within Judaism, the utilization of porcine-derived products in medical treatments is not forbidden. This nuanced understanding of religious law was explored in the works of Easterbrook and Maddern [37] and further elaborated by Rosner [63]. For this reason, animals may be used to serve the life and dignity of human beings, both for health-promoting and medical purposes [44,64].
Human beings are accorded a distinctive and elevated dignity in Judaism, rooted in the belief that they are created "in the image of God." This exalted valuation of human life is mirrored in the moral doctrines of the Talmud, which state: "Adam [the progenitor of humanity] was created singly to teach that whoever destroys a single life is as if they have destroyed an entire world, and whoever saves a single life is as if they have saved an entire world." (Babylonian Talmud, Sanhedrin, 37a). In this context, the use of genetically engineered pigs as kidney donors aligns with the maxim "whoever saves a single life saves the entire world," receiving endorsement from prominent Jewish legal scholars. The utilization of porcine aortic valves for transplantation has gained universal acceptance and is permitted by leading rabbinical authorities, as noted by Rabbi Moshe Feinstein [65]. Historical precedents as far back as the 1500s indicate rabbinical support for the use of animals in medical research, including testing the health benefits and side effects of new drugs [63].
According to Jewish law, any commandment in the Bible, with the exceptions of idolatry, murder, and forbidden sexual relationships, may be transgressed to save a life. This doctrine implies that utilizing pig organs to save human lives does not constitute a violation of religious law [66]. Thus, the use of porcine products to improve health reflects the value of human life as stated in Leviticus 18:5: “You shall keep My statutes and My laws, which a person shall do and live by them". The traditional rabbinical interpretation of the phrase “and live by them” emphasizes the Jewish view that preservation of life and health is paramount in Jewish law. For decades, rabbis have sanctioned the use of insulin derived from pigs for diabetics in addition to the transplantation of porcine heart valves, as documented by Loike and Krupka [64] and Hunter [67].
Muslim and Jewish patients may experience distress when a medicine or organ transplant derived from pigs is recommended by the attending physician for fear of violating religious prohibitions. Despite the importance of this issue, there is little empirical data that investigates the knowledge of Muslims and Jews regarding the permissibility of these treatments and their attitude towards the use of these substances. A study that examined attitudes regarding the use of intraoperative biological products among patients from different religious backgrounds revealed that 37 percent of the Muslim participants opposed this option [40].
The current study aims to fill the gap in the literature and describe the results of a large-scale research project conducted on this topic in Israel, where 73.9 percent of its citizens are Jewish, 21.1 percent are Muslim, and 1.9 percent are Christian [68]. Specifically, we seek to answer the following research questions
(1) What do Muslims and Jews know about the permissible use of organs of porcine origin for medical purposes?
(2) What is the opinion of Muslims and Jews regarding the permissibility of using organs of porcine origin for medical purposes?
(3) Is thinking that the use of organs of porcine origin for medical purposes is permissible positively correlated with a positive attitude towards it? And conversely, is thinking that the use of organs of porcine origin for medical purposes is prohibited negatively correlated with a positive attitude towards it?
(4) Is there a difference between the knowledge of Muslims and that of Jews regarding the permissibility of using organs derived from pigs for medical purposes?
(5) Is there a difference between the opinions of Muslims and the opinions of Jews regarding the permissibility of using organs derived from pigs for medical purposes?
We describe the methodological aspects of the study. Then we will present the results of the survey we conducted, and finally, we will discuss the meaning of these results and their practical implications.
2. METHODS
2.1. Participants
The study focused on a diverse sample of Jewish and Muslim Israelis, with different levels of religious observance, age, socio-economic status, and educational background. Snowball and convenience sampling methods were used, with participants recruited through an advertisement posted on social media who agreed to fill out an online questionnaire. Prior to the study, the researchers had no previous interaction with the participants who were informed that the study concerned the medical applications of organ transplantation from rodents. The main inclusion criterion was that participants must be at least eighteen years old. The study included 884 Muslim and 916 Jewish participants, a total of 1,800 people.
Demographic characteristics of the sample are as follows, with Muslim information first and Jewish information following inside the parentheses: 427 (457) which are 48.3% (49.9%) males in the sample; the rest are female. There are 439 (435) which are 49.7% (47.5%), without academic education; the rest have academic education. There are 402 (450) which are 45.5% (49.1%) secular (non-religious) individuals; the rest are religious. Most of the participants are in a relationship of some kind (e.g., married), that is 798 (759) which are 90.3% (82.9%) individuals, while the rest are not in a relationship (e.g., divorced). In terms of age, the respondents are between 18-81 years with a mean of 49.41 (51.13) and a standard deviation of 20.43 (20.78). As for number of children, Muslim families had between 0-13 children, with a mean of 4.43 and a standard deviation of 2.84; Jewish families had between 0-10 children, with a mean of 3.96 and a standard deviation of 2.73.
2.2. Measures
We composed the research questionnaire that was then validated by five experts in the field, and afterwards translated into English, Hebrew, and Arabic. We conducted a pilot study on 40 participants to test the factor analysis =0.78. The questionnaire is made up of three parts: the first part included demographic data, age, gender, education, religion, level of religiosity, family status, number of children. The second part examined the level of knowledge and awareness regarding organ donation from a religious point of view. The third part asked respondents to express their opinion on whether, from a religious point of view, it is permissible to use the organs of a pig.
The research questionnaire presents six types of pig organ transplants: heart, lung, kidney, pancreas, knee cartilage, and skin. We included organ transplants, some of which were used for saving lives and some not. The respondents were asked to respond to each medical treatment twice: first, to express their knowledge to what extent each pig-based treatment is allowed according to their religion, on a six-point Likert scale, with an additional optional answer "I know" or "I don't know". Second, they were asked to state on a seven-point Likert scale the extent to which they believe that pig-based treatment should be allowed according to their religion (Appendix B to the research questionnaire). Two indices were constructed by averaging the responses regarding six organ transplants from a pig, with reference to the participants’ knowledge of permissibility and similarly, the average of the responses to six organ transplants regarding their opinion of whether these uses should be permitted.
2.3. Ethical approval
The study was approved by the appropriate institutional review board: approval number 2022-1081. Respondents signed informed consent forms to participate in the survey and allow the research team to use their data.
2.4. Data analysis
Statistical analyses were conducted using the statistical package SPSS-PC (v28). Prior to data analysis, data cleaning and distribution characteristics including normality checks were conducted. Descriptive statistics were used to describe the sample. We designed a path analysis model to explain the attitude towards the use of materials derived from pigs for medical purposes. The level of significance was set to p<0.05.
3. Results
As previously mentioned, the Knowledge and Opinion measures consist of 6 corresponding items each. Table 1 presents the means and standard deviations of each of the items and the zero-order correlations between each dyadic set of items. Additionally, to assess statistical differences in correlation coefficients between the two samples, Fisher’s Z tests were used. Table 1 also includes results of independent-samples t-tests to compare item-wise means between the samples. These means are also depicted in Figure 1.
Table 1 indicates that there are significant differences between the correlations of items from both measures in the Jewish and the Muslim samples, as follows; the correlation between: (1) items 1 (i.e., item 1 in Knowledge and item 1 in Opinion) is stronger in the Muslim sample, (2) items 2 is stronger in the Muslim sample, (3) items 3 is stronger in the Jewish sample, (4) items 4 is stronger in the Muslim sample, (5) items 5 is stronger in the Muslim sample, and (6) items 6 is stronger in the Muslim sample,
As can be seen in Table 1, most of the item-wise means are not significantly different between groups/samples, apart from: (1) Item 3 in Knowledge (Jewish > Muslim), (2) Item 6 in Knowledge (Muslims > Jews), (3) Item 2 in Opinion (Muslims > Jews), (4) Item 5 in Opinion (Muslims > Jews), and (5) Item 6 in Opinion (Muslims > Jews). Moreover, to test the difference in Knowledge and Opinion (as total latent variables) between the Muslim and the Jewish groups, One-way MANOVA (multivariate analysis of variance) was used. Religion does not have a general significant effect on the variables: F(2, 1797) = 1.46, p = .234, Wilk’s = .99. As such, further (specific) F-tests and results are not displayed further. Also, in order to enhance the understanding of the underlying factors predicting the changes in Opinion, firstly a correlation matrix was gleaned from the data (Table 2).
Furthermore, path analysis and SEM (structural equation modeling) with Multiple-Group Comparison were employed to test a mediation model, in which the demographic parameters act as predictors; the Knowledge is the mediator, and the Opinion is the criterion. The model boasts fit in the absolute sense [69] apart from the chi-square test: 2(8) = 16.72, p = .008, 2/df = 2.09, SRMR = .08, CFI = .95, GFI = .98, NFI = .96, TLI = .95, RMSEA (90% CI) = .07 (.03-.12), p-close = .308. In addition, in the path analysis, bootstrapping method was used to assess the mediation effect (5,000 resamples, 95% bias-corrected confidence interval). The results of the analyses for both samples, are depicted in Table 5 and Table 6 and Figure 2. Also, Z-tests were used to test the statistical significance of the differences between path coefficients from both samples respectively (i.e., whether a certain path coefficient is significantly different in one sample as opposed to the other).
Table 5 and Table 6 indicate that Muslims and Jews exhibit quite different path coefficients (i.e., the association between age and Opinion is negative in the Muslim sample, = -.48, but is positive in the Jewish sample, = .24). It is evident that most of the associations are statistically significant, apart from very few (marked in bold in Table 3)
Moreover, as can be seen in Table 4, most of the indirect effects were significant (i.e., the zero is outside the confidence interval’s limits), rendering Knowledge to be a partial mediator between the set of predictors (age, gender, education, religiosity, marital status, number of children) and the criterion (i.e., Opinion), apart from one instance in which the path was not statistically significant.
Table 5 and Table 6 indicate that Muslims and Jews exhibit quite different path coefficients (i.e., the association between age and Opinion is negative in the Muslim sample, = -.48, but is positive in the Jewish sample, = .24). It is evident that most of the associations are statistically significant, apart from a very few (marked in bold in Table 3). Moreover, as can be seen in Table 4, most of the indirect effects were significant (i.e., the zero is outside the confidence interval’s limits), rendering Knowledge to be a partial mediator between the set of predictors (age, gender, education, religiosity, marital status, number of children) and the criterion (i.e., Opinion), apart from one instance in which the path was not statistically significant.

Table 5.
Path analysis results with standardized regression coefficients and difference tests.
| Muslim (n = 884) | Jewish (n = 916) | Difference test | |||||
| Path | Sig. | Sig. | Z-scores | ||||
| Age | → | KNOWLEDGE | -.90 | .000 | .29 | .000 | 19.07*** |
| Gender | → | KNOWLEDGE | -.12 | .000 | -.05 | .000 | 2.37** |
| Education | → | KNOWLEDGE | .10 | .000 | .29 | .000 | 6.02*** |
| Religiosity | → | KNOWLEDGE | .19 | .000 | .51 | .000 | 8.99*** |
| Marital Status | → | KNOWLEDGE | .32 | .000 | -.26 | .000 | 17.26*** |
| Children | → | KNOWLEDGE | -.05 | .282 | .56 | .000 | 8.97*** |
| Age | → | OPINION | -.48 | .000 | .24 | .000 | 21.97*** |
| Gender | → | OPINION | -.01 | .186 | -.04 | .000 | 1.97** |
| Education | → | OPINION | -.03 | .000 | .05 | .000 | 5.17*** |
| Religiosity | → | OPINION | .01 | .718 | .20 | .000 | 9.77*** |
| Marital Status | → | OPINION | -.17 | .000 | .15 | .000 | 18.30*** |
| Children | → | OPINION | -.31 | .000 | .01 | .848 | 10.31*** |
| Knowledge | → | OPINION | .15 | .000 | .65 | .000 | 19.46*** |
*p < .05, **p < .01, ***p < .001. Children = number of children. Gender: 0 = female, 1 = male. Education: 0 = not academic, 1 = academic. Religiosity: 0 = secular, 1 = religious. Marital status: 0 = no relationship, 1 = in a relationship.
Table 6.
Mediation (indirect) effects analyses.
| Muslim (n = 809) | Jewish (n = 714) | |||||||||||
| Path | Eff. | LL | UL | Sig. | Eff. | LL | UL | Sig. | ||||
| Age | → | KNOWLEDGE | → | OPINION | -.13 | -.19 | -.09 | .001 | .19 | .14 | .25 | .000 |
| Gender | → | KNOWLEDGE | → | OPINION | -.02 | -.03 | -.01 | .000 | -.03 | -.06 | -.01 | .020 |
| Education | → | KNOWLEDGE | → | OPINION | .02 | .01 | .03 | .000 | .19 | .15 | .22 | .000 |
| Religiosity | → | KNOWLEDGE | → | OPINION | .03 | .02 | .04 | .000 | .33 | .30 | .37 | .000 |
| Marital Status | → | KNOWLEDGE | → | OPINION | .05 | .03 | .07 | .000 | -.17 | -.21 | -.13 | .000 |
| Children | → | KNOWLEDGE | → | OPINION | -.01 | -.02 | .01 | .321 | .38 | .30 | .43 | .001 |
Analyses used bootstrapping (95% bias-corrected, 5,000 resamples). Eff. = standardized indirect effect (predictor→through mediator→criterion). LL = lower limit of the confidence interval; UL = upper limit of the confidence interval. Children = number of children. Gender: 0 = female, 1 = male. Education: 0 = not academic, 1 = academic. Religiosity: 0 = secular, 1 = religious. Marital status: 0 = no relationship, 1 = in a relationship.
The coefficients presented in the path analysis indicate that among the Muslims, the participants are younger people. Those who are less educated, who report a higher level of religious observance, and who are not in a relationship had better knowledge about the permissibility of transplanting organs derived from pigs. Jewish participants were on average older. Those with less education, those reporting a lower level of religious observance, and those involved in a relationship had better knowledge about the permissibility of organ transplantation from pigs.
As for their opinion regarding whether organ transplantation from pigs should be allowed, younger Muslim participants, women, those less educated, those who report a higher level of observance of religious observance, and those who are in a relationship expressed a higher level of support for the opinion that transplants of these organs should be allowed. Among the Jewish participants, those who were older, female, less educated, report a higher level of observance, and are not in a relationship expressed greater support for this view. A positive beta coefficient between Knowledge and Opinion in both the Muslim and Jewish samples indicates that the more the participant believes that their religion permits transplantation of organs of porcine origin, the greater their support for the view that they should be permitted.
4. Discussion
Monotheistic faiths, specifically Islam and Judaism, hold the belief that God fashioned humans in His likeness and bestowed upon them sovereignty over all other forms of life. In practical terms, these religions generally endorse the practice of xenotransplantation, asserting that the preservation of human life takes precedence over any restrictions regarding the use of porcine biological materials. It is important to note, however, that there may be varying perspectives between liberal and conservative factions within these religious groups. A limited number of studies have explored the relationship between religious beliefs and attitudes towards xenotransplantation [8,58,70].
Extensive research has demonstrated that patients frequently turn to their religious faith as a means of coping with illness [17,26,38,71,72]. As a result, some individuals may refuse organ transplants from pigs, i.e., for use in heart valves or skin, and eschew pharmaceuticals derived from elements they consider to be in conflict with their religious doctrines, since, they did not undergo the Istihala transformation [38,61]. In Jewish dietary law, pork is explicitly prohibited in the Bible Leviticus 11 and Deuteronomy 14, which detail dietary restrictions. In Islam, the consumption of pork is similarly forbidden, with the Qur'an explicitly mentioning this prohibition in various verses, i.e., the Surat al-Baqarah (Sura 2, 172-173), and commenting on the prohibitions shared by Jews and Muslims, albeit critiquing the Jewish extension of these prohibitions beyond what is mandated (Sura 16, 115-118).
Considering the designation of pigs as impure in both Jewish and Muslim traditions, potential recipients of porcine-derived organ transplants may feel a significant aversion [16,73,74] Moreover, there is a notable risk of psychological harm to patients inadvertently treated with animal-derived substances [34]. Thus, our study aims to: 1) investigate Muslim and Jewish perspectives on the religious acceptability of utilizing pig-derived organs in medical treatments; 2) assess their views on the religious appropriateness of pig organ transplants; and 3) juxtapose and analyze the knowledge and opinions of Muslims and Jews on this matter.
Our research makes a substantial contribution to the evolving field of medical ethics, particularly, in acknowledging the increasing necessity for transparency in informed consent practices. This includes informing patients as to the precise nature of organ transplants and when there is reluctance, exploring non-biological alternatives [35,40,73].
This study is significant in several respects. Firstly, it is a comprehensive pioneering investigation into a broad spectrum of organ transplants from pigs. Secondly, the extensive participation of Jewish and Muslim individuals, adherents of the two principal monotheistic religions that view pigs as unclean, facilitates a comparative analysis of knowledge and attitudes within these communities. Thirdly, the research uniquely focuses on individuals' awareness of their religious stance on pig organ transplants- on whether they are deemed prohibited or permissible and how this awareness influences their perspectives on the use of pork products. This aspect offers insights into viewpoints regarding pig xenotransplants including those of hearts, lungs, kidneys, pancreases, knee cartilage, and skin.
Our study is the first large-scale comprehensive project to examine the extent to which Muslims and Jews believe that their religion allows medical organ transplantation based on organ transplantation porcine origin and to what extent they think these treatments should be permitted according to religious laws and rulings. Our findings indicate that the general public in both samples is unaware of the fact that life-saving organ transplantation based on pig organs is religiously permitted by almost all religious scholars and according to most interpretations. When we examined the knowledge of each respondent regarding the permissibility of materials derived from pigs, according to their religion for each of six organ transplants, for all Muslims 20.38% do not know and for all Jews 9.03% do not know, and about 28.136% of the respondents in both groups answered for each of these six transplants that they do not know. In addition the Jewish participants knew and believed more than their Muslim counterparts that their religion permits the use of porcine organs. They also believed that there was more awareness of the permissibility of these organ transplantations according to Jewish religious law than the Muslim participants.
Both the Jews and the Muslims approved the transplantation of organs to save lives according to the degree of danger. The uses of the life-saving organs of pigs included in our research questionnaire in both groups, ranked the transplantation in order of priority for saving lives: 1) heart transplantation 2) lung transplantation 3) kidney transplantation 4) pancreas transplantation; 5) knee cartilage transplantation; and 6) skin grafting. Another study carried out among the Jewish population regarding the use of porcine products indicated a higher ranking regarding heart valve transplantation, knee cartilage transplantation, and post-burn skin graft in a higher order of priority than the Muslim population [23,33,74].
Jewish respondents expressed a high level of support for the opinion that transplantation of porcine organs should be allowed in these life-saving situations. The Muslim respondents had a lower level of belief as to the permissibility of all the transplants presented in the questionnaire. These findings prove that it is very important for the doctor, surgeon, or transplant coordinator to understand that some considerations that they do not consider important, can be significant for the patient [20]. For some patients, fulfilling their religious, cultural and ethical beliefs may be more important than achieving an improvement in their physical health [61]. In some cases, the patient may wish to consult with a clergyman or religious leader. The medical staff must respect this request and delay treatment insofar as possible until the patient feels that he has received the appropriate advice [24,75].
The tendency to obey religious rulings is reflected in the positive Pearson correlations (as well as the beta coefficients in the path analysis) between the Knowledge and the Opinion indices: the more the respondent (both Muslim and Jewish) believed that a certain medical treatment originating from pigs was allowed, the higher their tendency to support this treatment. All these correlations were in the range of 0.61-0.92, with some being stronger among Muslims and some stronger among Jews, but both populations gave a higher rank and high support regarding the use of the vital organs that save lives in the order listed: heart, lungs, kidney, pancreas, knee cartilage and skin, in six Fisher's Z-tests. The Pearson's correlations were significantly different between Muslims and Jew.
Along with the strengths of this study, we acknowledge potential limitations. One of them refers to the fact that nuanced attitudes towards advanced organ transplants as described in our questionnaire may be too complicated to be assessed by conventional quantitative research methodology [60]. Another limitation concerns the potential self-selection bias that usually appears in volunteer sampling, when respondents who agreed to take part in the study may have different tendencies and attitudes towards the research topic than those who chose not to participate [33]. The important point is that a theologically informed XTx program is one that has the greatest potential to maximize benefits to patients' futures, and more likely to receive broad public support.
From an individual perspective, Judaism is not opposed to XTx to prolong and save human life, even with non-kosher animal donors with genetic modifications. The commandment in the Torah to "choose life" over death means that preservation of life trumps other values almost without exception. XTx, even from pigs, is welcomed as a life-sustaining medical intervention from a Jewish ethical perspective. Since human beings are allowed to use animals, including those defined as “unclean” to achieve greater human well-being, XTx can be justified in terms of promoting human health as long as human dignity and integrity are preserved. The pig is treated according to accepted ethical standards, and the risk ratio/ total benefit is presented to the patient.
The safest concluding comment as to the Sunni Islamic bioethical perspectives on XTx would be that, given the state of science, a final ethical-legal determination remains elusive and unclear. In general, it can be argued that there will be a conditional authorization for XTx as a therapeutic method given the following conditions: the therapeutic effects are lifesaving and the health benefits of the treatment outweigh its harms; the recipient is able to give informed consent based on a sufficient understanding of the risks involved.
4.1. Implications for practice
An awareness by the transplant medical staff and transplant coordinating nurses of the differences in religious beliefs can contribute to achieving quality patient-centered care. Both Islam and Judaism offer a remedy in their laws for permitting the forbidden in life-threatening and other extreme circumstances. Religious leaders and organ transplant doctors should find platforms for discussing these issues together and seeking solutions. At the same time, religious leaders should be brought up to date on the latest medical technologies that relate to using porcine products and organs so that they can make informed religious rulings in cases where there are no alternatives and failure to treat would result in death. Transplant physicians should similarly be alert to the religious sensitivities of their patients and be prepared to refer them to knowledgeable religious authorities so that their concerns and misgivings may be addressed, particularly, when there is religiously sanctioned permission to use the porcine organ or product. To respect patient autonomy, organ transplant coordinators should understand religious views and be sensitive to religious beliefs.
Surveys do not constitute direct dialogue with the public; interviews with clergymen and more importantly opinion leaders hold a greater impact. Moreover, public opinion is inherently dynamic, influenced by cultural and religious contextual factors and experiences. However, when survey results inform formal discussions and decisions, especially, for people outside academic or scientific circles, media narratives serve as a major conduit for information regarding scientific progress. Therefore, it is imperative to present issues in a way that offer the general public an accurate, comprehensive and unbiased understanding that presents the main points of view without being overly technical.
In terms of xenografts, there was no significant consensus among followers of Judaism and Islam, although opposition seemed to be gradually diminishing over time, influenced by various religious, educational and socio-economic factors. The effect of gender, education, and religious beliefs regarding the attitudes towards xenotransplantation mirrors trends observed in other fields such as the use of animals in biomedical research and biotechnology/genetic engineering applications. Providing information on alternative organ transplants available is part of informed consent. Knowing the patient's culture and religious belief is an extremely important factor in the interaction between doctor and patient to obtain informed consent for any medical treatment [26,75]. Failure to respect religious sensitivities on the use of biological products such as porcine organ transplants may have serious consequences, including litigation [57]. According to Rodger, informing the patient about the use of animal organs should become routine practice [34]. Similarly, we believe that Jewish and Muslim patients should be informed about transplants of reparative origin. and alternative treatments to give them the opportunity to consult with clergy and religious authorities.
We also believe that this topic should be taught to healthcare professionals, doctors and nurses together during their training. Guidelines developed from the from the present study may be useful in identifying individual patients for whom a comprehensive explanation of their religious rulings is recommended to obtain their informed consent for using transplanted organs. In a life-threatening situation, it is mandatory to inform the Muslim or Jewish patient and/or his relatives that the use of the organs of porcine origin is religiously permissible to save lives. This may ease and ease their concerns during the decision-making about whether to receive treatment and ease their potential distress or guilt. Furthermore, the informed consent form to be signed by the patient should also include an explicit explanation regarding the porcine origin of the medical treatment, in treatments that require an explicit informed consent.
It is the hope of the authors that the findings of the research project will serve as an evidence-based source for future discussions between physicians, religious leaders, and theologians to promote cultural competence among the medical staff as well as respecting the autonomy of the individual patient on the subject of organ transplantation.
There is cause for optimism on the subject of xenotransplants. In a pioneering medical procedure, performed in March 2024, physician-scientists at Harvard Medical School, Massachusetts General Hospital transplanted a genetically edited pig kidney into a human suffering from type 2 diabetes and hypertension, the most common causes of chronic kidney disease. This raises hopes about improving and saving lives where there is a shortage of available human organs. And while the patient survived only two months, his death was not been attributed to the transplantation procedure and marks an important milestone in the mission to alleviate a critical shortage of human kidneys for end-stage renal disease patients [76].
Author Contributions
Conceptualization, M.T.; design; MT; Data analysis and interpretation, M.T., D.W.L; writing-review and editing, M.T. and W.N. D.W.L, critically revised the article,. W.N., approved the article. M.T., performed statistical analysis; M.T.; D.W.L. data collection.
Funding
This research received no funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board of the Ramat Gan Academic College, approval code: #2022-1081, approval date: 31.12.2022. On the Appendix B: Informed consent form for online studies, Part I: Informed Consent Form for Online Studies it is written to each participant who answered the questionnaire that “by clicking the "I agree" button, you express your consent to participate in the study. Thereby, each patient who filled out the questionnaire had given his/her informed consent.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. The participants were given a detailed explanation of the study in their native language (Arabic or English) and were asked online to provide an informed consent form.
Data Availability Statement
Individual level data cannot be made publicly available due to legal and ethical restrictions. Aggregative data might be provided upon reasonable request to the corresponding author.
Acknowledgements
The authors wish to express their sincere gratitude to the anonymous reviewers for their helpful comments and suggestions. We thank the Jewish and Muslim students from the Academic College of Tel-Aviv-Yaffo, Israel.
Conflicts of Interest
The authors declare no conflict of interest.
Correspondence
Mahdi Tarabeih, PhD, School of Nursing Sciences, The Academic College of Tel-Aviv-Yaffo, 2 Rabenu Yerucham St., Tel Aviv, 6161001, Israel. Email: mahdita@mta.ac.il
Appendix A. Informed Consent Form for Online Studies
- Part I: Informed Consent Form for Online Studies
- Greetings,
- You are invited to participate in a study examining patient knowledge and attitudes towards donating organs that are produced from a pig in the Jewish and Islamic religions. This study was conducted by researchers at the School of Nursing Sciences, Tel Aviv-Jaffa Academic College. We thank you for dedicating your time and participating in the study.
- The primary aim of this study was to assess the level of knowledge among Muslim and Jewish individuals regarding religious rulings that allow the use of porcine organs in life-saving situations. Additionally, the study sought to evaluate participants’ personal attitudes toward the permissibility of such transplants within their religious and cultural frameworks.
- The time required to fill out the questionnaire is about 15 minutes. The questionnaire is anonymous and will be filled out anonymously, your answers are completely confidential, and will not be used in any way except for research purposes.
- In this questionnaire, you will be presented with several different questions regarding the effect of treatments on the quality of life and emotional reactions of transplant recipients. You are asked to mark the correct answer next to each question.
- You do not have to answer all the questions. If you feel uncomfortable, you may stop filling out the questionnaire at any stage.
- By agreeing to fill out this questionnaire, you declare that you are over 18 years old.
- It is assumed that participating in the research will not bring you any personal profit or advantage, but we hope that your participation will contribute to general knowledge in this research field.
- It should be noted that we are not aware of any risks by participating in the study, but as with any online activity there is a certain risk of breach of privacy. We make every effort to reduce this risk by have the questionnaire filled out anonymously and not using the details except for the purpose of the study.
- At the end of the study, you can get more information from the Ethics Committee of the Tel Aviv-Jaffa Academic College using the Debriefing form. In addition, you can contact the research team by email:
- We thank you very much for filling out the questionnaires in full.
- Sincerely yours,
- Dr. Mahdi Tarabia
- mahdita@mat.ac.il
- By clicking the "I agree" button, you express your consent to participate in the study. By clicking on the "I do not agree" button, you terminate your participation in the study.
Appendix B. The research questionnaire
- - Age (in years):
- 2- Gender: 1 - Male 2- Female
- 3- Education: 1. Academic 2. Non-academic
- 4- Religion: 1. Muslim 2. Jew
- 5- Level of religiosity: 1- Religious, 2- Secular
- 6- Family status: 1. In a relationship 2. Not in a relationship
- 7. Number of children…….
- The first part of the questionnaire presents you with a number of medical treatment scenarios. Please indicate, to the best of your knowledge, to what extent Jewish/Islamic religion allows medical treatment as described in the scenario:
1. Is it permitted according to the Jewish/Islamic religion to transplant a heart or a heart valve taken from a pig into a patient suffering from a heart problem whose life is in danger?
| 1 It is 100% forbidden |
2 It is almost always forbidden |
3 It is permitted infrequently |
4 It is permitted in exceptional cases |
5 It is always permitted |
6 It is totally 100% permitted |
7 I don’t know |
2. Is it permitted according to the Jewish/Islamic religion to do a lung transplant in a patient suffering from severe obstructive pulmonary disease, using a lung taken from a pig?
| 1 It is 100% forbidden |
2 It is almost always forbidden |
3 It is permitted infrequently |
4 It is permitted in exceptional cases |
5 It is always almost permitted |
6 It is totally (100%) permitted ` |
7 I don’t know |
3. Is it permitted according to the Jewish/Islamic religion to do a kidney transplant in a patient suffering from severe renal insufficiency using a kidney taken from a pig?
| 1 It is 100% forbidden |
2 It is almost always forbidden |
3 It is permitted infrequently |
4 It is permitted in exceptional cases |
5 It is always almost permitted |
6 It is totally 100% permitted ` |
7 I don’t know |
4. Is it permitted according to the Jewish/Islamic religion to treat a patient who is in danger of dying from pancreatic insufficiency by doing a transplant of a pancreas/pancreatic cells taken from a pig?
| 1 It is 100% forbidden |
2 It is almost always forbidden |
3 It is permitted infrequently |
4 It is permitted in exceptional cases |
5 It is always almost permitted |
6 It is totally 100% permitted ` |
7 I don’t know |
5. Is it permitted according to the Jewish/Islamic religion to implant in a patient’s knee cartilage taken from a pig, in order to replace worn cartilage?
| 1 It is 100% forbidden |
2 It is almost always forbidden |
3 It is permitted infrequently |
4 It is permitted in exceptional cases |
5 It is always almost permitted |
6 It is totally 100% permitted ` |
7 I don’t know |
6. Is it permitted according to the Jewish/Islamic religion to use skin tissue of a pig to do a skin graft in a patient with serious burn injuries?
| 1 It is 100% forbidden |
2 It is almost always forbidden |
3 It is permitted infrequently |
4 It is permitted in exceptional cases |
5 It is always almost permitted |
6 It is totally 100% permitted ` |
7 I don’t know |
In the second part of the questionnaire, you are asked to read each scenario and state your personal opinion on whether and to what extent you support providing the medical treatment described in the scenario.
7. Do you think one should approve transplanting in a Jewish/Muslim patient a heart or a heart valve taken from a pig?
| 1 Totally disagree |
2 Disagree somewhat |
3 Agree slightly |
4 Agree moderately |
5 Agree to a large extent |
6 Agree strongly |
7 Totally agree |
8. Do you think one should approve, according to the Jewish/Islamic religion, to transplant a lung taken from a pig in a patient suffering from obstructive pulmonary disease?
| 1 Totally disagree |
2 Disagree somewhat |
3 Agree slightly |
4 Agree moderately |
5 Agree to a large extent |
6 Agree strongly |
7 Totally agree |
9. Is it permitted by Jewish/Islamic religion to do a kidney transplant using a kidney taken from a pig?
| 1 Totally disagree |
2 Disagree somewhat |
3 Agree slightly |
4 Agree moderately |
5 Agree to a large extent |
6 Agree strongly |
7 Totally agree |
10. In your opinion should one approve treatment to a Jewish/Muslim patient who is in danger of death because of pancreatic insufficiency to undergo a transplant of a pancreas/pancreatic cells taken from a pig?
| 1 Totally disagree |
2 Disagree somewhat |
3 Agree slightly |
4 Agree moderately |
5 Agree to a large extent |
6 Agree strongly |
7 Totally agree |
11. In your opinion should one approve, for a Jewish/Muslim patient, to receive an implant of knee cartilage taken from a pig, in order to replace worn cartilage?
| 1 Totally disagree |
2 Disagree somewhat |
3 Agree slightly |
4 Agree moderately |
5 Agree to a large extent |
6 Agree strongly |
7 Totally agree |
12. In your opinion should one approve, for a Jewish/Muslim patient, to use skin tissue of a pig for a skin graft after serious burn injuries?
| 1 Totally disagree |
2 Disagree somewhat |
3 Agree slightly |
4 Agree moderately |
5 Agree to a large extent |
6 Agree strongly |
7 Totally agree |
References
- Worldometers.info. Current World Population. Available online: https://www.worldometers.info/world-population/ (accessed on 3 October 2023).
- Padela, A.I.; Auda, J. The Moral Status of Organ Donation and Transplantation within Islamic Law: The Fiqh Council of North America's Position. Transplant. Direct. 2020, 6, e536. [Google Scholar] [CrossRef]
- Paris, W.; Seidler, R.J.H.; FitzGerald, K.; Padela, A.I.; Cozzi, E.; Cooper, D.K.C. Jewish, Christian, and Muslim Theological Perspectives about Xenotransplantation. Xenotransplantation 2018, 25, e12400. [Google Scholar] [CrossRef]
- Nur Syahadah binti Mod Ali, S.; Gunardi, S. Porcine DNA in Medicine toward Postpartum Patients from Medical and Islamic Perspectives in Malaysia. Int. J. Halal Res. 2021, 3, 29–41. [Google Scholar] [CrossRef]
- Moritsugu, K.P.; Transplant Patients Need Hope—Not Waiting Lists—and Science May Finally Catch Up. Real Clear Policy [website] 2022, 30 November. Available online: https://www.realclearpolicy.com /2022/12/01/transplant_patients_need_hope_not_waiting_lists_867797.html (accessed on 21 September 2023).
- Mohiuddin, M.M.; Reichart, B.; Byrne, G.W.; McGregor, C.G.A. Current Status of Pig Heart Xenotransplantation. Int. J. Surg. 2015, 23 (Pt B), 234–239. [Google Scholar] [CrossRef]
- Cooper, D.K.C. A Brief History of Cross-Species Organ Transplantation. Proc. Bayl. Univ. Med. Cent. 2012, 25, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; He, W.; Ruan, Y.; Geng, Q. First Pig-to-Human Heart Transplantation. Innovation (Camb.). 2022, 3, 100223. [Google Scholar] [CrossRef] [PubMed]
- Reardon, S. First Pig-to-Human Heart Transplant: What Can Scientists Learn? Nature. 2022, 601, 305–306. [Google Scholar] [CrossRef]
- Pierson, R.N., 3rd; Burdorf, L.; Madsen, J.C.; Lewis, G.D.; D'Alessandro, D.A. Pig-to-Human Heart Transplantation: Who Goes First? Am. J. Transplant. 2020, 20, 2669–2674. [Google Scholar] [CrossRef]
- Elisseeff, J.; Badylak, S.F.; Boeke, J.D. Immune and Genome Engineering as the Future of Transplantable Tissue. N. Engl. J. Med. 2021, 385, 2451–2462. [Google Scholar] [CrossRef]
- Locke, J.E.; Kumar, V.; Anderson, D.; Porrett, P.M. Normal Graft Function after Pig-to-Human Kidney Xenotransplant. JAMA Surg. 2023, 158, 1106–1108. [Google Scholar] [CrossRef]
- Porrett, P.M.; Orandi, B.J.; Kumar, V.; et al. First Clinical-Grade Porcine Kidney Xenotransplant Using a Human Decedent Model. Am. J. Transplant. 2022, 22, 1037–1053. [Google Scholar] [CrossRef] [PubMed]
- Montgomery, R.A.; Stern, J.M.; Lonze, B.E.; et al. Results of Two Cases of Pig-to-Human Kidney Xenotransplantation. N. Engl. J. Med. 2022, 386, 1889–1898. [Google Scholar] [CrossRef] [PubMed]
- Godehardt, A.W.; Tönjes, R.R. Xenotransplantation of Decellularized Pig Heart Valves—Regulatory Aspects in Europe. Xenotransplantation 2020, 27, e12609. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, E.D.; Yip, M.; Melman, L.; Frisella, M.M.; Matthews, B.D. Informed Consent: Cultural and Religious Issues Associated with the Use of Allogeneic and Xenogeneic Mesh Products. J. Am. Coll. Surg. 2010, 210, 402–410. [Google Scholar] [CrossRef]
- Padela, A.I.; Duivenbode, R. The Ethics of Organ Donation, Donation after Circulatory Determination of Death, and Xenotransplantation from an Islamic Perspective. Xenotransplantation 2018, 25, e12401. [Google Scholar] [CrossRef]
- Bona, M.D.; Canova, D.; Rumiati, R.; et al. Understanding of and Attitudes to Xenotransplantation: A Survey among Italian University Students. Xenotransplantation 2004, 11, 133–140. [Google Scholar] [CrossRef]
- Padilla, L.A.; Hurst, D.; Lopez, R.; Kumar, V.; Cooper, D.K.C.; Paris, W. Attitudes to clinical pig kidney xenotransplantation among medical providers and patients. Kidney360 2020, 1, 657–662. [Google Scholar] [CrossRef]
- Eriksson, A.; Burcharth, J.; Rosenberg, J. Animal Derived Products May Conflict with Religious Patients’ Beliefs. BMC Med. Ethics 2013, 14, 1–5. [Google Scholar] [CrossRef]
- Tatham, K.C.; Patel, K.P. Suitability of Common Drugs for Patients Who Avoid Animal Products. BMJ 2014, 348, g401. [Google Scholar] [CrossRef]
- Karim, H.M.R.; Khan, T.H. Religious Belief as Determinant of Animal Derived Medications in Health Care: How Much Is Fairly Good? Anaesth. Pain Intensive Care 2018, 22, 151–154. [Google Scholar]
- Abdulla, A.; Hossain, M.; Barla, C. Toward Comprehensive Medicine: Listening to Spiritual and Religious Needs of Patients. Gerontol. Geriatr. Med. 2019, 5, 2333721419843703. [Google Scholar] [CrossRef] [PubMed]
- Babos, M.B.; Perry, J.D.; Reed, S.A.; et al. Animal-Derived Medications: Cultural Considerations and Available Alternatives. J. Osteopath. Med. 2021, 121, 361–370. [Google Scholar] [CrossRef]
- Goyal, D.; Goyal, A.; Brittberg, M. Consideration of Religious Sentiments While Selecting a Biological Product for Knee Arthroscopy. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 1577–1586. [Google Scholar] [CrossRef] [PubMed]
- Shiwani, M.H. The Use of Porcine Mesh Implants in the Repair of Abdominal Wall Hernia: An Islamic Perspective for an Informed Consent. J. Br. Islam. Med. Assoc. 2020, 4, 30–37. [Google Scholar]
- Haller, H.L.; Blome-Eberwein, S.E.; Branski, L.K.; et al. Porcine Xenograft and Epidermal Fully Synthetic Skin Substitutes in the Treatment of Partial-Thickness Burns: A Literature Review. Medicina 2021, 57, 432. [Google Scholar] [CrossRef] [PubMed]
- Omar, A.; Firas, A.; Hazim, R. The Use of Porcine Bioprosthetic Valves: An Islamic Perspective and a Bio-Ethical Discussion. J. Br. Islam. Med. Assoc. 2020, 4, 30–37. [Google Scholar]
- Padela, A.I.; Furber, S.W.; Kholwadia, M.A.; Moosa, E. Dire Necessity and Transformation: Entry-Points for Modern Science in Islamic Bioethical Assessment of Porcine Products in Vaccines. Bioethics 2014, 28, 59–66. [Google Scholar] [CrossRef]
- Manji, R.A.; Menkis, A.H.; Ekser, B.; Cooper, D.K. Porcine Bioprosthetic Heart Valves: The Next Generation. Am. Heart J. 2012, 164, 177–185. [Google Scholar] [CrossRef]
- Yamamoto, T.; Iwase, H.; King, T.W.; Hara, H.; Cooper, D.K.C. Skin Xenotransplantation: Historical Review and Clinical Potential. Burns 2018, 44, 1738–1749. [Google Scholar] [CrossRef]
- Sommaggio, R.; Uribe-Herranz, M.; Marquina, M.; Costa, C. Xenotransplantation of Pig Chondrocytes: Therapeutic Potential and Barriers for Cartilage Repair. Eur. Cell Mater. 2016, 32, 24–39. [Google Scholar] [CrossRef]
- Bokek-Cohen, Y.; Tarabeih, M. The Use of Porcine-Derived Materials for Medical Purposes: What Do Muslim and Jewish Individuals Know and Opine about It? J. Bioeth. Inq. 2022, 19, 599–612. [Google Scholar] [CrossRef] [PubMed]
- Rodger, D. Why We Should Stop Using Animal-Derived Products on Patients without Their Consent. J. Med. Ethics 2021, 47, medethics–2021. [Google Scholar] [CrossRef]
- Rodger, D.; Blackshaw, B.P. Using Animal-Derived Constituents in Anaesthesia and Surgery: The Case for Disclosing to Patients. BMC Med. Ethics 2019, 20, 14. [Google Scholar] [CrossRef]
- Bhamra, N. ; Jolly, K.; Darr, A.; Bowyer, D.J.; Ahmed, S.K. Intra-Operative Use of Biological Products—Are We Aware of Their Derivatives? Int. J. Clin. Pract. 2021, 75, e14633. [Google Scholar] [CrossRef]
- Easterbrook, C.; Maddern, G. Porcine and Bovine Surgical Products: Jewish, Muslim, and Hindu Perspectives. Arch. Surg. 2008, 143, 366–370. [Google Scholar] [CrossRef]
- Sattar, S.P.; Shakeel Ahmed, M.; Majeed, F.; Petty, F. Inert Medication Ingredients Causing Nonadherence Due to Religious Beliefs. Ann. Pharmacother. 2004, 38, 621–624. [Google Scholar] [CrossRef] [PubMed]
- Vissamsetti, B.; Payne, M.; Payne, S. Inadvertent Prescription of Gelatin-Containing Oral Medication: Its Acceptability to Patients. Postgrad. Med. J. 2012, 88, 499–502. [Google Scholar] [CrossRef]
- Jolly, K.; Darr, A.; Aslanidou, A.; Bowyer, D.; Ahmed, S. The Intra-Operative Use of Biological Products: A Multi-Centre Regional Patient Perspective of a Potential Consenting Conundrum. Clin. Otolaryngol. 2019, 44, 831–835. [Google Scholar] [CrossRef]
- Hedayat, K.M.; Pirzadeh, R. Issues in Islamic Biomedical Ethics: A Primer for the Pediatrician. Pediatrics 2001, 108, 965–971. [Google Scholar] [CrossRef]
- Van den Branden, S.; Broeckaert, B. The Ongoing Charity of Organ Donation: Contemporary English Sunni Fatwas on Organ Donation and Blood Transfusion. Bioethics 2011, 25, 167–175. [Google Scholar] [CrossRef]
- Daar, A.S.; Al Khitamy, A.B. Bioethics for Clinicians: 21. Islamic Bioethics. CMAJ 2001, 164, 60–63 https://wwwcmajca/content/164/1/60. [Google Scholar] [PubMed]
- Bokek-Cohen, Y. The Need to Adjust the Informed Consent for Jewish Patients for Treatments Involving Porcine Medical Constituents. J. Immigr. Minor Health 2023, 25, 142–150. [Google Scholar] [CrossRef] [PubMed]
- Gold, E.R.; Adams, W.A. Reconciling Private Benefit and Public Risk in Biotechnology: Xenotransplantation as a Case Study in Consent. Health Law J. 2002, 10, 31–75. [Google Scholar]
- Dorff, E.N. End-of-Life: Jewish Perspectives. Lancet 2005, 366, 862–865. [Google Scholar] [CrossRef]
- Tarabeih, M.; Amiel, A.; Na'amnih, W. The View of the Three Monotheistic Religions toward Xenotransplantation. Clin. Transplant. 2024, 38, e15192. [Google Scholar] [CrossRef] [PubMed]
- Loike, J.D.; Kadish, A. Ethical Rejections of Xenotransplantation? The Potential and Challenges of Using Human-Pig Chimeras to Create Organs for Transplantation. EMBO Rep. 2018, 19, e46337. [Google Scholar] [CrossRef]
- Moosa, E. Medicine and Shariah: A Dialogue in Islamic Bioethics; University of Notre Dame Press: Notre Dame, IN, USA, 2021. [Google Scholar]
- Fadel, H. The Islamic Viewpoint on New Assisted Reproductive Technologies. Fordham Urban Law J. 2002, 30, 147–157. [Google Scholar]
- Fadel, H. Prospects and Ethics of Stem Cell Research: An Islamic Perspective. J. Islamic Med. Assoc. North America 2007, 39, 73–78. [Google Scholar] [CrossRef]
- Fadel, H. Developments in Stem Cell Research and Therapeutic Cloning: Islamic Ethical Positions, A Review. Bioethics 2012, 26, 128–235. [Google Scholar] [CrossRef]
- Al-Zuhayli, W. al-Fiqh al-Islami wa-Adillatuh; Dar al-Fikr: Damascus, Syria, 1997. [Google Scholar]
- Ahmed, I.; Musarrat Nawaz, M. An Exploration of Students' Knowledge and Understanding of Istihalah. J. Islamic Marketing 2016, 7, 213–231. [Google Scholar] [CrossRef]
- Jamaludin, M.A. Fiqh Istihala: Integration of Science and Islamic Law. Revelation and Science 2012, 2, 49–55. [Google Scholar]
- Hurst, D.J.; Padilla, L.A.; Cooper, D.K.C.; Paris, W. Factors Influencing Attitudes Toward Xenotransplantation Clinical Trials: A Report of Focus Group Studies. Xenotransplantation 2021, 28, e12684. [Google Scholar] [CrossRef] [PubMed]
- Enoch, S.; Shaaban, H.; Dunn, K.W. Informed Consent Should Be Obtained from Patients to Use Products (Skin Substitutes) and Dressings Containing Biological Material. J. Med. Ethics 2005, 31, 2–6. [Google Scholar] [CrossRef]
- Hagelin, J.; Hau, J.; Schapiro, S.J.; Suleman, M.A.; Carlsson, H.E. Religious Beliefs and Opinions on Clinical Xenotransplantation–A Survey of University Students from Kenya, Sweden and Texas. Clin. Transplant. 2001, 15, 421–425. [Google Scholar] [CrossRef] [PubMed]
- Bokek-Cohen, Y.; Abu-Rakia, R.; Azuri, P.; Tarabeih, M. The View of the Three Monotheistic Religions Toward Cadaveric Organ Donation. Omega (Westport) 2022, 85, 429–444. [Google Scholar] [CrossRef]
- Hagelin, J. Public Opinion Surveys about Xenotransplantation. Xenotransplantation 2004, 11, 551–558. [Google Scholar] [CrossRef]
- Sattar, S.P.; Ahmed, M.S.; Madison, J.; et al. Patient and Physician Attitudes to Using Medications with Religiously Forbidden Ingredients. Ann. Pharmacother. 2004, 38, 1830–1835. [Google Scholar] [CrossRef]
- Kranenburg, L.W.; Kerssens, C.; Ijzermans, J.N.; Zuidema, W.; Weimar, W.; Busschbach, J.J. Reluctant Acceptance of Xenotransplantation in Kidney Patients on the Waiting List for Transplantation. Soc. Sci. Med. 2015, 61, 1828–1834. [Google Scholar] [CrossRef]
- Rosner, F. Pig Organs for Transplantation into Humans: A Jewish View. Mt. Sinai J. Med. 1999, 66, 314–319. [Google Scholar] [CrossRef]
- Loike, J.D.; Krupka, R.M. The Jewish Perspectives on Xenotransplantation. Rambam Maimonides Med. J. 2023, 14, e0024. [Google Scholar] [CrossRef]
- Feinstein, M. 1895-1986 Igros Moshe, Yore Deah, 229 and 230; Beth Medrash L’Torah V’Horaah: New York, NY, USA, 2012. [Google Scholar]
- Zilberstein, Y. Shiurei Torah laRofim. II; Maimonides Research Institute: Brooklyn, NY, USA, 2018. [Google Scholar]
- Hunter, J. Three Ethical Issues Around Pig Heart Transplants. BBC News, /: Jan 11. [Accessed , 2023]. Available online: https, 21 September 2023. [Google Scholar]
- Israel Central Bureau of Statistics. Population of Israel on the Eve of 2024. Available online: https://www.cbs.gov.il (accessed on 13 December 2023).
- Byrne, B.M. Structural Equation Modeling with Mplus: Basic Concepts, Applications, and Programming; Routledge: New York, NY, USA, 2013. [Google Scholar]
- Julvez, J.; Tuppin, P.; Cardoso, J.; Borsarelli, J.; Cohen, S.; Jouan, M.C. Population and Xenograft Investigation. Preliminary Results. Pathol. Biol. 2000, 48, 415–418. [Google Scholar] [CrossRef] [PubMed]
- Tarabeih, M.; Bokek-Cohen, Y.; Azuri, P. Health-Related Quality of Life of Transplant Recipients: A Comparison Between Lung, Kidney, Heart, and Liver Recipients. Qual. Life Res. 2020, 29, 1631–1639. [Google Scholar] [CrossRef]
- Curlin, F.A.; Roach, C.J.; Gorawara-Bhat, R. When Patients Choose Faith over Medicine: Physician Perspectives on Religiously Related Conflict in the Medical Encounter. Arch. Intern. Med. 2005, 165, 88–91. [Google Scholar] [CrossRef] [PubMed]
- Ebner, K.; Ostheimer, J.; Sautermeister, J. The Role of Religious Beliefs for the Acceptance of Xenotransplantation: Exploring Dimensions of Xenotransplantation in the Field of Hospital Chaplaincy. Xenotransplantation 2020, 27, e12579. [Google Scholar] [CrossRef] [PubMed]
- Bokek-Cohen, Y.; Gonen, L.D.; Tarabeih, M. The Muslim Patient and Medical Treatments Based on Porcine Ingredients. BMC Med. Ethics 2023, 24, 89. [Google Scholar] [CrossRef]
- Bokek-Cohen, Y.; Ravitsky, V. Cultural and Personal Considerations in Informed Consent for Fecal Microbiota Transplantation. Am. J. Bioethics 2017, 17, 55–57. [Google Scholar] [CrossRef]
- Mallapaty, S.; Kozlov, M. First Pig Kidney Transplant in a Person: What It Means for the Future. Nature 2024, 628, 13–14. [Google Scholar] [CrossRef]
Figure 1.
Bar graph for Knowledge and Opinion item means M = mean. An indication of the letters k and o refer to the different measures, whereas, k = Knowledge measure, and o = Opinion measure. An indication of the letters m and j refer to the different samples, whereas m = Muslim sample, and j = Jewish sample. Jewish sample is n = 916, and Muslim sample is n = 884. Item 1 = Is it permitted according to the Jewish/Islamic religion to transplant a heart or a heart valve taken from a pig into a patient suffering from a heart problem whose life is in danger? Item 2 = Is it permitted according to the Jewish/Islamic religion to do a lung transplant in a patient suffering from severe obstructive pulmonary disease, using a lung taken from a pig? Item 3 = Is it permitted according to the Jewish/Islamic religion to do a kidney transplant in a patient suffering from severe renal insufficiency using a kidney taken from a pig? Item 4 = Is it permitted according to the Jewish/Islamic religion to treat a patient who is in danger of death from pancreatic insufficiency by doing a transplant of a pancreas/pancreatic cells taken from a pig? Item 5 = Is it permitted according to the Jewish/Islamic religion to implant in a patient’s knee cartilage taken from a pig, in order to replace worn cartilage? Item 6 = Is it permitted according to the Jewish/Islamic religion to use the skin tissue of a pig to do a skin graft in a patient with serious burn injuries?
Figure 1.
Bar graph for Knowledge and Opinion item means M = mean. An indication of the letters k and o refer to the different measures, whereas, k = Knowledge measure, and o = Opinion measure. An indication of the letters m and j refer to the different samples, whereas m = Muslim sample, and j = Jewish sample. Jewish sample is n = 916, and Muslim sample is n = 884. Item 1 = Is it permitted according to the Jewish/Islamic religion to transplant a heart or a heart valve taken from a pig into a patient suffering from a heart problem whose life is in danger? Item 2 = Is it permitted according to the Jewish/Islamic religion to do a lung transplant in a patient suffering from severe obstructive pulmonary disease, using a lung taken from a pig? Item 3 = Is it permitted according to the Jewish/Islamic religion to do a kidney transplant in a patient suffering from severe renal insufficiency using a kidney taken from a pig? Item 4 = Is it permitted according to the Jewish/Islamic religion to treat a patient who is in danger of death from pancreatic insufficiency by doing a transplant of a pancreas/pancreatic cells taken from a pig? Item 5 = Is it permitted according to the Jewish/Islamic religion to implant in a patient’s knee cartilage taken from a pig, in order to replace worn cartilage? Item 6 = Is it permitted according to the Jewish/Islamic religion to use the skin tissue of a pig to do a skin graft in a patient with serious burn injuries?
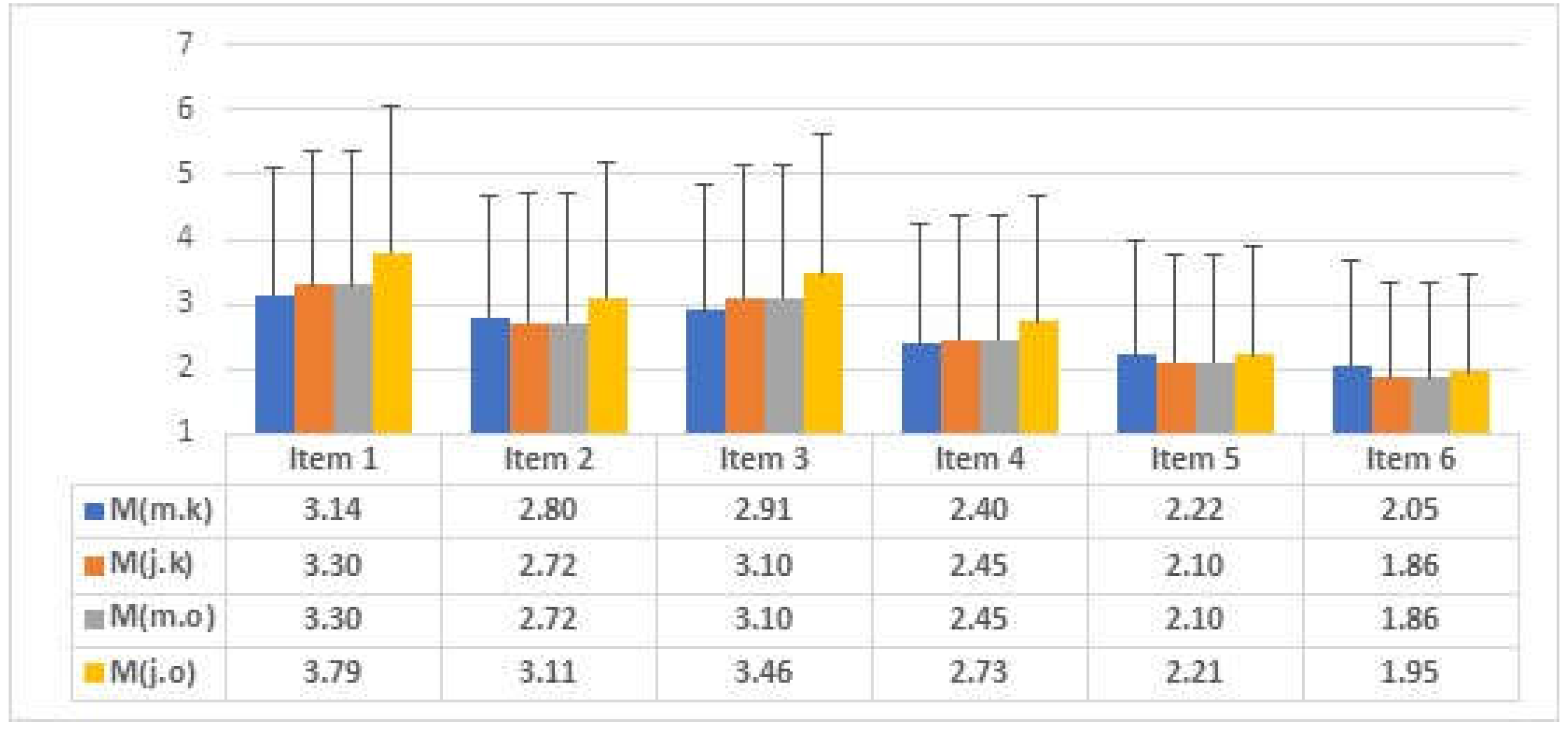
Figure 2.
Mediation model path diagram with standardized regression coefficients (Data for Jews are in parenthesis). All paths are significant at p < .001. Bolded paths are non-significant. Gender: 0 = female, 1 = male. Education: 0 = not academic, 1 = academic. Religiosity: 0 = secular, 1 = religious. Marital status: 0 = no relationship, 1 = in a relationship.
Figure 2.
Mediation model path diagram with standardized regression coefficients (Data for Jews are in parenthesis). All paths are significant at p < .001. Bolded paths are non-significant. Gender: 0 = female, 1 = male. Education: 0 = not academic, 1 = academic. Religiosity: 0 = secular, 1 = religious. Marital status: 0 = no relationship, 1 = in a relationship.
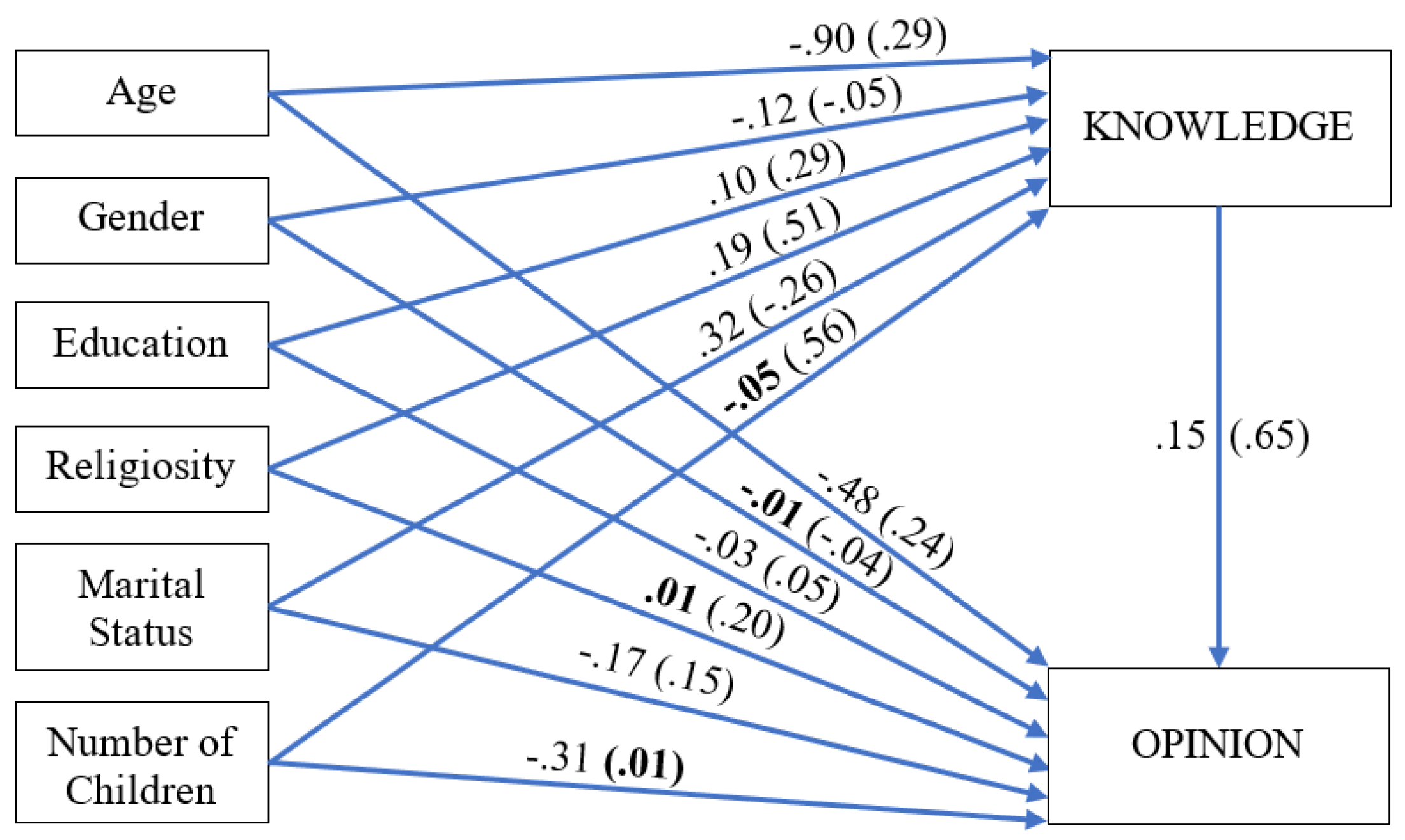
Table 1.
Demographic data for Jews and Muslims (Jewish data in parentheses).
| Variable | Category | Nm (Nj) | %m (%j) | Mm (Mj) | SDm (SDj) | Rm (Rj) |
| Gender | Male | 427 (457) | 48.3 (49.9) | - | - | - |
| Female | 457 (459) | 51.7 (50.1) | - | - | - | |
| Education | Not academic | 439 (435) | 49.7 (47.5) | - | - | - |
| Academic | 445 (481) | 50.3 (52.5) | - | - | - | |
| Religiosity | Secular | 402 (450) | 45.5 (49.1) | - | - | - |
| Religious | 482 (466) | 54.5 (50.9) | - | - | - | |
| Marital Status | No relationship | 86 (157) | 9.7 (17.1) | - | - | - |
| In a relationship | 798 (759) | 90.3 (82.9) | - | - | - | |
| Age | - | - | 49.41 (51.13) | 20.43 (20.78) | 18-81 | |
| Children | - | - | 4.43 (3.96) | 2.84 (2.73) | 0-13 (0-10) |
An indication of the letters m and j refer to the different samples, whereas m = Muslim sample, and j = Jewish sample. N = frequency. % = relative percent. M = mean. SD = standard deviation. R = range. Children = number of children.
Table 2.
Means, standard deviations, Pearson zero-order correlations and difference tests for all KNOWLEDGE and OPINION items.
Table 2.
Means, standard deviations, Pearson zero-order correlations and difference tests for all KNOWLEDGE and OPINION items.
| Jewish (n = 916) | Muslim (n = 884) | ||||||||
| Item | Mk (Mo) | SDk (SDo) | rp | Mk (Mo) | SDk (SDo) | rp | Fisher’s Z | ||
| 1. Is it permitted according to the Jewish/Islamic religion to transplant a heart or a heart valve taken from a pig into a patient suffering from a heart problem whose life is in danger? | 3.14 (3.30) | 1.95 (2.06) | .92 | 3.30 (3.79) | 2.06 (2.28) | .96 | 7.56*** | ||
| 2. Is it permitted according to the Jewish/Islamic religion to do a lung transplant in a patient suffering from severe obstructive pulmonary disease, using a lung taken from a pig? | 2.80 (2.72) | 1.88 (1.97) | .95 | 2.72 (3.11) | 1.97 (2.09) | .96 | 2.42* | ||
| 3. Is it permitted according to the Jewish/Islamic religion to do a kidney transplant in a patient suffering from severe renal insufficiency using a kidney taken from a pig? | 2.91 (3.10) | 1.94 (2.04) | .96 | 3.10 (3.46) | 2.04 (2.17) | .93 | 6.09*** | ||
| 4. Is it permitted according to the Jewish/Islamic religion to treat a patient who is in danger of death from pancreatic insufficiency by doing a transplant of a pancreas/pancreatic cells taken from a pig? | 2.40 (2.45) | 1.82 (1.92) | .94 | 2.45 (2.73) | 1.92 (1.94) | .95 | 1.98* | ||
| 5. Is it permitted according to the Jewish/Islamic religion to implant in a patient’s knee cartilage taken from a pig, in order to replace worn cartilage? | 2.22 (2.10) | 1.74 (1.66) | .88 | 2.10 (2.21) | 1.66 (1.68) | .96 | 12.07*** | ||
| 6. Is it permitted according to the Jewish/Islamic religion to use skin tissue of a pig to do a skin graft in a patient with serious burn injuries? | 2.05 (1.86) | 1.65 (1.46) | .79 | 1.86 (1.95) | 1.46 (1.50) | .95 | 16.10*** | ||
Table 3.
Means, standard deviations, t-tests results, comparing Muslim and Jewish samples in item-wise means for all KNOWLEDGE and OPINION items.
Table 3.
Means, standard deviations, t-tests results, comparing Muslim and Jewish samples in item-wise means for all KNOWLEDGE and OPINION items.
| KNOWLEDGE items | OPINION items | |||||
| Item | Mm (Mj) | SDm (SDj) | t-test | Mm (Mj) | SDm (SDj) | t-test |
| 1. Is it permitted according to the Jewish/Islamic religion to transplant a heart or a heart valve taken from a pig into a patient suffering from a heart problem whose life is in danger? | 3.14 (3.30) | 1.95 (2.06) | 1.58 | 3.81 (3.79) | 2.51 (2.28) | 0.12 |
| 2. Is it permitted according to the Jewish/Islamic religion to do a lung transplant in a patient suffering from severe obstructive pulmonary disease, using a lung taken from a pig? | 2.80 (2.72) | 1.88 (1.97) | 0.78 | 3.45 (3.11) | 2.49 (2.09) | 3.09*** |
| 3. Is it permitted according to the Jewish/Islamic religion to do a kidney transplant in a patient suffering from severe renal insufficiency using a kidney taken from a pig? | 2.91 (3.10) | 1.94 (2.04) | 1.84* | 3.55 (3.46) | 2.53 (2.17) | 0.85 |
| 4. Is it permitted according to the Jewish/Islamic religion to treat a patient who is in danger of death from pancreatic insufficiency by doing a transplant of a pancreas/pancreatic cells taken from a pig? | 2.40 (2.45) | 1.82 (1.92) | 0.61 | 2.82 (2.73) | 2.35 (1.94) | 0.94 |
| 5. Is it permitted according to the Jewish/Islamic religion to implant in a patient’s knee cartilage taken from a pig, in order to replace worn cartilage? | 2.22 (2.10) | 1.74 (1.66) | 1.41 | 2.47 (2.21) | 2.18 (1.68) | 2.84** |
| 6. Is it permitted according to the Jewish/Islamic religion to use skin tissue of a pig to do a skin graft in a patient with serious burn injuries? | 2.05 (1.86) | 1.65 (1.46) | 2.38** | 2.13 (1.95) | 1.95 (1.50) | 2.29** |
**p < .01, ***p < .001. An indication of the letters m and j refer to the different samples, whereas m = Muslim sample, and j = Jewish sample. Jewish sample is n = 916, and Muslim sample is n = 884.
Table 4.
Pearson zero-order correlations (Jewish data is above the diagonal with n = 916; Muslim data is below the diagonal with n = 884).
Table 4.
Pearson zero-order correlations (Jewish data is above the diagonal with n = 916; Muslim data is below the diagonal with n = 884).
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |
|
- | -.02 | .06 | .02 | .63*** | .83*** | .62*** | .75*** |
|
.02 | - | -.01 | .01 | .13*** | .10*** | -.03 | -.05 |
|
.01 | .00 | - | .01 | -.01 | -.19*** | .21*** | .19*** |
|
.07* | -.04 | .02 | - | -.11** | -.27*** | .39*** | .44*** |
|
.47*** | .13*** | -.11*** | -.03 | - | .65*** | .22*** | .43*** |
|
.79*** | .06 | -.24*** | -.33*** | .51*** | - | .44*** | .52*** |
|
-.77*** | -.10** | .08* | .14*** | -.15*** | -.68*** | - | .93*** |
|
-.92*** | -.08* | .07* | .10** | -.57*** | -.87*** | .75*** | - |
*p < .05, **p < .01, ***p < .001. Children = number of children. Gender: 0 = male, 1 = female. Education: 0 = not academic, 1 = academic. Religiosity: 0 = religious, 1 = secular. Marital status: 0 = not in a relationship, 1 = in a relationship.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



