Submitted:
31 March 2025
Posted:
01 April 2025
You are already at the latest version
Abstract
Cancer remains a leading global health challenge, with conventional diagnostic and treatment methods often lacking precision and adaptability. This review explores transformative advancements that are reshaping oncology by addressing these limitations. It begins with an overview of cancer’s complexity, emphasizing the shortcomings of conventional tools such as imaging and chemotherapy, which frequently fail to deliver targeted care. The discussion then shifts to biomarkers, a groundbreaking frontier in early detection, enabling the identification of unique biological signatures that signal the presence of cancer with heightened sensitivity. Building on this foundation, the review examines personalized molecular therapies, which target the specific genetic and molecular vulnerabilities of tumors. These therapies not only enhance treatment efficacy but also minimize adverse effects, offering patients improved outcomes and quality of life. By integrating biomarker-driven diagnostics with tailored therapeutic strategies, a new paradigm of precision oncology emerges, bridging the gap between early detection and effective intervention. Real-world case studies highlight both successes such as significantly improved survival rates and persistent challenges, including accessibility and cost barriers. Looking ahead, the review outlines pathways to scale these innovations, emphasizing the critical need for robust infrastructure, sustained research investment, and equitable healthcare policies. It concludes by envisioning a future where biomarkers and personalized therapies converge to redefine cancer care, offering earlier detection, precise interventions, and better patient experiences. This work underscores the urgency of adopting cutting-edge approaches to overcome cancer’s persistent threats, paving the way for a more effective and humane era in oncology.
Keywords:
cancer diagnosis
; cancer treatment
; biomarkers
; molecular-targeted therapies
; oncology
; cancer challenges
1. Introduction
Cancer is a relentless enemy, a disease where cells go rogue, growing and dividing without the usual checks and balances that keep our bodies in harmony. Normally, cells follow a tight script: they grow when needed, divide to replace old ones, and die off through a process called apoptosis when their job is done [1]. But in cancer, this script gets scrambled sometimes by genetic mutations passed down through families, other times causes such as cigarette smoke, UV rays, or viruses like HPV [2]. The result Cells multiply uncontrollably, forming tumors that can stay local or, in the worst cases, break away and spread throughout the body in a process called metastasis [3]. It is a global crisis, claiming around 10 million lives each year, according to the World Health Organization (WHO), and the burden is not shared equally, 70% of those deaths happen in low- and middle-income countries where spotting cancer early or treating it effectively often feels like a distant dream [4].
For too long, cancer diagnosis has relied on tools that often fall short symptoms like fatigue or a persistent cough, are easily dismissed, and even when concerns arise, traditional tests can be unreliable, either producing false alarms or failing to detect real cancerous threats. But here is the good news: the future of cancer care is on the brink of a revolution, driven by two powerful allies’, biomarkers and personalized molecular-targeted therapies. These are not just upgrades to the old playbook; they are a whole new game, promising to catch cancer sooner and fight it smarter [5,6].
Think about how we have traditionally hunted for cancer. A patient feels off, maybe loses some weight or notices a lump, and the doctor orders a battery of tests like X-rays, biopsies, blood work. Too often, though, the disease stays silent in its early stages, hiding behind vague clues that could just as easily point to a cold or stress. By the time it is loud enough to detect, it is already dug in, tougher to treat, and more likely to have spread. Even our best tools have limits: a biopsy might miss a tiny tumor, an imaging scan might confuse a benign growth for something sinister, and in many parts of the world, those tools are not even an option [7]. This is where biomarkers come in, flipping the script on how we smartly find cancer. Picture a simple blood draw that acts like a crystal ball, revealing the disease before it even whispers a symptom. That is the magic of plasma proteomics a cutting-edge technique that filters through thousands of proteins floating in our blood to spot patterns unique to cancer. These protein signatures are like fingerprints, telling us not just that cancer is there, but what kind it is and how it might behave. Currently, researchers are already using this to pinpoint lung cancer in smokers or breast cancer in women with murky mammograms, catching it when it is still small and manageable. And it is not just about detection it is about precision. Furthermore, biomarkers can flag which patients will respond to certain drugs, sparing others from treatments that will not work and getting the right therapy to the right person faster [8,9].
However, finding cancer early is only half the battle; beating it is where personalized molecular-targeted therapies shine. In the past, we have thrown everything at cancer, surgery to cut it out, radiation to zap it, chemotherapy to poison it hoping something sticks. All these shotgun approaches can work, but they often hit healthy cells too, leaving patients exhausted, sick, and sometimes no better off [10,11]. For instance, in the past, all breast cancer patients were treated with a combination of surgery, chemotherapy, and radiation, regardless of their tumor types. However, researchers discovered that some breast cancers overexpress the HER2 (human epidermal growth factor receptor 2) protein, which promotes rapid tumor growth. Instead of using traditional chemotherapy alone, targeted drugs like trastuzumab (Herceptin) and pertuzumab (Perjeta) were developed to specifically block HER2 signaling [12]. This breakthrough dramatically improved survival rates for HER2-positive breast cancer patients while reducing the side effects associated with traditional chemotherapy. This approach exemplifies how personalized molecular-targeted therapies can identify and attack cancer more precisely, leading to better outcomes with fewer harmful effects on healthy cells [13].
Now, imagine a treatment that is more like a sniper rifle, zeroing in on the exact genetic traits driving a tumor while leaving the rest of the body alone. That is what molecular-targeted therapies do. They are built on the idea that every cancer has a molecular weak spot a mutated gene or overactive protein that keeps it alive [14]. Drugs like imatinib, for example, target a specific protein in chronic myeloid leukemia, turning a once-deadly disease into something people live with for decades [15].
These treatments not only improve survival but also reduce severe side effects, enhancing patients' quality of life. Their impact is even greater when combined with biomarkers. For example, a simple blood test might reveal that a lung cancer patient has an EGFR mutation, allowing doctors to bypass chemotherapy and prescribe a targeted drug like osimertinib, which directly targets the mutation. Real-world evidence supports this approach; a recent cervical cancer trial found that adding a brief round of chemotherapy before standard treatment reduced mortality by 40%, highlighting the potential of tweaking therapy based on a tumor’s unique profile [16,17].
This integrated approach is not science fiction; it is happening now, and it is advancing rapidly. Around the world, scientists are racing to map more biomarkers, from DNA fragments and RNA signals to tiny vesicles released by cells that could detect cancer early or predict treatment responses [18]. In laboratories from Boston to Bangalore, teams are decoding the molecular chaos of tumors, uncovering targets we did not even know existed a decade ago. Consider melanoma, the deadliest skin cancer; once a death sentence, it is now often tamed by drugs like pembrolizumab, which boosts the immune system to attack cancer cells flagged by specific biomarkers [19]. Meanwhile, technology like artificial intelligence (AI) is stepping in, analyzing data from millions of patients to spot biomarker patterns humans might miss. The result diagnostics that do not just say “cancer” but tell us which cancer, where it is headed, and how to stop it. What is more, the focus is not just on advancing science but on making these tools accessible to everyone, so that a farmer in rural Ethiopia or a factory worker in Ohio can benefit, not just patients in high-tech hospitals. While challenges remain; such as the setbacks caused by the COVID-19 pandemic and the difficulty of scaling these innovations globally there is no denying the momentum of progress [20,21].
This review offers a front-row seat to the future of cancer care. We explored how biomarkers and personalized molecular-targeted therapies are transforming treatment, from detecting cancer in its early, treatable stages to designing therapies that match to a tumor’s unique genetic makeup. These are not distant dreams; they are real, life-saving tools, with even more on the horizon. We delved into the science behind plasma proteomics and related technologies, showing how they are turning blood into a rich source of diagnostic clues. We highlighted therapies that directly target cancer, supported by stories of patients who have gone from hopeless to thriving. Finally, we looked ahead to how these innovations could reduce cancer’s global impact, bridge healthcare gaps, and shift the focus from treatment to prevention. Cancer has held the upper hand for too long, but by unlocking the potential of biomarkers and targeted therapies, we are not just fighting back, we are creating a future where cancer no longer wins.
2. The Limits of Today’s Cancer Diagnosis and Treatment Toolbox
Cancer remains one of the most complex and challenging diseases to diagnose and treat. Despite significant advancements in medical science, technology, and treatment strategies, there are still substantial limitations in today's cancer diagnosis and treatment toolbox. These limitations span across several areas, including early detection, personalized medicine, treatment efficacy, side effects, and accessibility [7,22]. For instance, investigating the primary site of a tumor is crucial for standardized cancer diagnosis and treatment. However, 3–5% of cancer cases remain without a determined primary site after pathological diagnosis, classified as cancer of unknown primary (CUP). The incidence of CUP ranges from 6 to 16 cases per 100,000 people, accounting for 2.3% to 7.8% of all malignant tumors, and it ranks as the fourth leading cause of cancer-related deaths. One of the biggest challenges in diagnosing CUP is the lack of effective detection methods. As a result, 20–50% of patients never have their primary site identified, and most CUP primary lesions discovered during autopsies are smaller than 1 cm; too small to be detected with current technologies [23,24]. This highlights the urgent need for more advanced diagnostic approaches to accurately determine the tumor’s origin and tissue type. Early and precise identification of the primary site is essential, as it allows clinicians to select the most effective treatment strategy based on the specific type of cancer, ultimately improving patient outcomes [25].
Cancer is a master of disguise, making early detection a significant challenge. Many conventional diagnostic tools lack accuracy, often failing to identify cancer in its earliest stages or provide a complete understanding of tumor biology (see Table 1) [26]. Imagine a patient feeling unusually fatigued for weeks, dealing with a persistent cough, or experiencing a lingering, dull ache. Seeking answers, they visit a doctor, only to find that early-stage cancer does not announce itself with clear warning signs; it hides behind vague symptoms like fatigue, weight loss, or mild discomfort, which could easily be mistaken for stress, a common cold, or a minor injury. A persistent cough might simply be bronchitis, or it could be an early sign of lung cancer quietly advancing. By the time symptoms become severe enough to raise concern, the disease may have already spread, turning a once-treatable condition into a life-threatening battle. This delay is not just unfortunate; it highlights a critical weakness in our approach to cancer detection. Relying on late-stage symptoms and diagnostic tests that are not sensitive enough means we often detect cancer too late, when treatment options are more limited and less effective [27,28].
Even when cancer is suspected, diagnosing it with precision remains a challenge. Doctors rely on various tools such as blood tests, X-rays, CT scans, and biopsies, but each has its own limitations [29]. For instance, consider mammograms, the standard screening method for breast cancer: they fail to detect about 1 in 5 cases in women with dense breast tissue, allowing tumors to grow unnoticed until they become more difficult to treat. Blood tests, such as the PSA test for prostate cancer, can indicate potential issues but are notorious for false positives, often leading to unnecessary anxiety and invasive follow-ups for what turns out to be harmless [30]. A 2020 UK study revealed that 30% of ovarian cancer cases were initially misdiagnosed, as vague symptoms like abdominal pain and bloating were mistaken for less serious conditions [31]. Limited access to advanced imaging further allowed the disease to go undetected until it reached an advanced stage. These gaps in detection highlight the urgent need for more reliable, early-stage diagnostic methods to improve treatment processes and patient outcomes [32].
On the other hand, false negatives results can be just as dangerous. For instance, a biopsy that samples the wrong area may falsely reassure a patient while cancer continues to spread undetected. Some tumors, like those in the pancreas or ovaries, are especially elusive, hiding deep within the body where routine screenings struggle to reach [33]. A well-known example is the case of actor Patrick Swayze, who was diagnosed with pancreatic cancer only after it had already advanced to stage IV, despite experiencing symptoms months earlier [34]. Similarly, many women with ovarian cancer, like the late journalist Julie Yip-Williams, receive diagnoses too late because early symptoms are mistaken for common digestive issues [35]. The challenge is even greater in rural clinics and underserved regions, where limited access to specialists and advanced imaging means patients may wait months for a diagnosis or miss the opportunity for early detection altogether. These gaps in care allow cancer to go unnoticed until it reaches an advanced, often untreatable stage [36].
Cancer treatment presents another major challenge, as current diagnostic and therapeutic tools often fall short. While treatment strategies have become more advanced, they still face significant hurdles such as drug resistance, severe side effects, and limited effectiveness across different cancer types. For decades, the standard approach has relied on three primary methods: surgery, radiation, and chemotherapy [37,38]. Surgery can be highly effective if cancer is caught early and remains localized. for instance, removing a small breast tumor before it spreads to the lymph nodes. However, once cancer metastasizes, surgery alone is rarely enough. On the other hand, radiation therapy uses high-energy beams to shrink tumors or slow their uncontrolled growth, but it also damages healthy tissue, leaving patients fatigued or permanently scarred [39,40]. The other treatment option, chemotherapy, the most aggressive approach, floods the body with drugs that kill rapidly dividing cells; both cancerous and healthy. While it has saved countless lives, its side effects are often brutal, causing hair loss, nausea, immune suppression, and, in some cases, only minimal benefit. For instance, in advanced lung cancer, chemotherapy might extend life by a few months, but only about 25% of patients respond well, while the rest endure the toxic side effects with little improvement from their disease situations [41,42]. The numbers starkly reveal the limitations of current cancer diagnosis and treatment.
These conventional treatments follow “a one-size-fits-all” approach, attacking cancer broadly without considering its unique genetic and molecular characteristics. This day, emerging therapies like immunotherapy and precision medicine offer more targeted options by harnessing the immune system or tailoring treatments to specific genetic mutations. However, these innovations remain expensive, inaccessible in many regions, and inconsistent in their success rates, leaving many patients without viable options [43,44]. Consider a farmer in rural Ethiopia, who experiences persistent stomach pain for months before finally seeing a doctor only to be diagnosed with gastric cancer that has already spread to his liver. With no access to routine screenings, his cancer goes undetected until it is too late. Even in wealthier countries with better healthcare infrastructure, survival rates for certain cancers remain dismally low. Pancreatic cancer, for instance, is rarely detected before reaching stage IV, leading to a five-year survival rate of just 10% [45].
These disparities are not just medical; they are deeply personal. Families around the world watch loved ones succumb to cancer not because the disease is invincible, but because our current detection and treatment methods fail too often. The reality is frustrating: we are battling a highly adaptable enemy with tools that are often outdated and imprecise to hit the target in the field of oncology diagnosis and treatment. The urgent need for sharper, more personalized approaches is clear, and the next wave of innovation may finally provide the breakthrough we have been waiting for [46].
3. Biomarkers: The New Frontier in Cancer Detection
Cancer remains a major global health challenge, highlighting the urgent need for continuous advancements in diagnostic and treatment strategies. Despite significant progress in cancer care, many treatment options are still limited by the inability to detect cancer in its early stages, when it is most treatable. Therefore, improving early detection methods, refining treatment precision, and expanding access to innovative therapies are critical steps toward reducing cancer-related mortality and improving patient outcomes worldwide. As cancer becomes an increasingly complex disease, it is essential to explore novel approaches that offer hope for earlier diagnosis and more effective treatment options [26,47].
One of the most promising developments in cancer research is the rapid evolution of biomarker technology, which is transforming how we detect and diagnose cancer. Biomarkers are biological molecules found in blood, urine, or tissue samples that are providing a way to identify the presence of cancer long before symptoms appear, enabling earlier intervention that can significantly improve patient outcomes. Unlike conventional detection approaches and technologies, such as imaging and biopsies, which often identify cancer at later stages when treatment options are more limited, biomarkers can detect malignancies at their initiations [19,29,48]. This approach not only allows for more timely treatment but also offers a non-invasive or minimally invasive means of monitoring the disease. As advancements in biomarker research continue, they hold the potential to revolutionize cancer care by providing a more personalized and efficient way to detect and manage the disease at its earliest and most treatable stages [49,50].
Cancer’s ability to hide has kept us on the defensive for far too long, however, biomarkers are transforming the game, shifting the focus from reactive treatment to proactive detection. So, what exactly are biomarkers? They are measurable indicators of biological state or conditions. These include molecules such as enzyme levels, protein expressions, fragments of DNA, and other cellular signals that cancer leaves behind as it grows (see Figure 1). Think of biomarkers as a tumor’s unique fingerprints, circulating in blood, urine, or tissue, waiting to reveal their secrets if we know where and how to look [18,51].
Unlike traditional approachess that wait for symptoms, such as a lump or persistent cough, biomarkers enable us to detect cancer at its earliest stages, often before it grows large enough to cause significant problems. They not only indicate that something is wrong but also provide detailed insights, helping to identify the type of cancer, its location, and even its potential aggressiveness. This shift represents more than just refining existing diagnostic methods; it involves creating an entirely new diagnostic toolbox. This toolbox is precise and sharp enough to catch cancer when it is still manageable, rather than when it has become a formidable, advanced disease. By detecting cancer at this early stage, biomarkers could fundamentally change our approach to treatment, transitioning from a desperate fight against an already aggressive disease to a proactive strategy that addresses cancer before it gains a foothold [52,53].
Cancer biomarkers can be classified into four main types (see Table 2), each playing a crucial role in the detection, management, and treatment of the disease [50]. Among these, diagnostic biomarkers are vital for detecting cancer at an early stage, often before symptoms even appear. For instance, PSA (prostate-specific antigen) for prostate cancer and CA-125 for ovarian cancer can signal the presence of cancer, enabling earlier intervention. As a result, early detection improves treatment options, often before the disease spreads, significantly increasing the chances of successful outcomes [28,54].
Another significant category of biomarkers is prognostic biomarkers, which provide valuable insights into the aggressiveness of a cancer and can help predict its likely progression. By offering these insights, prognostic biomarkers allow doctors to assess the severity of the disease and make informed decisions regarding treatment plans. For instance, the presence of specific biomarkers can indicate whether the cancer is likely to spread quickly, enabling doctors to tailor more aggressive treatments when necessary [55,56].
The third type of biomarker is predictive biomarkers, which are crucial for determining how well a patient might respond to specific therapies. An example of this is HER2 in breast cancer, which helps guide the use of targeted treatments like trastuzumab (Herceptin). By specifically targeting cells that overexpress the HER2 protein, these predictive biomarkers increase the likelihood of treatment success [56,57].
Finally, monitoring biomarkers are essential for tracking the effectiveness of treatment over time and detecting any potential recurrence of cancer. By utilizing these biomarkers, healthcare providers can adjust therapies as needed, ensuring that patients receive the most effective treatment throughout their care. By understanding and applying all four types of biomarkers, healthcare providers can significantly improve early diagnosis, make more precise treatment selections, and ultimately enhance patient outcomes [58,59].
The study of cancer biomarkers is full of exciting possibilities, and one key area is plasma proteomics. Think of it as a high-tech filter that analyzes thousands of proteins in our blood to find those that signal the presence of cancer. This method is becoming very good at accurately identifying cancer markers (see Table 3). At the same time, circulating tumor DNA (ctDNA) is important because it reveals genetic material that tumors release into the bloodstream, like breadcrumbs. This DNA can show the mutations that help cancer grow. By examining these genetic fragments, doctors gain valuable insights into how the tumor behaves, helping them understand the disease better [8,60].
In addition to plasma proteomics and circulating tumor DNA, other biomarkers like RNA and exosomes (tiny vesicles released by cells) further enhance our understanding of what's happening inside the body. These biomarkers add more depth to our insights into cancer. Moreover, the tools used to analyze them are becoming increasingly sophisticated. Thanks to machine learning, algorithms are now able to identify patterns and trends in these biomarkers that might otherwise go unnoticed, providing doctors with even more valuable information to guide treatment decisions [61,62].
The benefits are significant: biomarkers enable faster, less invasive, and much more precise detection of cancer compared to the traditional biopsies and scans we have relied on for so long. It’s like upgrading from a dim flashlight to a powerful spotlight, illuminating cancer’s hidden corners before it has a chance to take hold. Furthermore, biomarkers not only help identify cancer but also provide doctors with a detailed roadmap for treatment. By pinpointing specific cancer mutations and characteristics, biomarkers guide clinicians toward targeted therapies, greatly enhancing the chances of success while minimizing unnecessary treatments. This represents a new era in cancer detection and treatment, and it continues to improve [51,63].
The evidence is mounting, and the examples are truly impressive. For instance, in the case of lung cancer; where timely intervention is especially critical for smokers, tests like early CDT-Lung utilize a panel of protein biomarkers to detect the disease early. Studies have demonstrated that this test can identify suspicious cases up to a year before a traditional CT scan would. This early detection provides patients with a vital head start on treatment, potentially enhancing their chances of a positive outcome [64,65].
For colorectal cancer, the blood test Septin9 identifies circulating tumor DNA (ctDNA) and provides an early detection tool with over 80% accuracy. This test serves as a less invasive alternative to the dreaded colonoscopy, sparing patients from the discomfort and extensive preparation typically associated with the procedure while still allowing for the detection of cancer at its earliest stages. In prostate cancer, the long-established PSA test has faced criticism due to its unreliability and high false-positive rates. However, newer biomarker panels like the 4Kscore improve accuracy by combining multiple proteins, helping doctors identify genuine threats and minimize unnecessary procedures, ultimately reducing patient anxiety [66,67,68].
In breast cancer, the Oncotype DX test analyzes tumor RNA to evaluate the risk of recurrence. This enables doctors to make more informed treatment decisions, determining whether chemotherapy is necessary or if a less aggressive approach could be effective. These advancements are not isolated examples; they represent a broader trend in personalized medicine, where biomarker testing plays a crucial role in tailoring treatments to individual patient needs [69]. They provide a glimpse into a future where a simple blood draw or urine sample could detect cancers like pancreatic cancer before it becomes a death sentence, or identify ovarian cancer before it is misdiagnosed as a minor stomach issue. These breakthroughs are transforming what once seemed like a distant dream of early cancer detection into a tangible reality, one that could save countless lives by making early diagnosis the norm rather than the exception [70,71].
This new frontier is so exciting because it is not just about detecting cancer earlier; it is also about doing so with greater accuracy. Biomarkers eliminate much of the uncertainty that has long been a challenge, replacing outdated and unclear methods with sharp, precise tools. While biomarkers are not yet flawless, some tests can be costly, and others still need refinement to catch every case, the progress is undeniable. Researchers are diligently working to discover more markers, ranging from rare genetic changes to subtle protein shifts, and they are combining these findings with advanced technologies like artificial intelligence to help identify patterns that might otherwise go unnoticed [72]. The ultimate vision is a future where cancer screening is as simple and routine as an annual check-up, catching the disease early enough that it doesn’t stand a chance. After years of grappling with methods that often-missed critical cases, biomarkers are paving the way for earlier and more reliable detection. With ongoing advancements, we are getting closer to a world where early cancer detection becomes the norm rather than the exception [73].
4. Personalized Molecular Therapies: Targeting Cancer’s Weak Spots
Cancer is a complex and heterogeneous disease marked by uncontrolled cell growth driven by genetic mutations, epigenetic alterations, and dysregulated signaling pathways. Traditional treatments like chemotherapy and radiation often target rapidly dividing cells indiscriminately, resulting in significant side effects and limited effectiveness for some patients. However, recent advancements in genomics, transcriptomics, proteomics, metabolomics, and computational biology have opened the door to personalized molecular therapies. These therapies aim to target specific vulnerabilities within individual tumors by identifying and exploiting their unique genetic and molecular characteristics, ultimately enhancing treatment efficacy [11,74].
For a long time, cancer treatment has been a blunt instrument, but we are entering a new era with personalized molecular-targeted therapies that directly address the disease's underlying mechanisms. At the core of personalized molecular therapy is genomic profiling, which involves analyzing the DNA, RNA, and proteins of a patient’s tumor to identify actionable mutations or biomarkers. Advanced techniques such as next-generation sequencing (NGS), whole-exome sequencing (WES), and transcriptomics facilitate a comprehensive molecular characterization of tumors. Each patient's cancer harbors unique genetic mutations that drive tumor growth and contribute to treatment resistance. By leveraging NGS and other molecular profiling techniques, oncologists can pinpoint key genetic alterations that render a cancer susceptible to targeted therapies [10,75].
Cancer's "weak spots" refer to specific genetic, molecular, or biological vulnerabilities that treatments can exploit to disrupt tumor growth and survival. These vulnerabilities often stem from oncogenic driver mutations, such as EGFR in lung cancer or BRAF V600E in melanoma. These mutations play crucial roles in cancer progression and can be effectively inhibited by targeted therapies, such as osimertinib for EGFR mutations and vemurafenib for BRAF V600E mutations [76]. Dysregulated signaling pathways, such as the PI3K/AKT/mTOR pathway, present another critical avenue for intervention. Drugs like everolimus target these pathways to halt cell proliferation. Additionally, tumors rely on their microenvironment for essential resources and to evade the immune system. This reliance makes targets like VEGF, which is involved in anti-angiogenesis, and immune checkpoint inhibitors, such as pembrolizumab, effective strategies for treatment [77]. Synthetic lethality provides another layer of targeted therapy, as drugs like PARP inhibitors exploit deficiencies in DNA repair mechanisms found in cancers with BRCA mutations. Additionally, epigenetic alterations that modify gene expression without altering the DNA sequence offer opportunities for therapies aimed at reversing these changes. By identifying and leveraging these diverse weak spots, personalized molecular therapies can deliver precise and effective treatments tailored to each patient's unique tumor biology [78,79].
Unlike traditional treatments that broadly target cancer with surgery, radiation, or chemotherapy, personalized therapies focus on the specific molecular quirks that drive tumor growth such as mutated genes, overactive proteins, or disrupted signaling pathways. The concept is both simple and revolutionary: every cancer has a unique weak spot, a flaw in its machinery that sustains its growth. By precisely targeting these vulnerabilities, it is possible to halt the disease without damaging surrounding healthy tissue. This approach is not a "one-size-fits-all" solution; instead, it is a customized strategy tailored to the unique profile of each patient's tumor. While traditional treatments often swing a wrecking ball, these therapies act with the precision of a scalpel, effectively dismantling cancer's defenses and rewriting survival stories [76,80].
Personalized molecular therapies represent a transformative approach to cancer treatment by targeting specific vulnerabilities unique to each patient’s tumor (see Figure 2). A cornerstone of these therapies is the use of targeted therapies, which block molecular pathways essential for cancer cell survival. For example, tyrosine kinase inhibitors (TKIs) like imatinib target the BCR-ABL fusion protein in chronic myeloid leukemia, while trastuzumab inhibits HER2 in HER2-positive breast cancer, and vemurafenib blocks the BRAF mutation in melanoma [11,81].
Another key strategy involves immunotherapies, which leverage the immune system to combat cancer based on the tumor's molecular profile. Immune checkpoint inhibitors, such as pembrolizumab, have proven effective in tumors with high PD-L1 expression or mismatch repair deficiency. Additionally, CAR-T cell therapy involves engineering a patient’s T cells to specifically recognize and attack cancer antigens, enhancing the body’s ability to target and destroy malignant cells [82]. Additionally, RNA-based therapies are emerging as a powerful tool, utilizing RNA interference (RNAi) or mRNA technologies to target cancer-driving genes. Small interfering RNAs (siRNAs) can silence oncogenic genes, while mRNA vaccines similar to those developed for COVID-19 are being explored to stimulate anti-cancer immune responses. Together, these approaches highlight the versatility and precision of personalized molecular therapies in combating cancer through tailored, mechanism-specific treatments [83,84].
Imagine a tumor as a factory operating out of control, relentlessly producing cells because a critical switch, such as a protein like EGFR or HER2, has become stuck in the "on" position. Molecular therapies target these faulty switches, either flipping them off or blocking them entirely, effectively cutting off the resources that cancer needs to grow. By disrupting these essential signals, these therapies can halt the relentless production of cancer cells and restore balance to the body [85]. For instance, drugs like tyrosine kinase inhibitors interfere with the signals that tell cancer cells to multiply, while monoclonal antibodies bind to specific markers on the surface of tumor cells, flagging them for destruction by the immune system. The power of these therapies lies in their precision: unlike chemotherapy, which indiscriminately attacks both healthy and cancerous cells, molecular therapies zero in on rogue signals that are unique to cancer cells. This specificity spares healthy tissues, dramatically reducing the harsh side effects associated with traditional treatments. When combined with biomarker testing, this approach becomes even more effective. Biomarkers act as a roadmap, identifying the specific mutations or proteins fueling a patient’s cancer, allowing doctors to select the therapy most likely to hit the tumor’s weak spot with pinpoint accuracy. It is a shift from the “carpet-bombing” approach of conventional chemotherapy to the “sniper fire” of personalized medicine and the results are proving that this targeted strategy is not just a scientific breakthrough but a life-changing reality for many patients [86,87].
The success stories of personalized molecular therapies are truly remarkable, providing hope where there was once little. Take chronic myeloid leukemia (CML), for example, a disease that was once considered a death sentence. Today, it has been transformed into a manageable condition thanks to imatinib. This drug specifically targets the BCR-ABL protein that drives the cancer, enabling over 80% of patients to live for decades after diagnosis. This shift illustrates the power of targeted therapies in improving survival and quality of life for cancer patients [88]. In breast cancer, approximately 20% of cases involve the overproduction of the HER2 protein. This is where trastuzumab (Herceptin) comes into play; it binds to HER2 and slows tumor growth, significantly enhancing survival rates. Studies have shown that adding trastuzumab to standard care reduces the risk of recurrence by half, effectively transforming aggressive tumors into treatable conditions. This advancement highlights the critical role of targeted therapies in improving outcomes for patients with HER2-positive breast cancer [89].
For lung cancer patients with EGFR mutations a common feature in non-smokers, osimertinib offers a lifeline by specifically targeting the mutation and doubling progression-free survival compared to traditional chemotherapy, with some patients remaining stable for nearly two years without their cancer worsening. Similarly, in melanoma, the BRAF mutation drives tumor growth in about half of cases, and vemurafenib effectively targets this mutation, rapidly shrinking tumors where chemotherapy often fails and transforming bleak prognoses into months or even years of extended life. These breakthroughs are not just laboratory victories; they represent real-world miracles, providing patients with the chance to walk away from what were once considered fatal diagnoses [90,91].
This is where cancer treatment evolves from a blunt, one-size-fits-all approach to something sharper, smarter, and more humane (see Table 4). Personalized therapies aim not just to destroy cancer but to outsmart it, using the tumor’s own biology as its critical vulnerability. While these treatments face challenges such as some cancers developing resistance over time and the staggering costs that can reach tens of thousands of dollars annually, the momentum behind this revolution is undeniable. These innovative approaches continue to reshape the landscape of cancer treatment, offering hope and improved outcomes for many patients [92].
Researchers are discovering new targets for treatment, like KRAS in pancreatic cancer and ALK in lung cancer, and are improving combination therapies to stay ahead of resistance. The real strength of personalized medicine comes when these treatments are guided by biomarkers: simple blood tests can identify the tumor’s weak spot, allowing the drug to make a precise attack. This gives us a glimpse of a future where cancer is not just a devastating diagnosis but a complex puzzle that we can solve step by step. This future offers patients not only more time but also a better quality of life. After years of using broad strategies, we are finally learning to focus our efforts and make the most effective impact where it matters [93].
While traditional methods of cancer diagnosis and treatment remain essential, cutting-edge technologies are transforming the field by enabling earlier detection, greater precision, and more effective treatment interventions. These advancements empower healthcare providers to catch cancers at their most treatable stages, significantly improving the likelihood of successful outcomes [94]. Currently, personalized medicine is becoming more precise by incorporating tools like genomic sequencing, molecular diagnostics, and AI-driven technologies into cancer care, tailoring therapies to each patient’s unique genetic profile and tumor biology. This targeted approach effectively addresses the underlying causes of cancer while minimizing damage to healthy cells, reducing side effects and enhancing patients’ quality of life. As these innovations evolve, they hold the potential to further improve cancer care, with AI and machine learning providing clinicians with real-time insights to guide smarter, data-driven decisions. The result is a new era of individualized cancer treatment, offering hope for better outcomes, improved survival rates, and a brighter future for those facing this challenging disease [95,96].
5. Bridging Cancer Diagnosis and Treatment: The Power of Integration for Better Health Care
The integration of cancer diagnosis and treatment marks a crucial shift in modern oncology, aiming to improve patient outcomes through a multifaceted approach. This seamless connection ensures that patients have a smoother journey from detection to recovery. Traditionally, delays between diagnosis and the start of treatment have been problematic, often due to logistical challenges, fragmented healthcare systems, and poor communication among specialists. However, cancer care is evolving. It is no longer just about identifying the disease and then choosing a treatment; instead, diagnosis and treatment now work together from the very beginning. By combining biomarkers with personalized molecular-targeted therapies, we create a powerful alliance that is changing the landscape of oncology and offering new hope for patients [97,98].
Early and accurate diagnosis is essential for effective cancer treatment, and advancements in diagnostic technologies are transforming how cancers are detected and characterized. For example, genomic profiling helps clinicians identify specific mutations driving a patient’s tumor, while liquid biopsies allow for real-time monitoring of disease progression and treatment response through circulating tumor DNA. These innovations not only enable earlier detection but also provide valuable insights into the changing biology of a tumor, ensuring that treatment strategies can adapt and remain precise. When these diagnostic tools are effectively integrated with treatment options, they unlock the full potential of personalized medicine [99,100]. For instance, identifying actionable biomarkers through genomic testing can guide the selection of targeted therapies, such as tyrosine kinase inhibitors or immune checkpoint blockers, tailored to the genetic makeup of an individual’s cancer. Similarly, AI and machine learning algorithms can analyze vast datasets to predict treatment responses, optimize drug combinations, and anticipate resistance mechanisms, empowering clinicians to make informed decisions at every stage of care [101].
Biomarkers serve as detectives, accurately locating cancer through blood tests or tissue samples. At the same time, targeted therapies act like sharpshooters, hitting the tumor's weak spots while protecting healthy cells from harm. When these two innovations work together, they create a powerful system where identifying the cancer leads directly to the most effective treatment plan. This tailored approach eliminates guesswork and focuses on the best solution. This integration represents not just a small improvement over traditional methods but a significant leap into a future where every aspect of cancer care, from detection to treatment, is carefully designed based on each patient's unique disease biology. It is a bold move toward truly personalized medicine, offering hope for more efficient, effective, and compassionate care [5,93].
The true power of personalized cancer care comes from how biomarkers not only indicate the presence of cancer but also uncover its strategies. They reveal the specific mutations and pathways that are driving the disease [102]. For example, a simple blood test might reveal an ALK gene rearrangement in a lung cancer patient. Instead of using a trial-and-error approach with chemotherapy, doctors can prescribe crizotinib, a drug that specifically targets this mutation. The outcome? Tumors can shrink in weeks instead of months, reducing unnecessary suffering for patients [103]. Similarly, in colorectal cancer, if a biopsy reveals no KRAS mutations, it signals a green light for cetuximab, a therapy that targets EGFR, tripling response rates compared to standard treatments. Without this biomarker insight, the same therapy would be a shot in the dark, ineffective against cancers with KRAS mutations. This synergy between biomarkers and therapies cuts through the overwhelming diversity of cancer over 200 types, each with its own subtypes and transforms it into a manageable challenge. It is like having a GPS for a maze: the biomarker points the way, and the therapy charts the route, dodging dead ends that waste time and hope [104,105].
The evidence supporting this approach is growing and extends beyond laboratory experiments; it's saving lives. In breast cancer, the MammaPrint test analyzes a 70-gene signature to predict the risk of recurrence. If the risk is low, patients can skip the harsh side effects of chemotherapy altogether. If the risk is high, doctors can customize treatment, such as combining trastuzumab with standard care for HER2-positive cases, which reduces the chances of relapse by 50% [106]. A groundbreaking trial in cervical cancer in 2022 took this a step further. By using tumor protein markers to guide a brief course of chemotherapy before standard treatment, researchers were able to reduce the risk of mortality by 40%. This life-saving achievement came from effectively matching the right drug to the right indicators [107]. Melanoma provides another clear example: PD-L1 biomarkers help identify patients who are likely to respond to pembrolizumab, an immunotherapy that boosts the immune system. For some patients, this means enjoying years of remission, while chemotherapy might have only offered months. Even rare cancers like gastrointestinal stromal tumors (GIST) benefit from this strategy. When biomarkers detect KIT mutations, imatinib can be used, increasing the survival rate from a dismal 10% to over 80%. These effective pairings aren’t just coincidences; they demonstrate that connecting diagnosis to treatment is not only smart but also transformative [108,109].
The integration of biomarkers and targeted therapies is not a fixed process; it is a dynamic and evolving approach that adjusts as cancer changes. Researchers are increasingly using combination treatments, such as pairing targeted drugs with immunotherapy or radiation. This is guided by multi-marker panels that provide a comprehensive view of a tumor’s biology, including its DNA, proteins, and microenvironment. For example, in lung cancer, patients with EGFR mutations might begin treatment with osimertinib. If resistance develops, a circulating tumor DNA (ctDNA) test can identify new mutations like T790M, allowing for a switch to a next-generation drug that is tailored to the tumor’s evolving characteristics [5,110]. This adaptive process transforms cancer care into a responsive and personalized strategy. It reduces reliance on toxic treatments, leading to shorter hospital stays, less strain on patients, and greater potential for use in resource-limited settings. However, challenges such as high costs, limited access to advanced diagnostics, and gaps in training for healthcare providers mean this approach is not yet widely available. Despite these obstacles, the vision remains clear: a future where a cancer diagnosis not only identifies the disease but also provides the tools to fight it with precision, offering unprecedented control over what was once an overwhelming adversary [92,111].
The integration of cancer diagnosis and treatment has the potential to revolutionize patient outcomes by fostering multidisciplinary collaboration, leveraging advanced technologies, and streamlining healthcare processes to connect detection and therapy. When diagnosis and treatment are aligned, healthcare systems can reduce redundancies, optimize workflows, and allocate resources more efficiently, ultimately lowering costs and improving accessibility. For patients, this approach creates a cohesive and supportive care journey, addressing their unique needs holistically from early detection and risk assessment to personalized therapies and survivorship planning. This unified strategy not only enhances survival rates but also improves the overall patient experience, paving the way for a future where cancer care is precise, personalized, and profoundly effective [112,113].
Looking ahead, the ongoing improvement of integrated cancer care holds great promise. New technologies like single-cell sequencing, CRISPR-based diagnostics, and nanotechnology for drug delivery are making it easier to combine diagnosis and treatment into a smooth process. This teamwork not only boosts our ability to fight cancer but also changes the way we think about compassionate, patient-centered healthcare. Connecting diagnosis and treatment is more than just a scientific breakthrough; it represents a major shift toward better health outcomes and a higher quality of life for patients. By encouraging collaboration across different fields and using the latest technologies, we are creating a future where cancer care is proactive, predictive, and truly personalized [114,115].
6. In Cancer: Real-World Wins and Challenges Ahead
The fight against cancer has made significant strides, largely due to the emergence of personalized medicine and targeted therapies. For many years, cancer research felt like a relentless race against time, but now the finish line appears nearer than ever. Real-world successes achieved through biomarkers and tailored treatments are transforming lives, turning once grim diagnoses into narratives of resilience and hope. These breakthroughs illustrate that combining advanced detection methods with customized treatment plans can effectively counteract cancer’s elusive strategies [92]. Patients are experiencing fewer side effects from chemotherapy or even avoiding it altogether, while others are surpassing survival expectations once thought unattainable. Each success is backed by hard data and human stories, proving just how far science has come. Yet, for every step forward, challenges remain: high costs, limited access, and unforeseen setbacks remind us that this revolution is far from complete. This section explores what is working, who is benefiting, and the obstacles still standing in the way, offering a clear-eyed view of both progress and the road ahead [116,117].
The successes in cancer diagnosis and treatment are undeniable. Take melanoma, once viewed as a relentless killer; it is now responding to therapies like pembrolizumab. Patients with PD-L1 biomarkers have experienced significant tumor shrinkage, with some achieving five-year survival milestones that seemed unimaginable just a decade ago, when chemotherapy provided only a few extra months of life [118]. In lung cancer, drugs like osimertinib are doubling progression-free survival for patients with EGFR mutations, extending stable health to nearly two years compared to less than one with older treatments [119]. Breast cancer patients with low-risk MammaPrint scores are now able to forgo chemotherapy altogether, thriving instead on lighter therapies. Meanwhile, HER2-positive cases are benefiting from trastuzumab, which has halved recurrence rates. Even rare cancers, like gastrointestinal stromal tumors (GIST), are experiencing remarkable outcomes: imatinib effectively targets KIT mutations, boosting survival rates to 80%, a staggering increase from just 10% in the past. These successes are not isolated; global statistics support this encouraging trend [120,121].
According to the American Cancer Society, targeted therapies have significantly increased five-year survival rates for various cancer types by 10-20% since 2010. These statistics represent profound advancements in cancer treatment that are changing lives. Behind these numbers are real individuals, such as a 60-year-old teacher in Texas. After being diagnosed with lung cancer, she underwent an ALK test that identified her as a suitable candidate for crizotinib. The results were remarkable; her cancer responded dramatically to the treatment, allowing her to regain her health and continue her teaching career. Stories like hers underscore that this progress is not merely about data; it represents real deliverance for patients and their families, offering hope and renewed possibilities in the face of a daunting diagnosis. Each success story reflects the transformative power of personalized medicine and the impact it has on the lives of those it touches [122,123].
This progress reflects not only scientific creativity but also the profound impact of precision medicine. By understanding the unique genetic and molecular profiles of individual cancers, researchers and clinicians are developing treatments that work smarter, not harder. However, as transformative as these advancements are, they also reveal significant disparities in access and affordability, raising concerns about whether the benefits will reach everyone equally. While the strides made thus far inspire optimism and hope, it is crucial to address these barriers to ensure that the fight against cancer becomes a victory for all. Ensuring equitable access to these innovative therapies will be essential in making sure that no one is left behind in this battle, allowing every patient the opportunity for a better outcome and a chance at life [124].
Despite the remarkable progress in cancer diagnosis and treatment, not everyone benefits equally, and this is where the challenges become most evident. Resistance to targeted therapies continues to pose a significant obstacle, as cancers can evolve and develop new mutations that enable them to evade even the most advanced treatments. Additionally, financial barriers exacerbate the issue: these life-saving therapies often come with astronomical costs. For instance, osimertinib can exceed $15,000 per month, and insurance coverage is far from guaranteed. This leaves patients in wealthier nations grappling with affordability, while those in low-income regions face even greater challenges in accessing necessary care. Addressing these inequities is crucial to ensure that the advancements in cancer treatment benefit everyone, regardless of their financial situation [125]. Access is an even greater challenge; 70% of cancer deaths occur in places like sub-Saharan Africa and rural Asia, where access to biomarker testing and targeted drugs is severely limited. Imagine a farmer in Kenya waiting months or even a year for a basic diagnostic scan, let alone cutting-edge tools like ctDNA panels. The COVID-19 pandemic further exacerbated these disparities, disrupting screening programs and creating significant backlogs. According to the World Health Organization (WHO), early detection rates dropped by 30% in 2020 alone, giving cancer a dangerous head start [126,127].
Resistance to treatments adds another layer of complexity in the fight against cancer. Tumors can adapt rapidly, rendering drugs like vemurafenib ineffective within just a few months, which forces researchers to race against time to develop next-generation solutions [128]. For instance, resistance to EGFR inhibitors in lung cancer often occurs due to secondary mutations such as T790M, highlighting the need for newer, more sophisticated drugs. However, tackling resistance requires more than just innovation; it necessitates systemic changes across the healthcare landscape. Doctors need specialized training, laboratories must be equipped with advanced technology, and healthcare systems need adequate funding to bridge gaps in care delivery. Even when there is a strong desire to implement these changes, resource constraints can significantly slow the rollout of breakthroughs. High costs and unequal access to cutting-edge therapies perpetuate stark disparities in care, especially in low-resource settings. Moreover, the complexity of diagnosing and treating cancer continues to increase, underscoring the urgent need for ongoing innovation. Tools like liquid biopsies and AI-driven analytics hold immense promise for staying ahead of the disease, but they require substantial investments in research, infrastructure, and training. Ensuring that these advancements reach all patients will be crucial in the collective fight against cancer [129,130].
Looking ahead, the key to progress lies in addressing these challenges while building on the successes already achieved. These obstacles are not impossible to overcome; they represent the next frontier in the fight against cancer. The victories we have seen thus far demonstrate what is possible: lives extended, suffering reduced, and hope restored. Bridging the gaps requires scaling up effective strategies, such as developing more affordable diagnostic tests, expanding access to therapies, and combining treatments in innovative ways to improve outcomes for patients worldwide. While the journey is complex and uneven, every patient thriving today stands as a beacon of hope for the future. For instance, combining therapies such as pairing targeted drugs with immunotherapy or radiation offers promising opportunities to outsmart resistant tumors. Biomarkers and targeted therapies are fundamentally rewriting cancer’s narrative, transforming it from one of despair into one of possibility. Now, the mission is clear: we must ensure that this transformative progress reaches every corner of the globe, leaving no patient behind. This commitment to equity in cancer care will be essential in turning hope into reality for all those affected by this disease [93,131].
7. The Road Forward: Scaling the Revolution Against Cancer
The road forward in the fight against cancer is defined by innovation, collaboration, and a strong determination to transform how we approach this disease on a global scale. The next chapter in cancer care is not just about refining existing tools; it is about reimagining how we prevent, detect, and treat cancer to create a future where its burden is significantly reduced. At the heart of this transformation are emerging technologies like artificial intelligence (AI) and liquid biopsies, which together have the potential to shift the focus from reactive treatment to proactive prevention. By harnessing these advancements, we can pave the way for earlier diagnoses and more effective interventions, ultimately improving outcomes for patients everywhere [132,133].
AI is already proving its value in analyzing vast datasets of biomarker profiles, providing insights that can predict patient outcomes with impressive accuracy. For instance, algorithms are being developed to sift through genetic and proteomic data to forecast how lung cancer patients might respond to immunotherapy. This breakthrough has been demonstrated in recent studies at institutions like Stanford, showcasing the potential of AI to enhance personalized treatment strategies and improve patient care. By leveraging these technologies, we can better tailor therapies to individual needs, ultimately leading to more effective interventions and better outcomes for patients [133]. Meanwhile, liquid biopsies are revolutionizing early detection by offering a minimally invasive way to monitor the evolution of cancer. These tests analyze circulating tumor DNA from a simple blood draw, allowing for the identification of early-stage cancers or recurrences long before traditional imaging methods can. Companies like Guardant Health are at the forefront of this innovation, demonstrating the potential of this technology to detect aggressive cancers, such as pancreatic cancer, before they have a chance to spread. By enabling earlier intervention, liquid biopsies can significantly improve treatment outcomes and patient survival rates [134,135].
However, the true revolution lies in scaling these innovations so they extend far beyond elite research centers and into communities worldwide. Prevention will play a pivotal role in this vision. Imagine AI-driven risk models that identify individuals with inherited mutations, such as BRCA1, for closer monitoring, or population-wide screening programs using liquid biopsies to detect aggressive cancers before they metastasize. Democratizing access to these tools is equally critical. Initiatives like the World Health Organization’s push for affordable diagnostics in low-income countries, along with partnerships between biotech firms and governments to subsidize AI-powered pathology tools, exemplify efforts to make cutting-edge technologies accessible to all. For instance, PathAI’s work in streamlining tumor analysis could soon be adapted for rural clinics, reducing costs and accelerating diagnoses in areas where specialists are scarce. By ensuring that everyone has access to these advancements, we can make significant strides in cancer prevention and treatment on a global scale [136,137].
This forward-looking vision has the potential to dramatically reduce cancer's toll. By catching diseases earlier, tailoring treatments more precisely, and ensuring that no patient is left behind due to geography or income, these advancements could significantly lower the global mortality rate, which currently stands at 10 million annually, according to the International Agency for Research on Cancer. Moreover, easing the economic strain on healthcare systems would create ripple effects, enhancing the quality of life for millions. By prioritizing equitable access to innovative technologies and treatments, we can create a healthier future for everyone, regardless of their circumstances [26].
Generally, "The Road Forward" in the fight against cancer is not just a hopeful slogan; it’s a call to action. It urges scientists, policymakers, and innovators to connect today’s breakthroughs with tomorrow’s reality, transforming cancer into a manageable chapter in human health rather than a defining one. Through collaboration and commitment, we can turn the promise of these innovations into tangible progress, ensuring that the fight against cancer becomes a victory for everyone, everywhere. By working together, we can create a future where effective prevention, early detection, and personalized treatment are accessible to all, ultimately improving lives across the globe [138].
8. Conclusion: A New Era in Cancer Care
Cancer care is undergoing a revolutionary transformation, driven by the integration of biomarker-based diagnosis and personalized molecular targeted treatments. Traditional approaches like chemotherapy and radiation, while effective in many cases, often come at a high cost to patients due to their non-specific nature, impacting both malignant and healthy cells alike. However, advancements in genomics and molecular diagnostics have ushered in the era of precision medicine, enabling oncologists to provide therapies that are not only more effective but also significantly less toxic. This shift marks a pivotal moment in cancer treatment, offering hope for better outcomes and improved quality of life for patients around the world [49,139].
At the heart of this revolution are biomarkers, genetic mutations, protein expressions, and circulating tumor DNA, that serve as critical tools for early detection, accurate prognosis, and tailored therapeutic strategies. The identification of actionable genetic alterations has transformed how tumors are classified and treated, allowing oncologists to predict responses to specific therapies with unprecedented precision [51]. Cutting-edge techniques such as next-generation sequencing (NGS) and liquid biopsies have further enhanced this capability, enabling non-invasive, real-time monitoring of tumor evolution and resistance mechanisms. For example, detecting HER2 amplification in breast cancer or EGFR mutations in lung cancer has already led to the development of highly successful targeted therapies, turning once-dire diagnoses into manageable conditions [140].
Personalized molecular targeted treatments take this progress a step further by leveraging the unique molecular profile of an individual’s tumor to design customized therapeutic strategies. Unlike conventional treatments, these therapies focus on specific molecular pathways that drive cancer progression, sparing healthy tissues and minimizing side effects. Small molecule inhibitors, monoclonal antibodies, and immune checkpoint inhibitors have emerged as powerful tools in the oncologist’s arsenal. For instance, tyrosine kinase inhibitors (TKIs) have revolutionized the treatment of chronic myeloid leukemia by targeting aberrant signaling pathways, while immune checkpoint inhibitors have redefined cancer immunotherapy by empowering the body’s immune system to recognize and attack tumor cells. This targeted approach not only enhances the effectiveness of treatments but also significantly improves the quality of life for patients, as it reduces the harmful side effects commonly associated with traditional therapies. As research continues to uncover more about the molecular underpinnings of cancer, the potential for personalized medicine to transform cancer care grows ever more promising [11,92].
Looking ahead, the future of cancer care lies in the continued integration of artificial intelligence (AI) and multi-omics data to refine biomarker discovery and optimize therapeutic strategies. AI-driven predictive models can analyze vast genomic datasets, accelerating drug development and enabling even more precise treatment personalization [141]. Moreover, the convergence of biomarker-based diagnosis with innovative gene-editing technologies like CRISPR holds immense potential to unlock new frontiers in targeted cancer therapy. These advances promise to deepen our understanding of cancer biology and further enhance the precision and efficacy of treatments, paving the way for a new era in oncology where therapies are tailored to the unique genetic makeup of each patient’s cancer [142,143].
As research continues to unravel the complexities of cancer, the era of precision oncology is poised to redefine how we manage this disease. By offering patients more effective, individualized, and less toxic treatment options, this new paradigm not only improves survival rates but also restores hope and dignity to those facing a cancer diagnosis. The journey is far from over, but the progress achieved so far underscores the transformative power of science, innovation, and collaboration in the fight against cancer. This is not just the future of cancer care; it is the dawn of a new era, where advancements in technology and a deeper understanding of cancer biology come together to create a more hopeful and effective approach to treatment [47,144].
Author Contributions
G.M and M.B. conceptualized and wrote the manuscript. All authors contributed to the article and approved the submitted version. All authors have read and agreed to the published version of the manuscript.
Funding
No funding was received.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AI | Artificial Intelligence |
| AKT | Protein Kinase B |
| ALK | Anaplastic Lymphoma Kinase |
| BRCA | Breast Cancer Gene |
| CAR-T | Chimeric Antigen Receptor T-cell |
| CDT | Carbohydrate-Deficient Transferrin |
| CML | Chronic Myelogenous Leukemia |
| CRISPR | Clustered Regularly Interspaced Short Palindromic Repeats |
| ctDNA | Circulating Tumor DNA |
| CUP | Cancer of Unknown Primary |
| DNA | Deoxyribonucleic Acid |
| DX | Diagnosis |
| EGFR | Epidermal Growth Factor Receptor |
| GIST | Gastrointestinal Stromal Tumor |
| GPS | Global Positioning System |
| HER2 | Human Epidermal Growth Factor Receptor 2 |
| HPV | Human Papillomavirus |
| KIT | V-Kit Hardy-Zuckerman 4 Feline Sarcoma Viral Oncogene Homolog |
| KRAS | Kirsten Rat Sarcoma Viral Oncogene Homolog |
| mRNA | Messenger Ribonucleic Acid |
| mTOR | Mechanistic Target of Rapamycin |
| NGS | Next-Generation Sequencing |
| PD-L1 | Programmed Death-Ligand 1 |
| PI3K | Phosphoinositide 3-Kinase |
| PSA | Prostate-Specific Antigen |
| RNA | Ribonucleic Acid |
| RNAi | RNA interference |
| T790M | refers to a mutation in the EGFR (Epidermal Growth Factor Receptor) gene |
| TKI | Tyrosine Kinase Inhibitor |
| VEGF | Vascular Endothelial Growth Factor |
| WES | Whole Exome Sequencing |
References
- Carneiro, B.A.; El-Deiry, W.S. Targeting apoptosis in cancer therapy. Nat. Rev. Clin. Oncol. 2020, 17, 395–417. [Google Scholar]
- Carrillo-Beltrán, D.; et al. Interaction between cigarette smoke and human papillomavirus 16 E6/E7 oncoproteins to induce SOD2 expression and DNA damage in head and neck cancer. Int. J. Mol. Sci. 2023, 24, 6907. [Google Scholar] [CrossRef] [PubMed]
- Tigu, A.B.; Tomuleasa, C. Exploring Novel Frontiers in Cancer Therapy. Biomedicines 2024, 12, 1345. [Google Scholar] [CrossRef]
- Huerta, E.; Grey, N. Cancer control opportunities in low-and middle-income countries; Wiley Online Library, 2007; pp. 72–74. [Google Scholar]
- Nakamura, Y.; Kawazoe, A.; Lordick, F.; Janjigian, Y.Y.; Shitara, K. Biomarker-targeted therapies for advanced-stage gastric and gastro-oesophageal junction cancers: an emerging paradigm. Nat. Rev. Clin. Oncol. 2021, 18, 473–487. [Google Scholar] [CrossRef] [PubMed]
- Buzdin, A.; Sorokin, M.; Garazha, A.; Sekacheva, M.; Kim, E.; Zhukov, N.; Wang, Y.; Li, X.; Kar, S.; Hartmann, C.; et al. Molecular pathway activation – New type of biomarkers for tumor morphology and personalized selection of target drugs. Semin. Cancer Biol. 2018, 53, 110–124. [Google Scholar] [CrossRef] [PubMed]
- Pashayan, N.; Pharoah, P.D. The challenge of early detection in cancer. Science 2020, 368, 589–590. [Google Scholar]
- Huang, Z.; Ma, L.; Huang, C.; Li, Q.; Nice, E.C. Proteomic profiling of human plasma for cancer biomarker discovery. Proteomics 2016, 17. [Google Scholar] [CrossRef]
- Landegren, U.; Hammond, M. Cancer diagnostics based on plasma protein biomarkers: hard times but great expectations. Mol. Oncol. 2020, 15, 1715–1726. [Google Scholar] [CrossRef]
- Sicklick, J.K.; Kato, S.; Okamura, R.; Schwaederle, M.; Hahn, M.E.; Williams, C.B.; De, P.; Krie, A.; Piccioni, D.E.; Miller, V.A.; et al. Molecular profiling of cancer patients enables personalized combination therapy: the I-PREDICT study. Nat. Med. 2019, 25, 744–750. [Google Scholar] [CrossRef]
- Kim, K.B. Personalized therapy in oncology: melanoma as a paradigm for molecular-targeted treatment approaches. Clin. Exp. Metastasis 2024, 41, 465–471. [Google Scholar] [CrossRef]
- Nami, B.; Maadi, H.; Wang, Z. Mechanisms Underlying the Action and Synergism of Trastuzumab and Pertuzumab in Targeting HER2-Positive Breast Cancer. Cancers 2018, 10, 342. [Google Scholar] [CrossRef] [PubMed]
- Kunte, S.; Abraham, J.; Montero, A.J. Novel HER2–targeted therapies for HER2–positive metastatic breast cancer. Cancer 2020, 126, 4278–4288. [Google Scholar] [CrossRef]
- Ke, X.; Shen, L. Molecular targeted therapy of cancer: The progress and future prospect. Front. Lab. Med. 2017, 1, 69–75. [Google Scholar] [CrossRef]
- Nasser, A.; Hussein, A.; Chamba, C.; Yonazi, M.; Mushi, R.; Schuh, A.; Luzzatto, L. Molecular response to imatinib in patients with chronic myeloid leukemia in Tanzania. Blood Adv. 2021, 5, 1403–1411. [Google Scholar] [CrossRef]
- Wu, J.; Lin, Z. Non-Small Cell Lung Cancer Targeted Therapy: Drugs and Mechanisms of Drug Resistance. Int. J. Mol. Sci. 2022, 23, 15056. [Google Scholar] [CrossRef] [PubMed]
- Hochhaus, A.; Larson, R.A.; Guilhot, F.; Radich, J.P.; Branford, S.; Hughes, T.P.; Baccarani, M.; Deininger, M.W.; Cervantes, F.; Fujihara, S.; et al. Long-Term Outcomes of Imatinib Treatment for Chronic Myeloid Leukemia. N. Engl. J. Med. 2017, 376, 917–927. [Google Scholar] [CrossRef]
- Tenchov, R.; Sapra, A.K.; Sasso, J.; Ralhan, K.; Tummala, A.; Azoulay, N.; Zhou, Q.A. Biomarkers for Early Cancer Detection: A Landscape View of Recent Advancements, Spotlighting Pancreatic and Liver Cancers. ACS Pharmacol. Transl. Sci. 2024, 7, 586–613. [Google Scholar] [CrossRef]
- Han, X.; Wang, J.; Sun, Y. Circulating Tumor DNA as Biomarkers for Cancer Detection. Genom. Proteom. Bioinform. 2017, 15, 59–72. [Google Scholar] [CrossRef]
- Hunter, B.; Hindocha, S.; Lee, R.W. The Role of Artificial Intelligence in Early Cancer Diagnosis. Cancers 2022, 14, 1524. [Google Scholar] [CrossRef]
- Mahmood, H.; Shaban, M.; Rajpoot, N.; Khurram, S.A. Artificial Intelligence-based methods in head and neck cancer diagnosis: an overview. Br. J. Cancer 2021, 124, 1934–1940. [Google Scholar] [CrossRef]
- Dessale, M.; Mengistu, G.; Mengist, H.M. Nanotechnology: A Promising Approach for Cancer Diagnosis, Therapeutics and Theragnosis. Int. J. Nanomed. 2022, ume 17, 3735–3749. [Google Scholar] [CrossRef]
- Schaffer, A.L.; Pearson, S.-A.; Perez-Concha, O.; Dobbins, T.; Ward, R.L.; van Leeuwen, M.T.; Rhee, J.J.; Laaksonen, M.A.; Craigen, G.; Vajdic, C.M. Diagnostic and health service pathways to diagnosis of cancer-registry notified cancer of unknown primary site (CUP). PLOS ONE 2020, 15, e0230373. [Google Scholar] [CrossRef] [PubMed]
- Pauli, C.; Bochtler, T.; Mileshkin, L.; Baciarello, G.; Losa, F.; Ross, J.S.; Pentheroudakis, G.; Zarkavelis, G.; Yalcin, S.; Özgüroğlu, M.; et al. A Challenging Task: Identifying Patients with Cancer of Unknown Primary (CUP) According to ESMO Guidelines: The CUPISCO Trial Experience. Oncol. 2021, 26, e769–e779. [Google Scholar] [CrossRef]
- Mathew, B.G.; Aliyuda, F.; Taiwo, D.; Adekeye, K.; Agada, G.; Sanchez, E.; Ghose, A.; Rassy, E.; Boussios, S. From Biology to Diagnosis and Treatment: The Ariadne’s Thread in Cancer of Unknown Primary. Int. J. Mol. Sci. 2023, 24, 5588. [Google Scholar] [CrossRef] [PubMed]
- Crosby, D.; et al. Early detection of cancer. Science 2022, 375, eaay9040. [Google Scholar] [CrossRef]
- Gillies, R.J.; Schabath, M.B. Radiomics Improves Cancer Screening and Early Detection. Cancer Epidemiology Biomarkers Prev. 2020, 29, 2556–2567. [Google Scholar] [CrossRef]
- Anghel, S.A.; Ioniță-Mîndrican, C.-B.; Luca, I.; Pop, A.L. Promising Epigenetic Biomarkers for the Early Detection of Colorectal Cancer: A Systematic Review. Cancers 2021, 13, 4965. [Google Scholar] [CrossRef]
- Wu, L.; Qu, X. Cancer biomarker detection: recent achievements and challenges. Chem. Soc. Rev. 2015, 44, 2963–2997. [Google Scholar] [CrossRef]
- Haga, Y.; Uemura, M.; Baba, S.; Inamura, K.; Takeuchi, K.; Nonomura, N.; Ueda, K. Identification of Multisialylated LacdiNAc Structures as Highly Prostate Cancer Specific Glycan Signatures on PSA. Anal. Chem. 2019, 91, 2247–2254. [Google Scholar] [CrossRef]
- Ebell, M.H.; Culp, M.B.; Radke, T.J. A Systematic Review of Symptoms for the Diagnosis of Ovarian Cancer. Am. J. Prev. Med. 2016, 50, 384–394. [Google Scholar] [CrossRef]
- Orr, B.; Edwards, R.P. Diagnosis and treatment of ovarian cancer. Hematol. /Oncol. Clin. 2018, 32, 943–964. [Google Scholar] [CrossRef] [PubMed]
- Bang, J.Y.; Krall, K.; Jhala, N.; Singh, C.; Tejani, M.; Arnoletti, J.P.; Navaneethan, U.; Hawes, R.; Varadarajulu, S. Comparing Needles and Methods of Endoscopic Ultrasound–Guided Fine-Needle Biopsy to Optimize Specimen Quality and Diagnostic Accuracy for Patients With Pancreatic Masses in a Randomized Trial. Clin. Gastroenterol. Hepatol. 2021, 19, 825–835.e7. [Google Scholar] [CrossRef] [PubMed]
- Williamson, J.M.; Hocken, D.B. Pancreatic cancer in the media: the Swayze shift. Ann. R. Coll. Surg. Engl. 2010, 92, 537–538. [Google Scholar] [CrossRef]
- Neighbors, J.; Chase, D.; Harrow, B.; Perhanidis, J.; Monk, B. Gastrointestinal Symptoms and Diagnosis Preceding Ovarian Cancer Diagnosis: Delays in Diagnosis and Resulting Effects on Treatment Allocation. Gynecol. Oncol. 2020, 156, e25–e26. [Google Scholar] [CrossRef]
- Dilley, J.; et al. Ovarian cancer symptoms, routes to diagnosis and survival–Population cohort study in the ‘no screen’arm of the UK Collaborative Trial of Ovarian Cancer Screening (UKCTOCS). Gynecol. Oncol. 2020, 158, 316–322. [Google Scholar] [CrossRef]
- Wang, X.; Zhang, H.; Chen, X. Drug resistance and combating drug resistance in cancer. Cancer Drug Resist. 2019, 2, 141. [Google Scholar] [CrossRef]
- Chatterjee, N.; Bivona, T.G. Polytherapy and targeted cancer drug resistance. Trends Cancer 2019, 5, 170–182. [Google Scholar] [CrossRef]
- Cao, C.; Wang, D.; Chung, C.; Tian, D.; Rimner, A.; Huang, J.; Jones, D.R. A systematic review and meta-analysis of stereotactic body radiation therapy versus surgery for patients with non–small cell lung cancer. J. Thorac. Cardiovasc. Surg. 2019, 157, 362–373.e8. [Google Scholar] [CrossRef] [PubMed]
- Cheng, B.; He, H.; Chen, B.; Zhou, Q.; Luo, T.; Li, K.; Du, T.; Huang, H. Assessment of treatment outcomes: cytoreductive surgery compared to radiotherapy in oligometastatic prostate cancer – an in-depth quantitative evaluation and retrospective cohort analysis. Int. J. Surg. 2024, 110, 3190–3202. [Google Scholar] [CrossRef]
- Camerini, A.; Mazzoni, F.; Scotti, V.; Tibaldi, C.; Sbrana, A.; Calabrò, L.; Caliman, E.; Ciccone, L.P.; Bernardini, L.; Graziani, J.; et al. Efficacy and Safety of Chemotherapy after Immunotherapy in Patients with Advanced Non-Small-Cell Lung Cancer. J. Clin. Med. 2024, 13, 3642. [Google Scholar] [CrossRef]
- D’cunha, R.; D’cunha, P.; Swarup, S.; Sultan, A.; Mogollon-Duffo, F.; Jahan, N.; Htut, T.W.; Wongsaengsak, S.; Adhikari, N.; Mon, A.; et al. Treatment-related adverse events and tolerability in patients with advanced non-squamous non-small cell lung cancer treated with first-line checkpoint inhibitors in combination with chemotherapy. Ann. Oncol. 2019, 30, v729. [Google Scholar] [CrossRef]
- Mukherjee, S. Genomics-Guided Immunotherapy for Precision Medicine in Cancer. Cancer Biotherapy Radiopharm. 2019, 34, 487–497. [Google Scholar] [CrossRef] [PubMed]
- Scheetz, L.; Park, K.S.; Li, Q.; Lowenstein, P.R.; Castro, M.G.; Schwendeman, A.; Moon, J.J. Engineering patient-specific cancer immunotherapies. Nat. Biomed. Eng. 2019, 3, 768–782. [Google Scholar] [CrossRef]
- Pereira, S.P.; et al. Early detection of pancreatic cancer. Lancet Gastroenterol. Hepatol. 2020, 5, 698–710. [Google Scholar] [CrossRef]
- Farr, K.P.; Moses, D.; Haghighi, K.S.; Phillips, P.A.; Hillenbrand, C.M.; Chua, B.H. Imaging Modalities for Early Detection of Pancreatic Cancer: Current State and Future Research Opportunities. Cancers 2022, 14, 2539. [Google Scholar] [CrossRef]
- Tsimberidou, A.M.; Fountzilas, E.; Nikanjam, M.; Kurzrock, R. Review of precision cancer medicine: Evolution of the treatment paradigm. Cancer Treat. Rev. 2020, 86, 102019. [Google Scholar] [CrossRef] [PubMed]
- Kwong, G.A.; Ghosh, S.; Gamboa, L.; Patriotis, C.; Srivastava, S.; Bhatia, S.N. Synthetic biomarkers: a twenty-first century path to early cancer detection. Nat. Rev. Cancer 2021, 21, 655–668. [Google Scholar] [CrossRef]
- Kalia, M. Biomarkers for personalized oncology: recent advances and future challenges. Metabolism 2015, 64, S16–S21. [Google Scholar] [CrossRef] [PubMed]
- Zakari, S.; Niels, N.K.; Olagunju, G.V.; Nnaji, P.C.; Ogunniyi, O.; Tebamifor, M.; Israel, E.N.; Atawodi, S.E.; Ogunlana, O.O. Emerging biomarkers for non-invasive diagnosis and treatment of cancer: a systematic review. Front. Oncol. 2024, 14, 1405267. [Google Scholar] [CrossRef]
- Sarhadi, V.K.; Armengol, G. Molecular biomarkers in cancer. Biomolecules 2022, 12, 1021. [Google Scholar] [CrossRef]
- Gautam, S.K.; Khan, P.; Natarajan, G.; Atri, P.; Aithal, A.; Ganti, A.K.; Batra, S.K.; Nasser, M.W.; Jain, M. Mucins as Potential Biomarkers for Early Detection of Cancer. Cancers 2023, 15, 1640. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Guan, X.; Fan, Z.; Ching, L.-M.; Li, Y.; Wang, X.; Cao, W.-M.; Liu, D.-X. Non-Invasive Biomarkers for Early Detection of Breast Cancer. Cancers 2020, 12, 2767. [Google Scholar] [CrossRef]
- Mohamed, E.; Martínez, D.J.G.; Hosseini, M.-S.; Yoong, S.Q.; Fletcher, D.; Hart, S.; Guinn, B.-A. Identification of biomarkers for the early detection of non-small cell lung cancer: a systematic review and meta-analysis. Carcinog. 2023, 45, 1–22. [Google Scholar] [CrossRef]
- Nicolini, A.; Ferrari, P.; Duffy, M.J. Prognostic and predictive biomarkers in breast cancer: Past, present and future. In Seminars in cancer biology; Elsevier: Amsterdam, The Netherlands, 2018. [Google Scholar]
- Das, V.; Kalita, J.; Pal, M. Predictive and prognostic biomarkers in colorectal cancer: A systematic review of recent advances and challenges. Biomed. Pharmacother. 2017, 87, 8–19. [Google Scholar] [CrossRef]
- Pabst, L.; Lopes, S.; Bertrand, B.; Creusot, Q.; Kotovskaya, M.; Pencreach, E.; Beau-Faller, M.; Mascaux, C. Prognostic and Predictive Biomarkers in the Era of Immunotherapy for Lung Cancer. Int. J. Mol. Sci. 2023, 24, 7577. [Google Scholar] [CrossRef] [PubMed]
- Duffy, M.; Harbeck, N.; Nap, M.; Molina, R.; Nicolini, A.; Senkus, E.; Cardoso, F. Clinical use of biomarkers in breast cancer: Updated guidelines from the European Group on Tumor Markers (EGTM). Eur. J. Cancer 2017, 75, 284–298. [Google Scholar] [CrossRef]
- Harris, L.N.; Ismaila, N.; McShane, L.M.; Andre, F.; Collyar, D.E.; Gonzalez-Angulo, A.M.; Hammond, E.H.; Kuderer, N.M.; Liu, M.C.; Mennel, R.G.; et al. Use of Biomarkers to Guide Decisions on Adjuvant Systemic Therapy for Women With Early-Stage Invasive Breast Cancer: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2016, 34, 1134–1150. [Google Scholar] [CrossRef]
- Cha, Y.; Kim, S.; Han, S.-W. Utilizing Plasma Circulating Tumor DNA Sequencing for Precision Medicine in the Management of Solid Cancers. Cancer Res. Treat. 2023, 55, 367–384. [Google Scholar] [CrossRef]
- Ko, J.; Bhagwat, N.; Yee, S.S.; Ortiz, N.; Sahmoud, A.; Black, T.; Aiello, N.M.; McKenzie, L.; O’hara, M.; Redlinger, C.; et al. Combining Machine Learning and Nanofluidic Technology To Diagnose Pancreatic Cancer Using Exosomes. ACS Nano 2017, 11, 11182–11193. [Google Scholar] [CrossRef]
- Li, B.; Kugeratski, F.G.; Kalluri, R. A novel machine learning algorithm selects proteome signature to specifically identify cancer exosomes. Elife 2024, 12, RP90390. [Google Scholar]
- Das, S.; et al. Biomarkers in cancer detection, diagnosis, and prognosis. Sensors 2023, 24, 37. [Google Scholar] [CrossRef] [PubMed]
- Pan, J.; Song, G.; Chen, D.; Li, Y.; Liu, S.; Hu, S.; Rosa, C.; Eichinger, D.; Pino, I.; Zhu, H.; et al. Identification of Serological Biomarkers for Early Diagnosis of Lung Cancer Using a Protein Array-Based Approach. Mol. Cell. Proteom. 2017, 16, 2069–2078. [Google Scholar] [CrossRef] [PubMed]
- El-Khoury, V.; Schritz, A.; Kim, S.-Y.; Lesur, A.; Sertamo, K.; Bernardin, F.; Petritis, K.; Pirrotte, P.; Selinsky, C.; Whiteaker, J.R.; et al. Identification of a Blood-Based Protein Biomarker Panel for Lung Cancer Detection. Cancers 2020, 12, 1629. [Google Scholar] [CrossRef]
- Loomans-Kropp, H.A.; Song, Y.; Gala, M.; Parikh, A.R.; Van Seventer, E.E.; Alvarez, R.; Hitchins, M.P.; Shoemaker, R.H.; Umar, A. Methylated Septin9 (mSEPT9): A Promising Blood-Based Biomarker for the Detection and Screening of Early-Onset Colorectal Cancer. Cancer Res. Commun. 2022, 2, 90–98. [Google Scholar] [CrossRef]
- Sun, G.; Meng, J.; Duan, H.; Zhang, D.; Tang, Y. Diagnostic Assessment of septin9 DNA Methylation for Colorectal Cancer Using Blood Detection: A Meta-Analysis. Pathol. Oncol. Res. 2018, 25, 1525–1534. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Liu, D.; Zhang, X.; Johnson, H.; Feng, X.; Zhang, H.; Wu, A.H.B.; Chen, L.; Fang, J.; Xiao, Z.; et al. Establishing a Urine-Based Biomarker Assay for Prostate Cancer Risk Stratification. Front. Cell Dev. Biol. 2020, 8. [Google Scholar] [CrossRef]
- Curtit, E.; Vannetzel, J.-M.; Darmon, J.-C.; Roche, S.; Bourgeois, H.; Dewas, S.; Catala, S.; Mereb, E.; Fanget, C.F.; Genet, D.; et al. Results of PONDx, a prospective multicenter study of the Oncotype DX® breast cancer assay: Real-life utilization and decision impact in French clinical practice. Breast 2019, 44, 39–45. [Google Scholar] [CrossRef]
- Chen, X.; Gole, J.; Gore, A.; He, Q.; Lu, M.; Min, J.; Yuan, Z.; Yang, X.; Jiang, Y.; Zhang, T.; et al. Non-invasive early detection of cancer four years before conventional diagnosis using a blood test. Nat. Commun. 2020, 11, 1–10. [Google Scholar] [CrossRef]
- Liu, M.C. Transforming the landscape of early cancer detection using blood tests—Commentary on current methodologies and future prospects. Br. J. Cancer 2021, 124, 1475–1477. [Google Scholar] [CrossRef]
- Echle, A.; Rindtorff, N.T.; Brinker, T.J.; Luedde, T.; Pearson, A.T.; Kather, J.N. Deep learning in cancer pathology: a new generation of clinical biomarkers. Br. J. Cancer 2020, 124, 686–696. [Google Scholar] [CrossRef]
- Wang, H.-Y.; Lin, W.-Y.; Zhou, C.; Yang, Z.-A.; Kalpana, S.; Lebowitz, M.S. Integrating Artificial Intelligence for Advancing Multiple-Cancer Early Detection via Serum Biomarkers: A Narrative Review. Cancers 2024, 16, 862. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.T.; Tan, Y.J.; Oon, C.E. Molecular targeted therapy: Treating cancer with specificity. Eur. J. Pharmacol. 2018, 834, 188–196. [Google Scholar] [CrossRef]
- Wang, M.; Herbst, R.S.; Boshoff, C. Toward personalized treatment approaches for non-small-cell lung cancer. Nat. Med. 2021, 27, 1345–1356. [Google Scholar] [CrossRef]
- Seebacher, N.A.; Stacy, A.E.; Porter, G.M.; Merlot, A.M. Clinical development of targeted and immune based anti-cancer therapies. J. Exp. Clin. Cancer Res. 2019, 38, 1–39. [Google Scholar] [CrossRef]
- Taghiloo, S.; Norozi, S.; Asgarian-Omran, H. The Effects of PI3K/Akt/mTOR Signaling Pathway Inhibitors on the Expression of Immune Checkpoint Ligands in Acute Myeloid Leukemia Cell Line. Iran. J. Allergy, Asthma Immunol. 2022, 21, 178–188. [Google Scholar] [CrossRef] [PubMed]
- Ashworth, A.; Lord, C.J. Synthetic lethal therapies for cancer: what’s next after PARP inhibitors? Nat. Rev. Clin. Oncol. 2018, 15, 564–576. [Google Scholar] [PubMed]
- Hu, Y.; Guo, M. Synthetic lethality strategies: Beyond BRCA1/2 mutations in pancreatic cancer. Cancer Sci. 2020, 111, 3111–3121. [Google Scholar]
- Hosea, R.; Hillary, S.; Wu, S.; Kasim, V. Targeting Transcription Factor YY1 for Cancer Treatment: Current Strategies and Future Directions. Cancers 2023, 15, 3506. [Google Scholar] [CrossRef]
- Blass, E.; Ott, P.A. Advances in the development of personalized neoantigen-based therapeutic cancer vaccines. Nat. Rev. Clin. Oncol. 2021, 18, 215–229. [Google Scholar] [CrossRef]
- Tan, S.; Li, D.; Zhu, X. Cancer immunotherapy: Pros, cons and beyond. Biomed. Pharmacother. 2020, 124, 109821. [Google Scholar]
- Li, M.; Zhu, J.; Lv, Z.; Qin, H.; Wang, X.; Shi, H. Recent Advances in RNA-Targeted Cancer Therapy. ChemBioChem 2023, 25, e202300633. [Google Scholar] [CrossRef] [PubMed]
- Haque, S.; Cook, K.; Sahay, G.; Sun, C. RNA-Based Therapeutics: Current Developments in Targeted Molecular Therapy of Triple-Negative Breast Cancer. Pharmaceutics 2021, 13, 1694. [Google Scholar] [CrossRef]
- Kang, J.-X.; Li, C.; Cheng, Y.-M.; Huang, M.-X.; Zhao, G.-K.; Jin, Z.-L.; Qi, X.-W.; Gu, J.; Ouyang, Q. Advances in Small-Molecule Dual Inhibitors Targeting EGFR and HER2 Receptors as Anti-Cancer Agents. Curr. Med. Chem. 2024, 31, 1–46. [Google Scholar] [CrossRef]
- Taieb, J.; Jung, A.; Sartore-Bianchi, A.; Peeters, M.; Seligmann, J.; Zaanan, A.; Burdon, P.; Montagut, C.; Laurent-Puig, P. The Evolving Biomarker Landscape for Treatment Selection in Metastatic Colorectal Cancer. Drugs 2019, 79, 1375–1394. [Google Scholar] [CrossRef]
- Restrepo, J.C.; Guevara, D.M.; López, A.P.; Palacios, J.F.M.; Liscano, Y. Identification and Application of Emerging Biomarkers in Treatment of Non-Small-Cell Lung Cancer: Systematic Review. Cancers 2024, 16, 2338. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, Y.-C.; Kirschner, K.; Copland, M. Improving outcomes in chronic myeloid leukemia through harnessing the immunological landscape. Leukemia 2021, 35, 1229–1242. [Google Scholar] [CrossRef] [PubMed]
- O’shaughnessy, J.; Robert, N.; Annavarapu, S.; Zhou, J.; Sussell, J.; Cheng, A.; Fung, A. Recurrence rates in patients with HER2+ breast cancer who achieved a pathological complete response after neoadjuvant pertuzumab plus trastuzumab followed by adjuvant trastuzumab: a real-world evidence study. Breast Cancer Res. Treat. 2021, 187, 903–913. [Google Scholar] [CrossRef]
- Huo, K.-G.; Notsuda, H.; Fang, Z.; Liu, N.F.; Gebregiworgis, T.; Li, Q.; Pham, N.-A.; Li, M.; Liu, N.; Shepherd, F.A.; et al. Lung Cancer Driven by BRAFG469V Mutation Is Targetable by EGFR Kinase Inhibitors. J. Thorac. Oncol. 2022, 17, 277–288. [Google Scholar] [CrossRef]
- Breadner, D.A.; Vincent, M.D.; Liu, G.; Rothenstein, J.; Menjak, I.B.; Cheema, P.K.; Juergens, R.A.; Mithoowani, H.; Bains, P.; Wang, Y.; et al. Osimertinib then chemotherapy in EGFR-mutated lung cancer with osimertinib third-line rechallenge (OCELOT). J. Clin. Oncol. 2023, 41, TPS9160. [Google Scholar] [CrossRef]
- Gambardella, V.; Tarazona, N.; Cejalvo, J.M.; Lombardi, P.; Huerta, M.; Roselló, S.; Fleitas, T.; Roda, D.; Cervantes, A. Personalized Medicine: Recent Progress in Cancer Therapy. Cancers 2020, 12, 1009. [Google Scholar] [CrossRef]
- Walcher, L.; Kistenmacher, A.-K.; Suo, H.; Kitte, R.; Dluczek, S.; Strauß, A.; Blaudszun, A.-R.; Yevsa, T.; Fricke, S.; Kossatz-Boehlert, U. Cancer Stem Cells—Origins and Biomarkers: Perspectives for Targeted Personalized Therapies. Front. Immunol. 2020, 11, 1280. [Google Scholar] [CrossRef]
- Bankó, P.; Lee, S.Y.; Nagygyörgy, V.; Zrínyi, M.; Chae, C.H.; Cho, D.H.; Telekes, A. Technologies for circulating tumor cell separation from whole blood. J. Hematol. Oncol. 2019, 12, 1–20. [Google Scholar] [CrossRef]
- Ding, S.; Xing, X.-M.; Ding, Y.; Huang, Q. OncoGPT: An AI assistant for genomic-driven precision oncology. J. Clin. Oncol. 2024, 42, 160. [Google Scholar] [CrossRef]
- Shaikh, N.P.; Barua, J.D.; Shaikh, A.P.; Adhav, S.; Petrovic, N.; Jahja, E.; Peshkova, T.; Nakashidze, I. Genetic polymorphism and current biotechnology approaches of therapeutic aspects within endometrial tumors. Euchembioj Rev. 2025, 1–23. [Google Scholar] [CrossRef]
- Rodriguez, H.; Zenklusen, J.C.; Staudt, L.M.; Doroshow, J.H.; Lowy, D.R. The next horizon in precision oncology: Proteogenomics to inform cancer diagnosis and treatment. Cell 2021, 184, 1661–1670. [Google Scholar] [CrossRef]
- Boehm, K.M.; Khosravi, P.; Vanguri, R.; Gao, J.; Shah, S.P. Harnessing multimodal data integration to advance precision oncology. Nat. Rev. Cancer 2021, 22, 114–126. [Google Scholar] [CrossRef] [PubMed]
- Pulumati, A.; et al. Technological advancements in cancer diagnostics: Improvements and limitations. Cancer Rep. 2023, 6, e1764. [Google Scholar]
- Zubair, M.; Wang, S.; Ali, N. Advanced Approaches to Breast Cancer Classification and Diagnosis. Front. Pharmacol. 2021, 11. [Google Scholar] [CrossRef]
- Dienstmann, R.; Jang, I.S.; Bot, B.M.; Friend, S.; Guinney, J. Database of genomic biomarkers for cancer drugs and clinical targetability in solid tumors. Cancer Discov. 2015, 5, 118–123. [Google Scholar] [CrossRef]
- Kamel, H.F.M.; Al-Amodi, H.S.A.B. Exploitation of gene expression and cancer biomarkers in paving the path to era of personalized medicine. Genom. Proteom. Bioinform. 2017, 15, 220–235. [Google Scholar]
- Song, Z.; Lian, S.; Mak, S.; Chow, M.Z.-Y.; Xu, C.; Wang, W.; Keung, H.Y.; Lu, C.; Kebede, F.T.; Gao, Y.; et al. Deep RNA Sequencing Revealed Fusion Junctional Heterogeneity May Predict Crizotinib Treatment Efficacy in ALK-Rearranged NSCLC. J. Thorac. Oncol. 2022, 17, 264–276. [Google Scholar] [CrossRef] [PubMed]
- Yaeger, R.; Weiss, J.; Pelster, M.S.; Spira, A.I.; Barve, M.; Ou, S.-H.I.; Leal, T.A.; Bekaii-Saab, T.S.; Paweletz, C.P.; Heavey, G.A.; et al. Adagrasib with or without Cetuximab in Colorectal Cancer with Mutated KRAS G12C. New Engl. J. Med. 2023, 388, 44–54. [Google Scholar] [CrossRef]
- Chen, P.; Li, X.; Zhang, R.; Liu, S.; Xiang, Y.; Zhang, M.; Chen, X.; Pan, T.; Yan, L.; Feng, J.; et al. Combinative treatment of β-elemene and cetuximab is sensitive to KRAS mutant colorectal cancer cells by inducing ferroptosis and inhibiting epithelial-mesenchymal transformation. Theranostics 2020, 10, 5107–5119. [Google Scholar] [CrossRef] [PubMed]
- Donovan, M.J.; Meurs, C.; Fernandez, G.; Madduri, A.S.; Feliz, A.; Zeineh, J.; DeAngel, R.; Westenend, P. AI-enabled digital test to predict disease recurrence for patients with early-stage invasive breast cancer and performance in a MammaPrint low-risk cohort from the Netherlands with a median 6-year follow-up. J. Clin. Oncol. 2024, 42, 1569. [Google Scholar] [CrossRef]
- Jeong, S.Y.; Chung, J.-Y.; Byeon, S.-J.; Kim, C.J.; Lee, Y.-Y.; Kim, T.-J.; Lee, J.-W.; Kim, B.-G.; Chae, Y.L.; Oh, S.Y.; et al. Validation of Potential Protein Markers Predicting Chemoradioresistance in Early Cervical Cancer by Immunohistochemistry. Front. Oncol. 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- Khattak, M.A.; Reid, A.; Freeman, J.; Pereira, M.; McEvoy, A.; Lo, J.; Frank, M.H.; Meniawy, T.; Didan, A.; Spencer, I.; et al. PD-L1 Expression on Circulating Tumor Cells May Be Predictive of Response to Pembrolizumab in Advanced Melanoma: Results from a Pilot Study. Oncol. 2019, 25, e520–e527. [Google Scholar] [CrossRef]
- Incorvaia, L.; Rinaldi, G.; Badalamenti, G.; Cucinella, A.; Brando, C.; Madonia, G.; Fiorino, A.; Pipitone, A.; Perez, A.; Pomi, F.L.; et al. Prognostic role of soluble PD-1 and BTN2A1 in overweight melanoma patients treated with nivolumab or pembrolizumab: finding the missing links in the symbiotic immune-metabolic interplay. Ther. Adv. Med Oncol. 2023, 15. [Google Scholar] [CrossRef]
- Camidge, D.R.; Doebele, R.C.; Kerr, K.M. Comparing and contrasting predictive biomarkers for immunotherapy and targeted therapy of NSCLC. Nat. Rev. Clin. Oncol. 2019, 16, 341–355. [Google Scholar] [CrossRef]
- Jackson, S.E.; Chester, J.D. Personalised cancer medicine. Int. J. Cancer 2015, 137, 262–266. [Google Scholar] [CrossRef]
- Fulton, J.J.; LeBlanc, T.W.; Cutson, T.M.; Starr, K.N.P.; Kamal, A.; Ramos, K.; E Freiermuth, C.; McDuffie, J.R.; Kosinski, A.; Adam, S.; et al. Integrated outpatient palliative care for patients with advanced cancer: A systematic review and meta-analysis. Palliat. Med. 2018, 33, 123–134. [Google Scholar] [CrossRef]
- Balitsky, A.K.; et al. Patient-reported outcome measures in cancer care: an updated systematic review and meta-analysis. JAMA Network Open 2024, 7, e2424793. [Google Scholar]
- Liu, Q.; Wang, C.; Zheng, Y.; Zhao, Y.; Wang, Y.; Hao, J.; Zhao, X.; Yi, K.; Shi, L.; Kang, C.; et al. Virus-like nanoparticle as a co-delivery system to enhance efficacy of CRISPR/Cas9-based cancer immunotherapy. Biomaterials 2020, 258, 120275. [Google Scholar] [CrossRef]
- Aghamiri, S.; Talaei, S.; Ghavidel, A.A.; Zandsalimi, F.; Masoumi, S.; Hafshejani, N.H.; Jajarmi, V. Nanoparticles-mediated CRISPR/Cas9 delivery: Recent advances in cancer treatment. J. Drug Deliv. Sci. Technol. 2020, 56. [Google Scholar] [CrossRef]
- Mao, X.; Wu, S.; Huang, D.; Li, C. Complications and comorbidities associated with antineoplastic chemotherapy: Rethinking drug design and delivery for anticancer therapy. Acta Pharm. Sin. B 2024, 14, 2901–2926. [Google Scholar] [CrossRef]
- Levy, R.; Zhen, S.; Zhang, C.; Moon, J.-Y.; Bteich, F.; Kuang, C. Impact of adjuvant chemotherapy on outcomes after curative-intent surgery for biliary tract cancer: A 10-year retrospective single-center study. J. Clin. Oncol. 2024, 42, e16273. [Google Scholar] [CrossRef]
- Olson, D.J.; Eroglu, Z.; Brockstein, B.; Poklepovic, A.S.; Bajaj, M.; Babu, S.; Hallmeyer, S.; Velasco, M.; Lutzky, J.; Higgs, E.; et al. Pembrolizumab Plus Ipilimumab Following Anti-PD-1/L1 Failure in Melanoma. J. Clin. Oncol. 2021, 39, 2647–2655. [Google Scholar] [CrossRef] [PubMed]
- Helena, A.Y.; et al. Effect of osimertinib and bevacizumab on progression-free survival for patients with metastatic EGFR-mutant lung cancers: a phase 1/2 single-group open-label trial. JAMA Oncol. 2020, 6, 1048–1054. [Google Scholar]
- O'Shaughnessy, J.; Graham, C.L.; Whitworth, P.; Beitsch, P.D.; Osborne, C.R.C.; Rahman, R.L.; Brown, E.A.; Gold, L.P.; Johnson, N.M.; Brufsky, A.; et al. Association of MammaPrint index and 3-year outcome of patients with HR+HER2- early-stage breast cancer treated with chemotherapy with or without anthracycline. J. Clin. Oncol. 2024, 42, 511. [Google Scholar] [CrossRef]
- Guarneri, V.; Griguolo, G.; Miglietta, F.; Conte, P.; Dieci, M.; Girardi, F. Survival after neoadjuvant therapy with trastuzumab–lapatinib and chemotherapy in patients with HER2-positive early breast cancer: a meta-analysis of randomized trials. ESMO Open 2022, 7, 100433. [Google Scholar] [CrossRef]
- Solomon, B.; Loong, H.; Summers, Y.; Thomas, Z.; French, P.; Lin, B.; Sashegyi, A.; Wolf, J.; Yang, J.-H.; Drilon, A. Correlation between treatment effects on response rate and progression-free survival and overall survival in trials of targeted therapies in molecularly enriched populations. ESMO Open 2022, 7, 100398. [Google Scholar] [CrossRef]
- Tsimberidou, A.; Fu, S.; Hong, D.; Piha-Paul, S.; Naing, A.; Rodon, J.; Yap, T.; Karp, D.; Dumbrava, E.; Heymach, J.; et al. 638P Final results of IMPACT 2, a randomized study evaluating molecular profiling and targeted agents in metastatic cancer at MD Anderson Cancer Center. Ann. Oncol. 2024, 35, S506–S507. [Google Scholar] [CrossRef]
- Neagu, A.-N.; Bruno, P.; Johnson, K.R.; Ballestas, G.; Darie, C.C. Biological Basis of Breast Cancer-Related Disparities in Precision Oncology Era. Int. J. Mol. Sci. 2024, 25, 4113. [Google Scholar] [CrossRef] [PubMed]
- Aldea, M.; Andre, F.; Marabelle, A.; Dogan, S.; Barlesi, F.; Soria, J.-C. Overcoming Resistance to Tumor-Targeted and Immune-Targeted Therapies. Cancer Discov. 2021, 11, 874–899. [Google Scholar] [CrossRef]
- Sharma, K.; Mayer, T.; Li, S.; Qureshi, S.; Farooq, F.; Vuylsteke, P.; Ralefala, T.; Marlink, R. Advancing oncology drug therapies for sub-Saharan Africa. PLOS Glob. Public Heal. 2023, 3, e0001653. [Google Scholar] [CrossRef]
- Twahir, M.; Oyesegun, R.; Yarney, J.; Gachii, A.; Edusa, C.; Nwogu, C.; Mangutha, G.; Anderson, P.; Benjamin, E.; Müller, B.; et al. Real-world challenges for patients with breast cancer in sub-Saharan Africa: a retrospective observational study of access to care in Ghana, Kenya and Nigeria. BMJ Open 2021, 11, e041900. [Google Scholar] [CrossRef] [PubMed]
- Fu, Y.; Saraswat, A.; Wei, Z.; Agrawal, M.Y.; Dukhande, V.V.; Reznik, S.E.; Patel, K. Development of Dual ARV-825 and Nintedanib-Loaded PEGylated Nano-Liposomes for Synergistic Efficacy in Vemurafnib-Resistant Melanoma. Pharmaceutics 2021, 13, 1005. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Tsui, S.T.; Liu, C.; Song, Y.; Liu, D. EGFR C797S mutation mediates resistance to third-generation inhibitors in T790M-positive non-small cell lung cancer. J. Hematol. Oncol. 2016, 9, 1–5. [Google Scholar] [CrossRef]
- Helena, A.Y.; et al. Acquired resistance of EGFR-mutant lung cancer to a T790M-specific EGFR inhibitor: emergence of a third mutation (C797S) in the EGFR tyrosine kinase domain. JAMA Oncol. 2015, 1, 982–984. [Google Scholar]
- Liu, D. Cancer biomarkers for targeted therapy. Biomark. Res. 2019, 7, 25. [Google Scholar] [CrossRef]
- Dong, P.; Mao, A.; Qiu, W.; Li, G. Improvement of Cancer Prevention and Control: Reflection on the Role of Emerging Information Technologies. J. Med Internet Res. 2024, 26, e50000. [Google Scholar] [CrossRef]
- Hesse, B.W.; Kwasnicka, D.; Ahern, D.K. Emerging digital technologies in cancer treatment, prevention, and control. Transl. Behav. Med. 2021, 11, 2009–2017. [Google Scholar] [CrossRef] [PubMed]
- Fu, S.W.; Tang, C.; Tan, X.; Srivastava, S. Liquid biopsy for early cancer detection: technological revolutions and clinical dilemma. Expert Rev. Mol. Diagn. 2024, 24, 937–955. [Google Scholar] [CrossRef] [PubMed]
- Yu, W.; Hurley, J.; Roberts, D.; Chakrabortty, S.; Enderle, D.; Noerholm, M.; Breakefield, X.; Skog, J. Exosome-based liquid biopsies in cancer: opportunities and challenges. Ann. Oncol. 2021, 32, 466–477. [Google Scholar] [CrossRef]
- Jin, D.; Khan, N.U.; Gu, W.; Lei, H.; Goel, A.; Chen, T. Informatics strategies for early detection and risk mitigation in pancreatic cancer patients. Neoplasia 2025, 60, 101129. [Google Scholar] [CrossRef]
- Rolfo, C.; Russo, A. Moving Forward Liquid Biopsy in Early Liver Cancer Detection. Cancer Discov. 2023, 13, 532–534. [Google Scholar] [CrossRef]
- Milner, D.A., Jr.; Lennerz, J.K. Technology and future of multi-cancer early detection. Life 2024, 14, 833. [Google Scholar] [CrossRef] [PubMed]
- Passaro, A.; Al Bakir, M.; Hamilton, E.G.; Diehn, M.; André, F.; Roy-Chowdhuri, S.; Mountzios, G.; Wistuba, I.I.; Swanton, C.; Peters, S. Cancer biomarkers: Emerging trends and clinical implications for personalized treatment. Cell 2024, 187, 1617–1635. [Google Scholar] [CrossRef]
- Chen, M.; Zhao, H. Next-generation sequencing in liquid biopsy: cancer screening and early detection. Hum. Genom. 2019, 13, 34. [Google Scholar] [CrossRef]
- Molla, G.; Bitew, M. Revolutionizing Personalized Medicine: Synergy with Multi-Omics Data Generation, Main Hurdles, and Future Perspectives. Biomedicines 2024, 12, 2750. [Google Scholar] [CrossRef]
- Cai, Z.; Poulos, R.C.; Liu, J.; Zhong, Q. Machine learning for multi-omics data integration in cancer. iScience 2022, 25, 103798. [Google Scholar] [CrossRef]
- Zhang, Y.; Ma, W.; Huang, Z.; Liu, K.; Feng, Z.; Zhang, L.; Li, D.; Mo, T.; Liu, Q. Research and application of omics and artificial intelligence in cancer. Phys. Med. Biol. 2024, 69, 21TR01. [Google Scholar] [CrossRef]
- Song, I.-W.; Vo, H.H.; Chen, Y.-S.; Baysal, M.A.; Kahle, M.; Johnson, A.; Tsimberidou, A.M. Precision Oncology: Evolving Clinical Trials across Tumor Types. Cancers 2023, 15, 1967. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Different types of cancer biomarkers such as DNA, mRNAs, proteins and enzymes. The picture is assembled using dynamic BioRender.
Figure 1.
Different types of cancer biomarkers such as DNA, mRNAs, proteins and enzymes. The picture is assembled using dynamic BioRender.
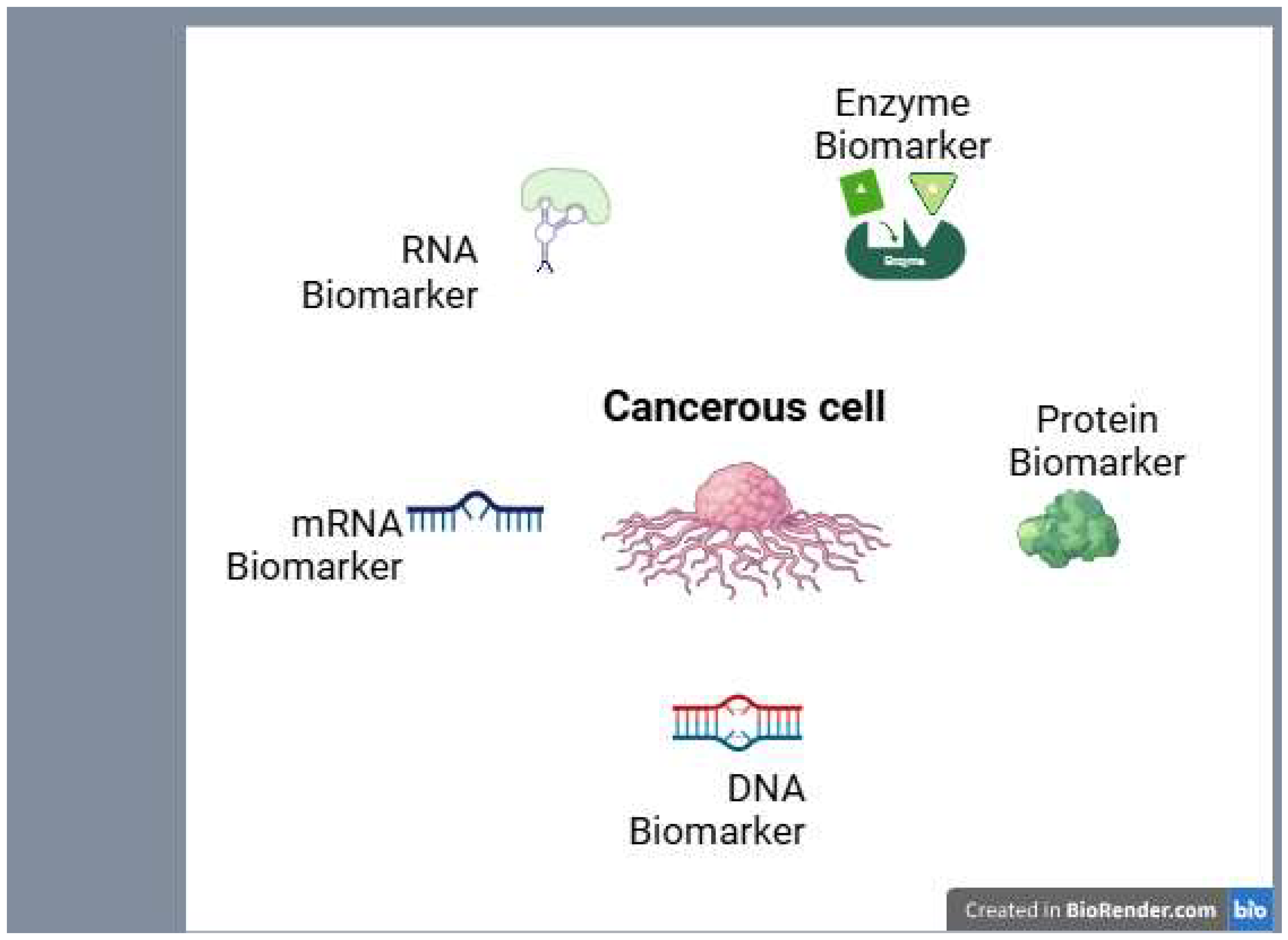
Figure 2.
Personalized molecular treatment and AI therapies vs conventional treatment techniques in cancer. The picture is assembled using dynamic BioRender.
Figure 2.
Personalized molecular treatment and AI therapies vs conventional treatment techniques in cancer. The picture is assembled using dynamic BioRender.
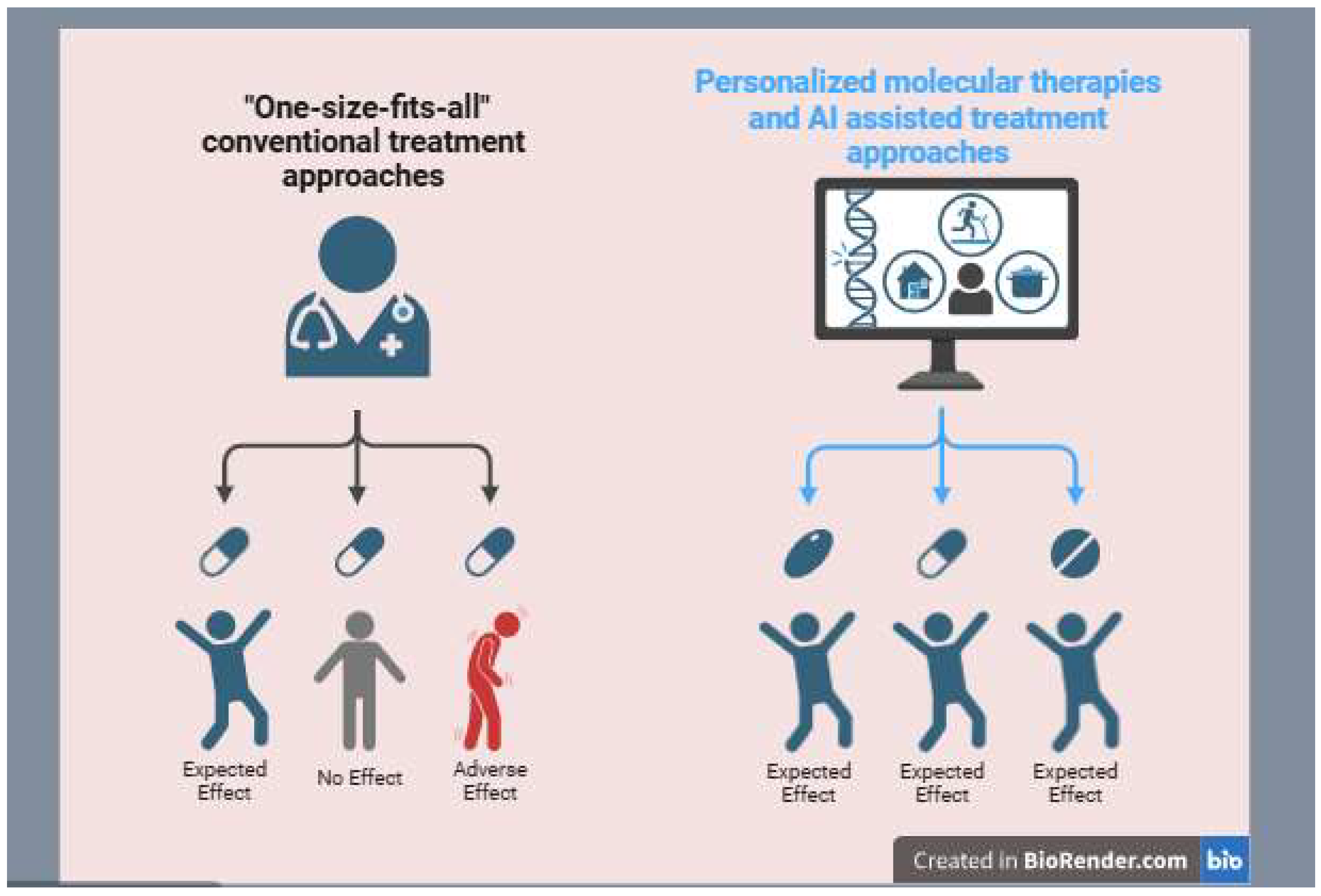

Table 1.
Cancer diagnosis: Conventional vs. Advanced Methods.
| Aspect | Conventional diagnosis | Advanced diagnosis |
|---|---|---|
| Techniques | - Biopsy (tissue examination) - Imaging (X-ray, CT, MRI, Ultrasound) - Blood tests (tumor markers like PSA, CA-125) |
-Liquid biopsy (circulating tumor DNA, CTCs) - Next-generation sequencing (NGS) - AI-powered imaging analysis - Single-cell RNA sequencing (scRNA-seq) - multi-omics profiling (genomics, proteomics, metabolomics) |
| Accuracy | Moderate, requires invasive procedures and may not detect early-stage cancer | High, enables early detection and real-time monitoring of tumor evolution |
| Personalization | “One-size-fits-all” approach, based on histology and general tumor characteristics | Highly personalized, identifying genetic mutations and molecular signatures for tailored treatment |
| Speed of Results | Can take weeks due to tissue processing and pathology | Faster, especially with AI-driven and liquid biopsy techniques |
Table 2.
Types of biomarkers and their purpose.
| Biomarker types | Purpose | Examples |
|---|---|---|
| Diagnostic biomarker | Detect cancer presence | PSA, CA-125, CTCs |
| Prognostic biomarker | Predict cancer outcome | HER2, Ki-67, TP53 mutations |
| Predictive biomarker | Guide treatment selection | EGFR mutations, PD-L1 expression |
| Monitoring biomarker | Track disease progression | CEA, ctDNA, imaging-based markers |
Table 3.
list of various cancer types along with their associated biomarker types.
| Cancer types | Biomarker Types | Monitoring Biomarker |
|---|---|---|
| Prostate cancer | Diagnostic (PSA) | Monitoring PSA levels |
| Ovarian cancer | Diagnostic (CA-125) | Monitoring CA-125 levels |
| Breast cancer | Predictive (HER2) | Monitoring HER2 levels |
| Lung cancer | Diagnostic (Early CDT-Lung) | Monitoring CTDNA |
| Colorectal cancer | Diagnostic (CEA) | Monitoring CEA levels |
| Melanoma | Prognostic (BRAF mutations) | Monitoring LDH levels |
| Pancreatic cancer | Diagnostic (CA 19-9) | Monitoring CA 19-9 levels |
| Liver cancer | Diagnostic (AFP) | Monitoring AFP levels |
| Bladder cancer | Diagnostic (NMP22) | Monitoring NMP22 levels |
| Testicular cancer | Diagnostic (AFP, hCG) | Monitoring AFP levels |
Table 4.
Cancer treatment: Conventional vs. Advanced Methods.
| Aspect | Conventional Treatment | Advanced Treatment |
|---|---|---|
| Techniques | - Surgery (tumor removal) - Chemotherapy - Radiation therapy |
- Targeted therapy (EGFR inhibitors, BRAF inhibitors) - Immunotherapy (CAR-T cells, checkpoint inhibitors) - CRISPR gene editing - Personalized medicine (based on genetic profiling) - AI-driven drug discovery |
| Specificity | Non-specific, affecting both cancerous and healthy cells | Highly specific, targeting cancer cells while minimizing damage to normal cells |
| Side Effects | High, including nausea, hair loss, immune suppression | Reduced, as treatments are more focused and personalized |
| Effectiveness | Variable, depends on cancer type and stage | Higher efficacy in many cases, especially for resistant or rare cancers |
| Recurrence Rate | Often high due to incomplete tumor eradication | Lower, as targeted treatments disrupt cancer pathways effectively |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



