
Submitted:
28 January 2025
Posted:
28 January 2025
You are already at the latest version
Abstract
Background. Breast cancer (BC) is the most prevalent neoplasm in the female gender, being also the leading cause of mortality in women worldwide. In Latin American countries such as Mexico, locally advanced and metastatic stages remain prevalent at the time of diagnosis. Factors involved in the progression of BC are highly interdependent elements, where non-modifiable risk factors, such as premenopausal and menopause play a significant role in BC prognosis[SG1] .Methods. Retrospective cohort study that analyzed clinicopathological variables of 292 cases of BC evaluating individual risk within premenopausal and postmenopausal women and probability of survival with a 5-year median follow-up.Results. Our results showed that overall survival (OS) rate for premenopausal and postmenopausal women at 5-years was 88.1% and 92.6%, respectively. Premenopausal showed over 3.6-fold increased risk of recurrence at early stages (p=0.0003), and decreased OS associated to larger tumors (>2 cm) (p=0.0290; HR 4.54; 95%CI 1.58-13.07). In postmenopausal women, we observed a significant effect on OS associated to negative estrogen receptor (ER–) status tumors (p=0.0014; HR 3.71; 95%CI 1.21-11.39), and Triple Negative (TN) subtype (p=0.0021; HR 4.72; 95%CI 1.05-21.28). These findings show differences between cohorts and briefly informs prognosis by menopausal status in a Mexican population-based study, in hopes of improved prevention and detection programmes.
Keywords:
Breast cancer
; risk factors
; prognosis
; survival
1. Introduction
Breast cancer (BC) is the most prevalent neoplasm in women, with an estimated global incidence in 2020 of 2,261,419 cases [1], being also the leading cause of mortality in women worldwide. BC prognosis associates to risk factors within the clinical context of patients as well as tumor related features [2,3], which are highly interdependent elements. Non-modifiable risk factors, such as endocrine environment related to menopausal status play a leading role in prognosis [4], linked to biological features of the tumor and progression of cancer [5]. In Mexico, most cases represent locally advanced and metastatic stages at the time of diagnosis [6,7], whereas younger women are diagnosed with BC [8,9,10] compared to developed countries [11].
2. Materials and Methods
2.1. Study population
The present retrospective cohort study was carried out with clinicopathological information from female patients affiliated to the Regional General Hospital No. 1 (HGR1) of the IMSS and the State Center for Oncology Care (CEOM) in Morelia, Mexico, following the approval by the local ethical committee of both institutions. Of a total of 1883 patients initially retrieved from January 2015 to December 2017, only 292 primary breast cancer patients met our inclusion criteria for the present study.
2.2. Clinicopathological variables
Patients’ demographic information was retrieved from clinical records. We defined the Estrogenic Index (EI) as the years of endogenous estrogen exposure [12]. We categorized our population according to menopausal status; as well as TNM prognostic stage groups [13], histological grade [14,15], and molecular subtypes guidelines [6,16]. Overall survival (OS) was defined as the time from the initial diagnosis to the date of follow-up cutoff. Patients who were lost to follow-up were considered as censored data in the analysis. The median follow-up was 5 years.
2.3. Statistical analysis
Data processing and comparisons test were performed using GraphPad Prism version 9.1.1, GraphPad Software, San Diego, California USA. Pearson's χ2 test was used for bivariate analysis considering p<0.05 as statistically significant. Relative risk and hazard ratios were calculated with 95% confidence intervals. Survival curves were calculated using the Kaplan-Meier method, significance was evaluated with Mantel-Cox log-rank test.
3. Results
3.1. Overall clinicopathologic characteristics
The mean age of diagnosis was 53.5 years; mainly overweight and obese (BMI >25 kg/m2) patients (78.4%; 229/292). Most patients (61.3%) were postmenopausal at the time of diagnosis (Table I).
3.2. Overall survival
During the median observation time of 64 months, 23.6% (69/292) of patients had evidence of recurrence/metastasis, 8.9% (26/292) patients died of breast cancer (BC) related causes. The overall survival (OS) rate of premenopausal and postmenopausal women at 5-years was 88.1% and 92.6%, respectively. The lung was the most common site of metastasis (23 cases), followed by bone (21 cases) (Figure 1).
Significant associations in premenopausal and postmenopausal patients’ OS are enlisted in Table II.
3.3. Decreased OS associated to premenopausal women with larger tumors, and postmenopausal women with ER– and TN tumors.
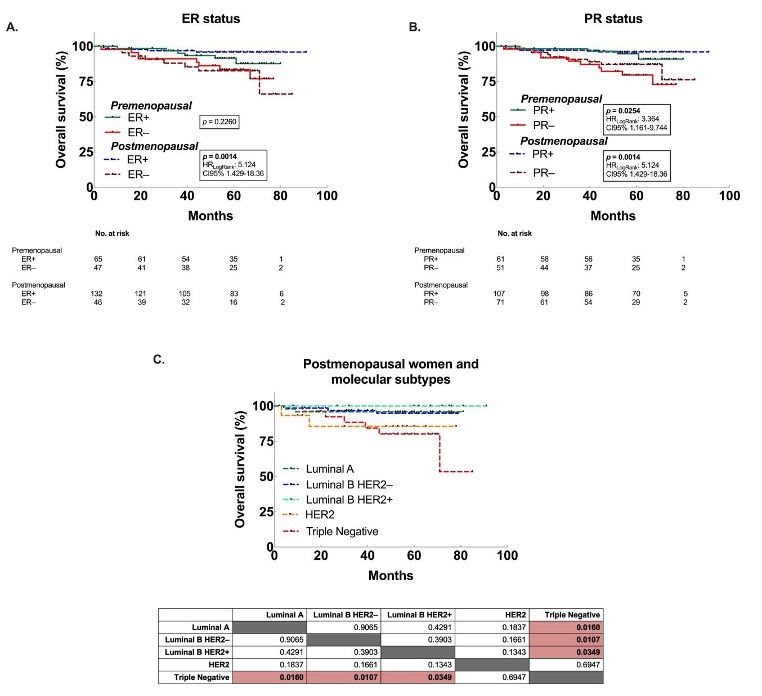
Premenopausal women showed diminished OS when presenting larger tumors (>2 cm), lymph nodes metastasis and progesterone receptor (PR) status. As seen in premenopausal women, postmenopausal presented diminished survival associated to nodules and PR status; nevertheless, estrogen receptor (ER) status had a significant effect on OS (p=0.0014) as well as Triple Negative (TN) tumors, not shared by their counterparts. Along with these findings, recurrence conditioned OS in both cohorts (p<0.0001) (Figure 2).
4. Discussion
Menopausal status represents a non-modifiable risk factor for breast cancer (BC) prognosis [17], due to hormonal and molecular traits between premenopausal and postmenopausal population. Most BC cases are diagnosed in older women [18], in our study the mean age of diagnosis was 53.5 years, similar to previous reports in Mexican population [8,9,10], with 13.7% of cases identified at young ages (<40 years), a higher incidence than developed countries [19]; furthermore, premenopausal women showed over 3.6-fold increased risk of recurrence at early stages, and poor outcome in younger women [20]. Molecular subtypes have different age–incidence profiles at the time of menopause [21]; in our study, postmenopausal women with Triple Negative (TN) subtype tumor showed a significantly lower OS. ER+ status was significantly higher in postmenopausal women, which correlates to previous findings [22].
Numerous studies have indicated that obesity is a risk factor for breast cancer, especially in postmenopausal women [23], however, this association was not found in our study. Menopausal status had no direct impact in overall survival [24], which can be attributed to advances in treatment, early diagnosis at all ages, and mammography screening.
5. Conclusions
Lymph node metastases, PR status and recurrence showed significant effect on OS in both cohorts, while larger tumor size represented a significant effect on overall survival of premenopausal women, and ER status and TN represented significant effect on OS of postmenopausal women. Body mass index and HER2 status association was not significant with OS. These findings underline the need to investigate the breast cancer burden in Mexican population-based studies by menopausal status to inform prognosis, prevention, and improved detection programs.
Author Contributions
A.G.R.-L. conceived of and coordinated the project, designed the study, wrote the paper and collected clinical data; A.G.-G. analyzed the data, prepared the figures, and contributed to writing the paper; G.S.-C. made statistical analyses and helped in the writing of the paper; M.M.-A. assisted with the immunohistochemistry experiments and carried out the bioinformatic analysis; S.G.-C. and. collected samples, clinical data, and identified tumor areas; A.G.-G, and S.G.S-C. also conducted statistical analyses; S.H.-Y and S.G.-C. contributed to project coordination; All authors have read and agreed to the published version of the manuscript.
Funding
This work was funded by grant from the Instituto Mexicano del Seguro Social (Residency Fellowship of A.G.R-L.) recipient of a Medical Specialty’s degree from UNAM/CONACyT, CVU: 1030352.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (that included Ethics Committee) Registration Number: R-2022-1602-025
Informed Consent Statement
Not applicable, we used tissue samples left from routine diagnostic of the patients.
Acknowledgments
This research was able to the work team that made this study possible, with special mention to the Department of Pathological Anatomy of the HGR1.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Ferlay J, Colombet M, Soerjomataram I, Parkin DM, Piñeros M, Znaor A, et al. Cancer statistics for the year 2020: An overview. Int J Cancer. 2021. [CrossRef]
- Harris LN, Ismaila N, McShane LM, Andre F, Collyar DE, Gonzalez-Angulo AM, et al. Use of Biomarkers to Guide Decisions on Adjuvant Systemic Therapy for Women With Early-Stage Invasive Breast Cancer: American Society of Clinical Oncology Clinical Practice Guideline. J Clin Oncol. 2016;34(10):1134-50. [CrossRef]
- Weigel MT, Dowsett M. Current and emerging biomarkers in breast cancer: prognosis and prediction. Endocrine-Related Cancer. 2010;17(4):R245-R62. [CrossRef]
- Łukasiewicz S, Czeczelewski M, Forma A, Baj J, Sitarz R, Stanisławek A. Breast Cancer—Epidemiology, Risk Factors, Classification, Prognostic Markers, and Current Treatment Strategies—An Updated Review. Cancers. 2021;13(17):4287. [CrossRef]
- Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell. 2011;144(5):646-74. [CrossRef]
- Cárdenas-Sánchez J, Valle-Solís AA, Arce-Salinas C, Bargalló-Rocha JE, Bautista-Piña V, Cervantes-Sánchez MG, et al. Consenso Mexicano sobre diagnóstico y tratamiento del cáncer mamario. 9 ed. Colima, México. 2021. 233 p.
- Justo N, Wilking N, Jönsson B, Luciani S, Cazap E. A Review of Breast Cancer Care and Outcomes in Latin America. The Oncologist. 2013;18(3):248-56. [CrossRef]
- Reynoso-Noverón N, Villarreal-Garza C, Soto-Perez-De-Celis E, Arce-Salinas C, Matus-Santos J, Ramírez-Ugalde MT, et al. Clinical and Epidemiological Profile of Breast Cancer in Mexico: Results of the Seguro Popular. Journal of Global Oncology. 2017;3(6):757-64. [CrossRef]
- Hortobagyi GN, de la Garza Salazar J, Pritchard K, Amadori D, Haidinger R, Hudis CA, et al. The global breast cancer burden: variations in epidemiology and survival. Clin Breast Cancer. 2005;6(5):391-401. [CrossRef]
- Flores-Diaz D, Arce C, Flores-Luna L, Reynoso-Noveron N, Lara-Medina F, Matus JA, et al. Impact of invasive lobular carcinoma on long-term outcomes in Mexican breast cancer patients. Breast Cancer Res Treat. 2019;176(1):243-9. [CrossRef]
- Howlader N, Noone AM, Krapcho M, Miller D, Brest A, Yu M RJ, Tatalovich Z, Mariotto A, Lewis DR, Chen HS, Feuer EJ, Cronin KA (eds). SEER Cancer Statistics Review, 1975-2018, National Cancer Institute. Bethesda, MD, , based on November 2020 SEER data submission, posted to the SEER web site, April 2021. SEER Cancer Statistics Review, 1975-2018. National Cancer Institute; 2021.
- Rojas-Lima E, Gamboa-Loira B, Cebrián ME, Rothenberg SJ, López-Carrillo L. A cumulative index of exposure to endogenous estrogens and breast cancer by molecular subtypes in northern Mexican women. Breast Cancer Research and Treatment. 2020;180(3):791-800. [CrossRef]
- Hortobagyi GN, Edge SB, Giuliano A. New and Important Changes in the TNM Staging System for Breast Cancer. Am Soc Clin Oncol Educ Book. 2018;38:457-67. [CrossRef]
- Bloom HJ, Richardson WW. Histological grading and prognosis in breast cancer; a study of 1409 cases of which 359 have been followed for 15 years. Br J Cancer. 1957;11(3):359-77. [CrossRef]
- Elston CW, Ellis IO. Pathological prognostic factors in breast cancer. I. The value of histological grade in breast cancer: experience from a large study with long-term follow-up. Histopathology. 1991;19(5):403-10. [CrossRef]
- Allison KH, Hammond MEH, Dowsett M, McKernin SE, Carey LA, Fitzgibbons PL, et al. Estrogen and Progesterone Receptor Testing in Breast Cancer: American Society of Clinical Oncology/College of American Pathologists Guideline Update. Arch Pathol Lab Med. 2020;144(5):545-63. [CrossRef]
- Lao C, Elwood M, Kuper-Hommel M, Campbell I, Lawrenson R. Impact of menopausal status on risk of metastatic recurrence of breast cancer. Menopause. 2021;28(10):1085-92. [CrossRef]
- Benz CC. Impact of aging on the biology of breast cancer. Crit Rev Oncol Hematol. 2008;66(1):65-74. [CrossRef]
- Nasim Z, Girtain C, Gupta V, Patel I, Hossain MA. Breast Cancer Incidence and Behavior in Younger Patients: A Study From the Surveillance, Epidemiology and End Results Database. World Journal of Oncology. 2020;11(3):88-97. [CrossRef]
- Dubsky PC, Gnant MF, Taucher S, Roka S, Kandioler D, Pichler-Gebhard B, et al. Young age as an independent adverse prognostic factor in premenopausal patients with breast cancer. Clin Breast Cancer. 2002;3(1):65-72. [CrossRef]
- Anderson WF, Rosenberg PS, Prat A, Perou CM, Sherman ME. How many etiological subtypes of breast cancer: two, three, four, or more? J Natl Cancer Inst. 2014;106(8). [CrossRef]
- Barnes BB, Steindorf K, Hein R, Flesch-Janys D, Chang-Claude J. Population attributable risk of invasive postmenopausal breast cancer and breast cancer subtypes for modifiable and non-modifiable risk factors. Cancer Epidemiol. 2011;35(4):345-52. [CrossRef]
- Rose DP, Komninou D, Stephenson GD. Obesity, adipocytokines, and insulin resistance in breast cancer. Obes Rev. 2004;5(3):153-65. [CrossRef]
- Mahmood H, Faheem M, Mahmood S, Sadiq M, Irfan J. Impact of age, tumor size, lymph node metastasis, stage, receptor status and menopausal status on overall survival of breast cancer patients in Pakistan. Asian Pac J Cancer Prev. 2015;16(3):1019-24. [CrossRef]
Figure 1.
Kaplan-Meier estimates of percent overall survival in premenopausal and postmenopausal women in relation to (A) ER status and (B) PR status. C. Overall survival in postmenopausal women according to molecular subtypes. ER: Estrogen receptors; PR: progesterone receptors.
Figure 1.
Kaplan-Meier estimates of percent overall survival in premenopausal and postmenopausal women in relation to (A) ER status and (B) PR status. C. Overall survival in postmenopausal women according to molecular subtypes. ER: Estrogen receptors; PR: progesterone receptors.
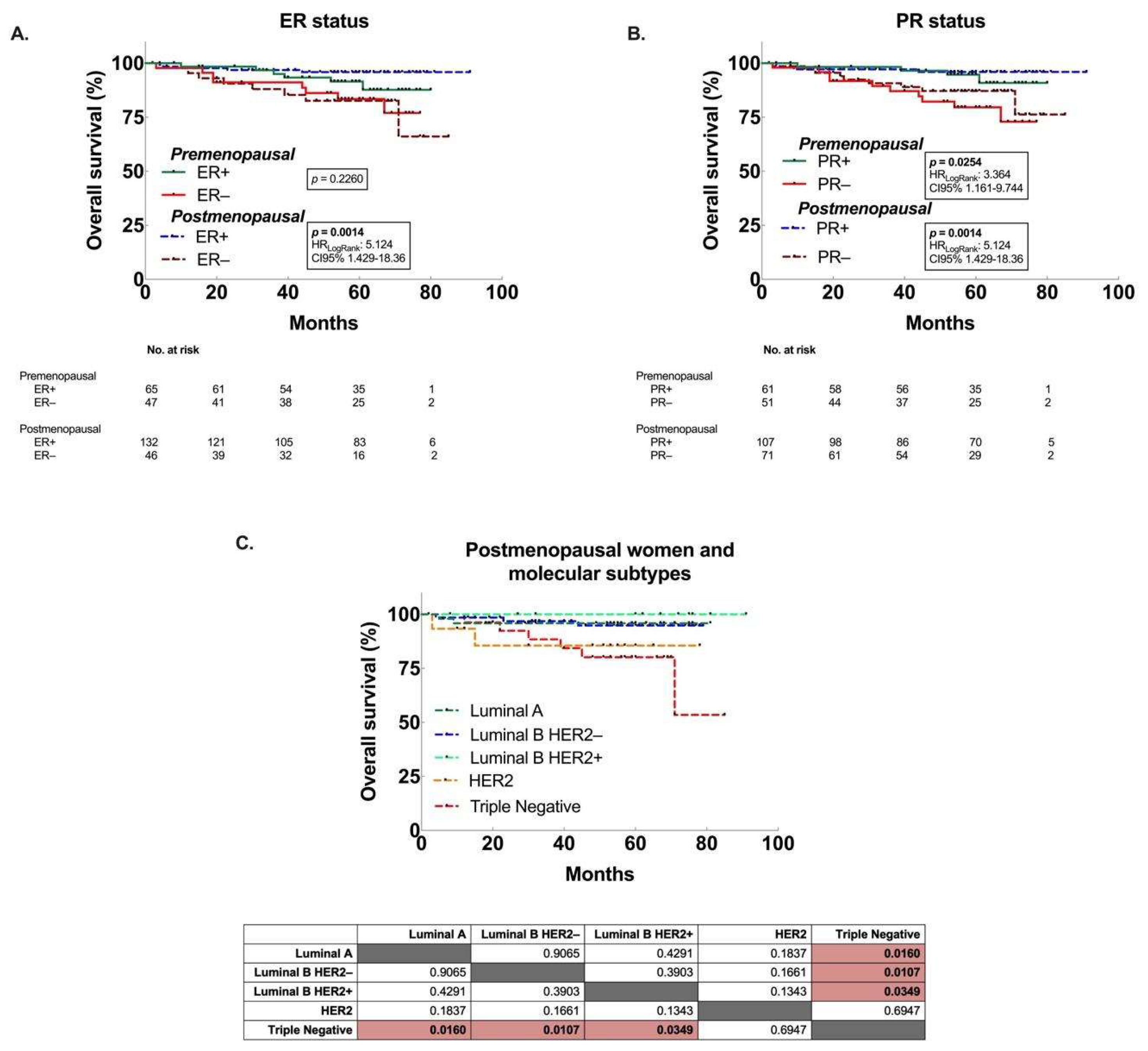
Figure 1.
Kaplan-Meier estimates of percent overall survival in premenopausal and postmenopausal women in relation to (A) tumor size (tumor dimensions of >2 vs ≤ 2 cm at major axis) (B) nodules and (C) recurrence. pN: nodules according to TNM anatomical staging.
Figure 1.
Kaplan-Meier estimates of percent overall survival in premenopausal and postmenopausal women in relation to (A) tumor size (tumor dimensions of >2 vs ≤ 2 cm at major axis) (B) nodules and (C) recurrence. pN: nodules according to TNM anatomical staging.
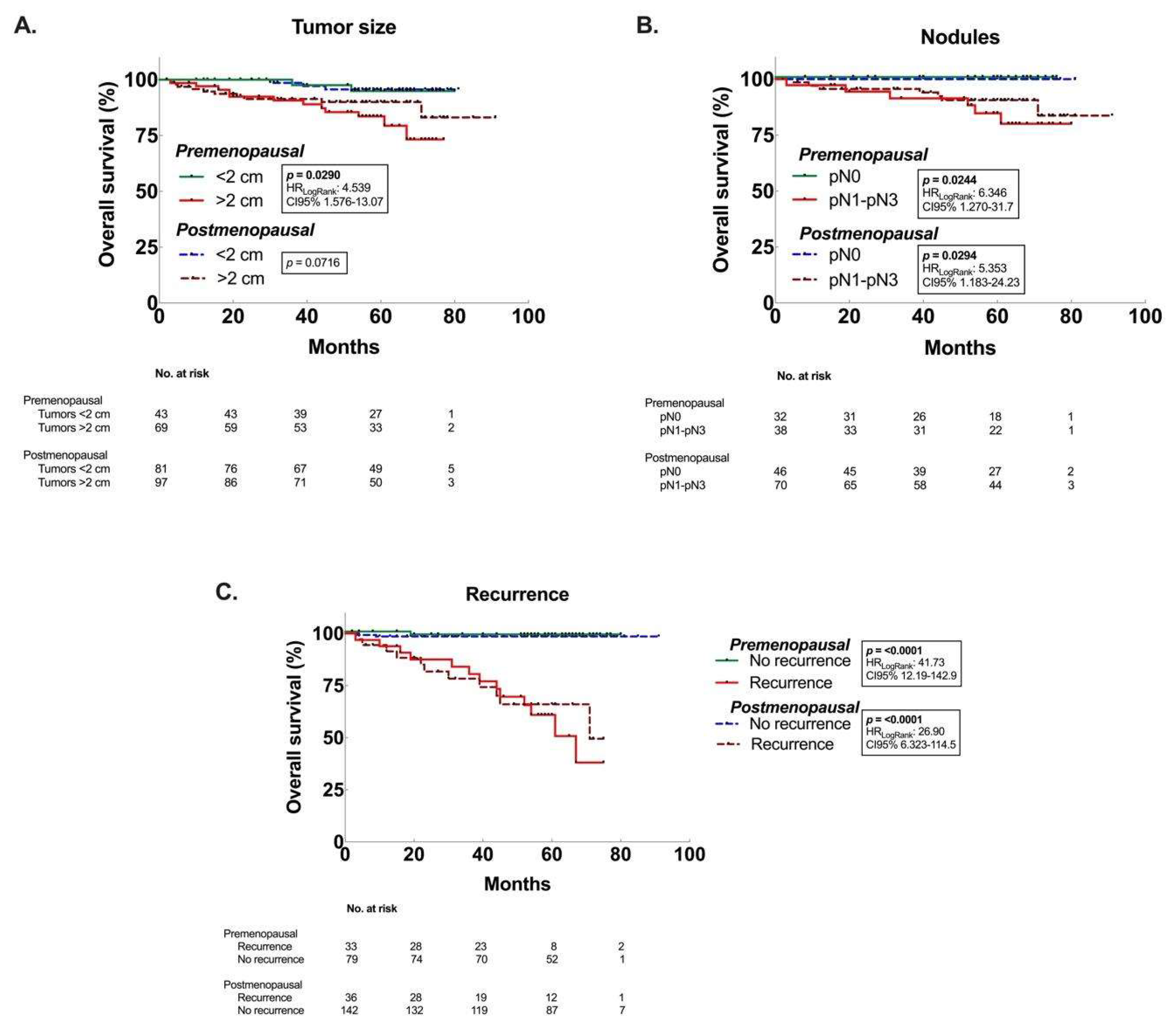

Table 1.
Demographics, baseline characteristics of the patients.
| Variable | Premenopausal n/% |
Postmenopausal n/% |
p value† |
|---|---|---|---|
| No. of patients | 113/38.7 | 179/61.3 | |
| Age, year, mean (SD) | 42.9 ±5.9 | 60.2 ±9.6 | <0.0001 |
| <30 | 4/1.4 | - | - |
| 31-40 | 34/11.6 | 1/0.3 | - |
| 41-50 | 64/21.9 | 30/10.3 | - |
| 51-60 | 11/3.8 | 66/22.6 | - |
| >61 | - | 82/28.1 | |
| BMI⊥ | 28.3 ±5.4 | 29.7 ±5.6 | 0.5943 |
| <18.4 | 2/0.7 | 1/0.4 | - |
| 18.5-24.9 | 26/9.5 | 34/12.4 | - |
| 25-29.9 | 43/15.6 | 62/22.5 | - |
| 30-34.9 | 23/8.4 | 45/16.4 | - |
| 35-39.9 | 9/3.3 | 14/5.1 | - |
| >40 | 4/1.5 | 12/4.4 | - |
| Age at menarche, year, mean (SD) | 12.4 ±1.6 | 13.0 ±1.5 | 0.0665 |
| <10 | 9/4.6 | 3/1.5 | |
| 11-12 | 50/25.5 | 74/37.8 | - |
| >13 | 25/12.8 | 35/17.9 | - |
| Age at 1st gestation, year, mean (SD) | 22.0 ±5.3 | 22.2 ±5.9 | 0.8607 |
| <19 | 22/16.8 | 28/21.4 | - |
| 20-34 | 36/27.5 | 38/29.0 | - |
| >35 | 3/2.3 | 4/3.1 | - |
| Parity | - | - | 0.0015 |
| Nullipara | 18/7.9 | 26/11.5 | - |
| 1-2 | 25/11.0 | 27/11.9 | - |
| 3-4 | 39/17.2 | 38/16.7 | - |
| >5 | 10/4.4 | 44/19.4 | - |
| No. gestations | 3.2 ±1.3 | 4.4 ±2.7 | - |
| Breastfeeding, months, mean (SD) | 6.6 ±5.6 | 6.3 ±6.5 | 0.1820 |
| <6 | 24/13.1 | 46/25.1 | - |
| >6 | 50/27.3 | 63/34.4 | - |
| Age at menopause, year, mean (SD) | - | 47.2 ±5.8 | - |
| <40 | - | 18/16.1 | - |
| 41-54 | - | 86/76.8 | - |
| >55 | - | 8/7.1 | - |
| EIλ, year, mean (SD) | 28.0 ±6.5 | 30.8 ±5.6 | 0.0020 |
| Low | 30/16.0 | 16/8.6 | - |
| Medium | 39/20.9 | 55/29.4 | - |
| High | 14/7.5 | 33/17.6 | - |
| Tumor size, cm, mean (SD) | 3.7 ±3.1 | 3.3 ±2.9 | 0.2255 |
| ≤2 | 43/14.7 | 81/27.7 | - |
| >2 | 70/24.0 | 98/33.6 | - |
| pT | - | - | 0.1868 |
| pT1 | 41/14.0 | 77/26.4 | - |
| pT2 | 37/12.7 | 61/20.9 | - |
| pT3 | 15/5.1 | 11/3.8 | - |
| pT4 | 20/6.8 | 30/10.3 | - |
| No. Nodules w/ Mets | 2.7 ±4.7 | 2.7 ±3.7 | 0.8536 |
| pN0 | 32/17.2 | 46/24.7 | - |
| pN1 | 21/11.3 | 41/22.0 | - |
| pN2 | 12/6.5 | 21/11.3 | - |
| pN3 | 5/2.7 | 8/4.3 | - |
| Metastasis | - | - | 0.8191 |
| M0 | 110/37.7 | 175/59.9 | - |
| M1 | 3/1.0 | 4/1.4 | - |
| Histologic grade | - | - | 0.6485 |
| 1 | 24/8.3 | 38/13.1 | - |
| 2 | 58/20.1 | 98/33.9 | - |
| 3 | 31/10.7 | 40/13.8 | - |
| Hormone receptors | - | - | 0.0245 |
| Positive (ER+/PR+) | 55/22.3 | 106/42.9 | - |
| Negative (ER-/PR-) | 42/17.0 | 44/17.8 | - |
| Estrogen receptor | - | - | 0.0028 |
| Positive | 65/22.3 | 133/45.5 | - |
| Negative | 48/16.4 | 46/15.8 | - |
| Progesterone receptor | - | - | 0.2842 |
| Positive | 61/20.9 | 108/37.0 | - |
| Negative | 52/17.8 | 71/24.3 | - |
| Molecular subtype | - | - | 0.0397 |
| Luminal A | 28/9.9 | 50/17.6 | - |
| Luminal B | 36/12.7 | 84/29.6 | - |
| HER2 | 12/4.2 | 16/5.6 | - |
| Triple negative | 30/10.6 | 28/9.9 | - |
| Overall Survival (mo.) | 53.6 ±19.4 | 52.3 ±20.7 | 0.5928‡ (ratio 0.5354) |
| Diseased* (mo.) | 31.4 ±19.4 | 28.9 ±18.9 | 0.2768‡ (ratio 1.090) |
| Recurrence (mo.) | 22.1 ±13.4 | 29.6 ±19.0 | 0.0003‡ (ratio 3.660) |
⊥Body mass index (kg/m2); λEstrogenic index; †Chi squared test; ‡Multiple t-tests. Abbreviations: CI = confidence interval; RR = relative risk.
Table 2.
Survival in premenopausal and postmenopausal patients.
| Premenopausal, OS | Postmenopausal, OS | |||
|---|---|---|---|---|
| Variable | p value1 | HR (95%CI) | p value | HR (95%CI) |
| Premenopausal | - | - | 0.1926 | 1.64 (0.76 - 3.55) |
| Postmenopausal | 0.1926 | 0.61 (0.28 - 1.32) | - | - |
| Tumor size | ||||
| >2 cm | 0.0290 | 4.54 (1.58 - 13.07) | 0.0716 | 3.08 (1.04 - 9.14) |
| <2 cm | 0.22 (0.08 - 0.63) | 0.33 (0.11 - 0.96) | ||
| Nodules | ||||
| pN0 | 0.0244 | 0.16 (0.03 - 0.79) | 0.0294 | 0.19 (0.04 - 0.85) |
| pN1-pN3 | 6.35 (1.27 - 31.7) | 5.35 (1.18 - 24.23) | ||
| ER | ||||
| Positive | 0.2260 | 0.53 (0.18 - 1.53) | 0.0014 | 0.2 (0.05 - 0.7) |
| Negative | 1.9 (0.66 - 5.51) | 5.12 (1.43 - 18.36) | ||
| PR | ||||
| Positive | 0.0254 | 0.29 (0.1 - 0.84) | 0.0189 | 0.27 (0.09 - 0.83) |
| Negative | 3.45 (1.2 - 9.98) | 3.71 (1.21 - 11.39) | ||
| Molecular subtype | ||||
| Triple Negative | 0.1599 | 2.1 (0.64 - 6.89) | 0.0021 | 4.72 (1.05 - 21.28) |
| All subtypes | 0.48 (0.15 - 1.57) | 0.21 (0.05 - 0.96) | ||
| Recurrence | ||||
| Yes | <0.0001 | 41.73 (12.19 - 142.9) | <0.0001 | 26.9 (6.32 - 114.5) |
| No | 0.02 (0.01 - 0.08) | 0.04 (0.01 - 0.16) | ||
| 1p value calculated withMantel-Cox test (Log-Rank); OS: overall survival; HR: hazard ratio; CI: confidence interval.ER: estrogen receptors; PR: progesterone receptors. | ||||
Also
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



