Submitted:
01 July 2024
Posted:
01 July 2024
You are already at the latest version
Abstract
Ambiguity exists over treatment and surveillance strategies after endoscopic submucosal dissec-tion (ESD) for esophageal squamous cell neoplasia (ESCN) with unfavorable histologic features. This study investigated the long-term outcomes of ESD in high-risk ESCN patients. We retro-spectively included early ESCN patients treated with ESD at two medical centers in Taiwan be-tween August 2010 and December 2023. Demographic, endoscopic, and pathological data were collected. Among 146 patients (mean age 59.17 years) with 183 lesions, 73 (50%) had a history of head and neck cancer (HNC). En bloc and R0 resection were achieved in 100% and 95.6% of the lesions, respectively. The 5-year overall survival (OS), disease-specific survival (DSS) and local recurrence rates were 42.7%, 94.7% and 11%. R0 resection was significantly associated with re-currence in univariate analysis (adjusted OR: 0.23, 95% CI: 0.05-0.99, P=0.05). Alcohol abstinence was independently associated with lower recurrence (adjusted OR: 0.20, 95% CI: 0.08-0.48, P
Keywords:
Esophageal squamous cell carcinoma
; Endoscopic submucosal dissection
; Second primary tumor
; Head and neck cancer
; Expanded indication
1. Introduction
Although the overall prognosis of esophageal squamous cell carcinoma (ESCC) is poor, with 5-year overall survival (OS) rates ranging from 15% to 25% [1], early esophageal squamous cell neoplasia (ESCN) is considered a curable disease [2,3]. The reported 5-year OS rate for patients diagnosed with early ESCC is approximately 80% following esophagectomy [4]. Endoscopic submucosal dissection (ESD) is an advanced endoscopic technique that was introduced to manage early gastrointestinal tract neoplasia in the 1990s. For selected patients with early ESCN, ESD has emerged as an alternative minimally invasive treatment option, with comparable outcomes to surgical esophagectomy [5]. A real-world cohort study with a 21-month follow-up of patients with early ESCN found no statistically significant differences in all-cause mortality (7.4% vs 10.9%; P=0.209) and rate of cancer recurrence or metastasis (9.1% vs 8.9%; P=0.948) between ESD and esophagectomy [6]. Moreover, the authors reported a lower risk of non-fatal severe adverse events in the patients who underwent ESD (15.2% vs 27.7%; P=0.001) [6].
Favorable long-term outcomes have been reported in early ESCN patients undergoing ESD, particularly when the invasion is limited to the epithelium/lamina propria/muscularis mucosa (pT1a-EP/LPM/MM) or involves the superficial submucosa limited to 200 μm (pT1b-SM1), with 5-year OS rates of 90.5% to 95.1% for pT1a–EP/LPM, 71.1% to 84.2% for pT1a-MM, and 70.8% for pT1b-SM1, respectively [7,8,9,10,11,12]. However, these data were mostly obtained from Japanese cohorts, with only a few from Western countries. Furthermore, many of these studies excluded individuals with a history of synchronous second primary cancer [7,8,9].
In Taiwan, the rate of synchronous second primary ESCN has been reported to range from 15.2~23.3% in head and neck cancer (HNC) patients [13,14], and worse OS has been demonstrated in HNC patients with synchronous ESCN compared to those without [15]. According to recent studies, endoscopic screening for second primary esophageal cancer in patients with oral cavity and hypopharyngeal cancer can significantly enhance early detection and decrease all-cause mortality [16,17]. Nevertheless, long-term outcome data for ESD in patients with second primary esophageal neoplasia and HNC are still insufficient [12]. Therefore, this study aimed to examine the long-term outcomes of ESD for second primary ESCN among high-risk patients, particularly focusing on expanded indications.
2. Materials and Methods
2.1. Study Design and Patient Enrollment
This retrospective cohort study enrolled patients with early ESCN treated with ESD between August 2010 and December 2023 at two medical centers in Taiwan. All patients met the inclusion criteria, which were: (1) histologically confirmed low-grade intraepithelial neoplasia, high-grade intraepithelial neoplasia (HGIN) of the esophagus, or early ESCC including pT1a–EP/LPM, pT1a-MM and pT1b-sm1/sm2; (2) absence of lymph node or distant metastases on radiological investigations; and (3) no history of prior chemo- or radiation therapy for ESCC. Long-term outcome data were collected from medical records, and any missing information was obtained through telephone conversations with the patients or their family. Alcohol abstinence is defined as having abstained from alcohol for at least one year after ESD and continuing to abstain until the last follow-up date. This study was approved by the Institutional Review Board of Far Eastern Memorial Hospital (FEMH-106090-E), and the requirement for written informed consent was waived because of the absence of identifiable information in the data analyzed.
2.2. ESD Procedure and Surveillance Methods
All enrolled patients underwent magnifying endoscopy with narrow-band imaging (ME-NBI) and optional chromoendoscopy using 2% Lugol’s solution to evaluate the intraepithelial papillary capillary loops and Lugol-voiding areas [18,19]. Overnight fasting and prophylactic antibiotics were given, and the patients were placed in the supine or left decubitus position under intravenous sedation or general anesthesia. ESD with mucosal marking and incision, followed by submucosal dissection and specimen retrieval was performed using dedicated endoknives and accessories. The resected specimens were sliced into 2 mm sections and fixed in formalin using standard methods following the Japan Esophageal Society recommendations, and all specimens were reviewed by experienced pathologists [20]. The pathological invasion depth, lymphovascular and perineural invasion, histological subtype and differentiation degree, vertical and lateral margins were evaluated.
The first follow-up endoscopy in all cases was performed at 3 to 6 months after ESD. Subsequent endoscopic surveillance was repeated every 6 months. Computed tomography (CT) was performed for follow-up in all patients with components of invasive carcinoma in resected specimens.
2.3. Definition of Outcomes
OS, disease-free survival (DFS) and disease-specific survival (DSS) were compared among patients with different invasion depths and those with or without HNC. OS was defined as the time from ESD to decease from any cause. DFS was defined as the time from ESD to esophageal cancer recurrence or death from any cause. DSS was defined as the duration from ESD to death specifically attributed to the ESCN. Complete local remission (CLR) was defined as R0 resection plus normal first follow-up endoscopy.
Local recurrence and metastatic recurrence were evaluated by endoscopy, CT and/or positron emission tomography. Local recurrence was defined as the development of ESCN at the ESD site of the primary lesion, while metastatic recurrence was defined as a relapse involving other organs or lymph nodes. Metachronous recurrence was defined as the development of an ESCN at a location different from the primary lesion site over 6 months after the index ESD. Furthermore, we also investigated potential correlations between the occurrence of any recurrence and baseline characteristics of the patients as well as lesions.
In terms of adverse events from ESD procedures, esophageal stricture was defined as narrowing of the lumen that a standard adult gastroscope could not pass or required endoscopic dilation. Post-ESD bleeding was defined as bleeding occurring after the ESD, characterized by a decrease in hemoglobin level > 2 g/dL, presence of hematemesis or melena or confirmation of bleeding through endoscopic, radiological, or surgical evidence. Esophageal perforation was defined as the presence of a visible defect in the esophageal wall exposing the mediastinal cavity.
2.4. Statistical Analysis
Basic characteristics of the patients were evaluated by descriptive statistics. Discrete data are presented as numbers and percentages, and continuous variables are expressed as mean values ( ± standard deviation; SD). The chi-square test was used to evaluate categorical variables. Two-tailed P-values of < 0.05 were used to determine statistical significance. Univariate and multivariate logistic regression analyses were used to identify risk factors associated with outcomes. Variables from univariate analysis with P values < 0.10 were included in the multivariate model. Survival analysis was done using the Kaplan-Meier method along with a log-rank test to assess the statistical significance of differences in survival curves among different groups. All statistical analyses were performed with SPSS for Windows, version 26.0 (IBM Corp., Armonk, NY, USA). The study results were reviewed by expert biostatistician Dr. Hsiu-Jung Liao.
3. Results
3.1. Patients, Endoscopic and Pathologic Characteristics
A total of 183 lesions in 146 patients were enrolled. Table 1 summarizes the demographic characteristics of the study population. The mean (±SD) patient age was 59.17 (±9.45) years, and 89% (130/146) of the patients were male. The study included 132 (90.4%) patients who were alcohol drinkers, 68.9% of whom abstained from alcohol prior to enrollment. A total of 73 (50%) patients had a history of HNC. Table A1 details the location and stage of HNC in this study. The endoscopic and pathological characteristics are also summarized in Table 1. Among the lesions, 43 (23.5%) extended to more than three-fourths of the circumference. The pathologic stage was low-grade intraepithelial neoplasia in 16 (8.7%) lesions, HGIN/T1am1 in 90 (49.1%), T1am2 in 10 (5.5%), T1am3 in 42 (23%), T1bsm1 in 10 (5.5%), and T1bsm2 in 15 (8.2 %) lesions. The frequencies of lymphovascular invasion (LVI) and perineural invasion were 14/183 (7.6%) and 3/183 (1.6%), respectively.
3.2. Short-Term Outcomes and ESD-Related Complications
The short-term outcomes and complications are shown in Table 2. En bloc, R0 resection and CLR were achieved in 183 (100%), 175 (95.6%) and 161 (88%) of the 183 lesions, respectively. Post-ESD stricture developed in 18 (9.8%) of the 146 patients, with no cases developing bleeding or perforation, and no cases of procedure-related mortality.
3.3. Long-Term Outcomes
The long-term outcomes are presented in Table 2. The mean (±SD) follow-up time was 37.05 months (±26.79), and the 5-year OS and DSS rates were 42.7% and 94.7%, respectively. Over the 10-year follow-up period, the cumulative recurrence rate was 20.5%. Specifically, the 5-year local recurrence rate was 11%, and metachronous recurrence occurred in 14 cases (9.5%). The 5-year cumulative incidence of metastatic recurrence was 2.8% in the pT1a-EP/LPM group and 7.8% in the pT1a-MM group.
Figure 1a and 1b show that pathologic stage had statistically significant impacts on OS (P=0.022) and DSS (P=0.007). In the HGIN/pT1a–EP/LPM group, the 3-year and 5-year OS rates were 67.5% and 50%, respectively, compared to 68.8% and 52% in the pT1a-MM group (P=0.82, Figure 2a). Kaplan Meier curve showed no statistically significant difference in OS when comparing the HGIN/pT1a–EP/LPM group with the pT1a-MM group without LVI (P=0.793, Figure 2b). The 5-year DSS rates were 96.7% and 100% in the HGIN/pT1a–EP/LPM and pT1a-MM groups, respectively (P=0.617, Figure 2c). In the patients with pT1a-MM, the presence of LVI did not affect OS (P=0.96, Figure 2d). The causes of death in our study population are detailed in Table A2.
Table A3 provides the analysis of the impact of HNC on OS, DSS, and DFS. The patients with HNC had a lower 5-year OS rate than those without HNC (adjusted odds ratio [aOR]: 0.31, 95% confidence interval [CI]: 0.12-0.82, P=0.018). In addition, a higher DFS was also found in the patients without HNC in Kaplan-Meier curve (P=0.013, Figure A1). No significant difference was observed in the recurrence rate among different locations of HNC (P=0.915, Figure A2-A4).
The descriptive data of the patients who underwent additional therapy are shown in Table A4. Following ESD, a total of 19 patients received additional therapy, with 13 patients (68.4%) undergoing concurrent chemoradiotherapy. The primary reason for additional therapy was failure to achieve R0 resection (8 patients, 42.1%), followed by deep submucosal invasion (5 patients, 26.3%).
3.4. Predictors Associated with Recurrence
The results of univariate and multivariate analyses for the factors associated with recurrence after ESD are demonstrated in Table 3. The patients who achieved R0 resection and CLR, and those who abstained from alcohol consumption had a lower rate of recurrence. Multivariate analysis showed that alcohol abstinence was the only independent factor associated with a decreased recurrence rate (aOR: 0.20, 95% CI: 0.08-0.48, P<0.001). Kaplan-Meier curve demonstrated no statistically significant difference in recurrence between the patients with HGIN/pT1a–EP/LPM and those with pT1a-MM (p=0.63) (Figure 3a and 3b).
4. Discussion
In this study, we investigated the long-term outcomes of patients with early ESCN after ESD with expanded indications, and observed favorable 5-year DSS (94.7%), en bloc resection (100%) and R0 resection (95.6%) rates following ESD for early ESCN in high-risk HNC patients. Regarding survival and disease recurrence, we found no significant difference between the patients with pT1a–MM and those with pT1a–EP/LPM. Our results suggest that ESD without additional therapy may be a reasonable treatment option for patients with ESCN involving pT1a-MM.
In contrast to the significant perioperative mortality rate associated with esophagectomy (previously reported as ranging from 1.5% to 12.5%),[6,21,22] ESD, as a minimally invasive procedure, has been associated with fewer perioperative comorbidities in selected patients with early ESCN [7,8,9,10]. Moreover, a previous study found that patients who underwent ESD had a lower risk of non-fatal severe adverse events compared to those who underwent esophagectomy for early ESCN (15.2% vs 27.7%; P=0.001) [6]. In the present study, ESD was not associated with any cases of perioperative mortality, and the post-ESD stricture rate was only 9.8%, which is consistent with the rates of 6% to 18.1% reported in large cohort studies with adequate stricture prevention [7,8,10,12,23]. Other advantages of ESD include the high en bloc and R0 resection rates, which have been reported to reach 95% to 100% and 84.5% to 99.3%, respectively, in Asian studies [23,24,25,26]. In comparison, reports from Western countries indicate varying R0 resection rates for ESD in early ESCN, ranging from 69.6% to 96.7% [11,27,28]. A previous prospective study reported a higher en bloc resection rate with ESD compared with endoscopic mucosal resection for early ESCN (100% vs 53.3%; P=0.009) [29]. In our study, we achieved favorable en bloc and R0 resection rates of 100% and 95.6%, respectively, consistent with previous research. In addition, the CLR rate in our study was 88%. Only a few studies have reported the CLR rate, including one study with a rate of 95.7% for ESD in cases with early ESCN [30], and another with a rate of 96.6% for Barrett's esophagus [31].
Regarding disease recurrence, a real-world cohort study comparing ESD with esophagectomy in selected patients with pT1a-LPM/MM and pT1b-SM (invading the submucosa layer) found no statistically significant difference in cancer recurrence or metastasis during the 21-month follow-up period (9.1% vs 8.9%; P=0.948) [6]. This suggests favorable long-term outcomes of ESD in selected early ESCN patients. In the present study, the only independent factor associated with disease recurrence was alcohol abstinence, aligning with findings from a previous prospective cohort study [32]. In multivariate analysis, neither R0 resection nor CLR was associated with a higher recurrence rate. This may be because all the patients who did not achieve R0 resection after ESD received additional therapy. Our 5-year local recurrence rate of 11% is in line with the range of 3.9% to 16.8% reported in patients without HNC in large Japanese cohort studies [7,8,9]. Furthermore, the high metachronous recurrence rate of 17.9% after ESD in HNC patients reported in previous research was not observed in our study [12]. This finding may be associated with our high R0 resection rate and the significant prevalence of alcohol abstinence after education, notably among the patients with HNC.
Previous studies have reported cumulative 5-year metastatic recurrence rates for patients diagnosed with pT1a-EP/LPM and pT1a-MM ranging between 0%- 0.5% and 3.3%- 8.7%,[7,9,10] respectively, which is consistent with our results. Due to an elevated rate of lymph node metastasis, the Japan Esophageal Society guidelines in 2017 recommended additional treatment after ESD for pT1a-MM ESCC patients [3]. However, an increasing number of studies suggests a positive prognosis in pT1a-MM patients after ESD even without additional therapy [10,33]. A recent study conducted in Japan found that ESD for pT1a-MM patients without LVI exhibited comparable DSS to pT1a-EP/LPM patients (99.3% vs 96.6%, P=0.118), with no significant differences in the cumulative incidence of metastatic and local recurrence (P=0.121 and P=0.455, respectively) [10]. Our data support these results, in that we observed no significant differences in OS, DSS or recurrence after ESD between the patients with pT1a-MM without additional therapy and those with pT1a-EP/LPM without additional therapy (Figure 2a-2d and Figure 3b). Even when considering the presence or absence of LVI, no statistically significant differences were observed between the two groups (Figure 2b and 2c). Our findings suggest that expanding the indications for ESD without additional therapy to include pT1a-MM patients without LVI seems reasonable, and consistent with previous research [10]. Further research is required to confirm the clinical outcomes of pT1a-MM patients after ESD, and appropriate follow-up strategies need to be established.
The favorable outcomes of ESD for second primary early ESCN in the high-risk HNC patients in this study are also noteworthy. Even though the 5-year OS rate in our patients was only 48%, which is lower than the 95.1% to 99% reported in Japanese cohorts,[8,9] the 5-year DSS reached 94.7%, which is not far from the 99.1% to 100% reported previously [8,9]. The lower OS in our cohort may be due to the significant proportion of patients with HNC (50%), among whom 53.4% were at stage IV (Table A1), with 50% of deaths related to HNC (Table A2). Similar findings were reported in a retrospective study involving 167 patients, 61.7% of whom were diagnosed with HNC [12]. The 10-year disease-related survival rate was more than 90%, whereas the OS rate was less than 70% [12]. We previously reported that screening and surveillance of ESCN by ME-NBI can provide opportunities for early treatment and even improve the survival of hypopharyngeal cancer patients [17]. Given the positive short-term and long-term outcomes observed in this study, we believe that ESD with expanded indications for second primary ESCN can provide clinical benefits with a favorable DSS rate. In addition, in our previous case-control study, tumors located in the hypopharynx and pharynx were associated with a higher risk of developing second primary ESCN in HNC patients (aOR 4.52, 95% CI: 1.46-13.99, P=0.009 and aOR 5.70, 95% CI: 1.08-29.99, P=0.04) [13]. However, the impact of HNC tumor site on recurrence after ESD for second primary early ESCN remains unclear. In the present study, although the presence of HNC was not significantly associated with recurrence (Table 3), there appeared to be a trend suggesting a higher incidence of recurrence in laryngeal and hypopharyngeal cancers compared to cancers of the oral cavity and oropharynx (Figure A2-A4). More studies are needed to determine the relationship between HNC tumor site and recurrence of second primary early ESCN after ESD.
Some limitations of this study should be noted. First, this study adopted a retrospective design, which may have introduced potential selection and measurement bias. Second, the limited number of pT1a-MM patients with concurrent LVI in this study undermines the reliability of assessing the statistical significance of LVI on clinical outcomes in the pT1a-MM subgroup. Third, the heterogeneity of the study population, including patients with HNC from various primary sites and those without HNC, may impact the generalizability of the findings.
5. Conclusions
In summary, our results showed favorable outcomes of ESD for second primary early ESCN in patients with HNC. We also found that ESD in patients with pT1a-MM yielded comparable results to those with pT1a-EP/LPM in terms of survival and disease recurrence. This highlights the potential for expanding the indications for ESD in managing pT1a-MM patients without additional therapy. Further research is necessary to validate these findings.
Author Contributions
Conceptualization, Tze-Yu Shieh and Chen-Shuan Chung; Data curation, Tzong-Hsi Lee and Chen-Shuan Chung; Formal analysis, Chen-Huan Yu and Chen-Shuan Chung; Investigation, Chen-Huan Yu, Yueh-Hung Chou and Chen-Shuan Chung; Methodology, Yueh-Hung Chou and Chen-Shuan Chung; Project administration, Chen-Shuan Chung; Resources, Chao-Yu Liu, Jiann-Ming Wu, Chen-Hsi Hsieh and Tzong-Hsi Lee; Software, Chen-Huan Yu; Supervision, Tzong-Hsi Lee; Validation, Chao-Yu Liu, Jiann-Ming Wu and Chen-Hsi Hsieh; Writing – original draft, Chen-Huan Yu and Yueh-Hung Chou; Writing – review & editing, Tze-Yu Shieh and Chen-Shuan Chung; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Far Eastern Memorial Hospital (FEMH-106090-E).
Informed Consent Statement
The requirement for written informed consent was waived because of the absence of identifiable information in data analysis.
Data Availability Statement
The data presented in this study are available on request from the
corresponding author.
Acknowledgments
We thanked Dr. Hsiu-Jung Liao for reviewing the results of statistical analysis.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix
Figure A1.
Kaplan-Meier curve of the impact of head and neck cancer on disease free survival. Significantly higher survival was observed in patients without head and neck cancer (p=0.013).
Figure A1.
Kaplan-Meier curve of the impact of head and neck cancer on disease free survival. Significantly higher survival was observed in patients without head and neck cancer (p=0.013).
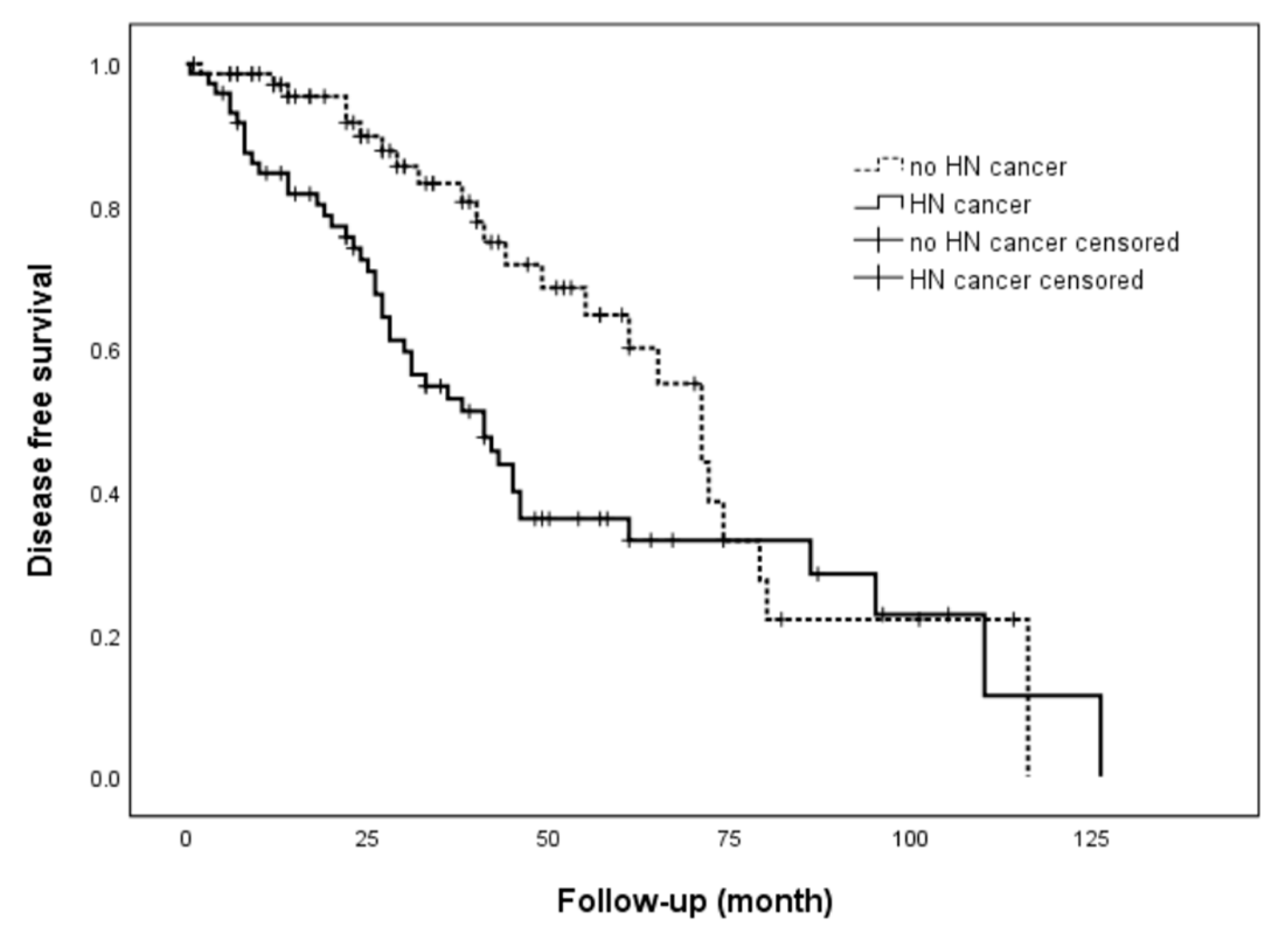
Figure A2.
Kaplan-Meier curve of the impact of head and neck cancer location on recurrence. No statistically significant was observed (p=0.915).
Figure A2.
Kaplan-Meier curve of the impact of head and neck cancer location on recurrence. No statistically significant was observed (p=0.915).
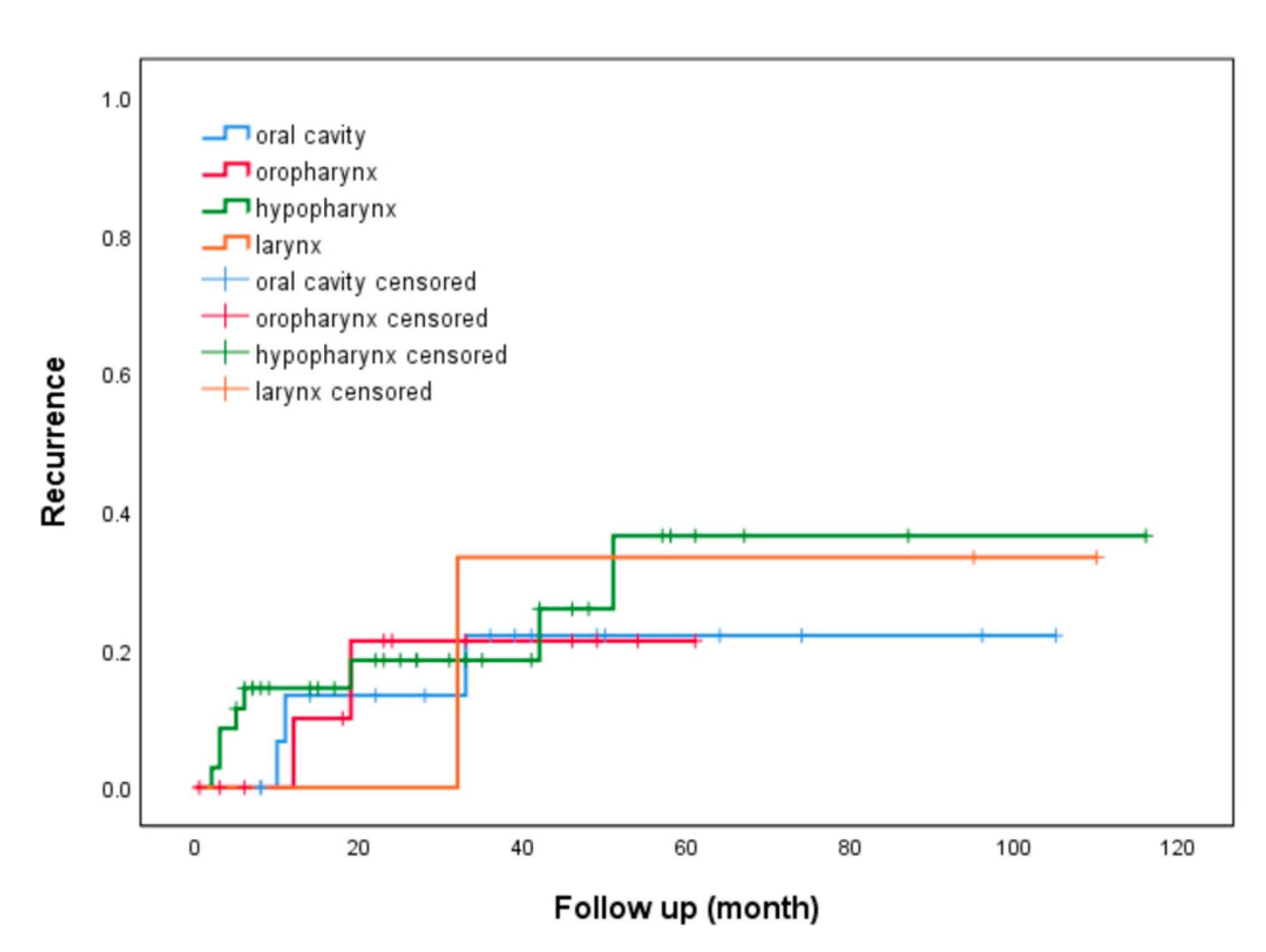
Figure A3.
Kaplan-Meier curve of recurrence in patients with oral cavity/oropharyngeal cancer and hypopharyngeal/laryngeal cancer. No statistically significant was observed (p=0.476).
Figure A3.
Kaplan-Meier curve of recurrence in patients with oral cavity/oropharyngeal cancer and hypopharyngeal/laryngeal cancer. No statistically significant was observed (p=0.476).
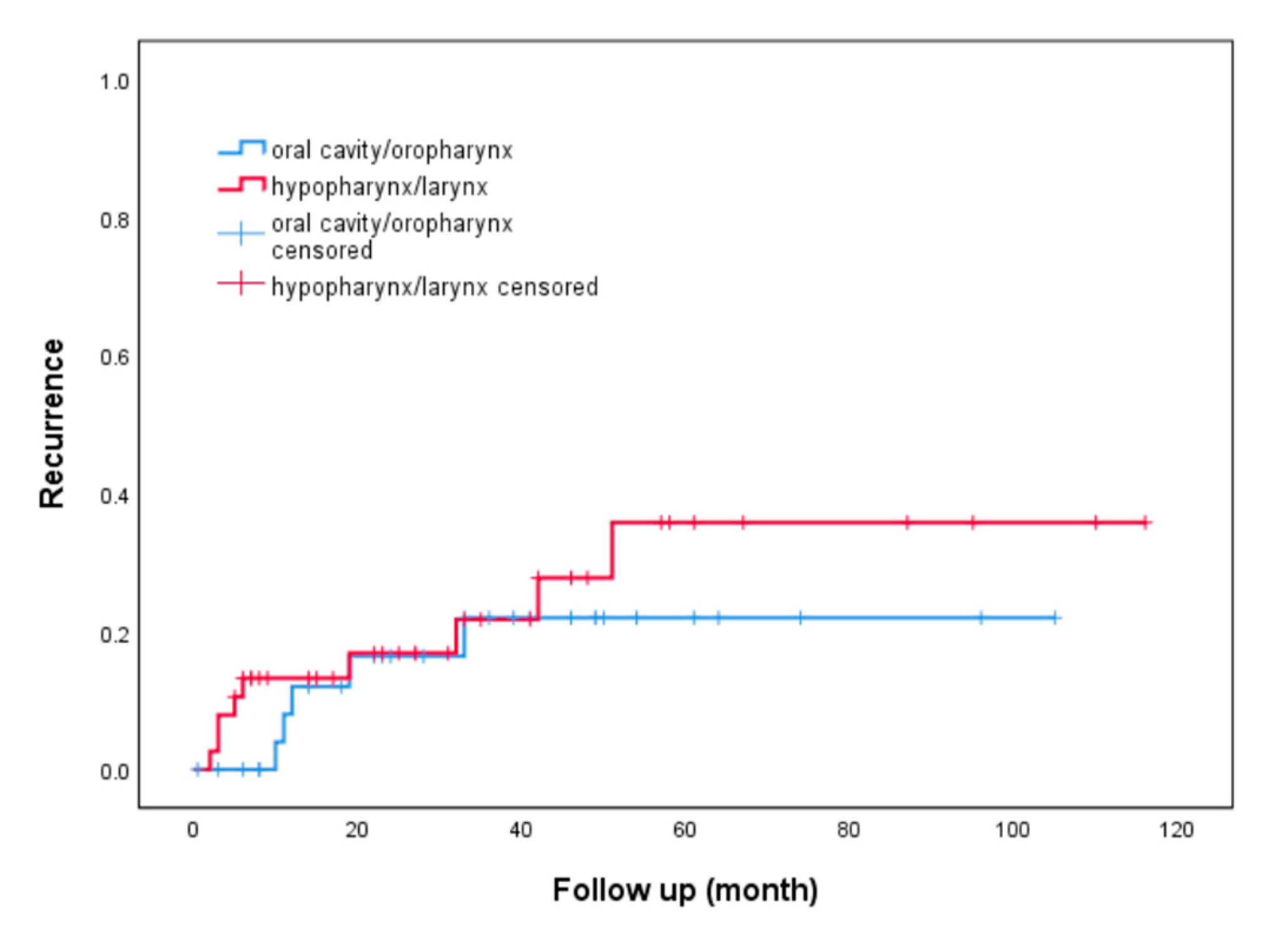
Figure A4.
Kaplan-Meier curve of recurrence in patients with oral cavity cancer and oropharyngeal/hypopharyngeal/laryngeal cancer. No statistically significant was observed (p=0.61).
Figure A4.
Kaplan-Meier curve of recurrence in patients with oral cavity cancer and oropharyngeal/hypopharyngeal/laryngeal cancer. No statistically significant was observed (p=0.61).
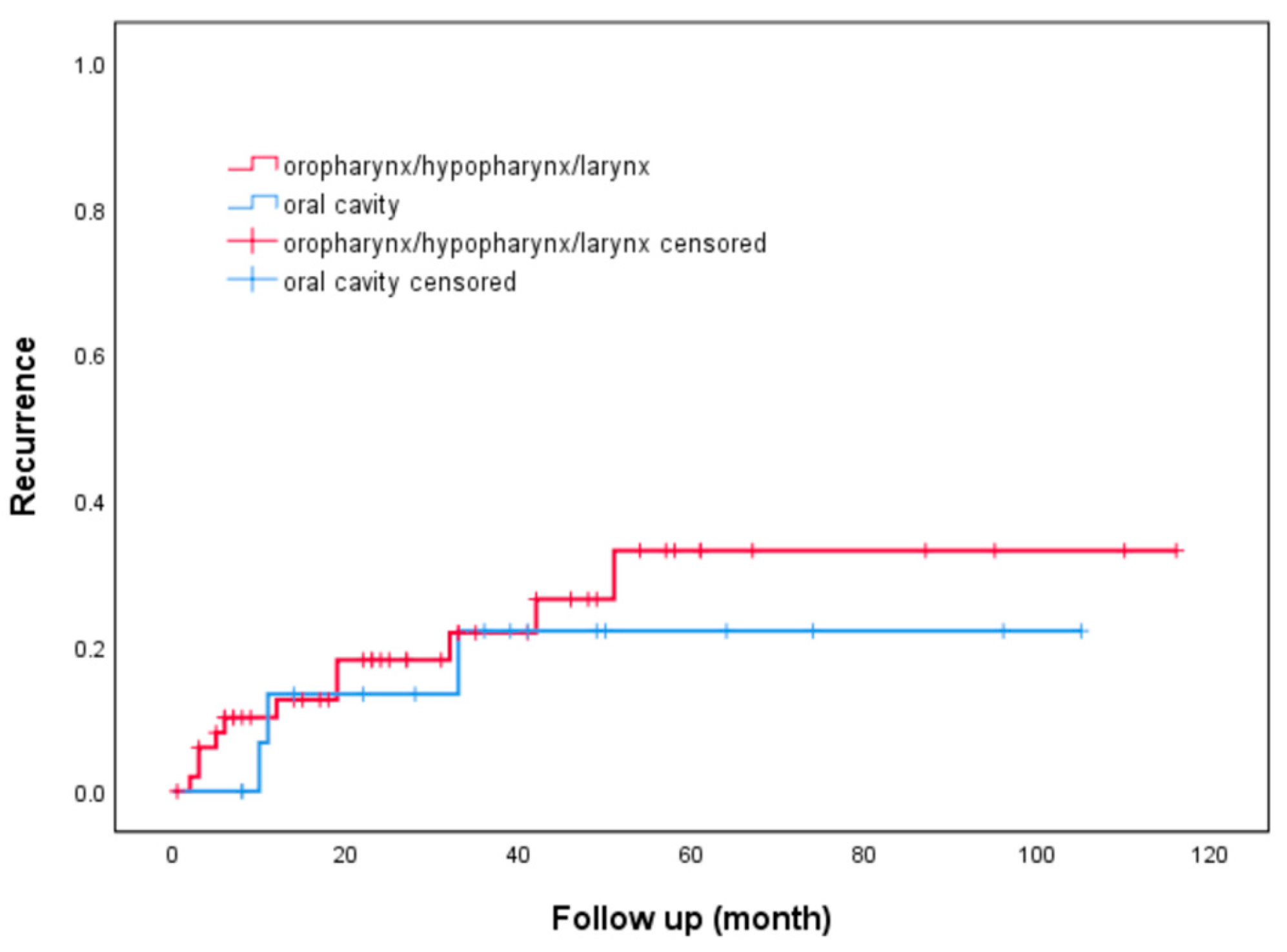

Table A1.
Location and staging of 73 head and neck cancer patients.
| Number of patients (%) | |
|---|---|
| Location of head and neck cancer Oral cavity |
|
| 18 (24.7) | |
| Oropharynx | 13 (17.8) |
| Hypopharynx | 36 (49.3) |
| Larynx | 3 (4.1) |
| Other location1 | 3 (4.1) |
| Stage of head and neck cancer | |
| I | 5 (6.8) |
| II | 8 (11.0) |
| III | 21 (28.8) |
| IV | 39 (53.4) |
1 Other location of head and neck cancer includes tracheal cancer and thyroid cancer.
Table A2.
Causes of death.
| Number of patients (%) | |
|---|---|
| Head and neck cancer Pulmonary comorbidities1 |
24 (50) |
| 8 (16.7) | |
| Other cancer2 | 4 (8.3) |
| Esophageal cancer | 3 (6.3) |
| Liver cirrhosis | 2 (4.2) |
| Complication of esophagectomy | 1 (2.1) |
| Other3 | 6 (12.5) |
1 Pulmonary comorbidities includes pneumonia with respiratory failure, chronic obstruction pulmonary disease and idiopathic pulmonary fibrosis. 2 Other cancer includes lymphoma, colon cancer and lung cancer. 3 Other causes of death includes myocardial infarction, cerebral vascular accident and complication of tracheostomy.
Table A3.
Outcomes of patients with and without HN cancer after ESD.
| Variable, Patients No. (%) | All patients (n=146) |
HN cancer (n=73) |
Without HN cancer (n=73) |
P Value (HN cancer vs without HN cancer) |
|---|---|---|---|---|
| Overall survival | ||||
| 1-year | 124 (91.9) | 60 (85.7) | 64 (98.5) | 0.007 |
| 3-year | 66 (67.3) | 30 (53.6) | 36 (85.7) | 0.001 |
| 5-year | 36 (48) | 17 (37) | 19 (65.5) | 0.018 |
| Disease-specific survival | ||||
| 1-year | 134 (99.3) | 69 (98.6) | 65 (100) | 0.33 |
| 3-year | 96 (98) | 55 (98.2) | 41 (97.6) | 0.84 |
| 5-year | 71 (94.7) | 45 (97.8) | 26 (89.7) | 0.13 |
| Disease-free survival | ||||
| 1-year | 112 (83.6) | 52 (75.4) | 60 (92.3) | 0.008 |
| 3-year | 49 (51.6) | 26 (46.4) | 23 (59) | 0.23 |
| 5-year | 24 (32.9) | 14 (31.8) | 10 (34.5) | 0.81 |
| Local recurrence | 30 (20.5) | 16 (21.9) | 14 (19.2) | 0.68 |
HN cancer: head and neck cancer; ESD: endoscopic submucosal dissection.
Table A4.
Additional therapy utilization in 19 Patients, 8 due to R1 resection.
| Number of patients (%) | |
|---|---|
| Type of additional therapy CCRT |
|
| 13 (68.4) | |
| Esophagectomy | 5 (26.3) |
| RT alone | 1 (5.3) |
| Stage | |
| HGIN | 1 (5.2) |
| T1am3 | 4 (21.1) |
| T1bsm1 | 3 (15.8) |
| T1bsm2 | 11 (57.9) |
| Reasons of additional therapy | |
| R1 resection | 8 (42.1) |
| pT1bsm2 | 5 (26.3) |
| pT1bsm1, LVI(+) | 2 (10.5) |
| pT1am3, LVI(+) | 2 (10.5) |
| pT1am3, LVI(-) | 1 (5.3) |
| Other1 | 1 (5.3) |
CCRT: concurrent chemoradiotherapy; ESD: endoscopic submucosal dissection; RFA: radiofrequency tumor ablation; RT: radiotherapy; LVI: lymphovascular invasion. 1 One patient underwent esophagectomy due to initial pathological misdiagnosis.
References
- Pennathur, A.; Gibson, M. K.; Jobe, B. A.; Luketich, J. D. , Oesophageal carcinoma. Lancet 2013, 381, 400–412. [Google Scholar] [CrossRef] [PubMed]
- Kitagawa, Y.; Uno, T.; Oyama, T.; Kato, K.; Kato, H.; Kawakubo, H.; Kawamura, O.; Kusano, M.; Kuwano, H.; Takeuchi, H.; Toh, Y.; Doki, Y.; Naomoto, Y.; Nemoto, K.; Booka, E.; Matsubara, H.; Miyazaki, T.; Muto, M.; Yanagisawa, A.; Yoshida, M. , Esophageal cancer practice guidelines 2017 edited by the Japan Esophageal Society: part 1. Esophagus 2019, 16, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Kitagawa, Y.; Uno, T.; Oyama, T.; Kato, K.; Kato, H.; Kawakubo, H.; Kawamura, O.; Kusano, M.; Kuwano, H.; Takeuchi, H.; Toh, Y.; Doki, Y.; Naomoto, Y.; Nemoto, K.; Booka, E.; Matsubara, H.; Miyazaki, T.; Muto, M.; Yanagisawa, A.; Yoshida, M. , Esophageal cancer practice guidelines 2017 edited by the Japan esophageal society: part 2. Esophagus 2019, 16, 25–43. [Google Scholar] [CrossRef] [PubMed]
- Hölscher, A. H.; Bollschweiler, E.; Schröder, W.; Metzger, R.; Gutschow, C.; Drebber, U. , Prognostic impact of upper, middle, and lower third mucosal or submucosal infiltration in early esophageal cancer. Ann Surg 2011, 254, 802–807. [Google Scholar] [CrossRef] [PubMed]
- Das, A.; Singh, V.; Fleischer, D. E.; Sharma, V. K. , A comparison of endoscopic treatment and surgery in early esophageal cancer: an analysis of surveillance epidemiology and end results data. Am J Gastroenterol 2008, 103, 1340–1345. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Ding, H.; Chen, T.; Zhang, X.; Chen, W. F.; Li, Q.; Yao, L.; Korrapati, P.; Jin, X. J.; Zhang, Y. X.; Xu, M. D.; Zhou, P. H. , Outcomes of Endoscopic Submucosal Dissection vs Esophagectomy for T1 Esophageal Squamous Cell Carcinoma in a Real-World Cohort. Clin Gastroenterol Hepatol 2019, 17, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Yamashina, T.; Ishihara, R.; Nagai, K.; Matsuura, N.; Matsui, F.; Ito, T.; Fujii, M.; Yamamoto, S.; Hanaoka, N.; Takeuchi, Y.; Higashino, K.; Uedo, N.; Iishi, H. , Long-term outcome and metastatic risk after endoscopic resection of superficial esophageal squamous cell carcinoma. Am J Gastroenterol 2013, 108, 544–551. [Google Scholar] [CrossRef] [PubMed]
- Nagami, Y.; Ominami, M.; Shiba, M.; Minamino, H.; Fukunaga, S.; Kameda, N.; Sugimori, S.; Machida, H.; Tanigawa, T.; Yamagami, H.; Watanabe, T.; Tominaga, K.; Fujiwara, Y.; Arakawa, T. , The five-year survival rate after endoscopic submucosal dissection for superficial esophageal squamous cell neoplasia. Dig Liver Dis 2017, 49, 427–433. [Google Scholar] [CrossRef]
- Oda, I.; Shimizu, Y.; Yoshio, T.; Katada, C.; Yokoyama, T.; Yano, T.; Suzuki, H.; Abiko, S.; Takemura, K.; Koike, T.; Takizawa, K.; Hirao, M.; Okada, H.; Yoshii, T.; Katagiri, A.; Yamanouchi, T.; Matsuo, Y.; Kawakubo, H.; Kobayashi, N.; Shimoda, T.; Ochiai, A.; Ishikawa, H.; Yokoyama, A.; Muto, M. , Long-term outcome of endoscopic resection for intramucosal esophageal squamous cell cancer: a secondary analysis of the Japan Esophageal Cohort study. Endoscopy 2020, 52, 967–975. [Google Scholar] [CrossRef] [PubMed]
- Iwai, N.; Dohi, O.; Yamada, S.; Ishida, T.; Fukui, A.; Horie, R.; Yasuda, T.; Yamada, N.; Horii, Y.; Majima, A.; Zen, K.; Yagi, N.; Naito, Y.; Itoh, Y. , Clinical Outcomes of Follow-Up Observation After Endoscopic Submucosal Dissection for Esophageal Squamous Cell Carcinoma Invading the Muscularis Mucosa Without Lymphovascular Involvement. Dig Dis Sci 2023, 68, 3679–3687. [Google Scholar] [CrossRef]
- Rodríguez de Santiago, E.; van Tilburg, L.; Deprez, P. H.; Pioche, M.; Pouw, R. E.; Bourke, M. J.; Seewald, S.; Weusten, B.; Jacques, J.; Leblanc, S.; Barreiro, P.; Lemmers, A.; Parra-Blanco, A.; Küttner-Magalhães, R.; Libânio, D.; Messmann, H.; Albéniz, E.; Kaminski, M. F.; Mohammed, N.; Zabala, F. R.; Herreros-de-Tejada, A.; Koecklin, H. U.; Wallenhorst, T.; Santos-Antunes, J.; Cunha Neves, J. A.; Koch, A. D.; Ayari, M.; Duran, R. G.; Ponchon, T.; Rivory, J.; Bergman, J.; Verheij, E. P. D.; Gupta, S.; Groth, S.; Lepilliez, V.; Franco, A. R.; Belkhir, S.; White, J.; Ebigbo, A.; Probst, A.; Legros, R.; Pilonis, N. D.; de Frutos, D.; González, R. M.; Dinis-Ribeiro, M. , Western outcomes of circumferential endoscopic submucosal dissection for early esophageal squamous cell carcinoma. Gastrointest Endosc 2023. [Google Scholar] [CrossRef] [PubMed]
- Hsu, M. H.; Wang, W. L.; Chen, T. H.; Tai, C. M.; Wang, H. P.; Lee, C. T. , Long-term outcomes of endoscopic submucosal dissection for superficial esophageal squamous cell carcinoma in Taiwan. BMC Gastroenterol 2021, 21, 308. [Google Scholar] [CrossRef]
- Chung, C. S.; Liao, L. J.; Lo, W. C.; Chou, Y. H.; Chang, Y. C.; Lin, Y. C.; Hsu, W. F.; Shueng, P. W.; Lee, T. H. , Risk factors for second primary neoplasia of esophagus in newly diagnosed head and neck cancer patients: a case-control study. BMC Gastroenterol 2013, 13, 154. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y. K.; Chuang, Y. S.; Wu, T. S.; Lee, K. W.; Wu, C. W.; Wang, H. C.; Kuo, C. T.; Lee, C. H.; Kuo, W. R.; Chen, C. H.; Wu, D. C.; Wu, I. C. , Endoscopic screening for synchronous esophageal neoplasia among patients with incident head and neck cancer: Prevalence, risk factors, and outcomes. Int J Cancer 2017, 141, 1987–1996. [Google Scholar] [CrossRef]
- Chung, C. S.; Lo, W. C.; Wen, M. H.; Hsieh, C. H.; Lin, Y. C.; Liao, L. J. , Long Term Outcome of Routine Image-enhanced Endoscopy in Newly Diagnosed Head and Neck Cancer: a Prospective Study of 145 Patients. Sci Rep 2016, 6, 29573. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y. H.; Ho, C. M.; Wu, M. S.; Hsu, W. H.; Wang, W. Y.; Yuan, S. F.; Hsieh, H. M.; Wu, I. C. , Effect of esophageal cancer screening on mortality among patients with oral cancer and second primary esophageal cancer in Taiwan. Am J Otolaryngol 2023, 44, 103856. [Google Scholar] [CrossRef] [PubMed]
- Chung, C.-S.; Wu, C.-Y.; Lin, Y.-H.; Lo, W.-C.; Cheng, P.-C.; Hsu, W.-L.; Liao, L.-J. , Screening and surveillance of esophageal cancer by magnifying endoscopy with narrow band imaging improves the survival of hypopharyngeal cancer patients. Frontiers in Oncology 2024, 13. [Google Scholar] [CrossRef] [PubMed]
- Oyama, T.; Inoue, H.; Arima, M.; Momma, K.; Omori, T.; Ishihara, R.; Hirasawa, D.; Takeuchi, M.; Tomori, A.; Goda, K. , Prediction of the invasion depth of superficial squamous cell carcinoma based on microvessel morphology: magnifying endoscopic classification of the Japan Esophageal Society. Esophagus 2017, 14, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, Y.; Omori, T.; Yokoyama, A.; Yoshida, T.; Hirota, J.; Ono, Y.; Yamamoto, J.; Kato, M.; Asaka, M. , Endoscopic diagnosis of early squamous neoplasia of the esophagus with iodine staining: high-grade intra-epithelial neoplasia turns pink within a few minutes. J Gastroenterol Hepatol 2008, 23, 546–550. [Google Scholar] [CrossRef]
- Japanese Classification of Esophageal Cancer, 11th Edition: part I. Esophagus 2017, 14, 1–36. [CrossRef]
- Wright, C. D.; Kucharczuk, J. C.; O'Brien, S. M.; Grab, J. D.; Allen, M. S. , Predictors of major morbidity and mortality after esophagectomy for esophageal cancer: a Society of Thoracic Surgeons General Thoracic Surgery Database risk adjustment model. J Thorac Cardiovasc Surg 2009, 137, 587–595. [Google Scholar] [CrossRef] [PubMed]
- Funk, L. M.; Gawande, A. A.; Semel, M. E.; Lipsitz, S. R.; Berry, W. R.; Zinner, M. J.; Jha, A. K. , Esophagectomy outcomes at low-volume hospitals: the association between systems characteristics and mortality. Ann Surg 2011, 253, 912–917. [Google Scholar] [CrossRef] [PubMed]
- Tsujii, Y.; Nishida, T.; Nishiyama, O.; Yamamoto, K.; Kawai, N.; Yamaguchi, S.; Yamada, T.; Yoshio, T.; Kitamura, S.; Nakamura, T.; Nishihara, A.; Ogiyama, H.; Nakahara, M.; Komori, M.; Kato, M.; Hayashi, Y.; Shinzaki, S.; Iijima, H.; Michida, T.; Tsujii, M.; Takehara, T. , Clinical outcomes of endoscopic submucosal dissection for superficial esophageal neoplasms: a multicenter retrospective cohort study. Endoscopy 2015, 47, 775–783. [Google Scholar] [CrossRef] [PubMed]
- Iizuka, T.; Kikuchi, D.; Hoteya, S.; Kajiyama, Y.; Kaise, M. , Efficacy and safety of endoscopic submucosal dissection for superficial cancer of the cervical esophagus. Endosc Int Open 2017, 5, E736–e741. [Google Scholar] [CrossRef] [PubMed]
- Toyonaga, T.; Man-i, M.; East, J. E.; Nishino, E.; Ono, W.; Hirooka, T.; Ueda, C.; Iwata, Y.; Sugiyama, T.; Dozaiku, T.; Hirooka, T.; Fujita, T.; Inokuchi, H.; Azuma, T. , 1,635 Endoscopic submucosal dissection cases in the esophagus, stomach, and colorectum: complication rates and long-term outcomes. Surg Endosc 2013, 27, 1000–1008. [Google Scholar] [CrossRef] [PubMed]
- Qi, Z. P.; Chen, T.; Li, B.; Ren, Z.; Yao, L. Q.; Shi, Q.; Cai, S. L.; Zhong, Y. S.; Zhou, P. H. , Endoscopic submucosal dissection for early esophageal cancer in elderly patients with relative indications for endoscopic treatment. Endoscopy 2018, 50, 839–845. [Google Scholar] [CrossRef] [PubMed]
- Stephant, S.; Jacques, J.; Brochard, C.; Legros, R.; Lepetit, H.; Barret, M.; Lupu, A.; Rostain, F.; Rivory, J.; Ponchon, T.; Pioche, M.; Wallenhorst, T. , High proficiency of esophageal endoscopic submucosal dissection with a "tunnel + clip traction" strategy: a large French multicentric study. Surg Endosc 2023, 37, 2359–2366. [Google Scholar] [CrossRef]
- Probst, A.; Ebigbo, A.; Eser, S.; Fleischmann, C.; Schaller, T.; Märkl, B.; Schiele, S.; Geissler, B.; Müller, G.; Messmann, H. , Endoscopic submucosal dissection for superficial esophageal squamous cell carcinoma: long-term follow-up in a Western center. Clin Endosc 2023, 56, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, H.; Arimura, Y.; Masao, H.; Okahara, S.; Tanuma, T.; Kodaira, J.; Kagaya, H.; Shimizu, Y.; Hokari, K.; Tsukagoshi, H.; Shinomura, Y.; Fujita, M. , Endoscopic submucosal dissection is superior to conventional endoscopic resection as a curative treatment for early squamous cell carcinoma of the esophagus (with video). Gastrointest Endosc 2010, 72, 255–264. [Google Scholar] [CrossRef]
- Kollar, M.; Krajciova, J.; Prefertusová, L.; Sticova, E.; Malušková, J.; Pazdro, A.; Harustiak, T.; Kodetova, D.; Vackova, Z.; Spicak, J.; Martínek, J. , Su1124 – Long Term Results of Endoscopic Treatment Vs. Esophagectomy with Lymphadenectomy in Patients with High-Risk Early Esophageal Cancer Including Detailed Analysis of Lymph Node Micrometastases. Gastroenterology 2019, 156, S–511. [Google Scholar] [CrossRef]
- Pech, O.; Behrens, A.; May, A.; Nachbar, L.; Gossner, L.; Rabenstein, T.; Manner, H.; Guenter, E.; Huijsmans, J.; Vieth, M.; Stolte, M.; Ell, C. , Long-term results and risk factor analysis for recurrence after curative endoscopic therapy in 349 patients with high-grade intraepithelial neoplasia and mucosal adenocarcinoma in Barrett's oesophagus. Gut 2008, 57, 1200–1206. [Google Scholar] [CrossRef]
- Katada, C.; Yokoyama, T.; Yano, T.; Kaneko, K.; Oda, I.; Shimizu, Y.; Doyama, H.; Koike, T.; Takizawa, K.; Hirao, M.; Okada, H.; Yoshii, T.; Konishi, K.; Yamanouchi, T.; Tsuda, T.; Omori, T.; Kobayashi, N.; Shimoda, T.; Ochiai, A.; Amanuma, Y.; Ohashi, S.; Matsuda, T.; Ishikawa, H.; Yokoyama, A.; Muto, M. , Alcohol Consumption and Multiple Dysplastic Lesions Increase Risk of Squamous Cell Carcinoma in the Esophagus, Head, and Neck. Gastroenterology 2016, 151, 860–869. [Google Scholar] [CrossRef] [PubMed]
- Minashi, K.; Nihei, K.; Mizusawa, J.; Takizawa, K.; Yano, T.; Ezoe, Y.; Tsuchida, T.; Ono, H.; Iizuka, T.; Hanaoka, N.; Oda, I.; Morita, Y.; Tajika, M.; Fujiwara, J.; Yamamoto, Y.; Katada, C.; Hori, S.; Doyama, H.; Oyama, T.; Nebiki, H.; Amagai, K.; Kubota, Y.; Nishimura, K.; Kobayashi, N.; Suzuki, T.; Hirasawa, K.; Takeuchi, T.; Fukuda, H.; Muto, M. , Efficacy of Endoscopic Resection and Selective Chemoradiotherapy for Stage I Esophageal Squamous Cell Carcinoma. Gastroenterology 2019, 157, 382–390. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Kaplan-Meier curve for the impact of pathologic stage on overall survival and disease-specific survival (a) Statistically significant difference was observed (P = 0.022) for overall survival.; (b) Statistically significant difference was observed (P = 0.007) for disease-specific survival.
Figure 1.
Kaplan-Meier curve for the impact of pathologic stage on overall survival and disease-specific survival (a) Statistically significant difference was observed (P = 0.022) for overall survival.; (b) Statistically significant difference was observed (P = 0.007) for disease-specific survival.
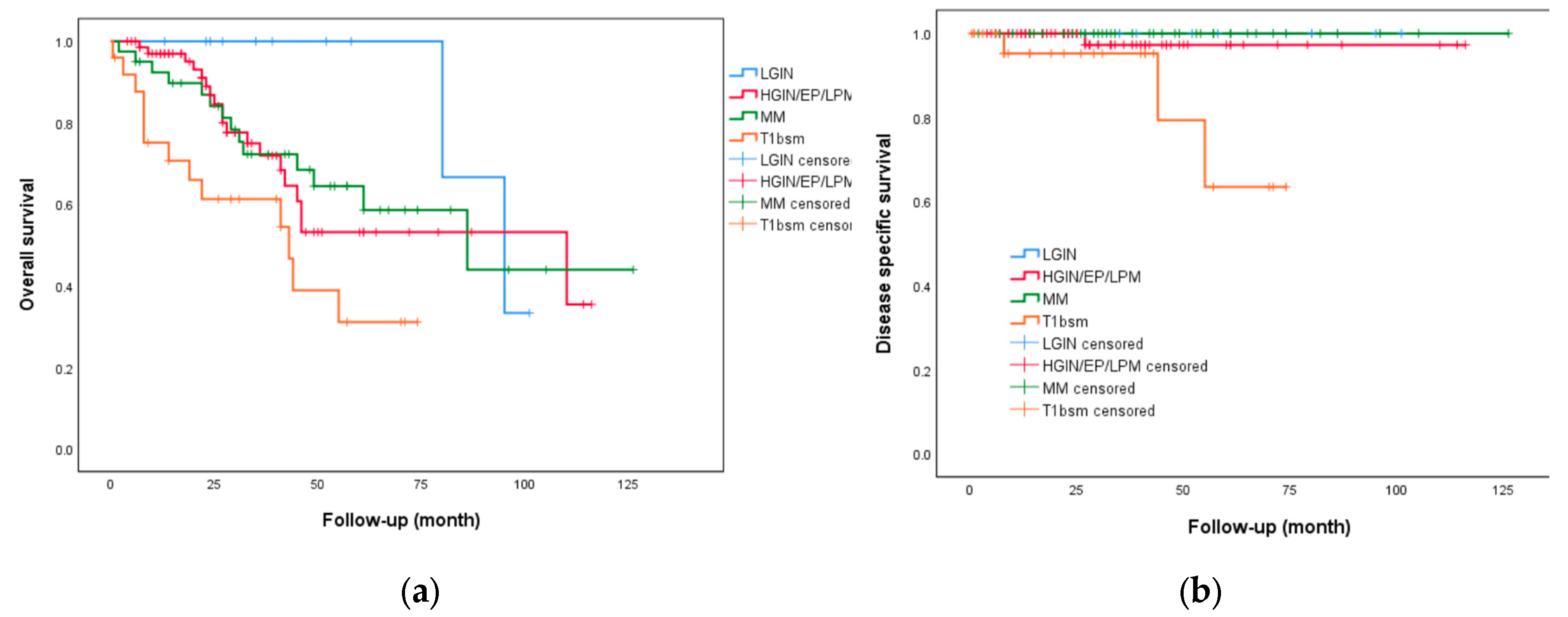
Figure 2.
Kaplan meier curve of patients with HGIN/pT1a–epithelium/lamina propria mucosa (HGIN/EP/LPM) without additional therapy and patients with pT1a–muscularis mucosa (MM), LVI negative and no additional therapy (a) overall survival between patients with HGIN/EP/LPM and those with MM (P = 0.82); (b) overall survival between HGIN/EP/LPM patients and MM patients without LVI (P=0.793); (c) disease-specific survival between HGIN/EP/LPM patient and MM patients without LVI (P=0.617); (d) overall survival with respect to the presence of lymphovascular invasion (LVI) in T1am3 (pT1a–muscularis mucosa) patients (P = 0.96).
Figure 2.
Kaplan meier curve of patients with HGIN/pT1a–epithelium/lamina propria mucosa (HGIN/EP/LPM) without additional therapy and patients with pT1a–muscularis mucosa (MM), LVI negative and no additional therapy (a) overall survival between patients with HGIN/EP/LPM and those with MM (P = 0.82); (b) overall survival between HGIN/EP/LPM patients and MM patients without LVI (P=0.793); (c) disease-specific survival between HGIN/EP/LPM patient and MM patients without LVI (P=0.617); (d) overall survival with respect to the presence of lymphovascular invasion (LVI) in T1am3 (pT1a–muscularis mucosa) patients (P = 0.96).
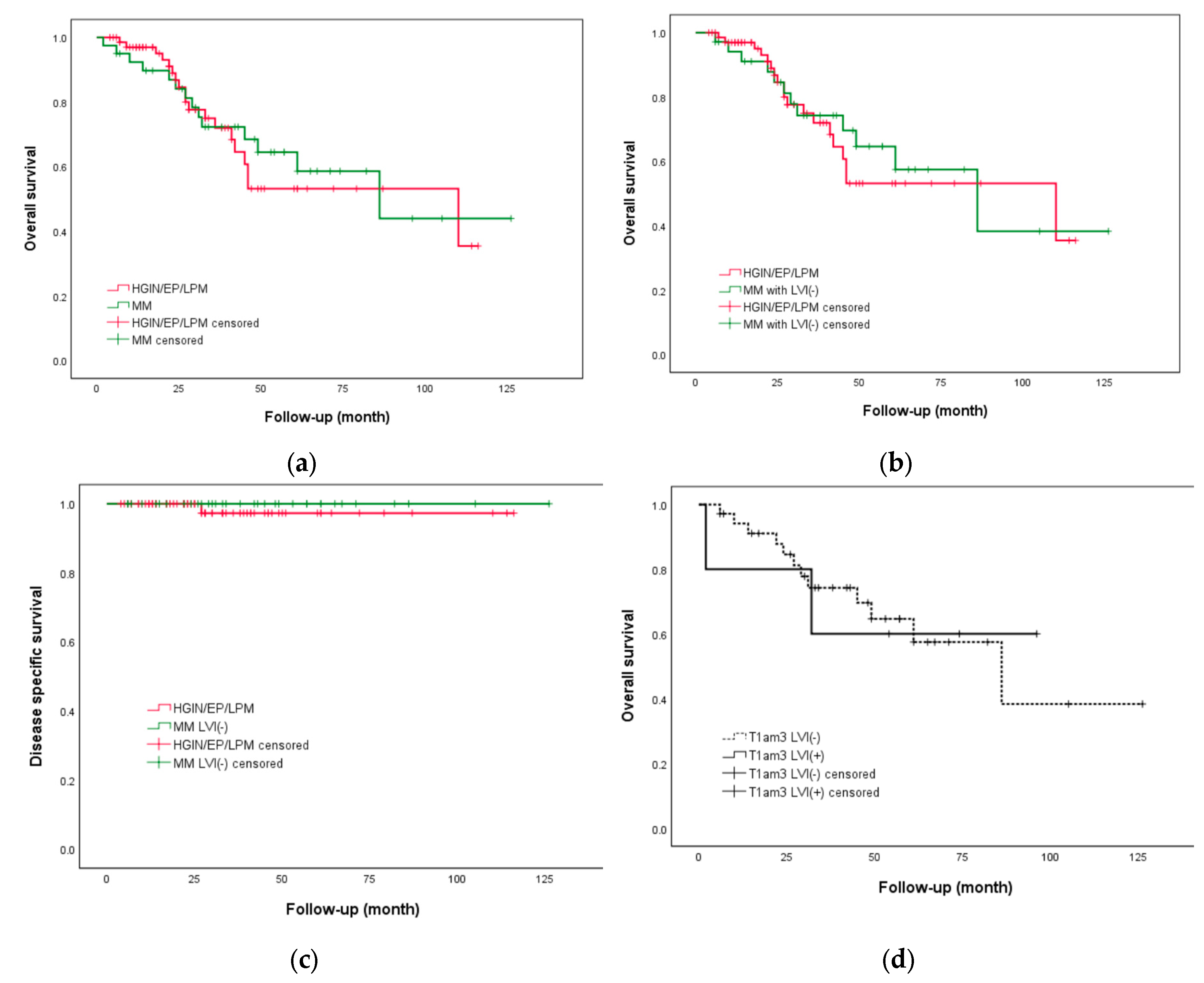
Figure 3.
Kaplan-Meier curve for cumulative incidence of recurrence (a) No statistically significant difference was observed (p=0.229) from different pathologic stage.; (b) No statistically significant difference was observed (p=0.63) in HGIN/EP/LPM patients without additional therapy and MM patients without additional therapy.
Figure 3.
Kaplan-Meier curve for cumulative incidence of recurrence (a) No statistically significant difference was observed (p=0.229) from different pathologic stage.; (b) No statistically significant difference was observed (p=0.63) in HGIN/EP/LPM patients without additional therapy and MM patients without additional therapy.
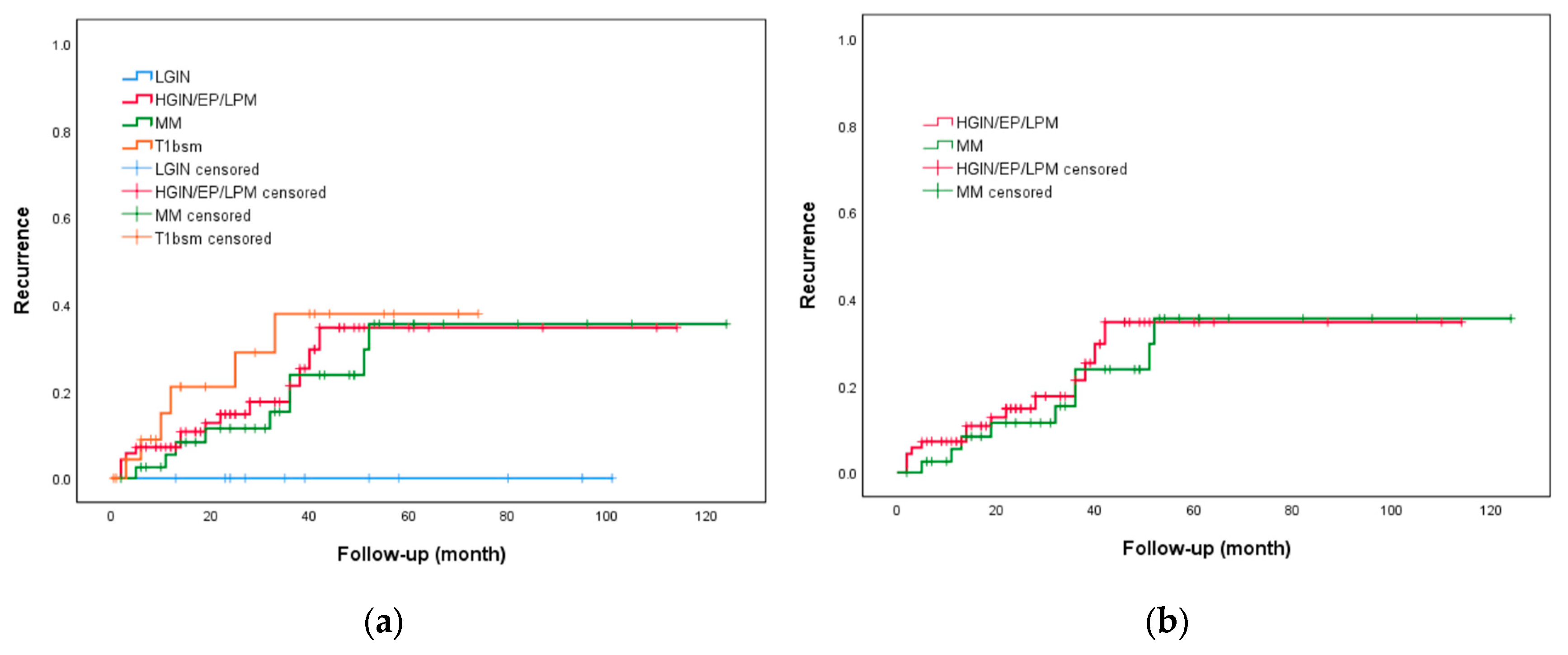
Table 1.
Clinical characteristics of 183 lesions in 146 patients.
| Variable | Lesion No. (%) |
|---|---|
| Patient characteristics Age (mean ± SD), years |
|
| 59.17 ± 9.45 | |
| Sex | |
| Male | 130 (89) |
| Female | 16 (11) |
| Smoking | 125 (85.6) |
| Alcohol drinker | 132 (90.4) |
| Betel nut chewing | 64 (43.8) |
| Smoking cessation | 48 (38.4) |
| Alcohol abstinence | 91 (68.9) |
| Betel nut cessation | 45 (70.3) |
| HN cancer history | 73 (50) |
| Endoscopic characteristics | |
| Tumor location | |
| Upper third of the esophagus | 24 (13.1) |
| Middle third of the esophagus | 102 (55.7) |
| Lower third of the esophagus | 57 (31.1) |
| Endoscopic tumor size (mean ± SD), cm | 2.48 ± 1.90 |
| Circumference of the tumor | |
| < 1/2 | 71 (38.8) |
| < 3/4 | 140 (76.5) |
| ≥ 3/4 | 43 (23.5) |
| JES type | |
| B1 | 140 |
| LGIN/HGIN/T1am1/T1am2 | 109 (77.9) |
| T1am3/ T1bsm1 | 28 (20) |
| T1bsm2 | 3 (2.1) |
| B2 | 43 |
| LGIN/HGIN/T1am1/T1am2 | 7 (16.3) |
| T1am3/ T1bsm1 | 24 (55.8) |
| T1bsm2 | 12 (27.9) |
| Pathological characteristics | |
| Histological subtype | |
| Well differentiated (G1) | 18 (23.3) |
| Moderately differentiated (G2) | 55 (71.4) |
| Poorly differentiated (G3) | 4 (5.1) |
| LVI | 14 (7.6) |
| Perineural invasion | 3 (1.6) |
| Pathologic stage | |
| LGIN | 16 (8.7) |
| HGIN/T1am1 | 90 (49.1) |
| T1am2 | 10 (5.5) |
| T1am3 | 42 (23) |
| T1bsm1 | 10 (5.5) |
| T1bsm2 | 15 (8.2) |
SD: standard deviation; HN cancer: head and neck cancer; LVI: lymphovascular invasion.
Table 2.
Outcomes and complications of patients treated with ESD.
| Variable | Lesion No. (%) |
|---|---|
| Short term outcomes En bloc resection, lesions No. (%) |
|
| 183 (100) | |
| R0 resection, lesions No. (%) | 175 (95.6) |
| Complete local remission, lesions No. (%) | 161 (88) |
| Overall post-ESD AE | 18 (9.8) |
| Stricture | 18 (9.8) |
| Bleeding | 0 |
| Perforation | 0 |
| Long term outcomes | |
| Mean follow-up period (mean ± SD), month | 37.05 ± 26.79 |
| Overall survival | |
| 1-year | 124 (91.9) |
| 3-year | 66 (67.3) |
| 5-year | 36 (48) |
| Disease-specific survival | |
| 1-year | 134 (99.3) |
| 3-year | 96 (98) |
| 5-year | 71 (94.7) |
| Recurrence | 30 (20.5) |
| Local recurrence | 16 (11.0) |
| Metachronous recurrence | 14 (9.5) |
| Time to recurrence (mean ± SD), month | 24.50 ± 24.31 |
ESD: endoscopic submucosal dissection; AE: adverse event; SD: standard deviation.
Table 3.
Univariate and multivariate analysis of factors associated with recurrence.
| Recurrence | Non-recurrence | Univariate | Multivariate | |||
|---|---|---|---|---|---|---|
| (n=30) | (n=116) | P Value | OR (95% CI) | P Value | OR (95% CI) | |
| Males | 27 (90%) | 103 (89%) | 0.85 | 1.14 (0.30-4.27) | ||
| Age (mean±SD), years | 56.63±9.59 | 59.83±9.34 | 0.10 | 0.96 (0.92-1.01) | ||
| Smoking | 26 (87%) | 99 (85%) | 0.85 | 1.12 (0.35-3.60) | ||
| Alcohol | 30 (100%) | 102 (88%) | ||||
| Betel nut | 15 (50%) | 49 (42%) | 0.45 | 1.37 (0.61-3.06) | ||
| Smoking cessation | 13 (50%) | 35 (35%) | 0.17 | 1.82 (0.76-4.37) | ||
| Alcohol abstinence | 12 (40%) | 79 (78%) | <0.001 | 0.19 (0.08-0.46) | <0.001 | 0.20 (0.08-0.48) |
| Betel nut cessation | 11 (73%) | 34 (69%) | 0.77 | 1.21 (0.33-4.43) | ||
| HN cancer | 16 (53%) | 57 (49%) | 0.68 | 1.18 (0.53-2.64) | ||
| Oral cavity cancer | 3 (19%) | 15 (26%) | 0.57 | 0.67 (0.17-2.70) | ||
| HPC and laryngeal cancer | 10 (63%) | 30 (53%) | 0.49 | 1.50 (0.48-1.68) | ||
| LVI | 5 (17%) | 9 (8%) | 0.15 | 2.38 (0.73-7.71) | ||
| Perineural invasion | 0 | 3 (3%) | ||||
| T1am3/T1bsm | 16 (53%) | 49 (42%) | 0.28 | 1.56 (0.70-3.50) | ||
| T1bsm | 6 (20%) | 19 (16%) | 0.64 | 1.28 (0.46-3.54) | ||
| Histology subtype G2/G3 | 13 (62%) | 45 (76%) | 0.21 | 0.51 (0.17-1.47) | ||
| Histology subtype G3 | 0 | 4 (3%) | ||||
| Endoscopy tumor size (mean±SD),cm | 3.60±2.01 | 3.23±2.18 | 0.41 | 1.08 (0.90-1.29) | ||
| Circumference over 3/4 | 8 (27%) | 30 (26%) | 0.93 | 1.04 (0.42-2.59) | ||
| Circumference over 1/2 | 23 (77%) | 78 (67%) | 0.32 | 1.60 (0.63-4.06) | ||
| R0 resection | 26 (87%) | 112 (97%) | 0.05 | 0.23 (0.05-0.99) | 0.31 | 0.36 (0.05-2.60) |
| CLR | 22 (73%) | 103 (89%) | 0.04 | 0.35 (0.13-0.94) | 0.56 | 0.66 (0.17-2.63) |
OR: odds ratio; CI: confidence interval; IQR: interquartile range; HN cancer: head and neck cancer; HPC: hypopharyngeal cancer; LVI: lymphovascular invasion; CLR: complete local remission.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



