Submitted:
11 April 2025
Posted:
14 April 2025
You are already at the latest version
Abstract
Cardiac arrest (CA) is a hemostatic state only reversible via dynamics intracardiac action potentials implementing hemorheological-biochemical reactions of adequate blood volumes (BV). Undeniably exclusive electrophysiological processes that began since intrauterine life remain compromised by cardiopulmonary resuscitation (CPR). Failure of CPR to adapt these hemostatic-electrophysiological conditions as well as human cardiotorsal anatomy, and thoracic biomechanics results in a staggering number of CA mortalities worldwide. Except for mechanical circulatory support (MCS), CPR induces a pointless back-and-forth mode of perfusion that worsens the stalled metabolism. Since the heart and respiratory pump, the main generators of endothelial shear stress (ESS) that control organs microcirculation, thereby metabolism, no longer function. Accordingly, we propose ESS-induced meditators as a potential solution in CA, mechanically with pulsatile MCSs providing rapid circulatory flow restoration (CFR), regardless of return of spontaneous circulation (ROSC). And manually with a novel technique of cardiac massage inducing snaping atrial wall shear stress with adequate BV, promoting a less-traumatic ROSC. Our goal is to evaluate the therapeutic proposal through an in-depth analysis that could change the fierce strain in evolving current CPR doctrine, thus improving the dismal outcomes of CA victims.
Keywords:
cardiac arrest (CA)
; cardiopulmonary resuscitation (CPR)
; circulatory flow resuscitation (CFR)
; microcirculation
; endothelial dysfunction
; endothelial shear stress (ESS)
; mechanical circulatory support (MCS)
1. Introduction
Cardiac arrest (CA) still claims a staggering number of lives annually, causing widespread disabilities over six decades of CPR employment [1,2].
Current CPR modalities may combine mid-sternal chest compressions (manually, mechanically); automated external defibrillators (AEDs), ventilation and invasive procedures like drug injection, implantable cardioverter defibrillators (IDC), extracorporeal membrane oxygenation (ECMO) or E-CPR, and cardiopulmonary bypass (CPB) [3,4,5,6,7,8,9,10,11].
Despite progress in CPR, out-of-hospital CA (OHCA) still results in a 30-day brain injury-free survival of approximately 2% [12,13,14].
Apart from E-CPR, which is still a work in progress, none of CPR modalities can achieve a single metabolic process before return of spontaneous circulation (ROSC).
Difficulties encountered in achieving ROSC with CPR can be attributed to the pathophysiological challenges posed by the CA state, summarized in (Figure 1).
As is known, ROSC occurs due to intracardiac action potentials requiring at least ≥ 15 mmHg coronary perfusion pressure, provided by adequate blood volumes (BV) dynamics, electrolytes, neurohumoral factors, and wall shear stresses [15]. Meanwhile, the arrested heart be-comes almost empty due to massive shifts of BV to low-pressure zones increasing the hepatosplanchnic venous capacitance. Also, the heart will be pulled even further away from the sternum by the cardiotorsal gravitational effect in the supine position. In addition, vigorous mid-sternal chest compressions, disregarding the cylindrical ribcage biomechanics, especially ribs’ orientations and axis of their movements, cause frequent CPR-related trauma [16].
Ultimately, performing CPR in a hemostatic condition induces a back-and-forth ineffective perfusion momentum.
As a result, most CPR survivors succumbing to multiorgan failure shortly due to inadequate organs perfusion during the procedure [17,18,19,20].
Such shortcomings of CPR represent a significant burden for global health authorities, requiring a thorough analysis of the entire structure of CA.
In-Depth Glance at CA
Literally, CA defines an abrupt discontinuity of organs perfusion following sudden asystole of the systemic ventricle, whether fibrillated, dysfunctional by cardiac-extracardiac events (e.g., myocardial injury, asphyxia), or knocked-out (e.g., Zwaardemaker-Libbrecht effect) [21,22,23,24,25,26].
This means that regardless of cardiac conditions, we must restore organs perfusion and metabolism as quickly as possible before irreversible cellular damage occurs [27]
Since salvage of cellular metabolism, either with rapid ROSC or E-CPR, depends on microcirculations controlled by endothelial shear stress (ESS)-induced mediators [28]
Therefore, in this study we present novel techniques implementing rational mobilizations of the massive stagnant BV, inducing physiological pulse-pressure, thus ESS across the aorta.
These include proven methods employing invasive as well as noninvasive pulsatile mechanical circulatory support (MCS), tested in beatless-heart and CA neonatal piglets, respectively [29,30,31,32,33]. In addition, a novel chest compression technique inducing an intracardiac hemorheological effect with adequate BV promoting less traumatic ROSC has recently been used in two drownings [34,35].
Our aim is to corroborate ESS as a potentially effective method to significantly improve the dismal outcomes of CA.
2. Results
Novel Concept
ESS-mediated endothelial functions are mainly generated by the cardiopulmonary pump through the closed pressurized hydraulic left and right heart-circuits. Under the hydrostatic state of CA, the human body (Soma) becomes like a container composed of an inner sphere (A) containing stagnant amounts of fluids (blood, air,) surrounded by a barrier sphere (B) of endothelium (vascular, alveolar), overlapped by an outer sphere (C) of covering layers e.g., muscles, ribcage… (Somarheology theory) [29,30]. Therefore, creating a shear momentum across (A) inducing ESS at (B) can be achieved by direct intraluminal stimuli or indirect extraluminal impacts on (C) with pulsatile MCS.
STUDIES
To address factors compromising rapid ROSC as well as ESS suppression by conventional E-CPR during CA. Details are available in the corresponding references of each study.
1- A noninvasive MCS composed of multi-layer Vest and Corset driven by a low-pressure alternating pulsatile generator. Functionally, the device depicted in (Figure 2), can induce extracorporeal pulsatile impacts on several covering C-zones, circulating a massive amount of stagnant BV in regular rhythm. As detailed in references [29,30], prototypes were used in refractory CA models (≥20min). Results showed significant hemodynamics improvement, presented in (Figure 3), with near-physiological AP (systolic AP ≥100mmHg) and improved cerebral perfusion manifested by recovered carotid artery echo-doppler. In addition, a laser flowmeter (Perimed PeriScan PIM 3 System) measurements from the tip of the tongue showed significant improvements in microcirculation. There were increased urine output and global vasodilation compensated with IV fluids (1–2 L). The TUNEL test showed inferior apoptotic cells in the treated animal with an obvious dilation of the intracardiac coronary bed (Figure 4).
2- Invasive MCS (pulsatile Tube) tested as pulsatile CPB versus conventional CPB in beatless-heart model [31,32,33]. Fourteen neonatal piglets were divided into three groups: Group I (Gr-I, n=6) underwent pulsatile CPB at 100 bpm. Group II (Gr-II, n=6) underwent non-pulsatile CPB, with all subjects in these groups exposed to normothermic CPB for 120 minutes. A third sham group (n=2) technically managed like the other groups but without CPB. Hemodynamic, biochemical and histopathological data were collected and compared between groups. These include post-sternotomy insertion of right atrium, left atrium, left internal mammary and intra-infundibular catheters, for RAP, LAP, AP and PAP measurements, respectively. Cardiac output (CO) measured with transit time probe temporary placed around the PA (Transonic System Inc. Flowmeter). Cardiac index (CI), systemic vascular resistance index (SVRI) and pulmonary vascular resistance index (PVRI) were calculated according to the following formulae: SVRI= (mean AP-RAP)/CI X 79.9; PVRI= (mean PA-LAP)/CI X 79.9; CI=CO/Weight. Endothelial function and vasorelaxation (induced by acetylcholine and nitroprusside) were assessed in segments collected from the pulmonary artery (PA), carotid artery (CA), femoral artery (FA), and renal artery (RA) in all groups. Apoptosis was evaluated using the TUNEL test on myocardial and pulmonary tissue samples collected from all groups. Data collection points included: before CPB (T0), at the start of CPB (T1), one hour after CPB (T2), and at the end of CPB (T3). Results: As shown in (Figure 5), the device induced near-physiological AP (≥80mmHg) with a mean pulse-pressure of 46±7.55 mmHg in Gr-I versus 1.6±0.54 mmHg in the steady-flow Gr-II (P<0.05). SVRI was 1.372±0.35 versus 3.140±0.344 dynes.s.cm-5/m2 in Gr-I versus Gr-II, respectively. PVRI was 0.3±0.06 versus 0.85±0.05 dynes.s.cm-5/m2 in Gr-I versus Gr-II, respectively (P<0.05). Unlike Gr-II, acetylcholine reactivity test showed significant endothelial function restoration of endothelial function almost closer to sham in Gr-I as presented in (Figure 6) and (Table 1). The TUNEL test presented (Figure 7) revealed myocardial apoptotic cells in Gr-II and none in Gr-I as well as Sham. Hemolysis were higher and lactic acid were lower in Gr-I versus Gr-II (p≤0.05).
3- Novel technique of chest compressions through the 5th intercostal space while placing the victim in the left lateral decubitus position to bypass the sternal barrier, with wrapped abdomen and raised legs. In short, refill-recoil-rebound the chest (3R /CPR), within the axis of the cylindrical ribcage will create a sudden intracardiac water hammer-like mechanism with an adequate BV hemorheological-biochemical effect promoting less-traumatic ROCS. The technique was recently used successfully by a skilled lifeguard instructor as a last-chance intervention in two drownings incidents after failed CPR. ROSC occurred instantly with the refill maneuver in one victim, and several times with recoil-rebound chest compressions in another victim despite CA ≥ 25 minutes with ultimately severely depleted myocardial oxygen reserves and alcoholemia [34,35].
3. Discussion
Results demonstrated the feasibility and potential advantages of rapid CFR-inducing ESS in significantly improving hemodynamics, microcirculation, regardless of heartbeats.
Notably, rapid CFR-inducing ESS, either with the lifeguard’s Heimlich maneuver or with the cardiac surgeons’ CPB, induces ROSC in ≥70% of drowning victims, and in ≥90% of open-heart patients, respectively [36]. This phenomenon was also observed in our study with shorter durations of CA (≤8 minutes), when immediate ROSC occurred with first pulsations of abdominal Corset. Similarly, we modeled the novel chest compressions technique in order to create intracardiac ESS with adequate BV. Unlike CPR, the technique adapts to and overcomes the pathophysiological conditions of CA (Figure 1). Thus, it can promote rapid ROSC in complete harmony with thoracic biomechanics, thereby less-traumatic, less-exhausting for rescuers. In addition, the rescuer can secure the victim’s airway and easily check for heartbeats so as not to confuse CA with syncope or cardiogenic shock.
As stated by Feynman and demonstrated in our study, ESS-mediated endothelial function must be induced according to the Newton’s principles by maintaining an almost physiological arterial pulse-pressure [37].
In both animal studies, near-physiological AP was successfully induced in beatless-heart, either invasively or noninvasively with pulsatile MCSs, in correspondence to cardiovascular biophysics and pathophysiological conditions.
For example, the right-heart circuit can adjust pressurized BV and ESS at five different anatomical zones to maintain low-level remodeling [38]. So, it is fundamental keep its low-level remodeling as delivery of ESS in high pulse-pressure can induce serious irreversible conditions such as Eisenmenger syndrome [39]. Therefore, in the 1st study, ESSs were delivered in alternating low-pressure pulsatile impacts on multiple C-zones at the right-heart-side, at a rate of 40 bpm according to the capillary pressure cycle [40].
At the left-heart circuit, ESS inside the Valsalva sinuses determines coronary ostia morphogenesis and may contribute to a severe hemodynamic deterioration [40]. Accordingly, in the 2nd study, pulsatile impacts of ESS were delivered from the aortic root to minimize the constitution of intravascular vortices [41]. However, this study showed significant hemolysis in the treated group (Gr-I) caused by the preliminary concept, which was subsequently resolved and tested effectively [33].
On the other hand, current CPR procedures contradict the most fundamental principles of hydrostatic circuits, leading to illusory and inconclusive benefits for CA victims. Oddly, most recent CPR publications ignore previously reported hemostatic data showing flattened zero AP and central venous pressure (CVP) exceeding ≥80 mmHg during chest compressions [42,43]. Such severe hemostatic disorders compromise invasive CPR procedures such as drug injections or ventilation due lack of interalveolar gas-exchanges [44].
Therefore, it is strongly recommended to use E-CPR promptly to salvage cellular metabolism instead of exhorting ROSC through a pointless Yoyo-perfusion mode of CPR [45]. However, E-CPR remains an invasive and time-consuming procedure requiring skilled squad and ultra-sound-guided installation through flattened arteries, which compromises its effectiveness in OHCA. In addition, suppression of ESS by the constant flow of E-CPR creates a vicious emerging cycle of energy losses and endothelial dysfunction. This phenomenon could be aggravated by ROSC, leading to countercurrent intravascular vortices (Reynolds stresses) [46].
These issues were addressed in our study demonstrating significant restoration of endothelial function, confirmed by histopathological and biochemical results in piglets, animal models well-known for lack of coronary network [47]. Interestingly, as shown in (Figure 5), the supposedly stunned PA due to no-flow perfusion, in both groups, showed quasi complete recovery, like sham. These prove the crucial role of ESS in improving endothelial function via pulmonary collaterals and myocardial microcirculatory pathways. Evidence of restored endothelial function in vitro as demonstrated in (Table 1) and (Figure 6 and Figure 7), can significantly improve postarrest multiorgan failure mortality caused by poor CPR perfusion.
Limitations: To avoid tedious repetitions of published materials and methods available in the literature for further details,, we limited our study to the means and potential for restoring ESS-mediated endothelial function under hemostatic condition of CA.
4. Conclusions
Optimal goal of CPR, namely rapid ROSC while ensuring adequate perfusion of vital organs, remains elusive, leading to high mortality and morbidity. Prioritizing rapid CFR-inducing ESS over exhorting heartbeat return may improve the dismal outcomes of CA.
5. Patents
S.N. author of several patents, available from the corresponding media.
Author Contributions
S.N. developed the concept, designed and conducted experimental studies and wrote the corresponding publications.
Funding
None.
Institutional Review Board Statement
“Not applicable”.
Informed Consent Statement
“Not applicable”.
Data Availability Statement
Data are available upon reasonable request.
Acknowledgments
We thank our Colleagues and Friends from Sun Yat Sen University, GZ, China; HEGP and Marie-Lannelongue Hospitals, Universities of Paris, France.
Conflicts of Interest
Nothing to declare.
Abbreviations
The following abbreviations are used in this manuscript:
| CA | Cardiac arrest |
| CPR | Cardiopulmonary resuscitation |
| AED | Automated external defibrillators |
| ICD | Implantable cardioverter defibrillators |
| ECMO | Extracorporeal membrane oxygenation |
| CPB | Cardiopulmonary bypass |
| OHCA | Out-of-hospital cardiac arrest |
| ROSC | Return of spontaneous circulation |
| ESS | Endothelial shear stress |
| CFR | Circulatory flow restoration |
| MCS | Mechanical circulatory support |
| bpm | beats per minute |
| BV | Blood volume |
| AP | Arterial pressure |
| PA | Pulmonary artery |
| PAP | Pulmonary artery pressure |
| RV | Right ventricle |
| LV | Left ventricle |
| IV | Intravenous |
| CVD | Cardiovascular disease |
| CO | Cardiac output |
| CI | Cardiac index |
References
- Sandroni, C.; Cronberg, T.; Sekhon, M. Brain injury after cardiac arrest: pathophysiology, treatment, and prognosis. Intensive Care Med. 2021, 47, 1393–1414. [Google Scholar] [CrossRef] [PubMed]
- Toy, J.; Friend, L.; Wilhelm, K.; Kim, M.; Gahm, C.; Panchal, A.R.; Dillon, D.; Donofrio-Odmann, J.; Montroy, J.C.; Gausche-Hill, M.; Bosson, N.; Coute, R.; Schlesinger, S.; Menegazzi, J. Evaluating the current breadth of randomized control trials on cardiac arrest: A scoping review. J Am Coll Emerg Physicians Open. 2024, 5, e13334. [Google Scholar] [CrossRef] [PubMed]
- Truong, H.T.; Low, L.S.; Kern, K.B. Current Approaches to Cardiopulmonary Resuscitation. Curr Probl Cardiol. 2015, 40, 275–313. [Google Scholar] [CrossRef] [PubMed]
- Peberdy, M.A.; Gluck, J.A.; Ornato, J.P.; Bermudez, C.A.; Griffin, R.E.; Kasirajan, V.; Kerber, R.E.; Lewis, E.F.; Link, M.S.; Miller, C.; Teuteberg, J.J.; Thiagarajan, R.; Weiss, R.M.; O’Neil, B. American Heart Association Emergency Cardiovascular Care Committee; Council on Cardiopulmonary, Critical Care, Perioperative, and Resuscitation; Council on Cardiovascular Diseases in the Young; Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular and Stroke Nursing; and Council on Clinical Cardiology. Cardiopulmonary Resuscitation in Adults and Children With Mechanical Circulatory Support: A Scientific Statement From the American Heart Association. Circulation. 2017, 135, e1115–e1134. [Google Scholar] [CrossRef]
- Homma, P.C.M.; de Graaf, C.; Tan, H.L.; Hulleman, M.; Koster, R.W.; Beesems, S.G.; Blom, M.T. Transfer of essential AED information to treating hospital (TREAT). Resuscitation. 2020, 149, 47–52. [Google Scholar] [CrossRef]
- Deakin, C.D.; Koster, R.W. Chest compression pauses during defibrillation attempts. Curr Opin Crit Care. 2016, 22, 206–11. [Google Scholar] [CrossRef]
- van Eijk, J.A.; Doeleman, L.C.; Loer, S.A.; Koster, R.W.; van Schuppen, H.; Schober, P. Ventilation during cardiopulmonary resuscitation: A narrative review. Resuscitation. 2024, 203, 110366. [Google Scholar] [CrossRef]
- Kubo, A.; Hiraide, A.; Shinozaki, T.; Shibata, N.; Miyamoto, K.; Tamura, S.; Inoue, S. Impact of epinephrine on neurological outcomes in out-of-hospital cardiac arrest after automated external defibrillator use in Japan. Sci Rep. 2025, 15, 274. [Google Scholar] [CrossRef]
- Morton, M.B.; Mariani, J.A.; Kistler, P.M.; Patel, H.; Voskoboinik, A. Transvenous versus subcutaneous implantable cardioverter defibrillators in young cardiac arrest survivors. Intern Med J. 2023, 53, 1956–1962. [Google Scholar] [CrossRef]
- Kobayashi, R.L.; Gauvreau, K.; Alexander, P.M.A.; Teele, S.A.; Fynn-Thompson, F.; Lasa, J.J.; Bembea, M.; Thiagarajan, R.R.; American Heart Association’s (AHA) Get With The Guidelines-Resuscitation (GWTG-R) Investigators. Higher Survival With the Use of Extracorporeal Cardiopulmonary Resuscitation Compared With Conventional Cardiopulmonary Resuscitation in Children Following Cardiac Surgery: Results of an Analysis of the Get With The Guidelines-Resuscitation Registry. Crit Care Med. 2024, 52, 563–573. [Google Scholar] [CrossRef]
- Sawamoto, K.; Tanno, K.; Takeyama, Y.; Asai, Y. Successful treatment of severe accidental hypothermia with cardiac arrest for a long time using cardiopulmonary bypass - report of a case. Int J Emerg Med. 2012, 5, 9. [Google Scholar] [CrossRef] [PubMed]
- Yan, S.; Gan, Y.; Jiang, N.; Chen, Y.; Luo, Z.; Zong, Q.; Chen, S.; Lv, C. The global survival rate among adult out-of-hospital cardiac arrest patients who received cardiopulmonary resuscitation: a systematic review and meta-analysis. Crit Care. 2020, 24, 61. [Google Scholar] [CrossRef]
- Rubertsson, S.; Lindgren, E.; Smekal, D.; Östlund, O.; Silfverstolpe, J.; Lichtveld, R.A.; Boomars, R.; Ahlstedt, B.; Skoog, G.; Kastberg, R.; Halliwell, D.; Box, M.; Herlitz, J.; Karlsten, R. Mechanical chest compressions and simultaneous defibrillation vs conventional cardiopulmonary resuscitation in out-of-hospital cardiac arrest: the LINC randomized trial. JAMA. 2014, 311, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Avishay, D.M.; Jones, C.R.; Shaikh, J.D.; Kaur, R.; Aljadah, M.; Kichloo, A.; Shiwalkar, N.; Keshavamurthy, S. Sudden cardiac death: epidemiology, pathogenesis and management. Rev Cardiovasc Med. 2021, 22, 147–158. [Google Scholar] [CrossRef]
- Reynolds, J.C.; Salcido, D.D.; Menegazzi, J.J. Coronary perfusion pressure and return of spontaneous circulation after prolonged cardiac arrest. Prehosp Emerg Care 2010, 14, 78–84. [Google Scholar] [CrossRef]
- Arbogast, K.B.; Maltese, M.R.; Nadkarni, V.M.; Steen, PA.; Nysaether, J.B. Anterior-posterior thoracic force-deflection characteristics measured during cardiopulmonary resuscitation: comparison to post-mortem human subject data. Stapp Car Crash J. 2006, 50, 131–45. [Google Scholar]
- Panchal, A.R.; Bartos, J.A.; Cabañas, J.G.; Donnino, M.W.; Drennan, I.R.; Hirsch, K.G.; Kudenchuk, P.J.; Kurz, M.C.; Lavonas, E.J.; Morley, P;T.; O’Neil, B.J.; Peberdy, M.A.; Rittenberger, J.C.; Rodriguez, A.J.; Sawyer, K.N.; Berg, K.M.; Adult basic and advanced life support writing group. Part 3: Adult Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2020,142(16-suppl-2),S366-S468. [CrossRef]
- Berg, K.M.; Cheng, A.; Panchal, A.R.; Topjian, A.A.; Aziz. K.; Bhanji, F.; Bigham, B.L.; Hirsch, K.G.; Hoover, A.V.; Kurz, M.C.; Levy, A.; Lin, Y.; Magid. D.J.; Mahgoub, M.; Peberdy, M.A.; Rodriguez, A.J.; Sasson. C.; Lavonas, E.J.; Adult Basic and Advanced Life Support, Pediatric Basic and Advanced Life Support, Neonatal Life Support, and Resuscitation Education Science Writing Groups. Part 7: Systems of Care: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation.2020,142(16_suppl_2),S580-S604. [CrossRef]
- Oeser, C. Cardiac resuscitation: Continuous chest compressions do not improve outcomes. Nat Rev Cardiol. 2016, 13, 5. [Google Scholar] [CrossRef]
- Srinivasan, N.T.; Schilling, R.J. Sudden Cardiac Death and Arrhythmias. Arrhythm Electrophysiol Rev. 2018, 7, 111–117. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- de Noronha, S.V.; Sharma, S.; Papadakis, M.; Desai, S.; Whyte, G.; Sheppard, M.N. Aetiology of sudden cardiac death in athletes in the United Kingdom: a pathological study. Heart. 2009, 95, 1409–14. [Google Scholar] [CrossRef]
- Link, M.S. Mechanically induced sudden death in chest wall impact (commotio cordis). Prog Biophys Mol Biol. 2003, 82, 175–86. [Google Scholar] [CrossRef]
- Thygesen, K.; Uretsky, B.F. Acute ischaemia as a trigger of sudden cardiac death. Eur Heart J. 2004, 6, D88–D90. [Google Scholar] [CrossRef]
- Deshpande, S.R.; Herman, H.K.; Quigley, P.C.; Shinnick, J.K.; Cundiff, C.A.; Caltharp, S. Shehata, B.M. Arrhythmogenic Right Ventricular Cardiomyopathy/Dysplasia (ARVC/D): Review of 16 Pediatric Cases and a Proposal of Modified Pediatric Criteria. Pediatr Cardiol. 2016,37,646-55. [CrossRef]
- Surawicz, B.; Gettes, L.S. Two mechanisms of cardiac arrest produced by potassium. Circ Res. 1963, 12, 415–21. [Google Scholar] [CrossRef]
- Donoghue, A.J.; Nadkarni, V.; Berg, R.A.; Osmond, M.H.; Wells, G.; Nesbitt, L.; Stiell, I.G.; CanAm Pediatric Cardiac Arrest Investigators. Out-of-hospital pediatric cardiac arrest: an epidemiologic review and assessment of current knowledge. Ann Emerg Med. 2005, 46, 512-22. [Google Scholar] [CrossRef]
- van Empel, V.P.; Bertrand, A.T.; Hofstra, L.; Crijns, H.J.; Doevendans, P.A.; De Windt, L.J. Myocyte apoptosis in heart failure. Cardiovasc Res. 2005, 67, 21–9. [Google Scholar] [CrossRef]
- Manning, D.; Rivera, E.J.; Santana, L.F. The life cycle of a capillary: Mechanisms of angiogenesis and rarefaction in microvascular physiology and pathologies. Vascul Pharmacol. 2024, 156, 107393. [Google Scholar] [CrossRef]
- Nour. S.; Carbognani, D.; Chachques, J.C. Circulatory flow restoration versus cardiopulmonary resuscitation: new therapeutic approach in sudden cardiac arrest. Artif Organs. 2017,41,356-366.
- Nour, S. Endothelial shear stress enhancements: a potential solution for critically ill Covid-19 patients. BioMed Eng OnLine. 2020, 19, 91. [Google Scholar] [CrossRef]
- Nour, S. Preliminary study of pulsatile versus conventional pediatric cardiopulmonary bypass with a new device tested in piglets. Univ. of Paris XI, France. Master’s degree in Surgical Sciences (2003). University of Paris-Saclay, France.
- Nour, S. Shear Stress, Energy losses and Cost: The Resolved Dilemma of Pediatric Heart Lung Machines with a Pulsatile tube. 16th Annual Meeting of The Asian Society For Cardiovascular And Thoracic Surgery. SINGAPORE. 13-16 March 2008.
- Nour, S.; Liu, J.; Dai, G.; Carbognani, D.; Yang, D.; Wu, G.; Wang, Q.; Chachques, J.C. Shear stress, energy losses, and costs: a resolved dilemma of pulsatile cardiac assist devices. Biomed Res Int. 2014, 2014, 651769. [Google Scholar] [CrossRef]
- Nour, S. Time to Resuscitate Cardiopulmonary Resuscitation: The 3R/CPR Refill-Recoil-Rebound. Cardiology and Angiology: An International Journal. 2022, 11, 363–75. [Google Scholar] [CrossRef]
- Tsoungani, G.; Nour, S. Application of Refill, Recoil, Rebound (3R) as a Novel Chest Compression Technique in Cardiopulmonary Resuscitation; Report of Two Cases. Arch Acad EmergMed. 2025, 13, e30. [Google Scholar] [CrossRef]
- Heimlich, H.J. Subdiaphragmatic pressure to expel water from the lungs of drowning persons. Ann Emerg Med. 1981, 10, 476–480. [Google Scholar] [CrossRef]
- Feynman, R.P.; Leighton, R.B.; Sands, M. The Feynman Lectures on Physics. Vol. 1 (2nd ed.). Pearson/Addison-Wesley, USA, 2005. ISBN 0805390499.
- Nour, S.; Zhensheng, Z.; Wu, G.; Chachques, J.C.; Carpentier, A.; Payen, D. The forgotten driving forces in right heart failure: new concept and device. Asian Cardiovasc Thorac Ann. 2009, 17, 525–30. [Google Scholar] [CrossRef]
- D’Alto, M.; Vizza, C.D.; Romeo, E.; Badagliacca, R.; Santoro, G.; Poscia, R.; Sarubbi, B.; Mancone, M.; Argiento, P.; Ferrante, F.; Russo, M.G.; Fedele, F.; Calabrò, R. Long term effects of bosentan treatment in adult patients with pulmonary arterial hypertension related to congenital heart disease (Eisenmenger physiology): safety, tolerability, clinical, and haemodynamic effect. Heart. 2007, 93, 621–5. [Google Scholar] [CrossRef]
- Mueller, M.; Holzer, M.; Losert, H.; Grassmann, D.; Ettl, F.; Gatterbauer, M.; Magnet, I.; Nuernberger, A.; Kienbacher, CL.; Gelbenegger, G.; Girsa, M.; Herkner, H.; Krammel, M. The association of capillary refill time and return of spontaneous circulation during out-of-hospital cardiac arrest: an observational study. Crit Care. 2025, 29, 37. [Google Scholar] [CrossRef]
- Nour, S.; Dai, G.; Carbognani, D.; Feng, M.; Yang, D.; Lila, N.; Chachques, J.C.; Wu, G. Intrapulmonary shear stress enhancement: a new therapeutic approach in pulmonary arterial hypertension. Pediatr Cardiol. 2012, 33, 1332–42. [Google Scholar] [CrossRef] [PubMed]
- Hutchins, G.M.; Kessler-Hanna, A.; Moore, G.W. Development of the coronary arteries in the embryonic human heart. Circulation. 1988, 77, 1250–7. [Google Scholar] [CrossRef]
- Nour, S. Flow and Rate: Concept and Clinical Applications of a New Hemodynamic Theory. In Biophysics, Misra, A.N.; Intech: Rijeka, Croatia, 2012; pp.1-62. Crossref. [CrossRef]
- Putzer, G.; Martini, J.; Spraider, P.; Abram, J.; Hornung, R.; Schmidt, C., Bauer, M.; Pinggera, D.; Krapf, C.; Hell, T.; Glodny, B.; Helbok, R.; Mair, P. Adrenaline improves regional cerebral blood flow, cerebral oxygenation and cerebral metabolism during CPR in a porcine cardiac arrest model using low-flow extracorporeal support. Resuscitation. 2021,168,151-159.
- Swenson, R.D.; Weaver, W.D.; Niskanen, R.A.; Martin, J.; Dahlberg, S. Hemodynamics in humans during conventional and experimental methods of cardiopulmonary resuscitation. Circulation. 1988, 78, 630–9. [Google Scholar] [CrossRef] [PubMed]
- Perkins, G.D.; Ji, C. Deakin, C.D.; Nolan, J.P.; Scomparin, C.; Regan, S.; Long, J.; Slowther, A.; Pocock, H.; Black, J.J.M.; Moore, F.; Fothergill, R.T.; Rees, N.; O’Shea, L.; Docherty, M.; Gunson, I.; Han, K.; Charlton, K.; Finn, J.; Petrou, S.; Stallard, N.; Gates, S.; Lall, R.; PARAMEDIC2 Collaborators. A randomized trial of epinephrine in out-of-hospital cardiac arrest. N Engl J Med. 2018,379,711-72.
- Pound, G.; Eastwood, G.M.; Jones, D.; Hodgson, C.L.; ANZ-CODE Investigators. ANZ-CODE management committee; Sites and Site Investigators. Potential role for extracorporeal membrane oxygenation cardiopulmonary resuscitation (E-CPR) during in-hospital cardiac arrest in Australia: A nested cohort study. Crit Care Resusc. 2023,25,90-96. [CrossRef]
- Jones, S.A. A relationship between Reynolds stresses and viscous dissipation: implications to red cell damage. Ann Biomed Eng. 1995, 23, 21–8. [Google Scholar] [CrossRef]
- Gorge, G.; Schmidt, T.; Ito, B.R.; Pantely, G.A.; Schaper, W. Microvascular and collateral adaptation in swine hearts following progressive coronary artery stenosis. Basic Res Cardiol. 1989, 84, 524–35. [Google Scholar] [CrossRef]
Figure 1.
Schema demonstrating outcomes of cardiopulmonary resuscitation (CPR) collision with the pathophysiological conditions of cardiac arrest (CA).
Figure 1.
Schema demonstrating outcomes of cardiopulmonary resuscitation (CPR) collision with the pathophysiological conditions of cardiac arrest (CA).
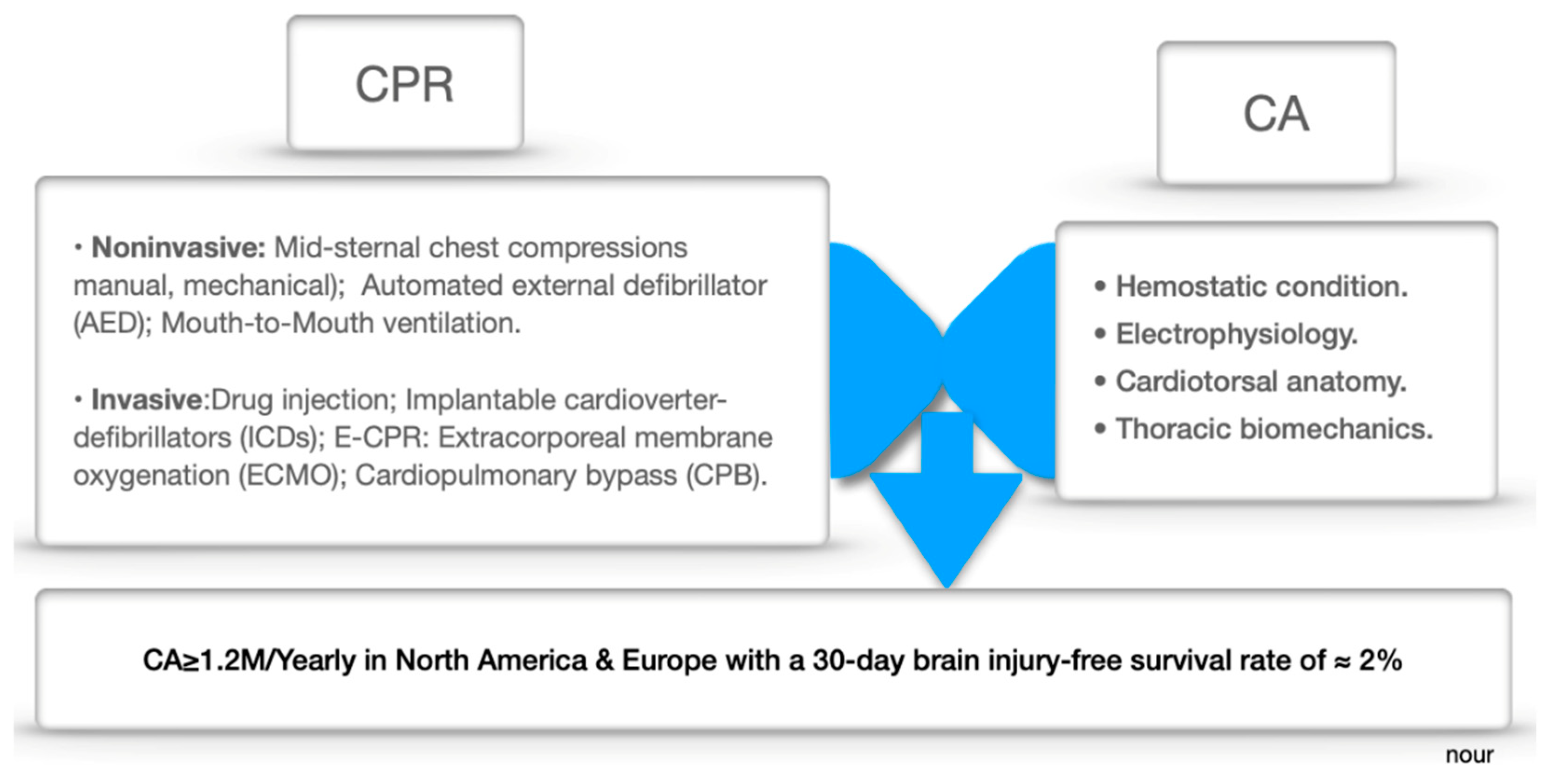
Figure 2.
Diagram representing the mechanism of the CFR device alternating pulsations between Corset and Vest on several covering zones (C): Mediastinal (C-I), Parenchyma (C-II), Diaphragm C-III, and hepatosplanchnic (C-IV) compartments.
Figure 2.
Diagram representing the mechanism of the CFR device alternating pulsations between Corset and Vest on several covering zones (C): Mediastinal (C-I), Parenchyma (C-II), Diaphragm C-III, and hepatosplanchnic (C-IV) compartments.
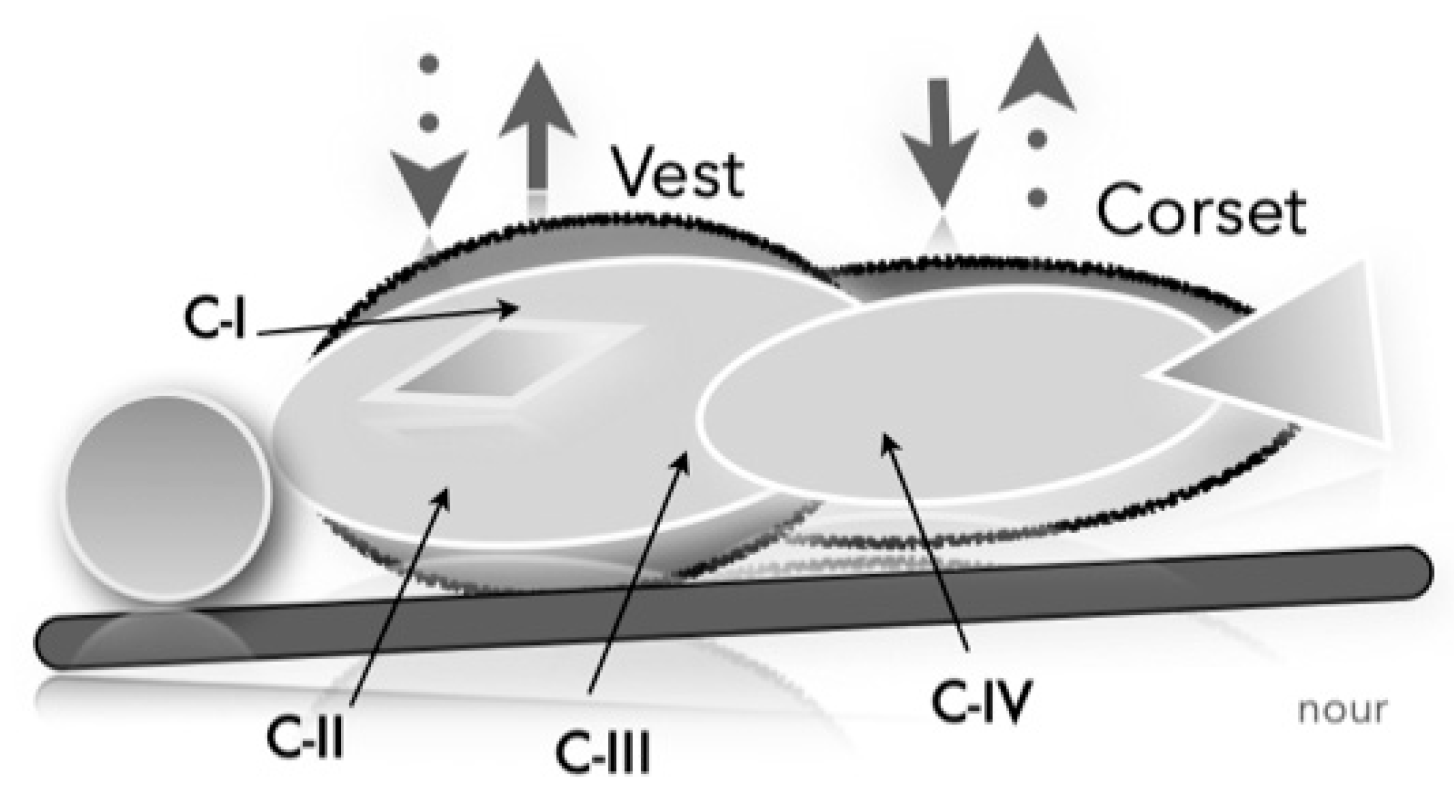
Figure 3.
Hemodynamic data obtained in refractory CA model (≥30min) with noninvasive MCS, showing near-physiological AP (middles line) and carotid artery flow (lower line), without return of heartbeats (upper line).
Figure 3.
Hemodynamic data obtained in refractory CA model (≥30min) with noninvasive MCS, showing near-physiological AP (middles line) and carotid artery flow (lower line), without return of heartbeats (upper line).
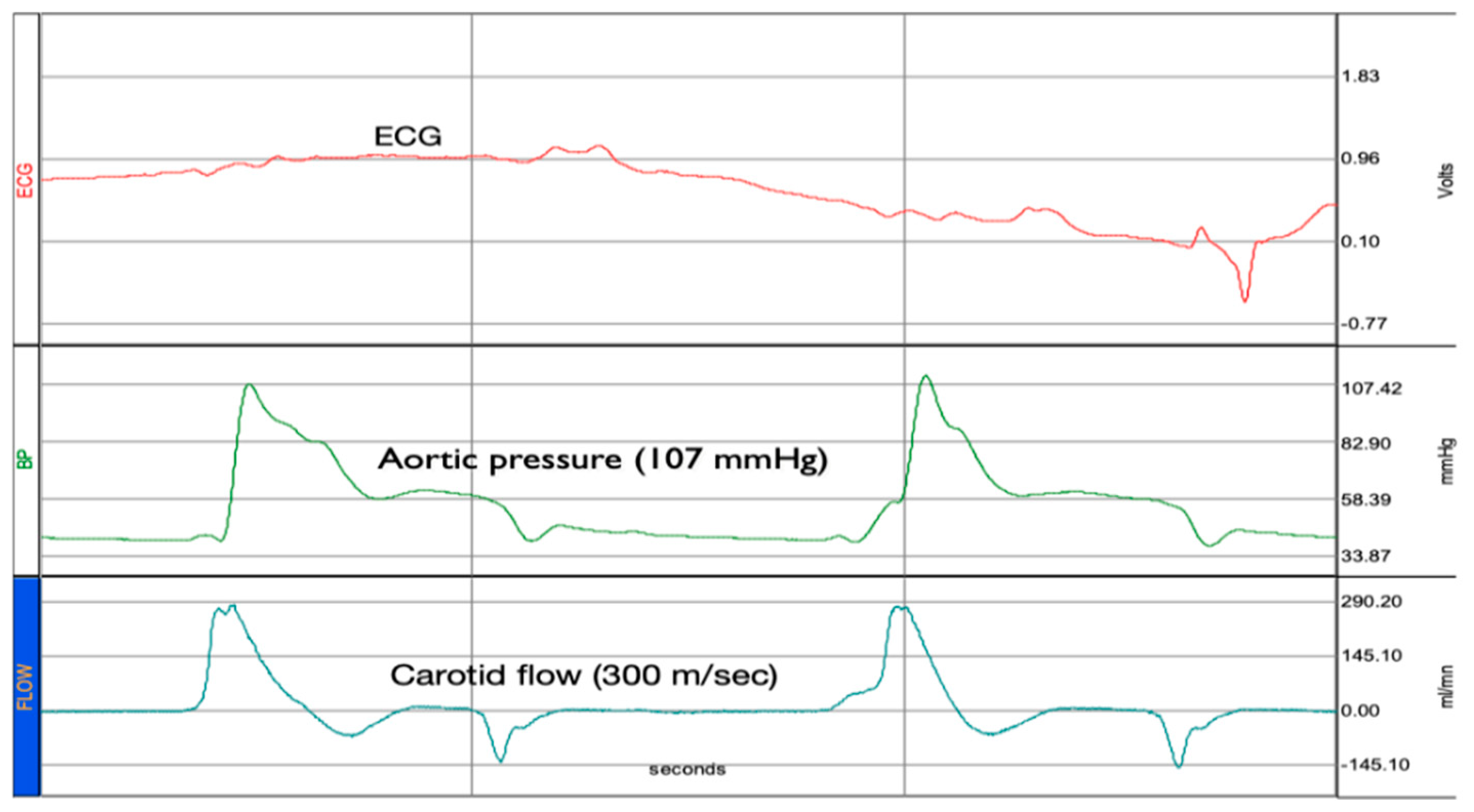
Figure 4.
TUNEL test (X400). Left image showing few myocardial apoptotic cells with dilated coronary bed in same treated animal model (CA with asphyxia ≥30min). Right image shows myocardial apoptosis in animal model treated with conventional CPR after 8 min of CA and kept alive for 6H.
Figure 4.
TUNEL test (X400). Left image showing few myocardial apoptotic cells with dilated coronary bed in same treated animal model (CA with asphyxia ≥30min). Right image shows myocardial apoptosis in animal model treated with conventional CPR after 8 min of CA and kept alive for 6H.
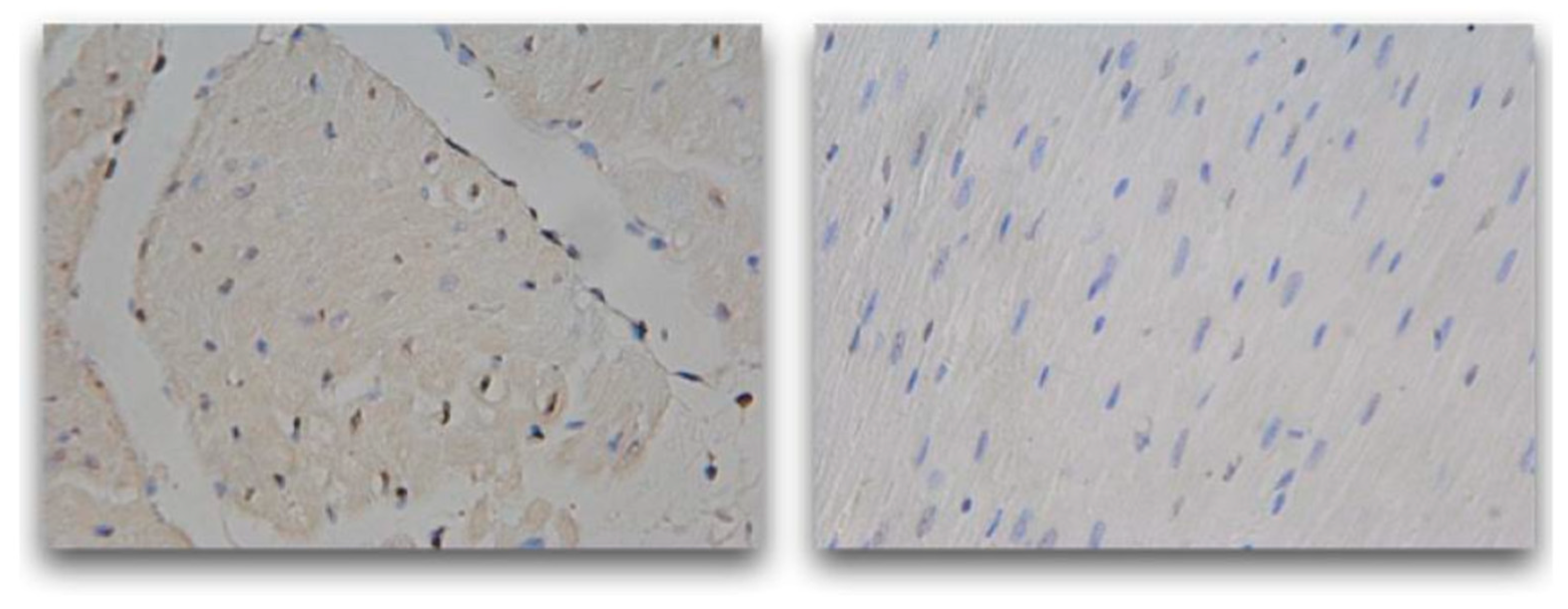
Figure 5.
Hemodynamic data of conventional (upper panel) versus pulsatile (lower panel) cardiopulmonary bypass (CBP). AP: Aortic pressure. PAP: Pulmonary artery pressure was 0 mmHg as the heart was fully discharged and taken over by CPB in both groups.
Figure 5.
Hemodynamic data of conventional (upper panel) versus pulsatile (lower panel) cardiopulmonary bypass (CBP). AP: Aortic pressure. PAP: Pulmonary artery pressure was 0 mmHg as the heart was fully discharged and taken over by CPB in both groups.
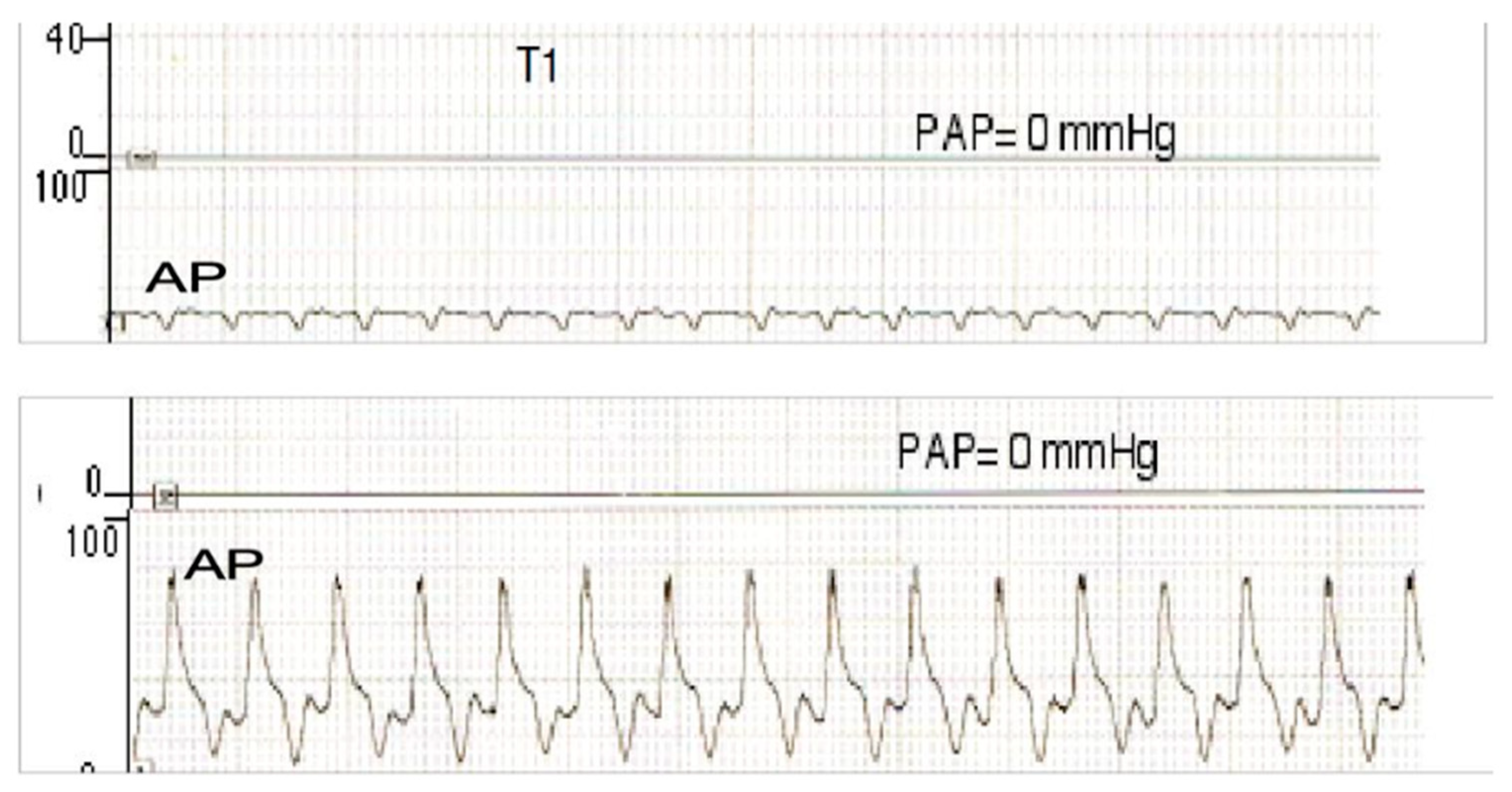
Figure 6.
Acetylcholine endothelial reactivity test, showing restored endothelial function in the pulsatile group, versus sham and control groups. P<0.01 (ANOVA test).
Figure 6.
Acetylcholine endothelial reactivity test, showing restored endothelial function in the pulsatile group, versus sham and control groups. P<0.01 (ANOVA test).
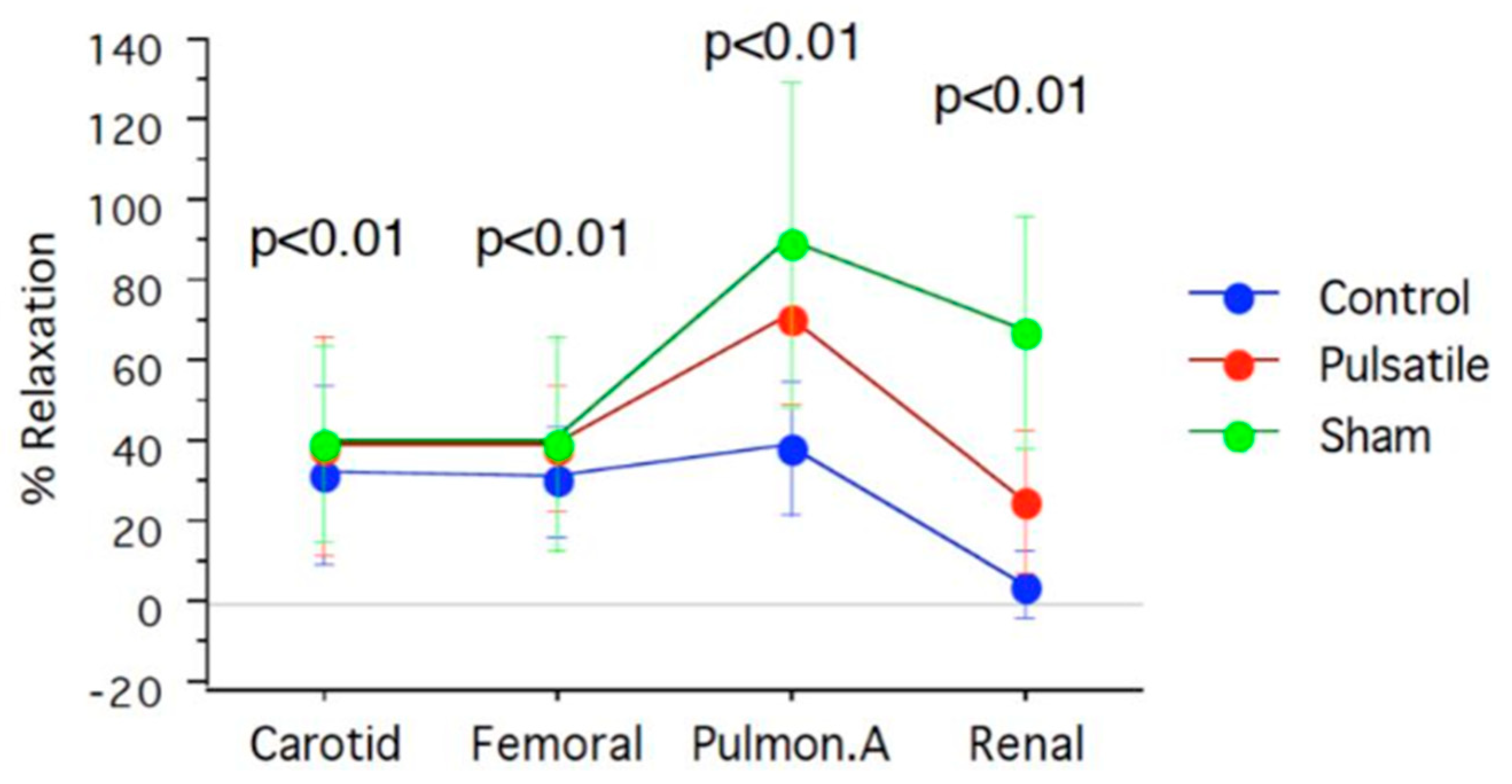
Figure 7.
TUNEL test, showing myocardial apoptotic cells in the control group (right image) versus pulsatile group (left image).
Figure 7.
TUNEL test, showing myocardial apoptotic cells in the control group (right image) versus pulsatile group (left image).
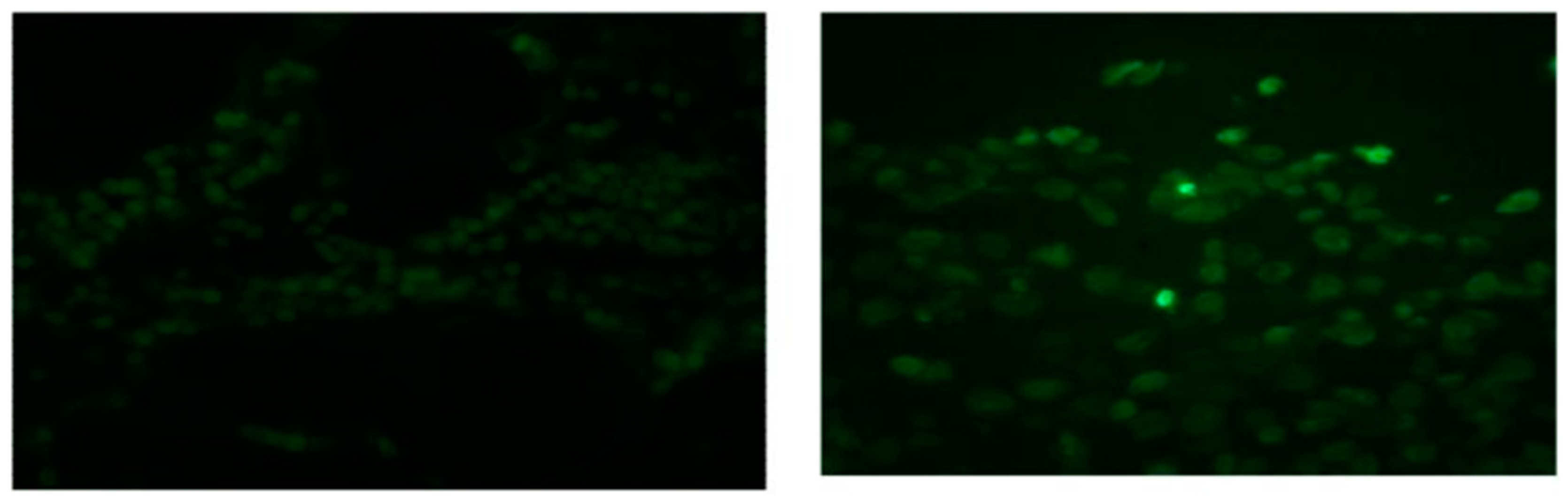

Table 1.
Acetylcholine endothelial reactivity test.
| Arterial segments | Sham | Pulsatile CPB | Control | Acetylcholine |
|---|---|---|---|---|
| Carotid | 40±24.4 | 39.4±27.6 | 32.3±22.03 | |
| Femoral | 40±26.7 | 39.3±15.6 | 30.6±14.2 | % |
| Pulmonary | 78±37.5 | 72.2±25.9 | 39.3±16.6 | |
| Renal | 67±28.9 | 26±17.7 | 5.3±8.7 |
Endothelial dependent vascular relaxation Acetylcholine Test in 3 groups of newborn piglets, underwent pulsatile and conventional cardiopulmonary bypass (CPB) and Sham. P<0.01, ANOVA test.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



