Submitted:
20 March 2025
Posted:
20 March 2025
You are already at the latest version
Abstract
Background/Objectives: Elevated human epididymis protein 4 (HE4) expression has been observed in breast cancer and is linked to cancer progression; however, its role in ductal carcinoma in situ (DCIS) remains unclear. This study evaluated HE4 levels in DCIS serum and tissue and their correlation with clinicopathological features. Methods: Preoperative serum HE4 levels were measured in 59 DCIS patients. HE4 mRNA and protein expression were assessed in DCIS and adjacent normal tissues via RNAscope in situ hybridization and immunohistochemistry. An independent tissue microarray of 41 DCIS cases was also analyzed, and the BreastMark database was applied to explore the prognostic relevance of HE4. Results: Serum HE4 levels (mean ± SD: 39.4 ± 11.9 pmol/L) were within the normal range and did not significantly correlate to clinicopathological parameters except menopause status. HE4 expression was significantly higher in DCIS tissues than in adjacent normal tissues, with mRNA and protein levels positively correlated (r = 0.771, p < 0.001). High HE4 mRNA and protein expression was associated with ER positivity, HER2 negativity, low stromal tumor-infiltrating lymphocyte density, and HR+/HER2- subtypes but did not predict DCIS recurrence. High HE4 expression in breast cancer patients correlated with better survival outcomes. Conclusions: While serum HE4 is not elevated in DCIS, high HE4 expression in tissues is linked to favorable clinicopathological characteristics; thus, further research is warranted on its potential prognostic role.
Keywords:
ductal carcinoma in situ
; breast
; HE4
; serum
; mRNA
; protein
; biomarker
1. Introduction
Ductal carcinoma in situ (DCIS), a non-obligate precursor of breast cancer, is a neoplastic proliferation of mammary ductal epithelial cells confined to the ductal–lobular system [1,2]. DCIS comprises 15% to 20% of all newly detected breast cancer cases in Korea, and its incidence increased following the routine use of mammographic screening [3]. However, the ability of mammography to detect small lesions, including DCIS, is significantly reduced in younger patients [4]. DCIS is a heterogeneous disease with biologically diverse outcomes [1,2]. There has been a need to discover a diagnostic and prognostic biomarker for the presence of DCIS or recurrence after DCIS surgery and/or treatment.
Human epididymis protein 4 (HE4), also known as WFDC2, is a secretory protein that is a member of the whey acidic protein (WAP) domain family [5]. This protein has a variety of functions, including protease inhibitors, and has a role in the innate immune defense of multiple epithelia [6]. HE4 has been expressed in the normal epithelium of the reproductive tract and proximal airways [5.6]. Increased HE4 expression has been reported in many cancer types, especially in gynecologic and pulmonary cancers [7,8,9]. HE4 has been reported as an important serum biomarker for the diagnosis of epithelial ovarian cancer and can be used to monitor the recurrence or disease progression of this cancer [10,11,12].
Recent research has demonstrated elevated serum HE4 levels in breast cancer patients and may be used as a diagnostic marker of breast carcinoma [13,14,15,16,17,18,19]. HE4 is also expressed in breast cancer tissues [18,20,21,22], and the expression of HE4 is a possible predictive factor of breast cancer recurrence [18,21]. However, the expression of HE4 in DCIS and its clinical value have yet to be properly characterized.
This study aimed to evaluate serum and tissue levels of HE4 in DCIS and their correlations with clinicopathological characteristics of DCIS. We determined preoperative serum HE4 levels in 59 DCIS patients. Moreover, we detected mRNA and protein in DCIS and surrounding normal tissues from these patients by RNAscope in situ hybridization (ISH) and immunohistochemistry analysis, respectively. The HE4 mRNA and protein expression levels were also detected in 41 DCIS tissues. The prognostic potential of HE4 in breast cancer patients has been tested using the BreastMark database.
2. Materials and Methods
2.1. Serum and Tissues Samples
Serum samples from 59 patients with DCIS and tissue microarrays containing DCIS tissues that had been matched with adjacent normal tissues from these patients were provided by Chonnam National University Hwasun Hospital (CNUHH) Biobank. The serum samples were collected before surgery and stored in a liquid nitrogen freezer. Tissue microarrays were constructed to contain DCIS tissues and adjacent normal tissues. From each formalin-fixed-paraffin-embedded (FFPE) DCIS sample, two to three cores and one to two cores with a diameter of 2.0 were taken from the DCIS cancer area and adjacent normal tissue area, respectively. Additionally, we obtained tissue microarrays containing only DCIS cancer tissues from CNUHH biobanks. These tissue microarrays contained two or three DCIS cancer cores from 41 patients.
2.2. Serum Concentrations of HE4
HE4 serum levels were measured using chemiluminescent microparticle immunoassays on the fully automated ARCHITECT instrument (Abbott Diagnostics Division) at the Department of Laboratory Medicine at CNUHH. According to the indications of the HE4 manufacturer, the abnormal ranges were > 70.4 pmol/L for premenopausal women and > 140.0 pmol/L for postmenopausal women [12].
2.3. RNAscope In Situ Hybridization (ISH) Assay
Chromogenic RNAscope ISH for HE4 mRNA transcripts was conducted using the RNAscope FFPE Assay kit (Advanced Cell Diagnostics) following previously described protocols [23]. In summary, serially sectioned TMA block slides underwent deparaffinization, dehydration, heat treatment, and protease digestion before hybridization with target probes for human Hs-WFDC2 (Cat# 524781, Advanced Cell Diagnostics), peptidylprolyl isomerase B (Hs-PPIB) as a positive control, and bacterial dihydrodipicolinate reductase (DapB) as a negative control. The hybridization signal was detected using the RNAscope 2.0 HD Reagent kit (Brown) (Advanced Cell Diagnostics) with 3,3'-diaminobenzidine solution as the chromogen. Slides were counterstained using Gill’s hematoxylin.
RNAscope amplification was interpreted semi-quantitatively according to the manufacturer’s guidelines: 0: no staining or < 1 dot/10 cells at 40×; 1: 1–3 dots/cell at 20–40×; 2: 4–10 dots/cell at 20–40×; 3: > 10 dots/cell with < 10% of positive cells having dot clusters visible at 20×; 4: > 10 dots/cell with > 10% of positive cells having dot clusters at 20×. Slides with PPIB scores of ≥ 2 and DapB background scores of ≤ 1 were considered suitable to pass the qualification of tissue mRNA. The HE4 mRNA expression level was classified as low (score: 0–2) or high (score: 3–4) [23].
2.4. Immunohistochemistry
HE4 immunohistochemical staining was conducted using a Bond-max Autostainer (Leica Microsystems, Bannockburn, IL), as previously described, alongside a HE4 rabbit polyclonal antibody (1:800; Atlas Antibodies) [24]. HE4 immunoreactivity was semi-quantitatively evaluated based on the cytoplasmic staining intensity (no staining; 1: weak staining; 2: moderate staining; 3: strong staining) and the percentage of stained cells (0: no positive cells; 1: 1%–24%; 2: 25%–49%; 3: 50–74%; 4: 75–100%) according to a previous report [20]. The intensity and extent scores were multiplied to determine the final staining score. For the statistical analysis, samples with final scores between 0 and 4 were categorized as having low HE4 expression, while those with scores ≥ 4 were classified as having high HE4 expression [20].
2.5. Clinicopathological Characteristics of DCIS Patients
Clinicopathological characteristics, including patient age, menopausal status, tumor size, nuclear grade, comedo-type necrosis, and patient outcomes (local recurrence and survival), were obtained from medical records. Local recurrence was defined as any in situ or invasive carcinoma recurrence in the ipsilateral breast, axilla, or chest wall. Estrogen receptor (ER), PR (progesterone receptor), and human epidermal growth factor receptor 2 (HER2) expressions were assessed for all samples. ER or PR positivity was defined as at least 1% of tumor nuclei showing positive staining [25]. HER2 positivity (HER2+) was determined by an immunohistochemical staining score of 3+, following the American Society of Clinical Oncology (ASCO)/College of American Pathologists (CAP) guidelines [26]. DCIS was classified into four subtypes based on hormone receptor (HR) (ER or PR) and HER2 expression status: HR+/HER2-, HR+/HER2+, HR-/HER2+, and triple-negative (ER-/PR-/HER2-).
The density of stromal tumor-infiltrating lymphocytes (TILs) was defined as the percentage of the tumor stroma occupied by lymphocytic infiltrates without direct contact with DCIS cells. TILs were categorized into four groups: 0 (no TILs), 1 (< 5% stromal area with TILs), 2 (5–50% stromal area with TILs), and 3 (> 50% stromal area with TILs) [27].
2.6. HE4 as Prognostic Biomarker in Patients with Breast Cancer Using BreastMark
HE4 was analyzed in patients with breast cancer according to its prognostic significance using a BreastMark database, as previously described [28]. Disease-free survival was analyzed, and the median expression was used to dichotomize the data. Disease-free survival was evaluated for breast cancer overall, as well as for lymph node-positive and lymph node-negative cases, and across molecular subtypes classified by the Pam50 system, including luminal A, luminal B, HER2, and basal types. Survival curves were generated using the Kaplan–Meier method, with differences assessed via the log-rank test. Cox regression analysis was used to calculate hazard ratios (HRs) with 95% confidence intervals (95% CIs).
2.7. Statistical Analysis
Statistical analyses were performed using the SPSS program (Version 13.5, SPSS Inc., Chicago, IL). The serum HE4 level was evaluated using the independent t-test, one-way ANOVA, and Kruskal–Wallis tests. The Mann–Whitney U test was used to assess differences in HE4 mRNA and protein expression between DCIS and their adjacent normal breast tissues. Spearman’s correlation was used to evaluate the association between variables. Categorical nominal variables were tested using the χ2 test or Fisher's exact test. Linear-by-linear association was added to test for the trend. A probability of p < 0.05 was considered statistically significant.
3. Results
3.1. HE4 Serum Level in Patients with DCIS and HE4 mRNA and Protein Expression in DCIS Tissues and Their Adjacent Normal Breast Tissues
All 59 DCIS cases were successfully analyzed for HE4 serum concentration. HE4 levels ranged from 23.5 to 86.3 pmol/L (mean ± SD: 39.4 ± 11.9). There were no abnormal cases according to the manufacturer's proposed cutoff level for HE4 (70.4 pmol/L for premenopausal women and 140.0 pmol/L for postmenopausal women). HE4 serum levels in DCIS patients did not differ according to clinicopathological parameters except for menopause status (Table 1).
HE4 concentration was significantly higher in postmenopausal DCIS patients than in premenopausal DCIS patients (42.9 ± 14.4 pmol/L vs. 35.3 ± 6.4 pmol/L; p < 0.05; Figure 1).
ISH and immunohistochemical analyses were performed to examine HE4 mRNA and protein expression in DCIS tissues and adjacent normal breast tissues. Among 59 cases, mRNA ISH and immunohistochemical data were interpretable in 58 cases. HE4 mRNA ISH signals, if present, were detectable in cancer cells from DCIS (Figure 2a,b), while the HE4 mRNA expression was reduced in epithelial cells of normal breast tissue (Figure 2c,d). Comparative analysis of HE4 mRNA amplification scores revealed that HE4 levels in DCIS tissues were higher than in their corresponding normal tissues (1.9 ± 0.9 vs. 1.3 ± 0.5; p < 0.001; Figure 3a).
The HE4 immunohistochemical staining results were similar to the mRNA ISH results. Immunohistochemical staining for HE4 is restricted to the epithelial compartment of normal and DCIC tissues, with no positivity in adjacent stromal cells (Figure 2e–h). The positive staining in DCIS appeared cytoplasmic (Figure 2e,f). Normal breast epithelium was negative to weakly positive, and luminal secretion was also positive (Figure 2g,h). HE4 immunohistochemical staining scores were significantly higher in DCIS tissues than in adjacent normal tissues (3.2 ± 2.6 vs. 1.8 ± 0.6; p < 0.001; Figure 3b).
Spearman’s correlation analyses revealed no significant correlation between serum and DCIS tissue levels of HE4 (r = 0.022, p = 0.871 for serum vs. mRNA; r = 0.040, p = 0.766 for serum vs. protein). Serum HE4 concentrations did not show a significant difference between low and high mRNA/protein expression in DCIS tissues (39.9 ± 12.7 pmol/L vs. 38.9 ± 10.2 pmol/L, p = 0.788, for mRNA; 39.8 ± 13.4 pmol/L vs. 39.1 ± 9.1 pmol/L, p = 0.838, for protein).
3.2. Expression of HE4 mRNA and Protein in DCIS Tissues and Correlation with Clinicopathological Features
3.2.1. Clinical Characteristics of DCIS Patient Cohorts
Of the 100 DCIS patients, 52 were premenopausal, and 48 were postmenopausal. The DCIS tumor sizes ranged from 0.8 to 10.0 cm in diameter (median: 2.2 cm, mean: 2.8 cm). Most cases were classified as nuclear grade 2 (55 cases, 55.0%) or grade 3 (42 cases, 42.0%). Comedo-type necrosis was present in 77 cases (77.0%). Stromal TILs were identified in all DCIS cases, with 68 cases (68.0%) scoring 1, 30 cases (30.0%) scoring 2, and 2 cases (2.0%) scoring 3. The DCIS subtypes included 48 cases (48.0%) of HR+/HER2-, 17 cases (17.0%) of HR+/HER2+, 29 cases (29.0%) of HR-/HER2+, and 6 cases (6.0%) of the triple-negative subtype. In the analysis, the median follow-up duration was 96 months (range: 7–178 months); recurrence occurred in nine cases (9.0%), but no cancer-related deaths were reported.
3.2.2. Expression of HE4 mRNA and Protein in DCIS Tissues
Among 100 DCIS tissues, HE4 mRNA ISH and immunohistochemical staining were interpretable in 99 cases. HE4 mRNA ISH scores and HE4 immunohistochemical staining scores in DCIS tissues showed positive correlations (r = 0.771, p < 0.001). HE4 expression was evaluated based on cutoff point. High mRNA and protein expression of HE4 were observed in 25 of 99 (25.3%) and 34 of 99 (34.3%) cases, respectively. The concordance between HE4 mRNA ISH and protein immunohistochemistry was summarized in Table 2. The results showed coincidence rates of HE4 expression using two different methods was 88.9%, and indicated two methods have a consistent trends.
Next, the relationship between HE4 expression and clinicopathological features in DCIS was analyzed (Table 3). High HE4 mRNA expression was significantly associated with lower stromal TIL density, ER positivity, HER2 negativity, and the HR+/HER2- subtype. Similarly, high HE4 protein expression correlated with the absence of comedo-type necrosis, lower stromal TIL density, ER positivity, HER2 negativity, and the HR+/HER2- subtype. However, HE4 mRNA and protein expression did not correlate with DCIS recurrence.
3.3. HE4 for Prognostic Biomarker in Patients with Breast Cancer
Following BreastMark analysis, higher HE4 expression in breast cancer patients was significantly associated with improved survival in the overall group (HR = 0.838, p = 0.003, n = 2,652) and lymph node-negative group (HR = 0.791, p = 0.029, n = 1,183) (Figure 4).
4. Discussion
To our knowledge, this study is the first to determine HE4 serum and tissue levels in patients with DCIS. Although serum HE4 was not increased above the cutoff value in patients with DCIS, high HE4 mRNA and protein expression in DCIS tissues were associated with good clinicopathological characteristics.
DCIS is a non-invasive form of breast cancer; the routine use of mammography screening has led to a significant increase in DCIS diagnoses, which nowadays account for 15–20% of all newly detected breast cancer cases in Korea [3]. Although mammography is the only available screening method to detect DCIS, the technique has limitations [4]. DCIS is a heterogeneous disease that progresses both rapidly and slowly [1,2]. Therefore, diagnostic and prognostic biomarkers to detect the presence and recurrence of DCIS are needed for timely treatment and better management.
HE4 was originally described as an epididymis-specific protein; however, HE4 has recently been proposed as a putative serum biomarker in diagnosing and monitoring some tumors, especially in gynecologic and pulmonary cancers. [7,8,9]. HE4 expression in epithelial ovarian cancer tissues is higher than those in borderline ovarian tumors, benign ovarian tumors, and normal ovarian tissues [12]. HE4 is also released significantly into the blood by epithelial ovarian cancer. Serum HE4 has been identified as the most promising biomarker for the diagnosis of epithelial ovarian cancer and has been used in monitoring the follow-up and relapse of ovarian cancer patients [10,11,12].
Several studies have investigated the role of HE4 in blood and cancer tissues as a diagnostic and prognostic biomarker in breast cancer [13,14,15,16,17,18,19,20,21,22]. However, the expression of HE4 in DCIS and its diagnostic and prognostic value has yet to be properly characterized. Most studies measuring HE4 in blood measure the HE4 serum and plasma levels in breast cancer patients using the enzyme-linked immunosorbent assay [13,14,15,16,17,18,19]. HE4 levels in the blood of breast cancer patients were significantly higher than those in benign breast tumor patients or healthy individuals, suggesting that HE4 may be useful as a marker for breast cancer diagnoses [13,15,16,17,18,19]. However, no studies have investigated diagnostic accuracy using the cutoff value suggested by the HE4 manufacturer. The present study measured serum HE4 levels using chemiluminescent microparticle immunoassays on a fully automated ARCHITECT instrument. The HE4 levels in 59 DCIS patients ranged from 23.5 to 86.3 pmol/L. Based on the reference limit provided by the manufacturer, there were no abnormal cases relating to HE4 levels, which suggests that serum HE4 cannot be used as a marker for detecting breast DCIS.
The HE4 mRNA and protein expression levels in breast cancer tissues have been measured previously using real-time PCR and immunohistochemistry [18,20,21,22]. Immunohistochemically, HE4 was expressed in the cytoplasm of breast cancer cells. HE4 was also expressed in normal breast tissues, particularly in duct epithelial cells [20,22]. In breast cancer, positive HE4 expression has been shown to range from 9.6 to 98.8%, depending on different interpretation criteria [18,20,21,22]. Mirmohseni Namini et al. found that HE4 was positively expressed in 3 of 31 (9.6%) breast cancer tissues but not in adjacent normal breast tissues [18]. HE4 mRNA expression in breast cancer tissues was increased compared to adjacent normal tissues [18,21].
Using RNAscope ISH and immunohistochemistry, we analyzed HE4 mRNA and protein levels in DCIS and adjacent normal breast tissues. Both methods confirmed that HE4 mRNA and protein expression were localized in the epithelial compartment of normal and DCIS tissues, with significantly higher expression in DCIS tissues. Furthermore, HE4 mRNA levels in DCIS tissues correlated positively with HE4 protein levels. Meanwhile, despite the underlying mechanism of HE4 increase in DCIS tumor cells remaining unclear, our data confirmed that HE4 mRNA and protein expression levels increased in cancer cells of DCIS tissues. Thus, HE4 expression in DCIS tissues may be regulated primarily at the transcriptional level.
In the present study, we compared the serum levels of HE4 in DCIS patients with the expression of HE4 mRNA and protein in DCIS tumor tissues; however, no correlation was noted between HE4 serum and DCIS tissue levels. Serum HE4 concentrations did not significantly differ between low and high mRNA/protein expression in DCIS tissues. Several studies on other cancers have also revealed a lack of correlation between HE4 serum and tissue levels. Indeed, there was no significant association between serum HE4 and immunohistochemically detected tissue HE4 levels for endometrial cancer [29,30]. This discrepancy could be partially due to the semi-quantitative detection methods used to measure HE4 mRNA and protein tissue levels, which might not possess adequate sensitivity to identify subtle differences in HE4 expression. This discrepancy could also be due to the heterogeneous nature of HE4 expression. Although all lesions can affect serum levels, we only evaluated mRNA or protein expression as a snapshot of a small portion of the tumor.
The potential prognostic role of HE4 in breast cancer is not conclusive. Serum HE4 did not correlate with breast cancer clinicopathologic features [14,15]. However, reports by Lu et al. [16] and Mirmohseni Namini et al. [18] showed an association between HE4 expression and poor prognostic factors in patients with breast cancer. The median value of HE4 in stage III breast cancer patients was significantly higher than in stage I/II individuals [16]. Mirmohseni Namini et al. reported a significant correlation between plasma HE4 levels and adverse prognostic features such as grade, stage, and tumor size [18]. Moreover, plasma HE4 levels were significantly upregulated in breast cancer patients with metastasis compared with non-metastatic breast cancer patients. The relative expression of HE4 mRNA in BC patients significantly correlated with the breast cancer grade [18]. However, Kamei et al. determined HE4 mRNA expression in breast cancer and found no difference between positive and negative expressions for disease-free survival [21]. Kamei et al. also determined HE4 expression in breast cancer tissues via immunohistochemistry. No correlation was found between HE4 expression in the immunohistochemistry analysis and any clinical factors except nodal involvement. HE4 expression was associated with lymph node involvement. Although HE4 expression following multivariate analysis did not show the prognostic significance of disease-free survival, the five-year disease-free survival in the HE4-positive group was significantly worse than in the negative group. Akoz et al. found that HE4 immunohistochemical staining intensity was strongly associated with tumor grade and HER2 status based on immunohistochemistry and fluorescence in situ hybridization [22]. However, median lifespans of the breast cancer patients based on HE4 staining intensity did not differ significantly. Overall, increased HE4 expression has been suggested to be associated with adverse clinical factors in breast cancer patients, but its relationship to clinical outcomes has not yet been elucidated.
The clinicopathological factors of DCIS that have been associated with increased risk of local recurrence include large lesion size, high nuclear grade (grade III), presence of comedonecrosis, positive margins, high stromal TILs, and HER2-positive or triple-negative intrinsic subtypes [1,2,31]. In the present study, HE4 serum levels in DCIS patients did not differ according to clinicopathological parameters, except menopause status. However, HE4 was not correlated with menopause status in breast cancer patients [15,16]. Consistent with our results, the HE4 level in postmenopausal patients with ovarian cancer was higher than in premenopausal patients with ovarian cancer [12]. High HE4 mRNA and protein expression were observed in 25.3% and 34.3% of DCIS cases, respectively. We employed the interpretation criteria used by Galgano et al. [20]. Although HE4 mRNA and protein expression did not correlate with the recurrence of DCIS, HE4 mRNA and protein expression were associated with good prognostic and predictive clinicopathological factors, including absence of comedonecrosis, low stromal TIL density scores, ER positivity, HER2 negativity, and HR+/HER2- subtypes. We verified HE4 mRNA expression as a prognostic biomarker for breast cancer using the public BreastMark database. High HE4 mRNA expression was significantly associated with good survival in the overall and lymph node-negative groups. These results suggest that high HE4 mRNA and protein expression may be used as a good prognostic marker in patients with breast cancer, including DCIS. Considering the potential prognostic value of HE4 expression in patients with DCIS, further studies with a large cohort of DCIS cases and a long-term follow-up are needed.
5. Conclusions
Our results characterize the HE4 serum and tissue levels in patients with DCIS. Serum HE4 was not increased above the cutoff value in patients with DCIS, indicating that HE4 is not suitable for screening and diagnosing DCIS. Meanwhile, high HE4 mRNA and protein in DCIS tissues were associated with good clinicopathological characteristics, suggesting the possibility of using the expression of tissue HE4 as a predictor of prognosis in DCIS patients. However, further studies with larger sample sizes are needed to confirm the current findings.
Author Contributions
Kim: Formal analysis, data curation, methodology, writing—original draft, supervision; Park: Formal analysis, data curation, methodology, writing review and editing, supervision; Lee: conceptualization, writing—review and editing, supervision. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by a grant (HCRI24021) from Chonnam National University, Hwasun Hospital Institute for Biomedical Science.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board of Chonnam National University Hwasun Hospital (Jeollanam-do, Korea) (approval number: CNUHH-2021-101).
Informed Consent Statement
All cases have obtained written informed consent, and the Institutional Review Board of Chonnam National University Hwasun Hospital approved the informed consent forms.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
This article was partly presented at the 2024 European Congress of Pathology, which took place in Florence, Italy, from September 7 to 10, 2024. Ji Shin Leee, Nah Ihm Kim, Min Ho Park. Assessment of human epididymis protein four expression in ductal carcinoma in situ of the breast [abstract]. In: Proceedings of the 2024 European Congress of Pathology; 2024 Sep 7-10; Florence, Italy; Virchows Archiv 2024;485(Suppl 1):Abstract nr PS-02-019.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| HE4 | Human epididymis protein 4 |
| DCIS | Ductal carcinoma in situ |
| ER | Estrogen receptor |
| PR | Progesterone receptor |
| HER2 | Human epidermal growth factor receptor 2 |
| HR | Hormone receptor |
| WAP | Whey acidic protein |
| ISH | In situ hybridization |
| FFPE | Formalin-fixed-paraffin-embedded |
| CNUHH | Chonnam National University Hwasun Hospital |
| TILs | Tumor-infiltrating lymphocytes |
References
- Pinder, S.E.; Collins, L.C.; Fox, S.B.; Schnitt, S.J.; van Deurzen, C.H.M.; Weaver, D.L.; Wesseling, J. Ductal carcinoma in situ. In WHO Classification of Tumors Editorial Board. Breast Tumours. WHO Classification of Tumors, 5th ed.; Allison, K.H., Brogi, E., Ellis, I.O., Fox, S.B., Morris, E.A., Sahin, A., Salgado, R., Sapino, A., Sasano, H., Schnit, S.J., Sotiriou, C., van Diest, P.J., Eds.; IARC: Lyon, France, 2019; pp. 76–81. [Google Scholar]
- Hoda, S.A. Ductal carcinoma in situ. In Rosen’s Breast Pathology, 5th ed.; Hoda, S.A., Brogi, E., Koerner, F.C., Rosen, P.P., Eds.; Wolters Kluwer: Philadelphia, 2021; pp. 363–450. [Google Scholar]
- Cha,C.D.; Park, C.S.; Shin, H.C.; Han, J.; Choi, J.E.; Kim, J.H.; Jung, K.W.; Lee, S.B.; Nam, S.E.; Yoon, T.I.; et al. Breast cancer statistics in Korea, 2021. J. Breast. Cancer 2024, 27, 351–361.
- Lacombe, J.; Mangé, A.; Bougnoux, A.C.; Prassas, I.; Solassol, J. A multiparametric serum marker panel as a complementary test to mammography for the diagnosis of node-negative early-stage breast cancer and DCIS in young women. Cancer Epidemiol. Biomarkers Prev. 2014, 23, 1834–1842. [Google Scholar] [CrossRef]
- Bingle, L.; Singleton, V.; Bingle, C.D. The putative ovarian tumour marker gene HE4 (WFDC2), is expressed in normal tissues and undergoes complex alternative splicing to yield multiple protein isoforms. Oncogene 2002, 21, 2768–2773. [Google Scholar] [CrossRef] [PubMed]
- Bingle, L.; Cross, S.S.; High, A.S.; Wallace, W.A.; Rassl, D.; Yuan, G.; Hellstrom, I.; Campos, M.A.; Bingle, C.D. WFDC2 (HE4): a potential role in the innate immunity of the oral cavity and respiratory tract and the development of adenocarcinomas of the lung. Respir. Res. 2006, 7, 61. [Google Scholar] [CrossRef] [PubMed]
- James, N.E.; Chichester, C.; Ribeiro, J.R. Beyond the biomarker: understanding the diverse roles of human epididymis protein 4 in the pathogenesis of epithelial ovarian cancer. Front. Oncol. 2018, 8, 124. [Google Scholar] [CrossRef]
- Capriglione, S.; Plotti, F.; Miranda, A.; Lopez, S.; Scaletta, G.; Moncelli, M.; Luvero, D.; De Cicco Nardone, C.; Terranova, C.; Montera, R.; et al. Further insight into prognostic factors in endometrial cancer: the new serum biomarker HE4. Expert Rev. Anticancer Ther. 2017, 17, 9–18. [Google Scholar] [CrossRef]
- He, Y.P.; Li, L.X.; Tang, J.X.; Yi, L.; Zhao, Y.; Zhang, H.W.; Wu, Z.J.; Lei, H.K.; Yu, H.Q.; Nian, W.Q.; Gan, L. HE4 as a biomarker for diagnosis of lung cancer: A meta-analysis. Medicine (Baltimore). 2019, 98, e17198. [Google Scholar] [CrossRef]
- Cao, H.; You, D.; Lan, Z.; Ye, H.; Hou, M.; Xi, M. Prognostic value of serum and tissue HE4 expression in ovarian cancer: a systematic review with meta-analysis of 90 studies. Expert Rev. Mol. Diagn. 2018, 18, 371–383. [Google Scholar] [CrossRef]
- Zhu, L.; Gou, R.; Guo, Q.; Wang, J.; Liu, Q.; Lin, B. High expression and potential synergy of human epididymis protein 4 and Annexin A8 promote progression and predict poor prognosis in epithelial ovarian cancer. Am. J. Transl. Res. 2020, 12, 4017–4030. [Google Scholar]
- Uno, M.; Matsuo, R.; Maezawa, N.; Kato, T. Evaluation of follow-up observation using human epididymis protein 4, a tumor marker, in patients with ovarian cancer. Obstet. Gynecol. Sci. 2023, 66, 290–299. [Google Scholar] [CrossRef]
- Hertlein, L.; Stieber, P.; Kirschenhofer, A.; Krocker, K.; Nagel, D.; Lenhard, M.; Burges, A. Human epididymis protein 4 (HE4) in benign and malignant diseases. Clin. Chem. Lab. Med. 2012, 50, 2181–2188. [Google Scholar] [CrossRef] [PubMed]
- Durur-Karakaya, A.; Durur-Subasi, I.; Karaman, A.; Akcay, M.N.; Palabiyik, S.S.; Erdemci, B.; Alper, F.; Acemoglu, H. The use of breast magnetic resonance imaging parameters to identify possible signaling pathways of a serum biomarker, HE4. J. Comput. Assist. Tomogr. 2016, 40, 436–441. [Google Scholar] [CrossRef] [PubMed]
- Gündüz, U.R.; Gunaldi, M.; Isiksacan, N.; Gündüz, S.; Okuturlar, Y.; Kocoglu, H. A new marker for breast cancer diagnosis, human epididymis protein 4: A preliminary study. Mol. Clin. Oncol. 2016, 5, 355–360. [Google Scholar] [CrossRef]
- Lu, M.; Ju, S.; Shen, X.; Wang, X.; Jing, R.; Yang, C.; Chu, H.; Cong, H. Combined detection of plasma miR-127-3p and HE4 improves the diagnostic efficacy of breast cancer. Cancer Biomark. 2017, 18, 143–148. [Google Scholar] [CrossRef]
- Sai Baba, K.S.S.; Rehman, M.A.; Pradeep Kumar, J.; Fatima, M.; Raju, G.S.N.; Uppin, S.G.; Mohammed, N. Serum human epididymis protein-4 (HE4) - a novel approach to differentiate malignant from benign breast tumors. Asian Pac. J. Cancer Prev. 2021, 22, 2509–2507. [Google Scholar] [CrossRef]
- Mirmohseni Namini, N.; Abdollahi, A.; Movahedi, M.; Emami Razavi, A.; Saghiri, R. HE4, A new potential tumor marker for early diagnosis and predicting of breast cancer progression. Iran J. Pathol. 2021, 16, 284–296. [Google Scholar] [CrossRef]
- Abdelrazek, M.A.; Nageb, A.; Barakat, L.A.; Abouzid, A.; Elbaz, R. BC-DETECT: combined detection of serum HE4 and TFF3 improves breast cancer diagnostic efficacy. Breast Cancer 2022, 29, 507–515. [Google Scholar] [CrossRef]
- Galgano, M.T.; Hampton, G.M.; Frierson, H.F. Jr. Comprehensive analysis of HE4 expression in normal and malignant human tissues. Mod. Pathol. 2006, 19, 847–853. [Google Scholar] [CrossRef]
- Kamei, M,; Yamashita, S.; Tokuishi, K.; Hashioto, T.; Moroga, T.; Suehiro, S.; Ono, K.; Miyawaki, M.; Takeno, S.; Yamamoto, S.; et al. HE4 expression can be associated with lymph node metastases and disease-free survival in breast cancer. Anticancer Res. 2010, 30, 4779–4783.
- Akoz, G.; Diniz, G.; Ekmekci, S.; Ekin, Z.Y.; Uncel, M. Evaluation of human epididymal secretory protein 4 expression according to the molecular subtypes (luminal A, luminal B, human epidermal growth factor receptor 2-positive, triple-negative) of breast cancer. Indian J. Pathol. Microbiol. 2018, 61, 323–329. [Google Scholar]
- Kim, G.E.; Kim, N.I.; Park, M.H.; Lee, J.S. B7-H3 and B7-H4 expression in phyllodes tumors of the breast detected by RNA in situ hybridization and immunohistochemistry: association with clinicopathological features and T-cell infiltration. Tumour Biol. 2018, 40, 1010428318815032. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.E.; Kim, J.H.; Lee, K.H.; Choi, Y.D.; Lee, J.S.; Lee, J.H.; Nam, J.H.; Choi, C.; Park, M.H.; Yoon, J.H. Stromal matrix metalloproteinase-14 expression correlates with the grade and biological behavior of mammary phyllodes tumors. Appl. Immunohistochem. Mol. Morphol. 2012, 20, 298–303. [Google Scholar] [CrossRef] [PubMed]
- Hammond, M.E.; Hayes, D.F.; Dowsett, M.; Allred, D.C.; Hagerty, K.L.; Badve, S.; Fitzgibbons, P.L.; Francis, G.; Goldstein, N.S.; Hayes, M.; et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for immunohistochemical testing of estrogen and progesterone receptors in breast cancer. Arch. Pathol. Lab. Med. 2010, 134, 907–922. [Google Scholar]
- Wolff, A.C.; Hammond, M.E.; Schwartz, J.N.; Hagerty, K.L.; Allred, D.C.; Cote, R.J.; Dowsett, M.; Fitzgibbons, P.L.; Hanna, W.M.; Langer, A.; et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for human epidermal growth factor receptor 2 testing in breast cancer. J. Clin. Oncol. 2007, 25, 118–145. [Google Scholar] [CrossRef]
- Salgado, R.; Denkert, C.; Demaria, S.; Sirtaine, N.; Klauschen, F.; Pruneri, G.; Wienert, S.; Van den Eynden, G.; Baehner, F.L.; Penault-Llorca, F.; et al. The evaluation of tumor-infiltrating lymphocytes (TILs) in breast cancer: recommendations by an International TILs Working Group 2014. Ann. Oncol. 2015, 26, 259–271. [Google Scholar] [CrossRef]
- Madden, S.F.; Clarke, C.; Gaule, P.; Aherne, S.T.; O'Donovan, N.; Clynes, M.; Crown, J.; Gallagher, W.M. BreastMark: an integrated approach to mining publicly available transcriptomic datasets relating to breast cancer outcome. Breast Cancer Res. 2013, 15, R52. [Google Scholar] [CrossRef]
- Bignotti, E.; Ragnoli, M.; Zanotti, L.; Calza, S.; Falchetti, M.; Lonardi, S.; Bergamelli, S.; Bandiera, E.; Tassi, R.A.; Romani, C.; et al. Diagnostic and prognostic impact of serum HE4 detection in endometrial carcinoma patients. Br. J. Cancer 2011, 104, 1418–1425. [Google Scholar] [CrossRef] [PubMed]
- Behrouzi, R.; Ryan, N.A.J.; Barr, C.E.; Derbyshire, A.E.; Wan, Y.L.; Maskell, Z.; Stocking, K.; Pemberton, P.W; Bolton, J.; McVey, R.J.; et al. Baseline serum HE4 but not tissue HE4 expression predicts response to the Levonorgestrel-releasing intrauterine system in atypical hyperplasia and early stage endometrial cancer. Cancers (Basel) 2020, 12, 276. [Google Scholar] [CrossRef]
- Hanna, W.M.; Parra-Herran, C.; Lu, F.I.; Slodkowska, E.; Rakovitch, E.; Nofech-Mozes, S. Ductal carcinoma in situ of the breast: an update for the pathologist in the era of individualized risk assessment and tailored therapies. Mod. Pathol. 2019, 32, 896–915. [Google Scholar] [CrossRef]
Figure 1.
Box plots of serum HE4 levels according to the menopausal status. The whiskers show the maximum and minimum values, with the exception of outliers (circles).
Figure 1.
Box plots of serum HE4 levels according to the menopausal status. The whiskers show the maximum and minimum values, with the exception of outliers (circles).
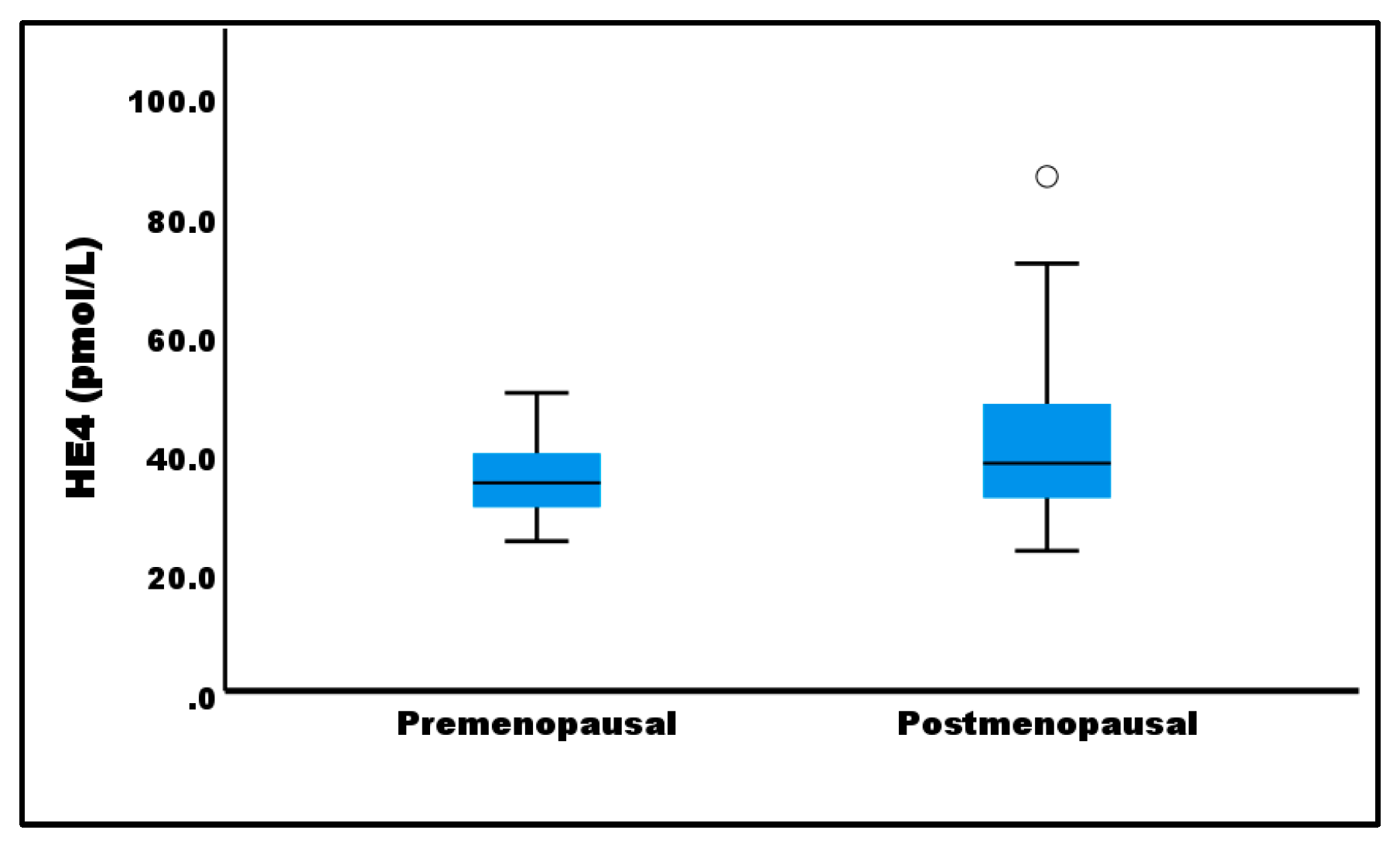
Figure 2.
Expression and localization of HE4 mRNA (a-d) and protein (e-h) in ductal carcinoma in situ (a, b, e, f) and adjacent normal breast tissues (c, d, g, h). mRNA and protein expression levels of HE4 are higher in DCIS tissues compared with adjacent normal tissues. a, c, e, g,×4; b, d, ×400; f, h, ×200.
Figure 2.
Expression and localization of HE4 mRNA (a-d) and protein (e-h) in ductal carcinoma in situ (a, b, e, f) and adjacent normal breast tissues (c, d, g, h). mRNA and protein expression levels of HE4 are higher in DCIS tissues compared with adjacent normal tissues. a, c, e, g,×4; b, d, ×400; f, h, ×200.
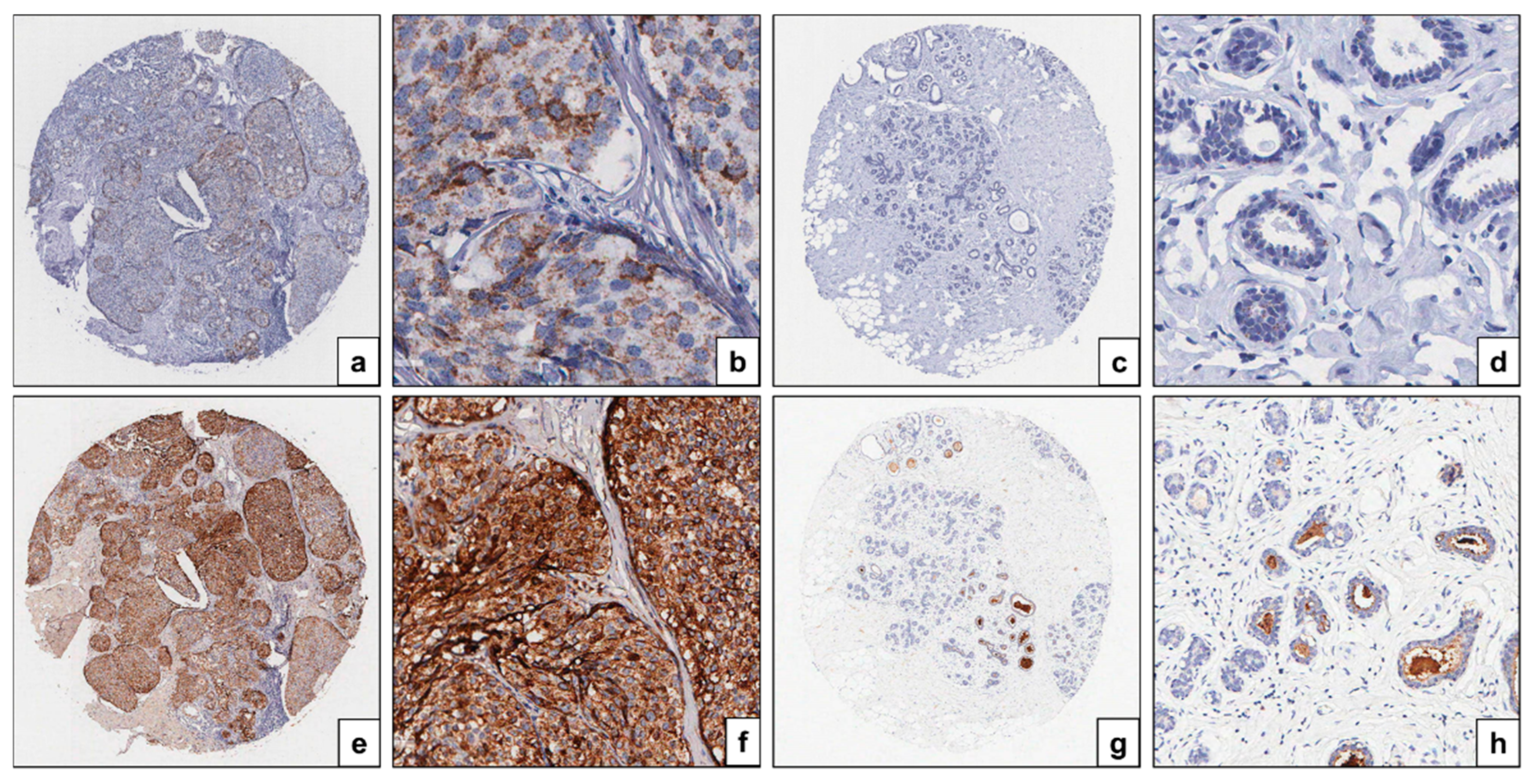
Figure 3.
Box plots of HE4 mRNA in situ hybridization (ISH) staining scores (a) and immunohistochemical (IHC) staining scores in ductal carcinoma in situ (DCIS) and adjacent normal breast tissues. The whiskers show the maximum and minimum values, with the exception of outliers (circles).
Figure 3.
Box plots of HE4 mRNA in situ hybridization (ISH) staining scores (a) and immunohistochemical (IHC) staining scores in ductal carcinoma in situ (DCIS) and adjacent normal breast tissues. The whiskers show the maximum and minimum values, with the exception of outliers (circles).
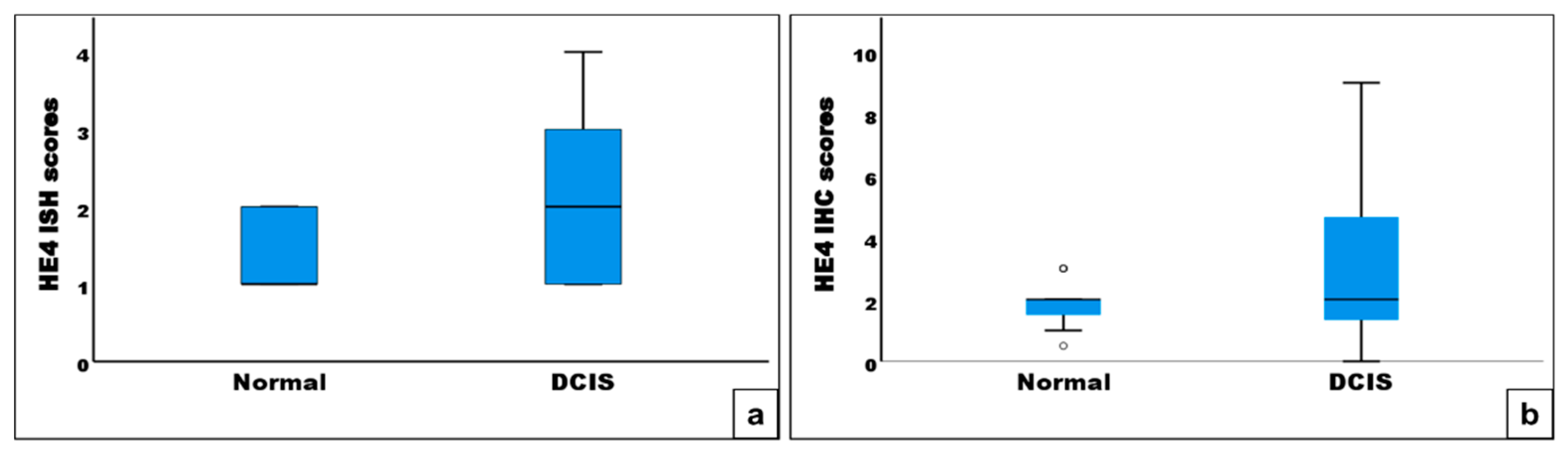
Figure 4.
Prognostic role of HE4 expression in breast cancer assessed using BreastMark.
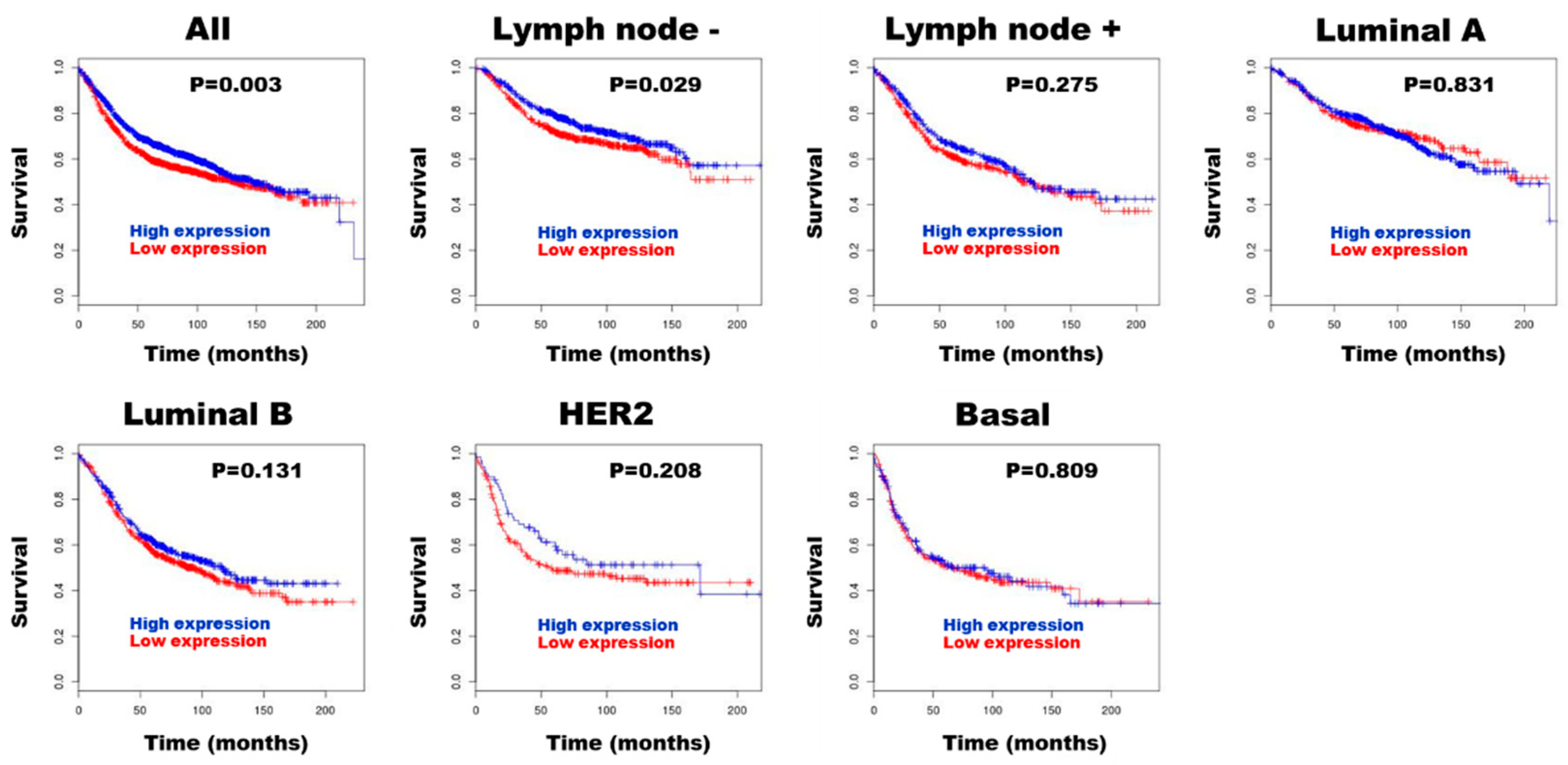

Table 1.
Correlation between serum HE4 levels and clinicopathologic parameters in patients with ductal carcinoma in situ.
Table 1.
Correlation between serum HE4 levels and clinicopathologic parameters in patients with ductal carcinoma in situ.
| Characteristics | Serum HE4 levels Number (Mean ± S.D.) |
p value |
|---|---|---|
| Menopause | < 0.05 | |
| Pre | 27 (35.3 ± 6.4) | |
| Post | 32 (42.9 ± 14.4) | |
| Size (cm) | 0.881 | |
| < 2.8 | 36 (39.6 ± 12.8) | |
| ≥ 2.8 | 23 (39.1 ± 10.8) | |
| Nuclear grade | 0.516 | |
| 1 | 1 (31.3) | |
| 2 | 27 (37.9 ± 9.1) | |
| 3 | 31 (40.9 ± 14.1) | |
| Comedo-type necrosis | 0.594 | |
| No | 10 (37.5 ± 10.3) | |
| Yes | 49 (39.8 ± 12.3) | |
| Stromal TILs density score | 0.716 | |
| 1 | 39 (40.3 ± 11.6) | |
| 2 | 19 (37.6 ± 13.0) | |
| 3 | 1 (41.7) | |
| Estrogen receptor- α | 0.868 | |
| Negative | 25 (39.1 ± 14.5) | |
| Positive | 34 (39.7 ± 9.9) | |
| HER-2 | 0.692 | |
| Negative | 31 (38.8 ± 11.5) | |
| Positive | 28 (40.1 ± 12.6) | |
| Molecular subtypes | 0 | |
| HR+/HER2- | 27 (38.5 ± 10.3) | |
| HR+/HER2+ | 11 (41.2 ± 7.3) | |
| HR-/HER2+ | 17 (39.4 ±15.3) | |
| Triple-negative | 4 (41.4 ± 20.2) | |
| Recurrence | 0.222 | |
| No | 53 (40.1 ± 12.3) | |
| Yes | 6 (33.8 ± 6.9) |
S.D., standard deviation; ns, not significant; TILs, tumor infiltrating lymphocytes.
Table 2.
Crosstabulation of HE4 status by mRNA RNAscope in situ hybridization and protein immunohistochemistry in DCIS tissues.
Table 2.
Crosstabulation of HE4 status by mRNA RNAscope in situ hybridization and protein immunohistochemistry in DCIS tissues.
| RNAscope in situ hybridization | Immunohistochemistry | Total | Concordance | κ value | p value | |
| Low | High | |||||
| Low High Total |
64 1 65 |
10 24 34 |
77 25 99 |
88.9 | 0.658 | < 0.001 |
Table 3.
Relationship between HE4 mRNA and protein expression and clinicopathologic parameters in ductal carcinoma in situ.
Table 3.
Relationship between HE4 mRNA and protein expression and clinicopathologic parameters in ductal carcinoma in situ.
| Characteristics | High mRNA HE4 expression N/total N (%) | p value | High protein HE4 expression N/total N (%) | p value |
| Menopause | 0.525 | 0.942 | ||
| Pre | 14/53 (26.4) | 18/53 (34.0) | ||
| Post | 11/46 (23.9) | 16/46 (34.8) | ||
| Size (cm) | 0.689 | 0.108 | ||
| < 2.8 | 15/56 (26.8) | 23/56 (41.1) | ||
| ≥2.8 | 10/43 (23.3) | 11/43 (25.6) | ||
| Nuclear grade | 0.129 | 0.068 | ||
| 1 | 1/3 (33.3) | 1/3 (33.3) | ||
| 2 | 17/55 (30.9) | 25/55 (45.5) | ||
| 3 | 7/41 (17.1) | 8/41 (19.5) | ||
| Comedo-type necrosis | 0.080 | < 0.05 | ||
| No | 9/23 (39.1) | 13/23 (56.5) | ||
| Yes | 16/76 (21.1) | 21/76 (27.6) | ||
| Stromal TILs density score | < 0.05 | < 0.05 | ||
| 1 | 22/67 (32.8) | 28/67 (41.8) | ||
| 2 | 3/30 (10.0) | 6/30 (20.0) | ||
| 3 | 0/2 (0) | 0/2 (0) | ||
| Estrogen receptor- α | < 0.01 | < 0.001 | ||
| Negative | 4/40 (10.0) | 5/40 (12.5) | ||
| Positive | 21/59 (35.6) | 29/59 (49.2) | ||
| HER-2 | < 0.05 | < 0.001 | ||
| Negative | 18/54 (33.3) | 27/54 (50.0) | ||
| Positive | 7/45 (15.6) | 7/45 (15.6) | ||
| Molecular subtypes | 0.099 | < 0.01 | ||
| HR+/HER2- | 17/48 (35.4) | 25/48 (52.1) | ||
| HR+/HER2+ | 4/16 (25.0) | 4/16(25.0) | ||
| HR-/HER2+ | 3/29 (10.3) | 3/29 (10.3) | ||
| Triple-negative | 1/6 (16.7) | 2/6 (33.3) | ||
| Recurrence | 0.688 | 0.489 | ||
| No | 22/90 (24.4) | 30/90 (33.3) | ||
| Yes | 3/9 (33.3) | 4/9 (44.4) |
N, number; TILs, tumor infiltrating lymphocytes.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



