Submitted:
15 January 2025
Posted:
16 January 2025
You are already at the latest version
Abstract
Background: The death of a child due to complex congenital heart disease (CCHD) in pediatric intensive care units profoundly affects families, often resulting in lasting grief and emotional distress. Despite advancements in pediatric palliative care (PPC), significant gaps persist in communication and end-of-life (EoL) planning. This study explores the experiences and perceptions of bereaved parents to identify areas for improvement in PPC delivery. Methods: A qualitative phenomenological design was used to analyze the lived experiences of 18 bereaved parents whose children died from CCHD at a tertiary cardiac center. Semi-structured telephone interviews were conducted, incorporating five open-ended questions. Data were analyzed inductively using Colaizzi’s method to identify recurring themes and subthemes. Results: Four key thematic areas emerged: communication issues, the parental role, child care, and bereavement support. Parents highlighted inconsistent communication, lack of preparedness for EoL decisions, and emotional isolation as major challenges. Positive experiences often involved compassionate healthcare providers and structured psychological support. A significant proportion of parents identified family support and faith as key coping mechanisms, while others expressed dissatisfaction with post-mortem follow-up and absence of long-term bereavement care. Conclusions: Bereaved parents’ experiences underscore the need for improved communication strategies, greater parental involvement in care, and enhanced bereavement support. Integrating structured decision-making pathways early in the care trajectory may help mitigate parental distress and improve the quality of EoL experiences for children with CCHD.
Keywords:
1. Introduction
2. Methods
2.1. Participants and Setting
2.2. Study Context
2.3. Qualitative Approach
2.4. Analytical Process
2.5. Quantitative Analysis
3. Results
3.1. Participants and Recruitment
3.2. Patient Characteristics
3.3. Parent Characteristics
3.4. Open-Ended Questions
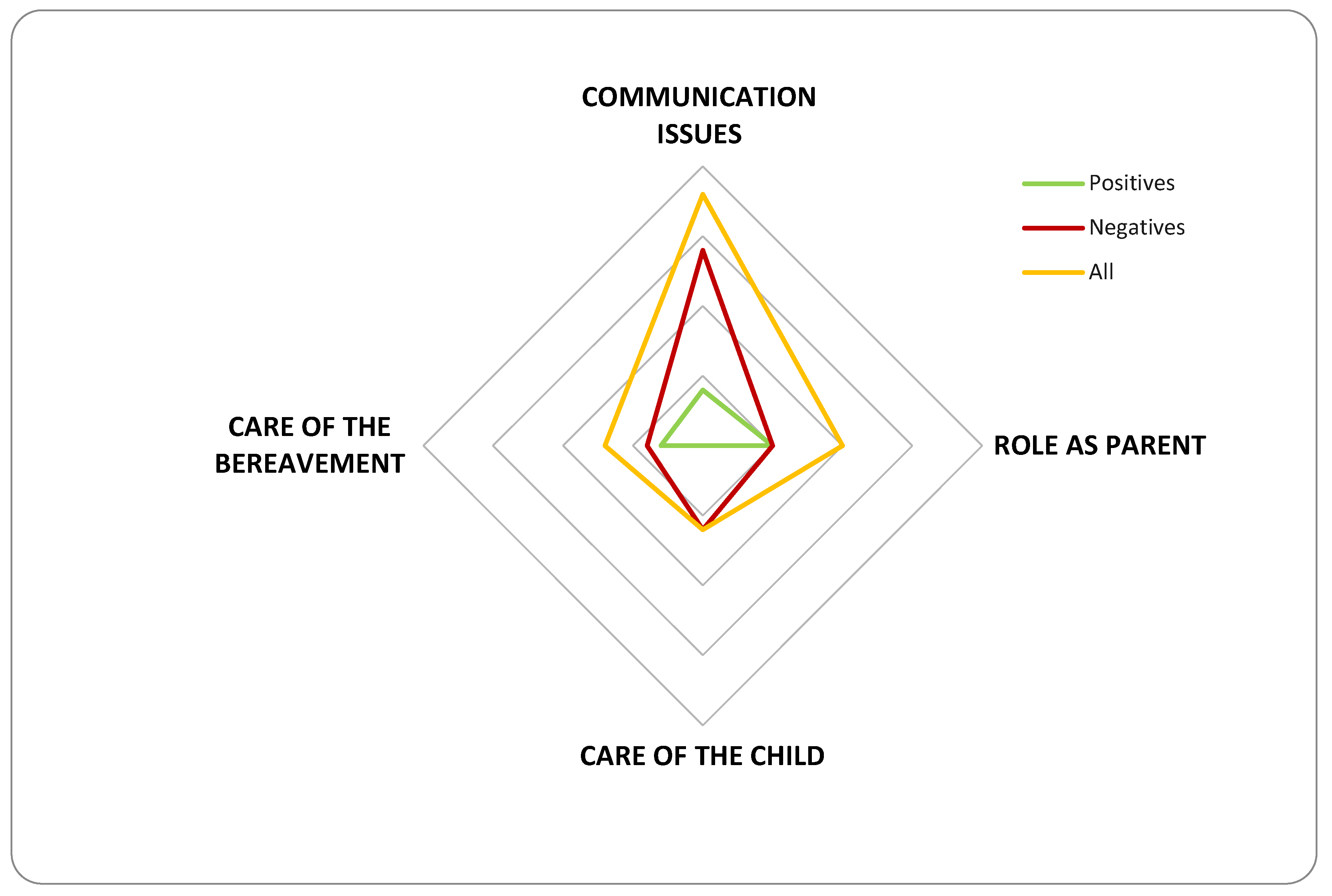
3.5. Spontaneous Comments
4. Discussion
Insights from Open-Ended Questions
Insights from Spontaneous Comments
Communication Issues
Role as a Parent
Care of the Child
Care of Bereavement
Miscellaneous
Implications for Clinical Practice
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Benini, F.; Papadatou, D.; Bernadá, M.; Craig, F.; De Zen, L.; Downing, J.; et al. International standards for pediatric palliative care: From IMPaCCT to GO-PPaCS. J Pain Symptom Manage. 2022, 63, e529-e543.
- Delgado-Corcoran, C.; Wawrzynski, S.E.; Mansfield, K.; Fuchs, E.; Yeates, C.; Flaherty, B.F.; et al. Grieving children’s death in an intensive care unit: Implementation of a standardized process. J Palliat Med. 2024, 27, 236-240. [CrossRef]
- Johnson, K.T.; Dahl, N. Paediatrics and discomfort with death and dying. Paediatr Child Health. 2023, 29, 303-305. [CrossRef]
- Blume, E.D.; Kirsch, R.; Cousino, M.K.; Walter, J.K.; Steiner, J.M.; Miller, T.A.; et al. Palliative care across the life span for children with heart disease: A scientific statement from the American Heart Association. Circ Cardiovasc Qual Outcomes. 2023, 16, e000114. [CrossRef]
- Adistie, F.; Neilson, S.; Shaw, K.L.; Bay, B.; Efstathiou, N. The elements of end-of-life care provision in paediatric intensive care units: A systematic integrative review. BMC Palliat Care. 2024, 23, 184. [CrossRef]
- Davis, S.; Nunn, M. Palliative communication in the pediatric intensive care unit. Crit Care Nurs Clin North Am. 2023, 35, 287-294. [CrossRef]
- Porteri, C.; Ienco, G.; Turla, E.M.; Petrini, C.; Pasqualetti, P. Italian law n. 219/2017 on consent and advance directives: Survey among ethics committees on their involvement and possible role. BMC Med Ethics. 2022, 23, 114.
- Bertaud, S.; Lloyd, D.F.; Laddie, J.; Razavi, R. The importance of early involvement of paediatric palliative care for patients with severe congenital heart disease. Arch Dis Child. 2016, 101, 984-987. [CrossRef]
- Agosto, C.; Benedetti, F.; De Tommasi, V.; Milanesi, O.; Stellin, G.; Padalino, M.A.; et al. End-of-life care for children with complex congenital heart disease: Parents’ and medical caregivers’ perceptions. J Paediatr Child Health. 2021, 57, 696-701.
- Baughcum, A.E.; Fortney, C.A.; Winning, A.M.; Dunnells, Z.D.O.; Humphrey, L.M.; Gerhardt, C.A. Healthcare satisfaction and unmet needs among bereaved parents in the NICU. Adv Neonatal Care. 2020, 20, 118-126. [CrossRef]
- Hasan, F.; Widger, K.; Sung, L.; Wheaton, L. End-of-life childhood cancer research: A systematic review. Pediatrics. 2021, 147, e2020003780. [CrossRef]
- Woolf-King, S.E.; Arnold, E.; Weiss, S.; Teitel, D. “There’s no acknowledgement of what this does to people”: A qualitative exploration of mental health among parents of children with critical congenital heart defects. J Clin Nurs. 2018, 27, 2785-2794.
- Krick, J.A.; Weiss, E.M.; Snyder, A.; Haldar, S.; Campelia, G.D.; Opel, D.J. Living with the unknown: A qualitative study of parental experience of prognostic uncertainty in the neonatal intensive care unit. Am J Perinatol. 2021, 38, 821-827. [CrossRef]
- Alzawad, Z.; Lewis, F.M.; Kantrowitz-Gordon, I.; Howells, A.J. A qualitative study of parents’ experiences in the pediatric intensive care unit: Riding a roller coaster. J Pediatr Nurs. 2020, 51, 8-14. [CrossRef]
- Colaizzi, P.F. Psychological research as a phenomenologist views it. In: King, R.V.M., Ed.; Existential phenomenological alternatives for psychology. New York: Oxford University Press, 1978; pp. 48–71.
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual Res Psychol. 2006, 3, 77–101.
- Verdinelli, S.; Scagnoli, N.I. Data Display in Qualitative Research. Int J Qual Methods. 2013, 12, 359–381. [CrossRef]
- Songer, K.L.; Wawrzynski, S.E.; Olson, L.M.; Harousseau, M.E.; Meeks, H.D.; Moresco, B.L.; Delgado-Corcoran, C. Timing of Palliative Care Consultation and End-of-Life Care Intensity in Pediatric Patients With Advanced Heart Disease: Single-Center, Retrospective Cohort Study, 2014-2022. Pediatr Crit Care Med. 2025, 26, e23-e32. [CrossRef]

| Question Number | Question |
|---|---|
| 1 | What was most difficult for your child? |
| 2 | What was most difficult for you as a parent? |
| 3 | Is there anything that made things easier for you during this experience? |
| 4 | What advice would you give to other parents in a similar situation? |
| 5 | What advice would you give to physicians caring for families like yours? |
| Number of Children (N = 18) | |
|---|---|
| Gender | 56% male (10/18) |
| Median Age at Death | 45 days (range: 15 days to 9 months) |
| Age at Death | 100% < 1 year |
| Median Length of Final Hospital Stay | 27 days (range: 10 to 130 days) |
| Single-Ventricle Physiology | 50% (9/18) |
| Place of Death | 94% (17/18) in CICU; 6% (1/18) in pediatric cardiology ward |
| Intubated and Sedated During EoL | 95% (17/18) |
| Receiving ECMO During EoL | 77% (14/18) |
| Cause of Death | 72% (13/18) MOF; 11% (2/18) cardiogenic shock; 11% (2/18) respiratory failure; 6% (1/18) cerebrovascular accident |
| Modes of Death | 11% (2/18) after failed CPR; 89% (16/18) after withholding treatment |
| DNR Orders | Documented in 3 cases during withholding treatment |
| Themes | Positive Comments | Negative Comments |
|---|---|---|
| Communication Issues |
|
|
| Role as Parents |
|
|
| Care of the Child |
|
|
| Care of Bereavement |
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



