Submitted:
01 August 2024
Posted:
02 August 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Breakthrough COVID-19 (occurring in fully vaccinated people) has been described. Data on its characteristics among immune mediated rheumatic disesases (IMRD) patients are scarce. This study describes breakthrough COVID-19 among IMRD patients participating of SAFER-study, a Brazilian multicentric cohort evaluating safety, effectiveness and immunogenicity of SARS-Cov-2 vaccines in autoimmune diseases. Descriptive analysis and a binary logistic regression model, to evaluate predictors of COVID-19-related hospitalization, were performed. P-value < 0.05 was significant. The included 160 patients were predominantly females (83.1%), with mean (SD) age 40.23 (13.19) years. Patients received 2 (19%), 3 (70%) or 4 (11%) vaccine doses. The initial two-dose series was mainly with ChAdOx1 (Oxford/AstraZeneca) (58%) or BBIBP-CorV (Sinopharm-Beijing) (34%). The first booster (n=150) was with BNT162b2 (BioNtech/Fosun Pharma/Pfizer) (63%) or ChAdOx1 (29%). The second booster (n=112) was with BNT162b2 (40%) or ChAdOx1 (26%). COVID-19 hospitalization rate was 17.5%. IMRD moderate/high activity (OR: 5.84, CI: 1.9-18.5, p=0.002) and treatment with corticosteroids (OR: 2.94, CI: 1.02-8.49, p=0.0043) associated with higher odds of hospitalization, while the increasing number of vaccine doses was protective (OR: 0.37, CI: 0.15-0.9, p=0.032). These findings, along with previous reassuring results about the safety of the COVID-19 vaccines, argue in favour of booster vaccination in IMRD patients.
Keywords:
COVID-19
; COVID-19 vaccines
; health disparities
; breakthrough COVID-19 infections
; rheumatic diseases
; vaccination of immune compromised patients
; COVID-19 vaccine booster shot
Introduction
The coronavirus disease 2019 (COVID-19) pandemic has been a serious cause for concern among patients with immune mediated inflammatory and rheumatic diseases (IMID and IMRD). These patients are a unique vulnerable subgroup, as they typically require long-term treatment with multiple immunosuppressive and immunomodulatory (IS/IM) therapy, which is associated with impaired host response to infections and vaccination and may also have multiple sequelae of their disease (e.g., impaired strength, lung fibrosis, chronic kidney disease) and frequent comorbidities (e.g., cardiovascular disease, obesity, and diabetes). Thus, this patient subgroup may be at greater risk of getting SARS-Cov-2 infection and severe COVID-19 complications than healthy controls [1].
Data from the registries from Argentine, Mexico and Brazil, including more than 4000 adult IMID patients with COVID-19, reported a hospitalization rate of 22.7% and a mortality rate of 5.3%. Although these registries did not include a control group, the general population mortality from COVID-19 in these countries was nearly 50% lower than that found in this study [2].
In patients with IMID, SARS-CoV-2 vaccines is well tolerated and not associated with a significant increase of disease activity, thus, current evidence suggests that the benefits of vaccination outweigh the potential risks of adverse effects [3].
A major concern is the possibility of attenuated immunogenicity and, consequently, reduced efficacy of vaccines induced by the concomitant use of IS/IM therapies in these patients, which could leave them vulnerable to breakthrough COVID-19 infections [4,5,6]. A systematic review highlighted the risk of low immunogenicity of COVID-19 vaccines in immunocompromised populations. It included 31 studies reporting immunogenicity in 4680 patients with IMID. Non-response rates (antibody and/or cellular responses) ranged from 0% to 63%. Specific treatments of the inflammatory disease negatively impacted post-vaccine response included B-cell depleting agents, methotrexate, and other disease-modifying anti-rheumatic drugs (DMARDs) or corticosteroids [7].
Some evidence indeed supports the recommendation to administer a third dose of COVID-19 vaccine in patients with IMID, since, in this group, double and triple-vaccinated patients showed a lower rate of COVID-19-related hospitalization and triple-vaccinated patients presented a reduction of COVID-19-related deaths [3].
Data on the presentation and the severity of breakthrough infections in patients with IMRD vaccinated against COVID-19 in Brazil are lacking.
This study presents an analysis of the SARS-CoV-2 breakthrough infections among fully vaccinated individuals with immune-mediated rheumatic diseases from the “Study of safety, effectiveness and immunogenicity duration after vaccination against the new SARS-Cov-2 in patients with immune mediated inflammatory diseases (SAFER-Study)”, of the Brazilian Society of Rheumatology. It intends to describe the profile and the severity of SARS-Cov-2 infection in fully vaccinated IMRD patients presenting breakthrough COVID-19, and the predictors of hospitalization among these patients.
Materials and Methods
SAFER-Study
The “Study of safety, effectiveness and immunogenicity duration after vaccination against the new SARS-Cov-2 in patients with immune mediated inflammatory diseases (SAFER-Study)” is a Brazilian national, multicenter, observational, longitudinal real-world cohort of consecutive patients with IMRD or IMID who have been vaccinated for SARS-CoV-2 evaluating the safety, effectiveness and immunogenicity of SARS-CoV-2 vaccines in this population. The inclusion period was held from June/2021 to March/2024. Follow-up is still ongoing. The present study presents data on the occurrence of breakthrough COVID-19 among patients participating of the SAFER-Study. Data from June/2021 to February/2023 were included.
SAFER-Study has included pediatric or adult patients, with a prior diagnosis of IMID or IMRD. IMRD diagnosis, according to the American College of Rheumatology (ACR) or European League against Rheumatism (EULAR) classification criteria, were rheumatoid arthritis, juvenile idiopathic arthritis, spondylarthritis and other inflammatory joint diseases, and systemic lupus erythematosus, Sjögren’s disease, inflammatory myopathies, systemic vasculitis, systemic sclerosis, mixed connective tissue, disease and other connective tissue diseases or other rheumatic diseases. IMID patients participating in SAFER-Study were those diagnosed with inflammatory bowel disease (IBD) or psoriasis. All patients gave written informed consent. SAFER-Study is a non-probability sampling study with enrollment of consecutive patients who met the selection criteria.
All patients included in this study received one to four doses of a SARS-CoV-2 vaccine. The vaccines available in Brazil during the data assessment for breakthrough COVID-19 infection were the CoronaVac vaccine (Sinovac Biotech), the AstraZeneca vaccine (ChAdOx1), and the vaccines developed by Pfizer (BNT162b2) and Janssen (Ad26.COV2.S). SAFER-study patients will be followed-up from the inclusion until December of 2024.
Baseline evaluation took place before the first dose of SARS-CoV-2 vaccine application. Follow-up visits occurred 4-weeks after each vaccine dose and, later, every 3 months until 12 months of complete follow-up.
Sociodemographic data, the presence of comorbidities, characteristics and severity of IMRD or IMID, treatments received, and clinical characteristics and outcomes of SARS-CoV-2 infection were recorded (previous or acquired during the study).
In addition, the date and place of vaccination, type of vaccine applied, scheme, and indication were registered. Blood samples were collected for immunogenicity analysis. Adverse events, disease flares, and new immune-mediated manifestations related to the vaccines were registered.
Breakthrough COVID-19
Breakthrough infection among fully vaccinated individuals was defined according to the US Centers for Disease Control and Prevention (CDC) as infection occurring ≥14 days after the second dose in a two-dose series or ≥14 days after a single-dose vaccine [8].
COVID-19 diagnosis
COVID-19 was confirmed by a positive reverse transcriptase-polymerase chain reaction (RT-PCR) or antigen (Ag) test for SARS-CoV-2 virus from nasopharyngeal or oropharyngeal swab.
Outcomes
The primary outcomes of this study were the clinical presentation of breakthrough COVID-19. The secondary outcomes were COVID-19-related severe outcomes (need of supplemental oxygen or ventilatory assistance, hospitalization, infectious complications, and death).
Inclusion and exclusion criteria
Adult patients, fully vaccinated against SARS-Cov-2, with the diagnosis of an IMRD, developing COVID-19 confirmed by RT-PCR or Antigen-COVID-19 test were included. Patients reporting COVID-19 before the inclusion in SAFER-Study or when partially vaccinated (after the first dose or 14 days after the second dose in a two-dose series, or of a single-dose vaccine), those with the diagnosis of IBD or psoriasis (IMID), and patients not presenting COVID-18 were excluded. Patients presenting chronic infections (e.g. HIV infection, chronic viral B or C-hepatitis) or neoplasms as comorbidities were also excluded.
Study variables
Demographic variables including age, sex and self-declared color were registered.
The presence and the number of comorbidities (cardiomyopathy, diabetes mellitus, pulmonary disease, chronic kidney disease, systemic arterial hypertension, obesity) was recorded. IMRD diagnosis, treatment and activity at the time of SARS-CoV-2 vaccination and infection were recorded.
Immune-mediated inflammatory diseases differ regarding the DMARDs approved for their treatment. To minimize the impact of this heterogeneity on the associations of interest, diagnostic categories were defined according to what was done by COVID-19 Global Rheumatology Alliance (C19-GRA): inflammatory joint diseases (IJDs), connective tissue diseases (CTDs)/vasculitis, and other rheumatic diseases. In addition, treatments were categorized as follows: glucocorticoids, conventional DMARDs (cDMARDs; antimalarials, leflunomide, methotrexate, sulfasalazine), immunosuppressants (IS): (azathioprine, cyclophosphamide, cyclosporine, mycophenolate mofetil/mycophenolic acid, tacrolimus), tumor necrosis factor (TNF) inhibitors, rituximab, biologic DMARDs (bDMARDs; abatacept, belimumab, interleukin 1 [IL-1], IL-6, IL-12/23, IL-17, and IL-23 inhibitors), targeted synthetic DMARDs (tsDMARDs; Janus kinase inhibitors [JAKi)] [9].
IMRD activity was stratified into categories based on the treating physician criteria, and grouped as remission/low or moderate/high disease activity.
Regarding SARS-CoV-2 vaccination, date, and vaccine type (CoronaVac vaccine (Sinovac Biotech), the AstraZeneca vaccine (ChAdOx1), and the vaccines developed by Pfizer (BNT162b2) and Janssen (Ad26.COV2.S) were recorded. The completion of the initial two-dose or single dose regimen and the receiving of one to two booster doses were registered.
Breakthrough COVID-19 clinical presentation (asymptomatic, cough, dyspnea, sore throat, fever, dysgeusia, hyposmia, myalgia, malaise, headache, rhinorrhea), date of diagnosis, confirmatory test performed and outcomes of interest (hospitalization, death) were recorded.
Data management and monitoring
All variables were collected face-to-face, virtual, or by telephone and the review of medical records, according to availability. The data was entered into the Research Electronic Data Capture Platform (Redcap, https://redcap.reumatologia.org.br/). Datasets of this study are not deposited in a publicly available database study. Data will be available upon reasonable request.
Ethical considerations
The study protocol and its corresponding informed consent form were approved by the coordinator center ethics committee (CAAE: 43479221.0.1001.5505) and the independent ethics committee of all participating centers. All patients signed the informed consent before data collection.
This study was conducted in accordance with Good Clinical Practice (GCP) guidelines, the International Conference on Harmonization (ICH), the ethical principles established in the Declaration of Helsinki, the law 3301/09, and the guidelines of the local ethics committee.
Personal identification data was kept anonymous and protected according to international and national regulations to guarantee confidentiality, in accordance with the Law on Protection of Personal Data.
For the purposes of this project, only medical researchers had access to patients’ medical records to obtain the data required for the investigation, thus ensuring their confidentiality.
Statistical analysis
Descriptive analysis of sociodemographic and clinical data was carried out. Continuous variables are expressed as mean and standard deviation when the distribution was considered normal, or as median and interquartile range otherwise. Categorical variables are presented as frequencies and percentages.
Comparative analysis of patients requiring hospitalization due to COVID-19 versus those not requiring hospitalization was performed applying T-Student or Mann-Whitney tests for continuous variables, according to a normal or non-normal distribution. Categorial variables were compared using the Chi-square or Fisher’s exact test, as appropriate.
A binary logistic multiple regression, applying a backward stepwise selection was performed to evaluate the variables associated with breakthrough COVID-19-related hospitalization. Variables presenting a p-value ≤ 0.2 were included in the initial model and excluded until only significant variables persisted in the final model. A p < 0.05 was considered significant. Statistical analyses and model development were performed with
R version 4.3.1 (R Core Team, 2023), with the software RStudio version 2023.6 (Posit Team, 2023), along with the packages “tidyverse” (Wickham et al., 2019) and “gtsummary” (Sjoberg et al., 2021).
Results
Study population
By the time the data for this analysis were extracted, SAFER-Study had included 1600 IMID patients. In this analysis, 162 cases of breakthrough COVID-19 reported in the study database are described. Figure 1 depicts the algorithm with selection of the population of this study.
In SAFER-Study database, 162 cases of breakthrough COVID-19 were described: 132 presented no severe outcomes, 28 were hospitalized and two died.
The characteristics of the 160 patients surviving breakthrough COVID-19, and the comparative analysis between the hospitalized (n=28, 17.5%) and the patients not developing severe outcomes (n=132, 82.5%) are shown on Table 1.
The distribution of the different rheumatic diseases and comorbidities between non-severe and hospitalized patients was similar.
Vaccination
Thirty-one (19.4%) patients received only the two-dose regimen of vaccines, while 112 (70%) and 17 (10.6%) received respectively one and two booster doses. The number of vaccine doses was higher in the non-hospitalized group (p=0.028).
The initial two-dose regimen was mainly with the AstraZeneca vaccine (ChAdOx1) in 93 (58.1%), followed by the CoronaVac vaccine (Sinovac Biotech) in 53 (34.4%), and the Pfizer (BNT162b2) vaccine in 12 (7.5%) patients. The first booster dose was mainly with the Pfizer (BNT162b2) vaccine [n=101 (63.1%)], followed by the AstraZeneca vaccine (ChAdOx1) [n=46 (28.7%)] and the CoronaVac vaccine (Sinovac Biotech) [n=3(1.9%)]. The second booster dose again presented a predominance of the Pfizer (BNT162b2) vaccine [n=64 (40%)], followed by the AstraZeneca vaccine (ChAdOx1) [n=41 (25.6%)] and Janssen (Ad26.COV2.S) [n=7 (4.4%)]. The multiple vaccination schemes applied were not associated to hospitalization.
Before vaccination, patients were using oral glucocorticoids (n=28), csDMARDs (n=133), bDMARDs (n=41), rituximab (n=13), immnosuppressants (n=35) and tsDMARDs (n=2). These frequencies were similar between non-hospitalized and hospitalized individuals.
Breakthrough COVID-19
Breakthrough COVID-19 occurred [Median (IQR)] 113.46 (75.25-134.75) days after the last vaccine dose received. This interval was similar between non-hospitalized and hospitalized patients (Median 102 versus 94 days, p=0.3).
Confirmatory tests were RT-PCR in 73 (46%) and antigen test in 77 (48%) individuals. By the time of COVID-19 diagnosis, 47 (29%) patients were not receiving antirheumatic drugs.
Most (96%) patients reported COVID-19 symptoms: headache (57%), cough (54%), rhinorrhea (51%), sore throat (49%), fever (46%), fatigue (32%), astenia (31%) hyposmia (20%), dysgeusia (18%), and dyspnea (18%), diarrhea (17%), nausea (14%), dizziness (9%), vomiting (4%), myalgia (3%), arthralgias (3%). COVID-19 symptoms lasted 1 to 60 [Median (IQR): 8.95 (5-12)] days. Patients requiring hospitalization had an in-hospital stay of 1 to 33 [Median (IQR): 10.2 (1-23.5)] days. Six hospitalized patients required supplemental oxygen, one needed non-invasive ventilation and no invasive ventilation was reported. Five patients presented an infectious complication (bacterial pneumonia) of COVID-19.
Discussion
This study brings important information on breakthrough COVID-19 clinical presentation and hospitalization determinants in a Brazilian populaiton of IMRD patients. It corroborates previous data on the association of IMRD moderate to high activity and using glucocorticoids, and COVID-19 symptoms of fever or dyspnea, with severe outcome of hospitalization associated with this infection. It also suggests a protective effective of the increased number of vaccine doses, highlighting the importance of booster doses in these patients.
In this cohort, only two (1.2%) COVID-19 related deaths were reported in fully vaccinated individuals, precluding the authors from the evaluation of the determinants of death in these patients. In the study by Global Rheumatology Alliance (GRA) reporting breakthrough COVID-19 in 86 fully vaccinated people with RD, five (6%) deaths occurred. The determinants of COVID-19-related deaths were not evaluated in that study also, but four of these five individuals were older than 60 years and three individuals were on B-cell depleting therapy (BCDT) at the time of vaccination [4]. In the present study, from the two patients who died, one patient was older than 60 years and none received rituximab before vaccination, however, both were using glucocorticoids, one of the predictors of hospitalization in our population.
The hospitalization rate for COVID-19 in this study (17.5%) was lower than the reported in a Latin America study (22.7%), in which data on vaccination were not available [2]. Accordingly, better outcomes, with lower mortality and hospitalization rates, in partially or fully vaccinated IMRD, compared to unvaccinated individuals, have been described [10].
The hospitalization rate described in the present study, was lower than that reported in the study by Global Rheumatology Alliance (GRA), reporting COVID-19 in 86 fully vaccinated people with RD, in which 22 (26%) patients were hospitalized and 5 (6%) died [4]. The lower hospitalization rate may be attributed to different vaccination schemes and genetic backgrounds from the different populations from both works, and to the high frequency of patients receiving booster doses of the vaccine in the present study. Booster vaccination has been shown to further reduce the frequency of COVID-19-related hospital admissions and deaths in people with systemic RDs [11].
The mean period between the infection and the second vaccine dose, or the first or second booster, and the breakthrough COVID-19 was similar to previous studies, as well as the clinical presentation of the COVID-19 [4,5,6].
Despite the established efficacy of COVID-19 vaccines, breakthrough infections occur in those who are fully vaccinated. In IMRD patients, studies have shown that specific classes of medications, e.g. BCDT, bDMARDS, TNFI, immunosuppressants, JAKi, and glucocorticoids, can hamper the humoral response and have negative impact on the T cell-mediated response. Moreover, the decreased severity of breakthrough COVID-19 after booster doses of the vaccines in patients with systemic RDs, in combination with the reassuring results about the safety of vaccines, argues in favour of booster vaccination in patients with IMRDs. Thus, the decrease in hospitalization attributable to the increased number of vaccine doses found by the present work highlight the need for additional booster doses in this population [4,5,6,11,12].
To the authors knowledge, this is the first Brazilian study describing breakthrough COVID-19 in IMRD patients. The main strength of this study is that the population was extracted from a multicenter cohort, conducted by experienced rheumatologists from tertiary Rheumatology Services across Brazil. The number of confirmed cases and their in-depth description shall also be highlighted.
This study has certain limitations, mainly the lack of a control group of healthy individuals presenting breakthrough COVID-19. Moreover, the loss of asymptomatic breakthrough infections, because we only included patients who presented for testing, and the exclusion of symptomatic patients that did not perform a diagnostic test, may have underestimated the frequency of breakthrough COVID-19. Still, the low occurrence of COVID-19 related deaths precluded the researchers from performing the evaluation of the predictors of death in these patients. The evaluation of the immunogenicity of COVID-19 vaccines in the population of this study is ongoing and will be published in another report, allowing further conclusions on the effectiveness of these vaccines in this populations.
Conclusions
In this large cohort study, consisting of fully vaccinated IMRD patients, higher disease activity or chronic use of corticosteroids increased the chance of hospitalization due to COVID-19, while booster vaccine showed protective effect. The decreased severity of breakthrough COVID-19 after booster doses of the vaccines in patients with IMRDs, in combination with the reassuring results about the safety of vaccines, argues in favour of booster vaccination in patients with IMRD. New studies, evaluating the impact of breakthrough COVID-19 and the effects of vaccine booster doses in these patients, are warranted.
Author Contributions
Conceptualization, DCC, VV, GAF, ATC, ETR-N, EIS, MMP, OAM, RMX, VAS, GSP; methodology, DCC, VV, GAF, ATC, ETR-N, EIS, MMP, OAM, RMX, VAS, GSP; software, DCC, VV, GAF, KLLLM, PDCR, SLER, NSS, RPVR, AKGM, VAC, ASRV, AMK, ATL, APNB, FMMMCP, CMPFT, RCES, KLB, YGPO, VOM , RLL, EB, PZL, ATC, ETR-N, EIS, MMP, OAM, RMX, VAS, GSP; methodology, DCC, VV, GAF, ATC, ETR-N, EIS, MMP, OAM, RMX, VAS, GSP.; validation, DCC, VV, GAF, KLLLM, PDCR, SLER, NSS, RPVR, AKGM, VAC, ASRV, AMK, ATL, APNB, FMMMCP, CMPFT, RCES, KLB, YGPO, VOM , RLL, EB, PZL, ATC, ETR-N, EIS, MMP, OAM, RMX, VAS, GSP; methodology, DCC, VV, GAF, ATC, ETR-N, EIS, MMP, OAM, RMX, VAS, GSP.; formal analysis, DCC, investigation, DCC, VV, GAF, KLLLM, PDCR, SLER, NSS, RPVR, AKGM, VAC, ASRV, AMK, ATL, APNB, FMMMCP, CMPFT, RCES, KLB, YGPO, VOM , RLL, EB, PZL, ATC, ETR-N, EIS, MMP, OAM, RMX, VAS, GSP; methodology, DCC, VV, GAF, ATC, ETR-N, EIS, MMP, OAM, RMX, VAS, GSP; resources, VV, GAF, ATC, ETR-N, EIS, MMP, OAM, RMX, VAS, GSP.; data curation, DCC, VV, GAF, KLLLM, PDCR, SLER, NSS, RPVR, AKGM, VAC, ASRV, AMK, ATL, APNB, FMMMCP, CMPFT, RCES, KLB, YGPO, VOM , RLL, EB, PZL, ATC, ETR-N, EIS, MMP, OAM, RMX, VAS, GSP; methodology, DCC, VV, GAF, ATC, ETR-N, EIS, MMP, OAM, RMX, VAS, GSP; writing—original draft preparation, DCC, VV, GAF, GSP; writing—review and editing, DCC, VV, GAF, GSP.; visualization, DCC, VV, GAF, KLLLM, PDCR, SLER, NSS, RPVR, AKGM, VAC, ASRV, AMK, ATL, APNB, FMMMCP, CMPFT, RCES, KLB, YGPO, VOM , RLL, EB, PZL, ATC, ETR-N, EIS, MMP, OAM, RMX, VAS, GSP; methodology, DCC, VV, GAF, ATC, ETR-N, EIS, MMP, OAM, RMX, VAS, GSP; supervision, DCC, VV, GAF, KLLLM, PDCR, SLER, NSS, RPVR, AKGM, VAC, ASRV, AMK, ATL, APNB, FMMMCP, CMPFT, RCES, KLB, YGPO, VOM , RLL, EB, PZL, ATC, ETR-N, EIS, MMP, OAM, RMX, VAS, GSP; methodology, DCC, VV, GAF, ATC, ETR-N, EIS, MMP, OAM, RMX, VAS, GSP; project administration, VV, GAF, ATC, ETR-N, EIS, MMP, OAM, RMX, VAS, GSP; methodology, DCC, VV, GAF, ATC, ETR-N, EIS, MMP, OAM, RMX, VAS, GSP; funding acquisition, VV, GAF, ATC, ETR-N, EIS, MMP, OAM, RMX, VAS, GSP; methodology, DCC, VV, GAF, ATC, ETR-N, EIS, MMP, OAM, RMX, VAS, GSP. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Brazilian Society of Rheumatology and the Brazilian Minitry of Health.
Institutional Review Board Statement
The study protocol and its corresponding informed consent form were approved by the coordinator center ethics committee (CAAE: 43479221.0.1001.5505) and the independent ethics committee of all participating centers. All patients signed the informed consent before data collection. This study was conducted in accordance with Good Clinical Practice (GCP) guidelines, the International Conference on Harmonization (ICH), the ethical principles established in the Declaration of Helsinki, the law 3301/09, and the guidelines of the local ethics committee. Personal identification data was kept anonymous and protected according to international and national regulations to guarantee confidentiality, in accordance with the Law on Protection of Personal Data. For the purposes of this project, only medical researchers had access to patients’ medical records to obtain the data required for the investigation, thus ensuring their confidentiality.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The research dataset of this study is not publicly available due to privacy restricitons, but will be shared upon reasonable request.
Acknowledgments
To the participating centers: Universidade Federal Fluminense (UFF), Universidade Federal do Espírito Santo (UFES), Universidade Federal de Minas Gerais (UFMG), Universidade Federal da Paraíba (UFPB), Universidade Federal de São Paulo (UNIFESP), Universidade Federal de Juiz de Fora (UFJF), Universidade federal de Goiás (UFG), Universidade Federal do Rio Grande do Sul (UFRGS), Hospital universitário da Universidade Federal do Amazonas (UFAM); Hospital Geral da universidade Federal do Ceará (UFCE), Centro EDUMED de pesquisa de Curitiba em conjunto com Universidade Federal do Paraná (UFPR), Serviços Especializados em Reumatologia da Bahia (SER) e centros de referência em Gastroenterologia com pesquisadores cadastrados do GEDIIB. Para o seguimento do estudo no acompanhamento da etapa de vacinação bivalente no país, o estudo contará com a participação dos centros das Universidade Federal do Espírito Santo (UFES), Universidade Federal de São Paulo (UNIFESP), Universidade federal de Goiás (UFG), Universidade Federal do Rio Grande do Sul (UFRGS), Hospital universitário da Universidade federal do Amazonas (UFAM) e Hospital Geral da Universidade Federal do Ceará (UFCE). To the collaborating researchers integrating the Safer-Study task force: Adah Sophia Rodrigues Vieira, Adriana Maria kakehasi, Adriana Ribas Andrade, Alexandre Wagner Silva de Souza, Aline Teixeira de Landa, Ana Karla Guedes de Melo, Ana Luisa Souza Pedreira, Ana Paula Neves Burian, André Gustavo Cunha Trolese, Andréa Teixeira-Carvalho, Andrese Aline Gasparin, Andrieli Caroline Mehl, Anna Carolina Faria Moreira Gomes Tavares, Anna Carolina Simões Moulin, Antonio Luiz Boechat, Artur José Azevedo Pereira, Bárbara Oliveira Souza, Barbara Polli, Camila da Silva Cendon Duran, Camila Maria Paiva França Telles, Carolina Strauss Estevez Gadelha, Catherine Pancotto, Charlles Heldan de Moura Castro, Clara Lyra de Andrade Stefanon, Clarissa Ruas Yasuda, Cristiane Kayser, Cyrla Zaltman, Danielle Cristina Filgueira Alves Batista, Débora Cerqueira Calderaro, Débora Marques Veghini, Edgard Torres dos Reis-Neto, Eduardo Yasuda, Emilia Inoue Sato, Erica Vieira Serrano, Erika Biegelmeyer, Fernanda Dazilio dos Reis, Filipe Faé, Flávia Maria Matos Melo Campos Peixoto, Flavia Zon Pretti, Gabriel Smith Sobral Vieira, Gabriela Guimarães Nogueira, Gecilmara Salviato Pileggi, Gilda Aparecida Ferreira, Guilherme Leví Tres, Heitor Filipe Surlo, Helena da Silva Corona, Isabella Vargas de Souza Lima, Isac Ribeiro Moulaz, João Gabriel Leão Sperancini Amaral, João Pedro Sarcinelli Chagas, Jônatas Almeida Amorim, Jonathan Willian Da Silva Rodrigues, José Geraldo Mill, Jozelia Rêgo, Julia Fagundes Fracasso, Juliana Bühring, Juliana Ribeiro de Oliveira, karina Rosemarie Lallemand Tapia, Katia Lino Baptista, Ketty Lysie Libardi Lira Machado, Kimberly Rossana da Silva Gonçalves, Laís Pizzol Pasti, Laissa Fiorotti Albertino, Laiza Hombre Dias, Laura Gonçalves Rodrigues Aguiar, Leonardo Barbosa da Silva, Leonardo Rodrigues Campos, Lucélia Paula Cabral Schmidt, Ludmila Arrebola Rubin de Celis Mori, Luigi Marangão Calil, Luiza Helena Coutinho Ribeiro, Luiza Lorenzoni Grillo, Lunara Baptista Ferreira, Maisa Brito Nunes, Marcelo de Medeiros Pinheiro, Marcos Mavignier Sousa Dias, Maressa Barbosa Beloni Lirio, Maria Cecília Dias Corrêa, Maria da Penha Gomes Gouvea, Mariana de Oliveira Macabú, Mariana Freitas de Aguiar, Marina Deorce de Lima, Mittermayer Barreto Santiago, Nadja Maria Santiago de Mattos, Natália Rodrigues Querido Fortes, Natália Sarzi Sartori, Natália Seixas de Melo, Nicole Pamplona Bueno de Andrade, Nilzio Antonio da Silva, Odirlei André Monticielo, Olindo Assis Martins-Filho, Paula dos Santos Athayde, Pedro Matos, Pietra Zava Lorencini, Pollyana Vitoria Thomaz da Costa, Priscila Dias Cardoso Ribeiro, Rafaela Cavalheiro do Espírito Santo, Ranielly Corrêa Lube Santos Brum, Raquel Lima de Lima, Rebeca Silva Moreira da Fraga, Regiane Lima, Rejane Maria Rodrigues de Abreu Vieira, Renata Henriques de Azevedo, Ricardo Machado Xavier, Roberta Beatriz Nazareth Alagia, Rodrigo Cutrim Gaudio, Rodrigo Poubel Vieira de Rezende, Rosely Holanda da Silva Sanches, Russian Teixeira Rebello, Sabrina de Souza Ramos, Samira Tatiyama Miyamoto, Sandra Lúcia Euzébio Ribeiro, Tâmara Santos Melo, Thaís Evelyn Karnopp, Thaisa de Moraes Ribeiro Espirito Santo, Valderilio Feijó Azevedo, Valéria Bezerra da Silva, Valeria Valim, Vanessa de Oliveira Magalhães, Vanessa Hax, Vanessa Peruhype-Magalhães, Victória Dornelas Paz Carvalho, Vinícius de Pádua Sanders Medeiros, Vitor Alves Cruz, Viviane Angelina de Souza, Yasmin Gurtler Pinheiro de Oliveira.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Hoff, L. S., Ravichandran, N., Shinjo, S. K., Day, J., Sen, P., Junior, J. G., Lilleker, J. B., Joshi, M., Agarwal, V., Kardes, S., Kim, M., Milchert, M., Makol, A., Gheita, T., Salim, B., Velikova, T., Gracia-Ramos, A. E., Parodis, I., O'Callaghan, A. S., Nikiphorou, E., … COVAD Study Group (2023). COVID-19 severity and vaccine breakthrough infections in idiopathic inflammatory myopathies, other systemic autoimmune and inflammatory diseases, and healthy controls: a multicenter cross-sectional study from the COVID-19 Vaccination in Autoimmune Diseases (COVAD) survey. Rheumatology international, 43(1), 47–58. [CrossRef]
- Isnardi, C. A., Alpizar-Rodriguez, D., Calderaro, D. C., Marques, C. D. L., Pons-Estel, G. J., Xavier, R. M., Saurit, V., Pisoni, C. N., Tissera, Y. S., D'Angelo Exeni, M. E., Alba, P., Pereira, D., Gobbi, C. A., Gamba, M. J., Alfaro, M. A., Virasoro, B. M., Colunga-Pedraza, I. J., Irazoque-Palazuelos, F., Reyes-Cordero, G., Rodriguez-Reyna, T. S., … Martínez-Martínez, M. U. (2024). Factors Associated With Mortality in Patients With Immune-Mediated Rheumatic Diseases and COVID-19 From Latin America: Data From Argentina, Mexico, and Brazil. Journal of clinical rheumatology : practical reports on rheumatic & musculoskeletal diseases, 30(1), e9–e17. [CrossRef]
- Hasseli, R., Richter, J. G., Hoyer, B. F., Lorenz, H. M., Pfeil, A., Regierer, A. C., Schmeiser, T., Strangfeld, A., Voll, R. E., Krause, A., Reckert, S., Gräßler, A., Saar, P., Kapelle, A., Backhaus, M., Blank, N., Henes, J., Osiek, S., Knothe, A., Hoese, G., … COVID19-Rheuma.de collaborators (2023). Characteristics and outcomes of SARS-CoV-2 breakthrough infections among double-vaccinated and triple-vaccinated patients with inflammatory rheumatic diseases. RMD open, 9(2), e002998. [CrossRef]
- Liew, J., Gianfrancesco, M., Harrison, C., Izadi, Z., Rush, S., Lawson-Tovey, S., Jacobsohn, L., Ja, C., Hyrich, K. L., Gossec, L., Strangfeld, A., Carmona, L., Schäfer, M., Frãzao-Mateus, E., Bulina, I., Stafford, F., Tufan, A., Graver, C., Yardımcı, G. K., Zepa, J., … Yazdany, J. (2022). SARS-CoV-2 breakthrough infections among vaccinated individuals with rheumatic disease: results from the COVID-19 Global Rheumatology Alliance provider registry. RMD open, 8(1), e002187. [CrossRef]
- Cook, C., Patel, N. J., D'Silva, K. M., Hsu, T. Y., DiIorio, M., Prisco, L., Martin, L. W., Vanni, K., Zaccardelli, A., Todd, D., Sparks, J. A., & Wallace, Z. S. (2022). Clinical characteristics and outcomes of COVID-19 breakthrough infections among vaccinated patients with systemic autoimmune rheumatic diseases. Annals of the rheumatic diseases, 81(2), 289–291. [CrossRef]
- Alshukairi, A. N., Al-Omari, A., Albeity, A., Alandijany, T. A., Hassan, A. M., El-Kafrawy, S. A., Dada, A., Al Hroub, M. K., El-Saed, A., Bissar, L. S., Daghmush, R. M., Al-Ghamdi, S. M. G., Perlman, S., Azhar, E. I., & Halabi, H. (2022). COVID-19 breakthrough infections in rheumatic diseases patients after vaccination. Journal of infection and public health, 15(6), 685–688. [CrossRef]
- Galmiche, S., Luong Nguyen, L. B., Tartour, E., de Lamballerie, X., Wittkop, L., Loubet, P., & Launay, O. (2022). Immunological and clinical efficacy of COVID-19 vaccines in immunocompromised populations: a systematic review. Clinical microbiology and infection : the official publication of the European Society of Clinical Microbiology and Infectious Diseases, 28(2), 163–177. [CrossRef]
- CDC COVID-19 study shows mRNA vaccines reduce risk of infection by 91 percent for fully vaccinated people, 2021. Available: https://www.cdc.gov/media/releases/2021/p0607-mrna-reduce-risks.html [Accessed 28 Oct 2023].
- Strangfeld, A., Schäfer, M., Gianfrancesco, M. A., Lawson-Tovey, S., Liew, J. W., Ljung, L., Mateus, E. F., Richez, C., Santos, M. J., Schmajuk, G., Scirè, C. A., Sirotich, E., Sparks, J. A., Sufka, P., Thomas, T., Trupin, L., Wallace, Z. S., Al-Adely, S., Bachiller-Corral, J., Bhana, S., … COVID-19 Global Rheumatology Alliance (2021). Factors associated with COVID-19-related death in people with rheumatic diseases: results from the COVID-19 Global Rheumatology Alliance physician-reported registry. Annals of the rheumatic diseases, 80(7), 930–942. [CrossRef]
- Papagoras, C., Fragoulis, G. E., Zioga, N., Simopoulou, T., Deftereou, K., Kalavri, E., Zampeli, E., Gerolymatou, N., Kataxaki, E., Melissaropoulos, K., Panopoulos, S., Fragiadaki, K., Evangelatos, G., Bournia, V. K., Arida, A., Karamanakos, A., Pappa, M., Panagiotopoulos, A., Koutsianas, C., Mparouta, G., … Sfikakis, P. P. (2022). Better outcomes of COVID-19 in vaccinated compared to unvaccinated patients with systemic rheumatic diseases. Annals of the rheumatic diseases, 81(7), 1013–1016. [CrossRef]
- Fragoulis, G. E., Karamanakos, A., Arida, A., Bournia, V. K., Evangelatos, G., Fanouriakis, A., Fragiadaki, K., Kravvariti, E., Laskari, K., Panopoulos, S., Papazoglou, N., Pappa, M., Tektonidou, M. G., & Sfikakis, P. P. (2022). Clinical outcomes of breakthrough COVID-19 after booster vaccination in patients with systemic rheumatic diseases. RMD open, 8(1), e002279. [CrossRef]
- Patel, N. J., Wang, X., Fu, X., Kawano, Y., Cook, C., Vanni, K. M. M., Qian, G., Banasiak, E., Kowalski, E., Zhang, Y., Sparks, J. A., & Wallace, Z. S. (2023). Factors associated with COVID-19 breakthrough infection among vaccinated patients with rheumatic diseases: A cohort study. Seminars in arthritis and rheumatism, 58, 152108. [CrossRef]
Figure 1.
Patient selection from the SAFER-Study.
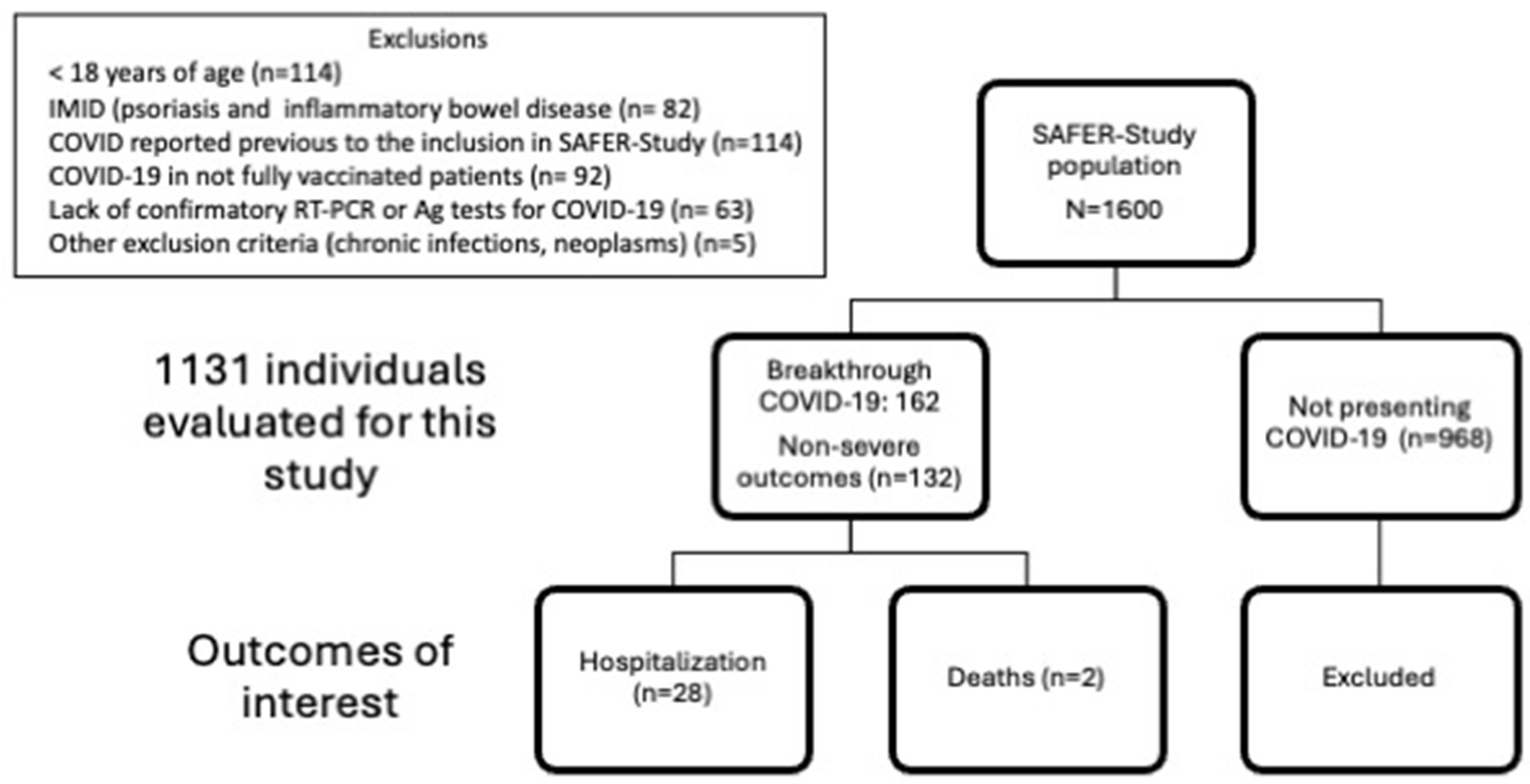
Figure 2.
COVID-19-related hospitalization determinants.
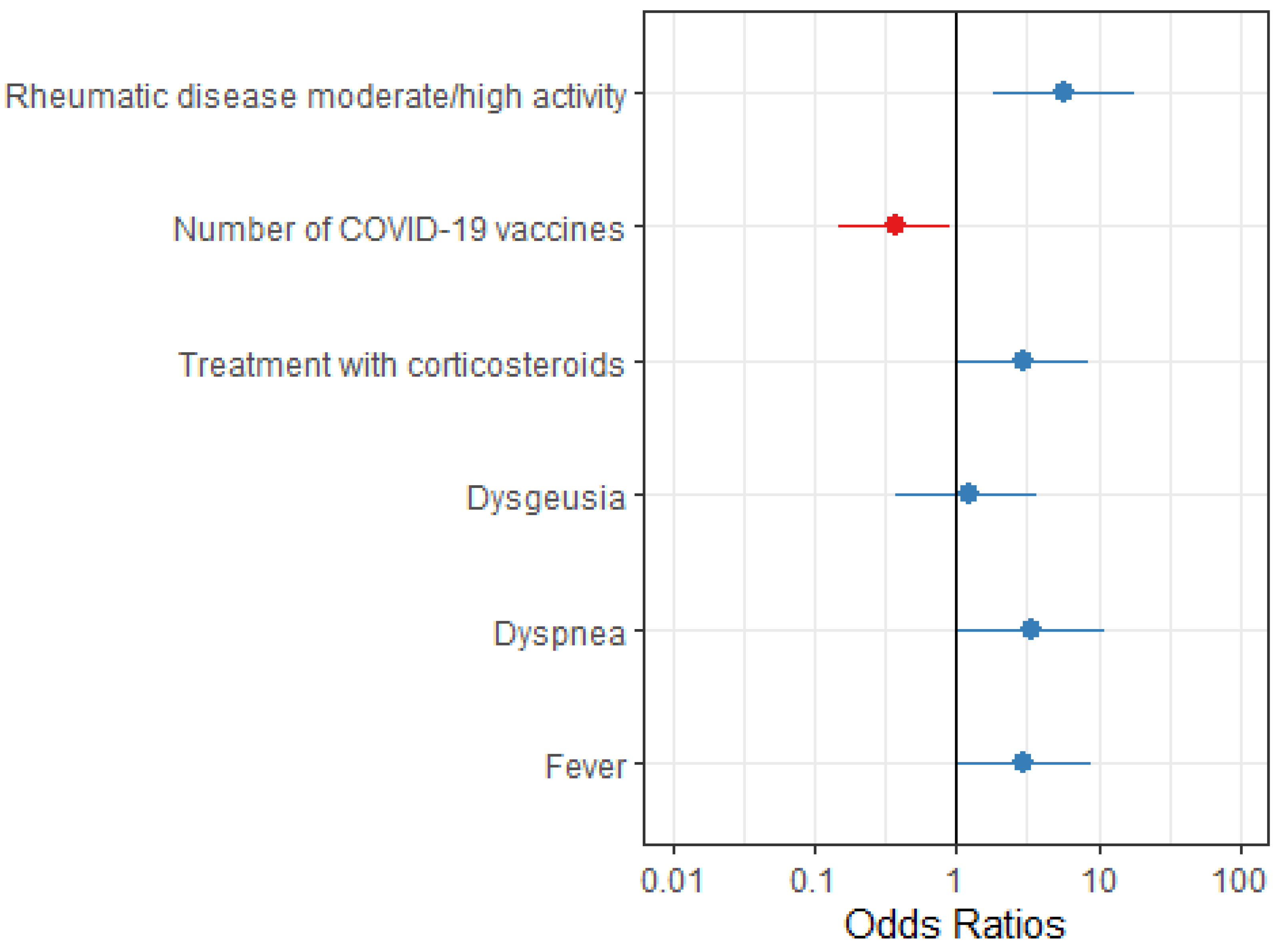

Table 1.
Comparative analysis of the breakthrough COVID-19 patients not hospitalized (n=132) versus hospitalized (n=28). .
Table 1.
Comparative analysis of the breakthrough COVID-19 patients not hospitalized (n=132) versus hospitalized (n=28). .
| Characteristic |
Overall (N = 160)1 |
No (N = 132)1 |
Yes, (N = 28)1 |
p-value2 |
| Age (years) | 44.08 (12.81) | 44.21 (13.21) | 43.46 (10.93) | 0.9 |
| Gender [Female] | 133 (83.1%) | 110 (83.3%) | 23 (82.1%) | >0.9 |
| Self-declared white color | 97 (60.6%) | 77 (58.3%) | 20 (71.4%) | 0.2 |
| CTD/Vasculitis/Other RD | 96 (60.0%) | 78 (60%) | 18 (64%) | 0.67 |
| IJD | 62 (39%) | 52 (40%) | 10 (36%) | 0.67 |
| RD time length (years) | 9.50 (4.00 - 15.00) | 10.00 (4.00 - 15.00) | 8.50 (3.00 - 16.00) | 0.5 |
| RD moderate/high activity before breakthrough COVID-19 | 23 (14%) | 14 (11.5%) | 9 (37.5%) | 0.001 |
| Comorbidity (any) | 102 (63.8%) | 83 (62.9%) | 19 (67.9%) | 0.6 |
| Number of comorbidities | 1 (0-1) | 1 (0-1.25) | 1 (0-1) | 0.3 |
| Number of COVID-19 vaccine doses | 3 (3-4) | 3 (2-4) | 3 (2-3) | 0.028 |
| RD treatment before COVID-19 | ||||
| Glucocorticoids use | 34 (21%) | 24 (10%) | 10 (34%) | 0.04 |
| Glucocorticoids daily doses (mg/Prednisone) | 7.5 (5-10) | 8.75 (5-10) | 5 (5-7.5) | 0.5 |
| cDMARDs | 96 (60%) | 79 (60%) | 17 (60%) | 0.16 |
| bDMARDs | 19 (12%) | 15 (11.5%) | 4 (15%) | 0.4 |
| tsDMARDs | 3 (1.9%) | 1 (0.8%) | 2 (7.1%) | 0.08 |
| Rituximab | 1 (0.6%) | 1 (1%) | 0 (0%) | 0.6 |
| IS | 14 (9%) | 14 (11%) | 0 (0%) | 0.13 |
CTD: connective tissue diseases. RD: rheumatic diseases. IDJ: inflammatory joint diseases. CTD/vasculitis/other rheumatic diseases: 44 systemic lupus erythematosus, 16 vascutitis, 5 systemic sclerosis, 4 inflammatory myopathy, 20 Sjögren’s disease, 3 mixed connective tissue disease and 6 connective diseases overlapping syndrome). IJD (31 rheumatoid arthritis, 1 juvenile idiopathic arthritis, 24 anquilosing spondylitis, 5 psoriasic arthritis, 1 enteropatic arthritis). Comorbidities were cardiomyopathy (n=4), diabetes mellitus (n=8), pulmonary disease (n=8), chronic kidney disease (n=3), arterial hypertension (n=54), obesity (n=20), other comorbidities (n=53), smoking (n=2), alcoholism (n=9). cDMARDs: conventional DMARDs (Methotrexate, Leflunomide, Sulfasalazine, antimalarials). bDMARDs: biologic DMARDs other than Rituximab (abatacept, TNF inhibitors, belimumab, IL-1, IL-6, IL-12/23, IL-17 and IL/23 inhibitors). tsDMARDs: Janus kinase inhibitors (tofacitinib, baricitinib, upadacitinib). IS: immunosuppressants: azathioprine, cyclosporine, tacrolimus, mycophenolate mofetil/mycophenolic acid, cyclophosphamide). 1Mean (SD); Median (IQR); n (%). 2Mann-Whitney test; Fisher's exact test; Pearson's Chi-squared tests.
Table 2.
Univariate and multivariate analysis of the COVID-19-related hospitalization determinants.
| Univariate analysis | Multivariate analysis | ||||
|---|---|---|---|---|---|
| Characteristic | N | OR (95%CI) | p-value | OR (95%CI) | p-value |
| White color | 160 | 1.83 (0.78-4.7) | 0.2 | - | - |
| RD moderate/high activity | 146 | 4.63 (1.68-12.6) | 0.003 | 5.73 (1.85-18.3) | 0.002 |
| Number of COVID-19 vaccine doses | 160 | 0.42 (0.19-0.92) | 0.003 | 0.38 (0.15-0.91) | 0.035 |
| Treatment with glucocorticoids before COVID-19 | 160 | 2.40 (0.95-5.86 | 0.056 | 2.92 (1.01-8.45) | 0.045 |
| Lack of treatment with antirheumatic drugs before COVID-19 | 160 | 0.46 (0.14-1.2 | 0.14 | - | - |
| COVID-19 manifestations | |||||
| Dysgeusia | 160 | 2.58 (1.03-6.27) | 0.038 | - | - |
| Dyspnea | 160 | 4.30 (1.7-10.8 | 0.002 | 3.44 (1.05-11.2) | 0.038 |
| Sore throat | 160 | 2.10 (0.92-5.06 | 0.086 | - | - |
| Fever | 160 | 2.45 (1.07-5.92) | 0.038 | 2.95 (1.05-9.08) | 0.047 |
| Hyposmia | 160 | 2.20 (0.86-5.4) | 0.090 | - | - |
| Cough | 160 | 2.42 (1.03-6.21) | 0.051 | - | - |
1OR: Odds Ratio, CI: Confidence interval.
Table 3.
COVID-19-related deaths.
| Characteristic | Case 1 | Case 2 | Case 3 |
|---|---|---|---|
| SEX | Female | Male | Female |
| AGE (YEARS) | 43 | 63 | 62 |
| IMRD DIAGNOSIS | SLE | IgA-vasculitis | SLE |
| NUMBER OF COVID-19 VACCINE DOSES | 3 | 3 | 1 |
| DATES AND TYPES OF COVID-19 VACCINES ADMINISTERED | Dose 1: CoronaVac (11Sep2021) Dose 2: CoronaVac (13Oct2021) Dose 3: ChAdOx1 (13Oct2022) |
Dose 1: ChAdOx1 (05May2021) Dose 2: ChAdOx1 (27May2021) Dose 3: ChAdOx1 (27Sep2021) |
Dose 1: ChAdOx1 (05May2021) |
| COMORBIDITIES | CKD stage II, arterial hypertension, obesity (BMI: 41) | None | CKD stage II-III, arterial hypertension, type 2 diabetes mellitus |
| IMRD TREATMENT | PDN 12,5 mg + MMF | PDN 10 mg | HCQ |
| COVID-19 MANIFESTATIONS | NR |
Flu-like symptoms, fever and cough starting on 14Nov2021. Positive COVID-19 on 17Nov2021. Hospitalized on 19Nov2021. Was transferred to the ICU on 23Nov2021. Developed SARS with acute respiratory failure and the need for invasive mechanical ventilation, and AKI and died on 29Nov2021. |
Flu-like symptoms starting on 03Jun2021. Positive COVID-19 RT-PCR on 04Jun2021. Hospitalized for respiratory support. Developed SARS and died com 03Jul2021 |
| DEATH DATE | 19Nov2022 | 29Nov2021 | 03Jul2021 |
IMRD: Immune-mediated rheumatic disease. SLE: Systemic lupus erythematosus. CKD: chronic kidney disease. BMI: body mass index. PDN: prednisone. MMF: mophetil mycophenolate. HCQ: Hydroxychloroquine. NR: Not reported. SARS: Severe acute respiratory syndrome. ICU: Intensive care unit. AKI: Acute kidney injury.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



