Submitted:
11 February 2025
Posted:
12 February 2025
You are already at the latest version
Abstract
Background: Although many industries have seen quick technological advancements, the healthcare industry, particularly the emergency departments, struggles with slow adoption. The majority of research, despite the fact that many have examined the factors that influence medical officers' acceptance of new technologies, concentrates on healthcare as a whole rather than specific departments, such as emergency departments. Methods: This study examines the barriers and facilitators affecting technology adoption in emergency departments by reviewing 30 peer-reviewed articles published between 2019 and 2024 by using keywords such as "technology adoption," "influence factors," "medical technology," "barriers," "healthcare," "emergency departments," "ED," and so on. Results: Several barriers were discovered in this study, including high labour turnover rates, accessibility issues, a lack of technology availability, and a lack of willingness to change owing to heavy workloads. Meanwhile, excellent collaboration and communication, a supportive and active management team, and rigorous education and training all played crucial roles as facilitators. Conclusion: This study highlighted the necessity of customised approaches and cooperative endeavours to tackle the different barriers encountered by emergency departments. This will result in a faster introduction of critical technologies that will improve patient outcomes and operational effectiveness in emergency departments. Further research should go further into these findings and investigate creative techniques to improve technology integration and establish higher standards of care inside emergency departments.
Keywords:
technology adoption
; influence factors
; medical technology
; barriers
; healthcare
; emergency
; emergency room
; ER
; emergency departments
; ED
; acute care
; emergency care
; emergency medicine
; accident and emergency
; A&E
1. Introduction
Numerous industries have advanced significantly and become more convenient in recent years due to the rapid growth of technology [1], [2]. The food and beverage and transportation industries have seen the most significant changes among those industries. The use of technology has greatly improved their productivity and quality [1], [2]. For example, the food and beverage industry has effectively accomplished a safer and more efficient production process with the use of automated manufacturing lines and advanced monitoring systems [2]. Meanwhile, the deployment of autonomous driving technologies and intelligent transportation systems has improved the standard for traffic management and safety [3].
Both industries are growing rapidly as they are vital to human civilization and have an impact on many aspects of daily life. Therefore, emerging technologies are typically initially implemented and promoted in these domains. Nevertheless, although being closely tied to human health and life safety, the healthcare industry, another essential industry to humans, is lagging behind the food and beverage and transportation industries in terms of science and technology adoption and application [4].
The healthcare industry has an extremely heavy workload due to its uniqueness. Healthcare professionals such as medical officers frequently deal with excessive workloads in the absence of technology, which is a widespread issue around the globe [5], [6]. This is because of the reluctance of the healthcare industry to adopt new technology has caused many advanced medical innovations to move slowly in real-world applications [7]. Although many cutting-edge technologies have been demonstrated to dramatically increase the effectiveness and quality of medical services, for a variety of reasons, their adoption has not followed the same trajectory as other industries [7].
The hospital normally consisted of several departments, each with a different perspective about the integration of novel technologies. As one of the most important departments in the hospital, the emergency department has been found to be relatively resistant to the introduction of new technologies in previous studies. This is mostly because of the unique challenges it encounters. First of all, medical officers working in the emergency department are under a lot of pressure to make swift judgements [8], which leaves little time for training and system adaptation. Additionally, due to the fact that the emergency department has to treat a high number of patients [9], the implementation of new technology may disrupt current workflow and cause delays in treatment [10], particularly in emergency scenarios when unfamiliar technologies may cause a delay in making crucial judgements. Furthermore, the intricacy of situations presented in emergency departments necessitates adaptable technology, which frequently prompts questions about how well-usable cutting-edge technology will be [11], [12]. In addition, different degrees of technological proficiency of the medical officers also made adoption more difficult [13], and a lack of training time made it difficult for medical officers to become proficient with new technologies due to the heavy workload of the emergency department [14]. Lastly, medical officers in the emergency department may exhibit resistance to change because they may be hesitant to give up tried-and-true techniques that have worked well in high-risk circumstances [15], [16].
According to Chen et al. (2020) [17], medical officers have a poor adoption of new technologies, even though academics typically agree that technology has major benefits for the healthcare industry. However, the perspectives of medical officers have a significant influence on how technology is used in the medical industry as they are the ones who are directly involved with these innovations [18].
Although several studies have sought to evaluate the variables that encourage medical officers to adopt new technology, the majority of them have examined the healthcare sector as a whole rather than concentrating on specific parts of the industry. However, different perspectives on the need for new technological applications have resulted from differences in sectoral priorities. Therefore, the purpose of this study is to perform a thorough analysis of the variables that facilitate and hinder the adoption of technology in the emergency department and to determine how these factors influence the growth of technology in the healthcare industry.
By identifying and eliminating the barriers to technology adoption in the emergency department and exploring variables that may enhance technology acceptance, this study aims to increase medical officers' acceptance of new technologies, as well as to accelerate technological advancement in the healthcare industry, especially in emergency departments. In addition, it is anticipated that the findings of this study will be a valuable resource for further research in this area, as this detailed approach could more clearly differentiate the challenges faced in different emergency department settings and provide insights specific to these unique settings. Furthermore, the study's findings will also provide medical policymakers with a solid scientific foundation for developing more effective technology adoption strategies, as well as valuable feedback to technology developers on the usability and design of their products.
2. Literature Review
As technology advances, workflows are continually adapting in order to incorporate these innovations. However, adopting new technology may be extremely difficult in some industries, the most notable is the healthcare. This is frequently because of the special requirements and the environment that the industry has.
The healthcare industry is among those with the most challenges when it comes to technology adoption. Despite the industry's vital role in public health, healthcare workers have difficulty adjusting to new technology [19]. The adoption and use of technological advancements in healthcare organisations have been impacted by a number of variables that have come together to limit the introduction of technology. Numerous studies have examined the barriers to medical technology adoption, by employing various approaches and examining the barriers and facilitators in technology use from different perspectives. However, the advantages of using technology are not clear, even though these studies offer deep insights and encompass the whole healthcare system. This might be because various departments deal with different kinds of challenges.
Emergency departments, being one of the departments that regularly experience work overload in the healthcare industry, found particularly complicated technology application challenges due to their high-pressure emergency work environment [20]. For example, given the enormous volume of work in the emergency room many technologies that function effectively in standard medical settings could be challenging to deploy successfully. Therefore, a more thorough knowledge of the obstacles and enablers of technology adoption may be obtained by carefully integrating studies relating to emergency departments.
As a result, this study will concentrate on the particular difficulties and potential opportunities of implementing technology in the emergency department. It will also examine the main obstacles to technology acceptance in this setting and evaluate efficient methods for encouraging technology use. This study seeks to give a more in-depth analysis to support the further development of technology applications by thorough assessment and summary of the literature related to emergency departments in the healthcare industry.
2.1. Reviewed Studies
Hall et al. (2022) [21] conducted a study that evaluated the introduction of virtual urgent care (VUC) services in Ontario, Canada and identified several facilitators and barriers. According to their study, the facilitators included patient engagement through the integration of feedback to address needs, provincial funding that supported the programs' launch and sustainability, local champions who guided the effective delivery of the programs, and successful marketing strategies that promoted awareness and encouraged participation. Meanwhile, they also identified the barriers, which are the need for behaviour change strategies to assist healthcare providers and patients in adjusting to virtual care, challenges with IT infrastructure and system integration, ensuring equitable access to services for all patients regardless of socioeconomic status, and the need for standardised data collection to assess program impact and effectiveness. This study indicated that even though the VUC programs were designed to expeditiously establish safe medical care and divert low-acuity patients from emergency departments during the COVID-19 pandemic, regional autonomy led to customised solutions that presented challenges for long-term sustainability and future funding. Finally, the study's findings highlight the importance of ongoing quality control and data collection in ensuring the programs' long-term survival.
Fujimori et al. (2022) [22] used a mixed methods approach to assess the acceptability, barriers, and facilitators of these systems, integrating the quantitative and qualitative assessments. In this study, the respondents were 14 doctors from two community tertiary care hospitals in Japan who have experienced a real-time AI-based CDSS intended to predict aortic dissection. By conducting this study, several important barriers were found, which included worries about alert fatigue and system performance, compatibility problems like typing speed impacts, and system failure anxiety. On the other hand, the study also revealed key facilitators, such as the quality of design, with an easy-to-use interface and real-time alerts boosting its usability, and the strength of evidence, as trust in the system's data properly mirrored local illness patterns. By conducting this study, they highlighted that enhancing the system performance and the system compatibility while using the evidence-based design and user-friendly interfaces is essential for gaining excellent user acceptability of AI-based CDSSs in the emergency departments.
Anaraki et al. (2024) [12] have conducted a study to examine the barriers and facilitators associated with implementing SurgeCon, a quality improvement program designed to boost the efficiency and patient satisfaction in the emergency departments (EDs) throughout Canada. In this study, they have included multiple hospitals from both urban and rural areas in order to capture a range of experiences. By conducting this study, they have revealed several important facilitators, such as engaged and supportive management, sufficient personnel and resources, efficient departmental communication, successful prior intervention experiences, and a strong drive for progress. Effective supervisors foster success by encouraging employees and guaranteeing resources, and positive reinforcement of new endeavours stems from effective communication and past achievements. On the other hand, they also discovered the barriers, including limited management participation, authoritarian leadership, a lack of personnel, frequent turnover, inadequate communication, a lack of cooperation, unfavourable prior experiences, aversion to change, and excessive workloads that impede advancement and incite opposition among employees. This research has shown that a comprehensive understanding of the facilitators and barriers associated with healthcare quality improvement programs is crucial for their successful implementation. Besides that, it also suggested strategies including employee education, appointing advocates to spearhead projects, and encouraging proactive participation in order to overcome barriers and enhance emergency deparment effectiveness and patient outcomes.
Huilgol et al. (2024) [23] examined the difficulties faced and the ways in which emergency department physicians made decisions in response to novel developments during the COVID-19 pandemic. A total of 49 healthcare professionals, including 17 doctors, 7 advanced practice providers, 18 nurses, and 7 respiratory therapists, participated in the study from 8 hospital-based emergency departments in the United States. By conducting this study, they identified several facilitators of the innovation, including the use of the social media, clinician autonomy, organisational culture, supportive leadership, and external experiences. On the other hand, barriers included a dearth of information supported by research, evolving recommendations, anxiety, moral discomfort, and clinical opposition. According to the study's findings, organizations may foster innovation by designating capable leaders, guaranteeing the psychological stability of their staff, offering the required procedures and resources, and acknowledging accomplishments.
Zachrison et al. (2020) [24] conducted a study aimed at understanding the barriers to telemedicine implementation in rural emergency departments (EDs) and analyzing the characteristics of rural EDs that do and do not use telemedicine. Data from the 2016 National Emergency Department Inventory (NEDI) survey as well as follow-up questionnaires were used in the study. Through this study, they discovered several barriers and the most important of which was the cost, which was mentioned by 37% of rural EDs. Besides that, staffing concerns, transfer patterns, and the perception of telemedicine system complexity are additional barriers. Meanwhile, this study also found the key facilitators of telemedicine adoption, which are the support from the hospital, EDs, and health system leadership. The results of this study revealed the need to address financial restrictions as well as other challenges in order to increase telemedicine adoption and improve rural healthcare access.
Boyle et al. (2023) [25] conducted an investigation that focused on the barriers, facilitators, and readiness of New England hospitals in the United States to implement a regional catastrophe teleconsultation system intended to provide quick access to medical specialists in times of crisis. In this study, a cross-sectional survey was conducted either via phone or online with emergency managers from hospital-based and freestanding emergency departments (EDs) across New England. One of the main barriers that has been noted is the difficulty in reaching burn, toxicological, radiation, and trauma specialists, which can cause a delay in receiving critical treatment. Another significant barrier was the potential for credentialing delays, which might impede expert consults. This issue to the fact that a total of 70% of hospitals required catastrophe credentialing, which could take up to 72 hours. Additionally, the usage of the technology was further complicated by the unreliability of cellphone connectivity and internet in rural hospitals. Fortunately, the majority of the hospitals supported the deployment of the system by having sufficient emergency alerting systems and telecommunications equipment. Furthermore, considering the advantages of quick expert access, 81% of hospitals, especially smaller and rural ones, expressed a strong readiness to employ teleconsultation technology. The results of the study showed that, despite the system's great demand, improvements in communications redundancy and consistent credentialing procedures are crucial to both its successful deployment and capacity to optimise benefits in emergency scenarios.
Pu et al. (2024) [26] examined the increasing usage of virtual emergency departments (VEDs) in Victoria, Australia, particularly during the COVID-19 pandemic, and found a number of barriers and facilitators for their adoption. The study investigated the benefits, shortcomings, and scalability of VEDs through interviews with 20 individuals, including emergency medicine doctors, healthcare providers, and other experts. By conducting this study, several key barriers were the challenge of doing comprehensive virtual physical exams, the deficiency of solid data and standardised protocols for VEDs, and the increased workload and resource limitations experienced by emergency department personnel. On the other hand, they have also identified several facilitators, such as the ease of use and availability of VEDs for patients and medical professionals, better follow-up and coordination, and increased safety through lowered infection risks and lessened patient anxiety. In conclusion, the findings of this study revealed that although the virtual evaluations (VEDs) can be a useful and practical substitute for in-person visits, they are not a perfect substitute because they still have limitations in real-life use, particularly for the user, older adults receiving residential care. Therefore, further research, the development of standards, and the provision of resources are needed to enable the wider application of VEDs.
Antor et al. (2024) [27] performed a study to assess the adoption and usability of Electronic Health Records (EHRs) at Ghana's Komfo Anokye Teaching Hospital, focusing on variables influencing adoption and obstacles experienced by healthcare workers. Using a cross-sectional survey, healthcare personnel shared their experiences with EHRs. This study found several barriers that impede efficient healthcare delivery, such as inadequate system training, frequent malfunctions, power outages, privacy issues, and poor maintenance. Positively, they also discovered the facilitators that encouraged EHR adoption were system comfort, dependability, and higher-quality patient care. To sum up, this study highlighted the importance of the EHRs in improving healthcare and it has also emphasised how the barriers must be overcome and how EHR advantages must be fully realised through continual training, technical assistance, and infrastructure updates.
An investigation of the technology barriers and facilitators in providing paediatric mental and behavioural healthcare in emergency departments (EDs) was carried out by Bhosekar et al. (2023) [28]. Through the semi-structured interviews and observational studies involving four healthcare professionals from two different institutions, this study identified several significant barriers and facilitators. According to their study, barriers included worries over the calibre of third-party services like telehealth platforms, poor training on new software capabilities that led to underutilisation, and software usability difficulties such as complicated interfaces and frequent changes that doctors found difficult to traverse. On the other hand, effective safety measures that guaranteed the protection of patients and staff, easily accessible clinician notes that enhanced continuity of care, and effective communication systems that simplified information exchange among healthcare practitioners were the facilitators that found in this study. According to this study, it concluded that although the technology can improve treatment, there are drawbacks that need to be taken into consideration when employing this technology in order to increase patient safety and lessen physician burnout. In conclusion, the results of this study suggested that the regular training and human-centred design might reduce these barriers and enhance the process of providing treatment in emergency departments.
In order to improve the access to treatments for marginalised patients in the Toronto's emergency departments (EDs) and lessen digital health inequities, Hodwitz et al. (2024) [29] conducted a study to evaluate a hospital-based phone prescription scheme. A total of 12 healthcare professionals were interviewed for the study, which focused on 5 main goals, which are establishing patient trust, giving patients the authority to manage their own care, bridging gaps in the system, providing equitable treatment for marginalised communities, and reducing moral distress among the personnel. However, the programme faced challenges such as unclear eligibility criteria, inconsistent phone availability, and potential bias in administration. On the positive side, healthcare staff’s non-judgemental, anti-oppressive approach, smooth enrolment process, and deep understanding of marginalised patients’ needs were important facilitators. The study concluded that providing phones to marginalised patients can help bridge gaps in both digital and social health, but its success depends on building trust, understanding patients’ unique needs, and adopting a holistic, biopsychosocial approach to healthcare.
The factors influencing the uptake and sustainability of the telehealth in rural emergency departments in the United States were examined by Nataliansyah et al. (2022) [30]. They identified numerous barriers and facilitators by conducting the semi-structured interviews with 18 important informants from six different healthcare systems. One of the barriers was the lack of adequate needs assessments, which led to services that did not meet the unique requirements of rural areas. In addition, the lack of proper training for local employees resulted in problems with unsuccessful consultations since they were not familiar with the technology. Furthermore, the other barrier was that the regular provision of telehealth services in remote hospitals was impeded by resource limits. Aside from these impediments, this study identified other barriers caused by political and regulatory difficulties. Additionally, they discovered that the facilitators included in-depth needs evaluations, guaranteeing that the services were customised to satisfy regional needs. Besides that, a thorough staff training initiatives contributed to the efficient application of telehealth technology, which is also considered as one of the facilitators. Furthermore, strong ties between the hub and spoke locations fostered cooperation and trust, which are essential for operational success, and adequate service capacity and backup mechanisms allowed for more dependable service delivery. In conclusion, this study highlighted the significance of addressing regional issues and focussing on these facilitators to ensure the effectiveness and sustainability of telehealth adoption.
Kennedy et al. (2024) [31] carried out a study to understand how the HIRAID® emergency nursing framework was being used in rural emergency departments in Southern New South Wales, Australia. The research focused on exploring its application in these settings. Therefore, they used a mixed methods approach to poll 102 emergency nurses from 11 departments. The average experience of the participants was 16 years in nursing and 8 years in emergency care. By conducting this study, they discovered numerous barriers to the implementation of the HIRAID®, such as time and resource restrictions, a lack of understanding of the framework, a lack of management support, and the uncertainties over the framework's efficacy. The nurses' excitement for novel approaches and their belief that HIRAID® may enhance nursing procedures and patient outcomes, on the other hand, have also been recognised as facilitators. This study emphasised the importance of developing strategies to address the unique challenges, especially in smaller departments, to ensure the successful implementation of HIRAID®. It concluded that customised approaches are necessary to overcome resource limitations and provide essential support and training, while also tackling the specific difficulties of adopting new practices in rural emergency settings. The findings of this study are intended to lead to the development of a solid, realistic plan for implementing the HIRAID® throughout the district.
The effects of workflow fragmentation and electronic health records (EHR) on the amount of paperwork required in the emergency departments (EDs) were investigated by Moy et al. (2023) [32]. Using the EHR from Epic Systems, the researchers conducted semistructured interviews with 24 US emergency department physicians and registered nurses. The study revealed numerous barriers to efficient recordkeeping. Notable barriers include EHR shortcomings, such as inadequate functionality and a poorly designed user interface, which lead to an increase in manual labour and disruptions in workflow. Meanwhile, frequent job switching and the interruptions exacerbate these difficulties by increasing cognitive strain and lowering the calibre of documentation. Additionally, the study found a number of facilitators who may assist in resolving these issues, which include incorporating patient-specific EHR features, minimising manual data entry through the use of sophisticated data collection techniques, and improving EHR displays and setups for improved usability. The study indicated that although EHRs improve patient care, in order to minimise paperwork load, their design has to be more closely linked with the unique requirements of emergency department processes. To determine if optimising the current EHR systems would be sufficient or whether a thorough redesign is necessary, further input from stakeholders is needed.
The rapid adoption of the telehealth in American emergency departments (EDs) during the first nine months of the COVID-19 pandemic was studied by Uscher-Pines et al. (2021) [33]. They investigated the implementation of telehealth solutions using semi-structured interviews with 15 emergency department leaders from 14 institutions spread across 10 states. The leaders were selected via literature review and snowball sampling. The study revealed that prior experience with telehealth facilitated the swift implementation of virtual post-discharge evaluations, tele-isolation, tele-triage, and teleconsultation. However, many of these solutions were temporary as their relevance diminished over time. By conducting this study, they found a number of facilitators and barriers. Two key barriers were the necessity for the direct support inside the emergency department and technological challenges. Facilitators included higher compensation, more lenient licensure standards, and loosened HIPAA rules. This study highlighted how the pandemic sped up telehealth usage, though many projects were discontinued once demand decreased. The insights from this study could inform future disaster response planning and underline the importance of a robust telehealth infrastructure and ongoing support to address future logistical and technological challenges.
Wong et al. (2024) [34] carried out a research procedure to assess emergency department-manage, a clinical decision support system (CDS) intended to manage agitation symptoms in emergency departments (EDs). This study aims to identify individuals who may become agitated and to assist emergency department physicians in treating these patients appropriately to reduce the need for restraints and enhance patient outcomes. The approach includes a formative assessment as well as qualitative data gathered from emergency department physicians, nurses, technicians, and patients who have been restrained. A pilot randomised controlled trial will be conducted at two adult emergency department locations in the Northeastern United States with the aim of enroling a minimum of 26 eligible participants. Implementing optimal practices for agitation control might be difficult due to time restraints, inconsistent workloads, and restricted access to professional psychiatric evaluations. Meanwhile, a user-centred design approach that integrates end-user feedback continuously, proactive interventions, and the use of systematic risk assessments are among the facilitators. The findings of this study suggested that if emergency department-TREAT is implemented successfully, it may be able to identify patients who are more likely to be at-risk, reduce the need for restraints, and enhance patient outcomes. If successful, a follow-up clinical efficacy trial will compare emergency department-TREAT to standard care at other emergency department sites.
Barton et al. (2024) [35] conducted a study to explore how academic detailing could support the design and implementation of a clinical decision support (CDS) tool aimed at preventing falls in the emergency departments. The study, which featured 16 semi-structured interviews with emergency medicine residents and advanced practice physicians who had used the CDS tool, was carried out at a sizable university medical centre in the Midwest of the United States. The study focused on individuals aged 65 and older. Several facilitators and impediments have been identified that will effect the use of the CDS tool. Barriers encompassed the hectic atmosphere of the emergency room, physicians' misinterpretations of the CDS tool or the referral procedure, and the absence of clarity in the referral process. Facilitators, on the other hand, included the tool’s ease of use, minimal input requirements, and its automated identification of high-risk patients, enabling timely interventions. Academic detailing interviews were designed to clarify misconceptions and enhance understanding of the CDS tool and the referral process. The study's findings showed that academic detailing may successfully promote the adoption of health information technology by identifying the factors that affect utilisation and teaching physicians. This strategy allows for larger-scale redesigns and real-time changes, which helps to align technology to the evolving demands of the clinical workforce.
A qualitative interview study was conducted by Billah et al. (2022) [36] to investigate the use of the patient decision aids (DAs) in emergency departments (EDs). A total of 20 emergency doctors from a variety of New York health systems, including attending physicians, residents, and physician assistants, were participated in the study. The goal of the study was to determine what barriers and facilitators individuals presenting with low-risk chest discomfort and unexplained syncope have while utilising DAs. The study identified six main barriers, which were patients' worries, such as inadequate health literacy, uncertainties about the validity of the DAs, concerns about increased medicolegal risk, a perception that DAs are unnecessary, and a lack of time to apply them. Meanwhile, the 6 positive attitudes regarding shared decision-making (SDM), patient access to follow-up care, the possibility of increased patient satisfaction, better risk communication, efficient integration of DAs into clinical workflows, and institutional support were found to be facilitators. Based on the identified facilitators and these barriers, the study indicated that enhancing the use of DAs in EDs is imperative. The findings of this study might influence the future strategies to enhance the use of DAs and support standardised SDM in emergency care settings.
The difficulties and facilitators of introducing digital psychological therapies for senior citizens in emergency rooms (EDs) were examined by Davison et al. (2024) [37]. Their scoping review will encompass both qualitative and quantitative studies, adhering to the PRISMA-ScR checklist and the Joanna Briggs Institute recommendations. These research will focus on patient, family, and emergency department staff perspectives, attitudes, experiences, and perceptions of digital psychological therapies. The evaluation will focus on people 70 years of age and older, their families, and emergency department staff. Four databases, including Medline, Embase, PsycINFO, and Scopus, as well as the top 100 results from a Google Scholar search, will be searched thoroughly. Several barriers were identified in this study, including the complexity of health problems older adults face, the need for care that is urgent, and the possibility that older adults are not tech-savvy. Meanwhile, the facilitators have also been identified, including the acceptance of older individuals using portable electronic devices (PEDs) to evaluate themselves and the potential for these therapies to improve care and decrease unforeseen hospital visits.. It is predicted that new psychosocial digital health technologies for use in emergency departments (EDs) would be created with the results of the scoping study as a guide to enhance the psychosocial evaluation and care of older adults.
Salwei et al. (2022) [38] investigated the usability problems and enhancers of a clinical decision support (CDS) system based on human factors engineering (HFE) to detect pulmonary embolism (PE) in emergency departments (EDs). For the study, 32 emergency care professionals, including attending doctors and residents, were debriefed via a scenario-based simulation. Through interviews and deductive content analysis using Scapin and Bastien’s usability criteria, the team identified 271 usability issues, comprising 94 barriers and 177 facilitators. Facilitators included features like the CDS’s ability to automatically display vital signs, saving doctors time in finding information, and its support in ordering diagnostic tests and generating paperwork. However, challenges arose from the system’s incompatibility with certain workflows, such as those of doctors preferring single risk assessments or simultaneous orders, as well as limited support for collaboration between residents and attending physicians. The study concluded that applying HFE principles improves usability in CDS design, but emphasised that better integration into existing workflows is crucial to overcoming usability challenges. The findings highlight the importance of considering both broad and detailed usability factors to ensure the successful adoption of CDS technology in clinical practice.
The parameters impacting the acceptance, use, and upkeep of a clinical decision support (CDS) tool for buprenorphine initiation in emergency departments (EDs) were investigated by Simpson et al. (2023) [39]. The study discovered several facilitators and barriers through 28 interviews with clinicians from five different healthcare systems who were participating in the EMBED experiment, including attending doctors, physician assistants, and residents. Barriers encompassed clinical training, organisational culture, patient referrals for further care, and customisation of implementation for each emergency department. In the meantime, several factors played a crucial role in facilitating the adoption of the CDS tool. These included the efforts of local activists, effective training programs, a supportive environment, and efficient referral tools. This study revealed that while the CDS tool alone had a minimal impact, significant adoption benefits come from a comprehensive, multilevel approach. To truly enhance the effectiveness of CDS in promoting evidence-based practices in emergency care, it’s essential to tailor its implementation, ensure robust organisational support, and provide practical, hands-on training.
Shin et al. (2024) [40] examined the factors influencing the adoption of digital applications for suicide safety planning in a psychiatric emergency department. The researchers used the Theoretical Domains Framework (TDF) and the COM-B model, which are the capability, opportunity, motivation, and behaviour, to conduct semi-structured interviews with a total of 29 emergency department professionals, including nurses, psychiatrists, social workers, program assistants, and chemists. The app's potential to enhance patient accessibility and care efficiency, as well as the physicians' strong incentive to utilise it stemming from their feeling of professional identity and duty, were highlighted as key facilitators. However, adoption was hampered by problems with paperwork, communication, and patient access to cell phones. By conducting this study, they found that the lack of connectivity between the app and the existing electronic health record systems posed a significant barrier to its easy integration into standard clinical processes. Besides that, this study also highlighted the importance of developing targeted strategies to overcome these barriers and capitalize on facilitating factors. Continuous evaluation and modification of these strategies will greatly facilitate suicide prevention programs for psychiatric EDS patients, as new barriers may emerge and facilitating factors may change. This will guarantee the app's long-term viability.
Shuldiner et al (2023) [41] conducted a study in an Ontario hospital to investigate the creation and evaluation of a virtual emergency department (VED) prototype. The study evaluated VED acceptance, reliability of implementation, and impact on continuity, quality, and access to care. By conducting research, they found that providing a safe, quiet environment for virtual visits, quick and convenient access to treatment, and high patient satisfaction were all factors in VED success. The service's iterative expansion approach is another key factors that enables it to adjust to the demands of patients and doctors. On the other side, they discovered that barriers include problems in scheduling follow-up meetings and testing via the platform, as well as concerns among medical specialists that their experience would not be efficiently exploited in a distant setting. The VED has an average of 153 visits per month and has an overall positive response, improving patient satisfaction and access to care. However, ensuring the long-term viability of the service depends on removing these barriers and continuously improving them.
The study undertaken by Sharifi Kia et al. (2023) [42] aimed to provide a comprehensive analysis of the benefits and challenges associated with the use of telemedicine in emergency departments (EDs). A total of 12 of the 18 studies that were included in the analysis had a high risk of bias after undergoing a thorough methodological quality evaluation. According to the analysis, 9 studies support real-time video conferencing as the most recommended telemedicine technology for emergency departments. Meanwhile, the 8 of the studies cited cost savings as a major advantage, while 6 pointed out infrastructural and technological difficulties. The study found that increasing the general efficacy of emergency services requires telemedicine adoption for two main reasons, including improving patient care and reducing costs. Despite these advantages, there are still a lot of obstacles to be solved, such as poor infrastructure, difficult technology, and the need for substantial evidence to support viability. The study concluded that, despite telemedicine's great potential to improve patient care, more extensive study is necessary before emergency rooms can employ it.
Hose et al. (2023) [43] explored the challenges and enablers of adopting health information technology (HIT) in team-based healthcare environments. They were able to identify key factors that influenced the deployment of HIT by conducting interviews with 36 healthcare workers in 12 different professions. The study revealed that major barriers include technical issues, such as system incompatibilities and software malfunctions, which can disrupt workflows and reduce efficiency, as well as inadequate training and resistance to change among staff. These barriers highlighted the necessity of the solid technical assistance and ongoing training to guarantee integration goes well. Positively, the study also found that strong leadership, sufficient money, and thorough training were essential for the successful implementation of HIT. It became clear that organisational commitment to technology and human resources was essential to bringing about this transformation. They concluded that HIT could be made much more effective and efficient by utilising the facilitators and eliminating the barriers that had been discovered. This would eventually improve patient care and streamline healthcare operations.
Tyler et al. (2024) [44] explored how artificial intelligence (AI) and machine learning (ML) can enhance triage processes in emergency departments (EDs). In the study, they examined a total of 1142 publications from databases such as EMBASE, Ovid MEDLINE, and Web of Science as part of a systematic review of the literature up to September 2023. After a comprehensive screening process, 29 publications were selected for in-depth analysis. The findings indicated that AI has significant potential for boosting the consistency, efficiency, and accuracy of patient assessments. Over time, these advancements could result in improved patient care and more efficient use of resources. Nevertheless, the study identified several barriers to the successful integration of AI in triage emergency departments. Among these barriers are staff resistance, worries about data security, high initial costs, and the need for algorithms that are clear and understandable. In conclusion, while AI offers exciting possibilities for emergency medical care, addressing these challenges is essential for fostering collaboration, building trust, and ensuring smooth integration into healthcare systems.
Hudson et al. (2023) [45] investigated the potential use of AI-driven social robots to reduce children's anxiety and pain during intravenous procedures in paediatric emergency departments (EDs). A total of 11 medical professionals from two paediatric emergency departments in Canada were interviewed for the study. By conducting the study, they discovered several facilitators, which included the procedure-related stress might be considerably decreased by providing each kid with individualised emotional support and diversions based on their preferences. It was also thought to be advantageous to employ the robots' positive reinforcement. Besides that, they also identified several barriers, which included the need for age-appropriate interactions, space constraints in EDs, and the robot's capacity for independent situational adaptation. The study concluded that although lowering distress levels using AI-enhanced social robots might improve paediatric care, overcoming these barriers is necessary for widespread adoption. In order to achieve that, the involvement of healthcare professionals is critical to the development of effective robots that function effectively in busy emergency departments.
In a review by Katzman et al. (2023) [46], the expanding role of AI in emergency radiology was analyzed through the lens of both interpretive and non-interpretive applications. They studied a total of 44 studies that addressed the use of AI in workflow optimisation, image quality assurance, picture protocol management, and common emergency condition diagnosis. The study focused on the possible benefits of AI, such as how it may speed up patient treatment and automate tedious tasks, which would reduce radiologists' workload and improve outcomes. In the study, several significant barriers have been identified to the widespread application of AI in radiology. These barriers included costly costs, the need for medical education, and doubts over the reliability of algorithms. The study suggested that both a financial investment and a cultural change in medical practice are necessary to overcome these challenges.
In order to examine the role of AI technologies in the emergency medical treatment, Piliuk and Tomforde (2023) [47] conducted a systematic evaluation of 116 studies from 380 publications gathered from reputable databases such as IEEE Xplore, ACM Digital Library, Springer Library, ScienceDirect, and Nature. The focus of the selected articles was on using machine learning and deep learning techniques in emergency medical services. By conducting the study, they discovered that AI can handle large volumes of data quickly, which improves diagnosis, optimises patient flow, enhances decision-making, and manages resources more effectively. These benefits might lead to a better patient outcome. However, the study also revealed several barriers, including the expensive cost of AI, the need for extensive training, concerns about data privacy, and unequal AI performance in different clinical settings. The study concluded that further quality, prospective research is required to validate the benefits of artificial intelligence and address the challenges associated with integrating it into emergency medicine.
Jordan et al. (2023) [48] studied the introduction of KATE, an artificial intelligence clinical decision support tool, into the emergency department triage system of a community hospital in the United States. A total of 13 triage nurses from the emergency room participated in the study, and semi-structured interviews were used to gather data. Initially, the AI tool was considered with distrust due to its purported inability to take into account the contextual requirements of the scenario. However, as time passed, the nurses began to regard the tool as a helpful aid for supporting decisions. The study revealed several critical facilitators for its successful adoption, including enhanced patient safety, efficient assistance for decision-making, thorough training, and easy integration into current processes. However, barriers included aversion to change, a reliance on clinical expertise, and scepticism over the AI's capacity to take into account contextual and cultural elements. The study emphasised the significance of taking clinical staff knowledge and cultural aspects into account while deploying Al solutions in healthcare settings.
In order to help the reduce congestion in physical emergency departments, Australia established the Victorian Virtual Emergency Department (VVED) to provide virtual care for non-emergency situations. Talevski et al. (2024) [49] examined the program's development and success. Over 300,000 patients in Victoria have received consultations via the VVED since its introduction, with an average of over 600 virtual consultations every day. The study findings indicated that several factors contributed to the program's efficacy, such as robust institutional backing, progressions in digital healthcare, and the necessity for substitute care approaches amid the COVID-19 outbreak. However, barriers included technical difficulties, resistance from healthcare professionals, and concerns about the quality of care provided virtually. Although virtual emergency departments (VEDs) can significantly reduce overcrowding and improve patient outcomes, the study, which used 500 patients who used the VVED service as a sample, concluded that the continued improvements are necessary to ensure the feasibility and usefulness of such programs.
2.2. Overview of Reviewed Studies
Through examination of these studies, numerous barriers and facilitators to the implementation of technology in emergency departments were identified. High employee turnover and limited resources, particularly in rural areas, are significant barriers. For example, manpower shortages, high costs, and inadequate infrastructure were noted by Zachrison et al. (2020) [24] and Nataliansyah et al. (2022) [30] as major telemedicine adoption barriers in rural areas. However, Fujimori et al. (2022) [22] and Jordan et al. (2023) [48], who performed their investigations in urban areas, observed system usability issues such as incompatibilities and integration challenges, particularly when implementing AI-based decision support systems.
On the other hand, some studies emphasised facilitators including effective communication, proactive management, and good leadership. For example, Anaraki et al. (2024) [12] illustrated the significance of supportive management, effective teamwork and effective communication in implementing quality improvement programs, while Huilgol et al. (2024) [23] emphasised the importance of supportive leadership in the adoption of technology. Additionally, training and education tailored to specific needs were also acknowledged as significant facilitators, according to Salwei et al. (2022) [38] and Fujimori et al. (2022) [22].
These findings serve as the framework for the accompanying discussion of ideas for improving technology adoption in the emergency department.
3. Materials and Methods
3.1. Research Methodology
Throughout the thorough assessment, several criteria were used to guarantee the quality of this study. Firstly, the study's primary goal was to include existing research on the factors that encourage and hinder the adoption of new technologies, particularly in emergency rooms. As such, 30 peer-reviewed articles relevant to the use of technology in emergency departments were included.
Secondly, a comprehensive search was carried out with keywords like "technology adoption," "influence factors," "medical technology," "barriers," "healthcare," "emergency," "emergency room," "ER," "emergency departments," "ED," "acute care," "emergency care," "emergency medicine," "accident and emergency," and "A&E" to make sure that only relevant articles were included.
Third, only those articles that were published between 2019 and 2024 were taken into account in this study to ensure the review incorporates the most recent research and the latest data on the subject.
Lastly, the reviewed articles were gathered from credible and applicable sources, such as the JMIR, Frontiers, ScienceDirect, BMC Health Services Research, SpringerLink, ScienceDirect, MDPI, BMJ, Research Square, BMJ, NLM, and the Sage Journals.
The PRISMA flow diagram for this study is shown in Figure 1, which outlines the procedure followed in locating and choosing pertinent papers for inclusion.
First, 108 records were identified through database searches from sources such as Frontiers (n = 7), JMIR (n = 7), BMC (n = 6), ScienceDirect (n = 13), SpringerLink (n = 9), JAMIA (n = 9), BMJ (n = 12), Research Square (n = 11), MDPI (n = 7), NLM (n = 9), Sage Journals (n = 7), JACEP OPEN (n = 5), Nature (n = 3), and IEEE (n = 3). After removing 8 duplicates, a total of 100 records remained to be reviewed. 40 of these were then eliminated because their abstracts or titles did not discuss the use of technology in emergency rooms. Following that, 40 studies were determined to be ineligible after the remaining 60 articles were assessed for eligibility. Among them, 18 articles were eliminated for concentrating on other departments, 15 articles were eliminated for not being related to technology, and 7 articles were eliminated because their published time frame was not between the years 2019 to 2024. Subsequently, an additional 10 articles were incorporated into the review process, bringing the total number of studies selected for the final analysis up to 30. This was done since bigger sample sizes yield more reliable results. Due to this systematic process, only the most relevant publications were kept for examination.
3.2. Meta-Analysis
Narrative Synthesis (Qualitative Meta-Analysis)
This study was unable to employ the conventional meta-analysis due to the lacked specific quantitative results and offered no effect estimates, statistics, or raw data in those reviewed articles. To explore the barriers and facilitators that affect technology adoption in emergency departments across research, this study employed a narrative synthesis technique.
The evaluated studies contained both qualitative and quantitative methodologies, and there was a wide range in sample sizes and methodology. For example, a study done by Hall et al. (2022) [21] examined the deployment of virtual emergency care with 13 participants. On the other hand, a study done by Fujimori et al. (2022) [22] assessed the efficacy of an AI-based CDSS using a sample size of 27,550 patients. The range of sample sizes demonstrates the diversity of study environments, ranging from small-scale qualitative investigations to extensive quantitative assessments.
The results of the studies that were analysed in this study revealed the common barriers and facilitators to the technology adoption in the emergency department, notwithstanding the absence of precise figures. Numerous studies revealed the presence of barriers such as high turnover rates, limited personnel training, and system incompatibility. For instance, Zachrison et al. (2020) [24] emphasised the expense and complexity of the telehealth systems as important barriers facing rural emergency departments. Meanwhile, Anaraki et al. (2024) [12] underlined low management participation as a major barrier. In the meantime, Fujimori et al. (2022) [22] discovered that system incompatibility is one of the key barriers that influence novel technology acceptance. On the other hand, management that was supportive, good at communicating, and led with strength were often mentioned as factors that helped people accept technology. Studies such as Huilgol et al. (2024) [23] and Kennedy et al. (2024) [31] supported this perspective. Their study demonstrated that the successful implementation of new technologies in emergency departments requires strong leadership and an adequate workforce.
Although quantitative meta-analysis was unable to be employed for this study, the narrative synthesis provided a comprehensive understanding of the ongoing barriers and facilitators that influence technology use in the emergency departments. The results suggested that strengthening leadership support, staff training, and system usability are crucial to overcoming hurdles and expediting the adoption of the technology developments in emergency departments.
4. Discussion
4.1. Literature Analysis
This study's review includes detailed information about the topic, participants, and sample size of each study in Table 1. The comprehensive synopsis facilitated could provide a more in-depth examination of the research's individual approaches and settings while also making it simple to consult the studies.
Additionally, Table 2 focused on emphasising the barriers and facilitators identified in each of the studies that were analysed in this study. Due to the side-by-side presentation of these barriers and facilitators, provides a more comprehensive perspective, which makes it simpler to comprehend the difficulties that each study encountered and the elements that contributed to the system's successful implementation.
In order to get a better understanding of the problem of technology adoption that faced by the emergency departments, this study evaluated a significant number of papers on a variety of topics relevant to emergency departments, such as telemedicine, AI-based decision support systems, virtual urgent care, and quality improvement programs, as shown in Table 2. These evaluated papers were gathered from several countries, removing bias and demonstrating a desire to improve emergency care on a worldwide scale, including Ghana, Australia, the United States, Canada, Japan, and the United States, among others.
A successful adoption of technology in emergency departments requires feedback not just from doctors, but also from other emergency department stakeholders. As a result, participants in these examined studies came from a variety of backgrounds, including patients, managers, nurses, and doctors. This wide inclusion aids in providing a comprehensive picture of the problems encountered in emergency rooms as well as the perceptions and experiences of various remedies. Given the importance of the data from both methodologies, this study focused on both the qualitative and quantitative research methods to ensure a complete understanding of the subject. This study provided a comprehensive and patient-centred knowledge of how to enhance emergency medical treatment by combining a range of topics, viewpoints, countries, and research methodologies.
4.2. Comparative Analysis
In order to provide a more intuitive understanding of the findings, this study clustered the reviewed studies by rural and urban settings and highlighted notable trends in technology adoption in emergency departments. Studies carried out in rural areas often indicate that the resource and infrastructural constraints are the main barriers to the adoption of new technologies. For example, Zachrison et al. (2020) [24] discovered that staffing shortages and costly costs are frequent barriers that rural emergency departments in the US have when attempting to utilise the telemedicine. This viewpoint was further supported by Nataliansyah et al. (2022) [30], who determined that these two obstacles were the key barriers affecting the effective use of telemedicine in emergency departments in remote areas. Furthermore, the primary barriers to the continuous application of telemedicine technologies are those related to infrastructure, such as unstable internet and telecommunications networks.
On the other hand, studies conducted in urban emergency departments, particularly those with abundant resources, typically concentrate on advanced technology like clinical decision support systems (CDSS) and AI-based systems. For example, Fujimori et al. (2022) [22] investigated the adoption of an AI-based CDSS in a tertiary hospital. It was discovered that the key barriers faced by emergency departments in urban environments were mostly linked to usability, including incompatibility with the institution's existing systems, which varied from those in rural areas. These urban settings benefit from more robust IT infrastructure, enabling more reliable use of these advanced technologies. Similar to this, Pu et al. (2024) [26] also conducted a study and emphasised how Victoria, Australia's metropolitan virtual emergency departments (VEDs) have effectively expanded because of a stronger healthcare infrastructure and a higher wealth of resources.
Additionally, this study also grouped the reviewed studies according to the kind of technology and discovered various trends in the uptake of various technological advancements in emergency departments. For instance, AI-based systems typically face greater resistance because of their complexity. Studies conducted by Piliuk and Tomforde (2023) [47] and Fujimori et al. (2022) [22] have demonstrated that AI-driven CDSS frequently encounter the usability issues, such as the system integration problems and uncertainties regarding the precision and dependability of AI suggestions. These barriers exacerbate clinician resistance, as there is a perception that Al systems will complicate workflows and require extensive training to fully function. The complexity of it, coupled with concerns about system failures at critical moments in patient care, makes AI-based technologies more difficult to adopt, especially in high-pressure emergency department environments where quick decision is required.
In contrast, there is typically less opposition to technology like virtual emergency care systems and telemedicine platforms. Since they may expand on current communication channels and instantly increase access to care, particularly in rural or underserved regions, they are comparatively easy to adopt (Zachrison et al., 2020) [24]. Telemedicine solutions are thought to be useful, easy to use, and capable of rapidly improving patient outcomes. However, they still encounter obstacles, such as those related to infrastructure and worries about the calibre of virtual healthcare, but they are less formidable than sophisticated AI systems.
In conclusion, categorising emergency department technology adoption studies by rural and urban environments, as well as technology type, found significant tendencies across contexts. In rural emergency departments, lack of infrastructure and resources are the main barriers to technology adoption, especially telemedicine technologies, which are limited by cost, staff shortages, and unreliable communication networks. In urban settings, research focuses more on advanced technologies such as artificial intelligence (AI)-driven CDSS, but their adoption is often hindered by system compatibility and complexity in clinical use. Meanwhile, barriers to technology adoption might vary depending on the type of technology. The telemedicine and virtual emergency care systems are relatively simple to implement, as they are effective in improving access to care, especially in rural areas. In contrast, the AI-based systems face more usability and integration issues, increasing the resistance from clinicians.
4.3. Critical Analysis
This study examined 30 prior studies on technology adoption, as indicated in Table 2, in order to evaluate the challenges and enablers related to implementing new technologies in emergency rooms. By conducting this study, a detailed grasp of the elements that impact the technological adoption was provided, which also identified important facilitators that may improve adoption in these situations. Furthermore, as Table 1 shows, several studies incorporated perspectives from people who weren't in emergency rooms, such as patients and hospital administrators, because these people's opinions were thought to have an impact on how new technology is adopted in these environments.
Table 2 shows that there are several barriers that make it difficult to integrate new technology and practices in emergency departments. After analysing these studies, several common barriers that affected emergency departments' use of technology have been found. One of the most common barriers is high turnover rates and personnel shortages, which are frequently mentioned as major barriers. Based on these reviewed studies, it is more difficult for the current team to adapt to a new technologies when there is a shortage of staff or a high employee turnover rate. This is because the instability might interrupt the continuity needed to build expertise and harness the potential of the new systems. Besides that, the performance and access difficulties with technology are also one of the common barriers. Numerous studies demonstrate how personnel might become frustrated and prevent the efficient use of technology due to sluggish systems, frequent outages, and inadequate training. In addition, insufficient availability of technology, particularly in marginalised regions, may impede the optimal utilisation of novel systems. Furthermore, the combination of a high workload and resistance to change is another major barrier. Clinicians may be reluctant to accept changes when new systems or programs are implemented because they feel overburdened by the additional responsibilities. This aversion might be exacerbated by the weight of their current responsibilities, making it more difficult to incorporate new tools into their hectic schedules.
In the meanwhile, the review has identified several facilitators that can aid in the successful adoption of technology in emergency departments. One of the main facilitators is the management's support and involvement. Leaders who actively participate in the implementation process and provide the necessary resources are critical to ensuring a smooth transition. With support and commitment to the project, team confidence and morale are likely to soar, which will boost the adoption of new technology. In addition to good leadership, cooperation and efficient communication are critical facilitators. Effective collaboration and honest communication among team members ensures that everyone is working towards the same goals and is on the same page. This collaborative approach fosters a problem-solving culture that helps resolve any difficulties that may arise during implementation. Furthermore, the education and training also the important enabling factors are education and training. By giving them thorough training, employers may lessen their opposition to new technology by increasing their competence and self-assurance in utilising it. Continuous education also ensures that employees stay up to date with the latest developments, enabling them to make the most of technology. Together, these facilitators create a supportive environment that enhances the integration of new technologies in emergency departments.
From a theoretical standpoint, this study examined the facilitators and barriers that associated with the adoption of technology in the emergency department in various contexts and geographies. It clarifies the barriers that influenced the technology adoption, such as the restricted access to technology, a lack of employees, and training hurdles. Meanwhile, it has also emphasised those important facilitators, such as the helpful management, clear communication, and ample resources. In order to improve the efficacy and sustainability of emergency care innovations, this study analysed several studies, where highlighting the significance of context-specific techniques and cooperative efforts. By conducting this in-depth research, the study provides insightful information to healthcare professionals and policymakers, giving them the tools they need to make informed decisions. This understanding can lead to targeted interventions that improve services in emergency departments, ultimately benefiting both healthcare providers and the patients they serve.
From a practical standpoint, this study suggested many tactics to improve the efficacy of technology adoption. Firstly, it is important to investigate comprehensive training programs for employees since they may provide those employees with the confidence and information they need to effectively embrace the technology. Furthermore, the establishment of resilient support systems may efficiently tackle technical issues and offer ongoing assistance, hence reducing discontent and opposition. Thirdly, identifying and empowering local champions, which are the people who support and campaign for these changes, can also greatly accelerate acceptance and guarantee that advancements are maintained over time. Healthcare organisations may improve their performance by focusing on practical strategies to overcome hurdles while deploying new technology in emergency departments.
4.4. Strategies for Technology Adoption
In order to better adapt to new technologies, healthcare providers should consider developing a well-established change management approach. The two most popular change management frameworks that may be employed in this circumstance are Lewin’s Change Management Model and Kotter's eight phases to leading change [50]. These frameworks provide an organised method for handling the difficulties associated with organisational transformation. For instance, Kotter's strategy focuses on creating a feeling of urgency among the change's stakeholders in order to persuade them to embrace new technological developments [51]. It has also brought attention to the significance of building a coalition of leaders who can effectively advocate for change, articulate their vision, and share it with the entire organisation [51]. This cooperative approach is essential for managing resistance and ensuring consensus on shared goals.
In addition, the adoption of new technologies can be accelerated through the application of the Lewin’s Change Management Model. This is due to the fact that it explains the mental and emotional changes that individuals undergo throughout periods of change [52]. It defines three main processes, unfreeze, change, and refreeze, that assist firms in preparing their employees for change, making essential changes, and incorporating new practices into company culture [52]. Using these frameworks, healthcare organisations may introduce technology more methodically, addressing not just the technical issues of integration, but also the psychological and emotional factors that drive staff acceptance and engagement.
By applying a change management model and focusing on these practical strategies, healthcare organizations can enhance their operations and successfully handle the obstacles that come with integrating new technologies in the emergency department. The use of a structured change management strategy may facilitate the effective and sustainable adoption of technology by ensuring that all stakeholders are informed, involved, and provided with full assistance during the transition process.
4.5. Innovation and Contribution
The study examined several studies on the adoption of technology in the healthcare industry alongside the barriers and facilitators that they discovered. The most prevalent barriers and facilitators were identified through this study. Based on the study's findings, the healthcare industry and technology providers may either enhance their services and products or offer solutions that address the facilitators and barriers. It is anticipated that this will speed up and facilitate the uptake of technology.
Emergency departments in the healthcare industry may overcome these barriers by learning from successful models in other industries. For example, several common barriers highlighted in this study may be efficiently addressed by companies that have successfully adopted and implemented technology, such as the automobile, retail and e-commerce, food, technology, and aircraft industries.
First, the emergency departments may consult the automobile industry in order to address the issue of excessive turnover and a lack of personnel. By using Standard Operating Procedure (SOP), the majority of the automotive industry has standardised procedures and streamlined workflows to minimise dependency on large teams and boost productivity. They have also introduced cross-training to provide employees the flexibility to transition between roles [53], [54]. This method can help emergency departments streamline clinical operations, cut down on unnecessary labour, and free up medical staff time for more important duties. In the face of regular staff turnover, cross-training personnel for different positions helps guarantee work continuity and efficiency.
The second issue facing emergency departments is the impact of technology on performance and accessibility. Similar challenges have also been experienced by certain retailers and e-commerce companies, such as Amazon, however, they have been able to resolve scalability and performance concerns by utilising Amazon Web Services (AWS) and other cloud computing services [55], [56]. Emergency departments can similarly benefit from cloud technology to enhance system performance by minimising the system downtime, increasing data access speeds, and providing scalable storage solutions. By guaranteeing the continuous availability and stability of vital medical systems, this eventually increases user confidence in the technology and pushes for its more widespread adoption.
Insufficient availability of technology is also one of the common issues, particularly in places with minimal resources. Emergency departments can draw inspiration from the food industry's strategy since it has encountered comparable challenges. Starbucks is a prominent example in the food industry that has effectively surmounted this obstacle by employing a phased implementation approach [57] over several locations, all the while maintaining the conventional procedure. In underprivileged areas or marginalised regions, emergency departments should take a similar strategy by progressively using the digital technologies. This would preserve the functioning of current systems while enabling medical staff to become accustomed to new technologies.
Resistance to change and a heavy workload are two more significant barriers to the adoption of new technologies. The technology industry that has successfully adopted various advancements can offer useful lessons to emergency departments. The majority IT companies, like IBM, have discovered that including teams in decision-making enhances their ability to adapt to change and reduces resistance to new practices [58]. A similar strategy may be used by emergency departments, which would encourage the cooperation and transparent communication while implementing technology gradually. This method can ease employee worry about the new technologies while also resolving workload issues, thus enhancing the likelihood of effective adoption. By providing a supportive environment during the transition phase, employees will feel empowered and engaged in the process, which will further enhance the possibility of accepting the changes.
Lastly, training and ongoing education are critical to the effective adoption of new technology. The healthcare industry may learn from the aircraft industry since it is most similar to the healthcare industry out of all of them. Pilots receive ongoing simulation training from them to assist them become more competent and confident while interacting with new systems [59]. Therefore, emergency departments may guarantee that staff members are competent in using new medical equipment under pressure by providing frequent refresher courses and using simulation-based training to acquaint staff members with new technology in a low-risk setting.
4.6. Limitation and Future Research
The study has significant limitations. First, the number of studies analysed in this study is insufficient for providing more comprehensive and accurate findings. Larger research pools are known to provide more accurate results and more in-depth analysis. Therefore, the volume of reviewed studies plays a key role in enhancing the accuracy of research results. Conversely, a lower sample size might have an influence on the results and make it harder for them to accurately capture the distinctive features of emergency departments in the healthcare industry.
Furthermore, the study failed to distinguish across healthcare settings, as some of the examined studies were conducted in rural locations, while others were conducted in metropolitan areas. Because of these distinctions between the rural and urban areas, there may be variances in the barriers and facilitators. For example, rural areas may place a greater emphasis on the issue of the resources because they have fewer resources available, which has a significant impact on the adoption of new technologies. Since medical officers are the group of individuals who will be utilising the technology, their reluctance to change might pose a substantial obstacle to the adoption of the technology. Nevertheless, the acceptance of medical officers will be the focus of the urban setting. This constraint may make it challenging to combine the results of the study or use them broadly.
Thirdly, the majority of the responses collected in these reviewed studies were self-reported by the medical officers, which raises the possibility of recollection or response bias. Individuals from diverse backgrounds, such as varying roles in emergency rooms or hospitals, may contribute distinct reactions due to their exposure to disparate settings. This is because responses are influenced by institutional pressures or personal experiences, which may result in varied responses regarding barriers and facilitators.
Fourth, the lack of longitudinal data is another important limitation in this study. This is due to the fact that one-time data collection was used in the majority of the analysed studies in this study, which increases the possibility of bias. The reason for this is that it is challenging to fully understand how these technologies function over time without tracking the long-term adoption outcomes. The lack of the prolonged observation may make it more challenging to precisely identify both the barriers and the facilitators of adoption since some of the important factors that influence the adoption may only become evident or alter with continued usage. Because of this, the findings were unable to provide a comprehensive picture of the long-term dynamics related to technology adoption.
As a result, future research is encouraged to examine a wider range of the studies in order to improve more accurate and reliable results. Besides that, it is also important to differentiate between the healthcare environments in rural and urban areas due to the notable variations in different areas in barriers and facilitators. In addition, the self-reported data should not be the only source of the information used by researchers, as respondents to surveys or interviews may have inaccurate impressions of the technology. Furthermore, adding longitudinal data will give a more in-depth understanding of the long-term effects of technology adoption and a more thorough grasp of the contributing components. Thus, future studies should focus on gathering primary data from medical officers and patients in the emergency department by using method, including direct observation, interviews, and questionnaires. By using this method, researchers will be able to gain firsthand data with the technology adoption, which will help them better understand its complexities and minute changes in practical contexts. Furthermore, researching the long-term effects of technology adoption in emergency departments not only exposes changes over time but also aids in assessing the initial impact on efficiency and patient care. These longitudinal studies can identify patterns, areas of adaptation, and areas where technology use can be improved, and also will be able to provide important insights into a more complete understanding of the ultimate successful integration of technology into the emergency medical setting. By addressing these questions, future research can build on existing findings and make practical recommendations to promote the widespread use of technology in healthcare.
4.7. Conclusion
The complicated setting of the technology adoption in the emergency departments is clarified by this study, which also highlighted the barriers and facilitators that influence the adoption of new technologies. According to this study, there are several significant barriers that influenced the new system's adoption and leverage, such as the high turnover rates and a lack of qualified workers. This is because the instability of the employees might interrupt the continuity needed to build expertise and harness the potential of new systems. Besides that, the performance problems with technology, such as sluggish systems and insufficient training, exacerbate dissatisfaction and impede efficient utilisation. Furthermore, it is difficult to implement new technologies because of the excessive workload and aversion to change among practitioners, since the additional obligations might feel burdensome.
Conversely, the study identified a few potential facilitators that may help technology adoption go more smoothly. Firstly, supportive management is essential as it can greatly increase the likelihood of effective implementation when leaders take an active role and supply the required resources. Besides that, clear communication and efficient cooperation are also essential for ensuring that everyone is in agreement and equipped to handle any problems that may come up. Last but not least, the employees must get a thorough training and instruction in order to overcome the opposition and feel comfortable when using the new technology.
In light of these findings, policymakers and healthcare leaders must develop targeted strategies to address the specific challenges faced by emergency departments. In addition, policymakers should consider developing special directives that encourage collaborative efforts and tailored remedies to the unique needs of emergency departments. With these insights, the healthcare industry will be better able to encourage technological innovation, resulting in faster adoption of critical technologies and, ultimately, improved patient outcomes. On the other hand, healthcare leaders must create a culture of continuous learning and mentorship, ensuring that the newly medical officers have the support they need to adapt to new technologies. Continuous learning and mentoring programs are programs where experienced medical officers can mentor new medical officers, reduce turnover, and increase technology utilisation. Leaders should also focus on fostering open communication and removing any organizational barriers that slow down technology adoption.
In summary, this study highlighted the necessity of customised approaches and cooperative endeavours to tackle the different barriers encountered by emergency departments. By reducing these barriers and emphasising cooperation, technology innovation in the healthcare industry may be encouraged more successfully. This will result in a faster introduction of critical technologies that will improve patient outcomes and operational effectiveness in emergency departments. Further research should go further into these findings and investigate creative techniques to improving technology integration and establishing higher standards of care inside emergency departments.
Author Contributions
Funding acquisition, R.K.R.; methodology, R.K.R.; supervision, R.K.R.; writing—original draft, A.T.L.; writing—review and editing, R.K.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Telekom Research & Development Sdn Bhd (TM R&D) under Project ID: RDTC/241124, which also covered the page charges for this publication.
Institutional Review Board Statement
This study does not include human participants or any experimental procedures involving personal data. It is a review that uses publicly available data from peer-reviewed research that has already been published. No sensitive data, private information, or personally identifiable information was collected or analysed. Since this study complies with ethical guidelines for non-intervention studies, it does not require formal ethics approval. The analysed research cited in this article was carried out in accordance with the ethical guidelines established by the corresponding ethics committees or institutional review boards (IRBs). This ensures that the original research adhered to the principles of informed consent, data privacy, and participant protection.
Informed Consent Statement
Not applicable.
Data Availability Statement
This study does not create ethical issues about data security, privacy, or confidentiality because of the nature of the review and the lack of human participants in the research process.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| EDs | Emergency Department |
| VUC | Virtual Urgent Care |
| AI | Artificial Intelligence |
| CDSS | Clinical Decision Support System |
| OUD | Opioid Use Disorder |
| EHR | Electronic Health Records |
| HFE | Human Factors Engineering |
| PE | Pulmonary Embolism |
| DAs | Decision Aids |
| SDM | Shared Decision-Making |
| HIRAID® | History including Infection risk, Red flags, Assessment, Interventions, Diagnostics |
| PRISMA-ScR | Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews |
| PEDs | Portable Electronic Devices |
| AWS | Amazon Web Services |
| VEDs | Virtual Emergency Departments |
| SOP | Standard Operating Procedure |
References
- R. Hendayani and M. Y. Febrianta, “Technology as a driver to achieve the performance of family businesses supply chain,” Journal of Family Business Management, vol. 10, no. 4, pp. 361–371, Nov. 2020. [CrossRef]
- N. Pilevari and F. Yavari, “Journal of Industrial Strategic Management Industry Revolutions Development from Industry 1.0 to Industry 5.0 in Manufacturing,” Journal of Industrial Strategic Management, vol. 2020, no. 2, pp. 44–63, 2020.
- K. Yu, L. Lin, M. Alazab, L. Tan, and B. Gu, “Deep Learning-Based Traffic Safety Solution for a Mixture of Autonomous and Manual Vehicles in a 5G-Enabled Intelligent Transportation System,” IEEE Transactions on Intelligent Transportation Systems, vol. 22, no. 7, pp. 4337–4347, Jul. 2021. [CrossRef]
- S. Hermes, T. Riasanow, E. K. Clemons, M. Böhm, and H. Krcmar, “The digital transformation of the healthcare industry: exploring the rise of emerging platform ecosystems and their influence on the role of patients,” Business Research, vol. 13, no. 3, pp. 1033–1069, Nov. 2020. [CrossRef]
- A. Bohr and K. Memarzadeh, “The rise of artificial intelligence in healthcare applications,” in Artificial Intelligence in Healthcare, Elsevier, 2020, pp. 25–60. [CrossRef]
- M. A. Sujan, S. White, I. Habli, and N. Reynolds, “Stakeholder perceptions of the safety and assurance of artificial intelligence in healthcare,” Saf Sci, vol. 155, Nov. 2022. [CrossRef]
- I. Kulkov, A. Tsvetkova, and M. Ivanova-Gongne, “Identifying institutional barriers when implementing new technologies in the healthcare industry,” European Journal of Innovation Management, vol. 26, no. 4, pp. 909–932, Jun. 2023. [CrossRef]
- H. Bruun, L. Milling, S. Mikkelsen, and L. Huniche, “Ethical challenges experienced by prehospital emergency personnel: a practice-based model of analysis,” BMC Med Ethics, vol. 23, no. 1, Dec. 2022. [CrossRef]
- J. L. Hick and A. T. Pavia, “Duty to Plan: Health Care, Crisis Standards of Care, and Novel Coronavirus SARS-CoV-2,” National Library of Medicine, 2020. [CrossRef]
- O. J. Canfell et al., “Understanding the Digital Disruption of Health Care: An Ethnographic Study of Real-Time Multidisciplinary Clinical Behavior in a New Digital Hospital,” Appl Clin Inform, vol. 13, no. 5, pp. 1079–1091, Oct. 2022. [CrossRef]
- C. Østervang, C. M. Jensen, E. Coyne, K. B. Dieperink, and A. Lassen, “Usability and Evaluation of a Health Information System in the Emergency Department: A Mixed Methods Study (Preprint),” JMIR Hum Factors, Apr. 2023. [CrossRef]
- N. R. Anaraki et al., “A qualitative study of the barriers and facilitators impacting the implementation of a quality improvement program for emergency departments: SurgeCon.,” BMC Health Serv Res, vol. 24, no. 1, p. 855, Jul. 2024. [CrossRef]
- M. H. Alshammari and A. Alenezi, “Nursing workforce competencies and job satisfaction: the role of technology integration, self-efficacy, social support, and prior experience,” BMC Nurs, vol. 22, no. 1, Dec. 2023. [CrossRef]
- M. Vainieri, C. Panero, and L. Coletta, “Waiting times in emergency departments: A resource allocation or an efficiency issue?,” BMC Health Serv Res, vol. 20, no. 1, Jun. 2020. [CrossRef]
- N. T. Stefánsdóttir et al., “Implementing a new emergency department: a qualitative study of health professionals’ change responses and perceptions,” BMC Health Serv Res, vol. 22, no. 1, Dec. 2022. [CrossRef]
- R. Cheraghi, H. Ebrahimi, N. Kheibar, and M. H. Sahebihagh, “Reasons for resistance to change in nursing: an integrative review,” BMC Nurs, vol. 22, no. 1, Dec. 2023. [CrossRef]
- P. T. Chen, C. L. Lin, and W. N. Wu, “Big data management in healthcare: Adoption challenges and implications,” Int J Inf Manage, vol. 53, Aug. 2020. [CrossRef]
- Y. J. Kim, J. H. Choi, and G. M. N. Fotso, “Medical professionals’ adoption of AI-based medical devices: UTAUT model with trust mediation,” Journal of Open Innovation: Technology, Market, and Complexity, vol. 10, no. 1, Mar. 2024. [CrossRef]
- T. K. Mackey et al., “‘Fit-for-purpose?’ - Challenges and opportunities for applications of blockchain technology in the future of healthcare,” BMC Med, vol. 17, no. 1, Mar. 2019. [CrossRef]
- E. Elder, A. N. B. Johnston, M. Wallis, and J. Crilly, “The demoralisation of nurses and medical doctors working in the emergency department: A qualitative descriptive study,” Int Emerg Nurs, vol. 52, p. 100841, Sep. 2020. [CrossRef]
- J. N. Hall et al., “Designs, facilitators, barriers, and lessons learned during the implementation of emergency department led virtual urgent care programs in Ontario, Canada,” Front Digit Health, vol. 4, Aug. 2022. [CrossRef]
- R. Fujimori et al., “Acceptance, Barriers, and Facilitators to Implementing Artificial Intelligence–Based Decision Support Systems in Emergency Departments: Quantitative and Qualitative Evaluation,” JMIR Form Res, vol. 6, no. 6, Jun. 2022. [CrossRef]
- S. S. Huilgol, C. T. Berdahl, N. Qureshi, C. C. Cohen, P. Mendel, and S. H. Fischer, “Innovation adoption, use and implementation in emergency departments during the COVID-19 pandemic,” BMJ Innov, p. bmjinnov-2023-001206, Apr. 2024. [CrossRef]
- K. S. Zachrison, K. M. Boggs, E. M. Hayden, J. A. Espinola, and C. A. Camargo, “Understanding Barriers to Telemedicine Implementation in Rural Emergency Departments,” Ann Emerg Med, vol. 75, no. 3, pp. 392–399, Mar. 2020. [CrossRef]
- T. Boyle et al., “Hospital-Level Implementation Barriers, Facilitators, and Willingness to Use a New Regional Disaster Teleconsultation System: Cross-Sectional Survey Study,” JMIR Public Health Surveill, vol. 9, 2023. [CrossRef]
- D. Pu et al., “Virtual emergency care in Victoria: Stakeholder perspectives of strengths, weaknesses, and barriers and facilitators of service scale-up,” Australas Emerg Care, vol. 27, no. 2, pp. 102–108, Jun. 2024. [CrossRef]
- E. Antor, J. Owusu-Marfo, and J. Kissi, “Usability evaluation of electronic health records at the trauma and emergency directorates at the Komfo Anokye teaching hospital in the Ashanti region of Ghana,” BMC Med Inform Decis Mak, vol. 24, no. 1, Dec. 2024. [CrossRef]
- M. Bhosekar, S. Mena, S. Mihandoust, A. Joseph, and K. C. Madathil, “An Exploratory Study to Evaluate the Technological Barriers and Facilitators for Pediatric Behavioral Healthcare in Emergency Departments,” in Proceedings of the Human Factors and Ergonomics Society, SAGE Publications Inc., 2023, pp. 2560–2563. [CrossRef]
- K. Hodwitz et al., “Healthcare workers’ perspectives on a prescription phone program to meet the health equity needs of patients in the emergency department: a qualitative study,” Canadian Journal of Emergency Medicine, Aug. 2024. [CrossRef]
- M. M. Nataliansyah et al., “Managing innovation: a qualitative study on the implementation of telehealth services in rural emergency departments,” BMC Health Serv Res, vol. 22, no. 1, Dec. 2022. [CrossRef]
- B. Kennedy et al., “Establishing enablers and barriers to implementing the HIRAID® emergency nursing framework in rural emergency departments,” Australas Emerg Care, Aug. 2024. [CrossRef]
- A. J. Moy et al., “Understanding the perceived role of electronic health records and workflow fragmentation on clinician documentation burden in emergency departments,” Journal of the American Medical Informatics Association, vol. 30, no. 5, pp. 797–808, May 2023. [CrossRef]
- L. Uscher-Pines, J. Sousa, A. Mehrotra, L. H. Schwamm, and K. S. Zachrison, “Rising to the challenges of the pandemic: Telehealth innovations in U.S. emergency departments,” Journal of the American Medical Informatics Association, vol. 28, no. 9, pp. 1910–1918, Sep. 2021. [CrossRef]
- A. H. Wong et al., “Formative evaluation of an emergency department clinical decision support system for agitation symptoms: a study protocol,” BMJ Open, vol. 14, no. 2, Feb. 2024. [CrossRef]
- H. J. Barton et al., “Academic Detailing as a Health Information Technology Implementation Method: Supporting the Design and Implementation of an Emergency Department–Based Clinical Decision Support Tool to Prevent Future Falls,” JMIR Hum Factors, vol. 11, no. 1, Jan. 2024. [CrossRef]
- T. Billah, L. Gordon, E. M. Schoenfeld, B. P. Chang, E. P. Hess, and M. A. Probst, “Clinicians’ perspectives on the implementation of patient decision aids in the emergency department: A qualitative interview study,” JACEP Open, vol. 3, no. 1, Feb. 2022. [CrossRef]
- N. Davison et al., “Barriers and facilitators to implementing psychosocial digital health interventions for older adults presenting to emergency departments: a scoping review protocol,” BMJ Open, vol. 14, no. 8, p. e085304, Aug. 2024. [CrossRef]
- M. E. Salwei, P. Carayon, D. Wiegmann, M. S. Pulia, B. W. Patterson, and P. L. T. Hoonakker, “Usability barriers and facilitators of a human factors engineering-based clinical decision support technology for diagnosing pulmonary embolism,” Int J Med Inform, vol. 158, Feb. 2022. [CrossRef]
- M. J. Simpson et al., “Implementation strategies to address the determinants of adoption, implementation, and maintenance of a clinical decision support tool for emergency department buprenorphine initiation: a qualitative study,” Implement Sci Commun, vol. 4, no. 1, Dec. 2023. [CrossRef]
- H. D. Shin et al., “Barriers and Facilitators to Using an App-Based Tool for Suicide Safety Planning in a Psychiatric Emergency Department: A Qualitative Descriptive Study Using the Theoretical Domains Framework and COM-B Model,” 2024. [CrossRef]
- J. Shuldiner, D. Srinivasan, L. Desveaux, and J. N. Hall, “The Implementation of a Virtual Emergency Department: Multimethods Study Guided by the RE-AIM (Reach, Effectiveness, Adoption, Implementation, and Maintenance) Framework,” JMIR Form Res, vol. 7, no. 1, Jan. 2023. [CrossRef]
- A. Sharifi Kia, M. Rafizadeh, and L. Shahmoradi, “Telemedicine in the emergency department: an overview of systematic reviews,” Aug. 01, 2023, Institute for Ionics. [CrossRef]
- B. Z. Hose et al., “Work system barriers and facilitators of a team health information technology,” Appl Ergon, vol. 113, p. 104105, Nov. 2023. [CrossRef]
- S. Tyler et al., “Use of Artificial Intelligence in Triage in Hospital Emergency Departments: A Scoping Review,” Cureus, May 2024. [CrossRef]
- S. Hudson et al., “Perspectives of Healthcare Providers to Inform the Design of an AI-Enhanced Social Robot in the Pediatric Emergency Department,” Children, vol. 10, no. 9, Sep. 2023. [CrossRef]
- B. D. Katzman, C. B. van der Pol, P. Soyer, and M. N. Patlas, “Artificial intelligence in emergency radiology: A review of applications and possibilities,” Jan. 01, 2023, Elsevier Masson s.r.l. [CrossRef]
- K. Piliuk and S. Tomforde, “Artificial intelligence in emergency medicine. A systematic literature review,” Int J Med Inform, vol. 180, p. 105274, Dec. 2023. [CrossRef]
- M. Jordan, J. Hauser, S. Cota, H. Li, and L. Wolf, “The Impact of Cultural Embeddedness on the Implementation of an Artificial Intelligence Program at Triage: A Qualitative Study,” Journal of Transcultural Nursing, vol. 34, no. 1, pp. 32–39, Jan. 2023. [CrossRef]
- J. Talevski et al., “From concept to reality: A comprehensive exploration into the development and evolution of a virtual emergency department,” JACEP Open, vol. 5, no. 4, Aug. 2024. [CrossRef]
- Y. M. Arabi, A. A. Al Ghamdi, M. Al-Moamary, A. Al Mutrafy, R. H. AlHazme, and B. A. Al Knawy, “Electronic medical record implementation in a large healthcare system from a leadership perspective,” BMC Med Inform Decis Mak, vol. 22, no. 1, Dec. 2022. [CrossRef]
- R. B. D. Laig and F. T. Abocejo, “Change Management Process in a Mining Company: Kotter’s 8-Step Change Model,” Journal of Management, Economics, and Industrial Organization, pp. 31–50, Sep. 2021. [CrossRef]
- F. A. Memon, S. Shah, and U. Khoso, “IMPROVING EMPLOYEE’S ENGAGEMENT IN CHANGE: REASSESSING KURT LEWIN’S MODEL,” 2021. [Online]. Available: http://cusitjournals.com/index.php/CURJ.
- M. A. Kilby, “Creating Good Jobs in Automotive Manufacturing,” 2021.
- G. K. Gouda and B. Tiwari, “Talent agility, innovation adoption and sustainable business performance: empirical evidences from Indian automobile industry,” International Journal of Productivity and Performance Management, vol. 71, no. 6, pp. 2582–2604, Jun. 2022. [CrossRef]
- Uday Krishna Padyana, Hitesh Premshankar Rai, Pavan Ogeti, Narendra Sharad Fadnavis, and Gireesh Bhaulal Patil, “Server less Architectures in Cloud Computing: Evaluating Benefits and Drawbacks,” Innovative Research Thoughts, vol. 6, no. 3, pp. 1–12, Aug. 2024. [CrossRef]
- O. Ghandour, S. El Kafhali, and M. Hanini, “Computing Resources Scalability Performance Analysis in Cloud Computing Data Center,” J Grid Comput, vol. 21, no. 4, Dec. 2023. [CrossRef]
- P. Ullagaddi, “From Barista to Bytes: How Starbucks Brewed a Digital Revolution,” Journal of Economics, Management and Trade, vol. 30, no. 9, pp. 78–89, Sep. 2024. [CrossRef]
- F. Mızrak, “Effective Change Management Strategies,” in Perspectives on Artificial Intelligence in Times of Turbulence: Theoretical Background to Applications, IGI Global, 2023, pp. 135–162. [CrossRef]
- B. Moesl et al., “Towards a More Socially Sustainable Advanced Pilot Training by Integrating Wearable Augmented Reality Devices,” Sustainability (Switzerland), vol. 14, no. 4, Feb. 2022. [CrossRef]
Figure 1.
PRISMA flow diagram
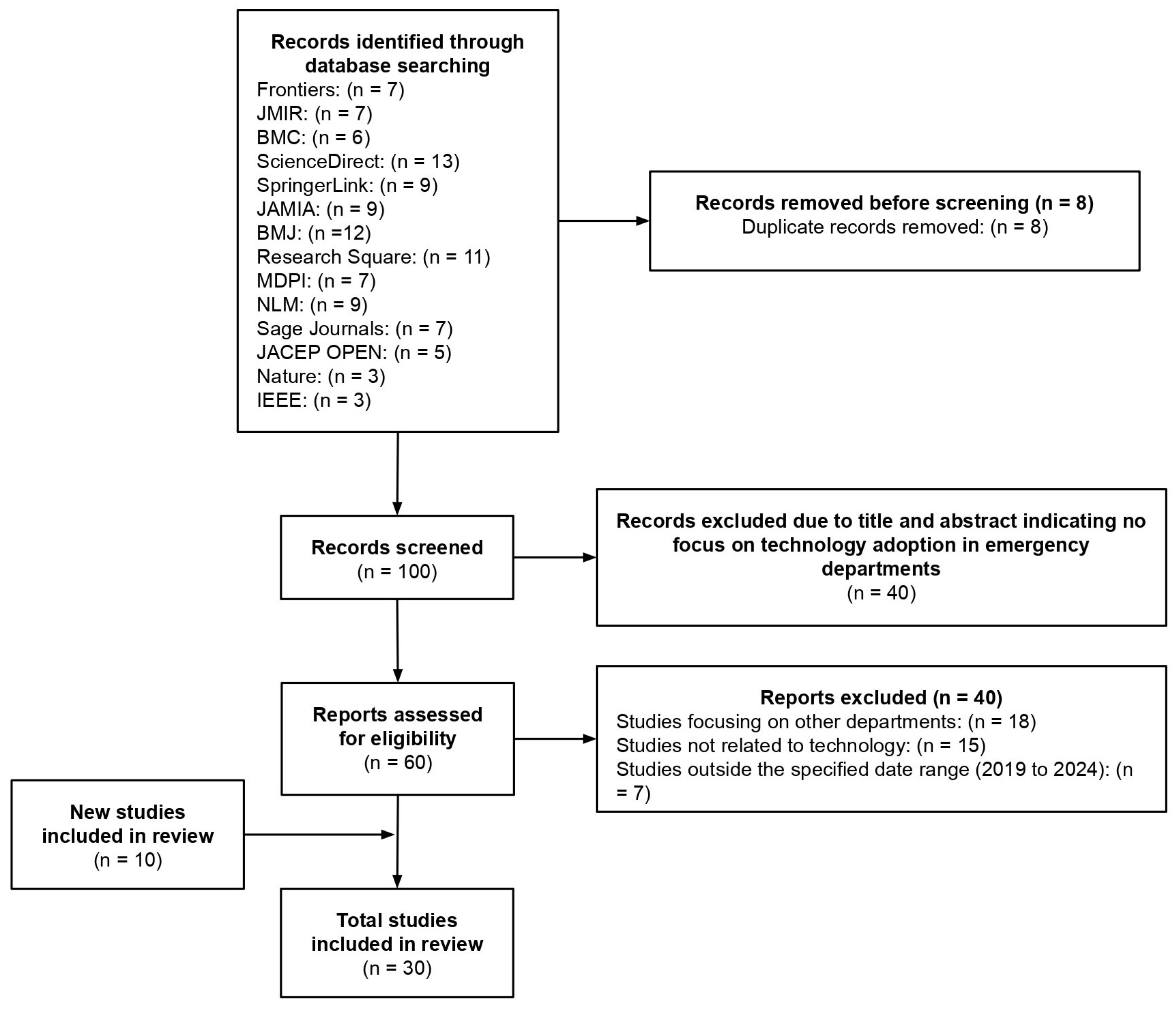

Table 1.
Reviewed Studies
| Author | Topic | Participants | Sample Size |
|---|---|---|---|
| Hall et al. (2022) [21] | Designs, facilitators, barriers, and lessons learned during the implementation of emergency department led virtual urgent care programs in Ontario, Canada | 13 emergency medicine physicians and researchers with experience in leading and implementing local VUC programs | 7 out of 14 VUC pilot programs across Ontario |
| Fujimori et al. (2022) [22] | Acceptance, Barriers, and Facilitators to Implementing Artificial Intelligence–Based Decision Support Systems in Emergency Departments: Quantitative and Qualitative Evaluation | 14 physicians from two community, tertiary care hospitals in Japan | Data from 27,550 emergency department patients from a tertiary care hospital in Japan |
| |||
| Anaraki et al. (2024) [12] | A qualitative study of the barriers and facilitators impacting the implementation of a quality improvement program for emergency departments: SurgeCon | Physicians, nurses, managers, patient care facilitators, program coordinators and patients | 31 clinicians and 341 patients were surveyed via telephone |
| Huilgol et al. (2024) [23] | Innovation adoption, use and implementation in emergency departments during the COVID-19 pandemic | Healthcare professionals from 8 hospital-based emergency departments in the United States | 49 healthcare professionals |
| |||
| Zachrison et al. (2020) [24] | Understanding Barriers to Telemedicine Implementation in Rural Emergency Departments | Rural Emergency Departments (EDs) in the United States |
|
| Boyle et al. (2023) [25] | Hospital-Level Implementation Barriers, Facilitators, and Willingness to Use a New Regional Disaster Teleconsultation System: Cross-Sectional Survey Study | Emergency managers from hospital-based and freestanding emergency departments (EDs) in New England states | 189 hospitals and EDs were identified, with 164 (87%) responding to the survey |
| Pu et al. (2024) [26] | Virtual emergency care in Victoria: Stakeholder perspectives of strengths, weaknesses, and barriers and facilitators of service scale-up | Emergency medicine physicians, health care consumers, other health care professionals, including residential aged care facility staff members and general practitioners | 20 participants:
|
| Antor et al. (2024) [27] | Usability evaluation of electronic health records at the trauma and emergency directorates at the Komfo Anokye teaching hospital in the Ashanti region of Ghana | Trauma and emergency department staff members at Komfo Anokye Teaching Hospital. | 234 trauma and emergency department staff members at Komfo Anokye Teaching Hospital |
| Bhosekar et al. (2023) [28] | An Exploratory Study to Evaluate the Technological Barriers and Facilitators for Pediatric Behavioral Healthcare in Emergency Departments | Assistant nurse manager, charge nurse, security accounts manager, and patient safety specialist | 4 healthcare providers across two hospitals |
| Hodwitz et al. (2024) [29] | Healthcare workers’ perspectives on a prescription phone program to meet the health equity needs of patients in the emergency department: a qualitative study | Healthcare workers | 12 interviews |
| Nataliansyah et al. (2022) [30] | Managing innovation: a qualitative study on the implementation of telehealth services in rural emergency departments | 18 key informants from six U.S. healthcare systems (hub sites) | 65 rural emergency departments (spoke sites) across 11 U.S. states |
| Kennedy et al. (2024) [31] | Establishing enablers and barriers to implementing the HIRAID® emergency nursing framework in rural emergency departments | Emergency nurses from 11 rural, regional emergency departments in Southern New South Wales, Australia | 102 nurses completed the survey |
| Moy et al. (2023) [32] | Understanding the perceived role of electronic health records and workflow fragmentation on clinician documentation burden in emergency departments | Physicians and registered nurses | 24 responses:
|
| Uscher-Pines et al. (2021) [33] | Rising to the challenges of the pandemic: Telehealth innovations in U.S. emergency departments | 15 emergency department leaders from 14 institutions across 10 states in the United States | A total of 35 individuals were invited to participate, resulting in a response rate of 43% |
| Wong et al. (2024) [34] | Formative evaluation of an emergency department clinical decision support system for agitation symptoms: a study protocol | Emergency department physicians, nurses, technicians, and patients with lived experience of restraint use during an emergency department visit |
|
| Barton et al. (2024) [35] | Academic Detailing as a Health Information Technology Implementation Method: Supporting the Design and Implementation of an Emergency Department–Based Clinical Decision Support Tool to Prevent Future Falls | Emergency medicine resident physicians and advanced practice providers | 16 participants (10 resident physicians and 6 advanced practice providers) |
| Billah et al. (2022) [36] | Clinicians' perspectives on the implementation of patient decision aids in the emergency department: A qualitative interview study | Emergency clinicians, including attending physicians, resident physicians, and physician assistants | 20 emergency clinicians |
| Davison et al. (2024) [37] | Barriers and facilitators to implementing psychosocial digital health interventions for older adults presenting to emergency departments: a scoping review protocol | The scoping review will consider articles that include older adults (70 years and older) who have received care in an emergency department setting, as well as other stakeholders such as patient families, clinical staff, and other hospital staff involved in the care of older adults in EDs | The review will include both qualitative and quantitative studies, but the exact sample size will depend on the studies identified and included in the review |
| Salwei et al. (2022) [38] | Usability barriers and facilitators of a human factors engineering-based clinical decision support technology for diagnosing pulmonary embolism | Emergency medicine physicians | 32 emergency medicine physicians:
|
| Simpson et al. (2023) [39] | Implementation strategies to address the determinants of adoption, implementation, and maintenance of a clinical decision support tool for emergency department buprenorphine initiation: a qualitative study | Clinicians from five different healthcare systems, including:
|
28 interviews |
| Shin et al. (2024) [40] | Barriers and Facilitators to Using an App-Based Tool for Suicide Safety Planning in a Psychiatric Emergency Department: A Qualitative Descriptive Study Using the Theoretical Domains Framework and COM-B Model | Nurses, psychiatrists, social workers, program assistants, and chemists | 29 emergency department professionals |
| Shuldiner et al. (2023) [41] | The Implementation of a Virtual Emergency Department: Multimethods Study Guided by the RE-AIM (Reach, Effectiveness, Adoption, Implementation, and Maintenance) Framework | Patients utilizing the virtual emergency department (VED) and medical specialists | Average of 153 visits per month |
| Sharifi Kia et al. (2023) [42] | Telemedicine in the emergency department: an overview of systematic reviews | Review-based study | Analysis of 18 studies (not direct participant data) |
| Hose et al. (2023) [43] | Work system barriers and facilitators of a team health information technology | Professionals from 12 different healthcare disciplines | 36 healthcare workers |
| Tyler et al. (2024) [44] | Use of Artificial Intelligence in Triage in Hospital Emergency Departments: A Scoping Review | Review-based study | 29 publications selected from an initial 1142 reviewed |
| Hudson et al. (2023) [45] | Perspectives of Healthcare Providers to Inform the Design of an AI-Enhanced Social Robot in the Pediatric Emergency Department | Medical professionals from 2 paediatric emergency departments in Canada | 11 medical professionals |
| Katzman et al. (2023) [46] | Artificial intelligence in emergency radiology: A review of applications and possibilities | Review-based study | 44 studies reviewed |
| Piliuk and Tomforde (2023) [47] | Artificial intelligence in emergency medicine. A systematic literature review | Review-based study | 116 studies reviewed |
| Jordan et al. (2023) [48] | The Impact of Cultural Embeddedness on the Implementation of an Artificial Intelligence Program at Triage: A Qualitative Study | Triage nurses in a community hospital’s emergency department in the United States | 13 triage nurses |
| Talevski et al. (2024) [49] | From concept to reality: A comprehensive exploration into the development and evolution of a virtual emergency department | Patients using the Victorian Virtual Emergency Department in Victoria, Australia | 500 patients who used the VVED service |
Table 2.
Summary of Studies
| Author | Topic | Barriers | Facilitators |
|---|---|---|---|
| Hall et al. (2022) [21] | Designs, facilitators, barriers, and lessons learned during the implementation of emergency department led virtual urgent care programs in Ontario, Canada |
|
|
| Fujimori et al. (2022) [22] | Acceptance, Barriers, and Facilitators to Implementing Artificial Intelligence–Based Decision Support Systems in Emergency Departments: Quantitative and Qualitative Evaluation |
|
|
| Anaraki et al. (2024) [12] | A qualitative study of the barriers and facilitators impacting the implementation of a quality improvement program for emergency departments: SurgeCon |
|
|
| Huilgol et al. (2024) [23] | Innovation adoption, use and implementation in emergency departments during the COVID-19 pandemic |
|
|
| Zachrison et al. (2020) [24] | Understanding Barriers to Telemedicine Implementation in Rural Emergency Departments |
|
|
| Boyle et al. (2023) [25] | Hospital-Level Implementation Barriers, Facilitators, and Willingness to Use a New Regional Disaster Teleconsultation System: Cross-Sectional Survey Study |
|
|
| Pu et al. (2024) [26] | Virtual emergency care in Victoria: Stakeholder perspectives of strengths, weaknesses, and barriers and facilitators of service scale-up |
|
|
| Antor et al. (2024) [27] | Usability evaluation of electronic health records at the trauma and emergency directorates at the Komfo Anokye teaching hospital in the Ashanti region of Ghana |
|
|
| Bhosekar et al. (2023) [28] | An Exploratory Study to Evaluate the Technological Barriers and Facilitators for Pediatric Behavioral Healthcare in Emergency Departments |
|
|
| Hodwitz et al. (2024) [29] | Healthcare workers’ perspectives on a prescription phone program to meet the health equity needs of patients in the emergency department: a qualitative study |
|
|
| Nataliansyah et al. (2022) [30] | Managing innovation: a qualitative study on the implementation of telehealth services in rural emergency departments |
|
|
| Kennedy et al. (2024) [31] | Establishing enablers and barriers to implementing the HIRAID® emergency nursing framework in rural emergency departments |
|
|
| Moy et al. (2023) [32] | Understanding the perceived role of electronic health records and workflow fragmentation on clinician documentation burden in emergency departments |
|
|
| Uscher-Pines et al. (2021) [33] | Rising to the challenges of the pandemic: Telehealth innovations in U.S. emergency departments |
|
|
| Wong et al. (2024) [34] | Formative evaluation of an emergency department clinical decision support system for agitation symptoms: a study protocol |
|
|
| Barton et al. (2024) [35] | Academic Detailing as a Health Information Technology Implementation Method: Supporting the Design and Implementation of an Emergency Department–Based Clinical Decision Support Tool to Prevent Future Falls |
|
|
| Billah et al. (2022) [36] | Clinicians' perspectives on the implementation of patient decision aids in the emergency department: A qualitative interview study |
|
|
| Davison et al. (2024) [37] | Barriers and facilitators to implementing psychosocial digital health interventions for older adults presenting to emergency departments: a scoping review protocol |
|
|
| Salwei et al. (2022) [38] | Usability barriers and facilitators of a human factors engineering-based clinical decision support technology for diagnosing pulmonary embolism |
|
|
| Simpson et al. (2023) [39] | Implementation strategies to address the determinants of adoption, implementation, and maintenance of a clinical decision support tool for emergency department buprenorphine initiation: a qualitative study |
|
|
| Shin et al. (2024) [40] | Barriers and Facilitators to Using an App-Based Tool for Suicide Safety Planning in a Psychiatric Emergency Department: A Qualitative Descriptive Study Using the Theoretical Domains Framework and COM-B Model |
|
|
| Shuldiner et al. (2023) [41] | The Implementation of a Virtual Emergency Department: Multimethods Study Guided by the RE-AIM (Reach, Effectiveness, Adoption, Implementation, and Maintenance) Framework |
|
|
| Sharifi Kia et al. (2023) [42] | Telemedicine in the emergency department: an overview of systematic reviews |
|
- |
| Hose et al. (2023) [43] | Work system barriers and facilitators of a team health information technology |
|
|
| Tyler et al. (2024) [44] | Use of Artificial Intelligence in Triage in Hospital Emergency Departments: A Scoping Review |
|
- |
| Hudson et al. (2023) [45] | Perspectives of Healthcare Providers to Inform the Design of an AI-Enhanced Social Robot in the Pediatric Emergency Department |
|
|
| Katzman et al. (2023) [46] | Artificial intelligence in emergency radiology: A review of applications and possibilities |
|
|
| Piliuk and Tomforde (2023) [47] | Artificial intelligence in emergency medicine. A systematic literature review |
|
- |
| Jordan et al. (2023) [48] | The Impact of Cultural Embeddedness on the Implementation of an Artificial Intelligence Program at Triage: A Qualitative Study |
|
|
| Talevski et al. (2024) [49] | From concept to reality: A comprehensive exploration into the development and evolution of a virtual emergency department |
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



