
Submitted:
15 March 2025
Posted:
17 March 2025
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Long Covid is now regarded as a chronic disease that follows from an acute infection of SARS-CoV-2. Patients themselves were at the forefront of developing the scientific understanding of the disease, which was followed up by government related health institutions. This analysis describes how the patient led research initiated the development of the institutions’ “case definitions” of long Covid and which of these definitions is the more suited to providing a set of “diagnostic criteria” for long Covid.
Keywords:
Long Covid
; SARS-CoV-2
; COVID-19
; diagnosis
; patient reported outcomes
Introduction
Chronic diseases that occur after an acute viral infection are a well known phenomena including diabetes, Parkinsons disease, and cancer. “Long Covid” is now considered just such a chronic disease. This review intends to help the reader consolidate their understanding of how long Covid has been defined by patients and government affiliated institutions. It also aims to identify the candidate definition that can be used to make a standardized set of diagnostic criteria.
The Genesis of the Term “Long Covid” and Its Synonyms
In May 2020, two months after the COVID-19 pandemic was declared by the WHO, patient-researchers who experienced “prolonged symptoms of COVID-19” published a report detailing the quantitative and qualitative data of the illness experience of 640 respondents [1]. They tracked the symptoms of patients with or without confirmed COVID-19 mostly, but not exclusively, two weeks after symptom onset. Approximately nine in ten respondents were symptomatic at eight weeks after the onset of symptoms [Table 1]. Respondents also volunteered what investigative tests they received during this time course. Data were also presented with symptoms grouped by “type” and COVID-19 test status. The patient-researchers also documented relapses of symptoms, as well as “fluctuations [of symptoms] both in the type… and intensity.”
At that time, the only “case definition” of COVID-19 was as an acute illness [Figure 1] [2]. These patient-investigators refrained from developing a definition or diagnostic criteria for “prolonged Covid-19 symptoms” as a separate disease state, but they were the first to quantify symptoms that extended past the “acute phase” of COVID-19 infection. Perhaps in this way the patients themselves can be said to have “made” the disease [3].
Though the phrase was not used in the patient-investigators’ report, “long Covid” has become the abbreviated form of “prolonged symptoms of COVID-19”. Another, closely aligned patient derived term, is “long haul Covid” [3]. Subsequent terms were developed by professional bodies, for instance, NICE [4], in the UK; the WHO [5]; and NASEM [6] and the CDC [7], both in the US: “post- COVID-19 syndrome”, “post-COVID-19 condition,” “post-acute sequelae of COVID-19,” and “chronic COVID syndrome.”
“Case Definition,” “Diagnostic Criteria” and the “Diagnostic Process”
“Case definition” is an epidemiological term which defines a disease entity by criteria (usually symptoms, clinical signs, and laboratory tests) which occurs within definite geographic and time boundaries. These boundaries are the “epidemiological criteria” of a case definition. A patient can be diagnosed as a “case” during an outbreak of a contagious disease in a particular locality when they experience symptoms in the timeframe that the contagion is endemic. An asymptomatic person can be diagnosed as a “case” if they only meet the epidemiological criteria, that is, if they come into contact with a patient suffering from the contagion. Another aspect of the epidemiological criteria of a case definition is to serve as a monitoring function. The rate of new case detection can be used to track the progress of an outbreak, whether it is expanding or contracting. A case definition is also applicable to non-communicable diseases. A “cancer cluster”, for example, is when a given type of cancer or cancers occur within a particular locality and timeframe. Once the epidemiological criteria of a case definition are removed, the remaining part of the case definition, when applied to a patient, becomes a “diagnostic criteria.”
When creating a case definition, there has to be some thought given to how accurate it will be. The aspects considered are whether the definition will successfully identify true cases, by preventing false negatives, and whether it will guard against misassigning a case, that is, minimizing false positives. “Sensitivity” is the ability to identify all true positives amongst false negatives and “specificity” is the ability to identify all true negatives amongst false positives. A case definition with perfect sensitivity would have no false negatives and a definition with perfect specificity would have no false positives. Usually, however, there is a trade off between the two. An example of balancing the competition between sensitivity and specificity is when the WHO revised the 1999 case definition of “influenza like illness” in 2011 [8]. The panellists opted to remove the phrase “absence of another diagnosis” from the 1999 definition. The intent was to allow patients with co-morbid diseases that could cause similar symptoms to be more readily defined as “true cases” of influenza; sensitivity of the new case definition would be increased. This would also necessarily, however, raise the chance that, say, a patient presenting due to a flare of asthma would be misclassified as a case of influenza; the asthmatic would be a false positive, which would count against the revised definition’s specificity. An example of a change that improves both sensitivity and specificity was when the panel also decided to remove “sore throat” from the 1999 definition, citing evidence that a sore throat was a negative predictor of influenza. This would enhance specificity and sensitivity as removing a qualifying symptom that actually correlated with the absence of the disease would reduce the false positive and false negative rates.
Medical diagnosis is a process of classifying a patient with a disease by interviewing a patient, conducting a physical examination, and interpreting laboratory tests. A physician is said to diagnose a “case” of a disease if the patient’s symptoms, clinical signs, and laboratory tests conform to a received definition of that disease. If these are either absent or only partly present, a separate disease classification may be relevant. The combination of the elements of a set of diagnostic criteria will also be subject to the same limitations of sensitivity and specificity that governed the derivation of a case definition. The discrimination between the various diagnostic probabilities, given a patient’s symptoms, signs, and laboratory results, is the measurable aim of the diagnostic process. Importantly, there are no “epidemiological criteria” involved in this diagnostic process.
Existing Case Definitions of Long Covid and Synonyms
There are four often cited case definitions for long Covid and synonymous terms: the WHO, NICE, NASEM, and the CDC [6]. Separate from these four, the RECOVER consortium maintain a disease registry and have produced a score based on a composite of symptoms, derived through data mining [9]. However, the consortium have yet to validate this score in another database, nor has the consortium constructed a case definition [9].
NICE Case Definition of “Post-COVID-19 Syndrome”
In December 2020, an “independent advisory expert panel” published the NICE case definition of “post-COVID-19 syndrome” [Figure 2] [4]. The definition stipulates that “post-COVID-19 syndrome” occurs twelve weeks after an “infection consistent with COVID-19” and classifies symptoms that occur four to twelve weeks after acute infection as “ongoing symptomatic COVID-19.” No symptoms are listed specifically, but they are described as occurring in “clusters… often overlapping which can fluctuate and change over time.” “Post-COVID-19 syndrome” can be diagnosed before or after twelve weeks so long as “symptoms are not explained by an alternative diagnosis.” The definition states that the term “long Covid” includes both “ongoing symptomatic COVID-19” and “post COVID-19 syndrome.” The definition does not mention functional impairment.
WHO Case Definition of “Post COVID-19 Condition”
In 2021, the WHO published their case definition for the “post COVID-19 condition.” The WHO definition noted the synonymous term “long Covid,” but preferred to use the former. The WHO used a two round Delphi consensus exercise to identify the diagnostic criteria for the “post COVID-19 condition,” which patients and patient-researchers participated in [Figure 3] [5]. The definition requires “probable or confirmed SARS CoV-2 infection” usually three months before the onset of symptoms, and symptoms must be present for at least two months and “cannot be explained by an alternative diagnosis.” The symptoms listed are not exhaustive but “fatigue, shortness of breath, [and] cognitive dysfunction” are described as “common.” Symptoms also “may…fluctuate or relapse over time… and generally have an impact on everyday functioning.” The definition states that there is no threshold number of symptoms required to make the “diagnosis,” though “symptoms involving different organs{sic} systems and clusters have been described.” The terms “fluctuate,” “relapse,” and “cluster” are also defined.
NASEM Case Definition of Long Covid
Though the WHO and NICE definitions have their differences, the approach taken by NASEM was very different. A committee was formed to create a definition for long Covid and, in 2023, a commercial marketing firm was contracted to conduct focus groups on the acceptability of the definition [Figure 4] [10]. The NASEM definition states long Covid “occurs after SARS-CoV-2 infection and is present for at least three months.” Also, “a complete enumeration of possible signs, symptoms, and diagnosable conditions of long Covid would have hundreds of entries.” The definition lists fourteen “manifest” symptoms and then lists nineteen separate diseases that can also “manifest” as long Covid. The definition states that SARS-CoV-2 infection is the initiator of long Covid, however, previous infections may have been “asymptomatic [and] unrecognized.” Long Covid can be “continuous from the time of acute SARS-CoV-2 infection” or have a delayed onset after an unspecified amount of time. The NASEM definition emphasises the importance of patient identity, stating that it can affect patients “regardless of health, disability, or socioeconomic status, age, sex, sexual orientation, race, ethnic group, or geographic location.” Also, the “diagnosis” can be made on “clinical grounds” as there is “no biomarker” to indicate long Covid. When defining the functional impairment of long Covid, NASEM have included an epidemiologic criterion: long Covid can result in “profound emotional and physical effects on [patients’] families and caregivers.”
CDC Definition of “Post-COVID Conditions”
The US CDC adopted the term “long Covid” while at the same time nominating a separate term “Post-COVID Conditions” for their case definition in 2020 [Figure 5] [7]. The definition states long Covid occurs after SARS-CoV-2 infection and is “present for at least three months.” No qualifying symptoms are listed but they are described as “new or recurrent after the symptoms of initial acute COVID-19 illness have resolved; [they] can emerge, persist, resolve, and reemerge over varying lengths of time; [symptoms can be] continuous, relapsing and remitting, or progressive… [and affect] one or more organ system.” The CDC mentions the recovery timeframe for an “initial acute COVID-19 illness.” The definition states that “most patients appear to recover… within four weeks and many patients continue to recover between four and twelve weeks.” The definition includes “disability” as part of the functional impairment of long Covid.
Identifying the Elements for the “Diagnostic Criteria” of Long Covid
Etiology
The Patient Led Research Team did not exclude patient who tested negative to COVID-19 from participating in their survey [1]. All case definitions outlined above stipulate COVID-19 infection as necessary for long Covid. The NICE definition says long Covid follows “an infection consistent with COVID-19.” The NASEM definition says that SARS-CoV-2 infection can be “asymptomatic [and] unrecognized.” The CDC definition simply states it “can occur after SARS-CoV-2 infection.” The WHO definition is the only one that implies testing by stating previous SARS-CoV-2 infection must be “probable or confirmed.”
Qualifying Symptoms
The Patient Led Research Team did not list the qualifying symptoms for long Covid but they did list the most common symptoms eight weeks after the onset of illness [Table 1]. The NICE and CDC definitions do not mention any symptoms in particular. The NASEM lists fourteen symptoms, it is assumed in no order of importance; the WHO do not indicate any qualifying symptoms, but do list three “common” ones.
The Patient Led Research Team grouped symptoms by organ system. They showed patients whose symptoms were quiescent for at least one week were in the minority, five percent. Also, patients whose symptoms “remained the same” were only six percent. The remaining 89% had “symptoms [that] fluctuated in intensity and frequency.” Seventy per cent had “new symptoms [appear] at different times.” All four case definitions acknowledge that symptoms are not static and can change over time. The Research Team implied that symptoms cluster, usually by organ system, and this, too, is acknowledged by all case definitions. The WHO define “fluctuate,” “relapse,” and “cluster.”
Disease Onset and Duration of Symptoms
The Patent Led Research Team tracked the symptoms of respondents from acute COVID-19 infection onwards and presented data up to eight weeks after acute infection [1]. There was no minimum time symptoms had to be present, although the survey was targeted at patients whose symptoms were present for at least two weeks, nor was there a time cut off where symptoms could be attributed to long Covid and not the acute COVID-19 infection. The NICE, NASEM, and CDC definitions all stipulate a minimum of three months symptom duration. The NICE and CDC definitions also mention that symptoms of acute COVID-19 infection can persist for the first twelve weeks. The NICE and NASEM definitions allow for long Covid to be “diagnosed” before the three month threshold is reached, while the CDC does not. The WHO mirror the Patient Led Research Team’s original dataset in that symptoms must be of eight weeks duration, but stipulate that long Covid symptom onset is “usually three months” after acute infection.
Alternative Diagnoses
The Patient Led Research Team asked respondents to list their co-morbid diagnoses and medical investigative tests they had received for their symptoms [1]. The researchers did not tabulate the reasons why the investigations were done. Only the NICE and WHO definitions mention that “alternative diagnoses” need to be excluded, which implies a diagnostic process including history taking, physical examination, and investigative test interpretation. The CDC makes no mention of considering the possibility of alternative diagnoses to explain the patient’s symptoms.
The NASEM definition acknowledges a diagnostic process by mentioning that long Covid “can be diagnosed on clinical grounds.” However, NASEM is unique for listing nineteen separate diseases that can “manifest” as long Covid. The Patient Led Research Team noted that some respondents had “flare ups” of previous conditions, but they did not state if they regarded these “flares” as synonymous with long Covid [1].
The Similarities and Differences Between the Patient Led Research Team and Subsequent Health Institution Responses
The Patient Led Research Team did not aim to construct diagnostic criteria for long Covid, but did their research “because patients experiencing symptoms are in need of timely research and content relevant to them that is not currently available due to the novelty of [SARS-CoV-19]” [1]. There are three differences between the Research Team and the subsequent case definitions. First, none of the four institutions that promulgated their case definitions recapitulated the empirical research conducted by the Research Team. Second, the Research Team did not stipulate that it was necessary to test positive for SARS-CoV-19 to develop symptoms [1]. Only 23% of respondents tested positive [1]. All case definitions assume SARS-CoV-2 to be necessary for long Covid. The only case definition to explicitly mention testing, however, is the WHO, but the minimum threshold is “probable infection” not “confirmed.” The third difference is the timeframe for the illness. The Research Team’s survey was open for 12 days and “targeted patients with prolonged symptoms (patients with symptoms for over two weeks)” [1]. The CDC and NASEM definitions specify symptoms lasting a minimum of three months in duration, although NASEM follows more closely the Research Team’s intent when they state that long Covid can be “continuous from the time of SARS-CoV-19 infection.” The NICE definition also allows the diagnosis of long Covid within the first twelve weeks after acute COVID-19. The WHO is different again, requiring at least two months of symptoms, three months from the onset of COVID-19.
The case definitions all accept the Research Team’s finding of multiple, fluctuating symptoms, grouped by organ system. Only the WHO, however, defines terms like “fluctuate”, and states common symptoms.
A Candidate Set of Diagnostic Criteria for Long Covid
As none of the case definitions were based directly on empirical research, only a qualitative assessment can determine which of the case definitions are a suitable candidate for a set of diagnostic criteria. NICE and NASEM follow the Research Team’s approach by making it possible to diagnose long Covid even though the acute phase of COVID-19 is ongoing. The strength of the NICE definition is the reference to a diagnostic process to identify alternative diagnoses to explain a patent’s symptoms, but it lacks a list of “common” symptoms and does not define terms such as “cluster” or “fluctuate,” nor does it indicate the functional impairment of the disease. The CDC includes an expected timeframe for recovery from acute COVID-19 and outlines the functional effects of the disease. But they, too, refuse to list common symptoms or define symptom related terms like “progressive.” There is no direction to exclude alternative diagnoses, either. The NASEM definition references a diagnostic process, but this is not a direction to identify alternative diagnoses. Rather, the NASEM encourage alternative diagnoses to be considered as “manifestations” of long Covid. The WHO definition lists common symptoms, defines symptom related terminology, directs that alternative diagnoses must be excluded, and defines the functional effects of the disease. This combination of elements is more likely to produce a qualitatively better diagnostic criteria than the three alternatives.
Future Directions
It is still relevant to have separate well described cohorts of long Covid patients to quantify the relative performance of the various case definitions with respect to their sensitivity and specificity for diagnosing the disease. Further research in this direction must control for the very broad approach taken by NASEM and the lack of specificity that necessarily follows.
Competing interest statement: No competing interests.
Funding statement: No external funding was used.
Author declarations: I confirm all relevant ethical guidelines have been followed, and any necessary IRB and/or ethics committee approvals have been obtained.
| Abbreviations CDC Center for Disease Control COVID-19 Coronavirus disease 2019 NASEM National Academies of Sciences, Engineering, and Medicine NICE National Institute for Health and Care Excellence RECOVER Researching COVID to Enhance Recovery SARS-CoV-2 Severe acute respiratory syndrome coronavirus 2 WHO World Health Organization |
References
- Assaf G, L T, C A , S M, Mercier J, N L, H N, Davids JD et al. (2020). What Does COVID-19 Recovery Actually Look Like? An Analysis of the Prolonged COVID-19 Symptoms Survey by Patient-Led Research Team. [Accessed: 28 January 2025 https://docs.google.com/document/d/1KmLkOArlJem-PArnBMbSp-S_E3OozD47UzvRG4qM5Yk/edit?tab=t.0#heading=h.6k6pzd4mpduo].
- WHO. (2020). COVID-19: Case Definitions [Accessed 18 January 2023 https://www.who.int/publications/i/item/WHO-2019-nCoV-Surveillance_Case_Definition-2022.1].
- Callard F, Perego E. (2021). How and why patients made Long Covid. Soc Sci Med. 268:113426. [CrossRef]
- National Institute for Health and Care Excellence (NICE). (2020) COVID-19 rapid guideline: managing the long-term effects of COVID-19. London. [Accessed 2 February 2021 https://www.nice.org.uk/guidance/NG188].
- Soriano JB, Murthy S, Marshall JC, Relan P, Diaz JV. (2022) WHO Clinical Case Definition Working Group on Post-COVID-19 Condition. A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect Dis. 22(4):e102-e107. [CrossRef]
- Ely EW, Brown LM, Fineberg HV. National Academies of Sciences, Engineering, and Medicine Committee on Examining the Working Definition for Long Covid. (2024) Long Covid Defined. N Engl J Med. 391(18):1746-1753. [CrossRef]
- Centers for Disease Control and Prevention. Clinical overview of long COVID. [Accessed 25 December 2025 https://www.cdc.gov/covid/hcp/clinical-overview/?CDC_AAref_Val=https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/post-covid-conditions.html].
- Fitzner J, Qasmieh S, Mounts AW, Alexander B, Besselaar T, Briand S, et al. (2018). Revision of clinical case definitions: influenza-like illness and severe acute respiratory infection. Bull World Health Organ. 96(2):122-128. [CrossRef]
- Thaweethai T, Jolley SE, Karlson EW, et al. (2023) Development of a definition of postacute sequelae of SARS-CoV-2 infection. JAMA 329:1934-1946.
- EnSpark Consulting. What we heard: Engagement report on the working definition for long COVID. June 2023.
Figure 1.
WHO COVID-19 case definitions.
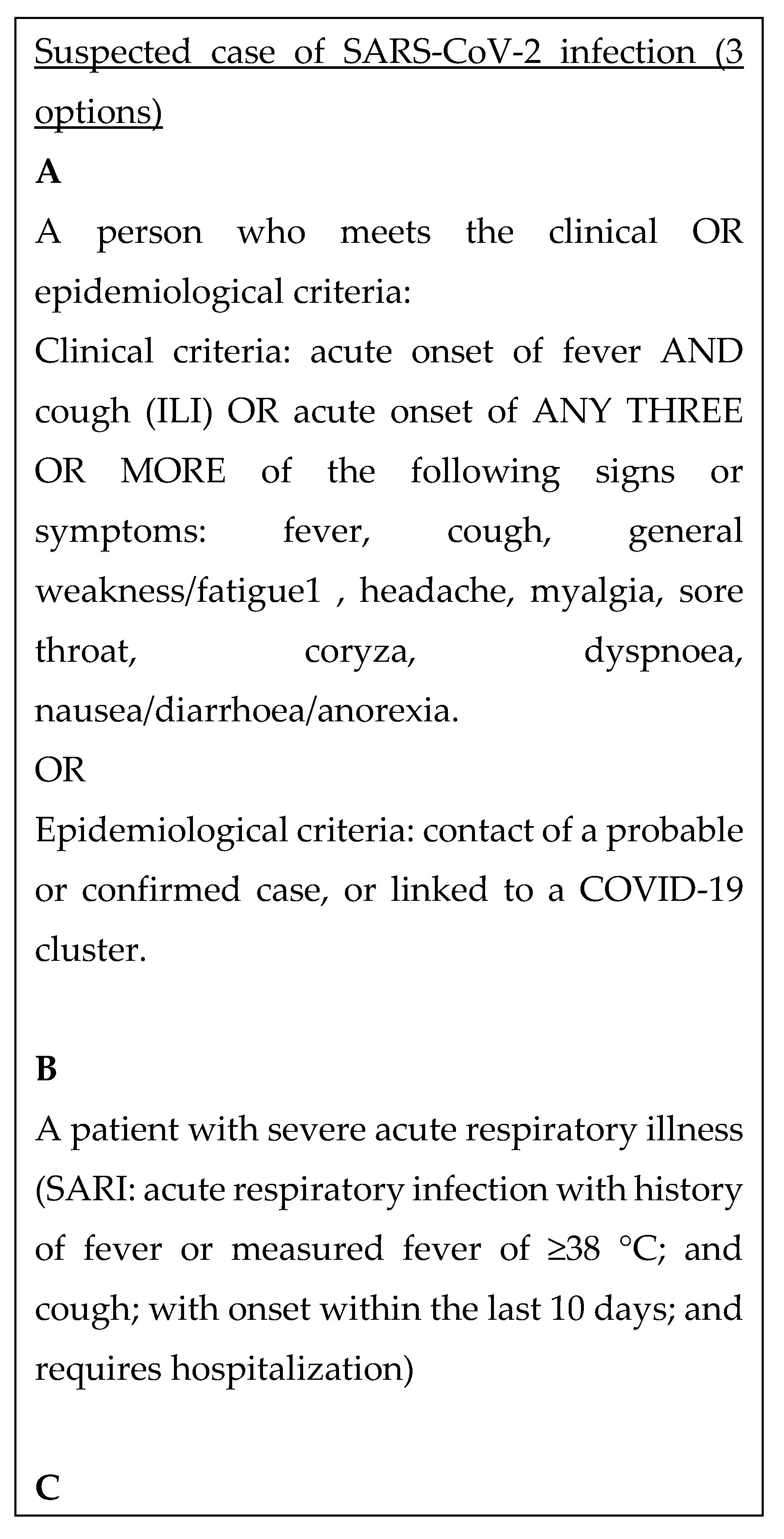
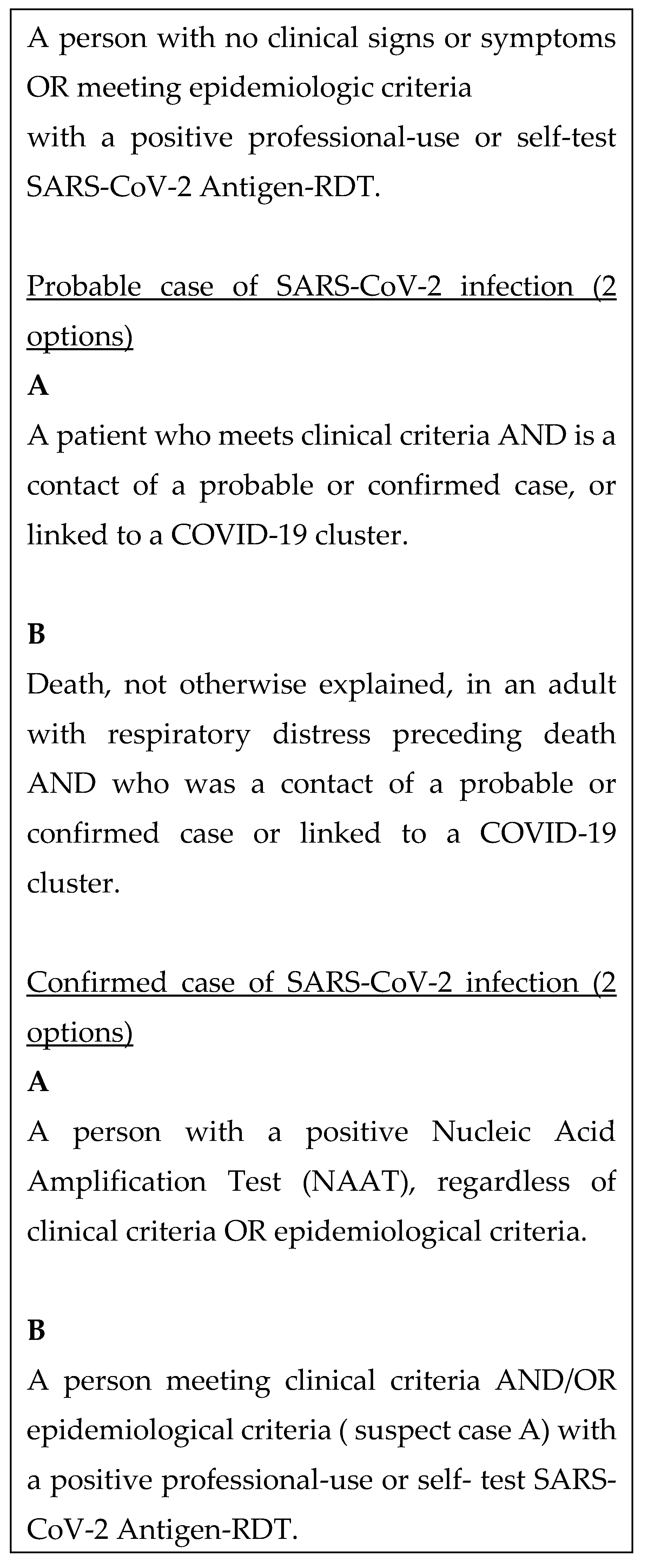
Figure 2.
NICE case definition of “post-COVID-19 syndrome.”.
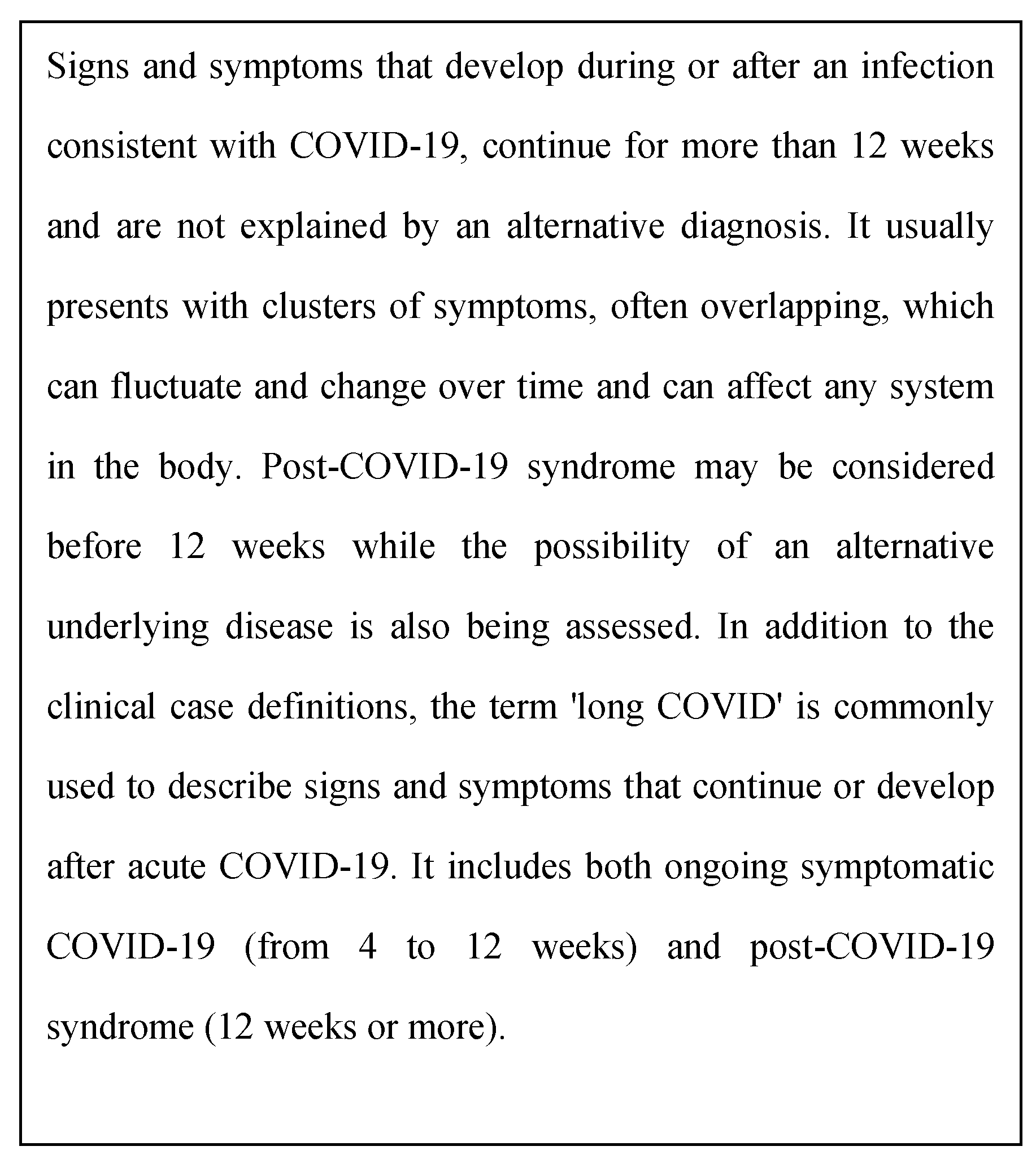
Figure 3.
WHO definition of “post COVID-19 condition.”.
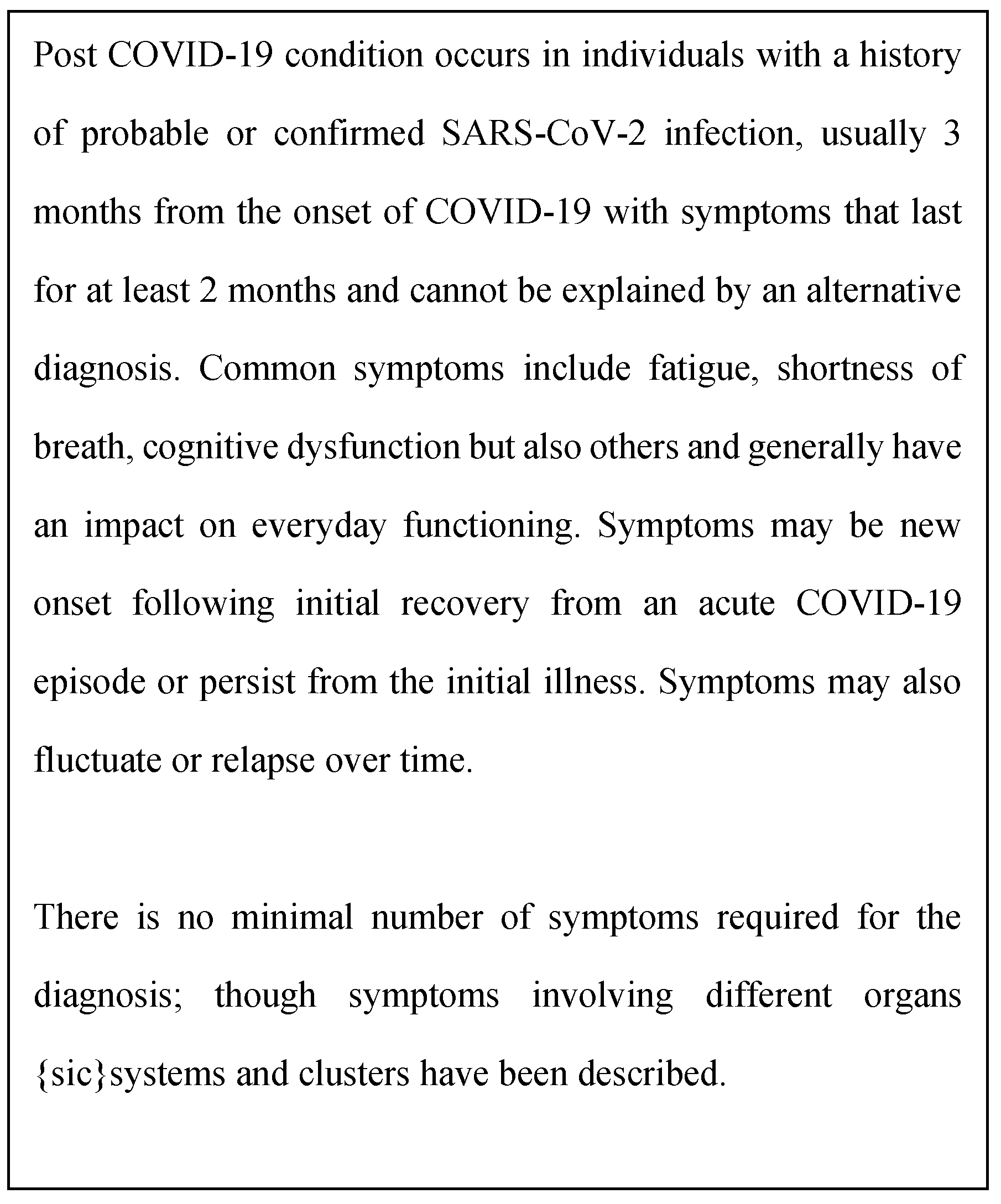
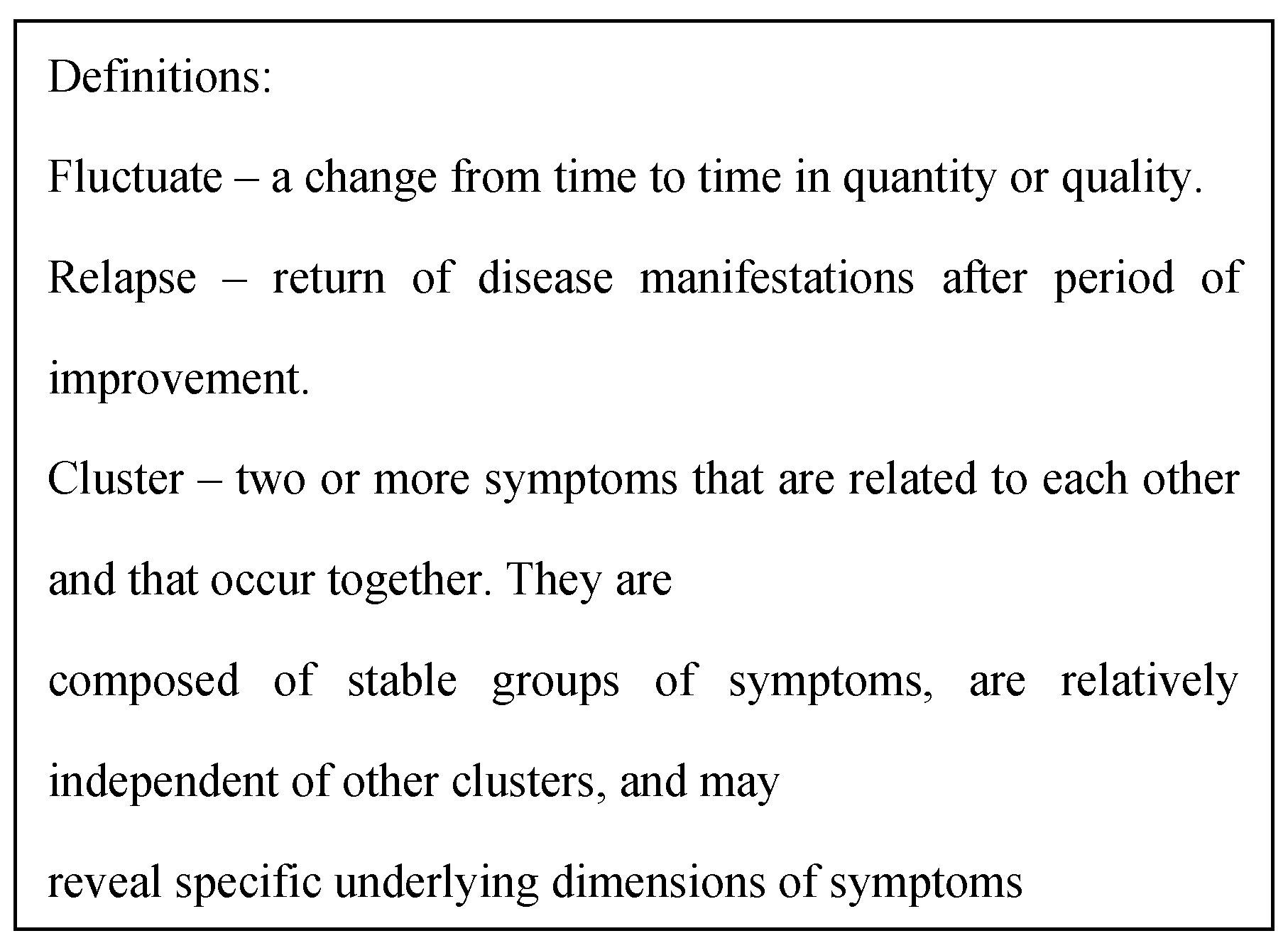
Figure 4.
NASEM long Covid definition.
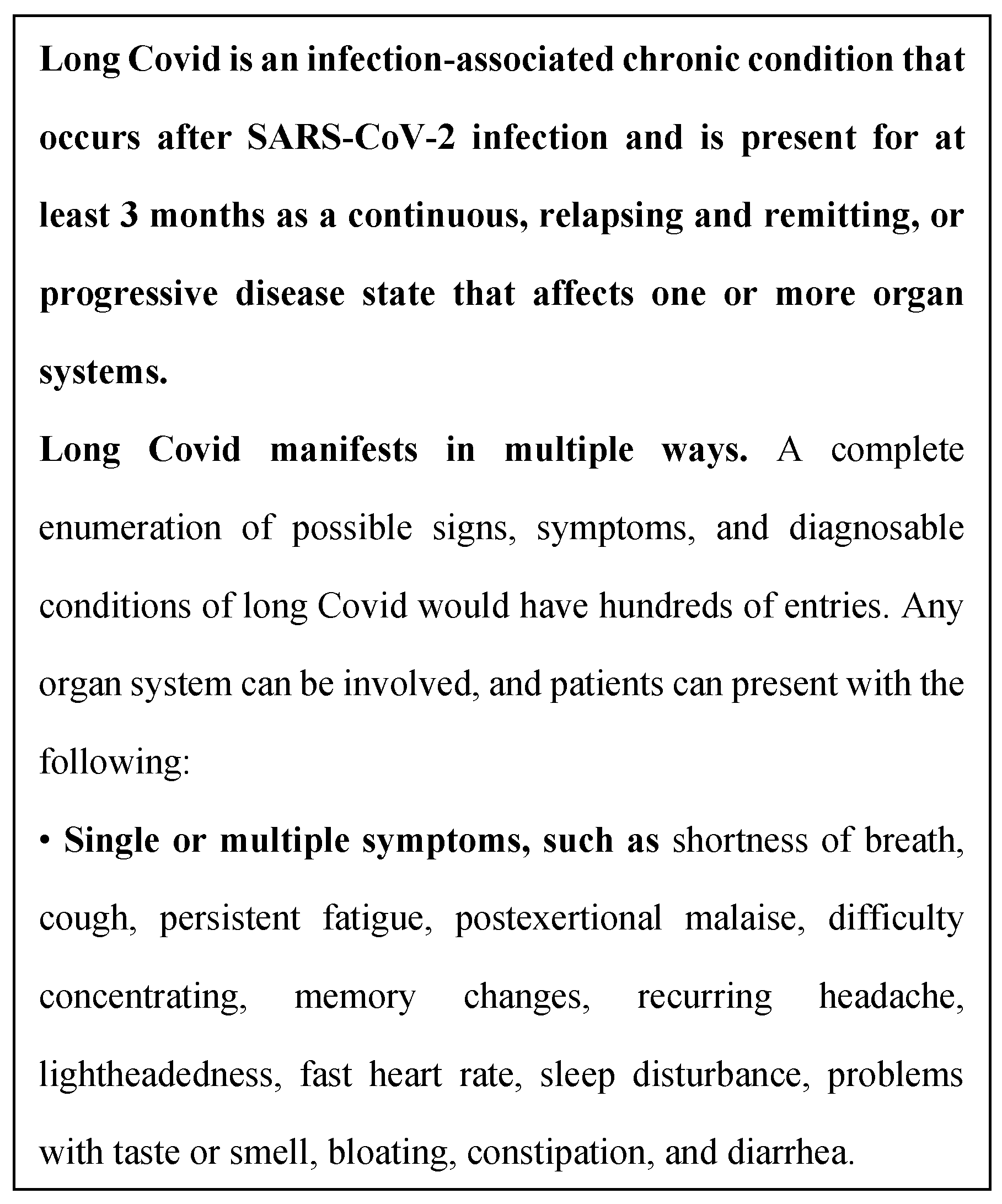
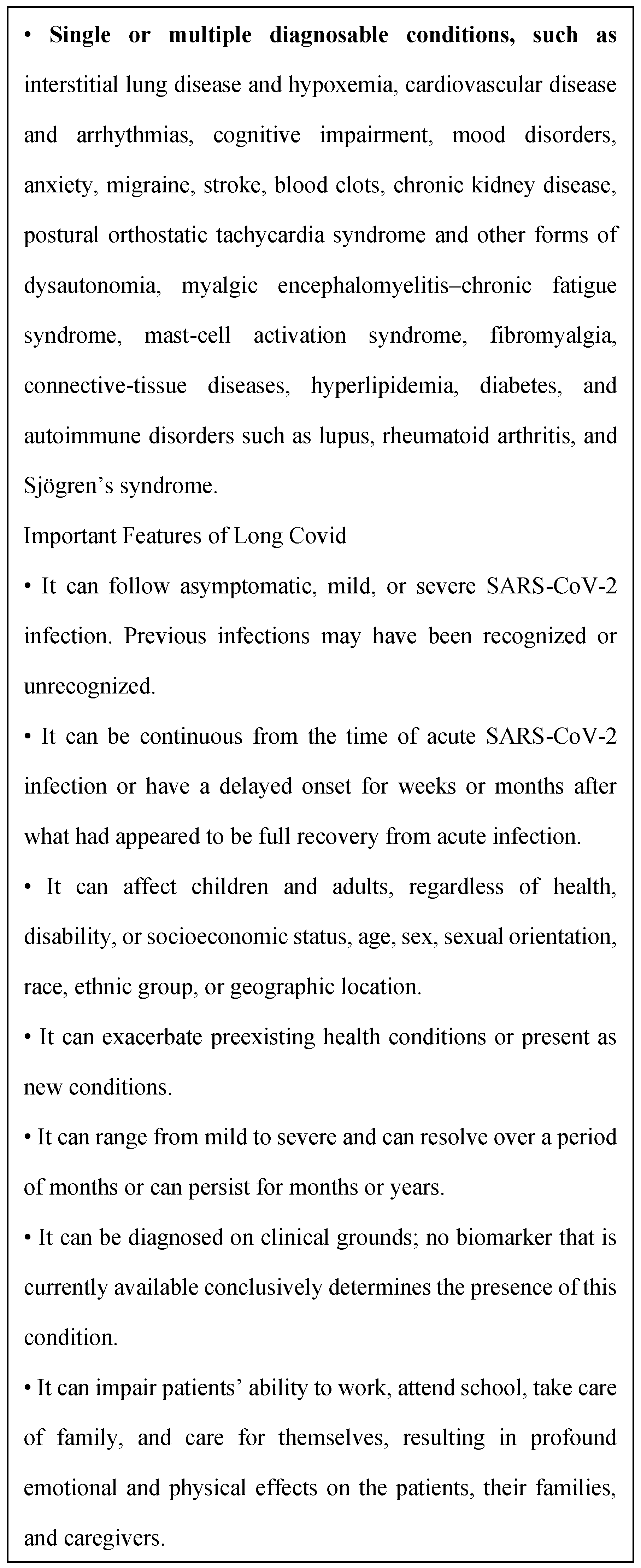
Figure 5.
CDC case definition of “Post-COVID Conditions.”.
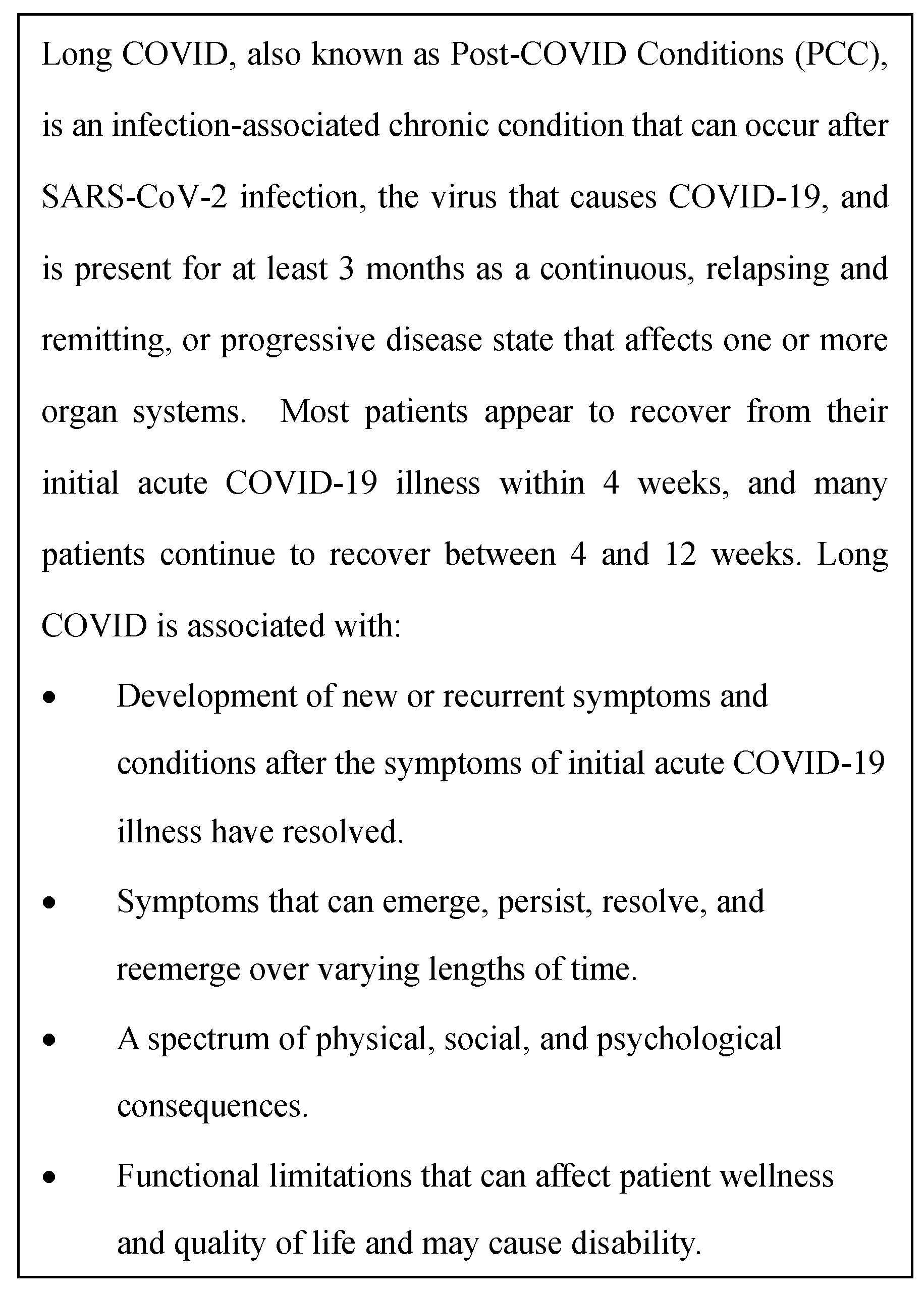

Table 1.
Most common symptoms at eight weeks after symptom onset, from the Patient Led Research Team Prolonged COVID-19 Symptoms Survey.
Table 1.
Most common symptoms at eight weeks after symptom onset, from the Patient Led Research Team Prolonged COVID-19 Symptoms Survey.
| Symptom | Per centage prevalence |
| Shortness of breath – mild Tightness of chest – mild Fatigue -mild Fatigue – moderate Dry cough Headache – mild Brain fog/concentration challenges Elevated temperature Body aches – mild Chills or sweats |
39 35 33 32 29 26 24 24 23 21 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



