Submitted:
03 September 2024
Posted:
04 September 2024
You are already at the latest version
Abstract
Background and aims: In recent years, a possible connection between HLA-Cw6 and a distinctive cardiometabolic (CM) profile in patients with psoriatic disease (PsD) has been proposed, although there is still little support for this. Our aim was to further investigate this possible association by studying a large population of PsD patients. Methods: For this study, three different cohorts of patients with PsD were analyzed: two with a majority of cutaneous psoriasis, pooled n: 600, and a third with only psoriatic arthritis -PsA- cases, n: 340. Potential relationships between HLA-Cw6 and the different CM risk factors (hypertension, diabetes, obesity, dyslipidemia) were analyzed using univariate and multivariate regression models, while the final net effect was assessed using fixed- or random-effects meta-analyses, as appropriate. Results: In the PsA cohort, no association was detected between HLA-Cw6 carriership and any of the CM comorbidity factors. In psoriasis cohorts, after correcting for age, sex, disease duration and arthritis, HLA-Cw6 carriers reduced diabetes risk (OR 0.49, 95%CI: 0.26-0.91, p = 0.026). This latter effect was confirmed by a fixed-effects meta-analysis of the included cohorts (pooled OR: 0.50, 95%CI: 0.27-0.90). Conclusion: This work demonstrates a potential protective effect of the HLA-Cw6 allele on the risk of diabetes in PsD. Our findings together with those of others seem to confirm the existence of a novel HLA-Cw6-linked cardiometabolic endotype in this disease.
Keywords:
psoriasis
; psoriatic arthritis
; psoriatic disease
; HLA-Cw6
; cardiometabolic comorbidity
; diabetes
1. Introduction
Psoriasis and psoriatic arthritis (PsA) are the two main poles on which the modern concept of psoriatic disease (PsD) is based. However, this concept is also supported by the numerous comorbid conditions that accompany both entities, so that today it is understood that there is a common link between psoriasis, PsA, and their comorbidities [1]. Regarding the latter, the strongest pathogenic connections are, above all, with those of a cardiometabolic (CM) nature [2,3,4]. In fact, obesity is considered one of the long-term risk factors for the development of arthritis among patients with skin psoriasis [2,3,4]. Although it is speculated that the deregulation of the IL23-Th17 axis would be the basis for the coexistence of PsD and its CM comorbidity, it is no less true that a shared genetic basis could contribute to the appearance of skin and joint manifestations along with the CM conditions so typical of PsD [5,6]. Therefore, the relationship between PsD and its CM comorbidity appears to be complex and possibly bidirectional, with chronic inflammation and immune dysregulation playing a critical role in the pathogenesis of both processes.
The histocompatibility antigen HLA-Cw6 is the main genetic biomarker of PsD. It not only establishes a clear risk of cutaneous psoriasis, but is also associated with a specific disease endotype (early onset, familial, severe skin disease). However, this allele is underrepresented among arthritis patients, while it is also linked to a longer psoriasis-arthritis latency time [7,8]. On the other hand, in the last few years a potential association between HLA-Cw6 and a better CM risk profile has been established [9,10,11]. However, it is possible that these links are more related to confounders such as age, sex, and above all, the presence of arthritis [12]. On the one hand, as mentioned, there is a negative relationship between HLA-Cw6 and arthritis. Furthermore, most CM comorbidity tends to be associated with increasing age. Finally, many studies associate PsA with a higher prevalence of both these factors and their core syndrome, the so-called metabolic syndrome [3,13,14]. Thus, the relationship between HLA-Cw6 positivity, skin involvement, early age of onset, and better CM profile may actually be a mirror relationship, where the other side of the mirror would be a negative HLA-Cw6 profile, later age of onset, worse CM profile, and arthritis. Thus, the question remains as to whether these potential connections between HLA-Cw6 and a lower risk of CM comorbidity are rather indirect relationships, where other factors such as age or arthritis better explain this entire apparent connection.
In previous studies, we have found an association between HLA-Cw6 carriership and a better CM risk profile, but we have also found that other factors (e.g., age, sex, arthritis) could better explain this connection [10,12]. However, in these and other studies, the majority of the study population has been patients with psoriasis without arthritis, so we do not know whether enriching these analyses by including more patients with PsA could contribute to shedding light on this controversial aspect of the disease. In the present study, which includes a large number of patients, we delve deeper into the possible connections between HLA-Cw6 and CM risk factors, but in a more balanced population in terms of the representativeness of PsA cases.
2. Materials and Methods
2.1. Study Population
For the purposes of this study, we have analyzed two cohorts of patients mostly represented by cutaneous psoriasis cases, and a third cohort, strictly represented by patients with PsA according to CASPAR criteria [15]. All patients included were over 18 years of age and were originally from a region in northwestern Spain (Principality of Asturias, total population of around one million inhabitants). Patients were recruited from the Dermatology and Rheumatology services of two university hospitals in that region. The recruitment period for these cohorts ran from January 2007 to December 2017. The ethical considerations, inclusion/exclusion criteria, main characteristics, and scientific exploits, relevant to these cohorts, have been published elsewhere [10,12,16,17,18,19]. Also, aligned with the study objectives, a first psoriasis cohort consisting of 400 patients [10] was merged with a second cohort consisting of 572 cases [12], but after checking for replicate data, the final psoriasis study cohort consisted of 600 patients, but keeping a third cohort of patients with PsA (n: 340) separate. Approximately 30% of patients included in the psoriasis cohort met CASPAR criteria for PsA, although this subpopulation was not characterized in detail and its presence was simply recorded (dichotomous variable). This study was conducted in full conformance with the Spanish SAS Order/3470/2009 of the Ministry of Health and Social Policy, local laws and regulations, and the ethical principles laid down in the Declaration of Helsinki. Compliance with the provisions of the new Regulation (EU) 2016/679 of the European Parliament and the Council of 27 April 2016 on Data Protection (GRDP) was also ensured.
2.2. Study Variables
Sociodemographic, anthropometric data, laboratory, activity, and outcome variables were included. Details of these variables and their definitions have been published elsewhere [10,12,16,17,18,19]. Briefly, family history of psoriasis and arthritis, age, sex, educational level, anthropometric data, disease duration, psoriasis types, nail involvement, BSA, PASI, arthritis patterns, associated manifestations (dactylitis, enthesitis, uveitis, IBD), composite arthritis activity indices, physical function, and data on structural damage were collected. Cardiometabolic comorbidities collected were obesity, hypertension, diabetes, and dyslipidemia. Accepted definitions for these comorbidities have been previously published [16,17,18,19].
2.3. HLA-Cw6 Typing
All patients were genotyped for the HLA-Cw6*0602 allele (SNP rs1050414 C/G).
2.4. Statistical Analysis
For the univariate descriptive analysis, the mean, standard deviation, median, minimum and maximum value of the quantitative variables, and the absolute and relative frequencies (percentages) of the categorical variables are included. For comparisons between groups and variables, parametric and non-parametric tests were chosen depending on whether their distribution was normal or not. In the PsA cohort, the frequency of CM factors was compared to that of 600 non-inflammatory outpatients matched by age (± 3 years) and sex (1:1) with the study population. To estimate the crude effect of the genetic marker (HLA-Cw6) on the different outcomes, simple linear regression models were constructed when the dependent variable was a quantitative one, and simple logistic regression models when the dependent variable was categorical. To estimate the adjusted effect, multiple regression models were created (linear or logistic, as appropriate) where covariates such as age, sex, time of evolution, and the presence of arthritis were introduced. Finally, to assess the net effect of the relationship between HLA-Cw6 and the different CM factors, meta-analyses were carried out, presenting the pooled Odds Ratios (OR) for fixed- and random-effect models. In the fixed effects model, it is assumed that the study populations were the same. It can be used when there is no heterogeneity between studies (p for heterogeneity > 0.05). The threshold for statistical significance was set at p < 0.05. Data were analyzed using R software (4.3.1 “Beagle Scouts”).
3. Results
3.1. Summary of the Study Population
The total population included 940 patients, 600 from the two merged psoriasis cohorts and 340 from the arthritis cohort. Psoriasis study cohort included 312 (52%) men and 288 (48%) women, mean age 46.7 ± 14.5 years, average disease duration of 20 ± 14.8 years. Psoriatic arthritis cohort included 190 (55.9%) men and 150 (44.1%) women, mean age 55 ± 13 years, average joint disease duration of 11 ± 6.3 years. The rest of the characteristics of the pooled psoriasis cohorts and the PsA cohort are summarized in Table 1.
3.2. Cardiometabolic Comorbidity in the PsA Cohort
The frequency of traditional CM factors was as follows: diabetes 13.8%, hypertension 36%, dyslipidemia 31%, obesity 35%, and overweight 24.1%. Compared to control non-PsA population, PsA patients showed higher frequency of CM comorbidity: hypertension (36 vs. 23%, OR 2.4, 95% CI: 1.6–2.7, p < 0.0001), diabetes (13.8 vs. 5%, OR 2.8, 95% CI: 1.7–4.3, p < 0.0001), obesity (35 vs. 22%, OR 2.1, 95% CI: 1.5–2.8, p < 0.0001) and tobacco use (26 vs. 21%, OR 1.4, 95% CI: 1.0–1.8, p <0.05). More females (18%) than males were diabetics (10.5%), p < 0.05. Also, more females (44%) than males (28.9%) were obese, p = 0.01.
3.3. Cardiometabolic Comorbidity in Psoriasis Cohorts
Regarding the anthropometric variables, the average weight was 77.8 kg (SD 16.5) with an average BMI of 27.7 (SD 5.04), with the average waist circumference being 97 cm (min: 60, max: 138). Just over a third (34%) of the patients were smokers, while the median alcohol consumption according to standard drink units (SDU) was 0 (min: 0, max: 30). Of the study patients, fatty liver disease was confirmed in 132 (22%). A total of 20% of the patients had hypertension and another 20% had dyslipidemia. In total, 33 patients showed adverse coronary events (5.5%), 22 patients were type I diabetics (3.6%), while 47 (7.8%) were type 2. More men (32%) than women (11.4%), had fatty liver disease (p < 0.01), while there were no significant differences in the distribution of the other CM factors.
3.4. Relationship between HLA-Cw6 and Cardiometabolic Comorbidity
The determinants of diabetes, obesity, hypertension, and dyslipidemia in the PsA cohort have been published elsewhere [16,17,18,19]. However, all of these factors also appeared to be linked to increasing age: hypertension OR 1.19 (95%CI: 1.09-1.30, p < 0.001), diabetes OR 1.12 (95%CI: 1.04-1.23, p = 0.006), dyslipidemia OR 1.08 (95%CI: 1.03-1.14, p = 0.002), and obesity OR 1.07 (95%CI: 1.01-1.15, p = 0.02). On the other hand, no association was detected between the HLA-Cw6 allele and any CM factor. Increasing age was also a driving force to explain CM comorbidity in psoriasis cohorts, but not the only one. Thus, for each decade of age the risk of hypertension increased by 11% (p < 0.001), but also arthritis increased this risk by 59% (p < 0.05). HLA-Cw6 subjects reduced the risk of hypertension by 48% (95%CI: 20–66). However, the model adjusted for age, sex, disease duration, and arthritis demonstrated a 21% reduction, without being statistically significant (95%CI: 0.47–1.30, p = 0.40). Diabetes risk increased by 8% per decade (p < 0.001). However, in adjusted regression models HLA-Cw6 carriers reduced diabetes risk (OR 0.49, 95%CI: 0.26-0.91, p = 0.026). For each decade of age, the risk of dyslipidemia increased by 6% (p < 0.001), while arthritis increased this risk by 82% (p = 0.010). The risk of fatty liver disease increased by 2% for each decade of age (p = 0.02) and was reduced by 74% in women compared to men (p < 0.001). Adverse coronary events increased by 11% per decade (p < 0.001).
3.5. Meta-Analysis of the Relationships between HLA-Cw6 and Cardiometabolic Comorbidity
No heterogeneity was detected between the cohorts (p for heterogeneity > 0.05), so a fixed-effects meta-analysis model was applied. In the case of hypertension, some heterogeneity was detected between cohorts (I2 64%), but the precept to use a fixed-effects meta-analysis was fulfilled (p for heterogeneity = 0.09). According to this, no relationship was found between HLA-Cw6 and the risk of hypertension (pooled OR 0.91, 95%CI: 0.57-1.47). A significant inverse association was found between HLA-Cw6 and diabetes with a pooled OR 0.50, 95%CI: 0.27-0.90 (Figure 1). A 16% reduction in obesity risk was found among HLA-Cw6 carriers, but this was not significant (95%CI: 0.57-1.22). No relationship was found between HLA-Cw6 and dyslipidemia (pooled OR 0.99, 95%CI: 0.65-1.52).
4. Discussion
In this study, which included a large number of patients with PsD, we detected an inverse association between HLA-Cw6 and diabetes (OR 0.50). Although this association was primarily detected in cohorts of patients with predominantly skin psoriasis, a fixed-effect meta-analysis including all cohorts confirmed the lower risk of diabetes associated with HLA-Cw6 carriage.
Some studies conducted in the last few years have detected an inverse association between the HLA-Cw6 allele and certain cardiovascular risk factors. Thus, at least two independent studies have linked the presence of this marker with a lower risk of hypertension [9,10]. This allele has also been linked to lower central adiposity and a lower risk of liver fibrosis, thus driving a potential protection conferred by HLA-Cw6 against a higher risk of cardiovascular comorbidity [9,10,11,20]. However, none of these studies has been able to definitively resolve the possibility of a false causal relationship between this marker and this type of comorbidity. Among other factors, the populations analyzed have been very different and mostly made up of patients with psoriasis without arthritis, the prevalence of HLA-Cw6 has also been quite heterogeneous, and the prevalence of the disease itself and its comorbidities has been uneven between studies, so comparisons between these studies are quite complex. We have even found a certain disparity in our own previous results, such that the associations in this regard found in a first study were not confirmed in a second larger study [10,12]. Therefore, the central idea of the present work was to seek a certain breaker in relation to our previous findings. To this end, we meta-analyzed three cohorts of patients (two merged into one, with a majority representation of psoriasis without arthritis, and a third, composed exclusively of patients with PsA). After correcting for age, sex, disease duration and arthritis, we confirmed a "protective" effect against diabetes conferred by HLA-Cw6.
Both PsD and diabetes are polygenic diseases resulting from a complex interplay between genetic, epigenetic, and environmental factors. In the case of diabetes, most experts agree that the HLA system is the principal region of risk for developing type 1 diabetes, and less important for type 2 [21,22]. Experimental research shows evidence of biochemical consequences of the nonenzymatic reaction of oxidative alterations in key components of the Major Histocompatibility Complex (MHC) in vivo under conditions of hyperglycemia-induced metabolic stress. These modifications were linked to epitope-specific changes in endosomal processing efficiency, MHC-II peptide binding, and editing activity [23]. These findings highlight a potential link between glycation reactions and altered MHC antigen presentation that may contribute to type 2 diabetes complications. Under these premises, it would be tempting to speculate on a possible pathogenic link between HLA-Cw6 and the risk of diabetes in the PsD population. Indeed, a recent study by Mendoza-Ramírez et al found links between certain HLA-C alleles (C*01:02:01:01) and the risk of type 2 diabetes, but HLA-C*06 (HLA-Cw6) was not among the risk alleles [24]. Therefore, the biological plausibility of our finding remains uncertain.
On the other side, there are some epidemiological clues that might support this connection. Eirís et al. demonstrated that genetic variations in the IL12/23 pathway were important not only to define both the risk and severity of PsD but also to define the risk of certain comorbidities such as type 2 diabetes. Thus, this group found significant associations between three SNP genotypes and type 2 diabetes: IL12B rs6887695-CC (OR=2.90), IL12B rs3212227-CC (OR=5.90) and IL23R rs2201841-GG (OR=2.69), demonstrating this way that the genetic risk of PsD-related diabetes might be governed by genes outside the HLA system [25]. Inerot et al. found endocrine disorders in 9% of their HLA-Cw6-negative psoriasis patients compared to only 1% among HLA-Cw6 carriers. In addition, no HLA-Cw6 positive patient was diabetic compared to a 5% overall prevalence of diabetes in the Swedish general population [26]. The latter seems to reinforce our finding on the protective potential of HLA-Cw6 on the risk of PsD-related diabetes. In Douroudis et al study, the five CM comorbidities studied (ischaemic heart disease; hypertension; dyslipidemia; type 2 diabetes; and a cardiovascular disease umbrella, including ischemic, cerebrovascular, and peripheral vascular disease) all exhibited lower prevalence in HLA-Cw6–positive patients with psoriasis than in HLA-Cw6–negative patients. However, only hypertension remained statistically significant after accounting for multiple testing (OR 0.73 in HLA-Cw6 carriers) [9]. These latest findings, together with our own, do seem to point to a relationship between HLA-Cw6 carriership and a better cardiovascular risk profile. The practical implications of this are unquestionable, since the presence of this specific type of comorbidity is increasingly helping clinicians to better plan therapy for patients with PsD [27,28].
A final consideration regarding the protective role of HLA-Cw6 against CM comorbidity is whether this could translate into a lower rate of future adverse cardiovascular events among HLA-Cw6 carriers. As this is an open question, it is worth highlighting that in a study by Eder et al, interestingly, HLA-B*13:02 and HLA-C*06:02 (HLA-Cw6) were associated with more severe atherosclerosis (age- and sex-adjusted OR 2.31 and OR 1.68, respectively) and these associations remained statistically significant after adjusting for cardiovascular risk factors [29].
In short, the HLA-Cw6-linked endotype has been gradually expanding, moving from a classic clinical endotype (type I disease) linked to a higher family burden, early-onset, and greater clinical severity, to a pharmacogenomic endotype linked to a better response to certain therapies (methotrexate and ustekinumab), to finally arrive at a novel cardiometabolic endotype that, if confirmed in other latitudes, would have clear implications for the overall management and prognosis of the disease [30]. Therefore, it may be time to incorporate HLA-Cw6 determination into clinical routine in order to improve the standard of care in this field.
This study obviously has several limitations. First, since the different outcomes analyzed and their results are subject to multiple influences, it may be the case that multivariate models cannot fully account for the influence of all possible mediating variables in all cases. Furthermore, the cross-sectional nature of the observations limits our ability to draw causal inferences. Moreover, the use of a meta-analysis to obtain a net effect of the investigated associations is not without criticism in this particular context, including the potential bias inherent in the analysis of cohorts from the same working group thus limiting its quality. Therefore, ideally, the associations found in our work should be confirmed in future adequately powered life-course studies. As advantages, we have included a significant number of cases with an adequate representation of one of the usual confounding factors in this type of association studies, such as arthritis.
Finally, it must be remembered that the relationship between PsD, its comorbidities, and their genetic drivers, cannot be seen as a unidirectional relationship but rather as the result of multiple interactions [31]. A good example of this can be found in the relationship between tobacco and psoriasis. Smoking damages the skin by increasing formation of reactive oxygen species and decreasing the gene expression of antioxidants. Nicotine also stimulates innate immune cells integral to the pathogenesis of psoriasis including dendritic cells, macrophages and keratinocytes. These cells release cytokines that activate T lymphocytes and perpetuate a cycle of chronic inflammation. Along with this, smoking also enhances expression of genes known to confer an increased risk of psoriasis, including HLA-Cw6 [32].
5. Conclusions
In summary, our work demonstrates a potential protective effect of the HLA-Cw6 allele on the risk of diabetes that was independent of the presence of arthritis and other confounders. Since the distribution of HLA-Cw6 is not homogeneous worldwide, additional well-designed studies from other latitudes are needed to support the existence of this novel HLA-Cw6-linked cardiometabolic endotype. It remains to be seen whether the benefits of this positive cardiometabolic endotype would be associated in the future with better cardiovascular outcomes in this entity.
Author Contributions
Conceptualization, R.Q., P.G.P. and P.A.; Data curation, E.P., S.B. and N.C.; Formal analysis, R.Q., I.B., E.P., M.L., S.B., P.G.P., P.A., M.A., S.A.; Investigation, I.B., E.P., M.L., P.G.P., P.A., N.C., S.A., M.A.; Methodology, R.Q., P.G.P., P.A., N.C.; Resources, R.Q., M.A., S.A.; Supervision, R.Q., M.A.; Validation, R.Q., P.G.P., P.A., N.C., E.P., S.B., I.B., M.L., S.A., M.A.; Visualization, R.Q., S.A., M.L., M.A.; Writing—original draft, R.Q.; Writing—review and editing, R.Q., P.G.P., P.A., N.C.. All authors have read and agreed to the published version of the manuscript.
Funding
Part of this work was supported by a grant from the Spanish Instituto de Salud Carlos III-European FEDER funds (no. PI16/01792 and grant RICOR2040-RD21/0005/0011). The psoriasis patient cohort was registered as a Biobank collection by the Spanish Instituto de Salud Carlos III (reference C.0003441).
Institutional Review Board Statement
This study was conducted in full conformance with the Spanish SAS Order/3470/2009 of the Ministry of Health and Social Policy, local laws and regulations, and the ethical principles laid down in the Declaration of Helsinki. Compliance with the provisions of the new Regulation (EU) 2016/679 of the European Parliament and the Council of 27 April 2016 on Data Protection (GRDP) was also ensured. The corresponding ethical approvals are reflected in the methods section and included in the references [10,12,16,17,18,19].
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The materials and raw data described in the manuscript will be freely available to any researcher without breaching any participant’s confidentiality. To facilitate the revision of the results by other researchers, a file with the patient data is available as an excel file upon request to the corresponding author.
Acknowledgments
We would like to thank Eva Fernández-Bretón (Statistics Unit of the Instituto de Investigación Sanitaria del Principado de Asturias, Oviedo-Spain) for her support in the statistical analysis of this study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Scarpa, R.; Caso, F.; Costa, L.; Peluso, R.; Spanò, A.; Lubrano, E.; Del Puente, A.; Moll, J.M. Psoriatic Disease: Clinical Staging. J. Rheumatol. Suppl. 2015; 93: 24–26. [CrossRef]
- Perez-Chada, L.M.; Merola, J.F. Comorbidities associated with psoriatic arthritis: Review and update. Clin. Immunol. 2020; 214: 108397. [CrossRef]
- Caso, F.; Chimenti, M.S.; Navarini, L.; Ruscitti, P.; Peluso, R.; Girolimetto, N.; Del Puente, A.; Giacomelli, R.; Scarpa, R.; Costa, L. Metabolic Syndrome and psoriatic arthritis: Considerations for the clinician. Expert. Rev. Clin. Immunol. 2020; 16: 409–420. [CrossRef]
- Puig, L. Cardiometabolic Comorbidities in Psoriasis and Psoriatic Arthritis. Int. J. Mol. Sci. 2017; 19: 58. [CrossRef]
- Piaserico, S.; Orlando, G.; Messina, F. Psoriasis and Cardiometabolic Diseases: Shared Genetic and Molecular Pathways. Int. J. Mol. Sci. 2022; 23: 9063. [CrossRef]
- Patrick, M.T.; Li, Q.; Wasikowski, R.; Mehta, N.; Gudjonsson, J.E.; Elder, J.T.; Zhou, X.; Tsoi, L.C. Shared genetic risk factors and causal association between psoriasis and coronary artery disease. Nat. Commun. 2022; 13: 6565. [CrossRef]
- Chen, L.; Tsai, T.F. HLA-Cw6 and psoriasis. Br. J. Dermatol. 2018; 178: 854–862. [CrossRef]
- Owczarek, W. The role of HLA-Cw6 in psoriasis and psoriatic arthritis. Reumatologia. 2022; 60(5): 303-305. [CrossRef]
- Douroudis, K.; Ramessur, R.; Barbosa, I.A.; Baudry, D.; Duckworth, M.; Angit, C.; Capon, F.; Chung, R.; Curtis, C.J.; Di Meglio, P.; et al. Differences in Clinical Features and Comorbid Burden between HLA-C∗06:02 Carrier Groups in >9000 People with Psoriasis. J. Investig. Dermatol. 2022; 142: 1617–1628. [CrossRef]
- Queiro, R.; Coto-Segura, P.; Braña, I.; Pino, M.; Burger, S. Potential Differences in the Cardiometabolic Risk Profile of Patients with Psoriatic Disease according to Their HLA-C∗06 Status. Biomed. Res. Int. 2022; 2022: 1451193. [CrossRef]
- Solvin, Å.Ø.; Bjarkø, V.V.; Thomas, L.F.; Berrospi, P.; Hveem, K.; Saunes, M.; Åsvold, B.O.; Løset, M. Body Composition, Cardiometabolic Risk Factors and Comorbidities in Psoriasis and the Effect of HLA-C*06:02 Status: The HUNT Study, Norway. Acta. Derm. Venereol. 2023; 103: adv5209. [CrossRef]
- Queiro, R.; Braña, I.; Pardo, E.; Loredo, M.; Burger, S.; González del Pozo, P.; Alvarez, P.; Fernández-Bretón, E.; Coto, P.; Coto, E. Influence of the HLA-Cw6 Allele and IFIH1/MDA5 Gene Variants on the Cardiometabolic Risk Profile of Patients with Psoriatic Disease. J. Clin. Med. 2024, 13, 845. [CrossRef]
- Karmacharya, P.; Ogdie, A.; Eder, L. Psoriatic arthritis and the association with cardiometabolic disease: a narrative review. Ther. Adv. Musculoskelet. Dis. 2021; 13: 1759720X21998279. [CrossRef]
- Verhoeven, F.; Prati, C.; Demougeot, C.; Wendling, D. Cardiovascular risk in psoriatic arthritis, a narrative review. Joint. Bone. Spine. 2020; 87(5): 413-418. [CrossRef]
- Taylor, W.; Gladman, D.; Helliwell, P.; Marchesoni, A.; Mease, P.; Mielants, H.; CASPAR Study Group. Classification criteria for psoriatic arthritis: development of new criteria from a large international study. Arthritis. Rheum. 2006; 54(8): 2665-2673. [CrossRef]
- Queiro, R.; Lorenzo, A.; Tejón, P.; Pardo, E.; Coto, P. Hypertension is associated with increased age at the onset of psoriasis and a higher body mass index in psoriatic disease. Clin. Rheumatol. 2019; 38: 2063–2068. [CrossRef]
- Queiro, R.; Fernández, S.; Pardo, E. Hyperlipidemia in psoriatic disease: Higher prevalence in psoriatic arthritis and inverse association with systemic therapy. Rheumatology. 2021; 60: 3949–3951. [CrossRef]
- Queiro, R.; Lorenzo, A.; Pardo, E.; Brandy, A.; Coto, P.; Ballina, J. Prevalence and type II diabetes-associated factors in psoriatic arthritis. Clin. Rheumatol. 2018; 37(4): 1059-1064. [CrossRef]
- Queiro, R.; Lorenzo, A.; Tejón, P.; Coto, P.; Pardo, E. Obesity in psoriatic arthritis: Comparative prevalence and associated factors. Medicine (Baltimore). 2019; 98(28): e16400. [CrossRef]
- Macía-Villa, C.; Morell-Hita, J.L.; Revenga-Martínez, M.; Díaz-Miguel Pérez, C. HLA-Cw6 allele and biologic therapy are protective factors against liver fibrosis in psoriatic arthritis patients. Clin. Exp. Rheumatol. 2023; 41: 1179–1182. [CrossRef]
- Ali, O. Genetics of type 2 diabetes. World. J. Diabetes. 2013; 4: 114–123. [CrossRef]
- Prasad, R.B.; Groop, L. Genetics of type 2 diabetes-pitfalls and possibilities. Genes. 2015; 6: 87–123. [CrossRef]
- Clement, C.C.; Nanaware, P.P.; Yamazaki, T.; Negroni, M.P.; Ramesh, K.; Morozova, K.; Thangaswamy, S.; Graves, A.; Kim, H.J.; Li, T.W.; et al. Pleiotropic consequences of metabolic stress for the major histocompatibility complex class II molecule antigen processing and presentation machinery. Immunity. 2021; 54: 721–736. [CrossRef]
- Mendoza-Ramírez, P.; López-Olaiz, M.A.; Morales-Fernández, A.L.; Flores-Echiveste, M.I.; de Jesus Casillas-Navarro, A.; Pérez-Rodríguez, M.A.; de Jesús Orozco-Luna, F.; Cortés-Romero, C.; Zuñiga, L.Y.; Sanchez Parada, M.G.; et al. Class I MHC Polymorphisms Associated with Type 2 Diabetes in the Mexican Population. Genes (Basel). 2022; 13(5): 772. [CrossRef]
- Eirís, N.; González-Lara, L.; Santos-Juanes, J.; Queiro, R.; Coto, E.; Coto-Segura, P. Genetic variation at IL12B, IL23R and IL23A is associated with psoriasis severity, psoriatic arthritis and type 2 diabetes mellitus. J. Dermatol. Sci. 2014; 75(3): 167-72. [CrossRef]
- Inerot, A.; Enerbäck, C.; Enlund, F.; Martinsson, T.; Samuelsson, L.; Wahlström, J.; Swanbeck, G. Collecting a set of psoriasis family material through a patient organisation; clinical characterisation and presence of additional disorders. BMC. Dermatol. 2005; 5: 10. [CrossRef]
- Wu, J.J.; Kavanaugh, A.; Lebwohl, M.G.; Gniadecki, R.; Merola, J.F. Psoriasis and metabolic syndrome: implications for the management and treatment of psoriasis. J. Eur. Acad. Dermatol. Venereol. 2022; 36(6): 797-806. [CrossRef]
- Toussirot, E.; Gallais-Sérézal, I.; Aubin, F. The cardiometabolic conditions of psoriatic disease. Front. Immunol. 2022; 13: 970371. [CrossRef]
- Eder, L.; Abji, F.; Rosen, C.F.; Chandran, V.; Cook, R.J.; Gladman, D.D. The Association of HLA-class I Genes and the Extent of Atherosclerotic Plaques in Patients with Psoriatic Disease. J. Rheumatol. 2016; 43:(10)1844-1851; [CrossRef]
- Queiro, R.; Braña, I.; Loredo, M.; Burger, S. HLA-C*06-defined endotype in psoriatic disease: an ever-widening landscape. Rheumatology (Oxford). 2024; 63(3): 581-583. [CrossRef]
- Yang, L.; Zhang, L.; Du, Q.; Gong, X.; Tian, J. Exploring the molecular mechanism underlying the psoriasis and T2D by using microarray data analysis. Sci Rep. 2023; 13(1): 19313. [CrossRef]
- Armstrong, A.W.; Armstrong, E.J.; Fuller, E.N.; Sockolov, M.E.; Voyles, S.V. Smoking and pathogenesis of psoriasis: a review of oxidative, inflammatory and genetic mechanisms. Br J Dermatol. 2011; 165(6): 1162-8. [CrossRef]
Figure 1.
Forest plot of the relationship between HLA-Cw6 and diabetes risk. Pooled ORs are presented for both the fixed-effects and the random-effects model. Psor2: psoriatic arthritis cohort. Psor3: pooled psoriasis cohorts. See text for details.
Figure 1.
Forest plot of the relationship between HLA-Cw6 and diabetes risk. Pooled ORs are presented for both the fixed-effects and the random-effects model. Psor2: psoriatic arthritis cohort. Psor3: pooled psoriasis cohorts. See text for details.
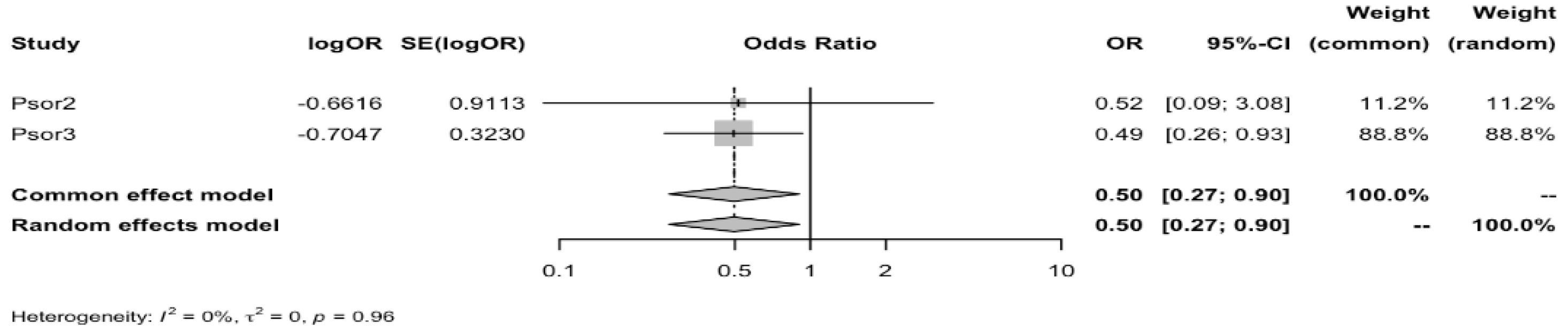

Table 1.
Disease characteristics of study cohorts.
| Variables | PsA. N: 340 | Psoriasis. N: 600* |
| Age (yr ± SD) | 55 ± 13 | 46.7 ± 14.5 |
| Age at onset (yr ± SD) Skin disease Joint disease |
33 ± 17 45 ± 14 |
23 ± 12.4 |
| Disease duration: Skin disease (yr ± SD) Joint disease (yr ± SD) |
21 ± 11 11 ± 6.3 |
20 ± 14.8 |
| Men (n, %) Women (n, %) |
190 (55.9) 150 (44.1) |
312 (52) 288 (48) |
| Education level: Primary (n, %) Secondary (n, %) Academic (n, %) |
180 (52.9) 85 (25) 75 (22.1) |
168 (28) 276 (46) 156 (26) |
| Psoriasis features: Plaque psoriasis (n, %) Onychopathy (n, %) Psoriasis in ≥ 3 body areas (n, %) |
295 (86.7) 142 (41.8) 150 (44.1) |
522 (87) 342 (57) PASI ≥ 10: 306 (51) |
| Family history: Psoriasis (n, %) PsA (n, %) |
156 (46) 51 (15) |
242 (40.3) 50 (8.3) |
| Joint pattern: Mono/oligoarthritis (n, %) Polyarthritis (n, %) Axial disease (n, %) Mixed (n, %) |
141 (41.5) 95 (28) 20 (5.9) 80 (23.5) |
|
| PsA features: Dactylitis (n, %) DIP joint disease (n, %) Mutilating arthritis (n, %) Erosive disease (n, %) |
93 (27.4) 74 (21.8) 5 (1.5) 68 (20) |
|
| HLA-Cw6 (n, %) | 129 (38) | 255 (42.5) |
| Treatment: Conventional systemics (n, %) Biologics (n, %) |
221 (65) 146 (43) |
370 (61.7) 240 (40) |
PsA: psoriatic arthritis, Yr: years, SD: standard deviation, N/n: numbers, PASI: psoriasis area and severity index, DIP: distal interphalangeal, HLA: human leukocyte antigen. * Among first 572 cases analyzed, 172 (30%) fulfilled CASPAR criteria for PsA. Upon multiple logistic regression analyses for the presence of PsA, significant associations were found with psoriasis severity (OR: 2.14, 95%CI: 1.46–3.16), female sex (OR: 1.63, 95%CI: 1.12–2.38), and the IFIH1/MDA5 rs1990760 TT genotype (OR: 1.62, 95%CI: 1.11–2.37), while HLA-Cw6 carriership was protective (OR: 0.65, 95%CI: 0.44–0.95) [12].
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



