Submitted:
26 March 2025
Posted:
26 March 2025
You are already at the latest version
Abstract
Although cemented total knee arthroplasty (TKA) is considered the standard fixation technique, the emerging trend toward cementless fixation has created the need for a detailed comparison. In a previous study, we reported the 5-year results comparing cementless and hybrid cemented TKAs using the same implant design. The purpose of this study was to assess the long-term follow-up at a minimum of 10 years. Methods: A retrospective analysis was performed on 120 TKAs (60 cementless, 60 hybrid cemented) conducted between 2003 and 2007. Demographic and clinical data were collected, ra-diographic follow-up was performed with attention to signs of loosening, while compli-cations and revision surgery were assessed using competing risk analysis. Operative time was recorded as an indicator of surgical efficiency. Results: At 10 years, 59 TKAs (54 patients) were available for long‐term follow‐up. Both fixation groups demonstrated significant improvement in Knee Society Scores (KSS) compared to preoperative values (p < 0.001). However, there was no significant difference in KSS between the two groups at 10 years follow-up (p = 0.480). The 10-year cumulative incidence of revision was 8.4% in both groups (p = 0.721), and that of aseptic loosening was identical at 3.4% (p = 0.967). Although radiolucent lines were noted in three tibial components of the cementless group, the difference was not statistically significant (p = 0.075). Notably, the cementless group demonstrated a significantly shorter operative time with a mean difference of 10 minutes (p = 0.017). Conclusions: At a minimum follow-up of 10 years, there were no significant differences between the hybrid cemented and cementless groups in revision rates, cu-mulative incidences, clinical scores, or radiological signs of loosening, confirming the long-term effectiveness of both fixation methods in clinical practice.
Keywords:
arthroplasty
; total knee arthroplasty
; cementless fixation
; cemented fixation
; complications
; aseptic loosening
1. Introduction
Despite the excellent survival rates and clinical outcomes of TKA, there is an ongoing debate regarding the optimal fixation of components. As the number of TKAs performed annually increases and the patient population trends younger, the longevity of the prostheses without the need for revision becomes an increasingly important consideration [1,2,3]. This concern is particularly relevant, as the most common indication for revision surgery is aseptic loosening, which occurs at higher rates in younger patients [4].
Cementless TKAs have been developed as an alternative to cemented fixation. They offer a promising option due to their potential to preserve bone stock, avoid cement particles, reduce operation time, achieve long-term biological fixation, and ultimately improve long-term implant survival rates [5]. However, in the early stages of development, cementless TKA implants were associated with higher rates of implant failure due to poor implant design [6,7].
Design advancements, including bioactive materials and osteoconductive coatings, have overcome the early limitations of cementless implants, resulting in better survival rates and lower revision rates due to improved bone ingrowth [8]. For instance, Nam et al. [9] analyzed data from the American Joint Replacement Registry and found that 3-dimensional (3D) printed cementless tibial baseplates had superior survivorship and lower revision rates compared to both aggregate cementless and cemented tibial baseplates after 5 years. In a more recent study, Hannon et al. [10] reported in a prospective randomized controlled trial (RCT) a 6-year survivorship of 100% for both cementless and cemented TKAs of the same design. In addition, Van der Lelij et al. [11] conducted a RCT on cementless 3D-printed TKAs using radiostereometric analysis. The study showed no significant difference in mean migration at the five-year follow-up compared to the cemented implants.
Although cementless TKA implants have shown promising short-term performance and positive clinical outcomes, the current literature lacks comprehensive mid- to long-term follow-up data. Therefore, this study aims to address this gap. Previously, we reported the minimum 5-year results from this study population comparing cementless and hybrid cemented TKAs of the same design. At a mean follow up of 6 years, there were no significant differences in revisions, clinical scores, or radiological signs of loosening between cemented TKAs and hybrid cemented TKAs [12].
The main aim of this study was to provide long-term follow-up data from the previous case-controlled study and compare the implant survivorship, clinical outcomes, and radiographic findings of cementless and hybrid cemented TKA implants with identical designs. The main hypothesis was that cementless TKAs would have similar long-term outcomes compared to hybrid cemented TKAs at a minimum follow-up of 10 years postoperatively.
2. Materials and Methods
Following approval from the ethical committees of the Medical University of Vienna and the General Hospital of Vienna, we retrospectively analyzed a consecutive series of 120 TKAs performed between July 2003 and January 2007 at the Department of Orthopaedics, Medical University of Vienna. As previously detailed in a case-control study [12], the cohort was divided equally into two groups: 60 cementless TKAs and 60 hybrid cemented TKAs. The selection of the fixation method was based on the operating surgeon’s established practice, thereby reflecting routine clinical decision-making. Inclusion criteria encompassed patients diagnosed with idiopathic arthritis, post-traumatic arthritis, or rheumatoid arthritis. Exclusion criteria were a history of revision surgery, prior joint infection, any primary or secondary cancer within the past 5 years, psychosocial disorders limiting rehabilitation, a valgus or varus deformity greater than 20°, or a flexion deficit exceeding 20°. The primary diagnosis was idiopathic arthritis (n = 106; 88.3%) followed by post-traumatic arthritis (n = 6; 5%), rheumatoid arthritis (n = 4; 3.3%), previous unicompartmental knee arthroplasty (n = 3; 2.5%), and avascular necrosis (n = 1; 0.8%). The mean age at surgery was 66.93 years (range: 33–90), with a total of 81 female and 39 male patients. Notably, the hybrid cemented group had a significantly higher proportion of female patients compared to the cementless group (76.67% vs. 58.33%, p = 0.032). The mean body mass index (BMI) was 30.28 kg/m, ranging from 19 to 51. The mean operative time was significantly shorter in the cementless group (125.7 minutes; range: 80–175) compared to the hybrid cemented group (135.7 minutes; range: 95–200) (p = 0.017). Apart from the differences in operative time and gender distribution, no other significant demographic or clinical differences were observed between the two cohorts (Table 1).
2.1. Surgical Procedure
All operations were performed by a team of experienced orthopedic surgeons in our department, following a standardized protocol to ensure consistency. A standard medial parapatellar approach was utilized in every case, with the OrthoPilot navigation system ensuring neutral mechanical alignment; no kinematic alignment techniques were employed, and alignment goals remained identical across groups. Following prophylactic antibiotic administration, a tourniquet was applied for a maximum of 120 minutes to optimize surgical conditions. All 120 TKAs were performed with the e.motion posterior cruciate-retaining knee prosthesis with a floating-platform mobile polyethylene bearing (Aesculap, Tuttlingen, Germany). 60 TKAs were performed uncemented using the e.motion prosthesis with a 350-μm titanium plasma-sprayed coating and an additional dicalcium phosphate dihydrate (μ-CaP) surface layer. The remaining 60 TKAs underwent a hybrid fixation technique, which involved a cemented tibial component and a cementless femoral component. In all cases, the patella was resurfaced with a cemented polyethylene component. Palacos R cement (Heraeus Medical GmbH, Wehrheim, Germany) was used for all patients. The implant design was the same for all patients, except for the surface of the uncemented tibial tray, as previously mentioned. Postoperative care included early mobilisation on crutches and partial weight-bearing with approximately 50% of body weight on the operated leg for a period of six weeks [12].
2.2. Study Parameters
Preoperative characterization of the study population included collecting patient-specific parameters including primary diagnosis, age, gender, weight, height, BMI, date of surgery, and the operated side (Table 1). Postoperative clinical and radiographic assessment followed the department’s standardized postoperative assessment protocol, which includes assessments at 6, 12, 24 weeks, 1 year, 2 years, and every 5 years thereafter. Patients who did not attend follow-up were contacted by telephone to gather patient-reported outcomes. Deceased patients were identified using the hospital's internal information software and a death registry inquiry. For clinical and functional evaluation, the KSS was measured at each follow-up. Revision surgery data, such as the timing and reason for revision, were extracted from surgical reports, discharge summaries, or follow-up examinations. Radiographs taken at each follow-up were analyzed for radiolucent lines or any alterations in the position of the implant. Radiolucent lines were evaluated based on their location, width (measured in millimeters), and progression, according to the guidelines established by the Knee Society. [13,14] The system assigns numerical scores for the prosthetic interface in different zones. The total score for each component was then calculated by adding up the widths of the radiolucent lines in all designated zones and rated as follows: Scores of 4 or less were considered non-progressive and typically insignificant. Scores between 5 and 9 indicated the need for careful monitoring for any increase. Scores of 10 or above indicated a potential or imminent failure of the component. All analyses were performed by a non-surgeon investigator.
2.3. Study Parameters
Descriptive data analysis was performed by calculating means, standard deviations (SDs), medians, ranges, and ratios based on the distribution of the measurements. In addition, the KSSs and results from the 'Knee Society endorsed roentgenographic knee evaluation system' were systematically analyzed at each follow-up visit. Age and BMI at baseline and pre- and post-operative scores were compared using two-tailed independent t-tests. The Kolmogorov-Smirnov test confirmed a normal distribution. Pearson's Chi-Square analysis was used for categorical data, such as gender or operative side. A competing risk analysis was conducted to determine the risk of revision. Cumulative incidence rates were calculated and visualized as cumulative incidence functions, with death treated as the competing event of interest. To evaluate differences between the two groups, Gray’s test was used [15]. All statistical tests were two-tailed, and a p-value of ≤ 0.05 was considered significant. All statistical calculations were performed using IBM SPSS Statistics version 29.0 and XLSTAT version 2023.3.1.
3. Results
3.1. Evaluable Cases
From the initial cohort of 120 TKAs (111 patients), 46 patients (49 TKAs, 40.8%) died from causes unrelated to the index procedure before the 10-year follow-up. An additional five patients (5 TKAs, 4.16%) were unable to be reviewed and therefore classified as 'lost to follow-up'. Notably, no complications or revisions were reported at their last assessment. Consequently, complete follow-up data were available for 54 patients, accounting for 59 TKAs. Among these, 30 TKAs (50.8%) were hybrid cemented and 29 (49.2%) were cementless, with a mean follow-up period of 15.34 years (range, 10 to 20) (Figure 1).
3.2. Revisions
In the entire cohort, a total of 20 complications required revision surgery, including 11 revisions in the hybrid cemented group and 9 in the cementless group. Polyethylene failure was the predominant cause of revision, with 4 cases in the hybrid cemented group and 3 in the cementless group, presenting median revision times of 186 months (IQR: 167–190) and 152 months (IQR: 151–161), respectively. Aseptic loosening was the second most common cause, resulting in 3 revisions in each group, with a median time to revision of 25 months (IQR: 14-57) for the hybrid cemented group and 10.5 months (IQR: 3-60) for the cementless group. In the hybrid cemented group, one case involved combined tibial and femoral component loosening at 122 months, whereas the other two cases were isolated tibial failures at 14 and 36 months, respectively. In the cementless group, one tibial component loosening occurred late at 188 months, another early revision at 3 months was attributed to a confirmed postoperative nickel allergy, and a third patient with a high BMI (35 kg/m²) required revision at 18 months postoperatively. Limited mobility accounted for 4 revisions: 1 in the hybrid cemented group and 3 in the cementless group with a median time to revision of 23 months (IQR: 23-23) for the hybrid cemented group and 5.5 months (IQR: 4-10) for the cementless group. Additionally, infection led to 3 revisions in the hybrid cemented group, with a median time to revision of 46 months (IQR: 11–94). Gray’s test indicated that there was no statistically significant difference in the revision rates between the two groups for any endpoint (Table 2).
3.3. Cumulative Incidence and Competing Risk Analysis
Competing risk analysis revealed that the overall 10-year cumulative incidence of revision was 8.4% for both groups, increasing to 13.5% for the hybrid cemented group and 12.0% for the cementless group at 15 years. At the final follow-up, the cumulative incidences were 21.5% for the hybrid cemented group (at 19.6 years) and 16.3% for the cementless group (at 20 years). Gray’s test confirmed no significant difference in overall cumulative revision incidence between the two fixation methods (p = 0.721) (Figure 2). For the endpoint aseptic loosening, both groups demonstrated an identical 10-year cumulative incidence of 3.4%. At final follow-up, the hybrid cemented group exhibited a cumulative incidence of 5.1% (at 19.6 years), compared to 5.5% for the cementless group (at 20 years), with no significant difference observed between the groups (p = 0.967) (Figure 3).
3.4. Clinical Outcomes
At a minimum of 10 years postoperatively, clinical and functional outcomes were evaluated in 42 patients (46 TKAs), after excluding 13 TKAs (10 revisions and 3 for health reasons). Of the evaluated cases, 22 TKAs (47.8%) were hybrid cemented and 24 TKAs (52.2%) were cementless implants. Specifically, the cementless group’s mean total KSS increased from 96.52 preoperatively to 168.63 at 10 years, while the hybrid cemented group improved from 91.52 to 168.18. Although a significant difference was noted in the preoperative clinical KSS (54.10 for cementless vs. 45.40 for hybrid cemented; p = 0.011), no significant differences were observed between the groups in clinical, functional, or total KSS at the 10-year follow-up (p = 0.736, p = 0.948, and p = 0.480, respectively) (Table 3).
3.5. Radiological Outcomes
In the radiological evaluation, no evidence of osteolysis was detected in either group. Radiolucent lines between 1-2 mm were found in 3 TKAs of 2 patients in the cementless group, but none in the hybrid cemented group. However, there was no significant difference (p = 0.075) in the incidence of loosening between the two techniques at a minimum follow-up of 10 years (Figure 4).
4. Discussion
The optimal fixation method in TKA cementless versus cemented remains a subject of ongoing debate. With the increasing adoption of cementless TKAs, it is essential to comprehensively evaluate their long-term performance to inform future surgical decision-making [16]. Historically, cemented TKAs have demonstrated superior implant survivorship compared to cementless alternatives; however, recent advancements in implant design have aimed to close this gap [5].
The main finding of this study was that cementless and hybrid cemented TKAs with the same implant design exhibited comparable long-term clinical, radiographic, and revision outcomes at a minimum follow-up of 10 years. The nearly identical cumulative incidence rates of revision and aseptic loosening observed between the two fixation methods suggest that modern design improvements such as bioactive coatings and enhanced geometries have effectively addressed the historical concerns regarding cementless fixation. These results align with recent literature documenting similar survival and functional outcomes between cementless and cemented (or hybrid) TKA systems [17]. For instance, Zhou et al. [18] reported no significant difference in survival in a meta-analysis of 812 TKAs, while Kim et al. [19] observed similar survivorship in bilateral TKAs with a mean follow-up of 16.6 years. Furthermore, research by Kim et al. [20] demonstrated survival rates of 97% for cementless and 98% for cemented implants over 23.8 years. More recently, Gibon et al. [21] found that both cementless and hybrid monoblock tibial components achieved 96% implant survivorship at 10 years, exceeding the 89% survivorship observed in the traditional cemented tibial components.
However, an increased revision rate was observed in both groups toward the end of the follow-up period. This increase is likely attributable to the 'floating platform' design, which has been linked to a higher incidence of inlay fractures and served as the primary cause of prosthesis failure in our cohort [22]. This finding contrasts with current literature, which often cites aseptic loosening followed by infection as predominant reasons for revision [23].
Another noteworthy finding was the significantly shorter operative time in the cementless group (p = 0.017), which may reduce intraoperative complications and potentially lower the risk of periprosthetic joint infections. This trend is further supported by the absence of infection-related revisions in the cementless group, although the difference did not reach statistical significance (p = 0.087).
Furthermore, both cementless and hybrid cemented TKAs achieved substantial improvement in clinical outcomes, as reflected by the significant increase in KSSs in both groups from baseline. Importantly, no significant differences in clinical scores were observed between the two groups at the 10-year follow-up (p = 0.480), indicating that cementless fixation does not compromise functional outcomes. These findings are consistent with previous research, including a systematic review and meta-analysis by Anoop K et al. [24], which reported no significant differences in functional scores between cemented and cementless TKAs (p > 0.05)
Radiological outcomes further support the equivalence of these fixation methods. Radiolucent lines were observed in three tibial components in the cementless group, whereas none were found in the hybrid cemented group. These radiolucencies were non-progressive, did not correlate with implant failure or clinical symptoms, and the difference between groups was not statistically significant (p = 0.075). As reported by Costales et al. [25], radiolucent lines are a common occurrence after cementless TKA.
4.1. Limitations
This study has several limitations. It was retrospective, which may have introduced sample bias due to loss to follow-up. The relatively modest sample size may limit the statistical power to detect differences in rare outcomes. The study compared cementless TKAs with hybrid cemented TKAs. However, recent studies indicate that there is no significant difference in survival, clinical scores, or radiological outcomes between cemented and cementless femoral components [26]. Furthermore, the study used TKAs with a unique rotating platform known as the 'floating platform', which was associated with a higher rate of inlay fractures in later studies and was subsequently withdrawn by the manufacturer due to this issue [22]. However, the same TKAs were used in both groups, resulting in PE wear in both groups.
5. Conclusions
In summary, this study provides robust evidence that modern cementless and hybrid cemented TKA fixation methods offer comparable long-term clinical, radiological, and survival outcomes at a minimum 10-year follow-up. Although slight differences in revision rates and time to revision were observed, these differences did not reach statistical significance, indicating that both fixation methods are viable for achieving long-term stability and function. Further research should focus on specific patient demographics, implant design variations, and evolving surgical techniques to further define the optimal fixation strategy in TKA
Author Contributions
Conceptualization, L.R., K.V., R.W. and R.L.; methodology, L.R., K.V. and R.L.; software, L.R. and KV; validation, L.R. and K.V.; formal analysis, L.R. K.V. and R.L.; investigation, K.V., A.G. R.W. and R.L; resources, R.L. and R.W.; data curation, L.R.; writing—original draft preparation, L.R.; writing—review and editing, L.R., K.V. and R.L..; visualization, L.R.; supervision, R.L.; project administration, L.R..; funding acquisition, R.W. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Medical University of Vienna (protocol code 1264/2021; 04/2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
The original contributions presented in this study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author(s).
Acknowledgments
In this section, you can acknowledge any support given which is not covered by the author contribution or funding sections. This may include administrative and technical support, or donations in kind (e.g., materials used for experiments).
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| TKA | Total Knee Arthroplasty |
| KSS | Knee Society Score |
| BMI | Body Mass Index |
| IQR | Interquartile Range |
| KSS | Knee Society Score |
| PE | Polyethylene |
| PJI | Periprosthetic Joint Infection |
| RCT | Randomized Controlled Trial |
| SD | Standard Deviation |
References
- Shichman, I.; Roof, M.; Askew, N.; Nherera, L.; Rozell, J.C.; Seyler, T.M.; Schwarzkopf, R. Projections and Epidemiology of Primary Hip and Knee Arthroplasty in Medicare Patients to 2040-2060. JBJS Open Access 2023, 8. [Google Scholar] [CrossRef] [PubMed]
- Singh, J.A.; Yu, S.; Chen, L.; Cleveland, J.D. Rates of Total Joint Replacement in the United States: Future Projections to 2020–2040 Using the National Inpatient Sample. J. Rheumatol. 2019, 46, 1134–1140. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, S.M.; Lau, E.; Ong, K.; Zhao, K.; Kelly, M.; Bozic, K.J. Future Young Patient Demand for Primary and Revision Joint Replacement: National Projections from 2010 to 2030. Clin. Orthop. Relat. Res. 2009, 467, 2606–2612. [Google Scholar] [CrossRef] [PubMed]
- Julin, J.; Jämsen, E.; Puolakka, T.; Konttinen, Y.T.; Moilanen, T. Younger age increases the risk of early prosthesis failure following primary total knee replacement for osteoarthritis. A follow-up study of 32,019 total knee replacements in the Finnish Arthroplasty Register. Acta Orthop. 2010, 81, 413–419. [Google Scholar] [CrossRef]
- Polizzotti, G.; Lamberti, A.; Mancino, F.; Baldini, A. New Horizons of Cementless Total Knee Arthroplasty. J. Clin. Med. 2023, 13, 233. [Google Scholar] [CrossRef]
- Duffy, G.P.; Berry, D.J.; Rand, J.A. Cement Versus Cementless Fixation In Total Knee Arthroplasty. Clin. Orthop. Relat. Res. 1998, 356, 66–72. [Google Scholar] [CrossRef]
- Berger, R.A.; Lyon, J.H.; Jacobs, J.J.; Barden, R.M.; Berkson, E.M.; Sheinkop, M.B.; Rosenberg, A.G.; Galante, J.O. Problems With Cementless Total Knee Arthroplasty at 11 Years Followup. Clin. Orthop. Relat. Res. 2001, 392, 196–207. [Google Scholar] [CrossRef]
- Hu, B.; Chen, Y.; Zhu, H.; Wu, H.; Yan, S. Cementless Porous Tantalum Monoblock Tibia vs Cemented Modular Tibia in Primary Total Knee Arthroplasty: A Meta-Analysis. J. Arthroplast. 2016, 32, 666–674. [Google Scholar] [CrossRef]
- Nam, D.; Bhowmik-Stoker, M.; Mahoney, O.M.; Dunbar, M.J.; Barrack, R.L. Mid-Term Performance of the First Mass-Produced Three-Dimensional Printed Cementless Tibia in the United States as Reported in the American Joint Replacement Registry. J. Arthroplast. 2022, 38, 85–89. [Google Scholar] [CrossRef]
- Hannon, C.P.; Salih, R.; Barrack, R.L.; Nunley, R.M. Cementless Versus Cemented Total Knee Arthroplasty: Concise Midterm Results of a Prospective Randomized Controlled Trial. J. Bone Jt. Surg. 2023, 105, 1430–1434. [Google Scholar] [CrossRef]
- van der Lelij, T.J.; de Mheen, P.J.M.-V.; Kaptein, B.L.; Toksvig-Larsen, S.; Nelissen, R.G. Continued Stabilization of a Cementless 3D-Printed Total Knee Arthroplasty: Five-Year Results of a Randomized Controlled Trial Using Radiostereometric Analysis. J. Bone Jt. Surg. 2023, 105, 1686–1694. [Google Scholar] [CrossRef] [PubMed]
- Lass, R.; Kubista, B.; Holinka, J.; Pfeiffer, M.; Schuller, S.; Stenicka, S.; Windhager, R.; Giurea, A. Comparison of Cementless and Hybrid Cemented Total Knee Arthroplasty. Orthopedics 2013, 36. [Google Scholar] [CrossRef] [PubMed]
- Ewald, F.C. The Knee Society total knee arthroplasty roentgenographic evaluation and scoring system. Clin. Orthop. Relat. Res. 1989, 248, 9–12. [Google Scholar] [CrossRef]
- Kumar, N.; Yadav, C.; Raj, R.; Anand, S. How to Interpret Postoperative X-rays after Total Knee Arthroplasty. Orthop. Surg. 2014, 6, 179–186. [Google Scholar] [CrossRef]
- Kremers, H.M.; Devick, K.L.; Larson, D.R.; Lewallen, D.G.; Berry, D.J.; Crowson, C.S. Competing Risk Analysis: What Does It Mean and When Do We Need It in Orthopedics Research? J. Arthroplast. 2021, 36, 3362–3366. [Google Scholar] [CrossRef]
- Hegde, V.; Stambough, J.B.; Levine, B.R.; Springer, B.D. Highlights of the 2022 American Joint Replacement Registry Annual Report. Arthroplast. Today 2023, 21, 101137. [Google Scholar] [CrossRef]
- Asokan, A.; Plastow, R.; Kayani, B.; Radhakrishnan, G.T.; Magan, A.A.; Haddad, F.S. Cementless knee arthroplasty: a review of recent performance. Bone Jt. Open 2021, 2, 48–57. [Google Scholar] [CrossRef]
- Zhou, K.; Yu, H.; Li, J.; Wang, H.; Zhou, Z.; Pei, F. No difference in implant survivorship and clinical outcomes between full-cementless and full-cemented fixation in primary total knee arthroplasty: A systematic review and meta-analysis. Int. J. Surg. 2018, 53, 312–319. [Google Scholar] [CrossRef]
- Kim, Y.-H.; Park, J.-W.; Lim, H.-M.; Park, E.-S. Cementless and cemented total knee arthroplasty in patients younger than fifty five years. Which is better? Int. Orthop. 2014, 38, 297–303. [Google Scholar] [CrossRef]
- Kim, Y.-H.; Park, J.-W.; Jang, Y.-S. The 22 to 25-Year Survival of Cemented and Cementless Total Knee Arthroplasty in Young Patients. J. Arthroplast. 2021, 36, 566–572. [Google Scholar] [CrossRef]
- Gibon, E.; Lewallen, D.G.; Larson, D.R.; Stuart, M.J.; Pagnano, M.W.; Abdel, M.P. John N. Insall Award: Randomized Clinical Trial of Cementless Versus Cemented Tibial Components: Durable and Reliable at a Mean 10-Years Follow-Up. J. Arthroplast. 2023, 38, S14–S20. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.-R.; Yang, J.-H. Unsatisfactory clinical outcomes of second-generation mobile bearing floating platform total knee arthroplasty: comparing outcomes with fixed bearing after five years minimum. Int. Orthop. 2018, 42, 2583–2589. [Google Scholar] [CrossRef] [PubMed]
- Sharkey, P.F.; Lichstein, P.M.; Shen, C.; Tokarski, A.T.; Parvizi, J. Why Are Total Knee Arthroplasties Failing Today—Has Anything Changed After 10 Years? J. Arthroplast. 2014, 29, 1774–1778. [Google Scholar] [CrossRef] [PubMed]
- Prasad, A.K.; Tan, J.H.; Bedair, H.S.; Dawson-Bowling, S.; Hanna, S.A. Cemented vs. cementless fixation in primary total knee arthroplasty: a systematic review and meta-analysis. EFORT Open Rev. 2020, 5, 793–798. [Google Scholar] [CrossRef]
- Costales, T.G.; Chapman, D.M.; Dalury, D.F. The Natural History of Radiolucencies Following Uncemented Total Knee Arthroplasty at 9 Years. J. Arthroplast. 2020, 35, 127–131. [Google Scholar] [CrossRef]
- Iosifidis, M.; Iliopoulos, E.; Neofytou, D.; Sakorafas, N.; Andreou, D.; Alvanos, D.; Kyriakidis, A. The Rotaglide mobile-bearing total knee arthroplasty: no difference between cemented and hybrid implantation. Knee Surgery, Sports Traumatol. Arthrosc. 2014, 22, 1843–1848. [Google Scholar] [CrossRef]
Figure 1.
Flow diagram of patients in the study.
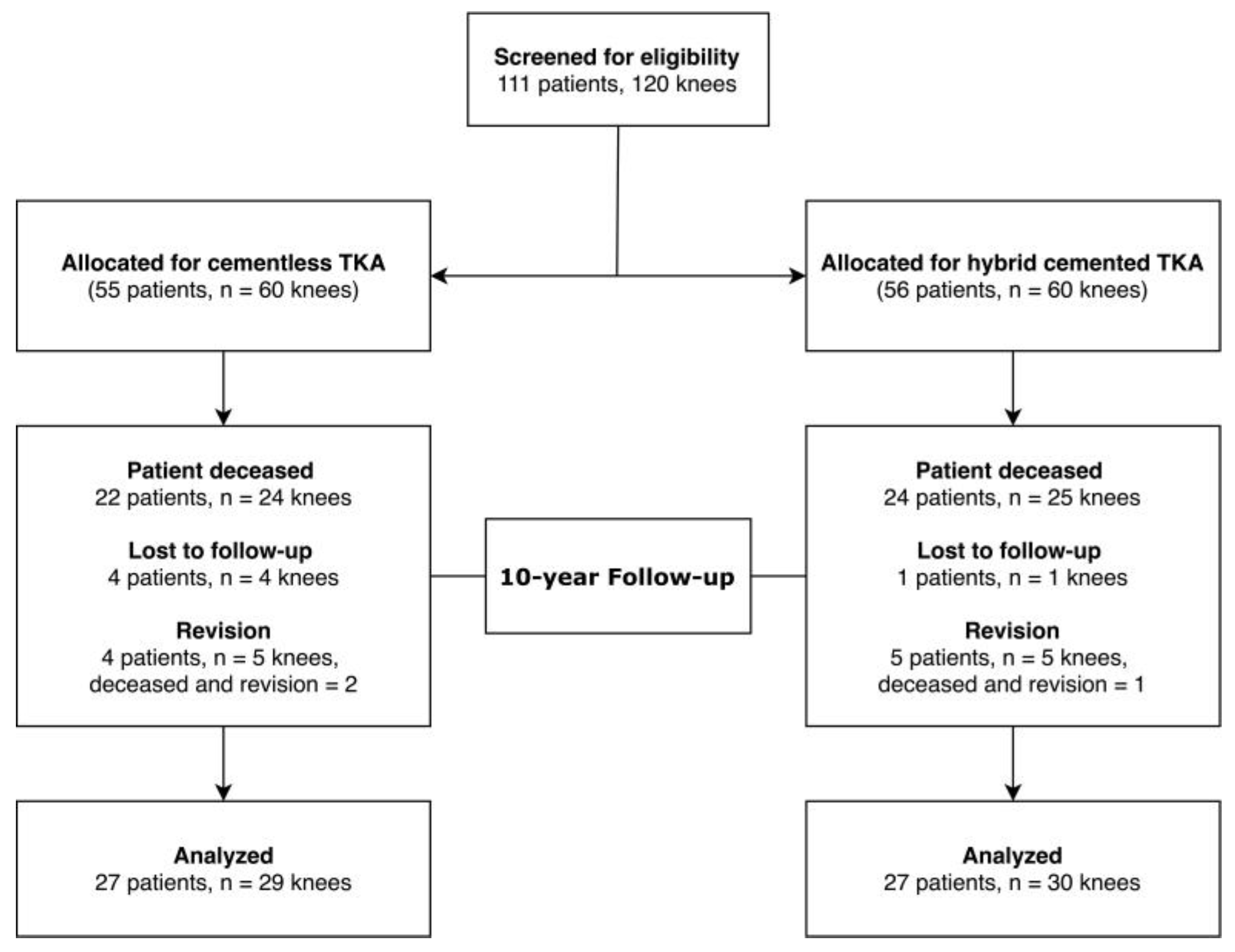
Figure 2.
Overall Cumulative incidence of revision. The hybrid cemented group showed an incidence of 6.7, 8.4, 13.5 and 21.5% after 5, 10, 15 years and at the end of follow-up (19.6 years). For the cementless group, the cumulative incidences were 8.4, 8.4, 12.0 and 16.3% after 5, 10, 15 years and at the end of the follow-up (20 years) (p = 0.721).
Figure 2.
Overall Cumulative incidence of revision. The hybrid cemented group showed an incidence of 6.7, 8.4, 13.5 and 21.5% after 5, 10, 15 years and at the end of follow-up (19.6 years). For the cementless group, the cumulative incidences were 8.4, 8.4, 12.0 and 16.3% after 5, 10, 15 years and at the end of the follow-up (20 years) (p = 0.721).
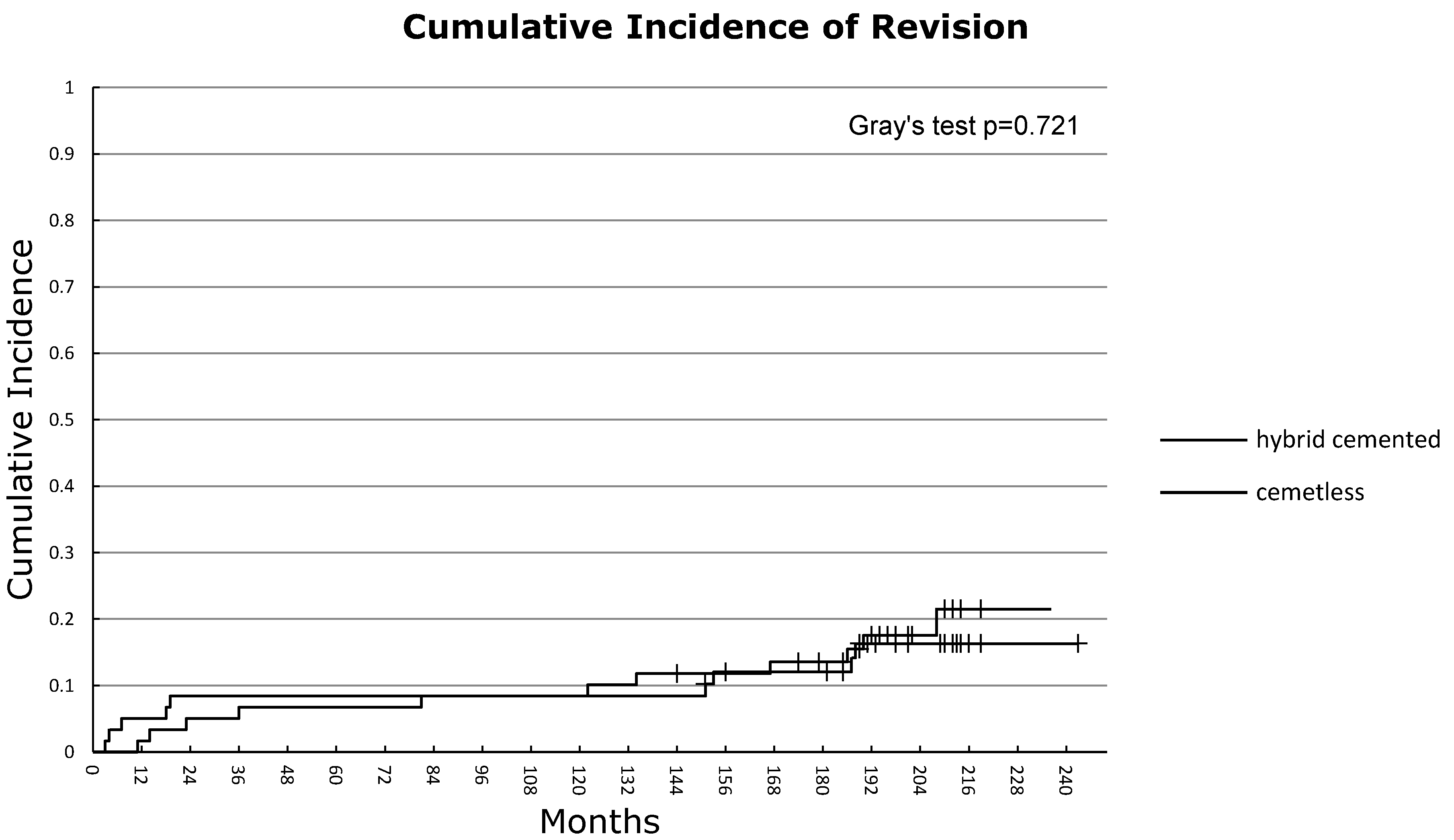
Figure 3.
Cumulative incidence of aseptic loosening. The hybrid cemented group showed an incidence of 3.4, 3.4, 5.1 and 5.1% after 5, 10, 15 years and at the end of follow-up (19.6 years). For the cementless group, the cumulative incidences were 3.4, 3.4, 3.4 and 5.5% after 5, 10, 15 years and at the end of the follow-up (20 years) (p = 0.967).
Figure 3.
Cumulative incidence of aseptic loosening. The hybrid cemented group showed an incidence of 3.4, 3.4, 5.1 and 5.1% after 5, 10, 15 years and at the end of follow-up (19.6 years). For the cementless group, the cumulative incidences were 3.4, 3.4, 3.4 and 5.5% after 5, 10, 15 years and at the end of the follow-up (20 years) (p = 0.967).
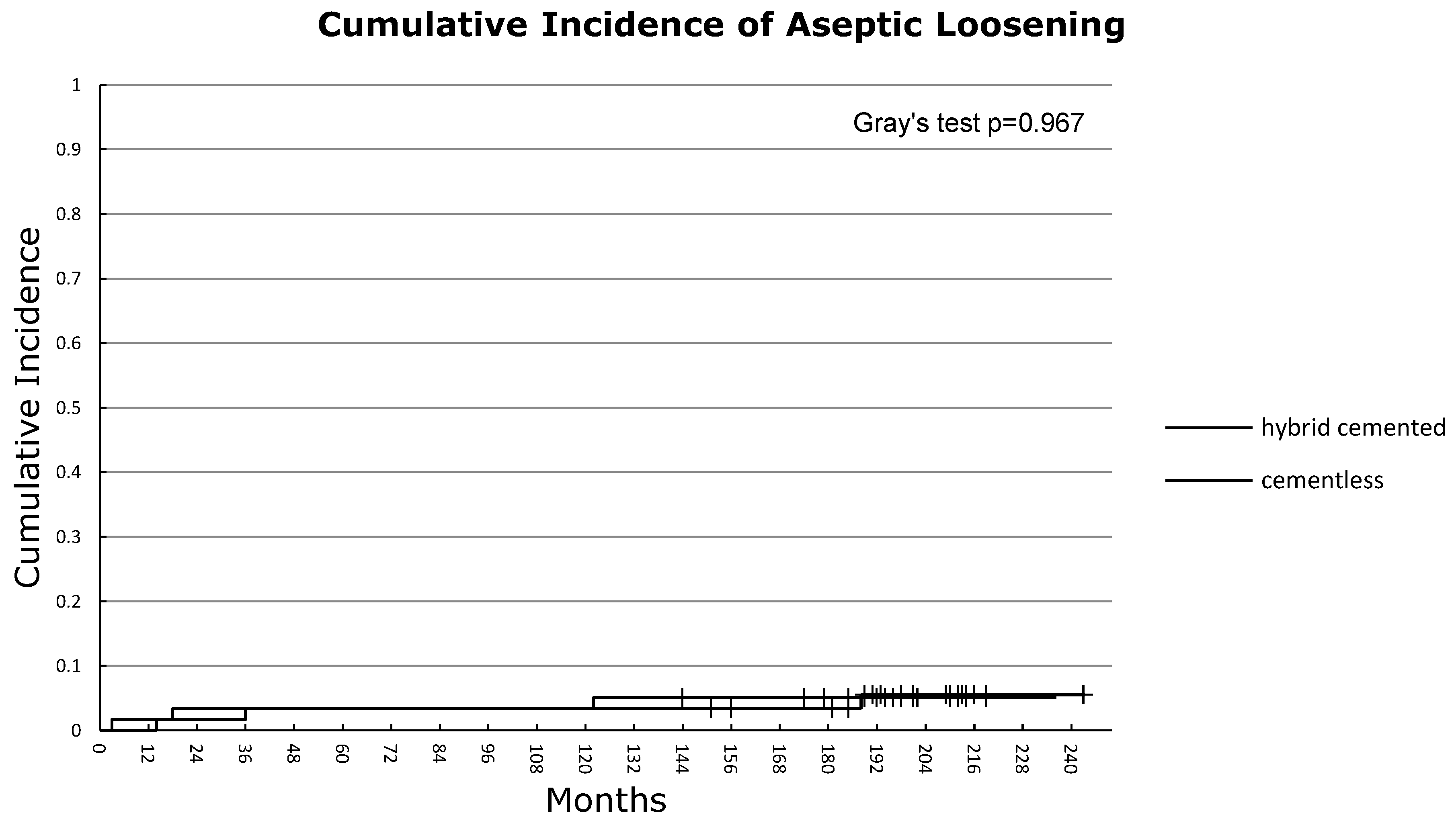
Figure 4.
Anteroposterior and lateral radiographs of cementless (Fig. 4-A–B) and hybrid cemented (Fig. 4-C–D) TKA implants, 10 years postoperatively.
Figure 4.
Anteroposterior and lateral radiographs of cementless (Fig. 4-A–B) and hybrid cemented (Fig. 4-C–D) TKA implants, 10 years postoperatively.
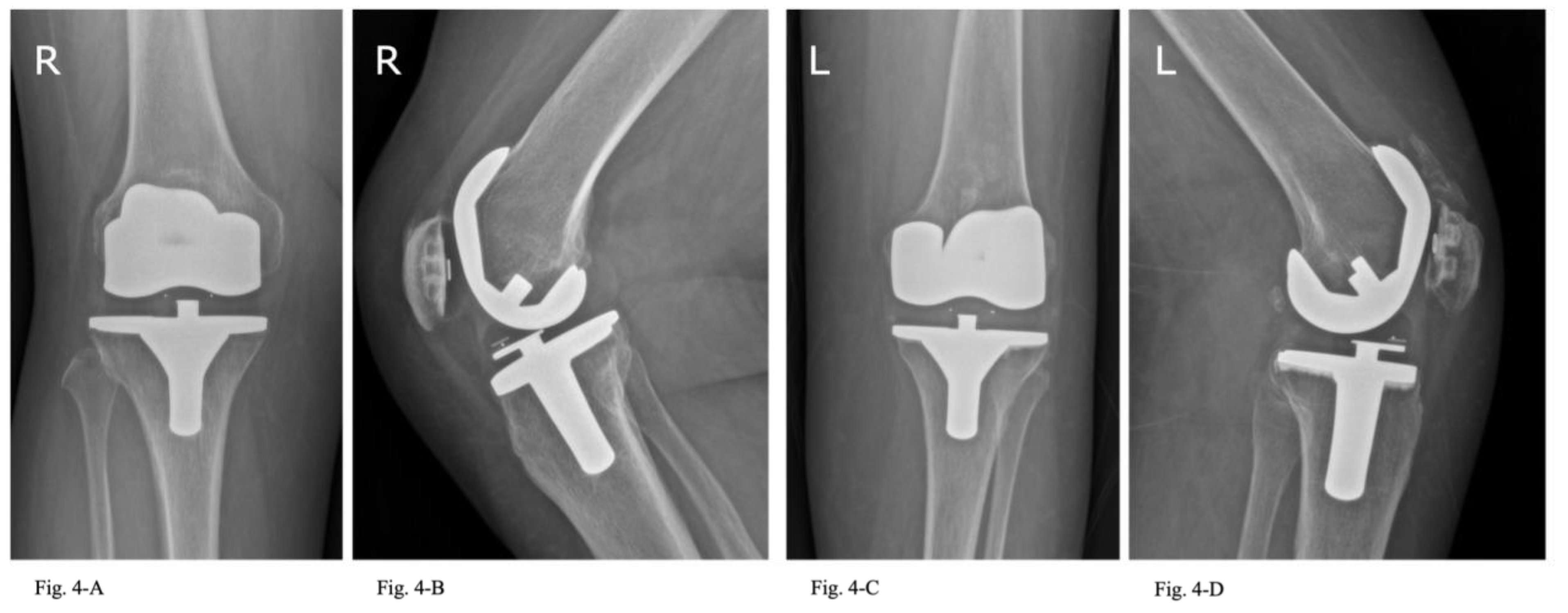

Table 1.
Demographic data of 120 patients, including 60 patients of the cementless group and 60 patients of the hybrid cemented group.
Table 1.
Demographic data of 120 patients, including 60 patients of the cementless group and 60 patients of the hybrid cemented group.
| Demographic data | All patients n = 120 |
Cementless n = 60 |
Hybrid cemented n = 60 |
P-value |
|---|---|---|---|---|
| Mean patient age, years (range) | 66.93 (33 to 90) | 65.72 (43 to 85) | 68.13 (35 to 90) | 0.189* |
| Female patients, n (%) | 81 (67.50) | 35 (58.33) | 46 (76.67) | 0.032†§ |
| Mean BMI kg/m2 (range) | 30.28 (19 to 51) | 30.03 (19 to 44) | 30.53 (23 to 51) | 0.615* |
| L:R knees | 56:64 | 29:31 | 27:33 | 0.714† |
| Operative time, minutes (range) | 130.71 (80 to 200) | 125.7 (80 to 175) | 135.7 (95 to 200) | 0.017*§ |
| Primary diagnosis, n (%) | ||||
| Idiopathic arthritis | 106 (88.3) | 52 (86.7) | 54 (90.0) | 0.570† |
| Posttraumatic arthritis | 6 (5) | 5 (8.3) | 1 (1.7) | 0.094† |
| Rheumatoid arthritis | 4 (3.3) | 2 (3.3) | 2 (3.3) | 1.000† |
| Avascular necrosis | 1 (0.8) | 1 (1.7) | 0 (0) | 0.331† |
| Unicondylar knee arthroplasty | 3 (2.5) | 0 (0) | 3 (5) | 0.079† |
*Student’s t-test, †Chi-square test, §Statistically significant, BMI, Body Mass Index; L, left; R, right.
Table 2.
Causes of Revision and Median Time to Revision, Following Primary TKA.
| Reasons for Revision | All patients (n= 120) |
Cementless (n = 60) |
Hybrid cemented (n = 60) |
P-value |
|---|---|---|---|---|
| Polyethylene failure, n (%) | 7 (35) | 3 (15) | 4 (20) | 0.761a |
| Aseptic loosening, n (%) | 6 (30) | 3 (15) | 3 (15) | 0.967a |
| PJI, n (%) | 3 (15) | 0 (0) | 3 (15) | 0.087a |
| Limited mobility, n (%) | 4 (15) | 3 (15) | 1 (5) | 0.299a |
| Total, n (%) | 20 (100) | 9 (45) | 11 (55) | 0.721a |
| Time to Revision | ||||
| Polyethylene failure, months (median, IQR) | 176.5 (151.5 to 187.7) | 152 (151.0 to 161.5) | 186 (167.0 to 190.0) | 0.761a |
| Aseptic loosening, months (median, IQR) | 18.0 (8.5 to 79.0) | 10.5 (3 to 60.5) | 25 (14.0 to 57.5) | 0.967a |
| PJI, months (median, IQR) | 46.0 (11 to 94.2) | 0 (0 to 0) | 46 (11.0 to 94.2) | 0.087a |
| Limited mobility, months (median, IQR) | 7.0 (4.0 to 19.0) | 5.5 (4.0 to 10.0) | 23 (23.0 to 23.0) | 0.299a |
| Overall time to Revision (median, IQR) | 81.0 (14.0 to 167.0) | 18.5 (4.7 to 152.5) | 101.5 (20.7 to 171.7) | 0.721a |
aGray`s test, §Statistically significant.
Table 3.
Clinical outcomes by Follow-Up Interval.
| KSS Outcome (Range) | Cementless (n = 24) | Hybrid cemented (n = 22) | P-value |
|---|---|---|---|
| Mean clinical score | |||
| Preoperative | 54.10 (10 to 95) | 45.40 (0 to 100) | 0.011*§ |
| 5-year Follow-up | 93.05 (55 to 100) | 89.17 (45 to 100) | 0.109* |
| 10-year Follow-up | 89.25 (65 to 100) | 88.18 (58 to 99) | 0.736* |
| Mean functional score | |||
| Preoperative | 42.45 (0 to 69) | 46.10 (10 to 77) | 0.180* |
| 5-year Follow-up | 91.69 (64 to 100) | 90.52 (63 to 100) | 0.492* |
| 10-year Follow-up | 80.42 (30 to 100) | 80.00 (30 to 100) | 0.948* |
| Mean total score | |||
| Preoperative | 96.52 (0 to 153) | 91.52 (44 to 142) | 0.291* |
| 5-year Follow-up | 184.75 (144 to 200) | 179.68 (113 to 200) | 0.146* |
| 10-year Follow-up | 168.63 (104 to 197) | 168.18 (93 to 199) | 0.480* |
*Student’s t-test , §Statistically significant, KSS, Knee Society Score.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



