
Submitted:
17 March 2025
Posted:
19 March 2025
You are already at the latest version
Abstract
Fungal infections occurring across the kingdom boundaries, a novel phenomenon to humans, will be discussed herein through the lens of plant pathogens that are now recognized as infecting humans. We highlight major pathogens among them, such as Fusarium species, Exserohilum rostratum, Sporothrix schenckii, and the more recently identified pathogen, Chondrostereum purpureum, which exemplify a wide spectrum of clinical manifestations ranging from superficial keratitis and lymphocutaneous infections to central nervous system involvement and deep-seated abscesses. This review compiles epidemiological data, detailed case studies and outbreak reports, including the 2012 Exserohilum rostratum meningitis outbreak in the USA and a solitary case of C. purpureum infection in a plant mycologist from Kolkata, India. This Reviews critically appraises diagnostic strategies that amalgamate traditional culture methods, imaging modalities and cutting-edge molecular techniques (e.g., PCR, DNA sequencing and MALDI-TOF mass spectrometry) to mitigate the challenges associated with rapid and accurate determination of pathogens. Several therapeutic strategies are discussed in depth, with the emphasis that pharmacological and surgical interventions should be based on the specific pathogen and clinical setting. The review also highlights the other public health and agricultural consequences of these infections and the potential contribution of environmental factors like climate change and agricultural fungicide use to pathogen evolution. This synthesis advocates for a One Health approach by endeavours to unite clinical medicine, plant pathology, and environmental science within the production of evidence, so as to inform future strategies for the surveillance, diagnosis and management of these complex and evolving infectious threats.
Keywords:
Cross-kingdom infections
; Fungal pathogens
; Fusarium
; Exserohilum rostratum
; Sporothrix schenckii
; Chondrostereum purpureum
; Outbreak management
; One Health
; Agricultural biosecurity
; Infectious diseases
; Epidemiology
Introduction
One recently published and alarming trend is cross-kingdom infections and cross pathogenicity with fungi formerly considered to be plant pathogens primarily being reported to infect humans. This parchment fungus is able to infect hosts from various kingdoms, contradicting the ubiquitous belief which contends that a particular fungus can only infect one type of host (Adalja et al., 2019). Fusarium species, which cause keratitis and systemic infections, are classic examples, as is Exserohilum rostratum, which was responsible for a national outbreak of fungal meningitis through the injection of contaminated steroids. Another organism that follows this trend is Sporothrix schenckii, the etiologic agent of sporotrichosis, or “rose gardener’s disease,” which enters the human host via traumatic inoculation of contaminated plant material.
We present here a more recent case, unique but substantial, with the fungal agent Chondrostereum purpureum, better known for its role in Silver Leaf disease in plants, reported in Kolkata, India. This case not only is an example of a plant pathogen crossing a species barrier but also indicates a potential expansion in the variety of fungal diseases that humans may experience − thus showcasing the importance of cross pathogenicity (Almuqamam et al., 2024; Balique et al., 2015). These developing infections are explained through the confluence of climate change, widespread agricultural use of the fungicide azoles, and increased human exposure to environmental fungi, which together are creating ideal environments for infections that do not follow traditional paradigms in either clinical or agricultural settings.
The aim of this overview is to outline documented cross-kingdom mycoses, with emphasis on the cross pathogenic potential of plant pathogens to human disease. Herein we will summarize epidemiologic data, case studies with diverse fungal pathogens like Fusarium, Exserohilum, Sporothrix, Alternaria, Bipolaris , and (De Hoog & Horré, 2002) the recent emerging pathogen Chondrostereum purpureum. It will assess diagnostic approaches that span traditional culture-based methods and novel molecular techniques, such as DNA sequencing and next-generation sequencing, to identify these rare pathogens accurately. The review also covers therapeutic strategies and clinical outcomes, highlighting the difficulties in controlling infections due to pathogens not normally linked to human disease, and also considers the environmental, occupational and regulatory determinants of the emergence and spread of these pathogens. Through exploring these dimensions, the review identifies current knowledge gaps and reinforces the need for integrated, multidisciplinary approaches, including a One Health approach, to combat this emerging threat.
These fungi should be viewed as serious threats to both human health and agriculture due to the increasing rates of cross-kingdom infections and the potential of these fungi to infect different hosts (Sun et al., 2020). These infections commonly have non-specific clinical features which can lead to significant delays in specific diagnosis and treatment (especially in immunocompromised patients). Emerging and subsequent outbreaks, including the large, multi-state outbreak of Exserohilum rostratum fungal meningitis, have demonstrated the potential of a rapid, widespread public health emergency when plant-related fungi can breach human barriers (Anaissie et al., 1989; Nnadi & Carter, 2021). Plant pathogenic fungi are already responsible for major economic losses in agriculture due to crop diseases. Their dual role as significant agricultural pests and potential human pathogens, because of cross pathogenicity, increases the need for surveillance and practical biosecurity (Ekwomadu & Mwanza, 2023).
Fungal infections in diverse kingdoms characterize a complex epidemiology pattern of sporadicity and high epidemic spread potential. While less common than the mycoses that humans commonly acquire, such infections frequently occur among those with high environmental or occupational exposure—agricultural workers and plant researchers, for example—particularly in the presence of immunosuppression (Wang et al., 2024). Major outbreaks, such as the 2012 Exserohilum rostratum meningitis outbreak in the United States, showcase how breakdowns in the pharmaceutical quality assurance pipeline can convert a plant pathogenic agent into an important risk to human health that will impact hundreds of people spanning multiple states (Matrose et al., 2021). In the United States, the geographical distribution is also significant; areas with warm, humid climates combined with intensive agricultural activity are more likely to report cases due to the ideal conditions for both fungal growth and dissemination of spores, while isolated cases in temperate areas highlight the global nature of these infections (Gkoutselis et al., 2021).
To reduce the risk of cross-kingdom transmission and protect food security and public health, integrated management approaches must account for the factors that influence the environmental and human health, as well as the livelihood of communities (Kirzinger et al., 2011). Overall, the convergence of plant pathology and medical mycology among these emerging infections emphasizes the need for increased surveillance, better diagnostic and therapeutic modalities, and stronger linkages between these two sectors (Köhler et al., 2017). This review should serve as a useful resource for the scientific community to help researchers, clinicians and government workers navigate the challenges posed by these unusual but important mycoses.
Overview of Plant Pathogenic Fungi
Plant pathogenic fungi represent a diverse assemblage spanning several taxonomic groups, primarily within the Ascomycota and Basidiomycota phyla. Key groups include:
Fusarium species are well-known both as devastating plant pathogens and as opportunistic human pathogens, responsible for diseases such as keratitis and systemic infections (Nucci & Anaissie, 2007).
Exserohilum species, notably Exserohilum rostratum, have gained attention following outbreaks in human populations linked to contaminated medical products (Katragkou et al., 2014).
Sporothrix schenckii is another prominent ascomycete, best known as the causative agent of sporotrichosis (“rose gardener’s disease”), which typically enters through traumatic inoculation from plant material (Barros et al., 2011).
Other genera such as Alternaria and Bipolaris—members of the Dothideomycetes—are primarily associated with plant diseases but have also been implicated in respiratory and sinus infections in humans (Pinto & Patriarca, 2016).
Chondrostereum purpureum, a fungus primarily associated with Silver Leaf disease in trees of the Rosaceae family, is a notable example of a plant pathogen that has recently been documented to cause human infection (Dutta & Ray, 2023).
This classification underscores the fact that while these fungi share a common ecological niche as plant pathogens, they encompass a wide range of morphologies, life cycles, and pathogenic strategies.
Mechanisms of Cross-Kingdom Infection
Plant pathogenic fungi have developed sophisticated strategies to establish infection in their host plants and maintain it. Fungal spores stick to plant surfaces via hydrophobic interactions and secreted adhesives that promote germination (Kim et al., 2020). Once established, most these fungi develop specialized structures (e.g. appressoria) that create both a mechanical force and secrete an arsenal of plant cell wall degrading enzymes (e.g. cellulases, pectinases, xylanases) (Van Baarlen et al., 2007). These enzymes degrade the plant cell wall, which facilitates the fungus to breach the cuticle and establish infection. At the same time, the fungi secrete toxins and protein effectors that disrupt the plant’s immune responses in the infected cells, sometimes inducing localized cell death (Sharma et al., 2014). This combination of physical penetration and biochemical assault not only aids in initial colonization but also enables systemic spread throughout the host, highlighting the complex interplay between fungal virulence factors and plant defense mechanisms (Rodriguez & Roossinck, 2012).
In contrast, upon entering human cells, these pernicious plant pathogens encounter a fundamentally different host environment. In humans it most commonly occurs through inhalation of aerosolized spores or through direct inoculation of skin lesions, particularly in people with substantial environmental or occupational exposure (Sukumaran et al., 2022). Speaking of which, once the pathogen gets in, it faces the daunting challenges of the human immune system and elevated body temperatures. Examples include ocular infections (keratitis) due to Fusarium species and invasive post-exposure infection following contaminated medical interventions (Szaliński et al., 2021). The first lines of defense for the human host rely on the innate immune system, where phagocytic cells (macrophages and neutrophils) recognize fungal cell wall components through pattern recognition receptors and trigger inflammatory responses (Karthikeyan et al., 2011). This is supplemented by the adaptive immune responses, especially T-cell mediated. This is complemented by adaptive immune responses, notably T-cell mediated immunity, which is critical for clearing the infection (Yang et al., 2021). However, these pathogens often deploy evasion strategies such as biofilm formation and the secretion of immunomodulatory molecules, which help them persist despite the host’s defenses (Cintra et al., 2024).
A comparative examination of these routes to infection shows both commonalities and divergence. Effective adhesion, enzymatic muscular degradation, and effector secretion are all necessary for plant and human infections to take place (Michelet et al., 2019). But the main challenges are different: plant pathogens have to deal with the stiff, carbohydrate-rich cell walls of plants and in humans they have to navigate a more complex, higher temperature environment with a multivalent immune system. Key molecular factors such as surface adhesins and secreted effectors are involved in host specificity (Fernandes et al., 2023). In plants, those factors have been adapted to identify and bind to the components of plant cell walls, and in humans, they have to bind to other receptors on various human cells and do its job efficiently at temperatures conducive to human survival (Sukumaran et al., 2022).
Thermotolerance, in particular, appears to control the capacity of a pathogen to cross the species barrier. Though, fungi that evolve and survive in both the settings display unique metabolic adjustments to live in the diverse physical and immunological surroundings offered by plant and human hosts (Félix et al., 2024). Herein, we have discussed the differences in infection strategies of two of the prevalent pathogenic fungal organisms but, considering the mixed etiology of the conditions especially in infected patients, it will require an integrated research approach to explore the underlying biology involved in cross-kingdom infections and their diagnostic and therapeutic options.
Documented Cases and Outbreaks
Cross-kingdom fungal infections, in which diseases usually caused by plant pathogens are able to infect humans, have been described in single cases and in limited outbreaks. Rare, these infections highlight major challenges for public health and agricultural biosecurity, especially as climate change, agricultural practices, and rising human contact with environmental fungi interact.
One of the most illustrative examples is the 2012 outbreak of fungal meningitis due to Exserohilum rostratum in the United States. In this case, contaminated batches of preservative-free methylprednisolone acetate — used in epidural steroid injections — accidentally injected fungal spores directly into patients’ systems (Katragkou et al., 2014). The outbreak itself unfolded quickly after an alert clinician recognized an unusual case of fungal meningitis, triggering an intensive investigation by state and federal agencies. Over the course of our investigation, nearly 750 cases in 20 states were documented. Not only did the incident reveal the catastrophic potential of a plant pathogen released through a contaminated medical product, but it also exposed critical failures of quality control and a breakdown in regulatory oversight (Pappas et al., 2013). The rapid spread and severity of the outbreak served as a wake-up call, prompting improvements in pharmaceutical compounding practices and reinforcing the importance of early detection and coordinated public health responses (Andes & Casadevall, 2013).
Besides large outbreaks, single cases also reveal much about cross-kingdom infection dynamics. One such striking case involved a 61-year-old self reported plant mycologist from Kolkata, India, who presented with deep neck infection which was ultimately traced back to being caused by the fungus, Chondrostereum purpureum (known primarily as the pathogen that causes Silver Leaf disease in plants) (Hamberg et al., 2021). The patient did not have significant underlying immunocompromising condition and he presented with symptoms of hoarseness voice, cough, recurrent pharyngitis, dysphagia, and anorexia. Dynamic imaging showed a right paratracheal abscess that was later aspirated with CT guidance. While standard fungal staining and culturing on Sabouraud dextrose agar for the initial molecular workup showed phenotypic features that were suggestive but inconclusive, DNA sequencing at reference high-throughput molecular liquid chromatography spectral flow vector centers confirmed the molecular identity of C. purpureum (Dutta & Ray, 2022). This case is particularly noteworthy because it marks the first documented instance of a human infection caused by this plant pathogen, emphasizing not only the evolving nature of fungal pathogenicity but also the potential for environmental fungi to breach traditional host barriers under certain conditions.
The Fusarium species also illustrate the plant pathogens with a dual nature. Fusarium species are well-known causal agents of major plant diseases as well as opportunistic pathogens in humans. They are known to cause diverse clinical manifestations—from superficial keratitis in contact lens wearers to life-threatening systemic infections in immunocompromised patients (Gupta et al., 2000). Although these infections are typically opportunistic, their presence in the agricultural and clinical settings highlight the ability of shared environmental exposure to be a pathway for cross-kingdom transmission (Antonissen et al., 2014).
Most of the Alternaria species are opportunistic pathogens causing a wide spectrum of infections in immunocompromised and immunocompetent hosts. More than 200 cases of alternariosis have been reported, with about 74% showing cutaneous or subcutaneous infections, while ocular infections (keratitis and endophthalmitis), rhinosinusitis, and onychomycosis are also reported (Pastor & Guarro, 2008). Classic laboratory diagnosis is dependent on morphological analysis of conidial traits and straightforward pigmentation, conidial chain characteristics, and their typical beak-like structures, in order to differentiate between genus and species level, that is to separate common species such as Alternaria alternata and A. tenuissima, from rare ones (Fernandes et al., 2023). Morphology-based misidentification, which is common, demonstrates the importance of molecular techniques for correct identification, including ITS region sequencing (Iturrieta-González et al., 2020).
The in vitro antifungal susceptibility studies show that although amphotericin B has unclear activity, fluconazole is systematically ineffective, azoles (itraconazole, voriconazole, and posaconazole) normally present moderate efficacy (MIC values often ≤0.5 mg/L) and other agents such as terbinafine and caspofungin have good activity (Hu et al., 2015). Clinically, major classes of infection dictate the treatment: ocular infections may require a combination of systemic and occasionally topical voriconazole, with adjunct measures including keratoplasty; rhinosinusitis is classically treated with amphotericin B and surgical debridement, whereas cutaneous or onychomycosis cases are generally treated with itraconazole (Botticher, 1966). Integrated diagnostic and therapeutic frameworks are critical to the optimization of outcomes in patients with Alternaria infections, particularly in severe or persistent cases.
These cases and outbreaks collectively provide a unified view of the epidemiology of cross-kingdom infections. They also reveal a tangled ecology where incidence is still low but the risk of swift, dramatic sequelae is high if pathogenic fungi spill over from their usual plant hosts into humans (Sharma et al., 2014). The events herein—the Exserohilum rostratum pandemic and the Chondrostereum purpureum infection - underscore the need for integrated surveillance systems, better diagnostics and coordinated public health interventions (Boonkorn et al., 2024). This also underlines the necessity of a One Health perspective, integrating agricultural, environmental, and clinical medicine disciplines for effective surveillance, management, and potential elimination of these emerging infectious risks (Katragkou et al., 2014).
Diagnostic Approaches
Fusarium species are an example of a class of fungal pathogen that shuttles between plants and humans. Fusarium infections are diagnosed in the clinical settings by a fusion of the traditional and advanced methods, ranging from keratitis in contact lens users, to the invasive disseminated disease seen in immunocompromised patients (van Diepeningen et al., 2015). Conventional practices consist of culture of clinical specimens on Sabouraud dextrose agar with typical rapid-growth, cottony colonies of Fusarium. Examination microscopically also reveals characteristic lands of macro and microconidia which helps in narrowing down the identification. However, due to the morphological similarities that exist between filamentous fungi, molecular techniques including PCR amplification and sequencing of specific regions of genes and MALDI-TOF mass spectrometry, have become of increasing importance for the accurate confirmation of diagnosis (Mule et al., 2005).
Exserohilum rostratum, an additional member of this family that was initially identified as a plant pathogen, gained infamy after being implicated in a fungal meningitis outbreak in 2012 associated with contaminated steroid injections. In these cases, diagnosis started with imaging studies — CT and MRI scans — to assess the extent of involvement of the central nervous system. Fungal stains and culture methods were used: methods included Gomori's Methenamine silver stain, which is used to visualize septate hyphae in specimens and culture methods using appropriate media to isolate the organism (Sharma et al., 2014). When PCR and subsequent sequencing placed Exserohilum among dematiaceous fungi, it was crucial in differentiating between them, and confirmed that the organism was responsible for the outbreak's spread.
Sporothrix schenckii, the most well-known cause of sporotrichosis or “rose gardener’s disease,” usually enters its human host through traumatic inoculation with contaminated plant material. Clinically the infection is usually presented as lymphocutaneous syndrome with nodular lesions that follow lymphatic routes (Oliveira et al., 2014). The fungus demonstrates dimorphism—growing on culture as a mold at room temperature and in a yeast form at body temperature—upon which diagnostic evaluation is based primarily on a high index of clinical suspicion backed by culture. Yeast cells can be demonstrated in tissue with histopathological studies using special fungal stains and have been identified with modern molecular methods, like PCR, which have contributed to its diagnosis, especially in atypical presentations (Barros et al., 2011).
The diagnostic approach for Alternaria infections begins with a thorough clinical evaluation, where patient history and the specific clinical presentation—be it cutaneous, ocular, or sinonasal—raise initial suspicion. Laboratory analysis then plays a crucial role, starting with the cultivation of clinical specimens on media such as Sabouraud dextrose agar, where Alternaria typically forms slow-growing, pigmented colonies (Pastor & Guarro, 2008). Microscopic examination of these colonies focuses on key morphological features such as the arrangement of conidia, distinctive pigmentation, and the presence of characteristic beak-like structures, which aid in differentiating common species like Alternaria alternata and A. tenuissima from others (Nagrale et al., 2016). Given the potential for misidentification when relying solely on morphology, molecular diagnostic techniques, particularly PCR amplification and sequencing of the internal transcribed spacer (ITS) region, are integrated into the workflow to ensure precise species-level identification (Kustrzeba-Wójcicka et al., 2014). This combination of clinical, morphological, and molecular methods forms a robust framework that enhances diagnostic accuracy and guides effective, targeted antifungal therapy.
A particularly intriguing case involves Chondrostereum purpureum, a fungus primarily known for causing Silver Leaf disease in plants, which was identified as the pathogen in a rare human infection reported in Kolkata, India. The affected patient, a plant mycologist, presented with symptoms including hoarseness, cough, dysphagia, and was found to have a paratracheal abscess on CT imaging (Dutta & Ray, 2022). While initial laboratory work—such as Gram staining and culture on Sabouraud dextrose agar—yielded inconclusive results, the use of advanced molecular diagnostics, including DNA sequencing performed at a specialized reference center, ultimately confirmed the presence of C. purpureum (Hamberg et al., 2021). This case underscores the necessity of integrating traditional diagnostic modalities with cutting-edge molecular techniques, especially when confronting rare or emerging pathogens.
Treatment and Management Strategies
Managing infections caused by plant pathogenic fungi that cross into human hosts involves a multifaceted approach, combining both medical and surgical interventions tailored to the organism and the clinical scenario. Below, we discuss the treatment strategies for each of the key fungi described in this review.
Fusarium species are notorious for their ability to cause a spectrum of diseases ranging from superficial keratitis to life-threatening invasive infections in immunocompromised patients (Antonissen et al., 2014). For ocular infections such as keratitis, treatment typically involves topical antifungal agents (e.g., natamycin) and may be supplemented with systemic therapy. In cases of invasive disease, systemic antifungals like amphotericin B and voriconazole are commonly used, although Fusarium’s intrinsic resistance to many agents often necessitates combination therapy (Gupta et al., 2000). In some instances, surgical debridement is required to remove necrotic tissue and reduce fungal load.
Exserohilum rostratum came to prominence following the 2012 outbreak of fungal meningitis linked to contaminated steroid injections. In managing such central nervous system (CNS) infections, aggressive systemic antifungal therapy is essential (Katragkou et al., 2014). High-dose regimens of voriconazole or amphotericin B are typically employed, sometimes in combination, to achieve therapeutic concentrations in the CNS. Due to the potential toxicities associated with these medications and the difficulty of drug penetration into the brain, treatment is carefully monitored, and adjunctive surgical interventions may be necessary in cases involving abscess formation or localized collections (Pappas et al., 2013).
The causative agent of sporotrichosis, Sporothrix schenckii, is classically associated with cutaneous and lymphocutaneous infections following traumatic inoculation from contaminated plant material (Barros et al., 2011). Itraconazole is the treatment of choice for most cases, with therapy often extending over several months to ensure complete resolution. In more severe or disseminated cases, especially in immunocompromised hosts, amphotericin B may be initiated before transitioning to oral itraconazole (Oliveira et al., 2014). Historically, potassium iodide was also used for cutaneous forms of sporotrichosis, particularly in resource-limited settings.
In the unique and first documented human infection caused by Chondrostereum purpureum, a comprehensive treatment strategy was critical. The patient, a plant mycologist from Kolkata, presented with a paratracheal abscess and systemic symptoms. Management included CT-guided surgical drainage of the abscess followed by a prolonged course of antifungal therapy (Hamberg et al., 2021). Oral voriconazole was administered—a high loading dose followed by a maintenance regimen over a 60-day period—with close monitoring over two years to detect any recurrence or late complications (Dutta & Ray, 2023).
Though primarily recognized as plant pathogens, Alternaria and Bipolaris species have occasionally been implicated in human infections, particularly in the respiratory tract or sinuses, as well as in cutaneous manifestations in vulnerable populations (Hu et al., 2015). Treatment strategies for these infections are based on the susceptibility profile of the isolate. Azole antifungals such as itraconazole and voriconazole are often effective, while amphotericin B may be reserved for severe or refractory cases. In select instances of localized infection, surgical excision may serve as an adjunct to medical therapy (Pastor & Guarro, 2008).
The management of these cross-kingdom fungal infections underscores the necessity for individualized treatment protocols that integrate both surgical and pharmacological strategies. Early and precise diagnosis, supported by advanced molecular techniques and imaging modalities, is critical to tailoring effective therapy and mitigating the risk of recurrence (Sharma et al., 2014). As these pathogens continue to evolve, a coordinated One Health approach—bridging clinical medicine, agriculture, and environmental science—remains essential for optimizing patient outcomes and preventing future outbreaks.
Discussion
Cross-kingdom fungal infections have emerged as a significant concern, bridging the gap between traditional plant pathology and human infectious diseases. This review has highlighted several key pathogens—including Fusarium species, Exserohilum rostratum, Sporothrix schenckii, Chondrostereum purpureum, and opportunistic fungi like Alternaria and Bipolaris—that underscore the dynamic and evolving nature of fungal pathogenicity. Although these infections are relatively rare, their occurrence in both isolated cases and outbreaks emphasizes the need for heightened awareness and a coordinated response across clinical and agricultural settings.
The ability of these fungi to transition from infecting plants to causing human disease is underpinned by a combination of virulence factors and adaptive mechanisms. For instance, Fusarium species not only produce cell wall–degrading enzymes and toxins that facilitate plant tissue colonization but also possess traits that allow them to invade human tissue, particularly in immunocompromised individuals. Similarly, the 2012 Exserohilum rostratum outbreak illustrated how breaches in medical sterility could introduce plant pathogens into the human body, resulting in severe CNS infections. The case of Sporothrix schenckii, traditionally associated with sporotrichosis in gardeners, further demonstrates how traumatic inoculation with contaminated plant material can lead to cutaneous and lymphocutaneous infections.
The singular case of Chondrostereum purpureum infection in a plant mycologist from Kolkata underscores the potential for even rare pathogens to cross species barriers under the right conditions. This case, along with others, illustrates how advanced diagnostic techniques—combining imaging, culture-based methods, and state-of-the-art molecular diagnostics—are essential for accurately identifying these atypical infections. Despite the advances, challenges persist. Traditional methods can be time-consuming and sometimes inconclusive, leading to delays in treatment. Emerging technologies such as multiplex PCR and MALDI-TOF mass spectrometry hold promise in overcoming these diagnostic hurdles by providing rapid and precise identification of fungal pathogens.
Therapeutic strategies must also be tailored to address the unique challenges posed by cross-kingdom infections. The treatment modalities discussed in this review range from topical and systemic antifungals for superficial infections to aggressive, combination therapies for invasive diseases. The complexity of these infections often necessitates an integrated approach that includes both surgical intervention and prolonged antifungal therapy, as exemplified by the management of the Chondrostereum purpureum case.
Importantly, the emergence of cross-kingdom infections reflects broader environmental and anthropogenic influences. Factors such as climate change, increased use of agricultural fungicides, and heightened exposure to environmental fungi contribute to the evolution of these pathogens. A One Health approach—which integrates human, animal, and environmental health—is crucial in addressing these interconnected challenges. By fostering collaboration across disciplines, we can develop more effective surveillance, diagnostic, and treatment strategies to mitigate the impact of these emerging infections.
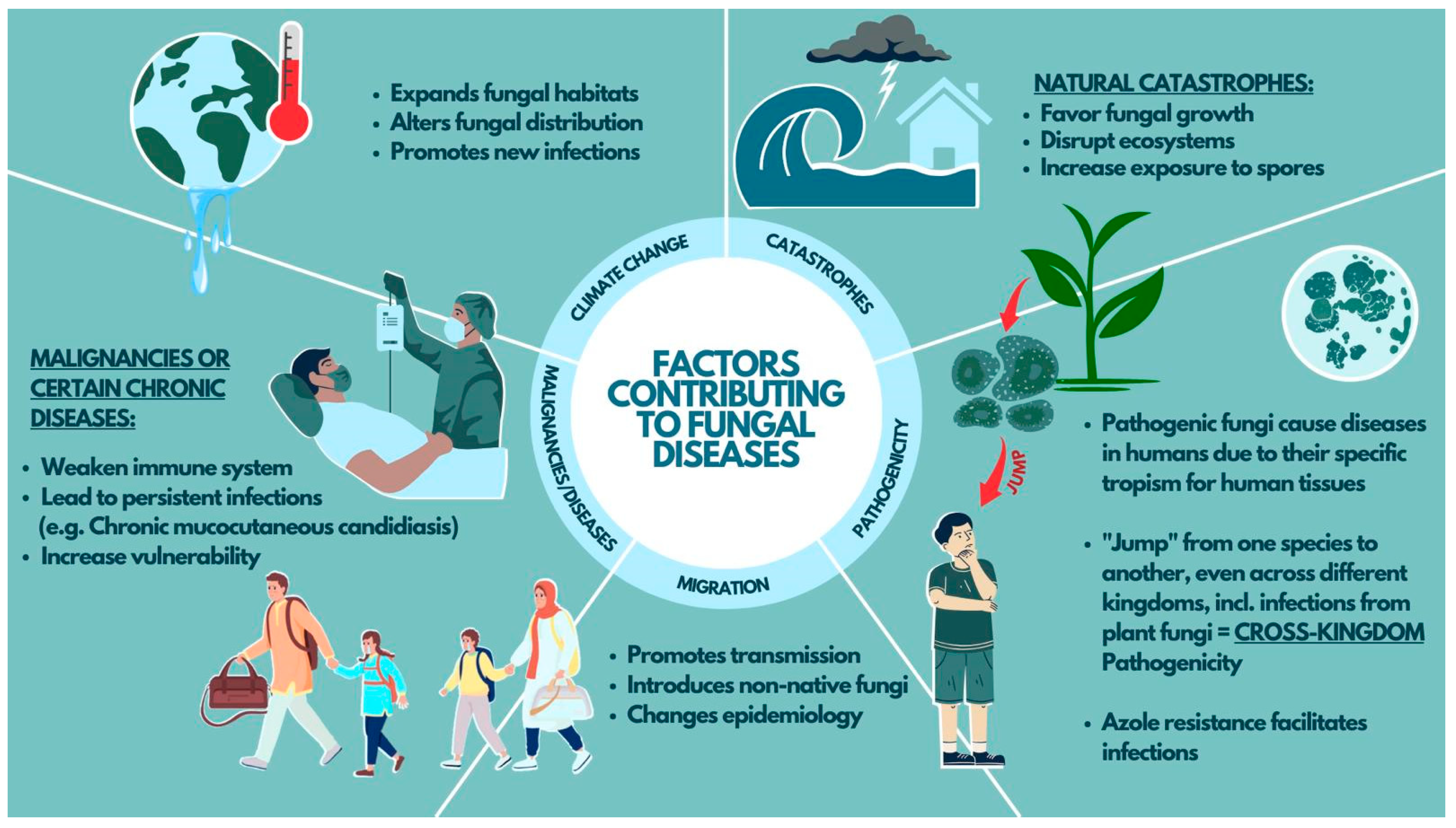
An illustrated overview of some of the important factors contributing to fungal diseases is presented in Figure 1, highlighting the key drivers such as climate change, natural catastrophes, migration, azole resistance, host susceptibility due to various health conditions, and cross-kingdom pathogenicity.
Author Contributions
Equal contributions in conceptualization, investigation, methodology, formal writing, and editing by Ahmad Reza Rezaei & Tarum Mishra.
Funding
No funding was obtained for this work
Conflict of Interest
The author declares that there is no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Ethics Approval
Not applicable
Consent of Participate
Not applicable
Data Availability
Not applicable
References
- Adalja, A. A., Watson, M., Toner, E. S., Cicero, A., & Inglesby, T. V. (2019). Characteristics of microbes most likely to cause pandemics and global catastrophes. Global catastrophic biological risks, 1-20.
- Almuqamam, M., Gonzalez, F. J., Sharma, S., & Kondamudi, N. P. (2024). Deep neck infections. In StatPearls [Internet]. StatPearls Publishing.
- Anaissie, E. J., Bodey, G. P., & Rinaldi, M. G. (1989). Emerging fungal pathogens. European Journal of Clinical Microbiology and Infectious Diseases, 8, 323-330.
- Andes, D., & Casadevall, A. (2013). Insights into fungal pathogenesis from the iatrogenic epidemic of Exserohilum rostratum fungal meningitis. Fungal Genetics and Biology, 61, 143-145.
- Antonissen, G., Martel, A., Pasmans, F., Ducatelle, R., Verbrugghe, E., Vandenbroucke, V., Li, S., Haesebrouck, F., Van Immerseel, F., & Croubels, S. (2014). The impact of Fusarium mycotoxins on human and animal host susceptibility to infectious diseases. Toxins, 6(2), 430-452.
- Balique, F., Lecoq, H., Raoult, D., & Colson, P. (2015). Can plant viruses cross the kingdom border and be pathogenic to humans? Viruses, 7(4), 2074-2098.
- Barros, M. B. d. L., de Almeida Paes, R., & Schubach, A. O. (2011). Sporothrix schenckii and Sporotrichosis. Clinical microbiology reviews, 24(4), 633-654.
- Boonkorn, Y., Tongsri, V., Piasai, O., & Songkumarn, P. (2024). Characterization, pathogenicity and fungicide response of Exserohilum rostratum causing leaf spot on rice in Thailand. European Journal of Plant Pathology, 170(3), 549-566.
- Botticher, W. W. (1966). Alternaria as a possible human pathogen. Sabouraudia: Journal of Medical and Veterinary Mycology, 4(4), 256-258.
- Cintra, M. E. C., da Silva Dantas, M., Al-Hatmi, A. M. S., Bastos, R. W., & Rossato, L. (2024). Fusarium Keratitis: A Systematic Review (1969 to 2023). Mycopathologia, 189(5), 74.
- De Hoog, G. S., & Horré, R. (2002). Molecular taxonomy of the Alternaria and Ulocladium species from humans and their identification in the routine laboratory. Mycoses, 45(7-8), 259-276.
- Dutta, S., & Ray, U. (2022). P187 Paratracheal abscess by plant fungus Chondrostereum purpureum. First case report of human infection. Medical Mycology, 60(Supplement_1), myac072P187.
- Dutta, S., & Ray, U. (2023). Paratracheal abscess by plant fungus Chondrostereum purpureum-first case report of human infection. Medical Mycology Case Reports, 40, 30-32.
- Ekwomadu, T. I., & Mwanza, M. (2023). Fusarium fungi pathogens, identification, adverse effects, disease management, and global food security: A review of the latest research. Agriculture, 13(9), 1810.
- Félix, C., Meneses, R., Gonçalves, M. F. M., Duarte, A. S., Jorrín-Novo, J. V., Van de Peer, Y., Deforce, D., Van Nieuwerburgh, F., Alves, A., & Esteves, A. C. (2024). How temperature modulates the expression of pathogenesis-related molecules of the cross-kingdom pathogen Lasiodiplodia hormozganensis. Science of the Total Environment, 927, 171917.
- Fernandes, C., Casadevall, A., & Gonçalves, T. (2023). Mechanisms of Alternaria pathogenesis in animals and plants. FEMS Microbiology Reviews, 47(6), fuad061.
- Gkoutselis, G., Rohrbach, S., Harjes, J., Obst, M., Brachmann, A., Horn, M. A., & Rambold, G. (2021). Microplastics accumulate fungal pathogens in terrestrial ecosystems. Scientific Reports, 11(1), 13214.
- Gupta, A. K., Baran, R., & Summerbell, R. C. (2000). Fusarium infections of the skin. Current opinion in infectious diseases, 13(2), 121-128.
- Hamberg, L., Saksa, T., & Hantula, J. (2021). Role and function of Chondrostereum purpureum in biocontrol of trees. Applied Microbiology and Biotechnology, 105, 431-440.
- Hu, W., Ran, Y., Zhuang, K., Lama, J., & Zhang, C. (2015). Alternaria arborescens infection in a healthy individual and literature review of cutaneous alternariosis. Mycopathologia, 179, 147-152.
- Iturrieta-González, I., Pujol, I., Iftimie, S., García, D., Morente, V., Queralt, R., Guevara-Suarez, M., Alastruey-Izquierdo, A., Ballester, F., & Hernández-Restrepo, M. (2020). Polyphasic identification of three new species in Alternaria section Infectoriae causing human cutaneous infection. Mycoses, 63(2), 212-224.
- Karthikeyan, R. S., Leal Jr, S. M., Prajna, N. V., Dharmalingam, K., Geiser, D. M., Pearlman, E., & Lalitha, P. (2011). Expression of innate and adaptive immune mediators in human corneal tissue infected with Aspergillus or fusarium. Journal of Infectious Diseases, 204(6), 942-950.
- Katragkou, A., Pana, Z.-D., Perlin, D. S., Kontoyiannis, D. P., Walsh, T. J., & Roilides, E. (2014). Exserohilum infections: review of 48 cases before the 2012 United States outbreak. Sabouraudia, 52(4), 376-386.
- Kim, J. S., Yoon, S. J., Park, Y. J., Kim, S. Y., & Ryu, C. M. (2020). Crossing the kingdom border: Human diseases caused by plant pathogens. Environmental Microbiology, 22(7), 2485-2495.
- Kirzinger, M. W. B., Nadarasah, G., & Stavrinides, J. (2011). Insights into cross-kingdom plant pathogenic bacteria. Genes, 2(4), 980-997.
- Köhler, J. R., Hube, B., Puccia, R., Casadevall, A., & Perfect, J. R. (2017). Fungi that infect humans. Microbiology spectrum, 5(3), 10-1128.
- Kustrzeba-Wójcicka, I., Siwak, E., Terlecki, G., Wolańczyk-Mędrala, A., & Mędrala, W. (2014). Alternaria alternata and its allergens: a comprehensive review. Clinical reviews in allergy & immunology, 47, 354-365.
- Matrose, N. A., Obikeze, K., Belay, Z. A., & Caleb, O. J. (2021). Plant extracts and other natural compounds as alternatives for post-harvest management of fruit fungal pathogens: A review. Food Bioscience, 41, 100840.
- Michelet, C., Danchin, E. G. J., Jaouannet, M., Bernhagen, J., Panstruga, R., Kogel, K.-H., Keller, H., & Coustau, C. (2019). Cross-kingdom analysis of diversity, evolutionary history, and site selection within the eukaryotic macrophage migration inhibitory factor superfamily. Genes, 10(10), 740.
- Mule, G., Gonzalez-Jaen, M. T., Hornok, L., Nicholson, P., & Waalwijk, C. (2005). Advances in molecular diagnosis of toxigenic Fusarium species: a review. Food Additives and Contaminants, 22(4), 316-323.
- Nagrale, D. T., Sharma, L., Kumar, S., & Gawande, S. P. (2016). Recent diagnostics and detection tools: implications for plant pathogenic Alternaria and their disease management. Current trends in plant disease diagnostics and management practices, 111-163.
- Nnadi, N. E., & Carter, D. A. (2021). Climate change and the emergence of fungal pathogens. PLoS pathogens, 17(4), e1009503.
- Nucci, M., & Anaissie, E. (2007). Fusarium infections in immunocompromised patients. Clinical microbiology reviews, 20(4), 695-704.
- Oliveira, M. M. E., Almeida-Paes, R., Gutierrez-Galhardo, M. C., & Zancope-Oliveira, R. M. (2014). Molecular identification of the Sporothrix schenckii complex. Revista iberoamericana de micologia, 31(1), 2-6.
- Pappas, P. G., Kontoyiannis, D. P., Perfect, J. R., & Chiller, T. M. (2013). Real-time treatment guidelines: considerations during the Exserohilum rostratum outbreak in the United States. Antimicrobial Agents and Chemotherapy, 57(4), 1573-1576.
- Pastor, F. J., & Guarro, J. (2008). Alternaria infections: laboratory diagnosis and relevant clinical features. Clinical Microbiology and Infection, 14(8), 734-746.
- Pinto, V. E. F., & Patriarca, A. (2016). Alternaria species and their associated mycotoxins. Mycotoxigenic fungi: Methods and protocols, 13-32.
- Rodriguez, R. J., & Roossinck, M. (2012). Viruses, fungi and plants: cross-kingdom communication and mutualism. In Biocommunication of Fungi (pp. 219-227). Springer.
- Sharma, K., Goss, E. M., Dickstein, E. R., Smith, M. E., Johnson, J. A., Southwick, F. S., & van Bruggen, A. H. C. (2014). Exserohilum rostratum: characterization of a cross-kingdom pathogen of plants and humans. PLOS ONE, 9(10), e108691.
- Sukumaran, A., Ball, B., Krieger, J. R., & Geddes-McAlister, J. (2022). Cross-kingdom infection of macrophages reveals pathogen-and immune-specific global reprogramming and adaptation. MBio, 13(4), e01687-01622.
- Sun, S., Hoy, M. J., & Heitman, J. (2020). Fungal pathogens. Current biology, 30(19), R1163-R1169.
- Szaliński, M., Zgryźniak, A., Rubisz, I., Gajdzis, M., Kaczmarek, R., & Przeździecka-Dołyk, J. (2021). Fusarium keratitis—review of current treatment possibilities. Journal of Clinical Medicine, 10(23), 5468.
- Van Baarlen, P., Van Belkum, A., Summerbell, R. C., Crous, P. W., & Thomma, B. P. H. J. (2007). Molecular mechanisms of pathogenicity: how do pathogenic microorganisms develop cross-kingdom host jumps? FEMS Microbiology Reviews, 31(3), 239-277.
- van Diepeningen, A. D., Brankovics, B., Iltes, J., Van der Lee, T. A. J., & Waalwijk, C. (2015). Diagnosis of Fusarium infections: approaches to identification by the clinical mycology laboratory. Current fungal infection reports, 9, 135-143.
- Wang, S., He, B., Wu, H., Cai, Q., Ramírez-Sánchez, O., Abreu-Goodger, C., Birch, P. R. J., & Jin, H. (2024). Plant mRNAs move into a fungal pathogen via extracellular vesicles to reduce infection. Cell host & microbe, 32(1), 93-105.
- Yang, R.-B., Wu, L.-P., Lu, X.-X., Zhang, C., Liu, H., Huang, Y., Jia, Z., Gao, Y.-C., & Zhao, S.-Z. (2021). Immunologic mechanism of fungal keratitis. International Journal of Ophthalmology, 14(7), 1100.
Figure 1.
Key factors influencing fungal disease emergence include environmental changes, pathogenicity, migration, and host vulnerabilities.
Figure 1.
Key factors influencing fungal disease emergence include environmental changes, pathogenicity, migration, and host vulnerabilities.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



