Submitted:
13 March 2025
Posted:
14 March 2025
You are already at the latest version
Abstract
The continuous need for simplified minimally invasive dental restorations using bio-materials with adequate mechanical, physical, and biological characteristics has led to an evolution in the field of flowable composites. Nanotechnology focuses on advancing highly filled flowable resin-based materials, which may be used in many restorative indications. Since these materials are a novel addition to the toolkit of restorative dentistry, the purpose of this review is to investigate their in vitro characteristics and clinical performance. Highly filled flowable composite resins proved to be a promising dental biomaterial. Considering that these materials show an ideal initial performance in the injection molding technique and in Class I and II cavities but simultaneously present several drawbacks in laboratory studies, caution should be exercised when selecting the applicable cases. Further, in vitro and clinical studies are needed to establish the precise indications and limitations of this type of biomaterials.
Keywords:
highly – filled flowable resin composites
; injection moulding technique
; biomaterials
; flowable resin
; injectable composites
1. Introduction
Until recently, the incrementally placed conventional, medium viscosity composite resins proved to be the gold standard in restoring both anterior and posterior teeth. Conservation of tooth structure, adequate shade matching, satisfactory mechanical properties and the lower cost compared to indirect restorative counterparts, represent their beneficial side [1]. However, their poor rheological characteristics lead to marginal defects due to unfavorable adaptability to cavity walls and voids between increments [2]. To confine these drawbacks, the first-generation flowable composites were introduced in the 1990s and have been proposed as liners prior to restoring a cavity with medium-viscosity composites. They included 20-25% less filler loading than medium-viscosity composite resins [3,4]. Their low viscosity equals ease – of – use, great flow, flexibility, good adaptability to cavity walls, preferable handling and wetting properties, and restricted entrapment of air bubbles in the mass of the material. Despite all the above-mentioned benefits, the reduced level of fillers had an undesirable effect on their mechanical and optical properties (inadequate wear resistance, inferior flexural strength, lower fracture toughness, subordinate color, gloss stability, and decreased modulus of elasticity), limiting their indications only as class V restorative materials, liners, pit and fissure sealants and as materials for marginal repair of restorations. Furthermore, the average volumetric polymerization shrinkage rate of 5% constitutes an additional disadvantage for traditional flowable resin composites [2].
Dental material manufacturers respond to clinicians’ demand for simpler, color-adaptive, and durable materials suitable for a wide range of indications, including Class I and II cavities, extensive tooth wear, full-mouth rehabilitations and novel restorative procedures such as the injection moulding technique, by developing novel nanotechnology-driven flowable composites. [5,6,7]. The injection moulding technique, first introduced by Douglas Terry and John Powers in 2014, is a restorative technique that uses transparent silicone molds based on a wax-up to generate the final restorations [5]. The flowable composite is injected into the mold to form the final shape of the restorations. The predictable reproduction of the anatomical contour, the more accurate execution of the procedure, and the use of easy – to – handle flowable resins proved to be factors that gained the interest of dental experts.
Continuous attempts to improve the mechanical properties of flowable composites are made, mainly through modifications in their formulation, such as the increase in filler loading, optimization of filler particle size, incorporation of refined monomers, and treatment of filler particles. Through these alterations, a significant improvement of their physical and mechanical properties is accomplished, maintaining their superior marginal adaptation [8]. The innovative formulation of these flowable composite resins is characterized by a higher filler content ranging from approximately 61 to 71 % by weight, which broadens their indication spectrum since they may now bear high occlusal loads [9,10]. According to a manufacturer’s recommendations, a “new-generation” flowable resin composite shows a more homogeneous dispersion of nano–sized glass filler particles. The developed silane treatment method, generating a favorable adhesion between the filler particles and the organic matrix, corresponds to the materials’ upgrade [11]. Until now, these statements have not been clearly verified. This new era of flowables is described mainly as highly filled flowable resin composites. The commercial terms next-generation flowable composites or injectable composite resins are interchangeably used, but may lead to confusion.
Despite their improved filler content, highly filled flowable resins still present challenges related to wear resistance, color stability, and polymerization shrinkage. This review aims to critically evaluate and shed light on the narrow spectrum of existent knowledge originating from up–to–date laboratory experiments, randomized controlled clinical trials, and case reports referring to highly filled flowable composites. Since these flowables are used as the preferable material for the injection moulding technique, a short reference on clinical cases implementing this novel technique is going to be made, and the clinical performance of the materials used will be discussed.
2. Materials and Methods
The article selection process started with a comprehensive search of the following databases: PubMed, Scopus, and Google Scholar. The search strategy was developed using the keywords presented in Figure 1. Date and language restrictions were applied. Studies in languages other than English are eliminated from the selection process. For this review, we included research published between 2016 and February 2025 to capture the evolution and the recent developments in the field of highly filled flowable composite resins. This data limitation has been adopted since a systematic review and meta-analysis on the clinical performance of flowable composites was published in early 2017 [12]. Two reviewers screened titles and abstracts for eligibility. When there was a conflict, a consensus was reached by discussion. Letters to the editor, patents, review articles, short communications, and conference papers are excluded. The procedure employed in this review is reflected in Figure 1.
3. Results
The first class of results recites clinical cases utilizing flowable materials, emphasizing the injection moulding technique, whereas the second class focuses on the laboratory behavior of highly filled flowable resin composites, as well as on their clinical performance in randomized controlled clinical trials.
3.1. Clinical Case Reports of Injectable Moulding Technique Using Flowable Resin Composites – Interpretation of the Clinical Outcome
Table 1 presents the total of clinical reports available, giving information on treated teeth, patient’s profile, material used, protocol followed and initial outcome of the procedure. Follow-up information is given where applied [13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36].
The injection moulding technique is described as a novel treatment modality with a direct/indirect character that translates an analog or digital wax up into a final resin composite restoration, without or with confined tooth preparation [13]. In order for the final restoration to be accomplished one or more transparent silicone indices based on the wax up (analog or digital) are fabricated, which allow the material – mainly flowable composite resins- to be passively inserted and cured, therefore minimizing the possibility of index and restoration distortion. It presents similarities to its ancestral technique named “index technique”, that uses a single transparent index and stamps the resin composite directly on the surface of the single prepared tooth [37,38]. Their main difference is based on the material used for the final restoration. At the “index technique” preheated conventional composite resin is used, whereas the material of choice for the injectable technique is a flowable composite resin. Furthermore, in a study of Kouri et al. in 2023 [39], the injection moulding technique and its modifications move from the diagnostic wax- up towards the final direct resin composite veneers in a more accurate and predictable manner compared to the “index technique”, which uses preheated resin composite. Douglas Terry and John Powers have been the first to present this alternative technique in 2014 and reported its numerous applications, among others the repair of fractured teeth and restorations, the fabrication of transitional restorations and pediatric composite crowns, the resurfacing of occlusal wear on posterior composite restorations, the development of composite prototypes for copy milling, the establishment of an alternated vertical dimension prior to restoring with final restorations and its use as a communication tool between patients and dental practitioners [5,40]. Diastema closure, reshaping crown morphologies, and correction of dental misalignments are additional indications implementing the injection technique in the restorative dentistry toolkit. The restorations generated from this treatment method may be either transitional or definitive [13,20]. Furthermore, this technique is nowadays used to fabricate an ideal shape and core size without additional tooth preparation [41] or even resin bonded fixed dental prosthesis [17,32]. The tremendous development of Digital Dentistry entails the incorporation of digital workflows in the injection moulding procedure by the fabrication of digital wax-ups and 3D-printed molds, rigid or soft indices and rigid holders of the soft transparent index [42].
The compositions of the flowable resin composite materials used in these clinical cases are presented in Table 2.
These materials have been used in a wide range of situations, such as single tooth restorations, teeth recontouring by fabricating four to six veneers on anterior maxillary and mandibular teeth, replacement of missing teeth as direct composite resin-bonded fixed dental prosthesis and full mouth rehabilitation with or without alteration of the vertical dimension. When minimal tooth structure loss is present, these materials proved to perform to the maximum [13,20,22,30]. When evaluating the use of highly filled flowable resin-based materials in full mouth treatments, no defects were present in the 6- month and one-year follow-up periods [21,31]. Staining on the material’s surface and/or in the tooth – material interface, minor chippings and presence of voids are defects related to some clinical cases [16,29]. These observations strengthen the belief that highly filled flowable resin composites may present inferior properties related to resistance to occlusal forces and color stability.
The results of the clinical reports should be interpreted with general reservation for the following reasons:
- Despite the material per se, external factors such as medical record, intraoral temperature and humidity, acid consumption, grinding, poor oral hygiene, parafunctional behaviors, and polishing procedures are additional influential factors affecting clinical outcomes [52].
- Very short follow-up periods are applied. In order to draw clear conclusions on a technique or a material, long-term follow-up periods are essential.
- The initial evaluation of a restoration or restorative procedure and its behavior through time should be based on specific guidelines and criteria and should not be only assessed by the presence of stains and wear. These criteria include esthetic, functional, and biological parameters, such as anatomical form, surface luster, and surface staining, fracture of material, marginal adaptation, postoperative sensitivity, reoccurrence of dental caries, tooth integrity, and the adjacent mucosa evaluation [53,54,55].
- We should keep in mind that although clinical cases belong to the evidence – based scientific pyramid, their quality as well as their amount of evidence is weak [56]. The selection of a dental biomaterial in conjunction with a restorative technique should be made through well-designed randomized controlled clinical trials reinforced by in vitro studies and by the conduction of well–structured systematic reviews and metanalysis.
3.2. In Vitro and Randomized Control Clinical Studies on Highly Filled Flowable Resin Composites
The presence of staining and discoloration on the surfaces of the highly filled flowable resin composites and on the tooth–material interface, in conjunction with the voids and minor wear defects presented in some clinical cases mentioned in 3.1 section, constitute the stimulus for investigating the performance of highly filled flowable materials based on laboratory studies and clinical trials, which are thoroughly described in Table 3 and Table 4 respectively [10,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90].
A total of 31 in vitro studies are included in this review. Each study evaluated single or multiple characterictics. Most studies focus on optical properties, color stability, surface roughness, microhardess, flexural properties and wear. Surface gloss, water sorption/solubility, filler content, handling properties, wettability, cuspal deflection, bonding properties, microleakage and marginal adaptation, microbial adhesion and viability, degree of conversion and polymerization shrinkage have been evaluated to a lesser extent.
Regarding optical properties and color stability, Nair et al. in 2017 demonstrated inferior performance for the highly filled flowable composite resin compared to nanofilled and nanohybrid conventional composite counterparts after coffee immersion and tooth brushing simulation [57]. On the contrary, Lai et al. in 2018 concluded that the color alterations caused by toothbrushing abrasion were acceptable for all materials tested (highly filled flowables, traditional flowables, and self-adhesive flowables) [58]. No statistically significant differences were found in color stability between highly filled flowable composite resins, a bulk fill flowable composite, and a conventional nanofilled composite resin, meaning that highly filled flowable composites’ optical properties after a 144-hour immersion in colorant solutions are relevant to controls [60]. Again, comparing the color change of bulk-fill composite resins and one conventional resin composite to that of a highly filled flowable composite resin, clinically invisible color changes between materials were observed after 60 days of storage either in dry or wet conditions [66]. When hand polished, the highly filled flowable composite resins performed adequately after beverage immersion [69]. Another research assessing optical properties highlighted that the highly filled G-aerial Universal Injectable flowable composite resin presented the highest translucency and opalescence values and the lowest chroma values. This material was compared to another highly filled flowable resin-based material and a conventional microhybrid composite resin originating from the same company [74]. The same conclusion is drawn in the research of Bai et al. in 2024, who also found that G-aenial Universal Injectable by GC presented the highest traslusency values this time compared to other highly filled flowable materials (Beautifil Injectable XSL by Shofu and Filtek Supreme Flowable, Solventum) and a compomer [77]. Interestingly, Bayrakrat et al. in 2024 demonstrated that the conventional composite resins of different companies presented lower fluorescence and color adjustment levels compared to their highly filled flowable formulations in class V restored cavities [82].
Proceeding to surface roughness properties the highly filled flowable resin material (G-aenial Universal Injectable, GC) showed the lowest Ra values among four other traditional flowable composites and a self-adhesive flowable [58]. Niyomsujarit et al. in 2021, revealed that two highly filled flowable restorative materials, did not present any differences in Ra values compared to a conventional, universal composite resin (control). Controversally, in this study, another highly filled injectable flowable material (Beautifil Injectable X, Shofu) presented higher Ra values than the control [63]. The same results were observed by Degirmenci et al. in 2023, Basheer et al. in 2024, and Checchi et al. in 2024, where all the highly filled flowable resin composites presented statistically similar Ra values compared to conventional nanohybrid composites [74,79,84]. In the study of Elsahn et al. in 2023, G-aenial Universal Injectable performed better in terms of Ra values, even compared to a CAD/CAM resin based material, when applied as a thin occlusal veneer [70]. When investigating a highly filled bulk flowable resin composite solely, the conclusion is focused on the fact that both polishing procedure systems and acidic challenges greatly impact the surface roughness of the material [72]. Vulovic et al. both in 2023 and 2024, comparing four highly filled flowable resin composites to each other concluded that the ones with either ultra – fine barium or strontium fillers and a full coverage silane technology (G-aenial Universal Injectable, GC and G-aenial Universal Flo, GC) presented favorable roughness values compared to other flowables (Filtek Supreme Flowable Restorative, 3M ESPE, and Tetric EvoFlow, Ivoclar Vivadent). The variation of polishing procedures and the immersion in acidic media in different time intervals played a pivotal role on this outcome [73,86]
Another vital aspect is surface gloss. G-aenial Universal Injectable by GC performed favorably by presenting the highest surface gloss values (GU) compared to other traditional flowables availble in the market [58]. Not to forget, the surface gloss of a dental material is influenced by polishing procedures, as presented by a research demonstrating that a multi-step polishing system reinforces the surface gloss of the restoration [72].
Microhardness is another multiply investigated crucial factor. In a plethora of in vitro studies included in this review, the highly filled flowable restorative materials presented inferior Vickers microhardness values either compared to conventional microfilled composites, nanofilled composites, bulk–fill composite resins, and CAD/CAM resin-based materials [57,64,66,70,71,79]. Additionally, one study demonstrated superior hardness values for a highly filled flowable restorative material compared to a traditional flowable counterpart [65]. When comparing highly filled flowable resin composites to each other, G-aenial Injectable GC presented the highest surface hardness values [86].
Emphasizing flexural properties, controversial results are to be seen. Although Imai et al., in 2019 concluded that highly filled flowable composite resins present lower elastic modulus compared to microhybrid and nanofilled conventional resin composites [10], Degirmenci et al., in 2022 presented higher flexural strength and elastic modulus values for the highly filled flowable materials compared to microhybrid conventional composite resins [64]. In a more recent study of 2024, no differences in flexural strength values between highly filled flowables and a nanohybrid conventinal resin composite were observed [79]. When comparing traditional flowable, bulk-fill flowable composites, and highly filled flowable composites, the latter exhibit favorable flexural strength and elastic modulus values [62]. G-aerial Universal Injectable by GC and Majesty ES Flow by Kuraray Noritake exhibited the greatest flexural strength and modulus values in comparison with other highly filled flowable and bulk-fill flowable resin products [61]. Lastly, Rajabi et al. in 2024 demonstrated that two highly filled flowable composites presented statistically higher mean flexural strength values than traditional and conventional nanohybrid composite resin [81].
The wear volume loss in conventional resin composites may be lower than that of highly filled flowable composites. This observation comes to agreement with the results of Turk et al. in 2023, stating that conventional nanohybrid and nanofilled resin composites perform better in terms of wear volume loss and maximum depth loss compared to their flowable composite resin counterparts [68]. G-aenial Universal Injectable surprisingly presented lower wear volume loss compared to CAD/CAM milled resin based material when fabricated for 1mm thin occlusal veneers [70]. Finally, some highly filled flowable resin composites (G-aenial Universal Flo by GC and Filtek Supreme Flow by 3M ESPE) and a highly filled bulk injectable composite (G-aenial Bulk Injectable by GC) exhibit less wear than other highly filled flowables, bulk fill flowables and older flowable resins [59]. Newly published studies demonstrate that the wear of highly filled flowable composites is comparable to that of conventional composites [81,84].
Other characteristics commonly investigated in dental biomaterial science are volumetric or linear polymerization shrinkage, polymerization shrinkage stress, depth of cure, and the degree of conversion of resin composites. According to the studies in this review, highly filled flowable resin composites display higher values of linear and volumetric polymerization shrinkage compared to either bulk fill flowables or conventional microfilled or nanofilled composites [62,67,75,80]. Referring to polymerization shrinkage stress, highly filled flowable resin composites present significantly higher values of stresses compared to traditional flowables and bulk fill flowables, but no differences when compared to conventional composite resins [62,80].
Unfortunately, only four randomized clinical trials are presently assessing the clinical performance of highly filled flowable resin-based materials. Three clinical studies investigated the clinical performance of highly filled flowable resin composites in direct posterior restorations [87,89,90], whereas one in non-cavitated cervical lesions [88]. Highly filled flowables performed equally or even better in marginal adaptation and surface gloss than the conventional materials used as controls [88,90].
3.2.1. Interpretation of the Results of the In Vitro Studies and Randomized Controlled Clinical Trials
Delving deeper into the aforementioned research, the results should be interpreted cautiously. Disparities among studies examining the same material, two or more highly filled flowable materials and variances between flowable materials, bulk fill materials and a nanofilled conventional resin composite present a multifactorial etiological pattern in which etiological factors are interdependent.
The mechanical, physical, and optical properties as well as the surface characteristics of an examined material are predominantly related to the material’s distinct composition, including the composition and structure of the organic matrix and inorganic filler particles, the filler-to-resin matrix ratio, and the silanization of the filler components. These characteristics are inextricably linked to other material characteristics such as degree of conversion and water sorption and solubility [10,71,77,91,92]. Despite material composition, additional factors may have a dominant impact on several properties tested. Among others, finishing and polishing procedures, storage conditions, and type of external aggravating stimuli (colorant solutions, acidic and abrasive challenges) modify materials performances.
A typical example is that optical performance is affected by surface roughness, gloss, and hardness [93]. Furthermore, surface roughness is dependent on filler content, filler type, and size, the surface area in percent occupied by filler particles, the degree of conversion, the interaction of filler with the organic matrix, the silane coupling agent, and eventually, the hardness of the material [63,94,95]. Subsequently, the inferior microhardness and color stability of highly filled flowable resin composite after immersion in instant coffee and tooth brushing simulation may be attributed to the type of fillers. Strontium glass fillers in G-aenial Universal Flo are related to inferior physical properties and difficult attachment to the organic matrix, compared to zirconia and silica fillers in the conventional resin composite [57,96]. The uniform pattern of filler content distribution has a profound positive effect on physical and optical properties [71]. The highly filled flowable G-aenial Universal Flo by GC consists of fillers ranging from 16nm to 200nm in size, whereas conventional resin composite’s fillers (Filtek Z350XT) range from 4nm to 20nm [43,97].
The optical performance of a biomaterial is intertwined to translucency, opalescence, chroma values and refractive indices of monomers and fillers [98]. The different filler composition and the different filler type may have an important effect on the translucency between the tested materials [99]. This statement is endorsed by Bai et al., in 2024, who found higher translucency in G-aenial Universal Injectable, GC compared to another highly filled flowable composite (Filtek Supreme Flowable, 3M ESPE), probably due to the zirconia fillers of the later, that have imperfect refractive index and translucency [77]. G –aenial Universal Injectable consisting of barium glass presented the highest translucency and opalescence values when compared to G-aenial Universal Flo consisting of strontium glass and a microhybrid conventional resin composite consisting of strontium glass and lanthanoid fluoride launched by the same company [74]. Furthermore, polishing systems and especially the hardness of the abrasive particles are strongly related to translucency values [100]. Diamond particles exhibit superior abrasive hardness in comparison to aluminum oxide particles, leading to abrasion of the resin matrix and protrusion of fillers causing differences in translucency even at the same material [101,102]. Lastly, the general rule that higher filler fraction may lead to increased strength and wear resistance, but simultaneously to decreased translucency and increased opacity, should not be forgotten [103,104,105].
The filler loading and the filler shape and size could be etiological factors for the differences in the surface roughness and surface gloss values between several resin composites [106,107]. Lower filler loading, irregular shaped fillers, homogeneous composition of filler particles, and greater average particle size result in increased surface roughness and decreased surface gloss. This is proven by the difference in surface gloss and surface roughness between the two highly filled flowables in the study of Miyashita – Kobayashi et al. in 2024 [78]. The one presenting supra – nano spherical fillers and an average particle size of 0.2 μm performed better than the one with the irregular shaped fillers and the average particle size of 0.8 μm. Another typical example is the increased surface roughness value of the highly filled flowable Beautifil Injectable X by Shofu compared to the highly filled flowables G-aenial Universal Injectable and Filtek Z350XT Flowable Restorative [63]. Beautifil Injectable X consists of bioactive surface pre – reacted glass ionomer (S-PRG) fillers with a 0.8μm average particle size, contrary to smaller average particle sizes present in the other two highly filled flowable resin composites. G-aenial Universal Flo and G-aenial Universal Injectable consist of strontium and barium glass fillers respectively and silica particles, forming a homogeneous filler pattern. On the other hand, Tetric EvoFlow and Filtek Supreme Flowable Restorative consist of Ytterbium trifluoride (YBF3) and three to four different, diverse, heterogeneous ingredients in their filler composition, a fact that may hinder their surface roughness values [73]. At this point, it should be highlighted that most of in vitro studies only analyze the Ra value, which is a single height parameter of a surface. Additional spatial, functional or hybrid (e.g., developed interfacial area ratio, Sdr) parameters may give a greater insight into surface texture and may alter the resulting behavior of some already analyzed highly filled flowable resin composite materials, based on surface characteristics [108].
Wear and elastic modulus are dependent not only on type, shape and size of fillers, but also on interfiller spacing, surface treatment of fillers, degree of conversion, hydrolytic degradation and water sorption, and the surface’s finishing and polishing procedures [3,8,10,59,109,110,111,112]. The smaller particle size of some highly filled flowables which proved to lead to lower friction coefficients and subsequently to lower internal shear stresses in the polymer matrix may be a partial explanation on the favorable wear performance of some highly filled flowable resin composites over other highly filled flowables and bulk – fill flowables [8,59,113]. Moreover, the small interparticle space of small-sized fillers may protect the resin matrix from its ongoing abrasion. The lowest volumetric wear of G-aenial Universal Injectable compared to a resin – based CAD CAM material in 1mm thin veneers should be interpreted with caution. Following the manufacturer’s recommendations, the proposed thickness of this CAD/CAM material is approximately 1.5mm [114]. Therefore, the design of this protocol could be considered as restrictive. All highly filled flowable resin materials performed unfavorable in terms of elastic modulus compared to conventional resin composites. The higher filler loading and the higher concentration of Bis-GMA monomers in the mass of conventional composite resins are known to positively affect the mechanical and physical properties of resin materials providing high elastic modulus [115]. This fact partially justifies their better wear performance compared to the majority of highly filled flowable composite resins. In contrast, G-aenial Universal Flo by GC demonstrated flexural strength similar to that of a nanofilled composite resin, which characterizes the theory of filler loading as a singular etiological factor rather incompetent and broadens the spectrum of possible explanations on this field. Different resin monomers have different molecular weights and viscosities; for all we know, they may have a determinable effect on wear, flexural strength and mechanical properties of flowables in general [116].
Dimensional changes, degradation and weakening of the bond between organic and inorganic components are present after exposure in the oral environment [10,117]. It is evident that higher filler content entails lower water sorption through the increased hydrophobic character of the material [118] and increased filler size leads to higher water sorption through the increased surface area available for the development of this phenomenon. Additionally, the type of the monomer and its quantitative allocation in the organic matrix has an impact on the water sorption of the material [119]. Higher Bis-GMA and TEGDMA contents lead to greater hydrolytic degradation than that of UDMA monomers [120,121]. By elevating the nano-sized fillers and creating a homogeneous, dispersed distribution the internal free volume available for water intake is confined. Complementary, each monomer with its unique molecular weight presents its own water sorption pattern [122,123]. TEGDMA absorbs more water than Bis – GMA due to the greater space between its clusters, its greater flexibility and its consequent higher swelling [124]. The sorption of water eventually leads to hydrolysis of the coupling agent, weakening the bond between organic matrix and fillers, deteriorating in that manner the characteristics of dental materials. These facts may explain the preferable water sorption values of a plethora of conventional composite resins compared to highly filled flowables. Discrepancies between different highly filled flowables are present and are mainly caused by the slightly different organic and inorganic composition of the materials. As an example Beautifil Injectable X by Shofu presents greater water sorption and degradation than G – aenial Universal Injectable after acidic challenges. This is speculated to be caused by the greater percentages of Bis – GMA and TEGDMA in its composition and by the fact that the fluorosilicate glass (S-PRG fillers) has a higher susceptibility to degradation by weak acids (higher affinity to water sorption) [63]. Lastly, we should keep in mind that the design of the study (sample size calculation, sample preparation, condition of observation, presented control groups, methodological parameters-errors) and the devices used have a great influence on the outcome of the study.
Concerning the interpretation of the four randomized controlled clinical trials, their ambiguous results should be assessed with caution. The number of randomized controlled clinical trials is predicatively low. The four clinical studies are not comparable, since different restorative procedures were applied; the number of participants is confined and the number of the final evaluated restorations is even more restricted. The clinical evaluation pattern (FDI criteria and modified USPHS criteria) is admissible. The moderate to high risk of bias, the dropouts and the short – term follow up duration are limitations that need to be taken into account before drawing vague conclusions [125].
4. Conclusions and Future Perspectives
Highly filled flowable resin composites are a new addition in the field of Adhesive Dentistry and should be further investigated so that their full potential could be unfolded. Since scarce evidence could be provided by the four available randomized controlled clinical trials, an emphasis on the establishment of well designed clinical trials should be given. The survival and success rates of several types of cavities restored with highly filled flowable composites remain vast and uncharted. It is common ground that the combination of highly filled flowable resin composites with the injectable moulding technique leads to predictable, highly esthetic clinical outcomes in terms of reproducing the anatomical contour. Highly filled flowable composite resins present a generally satisfactory material properties pattern – good optical properties, competent surface roughness and gloss – but their inferior microhardness values and wear resistance compared to conventional nanohybrid and nanofilled composites recommend their further amendment. Dental materials should perform the best possible way in the complex and not constant oral environment, where masticatory forces, occlusal and dietary habits, temperature fluctuations, biofilm formation, enzyme collection and salivary flow are constantly present. The interaction of these factors with dental materials may change their existing favorable laboratory physical, mechanical and optical behavior. It would have been interesting to start assessing the behavior of highly filled flowable resin based materials in oral conditions by conducting in situ studies, which may reveal potential interconnection between optical parameters, mechanical properties, surface characteristics, saliva and the oral microbiome.
Author Contributions
Conceptualization, K.T., E.P., and E.P.; methodology, K.T. and C.R.; validation, K.T., M.F. and C.R.; formal analysis, K.T.; investigation, K.T; data curation, K.T.; writing—original draft preparation, K.T.; writing—review and editing, E.P., C.R. and E.P; visualization, K.T.; supervision, E.P., C.R. and E.P; project administration, K.T., E.P., M.F., C.R. and E.P.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
Not applicable.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Alzraikat, H.; Burrow, M.F.; Maghaireh, G.A.; Taha, N.A. Nanofilled resin composite properties and clinical performance: A review. Oper Dent. 2018, 43, 173–190. [Google Scholar] [CrossRef]
- Vouvoudi, E.C. Overviews on the Progress of Flowable Dental Polymeric Composites: Their Composition, Polymerization Process, Flowability and Radiopacity Aspects. Polymers 2022, 14, 4182. [Google Scholar] [CrossRef] [PubMed]
- Baroudi, K.; Rodrigues, J.C. Flowable Resin Composites: A Systematic Review and Clinical Considerations. J Clin Diagn Res. 2015, 9, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Bayne, S.C.; Thompson, J.Y.; Swift, E.J.; Stamatiades, P.; Wilkerson, M. A characterization of first-generation flowable composites. J Am Dent Assoc. 1998, 129, 567–577. [Google Scholar] [CrossRef] [PubMed]
- Terry, D.; Powers, J. Using injectable resin composite: Part one. Int Dent Afr. 2014, 5, 52–62. [Google Scholar]
- Perdigão, J.; Araujo, E.; Ramos, R.Q.; Gomes, G.; Pizzolotto, L. Adhesive dentistry: Current concepts and clinical considerations. J Esthet Restor Dent. 2021, 33, 51–68. [Google Scholar] [CrossRef]
- Blasi, A.; Alnassar, T.; Chiche, G. Injectable technique for direct provisional restoration. J Esthet Restor Dent. 2018, 30, 85–88. [Google Scholar] [CrossRef]
- Sumino, N.; Tsubota, K.; Takamizawa, T.; Shiratsuchi, K.; Miyazaki, M.; Latta, M.A. Comparison of the wear and flexural characteristics of flowable resin composites for posterior lesions. Acta Odontol Scand. 2013, 71, 820–827. [Google Scholar] [CrossRef]
- Badr, C.; Spagnuolo, G.; Amenta, F.; Khairallah, C.; Mahdi, S.S.; Daher, E.; Battineni, G.; Baba, N.Z.; Zogheib, T.; Qasim, S.S.B.; et al. A Two-Year Comparative Evaluation of Clinical Performance of a Nanohybrid Composite Resin to a Flowable Composite Resin. J. Funct. Biomater. 2021, 12, 51. [Google Scholar] [CrossRef]
- Imai, A.; Takamizawa, T.; Sugimura, R.; Tsujimoto, A.; Ishii, R.; Kawazu, M.; Saito, T.; Miyazaki, M. Interrelation among the handling, mechanical, and wear properties of the newly developed flowable resin composites. J Mech Behav Biomed Mater. 2019, 89, 72–80. [Google Scholar] [CrossRef]
- G-aenial Universal Injectable from, GC. Technical Guide. Available online: https://www.gc.dental/europe/sites/europe.gc.dental/files/products/downloads/gaenialuniversalinjectable/manual/MAN_G-aenial_Universal_Injectable_Technical_Manual_en.pdf (accessed on 4 September 2024).
- Shaalan, O.O.; Abou-Auf, E.; El Zoghby, A.F. Clinical evaluation of flowable resin composite versus conventional resin composite in carious and noncarious lesions: Systematic review and meta-analysis. J Conserv Dent. 2017, 20, 380–385. [Google Scholar] [CrossRef]
- Geštakovski, D. The injectable composite resin technique: Minimally invasive reconstruction of esthetics and function. Clinical case report with 2-year follow-up. Quintessence Int. 2019, 50, 712–719. [Google Scholar] [CrossRef]
- Coachman, C.; De Arbeloa, L.; Mahn, G.; Sulaiman, T.A.; Mahn, E. An Improved Direct Injection Technique With Flowable Composites. A Digital Workflow Case Report. Oper Dent. 2020, 45, 235–242. [Google Scholar] [CrossRef]
- Hosaka, K.; Tichy, A.; Motoyama, Y.; Mizutani, K.; Lai, W.J.; Kanno, Z.; Tagami, J.; Nakajima, M. Post-orthodontic recontouring of anterior teeth using composite injection technique with a digital workflow. J Esthet Restor Dent. 2020, 32, 638–644. [Google Scholar] [CrossRef] [PubMed]
- Ypei Gia, N.R.; Sampaio, C.S.; Higashi, C.; Sakamoto, A.; Hirata, R. The injectable resin composite restorative technique: A case report. J Esthet Restor Dent. 2021, 33, 404–414. [Google Scholar] [CrossRef]
- Cortés-Bretón Brinkmann, J.; Albanchez-González, M.I.; Lobato Peña, D.M.; García Gil, I.; Suárez García, M.J.; Peláez Rico, J. Improvement of aesthetics in a patient with tetracycline stains using the injectable composite resin technique: Case report with 24-month follow-up. Br Dent J. 2020, 229, 774–778. [Google Scholar] [CrossRef] [PubMed]
- Hosaka, K.; Tichy, A.; Hasegawa, Y.; Motoyama, Y.; Kanazawa, M.; Tagami, J.; Nakajima, M. Replacing mandibular central incisors with a direct resin-bonded fixed dental prosthesis by using a bilayering composite resin injection technique with a digital workflow: A dental technique. J Prosthet Dent. 2021, 126, 150–154. [Google Scholar] [CrossRef] [PubMed]
- Ljubičić, M.; Živković, M. Multidisciplinary approach in treatment of spacing: Orthodontic treatment and partial ve-neers using the injectable composite resin technique. Serbian Dental Journal 2021, 68, 39–44. [Google Scholar] [CrossRef]
- Geštakovski, D. The injectable composite resin technique: Biocopy of a natural tooth - advantages of digital planning. Int J Esthet Dent. 2021, 16, 280–299. [Google Scholar]
- Hulac, S.; Kois, J.C. Managing the transition to a complex full mouth rehabilitation utilizing injectable composite. J Esthet Restor Dent. 2023, 35, 796–802. [Google Scholar] [CrossRef]
- Peumans, Μ. Geštakovski, D.; Mattiussi, J.; Karagiannopoulos, K. Injection moulding technique with injectable composites: Quick fix or long-lasting solution? Int Dent Afr. 2023, 13, 14–22. [Google Scholar]
- Hosaka, K.; Tichy, A.; Yamauti, M.; Watanabe, K.; Kamoi, K.; Yonekura, K.; Foxton, R.; Nakajima, M. Digitally Guided Direct Composite Injection Technique with a Bi-layer Clear Mini-Index for the Management of Extensive Occlusal Caries in a Pediatric Patient: A Case Report. J Adhes Dent. 2023, 25, 211–218. [Google Scholar] [CrossRef]
- Wu, J.; Zhu, J.; Yang, X.; Gao, J.; Yu, H. Technique to restore the midline space of central incisors using a two-in-one template: A clinical report. J Prosthodont. 2023, 32, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Villafuerte, K.R.V.; Obeid, A.T.; de Oliveira, N.A. Injectable Resin Technique as a Restorative Alternative in a Cleft Lip and Palate Patient: A Case Report. Medicina 2023, 59, 849. [Google Scholar] [CrossRef]
- Healy, M. Injectable composites in modern practice. Journal of the Irish Dental Association 2023, 69, 197–198. [Google Scholar] [CrossRef]
- Watanabe, K.; Tichy, A.; Kamoi, K.; Hiasa, M.; Yonekura, K.; Tanaka, E.; Nakajima, M.; Hosaka, K. Restoration of a Microdont Using the Resin Composite Injection Technique With a Fully Digital Workflow: A Flexible 3D-printed Index With a Stabilization Holder. Oper Dent. 2023, 48, 483–489. [Google Scholar] [CrossRef]
- Shui, Y.; Wu, J.; Luo, T.; Sun, M.; Yu, H. Three dimensionally printed template with an interproximal isolation design guide consecutive closure of multiple diastema with injectable resin composite. J Esthet Restor Dent. 2024, 1–7. [Google Scholar] [CrossRef]
- Rafeie, N.; Sampaio, C.S.; Hirata, R. Transitioning from injectable resin composite restorations to resin composite CAD/CAM veneers: A clinical report. J Esthet Restor Dent. 2024, 36, 1221–1227. [Google Scholar] [CrossRef]
- Muslimah, D.F.; Hasegawa, Y.; Antonin, T.; Richard, F.; Hosaka, K. Composite Injection Technique With a Digital Workflow: A Pragmatic Approach for a Protruding Central Incisor Restoration. Cureus. 2024, 16, e58712. [Google Scholar] [CrossRef]
- Branzan, R.; Taraboanta, I.; Tanasa, A.M.; Stoleriu, S.; Ghiorghe, A.C.; Pancu, G.; Georgescu, A.; Andra Taraboanta-Gamen, A.; Andrian, S. The use of flowable composite injection technique in a case of sever tooth wear. A case report. Int.J.Med.Dent. 2024, 28, 48–54. [Google Scholar]
- Watanabe, K.; Tanaka, E.; Kamoi, K.; Tichy, A.; Shiba, T.; Yonerakura, K.; Nakajima, M.; Han, R.; Hosaka, K. A dual composite resin injection molding technique with 3D-printed flexible indices for biomimetic replacement of a missing mandibular lateral incisor. J Prosthodont Res. 2024, 68, 667–671. [Google Scholar] [CrossRef] [PubMed]
- Rathod, P.; Patel, A.; Mankar, N.; Chandak, M.; Ikhar, A. Enhancing Aesthetics and Functionality of the Teeth Using Injectable Composite Resin Technique. Cureus. 2024, 16, e59974. [Google Scholar] [CrossRef]
- Alyahya, Y.; Alrebdi, A.; Farah, R.I.; Albazei, S.S.F. Esthetic Rehabilitation of Congenitally Peg-Shaped Lateral Incisors Using the Injectable Composite Resin Technique: A Clinical Report. J Pharm Bioallied Sci. 2024, 16, 1883–1887. [Google Scholar] [CrossRef]
- Zhu, J.; Wei, J.; Anniwaer, A.; Huang, C. Esthetic rehabilitation of labial tooth defects caused by caries of the anterior teeth using a composite resin injection technique with veneer-shaped 3D printing indices. J Prosthodont Res. 2025, 69, 127–132. [Google Scholar] [CrossRef]
- Spadoni, D.; Valeri, C.; Quinzi, V.; Schneider Moser, U.; Marzo, G. Advancing Orthodontic Aesthetics: Exploring the Potential of Injectable Composite Resin Techniques for Enhanced Smile Transformations. Dent. J. 2025, 13, 18. [Google Scholar] [CrossRef]
- Ammannato, R.; Ferraris, F.; Marchesi, G. The “index technique” in worn dentition: A new and conservative approach. Int J Esthet Dent 2015, 10, 68–99. [Google Scholar]
- Ammannato, R.; Rondoni, D.; Ferraris, F. Update on the “index technique” in worn dentition: A no-prep restorative approach with a digital workflow. Int J Esthet Dent 2018, 13, 516–537. [Google Scholar]
- Kouri, V.; Moldovani, D.; Papazoglou, E. Accuracy of Direct Composite Veneers via Injectable Resin Composite and Silicone Matrices in Comparison to Diagnostic Wax-Up. J. Funct. Biomater. 2023, 14, 32. [Google Scholar] [CrossRef]
- Terry, D.A.; Powers, J.M.; Mehta, D.; Babu, V. A predictable resin composite injection technique, part 2. Dent. Today. 2014, 33, 12. [Google Scholar]
- Jurado, C.A.; Tinoco, J.V.; Tsujimoto, A.; Barkmeier, W.; Fischer, N.; Markham, M. Clear matrix use for composite resin core fabrication. Int J Esthet Dent. 2020, 15, 108–117. [Google Scholar]
- Tolotti, T.; Sesma, N.; Mukai, E. Evolution of the Guided Direct Composite Resin Technique in Restorative Dentistry: A Systematic Review. J Esthet Restor Dent. 2024, 23, 1–18. [Google Scholar] [CrossRef]
- Beautifil Flow Plus: Safety Data Sheet. Available online: https://www.shofu.com/wp-content/uploads/Beautifil-Flow-Plus-SDS-US-Version-11.pdf (accessed on 5 September 2024).
- Kooi, T.J.; Tan, Q.Z.; Yap, A.U.; Guo, W.; Tay, K.J.; Soh, M.S. Effects of food-simulating liquids on surface properties of giomer restoratives. Oper Dent. 2012, 37, 665–671. [Google Scholar] [CrossRef] [PubMed]
- Tetric EvoFlow. Instructions for use. Available online: https://www.ivoclar.com/en_li/eifu?document-id=36624&show-detail=1 (accessed on 5 September 2024).
- G-aenial Universal Injectable. Available online: https://www.gc.dental/europe/sites/europe.gc.dental/files/products/downloads/gaenialuniversalinjectable/ifu/IFU_G-aenial_Universal_Injectable_W.pdf (accessed on 5 September 2024).
- G-aenial Universal Flo. Available online: https://www.gc.dental/europe/sites/europe.gc.dental/files/products/downloads/gaenialuniversalflo/ifu/IFU_G-aenial_Universal_Flo_W.pdf (accessed on 5 September 2024).
- Clearfil Majesty ES Flow. Available online: https://www.kuraraynoritake.eu/media/pdfs/IFU_CLEARFIL_MAJESTY_ES_Flow_1561R973R-007_WEB_22.pdf (accessed on 5th September 2024).
- Beautifil Injectable X: Safety Data Sheet. Available online: https://www.shofu.com.sg/wp-content/uploads/2020/05/SDS_BEAUTIFIL-Injectable-XVer.2.pdf (accessed on 15 February 2025).
- Tetric N-flow. Instructions for use. Available online: https://www.ivoclar.com/en_in/eifu?document-id=45433&show-detail=1 (accessed on 15 February 2025).
- Estelite Universal Flow. Product Instructions. Available online: https://www.tokuyama-us.com/estelite-universal-flow-dental-composite/ (accessed on 15 February 2025).
- Bonsor, S.J.; Pearson, G.J. A clinical guide to applied dental materials, 1st ed.; Churchill Livingstone Elsevier: London, UK, 2012; pp. 69–86. [Google Scholar]
- Hickel, R.; Peschke, A.; Tyas, M.; Mjör, I.; Bayne, S.; Peters, M.; Hiller, K.A.; Randall, R.; Vanherle, G.; Heintze, S.D. FDI World Dental Federation: Clinical criteria for the evaluation of direct and indirect restorations-update and clinical examples. Clin Oral Investig. 2010, 14, 349–366. [Google Scholar] [CrossRef] [PubMed]
- Larasati, N.; Rizal, M.F.; Fauziah, E. Comparing modified USPHS and FDI criteria for the assessment of glass ionomer restorations in primary molars utilising clinical and photographic evaluation. Eur Arch Paediatr Dent. 2024, 25, 367–373. [Google Scholar] [CrossRef]
- Marquillier, T.; Doméjean, S.; Le Clerc, J.; Chemla, F.; Gritsch, K.; Maurin, J.C.; Millet, P.; Pérard, M.; Grosgogeat, B.; Dursun, E. The use of FDI criteria in clinical trials on direct dental restorations: A scoping review. J Dent. 2018, 68, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Colwill, M.; Baillie, S.; Pollok, R.; Poullis, A. Using clinical cases to guide healthcare. World J Clin Cases. 2024, 12, 1555–1559. [Google Scholar] [CrossRef]
- Νair, S.R.; Niranjan, N.T.; Jayasheel, A.; Suryakanth, D.B. Comparative Evaluation of Colour Stability and Surface Hardness of Methacrylate Based Flowable and Packable Composite -In vitro Study. J Clin Diagn Res. 2017, 11, ZC51–ZC54. [Google Scholar] [CrossRef]
- Lai, G.; Zhao, L.; Wang, J.; Kunzelmann, K.H. Surface properties and color stability of dental flowable composites influenced by simulated toothbrushing. Dent Mater J. 2018, 37, 717–724. [Google Scholar] [CrossRef]
- Ujiie, M.; Tsujimoto, A.; Barkmeier, W.W.; Jurado, C.A.; Villalobos-Tinoco, J.; Takamizawa, T.; Latta, M.A.; Miyazaki, M. Comparison of occlusal wear between bulk-fill and conventional flowable resin composites. Am J Dent. 2020, 33, 74–78. [Google Scholar]
- Korkut, B.; Haciali, C. Color Stability of Flowable Composites in Different Viscosities. Clin Exp Health Sci. 2020, 10, 191–198. [Google Scholar] [CrossRef]
- Shimatani, Y.; Tsujimoto, A.; Barkmeier, W.W.; Fischer, N.G.; Nagura, Y.; Takamizawa, T.; Latta, M.A.; Miyazaki, M. Simulated Cuspal Deflection and Flexural Properties of Bulk-Fill and Conventional Flowable Resin Composites. Oper Dent. 2020, 45, 537–546. [Google Scholar] [CrossRef] [PubMed]
- Tsujimoto, A.; Irie, M.; Teixeira, E.C.N.; Jurado, C.A.; Maruo, Y.; Nishigawa, G.; Matsumoto, T.; Garcia-Godoy, F. Relationships between Flexural and Bonding Properties, Marginal Adaptation, and Polymerization Shrinkage in Flowable Composite Restorations for Dental Application. Polymers 2021, 13, 2613. [Google Scholar] [CrossRef]
- Niyomsujarit, N.; Worahan, A.; Chaichalothorn, M. Effects of cyclic acid challenge on the surface roughness of various flowable resin composites. M Dent J 2021, 41, 187–196. [Google Scholar]
- Degirmenci, A.; Degirmenci, B.U.; Salameh, M. Long-Term Effect of Acidic Beverages on Dental Injectable Composite Resin: Microhardness, Surface Roughness, Elastic Modulus, and Flexural Strength Patterns. Strength Mater 2022, 54, 331–343. [Google Scholar] [CrossRef]
- Ludovichetti, F.S.; Lucchi, P.; Zambon, G.; Pezzato, L.; Bertolini, R.; Zerman, N.; Stellini, E.; Mazzoleni, S. Depth of Cure, Hardness, Roughness and Filler Dimension of Bulk-Fill Flowable, Conventional Flowable and High-Strength Universal Injectable Composites: An In Vitro Study. Nanomaterials 2022, 12, 1951. [Google Scholar] [CrossRef] [PubMed]
- Jafarpour, D.; Ferooz, R.; Ferooz, M.; Bagheri, R. Physical and Mechanical Properties of Bulk-Fill, Conventional, and Flowable Resin Composites Stored Dry and Wet. Int J Dent. 2022, 2022, 7946239. [Google Scholar] [CrossRef]
- Khoramian Tusi, S.; Hamdollahpoor, H.; Mohammadi Savadroodbari, M.; Sheikh Fathollahi, M. Comparison of polymerization shrinkage of a new bulk-fill flowable composite with other composites: An in vitro study. Clin Exp Dent Res. 2022, 8, 1605–1613. [Google Scholar] [CrossRef] [PubMed]
- Turk, S.; Erden Kayalidere, E.; Celik, E.U.; Yasa, B. In vitro wear resistance of conventional and flowable composites containing various filler types after thermomechanical loading. J Esthet Restor Dent. 2024, 36, 643–651. [Google Scholar] [CrossRef]
- Uctasli, M.; Garoushi, S.; Uctasli, M.; Vallittu, P.K.; Lassila, L. A comparative assessment of color stability among various commercial resin composites. BMC Oral Health 2023, 23, 789. [Google Scholar] [CrossRef]
- Elsahn, N.A.; El-Damanhoury, H.M.; Shirazi, Z.; Saleh, A.R.M. Surface Properties and Wear Resistance of Injectable and Computer-Aided Design/Computer Aided Manufacturing-Milled Resin Composite Thin Occlusal Veneers. Eur J Dent. 2023, 17, 663–672. [Google Scholar] [CrossRef]
- Islam, M.S.; Nassar, M.; Elsayed, M.A.; Jameel, D.B.; Ahmad, T.T.; Rahman, M.M. In Vitro Optical and Physical Stability of Resin Composite Materials with Different Filler Characteristics. Polymers 2023, 15, 2121. [Google Scholar] [CrossRef] [PubMed]
- Elgammal, Y.A.; Temirek, M.M.; Hassanein, O.E.; Abdelaziz, M.M. The Effect of Different Finishing and Polishing Systems on Surface Properties of New Flowable Bulk-fill Resin Composite. J Contemp Dent Pract. 2023, 24, 587–594. [Google Scholar] [CrossRef]
- Vulović, S.; Stašić, J.N.; Ilić, J.; Todorović, M.; Jevremović, D.; Milić-Lemić, A. Effect of different finishing and polishing procedures on surface roughness and microbial adhesion on highly-filled composites for injectable mold technique. J Esthet Restor Dent. 2023, 35, 917–926. [Google Scholar] [CrossRef]
- Degirmenci, A.; Pehlivan, I.E.; Degirmenci, B.U. Effects of polishing procedures on optical parameters and surface roughness of composite resins with different viscosities. Dent Mater J. 2023, 42, 199–210. [Google Scholar] [CrossRef]
- Szczesio-Wlodarczyk, A.; Garoushi, S.; Vallittu, P.; Bociong, K.; Lassila, L. Polymerization shrinkage of contemporary dental resin composites: Comparison of three measurement methods with correlation analysis. J Mech Behav Biomed Mater. 2024, 152, 106450. [Google Scholar] [CrossRef]
- Chen, Y.; Bai, X.; Xu, M.; Zhou, T.; Loh, Y.M.; Wang, C.; Pow, E.H.N.; Tsoi, J.K.H. The mechanical, wear, antibacterial properties and biocompatibility of injectable restorative materials under wet challenge. J Dent. 2024, 146, 105025. [Google Scholar] [CrossRef] [PubMed]
- Bai, X.; Chen, Y.; Zhou, T.; Pow, E.H.N.; Tsoi, J.K.H. The chemical and optical stability evaluation of injectable restorative materials under wet challenge. J Dent. 2024, 146, 105031. [Google Scholar] [CrossRef] [PubMed]
- Miyashita-Kobayashi, A.; Haruyama, A.; Nakamura, K.; Wu, C.-Y.; Kuroiwa, A.; Yoshinari, N.; Kameyama, A. Changes in Gloss Alteration, Surface Roughness, and Color of Direct Dental Restorative Materials after Professional Dental Prophylaxis. J. Funct. Biomater. 2024, 15, 8. [Google Scholar] [CrossRef]
- Basheer, R.R.; Hasanain, F.A.; Abuelenain, D.A. Evaluating flexure properties, hardness, roughness and microleakage of high-strength injectable dental composite: An in vitro study. BMC Oral Health. 2024, 24, 546. [Google Scholar] [CrossRef]
- Szczesio-Wlodarczyk, A.; Garoushi, S.; Vallittu, P.; Bociong, K.; Lassila, L. Polymerization shrinkage stress of contemporary dental composites: Comparison of two measurement methods. Dent Mater J. 2024, 43, 155–163. [Google Scholar] [CrossRef]
- Rajabi, H.; Denny, M.; Karagiannopoulos, K.; Petridis, H. Comparison of Flexural Strength and Wear of Injectable, Flowable and Paste Composite Resins. Materials 2024, 17, 4749. [Google Scholar] [CrossRef] [PubMed]
- Tüter Bayraktar, E.; Kızıl Öztürk, E.; Saygılı, C.C.; Türkmen, C.; Korkut, B. Fluorescence and color adjustment potentials of paste-type and flowable resin composites in cervical restorations. Clin Oral Investig. 2024, 28, 649. [Google Scholar] [CrossRef]
- Gerges, P.; Labib, M.; Nabih, S.; Moussa, M. Fracture resistance of injectable resin composite versus packable resin composite in class II cavities: An in vitro study. Journal of Stomatology. 2024, 77, 153–160. [Google Scholar] [CrossRef]
- Checchi, V.; Generali, L.; Corciolani, L.; Breschi, L.; Mazzitelli, C.; Maravic, T. Wear and roughness analysis of two highly filled flowable composites. Odontology 2024, 113, 724–733. [Google Scholar] [CrossRef] [PubMed]
- Francois, P.; Attal, J.P.; Fasham, T.; Troizier-Cheyne, M.; Gouze, H.; Abdel-Gawad, S.; Le Goff, S.; Dursun, E.; Ceinos, R. Flexural Properties, Wear Resistance, and Microstructural Analysis of Highly Filled Flowable Resin Composites. Oper Dent. 2024, 49, 597–607. [Google Scholar] [CrossRef] [PubMed]
- Vulović, S.; Blatz, M.B.; Bukorović, J.; Živković, N.; Todorović, A.; Vencl, A.; Milić Lemić, A. Effect of acidic media on surface characteristics of highly filled flowable resin-based composites: An in vitro study. J Esthet Restor Dent. 2024, 2024, 1–12. [Google Scholar] [CrossRef]
- Kitasako, Y.; Sadr, A.; Burrow, M.F.; Tagami, J. Thirty-six month clinical evaluation of a highly filled flowable composite for direct posterior restorations. Aust Dent J. 2016, 61, 366–373. [Google Scholar] [CrossRef]
- Zhang, H.; Wang, L.; Hua, L.; Guan, R.; Hou, B. Randomized controlled clinical trial of a highly filled flowable composite in non-carious cervical lesions: 3-year results. Clin Oral Investig. 2021, 25, 5955–5965. [Google Scholar] [CrossRef]
- Elderiny, H.M.; Khallaf, Y.S.; Akah, M.M.; Hassanein, O.E. Clinical Evaluation of Bioactive Injectable Resin Composite vs Conventional Nanohybrid Composite in Posterior Restorations: An 18-Month Randomized Controlled Clinical Trial. J Contemp Dent Pract. 2024, 25, 794–802. [Google Scholar] [CrossRef]
- Hançer Sarıca, S.; Arslan, S.; Balkaya, H. Comparison of the 2-year clinical performances of class II restorations using different restorative materials. Clin Oral Investig. 2025, 29, 128. [Google Scholar] [CrossRef]
- Liu, J.; Zhang, H.; Sun, H.; Liu, Y.; Liu, W.; Su, B.; Li, S. The Development of Filler Morphology in Dental Resin Composites: A Review. Materials 2021, 14, 5612. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Wang, X.; Yang, J.; et al. Micromechanical interlocking structure at the filler/resin interface for dental composites: A review. Int J Oral Sci. 2023, 15, 21. [Google Scholar] [CrossRef]
- Lee, S.Y.; Kim, H.C.; Hur, B.; Park, J.K. Surface roughness and color stability of various composite resins. J Korean Acad Conserv Dent 2007, 32, 542–549. [Google Scholar]
- Draughn, R.A.; Harrison, A. Relationship between abrasive wear and microstructure of composite resins. J Prosthet Dent. 1978, 40, 220–224. [Google Scholar] [PubMed]
- Marghalani, H.Y. Effect of filler particles on surface roughness of experimental composite series. J Appl Oral Sci. 2010, 18, 59–67. [Google Scholar] [CrossRef]
- Abuelenain, D.A.; Neel, E.A.A.; Al-Dharrab, A. Surface and mechanical properties of different dental composites. Austin J Dent. 2015, 2, 1019. [Google Scholar]
- Filtek Z350XT. Technical Product Guide. Available online: https://multimedia.3m.com/mws/media/1363105O/3m-filtek-z350-xt-universal-restorative-tpp-la-apac.pdf (accessed on 15 February 2025).
- Oivanen, M.; Keulemans, F.; Garoushi, S.; Vallittu, P.K.; Lassila, L. The effect of refractive index of fillers and polymer matrix on translucency and color matching of dental resin composite. Biomater Investig Dent. 2021, 8, 48–53. [Google Scholar] [CrossRef]
- Yu, B.; Lee, Y.K. Differences in color, translucency and fluorescence between flowable and universal resin composites. J Dent. 2008, 36, 840–846. [Google Scholar] [CrossRef]
- Lee, Y.K.; Lim, B.S.; Rhee, S.H.; Yang, H.C.; Powers, J.M. Color and translucency of A2 shade resin composites after curing, polishing and thermocycling. Oper Dent 2005, 30, 436–442. [Google Scholar]
- Soliman, H.A.N.; Elkholany, N.R.; Hamama, H.H.; El-Sharkawy, F.M.; Mahmoud, S.H.; Comisi, J.C. Effect of Different Polishing Systems on the Surface Roughness and Gloss of Novel Nanohybrid Resin Composites. Eur J Dent. 2021, 15, 259–265. [Google Scholar] [CrossRef]
- Jefferies, S.R. Abrasive finishing and polishing in restorative dentistry: A state-of-the-art review. Dent Clin North Am 2007, 51, 379–397. [Google Scholar] [CrossRef]
- Karadas, M. The effect of different beverages on the color and translucency of flowable composites. Scanning. 2016, 38, 701–709. [Google Scholar] [CrossRef]
- Kim, K.H.; Ong, J.L.; Okuno, O. The effect of filler loading and morphology on the mechanical properties of contemporary composites. J Prosthet Dent. 2002, 87, 642–649. [Google Scholar] [CrossRef]
- Lee, Y.K. Influence of filler on the difference between the transmitted and reflected colors of experimental resin composites. Dent Mater. 2008, 24, 1243–1247. [Google Scholar] [CrossRef] [PubMed]
- Marghalani, H.Y. Effect of filler particles on surface roughness of experimental composite series. J Appl Oral Sci. 2010, 18, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Yu, P.; Yang, S.M.; Xu, Y.X.; Wang, X.Y. Surface roughness and gloss alteration of polished resin composites with various filler types after simulated toothbrush abrasion. J Dent Sci. 2023, 18, 1016–1022. [Google Scholar] [CrossRef] [PubMed]
- Pawlus, P.; Reizer, R.; Wieczorowski, M. Functional Importance of Surface Texture Parameters. Materials 2021, 14, 5326. [Google Scholar] [CrossRef]
- Turssi, C.P.; Ferracane, J.L.; Ferracane, L.L. Wear and fatigue behavior of nano-structured dental resin composites. J Biomed Mater Res B Appl Biomater. 2006, 78, 196–203. [Google Scholar] [CrossRef]
- Finlay, N.; Hahnel, S.; Dowling, A.H.; Fleming, G.J.P. The in vitro wear behavior of experimental resin-based composites derived from a commercial formulation. Dent Mater. 2013, 29, 365–374. [Google Scholar] [CrossRef]
- Osiewicz, M.A.; Werner, A.; Roeters, F.J.M.; Kleverlaan, C.J. Wear of direct resin composites and teeth: Considerations for oral rehabilitation. EurJ Oral Sci. 2019, 127, 156–161. [Google Scholar] [CrossRef]
- Mirică, I.C.; Furtos, G.; Bâldea, B.; Lucaciu, O.; Ilea, A.; Moldovan, M.; Câmpian, R.-S. Influence of Filler Loading on the Mechanical Properties of Flowable Resin Composites. Materials 2020, 13, 1477. [Google Scholar] [CrossRef] [PubMed]
- Heintze, S.D.; Reichl, F.X.; Hickel, R. Wear of dental materials: Clinical significance and laboratory wear simulation methods -A review. Dent Mater J. 2019, 38, 343–353. [Google Scholar] [CrossRef]
- Cerasmart. Instructions for Use. Available online: https://www.gc.dental/america/sites/america.gc.dental/files/products/downloads/cerasmart/ifu/cerasmart-ifu.pdf (accessed on 15 February 2025).
- Sideridou, I.; Tserki, V.; Papanastasiou, G. Effect of chemical structure on degree of conversion in light-cured dimethacrylate-based dental resins. Biomaterials. 2002, 23, 1819–1829. [Google Scholar] [CrossRef]
- Pratap, B.; Gupta, R.K.; Bhardwaj, B.; Nag, M. Resin based restorative dental materials: Characteristics and future perspectives. Jpn Dent Sci Rev. 2019, 55, 126–138. [Google Scholar] [CrossRef] [PubMed]
- McCabe, J.F.; Rusby, S. Water absorption, dimensional change and radial pressure in resin matrix dental restorative materials. Biomaterials. 2004, 25, 4001–4007. [Google Scholar] [CrossRef] [PubMed]
- Sideridou, I.D.; Karabela, M.M.; Vouvoudi, E.C. Dynamic thermomechanical properties and sorption characteristics of two commercial light cured dental resin composites. Dent Mater. 2008, 24, 737–743. [Google Scholar] [CrossRef] [PubMed]
- Gajewski, V.E.S. Monomers used in resin composites: Degree of conversion, mechanical properties and water sorption/solubility. Braz. Dent. J. 2012, 23, 508–514. [Google Scholar] [CrossRef] [PubMed]
- Imazato, S.; Tarumi, H.; Kato, S.; Ebi, N.; Ehara, A.; Ebisu, S. Water Sorption, Degree of Conversion, and Hydrophobicity Resins containing Bis-GMA and TEGDMA. Dent. Mater. J. 1999, 19, 124–132. [Google Scholar] [CrossRef]
- Szczesio-Wlodarczyk, A.; Kopacz, K.; Szynkowska-Jozwik, M.I.; Sokolowski, J.; Bociong, K. An Evaluation of the Hydrolytic Stability of Selected Experimental Dental Matrices and Composites. Materials 2022, 15, 5055. [Google Scholar] [CrossRef]
- Goņalves, F.; Kawano, Y.; Pfeifer, C.; Stansbury, J.W.; Braga, R.R. Influence of BisGMA, TEGDMA, and BisEMA contents on viscosity, conversion, and flexural strength of experimental resins and composites. Eur. J. Oral Sci. 2009, 117, 442–446. [Google Scholar] [CrossRef]
- Szczesio-Wlodarczyk, A.; Domarecka, M.; Kopacz, K.; Sokolowski, J.; Bociong, K. An Evaluation of the Properties of Urethane Dimethacrylate-Based Dental Resins. Materials 2021, 14, 2727. [Google Scholar] [CrossRef] [PubMed]
- Sideridou, I.; Tserki, V.; Papanastasiou, G. Study of water sorption, solubility and modulus of elasticity of light-cured dimethacrylate-based dental resins. Biomaterials. 2003, 24, 655–665. [Google Scholar] [CrossRef] [PubMed]
- Fleming, P.S.; Lynch, C.D.; Pandis, N. Randomized controlled trials in dentistry: Common pitfalls and how to avoid them. J Dent. 2014, 42, 908–914. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
A diagram illustrating the search process for the review.
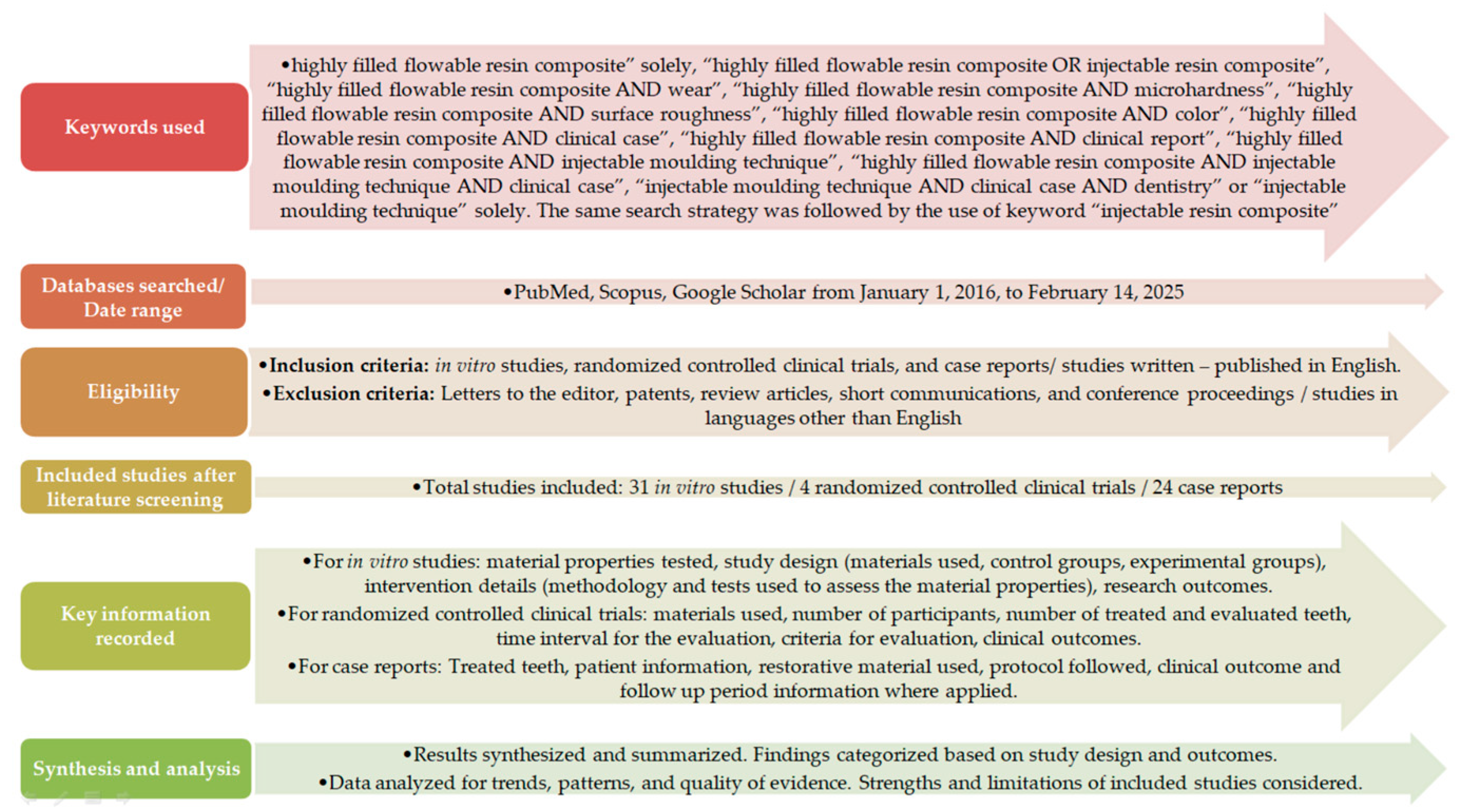

Table 1.
Clinical cases using flowable resin composites, emphasizing the injection moulding technique.
Table 1.
Clinical cases using flowable resin composites, emphasizing the injection moulding technique.
| Treated teeth | Patient record | Restorative material | Protocol | Follow up / Clinical outcome | Author/Year |
|---|---|---|---|---|---|
| 6 maxillary anterior teeth | 22 years old/ male | Beautiful Flow Plus F03 (Shofu Inc, Kyoto, Japan) | Analog workflow (one transparent silicon index and individual space holders from mock-ups) | 2-year follow-up → No soft tissue inflammation or significant wear | Gestakovski et al., 2019 [13] |
| 6 anterior teeth | 28 years old/ female | Tetric Evoflow (Ivoclar Vivadent, Lichtenstein) | Partially digital workflow (two transparent silicone indices based on the 3D printing models) | No follow-up period Excellent initial clinical outcomes |
Coachman et al.,2020 [14] |
| post-orthodontic recontouring of 4 maxillaty anterior teeth | 15 years old/ female | G-ænial Universal Injectable (GC, Japan) | Partially digital workflow (one transparent silicon index based on 3D printing models) | 5-month follow-up → no signs of wear and no defects | Hosaka et al., 2020 [15] |
| 8 maxillary teeth (upper right to left second premolars) | 28 years old/ female | G-aenial Universal Flo (GC, Japan) | Analog workflow (one transparent silicone index covered by 1 mm acetate plate expanded to adjacent teeth to achieve more stable fitting) | 1-year follow-up → staining of restoration and the tooth – material interface / presence of voids | Ypei Gia et al., 2020 [16] |
| 16 teeth with generalised tetracycline dental stains |
52 years old/ female | G-ænial Universal Injectable (GC, Japan) | Analog workflow (one transparent silicone index) | 2-year follow-up → no gingival infammation, bleeding on probing or wear | Cortés-Bretón Brinkmann et al., 2020 [17] |
| 2 missing mandibular incisors replaced with a direct bilayered resin bonded fixed dental prosthesis |
No information available | everX Flow for dentin and G-ænial Universal Injectable for enamel (GC Corp, Tokyo, Japan) |
Partially digital workflow: two 3d-printed casts (1st: dentin cast/ 2nd: anatomic wax-up cast) and two transparent silicon indices (Exaclear, GC) | 3-month follow-up → No signs of wear or soft tissue inflammation |
Hosaka et al., 2021 [18] |
| 4 maxillary anterior teeth (lateral incisors and canines) | 32 years old/ male | G-ænial Universal Injectable (GC, Japan) | Analog workflow (one transparent silicon index and stoppers made by C – silicone on the impression tray) | No follow-up period Excellent initial performance |
Ljubičić et al, 2021 [19] |
| maxillary lateral incisor and maxillary first premolar | 25 years old/ female | G-ænial Universal Injectable (GC, Japan) |
Partially digital workflow (one tansparent silicone index based on the 3D printed wax-up + two putty silicone stoppers) | 10-month follow-up → no wear, discoloration or periodontal problems | Gestakovski, 2021 [20] |
| transitional treatment of a complex full mouth rehabilitation | 53 years old/ male | G-aenial Universal Injectable (GC, Japan) | Analog workflow (two transparent silicon indices for each arch) | 6-month follow-up → no signs of tissue inflammation or wear |
Hulac et al., 2023 [21] |
| 4 clinical cases of: a. General wear in upper and lower jaw b. Six maxillary anterior teeth c. Full mandibular arch treatment d. Six maxillary anterior teeth |
No information except of the 4th case : 45 years old/ male |
G-ænial Universal Injectable (GC, Japan) | either digital or analog workflow either one or two indices |
12-month-, 20-month- and 24-month follow-up → smooth and shiny surfaces, absence of occlusal wear, chipping, marginal discoloration or tissue inflammation | Peumans et al., 2023 [22] |
| extensive posterior occlusal cavities | 13 years old/ female | Clearfil ES Flow Universal, (Kuraray Noritake, Tokyo, Japan) | Digital workflow (bi-layer clear mini-index with hard outer plastic layer and elastic inner silicone layer) | 1-year follow-up → Excellent outcome | Hosaka et al., 2023 [23] |
| symmetrical restoration of two central incisors | 50 years old/ female | Beautifil Flow Plus F00 (Shofu, Kyoto, Japan | Digital workflow (one custom-designed, two-in-one digital template) | No follow-up | Wu et al., 2023 [24] |
| re-recontouring of maxillary premolars to canines | 21 years old/ female | Tetric N-Flow (Ivoclar Vivadent, Schaan, Lichtenstein) |
Analog workflow (one transparent index) | 1-year follow-up → No marginal discoloration or fracture | Villafuerte et al., 2023 [25] |
| 2nd upper right premolar to upper left canine | 34 years old/ female | Not mentioned | Partially digital workflow (one transparent matrix based on digital wax up) | 1-year follow-up → no chipping and minimal staining | Healy, 2023 [26] |
| a microdont maxillary lateral incisor | 18 years old/ male | Clearfil ES Flow Universal (Kuraray Noritake, Japan) | Digital workflow (one 3d printed index including only two adjacent to the microdont lateral incisor teeth and labial and palatal extensions + digital stabilization holder) | 6-month follow-up → Excellent outcome | Watanabe et al., 2023 [27] |
| multiple diastema closure (6 teeth) | 41 years old/ female | Beautifil Flow Plus F00 (Shofu, Kyoto, Japan) | Digital workflow (3D-printed index with interproximal matrices to isolate interproximal contact areas) | 10-month follow-up → no signs of wear and soft tissue inflammation | Shui et al., 2024 [28] |
| 6 lower anterior teeth | 36 years old/ male | G-aenial Universal Flo (GC, Tokyo, Japan) |
Analog workflow (one transparent silicon index) | Annual follow-ups for 4 years → staining in the tooth – composite interface and chippings repaired every year | Rafeie et al., 2024 [29] |
| maxillary right central incisor | 42 years old/ male | Clearfil ES Flow Universal (Kuraray Noritake, Tokyo, Japan) | Partially digital workflow (one transparent silicone index based on 3D printed models) | 3-year follow-up → excellent clinical outcome | Muslimah et al., 2024 [30] |
| full mouth rehabilitation | 57 years old/ male | G-aenial Universal Injectable (GC, Tokyo, Japan) |
Partially digital workflow (one transparent silicone index based on 3D printing wax up models) | 1-year follow-up → No defects | Branzan et al., 2024 [31] |
| Replacement of a missing mandibular lateral incisor with direct composite resin-bonded fixed partial denture |
34 years old/ female | Estelite Universal Flow, (Tokuyama Dental Corp., Tokyo, Japan ) | Digital workflow (two 3D-printed indices representing the dentin layer index and the outer enamel layer index + stabilization holder) | 1-year follow-up → excellent treatment outcomes | Watanabe et al., 2024 [32] |
| six maxillary anterior teeth | 34 years old/ female |
Beautifil Injectable, (Shofu, Kyoto, Japan) | Analog workflow (one transparent silicone index) | 12-month follow-up → No wear, postoperative sensitivity, soft tissue inflammation |
Rathod et al., 2024 [33] |
| peg-shaped and malformed upper lateral incisors |
24 years old/ male | Beautifil Flow Plus F03 (Shofu, Kyoto, Japan) | Analog workflow (one transparent silicone index) | No follow-up | Alyahya et al., 2024 [34] |
| labial tooth defects caused by caries | 18 years old/ female | Beautifil Flow Plus F00; (Shofu, Kyoto, Japan) |
Digital workflow (veneer-shaped 3D printing indices) | 1-year follow-up → no signs of soft tissue inflammation or caries | Zhu et al., 2025 [35] |
| maxillary lateral incisors in two paediatric patients | 12.6 years old/ female 12.3 years old/ male |
G-ænial Universal Injectable (GC, Tokyo, Japan) | Digital workflow (one triple-layer transparent silicone index) | 6-year follow-up → no bleeding, staining or periodontal inflammation (Clinical case 1) 2-year follow up → no bleeding, no color change (Clinical case 2) |
Spadoni et al., 2025 [36] |
Table 2.
Composition of flowable composite resins used in the clinical cases.
| Flowable Composite Resin | Composition |
|---|---|
| Beautifil Flow Plus P03 or P00 (Shofu Inc., Kyoto, Japan) | 15 – 25 % by weight Bis-GMA, 10 – 20 %by weight TEGDMA S-PRG (surface pre reacted glass ionomer) filler based on 50 – 60 % by weight fluoroboroaluminosilicate glass, 1 – 5% by weight SiO2 and 1 – 5% by weight Al2O3, polymerization initiator, pigments and others. Particle size range: 0.01 to 4.0 μm Mean particle size: 0.8 μm [43,44] |
| Tetric Evoflow (Ivoclar Vivadent AG, Schaan, Lichtenstein) | Bis-GMA, UDMA, copolymer, barium glass, ytterbium trifluoride, Si-Zr mixed oxide, Inorganic filler content: 58% by weight / 30.7 - 33.7% by volume Particle size range: 0.11 μm to 15.5 μm [45] |
| G-aenial Universal Injectable (GC Corporation, Tokyo, Japan) | Dimethacrylate monomers and 69% by weight and approximately 50% by volume barium glass and silica fillers. Particle size range: 0.01 - 0.5 μm [46] |
| G-aenial Universal Flo (GC Corporation, Tokyo, Japan) | Dimethacrylate monomers and 69% by weight and approximately 50% by volume strontium glass and silica fillers. Particle size range: 0.01 - 1.0 μm [47] |
| Clearfil Majesty ES flow (Kuraray Noritake Dental, Tokyo, Japan) | Dimethacrylates and silanized barium glass and silica filler particles. Inorganic filler content: 48 to 64% by volume. Particle size range: 0.18 μm to 3.5 μm [48] |
| Beautifil Injectable X (Shofu Inc., Kyoto, Japan) | Bis-GMA, TEGDMA, Bis-MPEPP, S-PRG filler based on fluoroboroaluminosilicate glass, polymerization initiator, pigments and others. Inorganic filler content: 50-60% by weight [49] |
| Tetric N-Flow (Ivoclar Vivadent AG, Schaan, Lichtenstein) | Bis-GMA, UDMA, TEGDMA, ytterbium trifluoride, barium glass, bariumaluminium fluorosilicate glass, Si-Zr mixed oxide. Inorganic filler content: 38 – 40% by volume. Particle size range: 0.03 μm to 15.5 μm [50] |
| Estelite Universal Flow, Medium Viscosity (Tokuyama Dental Corporation, Tokyo, Japan) | Dimethacrylates (Bis-GMA, Bis-MPEPP, TEGDMA, UDMA) and spherical silica-zirconia filler and composite filler Inorganic filler content: 71% by weight/ 57% by volume Mean particle size: 200 nm Particle size range: 100 to 300 nm [51] |
Table 3.
In vitro studies incorporating highly filled flowable resin composites in their design.
| Parameters Tested | Type of Specimens/Type of Control Groups/Procedures | Tests | Conclusions | Author/Year |
|---|---|---|---|---|
| color stability - surface hardness |
(1) G-aenial Universal Flo (GC Corporation, Tokyo, Japan) (2) Filtek Z350XT (3M ESPE, St. Paul, MN, USA) (3) Tetric N Ceram (Ivoclar Vivadent AG, Schaan, Lichtenstein) immersion in coffee for 72 hours + tooth brushing simulation |
(a) Spectrophotometer measurements every 72 hours for 3 weeks (b) Microhardness tester |
color stability and surface hardness: Filtek Z350XT > Tetric N Ceram > G-aenial Universal Flo Inferior properties of G-aenial Universal Flo |
Nair et al., 2017 [57] |
| surface gloss - surface roughness - color stability |
(1) four traditional flowable composites: a. GrandioSO Flow (VOCO GmbH, Cuxhaven, Germany), b. Arabesk Flow (VOCO GmbH, Cuxhaven, Germany) c. Kerr Revolution Formula 2 (Kerr, Orange, CA, USA) d. Gradia Direct LoFlo (GC Corporation, Tokyo, Japan) (2) one self-adhering flowable composite: Kerr Vertise Flow (Kerr, Orange, CA, USA) (3) one universal injectable composite: G-ænial Universal Flo Experimental groups: toothbrushing simulation (Willytec, Munich, Germany) Control groups: No toothbrushing simulation Polishing procedure: Grinding up to 4000-grit by silicon carbide papers under running water + ultrasonication |
(a) glossmeter for Gloss Units measurements (b) optical profiler for Ra measurements (c) spectrophotometer for color change (ΔΕ) (d) Scanning Electron Microscopy (SEM) observation |
Highly filled flowable composite showed:
|
Lai et al., 2018 [58] |
| handling - mechanical properties - wear |
Experimental groups: Six flowable composite resins (1) Beautifil Flow Plus F00 (BF; Shofu Inc., Kyoto, Japan) (2) Clearfil Majesty ES Flow (CE; Kuraray Noritake Dental Inc., Tokyo, Japan) (3) Estelite Universal Flow (EU; Tokuyama Dental Corp, Tokyo, Japan) (4) Filtek Supreme Ultra Flowable Restorative (FS; 3M ESPE, St. Paul, MN, USA) (5) G-ænial Universal Flow (GU) (6) Gracefil Zero Flow (GZ; GC Corp., Tokyo, Japan) Control groups: two conventional resin composites: (7) micro hybrid, Clearfil AP-X (AP; Kuraray Noritake Dental Inc., Tokyo, Japan) (8) nano filled resin composite, Filtek Supreme Ultra (SU; 3M ESPE, St. Paul, MN, USA) Uniform polishing procedure: Grinding up to 1200-grit by silicon carbide paper discs |
(a) thermogravimetry/differential thermal analysis (TG/DTA) for filler content measurement (b) ISO 4049:2019 specifications and three-point bending test for flexural strength, flexural modulus and modulus of resilience evaluation (c) Confocal laser scanning microscope (CLSM) for maximum depth and volume loss of wear facets (d) universal testing machine for extrusion force measurement (e) creep meter for thread formation (stickiness) (f) SEM analysis |
Flowable resins show:
Conventional nanofilled resin presents significantly lower volume loss compared to the other materials. Significantly higher thread formation for GU compared to the other resin composites. Increasing the inorganic filler content did not enhance the physical properties of highly filled flowable resin composites. |
Imai et al., 2019 [10] |
| occlusal wear | (1) Filtek Bulk Fill Flowable Restorative (3M ESPE, St. Paul, MN, USA) (2) G-aenial Bulk Injectable (GC Corp., Tokyo, Japan) (3) SDR flow + (Dentsply, York, PA, USA) (4) Tetric EvoFlow Bulk Fill (Ivoclar Vivadent AG, Schaan, Lichtenstein) (5) Clearfil Majesty IC (Kuraray Noritake Dental Inc., Tokyo, Japan) (6) Filtek Supreme Ultra Flow (7) G-aenial Universal Flo (8) Herculite XRV Ultra Flow (Kerr, Orange, CA, USA) Universal polishing procedure: Grinding up to 4000-grit by silicon carbide paper discs Wear simulation by 400,000 cycles in a Leinfelder-Suzuki device with a stainless steel ball bearing antagonist |
Non-contact profilometer and SEM analysis for volume loss and maximum depth of wear evaluation | G-aenial bullk injectable, G-aenial Universal Flo and Filtek Supreme Ultra Flow showed significantly less wear and significantly lower volume loss than the other flowable materials | Ujiie et al., 2020 [59] |
| color stability | (1) two high-viscosity flowable composites (G-aenial Injectable, GC, Tokyo, Japan; Estelite Super Low Flow, Tokuyama Dental, Tokyo, Japan) (2) a bulk-fill flowable composite (Filtek Bulk-Fill Flowable) (3) a low viscosity flowable composite (Filtek Ultimate Flowable, 3M ESPE, St. Paul, MN, USA) (4) a packable composite (Filtek Ultimate, 3M ESPE, St. Paul, MN, USA) Uniform polishing procedure: Sof-Lex polishing discs (3M ESPE, St. Paul, MN, USA) Experimental groups: Immersion in various colorant solutions (coke, tea, coffee, red wine) Control group: Immersion in saline |
(a) spectrophotometer (EasyShade IV, Vita, Germany) (b) colorimeter (ShadeStar, Dentsply Sirona, USA) for color measurements in two time intervals: immediately after discoloration for 144 hours in an incubator at 37°C and after repolishing |
Color stability is material dependent and colorant solution dependent. Filtek Ultimate flowable presented the highest level of color change in both time intervals Color stability of high viscosity flowable composite materials is comparable to that of packable composite. |
Korkut et al., 2020 [60] |
| cuspal deflection - flexural properties |
Five bulk-fill flowable composite resins: (1) Beautifil Bulk Flowable (BF; Shofu, Kyoto, Japan) (2) Bulk Base (BB; Sun Medical, Shiga, Japan) (3) Filtek Fill and Core (FF; 3M ESPE, St Paul, MN, USA) (4) SDR (SD; Dentsply Sirona, York, PA, USA) (5) X-tra base (XB; VOCO GmbH, Cuxhaven, Germany) and six conventional flowable resin composites: (6) Clearfil Majesty ES Flow (CE) (7) Clearfil Majesty LV (CL) (8) Estelite Universal Flow (EU) (9) G-ænial Universal Injectable (GI) (10) Filtek Supreme Ultra Flowable (FS) (11) UniFil LoFlo Plus (UF; GC, Tokyo, Japan). Uniform polishing procedure: Silicon carbide papers of 600 – grit size. |
(a) Simulated cuspal deflection by the use of aluminium block milled for MOD (mesial – occlusal – distal) cavities assessed by 2 different measurement techniques: a. Micrometer b. CLSM (b) three-point bending test on a universal testing machine for flexural strength and modulus evaluation (c) SEM analysis |
Cuspal deflection, flexural strength and modulus are material dependent Higher cuspal deflection of the conventional flowable resin composites compared to bulk fill flowable resin composites Conventional highly filled flowable resin composites present the highest flexural strength and modulus Significant correlation between flexural properties and cuspal deflection of resin composites |
Shimatani et al., 2020 [61] |
| flexural properties - bonding properties - marginal adaptation - polymerization shrinkage |
4 highly filled flowable composites: (1) Beautifil Flow Plus X F03 (BF) (2) Clearfil Majesty ES Flow Low (CM) (3) Estelite Universal Flow Medium Flow (EU) (4) G-ænial Universal Injectable (GU). Traditional flowable composite (5) Unifil LoFlow Plus (UP, GC, Tokyo, Japan) Bulk fill flowable composite (6) Filtek Bulk Fill Flowable (FF) The adhesive system recommended by the manufacturer of each company was used. The materials properties were evaluated in two time intervals: t1: 10 min after curing t2: 24 h after curing |
(a) ISO 4049:2019 (3-point bending test by a universal testing machine) for flexural properties (b) shear bond strength to enamel and dentin by the universal testing machine (c) traveling microscope for marginal adaptation (d) bonded-disk method using a uni-axial linear variable displacement transducer (LVDT) for polymerization shrinkage (e) Aluminum cuspal deflection method for polymerization shrinkage stress |
The new generation flowable composites showed significantly higher:
|
Tsujimoto et al., 2021 [62] |
| surface roughness | 1. G-ænial Universal Injectable 2. Beautifil Injectable X 2. Filtek Z350XT Flowable Restorative 4. Filtek Z350XT Universal Universal finishing – polishing procedure: Abrasive sandpaper discs of 800-, 1200-, 2000-, 2400 grit size + ultrasonic cleansing Experimental groups: cyclic acid challenge with 0.5% citric acid (pH: 2.3) Control group: absence of cyclic acid challenge |
(a) Surface roughness evaluation (Ra parameter) by a contact stylus profilometer (b) Scanning Electron Microscopy (SEM) analysis |
Statistically significant differences in Ra values after citric acid challenge between all materials tested (conventional composite resin presented the most favorable surface roughness values) After cyclic acid challenge Beautifil Injectable X presented statistically significant higher Ra values when compared to the control. |
Niyomsujarit et al., 2021 [63] |
| surface roughness - microhardness - flexural strength - elastic modulus |
(1) Estelite Bulk Fill Flow, Tokuyama Corp., Tokyo, Japan (2) G-aenial Posterior, GC Europe N.V., Leuven, Belgium (3) G-aenial Universal Injectable Polishing procedure: Grinding up to 1200-grit by silicon carbide paper discs + ultrasonication randomly divided for immersion into: I. coke II. orange juice, III. into artificial saliva (control group) measured: A. before exposure to beverages B. on the first day C. first week D. first month E. first year |
(a) Surface roughness by 3D non-contact profilometer (Contour GT-K 3D Optical Microscope, Bruker, Izmir, Turkey) (Ra values) (b) Microhardness assessment by a Vickers microhardness device (HMV-G 31 Microhardness Tester, Shimadzu Corporation, Japan) (c) Elastic modulus and flexural strength measurements according to ISO 4049 recommendations (d) SEM analysis |
Microhardness values: Microhybrid > bulk fill > injectable composite Elastic modulus: Bulk fill > injectable > microhybrid composite Flexural strength: Injectable > bulk fill > microhybrid composite Surface roughness: Injectable > bulk fill > microhybrid composite Acidic beverages affected the surface roughness, microhardness, flexural strength, and elastic modulus values of all materials tested including the new injectable composite The injectable composite exposed to short- and long-term immersion cycles exhibited flexural strength values above the ISO 4049/2019 standard. |
Degirmenci et al., 2022 [64] |
| depth of cure (DOC) - hardness - surface roughness - filler dimensions |
(1) Filtek Bulk Fill Flowable Restorative (bulk fill flowable), (2) Tetric EvoFlow Bulk Fill (bulk fill flowable) (3) Filtek Supreme XTE Flowable Restorative (nanofilled flowable) (4) G-ænial Flo X (microhybrid flowable composite) (5) G-ænial Universal Injectable (high-strength injectable composite) |
a. ISO 4049 scrape technique for DOC b. 3D laser confocal microscope (LEXT OLS 4100; Olympus) for durface roughness (Ra values) c. Vickers diamond indenter (Vickers microhardness tester, Shimadzu, Kyoto, Japan) for hardness d. SEM images at 3000 and 9000 magnification for filler content |
DOC: Bulk-fill flowables > highly filled flowable > traditional flowables Hardness: Bulk fill flowables = highly filled injectable > traditional flowable resin Surface roughness: Bulk fill flowables > highly filled injectable |
Ludovichetti et al., 2022 [65] |
| filler weight (FW) - fracture toughness (FT) - Vickers hardness (VHN) - sorption/solubility (S/S) - color change (ΔE) |
(1) Aura bulk-fill (AB) (SDI, Bayswater, Victoria, Australia) (bulk fill composite resin) (2) Tetric EvoCeram (TE) (Ivoclar Vivadent) (bulk fill composite resin) (3) G-ænial Universal Flo (GUF) (GC) (highly filled flowable composite resin) (4) GC Kalore (GCK) (GC, Tokyo, Japan) (conventional composite resin) Stored: I. dry II. wet in distilled water subcategorized in three groups: A. Stored for one day B. Stored for 7 days C. Stored for 60 days |
a. standard ash method for filler weight b. 4-point test jig using a universal testing machine for fracture toughness c. Digital hardness tester for microhardness d. ISO 4049 for sorption/solubility e. Standard Commission Internationale de L’Eclairage (CIE Lab) for color stability |
Highly filled flowable resin composite had:
After 60 days, the color changes of all resin composites used in this study were clinically invisible. |
Jafarpour et al., 2022 [66] |
| polymerization shrinkage | (1) G-aenial Universal Flo (GUF) (2) Filtek Z250, 3M ESPE, St. Paul, MN, USA (3) G-aenial bulk injectable (GBI) (4) X-tra base (XB) (5) X-tra fil (XF), VOCO, Cuxhaven, Germany Polymerization shrinkage evaluation in 4 time intervals t1:1 sec t2:30 sec t3: 60sec t4:1800s |
Relative linear shrinkage assessment and shrinkage strain rate evaluation by numerical differentiation of the shrinkage strain data with respect to time | Polymerization shrinkage values: G-aenial Bulk Injectable = G-aenial Universal Flo > XF = Z250 =XB |
Khoramian Tusi et al., 2022 [67] |
| wear resistance |
Experimental groups: (1) nanohybrid conventional (G-aenial Posterior) and flowable (G-aenial Universal Injectable) composite resins, (2) a nanofilled bulk (Filtek One Bulk-fill Restorative) and flowable (Filtek Ultimate Flow) composite resin (3) submicron-filled conventional (Estelite Posterior Quick, Tokuyama, Tokyo, Japan) and flowable (Estelite Bulk-Fill Flow, Tokuyama, Tokyo, Japan) composite resin Control group: buccal surfaces of extracted human premolars thermomechanical chewing simulation for 240,000 cycles |
volume loss and maximum depth of loss calculation by laser scanner device | wear volume loss and loss depth:
|
Turk et al., 2023 [68] |
| color stability | (1) Filtek Universal Restorative (3M ESPE) (2) SDR flow+ (Dentsply) (3) everX Flow (GC, Tokyo, Japan) (4) G-ænial A’CHORD (GC, Tokyo, Japan) (5) G-ænial Universal Flo (GC) (6) G-ænial Universal Injectable (GC) Polishing procedure: a. By machine (1000-grit, 2000-grit and 4000-grit abrasive paper discs) b. Or by hand (3 M Sof-Lex Diamond Polishing System, 3M ESPE, St. Paul, MN, US) Immersed in five different beverages: a. Distilled water (control group) b. Coffee c. Red wine d. Energy drink e. Coke color change measurement in three time periods: i. Baseline ii. 84 days after immersion iii. After repolishing |
Color stability assessment by the use of a spectrophotometer (ΔE) | The flowable composites (traditional and highly filled) showed similar ΔΕ values to the conventional composite materials in the hand polished groups. SDR flow+ in coffee and wine presented the highest ∆E when compared to other tested materials (above the threshold of clinically acceptable color change) repolishing serves as an effective technique for eliminating surface discoloration in composite restorations |
Uctasli et al., 2023 [69] |
| microhardness - surface roughness - wear |
1mm thin, conservative occlusal veneers fabricated by: (1) Cerasmart blocks, Cerasmart, GC, Tokyo, Japan (CS) (indirect CAD/CAM technique) (2) Beautifil Injectable X (BF) (3) G-ænial Universal Injectable (GU) (4) SonicFill 2, Kerr, Orange, CA, USA (SF) |
(a) three-dimensional scanning i. before ii. after thermomechanical cyclic loading for wear assessment (b) optical profilometer for surface roughness (Ra value) (c) microhardness tester for VHN (d) SEM analysis |
VHN: CS> GU =SF > BF surface roughness: SF > BF > CS > GU volumetric wear: SF > BF > CS > GU GU injectable occlusal veneers are less influenced by thermomechanical cyclic loading than CS milled veneers BF and SF: significant volumetric loss and increased Ra values which might limit their clinical use as thin occlusal veneers |
Elsahn et al., 2023 [70] |
| physical stability - optical stability |
(1) Beautifil Injectable X (injectable flowable resin based material) (2) Beautifil II LS (low shrinkage paste resin based material), Shofu, Kyoto, Japan (3) CharmFil flow (flowable composite resin), Dentkist Inc, Gunpo-si, Gyeonggi-do, Korea (4) CharmFil Plus (nanofilled composite resin), Dentkist Inc, Gunpo-si, Gyeonggi-do, Korea No information available concerning the polishing procedure Aging after thermocycling and staining challenge |
(a) micro-hardness tester (Wilson Tukon 1102, Buehler, Echterdingen, Germany) for Vickers hardness (VH) (b) water sorption and solubility (WS/SL) tests (c) digital spectrophotometer for color change assessment |
Hardness values: packable – conventional resin > highly filled injectable flowable material > traditional flowables Beautifil Injectable X and II LS showed negative WS, whereas the other groups had positive values All groups showed significant color alterations after one week of the staining challenge |
Islam et al., 2023 [71] |
| surface roughness - surface gloss |
G-aenial Bulk Injectable flowable resin composite, GC 2 different polishing procedures: I. The two-step Sof-Lex spiral wheels system (Solventum) II. The multiple-step Sof-Le XT disks (Solventum) 2 different time intervals: A. After polishing B. After three months immersed in 2 different liquids: a. artificial saliva (control group) b. Coca-Cola. |
(a) optical profilometer for surface roughness (Ra measurment) (b) Horiba gloss checker |
Improved surface roughness and gloss by using the multiple-step polishing system Acidic media had a negative impact on surface roughness and surface gloss of the resin composite material |
Elgammal et al., 2023 [72] |
| surface roughness - microbial adhesion and viability of Streptococcus mutans |
(1) Filtek Supreme Flowable Restorative (2) Tetric EvoFlow (3) G-aenial Universal Flo (4) G-aenial Universal Injectable Four different polishing procedures: 1. Sof-Lex discs, 3M ESPE, St. Paul, MN, USA (SLD) 2. Sof-Lex Spirals, 3M ESPE, St. Paul, MN, USA (SLS) 3. One Gloss, Shofu, Tokyo, Japan (OG) 4. PoGo, Dentsply/Caulk, Milford, DE, USA (PG) |
(a) optical profiler(Ra and Rz) for surface roughness (b) Scanning electron microscopy (SEM) (c) colony forming unit (CFU) and cell viability assay for biofilm analysis |
Both material and polishing procedures affect surface roughness and microbial adhesion GUI adhered the lowest amount of Strep.mutans, due to the smoothest surfaces. The smoothest surfaces possess GUI and GUF, among materials and SLD and SLS, among polishing procedures |
Vulovic et al., 2023 [73] |
| optical properties - surface roughness |
(1) Microhybrid conventional composite resin (G-ænial Anterior, GC, Tokyo, Japan) (2) Highly filled flowable composite resin (G-ænial Universal Flo) (3) Highly filled injectable flowable composite resin (G-ænial Universal Injectable) Polishing procedure: specimens grinded for 180s manual grinding up to 1200-grit by silicon carbide papers Experimental groups: 1. Multi step rubber polishing discs (Sof-Lex polishing discs) 2. Two step flexible polishing discs (CLEARFIL Twist DIA, EVE Ernst Vetter, Keltern, Germany Control group: no further commercial polishing |
(a) spectrophotometer for optical properties analysis (L*a*b) translucency assessment: TP and TP00 equations opalescence evaluation: OP-BW equation chroma evaluation: C*ab formula (b) refractive index assessment (RI) by the use of Abbe refractometer (c) optical profilometer for surface roughness (d) SEM analysis (e) Atomic Force Microscopy (AFM) analysis |
Highly filled flowable injectable composite had the highest translucency and opalescence and the lowest chroma value the polishing procedure did not significantly affect the RI the composite type and polishing procedure show statistical significant effects on surface roughness |
Degirmenci et al., 2023 [74] |
| polymerization shrinkage | (1) EverX Posterior (GC, Tokyo, Japan) (2) EverX Flow Bulk (GC, Tokyo, Japan) (3) EverX Flow Dentin (GC, Tokyo, Japan) (4) G-aenial Anterior (5) G-aenial Posterior (6) G-aenial A’chord (GC, Tokyo, Japan) (7) G-aenial Universal Injectable (8) Filtek One Bulk Fill (9) Filtek Universal Restorative (10) SDR + Flow (11) Aura Bulk Fill (SDI, Bayswater, Victoria, Australia) |
(a) Polymerization shrinkage assessment by i. Buoyancy method ii. Linear strain gauge method iii. Depth measurements (b) filler content (wt. %) by ashing-in-air technique (c) flexural modulus by 3 point bending test following the ISO 4049:2019 specifications (d) degree of conversion (DOC) by Fourier Transformed Infrared Spectroscopy (FTIR) |
Shrinkage values, obtained by the buoyancy method, are greater than those of the strain gauge The highest volume shrinkage and linear shrinkage values were observed for the highly filled flowable composite resin Volumetric filler amount correlates with shrinkage values The lowest DOC is present in the highly filled flowable composite resin composite (G-aenial Universal Injectable) There are some differences (around 10 %) between the filler content (wt. %) measured by the ashing-in-air method and the data given by the manufacturers. |
Szczesio-Wlodarczyk et al., 2024 [75] |
| mechanical properties - wear - antibacterial properties - biocompatibility |
Three highly filled flowable composite resins: (1) G-aenial Universal Injectable, (GU) (2) Beautifil Injectable XSL (BI), (3) Filtek Supreme Flowable (FS) and a compomer: (4) Dyract Flow, Dentsply, York, PA, USA (DF) Uniform polishing procedure: silicon carbide abrasive papers (600-, 1000-, 2000- grit size) time intervals of investigation: a. immediately after preparation b. after 1-day c. 7-day d. 14-day e. 30-day water storage |
(a) three-point bending test in accordance with ISO 4049:2019 for flexural strength, modulus and elastic recovery (b) Three body wear test for volume loss and wear depth assessment (c) an optical interferometer (Ra values) for surface roughness (d) SEM analysis (e) CCK-8 test for cell viability (f) Confocal Laser Scanning Microscopy (CLSM) and SEM for cell morphology (g) CFU counting, CLSM, and SEM for S.mutans adherence |
Mechanical properties are material-dependent and sensitive to water storage CFU counting: no significant differences between the materials GU and FS had more favorable cell adhesion and morphology Flexural strength: GU > FS > BI > DF at all testing levels FS presented a slightly thicker biofilm and BI showed lower bacteria density Superior properties of highly filled injectable composite resins |
Chen et al., 2024 [76] |
| chemical stability - optical stability |
Highly filled flowable resin composites + compomer (1) G-aenial Universal Injectable (GU) (2) Beautifil Injectable XSL (BI), (3) Filtek Supreme Flowable (FS) (4) Dyract Flow (DF) Uniform polishing procedure: silicon carbide abrasive papers (up to 2000- grit) |
(a) ISO4049:2019 standard for water sorption/solubility (b) inductively coupled plasma optical emission spectroscopy (ICP-OES) and F-ion selective electrode for elemental release (c) FTIR for degree of convertion immediately after curing and 24 hours later (d) Contact angle measurement by sessile drop method for wettability (e) color difference (ΔE), lightness difference (ΔL) and translucency (TP) by a spectrophotometer and the CIEL*a*b* values |
G-aenial Universal Injectable exhibits:
Both material type and duration of water storage affected the optical properties |
Bai et al., 2024 [77] |
| surface gloss - surface roughness - color change |
1. Estelite Universal Flow (EUF) 2. Beautifil Flow Plus F00 (BFP) 3. GC Fuji II, GC, Tokyo, Japan (FLC) 4. GC Fuji IX GP EXTRA, GC, Tokyo, Japan (FGP) Divided into four groups of prophylaxis procedures: Group 1: Load of 100 gf, 10 s, 4× Group 2: Load of 100 gf, 30 s, 4× Group 3: Load of 300 gf, 10 s, 4× Group 4: Load of 300 gf, 30 s, 4× |
(a) glossmeter (GD-26, Murakami Color Research Laboratory, Tokyo, Japan) for surface gloss (b) surface profilometer (Surfcom 130A, Tokyo Seimitsu, Tokyo, Japan) (Ra, Rz, Ry values) (c) Spectrophotometer(Vita Easyshade V, Vita Zahnfabrik, Bad Sackingen, Germany) for color change (d) 3D Measuring Laser Microscope for surface observation (e) SEM observations |
Highly filled flowable resins presented favorable surface characteristics compared to glass ionomer cements The higher loadings and longer durations of dental prophylaxis might affect surface characteristics, depending on the material |
Miyashita-Kobayashi et al., 2024 [78] |
| physical and mechanical properties |
Experimental groups: Four types of highly filled flowable composites: (1) G-aenial Universal Flo (2) G-aenial Universal Injectable (3) Beautifl Injectable (4) Beautifl Flow Plus Control group: nanohybrid conventional resin composite (5) Filtek Z350 XT, 3M ESPE |
a. universal testing machine for flexural strength and elastic modulus b. optical profilometer (Ra parameter) for surface roughness c. microhardness tester (HMG-G; Shimadzu, Kyoto, Japan) for VHN d. Microleakage evaluation in class V cavities by the use of methylene blue solution |
Variations in highly filled flowable resins concerning physical and mechanical properties. Flexural strength: no statistically significant difference between all highly filled flowables and the control elastic modulus: Filtek Z350 presented higher elastic modulus compared to experimental groups VHN: Control group > experimental groups surface roughness: no differences observed between groups microleakage: control group > highly filled flowables |
Basheer et al., 2024 [79] |
| polymerization shrinkage stress | Conventional composite resins + highly filled flowable resin + bulk fill composite resin + flowable bulk-fill composite resins: (1) EverX Posterior (2) EverX Flow Bulk (3) G-aenial Anterior (4) G-aenial Posterior (5) G-aenial A’chord (6) G-aenial Universal Injectable (7) Filtek One Bulk Fill (8) Filtek Universal Restorative (9) SDR + Flow (10) Aura Bulk Fill |
Polymerization shrinkage stress evaluation by the use of two different methods a. Contraction forces measurement b. Photoelastic analysis |
Shrinkage stress values: photoelastic method > contraction forces measurements No differences in polymerization shrinkage stress values between conventional composite resins and the highly filled flowable resin composite. |
Szczesio – Wlodararczyk et al., 2024 [80] |
| wear - flexural strength |
1. G-aenial Universal Injectable 2. Beautifil Plus F00 3. Tetric EvoFlow and a conventional composite resin: 4. Empress Direct (Ivoclar Vivadent AG, Schaan, Lichtenstein) wear simulation by 200,000 cycles |
(a) Two-body wear test (b) Three-point bending test for flexural strength, flexural modulus and modulus of resilience (c) SEM observations |
G-aenial Universal Injectable and Beautifil Plus F00 presented:
Injectable, highly filled flowable composite resins may be suitable to use in occlusal, load-bearing areas |
Rajabi et al., 2024 [81] |
| Fluorescence adjustment level - Color adjustment level |
Class V cavities of 50 extracted human teeth restored by: Five paste-type resin composites: (1) Omnichroma (Tokuyama Dental Corporation, Tokyo, Japan) (2) G-aenial A-Chord (3) Estelite Asteria (Tokuyama Dental Corporation, Tokyo, Japan) (4) Clearfil Majesty ES-2 (Kuraray Noritake, Tokyo, Japan) (5) Charisma Diamond One (Kulzer Dental, Hanau, Germany) and five highly-filled flowable composites: (6) Omnichroma flow (Tokuyama Dental Corporation, Tokyo, Japan) (7) G-aenial Injectable (GC, Japan) (8) Estelite Universal Flow (Tokuyama Dental Corporation, Tokyo, Japan) (9) Clearfil Majesty Low Flow (Kuraray Noritake, Tokyo, Japan) (10) Charisma Diamond One Flow (Kulzer Dental, Hanau, Germany) Polishing procedure: two-step diamond spiral wheels |
color adjustment (ΔECP) and fuorescence adjustment (ΔEFI) levels evaluated by the use of (a) Cross-polarization (CP) (b) fuorescence illumination (FI) images |
Paste-type composites presented significantly lower ΔEFI and ΔECP values than the highly filled flowable composites The only clinically acceptable color adjustment was found for G-aenial Universal Injectable among the flowable composites. |
Bayraktar et al., 2024 [82] |
| Fracture resistance | 50 extracted maxillary premolars Control group: 10 intact, untreated premolars Experimental groups (40 extracted teeth) 1. small class II cavities restored with highly filled flowable resin (G-aenial Injectable) 2. extensive class II cavities restored with highly filled flowable resin 3. small class II cavities restored with packable resin (G-aenial Posterior) 4. extensive class II cavities restored with highly filled flowable resin |
(a) universal testing machine (model 3343, Instron Corporation, Canton, MA, USA) with stainless steel ball of 4mm diameter (b) Steromicroscope for mode of failyre assessment |
no statistically significant differences between:
|
Gerges et al., 2024 [83] |
| surface roughness - wear |
Two highly filled flowable composites: (1) Clearfl Majesty ES flow (2) G-aenial Universal Injectable two conventional resin composites (3) Clearfl Majesty ES-2 (4) G-aenial A’CHORD Polishing procedure: Up to 4000- grit size silicon carbide paper for 20 seconds |
(a) Wear assessment after chewing simulations (240.000 cycles, 20N) (b) surface roughness by a rugosimeter, before after chewing cycles (c) SEM observations |
Surface roughness and wear of highly filled flowable composites were comparable to that of conventional composites Highly filled flowables can be used in occlusal areas especially when overcured |
Checchi et al., 2024 [84] |
| flexural properties - wear resistance |
nine highly filled flowable resin composites viscous composites conventional low-filled flowable composites |
(a) Two-body wear test (b) Three-point bending test (c) SEM analysis |
The majority of highly filled composites exhibited:
|
Francois et al., 2024 [85] |
| surface roughness - surface hardnes |
4 highly filled flowable composite resins: (1) G-aenial Universal Flo (2) G-aenial Universal Injectable (3) Tetric EvoFlow (4) Filtek Supreme Flowable Restorative At different time intervals (a) t0: before immersion (b) t1: 9h after immersion (c) t2: 18h after immersion in different media i. gastric juice ii. fizzy drink iii. citric juice iv. artificial saliva |
(a) optical profiler (Ra measurement) (b) SEM analysis (c) Vickers hardness tester for surface hardness |
G-aenial Universal Injectable revealed lower surface roughness and higher hardness compared to other highly filled flowable composite resins both before and after exposure to acidic media | Vulovic et al., 2024 [86] |
Table 4.
Randomized controlled clinical trials on highly filled resin composites.
| Objective | Materials | Sample Size/Time Intervals | Evaluation Criteria | Results | Author/Year |
|---|---|---|---|---|---|
| Evaluation of direct posterior restorations after 36 months. | 1. Conventional composite resin (Estelite Sigma Quick, Tokuyama, Tokyo, Japan) 2. Highly filled flowable composite resin (G-aenial Universal Flo, GC) two-step self-etch adhesive applied to both materials |
58 mid-size to extensive posterior composite restorations in 32 patients Restoration evaluation: a. After placement (baseline) b. 6-months c. 12-months d. 24-months e. 36-months After 36 months 42 restorations were evaluated in 21 patients |
FDI (World Dental Federation) criteria | No statistically significant difference between cavities restored with highly filled flowable and conventional composite resins (p > 0.05/ Pearson’s X2 and Fisher’s exact tests for differences between restorative materials and Cochran’s Q test for differences between the same material in different time intervals) No secondary caries observed. |
Kitasako et al., 2016 [87] |
| Evaluation of direct non-carious cervical lesions (NCCLs) after 3 years | 1. Highly filled flowable composite (Clearfil Majesty ES Flow, Kuraray Noritake Dental Inc., Tokyo, Japan) 2. Conventional paste-type composite (Clearfil Majesty ES-2, Kuraray Noritake Dental Inc., Tokyo, Japan) Clearfil SE Bond (Kuraray Noritake Dental Inc., Tokyo, Japan) |
84 NCCLs in 27 subjects were included Restoration evaluation: a. baseline (BL) b. 1 year c. 2 years d. and 3 years |
FDI criteria | Regarding changes over time, significant differences were found within each group (p < 0.01) No significant difference between the two material groups at any time interval concerning functional properties The highly filled flowable resin composite presented significantly better: surface lustre (p<0.01) at the 1 year recall and marginal staining (p<0.05) at any time point (Wilcoxon signed-rank test) |
Zhang et al., 2021 [88] |
| Evaluation of direct posterior restorations after 18 months | 1. Bioactive injectable resin composite (Beautifil Flow Plus X F00, Shofu Inc., Kyoto, Japan) 2. Nanohybrid resin composite (Tetric N-Ceram, Ivoclar Vivadent AG, Schaan, Lichtenstein) |
18 patients with 26 class I and II carious cavities Restoration evaluation: a. baseline b. 6-months c. 12-months d. 18-months |
modified United States Public Health Service (USPHS) criteria |
no statistically significant difference between the two materials at different time intervals in terms of anatomical form, secondary caries, marginal staining, postoperative sensitivity (p=1.00) and marginal adaptation (p>0.05 / 95% confidence level/ 80% power / Chi-square test and Cochran’s Q test) |
Elderiny et al., 2024 [89] |
| Evaluation of class II restoration using different restorative materials after 2 years | 1. Conventional composite: Clearfil Majesty Posterior ( Kuraray Noritake Dental Inc., Tokyo, Japan) 2. Bulk-fill composite:Filtek One Bulk Fill Restorative (Solventum) 3. Highly filled flowable composite: G-aenial Universal Injectable (GC, Japan) |
110 patients with 259 Class II restorations Restoration evaluation: a. Baseline b. 1-year c. 2 years After 2 years: i. 59 conventional composite restorations ii. 68 bulk-fill composite restorations iii. 61 highly filled flowable composite restorations in 74 patients have been evaluated |
FDI criteria | The materials showed similar results in most of the scores. Highly filled flowable composite and bulk-fill composite presented better clinical performance regarding surface gloss compared to conventional composite (p<0.05, rank-based Friedman analysis) |
Hançer Sarıca et al., 2025 [90] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



