Submitted:
11 September 2024
Posted:
11 September 2024
You are already at the latest version
Abstract
This case report demonstrates the rare but potentially serious complication of pulmonary vein stenosis (PVS) diagnosed several years after radiofrequency ablation for atrial fibrillation. Pulmonary vein stenosis can remain asymptomatic until significant occlusion occurs, after which it can present with a variety of symptoms, mimicking numerous cardiovascular and pulmonary pathologies. Early diagnosis and treatment rely on consistent follow-up using appropriate diagnostic imaging modalities, which are paramount in preventing severe complications.
Keywords:
Pulmonary Vein Stenosis
; Catheter Ablation
; Atrial Fibrillation
; Radiofrequency Ablation (RFA)
; Cardiovascular Complications
; Multimodal Imaging
; Computed Tomography Angiography (CTA)
; Pulmonary Hypertension
; Stent Implantation
; Balloon Angioplasty
; Postablation Surveillance
; Pulmonary Vascular Disease
; Pulmonary Perfusion
; Pulmonary Vein Occlusion
; Pulse Electrical Field (PEF) Ablation
Introduction
This case report presents the comprehensive medical journey of a 69-year-old female patient with a history of chronic paroxysmal atrial fibrillation, chronic obstructive pulmonary disease (COPD), and obstructive sleep apnea (OSA). Through a series of six radiofrequency ablation (RFA) procedures done within a span of 5 years aimed at managing her cardiac arrhythmia, the patient's treatment course reflects a multidisciplinary approach encompassing cardiovascular and respiratory health. Recent exacerbation of symptoms prompted detailed evaluation, revealing significant vascular stenosis necessitating targeted interventions to restore pulmonary perfusion. Through diligent medication adherence and collaborative care across institutions, the patient's management exemplifies a holistic approach to optimizing health outcomes.
Case
The patient, a 73-year-old female, presented to our clinic October of 2016 with a history of chronic paroxysmal atrial fibrillation, COPD, OSA, and newly diagnosed pulmonary vein stenosis. She reported experiencing dyspnea during exertion but denied dyspnea at rest, cough, hemoptysis, or wheezing. The patient had a significant medical history, including multiple ablations for atrial fibrillation. Her treatment journey for atrial fibrillation involved six ablation procedures, all performed with RFA, aimed at managing her cardiac arrhythmia. The initial five ablations were performed in 2011 and the subsequent sixth ablation was performed in 2016. Following the last ablation, the patient reported resolution of symptomatic palpitations. However, she continued to endorse ongoing mild to moderate shortness of breath with activity. She also diligently adhered to Eliquis anticoagulation therapy to mitigate thromboembolic risks associated with any ongoing episodes of asymptomatic paroxysmal atrial fibrillation.
During her follow-up at a specialty pulmonary clinic visit in August 2018, further echocardiographic work-up of the patient showed indirect signs like increased pulmonary artery pressures or regional pulmonary hypertension. This was suspect for additional pulmonary pathology. Further referral to an outside specialty pulmonary hypertension clinic with CT angiography revealed left inferior pulmonary vein stenosis. At this time the patient continued to use supplemental oxygen at 2 liters per minute (lpm). The diagnosis of pulmonary vein stenosis added complexity to the patient's respiratory health management, potentially exacerbating symptoms of her pre-existing conditions.
In addition to her cardiac history, the patient faced challenges related to her respiratory health, including Stage II COPD and OSA, both diagnosed in her early 40’s. She had been using CPAP therapy regularly for greater than 15 years with good compliance rates exceeding 90% and minimal apnea-hypopnea index (AHI) levels. However, she reported her PAP generator ceased functioning in July 2019, necessitating a replacement. Her transition from Spiriva and Symbicort to Trelegy in November 2022 reflected optimized COPD management, with considerations for improved symptom control and cost-effectiveness.
Discussion
Acquired pulmonary vein stenosis (PVS) following radiofrequency ablation for atrial fibrillation (AF) has become the primary etiology of this condition, with recent studies indicating an incidence of approximately 2-3% after a single AF ablation procedure.1 Technological advancements in ablation techniques, such as alterations in ablation site and temperature modulation, have contributed to a decline in incidence rates. Initially, ablation techniques focusing on venous ostia resulted in a wide-ranging incidence of PVS, ranging from 3% to 42%, attributed to thermal injury-induced hyperplasia and fibrotic proliferation within the veins.1,2 Despite improvements, the true incidence of PVS remains uncertain due to underdiagnosis stemming from nonspecific symptoms, delayed presentation, and inadequate post-ablation surveillance. Current literature suggests onset of symptoms has been found to be, on average, 3–6 months following ablation.3–5
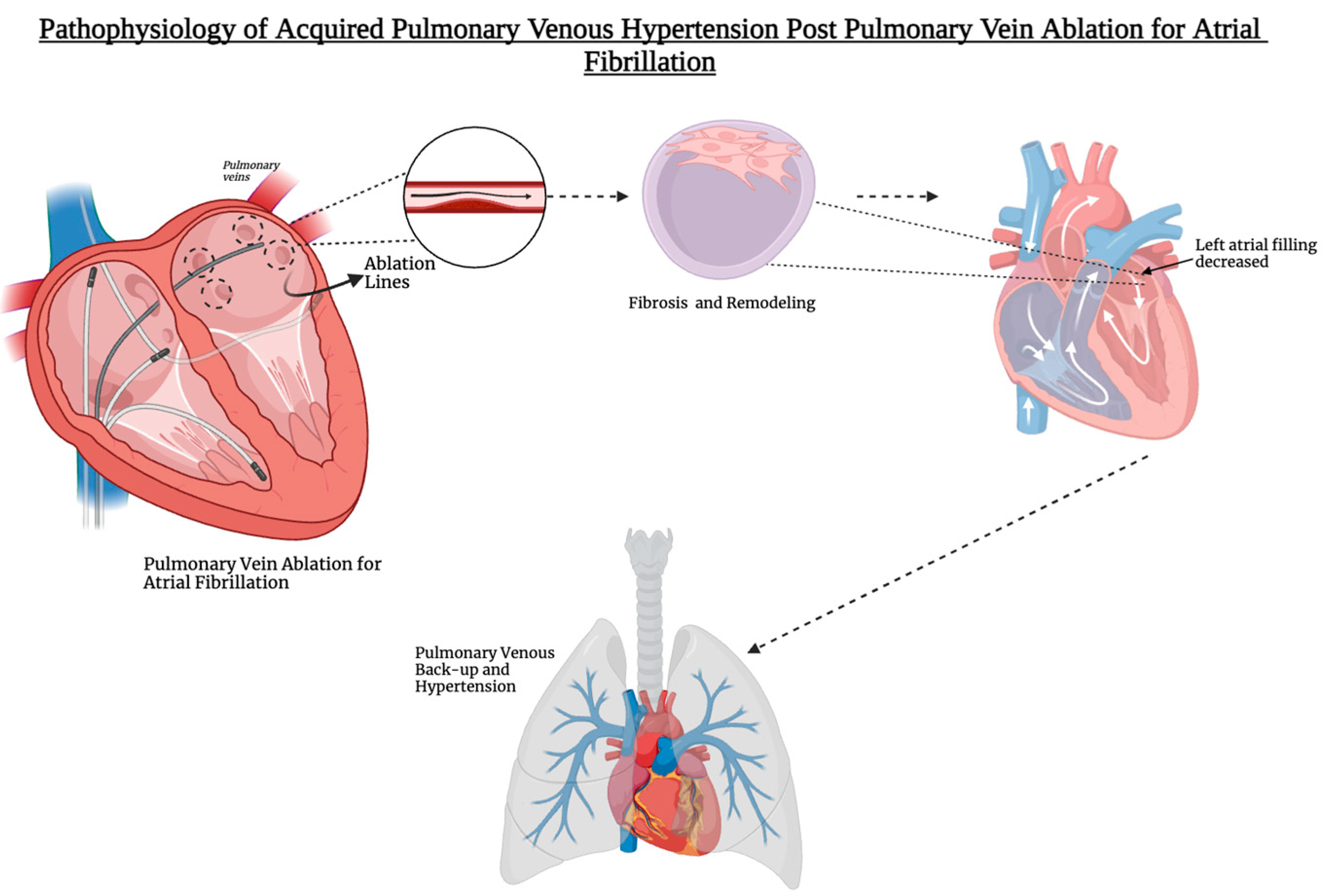
Figure 1.
This figure illustrates the pathophysiology of acquired pulmonary venous hypertension following pulmonary vein ablation for atrial fibrillation. The process begins with ablation lines placed around the pulmonary veins, leading to fibrosis and remodeling of the venous structures. Over time, this can decrease left atrial filling, contributing to pulmonary venous back-up and pulmonary hypertension.
Figure 1.
This figure illustrates the pathophysiology of acquired pulmonary venous hypertension following pulmonary vein ablation for atrial fibrillation. The process begins with ablation lines placed around the pulmonary veins, leading to fibrosis and remodeling of the venous structures. Over time, this can decrease left atrial filling, contributing to pulmonary venous back-up and pulmonary hypertension.
However, as with our patient, this cannot be the time frame used to rule out PVS as our patient developed symptoms and was diagnosed greater 2 years after her last ablation. Concerns regarding underestimation persist due to limited screening beyond the initial 3-month post-procedural period. Additionally, extrinsic compression from mediastinal processes such as sarcoidosis, fibrosing mediastinitis, and adjacent neoplasms, along with complications from cardiovascular surgeries, particularly in the pediatric population following repair of total anomalous pulmonary venous return, can induce PVS.
Clinical assessment, augmented by imaging modalities such as transesophageal echocardiography, computed tomography (CT), magnetic resonance imaging (MRI), and perfusion imaging, plays a pivotal role in diagnosing PVS. However, diagnosis can be complicated by non-specific radiographic findings, such as peripheral consolidations, often misinterpreted as more common conditions like pneumonia or pulmonary embolism.1,3 Ventilation/perfusion (V/Q) scans play a crucial role in detecting PVS-related perfusion defects, aiding in diagnosis and assessing occlusion severity, though they require correlation with other imaging modalities like CT or MRI.1 Transesophageal or transthoracic echocardiography post-ablation does not offer high diagnostic accuracy. Multi-slice CT angiography stands as the gold standard, providing direct visualization of pulmonary vein stenosis and indirect signs of pulmonary venous hypertension-related lung parenchymal changes.1,3,6 Although MRI offers insights into blood flow dynamics and ventricular function, its utility may be limited by long acquisition times and contraindications in patients with metal implants.
Management strategies vary based on patient presentation and include both surgical interventions such as endarterectomy and transcatheter therapies like stent implantation. While asymptomatic cases may warrant surveillance, symptomatic PVS requires early intervention to prevent irreversible complications such as pulmonary hypertension and pulmonary vein occlusion. Post-interventional antithrombotic therapy remains an area of ongoing research,4 typically involving anticoagulation combined with dual antiplatelet therapy, although optimal durations are yet to be determined. Routine surveillance screening post-ablation could facilitate early detection and intervention, potentially mitigating severe complications associated with PVS progression. The study by Raeisi-Giglou et al. published in Circulation: Arrhythmia and Electrophysiology, meticulously followed over 10,000 patients for 16 years, demonstrating the importance of routine contrast-enhanced spiral computed tomographic (CT) scans at 3 to 6 months post-ablation to assess for PVS. This thorough approach allowed for the detection of severe PVS in 0.5% of patients, emphasizing the necessity of post-procedural imaging in identifying and managing potentially life-threatening complications. While routine imaging post-ablation may not be cost-effective, heightened awareness of PVS symptoms is crucial for early diagnosis and management. 4
Pulmonary vein stenting, as demonstrated in the study, appears to offer better long-term outcomes compared to balloon angioplasty, emphasizing the importance of selecting optimal intervention strategies.4,5,7 Although interventional procedures like balloon angioplasty and stent placement offer promising outcomes, they are hindered by high rates of restenosis, emphasizing the need for enhanced surveillance protocols and therapeutic strategies in managing PVS.2,4 The transition from venous ostia to “Wide Area Circumferential Ablation” (WACA) has also contributed to reducing the incidence of PVS. With the advent of pulse electrical field (PEF) ablation, a new energy source that does not result in venous stenosis, there is potential for safer repeated ablations. In animal models, repeated PEF ablations in venous structures did not result in any immediate or late damage.8,9 Nonetheless, further research is needed to enhance outcomes in PVS management, underscoring the necessity for continued investigation and advancement in this field.
Conclusion
This case highlights the importance of considering pulmonary vein stenosis (PVS) in the differential diagnosis of patients presenting with nonspecific cardiorespiratory symptoms following radiofrequency ablation for atrial fibrillation. The delayed diagnosis in our patient underscores the need for routine surveillance screening post-ablation to facilitate early detection and intervention, especially in symptomatic patients. Multimodal imaging, including CT angiography, MRI, and V/Q scans, plays a crucial role in diagnosing and assessing the severity of PVS. Prompt recognition and management can mitigate complications and improve outcomes in affected individuals. Moving forward, clinicians should maintain a high index of suspicion for PVS in post-ablation patients with persistent respiratory symptoms, advocating for regular follow-up imaging to prevent delays in diagnosis and treatment initiation.
Patient Consent
A written informed consent was obtained from the patient for the publication of this case report.
Ethical Clearance
This project did not involve any research and no ethical clearance was required.
Acknowledgments
This project did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Competing interests
None. The authors declare that they have no conflicting interests and have not been supported or funded by any drug company or authority. The authors declare that this is their original work and they all approve the content of this manuscript. They confirm that this manuscript has not been published previously, in any language, in whole or in part, and is not currently under consideration elsewhere.
Conflict of Interest
The authors do not declare any conflict of interest regarding the publication of this manuscript.
References
- Pazos-López P, García-Rodríguez C, Guitián-González A, et al. Pulmonary vein stenosis: Etiology, diagnosis and management. World J Cardiol. 2016;8(1):81-88. doi:10.4330/wjc.v8.i1.81. [CrossRef]
- Shroff N, Choi W, Villanueva-Meyer J, Palacio DM, Bhargava P. Pulmonary vein occlusion: A delayed complication following radiofrequency ablation for atrial fibrillation. Radiol Case Rep. 2021;16(12):3666-3671. doi:10.1016/j.radcr.2021.09.015. [CrossRef]
- Carriço F, Gurioli C, Piciucchi S, Dubini A, Tomassetti S, Poletti V. Pulmonary vein stenosis mimicking interstitial lung disease. Pulmonology. 2021;27(6):584-589. doi:10.1016/j.pulmoe.2020.05.010. [CrossRef]
- Young L, Krishnaswamy A, Kapadia S. Treating Post-Ablation Pulmonary Vein Stenosis. Struct Heart. 2019;3(6):454-461. doi:10.1080/24748706.2019.1673919. [CrossRef]
- Padala SK, Ellenbogen KA. Pulmonary Vein Stenosis After Atrial Fibrillation Ablation. Circ Arrhythm Electrophysiol. 2018;11(5):e006461. doi:10.1161/CIRCEP.118.006461. [CrossRef]
- Vyas-Read S, Varghese NP, Suthar D, et al. Prematurity and Pulmonary Vein Stenosis: The Role of Parenchymal Lung Disease and Pulmonary Vascular Disease. Children. 2022;9(5):713. doi:10.3390/children9050713. [CrossRef]
- Fender EA, Widmer RJ, Hodge DO, et al. Severe Pulmonary Vein Stenosis Resulting From Ablation for Atrial Fibrillation. Circulation. 2016;134(23):1812-1821. doi:10.1161/CIRCULATIONAHA.116.021949. [CrossRef]
- Yang M, Wang P yu, Hao Y lu, et al. A real-world case–control study on the efficacy and safety of pulsed field ablation for atrial fibrillation. Eur J Med Res. 2023;28(1):519. doi:10.1186/s40001-023-01509-5. [CrossRef]
- Reduction in Pulmonary Vein Stenosis and Collateral Damage With Pulsed Field Ablation Compared With Radiofrequency Ablation in a Canine Model | Circulation: Arrhythmia and Electrophysiology. Accessed August 4, 2024. https://www.ahajournals.org/doi/10.1161/CIRCEP.120.008337. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



