Submitted:
28 March 2025
Posted:
31 March 2025
You are already at the latest version
Abstract
The osseus skeleton is the 3rd commonest site of metastasis due to malignancy, behind lung and liver.1 Metastatic bone disease (MBD), also known as secondary bone cancer, is a common event which signals increased morbidity and early mortality2. Recently, the duration of survival for patients with MBD has increased3, 4 likely due to advancements in medical and surgical techniques. MBD is therefore an increasingly common issue that orthopaedic surgeons are required to manage and investigate, and improvements in care have led to improved survival of this patient population. The British Orthopaedic Association have issued guidelines on Management of MBD in 20155 A recent audit of these guidelines demonstrated that current practice in the UK does not comply with national guidelines set out by BOOS/BOA1. This article will outline presentation, investigation and current recommended treatment of MBD, as well as prognosis, and future possibilities in managing MBD. This article aims to improve awareness and details appropriate management for patients presenting with MBD for UK based clinicians and surgeons.
Keywords:
metastasis
; skeleton
; management
1. Introduction
The skeleton is the 3rd commonest site of metastasis due to malignancy, behind lung and liver.[1] Metastatic bone disease (MBD) is a common event which signals increased morbidity and early mortality[2]. The malignancies which commonly spread to bone include prostate, breast, lung, kidney, thyroid and myeloma[6] however, metastatic bone disease (or secondary bone cancer) can develop in any bone in the body[6]. Although the incidence of MBD can be difficult to determine, a study of prevalence and prognosis of bone metastasis using the SEER database (An American Surveillance, Epidemiology and End Results program by the National cancer institute), between 2010 and 2015, found that 5.1% of patients with a newly diagnosed cancer were also diagnosed with metastatic bone disease [7]. The commonest primary site for adults over 25 years old with MBD was lung cancer, followed by breast and prostate as primary tumour sources.[8] A Cohort study by Danish researchers analysing cases from 1994-2010 demonstrated that only one in 10 patients with MBD from breast cancer survived 5 years. The median-survival from diagnosis of MBD is variable and is dependent on the primary source – a 2017 study demonstrated 6 months for melanoma and lung cancer, 12 months in renal cell carcinoma, and 48 months in thyroid cancer.
Recently, the duration of survival for patients with MBD has increased, likely contributed by both advancements in medical and surgical techniques – this has been confirmed by studies from Scandanvia[3] and North America[4]. With management improving patient outcomes, there is a responsibility on Orthopaedic surgeons to maintain Quality of Life (QoL) as far as possible, by reducing risk and treating SRE – Skeletal-Related Events[9] . SRE’s are defined as events such as spinal cord compression, severe pain or impending fracture (requiring radiation therapy to bone), pathologic fracture, and surgery to bone[10,11]. SREs can lead to severe pain, increased risk of death, increased health care costs and reduced quality of life[9].
The British Orthopaedic Association have issued guidelines on Management of MBD in 2015[5]. These guidelines state that patients with suspected MBD should be investigated along a defined pathway, from first investigation to long-term rehabilitation[9]. It sets out 16 standards for practice (Figure 1). Exceptions to these guidelines are Osteoporotic or stress fractures as well as spinal metastases. Included in the guidelines is any suspected MBD of the appendicular skeleton, pelvis and scapula.
The British Orthopaedic Oncology Management (BOOM) Audit, a prospective, multicentre study of Management of MBD in the UK in 2021, demonstrated that current practice in the UK does not comply with national guidelines set out by BOOS/BOA[12]. This specifically relates to blood/imaging investigations prior to surgery as well as when managing patients with solitary metastases [12].
MBD is an increasingly common issue that orthopaedic surgeons are required to manage and investigate, and improvements in care have led to improved survival of this patient population. This article aims to improve awareness, as well as outline presentation, investigation and appropriate management for patients presenting with MBD.
2. Clinical Presentation
Patients with MBD inevitably present in a variety of ways[9]. Some are diagnosed incidentally, presenting with few or no symptoms whilst others present with prodromal symptoms: pain on weight-bearing, nighttime pain or chronic pain not settling in primary care. This pain can range from a dull, mild ache to severe, intense, sharp pain at the site of MBD. Patients may also present more acutely with pathological fracture or, in instances of spinal metastasis, neurological compromise. Patients may also present with biochemical abnormalities, such as hypercalcaemia (corrected Calcium >2.6mmol/L). NICE guidance confirms that 90% of cases of hypercalcaemia are due to either primary hyperparathyroidism or malignancy[13].
Once a patient has presents with symptoms suggestive of suspected MBD, they should be investigated and treated as per these guidelines.[5]
3. Radiographic Presentation
Imaging techniques have different sensitivities for detecting MBD. A plain radiograph has sensitivity of approximately 50%, with CT 85% and MRI 90% for detection of MBD[14]. Bone scintigraphy or technetium bone scan 80% is the most sensitive at identifying both sclerotic and lytic lesions. Skeletal metastasis can incite 3 different responses from bone, dependent on the primary source. These are lytic/osteolytic, sclerotic/osteoblastic and mixed lytic/sclerotic disease[14,15].
Plain Radiographs are the initial radiological investigation of choice for patient presenting with pain originating from a bone, however, lesions may not be apparent until >1-2cm and with loss of 50% or more of bone mineral content at the site of MBD[16]. Plain radiographs are better at identifying osteolytic lesions that sclerotic lesions. Unlike primary bone tumours, secondary bone cancer (MBD) generally generates either no or a limited periosteal reaction.
BOOS guidelines advise that a radiograph demonstrating avulsion of the lesser trochanter is an indication of imminent hip fracture[9]. Phillips in 1998 highlights this, with 4 patients found to have metastatic carcinoma presenting with an isolated avulsion fracture of the lesser trochanter[17] and another case report conclude that LT avulsion fracture in adults with no or only minor associated trauma is rare and should always lead to further investigation to rule out MBD[18].
4. Mirel Classification
The Mirel classification is a points-based scoring system that can be used to predict the risk of pathological fracture of sites of metastatic bone disease in long bones.[19] The classification is based on site, location, type of lesion and presence/absence of pain.[20]

Table 1.
Mirel classification [20].
Table 1.
Mirel classification [20].
| Variable | Score | ||
| 1 | 2 | 3 | |
| Site of lesion | Upper limb | Lower limb | Trochanteric region |
| Size of lesion (cortical thickness) | <1/3rd diameter | 1/3-2/3rd diameter | >2/3rd diameter |
| Nature of lesion | Blastic | Mixed | Lytic |
| Pain | Mild | Moderate | Functional |
Prophylactic fixation confers more advantages over acute pathological fixation as there is evidence of decreased complications, reduced hospital length of stay[21] as well as reduced mortality[22]. A Score of >8 suggests prophylactic fixation is required. [23] A Score of 8 requires clinical judgement/ consideration, and a score of <8 means the lesion may be better suited to radiotherapy. [24] Mirel’s classification has a 91% sensitivity but a 35% specificity, meaning there will be more false positives, and therefore unnecessary fixations.[25] A previous classification used to predict pathological fracture risk was Harrington in 1980. This criterion is based on the following criteria: lesion involving >50% of cortical bone, the lesion >2.5 cm, presence of pain post-radiotherapy, fracture of the lesser trochanter.[26] This classification has not been fully validated[27] and the grading system does not account for pathology-specific disease[28].
5. Current Management Approach
The priorities of management in MBD are for patients to remain pain free, to be able to mobilize and retain independence[29]. Treatments include medical (biphosphates, or monoclonal antibody therapy - Denosumab [30]), immuno/hormonal/chemotherapy, radiotherapy and surgery, depending on the primary source[16] Often treatment involves a combination of the above and the orthopaedic treatment should form part of a multidisciplinary approach to patient managment[9].
Pathological fractures occur in 10-30% of all cancer patients[31]. Proximal aspects of the long bones have the highest frequency of fracture, with the femur accounting for over half all cases[30,31]. Depending on the site of the lesion, different fixation methods are preferred. For Peri-trochanteric lesions of the femur, intra-medullary nails are used to prophylactically treat the lesion. If the lesion is present in the femoral head/neck, a hemiarthroplasty is preferred. [23]
The BOA guideline outlines different techniques of fixation depending on site of MBD in the appendicular skeleton, but surgical fixation requires an individualized approach. In general, surgical options are between IM Nailing or occasionally plate/screws augmented with cement for internal fixation, or to replace the bone with an Endo prosthetic implant. Amputation may also be suitable, depending on individual patient circumstances.
The BOOS guidelines set out 5 general orthopaedic principles for managing pathological fractures/lesions with a high risk of pathological fracture.[9] They are:
1) Primary bone tumour should be excluded – this is important to prevent a ‘whoops’ procedure (detailed later in the article).
2) The surgeon(s) should provide immediate absolute stability, allowing weight-bearing – this is essential for maintaining mobility/independence where possible and reducing risks of complications such as thromboembolic events, deconditioning and atelectasis.
3) The surgeon must assume that the fracture will not unite.
4) The fixation should last a lifetime.
5) All lesions in affected bone should be stabilised if safe to do so, treatments should also be appropriate with regards to patient preference and patient general condition.
Pathological fractures are fractures that occur in abnormal bone and occur either spontaneously or following minimal trauma, that would not usually be expected to cause a fracture in a biomechanically normal bone[32]. They occur due to an imbalance in stresses placed onto the bone[33] and bone destruction may induce as stress riser, [9] which can lead to fracture. Generally, pathological fractures of the lower limb are more problematic and disabling for patients, as they limit weight-bearing[28]. Upper limb pathological fractures are generally under lower stress, as they are not essential for weight-bearing. The commonest areas of pathological fracture to occur are the subtrochanteric femur, humeral head and vertebral body[33]. Due to the lower energy force required to cause the pathological fracture, often soft tissue injury is less severe compared to traumatic fractures of normal bone[9].
The BOOS guidelines note that fractures due to MBD may go onto develop non-union, especially if given radiotherapy[8]. Radiotherapy is given as a treatment option to help manage pain and achieve local tumour control[34]. This in turn aims to improve quality of life by reducing analgesia requirements as well as keeping mechanical skeletal function[35]. Radiotherapy is used to prevent pathological fracture by treating osteolytic lesions[36]. It is crucial that the entire bone and operative site be included in post-operative radiotherapy, as IM Nailing has the potential to spread malignant cells via the medullary canal[9]. This is an acceptable risk in those who have multiple sites of metastasis.
There is also a role for embolization pre-operatively for patients with specific malignancies. Renal and Thyroid cancers are specific examples, which if operated on without embolization beforehand, have an increased risk of intra-operative blood loss and increase surgical complication, due to the hypervascular nature of the tumours[37]. Preoperative embolization of bony metastases has been extensively reported as both effective and safe to perform – there is evidence that it reduced intra-operative blood loss both for spinal metastases[32] and long bone metastases[39]. A literature review in 2020 stated that 36-75% of cases achieve successful embolization (defined as >70% vascularity being obliterated). This review notes complication from the procedure between 0-9%[3].It is important to note the timing of embolization is key, and it remains unclear as to the optimal interval timing to formally fix MBD after embolization A recent study from 2023 suggests that surgery may be safely delayed beyond 24 hours without significant different in outcomes – in terms of both time on table and bleeding risk[40]. One study notes no significant difference in blood loss between patients who underwent definitive fixation after more than 36 hours, compared to those fixed within 24 hours[41].
Bisphosphonates are a standard treatment of prevention and treatment of MBD. They inhibit osteoclast activity[42], therefore inhibiting bone resorption. Due to their mechanism of action, bisphosphonates are mainly used in the management of osteolytic lesions[43]. Examples of bisphosphonates used in treatment of symptomatic MBD include Clodronate, Pamidronate and Zoledronic acid. They are often indicated if a patient has multiple painful sites of MBD[35]. Bisphosphates are also indicated in management of MBD in situations of hypercalcemia, alongside fluid resuscitation[44] but should not be prescribed to patients with hypocalcaemia, severe CKD, or pregnant/breastfeeding women. The main adverse effects encountered with bisphosphonates are upper GI issues such as dysphagia, oesophageal disease (ulcers, strictures, oesophagitis), gastritis and peptic ulceration, as well as gastrointestinal upset – nausea, dyspepsia and abdominal pain. Patients can also develop bone/joint/muscle pains. Like Denosumab, Osteonecrosis of the Jaw can also occur[45]. Due to this risk, NHS England advises that all patients who are due to be prescribed bisphosphates should have a dental exam and have completed any ongoing dental treatment 2 weeks prior to stating therapy[46].
Denosumab is a monoclonal antibody. It is licenced in the BNF for both prevention of skeletal related events (SRE) in patient with MBD and for bone loss associated with hormone ablation in men with prostate cancer at increased risk of fractures[8,47]. By inhibiting RANKL (Receptor activator of nuclear factor kappa-Β ligand), it reduces osteoclast-mediated destruction of bone, which aims to reduce bone resorption and prevent skeletal events such as pathological fracture[48]. Contra-indications for its use include hypocalcaemia and unhealed lesions from dental/oral surgery. Cautions of Denosumab include osteonecrosis of the jaw/external auditory canal, increased risk of fracture in post-menopausal women and its main side effects are abdominal discomfort/GI upset, hypocalcaemia/hypophosphatemia, increased risk of infection, pain, sciatica and skin reactions. There is an uncommon side effect of atypical femoral fractures, and so any patient with new or unusual thigh/hip/groin pain on this therapy should be carefully reviewed. NICE guidelines advocate that adults with bony metastases from solid tumours (with the exception of prostate) could potentially be treated with Denosumab[49].
Thromboembolic prophylaxis is also a key aspect of management for patients with MBD. BOOS guidance has key points which specifically outlines that patients with MBD are at increased risk of thrombo-embolism, particularly their disease renders them less/immobile[9]. Accordingly, appropriate mechanical and chemical prophylaxis must be considered and documented for each patient. NICE guidelines risk assessment for VTE included multiple factors that would apply to most patients with MBD – active cancer, over age 60, significantly reduced mobility, surgery to lower limb/pelvis[50]. The NICE guidelines also outline the bleeding risk/ relative contraindications to giving thromboprophylaxis, with the specific consideration for the MBD population being Thrombocytopaenia (defined as platelets< 75x109 /l)[50]. NICE guidance on thrombocytopenia advises that Haematological malignancies such as myeloma, and metastatic cancer can cause patient to become thrombocytopenic, as well as treatment with radiotherapy or systemic chemotherapy[51]. As a result of this, regular blood count monitoring and consideration based on patient condition/treatment regarding thromboprophylaxis should occur.
6. Biopsy
The BOOS 2015 guidance advises biopsy is required with there is doubt about underlying pathology, to prevent a ‘whoops proceedure’[9]. This is where a cancerous lesion, which subsequently turns out to be a soft-tissue sarcoma, is operated on by a surgeon not aware of the diagnosis [52]. This is an issue as the type of operation is less likely to achieve clearance at the margins, with residual tumour being left behind, necessitating further surgery. The BOOS guidance (section 6.2) also states that Biopsy of a solitary bone lesion should always be carried out in consultation with a member of bone sarcoma MDT, and usually by that consultant.
Any patient with solitary bone lesion, they should therefore be investigated with a full history and examination and further investigations/ tests. These should include FBC, U+E, LFT, bone profile, CRP, ESR(or plasma viscosity) and tumour markers, as well as consideration of CT CAP, MRI scan of the lesion and isotope bone scanning. Patients with previously diagnosed disseminated malignancy in bone, do not usually require biopsy. Biopsy of the lesion can reveal an alternative diagnosis, either in terms of metastatic source, or reveal a benign diagnosis. Biopsy may also permit different treatment options, for example hormonal therapy in breast cancer. If a biopsy is appropriate to perform, it can be done with percutaneous instruments via image guidance, such as fluoroscopy, or CT.
Common Tumour markers may be detected from various tissues or fluids such as blood, urine, stool, soft tissues biopsy, bone and bone marrow[53]. Tumour markers are measurable substances that are either produced by or present in cancer cells [53]. These are usually proteins, but increasingly genomic markers are being used as tumour markers. Depending on the type of cancer and tumour marker, they have differing sensitivities and specificities[54], but there is potential for these markers to be used to aid in the screening, diagnosis, monitoring of response and detection of recurrence of malignancy[9], depending on type of cancer.
7. Tertiary versus Non-Specialised Centres
It is important to recognise which presentations, investigations and management can be safely facilitated in a primary hospital, and which presentations need to be referred to major/tertiary care centres. BOAST guidelines advises that all units, regardless of hospital, should have an agreed policy for MDT discussion and mangement, including pathways for ongoing referrals. It is important to highlight that specialist centres should have agreed pathways to allow efficient and quick advice/input and transfers to the local hospitals in their regions. The guidelines clearly advise that biopsy of a suspected primary bone tumour must be done at a bone sacroma centre. This is defined as a specialised commissioned service for the management of bone sarcoma. Referral to a bone sacroma centre should also be undertaken if the CT-TAP does not demonstrate malignancy, as this potentially indicates a primary bone tumour.
A Recognised Tertiary Centre is defined as a unit capable of managing complex MBD with appropriate multidisciplinary capabilities. Referral to a tertiary centre should be undertaken if a patient presents with a solitary bone metastatic.
BOOS guidelines advise that when considering potential endoprosthetic surgery, referral to a supra-regional or tertiary orthopaedic oncology centre should be considered. This is in part due to endoprostheses being principally being used in the management in primary bone tumours, where surgeons at these centres may be more experienced in their use. Regional centres can also carry our endoprosthesis surgery, if supported by local metastatic leads. BOOS guidelines also state that distal femoral, proximal tibial metaphyseal or periarticular lesions should be discussed with a local tumour centre. More specifically, complex acetabular defects (type IV on Harrington classification), often require dedicated orthopaedic oncology surgeon's input.
8. Prognosis
Ratasvuori et al developed a prognostic scoring system to evaluate patients who had undergone surgery as part of their management of MBD[56]. Data was collected from the Scandinavian Skeletal Metastasis Registry for patients with skeletal metastases in their extremities. They considered various factors that could shorten lifespan post-op. In their 2013 paper, they analysed over 1100 patients. They found that overall, 1-year survival was 36%, but this was dependant on primary tumour type and presence of visceral metastases. The data used was over a ten-year period, from 1999-2009. Below is their prognostic scoring system and estimated survival time, for patients undergoing surgery with MBD.
Table 3.
prognostic scoring for patients with MBD undergoing surgery with estimated survival[56].Table 4. Katagiri scoring for significant prognostic factors in patient with MBD[57].
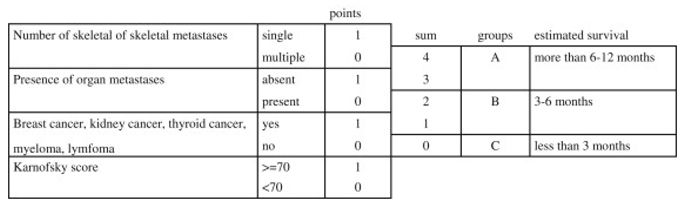
Patients are splint into groups A, B and C – statistical analysis found that patients in group A survived quite reliably over 6 months and at 1 year had an associated survival rate of over 2/3rd's. Patients in Group B were likely to survive over 3 months with half of these patients surviving over 6 months. Group C had the worse prognosis, a less than 3 months survival in 75% of cases. Ratasvuori et al, as part of the Scandinavian sarcoma group only analysed data for patients who had undergone operative management; their prognostic scoring system did not take into consideration patients who were for non-operative management. Regarding an overall view of prognosis, for patients presenting with MBD, Katagiri et al developed a different prognostic scoring system(see Table 4).
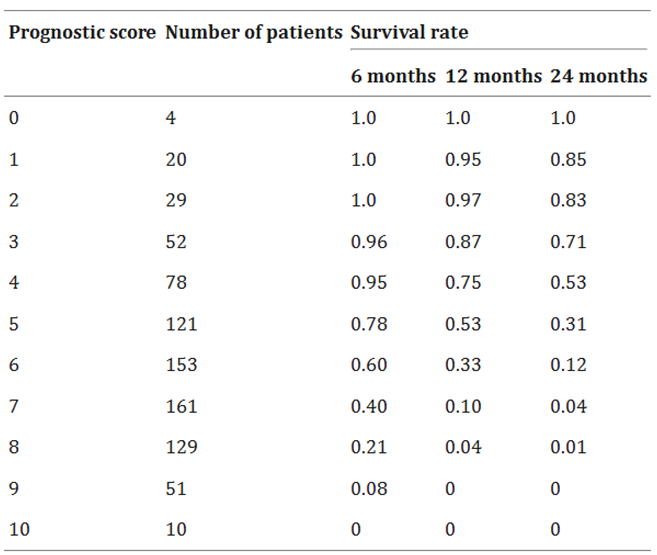
Katagiri et al’s modified scoring system aimed to quantify survival for patients diagnosed with symptomatic MBD. Prospectively analysing over 800 patients between 2005-2008, they identified prognostic factors and were able to quantify survival rates for patient regardless of their treatments/operative management[58]. The primary lesion, visceral/cerebral metastases and abnormal lab values were the 3 factors that had the largest impact on survival compared to the others, poor performance status, previous chemotherapy and multiple skeletal metastases. With a prognostic score of ≥7, the survival rate was 27% at 6 months, and only 6% at 1 year. In contrast, patients with a prognostic score of ≤3 had a survival rate of 91% at 1 year, and 78% at 2 years. See below prognostic scores and survival rate table. Estimated survival for each prognostic score is detailed in Table 5.
The British Orthopaedic Oncology Management (BOOM) audit was an Audit of 84 centres over a 3-month study period in 2021 across the UK[12]. A total of 846 patients with pelvic and appendicular MBD were analysed; those with spinal only metastatic disease were excluded. This audit found that the commonest locations of lesion were femur, pelvis and humerus, in-keeping with current literature. 13% of patients had multiple lesions at presentation. The commonest primary source was prostate, followed by breast and lung. Myeloma and renal cell carcinoma were 4th and 5th commonest respectively, again in-keeping with literature review. The audit also found that 39% of centres did not have an identifiable MBD lead. This is recommended in the key points – infrastructure – in BOOS guidelines 2015[9]. With regards to imaging, plain radiographs of the entire affected bone, and a CT CAP within 3 months of presentation are requirements, 81% and 71% of patients respectively had this investigation performed. 81% of patents underwent FBC, U+E, LFT and bone profile. 68% had CRP requested and 15% had ESR requested. 54 patients were operated on with a solitary lesion without discussion/referral with a MBD referral centre, again not in-keeping with BOOS guidance. The Audit also found that only 72% of patients operated on underwent surgical follow-up. In this cohort, 38% underwent surgery, with 80% of these fixations relating to the femur. They were treated with a combination of IM nailing, Hemiarthroplasty, Endoprosthesis and THA[12]. It is worth noting that patients treated in MBD centres are most likely to receive an endoprosthetic arthroplasty.
Another multicenter study of management of MBD took place in 2018. This study found that use of endoprostheses are increasing in trauma units, but IM Nailing is still the commonest method of surgical fixation of femoral MBD – either pathological fracture or high-risk lesions for pathological fracture[60].
9. Potential Future Treatment Options
There are a variety of treatments than in the future, could change the morbidity and mortality following a diagnosis of MBD. In lab models, an experimental cancer drug was found to eliminate bone metastasis due to breast cancer. The experimental drug, called RK-33, is an inhibitor of the DDx3 gene[61], a gene that has greatest expression in metastatic biopsy samples[6], creating the potential for the drug to be most potent in treating metastatic disease, the most difficult aspect of cancer to treat. A study led by Johns Hopkins medicine, published in 2024, demonstrated that RK-33 eliminated all evidence of MBD, while also preventing cancerous cells from spreading to other organ systems[63]. The researchers state this finding is bringing them closer to clinical trials.
MR-guided focused Ultrasound (MRgFUS) is a treatment aimed as a therapeutic option to relieve pain in patients with MBD. The guided high frequency sound waves are focused onto a small area, which generates heat and tissue damage, destroying cancerous cells and providing symptoms relief[64]. A meta-analysis of RCT and non-RCT for patients undergoing MRgFUS, concluded that it was a reliable therapeutic option to relieve cancer pain/symptoms in patients with MBD, as demonstrated by lowering of reported pain scores.[65]
Author Contributions
Conceptualization, JH, AA and PW; writing—original draft preparation, JH.; writing—review and editing, JH, AA and PW; visualization, JH and PW; supervision, AA and PW.; project administration, PW; All authors have read and agreed to the published version of the manuscript.
Funding
This article received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Jayarangaiah A, Theetha Kariyanna P. Bone Metastasis [Internet]. PubMed. Treasure Island (FL): StatPearls Publishing; 2020. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507911/.
- Chansky, HA. Metastatic Bone Disease: Practice Essentials, Pathophysiology and Etiology, Epidemiology [Internet]. Medscape.com. Medscape; 2024 [cited 2025 Mar 23]. Available from: https://emedicine.medscape.com/article/1253331-overview#a7?form=fpf.
- Storm HH, Kejs AMT, Engholm G, Tryggvadóttir L, Klint A, Bray F, et al. Trends in the overall survival of cancer patients diagnosed 1964-2003 in the Nordic countries followed up to the end of 2006: the importance of case-mix. Acta oncologica (Stockholm, Sweden) [Internet] 2010, 49, 713–724. [Google Scholar] [CrossRef] [PubMed]
- Rogers DL, Raad M, Rivera JA, Wedin R, Laitinen M, Sørensen MS, et al. Life Expectancy After Treatment of Metastatic Bone Disease: An International Trend Analysis. The Journal of the American Academy of Orthopaedic Surgeons [Internet] 2024, 32, e293–301. [Google Scholar]
- BOA. Management of Metastatic Bone Disease (MBD) [Internet]. BOA/BOOS; 2022 [cited 2025 Mar 23]. Available from: file:///C:/Users/7952080/AppData/Local/Temp/MicrosoftEdgeDownloads/00a0ed89-45d2-480a-a0a6-8b627fba7182/BOAST-Metastatic-Bone-Disease.pdf.
- About secondary bone cancer | Secondary cancer | Cancer Research UK [Internet]. Cancerresearchuk.org. 2017. Available from: https://www.cancerresearchuk.
- Zhang J, Cai D, Hong S. Prevalence and prognosis of bone metastases in common solid cancers at initial diagnosis: a population-based study. BMJ Open [Internet] 2023, 13, e069908. [Google Scholar] [CrossRef]
- Ryan C, Stoltzfus KC, Horn S, Chen H, Louie AV, Lehrer EJ, et al. Epidemiology of bone metastases. Bone 2020, 115783. [Google Scholar]
- BOOS & BOA. Metastatic Bone Disease: A Guide to Good Practice [Internet]. Tillman, Ashford, editors. BOOS/BOA; 2015 [cited 2025 Mar 23]. Available from: https://baso.org.uk/media/61543/boos_mbd_2016_boa.pdf.
- So A, Chin J, Fleshner N, Saad F. Management of skeletal-related events in patients with advanced prostate cancer and bone metastases: Incorporating new agents into clinical practice. Canadian Urological Association Journal [Internet] 2012, 6, 465–470. [Google Scholar] [CrossRef]
- Ibrahim A, Scher N, Williams G, Sridhara R, Li N, Chen G, et al. Approval Summary for Zoledronic Acid for Treatment of Multiple Myeloma and Cancer Bone Metastases. Clinical Cancer Research [Internet] 2003, 9, 2394–2399. [Google Scholar]
- Archer JE, Chauhan GS, Dewan V, Osman K, Thomson C, Nandra RS, et al. The British Orthopaedic Oncology Management (BOOM) audit. The bone & joint journal 2023, 105, 1115–1122. [Google Scholar]
- CKS is only available in the UK [Internet]. NICE. Available from: https://cks.nice.org.uk/topics/hypercalcaemia/background-information/causes/.
- Gaillard, F. Bone metastases | Radiology Reference Article | Radiopaedia.org [Internet]. Radiopaedia. Available from: https://radiopaedia.org/articles/bone-metastases-1?
- Macedo F, Ladeira K, Pinho F, Saraiva N, Bonito N, Pinto L, et al. Bone metastases: an Overview. Oncology Reviews [Internet] 2017, 11. [Google Scholar]
- Jayarangaiah A, Theetha Kariyanna P. Bone Metastasis [Internet]. PubMed. Treasure Island (FL): StatPearls Publishing; 2020. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507911/.
- Douglas Phillips C, Pope TL, Jones JE, Keats TE, Hunt MacMillan R. Nontraumatic avulsion of the lesser trochanter: a pathognomonic sign of metastatic disease? Skeletal Radiology 1988, 17, 106–110. [Google Scholar] [CrossRef]
- J. -L. Rouvillain, R. Jawahdou, Blanco OL, A. Benchikh-el-Fegoun, E. Enkaoua, Uzel M. Isolated lesser trochanter fracture in adults: An early indicator of tumor infiltration. Orthopaedics & Traumatology Surgery & Research 2011, 97, 217–220. [Google Scholar]
- Bell, DJ. Mirels classification (pathological fracture risk) [Internet]. Radiopaedia. Radiopaedia.org; 2024. Available from: https://radiopaedia.org/articles/mirels-classification-pathological-fracture-risk-1?lang=gb.
- Mirels, H. The Classic: Metastatic Disease in Long Bones A Proposed Scoring System for Diagnosing Impending Pathologic Fractures. Clinical Orthopaedics and Related Research 2003, 415, S4–S13. [Google Scholar] [CrossRef] [PubMed]
- Mosher ZA, Patel H, Ewing MA, Niemeier TE, Hess MC, Wilkinson EB, et al. Early Clinical and Economic Outcomes of Prophylactic and Acute Pathologic Fracture Treatment. Journal of Oncology Practice 2019, 15, e132–40. [Google Scholar] [CrossRef] [PubMed]
- Behnke N, Baker D. Prophylactic Fixation Of Impending Pathologic Fractures: In-Hospital Cost And Complication Analysis As Compared To Acute Fracture Fixation [Internet]. [cited 2025 Mar 23]. Available from: https://www.isols-msts.org/abstracts/files/abstracts-podium/isols-msts-abstract-140.pdf.
- Impending Fracture & Prophylactic Fixation - Pathology - Orthobullets [Internet]. www.orthobullets.com. Available from: https://www.orthobullets. 8002.
- Mirel’s classification to predict possible pathological fracture if boney metastasis [Internet]. Gpnotebook.com. 2018 [cited 2025 Mar 23]. Available from: https://gpnotebook.com/en-GB/pages/oncology/mirels-classification-to-predict-possible-pathological-fracture-if-boney-metastasis.
- Jawad MU, Scully SP. In Brief: Classifications in Brief. Clinical Orthopaedics & Related Research 2010, 468, 2825–2827. [Google Scholar]
- Harrington, KD. Impending pathologic fractures from metastatic malignancy: evaluation and management. Instructional course lectures [Internet] 1986, 35, 357–381. [Google Scholar]
- Knipe H, Bell D, Worsley C. Harrington criteria (pathological fracture risk). Radiopaediaorg [Internet]. 2015 Nov 1 [cited 2025 Mar 23]; Available from: https://radiopaedia.org/articles/harrington-criteria-pathological-fracture-risk-1.
- Rizzo SE, Kenan S. Pathologic Fractures [Internet]. www.ncbi.nlm.nih.gov. StatPearls Publishing; 2020. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559077/.
- Harvie P, Whitwell D. Metastatic bone disease. Bone & Joint Research 2013, 2, 96–101. [Google Scholar]
- O’Donnell, P. Metastatic Disease of Extremity - Pathology - Orthobullets [Internet]. Orthobullets.com. 2019. Available from: https://www.orthobullets.com/pathology/8045/metastatic-disease-of-extremity.
- Selvaggi G, Scagliotti GV. Management of bone metastases in cancer: a review. Critical Reviews in Oncology/Hematology [Internet] 2005, 56, 365–378. [Google Scholar] [CrossRef]
- Jones, J. Pathological fracture | Radiology Reference Article | Radiopaedia.org [Internet]. Radiopaedia. Available from: https://radiopaedia.org/articles/pathological-fracture?
- Marshall RA, Mandell JC, Weaver MJ, Ferrone M, Sodickson A, Khurana B. Imaging Features and Management of Stress, Atypical, and Pathologic Fractures. RadioGraphics 2018, 38, 2173–2192. [Google Scholar] [CrossRef]
- Tsukamoto S, Kido A, Tanaka Y, Facchini G, Peta G, Rossi G, et al. Current Overview of Treatment for Metastatic Bone Disease. Current Oncology 2021, 28, 3347–3372. [Google Scholar] [CrossRef]
- De Felice F, Piccioli A, Musio D, Tombolini V. The role of radiation therapy in bone metastases management. Oncotarget [Internet] 2017, 8. [Google Scholar]
- Saarto T, Janes R, Tenhunen M, Kouri M. Palliative radiotherapy in the treatment of skeletal metastases. European Journal of Pain 2002, 6, 323–330. [Google Scholar] [CrossRef]
- Haber, Z. Transarterial Embolization of Bone Metastases. Techniques in Vascular and Interventional Radiology 2023, 26, 100883. [Google Scholar] [CrossRef]
- Ma J, Tullius T, Van Ha TG. Update on Preoperative Embolization of Bone Metastases. Seminars in Interventional Radiology 2019, 36, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Geraets SEW, Bos PK, van der Stok J. Preoperative embolization in surgical treatment of long bone metastasis: a systematic literature review. EFORT Open Reviews 2020, 5, 17–25. [Google Scholar] [CrossRef]
- Acuña AJ, Vijayakumar G, Buac NP, Colman MW, Gitelis S, Blank AT. The effect of timing between preoperative embolization and surgery: A retrospective analysis of hypervascular bone metastases. Journal of Surgical Oncology 2023, 129, 416–423. [Google Scholar]
- Sun S, Lang EV. Bone Metastases from Renal Cell Carcinoma: Preoperative Embolization. Journal of Vascular and Interventional Radiology 1998, 9, 263–269. [Google Scholar] [CrossRef]
- Drake MT, Clarke BL, Khosla S. Bisphosphonates: Mechanism of Action and Role in Clinical Practice. Mayo Clinic Proceedings 2008, 83, 1032–1045. [Google Scholar] [CrossRef] [PubMed]
- Gralow J, Tripathy D. Managing Metastatic Bone Pain: The Role of Bisphosphonates. Journal of Pain and Symptom Management 2007, 33, 462–472. [Google Scholar] [CrossRef] [PubMed]
- CKS is only available in the UK [Internet]. NICE. Available from: https://cks.nice.org.uk/topics/hypercalcaemia/management/unconfirmed-cause/.
- CKS is only available in the UK [Internet]. NICE. Available from: https://cks.nice.org.
- Dental Management of Patients Prescribed Bisphosphonates -Clinical Guidance (Produced in conjunction with the Dental LPN for Shropshire and Staffordshire) [Internet]. 2015. Available from: https://www.england.nhs.uk/mids-east/wp-content/uploads/sites/7/2015/03/bisphosphonates-guidelines-2015.
- BNF is only available in the UK [Internet]. NICE. Available from: https://bnf.nice.org.uk/drugs/denosumab/#indications-and-dose.
- NICE. Denosumab for the prevention of skeletal[1]related events in adults with bone metastases from solid tumours [Internet]. National Institute for Health and Clinical Excellence. National Institute for Health and Clinical Excellence; 2012 [cited 2025 Mar 20]. Available from: https://www.nice.org.
- Overview | Denosumab for the prevention of skeletal-related events in adults with bone metastases from solid tumours | Guidance | NICE [Internet]. www.nice.org.uk. Available from: https://www.nice.org.uk/guidance/ta265.
- NICE. Risk assessment foR Venous thRomboembolism (Vte) [Internet]. 2010. Available from: https://www.nice.org.uk/guidance/ng89/resources/department-of-health-vte-risk-assessment-tool-pdf-4787149213.
- CKS is only available in the UK [Internet]. NICE. Available from: https://cks.nice.org.
- Kulkarni A, Grimer R, Carter S, Tillman R, Abudu A. How bad is a whoops procedure? – answers from a case matched series. Orthop Procs. 2005, 87, 3. [Google Scholar]
- National Cancer Institute. Tumor Markers [Internet]. National Cancer Institute. 2019. Available from: https://www.cancer.
- Motoo Y, Watanabe H, Sawabu N. [Sensitivity and specificity of tumor markers in cancer diagnosis]. Nihon Rinsho Japanese Journal of Clinical Medicine [Internet] 1996, 54, 1587–1591. [Google Scholar]
- National Cancer Institute. Tumor Markers in Common Use - National Cancer Institute [Internet]. www.cancer.gov. 2019. Available from: https://www.cancer.
- Ratasvuori M, Wedin R, Keller J, Nottrott M, Zaikova O, Bergh P, et al. Insight opinion to surgically treated metastatic bone disease: Scandinavian Sarcoma Group Skeletal Metastasis Registry report of 1195 operated skeletal metastasis. Surgical Oncology. 2013, 22, 132–138. [Google Scholar] [CrossRef]
- Table - PMC [Internet]. Cancer Med. 2014 Jul 10;3(5):1359–1367. Nih.gov. 2025 [cited 2025 Mar 23]. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC4302686/table/tbl4/. [CrossRef]
- Katagiri H, Okada R, Takagi T, Takahashi M, Murata H, Harada H, et al. New prognostic factors and scoring system for patients with skeletal metastasis. 2014, 3, 1359–1367.
- Table – PMC. Cancer Med. 2014 Jul 10;3(5):1359–1367. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC4302686/table/tbl5/. [CrossRef]
- Rai, P. Current surgical management of metastatic pathological fractures of the femur: A multicentre snapshot audit [Internet]. Clinical Key. European Journal of Surgical Oncology, 2020-08-01, Volume 46, Issue 8, Pages 1491-1495; 2020. Available from: https://www.clinicalkey.com/#!/content/playContent/1-s2.0-S0748798320301281?returnurl=https:%2F%2Flinkinghub.elsevier.com%2Fretrieve%2Fpii%2FS0748798320301281%3Fshowall%3Dtrue&referrer=https:%2F%2Fpubmed.ncbi.nlm.nih.gov%2F.
- Winnard PT, Farhad Vesuna, Bol GM, Gabrielson KL, Chenevix-Trench G, Ter ND, et al. Targeting RNA Helicase DDX3X with a Small Molecule Inhibitor for Breast Cancer Bone Metastasis Treatment. Cancer Letters. 2024, 604, 217260. [Google Scholar] [CrossRef] [PubMed]
- RK-33 [Internet]. Hopkinsmedicine.org. 2018. Available from: https://www.hopkinsmedicine.org/news/articles/2018/05/rk-33.
- Experimental Cancer Drug Eliminates Bone Metastases Caused by Breast Cancer in Lab Models [Internet]. Hopkinsmedicine.org. 2024. Available from: https://www.hopkinsmedicine.org/news/newsroom/news-releases/2024/10/experimental-cancer-drug-eliminates-bone-metastases-caused-by-breast-cancer-in-lab-models.
- MR Guided Focused Ultrasound [Internet]. stanfordhealthcare.org. Available from: https://stanfordhealthcare.org/medical-treatments/m/mr-guided-focused-ultrasound.html.
- Han X, Huang R, Meng T, Yin H, Song D. The Roles of Magnetic Resonance-Guided Focused Ultrasound in Pain Relief in Patients With Bone Metastases: A Systemic Review and Meta-Analysis. Frontiers in oncology 2021, 11. [Google Scholar]
Figure 1.
BOAST Guidelines[5].
Figure 1.
BOAST Guidelines[5].
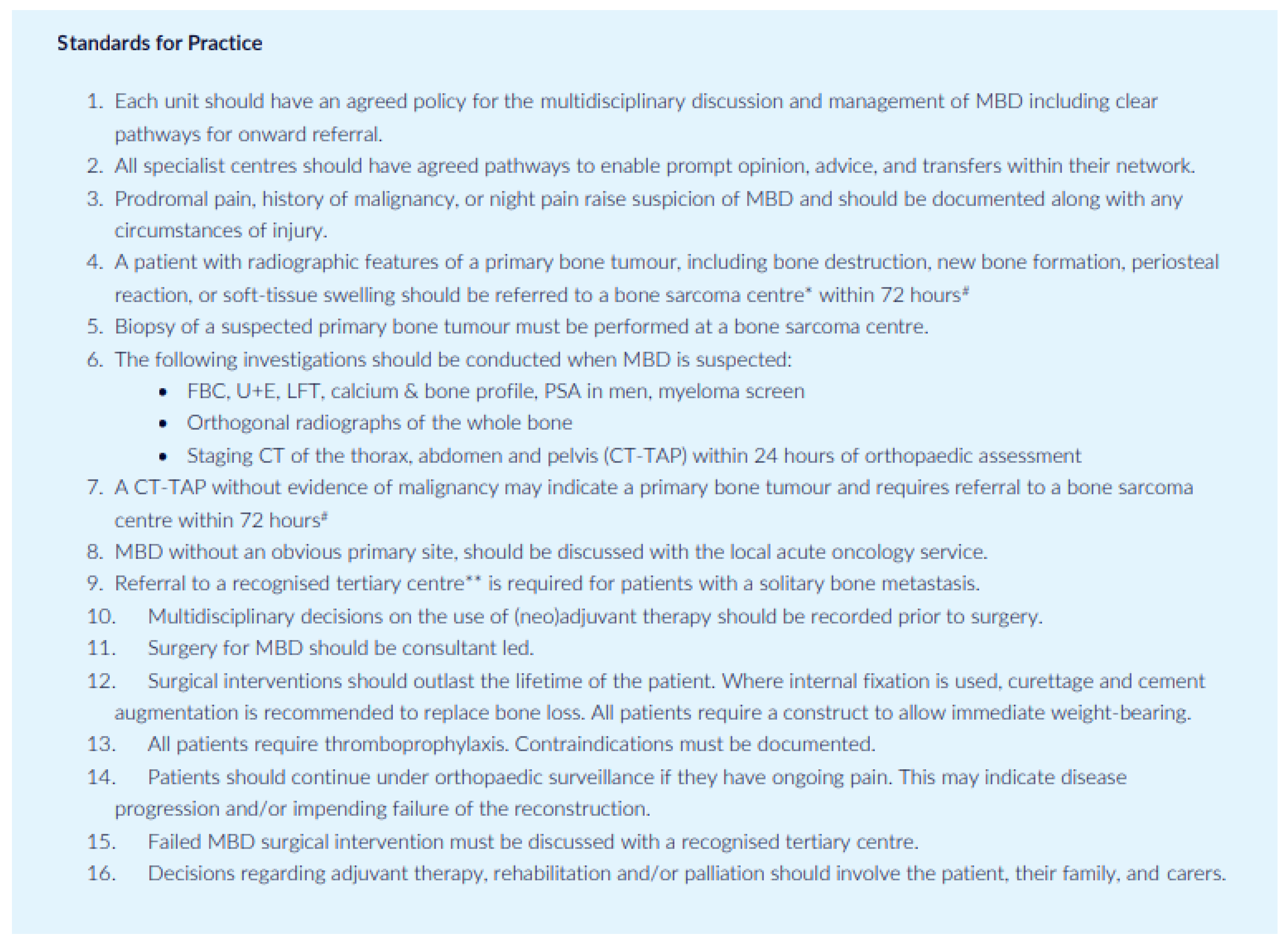
Table 2.
Tumour markers and associations with malignancy.
| Tumour Marker | Malignancy |
|---|---|
| Alpha-fetoprotein (AFP) | Liver cancer, ovarian cancer, and germ cell tumours |
| Beta-human chorionic gonadotropin (Beta-hCG) | Choriocarcinoma and germ cell tumours |
| CA19-9 | Pancreatic, gallbladder, bile duct, and gastric cancers |
| CA-125 | Ovarian cancer |
| Calcitonin | Medullary Thyroid Cancer |
| Carcinoembryonic antigen (CEA) | Colorectal cancer, breast and ovarian cancer |
| CD20 | Non-Hodgkin lymphoma |
| Oestrogen receptor (ER)/progesterone receptor (PR) | Breast cancer |
| 5-HIAA | Carcinoid tumors |
| Gastrin | Gastrin-producing tumour (gastrinoma) |
| Immunoglobulins | Multiple myeloma and Waldenström macroglobulinemia |
| Prostate-specific antigen (PSA) | Prostate cancer |
| Thyroglobulin | Thyroid cancer |
Table 4.
Katagiri scoring for significant prognostic factors in patient with MBD[57].
Table 4.
Katagiri scoring for significant prognostic factors in patient with MBD[57].
| Prognostic factor | Score | |
|---|---|---|
| Primary site | ||
| Slow growth | Hormone-dependent breast and prostate cancer, thyroid cancer, multiple myeloma, and malignant lymphoma | 0 |
| Moderate growth | Lung cancer treated with molecularly targeted drugs, hormone-independent breast and prostate cancer, renal cell carcinoma, endometrial and ovarian cancer, sarcoma, and others | 2 |
| Rapid growth | Lung cancer without molecularly targeted drugs, colorectal cancer, gastric cancer, pancreatic cancer, head and neck cancer, oesophageal cancer, other urological cancers, melanoma, hepatocellular carcinoma, gall bladder cancer, cervical cancer, and cancers of unknown origin | 3 |
| Visceral metastasis | Nodular visceral or cerebral metastasis | 1 |
| Disseminated metastasis (Pleural, peritoneal, or leptomeningeal dissemination.) | 2 | |
| Laboratory data | Abnormal (CRP ≥ 0.4 mg/dL, LDH ≥ 250 IU/L, or serum albumin <3.7 g/dL.) | 1 |
| Critical (platelet <100,000/μL, serum calcium ≥10.3 mg/dL, or total bilirubin ≥1.4) | 2 | |
| ECOG PS | 3 or 4 | 1 |
| Previous chemotherapy | Score if Yes | 1 |
| Multiple skeletal metastases | Score if Yes | 1 |
| Total | 10 |
Table 5.
Katagiri Prognostic score and survival rates at 6, 12 and 24 months - Katagiri et al 2014 [59].
Table 5.
Katagiri Prognostic score and survival rates at 6, 12 and 24 months - Katagiri et al 2014 [59].
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



