Submitted:
11 February 2025
Posted:
17 February 2025
You are already at the latest version
Abstract
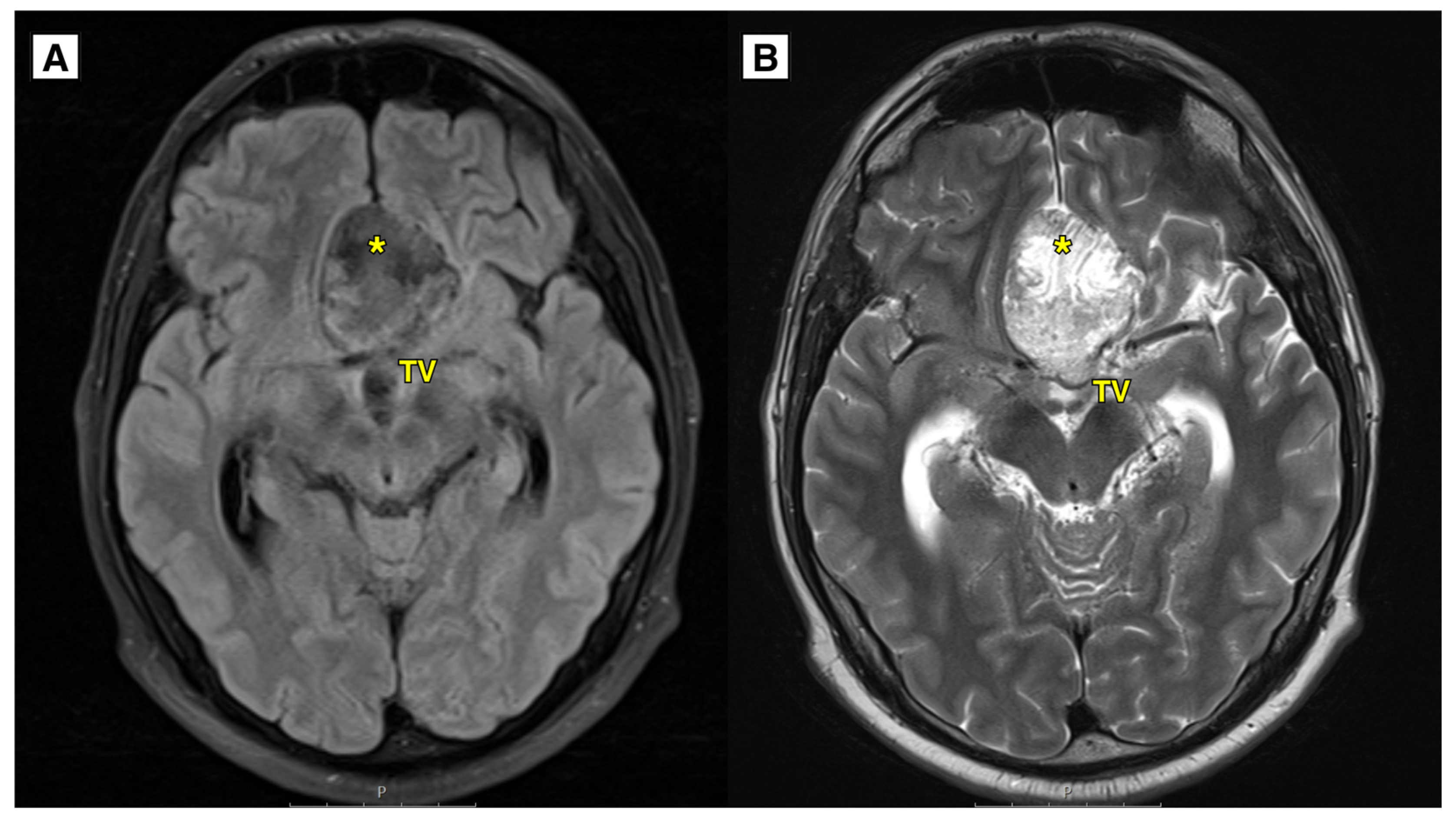
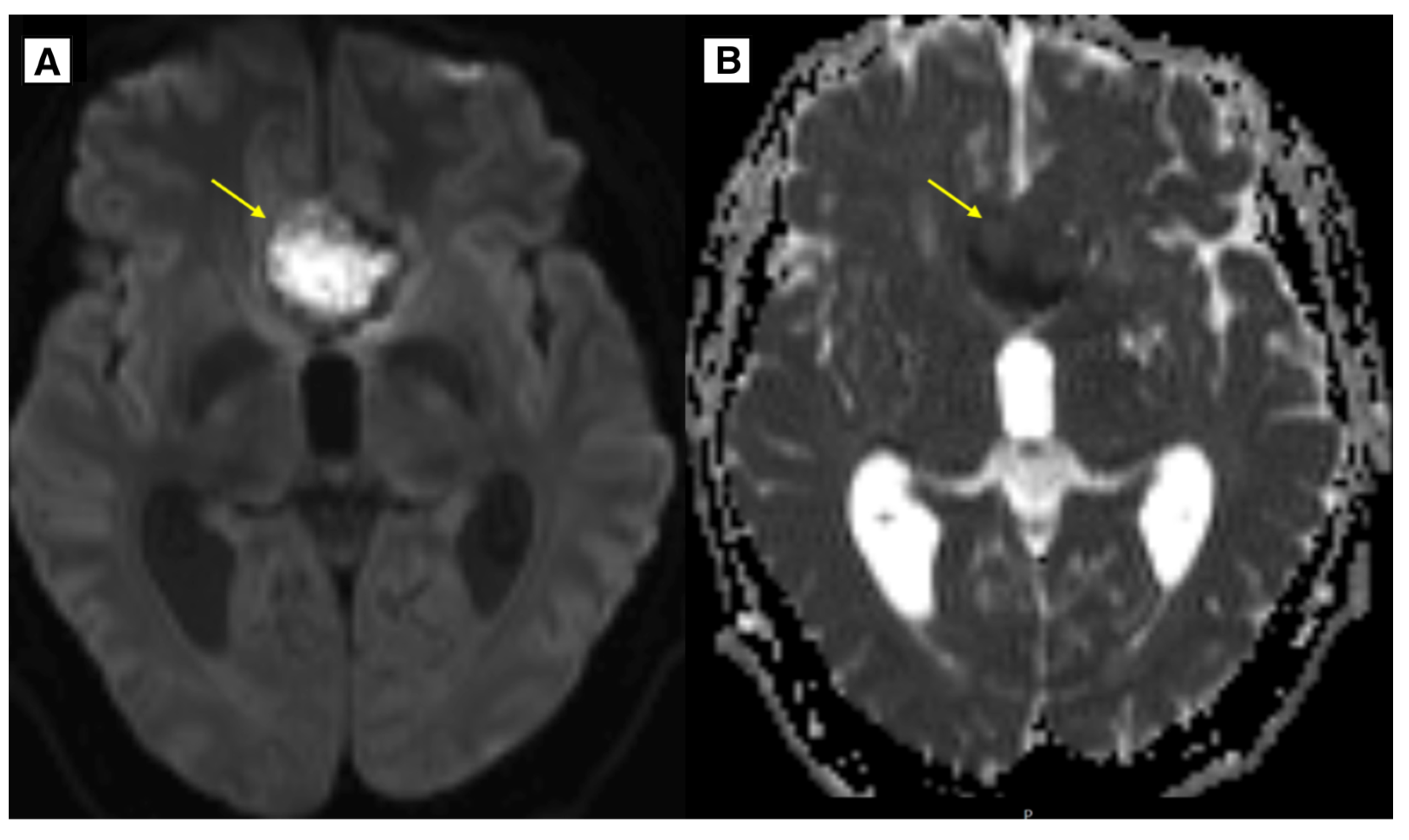
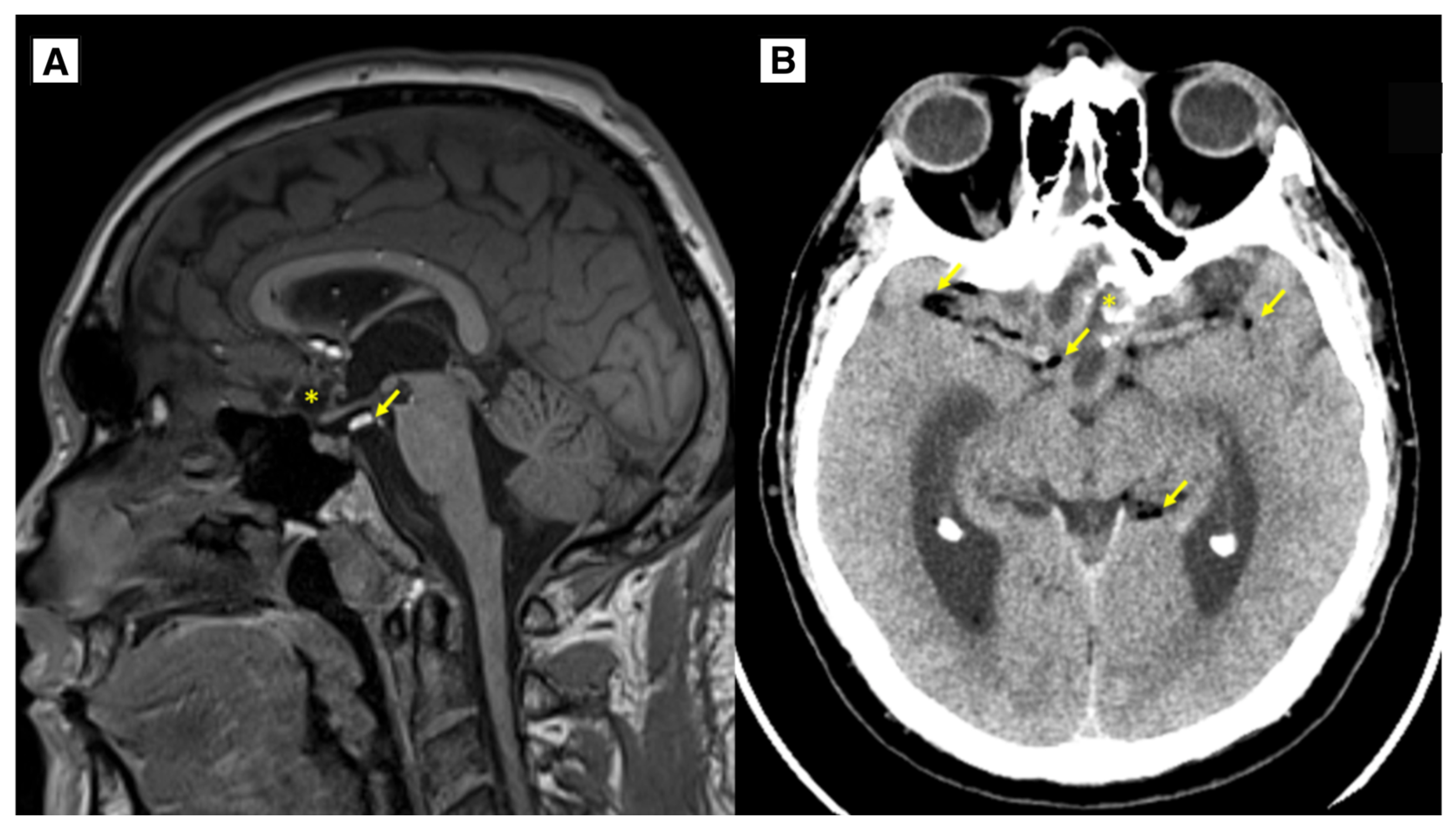
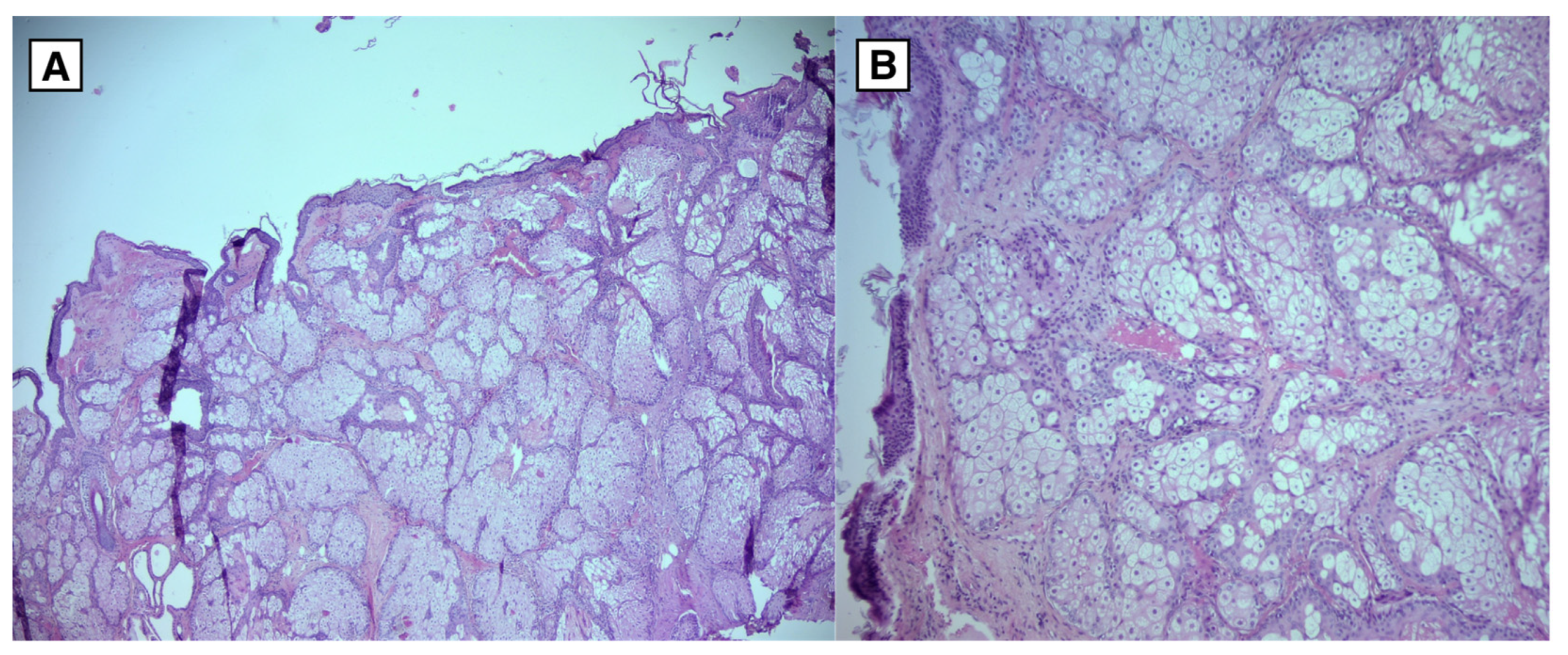
Background. Intracranial dermoid cysts (IDC) are rare benign congenital intracranial lesions. In the case of IDC rupture, these lesions may manifest clinically. Cysts may be visualized on non-enhanced computed tomography (NECT) and magnetic resonance imaging (MRI), facilitating discussions between clinicians and radiologists to determine cyst content and potential dissemination in cases of rupture. This case report describes an IDC rupture presenting as fat-containing lesions in the subarachnoid space and ventricular system, resembling a subarachnoid hemorrhage on MRI. Case report. A thirty-two-year-old Caucasian male patient was admitted to the hospital due to recurrent headache and visual impairment that began at the age of thirty-one. MRI revealed a lesion radiologically consistent with a ruptured dermoid or epidermoid cyst in the anterior fossa with a mass effect on the optic nerve intracranial segments, the chiasma opticum, and proximal optic tracts. The patient underwent a successful neurosurgical resection of the lesion, and histopathological analysis confirmed the diagnosis of a dermoid cyst. The postoperative period was uneventful. MRI follow-up revealed residual tissue of the IDC without any volume increase. Multiple punctate fat-containing lesions were noted, similar to previous MRI. The patient reported no complaints at discharge. Follow-up MRI imaging demonstrated no recurrence or progression of the dermoid cyst at 4 months, 1 year, and 2 years. Conclusion. IDC rupture is a rare event that may present clinically and appear as a blooming artifact on MRI, mimicking subarachnoid hemorrhage. Fat-containing lesions in the subarachnoid space and ventricular system can demonstrate findings indicative of an IDC rupture. MRI diffusion-weighted imaging (DWI) and decreased apparent diffusion coefficient (ADC) values may mimic an epidermoid cyst, a phenomenon rarely described in the literature, further complicating the diagnostic process.
Keywords:
1. Introduction
2. Case Presentation


3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brown JY, Morokoff AP, Mitchell PJ, Gonzales MF. Unusual imaging appearance of an intracranial dermoid cyst. AJNR Am J Neuroradiol. 2001 Nov-Dec;22(10):1970-2. PMID: 11733334; PMCID: PMC7973852.
- Smirniotopoulos JG, Chiechi MV. Teratomas, dermoids, and epidermoids of the head and neck. Radiographics. 1995 Nov;15(6):1437-55. [CrossRef]
- Sanjay Ballari, Gurubharath I. Intracranial ruptured dermoid cyst presenting as dysarthria: A case report. IAIM, 2018; 5(10): 171-178.A.
- Liu JK, Gottfried ON, Salzman KL, Schmidt RH, Couldwell WT: Ruptured intracranial dermoid cysts: clinical, radiographic, and surgical features. Neurosurgery. 2008, 62:377-84; discussion 384. [CrossRef]
- Emmanuel S, Inban P, Akuma O, Nouman Aslam M, Talat F, Nizamani A, Chenna VSH, Romain EM, Chu Carredo CK, Khan A. An Atypical Case of Intracranial Dermoid Cyst in an Adult Female: A Case Report and Literature Review. Cureus. 2023 May 31;15(5):e39807. [CrossRef]
- Stella Mouskou, Adiana Stamati, George Sfakianos, Astero Malama, Maria Gavra, George Vartzelis, Anastasia Korona, Sotiria Mastrogianni, Kostas Voudris, Ruptured intracranial dermoid cyst in a child. Cause of atypical neurological symptoms, Interdisciplinary Neurosurgery, Volume 20, 2020, 100482, ISSN 2214-7519. [CrossRef]
- Kucera JN, Roy P, Murtagh R. Ruptured intracranial dermoid cyst manifesting as new onset seizure: a case report. J Radiol Case Rep. 2011;5(4):10-8. [CrossRef]
- Shashidhar A, Sadashiva N, Prabhuraj AR, Narasingha Rao K, Tiwari S, Saini J, Shukla D, Devi BI. Ruptured intracranial dermoid cysts: A retrospective institutional review. J Clin Neurosci. 2019 Sep;67:172-177. [CrossRef]
- Sook Young Sim, Chan-Young Choi, Rupture of intracranial dermoid cyst by strenuous physical activity due to emotional stress: A case report, Interdisciplinary Neurosurgery, Volume 25, 2021, 101240, ISSN 2214-7519. [CrossRef]
- Traumatic rupture of an intracranial dermoid cyst: A case report. (2022). Eastern Journal of Medical Sciences, 6(4), 69-72. https://doi.org/10.32677/ejms.v6i4.3181 (Das U, Pandit N. Traumatic rupture of an intracranial dermoidcyst: A case report. East J Med Sci 2022;6:69-72).
- Kim KH, Cho JH. Ruptured intracranial dermoid cyst associated with rupture of cerebral aneurysm. J Korean Neurosurg Soc. 2011 Nov;50(5):453-6. [CrossRef]
- Stendel R, Pietilä TA, Lehmann K, Kurth R, Suess O, Brock M. Ruptured intracranial dermoid cysts. Surg Neurol. 2002 Jun;57(6):391-8; discussion 398. [CrossRef]
- Berrada K, Bougrin I, Ouali IE, Fikri M, Jiddane M, Touarsa F. Acute headache and seizures in psychiatric patient revealing atypical location of a ruptured dermoid cyst. Radiol Case Rep. 2023 Dec 22;19(3):1040-1045. [CrossRef]
- Das CJ, Tahir M, Debnath J, Pangtey GS. Neurological picture. Ruptured intracranial dermoid. J Neurol Neurosurg Psychiatry. 2007 Jun;78(6):624-5. [CrossRef]
- McArdle DJ, Karia SJ. Ruptured intracranial dermoid cyst. Pract Neurol. 2016 Dec;16(6):478-479. [CrossRef]
- Ray MJ, Barnett DW, Snipes GJ, Layton KF, Opatowsky MJ. Ruptured intracranial dermoid cyst. Proc (Bayl Univ Med Cent). 2012 Jan;25(1):23-5. [CrossRef]
- Castro S, Castelnovo G, Lebayon A, Fuentes S, Bouly S, Labauge P. Chemical meningitis in reaction to subarachnoid fatty droplets. Neurology. 2005 Sep 27;65(6):937. [CrossRef]
- Sanjay Bhatia, N. Khandelwal, Ashish Pathak, Harsh Mahaja, Ruptured supratentorial dermoid cysts, Computerized Medical Imaging and Graphics, Volume 17, Issue 6, 1993, Pages 461-464, ISSN 0895-6111. [CrossRef]
- Nayak HK, Kamble NL, Sinha NK, Daga MK. Ruptured frontal dermoid cyst: an unusual cause of seizure in a postpartum female. BMJ Case Rep. 2013 Apr 18;2013:bcr2013009107. [CrossRef]
- Murrone, Domenico & Romanelli, Bruno & Ierardi, Aldo. (2016). Ruptured intracranial dermoid cyst: a case report. Integrative Molecular Medicine. 3. 10.15761/IMM.1000247.
- Johnson DG, Stemper SJ, Withers TK. Ruptured "giant" supratentorial dermoid cyst. J Clin Neurosci. 2005 Feb;12(2):198-201. [CrossRef]
- Esquenazi Y, Kerr K, Bhattacharjee MB, Tandon N. Traumatic rupture of an intracranial dermoid cyst: Case report and literature review. Surg Neurol Int. 2013 Jun 12;4:80. [CrossRef]
- Taha A, Abdelrazek MA, Manalo N, Elsadek R, Morrin SJ, Brodski A, Augustynowiczd A, Mollashahi RS, Shenoy A. Traumatic Rupture of a Skull Base Dermoid Cyst Mimicking Chronic Meningitis. Cureus. 2022 May 17;14(5):e25066. [CrossRef]
- Albastaki A, AlThawadi R, Alajaimi J, Ali KF, Almayman T. An Intracranial Extradural Dermoid Cyst Presenting with Two Dermal Sinuses and an Abscess in a Child. Case Rep Neurol Med. 2021 Jul 26;2021:9917673. [CrossRef]
- Smith AS, Benson JE, Blaser SI, et al. Diagnosis of ruptured intracranial dermoid cyst: Value MR over CT. AJNR Am J Neuroradiol 1991;12:175-80.
- Altay H, Kitiş O, Calli C, Yünten N. A spinal dermoid tumor that ruptured into the subarachnoidal space and syrinx cavity. Diagn Interv Radiol. 2006 Dec;12(4):171-3.
- Ray MJ, Barnett DW, Snipes GJ, Layton KF, Opatowsky MJ. Ruptured intracranial dermoid cyst. Proc (Bayl Univ Med Cent). 2012 Jan;25(1):23-5. [CrossRef]
- Čatić A. R., Nikšić M., Kadenić Z. Ruptured intracranial dermoid cyst: a case report. Journal of Health Sciences. 2012;2(3) . [CrossRef]
- Watanabe K, Filomena CA, Nonaka Y, Matsuda M, Zomorodi AR, Friedman AH, Fukushima T. Extradural Dermoid Cyst of the Anterior Infratemporal Fossa. Case Report. J Neurol Surg Rep. 2015 Nov;76(2):e195-9. [CrossRef]
- Sadashiva N, Tiwari S, Narayan V, Shukla D. Ruptured Intracranial Dermoid and the Chemical Shift Artifact. J Neurosci Rural Pract. 2016 Dec;7(Suppl 1):S86-S87. [CrossRef]
- Jacków J, Tse G, Martin A, Sąsiadek M, Romanowski C. Ruptured intracranial dermoid cysts: a pictorial review. Pol J Radiol. 2018 Oct 19;83:e465-e470. [CrossRef]
- Sood S, Gupta R. Susceptibility artifacts in ruptured intracranial dermoid cysts: a poorly understood but important phenomenon. Neuroradiol J. 2014 Dec;27(6):677-84. [CrossRef]
- Survashe, P.T., Guthe, S.P., Velho, V. and Bhide, A. (2017) Ruptured Intracranial Dermoid: Case Report and Literature Review. Medical Journal of Dr. D.Y. Patil Vidyapeeth, 10, 297-299. [CrossRef]
- Aksoy FG, Aksoy OG, Gomori JM. Klippel-Feil syndrome in association with posterior fossa suboccipital dermoid cyst. Eur Radiol. 2001;11(1):142-4. [CrossRef]
- Shinoyama M, Kajiwara K, Harada K, Ideguchi M, Akimura T, Nishizaki T, Suzuki M (2002) [A case of a ruptured dermoid cyst in the sylvian fissure]. No Shinkei Geka 30:1197–1201.
- Orakcioglu B, Halatsch ME, Fortunati M, Unterberg A, Yonekawa Y. Intracranial dermoid cysts: variations of radiological and clinical features. Acta Neurochir (Wien). 2008 Dec;150(12):1227-34; discussion 1234. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



