Submitted:
10 January 2025
Posted:
13 January 2025
You are already at the latest version
Abstract
Everywhere, independently of the care setting, there is an urgent, unsatisfied need to take care of patients with combined kidney and heart disease. In May 2023 we launched the Kidney-Heart Outpatient Service in the Nephrology and Dialysis Unit of “Paolo Giaccone” University Hospital in Palermo. The clinical mission of our Kidney-Heart Service is to provide a coordinated, multi- disciplinary care for non hospitalized patients with coexisting kidney and heart disease, with the aim to significantly reduce admissions and readmissions in hospital, improving patient outcomes and optimizing utilization of economic resources. In this letter we present the clinical objectives and services provided of this new service and the 1-year results.
Keywords:
cardiorenal
; clinical nephrology
; referral and consultation
The number of patients with, or at risk for, coexisting kidney and heart disease, often named “cardiorenal” or “renocardiac” syndromes (CRS), is increasing worldwide. A lot of studies documented a higher mortality and a significant morbidity in this kind of patients [1,2].
There is a significant interplay between nephrology and cardiology across various aspects, including epidemiology, risk factors, pathophysiology, diagnosis, prognosis, prevention, treatment, monitoring, and research, all of which involve both the kidney and the heart in cardiorenal patients, particularly those with renocardiac syndromes.
The Acute Dialysis Quality Initiative outlined a consensus-based approach in 2008, which categorized cardiorenal syndromes (CRS) into two main groups—cardiorenal and renocardiac syndromes—based on the primum movens of the disease process [3]. This classification was further subdivided into five subtypes, considering the acuity of the disease and the sequential involvement of organs. A scientific statement from the American Heart Association has expanded on the central concept that in CRS, acute or chronic dysfunction in one organ can induce acute or chronic dysfunction in the other organ [4].
This interaction between of kidney and heart disease is attracting attention to the hemodynamic factors, physiochemical variables and biological processes and lead to a complex pathophysiology with typical disease features, and to the need of specific treatment and specialized care that may not be adequately addressed by either cardiologist or nephrologist alone [5].
To address these challenges, nephrologists must undergo specialized training to enhance their cardiological knowledge and skills, while cardiologists must similarly deepen their understanding of nephrological aspects. Both disciplines should collaborate in a multidisciplinary care setting to advance the subspecialty of cardionephrology and improve outcomes in cardiorenal care [6].
It thus clearly emerges that everywhere, independently of the care setting, there is an urgent, unsatisfied need to take care of patients with combined kidney and heart disease [7,8] with a personalized, patient-centered approach.
Historically, therapeutic practices have evolved significantly, moving from a “patient-centered” approach to one based on “evidence-based medicine.” This shift reflects a transition from an “holistic perspective” of disease to a focus on “specific causes for specific diseases” [9,10].
Currently in Italy as in many other countries, cardiologists primarily manage cardiorenal syndromes of types 1 and 2, while nephrologists primarily treat types 3 and 4. However, there is a lack of synergy in efforts for the prevention and management of CRS at various levels. Institutional collaboration is minimal, often occurring only occasionally through consultations, which frequently take place too late in the patient care process. An integrated, simultaneous multidisciplinary approach involving the relevant healthcare professionals in CRS management is still lacking, leaving patients to receive partial or restricted care due to the narrow perspective of the primary specialty and limited resources in an outpatient setting [11].
We hypothesize that a shift in a similar paradigm may occur in nephrology and cardiology, particularly regarding patient stratification and targeted management.
Moreover, in addition to new drugs, recent advances in medical technologies and devices could offer the opportunity to better treat these patients [12,13].
Cardiovascular diseases (CVD) are a leading cause of mortality in patients with chronic kidney disease (CKD), particularly in stage 5 (dialysis-dependent), where they account for up to 58% of deaths [14,15]. In addition to traditional cardiovascular risk factors (CVRFs) such as diabetes and hypertension, non-traditional risk factors associated with kidney disease itself appear to play a crucial role in the complex interaction between the kidney and the heart.
Admissions and readmissions for decompensated heart failure are among the most common causes for hospitalizations in Italy; therefore, reducing frequency and improving outcomes associated with heart failure hospitalizations is a public health priority [16,17]. AKI frequently complicates these hospitalizations and is associated with poor clinical outcomes and higher resources utilization [18].
Preliminary findings on the impact of cardiorenal units on the clinical outcomes of patients with AKI and HF are encouraging, but further validation in larger patient populations and extended follow-up periods is necessary.
Cardiorenal units for inpatients provide support to nephrologists and cardiologists in various clinical settings, including regular medical wards, telemetry units, and intensive care units. These units aim to facilitate more consistent interdisciplinary communication, creating a clinical and educational environment that enhances the expertise of both specialties in managing cardiorenal conditions.
Furthermore, cardiorenal units play a critical role in advancing research on cardiorenal syndrome (CRS) and renocardiac syndromes. Key scientific components of these units include the longitudinal collection of electronic health records from cardiorenal patients and their direct recruitment into clinical research studies. It is essential to recognize the existing gap in evidence-based therapies for patients with chronic cardiorenal syndrome, particularly those with advanced CKD and chronic heart failure [19].
However, these data pertain to a management context related to hospitalizations, and the experiences of outpatient management for patients requiring such a combined approach are unfortunately rarely shared in the literature.
For all of these reason, in May 2023 we launched the Kidney-Heart Outpatient Service in the Nephrology and Dialysis Unit of “Paolo Giaccone” University Hospital in Palermo and to the best of our knowledge, this is the first outpatient facility dedicated to nephrocardiology patients to have been established in our country.
The clinical mission of our Kidney-Heart Service is to provide a coordinated, multi- disciplinary care for non hospitalized patients with coexisting kidney and heart disease, with the aim to significantly reduce admissions and readmissions in hospital, improving patient outcomes and optimizing utilization of economic resources.
To achieve this goal, the Service offers consultation for patients booked every week from a reservation list made with the prescriptions of general practitioners. This Service has been staffed with a nephrologist and a cardiologist trained in point-of-care ultrasounds and it works once a week with five patients a time.
In a typical appointment, patients were asked about their medical history, then underwent to the medical examination: first, body weight, height, waist-to-hip ratio, arterial pressure (expressed ad a mean of three measurements) were collected. After that, a typical 12-derivations ECG was registered and biochemical exams were collected or prescribed. On this basis, further instrumental, blood and urine exams were proposed: 24-hours urine collection is routinary prescribed to have protein excretion and microalbuminuria, along with blood lipid profile.
To better assess the cardio-renal damage, Fundus Oculi is obtained by a trained ophtalmologist from every patient with a portable ophtalmoscope. If necessary and urgent, lung, heart and kidney ultrasound scanning is obtained in the same occasion; otherwise it is scheduled along with carotid doppler.
Finally, nephrologist and cardiologist finish the evaluation and give the medical report to the patient. In the report a complete, shared medical therapy is prescribed, according to the most recent guidelines.
The most important objectives are the reaching of blood pressure goals, the normalization of blood glucose levels and lipid profile; therefore diet, lifestyle modifications along with drugs are prescribed. Drugs’ dosage is obviously adjusted for eGFR obtained by CKD-EPI equation.
A combined-care model involving specialists in cardiology and nephrology could substantially redefine the management of pharmacological therapies commonly used in patients with cardiorenal syndrome. Specifically, it could lead to a more integrated approach in the use of inotropic agents, vasopressors, diuretics, and renin-angiotensin system inhibitors, as well as anticoagulants, lipid-lowering agents, and medications to modify electrolytes [ronco]
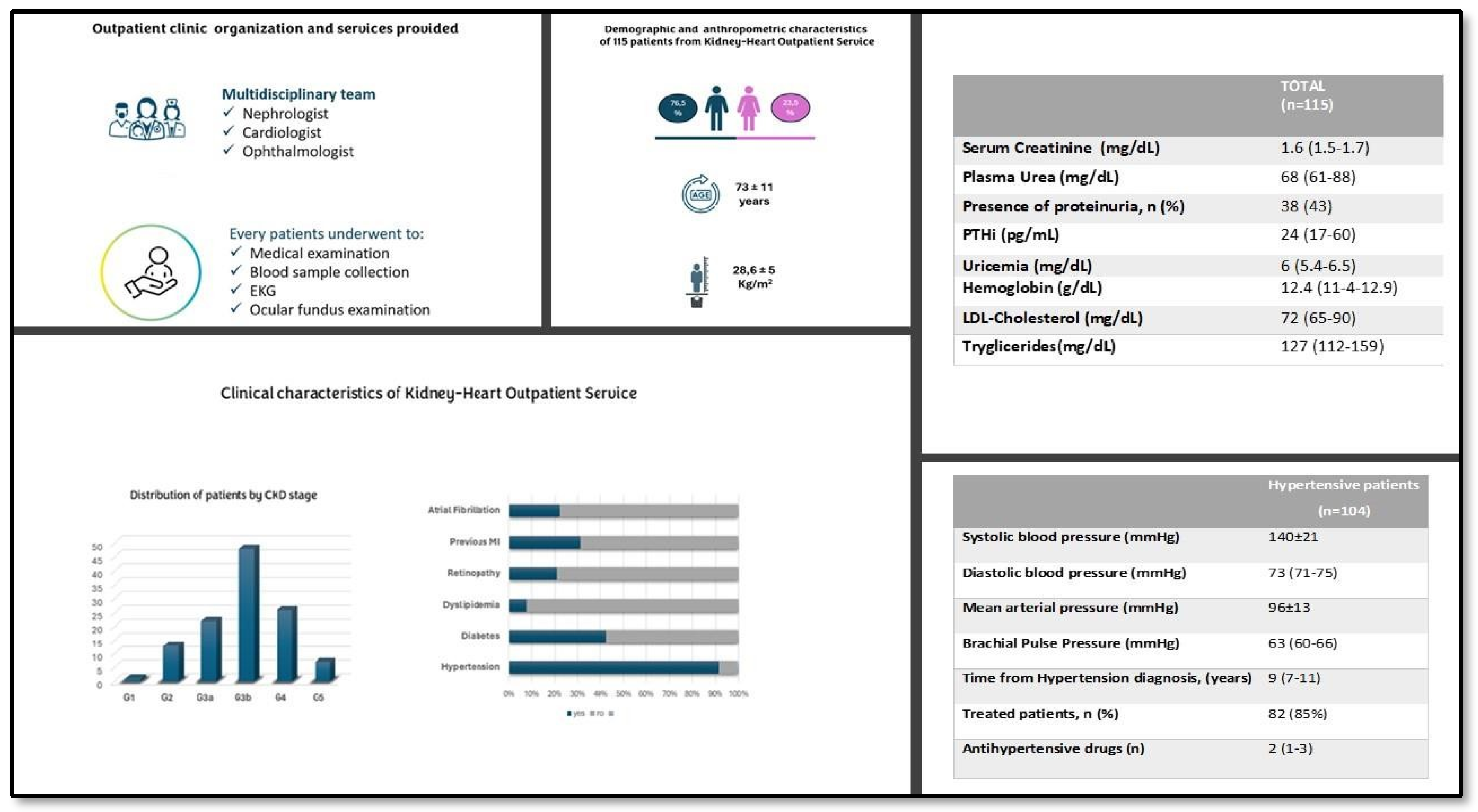
In the following figure we summarized the main features of the patients we evaluated from the launch of the Kidney-Heart Outpatient Service. As you can see, most of patients are male, aged over 70 y.
Hypertension and diabetes confirm their leading role both in inducing and accompanying kidney disease along with myocardial infarction and atrial fibrillation.
Regarding to the CKD Stage, G3b (KDIGO 2012) is the most frequent observed.
We registered three deaths (one for stroke, one for acute heart failure and the last for myocardial infarction). One of our patients underwent hemodialysis.
We found a high prevalence of arterial hypertension (91%) in our patients, the relative details of which are illustrated in the image below. (Figure 1)
To fulfill the requirements of a University Hospital, we involved postgraduate medical students both from Nephrology and Cardiology postgraduate medical schools in the decision making process, since our goal, is to encourage the acquisition of multidisciplinary knowledge and to prevent trainees from inheriting the outdated view of a clear separation between their respective areas of interest, we aim to ensure that future specialists do not enter into conflict or provide only partial consultations and therapeutic strategies with a limited perspective, to the detriment of productive cooperation.Also Internal Medicine postgraduate medical students have been welcome.
Our early preliminary data need to be confirmed over a longer period after the launch of the Kidney-Heart Outpatient Service. We have remained committed to our research objectives, which is why we are actively collecting and analyzing longitudinal medical record data from patients who have been seen by the Kidney-Heart Service. Our goal is to closely track the long-term progression of these patients, not only during their hospitalizations but also throughout their outpatient follow-ups. By monitoring their health outcomes both in and out of the hospital, we aim to gain a deeper understanding of the effectiveness of combined nephrocardiology treatments, identify potential gaps in care, and ultimately improve patient management strategies for individuals with complex cardiovascular and renal conditions. This longitudinal approach will allow us to assess trends, recognize early signs of complications, and refine treatment protocols to enhance patient care across both hospital and outpatient settings.
Author Contributions
All author equally contributed to this paper.
Funding
This research received no external funding
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of PALERMO CEL 1 (protocol n.28 10/12/2024).
Informed Consent Statement
Written informed consent has been obtained from the patients was obtained.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY: Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med 351: 1296–1305, 2004. [CrossRef]
- Rangaswami J, Bhalla V, Blair JEA, et al.; American Heart Association Council on the Kidney in Cardiovascular Disease and Council on Clinical Cardiology: Cardiorenal syndrome: Classification, pathophysiology, diagnosis, and treatment strategies: A scientific statement from the American Heart Association. Circulation 139: e840–e878, 2019. [CrossRef]
- Ronco C, McCullough P, Anker SD et al. Cardio-renal syndromes: report from the Consensus Conference of the Acute Dialysis Quality Initiative. Eur Heart J 2010;31:703–711. [CrossRef]
- Rangaswami J, Bhalla V, Blair JEA et al. Cardiorenal syndrome: Classification, pathophysiology, diagnosis, and treatment strategies: a scientific statement from the American Heart Association. Circulation 2019 ; 139e840–e878.
- House AA: Cardiorenal syndrome: Introduction. Clin J Am Soc Nephrol 8: 1798–1799, 2013. [CrossRef]
- Borja Quiroga, Alberto Ortiz, Juan F Navarro-González, Rafael Santamaría, Patricia de Sequera, Javier Díez, on behalf of the CaReSEN working group of the Spanish Society of Nephrology, From cardiorenal syndromes to cardionephrology: a reflection by nephrologists on renocardiac syndromes, Clinical Kidney Journal, Volume 16, Issue 1, January 2023, Pages 19–29. [CrossRef]
- Hatamizadeh, P: Introducing nephrocardiology. CJASN 17: 311–313, 2022.
- Sachdeva M, Shah AD, Singh HK, Malieckal DA, Rangaswami J, Jhaveri KD: Opportunities for subspecialization in nephrology. Adv Chronic Kidney Dis 27: 320–327.e1, 2020. [CrossRef]
- Hajar R. History of medicine timeline. Heart Views. 2015;16:43–45. [CrossRef]
- Weaver RR. Reconciling evidence-based medicine and patient-centred care: defining evidence-based inputs to patient-centred decisions. J Eval Clin Pract. 2015;21:1076–1080. [CrossRef]
- Soares DM, Pessanha JF, Sharma A, Brocca A, Ronco C: Delayed nephrology consultation and high mortality on acute kidney injury: a meta-analysis. Blood Purif 2017;43:57–67.
- Ross DW, Stevens GR, Wanchoo R, Majure DT,et al; Left ventricular assist devices and the kidney. Clin J Am Soc Nephrol 13: 348–355, 2018. [CrossRef]
- Jentzer JC, Bihorac A, Brusca SB et al.; Critical Care Cardiology Working Group of the Heart Failure and Transplant Section Leadership Council: Contemporary management of severe acute kidney injury and refractory cardiorenal syndrome: JACC Council perspectives. J Am Coll Cardiol 76: 1084–1101, 2020. [CrossRef]
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351:1296–1305. [CrossRef]
- Gansevoort RT, Correa-Rotter R, Hemmelgarn BR, Jafar TH, Heerspink HJ, Mann JF, Matsushita K, Wen CP. Chronic kidney disease and cardiovascular risk: epidemiology, mechanisms, and prevention. Lancet. 2013;382:339–352. [CrossRef]
- Virani SS, Alonso A, Aparicio HJ et al.; American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee: Heart disease and stroke statistics- 2021 update: A report from the American Heart Association. Circulation 143: e254–e743, 2021. [CrossRef]
- Alloatti S, Strippoli GF, Buccianti et al.; Italian Society of Nephrology. Current structure and organization for renal patient assistance in Italy. Nephrol Dial Transplant. 2008 Apr;23(4):1323-9. [CrossRef]
- Kevin Damman 1, Mattia A E Valente, Adriaan A Voors, Christopher M O’Connor, Dirk J van Veldhuisen, Hans L Hillege. Renal impairment, worsening renal function, and outcome in patients with heart failure: an updated meta-analysis. Eur Heart J. 2014 Feb;35(7):455-69. [CrossRef]
- Ortiz A, Navarro-González J, Núñez J et al. The unmet need of evidence-based therapy for patients with advanced chronic kidney disease and heart failure: Position paper from the Cardiorenal Working Groups of the Spanish Society of Nephrology and the Spanish Society of Cardiology. Clin Kidney J 2021 ; 15: 865–872.
Figure 1.
Kidney-heart outpatient clinic organization and main clinical features of our patients.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



