Submitted:
06 November 2024
Posted:
07 November 2024
You are already at the latest version
Abstract
Cisplatin-based chemotherapy has long been the standard first-line treatment for metastatic urothelial carcinoma (mUC). However, owing to comorbidities, up to 50% of patients are ineligible for cisplatin, necessitating alternative primary treatment options. Immune checkpoint inhibitors (ICIs) have emerged as a vital alternative for those unable to receive cisplatin. However, the prognosis for advanced urothelial carcinoma remains grim, with challenges persisting in optimizing first-line therapy. Recent advancements have redirected attention towards innovative combinations in primary treatment. The combination of enfortumab vedotin (EV) and pembrolizumab has significantly improved overall and progression-free survival compared to chemotherapy alone. This marks a critical shift in first-line treatment options for patients who are cisplatin-ineligible or require alternatives to standard chemotherapy. While platinum-based chemotherapy continues to be essential for many patients, the approval of EV and pembrolizumab as first-line treatments for cisplatin-ineligible patients signifies a significant breakthrough in primary care. These therapies offer new options and enhance outcomes in terms of survival and response rates, highlighting the increasing relevance of ICI-containing regimens in frontline care. This review provides an exhaustive overview of the current frontline treatment landscape for mUC, incorporating clinical trial evidence and exploring investigational agents to aid in clinical decision-making and guide future therapeutic strategies.
Keywords:
1. Introduction
2. Type and Mechanism of Drug Classes Used in the Frontline Treatment of mUC
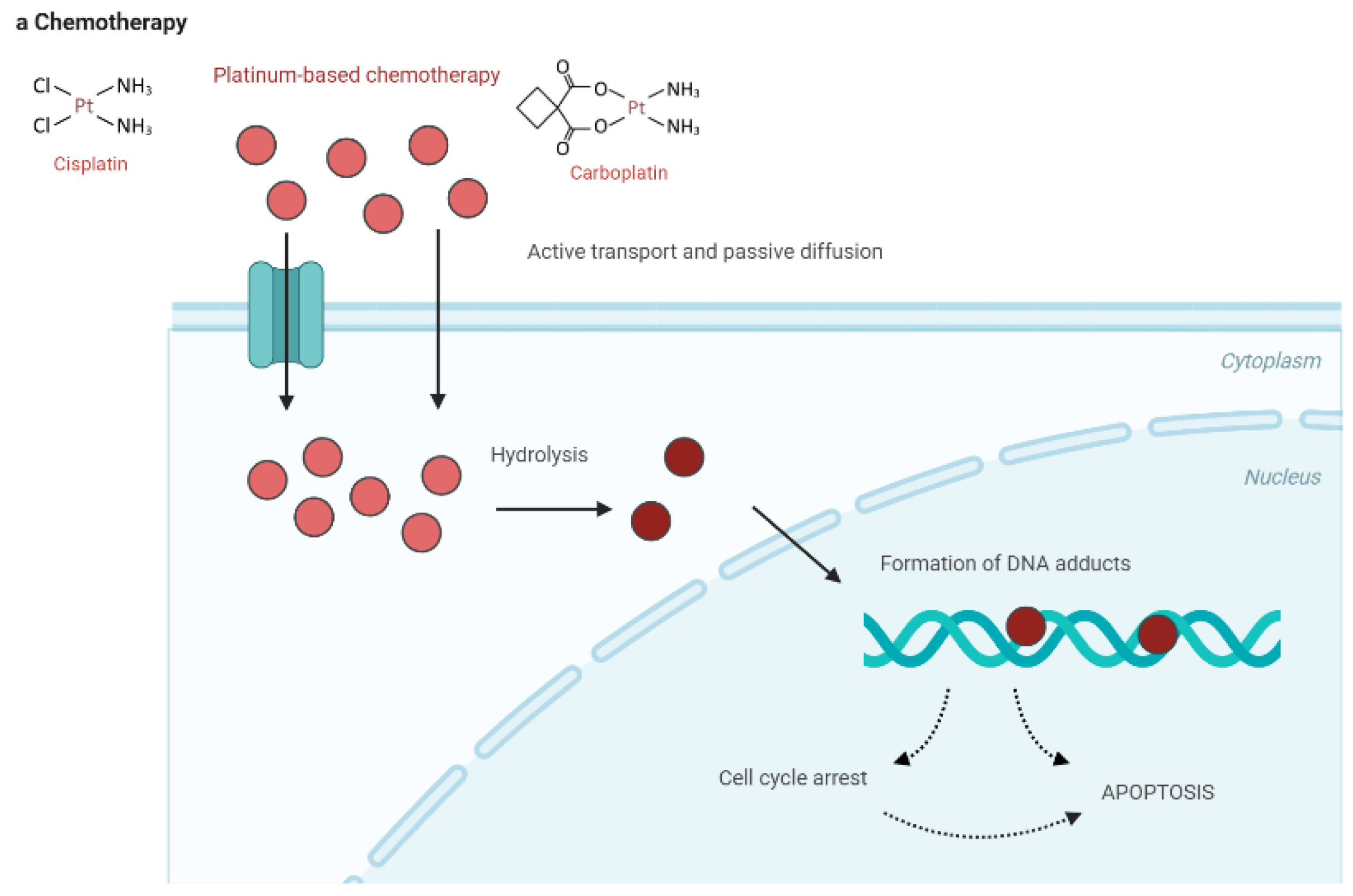
2.1. Platinum-Based Chemotherapy
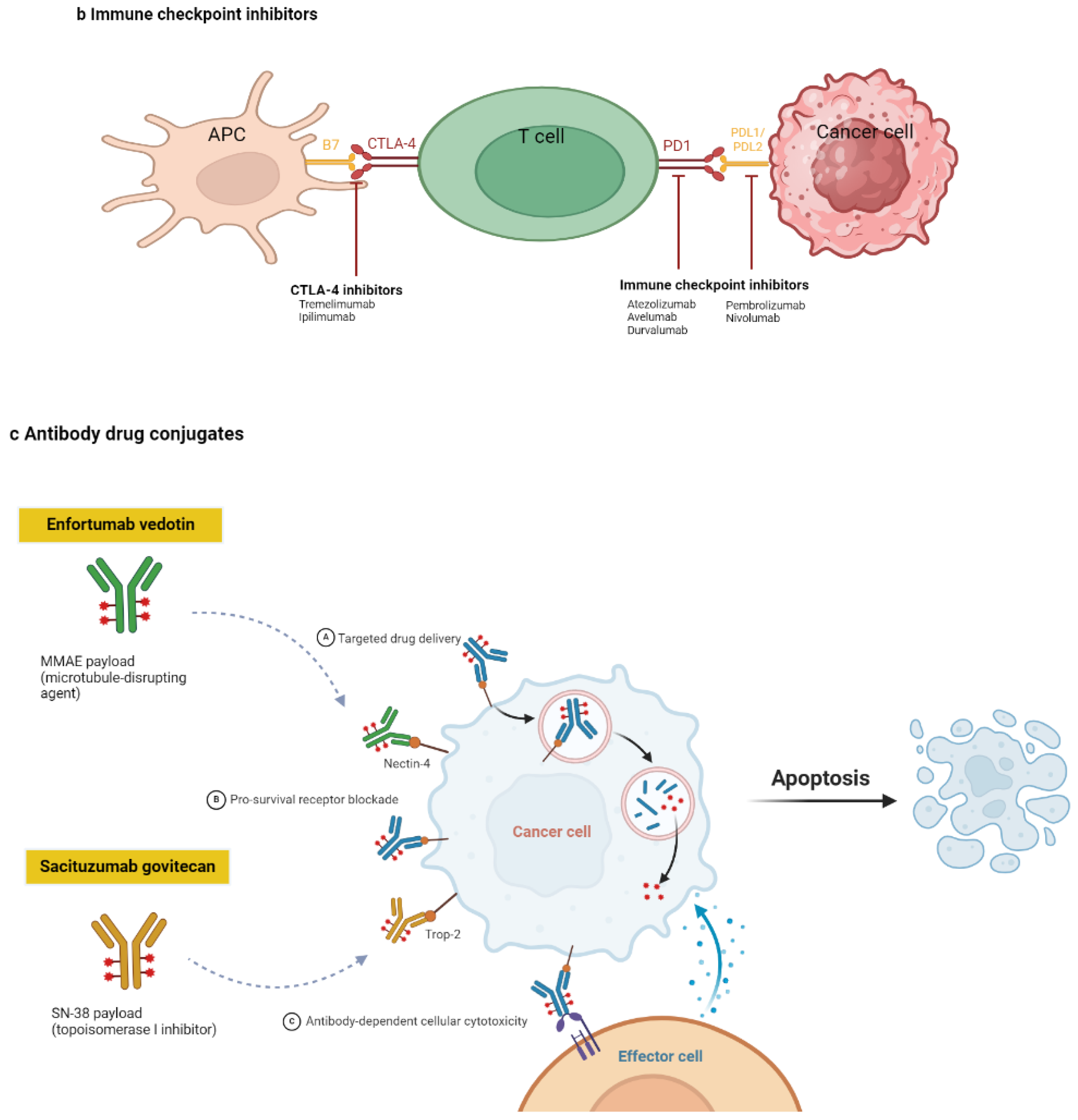
2.2. ICIs
2.3. ADCs

3. Patient Selection
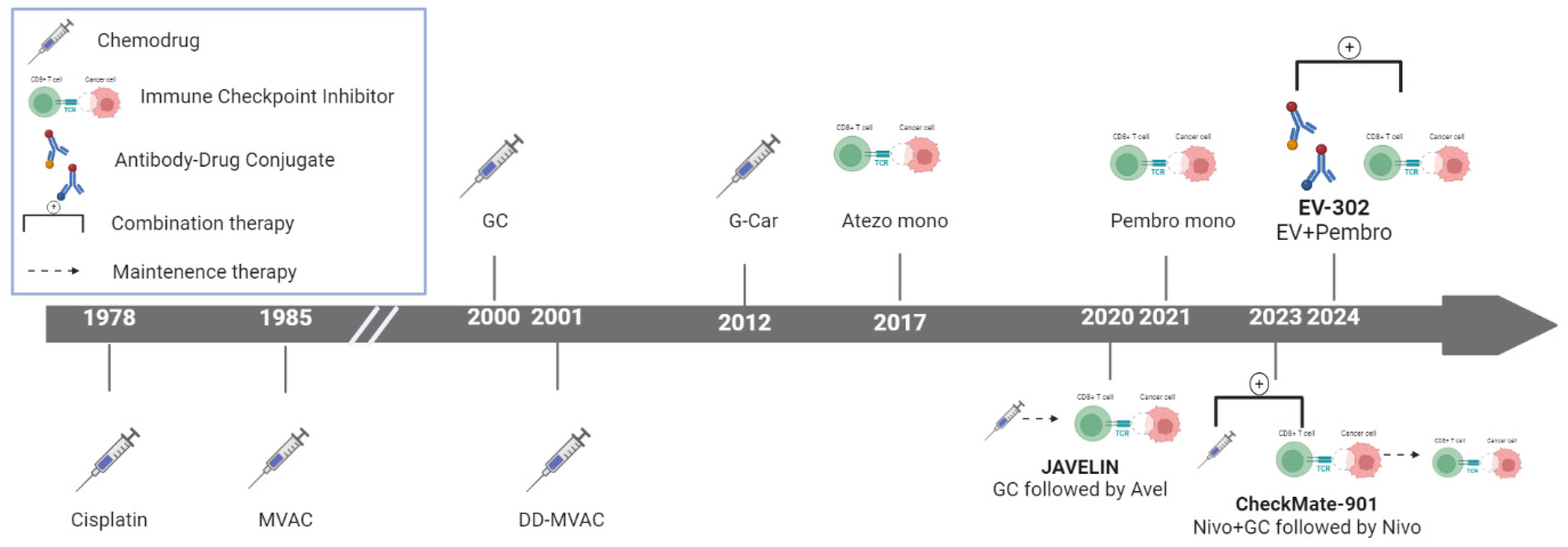
4. Clinical Development
4.1. Chemotherapy
4.2. Immunotherapy
4.2.1. First-Line Monotherapy for Platinum-Ineligible Patients
4.2.2. First-Line Combination Therapy
4.2.3. Maintenance Therapy
4.3. EV Combination Therapy
4.3.1. EV-302 and JAVELIN Paradigm Versus CheckMate-901

| Table 2. Trial. | Intervention arm | Control arm | Median PFS in the intervention arm (months) | Median PFS in the control arm (months) | Hazard ratio (HR) (95% CI) | P-value | Median OS in the intervention arm (months) | Median OS in the control arm (months) | Hazard ratio (HR) (95% CI) | P-value | CR (%) | Adverse events |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| De Santis et al. 2009 50 | Gemcitabine/Carboplatin | Methotrexate/Carboplatin/Vinblastine | Not available | Not available | 9.3 | 8.1 | ||||||
| Sternberg et al. 2006 48 | High-dose intensity M-VAC + G-CSF | Classic M-VAC | Not available | Not available | 15.9 | 14.2 | 0.075 | Reduced toxicity with dose-dense M-VAC | ||||
| GC vs MVAC 45 | Gemcitabine + Cisplatin | MVAC | 7.0 | 7.5 | Similar HR | 0.8 | 14.0 | 15.2 | Similar HR | 0.6 | GC better tolerability, lower toxicity (grade 3+ AE) | |
| KEYNOTE-901 67 | Nivolumab + GC | Gemcitabine-cisplatin | 7.9 | 7.6 | 0.78 (0.63–0.96) | 0.02 | 21.7 | 18.9 | 0.78 (0.63–0.96) | 0.02 | Grade 3+ TRAEs 61.8% vs 51.7% | |
| JAVELIN-100 71 | Avelumab (maintenance) | Best Supportive Care | 5.5 | 2.1 | 0.69 (0.56–0.86) | 0.001 | 21.4 | 14.3 | 0.69 (0.56–0.86) | 0.001 | Grade 3+ TRAEs 47% vs 25% | |
| DANUBE 51 | Durvalumab + tremelimumab | Chemotherapy | 6.7 | 6.9 | 0.85 (0.71–1.02) | 0.075 | 15.1 | 12.1 | 0.85 (0.72–1.02) | 0.054 | Grade 3+ TRAEs 61% vs 50% | |
| IMvigor130 52 | Atezolizumab + chemo | Chemotherapy alone | 8.2 | 6.3 | 0.82 (0.70–0.96) | 0.007 | 16.0 | 13.4 | 0.83 (0.69–1.00) | 0.027 | Grade 3+ TRAEs 81% vs 76% | |
| IMvigor210 59 | Atezolizumab (monotherapy) | No control (single-arm) | 2.7 | N/A | N/A | N/A | 7.9 | N/A | N/A | N/A | Grade 3–4 TRAEs 16% | |
| EV-103 95 | EV + Pembrolizumab | No control (single-arm) | 12.3 | N/A | N/A | N/A | 26.1 | N/A | N/A | N/A | Grade 3–4 TRAEs 54% | |
| EV-302 9 | EV + Pembrolizumab | Standard chemotherapy | 12.5 | 6.3 | 0.45 (0.38–0.54) | <0.001 | 31.5 | 16.1 | 0.47 (0.38–0.58) | <0.001 | Grade 3+ TRAEs 55.9% vs 69.5% | |
| KEYNOTE-052 61 | Pembrolizumab (monotherapy) | No control (single-arm) | 2.1 | N/A | N/A | N/A | 11.3 | N/A | N/A | N/A | Grade 3–4 TRAEs 16% | |
| KEYNOTE-361 64 | Pembrolizumab + chemo | Chemotherapy alone | 8.3 | 7.1 | 0.78 (0.65–0.93) | 0.003 | 17.0 | 14.3 | 0.86 (0.72–1.02) | 0.04 | Grade 3–4 TRAEs 67% vs 63% |
5. Future Perspectives
5.1. Challenges in Optimizing EV Plus Pembrolizumab for Frontline mUC Treatment
5.2. Biomarkers of Response
5.3. Managing Toxicities in Frontline Therapy
6. Conclusions
Author Contributions
Funding information
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nadal, R.; Valderrama, B.P.; Bellmunt, J. Progress in systemic therapy for advanced-stage urothelial carcinoma. Nat. Rev. Clin. Oncol. 2023, 21, 8–27. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Witjes, J.A.; Bruins, H.M.; Cathomas, R.; Compérat, E.M.; Cowan, N.C.; Gakis, G.; Hernández, V.; Espinós, E.L.; Lorch, A.; Neuzillet, Y.; et al. European Association of Urology Guidelines on Muscle-invasive and Metastatic Bladder Cancer: Summary of the 2020 Guidelines. Eur. Urol. 2020, 79, 82–104. [Google Scholar] [CrossRef] [PubMed]
- Moussa, M.J.; Campbell, M.T.; Alhalabi, O. Revisiting Treatment of Metastatic Urothelial Cancer: Where Do Cisplatin and Platinum Ineligibility Criteria Stand? Biomedicines 2024, 12, 519. [Google Scholar] [CrossRef] [PubMed]
- Kwon, W.-A.; Lee, S.-Y.; Jeong, T.Y.; Kim, H.H.; Lee, M.-K. Antibody-Drug Conjugates in Urothelial Cancer: From Scientific Rationale to Clinical Development. Cancers 2024, 16, 2420. [Google Scholar] [CrossRef]
- Suzman, D.L.; Agrawal, S.; Ning, Y.-M.; Maher, V.E.; Fernandes, L.L.; Karuri, S.; Tang, S.; Sridhara, R.; Schroeder, J.; Goldberg, K.B.; et al. FDA Approval Summary: Atezolizumab or Pembrolizumab for the Treatment of Patients with Advanced Urothelial Carcinoma Ineligible for Cisplatin-Containing Chemotherapy. Oncol. 2018, 24, 563–569. [Google Scholar] [CrossRef]
- Benjamin, D.J.; Hsu, R. Treatment approaches for FGFR-altered urothelial carcinoma: targeted therapies and immunotherapy. Front. Immunol. 2023, 14, 1258388. [Google Scholar] [CrossRef]
- Miyake, M.; Shimizu, T.; Oda, Y.; Tachibana, A.; Ohmori, C.; Itami, Y.; Kiba, K.; Tomioka, A.; Yamamoto, H.; Ohnishi, K.; et al. Switch-maintenance avelumab immunotherapy following first-line chemotherapy for patients with advanced, unresectable or metastatic urothelial carcinoma: the first Japanese real-world evidence from a multicenter study. Ultrasound Med. Biol. 2022, 53, 253–262. [Google Scholar] [CrossRef]
- Powles, T.; Valderrama, B.P.; Gupta, S.; Bedke, J.; Kikuchi, E.; Hoffman-Censits, J.; Iyer, G.; Vulsteke, C.; Park, S.H.; Shin, S.J.; et al. Enfortumab Vedotin and Pembrolizumab in Untreated Advanced Urothelial Cancer. New Engl. J. Med. 2024, 390, 875–888. [Google Scholar] [CrossRef]
- Yu, P.; Zhu, C.; You, X.; Gu, W.; Wang, X.; Wang, Y.; Bu, R.; Wang, K. The combination of immune checkpoint inhibitors and antibody-drug conjugates in the treatment of urogenital tumors: a review insights from phase 2 and 3 studies. Cell Death Dis. 2024, 15, 1–19. [Google Scholar] [CrossRef]
- Thomas, V.M.; Jo, Y.; Tripathi, N.; Roy, S.; Chigarira, B.; Narang, A.; Gebrael, G.; Chehade, C.H.; Sayegh, N.; Fortuna, G.G.; et al. Treatment Patterns and Attrition With Lines of Therapy for Advanced Urothelial Carcinoma in the US. JAMA Netw. Open 2024, 7, e249417–e249417. [Google Scholar] [CrossRef] [PubMed]
- Dasari, S.; Tchounwou, P.B. Cisplatin in cancer therapy: Molecular mechanisms of action. Eur. J. Pharmacol. 2014, 740, 364–378. [Google Scholar] [CrossRef] [PubMed]
- Forgie, B.N.; Prakash, R.; Telleria, C.M. Revisiting the Anti-Cancer Toxicity of Clinically Approved Platinating Derivatives. Int. J. Mol. Sci. 2022, 23, 15410. [Google Scholar] [CrossRef] [PubMed]
- Sazonova, E.V.; Kopeina, G.S.; Imyanitov, E.N.; Zhivotovsky, B. Platinum drugs and taxanes: can we overcome resistance? Cell Death Discov. 2021, 7, 1–10. [Google Scholar] [CrossRef]
- Shiravand, Y.; Khodadadi, F.; Kashani, S.M.A.; Hosseini-Fard, S.R.; Hosseini, S.; Sadeghirad, H.; Ladwa, R.; O’byrne, K.; Kulasinghe, A. Immune Checkpoint Inhibitors in Cancer Therapy. Curr. Oncol. 2022, 29, 3044–3060. [Google Scholar] [CrossRef]
- Meng, L.; Wu, H.; Wu, J.; Ding, P.; He, J.; Sang, M.; Liu, L. Mechanisms of immune checkpoint inhibitors: insights into the regulation of circular RNAS involved in cancer hallmarks. Cell Death Dis. 2024, 15, 1–26. [Google Scholar] [CrossRef]
- Cai, X.; Zhan, H.; Ye, Y.; Yang, J.; Zhang, M.; Li, J.; Zhuang, Y. Current Progress and Future Perspectives of Immune Checkpoint in Cancer and Infectious Diseases. Front. Genet. 2021, 12, 785153. [Google Scholar] [CrossRef]
- Qin, S.; Xu, L.; Yi, M.; Yu, S.; Wu, K.; Luo, S. Novel immune checkpoint targets: moving beyond PD-1 and CTLA-4. Mol. Cancer 2019, 18, 155. [Google Scholar] [CrossRef]
- Wojtukiewicz, M.Z.; Rek, M.M.; Karpowicz, K.; Górska, M.; Polityńska, B.; Wojtukiewicz, A.M.; Moniuszko, M.; Radziwon, P.; Tucker, S.C.; Honn, K.V. Inhibitors of immune checkpoints—PD-1, PD-L1, CTLA-4—new opportunities for cancer patients and a new challenge for internists and general practitioners. Cancer Metastasis Rev. 2021, 40, 949–982. [Google Scholar] [CrossRef]
- Martins, F.; Sofiya, L.; Sykiotis, G.P.; Lamine, F.; Maillard, M.; Fraga, M.; Shabafrouz, K.; Ribi, C.; Cairoli, A.; Guex-Crosier, Y.; et al. Adverse effects of immune-checkpoint inhibitors: Epidemiology, management and surveillance. Nat. Rev. Clin. Oncol. 2019, 16, 563–580. [Google Scholar] [CrossRef]
- Han Y, Liu D, Li L. PD-1/PD-L1 pathway: current researches in cancer. Am J Cancer Res. 2020, 10, 727–742.
- Gao, M.; Shi, J.; Xiao, X.; Yao, Y.; Chen, X.; Wang, B.; Zhang, J. PD-1 regulation in immune homeostasis and immunotherapy. Cancer Lett. 2024, 588, 216726. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, C.; Luong, G.; Sun, Y. A snapshot of the PD-1/PD-L1 pathway. J. Cancer 2021, 12, 2735–2746. [Google Scholar] [CrossRef] [PubMed]
- Fu, Z.; Li, S.; Han, S.; Shi, C.; Zhang, Y. Antibody drug conjugate: the “biological missile” for targeted cancer therapy. Signal Transduct. Target. Ther. 2022, 7, 1–25. [Google Scholar] [CrossRef]
- Parit, S.; Manchare, A.; Gholap, A.D.; Mundhe, P.; Hatvate, N.; Rojekar, S.; Patravale, V. Antibody-Drug Conjugates: A promising breakthrough in cancer therapy. Int. J. Pharm. 2024, 659, 124211. [Google Scholar] [CrossRef]
- Nguyen, T.D.; Bordeau, B.M.; Balthasar, J.P. Mechanisms of ADC Toxicity and Strategies to Increase ADC Tolerability. Cancers 2023, 15, 713. [Google Scholar] [CrossRef]
- Marei, H.E.; Cenciarelli, C.; Hasan, A. Potential of antibody–drug conjugates (ADCs) for cancer therapy. Cancer Cell Int. 2022, 22, 1–12. [Google Scholar] [CrossRef]
- Aggarwal, D.; Yang, J.; Salam, A.; Sengupta, S.; Al-Amin, Y.; Mustafa, S.; Khan, M.A.; Huang, X.; Pawar, J.S. Antibody-drug conjugates: the paradigm shifts in the targeted cancer therapy. Front. Immunol. 2023, 14, 1203073. [Google Scholar] [CrossRef]
- Hemenway, G.; Anker, J.F.; Riviere, P.; Rose, B.S.; Galsky, M.D.; Ghatalia, P. Advancements in Urothelial Cancer Care: Optimizing Treatment for Your Patient. Am. Soc. Clin. Oncol. Educ. Book 2024, 44, e432054. [Google Scholar] [CrossRef]
- Bellmunt, J.; Mottet, N.; De Santis, M. Urothelial carcinoma management in elderly or unfit patients. Eur. J. Cancer Suppl. 2016, 14, 1–20. [Google Scholar] [CrossRef]
- Galsky, M.D.; Ma, E.; Shah-Manek, B.; Mills, R.; Ha, L.; Krebsbach, C.; Blouin, E.; Tayama, D.; Ogale, S. Cisplatin Ineligibility for Patients With Metastatic Urothelial Carcinoma: A Survey of Clinical Practice Perspectives Among US Oncologists. Bl. Cancer 2019, 5, 281–288. [Google Scholar] [CrossRef]
- Motwani, S.S.; Sandhu, S.K.; Kitchlu, A. Cisplatin Nephrotoxicity: Novel Insights Into Mechanisms and Preventative Strategies. Semin. Nephrol. 2023, 42, 151341. [Google Scholar] [CrossRef] [PubMed]
- Powles, T.; Bellmunt, J.; Comperat, E.; De Santis, M.; Huddart, R.; Loriot, Y.; Necchi, A.; Valderrama, B.; Ravaud, A.; Shariat, S.; et al. ESMO Clinical Practice Guideline interim update on first-line therapy in advanced urothelial carcinoma. Ann. Oncol. 2024, 35, 485–490. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Andreev-Drakhlin, A.; Fajardo, O.; Fassò, M.; A Garcia, J.; Wee, C.; Schröder, C. Platinum ineligibility and survival outcomes in patients with advanced urothelial carcinoma receiving first-line treatment. JNCI J. Natl. Cancer Inst. 2023, 116, 547–554. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Bellmunt, J.; Plimack, E.R.; Sonpavde, G.P.; Grivas, P.; Apolo, A.B.; Pal, S.K.; Siefker-Radtke, A.O.; Flaig, T.W.; Galsky, M.D.; et al. Defining “platinum-ineligible” patients with metastatic urothelial cancer (mUC). J. Clin. Oncol. 2022, 40, 4577–4577. [Google Scholar] [CrossRef]
- de Wit, R. Overview of bladder cancer trials in the European Organization for Research and Treatment. Cancer 2003, 97, 2120–2126. [Google Scholar] [CrossRef]
- Galsky, M.D.; Hahn, N.M.; Rosenberg, J.; Sonpavde, G.; Hutson, T.; Oh, W.K.; Dreicer, R.; Vogelzang, N.; Sternberg, C.; Bajorin, D.F.; et al. A consensus definition of patients with metastatic urothelial carcinoma who are unfit for cisplatin-based chemotherapy. Lancet Oncol. 2011, 12, 211–214. [Google Scholar] [CrossRef]
- Côté, G.; Alqaisi, H.; Chan, C.T.; Jiang, D.M.; Kandel, C.; Pelletier, K.; Wald, R.; Sridhar, S.S.; Kitchlu, A. Kidney and Cancer Outcomes with Standard Versus Alternative Chemotherapy Regimens for First-Line Treatment of Metastatic Urothelial Carcinoma. Kidney360 2023, 4, e1203–e1211. [Google Scholar] [CrossRef]
- Yang, F.; Wang, J.F.; Wang, Y.; Liu, B.; Molina, J.R. Comparative Analysis of Predictive Biomarkers for PD-1/PD-L1 Inhibitors in Cancers: Developments and Challenges. Cancers 2021, 14, 109. [Google Scholar] [CrossRef]
- Maiorano, B.A.; Di Maio, M.; Cerbone, L.; Maiello, E.; Procopio, G.; Roviello, G.; MeetURO Group; Accettura, C. ; Aieta, M.; Alberti, M.; et al. Significance of PD-L1 in Metastatic Urothelial Carcinoma Treated With Immune Checkpoint Inhibitors. JAMA Netw. Open 2024, 7, e241215. [Google Scholar] [CrossRef]
- Claps, F.; Biasatti, A.; Di Gianfrancesco, L.; Ongaro, L.; Giannarini, G.; Pavan, N.; Amodeo, A.; Simonato, A.; Crestani, A.; Cimadamore, A.; et al. The Prognostic Significance of Histological Subtypes in Patients with Muscle-Invasive Bladder Cancer: An Overview of the Current Literature. J. Clin. Med. 2024, 13, 4349. [Google Scholar] [CrossRef] [PubMed]
- Kamat, A.M.; Apolo, A.B.; Babjuk, M.; Bivalacqua, T.J.; Black, P.C.; Buckley, R.; Campbell, M.T.; Compérat, E.; Efstathiou, J.A.; Grivas, P.; et al. Definitions, End Points, and Clinical Trial Designs for Bladder Cancer: Recommendations From the Society for Immunotherapy of Cancer and the International Bladder Cancer Group. J. Clin. Oncol. 2023, 41, 5437–5447. [Google Scholar] [CrossRef] [PubMed]
- Ascione, C.M.; Napolitano, F.; Esposito, D.; Servetto, A.; Belli, S.; Santaniello, A.; Scagliarini, S.; Crocetto, F.; Bianco, R.; Formisano, L. Role of FGFR3 in bladder cancer: Treatment landscape and future challenges. Cancer Treat. Rev. 2023, 115, 102530. [Google Scholar] [CrossRef] [PubMed]
- Lenis, A.T.; Lec, P.M.; Chamie, K. Bladder cancer: A review. JAMA 2020, 324, 1980–1991. [Google Scholar] [CrossRef]
- Von Der Maase, H.; Hansen, S.W.; Roberts, J.T.; Dogliotti, L.; Oliver, T.; Moore, M.J.; Bodrogi, I.; Albers, P.; Knuth, A.; Lippert, C.M.; et al. Gemcitabine and Cisplatin Versus Methotrexate, Vinblastine, Doxorubicin, and Cisplatin in Advanced or Metastatic Bladder Cancer: Results of a Large, Randomized, Multinational, Multicenter, Phase III Study. J. Clin. Oncol. 2000, 18, 3068–3077. [Google Scholar] [CrossRef]
- von der Maase, H.; Sengelov, L.; Roberts, J.T.; Ricci, S.; Dogliotti, L.; Oliver, T.; Moore, M.J.; Zimmermann, A.; Arning, M. Long-Term Survival Results of a Randomized Trial Comparing Gemcitabine Plus Cisplatin, With Methotrexate, Vinblastine, Doxorubicin, Plus Cisplatin in Patients With Bladder Cancer. J. Clin. Oncol. 2005, 23, 4602–4608. [Google Scholar] [CrossRef]
- Sternberg, C.N.; de Mulder, P.H.; Schornagel, J.H.; Théodore, C.; Fossa, S.D.; van Oosterom, A.T.; Witjes, F.; Spina, M.; van Groeningen, C.J.; de Balincourt, C.; et al. Randomized Phase III Trial of High–Dose-Intensity Methotrexate, Vinblastine, Doxorubicin, and Cisplatin (MVAC) Chemotherapy and Recombinant Human Granulocyte Colony-Stimulating Factor Versus Classic MVAC in Advanced Urothelial Tract Tumors: European Organization for Research and Treatment of Cancer Protocol No. 30924. J. Clin. Oncol. 2001, 19, 2638–2646. [Google Scholar] [CrossRef]
- Sternberg, C.; de Mulder, P.; Schornagel, J.; Theodore, C.; Fossa, S.; van Oosterom, A.; Witjes, J.; Spina, M.; van Groeningen, C.; Duclos, B.; et al. Seven year update of an EORTC phase III trial of high-dose intensity M-VAC chemotherapy and G-CSF versus classic M-VAC in advanced urothelial tract tumours. Eur. J. Cancer 2006, 42, 50–54. [Google Scholar] [CrossRef]
- Bamias, A.; Dafni, U.; Karadimou, A.; Timotheadou, E.; Aravantinos, G.; Psyrri, A.; Xanthakis, I.; Tsiatas, M.; Koutoulidis, V.; Constantinidis, C.; et al. Prospective, open-label, randomized, phase III study of two dose-dense regimens MVAC versus gemcitabine/cisplatin in patients with inoperable, metastatic or relapsed urothelial cancer: a Hellenic Cooperative Oncology Group study (HE 16/03). Ann. Oncol. 2012, 24, 1011–1017. [Google Scholar] [CrossRef]
- De Santis, M.; Bellmunt, J.; Mead, G.; Kerst, J.M.; Leahy, M.; Maroto, P.; Skoneczna, I.; Marreaud, S.; de Wit, R.; Sylvester, R. Randomized Phase II/III Trial Assessing Gemcitabine/ Carboplatin and Methotrexate/Carboplatin/Vinblastine in Patients With Advanced Urothelial Cancer “Unfit” for Cisplatin-Based Chemotherapy: Phase II—Results of EORTC Study 30986. J. Clin. Oncol. 2009, 27, 5634–5639. [Google Scholar] [CrossRef]
- Powles, T.; Castellano, D.; Loriot, Y.; Ogawa, O.; Park, S.H.; De Giorgi, U.; Bögemann, M.; Bamias, A.; Gurney, H.; Fradet, Y.; et al. Durvalumab alone and durvalumab plus tremelimumab versus chemotherapy in previously untreated patients with unresectable, locally advanced or metastatic urothelial carcinoma (DANUBE): a randomised, open-label, multicentre, phase 3 trial. Lancet Oncol. 2020, 21, 1574–1588. [Google Scholar] [CrossRef] [PubMed]
- Galsky, M.D.; Arija, J.Á.A.; Bamias, A.; Davis, I.D.; De Santis, M.; Kikuchi, E.; Garcia-Del-Muro, X.; De Giorgi, U.; Mencinger, M.; Izumi, K.; et al. Atezolizumab with or without chemotherapy in metastatic urothelial cancer (IMvigor130): a multicentre, randomised, placebo-controlled phase 3 trial. Lancet 2020, 395, 1547–1557. [Google Scholar] [CrossRef] [PubMed]
- Powles, T.; Park, S.H.; Voog, E.; Caserta, C.; Valderrama, B.P.; Gurney, H.; Kalofonos, H.; Radulović, S.; Demey, W.; Ullén, A.; et al. Avelumab Maintenance Therapy for Advanced or Metastatic Urothelial Carcinoma. New Engl. J. Med. 2020, 383, 1218–1230. [Google Scholar] [CrossRef] [PubMed]
- Osterman, C.K.; Babu, D.S.; Geynisman, D.M.; Lewis, B.; Somer, R.A.; Balar, A.V.; Zibelman, M.R.; Guancial, E.A.; Antinori, G.; Yu, S.; et al. Efficacy of Split Schedule Versus Conventional Schedule Neoadjuvant Cisplatin-Based Chemotherapy for Muscle-Invasive Bladder Cancer. Oncol. 2019, 24, 688–690. [Google Scholar] [CrossRef]
- Mourey, L.; Flechon, A.; Tosi, D.; Lacourtoisie, S.A.; Joly, F.; Guillot, A.; Loriot, Y.; Dauba, J.; Roubaud, G.; Rolland, F.; et al. Vefora, GETUG-AFU V06 study: Randomized multicenter phase II/III trial of fractionated cisplatin (CI)/gemcitabine (G) or carboplatin (CA)/g in patients (pts) with advanced urothelial cancer (UC) with impaired renal function (IRF)—Results of a planned interim analysis. J. Clin. Oncol. 2020, 38, 461–461. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network (NCCN) Guidelines Version 4.2024 "Bladder Cancer". Available online: https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1417 (accessed on 13 September 2024).
- Grivas, P.; Grande, E.; Davis, I.; Moon, H.; Grimm, M.-O.; Gupta, S.; Barthélémy, P.; Thibault, C.; Guenther, S.; Hanson, S.; et al. Avelumab first-line maintenance treatment for advanced urothelial carcinoma: review of evidence to guide clinical practice. ESMO Open 2023, 8, 102050. [Google Scholar] [CrossRef]
- Zhang, T.; Tan, A.; Shah, A.Y.; Iyer, G.; Morris, V.; Michaud, S.; Sridhar, S.S. Reevaluating the role of platinum-based chemotherapy in the evolving treatment landscape for patients with advanced urothelial carcinoma. Oncol. 2024. [Google Scholar] [CrossRef]
- Balar, A.V.; Galsky, M.D.; Rosenberg, J.E.; et al. Atezolizumab as first-line treatment in cisplatin-ineligible patients with locally advanced and metastatic urothelial carcinoma: a single-arm, multicentre, phase 2 trial. Lancet 2017, 389, 67–76. [Google Scholar] [CrossRef]
- Powles, T.; Walker, J.; Williams, J.A.; Bellmunt, J. The evolving role of PD-L1 testing in patients with metastatic urothelial carcinoma. Cancer Treat. Rev. 2019, 82, 101925. [Google Scholar] [CrossRef]
- Vuky, J.; Balar, A.V.; Castellano, D.; O’donnell, P.H.; Grivas, P.; Bellmunt, J.; Powles, T.; Bajorin, D.; Hahn, N.M.; Savage, M.J.; et al. Long-Term Outcomes in KEYNOTE-052: Phase II Study Investigating First-Line Pembrolizumab in Cisplatin-Ineligible Patients With Locally Advanced or Metastatic Urothelial Cancer. J. Clin. Oncol. 2020, 38, 2658–2666. [Google Scholar] [CrossRef]
- Ghatalia, P.; Zibelman, M.; Geynisman, D.M.; Plimack, E.R. First-line Immunotherapy in Metastatic Urothelial Carcinoma. Eur. Urol. Focus 2019, 6, 45–47. [Google Scholar] [CrossRef] [PubMed]
- Rhea, L.P.; Aragon-Ching, J.B. Advances and Controversies With Checkpoint Inhibitors in Bladder Cancer. Clin. Med. Insights: Oncol. 2021, 15. [Google Scholar] [CrossRef] [PubMed]
- Powles, T.; Matsubara, N.; Cheng, S.Y.-S.; Fradet, Y.; Oudard, S.; Vulsteke, C.; Barrera, R.M.; Gunduz, S.; Loriot, Y.; Rodriguez-Vida, A.; et al. Pembrolizumab alone or combined with chemotherapy versus chemotherapy as first-line therapy for advanced urothelial carcinoma (KEYNOTE-361): a randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 931–945. [Google Scholar] [CrossRef] [PubMed]
- Grande, E.; Bamias, A.; Galsky, M.D.; Kikuchi, E.; Davis, I.D.; Arranz, J.A.; Rezazadeh, A.; del Muro, X.G.; Park, S.H.; De Giorgi, U.; et al. Overall survival (OS) by response to first-line (1L) induction treatment with atezolizumab (atezo) + platinum/gemcitabine (plt/gem) vs placebo + plt/gem in patients (pts) with metastatic urothelial carcinoma (mUC): Updated data from the IMvigor130 OS final analysis. J. Clin. Oncol. 2023, 41, 4503–4503. [Google Scholar] [CrossRef]
- Galsky, M.D.; Necchi, A.; Sridhar, S.S.; Ogawa, O.; Angra, N.; Hois, S.; Xiao, F.; Goluboff, E.; Bellmunt, J. A phase III, randomized, open-label, multicenter, global study of first-line durvalumab plus standard of care (SoC) chemotherapy and durvalumab plus tremelimumab, and SoC chemotherapy versus SoC chemotherapy alone in unresectable locally advanced or metastatic urothelial cancer (NILE). J. Clin. Oncol. 2021, 39, TPS504–TPS504. [Google Scholar] [CrossRef]
- van der Heijden, M.S.; Sonpavde, G.; Powles, T.; Necchi, A.; Burotto, M.; Schenker, M.; Sade, J.P.; Bamias, A.; Beuzeboc, P.; Bedke, J.; et al. Nivolumab plus Gemcitabine–Cisplatin in Advanced Urothelial Carcinoma. New Engl. J. Med. 2023, 389, 1778–1789. [Google Scholar] [CrossRef]
- Houssiau, H.; Seront, E. Improving the role of immune checkpoint inhibitors in the management of advanced urothelial carcinoma, where do we stand? Transl. Oncol. 2022, 19, 101387. [Google Scholar] [CrossRef]
- Galsky, M.D.; Guan, X.; Banchereau, R.; Wang, L.; Zhu, J.; Yu, H.; Rishipathak, D.; Hajaj, E.; Herbst, R.; Davis, I.; et al. 658MO Cisplatin (cis)-related immunomodulation and efficacy with atezolizumab (atezo) + cis- vs carboplatin (carbo)-based chemotherapy (chemo) in metastatic urothelial cancer (mUC). Ann. Oncol. 2021, 32, S682–S683. [Google Scholar] [CrossRef]
- Kwon, W.-A.; Seo, H.K. Emerging agents for the treatment of metastatic urothelial cancer. Investig. Clin. Urol. 2021, 62, 243–255. [Google Scholar] [CrossRef]
- Powles, T.; Park, S.H.; Caserta, C.; Valderrama, B.P.; Gurney, H.; Ullén, A.; Loriot, Y.; Sridhar, S.S.; Sternberg, C.N.; Bellmunt, J.; et al. Avelumab First-Line Maintenance for Advanced Urothelial Carcinoma: Results From the JAVELIN Bladder 100 Trial After ≥2 Years of Follow-Up. J. Clin. Oncol. 2023, 41, 3486–3492. [Google Scholar] [CrossRef]
- Bracarda, S.; Antonuzzo, L.; Maruzzo, M.; Santini, D.; Tambaro, R.; Buti, S.; Carrozza, F.; Calabrò, F.; Di Lorenzo, G.; Fornarini, G.; et al. Subgroup analyses from READY: Real-world data from an Italian compassionate use program (CUP) of avelumab first-line maintenance (1LM) treatment for locally advanced or metastatic urothelial carcinoma (la/mUC). J. Clin. Oncol. 2024, 42, 558–558. [Google Scholar] [CrossRef]
- Barthelemy, P.; Loriot, Y.; Voog, E.; Eymard, J.C.; Ravaud, A.; Flechon, A.; Jaillon, C.A.; Chasseray, M.; Lorgis, V.; Hilgers, W.; et al. Full analysis from AVENANCE: A real-world study of avelumab first-line (1L) maintenance treatment in patients (pts) with advanced urothelial carcinoma (aUC). J. Clin. Oncol. 2023, 41, 471–471. [Google Scholar] [CrossRef]
- Srinivasalu, V.K.; Robbrecht, D. Advancements in First-Line Treatment of Metastatic Bladder Cancer: EV-302 and Checkmate-901 Insights and Future Directions. Cancers 2024, 16, 2398. [Google Scholar] [CrossRef] [PubMed]
- O'Donnell, P.H.; Milowsky, M.I.; Petrylak, D.P.; Hoimes, C.J.; Flaig, T.W.; Mar, N.; Moon, H.H.; Friedlander, T.W.; McKay, R.R.; Bilen, M.A.; et al. Enfortumab Vedotin With or Without Pembrolizumab in Cisplatin-Ineligible Patients With Previously Untreated Locally Advanced or Metastatic Urothelial Cancer. J. Clin. Oncol. 2023, 41, 4107–4117. [Google Scholar] [CrossRef]
- Lin, Y.-T.; Wang, C.; He, X.-Y.; Yao, Q.-M.; Chen, J. Comparative cost-effectiveness of first-line pembrolizumab plus chemotherapy vs. chemotherapy alone in persistent, recurrent, or metastatic cervical cancer. Front. Immunol. 2024, 14, 1345942. [Google Scholar] [CrossRef]
- Li A, Wu M, Xie O.; et al. Cost-effectiveness of First-Line Enfortumab Vedotin in Addition to Pembrolizumab for Metastatic Urothelial Carcinoma in the United States. Frontiers in Immunology. 15, 1464092.
- Rosenberg, J.E.; O’Donnell, P.H.; Balar, A.V.; McGregor, B.A.; Heath, E.I.; Yu, E.Y.; Galsky, M.D.; Hahn, N.M.; Gartner, E.M.; Pinelli, J.M.; et al. Pivotal Trial of Enfortumab Vedotin in Urothelial Carcinoma After Platinum and Anti-Programmed Death 1/Programmed Death Ligand 1 Therapy. J. Clin. Oncol. 2019, 37, 2592–2600. [Google Scholar] [CrossRef]
- Tang, M.; Garg, A.; Bonate, P.L.; Rosenberg, J.E.; Matsangou, M.; Kadokura, T.; Yamada, A.; Choules, M.; Pavese, J.; Nagata, M.; et al. Clinical Pharmacology of the Antibody–Drug Conjugate Enfortumab Vedotin in Advanced Urothelial Carcinoma and Other Malignant Solid Tumors. Clin. Pharmacokinet. 2024, 63, 423–438. [Google Scholar] [CrossRef]
- Bajorin, D.F.; Dodd, P.M.; Mazumdar, M.; Fazzari, M.; McCaffrey, J.A.; Scher, H.I.; Herr, H.; Higgins, G.; Boyle, M.G. Long-Term Survival in Metastatic Transitional-Cell Carcinoma and Prognostic Factors Predicting Outcome of Therapy. J. Clin. Oncol. 1999, 17, 3173–3181. [Google Scholar] [CrossRef]
- Sonpavde, G.; Manitz, J.; Gao, C.; Tayama, D.; Kaiser, C.; Hennessy, D.; Makari, D.; Gupta, A.; Abdullah, S.E.; Niegisch, G.; et al. Five-Factor Prognostic Model for Survival of Post-Platinum Patients with Metastatic Urothelial Carcinoma Receiving PD-L1 Inhibitors. J. Urol. 2020, 204, 1173–1179. [Google Scholar] [CrossRef]
- Liu, D.; Plimack, E.R.; Hoffman-Censits, J.; Garraway, L.A.; Bellmunt, J.; Van Allen, E.; Rosenberg, J.E. Clinical Validation of Chemotherapy Response BiomarkerERCC2in Muscle-Invasive Urothelial Bladder Carcinoma. JAMA Oncol. 2016, 2, 1094–1096. [Google Scholar] [CrossRef]
- Bellmunt, J.; Nadal, R. Enfortumab vedotin and pembrolizumab combination as a relevant game changer in urothelial carcinoma: What is left behind? Med 2024, 5, 490–492. [Google Scholar] [CrossRef] [PubMed]
- Santoni, M.; Takeshita, H.; Massari, F.; Bamias, A.; Cerbone, L.; Fiala, O.; Mollica, V.; Buti, S.; Santoni, A.; Bellmunt, J. Pembrolizumab plus enfortumab vedotin in urothelial cancer. Nat. Rev. Urol. 2024, 21, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Patel, D.M.; Mateen, R.; Qaddour, N.; Carrillo, A.; Verschraegen, C.; Yang, Y.; Li, Z.; Sundi, D.; Mortazavi, A.; Collier, K.A. A Comprehensive Review of Immunotherapy Clinical Trials for Metastatic Urothelial Carcinoma: Immune Checkpoint Inhibitors Alone or in Combination, Novel Antibodies, Cellular Therapies, and Vaccines. Cancers 2024, 16, 335. [Google Scholar] [CrossRef] [PubMed]
- Tan, W.S.; Tan, M.-Y.; Alhalabi, O.; Campbell, M.T.; Kamat, A.M.; Gao, J. Evolving systemic management of urothelial cancers. Curr. Opin. Oncol. 2023, 35, 186–199. [Google Scholar] [CrossRef]
- Grivas, P.; Pouessel, D.; Park, C.H.; Barthelemy, P.; Bupathi, M.; Petrylak, D.P.; Agarwal, N.; Gupta, S.; Fléchon, A.; Ramamurthy, C.; et al. Sacituzumab Govitecan in Combination With Pembrolizumab for Patients With Metastatic Urothelial Cancer That Progressed After Platinum-Based Chemotherapy: TROPHY-U-01 Cohort 3. J. Clin. Oncol. 2024, 42, 1415–1425. [Google Scholar] [CrossRef]
- Tonni, E.; Oltrecolli, M.; Pirola, M.; Tchawa, C.; Roccabruna, S.; D’agostino, E.; Matranga, R.; Piombino, C.; Pipitone, S.; Baldessari, C.; et al. New Advances in Metastatic Urothelial Cancer: A Narrative Review on Recent Developments and Future Perspectives. Int. J. Mol. Sci. 2024, 25, 9696. [Google Scholar] [CrossRef]
- Parent, P.; Marcq, G.; Adeleke, S.; Turpin, A.; Boussios, S.; Rassy, E.; Penel, N. Predictive biomarkers for immune checkpoint inhibitor response in urothelial cancer. Ther. Adv. Med Oncol. 2023, 15. [Google Scholar] [CrossRef]
- Queiroz, M.M.; de Souza, Z.S.; Gongora, A.B.L.; Barbosa, F.d.G.; Buchpiguel, C.A.; de Castro, M.G.; de Macedo, M.P.; Coelho, R.F.; Soko, E.S.; Camargo, A.A.; et al. Emerging biomarkers in metastatic urothelial carcinoma: tumour mutational burden, PD-L1 expression and APOBEC polypeptide-like signature in a patient with complete response to anti-programmed cell death protein-1 inhibitor. ecancermedicalscience 2021, 15, 1306. [Google Scholar] [CrossRef]
- Zhou, Y.; Tao, L.; Qiu, J.; Xu, J.; Yang, X.; Zhang, Y.; Tian, X.; Guan, X.; Cen, X.; Zhao, Y. Tumor biomarkers for diagnosis, prognosis and targeted therapy. Signal Transduct. Target. Ther. 2024, 9, 132. [Google Scholar] [CrossRef]
- Rodriguez, J.; Baldini, C.; Bayle, A.; Pages, A.; Danlos, F.X.; Vasseur, D.; Rouleau, E.; Lacroix, L.; de Castro, B.A.; Goldschmidt, V.; et al. Impact of Clonal Hematopoiesis–Associated Mutations in Phase I Patients Treated for Solid Tumors: An Analysis of the STING Trial. JCO Precis. Oncol. 2024, 8, e2300631. [Google Scholar] [CrossRef]
- Brower, B.; McCoy, A.; Ahmad, H.; Eitman, C.; Bowman, I.A.; Rembisz, J.; Milowsky, M.I. Managing potential adverse events during treatment with enfortumab vedotin + pembrolizumab in patients with advanced urothelial cancer. Front. Oncol. 2024, 14, 1326715. [Google Scholar] [CrossRef] [PubMed]
- Pretelli, G.; Mati, K.; Motta, L.; Stathis, A. Antibody-drug conjugates combinations in cancer treatment. Explor. Target. Anti-tumor Ther. 2024, 5, 714–741. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Rosenberg, J.E.; McKay, R.R.; Flaig, T.W.; Petrylak, D.P.; Hoimes, C.J.; Friedlander, T.W.; Bilen, M.A.; Srinivas, S.; Burgess, E.F.; et al. Study EV-103 dose escalation/cohort A: Long-term outcome of enfortumab vedotin + pembrolizumab in first-line (1L) cisplatin-ineligible locally advanced or metastatic urothelial carcinoma (la/mUC) with nearly 4 years of follow-up. J. Clin. Oncol. 2023, 41, 4505–4505. [Google Scholar] [CrossRef]
| Criteria | Category | Frontline therapy Options |
|---|---|---|
| Cisplatin Eligibility 4, 31, 34 | Cisplatin-Eligible (eGFR ≥ 60 mL/min/1.73 m²) | - Gemcitabine + Cisplatin (standard of care) - Dose-dense MVAC (Methotrexate, Vinblastine, Doxorubicin, and Cisplatin) - Avelumab maintenance therapy after a response or stable disease following 4-6 cycles of chemotherapy. |
| Cisplatin-Ineligible (eGFR < 60 mL/ min/1.73 m²) | - Gemcitabine + Carboplatin (standard alternative) - Atezolizumab or Pembrolizumab (in patients with high PD-L1 expression or those who are not candidates for any platinum therapy) - Avelumab maintenance therapy following stable disease or response to chemotherapy. |
|
| PD-L1 Expression | High PD-L1 (Cisplatin-Ineligible) | - Atezolizumab or Pembrolizumab (preferred for patients who cannot tolerate any platinum-based therapy and have high PD-L1 expression). These immune checkpoint inhibitors can be used as first-line monotherapy. |
| Low PD-L1 (Cisplatin-Ineligible) | - Gemcitabine + Carboplatin (preferred first-line for platinum-ineligible patients with low PD-L1 expression). Immunotherapy with pembrolizumab or atezolizumab is generally reserved for second-line use or maintenance therapy in these cases. | |
| Performance Status (ECOG) | ECOG 0-1 | - These patients typically tolerate platinum-based chemotherapy well, and cisplatin-based regimens are the standard. If cisplatin-ineligible, carboplatin-based regimens or PD-L1-targeted immunotherapy can be considered, especially in PD-L1 positive patients. |
| ECOG 2 | - For patients with moderate performance status (ECOG 2), carboplatin-based chemotherapy is preferred, as cisplatin may be too toxic. Immunotherapy is another option, especially in patients with high PD-L1 expression. | |
| ECOG ≥ 3 | - Patients with poor performance status are generally not good candidates for chemotherapy. Atezolizumab or pembrolizumab monotherapy may be considered, especially in those with high PD-L1 expression. Supportive care or clinical trials are also options. | |
| Other Factors | Comorbidities (e.g., cardiovascular disease) | - Patients with significant comorbidities that make cisplatin too toxic are typically treated with carboplatin-based chemotherapy or immunotherapy. Atezolizumab or pembrolizumab may be used for those who are cisplatin-ineligible and PD-L1 positive. |
| Molecular Profiling | FGFR3 or FGFR2 Mutations | - Patients with FGFR mutations who have progressed on platinum-based chemotherapy may be eligible for erdafitinib, an FGFR inhibitor, but this is not used in frontline therapy. However, molecular profiling can inform future treatment lines. |
| Trial. | Intervention arm | Status | Estimated Enrollment / Phase | Patients | Primary End Point |
|---|---|---|---|---|---|
| NCT03682068 (NILE) | Durvalumab + SoC (CT) or Durvalumab + Tremelimumab + SoC vs SoC | Active, not recruiting | 1292 / III | LA or mUC | OS |
| NCT03036098 | Nivolumab + ipilimumab or + SoC CT vs SoC | Active, not recruiting | 1307 / III | LA or mUC | OS, PFS |
| NCT05302284 | RC48-ADC + toripalimab vs CT alone | recruiting | 452 / III | LA or mUC with HER 2 expressing | OS, PFS |
| NCT03967977 | Cis/Car + G + tislelizumab vs Cis/Car + G + placebo | recruiting | 420 / III | LA or mUC | OS |
| NCT03288545 (EV-103) | EV alone or plus other anticancer agents | Active, not recruiting | 348 / I, II | mUC | ORR, pCR, dose escalation |
| NCT05845814 | Pembrolizumab + EV + MK-4280A vs pembrolizumab + EV | Active, not recruiting | 390 / I, IIb | LA or mUC | ORR, AEs, DLT |
| NCT05645692 | RO7247669 ± tiragolumab vs atezolizumab | Recruiting | 240 / II | LA or mUC platinum ineligible | ORR |
| NCT03237780 | Eribulin mesylate + atezolizumab vs atezolizumab alone | Active, not recruiting | 72 / II | LA or mUC cisplatin ineligible | AEs. ORR |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



