Submitted:
19 April 2025
Posted:
21 April 2025
You are already at the latest version
Abstract
Background:Disseminated fusariosis, caused by Fusarium solani, is a rare, life-threatening fungal infection primarily affecting immunocompromised individuals, including those with hematological malignancies like acute myeloid leukemia (AML). Its angioinvasive nature and multidrug resistance present significant diagnostic and therapeutic challenges, with high mortality rates despite aggressive treatment.Methods:This retrospective case report, following CARE guidelines, analyzed clinical data from electronic medical records, imaging, and diagnostic reports. A literature review on disseminated fusariosis was conducted, and a multidisciplinary approach guided therapeutic decisions.Case Presentation:A 27-year-old female with AML, undergoing intensive chemotherapy, developed prolonged neutropenia and immunosuppression. She presented with persistent headaches, progressive vision loss, necrotic skin lesions, and abdominal pain. Diagnostic tests confirmed disseminated Fusarium solani infection with multiorgan involvement, including the central nervous system, ocular, respiratory, dermatologic, and gastrointestinal systems. Early initiation of antifungal therapy with amphotericin B and fosmanogepix, along with a multidisciplinary approach, led to clinical stabilization. Due to recurrence risk, she remains on lifelong fosmanogepix therapy.Conclusion:This case highlights the need for early recognition and aggressive management of disseminated fusariosis in high-risk patients. A multidisciplinary strategy integrating infectious disease expertise, diagnostic imaging, and targeted antifungal therapy is crucial for improving outcomes. Further research is needed to enhance diagnostic tools and treatment protocols for invasive fungal infections in immunocompromised populations.
Keywords:
disseminated fusariosis
; Fusarium solani
; acute myeloid leukemia
; immunosuppression
; antifungal therapy
; multidrug resistance
; angioinvasive fungal infection
Introduction
Fusarium is a genus of ubiquitous filamentous fungi that can cause a range of infections, from localized lesions in healthy individuals to disseminated and life-threatening infections in immunocompromised patients, particularly those with hematological malignancies. The contamination of food and feed with Fusarium mycotoxins has been associated with outbreaks of human and animal mycotoxicosis, respectively [1]. Invasive fusariosis has emerged as an opportunistic fungal infection in immunocompromised patients, including those with leukemia, cancer, or AIDS. Invasive fungal infections pose a significant threat to immunocompromised individuals, particularly patients with hematologic malignancies such as acute myeloblastic leukemia [2,3]. One opportunistic fungal pathogen that has garnered increasing attention is Fusarium solani, a ubiquitous filamentous fungus capable of causing a range of infections from localized lesions to disseminated disease [3]. The ability of Fusarium species to produce mycotoxins, which can exacerbate the condition of immunocompromised individuals, further complicates the management of invasive fusariosis in acute myeloblastic leukemia patients. Early diagnosis and prompt antifungal therapy are critical to improving the survival of these patients, as the mortality rate associated with disseminated Fusarium infections remains high [4].
Ongoing research efforts are focused on developing more effective diagnostic and treatment strategies to combat the rising incidence of invasive fusariosis in immunocompromised populations, including those with acute myeloblastic leukemia. Acute myeloblastic leukemia is a malignant hematological disorder characterized by the rapid proliferation and accumulation of immature myeloid cells, known as myeloblasts, in the bone marrow and peripheral blood. This aggressive form of acute leukemia is the most common type in adults, accounting for 40% of all leukemias in the western world [5]. The incidence of acute myeloblastic leukemia increases with age, reaching up to 12.6 cases per 100,000 inhabitants per year in patients over 65 years of age [5]. The clinical presentation of acute leukemia is often nonspecific, with patients presenting with symptoms such as weakness, fatigue, dyspnea, fever, and bleeding due to the infiltration of bone marrow and extramedullary sites by the malignant blasts [6]. The immunocompromised state associated with the disease and the intensive chemotherapeutic regimens used in treatment can leave these patients vulnerable to opportunistic infections. Disseminated fusariosis in patients with acute leukemia is particularly problematic, as it is often difficult to diagnose due to the lack of specific clinical manifestations and the limitations of current diagnostic tools[4].
Methodology
Research Design
This case report adheres to established CARE (Case Report) guidelines following a structured, multi-phase process.
Participants: A 27-year-old female patient was engaged during her clinical management at a tertiary academic medical center.
Phase 1: Written informed consent was obtained from the patient to publish clinical details and imaging findings.
Phase 2: Face-to-face interactions with the patient were conducted during her hospital visit, and a signed medical record release was obtained to retrieve detailed clinical history, laboratory results, and imaging data.
Phase 3: A comprehensive literature review was conducted on disseminated fusariosis, its clinical manifestations, diagnostic approaches, and treatment strategies. Relevant databases were searched for case reports and studies on Fusarium solani infections in immunocompromised patients.
Phase 4: The case report was drafted, reviewed, and edited collaboratively by the authors through post-meetings, ensuring accuracy and adherence to research reporting standards.
Data Collection and Analysis
Data collection included detailed symptom documentation, multisystem physical examinations, and laboratory tests confirming Fusarium solani through blood, skin biopsy, and JP drain fluid cultures. Imaging revealed systemic dissemination, with CT scans showing hepatic, renal, and pancreatic abscesses, chest imaging identifying pleural effusions, and brain MRI demonstrating leptomeningeal enhancement and cranial nerve involvement. All findings were interpreted by radiologists and correlated with clinical data for a comprehensive evaluation.
Data analysis correlated clinical symptoms with laboratory and imaging findings to determine the timeline and extent of systemic dissemination, identify diagnostic challenges, and evaluate antifungal therapy efficacy.
Case Presentation
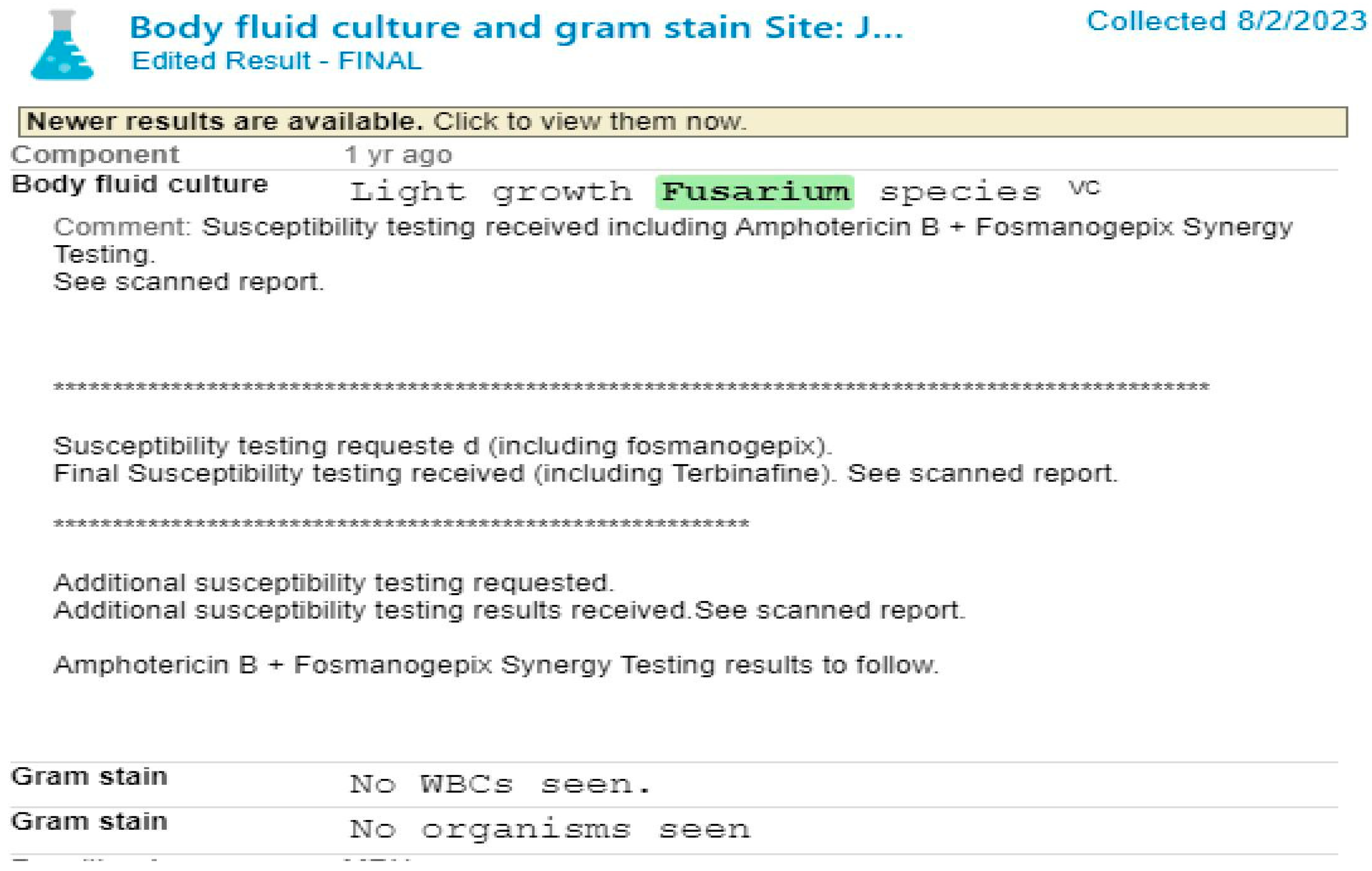
A 27-year-old female with a diagnosed case of acute myeloid leukemia (AML) presented to the outpatient clinic in June 2023 with complaints of persistent, intractable headaches, blurred vision and necrotic cutaneous lesions on extremities. The patient also had persistent fever and shortness of breath. She had undergone intensive chemotherapy with Venetoclax and a CLIA regimen (Cladribine, Cytarabine and Idarubicin) one month prior, resulting in prolonged neutropenia and subsequent immunosuppression. On ophthalmologic examination, retinal infarctions were observed. Vision assessment revealed no light perception (NLP) in the left eye and severe visual impairment in the right eye. Chest examination was consistent with pleural effusion. Laboratory evaluations showed elevated serum lipase levels (4600 U/L), C-reactive protein (CRP) (35.45 mg/L) and procalcitonin (PCT) (11.5 ng/mL). A CT-guided drainage procedure collected fluid from the left upper quadrant of the lungs, showing light growth of Fusarium species on culture, with gram stains showing no white blood cells or organisms. The tissue culture from the left thigh demonstrated light growth of Fusarium solani complex, while the gram stain showed no visible organisms and white blood cells rarely. The blood culture confirmed the presence of Fusarium solani, with gram staining revealing hyphae [Figure 1]. Body fluid cultures also confirmed the same [Figure 2]. Following an extensive diagnostic work-up, a diagnosis of disseminated fusariosis was confirmed. Fungal susceptibility testing revealed multi-drug resistance to amphotericin B with lower minimal inhibitory concentration (MIC) < 4 and higher MIC to itraconazole, posaconazole and voriconazole > 16. The patient was started on antifungal therapy, fosmanogepix, alongside chemotherapy with Venetoclax and the CLIA regimen (Cladribine, Cytarabine and Idarubicin). She also received prolonged antifungal therapy with intravenous liposomal amphotericin B, as she was less resistant to it. In July 2023, the patient developed abdominal pain accompanied by significant fluid accumulation. Laboratory findings revealed significantly elevated lipase levels (4600 U/L), indicative of acute pancreatitis along with elevated alkaline phosphatase (ALP) levels, ranging from 260 to 340 U/L and AST/ALT levels between 60 and 100 U/L. A Jackson Pratt drain was placed, resulting in the drainage of 800 mL of serosanguineous fluid, resolving the pancreatic fluid accumulation. By September 2023, the patient’s clinical condition progressed to multifocal pneumonia, but improved following antifungal therapy. By November 2023, the patient demonstrated clinical improvement, allowing for discharge on oral fosmanogepix alone. Maintenance chemotherapy with azacitidine was initiated but, in December 2023, the patient presented with persistent headaches and experienced one episode of visual hallucinations. The hallucinations resolved following the initiation of amphotericin B therapy at a dose of 10 mg/kg. Pain management was initiated with methadone (15 mg BID), pregabalin (150 mg BID), magnesium oxide (100 mg QHS) and as-needed hydromorphone for breakthrough pain. Upon discharge, fosmanogepix therapy was resumed as monotherapy. In 2024, the patient continued to receive combined antifungal and chemotherapy regimens. In January 2024, an EEG demonstrated diffuse encephalopathy without epileptiform discharges. MRI scan findings revealed leptomeningeal enhancement in the perimesencephalic and prepontine cisterns, thalamic lesions, frontal lobe involvement and oculomotor nerve palsy, consistent with CNS dissemination of Fusarium. The patient’s condition improved with continued antifungal therapy and comprehensive pain management. A bronchoscopy with bronchoalveolar lavage (BAL), performed in February 2024, was negative for fungal organisms. The patient demonstrated significant clinical improvement with continued antifungal therapy. In March 2024, the diagnosis of bilateral endogenous fungal endophthalmitis was confirmed, further highlighting the angioinvasive nature of the infection. It is important to note that despite antifungal therapy, the patient's visual prognosis remained poor. During her third cycle of maintenance azacitidine in June, she received a one-week infusion of liposomal amphotericin B. In July 2024, abdominal CT-scan imaging done to assess disease status revealed multiple low-density foci in the liver, spleen, kidneys and pancreas, consistent with abscesses or infectious sites. Additionally, a 12.4 × 10.9cm loculated collection in the left abdomen was identified, suggestive of an abscess or a pseudocyst. Despite ongoing antifungal therapy, including amphotericin B, the patient exhibited persistently elevated inflammation markers and recurrent abdominal symptoms, necessitating continued close monitoring and multidisciplinary management. Thus, she was admitted for another azacitidine cycle with prophylactic amphotericin B. Moreover, a repeat CT-scan of chest revealed bilateral pleural effusion with hazy and patchy opacities, consistent with worsening pneumonia. However, subsequent imaging identified nodular foci in both lungs, which showed a marked decrease on repeat CT-scan chest imaging in the same month, suggesting improvement in granulomatous inflammation with antifungal treatment. Repeat imaging in September revealed stable CNS findings and the patient continued fosmanogepix therapy without side effects. By November 2024, she remained clinically stable, reporting no symptoms and tolerating dose-reduced azacitidine alongside Zarzio (filgrastim). In December 2024, fosmanogepix therapy was extended indefinitely to mitigate recurrence risk, marking significant progress in managing her disseminated fungal infection and associated complications.
Discussion
Disseminated Fusarium infections are rare but severe complications primarily affecting immunocompromised individuals, particularly those undergoing treatment for hematologic malignancies such as acute myeloid leukemia (AML). The incidence of invasive fungal infections in AML patients ranges from 10%–25% [7]. The increasing use of antifungal prophylaxis with fluconazole has led to a shift in fungal infection patterns, with a reduced incidence of candidiasis and a rise in cases of invasive infections caused by Fusarium species [8]. These fungi are widely found in the environment, particularly in soil and water, with the Fusarium solani species complex accounting for approximately 60% of human infections. Entry into the body occurs predominantly through inhalation of spores or direct contact with compromised skin or mucosal barriers. In immunocompromised individuals, prolonged neutropenia induced by chemotherapy and the use of immunosuppressive medications significantly elevate the risk of disseminated Fusarium infections [9]. These infections frequently manifest with persistent fever, characteristic cutaneous lesions, and multi-organ involvement, including the CNS, respiratory system, and gastrointestinal organs [10]. In this case, the patient initially presented with ocular symptoms, including bilateral endophthalmitis, which likely represented the primary site of infection that subsequently disseminated hematogenous. Despite a normal neutrophil count at onset, the patient’s immunosuppressed status was a significant predisposing factor. Diagnosis of Fusarium infections is often challenging due to nonspecific clinical manifestations. This case highlights the importance of blood cultures and tissue biopsies for confirming infection, as both demonstrated the presence of Fusarium solani. While traditional diagnostic methods, such as cultures, are effective, advanced molecular diagnostics like PCR or multilocus sequence typing could enhance the precision and speed of diagnosis, especially in disseminated cases. Disseminated Fusarium infections are associated with high mortality rates, often exceeding 50%–70%, largely due to the pathogen’s resistance to many antifungal agents [9]. Standard treatment options include amphotericin B and voriconazole as first-line therapies, with posaconazole and newer agents like isavuconazole serving as alternatives or salvage therapies. In this case, the patient received a combination of amphotericin B, voriconazole, and fosmanogepix, which led to stabilization despite the infection's severity and multidrug resistance profile. Delays in intraocular antifungal interventions, however, may have contributed to the irreversible blindness. Surgical interventions, such as vitrectomy, can be critical in controlling intraocular infections and preventing further dissemination, although they were not performed in this case. Disseminated Fusarium infections remain highly lethal despite aggressive antifungal therapy and multidisciplinary management. Factors such as persistent neutropenia, fungemia, and extensive drug resistance contribute to the poor prognosis [9]. This case underscores the critical need for early detection, rapid initiation of antifungal therapy, and close collaboration among specialists to optimize treatment outcomes. Further research into more effective antifungal agents and diagnostic tools is essential to improve survival rates in patients with disseminated Fusarium infections.
Fusariosis in Immunocompromised Hosts
Fusarium species, particularly Fusarium solani, are opportunistic pathogens that are capable of causing severe invasive infections in immunocompromised patients, such as those with hematologic diseases undergoing chemotherapy [9]. The patient’s clinical presentation, characterized by systemic symptoms and multiple organ involvement, aligns with the known clinical spectrum of fusariosis, which can present with cutaneous lesions, pulmonary involvement, and dissemination to the central nervous system (CNS) and eyes [11]. These findings are consistent with the well-documented ability of Fusarium species to invade blood vessels and cause hematogenous spread. Our case emphasizes the significance of early identification of fungal infections [7], as the immunocompromised status of the patient, due to chemotherapy-induced neutropenia, heightened her susceptibility to invasive fungal diseases. The identification of Fusarium from blood, skin biopsy, and other body fluids was crucial for confirming the diagnosis and guiding antifungal therapy. Without timely intervention, such infections can rapidly progress and lead to multi-organ failure, as observed in this patient.
Diagnostic Challenges and Imaging Findings
The diagnostic approach to this case relied heavily on imaging, microbiological culture, and clinical evaluation. Imaging, particularly CT and MRI scans, played a critical role in identifying the extent of the disease. The CT scans revealed extensive pulmonary consolidation and fluid collections in the abdomen, consistent with the systemic dissemination of Fusarium. Notably, imaging findings of cranial involvement, including leptomeningeal enhancement and thalamic lesions, provided compelling evidence of CNS dissemination, which can complicate the management of fusariosis. The use of advanced imaging techniques, such as MRI, is essential for detecting CNS involvement in such infections, particularly when presenting with nonspecific neurological symptoms, such as headaches and visual disturbances.
Tissue biopsy should be obtained immediately for both tissue culture and histopathological Examination [12]. Vascular invasion with thrombosis and tissue necrosis has been observed with fusarial infections. On microscopic examination, there was a close similarity between Aspergillusa nd Fusarium. The identification of F. solani can be challenging and may take up to 5-7 days to speciate. The addition of PCR can aid in the diagnosis However, while CT scans helped to assess the improvement post-drainage of fluid collections, the absence of standardized quantitative metrics for evaluating fluid volume or lesion size limits the ability to objectively track treatment response over time. Ideally, further studies employing quantitative imaging techniques would enhance the precision of outcome assessment in cases of disseminated fusariosis.
Management and Treatment Considerations
The patient was initiated on appropriate antifungal therapy with amphotericin B, an agent commonly used for the treatment of invasive Fusarium infections due to its broad-spectrum antifungal activity. Despite the significant challenges posed by the patient’s immunocompromised state, early antifungal therapy, combined with supportive care such as drainage of fluid collections, helped to stabilize her condition. The use of other antifungal agents, such as voriconazole, could also be considered for Fusarium infections, but the choice of therapy depends on the clinical status of the patient, as well as the resistance profile of the organism [7]. While antifungal treatment was initiated promptly, the patient’s progress was closely monitored by a multidisciplinary team, including infectious disease specialists, ophthalmologists, neurologists, and radiologists, which proved to be critical in managing the complexities of this case. The integration of various specialist perspectives allowed for the tailored management of systemic fungal infection, organ-specific complications, and ongoing supportive care.
Clinical Implications and Limitations
This case highlights the importance of early diagnosis and aggressive treatment of disseminated fungal infections in patients with hematologic malignancies. Given the high mortality associated with invasive fusariosis, particularly in immunocompromised individuals, clinicians must maintain a high level of vigilance for signs of fungal infections, even in the presence of nonspecific symptoms. The multidisciplinary approach in this case, involving coordinated care across various specialties, was essential to optimize patient outcomes and ensure comprehensive management.
Despite the promising outcome with early antifungal therapy and drainage, this case has several limitations. The retrospective nature of the study, combined with the absence of quantitative imaging tools, limits the ability to objectively assess disease progression and response to treatment. Furthermore, the lack of molecular diagnostics, such as PCR-based fungal identification, represents a limitation in the identification of the pathogen and its potential resistance mechanisms. Future prospective studies with larger sample sizes and the use of quantitative imaging techniques, molecular diagnostics, and serial laboratory trend analysis would provide further insight into the management and outcomes of disseminated fusariosis in immunocompromised patients. Secondly, the retrospective design of this study, which relies on medical records and patient recall, introduces potential biases and the risk of incomplete data. Inconsistencies in symptom reporting and variations in medical history documentation may impact the accuracy and comprehensiveness of the information provided.
Conclusion
In conclusion, this case report underscores the complexity of diagnosing and managing disseminated fusariosis in an immunocompromised patient with AML. Prompt identification, early antifungal treatment, and multidisciplinary care were critical to stabilizing the patient. This report highlights the need for continued vigilance in diagnosing invasive fungal infections, particularly in patients undergoing chemotherapy, and calls for further studies to refine diagnostic and therapeutic strategies for these high-risk individuals. Clinicians should promptly consider potential pathogens by utilizing microbiological, serological, and radiological evaluations, initiating appropriate treatment without delay, particularly in cases of opportunistic infections.
Funding
No funding was received for this study.
Acknowledgment
We gratefully acknowledge the patient for providing consent to publish this case report and share her clinical journey. Our sincere thanks extend to the multidisciplinary healthcare team at the tertiary academic medical center for their exceptional care and collaboration in managing this complex case. We also appreciate the contributions of all authors and collaborators involved in the drafting, review, and editing of this report. Additionally, we acknowledge the valuable insights gained from existing medical literature on Fusarium solani infections, which informed and supported the development of this case report.
Informed Consent
Written informed consent was obtained from the patient.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Y. Sugiura et al., “Physiological characteristics and mycotoxins of human clinical isolates of Fusarium species,” Mycol. Res., vol. 103, no. 11, pp. 1462–1468, Nov. 1999. [CrossRef]
- L. Huang et al., “Disseminated Fusarium solani infection in a child with acute lymphocytic leukemia: A case report and literature review,” Med. Microecol., vol. 18, p. 100093, Dec. 2023. [CrossRef]
- J. Demonchy et al., “Multicenter Retrospective Study of Invasive Fusariosis in Intensive Care Units, France,” Emerg. Infect. Dis., vol. 30, no. 2, pp. 215–224, Feb. 2024. [CrossRef]
- “Empiric Amphotericin B Therapy in Patients with Acute Leukemia | Clinical Infectious Diseases | Oxford Academic.” Accessed: Mar. 07, 2025. [Online]. Available: https://academic.oup.com/cid/article-abstract/7/5/619/471480?redirectedFrom=PDF.
- C. Alarcón-Payer, M. D. M. Sánchez Suárez, A. Martín Roldán, J. M. Puerta Puerta, and A. Jiménez Morales, “Impact of Genetic Polymorphisms and Biomarkers on the Effectiveness and Toxicity of Treatment of Chronic Myeloid Leukemia and Acute Myeloid Leukemia,” J. Pers. Med., vol. 12, no. 10, p. 1607, Sep. 2022. [CrossRef]
- “Acute Leukemia Clinical Presentation | IntechOpen.” Accessed: Mar. 07, 2025. [Online]. Available: https://www.intechopen.com/chapters/44629.
- E. I. Boutati and E. J. Anaissie, “Fusarium, a Significant Emerging Pathogen in Patients With Hematologic Malignancy: Ten Years’ Experience at a Cancer Center and Implications for Management,” Blood, vol. 90, no. 3, pp. 999–1008, Aug. 1997. [CrossRef]
- R. Galimberti, A. C. Torre, M. C. Baztán, and F. Rodriguez-Chiappetta, “Emerging systemic fungal infections,” Clin. Dermatol., vol. 30, no. 6, pp. 633–650, Nov. 2012. [CrossRef]
- A. S. Gamis, T. Gudnason, G. S. Giebink, and N. K. Ramsay, “Disseminated infection with Fusarium in recipients of bone marrow transplants,” Rev. Infect. Dis., vol. 13, no. 6, pp. 1077–1088, 1991. [CrossRef]
- V. Letscher-Bru, F. Campos, J. Waller, R. Randriamahazaka, E. Candolfi, and R. Herbrecht, “Successful outcome of treatment of a disseminated infection due to Fusarium dimerum in a leukemia patient,” J. Clin. Microbiol., vol. 40, no. 3, pp. 1100–1102, Mar. 2002. [CrossRef]
- H. Fei et al., “Disseminated fusarium infection after allogeneic hematopoietic stem cell transplantation after CART: A case report,” Medicine (Baltimore), vol. 101, no. 45, p. e31594, Nov. 2022. [CrossRef]
- V. Letscher-Bru, F. Campos, J. Waller, R. Randriamahazaka, E. Candolfi, and R. Herbrecht, “Successful outcome of treatment of a disseminated infection due to Fusarium dimerum in a leukemia patient,” J. Clin. Microbiol., vol. 40, no. 3, pp. 1100–1102, Mar. 2002. [CrossRef]
Figure 1.
Blood culture report.
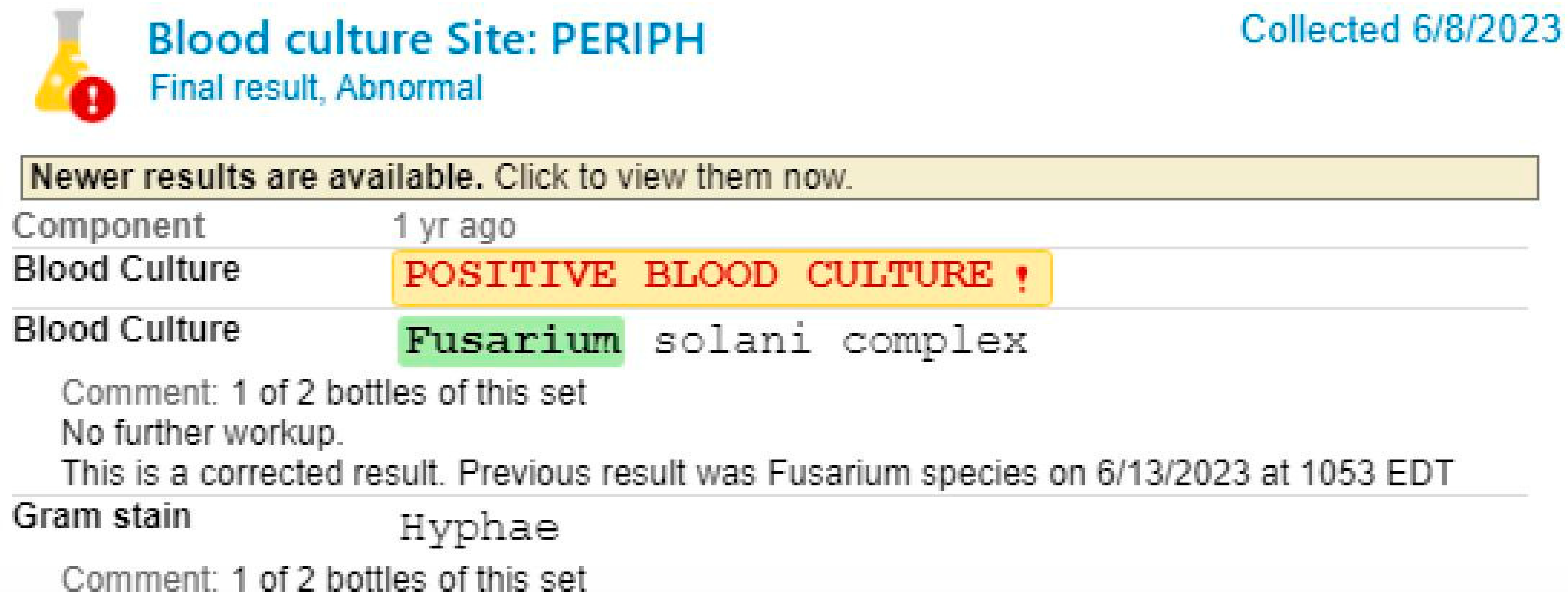
Figure 2.
Body fluid cultures.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



