Submitted:
20 November 2024
Posted:
20 November 2024
You are already at the latest version
Abstract
Wearable devices gain increasing attention for use in multifunctional applications related to health monitoring, particularly in research of the circadian rhythms of cognitive functions and metabolic processes. In this comprehensive review, we encompass how wearables can be used to study circadian rhythms in health and disease. We highlight the importance of these rhythms as markers of health and well-being, and as potential predictors for health outcomes. We focus on the use of wearable technologies in sleep research, circadian medicine, and chronomedicine beyond the -ircadian domain, with an emphasis on actigraphy as a validated tool for monitoring sleep, activity, and light exposure. We discuss various mathematical methods currently used to analyze actigraphic data, such as parametric and non-parametric approaches, applied to quantify circadian and non-circadian variability. We also introduce novel actigraphy-derived markers, which can be used as personalized proxies of health status, assisting in discriminating between health and disease, offering insights into neurobehavioral and metabolic status. We discuss how lifestyle factors such as physical activity and light exposure can modulate brain functions and metabolic health. We emphasize the importance of establishing reference standards for actigraphic measures to further refine data interpretation and improve clinical and research outcomes. The review calls for further research to refine existing tools and methods, deepen our understanding of circadian health, and develop personalized healthcare strategies.
Keywords:
wearables
; actigraphy
; circadian rhythms
; health
; monitoring
; chronobiology
; neurodegeneration
; metabolism
; risk factors
; epidemiology
; longevity
; biological age
1. Introduction
Rhythms are recognized as hallmarks of health [1]. These oscillations can be measured and quantified utilizing diverse mathematical methods and modeling approaches. When such oscillations deviate from their optimal ranges, they can be harnessed as early warning signs for the detection of impending risk and for the implementation of countermeasures to improve health outcomes [2,3,4,5,6,7], epitomizing a pivotal element in the burgeoning domain of circadian medicine [4,7,8,9]. Perturbations in circadian rhythms, both at the molecular and systemic levels, are correlated with the processes of aging and the pathogenesis of diseases [1,2,3,7,10,11]. The meticulous assessment of the normal range of physiological variables necessitates the employment of sophisticated monitoring techniques that involve both data collection and data analysis for a chronobiological interpretation of the results. In the field of circadian medicine research, and chronomedicine more generally, various wearable technologies are utilized to monitor and study sleep patterns, activity levels, and other physiological markers that align with our biological clocks. In the investigation of the optimal characteristics of rhythmic structures, quantitative measures are assessed, alongside deviations from the optimum that may be associated with health risks. These deviations typically encompass both parametric and non-parametric measures. Parametric measures are useful for many circadian functions, which can be described using sinusoidal curves or multi-component models. To accurately characterize the parameters of biological rhythms—namely amplitude, phase, and period length—data collection must occur at suitable intervals across one or, preferably, multiple cycles. Ideally, this collection should be sampled at regular, equidistant intervals; however, it is also feasible with irregular intervals [13,14]. Assessing the intrinsic period in real-life scenarios poses challenges, as its determination necessitates specific, controlled conditions within a laboratory setting, such as the 'constant routine' or 'forced desynchrony protocol' [15]. Conversely, amplitude and phase evaluations are more feasible in real-life circumstances. By collecting data over several cycles, researchers can introduce a 'regularity' domain to measure the stability of phase and amplitude across cycles. Non-parametric measures can be preferred for functions with abrupt transition points such as wake-sleep-wake states and include characteristics that eschew the sinusoidal rhythm model, yet still facilitate the characterization of amplitude, timing, stability, and fragmentation. Longitudinal and dense data sampling enables a thorough assessment of physiological variability and its divergence from normal range. Monitoring and wearable technologies offer excellent means to achieve this objective. Variables such as physical activity, temperature, heart rate, and light exposure are among most accessible and trackable via wearables. Moreover, these variables hold greater physiological significance and, in addition to mere step counts, allow for the sampling of quantified values. The selection of the most appropriate method for data analysis is contingent upon the specific physiological variable under consideration. For instance, physical activity may be best characterized through non-parametric approaches due to its non-sinusoidal patterns, whereas temperature typically exhibits a more sinusoidal nature. While wearable technologies offer significant advancements in health monitoring, they are not without limitations. For instance, measurements of wrist temperature, though less intrusive, are often marred by substantial noise in comparison to core body temperature. Their timing may be nearly, though not precisely in antiphase with those of core temperature. They reflect the work of a special mechanism that ensures a decrease in basal temperature in the evening/night due to heat dissipation, which is necessary for falling asleep and maintaining sleep [16,17]. On the other hand, professional-grade wearables, such as actigraphs, facilitate the assessment of phase alignment among various physiological variables. This is particularly pertinent when incorporating measurements of light exposure, which serves as the principal circadian synchronizer.
In the field of circadian medicine research, and chronomedicine more generally, various wearable technologies are utilized to monitor and study sleep patterns, activity levels, and other physiological markers that align with our biological clocks. Some types of wearables already in use or still being developed in this area are summarized in Table 1. Overall, modern wearable monitoring techniques offer unprecedented perspectives to define normal ranges for rhythm parameters and use them to track unspecific and disease-specific health risks [18,19,20,21,22,23,24,25]. It is advisable for innovative devices to be aimed specifically at certain patient groups. For instance, the association between actigraphy and single-channel EEG was found to be weakened in individuals with mild cognitive impairments and those diagnosed with Alzheimer's disease [26]. Analysis of electrocardiogram time series using machine learning (ML) algorithms made it possible to reliably identify sleep phases (REM/NREM) [27,28], which indicates great prospects for using ML in somnology and chronobiology. However, despite the variety of affordable multisensory wearable devices on the market, their wide public use and blue-tooth compatibility, actigraphy remains a scientifically best-validated tool for research in chronomedicine. It provides objective real-life insights into an individual's sleep, activity and light exposure patterns, providing full access to raw data, which is highly important in research [20]. Earlier actigraphs’ embedded accelerometer allowed the device to record body movements, providing a representation of activity levels over extended durations [29,30,31]. It was commonly used to assess sleep quality but also had applications in various medical fields [32,33], including psychiatry, neurology, oncology [34], and geriatrics. Actigraphy has proven to be a valuable tool in diagnosing and managing various conditions, including depression, narcolepsy [35], Alzheimer's disease, Parkinson's disease, and dementia [36,37,38]. Actigraphy also serves as a quantitative measure of physical activity throughout the day. Monitoring movement enables researchers to evaluate an individual's average activity, periods of sedentary behavior, and compliance with study protocols. To estimate measures of physical activity, including energy expenditure, wrist- and hip-worn devices produce comparable results [39]. Advanced actigraphy units are now equipped with sensors for wrist temperature and ambient light [40], allowing for a more comprehensive examination of rhythms and their perturbations. Through the analysis of activity patterns and wrist temperature, researchers can deduce information about the internal circadian clock and its influence on health.
2. Actigraphy Features: Beyond Sleep
Considering the thorough exploration of implications, constraints, and viewpoints of actigraphy within the realm of sleep medicine, as detailed in prior literature [24,41,42,43,44,45], this review aims to encompass the infrequently employed, yet increasingly acknowledged applications of actigraphy for the quantification of physical activity, assessment of metabolic health, and the prognostication of lifespan. Subsequently, this review will also deliberate on the imminent roles of commercially accessible wearable devices in the sphere of circadian medicine and chronomedicine more broadly. These applications do not solely revolve around sleep, as they also involve quantifying circadian and extra-circadian (ultradian, infradian) variability, based on dense sampling (usually every minute) and analyses of longitudinal (usually weeklong) records. To examine time structures of the rest-activity cycle as it changes over time, actigraphy can be empowered with mathematical tools, including parametric (MESOR, amplitude, phase [13], ultradian and infradian spectral analysis, [11,46,47], and non-parametric (M10, M10 Onset, L5, L5 Onset, inter-daily stability (IS), intra-daily variability (IV), relative amplitude, circadian function index, etc.) estimates of physical activity [48,49,50,51,52]. In addition, the same methods can be applied to the other variables (wrist temperature, ambient light measured at different wavelengths, e.g., red, green, blue, ultraviolet A, ultraviolet B, infrared, or even spectrally resolved). Furthermore, it can be used to calculate novel, more sensitive health markers such as indices of daytime light deficit and nocturnal light excess [53], scalar regression markers [54], phase angles between activity and light [55,56], or integrated variables such as TAP, which incorporates measures of three variables (Temperature, Activity and Position) [50]. A personalized approach to search for circadian markers of health and disease, quantified by wearable technologies, can be most fruitful as certain genetic-, gender-, or geographically-related phenotypes may be vulnerable to circadian disruption [53].
Actigraphy acquired a growing interest in studies of metabolic health and circadian syndrome, which can be a more precise definition of metabolic syndrome [57,58]. By continuously tracking physical activity and sleep duration, actigraphy provides valuable data that can be correlated to various metabolic endpoints, such as glucose concentrations, insulin sensitivity, and lipid profiles [56,59,60,61,62,63,64]. This approach offers a holistic view of daily habits and their putative effect on metabolic health. Furthermore, integrating actigraphy data with biobank big data enhances the depth of analysis, allowing researchers to explore correlations between activity patterns, genetic factors, and metabolic outcomes on a large scale. Biobanks, repositories of biological samples and associated health data, play a crucial role in advancing our understanding of complex diseases like diabetes, obesity, and cardiovascular disorders, in addition to neurodegenerative diseases and mood disorders that were extensively investigated previously. Actigraphy is promising in identifying early markers to predict cardiometabolic risks, and providing personalized preventive strategies. Furthermore, actigraphy can be used to evaluate the effectiveness of strategies for improving sleep or optimizing the amount and timing of physical activity.
3. Overview of Actigraphic Health Markers
Actigraphy and other wearable technologies provide a non-invasive and efficient method for continually monitoring physiological functions in real-world environments. These tools have a wide range of applications in research, clinical practice, and personal health monitoring, making them an invaluable resource for quantifying and comprehending various aspects of health and well-being. They are particularly useful when used in conjunction with the central synchronizer of the circadian clock, light, to measure circadian light hygiene and its influence on health and well-being. By combining objective data on light exposure with information on sleep patterns and circadian rhythms, actigraphy can help to pinpoint strategies for promoting optimal circadian alignment and enhancing overall health outcomes. Most common forms of circadian disruptions that are revealed by actigraphy are summarized in Table 2 and schematized in Figure 1.
A decline in circadian robustness with age and disease is considered a general biological feature and may serve as an unspecific marker of biological age to predict healthy aging and longevity [1,2,10,11,65,66,67,68]. The following parametric / non-parametric indices are commonly used to characterize circadian and 24-h variability of physiological variables such as activity, temperature, and light exposure.
Parametric [13]:
y(t) = M + ΣiAicos (2πt/τi + φi), i=1, …, k
(usually, τ1=24 h accounts for most of the variance and its parameters (A1, φ1) are useful biomarkers)
y – related data; t – time
acrophase (φi), moment in time when component with period τi reaches its peak in relation to a given reference time;
MESOR – Midline Estimating Statistics Of Rhythm (a rhythm-adjusted mean);
Ai –Amplitude of component with period τi.
Note that a multi-component cosinor is usually most appropriate (e.g., blood pressure and heart rate are usually fitted with a 2-component model, including the 12-h harmonic term. While composite models yield a better approximation of the rhythm’s waveform, the fundamental component, with a period of 24 h, often accounts for most of the variance, and its parameters can serve as valuable biomarkers.
Non-Parametric [48]:
M10 – the average of 10 h of maximum value.
M10 Onset – the start of the M10 period.
L5 – the average value of 5 h of lowest value.
L5 Onset – the start of the L5 period.
RA (Relative Amplitude); RA = (M10-L5 )/(M10+L5)
- IV (Intra-daily Variability) is calculated by the following formula:
Note that additional measures of activity-rest patterns were recently proposed [52]: the Activity balance index (ABI), Transition probability (TP), Self-similarity parameter (α), that may have merits beyond IV and IS, being independent of differentiation between rest/activity states that currently lack standardization. However, unlike IV or IS, ABI and α are sensitive to extreme values that could be observed in the data.
3. Interpretation of Deviant Parameters
- Reduced Relative Amplitude of activity: lower daytime physical activity or light exposure (M10) that can be accompanied by higher nocturnal activity or light exposure (L5) is indicative of poorer sleep or light hygiene.
- Reduced circadian amplitude of activity: similarly relates to lower daytime but higher evening physical activity, Figure 2. In addition, the regularity of physical activity or light exposure patterns can be assessed by comparing the ratio of the amplitude assessed by separate 24-h cycles (A24) to the amplitude approximated over the entire monitoring period, e.g., week (Aw). When activity or light exposure occurs irregularly, Aw/A24 is reduced.
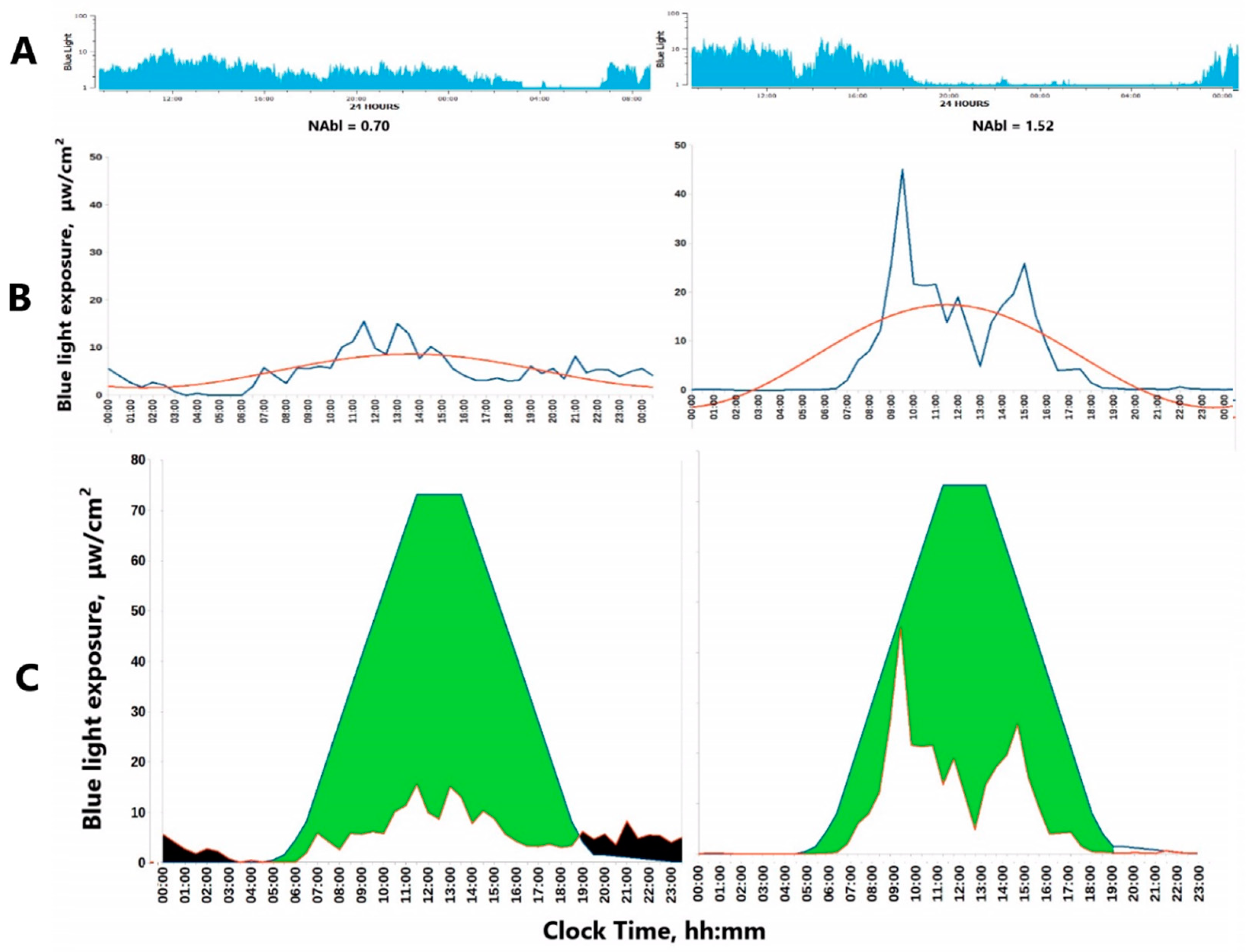
- The Normalized Amplitude (NA) can serve as a valuable metric to quantify both Physical Activity (PA) and light exposure (LE), Figure 3. It is particularly advantageous for LE, which often assumes extremely low or null values during the nighttime. Applying a log-transformation can effectively normalize these values, albeit at the cost of reducing daytime variations when LE is generally high.
- Phase deviations – both too late and too early maximal values may serve as health risk predictors. However, stronger evidence has accumulated to explain a phase delay since it is closely linked to and can be driven by a poor circadian light hygiene.
- Phase relationship – phase lag between light and activity (or sleep and melatonin) that can be predicted by wrist temperature (wT) provides more specific information, which, however, can strongly depend on the power of light signaling that varies profoundly depending on the local light environment and seasonal photoperiodism.
Figure 2.
Examples of cases with relatively high (left) and low (right) motor activity with about 2-fold MESOR and almost 3-fold Amplitude differences, while Acrophases are similar. A: 7-day actograms; b) average 24-h patterns, c) average 7-day patterns with approximated best-fitted 24-h cosine function with its parameters. PIM – activity data processed using Proportional Integration Mode, a measure of activity level or vigor of motion [41].
Figure 2.
Examples of cases with relatively high (left) and low (right) motor activity with about 2-fold MESOR and almost 3-fold Amplitude differences, while Acrophases are similar. A: 7-day actograms; b) average 24-h patterns, c) average 7-day patterns with approximated best-fitted 24-h cosine function with its parameters. PIM – activity data processed using Proportional Integration Mode, a measure of activity level or vigor of motion [41].
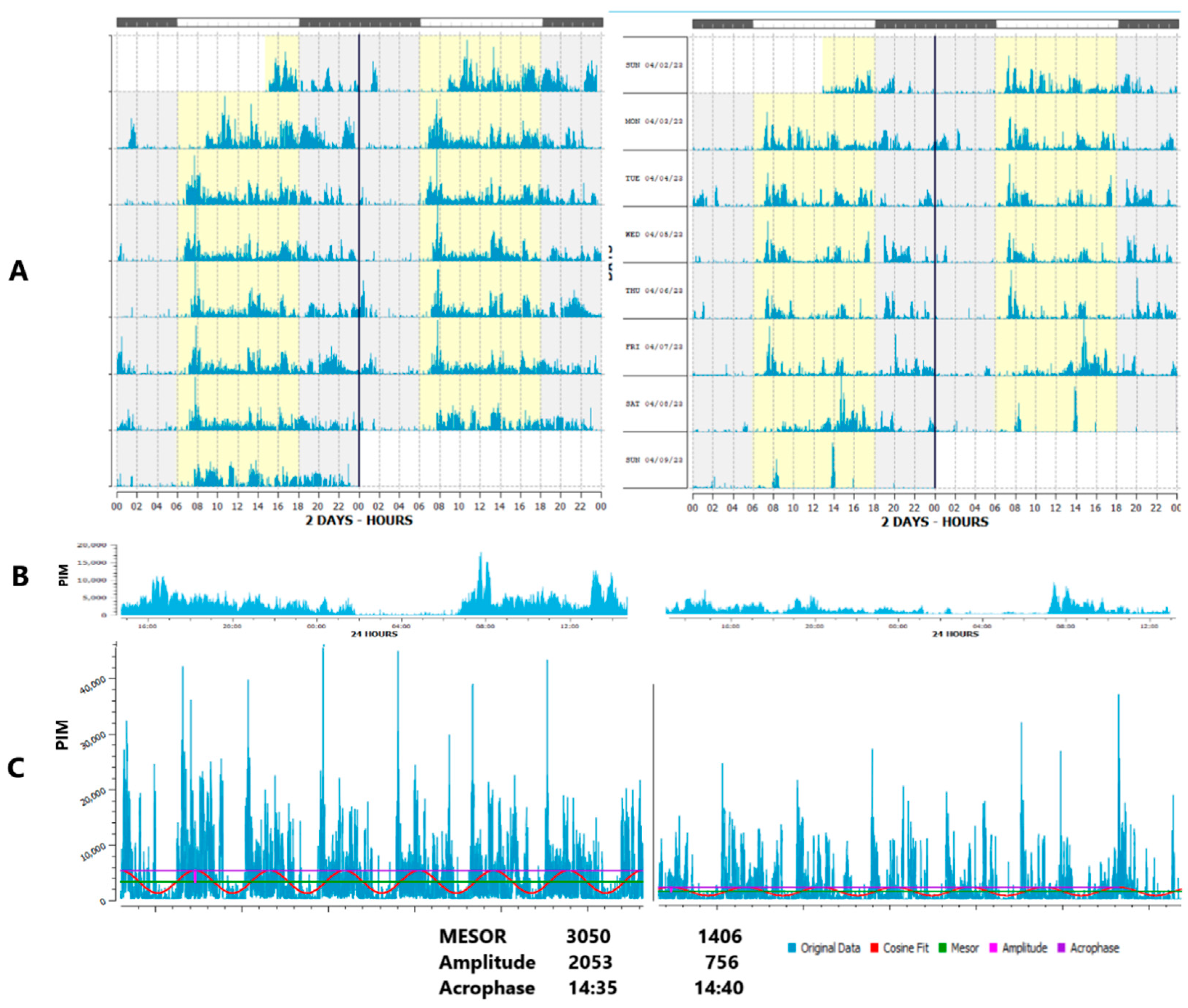
Figure 3.
Examples of light hygiene measures: A) 24-h average patterns of blue light exposure in patients with poor (left) and fair (right) circadian light hygiene; B) normalized circadian amplitude of light exposure (NAbl) of individuals with poor (NAbl=0.7, left) and fair (NAbl = 1.52, right) circadian light hygiene; and C) geometric indices of cumulative daylight deficit and nocturnal light excess [53], our reference curve modification, based on recommendations for light exposure [108], left: individual with poor circadian light hygiene (DDIbl=473 NEIbl=13.38); right: individual with fair light hygiene (DDIbl=397 NEIbl=0.17). DDIbl – Daylight deficit index for blue light exposure (green areas – area under the curve of recommended daylight); NEIbl – Nocturnal Excess Index of blue light exposure (black areas – area above the curve of recommended nocturnal light).
Figure 3.
Examples of light hygiene measures: A) 24-h average patterns of blue light exposure in patients with poor (left) and fair (right) circadian light hygiene; B) normalized circadian amplitude of light exposure (NAbl) of individuals with poor (NAbl=0.7, left) and fair (NAbl = 1.52, right) circadian light hygiene; and C) geometric indices of cumulative daylight deficit and nocturnal light excess [53], our reference curve modification, based on recommendations for light exposure [108], left: individual with poor circadian light hygiene (DDIbl=473 NEIbl=13.38); right: individual with fair light hygiene (DDIbl=397 NEIbl=0.17). DDIbl – Daylight deficit index for blue light exposure (green areas – area under the curve of recommended daylight); NEIbl – Nocturnal Excess Index of blue light exposure (black areas – area above the curve of recommended nocturnal light).
3.1. Faded Circadian Oscillation (Amplitude Decrease)
First of all, mean values for physical activity, ambient light, and wrist temperature (24-h, diurnal, such as M10, nocturnal such as L5) can be indicative – and serve as proxies – of health and as mortality and morbidity risk factors for certain diseases, Figure 1, Table 2. Examples are low 24-h physical activity, increased or decreased temperature, and low sunlight exposure. Mean values, however, can be restricted to the daytime or to the nighttime, and this information needs to be specified as it affects its interpretation. Indeed, health hazards stem from lowered diurnal, but elevated nocturnal activity, and from low daylight exposure but light-at-night. Therefore, deviations in circadian endpoints other than the mean value also deserve consideration. Changes in the 24-h amplitude and in circadian robustness are cases in point. They can be estimated by absolute measures of A or RA, or their normalized values (relative to the individual mean), NA/NRA. The latter may be preferred when inter-individual variability of averages (or MESORs) is high. Alternatively, a measure of circadian robustness can consider the spectral domain of ultradian and infradian frequencies to incorporate the analysis of the relative amplitudes among particular ultradian and infradian frequencies to the circadian, which adds valuable new information. The circadian rhythm is usually the dominant component with the highest power or amplitude in weeklong records of physiological variables that can be recorded with wearable monitoring devices. The relative decrease in circadian prominence to extra-circadian domains is defined as extra-circadian dissemination, ECD [2,10,11]. Another approach includes integrative values for three related actigraphy variables (temperature, position and activity, TAP), used to estimate the Circadian Function Index [50]. A decrease in circadian robustness, as gauged by either of these methods, is a feature associated with aging, diseases and health risks.
To ensure comparability among the aforementioned quantitative indices of circadian health, it is imperative to standardize the following essential sampling attributes across various studies: total duration of recording, frequency of observations within the time series, and the number, timing, and extent of interruptions in the dataset. When data are non-equidistant, a measure of the distribution in time of the observations can help determine the frequency region within which reliable results can be anticipated.
3.2. Phase Deviations
A diminution in circadian robustness may stem from a true reduction in amplitude or a deterioration of phase stability. For example, irregular circadian timing (e.g., irregular sleep-wake patterns), which has been associated with a higher mortality risk [69], leads to a reduced amplitude when data are analyzed over several days, but not when data are analyzed over a single day (cycle). Indeed, the most common health risks related to circadian disruption are a reduced amplitude, a deviation from sinusoidality, a delayed phase, a compromised phase alignment, and an increased day-to-day instability and fragmentation of the circadian activity rhythm, Table 2.
Phase instability usually means misalignment between circadian oscillations of the distinct circadian functions. It can be caused by a weakened light signaling due to poor circadian light hygiene [4,5,6,70,71,72,73] or by a compromised light perception due to issues with retinal ganglion cells [73,74,75,76,77,78]. As far as measurable overt rhythms are concerned, it also can be due to the uncoupling between peripheral oscillations, or the perception of central clock signaling to peripheral clocks [7,72,79,80]. Phase scattering may occur without changes in mean phase position, or it can be accompanied by a phase delay or phase advance. Accumulating evidence indicates that a phase delay, which is usually linked to a late chronotype, is a common health risk factor, Table 2. A phase delay is associated with evening light exposure and lack of diurnal light [73], or light perception [77,78], but it can also be attributed to certain clock genes or clock-controlled genes related to chronotype [81].
3.3. Fragmentation and Ultradian / Infradian Modifications
Modifications of circadian oscillations may occur within a cycle (fragmentation, or prominence in ultradian harmonics) or between consecutive cycles (scattered, unstable circadian parameters such as the 24-h phase, or higher prominence of infradian components). They can be accompanied by a greater deviation of the best-fitted model from an ideal sine curve, i.e., reduction in the percentage of rhythm. In actigraphy, the most commonly used indices are the non-parametric indices IV and IS [48], which can be used to predict numerous health hazards, Table 2. Quantified approaches to estimate the loss of regularity can be applied to characterize sleep and its stages [46,47].
In addition to deviations in characteristics of circadian rhythms, modifications can be observed in the relationships between circadian and extra-circadian components, such as regular oscillations in the ultradian (periods shorter than 20 h) or infradian (periods longer than 28 h) domains. Regular movement patterns during sleep (Locomotor Inactivity During Sleep) were first described by pioneers in sleep research [82]. They were observed using early accelerometer-based techniques [30] and again recently in modern actigraphy studies [46]. Regular ultradian oscillations with a period of about 110 minutes characterize activity during sleep. Such oscillations gradually fade across the night. The amplitude of this ultradian rhythm does not depend on sex, but is modified by sleep duration and shift-work, and gradually declines with age [46]. Ultradian sleep cycles may belong to endogenous biological rhythms, and are influenced by factors such as age, gender, and the balance of sleep needs; however, in individuals who are healthy and sleep well, these cycles do not directly change in response to moderate environmental stimuli [47]. Infradian rhythms can be related to geophysical and social cycles and include yearly, monthly and weekly fluctuations [83,84,85,86]. There is indirect evidence that circaseptan (about-weekly) rhythms [87,88] and circa-lunar cycles [89,90,91] may also be partly endogenous.
In addition to non-parametric indices, inter-daily stability and intra-daily variability can also be assessed by using an ECD model, such as the computation of ultradian-to-circadian, and/or infradian-to-circadian rhythm amplitude ratios [2,10,11]. The relative prominence of circadian, ultradian, and infradian rhythms changes with age and disease for different physiological variables such as heart rate, blood pressure, and temperature [11,12,66] and disease [11]. Due to the fact that changes in ultradian and infradian components are influenced by distinct physiological mechanisms [2,11], it is essential to utilize these methods to examine variability and identify disease-specific predictors. As modern wearables acquire a wider range of functions, which can be naturally more sinusoidal than physical activity, characterization of spectral domains (ultradian, circadian, infradian) and their interplay can become a fruitful approach.
3.4. Misalignment (Intrinsic Desynchrony)
Increased intrinsic desynchrony or circadian misalignment between variables has been shown to be a significant predictor of health risks, Table 2. Examples include the Light-Activity phase lag [56] and the surrogate index of phase of entrainment, specifically the sleep-temperature phase relationship [92,93]. The temperature phase can serve as a substitute for the golden standard of melatonin phase, as the phases of temperature and melatonin exhibit a relatively close relationship [94,95,96]. Misalignment between the central clock phase and phases of local or peripheral oscillations [75] can be assessed by the integration of novel sensors into wearables.
3.5. Social Jet Lag: Objective Characterization by Wearables
Social jet lag (SJL) refers to the regular misalignment between the personal endogenous circadian clock and social obligations, such as work or school schedules [97,98]. It can occur when individuals stay up later and sleep in on weekends or holidays, causing their internal body clock to be out of sync with their typical weekday routine. It can lead to fatigue, difficulty concentrating, and overall reduced well-being [98]. Greater SJL is associated with an increased risk of cardiometabolic [99,100,101,102,103] and mood [102,104,105,106] disorders. As actigraphy provides objective measures of activity and temperature, these data can be used to assess circadian health and phase changes on a daily basis in weeklong records [107]. The most abundant actigraphy data that were collected and made available for large database analysis include physical activity. When adopting sampling frameworks that account for weekly patterns, it becomes crucial to calibrate or rectify the data to reflect the actual number of workdays versus days off, including instances of shift-work or sporadic commitments that necessitate awakening outside the regular schedule. Furthermore, incorporating details regarding the timing and length of daytime naps enriches the dataset, particularly for the accurate calculation of sleep-related metrics. In older adults, SJL very often approaches zero, which is due to the fact that upon retirement, the main external factor (work schedule) ceases to affect them [103]. Therefore, studying the acute effects of SJL on the health of older people is usually ineffective. The most promising in this case is the study of the chronic effects of SJL on human health.
3.6. Composite Markers
Searching for markers that are specific to the risks of certain pathologies can yield positive results when analytical focus is placed on timeframes that correlate with phases of increased sensitivity and physiological response, Table 2. Examples are: 1) areas above (nocturnal excess index, NEI) or under (daylight deficit index, DDI) the curve of optimal 24-h exposure to light [53], where thresholds are based on existing consensus recommendations [108]; 2) MLiT500, the average clock time of all aggregated data above 500 lux [109]; and 3) FOSR (Function-On-Scalar regression), a method seeking time-of-day differences in a comparison of models fitted to groups defined by the presence or absence of a given risk factor or pathology [54]. NEI and MLiT500 were predictive of body mass index; NEI was also linked to metabolic issues within the 9:30 to 00:30 timeframe, specifically in carriers of common melatonin receptor gene polymorphism, MTNR1b rs10830963; DDI was linked to elevated cortisol concentrations [53]. The FOSR method detected daytime and evening timeframes of higher activity and variability in activity, which were predictive of Alzheimer’s disease with PET-confirmed beta-amyloid Aβ deposition [54]. Novel wearable-based digital markers, encompassing circadian amplitude, phase and physical activity for biological age evaluation [110] can be useful for further advancement in preventive strategies of circadian medicine / chronomedicine.
In relation to blood pressure and heart rate, chronobiological reference values were derived to assess the percentage time elevation/reduction, the amount of excess/deficit, and their timing along the 24-h scale. Similar reference values, qualified by gender and age, derived for all circadian parameters identified new risk factors related to the amplitude and phase. These abnormal features of the circadian variation in blood pressure and heart rate, known as Vascular Variability Disorders (VVDs) were shown to predict adverse cardiovascular outcomes in several outcome studies [111,112,113,114].
4. Circadian Health Markers from Actigraphy
As major markers of circadian disruption described in Table 2 are unspecific and can be related to frailty, aging, or different diseases, further study should seek more specific manifestations of compromised circadian robustness. They can be successful in tracking specific variables and specific indices, also seeking polymorphic gene variants in core-clock or clock-controlled genes [7]. Several genes (e.g.. CLOCK, BMAL1, PER1,2,3, and MTNR1B) have SNPs that were consistently linked to compromised circadian health related to cardiometabolic [5,53,115] or neurodegenerative [5,75,76,115,116,117] diseases.
Establishing reference standards for actigraphy-derived measures is a pressing need that has begun to be addressed. These standards are crucial for providing benchmarks or normal ranges against which individuals' sleep-wake patterns, activity patterns, circadian and light hygiene patterns can be compared. By defining these norms, we can better understand deviations that may indicate underlying health issues, facilitating more accurate diagnoses and personalized treatment strategies. Developing reference standards for actigraphy-based parametric and non-parametric indices is a significant step forward in the field of circadian medicine / chronomedicine, and sleep research. Establishing reference standards for different indices of the distinct measurable variables will allow better interpretation of wearable-collected data and facilitate comparisons across studies and populations. It will enable clinicians and researchers to identify deviations from normal ranges, which may indicate sleep disorders, circadian rhythm disturbances, or other health issues. When light exposure is tracked, drastic seasonal changes, especially at higher latitudes must be considered as well [53]. Certain individual phenotypic traits such as disease conditions [26] or skin color [20] that may have an effect on data quality should also be considered.
Recent studies have delved into deviations from optimal circadian health using actigraphy, with a significant portion of them utilizing extensive databases like the UK Biobank [36,118,119,120,121] and NHANES in the USA [68,122,123,124]. While many studies focused on disruptions in the circadian rhythm of physical activity, some also explored deviations in temperature and light exposure rhythms. The following sections outline key findings that highlight the associations between actigraphy or wearable-based circadian measures of health and various health outcomes, including morbidities, frailty, mortality, and longevity. Table 2 provides a comprehensive summary of these studies, detailing the specific aspects of circadian health that were found to be altered in relation to health status. These aspects, however, can strongly depend on the power of light signaling that varies profoundly depending on the local light environment and seasonal photoperiodism.
4.1. Circadian Markers of Morbidity and Mortality
The circadian rhythm of physical activity plays a crucial role in maintaining bodily [125,126,127,128] and mental [129,130,131] health. A recent retrospective assessment of actigraphy data from a large UK biobank cohort (over 100,000 participants 40-69 years of age) revealed that a large amplitude of the circadian activity rhythm is associated with lower risks of numerous health issues, including cardiovascular, metabolic, respiratory, infectious, cancer and all-cause morality [119]. Similar results were obtained in a prospective 16-year-long survey in over 1000 adults [120]. Moreover, 73 out of 423 (17%) disease phenotypes were significantly associated with a reduced circadian amplitude of the wrist temperature rhythm in actigraphy records from over 100,000 participants, the strongest associations found in relation to type 2 diabetes, non-alcoholic fatty liver disease, hypertension, and pneumonia [121]. A smaller amplitude and reduced circadian robustness were associated with an increased susceptibility to mood disorders such as major depressive disorder and bipolar disorder, mood instability and neuroticism [118]. Similar markers predicted cognitive deficits in Alzheimer’s and Parkinson’s diseases [36,38]. A larger RA and lesser fragmentation (higher IV, lower IS) of wrist temperature were associated with better sleep quality in Japanese adults [132]. In addition to amplitude and fragmentation, a deviant circadian phase or deviant non-parametric estimates of indices such as M10 or L5 Onset were also indicative of elevated morbidity/mortality risks. Besides a smaller amplitude, a delayed activity phase was related to higher mortality from cancer and stroke [125], higher risks of dementia or mild cognitive impairment in community-dwelling elderly women [129]. Earlier or later L5 Onset vs. intermediate values in the range of 3:00-3:29 from 7-day actigraphy records from 88,282 adults in the UK Biobank was linked to a 20% higher risk of all-cause mortality [133]. Another study including records from 103 ,712 UK Biobank participants found a relationship between earlier or later sleep onset (compared to optimal onset between 22:00 and 23:00) and the risk of developing cardiovascular diseases, particularly in women [134]. Given that the L5 Onset and sleep mid-time are markers of chronotype, both studies suggest that the relationship between chronotype and health hazards is nonlinear, as opposed to linear. Since chronotype changes with age (also in the 40-70 age range) sex-dependently [135,136], as shown in the UK Biobank database, a more sophisticated analysis is warranted that adjusts some metrics from the UK Biobank or other large databases for age and gender. Such adjustments in the estimation of circadian timing can be helpful to address the question whether the optimal circadian phase position can be assessed considering the circadian resonance concept, which links longevity to an intermediate morning chronotype. This concept is expected to be indicative of the precise intrinsic circadian clock phenotype in humans [81,137].
4.1. Circadian Markers of Metabolic Health
As was first revealed by self-measurements for body temperature, amplitude and phase disruptions are present in prediabetes and further worsen in diabetes [138]. Actigraphy validates and further develops approaches to quantify metabolic risks related to obesity and diabetes [53,56,61,62,63,139,140]. Again, a smaller circadian amplitude and a delayed phase [62], a weaker coupling between light and activity [56], and a reduced quality of circadian light hygiene, such as excessive evening light [53,63] , are linked to greater metabolic risks. In a study of 84,790 UK Biobank participants wearing light sensors for a week, the circadian amplitude and phase were modeled from light data, showing a relationship between exposure to light at night and type 2 diabetes risk [139]. A higher risk of type 2 diabetes was associated with brighter night light exposure, a smaller circadian amplitude, and a displaced position of the circadian phase, independently of genetic risk factors [139]. In this study, an association was also found between a higher type 2 diabetes risk and lower daytime light levels, which became non-significant when physical activity was included as a co-factor in the model. Given the interplay between physical activity and daylight on the circadian amplitude and robustness [141], it also suggests that physical activity may influence the relationship between light exposure and diabetes risk. However, another mechanism for the association between circadian misalignment and metabolic disorders cannot be ruled out. Zambrano et al. [142] showed that a simultaneous increase in insulin and melatonin levels leads to a deterioration in insulin signal transduction in adipocytes in vitro. It cannot be excluded that a similar effect will be caused by regular consumption of high-glycemic-index food late in the evening/at night, as well as regular intake of pharmacological preparations of melatonin before dinner. Overall, aligned circadian rhythms of physical activity and daylight exposure, with sufficient activity and light exposure during daytime hours, facilitate a strong circadian amplitude and robustness, also of the circadian rhythm in temperature [141,143,144,145,146]. Small amplitudes and shifted phases of circadian rhythms in physical activity are attributes of depressed individuals [147,148,149], and of individuals with binge eating disorder [150]. Fragmentation of the physical activity rhythm was linked to food addiction and emotional eating in young adults [151].
5. Effects of Physical Activity on Health: Daily Amount, Regularity, Timing and Amplitude
Subsequently, we explore the mechanisms that underpin the relationship between scheduled circadian physical activity and the maintenance of proper light hygiene, examining their role in promoting strong and stable circadian rhythms. Physical activity is closely linked to circadian health since it occurs regularly within the active phase of the 24-h rhythm, which is usually daytime for humans. The circadian clock can be entrained not only by light, but also by physical activity and meals [141,152,153]. This means that the timing of these daily routines can influence the body's internal clock, helping to regulate the sleep-wake cycle and other physiological processes. This complex interaction highlights the importance of maintaining consistent routines and healthy habits for overall well-being. Most common health risks related to circadian disruption, such as a reduced amplitude, a delayed phase, increased instability and fragmentation of rhythms, can be mitigated via physical activity. Animal studies showed the stabilizing effect of physical activity on the circadian rhythm [154,155]. The effect of stable circadian activity rhythms for learning and memory was also shown [156,157].
Furthermore, personalized physical activity adjusted for individual differences [158,159], including individual circadian clock features such as phase and amplitude, may both preserve robust circadian rhythms and enhance benefits of physical activity for systemic and mental health [141]. A study showed that similar to light or melatonin, phase response curves to exercise and physical activity exist [160], assuming that scheduled timing of regular physical activity may facilitate circadian phase correction. A high order of “fitness” or robustness of circadian rhythms is generally linked to a younger age and a better health status [11,12]. Recent UK Biobank-based studies found that engaging in moderate physical activity can help reduce the negative influence of both short and long sleep duration on the risk of all-cause mortality and cardiovascular disease [161], and the effect of short sleep on the incidence of type 2 diabetes [162]. The analysis of UK Biobank actigraphy data from 2,324 atrial fibrillation patients revealed that engaging in over 105 minutes of moderate-to-vigorous physical activity weekly reduces the risks of heart failure and all-cause mortality [163]. Intense sporadic “lifestyle physical activity” was correlated with a reduced incidence of cancer risk according to a prospective cohort study analyzing 22,398 self-reported sedentary adults from the UK Biobank accelerometry subsample [164]. Increased activity, even when concentrated within 1 to 2 days each week (“weekend-warrior” patterns), may be effective for improving cardiovascular risk profiles [165]. Similarly, both regular and weekend warrior patterns of moderate physical activity, above the 150 min per week recommended by the WHO, are associated with an equal reduction in Parkinson’s disease risk [166]. Another study suggested a linear relationship between physical activity and cardiovascular health, revealing that individuals with higher levels of physical activity consistently exhibit a reduced risk of cardiovascular disease, with the most substantial benefits observed in those who maintain the highest intensity of activity [167]. A longitudinal analysis of 86,556 UK Biobank participants over an average follow-up of 6 years demonstrated that greater overall physical activity and increased daily step count were significantly linked to a reduced incidence of cancers [168]. In a study of 81,717 UK Biobank participants, it was observed that increased engagement in physical activity correlated with reduced hospitalization risks for nine out of the twenty-five most frequent hospitalization causes, with the most significant risk reductions seen in gallbladder disease, diabetes, and urinary tract infections [169]. In a US cohort study involving 7,607 adults, an increased accumulation of light-intensity and moderate-to-vigorous-intensity physical activities was found to be inversely associated with stroke risk, whereas extended periods of sedentary behavior correlated with an elevated risk [170].
Our body's circadian rhythms govern various physiological processes, including the timing and intensity of physical activity. Disruptions to these rhythms, such as irregular sleep patterns or inconsistent exercise schedules, can have a detrimental effect on mental well-being. Vice versa, regular physical activity can contribute to improved mood, reduced stress levels, and enhanced cognitive functions [171,172,173,174]. Not only aspects of regularity and intensity of exercise were effective to improve health and reduce risks of cardiovascular and metabolic pathologies, timing of exercise is also important [175,176,177]. Recently accumulated evidence underlines benefits of exercise scheduled according to the circadian clock and chronotype, also on metabolic health [158]. Therefore, optimization of regular circadian timing of physical exercise can be an effective way to manage symptoms of anxiety, depression, and other mental health conditions. Aligning physical activity with our body's internal clock can help optimize performance, recovery, and overall psychological well-being. Incorporating exercise into our daily routine at consistent times can help regulate our circadian rhythms, leading to improved sleep quality, increased energy levels, and improved mental clarity. By synchronizing physical activity with our body's natural rhythms, we can promote psychological resilience, enhance brain function, and better cope with the demands of daily life. To date, personalized recommendations for timing exercise, while important, are usually overlooked. In the case of blood pressure, an N-of-1 study showed that exercise in the evening – but not in the morning - increased the 24-h amplitude. Since the participant had an excessive 24-h amplitude of blood pressure, the personalized recommendation was to exercise in the morning, while for others, evening exercise could be beneficial in strengthening a weakened circadian rhythm [178].
6. Molecular Insights on Interaction Between Timed Physical Activity and Brain Health
Regular physical activity and optimally scheduled exercise exert multifaceted effects on health and well-being, helping to improve metabolic health via modulating the lipid profile [152,179,180,181], and reducing inflammation [182]. Optimization of exercise by its timing can be particularly useful for maintaining healthy triglycerides, TG [183], and the ratio between TG and high-density lipids, HDL, since these lipids are closely coupled with circadian factors [53,184,185]. Effects of optimally scheduled physical activity involve the modulation of metabolomics [186], which establishes the molecular background for brain health [182,187]. Even short-term (about 30-min) bouts of physical activity improved inflammatory profiles by increasing adiponectin, while decreasing leptin and interleukin-6 [188], while also increasing brain-derived neurotrophic factor (BDNF) and insulin-like growth factor 1 (IGF-1) [189]. Regular physical activity can influence protein synthesis and breakdown, which can affect the 24-h balance of lipids and amino acids. For instance, scheduled physical activity can provide cardiometabolic protection via stimulating the production of lactoylphenylalanine, or Lac-Phe, by carnosine dipeptidase II (CNDP2) cells in diverse tissues that reduces food intake without affecting motor activity or energy expenditure [190]. It has potential effects on food addiction, mood, depression and anxiety, and it also regulates the timing of food intake, which can be a necessary co-factor for exercise to maintain metabolic health [191,192]. Acute moderate physical exercise improves lipid metabolism via increasing circulating 12,13-dihydroxy-9Z-octadecenoic acid (12,13-diHOME) in men and women of different age groups [193]. Activity modulates regulatory factors of the circadian rhythm (Dbp, Tef, Nr1d2, and Per3) in mesenchymal stem cells, the process that was shown to be crucial for multi-tissue molecular responses to exercise and obesity [194]. Physical activity is coupled with the central carbon metabolism, which involves glycolysis and the pentose-phosphate pathway (PPP) that works to oxidize glucose, resulting in the production of NADH and NADPH. NADPH metabolism modulates circadian rhythm parameters, including the period length of the circadian activity rhythm via the pentose-phosphate pathway [195]. Such interaction between the circadian clock and the timing of physical activity recruits the nuclear factor Nrf2 (erythroid-derived 2)-like 2) pathway. Nrf2 is a transcription factor involved in the expression of over 250 genes, i.e., providing feedback between redox oscillations and the circadian transciptional rhythms through the secondary core-clock loop gene NR1D [195,196]. Nrf2 also affects brain functions, increasing glucose uptake in neurons and astrocytes [197]. Nrf2 is also involved in maintaining large-amplitude circadian rhythms in organs and tissues by regulating expression of the core-clock Cry2 gene [198]. Therefore, major beneficial effects of timed exercise may rely on the interaction between Nrf2 and glucose metabolism [199]. Greater benefits of evening exercise in patients with metabolic disorders is hypothesized to be explained by the Nrf2-dependent activation of the antioxidant response element (ARE) region in skeletal muscles, binding to the promoter region of the interleukin 6 (IL-6) gene. Transcription and translation of IL-6 protein is thereby increased, which then stimulates AMP-activated protein kinase (AMPK), which itself is activated by exercise, and also activates Nrf2, closing this feedback loop [199]. Physical activity activates PPARs (peroxisome proliferator-activated receptors) [200] that help to integrate the circadian clocks with energy metabolism [201] and is expressed in mammalian tissues in a circadian-dependent manner [202]. Given that the balance between these factors differs between morning and evening, the effects of exercise at different times of day also vary [199]. In a mouse model, lifelong exercise exerted geroprotective effects by restoring (mainly by readjusting) the rhythmic machinery via the core circadian clock protein BMAL1 and resetting circadian transcriptomic programs of younger animals, mainly in the central nervous system and vascular endothelial cells [203]. Sustained physical activity exerts profound effects on the endogenous endocannabinoid system that may help to enhance mood and learning abilities, and modulate the endogenous 24-h balance of serotonin, melatonin and dopamine [204], especially in the presence of sufficient outdoor exposure to sunlight [141].
6.1. Weekly Schedules
The optimal time to exercise needs to be personalized not only in terms of daytime, but also on the weekly scale. Currently, there is a lack of agreement regarding the optimal duration, intensity, timing, and frequency of weekly physical activity for health maintenance. For instance, inconsistencies exist between research findings. One study [165] suggests that one to two weekly sessions of physical activity—termed "weekend warrior" sessions—are adequate for reducing cardiovascular risk comparably to physical activity that is more evenly distributed throughout the week. Other studies, however, conclude that such infrequent activity does not achieve an equivalent reduction in the cardiometabolic index [205], or lipid accumulation products [206]. A potential explanation for the differing results might be age of the target population, databases consulted, endpoints used, or the need for individualization. The UK study by Khurshid et al. [165] encompassed individuals aged 40-69 years from the UK Biobank, whereas the research by Xue et al. [205] focused on a distinct cohort from the US National Health and Nutrition Examination Survey (NHANES). The latter study determined that the correlation between physical activity and the cardiometabolic index was more significant in subgroups aged below 45 or above 60.
An additional crucial detail when studying weekly patterns pertains to the infradian rhythms of physical activity. Employing chronobiological and mathematical modeling to meticulously analyze the distribution of intensity patterns across the 24-h span and throughout the week could provide greater insight into this matter.
7. Wearables to Track Circadian Markers in Neurodegenerative Diseases
Alterations in the interaction between light exposure and circadian rhythms can be utilized to track early changes associated with neurobehavioral and neurodegenerative pathologies. Precision measurement is essential to increase statistical power and ensure reproducibility in human neuroscience, potentially revolutionizing the field through enhanced methodological rigor and improved scientific outcomes [207]. Research suggests a significant correlation between metabolic changes and the progression of neurodegenerative diseases. Epidemiological studies have consistently linked conditions like obesity and metabolic disorders to the onset of neurodegenerative diseases [208,209]. Hormones such as leptin, ghrelin, insulin, and IGF-1 play a central role in protecting against neuronal damage, resisting harmful stimuli, and other neurodegenerative mechanisms [209].
In addition to actigraphy, wearable GPS sensors and commercial accelerometers offer a noninvasive method for monitoring the mobility and physical activity of individuals with neurodegenerative disorders, potentially serving as biomarkers for disease tracking and treatment response. Despite challenges in standardizing remote monitoring methods [26], recent research [210] has shown limited use of GPS but extensive application of accelerometers in patients with neurodegenerative disorders, resulting in promising clinical trial outcomes and strong correlations with disease progression and patient activities. The next steps involve standardizing these technologies for broader application and validation of their effectiveness in larger patient populations to improve disease monitoring and management. A meta-analysis of 48 studies on circadian disruption in dementia using wearable technology revealed that adults with dementia exhibit lower activity levels, disrupted sleep-wake patterns, increased fragmentation, and reduced normal daily circadian rhythms compared to non-dementia individuals [211].
The main circadian brain clock synchronizers such as light [212,213] and melatonin [76,77,214,215,216] can be effective in preventing and/or mitigating neuroinflammation and neurodegeneration. Enhancement of circadian light signaling by daytime light exposure and/or melatonin administration at night can improve circadian robustness by increasing the circadian amplitude, aligning the phase, and strengthening signal robustness in overt phenotypic functions, measured by wearables. However, at the moment, very few studies addressed light or melatonin therapies using protocols that are personalized for an individual patient’s circadian phase or chronotype. However, a recent phase-2 clinical trial showed that biologically-directed daylight therapy improved restorative deep sleep in individuals with mild to moderate Parkinson's disease, with no significant difference between controlled daylight and melanopsin booster light [37]. The findings suggest that personalized indoor daylight therapy could be effective in improving sleep in early to moderate stages of the disease, calling for further research in advanced Parkinson's disease.
7.1. Intrinsically Disrupted Circadian Light Hygiene in Neurodegenerative Diseases
We recently reviewed newer actigraphs that are available to assess circadian light hygiene for appearance, dimensions, weight, mounting, battery, sensors, features, communication interface, and software [40]. Actigraphs equipped with light sensors can help to track the intensity and duration of light exposure throughout the day, analyze its effect on circadian rhythms, and adjust an individual's light exposure (circadian light hygiene) according to the recent recommendations [108]. These data help quantify the amount of light a person is exposed to during different times of the day, including natural light from the sun and artificial light sources indoors. The timing of light exposure can be analyzed relative to key circadian markers, such as the onset of melatonin secretion in the evening and the offset of melatonin secretion in the morning. This information helps assess whether individuals' light exposure aligns with their natural circadian rhythms. By correlating light exposure data from actigraphy with sleep patterns, researchers can evaluate how light exposure influences the timing and quality of sleep. In a recent study in Arctic residents [53] during the spring equinox, a higher BMI was found to be linked to higher blue light exposure within distinct time windows and also to a lower wrist temperature MESOR. An evening time window between 9:30 p.m. and 0:30 a.m. was identified when 95% confidence intervals of blue light exposure (BLE) were non-overlapping between groups with a BMI < 25 or BMI > 25 kg/m2. Such link was coupled to the MTNR1B rs10830963 G-allele. A novel Nocturnal Excess Index (NEI) was suggested to estimate evening light overexposure along with the Daylight Deficit Index (DDI), which was associated with morning cortisol values [53]. Another study used a method known as FOSR to divide an average 24-h activity signal into 48 30-minute segments and evaluate differences between two groups within each 30-minute segment. This approach found that the Aβ-positive group exhibited significantly higher activity levels than the Aβ-negative group between 1:00 p.m. and 3:30 p.m. Additionally, by analyzing the standard deviation of activity in each segment, the authors demonstrated that the Aβ-positive group displayed more consistent activity patterns during the early afternoon throughout the recording period [54]. In this study, light exposure was not assessed, although it is likely that episodes of elevated activity and corresponding variability could be attributed to simultaneous differences in light exposure. Indeed, some studies suggest that excessive evening light may be linked to cognitive impairment [217,218]. A characteristic motor activity profile in older adults with dementia has been previously described, termed “sundowning” – an increase in the level of motor activity in the late afternoon [210,220], occurring in approximately 20% of patients with Alzheimer's disease [221].
In neurodegenerative diseases, the function of retinal ganglion cells (RGCs), notably the intrinsically photosensitive cells (ipRGCs), are compromised [222,223,224]. Compromised light signaling due to progressive loss of ganglion cells, including ipRGCs, is most evident in advanced stages of glaucoma, being associated with complex circadian disruptions, including changes in circadian alignment and robustness [74,75,76,77,78,185], altered mood [117], and sleep [74,77,78,225]. Similarly in Alzheimer’s disease, impaired visual function is associated with sleep/wake disorders and cognitive decline [226]. Such alterations can be linked to a decreased amplitude of light-dark alternation, since both melatonin [76,77,78] and daylight [227] mitigate circadian disruptions. Similarly, enhancing spectral lens transmission after cataract replacement improves circadian health [228]. Besides neuroinflammation and neurogeneration, some other factors such as a history of SARS-Cov2 infection may change the susceptibility to circadian light hygiene, likely affecting light perception or sensitivity. A recent study showed that populations with a history of COVID-19 had lower daytime exposure to white, blue, and ultraviolet B light [229]. Those who had poor circadian light hygiene (estimated by a smaller normalized circadian amplitude) were more susceptible to circadian disruptions, manifested as a phase delay, small amplitude, and less robust circadian patterns of activity and delayed sleep. Furthermore, the longer the time elapsed since their COVID-19 diagnosis, the poorer circadian light hygiene the patients had.
7.2. Boosting Brain and Metabolic Health by Clock Enhancing Strategies
Circadian health improvement strategies can balance the timing and amount of melatonin and daylight. Boosting circadian signals through exposure to daylight [37,230,231,232,233,234] or administering melatonin during the nighttime [76,235,236] can strengthen the circadian system. Personalization of dose and timing of melatonin administration can be most important for its effective supplementation. Improving the lighting conditions in the surroundings with adaptable lighting systems positively influenced the mood and behavior of elderly individuals [234,237]. In agreement with phase-response curves [238,239,240], morning/daytime light and evening/nocturnal melatonin facilitate circadian phase advancements, preventing complex negative aspects of late chronotypes [241,242,243,244]. The combination of light therapy with melatonin [245,246] or physical activity [247] can be effective in neurodegenerative diseases. Also promising is timed physical activity [248]. Light regularity may help to maintain sleep regularity, even in healthy young adults [249]. Overall, circadian health rescue or enhancement implies maintenance of due amplitude, phase alignment and stability of the signals that govern overt bodily functions (activity, temperature, heart rate, blood pressure, etc.), trackable by wearable devices.
8. Perspectives of Actigraphy-Compatible Wearable Technologies / Next-Generation Comprehensive Monitoring Systems
The simultaneous tracking of different physiological variables provides a more complete picture of an individual's circadian health status. The ability to detect subtle changes in physiological and neurological patterns could lead to earlier and more accurate diagnoses of conditions like sleep disorders, depression, neurodegenerative or metabolic diseases. For research and diagnostic purposes, this integrated approach would require effective methods for combining data from different sources while maintaining data integrity, advanced computational methods to analyze the complex data, ways to extract meaningful patterns, and a strategy to rigorously test the results thus obtained and validate the clinical relevance of the findings.
8.1. Perspective Options
Focus on extra-circadian frequency domains: ultradian rhythms, or biological rhythms with a period shorter than 24 h, can reflect various physiological and neurological functions. Ultradian fluctuations in brain functions [47,250,251] are under-investigated, though a promising area of research that can utilize ultradian fluctuations and their beat harmonics to untangle complex interactions for a better understanding of biological processes and diagnostics applications. Beat harmonics refer to the composite frequencies produced when two or more ultradian rhythms interact, much like the overlapping waves in acoustics that create a new rhythm or 'beat,' providing deeper insights into the synchronization of biological rhythms. Furthermore, in-sync vs. out-of-sync ultradian harmonics may have different outputs such as non-overlapping lower-frequency oscillations that can be meaningful. The concept of using data from wearables to investigate extra-circadian modulations is innovative and holds potential for advancing medical diagnostics.
8.2. Novel Sensors
For example, integrating variables obtained by photoplethysmography [252,253,254,255,256,257] or functional near-infrared spectroscopy (fNIRS) [258,259] with next-generation wearables may offer a comprehensive approach to monitoring and analyzing physiological and neurological functions. fNIRS stands out as a hemodynamics method that offers significant advantages [260], particularly in terms of its portability and greater motion tolerance, areas where functional magnetic resonance imaging (fMRI) faces constraints [261]. Wearable fNIRS could be applied to better understand time-specified windows of global vs. local brain signal fluctuations and functional connectivity, as suggested by previous fMRI studies [262,263].The analysis of ECG data in specific frequency domains also offer insight into the functioning of specific brain areas [264,265,266,267,268].
8.3. Biochemical Analyses
Biochemical analyses are being developed and can be integrated in wearables in the proximal future [20,269,270,271,272,273,274,275]. Sweat-based wearable-enabling technology was recently proposed to track cortisol [276] and inflammation markers such as interleukin-1β and C-reactive protein [270,271]. To advance the understanding of perspiration's role in thermoregulation and its applied use for physiological monitoring, innovative microfluidic patches with hierarchical superhydrophilic biosponges and integrated sensors should be adopted for efficient, real-time sweat analysis during various activities and conditions [277]. Cutting-edge wearable technologies will have the capability to track the golden standard circadian phase marker, melatonin, but also leptin and ghrelin [20].
8.4. Improving Light Exposure Monitoring and Analytics
Melanopic Equivalent Daylight Illuminance (mEDI) is a metric used to quantify the effect of light on the melanopsin-containing intrinsically photosensitive retinal ganglion cells (ipRGCs) in the human eye [108,278,279,280,281]. These cells have a peak sensitivity in the shorter wavelength part of the visible spectrum and play an important role in regulating circadian rhythms. Melanopic EDI measures the effectiveness of light in stimulating these cells, relative to a standard daylight (D65) condition. It is a valuable measure for understanding how different light sources affect our biological clock and other non-image-forming (NIF) effects of light. To accurately determine the melanopic EDI, it is essential to measure irradiance and the spectral distribution of a light source. This is of importance because the color temperature of daylight fluctuates depending on the time of day and light sources found in various home environments and offices may have different spectral compositions. Further advancements in actigraphy capable of measuring the spectral distribution or directly the melanopic EDI are necessary for this purpose. Furthermore, positioning wearable light loggers or dosimeters closer to the eyes, such as with the lido [282] can refine the assessment of light exposure.
8.5. Future of Light Dosimeters as Wearable-Friendly Add-Ons
Understanding the user’s challenges of wearing light dosimeters is key to designing more acceptable devices and supporting research into light exposure and its effects on health and behavior. To improve the wearer’s experience and compliance, and therefore data quality, the device should be designed to be unobtrusive. Devices should be adapted to the needs of different patient populations and mounting / body location methods. In addition, comprehensive user training and motivational incentives can improve compliance of the wearer. The implementation of these recommendations will improve the quality of data collected by wearable light loggers. While most actigraph models cannot measure melanopic EDI directly, some are equipped with RGB light sensors [40]. For an overview of current wearable light loggers and their specifications, see [279]. Devices like the ActTrust, for example, can also monitor light intensity in the ultraviolet A (UVA), ultraviolet B (UVB) and infrared (IR) wavelength ranges. While this feature has not been extensively explored yet, the ability to gather precise data on UV and IR light exposure in real-time holds significant potential for various health and therapeutic uses [283,284,285]. For instance, it could be instrumental in managing conditions such as autoimmune diseases, mood and metabolic disorders, as well as addictions [286,287]. Scientifically valid information on UV exposure can also be collected by commercially available wearables [288]. Clinical records underscore the role of circadian rhythms in determining health results and guiding medical procedures, especially when using data from electronic health records. Yet, due to the lack of uniformity in collection methods and equipment, harnessing electronic health records for chronomedicine demands addressing built-in biases and data patterns unrelated to biology [289]. The precision of light logging can be further enhanced by improving light sensors and rendering their position closer to the eyes [282]. Improving their metrology [290] should improve the assessment of physiological effects of natural light and human-centric light technologies [291].
Many commercial light loggers lack transparency in critical technical aspects such as sensor types and data processing methods. This opacity can lead to inaccuracies, undetected errors, or incomplete data sets, making it difficult to ensure the accuracy and comparability of results between different devices. As a result, there is an urgent need for a standardized methodology to collect and analyze data from wearable light loggers. The project 'Metrology for Wearable Light Loggers and Optical Radiation Dosimeters' (22NRM05, MeLiDos) will develop the measurement and data analysis methods needed to characterize and validate wearable light loggers. In addition, The JTC 20 (D6/D2) technical report on wearable alpha-optic dosimetry and light logging will provide a comprehensive review of current practices in the scientific literature. Additional sensors incorporating heart rate [292], oxygen saturation [293,294], and functional near-infrared spectroscopy techniques fNIRS [295,296] may enhance the informative capacity of wearable technologies for digital phenotyping in the near future. Despite their limited precision, commercially available smartphones-compatible wearables are already used to evaluate sleep disorders, cardiometabolic, mental health and well-being, but the lack of standardization is causing marked disagreement between devices [297,298,299,300,301].
Furthermore, reference standards aid in the development of diagnostic criteria and treatment guidelines for sleep-related conditions. They serve as benchmarks for assessing treatment efficacy and monitoring patient progress over time. Overall, the development of reference standards for actigraphy-based indices enhances the utility of actigraphy in clinical practice and research, ultimately improving our understanding of sleep and circadian rhythms and advancing personalized approaches to healthcare.

Table 2.
Most common forms of circadian disruptions: typical and alternative features.
| Circadian disruption marker | Typical deviation | Alternatives / Comments |
|---|---|---|
| Circadian rhythm measures | ||
| Amplitude | ↓ [11,12,36,38,56,61,62,66,67,68,74,118,119,120,121,122,123,124,132,138,139,147,148,149,150] |
↑ Transient elevation of amplitude due to jet lag, or shift-work, over-swinging functions such as blood pressure [111,113,302,303] |
| Phase | Delay → [61,74,120,125,129,133,139,147,148,149] |
Both delay → or advance ← (optimal phase position is determined by circadian clock precision [76,133,143,148] |
| Waveform (circadian robustness) | Reduced fitness of the curve to predictable best-fitted model [36,61,62,120] |
Flexibility rather than rigidity can be useful for adaptive needs, i.e., heart rate variability |
| Variability measures | ||
| Fragmentation and regularity (activity and sleep) |
IV (Intra-daily Variability)↑ IS (Inter-daily Stability) ↓ [38,51,61,62,69,120,122,123,132,147] |
Can be beneficial in certain cases such as short-term adaptation requiring high vigilance [38,51,61,62,69,120,122,123,132,147] Large inter- and intra-individual differences in the duration of sleep cycles throughout the night [46,47] |
| Spectral composition | Extra-circadian dissemination (ECD): ratio between circadian and non-circadian (ultradian / infradian) amplitudes ↓ [2,10,11,12,236] |
Some ultradian and infradian components are built-in and beneficial for health [47,306,307,308,309,310] |
| Alignment | Misalignment: disturbed phase relationship between circadian marker rhythms [55,56,75] |
Optimal phase angles may vary depending on genotype, age, light environment: season and latitude; and meal timing if peripheral rhythms’ phases are considered. |
| Composite markers (Area Under Curev), AUCs; Function-On-Scalar regression (FOSR), etc. | ↑ or ↓ [53,54,63,109,124,311,312] |
Optimal reference curves may depend on genotype, age, light environment: season and latitude; and meal timing if peripheral rhythms’ phases are considered. |
| Social Jet Lag | ↑ [99,100,101,102,103,104,105,106] |
Largely varies with age [103] and social obligations [313], may depend on the number of actual working days per week. All these factors can modify hazards of SJL for health. |
Author Contributions
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following statements should be used “Conceptualization, X.X. and Y.Y.; methodology, X.X.; software, X.X.; validation, X.X., Y.Y. and Z.Z.; formal analysis, X.X.; investigation, X.X.; resources, X.X.; data curation, X.X.; writing—original draft preparation, X.X.; writing—review and editing, X.X.; visualization, X.X.; supervision, X.X.; project administration, X.X.; funding acquisition, Y.Y. All authors have read and agreed to the published version of the manuscript.” Please turn to the CRediT taxonomy for the term explanation. Authorship must be limited to those who have contributed substantially to the work reported.
Funding
This study was supported by the West-Siberian Science and Education Center, Government of Tyumen District, Decree of 20.11.2020, No. 928-rp. The funding organizations had no role in the design or conduct of this research. The author(s) have no proprietary or commercial interest in any materials discussed in this article.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
This a review which did not generate novel data.
Conflicts of Interest
The authors declare no conflicts of interest. The funder had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- López-Otín C, Kroemer G. Hallmarks of health. Cell. 2021 Apr 1;184(7):1929-1939. [CrossRef]
- Agadzhanian NA, Gubin DG. Desinkhronoz: mekhanizmy razvitiia ot molekuliarno-geneticheskogo do organizmennogo urovnia [Desynchronization: mechanisms of development from molecular to systemic levels]. Usp Fiziol Nauk. 2004 Apr-Jun;35(2):57-72. Russian.
- Cornelissen G, Otsuka K. Chronobiology of aging: a mini-review. Gerontology 2017; 63 (2): 118-128. [CrossRef]
- Cederroth CR, Albrecht U, Bass J, Brown SA, Dyhrfjeld-Johnsen J, Gachon F, Green CB, Hastings MH, Helfrich-Förster C, Hogenesch JB, Lévi F, Loudon A, Lundkvist GB, Meijer JH, Rosbash M, Takahashi JS, Young M, Canlon B. Medicine in the Fourth Dimension. Cell Metab. 2019 Aug 6;30(2):238-250. [CrossRef]
- Fishbein AB, Knutson KL, Zee PC. Circadian disruption and human health. J Clin Invest. 2021 Oct 1;131(19):e148286. [CrossRef]
- Roenneberg T, Foster RG, Klerman EB. The circadian system, sleep, and the health/disease balance: a conceptual review. J Sleep Res. 2022 Aug;31(4):e13621. [CrossRef]
- Gubin, D. Chronotherapeutic Approaches, in Chronobiology and Chronomedicine: From Molecular and Cellular Mechanisms to Whole Body Interdigitating Networks, ed. G. Cornelissen and T. Hirota, Royal Society of Chemistry, 2024, vol. 23, ch. 21, pp. 536–577. [CrossRef]
- Allada R, Bass J. Circadian Mechanisms in Medicine. N Engl J Med. 2021 Feb 11;384(6):550-561. [CrossRef]
- Kramer A, Lange T, Spies C, Finger AM, Berg D, Oster H. Foundations of circadian medicine. PLoS Biol. 2022 Mar 24;20(3):e3001567. [CrossRef]
- Gubin, DG. [Molecular basis of circadian rhythms and principles of circadian disruption]. Usp Fiziol Nauk. 2013 Oct-Dec;44(4):65-87. Russian.
- Gubin D, Cornelissen G, Weinert D, et al. Circadian disruption and Vascular Variability Disorders (VVD) — mechanisms linking aging, disease state and Arctic shift-work: applications for chronotherapy. World Heart J. 2013;5(4):285-306.
- Gubin DG, Weinert D, Bolotnova TV. Age-Dependent Changes of the Temporal Order--Causes and Treatment. Curr Aging Sci. 2016;9(1):14-25. [CrossRef]
- Cornelissen, G. Cosinor-based rhythmometry. Theor Biol Med Model. 2014 Apr 11;11:16. [CrossRef]
- Weinert, D. and Gubin D. Chronobiological Study Designs. in Chronobiology and Chronomedicine From Molecular and Cellular Mechanisms to Whole Body Interdigitating Networks, ed. G. Cornelissen and T. Hirota, Royal Society of Chemistry, 2024, vol. 23, ch. 22, pp. 579–609. [CrossRef]
- Usmani IM, Dijk DJ, Skeldon AC. Mathematical Analysis of Light-sensitivity Related Challenges in Assessment of the Intrinsic Period of the Human Circadian Pacemaker. J Biol Rhythms. 2024 Apr;39(2):166-182. [CrossRef]
- Kräuchi K, Cajochen C, Werth E, Wirz-Justice A. Functional link between distal vasodilation and sleep-onset latency? Am J Physiol Regul Integr Comp Physiol. 2000278(3):R741-8. [CrossRef]
- Kräuchi, K. The thermophysiological cascade leading to sleep initiation in relation to phase of entrainment. Sleep Med Rev. 2007;11(6):439-51. [CrossRef]
- Depner CM, Cheng PC, Devine JK, Khosla S, de Zambotti M, Robillard R, Vakulin A, Drummond SPA. Wearable technologies for developing sleep and circadian biomarkers: a summary of workshop discussions. Sleep. 2020 Feb 13;43(2):zsz254. [CrossRef]
- Li X, Kane M, Zhang Y, Sun W, Song Y, Dong S, Lin Q, Zhu Q, Jiang F, Zhao H. Circadian Rhythm Analysis Using Wearable Device Data: Novel Penalized Machine Learning Approach. J Med Internet Res. 2021 Oct 14;23(10):e18403. [CrossRef]
- Lujan MR, Perez-Pozuelo I, Grandner MA. Past, Present, and Future of Multisensory Wearable Technology to Monitor Sleep and Circadian Rhythms. Front Digit Health. 2021 Aug 16;3:721919. [CrossRef]
- Shandhi MMH, Wang WK, Dunn J. Taking the time for our bodies: How wearables can be used to assess circadian physiology. Cell Rep Methods. 2021 Aug 23;1(4):100067. [CrossRef]
- Tobin SY, Williams PG, Baron KG, Halliday TM, Depner CM. Challenges and Opportunities for Applying Wearable Technology to Sleep. Sleep Med Clin. 2021 Dec;16(4):607-618. [CrossRef]
- Lin C, Chen IM, Chuang HH, Wang ZW, Lin HH, Lin YH. Examining Human-Smartphone Interaction as a Proxy for Circadian Rhythm in Patients With Insomnia: Cross-Sectional Study. J Med Internet Res. 2023 Dec 15;25:e48044. [CrossRef]
- de Zambotti M, Goldstein C, Cook J, Menghini L, Altini M, Cheng P, Robillard R. State of the science and recommendations for using wearable technology in sleep and circadian research. Sleep. 2024 Apr 12;47(4):zsad325. [CrossRef]
- Moorthy P, Weinert L, Schüttler C, Svensson L, Sedlmayr B, Müller J, Nagel T. Attributes, Methods, and Frameworks Used to Evaluate Wearables and Their Companion mHealth Apps: Scoping Review. JMIR Mhealth Uhealth. 2024 Apr 5;12:e52179. [CrossRef]
- Della Monica C, Ravindran KKG, Atzori G, Lambert DJ, Rodriguez T, Mahvash-Mohammadi S, Bartsch U, Skeldon AC, Wells K, Hampshire A, Nilforooshan R, Hassanin H, The Uk Dementia Research Institute Care Research Amp Technology Research Group, Revell VL, Dijk DJ. A Protocol for Evaluating Digital Technology for Monitoring Sleep and Circadian Rhythms in Older People and People Living with Dementia in the Community. Clocks Sleep. 2024 Feb 29;6(1):129-155. [CrossRef]
- Sun H, Ganglberger W, Panneerselvam E, Leone MJ, Quadri SA, Goparaju B, Tesh RA, Akeju O, Thomas RJ, Westover MB. Sleep staging from electrocardiography and respiration with deep learning. Sleep. 2020; 43(7):zsz306. [CrossRef]
- Kranzinger, S., Baron, S., Kranzinger, C., Heib, D., & Borgelt, C. Generalisability of sleep stage classification based on interbeat intervals: validating three machine learning approaches on self-recorded test data. Behaviormetrika, 2024. 51(1), 341-358. [CrossRef]
- Kripke DF, Mullaney DJ, Messin S, Wyborney VG. Wrist actigraphic measures of sleep and rhythms. Electroencephalogr Clin Neurophysiol. 1978 May;44(5):674-6. [CrossRef]
- Wilde-Frenz J, Schulz H. Rate and distribution of body movements during sleep in humans. Percept Mot Skills. 1983 Feb;56(1):275-83. [CrossRef]
- Borbély, AA. New techniques for the analysis of the human sleep-wake cycle. Brain Dev. 1986;8(4):482-8. [CrossRef]
- Ancoli-Israel S, Cole R, Alessi C, Chambers M, Moorcroft W, Pollak CP. The role of actigraphy in the study of sleep and circadian rhythms. Sleep. 2003 May 1;26(3):342-92. [CrossRef]
- Patterson MR, Nunes AAS, Gerstel D, Pilkar R, Guthrie T, Neishabouri A, Guo CC. 40 years of actigraphy in sleep medicine and current state of the art algorithms. NPJ Digit Med. 2023 Mar 24;6(1):51. [CrossRef]
- Lévi F, Zidani R, Misset JL. Randomised multicentre trial of chronotherapy with oxaliplatin, fluorouracil, and folinic acid in metastatic colorectal cancer. International Organization for Cancer Chronotherapy. Lancet. 1997; 350(9079):681-6. [CrossRef]
- Kramer, G.; Dominguez-Vega, Z.T.; Laarhoven, H.S.; Brandsma, R.; Smit, M.; van der Stouwe, A.M.; Elting, J.W.J.; Maurits, N.M.; Rosmalen, J.G.; Tijssen, M.A. Similar association between objective and subjective symptoms in functional and organic tremor. Park. Relat. Disord. 2019, 64, 2–7. [Google Scholar] [CrossRef] [PubMed]
- Leng, Y., Blackwell T., Cawthon P.M., Ancoli-Israel S., Stone K.L., Yaffe K. Association of circadian abnormalities in older adults with an increased risk of developing Parkinson disease. JAMA Neurol. 2020;77:1270–1278. [CrossRef]
- Feigl B, Lewis SJG, Burr LD, Schweitzer D, Gnyawali S, Vagenas D, Carter DD, Zele AJ. Efficacy of biologically-directed daylight therapy on sleep and circadian rhythm in Parkinson's disease: a randomised, double-blind, parallel-group, active-controlled, phase 2 clinical trial. EClinicalMedicine. 2024 Feb 10;69:102474. [CrossRef]
- Winer JR, Lok R, Weed L, He Z, Poston KL, Mormino EC, Zeitzer JM. Impaired 24-h activity patterns are associated with an increased risk of Alzheimer's disease, Parkinson's disease, and cognitive decline. Alzheimers Res Ther. 2024 Feb 14;16(1):35. [CrossRef]
- Migueles JH, Cadenas-Sanchez C, Ekelund U, Delisle Nyström C, Mora-Gonzalez J, Löf M, Labayen I, Ruiz JR, Ortega FB. Accelerometer Data Collection and Processing Criteria to Assess Physical Activity and Other Outcomes: A Systematic Review and Practical Considerations. Sports Med. 2017 Sep;47(9):1821-1845. [CrossRef]
- Danilenko KV, Stefani O, Voronin KA, Mezhakova MS, Petrov IM, Borisenkov MF, Markov AA, Gubin DG. Wearable Light-and-Motion Dataloggers for Sleep/Wake Research: A Review. Applied Sciences. 2022; 12(22):11794. [CrossRef]
- Blackwell T, Redline S, Ancoli-Israel S, Schneider JL, Surovec S, Johnson NL, Cauley JA, Stone KL; Study of Osteoporotic Fractures Research Group. Comparison of sleep parameters from actigraphy and polysomnography in older women: the SOF study. Sleep. 2008 Feb;31(2):283-91. [CrossRef]
- Quante M, Kaplan ER, Cailler M, Rueschman M, Wang R, Weng J, Taveras EM, Redline S. Actigraphy-based sleep estimation in adolescents and adults: a comparison with polysomnography using two scoring algorithms. Nat Sci Sleep. 2018 Jan 18;10:13-20. [CrossRef]
- Smith MT, McCrae CS, Cheung J, Martin JL, Harrod CG, Heald JL, Carden KA. Use of Actigraphy for the Evaluation of Sleep Disorders and Circadian Rhythm Sleep-Wake Disorders: An American Academy of Sleep Medicine Systematic Review, Meta-Analysis, and GRADE Assessment. J Clin Sleep Med. 2018 Jul 15;14(7):1209-1230. [CrossRef]
- Fekedulegn D, Andrew ME, Shi M, Violanti JM, Knox S, Innes KE. Actigraphy-Based Assessment of Sleep Parameters. Ann Work Expo Health. 2020 Apr 30;64(4):350-367. [CrossRef]
- Lehrer HM, Yao Z, Krafty RT, Evans MA, Buysse DJ, Kravitz HM, Matthews KA, Gold EB, Harlow SD, Samuelsson LB, Hall MH. Comparing polysomnography, actigraphy, and sleep diary in the home environment: The Study of Women's Health Across the Nation (SWAN) Sleep Study. Sleep Adv. 2022 Feb 19;3(1):zpac001. [CrossRef]
- Winnebeck EC, Fischer D, Leise T, Roenneberg T. Dynamics and Ultradian Structure of Human Sleep in Real Life. Curr Biol. 2018 Jan 8;28(1):49-59.e5. [CrossRef]
- Cajochen C, Reichert CF, Münch M, Gabel V, Stefani O, Chellappa SL, Schmidt C. Ultradian sleep cycles: Frequency, duration, and associations with individual and environmental factors-A retrospective study. Sleep Health. 2024 Feb;10(1S):S52-S62. [CrossRef]
- Witting W, Kwa IH, Eikelenboom P, Mirmiran M, Swaab DF. Alterations in the circadian rest-activity rhythm in aging and Alzheimer's disease. Biol Psychiatry. 1990 Mar 15;27(6):563-72. [CrossRef]
- Van Someren EJ, Swaab DF, Colenda CC, Cohen W, McCall WV, Rosenquist PB. Bright light therapy: improved sensitivity to its effects on rest-activity rhythms in Alzheimer patients by application of nonparametric methods. Chronobiol Int. 1999 Jul;16(4):505-18. [CrossRef]
- Ortiz-Tudela E, Martinez-Nicolas A, Campos M, Rol MÁ, Madrid JA. A new integrated variable based on thermometry, actimetry and body position (TAP) to evaluate circadian system status in humans. PLoS Comput Biol. 2010 Nov 11;6(11):e1000996. [CrossRef]
- Borisenkov M, Tserne T, Bakutova L, Gubin D. Actimetry-Derived 24 h Rest–Activity Rhythm Indices Applied to Predict MCTQ and PSQI. Applied Sciences. 2022; 12(14):6888. [CrossRef]
- Danilevicz, I., van Hees, V., van der Heide, F. et al. Measures of fragmentation of rest activity patterns: mathematical properties and interpretability based on accelerometer real life data. BMC Med Res Methodol 24, 132. 2024. [CrossRef]
- Gubin D, Danilenko K, Stefani O, Kolomeichuk S, Markov A, Petrov I, Voronin K, Mezhakova M, Borisenkov M, Shigabaeva A, et al. Blue Light and Temperature Actigraphy Measures Predicting Metabolic Health Are Linked to Melatonin Receptor Polymorphism. Biology. 2024; 13(1):22. [CrossRef]
- Spira AP, Liu F, Zipunnikov V, et al. Evaluating a Novel 24-Hour Rest/Activity rhythm marker of preclinical β-Amyloid deposition. Sleep. 2024;47(5):1–8. [CrossRef]
- Blackwell TL, Figueiro MG, Tranah GJ, Zeitzer JM, Yaffe K, Ancoli-Israel S, Kado DM, Ensrud KE, Lane NE, Leng Y, Stone KL; Osteoporotic Fractures in Men (MrOS) Study Group. Associations of 24-Hour Light Exposure and Activity Patterns and Risk of Cognitive Impairment and Decline in Older Men: The MrOS Sleep Study. J Gerontol A Biol Sci Med Sci. 2023 Oct 9;78(10):1834-1843. [CrossRef]
- Xiao Q, Durbin J, Bauer C, Yeung CHC, Figueiro MG. Alignment Between 24-h Light-Dark and Activity-Rest Rhythms Is Associated With Diabetes and Glucose Metabolism in a Nationally Representative Sample of American Adults. Diabetes Care. 2023 Dec 1;46(12):2171-2179. [CrossRef]
- Zimmet P, Alberti KGMM, Stern N, Bilu C, El-Osta A, Einat H, Kronfeld-Schor N. The Circadian Syndrome: is the Metabolic Syndrome and much more! J Intern Med. 2019 Aug;286(2):181-191. [CrossRef]
- Shi Z, Tuomilehto J, Kronfeld-Schor N, Alberti G, Stern N, El-Osta A, Chai Z, Bilu C, Einat H, Zimmet P. The Circadian Syndrome Is a Significant and Stronger Predictor for Cardiovascular Disease than the Metabolic Syndrome-The NHANES Survey during 2005-2016. Nutrients. 2022 Dec 14;14(24):5317. [CrossRef]
- Whitaker KM, Lutsey PL, Ogilvie RP, Pankow JS, Bertoni A, Michos ED, Punjabi N, Redline S. Associations between polysomnography and actigraphy-based sleep indices and glycemic control among those with and without type 2 diabetes: the Multi-Ethnic Study of Atherosclerosis. Sleep. 2018 Nov 1;41(11):zsy172. [CrossRef]
- Huang T, Redline S. Cross-sectional and Prospective Associations of Actigraphy-Assessed Sleep Regularity With Metabolic Abnormalities: The Multi-Ethnic Study of Atherosclerosis. Diabetes Care. 2019 Aug;42(8):1422-1429. [CrossRef]
- Xiao Q, Qian J, Evans DS, Redline S, Lane NE, Ancoli-Israel S, Scheer FAJL, Stone K; Osteoporotic Fractures in Men (MrOS) Study Group. Cross-sectional and Prospective Associations of Rest-Activity Rhythms With Metabolic Markers and Type 2 Diabetes in Older Men. Diabetes Care. 2020 Nov;43(11):2702-2712. [CrossRef]
- Xiao Q, Matthews CE, Playdon M, Bauer C. The association between rest-activity rhythms and glycemic markers: the US National Health and Nutrition Examination Survey, 2011-2014. Sleep. 2022 Feb 14;45(2):zsab291. [CrossRef]
- Kim M, Vu TH, Maas MB, Braun RI, Wolf MS, Roenneberg T, Daviglus ML, Reid KJ, Zee PC. Light at night in older age is associated with obesity, diabetes, and hypertension. Sleep. 2023 Mar 9;46(3):zsac130. [CrossRef]
- Wallace DA, Qiu X, Schwartz J, Huang T, Scheer FAJL, Redline S, Sofer T. Light exposure during sleep is bidirectionally associated with irregular sleep timing: The multi-ethnic study of atherosclerosis (MESA). Environ Pollut. 2024 Mar 1;344:123258. [CrossRef]
- Gubin GD, Weinert D. Bioritmy i vozrast [Biorhythms and age]. Usp Fiziol Nauk. 1991 Jan-Feb;22(1):77-96. Russian.
- Gubin D, Cornélissen G, Halberg F, Gubin G, Uezono K, Kawasaki T. The human blood pressure chronome: a biological gauge of aging. In Vivo. 1997 Nov-Dec;11(6):485-94.
- Abbott SM, Malkani RG, Zee PC. Circadian disruption and human health: A bidirectional relationship. Eur J Neurosci. 2020 Jan;51(1):567-583. [CrossRef]
- Xu Y, Wang X, Belsky DW, McCall WV, Liu Y, Su S. Blunted Rest-Activity Circadian Rhythm Is Associated With Increased Rate of Biological Aging: An Analysis of NHANES 2011-2014. J Gerontol A Biol Sci Med Sci. 2023 Mar 1;78(3):407-413. [CrossRef]
- Cribb L, Sha R, Yiallourou S, Grima NA, Cavuoto M, Baril AA, Pase MP. Sleep regularity and mortality: a prospective analysis in the UK Biobank. Elife. 2023 Nov 23;12:RP88359. [CrossRef]
- Najjar RP, Wolf L, Taillard J, Schlangen LJ, Salam A, Cajochen C, Gronfier C. Chronic artificial blue-enriched white light is an effective countermeasure to delayed circadian phase and neurobehavioral decrements. PLoS One. 2014 Jul 29;9(7):e102827. [CrossRef]
- Baron KG, Reid KJ. Circadian misalignment and health. Int Rev Psychiatry. 2014 Apr;26(2):139-54. [CrossRef]
- Potter GD, Skene DJ, Arendt J, Cade JE, Grant PJ, Hardie LJ. Circadian Rhythm and Sleep Disruption: Causes, Metabolic Consequences, and Countermeasures. Endocr Rev. 2016 Dec;37(6):584-608. [CrossRef]
- Blume C, Garbazza C, Spitschan M. Effects of light on human circadian rhythms, sleep and mood. Somnologie (Berl). 2019 Sep;23(3):147-156. [CrossRef]
- Gubin DG, Malishevskaya ТN, Astakhov YS, Astakhov SY, Cornelissen G, Kuznetsov VA, Weinert D. Progressive retinal ganglion cell loss in primary open-angle glaucoma is associated with temperature circadian rhythm phase delay and compromised sleep. Chronobiol Int. 2019 Apr;36(4):564-577. [CrossRef]
- Neroev V, Malishevskaya T, Weinert D, Astakhov S, Kolomeichuk S, Cornelissen G, Kabitskaya Y, Boiko E, Nemtsova I, Gubin D. Disruption of 24-Hour Rhythm in Intraocular Pressure Correlates with Retinal Ganglion Cell Loss in Glaucoma. Int J Mol Sci. 2020 Dec 31;22(1):359. [CrossRef]
- Gubin D, Neroev V, Malishevskaya T, Cornelissen G, Astakhov SY, Kolomeichuk S, Yuzhakova N, Kabitskaya Y, Weinert D. Melatonin mitigates disrupted circadian rhythms, lowers intraocular pressure, and improves retinal ganglion cells function in glaucoma. J Pineal Res. 2021 May;70(4):e12730. [CrossRef]
- Gubin D, Weinert D. Melatonin, circadian rhythms and glaucoma: current perspective. Neural Regen Res. 2022 Aug;17(8):1759-1760. [CrossRef]
- Gubin, D., Malishevskaya T., Weinert D., Zaharova E., Astakhov S., Cornelissen G. Circadian Disruption in Glaucoma: Causes, Consequences, and Countermeasures. Frontiers in Biosciences-Landmark. 2024. 11. accepted. [CrossRef]
- Albrecht, U. 2012. Timing to perfection: the biology of central and peripheral circadian clocks. Neuron 74, 246–260. [CrossRef]
- Foster, RG. Sleep, circadian rhythms and health. Interface Focus. 2020 Jun 6;10(3):20190098. [CrossRef]
- Gubin DG, Kolomeichuk S N Weinert D. Circadian clock precision, health, and longevity. J. Chronomed. 2021;23 (1):3-15. [CrossRef]
- Dement W, Kleitman N. Cyclic variations in EEG during sleep and their relation to eye movements, body motility, and dreaming. Electroencephalogr Clin Neurophysiol. 1957 Nov;9(4):673-90. [CrossRef]
- Levi F, Halberg F. Circaseptan (about-7-day) bioperiodicity--spontaneous and reactive--and the search for pacemakers. Ric Clin Lab. 1982 Apr-Jun;12(2):323-70. [CrossRef]
- Coskun A, Zarepour A, Zarrabi A. Physiological Rhythms and Biological Variation of Biomolecules: The Road to Personalized Laboratory Medicine. Int J Mol Sci. 2023 Mar 27;24(7):6275. [CrossRef]
- Madden KM, Feldman B. Weekly, Seasonal, and Geographic Patterns in Health Contemplations About Sundown Syndrome: An Ecological Correlational Study. JMIR Aging. 2019 May 28;2(1):e13302. [CrossRef]
- Seizer L, Cornélissen-Guillaume G, Schiepek GK, Chamson E, Bliem HR, Schubert C. About-Weekly Pattern in the Dynamic Complexity of a Healthy Subject's Cellular Immune Activity: A Biopsychosocial Analysis. Front Psychiatry. 2022 Jun 20;13:799214. [CrossRef]
- Cornelissen, G., Hirota T. Quo Vadis. in Chronobiology and ChronomedicineFrom Molecular and Cellular Mechanisms to Whole Body Interdigitating Networks, ed. G. Cornelissen and T. Hirota, Royal Society of Chemistry, 2024, vol. 23, ch. 24, pp. 648–664.
- Reinberg AE, Dejardin L, Smolensky MH, Touitou Y. Seven-day human biological rhythms: An expedition in search of their origin, synchronization, functional advantage, adaptive value and clinical relevance. Chronobiol Int. 2017;34(2):162-191. [CrossRef]
- Cajochen C, Altanay-Ekici S, Münch M, Frey S, Knoblauch V, Wirz-Justice A. Evidence that the lunar cycle influences human sleep. Curr Biol. 2013 Aug 5;23(15):1485-8. [CrossRef]
- Reinberg A, Smolensky MH, Touitou Y. The full moon as a synchronizer of circa-monthly biological rhythms: Chronobiologic perspectives based on multidisciplinary naturalistic research. Chronobiol Int. 2016;33(5):465-79. [CrossRef]
- Hartstein LE, Wright KP Jr, Akacem LD, Diniz Behn C, LeBourgeois MK. Evidence of circalunar rhythmicity in young children's evening melatonin levels. J Sleep Res. 2023 Apr;32(2):e13635. [CrossRef]
- Van Someren, EJ. More than a marker: interaction between the circadian regulation of temperature and sleep, age-related changes, and treatment possibilities. Chronobiol Int. 2000 May;17(3):313-54. [CrossRef]
- Gompper B, Bromundt V, Orgül S, Flammer J, Kräuchi K. Phase relationship between skin temperature and sleep-wake rhythms in women with vascular dysregulation and controls under real-life conditions. Chronobiol Int. 2010 Oct;27(9-10):1778-96. [CrossRef]
- Bonmati-Carrion MA, Middleton B, Revell V, Skene DJ, Rol MA, Madrid JA. Circadian phase assessment by ambulatory monitoring in humans: correlation with dim light melatonin onset. Chronobiol Int. 2014 Feb;31(1):37-51. [CrossRef]
- Reid, KJ. Assessment of Circadian Rhythms. Neurol Clin. 2019 Aug;37(3):505-526. [CrossRef]
- Stone JE, Phillips AJK, Ftouni S, Magee M, Howard M, Lockley SW, Sletten TL, Anderson C, Rajaratnam SMW, Postnova S. Generalizability of A Neural Network Model for Circadian Phase Prediction in Real-World Conditions. Sci Rep. 2019 Jul 29;9(1):11001. [CrossRef]
- Wittmann M, Dinich J, Merrow M, Roenneberg T. Social jetlag: misalignment of biological and social time. Chronobiol Int. 2006;23(1-2):497-509. [CrossRef]
- Roenneberg T, Pilz LK, Zerbini G, Winnebeck EC. Chronotype and Social Jetlag: A (Self-) Critical Review. Biology (Basel). 2019 Jul 12;8(3):54. [CrossRef]
- Roenneberg T, Allebrandt KV, Merrow M, Vetter C. Social jetlag and obesity. Curr Biol. 2012 May 22;22(10):939-43. [CrossRef]
- Parsons MJ, Moffitt TE, Gregory AM, Goldman-Mellor S, Nolan PM, Poulton R, Caspi A. Social jetlag, obesity and metabolic disorder: investigation in a cohort study. Int J Obes (Lond). 2015 May;39(5):842-8. [CrossRef]
- Wong PM, Hasler BP, Kamarck TW, Muldoon MF, Manuck SB. Social Jetlag, Chronotype, and Cardiometabolic Risk. J Clin Endocrinol Metab. 2015 Dec;100(12):4612-20. [CrossRef]
- Caliandro R, Streng AA, van Kerkhof LWM, van der Horst GTJ, Chaves I. Social Jetlag and Related Risks for Human Health: A Timely Review. Nutrients. 2021 Dec 18;13(12):4543. [CrossRef]
- Roenneberg, T. How can social jetlag affect health? Nat Rev Endocrinol. 2023 Jul;19(7):383-384. [CrossRef]
- Henderson SEM, Brady EM, Robertson N. Associations between social jetlag and mental health in young people: A systematic review. Chronobiol Int. 2019 Oct;36(10):1316-1333. [CrossRef]
- Islam Z, Hu H, Akter S, Kuwahara K, Kochi T, Eguchi M, Kurotani K, Nanri A, Kabe I, Mizoue T. Social jetlag is associated with an increased likelihood of having depressive symptoms among the Japanese working population: the Furukawa Nutrition and Health Study. Sleep. 2020 Jan 13;43(1):zsz204. [CrossRef]
- Qu Y, Li T, Xie Y, Tao S, Yang Y, Zou L, Zhang D, Zhai S, Tao F, Wu X. Association of chronotype, social jetlag, sleep duration and depressive symptoms in Chinese college students. J Affect Disord. 2023 Jan 1;320:735-741. [CrossRef]
- Zerbini G, Winnebeck EC, Merrow M. Weekly, seasonal, and chronotype-dependent variation of dim-light melatonin onset. J Pineal Res. 2021 Apr;70(3):e12723. [CrossRef]
- Brown TM, Brainard GC, Cajochen C, Czeisler CA, Hanifin JP, Lockley SW, Lucas RJ, Münch M, O'Hagan JB, Peirson SN, Price LLA, Roenneberg T, Schlangen LJM, Skene DJ, Spitschan M, Vetter C, Zee PC, Wright KP Jr. Recommendations for daytime, evening, and nighttime indoor light exposure to best support physiology, sleep, and wakefulness in healthy adults. PLoS Biol. 2022 Mar 17;20(3):e3001571. [CrossRef]
- Reid KJ, Santostasi G, Baron KG, Wilson J, Kang J, Zee PC. Timing and intensity of light correlate with body weight in adults. PLoS One. 2014 Apr 2;9(4):e92251. [CrossRef]
- Shim J, Fleisch E, Barata F. Circadian rhythm analysis using wearable-based accelerometry as a digital biomarker of aging and healthspan. NPJ Digit Med. 2024 Jun 4;7(1):146. [CrossRef]
- Otsuka K, Cornélissen G, Halberg F, Oehlerts G. Excessive circadian amplitude of blood pressure increases risk of ischaemic stroke and nephropathy. J Med Eng Technol. 1997 Jan-Feb;21(1):23-30. [CrossRef]
- Cornelissen G, Halberg F, Bakken EE, Singh RB, Otsuka K, Tomlinson B, Delcourt A, Toussaint G, Bathina S, Schwartzkopff O, Wang ZR, Tarquini R, Perfetto F, Pantaleoni GC, Jozsa R, Delmore PA, Nolley E. 100 or 30 years after Janeway or Bartter, Healthwatch helps avoid "flying blind". Biomedicine & Pharmacotherapy 2004; 58 (Suppl 1): S69-S86.
- Cornélissen G, Delcourt A, Toussaint G, Otsuka K, Watanabe Y, Siegelova J, Fiser B, Dusek J, Homolka P, Singh RB, Kumar A, Singh RK, Sanchez S, Gonzalez C, Holley D, Sundaram B, Zhao Z, Tomlinson B, Fok B, Zeman M, Dulkova K, Halberg F. Opportunity of detecting pre-hypertension: worldwide data on blood pressure overswinging. Biomed Pharmacother. 2005 Oct;59 Suppl 1(Suppl 1):S152-7. [CrossRef]
- Halberg F, Powell D, Otsuka K, Watanabe Y, Beaty LA, Rosch P, Czaplicki J, Hillman D, Schwartzkopff O, Cornelissen G. Diagnosing vascular variability anomalies, not only MESOR-hypertension. Am J Physiol Heart Circ Physiol 2013; 305: H279-H294.
- Jagannath A, Taylor L, Wakaf Z, Vasudevan SR, Foster RG. The genetics of circadian rhythms, sleep and health. Hum Mol Genet. 2017 Oct 1;26(R2):R128-R138. [CrossRef]
- Bacalini MG, Palombo F, Garagnani P, Giuliani C, Fiorini C, Caporali L, Stanzani Maserati M, Capellari S, Romagnoli M, De Fanti S, Benussi L, Binetti G, Ghidoni R, Galimberti D, Scarpini E, Arcaro M, Bonanni E, Siciliano G, Maestri M, Guarnieri B; Italian Multicentric Group on clock genes, actigraphy in AD; Martucci M, Monti D, Carelli V, Franceschi C, La Morgia C, Santoro A. Association of rs3027178 polymorphism in the circadian clock gene PER1 with susceptibility to Alzheimer's disease and longevity in an Italian population. Geroscience. 2022 Apr;44(2):881-896. [CrossRef]
- Gubin D, Neroev V, Malishevskaya T, Kolomeichuk S, Cornelissen G, Yuzhakova N, Vlasova A, Weinert D. Depression scores are associated with retinal ganglion cells loss. J Affect Disord. 2023 Jul 15;333:290-296. [CrossRef]
- Lyall LM, Wyse CA, Graham N, Ferguson A, Lyall DM, Cullen B, Celis Morales CA, Biello SM, Mackay D, Ward J, Strawbridge RJ, Gill JMR, Bailey MES, Pell JP, Smith DJ. Association of disrupted circadian rhythmicity with mood disorders, subjective wellbeing, and cognitive function: a cross-sectional study of 91 105 participants from the UK Biobank. Lancet Psychiatry. 2018 Jun;5(6):507-514. [CrossRef]
- Feng H, Yang L, Ai S, Liu Y, Zhang W, Lei B, Chen J, Liu Y, Chan JWY, Chan NY, Tan X, Wang N, Benedict C, Jia F, Wing YK, Zhang J. Association between accelerometer-measured amplitude of rest-activity rhythm and future health risk: a prospective cohort study of the UK Biobank. Lancet Healthy Longev. 2023 May;4(5):e200-e210. [CrossRef]
- Cai R, Gao L, Gao C, Yu L, Zheng X, Bennett DA, Buchman AS, Hu K, Li P. Circadian disturbances and frailty risk in older adults. Nat Commun. 2023 Nov 16;14(1):7219. [CrossRef]
- Brooks TG, Lahens NF, Grant GR, Sheline YI, FitzGerald GA, Skarke C. Diurnal rhythms of wrist temperature are associated with future disease risk in the UK Biobank. Nat Commun. 2023 Aug 24;14(1):5172. [CrossRef]
- Xu Y, Su S, McCall WV, Isales C, Snieder H, Wang X. Rest-activity circadian rhythm and impaired glucose tolerance in adults: an analysis of NHANES 2011-2014. BMJ Open Diabetes Res Care. 2022 Mar;10(2):e002632. [CrossRef]
- Xu Y, Su S, McCall WV, Wang X. Blunted rest-activity rhythm is associated with increased white blood-cell-based inflammatory markers in adults: an analysis from NHANES 2011-2014. Chronobiol Int. 2022 Jun;39(6):895-902. [CrossRef]
- Shim J, Fleisch E, Barata F. Wearable-based accelerometer activity profile as digital biomarker of inflammation, biological age, and mortality using hierarchical clustering analysis in NHANES 2011-2014. Sci Rep. 2023 Jun 8;13(1):9326. [CrossRef]
- Tranah GJ, Blackwell T, Ancoli-Israel S, Paudel ML, Ensrud KE, Cauley JA, Redline S, Hillier TA, Cummings SR, Stone KL; Study of Osteoporotic Fractures Research Group. Circadian activity rhythms and mortality: the study of osteoporotic fractures. J Am Geriatr Soc. 2010 Feb;58(2):282-91. [CrossRef]
- Gabriel BM, Zierath JR. Circadian rhythms and exercise - re-setting the clock in metabolic disease. Nat Rev Endocrinol. 2019 Apr;15(4):197-206. [CrossRef]
- Martin RA, Esser KA. Time for Exercise? Exercise and Its Influence on the Skeletal Muscle Clock. J Biol Rhythms. 2022 Dec;37(6):579-592. [CrossRef]
- Martin RA, Viggars MR, Esser KA. Metabolism and exercise: the skeletal muscle clock takes centre stage. Nat Rev Endocrinol. 2023 May;19(5):272-284. [CrossRef]
- Tranah GJ, Blackwell T, Stone KL, Ancoli-Israel S, Paudel ML, Ensrud KE, Cauley JA, Redline S, Hillier TA, Cummings SR, Yaffe K; SOF Research Group. Circadian activity rhythms and risk of incident dementia and mild cognitive impairment in older women. Ann Neurol. 2011 Nov;70(5):722-32. [CrossRef]
- Rogers-Soeder TS, Blackwell T, Yaffe K, Ancoli-Israel S, Redline S, Cauley JA, Ensrud KE, Paudel M, Barrett-Connor E, LeBlanc E, Stone K, Lane NE, Tranah G; Osteoporotic Fractures in Men Study Research Group. Rest-Activity Rhythms and Cognitive Decline in Older Men: The Osteoporotic Fractures in Men Sleep Study. J Am Geriatr Soc. 2018 Nov;66(11):2136-2143. [CrossRef]
- Harada K, Masumoto K, Okada S. Physical Activity Components that Determine Daily Life Satisfaction Among Older Adults: An Intensive Longitudinal Diary Study. Int J Behav Med. 2024 Mar 19. [CrossRef]
- Tai Y, Obayashi K, Yamagami Y, Saeki K. Association between circadian skin temperature rhythms and actigraphic sleep measures in real-life settings. J Clin Sleep Med. 2023 Jul 1;19(7):1281-1292. [CrossRef]
- Saint-Maurice PF, Freeman JR, Russ D, Almeida JS, Shams-White MM, Patel S, Wolff-Hughes DL, Watts EL, Loftfield E, Hong HG, Moore SC, Matthews CE. Associations between actigraphy-measured sleep duration, continuity, and timing with mortality in the UK Biobank. Sleep. 2024 Mar 11;47(3):zsad312. [CrossRef]
- Nikbakhtian S, Reed AB, Obika BD, Morelli D, Cunningham AC, Aral M, Plans D. Accelerometer-derived sleep onset timing and cardiovascular disease incidence: a UK Biobank cohort study. Eur Heart J Digit Health. 2021 Nov 9;2(4):658-666. [CrossRef]
- Roenneberg T, Kuehnle T, Juda M, Kantermann T, Allebrandt K, Gordijn M, Merrow M. Epidemiology of the human circadian clock. Sleep Med Rev. 2007 Dec;11(6):429-38. [CrossRef]
- Fischer D, Lombardi DA, Marucci-Wellman H, Roenneberg T. Chronotypes in the US - Influence of age and sex. PLoS One. 2017 Jun 21;12(6):e0178782. [CrossRef]
- Borisenkov, M., Gubin, D., Kolomieichuk S. On the issue of adaptive fitness of chronotypes in high latitudes. Biological Rhythm Research, 2024. 1–5. [CrossRef]
- Gubin DG, Nelaeva AA, Uzhakova AE, Hasanova YV, Cornelissen G, Weinert D. Disrupted circadian rhythms of body temperature, heart rate and fasting blood glucose in prediabetes and type 2 diabetes mellitus. Chronobiol Int. 2017;34(8):1136-1148. [CrossRef]
- Windred DP, Burns AC, Rutter MK, Ching Yeung CH, Lane JM, Xiao Q, Saxena R, Cain SW, Phillips AJK. Personal light exposure patterns and incidence of type 2 diabetes: analysis of 13 million hours of light sensor data and 670,000 person-years of prospective observation. Lancet Reg Health Eur. 2024;42:100943. [CrossRef]
- Rao F, Xue T. Circadian-independent light regulation of mammalian metabolism. Nat Metab. 2024. [CrossRef]
- Weinert D, Gubin D. The Impact of Physical Activity on the Circadian System: Benefits for Health, Performance and Wellbeing. Applied Sciences. 2022; 12(18):9220. [CrossRef]
- Zambrano C, Garitaonaindia MT, Salmerón D, Pérez-Sanz F, Tchio C, Picinato MC, de Medina FS, Luján J, Scheer FAJL, Saxena R, Martínez-Augustin O, Garaulet M. Melatonin decreases human adipose tissue insulin sensitivity. J Pineal Res. 2024; 76(5):e12965. [CrossRef]
- Weinert D, Waterhouse J. The circadian rhythm of core temperature: effects of physical activity and aging. Physiol Behav. 2007 Feb 28;90(2-3):246-56. [CrossRef]
- Tranel HR, Schroder EA, England J, Black WS, Bush H, Hughes ME, Esser KA, Clasey JL. Physical activity, and not fat mass is a primary predictor of circadian parameters in young men. Chronobiol Int. 2015;32(6):832-41. [CrossRef]
- Dupont Rocher S, Bessot N, Sesboüé B, Bulla J, Davenne D. Circadian Characteristics of Older Adults and Aerobic Capacity. J Gerontol A Biol Sci Med Sci. 2016 Jun;71(6):817-22. [CrossRef]
- Gubin DG, Weinert D, Rybina SV, Danilova LA, Solovieva SV, Durov AM, Prokopiev NY, Ushakov PA. Activity, sleep and ambient light have a different impact on circadian blood pressure, heart rate and body temperature rhythms. Chronobiol Int. 2017;34(5):632-649. [CrossRef]
- Hori H, Koga N, Hidese S, Nagashima A, Kim Y, Higuchi T, Kunugi H. 24-h activity rhythm and sleep in depressed outpatients. J Psychiatr Res. 2016 Jun;77:27-34. [CrossRef]
- Merikanto I, Partonen T, Paunio T, Castaneda AE, Marttunen M, Urrila AS. Advanced phases and reduced amplitudes are suggested to characterize the daily rest-activity cycles in depressed adolescent boys. Chronobiol Int. 2017;34(7):967-976. [CrossRef]
- Minaeva O, Booij SH, Lamers F, Antypa N, Schoevers RA, Wichers M, Riese H. Level and timing of physical activity during normal daily life in depressed and non-depressed individuals. Transl Psychiatry. 2020 Jul 30;10(1):259. [CrossRef]
- Roveda E, Montaruli A, Galasso L, Pesenti C, Bruno E, Pasanisi P, Cortellini M, Rampichini S, Erzegovesi S, Caumo A, Esposito F. Rest-activity circadian rhythm and sleep quality in patients with binge eating disorder. Chronobiol Int. 2018 Feb;35(2):198-207. [CrossRef]
- Borisenkov MF, Tserne TA, Bakutova LA, Gubin DG. Food addiction and emotional eating are associated with intradaily rest-activity rhythm variability. Eat Weight Disord. 2022 Dec;27(8):3309-3316. [CrossRef]
- Healy KL, Morris AR, Liu AC. Circadian Synchrony: Sleep, Nutrition, and Physical Activity. Front Netw Physiol. 2021 Oct;1:732243. [CrossRef]
- Shen B, Ma C, Wu G, Liu H, Chen L, Yang G. Effects of exercise on circadian rhythms in humans. Front Pharmacol. 2023 Oct 11;14:1282357. [CrossRef]
- Weinert D, Schöttner K, Müller L, Wienke A. (2016). Intensive voluntary wheel running may restore circadian activity rhythms and improves the impaired cognitive performance of arrhythmic Djungarian hamsters. Chronobiol Int 33:1161-1170. [CrossRef]
- Weinert D, Weinandy R, Gattermann R. (2007). Photic and non-photic effects on the daily activity pattern of Mongolian gerbils. Physiol Behav 90:325-333. [CrossRef]
- Müller L, Fritzsche P, Weinert D. (2015). Novel object recognition of Djungarian hamsters depends on circadian time and rhythmic phenotype. Chronobiol Int 32:458-467. [CrossRef]
- Müller L, Weinert D. (2016). Individual recognition of social rank and social memory performance depends on a functional circadian system. Behav Processes 132:85-93. [CrossRef]
- Seo DY, Lee S, Kim N, Ko KS, Rhee BD, Park BJ, Han J. Morning and evening exercise. Integr Med Res. 2013 Dec;2(4):139-144. [CrossRef]
- Smith PJ, Merwin RM. The Role of Exercise in Management of Mental Health Disorders: An Integrative Review. Annu Rev Med. 2021 Jan 27;72:45-62. [CrossRef]
- Youngstedt SD, Elliott JA, Kripke DF. Human circadian phase-response curves for exercise. J Physiol. 2019 Apr;597(8):2253-2268. [CrossRef]
- Liang YY, Feng H, Chen Y, Jin X, Xue H, Zhou M, Ma H, Ai S, Wing YK, Geng Q, Zhang J. Joint association of physical activity and sleep duration with risk of all-cause and cause-specific mortality: a population-based cohort study using accelerometry. Eur J Prev Cardiol. 2023 Jul 12;30(9):832-843. [CrossRef]
- Jin X, Chen Y, Feng H, Zhou M, Chan JWY, Liu Y, Kong APS, Tan X, Wing YK, Liang YY, Zhang J. Association of accelerometer-measured sleep duration and different intensities of physical activity with incident type 2 diabetes in a population-based cohort study. J Sport Health Sci. 2024 Mar;13(2):222-232. [CrossRef]
- Ahn HJ, Choi EK, Rhee TM, Choi J, Lee KY, Kwon S, Lee SR, Oh S, Lip GYH. Accelerometer-derived physical activity and the risk of death, heart failure, and stroke in patients with atrial fibrillation: a prospective study from UK Biobank. Br J Sports Med. 2024 Apr 2;58(8):427-434. [CrossRef]
- Stamatakis E, Ahmadi MN, Friedenreich CM, Blodgett JM, Koster A, Holtermann A, Atkin A, Rangul V, Sherar LB, Teixeira-Pinto A, Ekelund U, Lee IM, Hamer M. Vigorous Intermittent Lifestyle Physical Activity and Cancer Incidence Among Nonexercising Adults: The UK Biobank Accelerometry Study. JAMA Oncol. 2023 Sep 1;9(9):1255-1259. [CrossRef]
- Khurshid S, Al-Alusi MA, Churchill TW, Guseh JS, Ellinor PT. Accelerometer-Derived "Weekend Warrior" Physical Activity and Incident Cardiovascular Disease. JAMA. 2023 Jul 18;330(3):247-252. [CrossRef]
- Lin F, Lin Y, Chen L, Huang T, Lin T, He J, Lu X, Chen X, Wang Y, Ye Q, Cai G. Association of physical activity pattern and risk of Parkinson's disease. NPJ Digit Med. 2024 May 23;7(1):137. [CrossRef]
- Ramakrishnan R, Doherty A, Smith-Byrne K, Rahimi K, Bennett D, Woodward M, Walmsley R, Dwyer T. Accelerometer measured physical activity and the incidence of cardiovascular disease: Evidence from the UK Biobank cohort study. PLoS Med. 2021 Jan 12;18(1):e1003487. 10.1371/journal.pmed.1003487. Erratum in: PLoS Med. 2021 Sep 29;18(9):e1003809. [CrossRef]
- Shreves AH, Small SR, Travis RC, Matthews CE, Doherty A. Dose-response of accelerometer-measured physical activity, step count, and cancer risk in the UK Biobank: a prospective cohort analysis. Lancet. 2023 Nov;402 Suppl 1:S83. [CrossRef]
- Watts EL, Saint-Maurice PF, Doherty A, Fensom GK, Freeman JR, Gorzelitz JS, Jin D, McClain KM, Papier K, Patel S, Shiroma EJ, Moore SC, Matthews CE. Association of Accelerometer-Measured Physical Activity Level With Risks of Hospitalization for 25 Common Health Conditions in UK Adults. JAMA Netw Open. 2023 Feb 1;6(2):e2256186. [CrossRef]
- Hooker SP, Diaz KM, Blair SN, Colabianchi N, Hutto B, McDonnell MN, Vena JE, Howard VJ. Association of Accelerometer-Measured Sedentary Time and Physical Activity With Risk of Stroke Among US Adults. JAMA Netw Open. 2022 Jun 1;5(6):e2215385. [CrossRef]
- Mandolesi L, Polverino A, Montuori S, Foti F, Ferraioli G, Sorrentino P, Sorrentino G. Effects of Physical Exercise on Cognitive Functioning and Wellbeing: Biological and Psychological Benefits. Front Psychol. 2018 Apr 27;9:509. [CrossRef]
- Thapa N, Kim B, Yang JG, Park HJ, Jang M, Son HE, Kim GM, Park H. The Relationship between Chronotype, Physical Activity and the Estimated Risk of Dementia in Community-Dwelling Older Adults. Int J Environ Res Public Health. 2020 May 24;17(10):3701. [CrossRef]
- Soldan A, Alfini A, Pettigrew C, Faria A, Hou X, Lim C, Lu H, Spira AP, Zipunnikov V, Albert M; BIOCARD Research Team. Actigraphy-estimated physical activity is associated with functional and structural brain connectivity among older adults. Neurobiol Aging. 2022 Aug;116:32-40. [CrossRef]
- Mahindru A, Patil P, Agrawal V. Role of Physical Activity on Mental Health and Well-Being: A Review. Cureus. 2023 Jan 7;15(1):e33475. [CrossRef]
- Feng H, Yang L, Liang YY, Ai S, Liu Y, Liu Y, Jin X, Lei B, Wang J, Zheng N, Chen X, Chan JWY, Sum RKW, Chan NY, Tan X, Benedict C, Wing YK, Zhang J. Associations of timing of physical activity with all-cause and cause-specific mortality in a prospective cohort study. Nat Commun. 2023 Feb 18;14(1):930. [CrossRef]
- Brito LC, Marin TC, Azevêdo L, Rosa-Silva JM, Shea SA, Thosar SS. Chronobiology of Exercise: Evaluating the Best Time to Exercise for Greater Cardiovascular and Metabolic Benefits. Compr Physiol. 2022 Jun 29;12(3):3621-3639. [CrossRef]
- Tian C, Bürki C, Westerman KE, Patel CJ. Association between timing and consistency of physical activity and type 2 diabetes: a cohort study on participants of the UK Biobank. Diabetologia. 2023 Dec;66(12):2275-2282. [CrossRef]
- Homolka P, Cornelissen G, Homolka A, Siegelova J, Halberg F. Exercise-associated transient circadian hypertension (CHAT)? Abstract, III International Conference, Civilization diseases in the spirit of V.I. Vernadsky, People's Friendship University of Russia, Moscow, Oct. 10-12, 2005, pp. 419–421.
- Bonekamp NE, May AM, Halle M, Dorresteijn JAN, van der Meer MG, Ruigrok YM, de Borst GJ, Geleijnse JM, Visseren FLJ, Koopal C. Physical exercise volume, type, and intensity and risk of all-cause mortality and cardiovascular events in patients with cardiovascular disease: a mediation analysis. Eur Heart J Open. 2023 Jun 13;3(3):oead057. [CrossRef]
- Franczyk B, Gluba-Brzózka A, Ciałkowska-Rysz A, Ławiński J, Rysz J. The Impact of Aerobic Exercise on HDL Quantity and Quality: A Narrative Review. Int J Mol Sci. 2023 Feb 28;24(5):4653. [CrossRef]
- Liu H, Liu S, Wang K, Zhang T, Yin L, Liang J, Yang Y, Luo J. Time-Dependent Effects of Physical Activity on Cardiovascular Risk Factors in Adults: A Systematic Review. Int J Environ Res Public Health. 2022 Oct 30;19(21):14194. [CrossRef]
- Schock S, Hakim A. The Physiological and Molecular Links Between Physical Activity and Brain Health: A Review. Neurosci Insights. 2023 Aug 17;18:26331055231191523. [CrossRef]
- Zhang H, Liu J, Cui M, Chai H, Chen L, Zhang T, Mi J, Guan H, Zhao L. Moderate-intensity continuous training has time-specific effects on the lipid metabolism of adolescents. J Transl Int Med. 2023 Mar 9;11(1):57-69. [CrossRef]
- Kent BA, Rahman SA, St Hilaire MA, Grant LK, Rüger M, Czeisler CA, Lockley SW. Circadian lipid and hepatic protein rhythms shift with a phase response curve different than melatonin. Nat Commun. 2022 Feb 3;13(1):681. 10.1038/s41467-022-28308-6. Erratum in: Nat Commun. 2022 Apr 20;13(1):2241. [CrossRef]
- Gubin D, Neroev V, Malishevskaya T, Kolomeichuk S, Weinert D, Yuzhakova N, Nelaeva A, Filippova Y, Cornelissen G. Daytime Lipid Metabolism Modulated by CLOCK Gene Is Linked to Retinal Ganglion Cells Damage in Glaucoma. Applied Sciences. 2022; 12(13):6374. [CrossRef]
- Wei W, Raun SH, Long JZ. Molecular Insights From Multiomics Studies of Physical Activity. Diabetes. 2024 Feb 1;73(2):162-168. [CrossRef]
- Chen C, Nakagawa S. Physical activity for cognitive health promotion: An overview of the underlying neurobiological mechanisms. Ageing Res Rev. 2023 Apr;86:101868. [CrossRef]
- Phillips CM, Dillon CB, Perry IJ. Does replacing sedentary behaviour with light or moderate to vigorous physical activity modulate inflammatory status in adults? Int J Behav Nutr Phys Act. 2017 Oct 11;14(1):138. [CrossRef]
- Tsai CL, Ukropec J, Ukropcová B, Pai MC. An acute bout of aerobic or strength exercise specifically modifies circulating exerkine levels and neurocognitive functions in elderly individuals with mild cognitive impairment. Neuroimage Clin. 2017 Oct 31;17:272-284. [CrossRef]
- Li VL, He Y, Contrepois K, Liu H, Kim JT, Wiggenhorn AL, Tanzo JT, Tung AS, Lyu X, Zushin PH, Jansen RS, Michael B, Loh KY, Yang AC, Carl CS, Voldstedlund CT, Wei W, Terrell SM, Moeller BC, Arthur RM, Wallis GA, van de Wetering K, Stahl A, Kiens B, Richter EA, Banik SM, Snyder MP, Xu Y, Long JZ. An exercise-inducible metabolite that suppresses feeding and obesity. Nature. 2022 Jun;606(7915):785-790. [CrossRef]
- Okauchi H, Hashimoto C, Nakao R, Oishi K. Timing of food intake is more potent than habitual voluntary exercise to prevent diet-induced obesity in mice. Chronobiol Int. 2019 Jan;36(1):57-74. [CrossRef]
- Cheng Q, Lu C, Qian R. The circadian clock regulates metabolic responses to physical exercise. Chronobiol Int. 2022 Jul;39(7):907-917. [CrossRef]
- Stanford KI, Lynes MD, Takahashi H, Baer LA, Arts PJ, May FJ, Lehnig AC, Middelbeek RJW, Richard JJ, So K, Chen EY, Gao F, Narain NR, Distefano G, Shettigar VK, Hirshman MF, Ziolo MT, Kiebish MA, Tseng YH, Coen PM, Goodyear LJ. 12,13-diHOME: An Exercise-Induced Lipokine that Increases Skeletal Muscle Fatty Acid Uptake. Cell Metab. 2018 May 1;27(5):1111-1120.e3. [CrossRef]
- Yang J, Vamvini M, Nigro P, Ho LL, Galani K, Alvarez M, Tanigawa Y, Renfro A, Carbone NP, Laakso M, Agudelo LZ, Pajukanta P, Hirshman MF, Middelbeek RJW, Grove K, Goodyear LJ, Kellis M. Single-cell dissection of the obesity-exercise axis in adipose-muscle tissues implies a critical role for mesenchymal stem cells. Cell Metab. 2022 Oct 4;34(10):1578-1593.e6. [CrossRef]
- Rey G, Valekunja UK, Feeney KA, Wulund L, Milev NB, Stangherlin A, Ansel-Bollepalli L, Velagapudi V, O'Neill JS, Reddy AB. The Pentose Phosphate Pathway Regulates the Circadian Clock. Cell Metab. 2016 Sep 13;24(3):462-473. [CrossRef]
- Fagiani F, Di Marino D, Romagnoli A, Travelli C, Voltan D, Di Cesare Mannelli L, Racchi M, Govoni S, Lanni C. Molecular regulations of circadian rhythm and implications for physiology and diseases. Signal Transduct Target Ther. 2022 Feb 8;7(1):41. [CrossRef]
- Esteras N, Blacker TS, Zherebtsov EA, Stelmashuk OA, Zhang Y, Wigley WC, Duchen MR, Dinkova-Kostova AT, Abramov AY. Nrf2 regulates glucose uptake and metabolism in neurons and astrocytes. Redox Biol. 2023 Jun;62:102672. [CrossRef]
- Wible RS, Ramanathan C, Sutter CH, Olesen KM, Kensler TW, Liu AC, Sutter TR. NRF2 regulates core and stabilizing circadian clock loops, coupling redox and timekeeping in Mus musculus. Elife. 2018 Feb 26;7:e31656. [CrossRef]
- Fasipe B, Laher I. Nrf2 modulates the benefits of evening exercise in type 2 diabetes. Sports Med Health Sci. 2023 Sep 9;5(4):251-258. [CrossRef]
- Thomas AW, Davies NA, Moir H, Watkeys L, Ruffino JS, Isa SA, Butcher LR, Hughes MG, Morris K, Webb R. Exercise-associated generation of PPARγ ligands activates PPARγ signaling events and upregulates genes related to lipid metabolism. J Appl Physiol (1985). 2012 Mar;112(5):806-15. [CrossRef]
- Chen L, Yang G. PPARs Integrate the Mammalian Clock and Energy Metabolism. PPAR Res. 2014;2014:653017. [CrossRef]
- Yang X, Downes M, Yu RT, Bookout AL, He W, Straume M, Mangelsdorf DJ, Evans RM. Nuclear receptor expression links the circadian clock to metabolism. Cell. 2006 Aug 25;126(4):801-10. [CrossRef]
- Sun S, Ma S, Cai Y, Wang S, Ren J, Yang Y, Ping J, Wang X, Zhang Y, Yan H, Li W, Esteban CR, Yu Y, Liu F, Izpisua Belmonte JC, Zhang W, Qu J, Liu GH. A single-cell transcriptomic atlas of exercise-induced anti-inflammatory and geroprotective effects across the body. Innovation (Camb). 2023 Jan 5;4(1):100380. [CrossRef]
- Matei D, Trofin D, Iordan DA, Onu I, Condurache I, Ionite C, Buculei I. The Endocannabinoid System and Physical Exercise. Int J Mol Sci. 2023 Jan 19;24(3):1989. [CrossRef]
- Xue H, Zou Y, Yang Q, Zhang Z, Zhang J, Wei X, Zhou J, Tao XL, Zhang C, Xia Y, Luo F. The association between different physical activity (PA) patterns and cardiometabolic index (CMI) in US adult population from NHANES (2007-2016). Heliyon. 2024 Mar 26;10(7):e28792. [CrossRef]
- Dai W, Zhang D, Wei Z, Liu P, Yang Q, Zhang L, Zhang J, Zhang C, Xue H, Xie Z, Luo F. Whether weekend warriors (WWs) achieve equivalent benefits in lipid accumulation products (LAP) reduction as other leisure-time physical activity patterns? -Results from a population-based analysis of NHANES 2007-2018. BMC Public Health. 2024 Jun 9;24(1):1550. [CrossRef]
- Nebe S, Reutter M, Baker DH, Bölte J, Domes G, Gamer M, Gärtner A, Gießing C, Gurr C, Hilger K, Jawinski P, Kulke L, Lischke A, Markett S, Meier M, Merz CJ, Popov T, Puhlmann LMC, Quintana DS, Schäfer T, Schubert AL, Sperl MFJ, Vehlen A, Lonsdorf TB, Feld GB. Enhancing precision in human neuroscience. Elife. 2023 Aug 9;12:e85980. [CrossRef]
- Muddapu VR, Dharshini SAP, Chakravarthy VS, Gromiha MM. Neurodegenerative Diseases - Is Metabolic Deficiency the Root Cause? Front Neurosci. 2020 Mar 31;14:213. [CrossRef]
- Procaccini C, Santopaolo M, Faicchia D, Colamatteo A, Formisano L, de Candia P, Galgani M, De Rosa V, Matarese G. Role of metabolism in neurodegenerative disorders. Metabolism. 2016 Sep;65(9):1376-90. [CrossRef]
- Breasail MÓ, Biswas B, Smith MD, Mazhar MKA, Tenison E, Cullen A, Lithander FE, Roudaut A, Henderson EJ. Wearable GPS and Accelerometer Technologies for Monitoring Mobility and Physical Activity in Neurodegenerative Disorders: A Systematic Review. Sensors (Basel). 2021 Dec 10;21(24):8261. [CrossRef]
- Cote AC, Phelps RJ, Kabiri NS, Bhangu JS, Thomas KK. Evaluation of Wearable Technology in Dementia: A Systematic Review and Meta-Analysis. Front Med (Lausanne). 2021 Jan 11;7:501104. [CrossRef]
- Nussbaumer-Streit B, Forneris CA, Morgan LC, Van Noord MG, Gaynes BN, Greenblatt A, Wipplinger J, Lux LJ, Winkler D, Gartlehner G. Light therapy for preventing seasonal affective disorder. Cochrane Database Syst Rev. 2019 Mar 18;3(3):CD011269. [CrossRef]
- Liu YL, Gong SY, Xia ST, Wang YL, Peng H, Shen Y, Liu CF. Light therapy: a new option for neurodegenerative diseases. Chin Med J (Engl). 2020 Dec 21;134(6):634-645. [CrossRef]
- Cardinali, DP. Melatonin: Clinical Perspectives in Neurodegeneration. Front Endocrinol (Lausanne). 2019 Jul 16;10:480. [CrossRef]
- Won E, Na KS, Kim YK. Associations between Melatonin, Neuroinflammation, and Brain Alterations in Depression. Int J Mol Sci. 2021 Dec 28;23(1):305. [CrossRef]
- Shin, JW. Neuroprotective effects of melatonin in neurodegenerative and autoimmune central nervous system diseases. Encephalitis. 2023 Apr;3(2):44-53. [CrossRef]
- Chen Y, Tan J, Liu Y, Dong GH, Yang BY, Li N, Wang L, Chen G, Li S, Guo Y. Long-term exposure to outdoor light at night and mild cognitive impairment: A nationwide study in Chinese veterans. Sci Total Environ. 2022 Nov 15;847:157441. [CrossRef]
- Mazzoleni E, Vinceti M, Costanzini S, Garuti C, Adani G, Vinceti G, Zamboni G, Tondelli M, Galli C, Salemme S, Teggi S, Chiari A, Filippini T. Outdoor artificial light at night and risk of early-onset dementia: A case-control study in the Modena population, Northern Italy. Heliyon. 2023 Jun 29;9(7):e17837. [CrossRef]
- Volicer L, Harper DG, Manning BC, Goldstein R, Satlin A. Sundowning and circadian rhythms in Alzheimer's disease. Am J Psychiatry. 2001;158(5):704-11. [CrossRef]
- Canevelli M, Valletta M, Trebbastoni A, Sarli G, D'Antonio F, Tariciotti L, de Lena C, Bruno G. Sundowning in Dementia: Clinical Relevance, Pathophysiological Determinants, and Therapeutic Approaches. Front Med (Lausanne). 2016;3:73. [CrossRef]
- Toccaceli Blasi M, Valletta M, Trebbastoni A, D'Antonio F, Talarico G, Campanelli A, Sepe Monti M, Salati E, Gasparini M, Buscarnera S, Salzillo M, Canevelli M, Bruno G. Sundowning in Patients with Dementia: Identification, Prevalence, and Clinical Correlates. J Alzheimers Dis. 2023;94(2):601-610. [CrossRef]
- Feng R, Li L, Yu H, Liu M, Zhao W. Melanopsin retinal ganglion cell loss and circadian dysfunction in Alzheimer's disease (Review). Mol Med Rep. 2016 Apr;13(4):3397-400. [CrossRef]
- La Morgia C, Ross-Cisneros FN, Koronyo Y, Hannibal J, Gallassi R, Cantalupo G, Sambati L, Pan BX, Tozer KR, Barboni P, Provini F, Avanzini P, Carbonelli M, Pelosi A, Chui H, Liguori R, Baruzzi A, Koronyo-Hamaoui M, Sadun AA, Carelli V. Melanopsin retinal ganglion cell loss in Alzheimer disease. Ann Neurol. 2016 Jan;79(1):90-109. [CrossRef]
- Shen Y, Lv QK, Xie WY, Gong SY, Zhuang S, Liu JY, Mao CJ, Liu CF. Circadian disruption and sleep disorders in neurodegeneration. Transl Neurodegener. 2023 Feb 13;12(1):8. [CrossRef]
- Gracitelli CP, Duque-Chica GL, Roizenblatt M, Moura AL, Nagy BV, Ragot de Melo G, Borba PD, Teixeira SH, Tufik S, Ventura DF, Paranhos A., Jr Intrinsically photosensitive retinal ganglion cell activity is associated with decreased sleep quality in patients with glaucoma. Ophthalmology. 2015;122:1139–48. [CrossRef]
- Mahanna-Gabrielli E, Kuwayama S, Tarraf W, Kaur S, DeBuc DC, Cai J, Daviglus ML, Joslin CE, Lee DJ, Mendoza-Santiesteban C, Stickel AM, Zheng D, González HM, Ramos AR. The Effect of Self-Reported Visual Impairment and Sleep on Cognitive Decline: Results of the Hispanic Community Health Study/Study of Latinos. J Alzheimers Dis. 2023;92(4):1257-1267. [CrossRef]
- Kawasaki A, Udry M, El Wardani M, Münch M. Can Extra Daytime Light Exposure Improve Well-Being and Sleep? A Pilot Study of Patients With Glaucoma. Front Neurol. 2021 Jan 15;11:584479. [CrossRef]
- Chellappa SL, Bromundt V, Frey S, Schlote T, Goldblum D, Cajochen C. Cross-sectional study of intraocular cataract lens replacement, circadian rest-activity rhythms, and sleep quality in older adults. Sleep. 2022 Apr 11;45(4):zsac027. [CrossRef]
- Gubin, D. , Boldyreva, J., Stefani, O., Kolomeichuk, S., Danilova, L., Markov, A., … Weinert, D. Light exposure predicts COVID-19 negative status in young adults. Biological Rhythm Research. 2024. 1–12. [CrossRef]
- Bano-Otalora B, Martial F, Harding C, Bechtold DA, Allen AE, Brown TM, Belle MDC, Lucas RJ. Bright daytime light enhances circadian amplitude in a diurnal mammal. Proc Natl Acad Sci U S A. 2021 Jun 1;118(22):e2100094118. [CrossRef]
- Münch M, Nowozin C, Regente J, Bes F, De Zeeuw J, Hädel S, Wahnschaffe A, Kunz D. Blue-Enriched Morning Light as a Countermeasure to Light at the Wrong Time: Effects on Cognition, Sleepiness, Sleep, and Circadian Phase. Neuropsychobiology. 2016;74(4):207-218. [CrossRef]
- Figueiro MG, Sahin L, Kalsher M, Plitnick B, Rea MS. Long-Term, All-Day Exposure to Circadian-Effective Light Improves Sleep, Mood, and Behavior in Persons with Dementia. J Alzheimers Dis Rep. 2020 Aug 4;4(1):297-312. [CrossRef]
- Juda M, Liu-Ambrose T, Feldman F, Suvagau C, Mistlberger RE. Light in the Senior Home: Effects of Dynamic and Individual Light Exposure on Sleep, Cognition, and Well-Being. Clocks Sleep. 2020 Dec 14;2(4):557-576. [CrossRef]
- Zang L, Liu X, Li Y, Liu J, Lu Q, Zhang Y, Meng Q. The effect of light therapy on sleep disorders and psychobehavioral symptoms in patients with Alzheimer's disease: A meta-analysis. PLoS One. 2023 Dec 6;18(12):e0293977. [CrossRef]
- Gubin DG, Gubin GD, Waterhouse J, Weinert D. The circadian body temperature rhythm in the elderly: effect of single daily melatonin dosing. Chronobiol Int. 2006;23(3):639-58. [CrossRef]
- Gubin DG, Gubin GD, Gapon LI, Weinert D. Daily Melatonin Administration Attenuates Age-Dependent Disturbances of Cardiovascular Rhythms. Curr Aging Sci. 2016;9(1):5-13. [CrossRef]
- Böhmer MN, Oppewal A, Valstar MJ, Bindels PJE, van Someren EJW, Maes-Festen DAM. Light up: an intervention study of the effect of environmental dynamic lighting on sleep-wake rhythm, mood and behaviour in older adults with intellectual disabilities. J Intellect Disabil Res. 2022 Oct;66(10):756-781. [CrossRef]
- Khalsa SB, Jewett ME, Cajochen C, Czeisler CA. A phase response curve to single bright light pulses in human subjects. J Physiol. 2003 Jun 15;549(Pt 3):945-52. [CrossRef]
- Lewy AJ, Ahmed S, Jackson JM, Sack RL. Melatonin shifts human circadian rhythms according to a phase-response curve. Chronobiol Int. 1992 Oct;9(5):380-92. [CrossRef]
- Burgess HJ, Revell VL, Molina TA, Eastman CI. Human phase response curves to three days of daily melatonin: 0.5 mg versus 3.0 mg. J Clin Endocrinol Metab. 2010 Jul;95(7):3325-31. [CrossRef]
- Partonen, T. Chronotype and Health Outcomes. Curr Sleep Medicine Rep 1, 205–211 (2015). [CrossRef]
- Knutson KL, von Schantz M. Associations between chronotype, morbidity and mortality in the UK Biobank cohort. Chronobiol Int. 2018 Aug;35(8):1045-1053. [CrossRef]
- Makarem N, Paul J, Giardina EV, Liao M, Aggarwal B. Evening chronotype is associated with poor cardiovascular health and adverse health behaviors in a diverse population of women. Chronobiol Int. 2020 May;37(5):673-685. [CrossRef]
- Baldanzi G, Hammar U, Fall T, Lindberg E, Lind L, Elmståhl S, Theorell-Haglöw J. Evening chronotype is associated with elevated biomarkers of cardiometabolic risk in the EpiHealth cohort: a cross-sectional study. Sleep. 2022 Feb 14;45(2):zsab226. [CrossRef]
- Dowling GA, Burr RL, Van Someren EJ, Hubbard EM, Luxenberg JS, Mastick J, et al. Melatonin and bright-light treatment for rest-activity disruption in institutionalized patients with Alzheimer's disease. J Am Geriatr Soc. 2008;56(2):239–246. [CrossRef]
- Riemersma-van Der Lek RF, Swaab DF, Twisk J, Hol EM, Hoogendijk WJ, Van Someren EJ. Effect of bright light and melatonin on cognitive and noncognitive function in elderly residents of group care facilities: a randomized controlled trial. JAMA. 2008;299(22):2642–2655. [CrossRef]
- McCurry SM, Pike KC, Vitiello MV, Logsdon RG, Larson EB, Teri L. Increasing walking and bright light exposure to improve sleep in community-dwelling persons with Alzheimer's disease: results of a randomized, controlled trial. J Am Geriatr Soc. 2011 Aug;59(8):1393-402. [CrossRef]
- Hodgson NA, McPhillips MV, Petrovsky DV, Perez A, Talwar S, Gooneratne N, Riegel B, Aryal S, Gitlin LN. Timed Activity to Minimize Sleep Disturbance in People With Cognitive Impairment. Innov Aging. 2023 Dec 8;8(1):igad132. [CrossRef]
- Hand AJ, Stone JE, Shen L, Vetter C, Cain SW, Bei B, Phillips AJK. Measuring light regularity: sleep regularity is associated with regularity of light exposure in adolescents. Sleep. 2023 Aug 14;46(8):zsad001. [CrossRef]
- Piarulli A, Bergamasco M, Thibaut A, Cologan V, Gosseries O, Laureys S. EEG ultradian rhythmicity differences in disorders of consciousness during wakefulness. J Neurol. 2016 Sep;263(9):1746-60. [CrossRef]
- Goh GH, Maloney SK, Mark PJ, Blache D. Episodic Ultradian Events-Ultradian Rhythms. Biology (Basel). 2019 Mar 14;8(1):15. [CrossRef]
- Castaneda D, Esparza A, Ghamari M, Soltanpur C, Nazeran H. A review on wearable photoplethysmography sensors and their potential future applications in health care. Int J Biosens Bioelectron. 2018;4(4):195-202. [CrossRef]
- Scholkmann F, Wolf U. The Pulse-Respiration Quotient: A Powerful but Untapped Parameter for Modern Studies About Human Physiology and Pathophysiology. Front Physiol. 2019 Apr 9;10:371. [CrossRef]
- Rafl J, Bachman TE, Rafl-Huttova V, Walzel S, Rozanek M. Commercial smartwatch with pulse oximeter detects short-time hypoxemia as well as standard medical-grade device: Validation study. Digit Health. 2022 Oct 11;8:20552076221132127. [CrossRef]
- Santos M, Vollam S, Pimentel MA, Areia C, Young L, Roman C, Ede J, Piper P, King E, Harford M, Shah A, Gustafson O, Tarassenko L, Watkinson P. The Use of Wearable Pulse Oximeters in the Prompt Detection of Hypoxemia and During Movement: Diagnostic Accuracy Study. J Med Internet Res. 2022 Feb 15;24(2):e28890. [CrossRef]
- Charlton PH, Kyriaco PA, Mant J, Marozas V, Chowienczyk P, Alastruey J. Wearable Photoplethysmography for Cardiovascular Monitoring. Proc IEEE Inst Electr Electron Eng. 2022 Mar 11;110(3):355-381. [CrossRef] [PubMed] [PubMed Central]
- Charlton PH, Allen J, Bailón R, Baker S, Behar JA, Chen F, Clifford GD, Clifton DA, Davies HJ, Ding C, Ding X, Dunn J, Elgendi M, Ferdoushi M, Franklin D, Gil E, Hassan MF, Hernesniemi J, Hu X, Ji N, Khan Y, Kontaxis S, Korhonen I, Kyriacou PA, Laguna P, Lázaro J, Lee C, Levy J, Li Y, Liu C, Liu J, Lu L, Mandic DP, Marozas V, Mejía-Mejía E, Mukkamala R, Nitzan M, Pereira T, Poon CCY, Ramella-Roman JC, Saarinen H, Shandhi MMH, Shin H, Stansby G, Tamura T, Vehkaoja A, Wang WK, Zhang YT, Zhao N, Zheng D, Zhu T. The 2023 wearable photoplethysmography roadmap. Physiol Meas. 2023 Nov 29;44(11):111001. [CrossRef]
- Yeung MK, Lin J. Probing depression, schizophrenia, and other psychiatric disorders using fNIRS and the verbal fluency test: A systematic review and meta-analysis. J Psychiatr Res. 2021 Aug;140:416-435. [CrossRef]
- Nishi R, Fukumoto T, Asakawa A. Possible effect of natural light on emotion recognition and the prefrontal cortex: A scoping review of near-infrared (NIR) spectroscopy. Adv Clin Exp Med. 2023 Dec;32(12):1441-1451. [CrossRef]
- Pereira J, Direito B, Lührs M, Castelo-Branco M, Sousa T. Multimodal assessment of the spatial correspondence between fNIRS and fMRI hemodynamic responses in motor tasks. Sci Rep. 2023 Feb 8;13(1):2244. [CrossRef]
- Scarapicchia V, Brown C, Mayo C, Gawryluk JR. Functional Magnetic Resonance Imaging and Functional Near-Infrared Spectroscopy: Insights from Combined Recording Studies. Front Hum Neurosci. 2017 Aug 18;11:419. [CrossRef]
- Orban C, Kong R, Li J, Chee MWL, Yeo BTT. Time of day is associated with paradoxical reductions in global signal fluctuation and functional connectivity. PLoS Biol. 2020 Feb 18;18(2):e3000602. [CrossRef]
- Murata EM, Pritschet L, Grotzinger H, Taylor CM, Jacobs EG. Circadian rhythms tied to changes in brain morphology in a densely-sampled male. bioRxiv [Preprint]. 2024 Apr 14:2024.04.10.588906. [CrossRef]
- Baria AT, Baliki MN, Parrish T, Apkarian AV. Anatomical and functional assemblies of brain BOLD oscillations. J Neurosci. 2011; 31(21):7910-9. [CrossRef]
- Chang C, Metzger CD, Glover GH, Duyn JH, Heinze HJ, Walter M. Association between heart rate variability and fluctuations in resting-state functional connectivity. Neuroimage. 2013; 68:93-104. [CrossRef]
- Chen JE, Glover GH. BOLD fractional contribution to resting-state functional connectivity above 0.1 Hz. Neuroimage. 2015;107:207-218. [CrossRef]
- Otsuka K, Cornelissen G, Furukawa S, Shibata K, Kubo Y, Mizuno K, Aiba T, Ohshima H, Mukai C. Unconscious mind activates central cardiovascular network and promotes adaptation to microgravity possibly anti-aging during 1-year-long spaceflight. Sci Rep. 2022;12(1):11862. [CrossRef]
- Otsuka K, Cornelissen G, Kubo Y, Shibata K, Mizuno K, Aiba T, Furukawa S, Ohshima H, Mukai C. Methods for assessing change in brain plasticity at night and psychological resilience during daytime between repeated long-duration space missions. Sci Rep. 2023; 13(1):10909. [CrossRef]
- Brothers MC, DeBrosse M, Grigsby CC, Naik RR, Hussain SM, Heikenfeld J, Kim SS. Achievements and Challenges for Real-Time Sensing of Analytes in Sweat within Wearable Platforms. Acc Chem Res. 2019 Feb 19;52(2):297-306. [CrossRef]
- Jagannath B, Lin KC, Pali M, Sankhala D, Muthukumar S, Prasad S. A Sweat-based Wearable Enabling Technology for Real-time Monitoring of IL-1β and CRP as Potential Markers for Inflammatory Bowel Disease. Inflamm Bowel Dis. 2020 Sep 18;26(10):1533-1542. [CrossRef]
- Hirten RP, Lin KC, Whang J, Shahub S, Churcher NKM, Helmus D, Muthukumar S, Sands B, Prasad S. Longitudinal monitoring of IL-6 and CRP in inflammatory bowel disease using IBD-AWARE. Biosens Bioelectron X. 2024 Feb;16:100435. [CrossRef]
- Liu D, Liu Z, Feng S, Gao Z, Chen R, Cai G, Bian S. Wearable Microfluidic Sweat Chip for Detection of Sweat Glucose and pH in Long-Distance Running Exercise. Biosensors. 2023; 13(2):157. [CrossRef]
- Ok J, Park S, Jung YH, Kim TI. Wearable and Implantable Cortisol-Sensing Electronics for Stress Monitoring. Adv Mater. 2024 Jan;36(1):e2211595. [CrossRef]
- Watkins Z, McHenry A, Heikenfeld J. Wearing the Lab: Advances and Challenges in Skin-Interfaced Systems for Continuous Biochemical Sensing. Adv Biochem Eng Biotechnol. 2024;187:223-282. [CrossRef]
- Zhang S, He Z, Zhao W, Liu C, Zhou S, Ibrahim OO, Wang C, Wang Q. Innovative Material-Based Wearable Non-Invasive Electrochemical Sweat Sensors towards Biomedical Applications. Nanomaterials (Basel). 2024 May 14;14(10):857. [CrossRef]
- Singh NK, Chung S, Chang AY, Wang J, Hall DA. A non-invasive wearable stress patch for real-time cortisol monitoring using a pseudoknot-assisted aptamer. Biosens Bioelectron. 2023 May 1;227:115097. [CrossRef]
- Ding H, Yang H, Tsujimura S. Nature-Inspired Superhydrophilic Biosponge as Structural Beneficial Platform for Sweating Analysis Patch. Adv Sci (Weinh). 2024 Jun 13:e2401947. [CrossRef]
- Brown, TM. Melanopic illuminance defines the magnitude of human circadian light responses under a wide range of conditions. J Pineal Res. 2020 Aug;69(1):e12655. [CrossRef]
- van Duijnhoven, J. , Hartmeyer S., Didikoğlu A., et al. Overview of wearable light loggers: State-of-the-art and outlook. TechRxiv. June 03, 2024. [CrossRef]
- Giménez MC, Stefani O, Cajochen C, Lang D, Deuring G, Schlangen LJM. Predicting melatonin suppression by light in humans: Unifying photoreceptor-based equivalent daylight illuminances, spectral composition, timing and duration of light exposure. J Pineal Res. 2022 Mar;72(2):e12786. [CrossRef]
- Trinh VQ, Bodrogi P, Khanh TQ. Determination and Measurement of Melanopic Equivalent Daylight (D65) Illuminance (mEDI) in the Context of Smart and Integrative Lighting. Sensors (Basel). 2023 May 23;23(11):5000. [CrossRef]
- Stampfli JR, Schrader B, di Battista C, Häfliger R, Schälli O, Wichmann G, Zumbühl C, Blattner P, Cajochen C, Lazar R, Spitschan M. The Light-Dosimeter: A new device to help advance research on the non-visual responses to light. Light Res Technol. 2023 Feb 13;55(4-5):474-486. [CrossRef]
- Juzeniene A, Moan J. Beneficial effects of UV radiation other than via vitamin D production. Dermatoendocrinol. 2012 Apr 1;4(2):109-17. [CrossRef]
- Giménez MC, Luxwolda M, Van Stipriaan EG, Bollen PP, Hoekman RL, Koopmans MA, Arany PR, Krames MR, Berends AC, Hut RA, Gordijn MCM. Effects of Near-Infrared Light on Well-Being and Health in Human Subjects with Mild Sleep-Related Complaints: A Double-Blind, Randomized, Placebo-Controlled Study. Biology (Basel). 2022 Dec 29;12(1):60. [CrossRef]
- Li H, Cui F, Wang T, Wang W, Zhang D. The impact of sunlight exposure on brain structural markers in the UK Biobank. Sci Rep. 2024 May 5;14(1):10313. [CrossRef]
- Slominski RM, Chen JY, Raman C, Slominski AT. Photo-neuro-immuno-endocrinology: How the ultraviolet radiation regulates the body, brain, and immune system. Proc Natl Acad Sci U S A. 2024 Apr 2;121(14):e2308374121. [CrossRef]
- Kallioğlu MA, Sharma A, Kallioğlu A, Kumar S, Khargotra R, Singh T. UV index-based model for predicting synthesis of (pre-)vitamin D3 in the mediterranean basin. Sci Rep. 2024 Feb 12;14(1):3541. [CrossRef]
- Hacker E, Horsham C, Allen M, Nathan A, Lowe J, Janda M. Capturing Ultraviolet Radiation Exposure and Physical Activity: Feasibility Study and Comparison Between Self-Reports, Mobile Apps, Dosimeters, and Accelerometers. JMIR Res Protoc. 2018 Apr 17;7(4):e102. [CrossRef]
- Kervezee L, Dashti HS, Pilz LK, Skarke C, Ruben MD. Using routinely collected clinical data for circadian medicine: A review of opportunities and challenges. PLOS Digit Health. 2024 May 23;3(5):e0000511. [CrossRef]
- Spitschan M, Zauner J, Tengelin MN, Bouroussis CF, Caspar P, Eloi F. Illuminating the future of wearable light metrology: Overview of the MeLiDos Project. Measurement. 2024. 114909. [CrossRef]
- Spitschan, M. Selecting, implementing and evaluating control and placebo conditions in light therapy and light-based interventions. Ann Med. 2024 Dec;56(1):2298875. [CrossRef]
- Bowman C, Huang Y, Walch OJ, Fang Y, Frank E, Tyler J, Mayer C, Stockbridge C, Goldstein C, Sen S, Forger DB. A method for characterizing daily physiology from widely used wearables. Cell Rep Methods. 2021 Aug 23;1(4):100058. [CrossRef]
- Buekers J, Theunis J, De Boever P, Vaes AW, Koopman M, Janssen EV, Wouters EF, Spruit MA, Aerts JM. Wearable Finger Pulse Oximetry for Continuous Oxygen Saturation Measurements During Daily Home Routines of Patients With Chronic Obstructive Pulmonary Disease (COPD) Over One Week: Observational Study. JMIR Mhealth Uhealth. 2019 Jun 6;7(6):e12866. [CrossRef]
- Hua J, Li J, Jiang Y, Xie S, Shi Y, Pan L. Skin-Attachable Sensors for Biomedical Applications. Biomed Mater Devices. 2022 Oct 3:1-13. [CrossRef]
- You Y, Liu J, Li X, Wang P, Liu R, Ma X. Relationship between accelerometer-measured sleep duration and Stroop performance: a functional near-infrared spectroscopy study among young adults. PeerJ. 2024 Feb 28;12:e17057. [CrossRef]
- Emish M, Young SD. Remote Wearable Neuroimaging Devices for Health Monitoring and Neurophenotyping: A Scoping Review. Biomimetics (Basel). 2024 Apr 16;9(4):237. [CrossRef]
- Huang Y, Mayer C, Walch OJ, Bowman C, Sen S, Goldstein C, Tyler J, Forger DB. Distinct Circadian Assessments From Wearable Data Reveal Social Distancing Promoted Internal Desynchrony Between Circadian Markers. Front Digit Health. 2021 Nov 16;3:727504. [CrossRef]
- Braund TA, Zin MT, Boonstra TW, Wong QJJ, Larsen ME, Christensen H, Tillman G, O'Dea B. Smartphone Sensor Data for Identifying and Monitoring Symptoms of Mood Disorders: A Longitudinal Observational Study. JMIR Ment Health. 2022 May 4;9(5):e35549. [CrossRef]
- Wu C, McMahon M, Fritz H, Schnyer DM. circadian rhythms are not captured equal: Exploring Circadian metrics extracted by different computational methods from smartphone accelerometer and GPS sensors in daily life tracking. Digit Health. 2022 Jul 18;8:20552076221114201. [CrossRef]
- Lin C, Chen IM, Chuang HH, Wang ZW, Lin HH, Lin YH. Examining Human-Smartphone Interaction as a Proxy for Circadian Rhythm in Patients With Insomnia: Cross-Sectional Study. J Med Internet Res. 2023 Dec 15;25:e48044. [CrossRef]
- Innominato PF, Macdonald JH, Saxton W, Longshaw L, Granger R, Naja I, Allocca C, Edwards R, Rasheed S, Folkvord F, de Batlle J, Ail R, Motta E, Bale C, Fuller C, Mullard AP, Subbe CP, Griffiths D, Wreglesworth NI, Pecchia L, Fico G, Antonini A. Digital Remote Monitoring Using an mHealth Solution for Survivors of Cancer: Protocol for a Pilot Observational Study. JMIR Res Protoc. 2024 Apr 30;13:e52957. [CrossRef]
- Borer KT, Cornelissen G, Halberg F, Brook R, Rajagopalan S, Fay W. Circadian blood pressure overswinging in a physically fit, normotensive African American woman. Am J Hypertens. 2002 Sep;15(9):827-30. [CrossRef]
- Velasquez MT, Beddhu S, Nobakht E, Rahman M, Raj DS. Ambulatory Blood Pressure in Chronic Kidney Disease: Ready for Prime Time? Kidney Int Rep. 2016 Jul;1(2):94-104. [CrossRef]
- Schlagintweit J, Laharnar N, Glos M, Zemann M, Demin AV, Lederer K, Penzel T, Fietze I. Effects of sleep fragmentation and partial sleep restriction on heart rate variability during night. Sci Rep. 2023 Apr 17;13(1):6202. [CrossRef]
- Laharnar N, Fatek J, Zemann M, Glos M, Lederer K, Suvorov AV, Demin AV, Penzel T, Fietze I. A sleep intervention study comparing effects of sleep restriction and fragmentation on sleep and vigilance and the need for recovery. Physiol Behav. 2020 Mar 1;215:112794. [CrossRef]
- Qian X, Droste SK, Lightman SL, Reul JM, Linthorst AC. Circadian and ultradian rhythms of free glucocorticoid hormone are highly synchronized between the blood, the subcutaneous tissue, and the brain. Endocrinology. 2012 Sep;153(9):4346-53. [CrossRef]
- Zhu B, Zhang Q, Pan Y, Mace EM, York B, Antoulas AC, et al. A Cell-Autonomous Mammalian 12 hr Clock Coordinates Metabolic and Stress Rhythms. Cell Metab. 2017;25(6):1305–19 e9. [CrossRef]
- Goh GH, Maloney SK, Mark PJ, Blache D. Episodic Ultradian Events-Ultradian Rhythms. Biology (Basel). 2019 Mar 14;8(1):15. [CrossRef]
- Grant AD, Newman M, Kriegsfeld LJ. Ultradian rhythms in heart rate variability and distal body temperature anticipate onset of the luteinizing hormone surge. Sci Rep. 2020 Nov 23;10(1):20378. [CrossRef]
- Otsuka K, Murakami S, Okajima K, Shibata K, Kubo Y, Gubin DG, Beaty LA, Cornelissen G. Appropriate Circadian-Circasemidian Coupling Protects Blood Pressure from Morning Surge and Promotes Human Resilience and Wellbeing. Clin Interv Aging. 2023 May 10;18:755-769. [CrossRef]
- Iimuro S, Imai E, Watanabe T, Nitta K, Akizawa T, Matsuo S, Makino H, Ohashi Y, Hishida A. Hyperbaric area index calculated from ABPM elucidates the condition of CKD patients: the CKD-JAC study. Clin Exp Nephrol. 2015 Feb;19(1):114-24. [CrossRef]
- Edgley K, Chun HY, Whiteley WN, Tsanas A. New Insights into Stroke from Continuous Passively Collected Temperature and Sleep Data Using Wrist-Worn Wearables. Sensors (Basel). 2023 Jan 17;23(3):1069. [CrossRef]
- Korman M, Tkachev V, Reis C, Komada Y, Kitamura S, Gubin D, Kumar V, Roenneberg T. COVID-19-mandated social restrictions unveil the impact of social time pressure on sleep and body clock. Sci Rep. 2020 Dec 17;10(1):22225. [CrossRef]
Figure 1.
Wearables available and schematics for the most typical circadian deviations. Left: Available monitoring technologies: actigraphy tracked variables (framed): activity, wrist temperature, wrist or hip light exposure; other wearables tracked variables: near-eye light dosimeters (Lidos), blood pressure, heart, photoplethysmography (PPG)s, biochemical variables (cortisol, interleukin-1β and C-reactive protein). Right: schematic markers of circadian disruptions: a) deviation of average value; b) changes in the duration of periods of activity, sleep, daylight exposure, etc; c) phase deviations; d) decrease in amplitude; e) changes in optimal parameters within the time epoch (example of light exposure); suboptimal circadian light hygiene implies deficit of daytime light and (or) excess of light at night, that can be approached as areas outside the curve of recommendations for optimal 24-hour light hygiene; see Figure 3 for further details).
Figure 1.
Wearables available and schematics for the most typical circadian deviations. Left: Available monitoring technologies: actigraphy tracked variables (framed): activity, wrist temperature, wrist or hip light exposure; other wearables tracked variables: near-eye light dosimeters (Lidos), blood pressure, heart, photoplethysmography (PPG)s, biochemical variables (cortisol, interleukin-1β and C-reactive protein). Right: schematic markers of circadian disruptions: a) deviation of average value; b) changes in the duration of periods of activity, sleep, daylight exposure, etc; c) phase deviations; d) decrease in amplitude; e) changes in optimal parameters within the time epoch (example of light exposure); suboptimal circadian light hygiene implies deficit of daytime light and (or) excess of light at night, that can be approached as areas outside the curve of recommendations for optimal 24-hour light hygiene; see Figure 3 for further details).
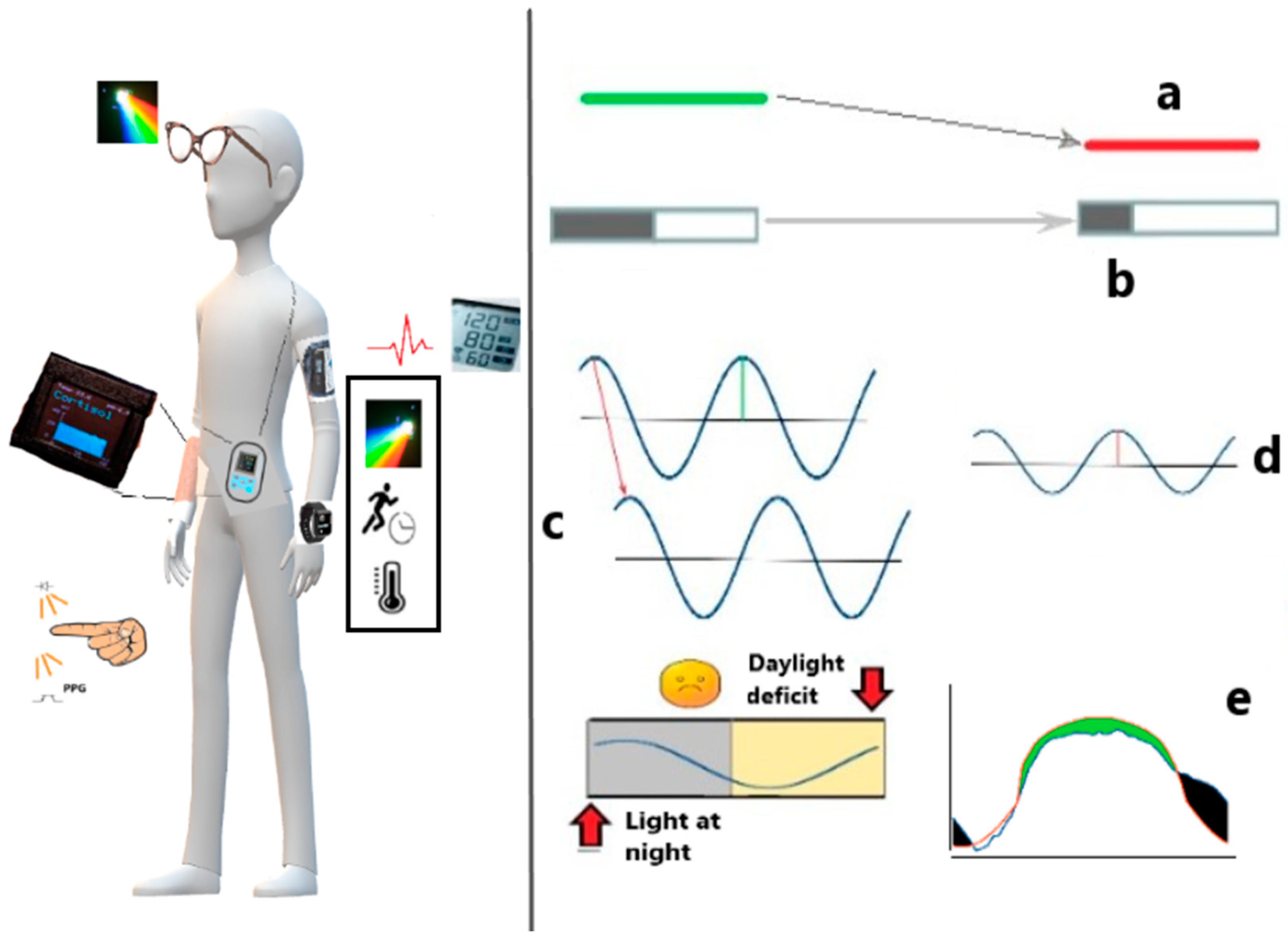
Table 1.
Wearables for circadian medicine / chronomedicine.
| Accelerometry-based: | Others: |
|---|---|
| Actigraphs: usually wrist-worn or hip-worn devices that track movement to estimate sleep patterns over extended periods, some can also measure physical activity, skin and ambient temperature, and light exposure. | Heart Rate Monitors: can be used as stand-alone devices or integrated into other wearables, offering data on heart rate variability, which can correlate with cardiovascular health, stress and sleep quality. |
| Sleep Trackers: specialized watches and bands that monitor sleep stages, and overall sleep quality. | Blood Pressure Monitors: Blood pressure monitors can be utilized in chronomedicine to track 24-h changes in blood pressure throughout the day and night and how these changes vary from day to day. |
| Smart Watches: commercially available devices that come with built-in features to track physical activity. | Continuous Glucose Monitors (CGMs): while not exclusively for circadian research, CGMs can provide data on metabolic changes throughout the day and night. From the viewpoint of diabetes research, glucose variability is now considered as important a biomarker as the A1c. |
| Fitness Trackers: similar to smartwatches, these devices track steps, activity, heart rate, all of which can be relevant to circadian rhythms. | Photopletysmography (PPG) Monitors: PPG monitors can be used to measure changes in blood volume in the body, providing valuable data on heart rate variability and respiration rate. By analyzing these metrics over a 24-h period, healthcare providers can gain insight into an individual's circadian rhythm and identify any deviations or abnormalities that may be indicative of increased risk of disease. |
| Smart Rings: devices like the Oura Ring track sleep, temperature, and activity, and light providing insights into 24-h rhythms. | Wearables for Monitoring Biochemicals: wearables that can monitor biochemicals such as C-reactive protein, interleukin-1b, and cortisol can provide important information on inflammation levels, immune system function, and stress levels throughout the day and night. By tracking these biochemical markers over time, healthcare providers can better understand how individuals’ circadian rhythm may be influencing their overall health and make informed treatment decisions. |
Footnote: Each accelerometry-based device can contribute to a better understanding of circadian rhythms and their effect on health, though it is important to note that not all are validated for research purposes to the same extent as actigraphy. .
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



