
Submitted:
30 June 2024
Posted:
02 July 2024
You are already at the latest version
Abstract
The IMbrave150 trial established atezolizumab with bevacizumab (A+B) as standard care for hepatocellular carcinoma (HCC), recommending an esophagogastroduodenoscopy (EGD) within 6 months of treatment initiation to prevent bleeding from esophagogastric varices. The necessity of mandatory EGD for all patients remains unclear. We retrospectively analyzed 112 HCC patients treated with A+B at five Canadian cancer centers from July 1, 2020, to August 31, 2022. A+B was the first-line therapy for 90% of patients, with median overall survival at 20.3 months and progression-free survival at 9.6 months. There was no survival difference between patients with bleeding and those without. Before A+B, 71%(79) of patients underwent an EGD within 6 months, revealing varices in 41%(32) and requiring intervention in 19%(15). The overall bleeding rate was 15%(17), with GI-specific bleeding occurring in 83%(5) of the EGD group and 17%(1) of the non-EGD group (p=0.24). Non-GI bleeding was observed in 10%(11) of patients. Outcomes for HCC patients treated with A+B in Canada were comparable to IMbrave150. Our study showed twice the rate of varices detection and treatment compared to IMbrave150, reflecting real-world treatment of high-risk populations. There was no increased GI bleeding in patients without pre-treatment EGD, supporting a selective EGD approach.
Keywords:
atezolizumab
; bevacizumab
; hepatocellular carcinoma
; EGD
; varices
; GI bleeding
1. Introduction
Hepatocellular carcinoma (HCC) constitutes 75-90% of primary liver cancer and ranks as the third leading cause of global cancer-related deaths.[1,2] Predictions indicate a 41% increase in global HCC mortality rates by 2040.[2,3] HCC is a tumor characterized by high vascularization,[4] and clinical trial data emphasize targeting vascular endothelial growth factor (VEGF)-mediated angiogenesis in HCC treatment.[5,6,7,8] Anti-VEGF agents including sorafenib, lenvatinib, and regorafenib have been standard systemic therapies, but they only provided a modest improvement in survival.[9] The IMbrave150 trial showed superior outcomes with atezolizumab with bevacizumab (A+B) in terms of overall survival (19.2 vs 13.4 months), progression-free survival (6.9 vs 4.3 months), and objective response rate (30% vs 11%) compared to sorafenib.[10,11] Based on these results, A+B has become a recognized first-line immunotherapy-based combination for untreated locally advanced or metastatic HCC.
More than 80% of HCC cases occur in the presence of cirrhosis, putting individuals at risk of portal hypertension thus complicating the management of HCC.[12,13] In the IMbrave150 trial, all participants were required to undergo esophagogastroduodenoscopy (EGD) within 6 months of starting treatment. This protocol aimed to detect and treat all esophagogastric varices to minimize potential GI-related bleeding complications related to the high-dose bevacizumab (15mg/kg) administered to patients in the experimental arm. The IMbrave150 trial reported a higher incidence of GI bleeding in A+B patients (7%) compared to the sorafenib arm (4.5%).[10] Similar results were recapitulated in the ORIENT-32 trial with the combination of sintilimab and IBI305, a bevacizumab biosimilar.[14] Given the increased risk of GI bleeding associated with bevacizumab despite mandated pre-treatment EGD in the IMBrave150 trial, current guidelines from the American Society of Clinical Oncology (ASCO), European Society for Medical Oncology (ESMO), American Association for Study of Liver Disease (AASLD), American Gastroenterological Association (AGA) and National Comprehensive Cancer Network (NCCN) suggest patients undergo EGD assessment within 6 months before commencing A+B.[15,16,17,18]
The necessity of pre-treatment EGD for all HCC patients has been a subject of debate among some medical oncologists and hepatologists. It remains uncertain whether every patient requires a screening EGD before A+B. In cases where cirrhosis is not documented by a hepatology team and there is a low risk of portal hypertension, initiation of A+B without a recent EGD may be a justifiable approach. This practice has been adopted at a few Canadian cancer centers, mainly to avoid delays associated with waiting for an EGD, which could hinder the timely commencement of systemic therapy. Mandating EGD for patients with a low risk of portal hypertension is also not a cost-effective practice. There are alternative non-invasive methods (i.e. transient elastography and platelet count) to predict clinically significant portal hypertension (CSPH) although their use in HCC cases is not fully verified.[19,20] Primary prophylaxis for preventing variceal bleeding has evolved in the last decade, with both endoscopic band ligation and non-selective beta-blockers considered acceptable strategies in patients with cirrhosis.[21,22] To our knowledge, limited data exist regarding the safety of selective EGD in HCC patients undergoing A+B.
The primary aims of this study were to evaluate the effectiveness of A+B in real-world clinical practice, the uptake of pre-treatment EGD, and treatment-related bleeding rates in HCC patients.
2. Materials and Methods
2.1. Study Design
We conducted a pooled population-based retrospective study of HCC patients who received A+B outside clinical trials. This study utilized the Hepatocellular Carcinoma Cancer Health Outcomes Research Database (HCC-CHORD) consortium, a national collaboration of oncologists at several Canadian cancer centers. Ethics approval was obtained from collaborating institutions for the HCC-CHORD project.
2.2. Study Population
We identified all patients with a confirmed histologic and/or radiographic diagnosis of HCC who received A+B in any line of treatment from July 1, 2020 to August 31, 2022. All patients with locally advanced or metastatic or unresectable HCC were eligible for inclusion. Patients who received A+B were identified through cancer center pharmacy database records. Patient charts were reviewed to confirm the HCC diagnosis and that each patient had received at least one treatment with A+B.
2.3. Data Collection
Data for this study was obtained from two cancer centers in the province of Ontario, all cancer centers in Alberta, and one cancer center in Manitoba. Data collection was completed using a uniform database template across all collaborating sites. Patient demographics included ethnicity, Eastern Cooperative Oncology Group (ECOG) performance status, underlying liver disease etiology, Child-Pugh class, Barcelona Clinic Liver Cancer (BCLC) staging, tumor-related characteristics, previous locoregional treatments, routine blood results, pre-treatment EGD, and the systemic therapy received. Bleeding is defined as clinical events that occur after starting A+B and consist of a drop in hemoglobin level, need for blood transfusion, or further intervention including temporarily or permanently discontinuing A+B. The bleeding is categorized into GI-related or non-GI-related events.
2.4. Statistical Analysis
The primary objective was to assess the real-world effectiveness of A+B. A comparative analysis was conducted to evaluate the patients’ outcomes in this study with those observed in the IMbrave150 trial. The primary outcome was overall survival (OS), measured in months from the start date of A+B until the date of death, considering censoring at the last follow-up. Secondary outcomes included progression-free survival (PFS) and objective response rate (ORR). PFS was defined as the duration from the start of A+B to either disease progression or death. ORR was determined based on the treating physician's assessment of radiographic imaging and/or radiologist reports as practical limitations prevented the imaging assessment with RECIST 1.1 and/or modified RECIST (mRECIST) criteria.
Patient demographics, treatment details, and toxicities were summarized using descriptive statistics. Categorical variables were presented as frequency counts and proportions, and continuous variables were presented as median and interquartile range (IQR). Pearson’s Chi-square test or Fisher’s exact test was employed to compare subgroups for categorical variables, while the Wilcoxon rank-sum test was used for continuous variables. The Kaplan-Meier method was used to assess time-to-event outcomes (i.e. PFS, OS) and statistical comparisons were made using the log-rank test. A Cox proportional hazards model was constructed, incorporating relevant clinical and pathological factors, to estimate their impact on bleeding risk and survival. All statistical tests were two-sided, and the significance level was defined a priori as <0.05. Analyses were performed using the FactoMineR package on the R software (version 4.3.0).
3. Results
3.1. Patient Population
We identified a total of 112 patients treated with A+B. Patient characteristics are shown in Table 1. The median age was 66 years, with 87% were male and 24% were East Asian. The proportion of patients with cirrhosis was 67%, diagnosed either histologically or radiologically, including transient elastography. The predominant etiologies of liver disease were hepatitis C virus (35%) and hepatitis B virus (26%). Before A+B, 95% had an ECOG 0-1, 91% were Child-Pugh A, and 71% had BCLC stage C disease. Portal vein thrombosis was present in 37% of patients. Before A+B, 72% of patients had received locoregional therapies.
At the time of data cut-off, 72% (81) of patients had discontinued A+B. Reasons for treatment discontinuation included disease progression (37%), patient choice (26%), toxicity (18.5%), and cancer-related death (18.5%). In terms of line of therapy, 90% (101) received A+B as first-line, 9% (10) as second-line, and 1% (1) as a third-line treatment option. All systemic treatments administered in this study population are shown in Table 2.
3.2. Effectiveness of Atezolizumab and Bevacizumab
Table 3 illustrates a comparative analysis of A+B treatment efficacy between this study and the IMbrave150 trial. During a follow-up period of 10.4 months (95% CI, 0.4-47.9), the overall median OS was 20.3 months (95% CI, 16.5-NR) [Figure 1A]. For the patients treated with A+B as first-line, the median OS was 20.3 months (95% CI, 14.4-NR). For patients who received A+B as a second or third-line treatment, the median OS was 27.0 months (95% CI, 16.1-NR; p=0.45) [Figure 1B]. The overall median PFS was 9.6 months (95% CI, 6.1-11.9). [Figure 2A] In the first-line treatment cohort, PFS was 8.0 months (95% CI, 5.8-11.0), and for subsequent lines was 15.8 months (95% CI, 10.3-NR) (p=0.082) [Figure 2B]. Baseline Albumin-bilirubin (ALBI) grade 1 was significantly associated with prolonged OS but did not seem to influence PFS. The OS and PFS did not differ by liver disease etiologies or the presence of portal vein tumor thrombosis. [Figures S1 and S2].
The overall ORR was 36%, including a complete response in 1 patient (1%). Overall, the disease control rate is 77%. This is consistently observed whether A+B was employed as a first-line (77%) or subsequent-line treatment (78%) (p=0.16).
3.3. EGD Utilization and Esophagogastric Varices
Among 112 patients who received A+B, 71% (79) underwent EGD within 6 months before starting A+B. The remaining 29% (33) patients proceeded with A+B without an EGD. The main reasons for not undergoing pre-treatment EGD are listed in Table 1. The reasons for not conducting EGD in 26 patients were not documented.
More patients in the EGD group had cirrhosis (68%) compared to the non-EGD group (32%), although this difference is not statistically significant (p=0.45). Table 4 compares patients who underwent EGD with those who did not. Patients in the EGD group had a lower median platelet count than the non-EGD group (162 x 109/L vs 189 x 109/L, p=0.17). Only 5% (6 out of 112) patients had a platelet count below 150 x 109/L, and 2% (2 out of 112) had a platelet count below 100 x 109/L.
Among the 79 patients in the EGD group, 41% (32) patients were found to have varices, and 19% (15) had received intervention for varices before A+B, either through endoscopic band ligation and/or oral beta-blockers.
3.4. Bleeding Events during A+B Treatment
A non-significant trend suggests that patients with evidence of varices experienced more bleeding during A+B (39% vs 10%, p=0.07). Patients with high-risk varices that required intervention developed more bleeding events compared to those not needing variceal treatment (47% vs 11%; p=0.003). The overall bleeding rate was 15% (17), with the GI-specific bleeding rate being relatively low at 5% (6). The rate of non-GI bleeding events was 10% (n=11; 6 epistaxis, 1 ecchymosis, 1 periodontal, and 3 unspecified. In terms of GI-specific bleeding was 83% (5) in the EGD group vs 17% (1) in the non-EGD group, attributable to diverticular bleeding.
There was a significant association between bleeding risk and patients with hepatitis B virus and those with a history of multiple TACE procedures (both p=0.03) [Table S1]. Patients with bleeding events also exhibited a lower platelet count of median 127 x 109/L [range 84-220], whereas those without bleeding had a platelet count of 188 x 109/L [range 49-574]; p=0.001.
Bleeding complications did not impact patient survival. Median OS was 20.3 months (95% CI, 13.0-NR) among patients with bleeding, compared to 19.7 months (95% CI, 16.5-NR) for those without bleeding; p=0.78. PFS also did not differ between patients with bleeding and those without (13.8 vs 14.8 months; p=0.95) [Table 3].
4. Discussion
Our results provide evidence that the real-world effectiveness of A+B in Canadian clinical practice appears similar to the outcomes observed in the IMbrave150 trial.[11] The higher PFS and ORR observed in our study may be attributed to the physician assessments documented in clinical notes, as opposed to the independently assessed RECIST 1.1 and HCC-specific mRECIST criteria used in the IMbrave150 trial. The significantly longer PFS seen in our patients receiving subsequent treatments may be due to the supportive care provided by the Canadian health system. This underscores the importance of optimal supportive management for patients even after treatment cessation. The median OS in this study is higher than other real-world studies (Casadei-Gardini et al., Fulgenzi et al., and D’Alessio et al.) which reported median OS in the range of 14.9 to 16.4 months.[23,24,25] Discrepancies may arise from variations in study populations in terms of HCC stage, underlying liver disease etiologies, liver function, and treatment availability. In contrast to Casadei-Gardini and Fulgenzi et al., this study recruited fewer patients with prior TACE (26%), a procedure recognized for its potential adverse impact on liver function. D'Alessio et al. involved 216 patients across Europe, the United States, and parts of Asia, and reported the lowest median OS of 14.9 months among all the studies conducted in a real-world setting.[23,26] This is likely related to the higher proportion of patients with Child-Pugh B liver function (24%), compared to 9% in our study.[23] Child-Pugh A patients showed superior OS with A+B than patients with Child-Pugh B (16.8 vs 6.7 months, respectively, p=0.0003).[23] Our study also had a slightly higher percentage of patients with viral etiology (61% vs 55% in Casadei-Gardini et al.).[25] This could serve as a contributing factor since patients with viral etiology may derive more benefit from immune checkpoint inhibition, as indicated by subgroup analyses [27]. A meta-analysis by Kulkarni et al. which included 5400 patients in a real-world setting demonstrated A+B effectiveness across liver disease etiologies.[26]
The IMbrave150 trial mandated pre-treatment EGD within 6 months of treatment initiation due to the higher GI bleeding risk in the A+B arm. This observation may be overestimated by the trial's 2:1 recruitment, with twice as many patients receiving A+B for a longer duration compared to the sorafenib arm. The incidence of bleeding complications related to TKIs is around 9%. [28,29] It is also important to note that the IMbrave 150 trial excluded patients with Child-Pugh B and macrovascular invasion, unlike the SHARP and REFLECT trials that included these populations. Despite our selective approach, with 71% of patients undergoing an EGD, our GI-specific bleeding incidence was comparable to the IMbrave150 trial (5% vs 3%).[11] Comparison between groups with EGD and without EGD revealed no significant differences in bleeding rates or baseline characteristics. No negative impact on treatment outcomes was observed among 29% of patients who did not undergo EGD. We observed a higher rate of varices detection (41% vs 26%) and treatment (19% vs 11%) than the IMbrave150 trial, reflecting a real-world treatment setting involving more advanced diseases and cirrhosis.[10] Although more bleeding occurred among patients who had received varices treatment (p=0.003), it is plausible that the observed bleeding may be attributed to early bleeding from post-banding ulcers. However, we lacked specific details of patients who underwent endoscopic band ligation.
High-risk varices defined by size > 5mm or red markings (indicating a thin wall) should receive prophylaxis, with either endoscopic band ligation or non-selective beta-blockers, to prevent bleeding consequences. Both options are considered acceptable standard treatment, as randomized clinical trials did not establish a preferred strategy.[17,21,22,30,31]. The PREDESCI trial, however, favored the beta-blockers option for preventing hepatic decompensation, which subsequently reduces the incidence of ascites, varices, and variceal bleeding.[21] Another study showed that the benefit of endoscopic band ligation in preventing variceal bleeding and improving OS is consistently observed across the whole HCC population, with beta-blockers being more effective in patients with BCLC stage C/D.[32]
Non-invasive tools such as liver stiffness measurement (LSM) using transient elastography have reshaped the management of chronic liver disease patients.[19] Based on BAVENO VI criteria, cirrhotic patients with LSM < 20 kPa and a platelet count > 150 x 109/L are unlikely to have high-risk varices (3%) and can therefore forgo EGD screening.[20] A meta-analysis involving 7,387 patients with cirrhosis confirmed the high sensitivity (97%) for BAVENO VI criteria in detecting high-risk varices.[33] This meta-analysis reported a lower prevalence of high-risk varices of 14%, as compared to 26% observed in the IMbrave150 trial, although not all varices identified were classified as high-risk. 10 The utilization of BAVENO VI criteria in the HCC cases is still limited, with studies reporting varying false negative rates. Wu et al. recently validated these criteria in a prospective study involving advanced HCC patients, demonstrating a 21% reduction in unnecessary EGD.[34] In this analysis, BAVENO VI criteria demonstrated a sensitivity of 87%, a negative predictive value of 85%, and a false negative of 3.5%.[34] In contrast, a retrospective French study involving 185 HCC patients demonstrated a minimum 8% false negative rate in applying the BAVENO VI criteria to exclude high-risk varices. The rate was higher in subgroups with larger infiltrative tumors (>5cm) or main portal vein thrombosis.[35] Otherwise, this study reported comparable rates of sensitivity 93% and negative predictive value 92%. [35]
The updated BAVENO VII consensus from 2022 continues to rely on the BAVENO VI criteria for determining which cirrhotic patients can safely avoid endoscopic investigation.[36] In HCC patients, more research is needed to establish specific cut-off values that would warrant an EGD, particularly in cases with confounding risk factors such as larger tumors, portal vein thrombosis, or previous varices. BAVENO VII suggests beta-blockers as a primary option for variceal bleeding prophylaxis in cirrhotic patients, and it may be reasonable to initiate beta-blockers in low-risk individuals.[31] EGD should be contemplated for patients deemed high risk or those needing endoscopic band ligation due to active bleeding, contraindications, or beta-blocker intolerance. This approach is preferred because endoscopic band ligation carries the risk of bleeding from post-banding ulcers and may necessitate multiple sessions for complete variceal eradication, potentially causing treatment delays. It is important to note that hypertension occurred in 28% of patients (39% Grade 3/4) undergoing A+B.[11,26] Ideally, oncologists should opt for beta-blockers over alternative anti-hypertensive drugs as this choice not only manages the treatment side effects but also provides preventive benefits against variceal bleeding.
The IMbrave150 trial indicated that most treatment-related bleeding events occurred later, often coinciding with disease progression.[11] Rather than strictly performing EGD before starting A+B, screening EGD could be conducted at different intervals during treatment based on personalized clinical risk features. Protocols allowing EGD within 12 months, rather than 6 months, are less burdensome on the healthcare system. PFS and OS did not differ significantly between our patients who experienced bleeding and those who did not. Whilst it is reassuring that bleeding events do not significantly affect survival in both EGD and non-EGD groups, it is crucial to note that most of the bleeding events in our study were non-GI in nature. A significantly increased bleeding risk was observed in patients with prior multiple TACE procedures or hepatitis B virus, however, the limited sample size in both cohorts warrants caution in drawing definitive conclusions. No significant correlations in bleeding incidence were found concerning baseline tumor factors.
Our study's main limitations include its retrospective design and small sample size, particularly in the non-EGD group, which may introduce biases and limit the establishment of causal relationships. Budgetary and logistical constraints also restricted the objective assessment of imaging according to RECIST 1.1 criteria. Our data analysis is further limited by the absence of time-dependent variables such as varices grade, severity of bleeding events, and the use of concurrent anticoagulants and beta-blockers before EGD. Medical records frequently lacked documentation explaining why some patients did not undergo EGD. Physicians likely selected candidates for EGD based on clinical risk factors for portal hypertension and bleeding. When documented, the most common reason for forgoing EGD was a collaborative decision with hepatologists due to the patient's clinical absence of cirrhosis or low likelihood of portal hypertension. Despite these considerations, insights from our retrospective analysis of 33 patients without EGD suggest that selective EGD in a well-defined HCC cohort may be a reasonable approach).
5. Conclusions
The effectiveness of A+B and the associated risk of GI bleeding in real-world practice appear similar to those observed in the IMbrave150 trial. Targeted EGD screening does not seem to adversely affect treatment outcomes or increase the risk of GI bleeding. We are conducting a prospective study (EVBER-HCC: Evaluating Gastrointestinal Bleeding Risks and EGD Requirement in Low-Risk HCC Patients Undergoing Atezolizumab and Bevacizumab; University Health Network institutional authorization CAPCR#:23-5915) to validate this finding. This study employs non-invasive stratification tools such as transient elastography and platelet count to identify HCC patients without hepatic decompensation and with a low risk of portal hypertension who can safely avoid pre-treatment EGD.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
All the authors contributed to data curation and revising of this manuscript. CL Lee contributed to conceptualization, project administration, data curation, formal analysis, investigation, visualization, methodology, writing original drafts, writing reviews, and editing. PQ Ding contributed to formal analysis and visualization; JJ Knox and VC Tam: conceptualization, resources, funding acquisition, project administration, data curation, supervision, validation, writing review, and editing.
Funding
This study received no funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Research Ethics Board at the University Health Network, Health Research Ethics Board of Alberta, and other participating cancer centers.
Informed Consent Statement
Patient consent was waived as this was a retrospective observational study.
Data Availability Statement
Research data supporting this publication are included within this article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Gao, X.; Zhao, R.; Ma, H.; Zuo, S. Efficacy and Safety of Atezolizumab plus Bevacizumab Treatment for Advanced Hepatocellular Carcinoma in the Real World: A Single-Arm Meta-Analysis. BMC Cancer 2023, 23, 635. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J Clin 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Rich, N.E.; Yopp, A.C.; Singal, A.G.; Murphy, C.C. Hepatocellular Carcinoma Incidence Is Decreasing Among Younger Adults in the United States. Clinical Gastroenterology and Hepatology 2020, 18, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Sperandio, R.C.; Pestana, R.C.; Miyamura, B.V.; Kaseb, A.O. Hepatocellular Carcinoma Immunotherapy. Annu. Rev. Med. 2022, 73, 267–278. [Google Scholar] [CrossRef] [PubMed]
- Morse, M.A.; Sun, W.; Kim, R.; He, A.R.; Abada, P.B.; Mynderse, M.; Finn, R.S. The Role of Angiogenesis in Hepatocellular Carcinoma. Clinical Cancer Research 2019, 25, 912–920. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.-F.; De Oliveira, A.C.; Santoro, A.; Raoul, J.-L.; Forner, A.; et al. Sorafenib in Advanced Hepatocellular Carcinoma. N Engl J Med 2008, 359, 378–390. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.-H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.-W.; Han, G.; Jassem, J.; et al. Lenvatinib versus Sorafenib in First-Line Treatment of Patients with Unresectable Hepatocellular Carcinoma: A Randomised Phase 3 Non-Inferiority Trial. The Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef] [PubMed]
- Finn, R.S.; Bentley, G.; Britten, C.D.; Amado, R.; Busuttil, R.W. Targeting Vascular Endothelial Growth Factor with the Monoclonal Antibody Bevacizumab Inhibits Human Hepatocellular Carcinoma Cells Growing in an Orthotopic Mouse Model. Liver International 2009, 29, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Raoul, J.-L.; Frenel, J.-S.; Raimbourg, J.; Gilabert, M. Current Options and Future Possibilities for the Systemic Treatment of Hepatocellular Carcinoma. Hepatic Oncology 2019, 6, HEP11. [Google Scholar] [CrossRef] [PubMed]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.-Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N Engl J Med 2020, 382, 1894–1905. [Google Scholar] [CrossRef]
- Cheng, A.-L.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.-Y.; Lim, H.Y.; Kudo, M.; Breder, V.; Merle, P.; et al. Updated Efficacy and Safety Data from IMbrave150: Atezolizumab plus Bevacizumab vs. Sorafenib for Unresectable Hepatocellular Carcinoma. J Hepatol 2022, 76, 862–873. [Google Scholar] [CrossRef] [PubMed]
- Blachier, M.; Leleu, H.; Peck-Radosavljevic, M.; Valla, D.-C.; Roudot-Thoraval, F. The Burden of Liver Disease in Europe: A Review of Available Epidemiological Data. Journal of Hepatology 2013, 58, 593–608. [Google Scholar] [CrossRef] [PubMed]
- Pinter, M.; Trauner, M.; Peck-Radosavljevic, M.; Sieghart, W. Cancer and Liver Cirrhosis: Implications on Prognosis and Management. ESMO Open 2016, 1, e000042. [Google Scholar] [CrossRef]
- Ren, Z.; Xu, J.; Bai, Y.; Xu, A.; Cang, S.; Du, C.; Li, Q.; Lu, Y.; Chen, Y.; Guo, Y.; et al. Sintilimab plus a Bevacizumab Biosimilar (IBI305) versus Sorafenib in Unresectable Hepatocellular Carcinoma (ORIENT-32): A Randomised, Open-Label, Phase 2–3 Study. The Lancet Oncology 2021, 22, 977–990. [Google Scholar] [CrossRef] [PubMed]
- Vogel, A.; Martinelli, E.; Vogel, A.; Cervantes, A.; Chau, I.; Daniele, B.; Llovet, J.M.; Meyer, T.; Nault, J.-C.; Neumann, U.; et al. Updated Treatment Recommendations for Hepatocellular Carcinoma (HCC) from the ESMO Clinical Practice Guidelines. Annals of Oncology 2021, 32, 801–805. [Google Scholar] [CrossRef]
- Gordan, J.D.; Kennedy, E.B.; Abou-Alfa, G.K.; Beg, M.S.; Brower, S.T.; Gade, T.P.; Goff, L.; Gupta, S.; Guy, J.; Harris, W.P.; et al. Systemic Therapy for Advanced Hepatocellular Carcinoma: ASCO Guideline. J Clin Oncol 2020, 38, 4317–4345. [Google Scholar] [CrossRef] [PubMed]
- Singal, A.G.; Llovet, J.M.; Yarchoan, M.; Mehta, N.; Heimbach, J.K.; Dawson, L.A.; Jou, J.H.; Kulik, L.M.; Agopian, V.G.; Marrero, J.A.; et al. AASLD Practice Guidance on Prevention, Diagnosis, and Treatment of Hepatocellular Carcinoma. Hepatology 2023. [Google Scholar] [CrossRef]
- Su, G.L.; Altayar, O.; O’Shea, R.; Shah, R.; Estfan, B.; Wenzell, C.; Sultan, S.; Falck-Ytter, Y. AGA Clinical Practice Guideline on Systemic Therapy for Hepatocellular Carcinoma. Gastroenterology 2022, 162, 920–934. [Google Scholar] [CrossRef] [PubMed]
- Abraldes, J.G.; Bureau, C.; Stefanescu, H.; Augustin, S.; Ney, M.; Blasco, H.; Procopet, B.; Bosch, J.; Genesca, J.; Berzigotti, A.; et al. Noninvasive Tools and Risk of Clinically Significant Portal Hypertension and Varices in Compensated Cirrhosis: The “Anticipate” Study. Hepatology 2016, 64, 2173–2184. [Google Scholar] [CrossRef]
- Pons, M.; Augustin, S.; Scheiner, B.; Guillaume, M.; Rosselli, M.; Rodrigues, S.G.; Stefanescu, H.; Ma, M.M.; Mandorfer, M.; Mergeay-Fabre, M.; et al. Noninvasive Diagnosis of Portal Hypertension in Patients With Compensated Advanced Chronic Liver Disease. Am J Gastroenterol 2021, 116, 723–732. [Google Scholar] [CrossRef]
- Villanueva, C.; Albillos, A.; Genescà, J.; Garcia-Pagan, J.C.; Calleja, J.L.; Aracil, C.; Bañares, R.; Morillas, R.M.; Poca, M.; Peñas, B.; et al. β Blockers to Prevent Decompensation of Cirrhosis in Patients with Clinically Significant Portal Hypertension (PREDESCI): A Randomised, Double-Blind, Placebo-Controlled, Multicentre Trial. The Lancet 2019, 393, 1597–1608. [Google Scholar] [CrossRef]
- Garcia-Tsao, G.; Abraldes, J.G. Nonselective Beta-Blockers in Compensated Cirrhosis: Preventing Variceal Hemorrhage or Preventing Decompensation? Gastroenterology 2021, 161, 770–773. [Google Scholar] [CrossRef]
- D’Alessio, A.; Fulgenzi, C.A.M.; Nishida, N.; Schönlein, M.; Von Felden, J.; Schulze, K.; Wege, H.; Gaillard, V.E.; Saeed, A.; Wietharn, B.; et al. Preliminary Evidence of Safety and Tolerability of Atezolizumab plus Bevacizumab in Patients with Hepatocellular Carcinoma and Child-Pugh A and B Cirrhosis: A Real-world Study. Hepatology 2022, 76, 1000–1012. [Google Scholar] [CrossRef]
- Fulgenzi, C.A.M.; Cheon, J.; D’Alessio, A.; Nishida, N.; Ang, C.; Marron, T.U.; Wu, L.; Saeed, A.; Wietharn, B.; Cammarota, A.; et al. Reproducible Safety and Efficacy of Atezolizumab plus Bevacizumab for HCC in Clinical Practice: Results of the AB-Real Study. European Journal of Cancer 2022, 175, 204–213. [Google Scholar] [CrossRef]
- Casadei-Gardini, A.; Rimini, M.; Tada, T.; Suda, G.; Shimose, S.; Kudo, M.; Cheon, J.; Finkelmeier, F.; Lim, H.Y.; Rimassa, L.; et al. Atezolizumab plus Bevacizumab versus Lenvatinib for Unresectable Hepatocellular Carcinoma: A Large Real-Life Worldwide Population. European Journal of Cancer 2023, 180, 9–20. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, A.V.; Tevethia, H.; Kumar, K.; Premkumar, M.; Muttaiah, M.D.; Hiraoka, A.; Hatanaka, T.; Tada, T.; Kumada, T.; Kakizaki, S.; et al. Effectiveness and Safety of Atezolizumab-Bevacizumab in Patients with Unresectable Hepatocellular Carcinoma: A Systematic Review and Meta-Analysis. eClinicalMedicine 2023, 63, 102179. [Google Scholar] [CrossRef] [PubMed]
- Rimini, M.; Rimassa, L.; Ueshima, K.; Burgio, V.; Shigeo, S.; Tada, T.; Suda, G.; Yoo, C.; Cheon, J.; Pinato, D.J.; et al. Atezolizumab plus Bevacizumab versus Lenvatinib or Sorafenib in Non-Viral Unresectable Hepatocellular Carcinoma: An International Propensity Score Matching Analysis. ESMO Open 2022, 7, 100591. [Google Scholar] [CrossRef]
- Kuo, Y.-H.; Lu, S.-N.; Chen, Y.-Y.; Kee, K.-M.; Yen, Y.-H.; Hung, C.-H.; Hu, T.-H.; Chen, C.-H.; Wang, J.-H. Real-World Lenvatinib Versus Sorafenib in Patients With Advanced Hepatocellular Carcinoma: A Propensity Score Matching Analysis. Front Oncol 2021, 11, 737767. [Google Scholar] [CrossRef] [PubMed]
- Pomej, K.; Balcar, L.; Shmanko, K.; Welland, S.; Himmelsbach, V.; Scheiner, B.; Mahyera, A.; Mozayani, B.; Trauner, M.; Finkelmeier, F.; et al. Clinical Characteristics and Outcome of Patients with Combined Hepatocellular-Cholangiocarcinoma—a European Multicenter Cohort. ESMO Open 2023, 8, 100783. [Google Scholar] [CrossRef]
- Rodrigues, S.G.; Mendoza, Y.P.; Bosch, J. Beta-Blockers in Cirrhosis: Evidence-Based Indications and Limitations. JHEP Rep 2020, 2, 100063. [Google Scholar] [CrossRef]
- McDowell, H.R.; Chuah, C.S.; Tripathi, D.; Stanley, A.J.; Forrest, E.H.; Hayes, P.C. Carvedilol Is Associated with Improved Survival in Patients with Cirrhosis: A Long-term Follow-up Study. Aliment Pharmacol Ther 2021, 53, 531–539. [Google Scholar] [CrossRef]
- Yang, T.-C.; Chen, W.-C.; Hou, M.-C.; Chen, P.-H.; Lee, P.-C.; Chang, C.-Y.; Lu, H.-S.; Chen, Y.-J.; Hsu, S.-J.; Huang, H.-C.; et al. Endoscopic Variceal Ligation versus Propranolol for the Primary Prevention of Oesophageal Variceal Bleeding in Patients with Hepatocellular Carcinoma: An Open-Label, Two-Centre, Randomised Controlled Trial. Gut, 2023; gutjnl-2023-330419. [Google Scholar] [CrossRef]
- Stafylidou, M.; Paschos, P.; Katsoula, A.; Malandris, K.; Ioakim, K.; Bekiari, E.; Haidich, A.-B.; Akriviadis, E.; Tsapas, A. Performance of Baveno VI and Expanded Baveno VI Criteria for Excluding High-Risk Varices in Patients With Chronic Liver Diseases: A Systematic Review and Meta-Analysis. Clinical Gastroenterology and Hepatology 2019, 17, 1744–1755.e11. [Google Scholar] [CrossRef]
- Wu, C.W.-K.; Lui, R.N.-S.; Wong, V.W.-S.; Yam, T.-F.; Yip, T.C.-F.; Liu, K.; Lai, J.C.-T.; Tse, Y.-K.; Mok, T.S.-K.; Chan, H.L.-Y.; et al. Baveno VII Criteria Is an Accurate Risk Stratification Tool to Predict High-Risk Varices Requiring Intervention and Hepatic Events in Patients with Advanced Hepatocellular Carcinoma. Cancers (Basel) 2023, 15, 2480. [Google Scholar] [CrossRef]
- Allaire, M.; Campion, B.; Demory, A.; Larrey, E.; Wagner, M.; Rudler, M.; Roux, C.; Blaise, L.; Carrie, N.G.; Thabut, D. Baveno VI and VII Criteria Are Not Suitable for Screening for Large Varices or Clinically Significant Portal Hypertension in Patients with Hepatocellular Carcinoma. Aliment Pharmacol Ther 2023, 58, 346–356. [Google Scholar] [CrossRef] [PubMed]
- de Franchis, R.; Bosch, J.; Garcia-Tsao, G.; Reiberger, T.; Ripoll, C.; Abraldes, J.G.; Albillos, A.; Baiges, A.; Bajaj, J.; Bañares, R.; et al. Baveno VII – Renewing Consensus in Portal Hypertension. Journal of Hepatology 2022, 76, 959–974. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions, and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions, or products referred to in the content. |
Figure 1.
Overall Survival in Patients Treated with Atezolizumab with Bevacizumab for (A) the entire study population and (B) different lines of treatment.
Figure 1.
Overall Survival in Patients Treated with Atezolizumab with Bevacizumab for (A) the entire study population and (B) different lines of treatment.
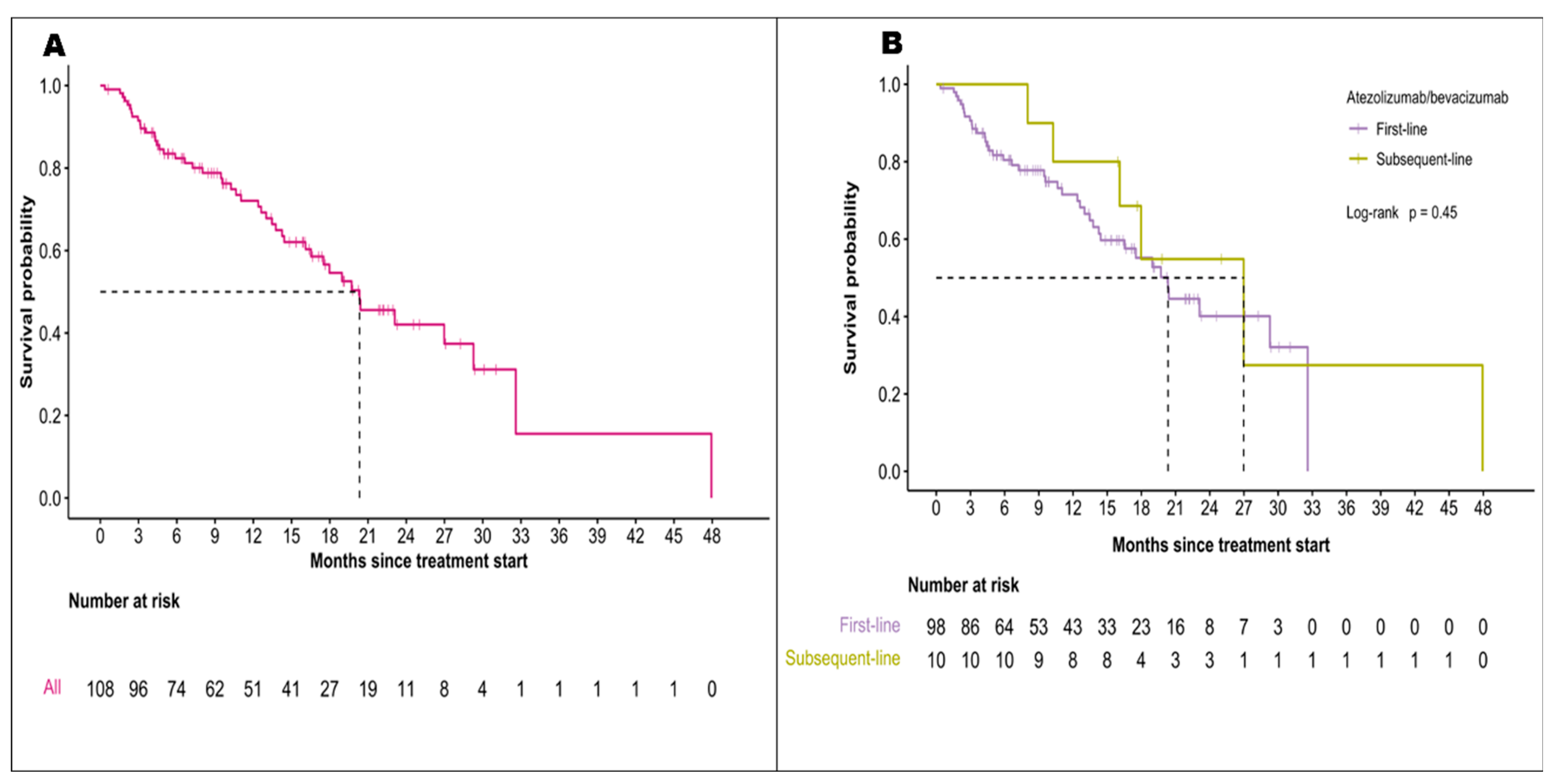
Figure 2.
Progression-free survival in Patients Treated with Atezolizumab with Bevacizumab for (A) the entire study population and (B) different lines of treatment.
Figure 2.
Progression-free survival in Patients Treated with Atezolizumab with Bevacizumab for (A) the entire study population and (B) different lines of treatment.
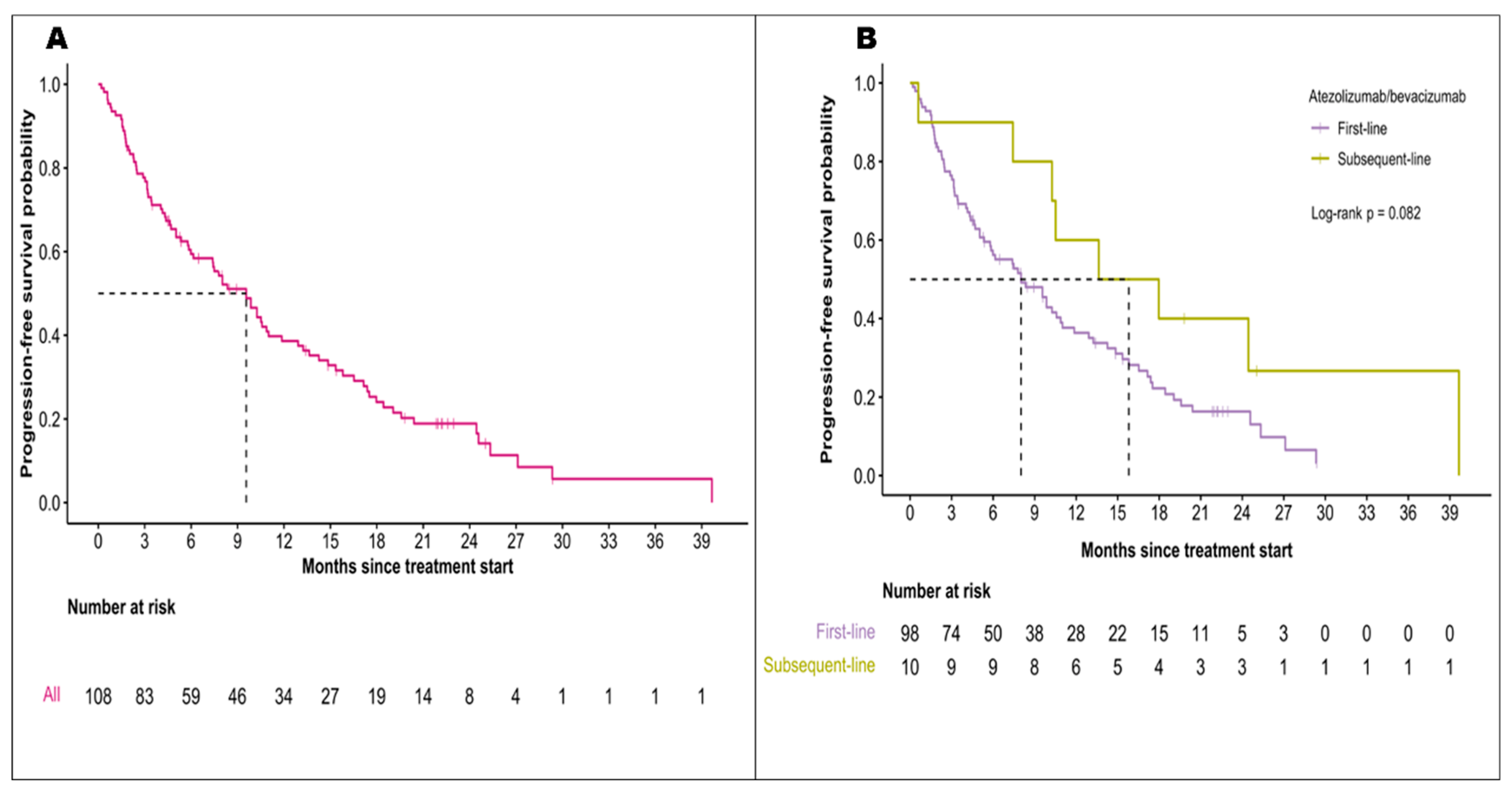

Table 1.
Patient Characteristics.
| Characteristic | Total (n=112) |
|---|---|
| Median Age (IQR), years | 66 (24-85) |
| Sex | |
| Male Female |
97 (87%) 15 (13%) |
| Ethnicity | |
| East-Asian | 27 (24%) |
| Other | 85 (76%) |
| Province | |
| Alberta | 60 (54%) |
| Ontario | 48 (43%) |
| Manitoba | 3 (3%) |
| Unknown | 1 |
| ECOG performance score | |
| 0 | 53 (47%) |
| 1 | 54 (48%) |
| 2 | 4 (4%) |
| 3 | 1 (1%) |
| Child-Pugh score | |
| A | 99 (91%) |
| B | 10 (9%) |
| Unknown | 3 |
| Albumin-bilirubin (ALBI) grade | |
| 1 | 50 (45%) |
| 2 | 60 (54%) |
| 3 | 1 (1%) |
| Unknown | 1 |
| Barcelona Clinic Liver Cancer (BCLC) stage | |
| A | 7 (6%) |
| B C |
26 (23%) 79 (71%) |
| Liver disease etiology | |
| Hepatitis C Hepatitis B Alcohol use |
37 (35%) 28 (26%) 25 (23%) |
| NASH Other |
17 (16%) 5 |
| Cirrhosis | |
| Yes | 75 (67%) |
| No | 37 (33%) |
| Liver resection | 29 (28%) |
| Prior locoregional therapy | |
| Yes | 57(72%) |
| No Unknown |
22 (28%) 33 |
| Type of locoregional therapy | |
| Radiofrequency Ablation (RFA) | 33 (29%) |
| Stereotactic Body Radiation Therapy (SBRT) | 17 (15%) |
| y-90 Radioembolization | 6 (5.4%) |
| Transarterial embolization (TAE) | 4 (3.6%) |
| Transarterial chemoembolization (TACE) | 29 (26%) |
| 1 | 11 (38%) |
| 2 | 14 (48%) |
| 3 | 4 (14%) |
| Tumor histology | |
| HCC | 73 (65%) |
| Mixed HCC-CCA | 3 (3%) |
| No biopsy/Unknown | 36 (32%) |
| Size of largest lesion, cm | |
| Median (IQR) Unknown |
3.8 (0.0-18.0) 16 |
| Tumor distribution | |
| Unilobar | 55 (50%) |
| Bilobar Unknown |
55 (50%) 2 |
| Macrovascular invasion | |
| Yes | 41 (37%) |
| No | 70 (63%) |
| Unknown | 1 |
| Presence of lymph node or extrahepatic metastasis | |
| Lymph node involvement Extrahepatic metastasis |
31 (28%) 41 (37%) |
| Completed EGD within 6 months | |
| Yes No |
79 (71%) 33 (29%) |
| Reasons for no EGD No radiological evidence of cirrhosis or varices Limited EGD availability Patient refusal (with EGD within 7 months) Unknown Varices |
4 (12%) 2 (6%) 1(3%) 26 (79%) |
| Detected on EGD | 32 (41%) |
| Required intervention before A+B No previous EGD/Unknown |
15 (19%) 34 |
| Baseline AFP level, µg/L | |
| Median (IQR) | 47.0 (1.0-86,709) |
| Unknown | 2 |
| Baseline platelet count, x109/L | |
| Median (IQR) Unknown |
177.0 (49.0- 574.0) 1 |
| Reasons for A+B discontinuation | |
| Disease progression Patient choice Toxicities Death |
30 (37%) 21 (26%) 15 (18.5%) 15 (18.5%) |
IQR: interquartile range; NASH: Non-alcoholic steatohepatitis; HCC: hepatocellular carcinoma; CCA: cholangiocarcinoma; EGD: Esophagogastroduodenoscopy; AFP: Alpha-fetoprotein.
Table 2.
Lines of Systemic Treatments.
| Characteristic | Total (n = 112) |
|---|---|
| First-line regimen (n=112) | |
| A+B | 101(90%) |
| Lenvatinib | 6 (5%) |
| Sorafenib | 4 (4%) |
| Chemotherapy | 1 (1%) |
|
Second-line regime (n=39) Lenvatinib |
25 (64%) |
| A+B | 10 (26%) |
| Sorafenib | 2 (5%) |
| Chemotherapy | 2 (5%) |
|
Third-line regime (n=7) Regorafenib |
2 (29%) |
| Lenvatinib | 2 (29%) |
| A+B | 1 (14%) |
| Cabozantinib | 1 (14%) |
| Sorafenib | 1 (14%) |
| A+B prior to TKIs | 101 (90%) |
| TKIs prior to A+B | 11 (10%) |
A+ B: Atezolizumab with bevacizumab; TKIs: tyrosine kinase inhibitors.
Table 3.
Comparison of Real-world Effectiveness of Atezolizumab with Bevacizumab Between Our Study and the IMbrave150 Trial. Our study utilized physician-assessed progression while the IMbrave150 trial employed RECIST 1.1 criteria.
Table 3.
Comparison of Real-world Effectiveness of Atezolizumab with Bevacizumab Between Our Study and the IMbrave150 Trial. Our study utilized physician-assessed progression while the IMbrave150 trial employed RECIST 1.1 criteria.
|
Characteristics |
This study (n=112) |
IMbrave150 [11] (n=336) |
||
| Median follow-up period (95% CI), months | 10.4 (0.4-47.9) | 17.6 (0.1-28.6) | ||
| Median treatment duration | 6.4 (0.2-29.8) | 8.4 (3.5-18.3) | ||
| Median OS (95% CI), months 18-month OS Median OS (patients with bleeding vs without bleeding) |
20.3 (16.5-NR) 55% 20.3 (13.0-NR) vs 19.7 (16.5-NR) p=0.86 |
19.2 (17.0-23.7) 52% |
||
| Median PFS* (95% CI), months Median PFS (patients with bleeding vs without bleeding) |
9.6 (6.1-11.9) 10.3 (5.0-27.1) vs 9.6 (7.4-13.6) p=0.95 |
6.9 (5.7-8.6) | ||
| ORR* | Overall (n=112) |
First-line (n=101) |
Subsequent-line (n=11) |
Overall (n=336) |
| Complete response no. (%) Partial response no. (%) Stable disease no. (%) Progressive disease no. (%) Could not be evaluated/Missing no. |
1(1%) 36 (35.0%) 42 (40.8%) 24 (23.3%) 9 |
0 (0%) 33 (35.1%) 39 (41.5%) 22 (23.4%) 7 |
1 (11.1%) 3 (33.3%) 3 (33.3%) 2 (22.2%) 2 |
25 (8%) 72 (22%) 144 (44%) 63(19%) 22 (7%) |
OS: overall survival, PFS: progression-free survival; NR: not reached; ORR: objective response rate.*PFS and ORR data are based on physician-reported assessment of response and progression.
Table 4.
Comparison of Baseline Clinical Characteristics and Bleeding Rates in Patients With and Without Pre-treatment Esophagogastroduodenoscopy (EGD).
Table 4.
Comparison of Baseline Clinical Characteristics and Bleeding Rates in Patients With and Without Pre-treatment Esophagogastroduodenoscopy (EGD).
| EGD within 6 months | ||||
|---|---|---|---|---|
| Characteristic | Total (n = 112) | Yes (n= 79) | No (n= 33) | p-value |
| Cirrhosis | 75 | 51(68%) | 24(32%) | 0.45 |
| Platelet count, x109/L | ||||
| Median (IQR) | 177 (49-574) | 162 (65-574) | 189 (49-486) | 0.17 |
| Albumin, g/L | ||||
| Median (IQR) | 39.0 (24-421) | 39 (26-421) | 39 (24-48) | 0.70 |
| INR | ||||
| Median (IQR) | 1.1 (0.9-1.8) | 1.1(0.9-1.4) | 1.1 (0.9-1.8) | 0.86 |
| Total Bilirubin, µmol/L | ||||
| Median (IQR) | 15 (3-72) | 15 (3-72) | 16 (3-57) | 0.56 |
| Size of largest tumor, cm | ||||
| Mean ± SD | 96 | 6.0 ± 4.3 | 5.7 ± 4.8 | 0.56 |
| Unknown | 16 | |||
| Macrovascular invasion | 41 | 6 (15%) | 35 (85%) | 0.88 |
| Unknown | 1 | |||
| Bleeding events | 17 | 14 (82%) | 3 (18%) | 0.24 |
| GI-specific bleeding | 6 | 5 (83%) | 1 (17%) | |
IQR: interquartile range; SD: standard deviation.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



