Submitted:
19 June 2024
Posted:
20 June 2024
You are already at the latest version
Abstract
Smoking a cigarette before bed or first thing in the morning is a common habit. In this review the relationship between smoking and sleep is investigated, based on the existing literature. Tobacco smoking disrupts sleep architecture by reducing slow wave and rapid eye movement (REM) sleep and undermining sleep quality. Furthermore, smoking affects sleep-related co-morbidities, such as obstructive sleep apnoea-hypopnea syndrome (OSAHS), insomnia, parasomnias, arousals, bruxism, restless legs but also non-sleep-related conditions such as cardiovascular, metabolic, respiratory, neurologic, psychiatric, inflammatory, gynecologic and pediatric. This review aims to consolidate all the existing knowledge about the relationship between smoking and sleep.
Keywords:
smoking
; tobacco
; sleep
; sleep disorders
1. Introduction
There are many studies which have demonstrated the relationship between smoking and sleep quality [1]. Poor sleep quality seems to be related with increased craving for tobacco smoke and reduced chances of a successful smoking cessation effort [2], while smoking itself alters sleep architecture [3], and has detrimental effects on sleep quality [4]. Furthermore, smoking seems to worsen many aspects of obstructive sleep apnoea-hypopnoea syndrome (OSAHS) [5], while it is also related with other sleep disorders like insomnia [6], parasomnias [7], arousals [8], bruxism [9] and restless legs [10]. In addition to that, poor sleep or OSAHS along with smoking have a multiplicative action in several other medical conditions, such as obesity and metabolic syndrome [11, 12], cardiovascular, respiratory and neuropsychiatric diseases [13-16], and complications in pregnancy or in infant growth [17, 18]. The aim of this review is to shed light in all these deleterious interactions between tobacco smoking and sleep.
2. Methods
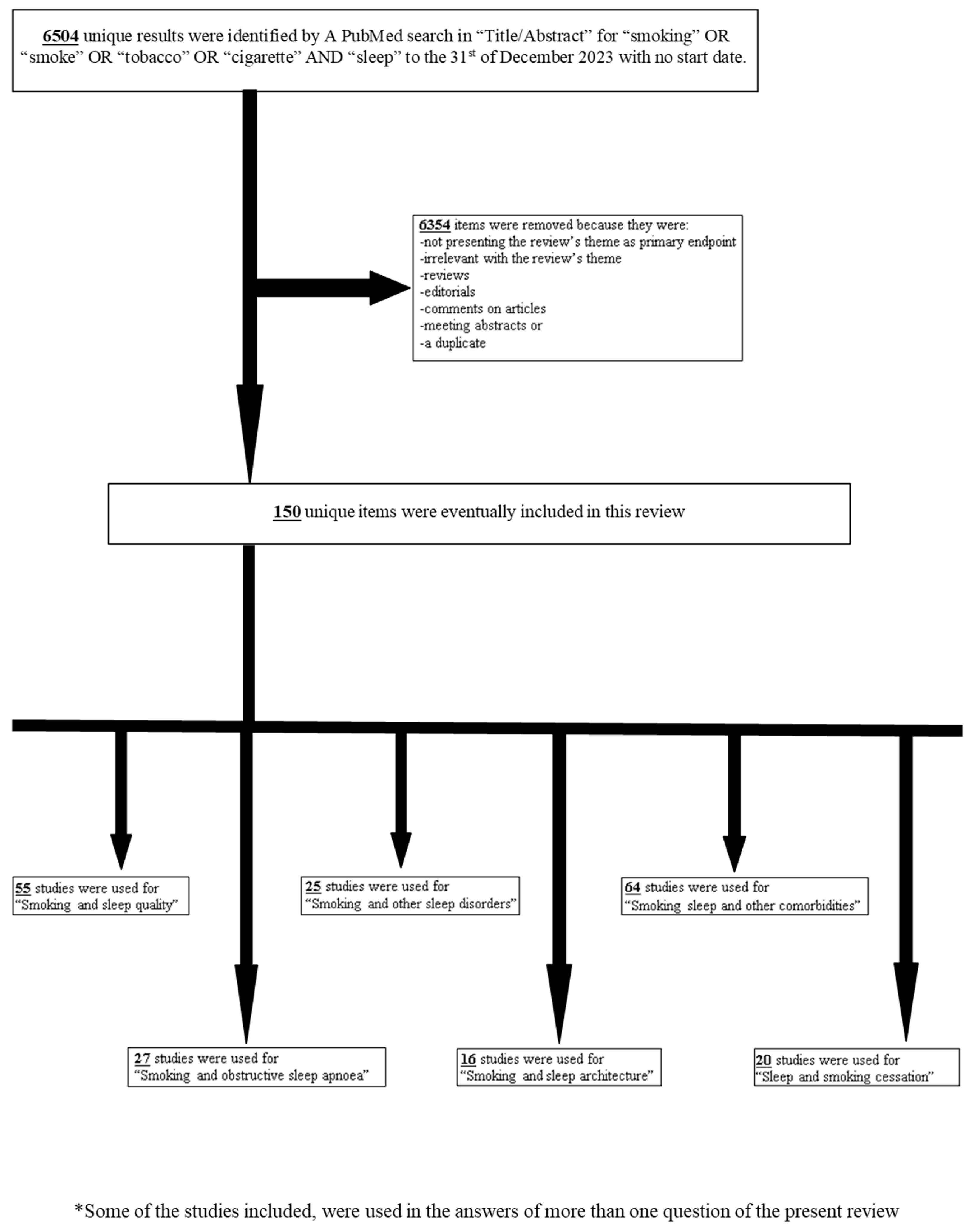
For the purpose of the present review, we performed a PubMed search in “Title/Abstract” for “smoking” OR “smoke” OR “tobacco” OR “cigarette” AND “sleep” to the 31st of December 2023 with no start date. This search identified 6504 unique results. Items were removed if they were reviews, editorials, comments on articles, meeting abstracts, a duplicate, irrelevant to the research theme or had not among the primary endpoints the relationship between smoking and sleep. As a result, 6354 items were removed and 150 were included in this review. Articles were categorized based on the thematic sectors of this review. Some of the studies included, were used in more than one thematic sector. For ‘smoking and sleep quality’, 55 studies were used. For the ‘smoking and obstructive sleep apnoea’ sector, 27 studies were used. For ‘smoking and other sleep disorders’, 25 studies were used. For ‘smoking and sleep architecture’, 16 studies were used. For ‘smoking, sleep and other comorbidities’ 64 studies were used. Finally, 20 studies were used for the ‘sleep and smoking cessation’ sector. The consort diagram is shown as Figure 1. For any studies written by one or more co-authors of the present review, an independent author, who did not participate in the study, reviewed it for suitability of inclusion.
3. Discussion
Smoking and Sleep Quality
The stimulant effect of nicotine has been reported more than 40 years ago [19]. Back in the 80s’ and 90s’, several studies had correlated smoking with various aspects of poor sleep quality, such as difficulty in initiating sleep, staying asleep and waking up, nightmares, snoring, excessive daytime sleepiness and minor accidents [20-22]. Sleep duration was inversely correlated with smoking even in athletes [23], whilst the effects of smoking on sleep were partly attributed to the fact that smokers consume greater quantities of caffeine and alcohol as well [24]. However, in a longitudinal, population-based cohort study with 7.960 participants, it was found that adolescents that had no sleep problems previously, reported sleep disorders at follow-up, with showing a dose-response relationship with smoking [25].
Numerous studies have been published on this topic; in many of them, the main tool used to measure sleep disturbance was the Pittsburgh Sleep Quality Index (PSQI). In these studies, PSQI scores were persistently higher in smokers compared to non-smokers [26-28]. In the same outcome also concluded a 6-week double-blind randomized controlled trial which investigated for possible augmented effects of naltrexone to nicotine patch in smoking cessation [29]. Furthermore, in two large cross-sectional surveys from Korea, which included cumulatively almost 400.000 participants, the same relationship was also found for both men and women separately [30], while in the latter, PSQI in smokers remained significantly higher after controlling for psychological factors as well [31]. Other study, which also used PSQI, described a quantitative relation of sleep disturbance and smoking with significantly longer sleep latency in heavy smokers compared to non-smokers [32, 33]. In a 12-week randomized controlled trial about the relationships between exercise, sleep, and smoking, higher PSQI scores were correlated with increased withdrawal, craving and total smoking urges assessed by the Minnesota Nicotine and Withdrawal Scale (MNWS) [4].
Apart from PSQI, there are also other sleep parameters that present deterioration with smoking. A study which examined the difficulty falling asleep (chronic or recent), difficulty staying asleep, and weekday and weekend sleep duration in relation with past 30-day smoking, found significant reciprocal, prospective relationships between smoking and sleep problems which were more evident to the black race compared to Caucasians [34]. Longer sleep latency, shorter sleep time and difficulty in maintaining sleep seem to present consistently more frequently in smokers compared to non-smokers in numerous studies [6, 35-37]. However, there were conflicting evidence about difficulty in initiating sleep and awakenings earlier than desired [36, 37]. In any case, many studies have demonstrated that sleep problems associated with smoking, come in a dose-response manner [38]. For example, e-cigarette users have lower odds to present inadequate sleep duration compared to cigarette users, while dual user present the highest odds [39], and the same goes for heavy smokers compared to regular smokers [40], or those who consume tobacco with higher nicotine concentration [41]. Furthermore, there is increasing evidence that those who are exposed to second-hand smoke are also more prone to develop sleep disturbances, such as short, insufficient or poor-quality sleep, than those who are not [42-45]. Another factor that possibly intervenes in the relationship between smoking and sleep disturbances is stress [46], something that was even more evident during the COVID-19 pandemic [47]. Finally, chronotype and shiftwork seem to also play some role in this relationship, with those who belong to late chronotypes and night shiftworkers being more vulnerable in the exacerbation of poor sleep quality due to smoking [17, 48, 49].
On the other hand, there are also studies that have not identified significant relationships between cigarette smoking and sleep quality, apart from an indirect confounding action along with other socioeconomic factors [50], or merely an insignificant effect in sleep hygiene [51]. However, all the aforementioned studies used mainly questionnaires, whilst the detrimental effect of smoking on sleep quality has also been demonstrated with biochemical and genetic examinations. More particularly, urine cotinine and 1-hydroxypyrene have been found increased in smokers with long sleep latency, short sleep time and poor sleep quality overall, compared to never or passive smokers [52, 53]. Moreover, a genetic study found negative genetic correlations between smoking initiation and sleep duration and smoking cessation and chronotype, while positive genetic correlations between smoking initiation and cigarettes per day with insomnia [54]. Yet another aspect in the relationship between smoking and poor sleep quality is their common effect on other unhealthy habits. In fact, many studies have shown this effect in bad nutrition, caffeine intake, alcohol consumption, illicit drug usage and lack of physical activity [55-61].
Since the majority of the studies that were included, so far, in this review are cross-sectional, a temporal relationship between smoking and poor sleep quality cannot be established. Thus, the boundaries as far as the causality between these two are vague. Two large longitudinal studies that investigated the relation between sleep problems in adolescence and subsequent smoking trajectories resulted in conflicting evidence, since the one found a significant relationship [62], whilst the other did not [63]. Another similar study linked poor sleep adequacy in adolescence with subsequent increased smoking behavior through delayed reward discounting mechanism due to adverse childhood experiences [64]. In any case, it seems that sleep deprivation or a transition from adequate to inadequate sleep causes increased tobacco cigarette consumption, probably due to the expectance that nicotine might reduce subjective sleepiness [65, 66]. This might also explain why night shiftworkers smoke more [67], or why poor sleep quality is associated with lower quit attempt efficacy [68]. Due to all that, it has been suggested that smoking cessation programs should target to the smokers with poor sleep and promote interventions in this direction [69, 70].
Smoking and Obstructive Sleep Apnoea
Various pathophysiological mechanisms have been proposed to explain the relationship between smoking and OSAHS. Increased thickness and edema, along with positive staining for calcitonin gene-related peptide (CGRP) -a neuroinflammatory marker for peripheral nerves- have been found in the uvular mucosa lamina propria of smokers. This suggests that smoking might worsen OSAHS through exacerbation of upper airway collapse at the level of the uvula via CGRP neurogenic inflammation leading to increased apnoea-hypopnoea and oxygen desaturation indices (AHI and ODI) [71]. Another mechanism is that of increased nasal mucociliary clearance time in smokers, with a dose-dependent manner [72]. Furthermore, increased total nasal resistance in a supine position also seems to play a role in smokers with history of habitual snoring [73].
Nevertheless, there is conflicting evidence about the relationship between smoking and OSAHS prevalence. A study which used STOP-Bang, found that former and current male smokers had moderately and severely increased risk for OSA respectively [74]. In another study, OSAHS was more prevalent in smokers compared to non-smokers [75], while in two more studies current, but not former smokers, presented higher odds ratio in a dose-dependent way, for sleep-disordered breathing or OSAHS, adjusted for confounders such as age, sex, body mass index (BMI) and alcohol [76, 77]. However, in three other studies, smoking was not related to the prevalence of OSAHS, when adjusted for the same covariates [13, 78, 79], apart from in younger females in one study [78], while OSAHS severity was related to smoking in patients with BMI < 30 in another [79].
As far as the relationship between smoking and OSAHS severity, things are rather clearer. Current smokers seem to present OSAHS earlier than their non-smoking counterparts [80]. Smokers also seem to present more severe OSAHS, at least in the majority of the studies [5, 7, 80-84], compared to non-smokers. Numerous OSA indices were deteriorated in smokers including ODI, mean and minimum SaO2, total sleep time and sleep time ratio with SaO2 below 90%, mean apnoea duration, nocturnal hypoxia index and COHb levels [5, 7, 80-89]. However, the relationship of AHI with smoking is not clear. Many studies concluded that AHI is deteriorated or affected in a dose-dependent manner with smoking, even after adjusting for covariates [5, 7, 80-84], while in other studies AHI seems not to be related with smoking [85-92]. As far as Epworth sleepiness scale (ESS), the majority of the studies concluded that it is worse in smokers [80, 82, 85, 87], although there were also a few notable exceptions in this topic [7, 91].
Furthermore, it is rather clear that smokers with OSAHS present significantly more frequently cardiovascular, metabolic, respiratory and gastrointestinal co-morbidities compared to non-smokers [5, 7, 80, 82, 84, 85, 93]. Additionally, it seems that smoking ameliorates the beneficial effect of the treatment of OSAHS with continuous positive airway pressure (CPAP) [92]. Finally, it is worth mentioning that in a genetic study about smoking, coffee, alcohol and OSA, in the univariate mendelian regression, smoking initiation was associated with an increased risk of OSA incidence; however, in the multivariate model this association was not significant after adjusting for BMI [94].
Smoking and Other Sleep Disorders
As shown previously, smoking is associated with increased sleep latency, difficulty in initiating and maintaining sleep, shorter total sleep time and earlier morning awakening, all of which are characteristic constituents of insomnia. Compared to nonsmoking, smoking has been associated with experiencing increased insomnia, while night-time smoking was significantly associated with greater insomnia and shorter sleep duration [6]. In night shiftworkers, smoking has been associated with insomnia after recent significant life events [67]. During the COVID-19 pandemic, the severity of insomnia index has been associated with pain in the elderly female patients who smoked [95]. Insomnia was more frequent in patients with rheumatic conditions who were also smokers, with chronic pain being a suggestive intermediate liaison [96]. Smoking was associated with insomnia in a dose dependent manner in two more studies, either with [58], or without alcohol consumption [57], while cognitive-behavioral therapy for insomnia plus smoking cessation counseling improved insomnia symptoms in another study [97]. Nevertheless, in two other studies, light but not heavy smoking was associated with insomnia, after controlling for covariates [37, 98]. Finally, in a recent genetic study, it was demonstrated that insomnia was positively correlated with both smoking initiation and the number of cigarettes per day [54].
A very rare type of parasomnia is that of sleep-related compulsive smoking behavior, which has been described with sleep-related eating disorder [8, 99]. Prenatal maternal smoking has been independently associated with an increased risk of offspring adolescent parasomnias including walking and talking in sleep and nightmares [100]. In college students, sleep related disorders have not been related with smoking in one study [101], however, in another study of patients attending a sleep clinic for suspected OSAHS, ever smokers, compared to never smokers, presented more frequent episodes of sleep talking, abnormal movements and restless sleep [7].
As far as periodic leg movements in sleep or restless legs syndrome, two studies have shown that these disorders deteriorate with smoking [26, 102], however another study demonstrated that they are not related [10]. In the same study, bruxism has been shown to worsen with smoking [10]. Bruxism also worsened with smoking in another study, in which it was accompanied by arousals, especially in N1 sleep stage and the non-supine position, indicating increased sleep fragmentation [9], however it was not improved with smoking cessation in a different study [103].
Concerning arousal index, it was found significantly increased in current and former smokers compared to non-smokers [89]. Furthermore, the same applied in patients with sleep-related compulsive smoking behavior [8]. Moreover, relative arousals were also increased in smokers who abstained from smoking [104], and to those who received varenicline for smoking cessation [105], although those who received 24-h nicotine patch experienced significantly less microarousals than those who received the 16-h one [106]. Finally, the arousal index was significantly decreased in maternal smoking infants, a factor that combined with the apneic episodes in this population, might contribute to the sudden infant death syndrome [107].
Smoking and Sleep Architecture
Current smokers tend to present a faster sleep electroencephalogram activity with lower delta power, which has a dose-dependent negative association with smoking, in non-rapid eye movement (REM) sleep compared with former and never smokers and higher alpha power compared with never smokers [3]. Evidence also exists about diminished sleep continuity and increased wake time after sleep onset [108]. As far as sleep stages, it seems that N3 stage or slow wave sleep is decreased in smokers, while N1 and N2 stages are increased, changes that seem to be dose dependent, as they are more evident to heavy smokers compared to mild smokers, or to current smokers compared to former smokers [5, 81, 86, 109]. In another study, smokers presented shorter sleep period time, longer sleep latency and consequently higher REM sleep density with no differences regarding parameters of spectral analysis of the sleep electroencephalogram as well as in the sleep efficiency measured by PSG [26]. During smoking abstinence, changes in sleep stages and awakenings have been observed [104]. Nicotine patches, especially the 24-hour compared to the 16-hour ones, increase significantly the proportion of slow wave sleep, REM density and REM beta activities, while decrease REM latency and N2 sleep stage duration [106, 110, 111]. On the other hand, the administration of varenicline does not cause changes in sleep macro architecture (N1, N2, N3, REM, Sleep Efficiency, Total Sleep Time) apart from prolongation of sleep latency, N2 and N3 latency [105]. Furthermore, uvulopalatopharyngoplasty improves N1 and N3 sleep stages significantly in smokers with OSAHS [93]. Finally, infants of mothers who smoke, sleep less, present a higher proportion of active sleep and a lower proportion of quiet sleep and more wakefulness after sleep onset, while they display more body movements and more disturbed sleep [112]. Moreover, in such infants, gastroesophageal reflux emerges more frequently in REM sleep stage [113].
Smoking, Sleep and Other Medical Conditions
There are plenty medical conditions that are affected by the simultaneous existence of smoking with a sleep problem. Obesity is significantly correlated, positively with the number of cigarettes, and negatively with the sleep duration [11, 114]. Leptin levels tend to increase in active smokers with OSAHS after treatement with CPAP compared to non-smokers, probably because smoking acts as a predisposing factor to leptin resistance [92]. Moreover, orexin-A levels were significantly lower in never smokers with OSAHS compared to ex- or current smokers [115]. The co-existence of OSA or short sleep duration with smoking has been related not only with excess body weight, but also with metabolic diseases such as resistance to insulin or type II diabetes mellitus, increased triglycerides, increased low density lipoprotein (LDL) cholesterol and decreased high-density lipoprotein (HDL) cholesterol levels and also with cardiovascular diseases such as hypertension and coronary artery disease [9, 12, 13, 82, 84, 116-120]. Furthermore, in patients with OSAHS, current smoking determines the circulating levels of myeloperoxidase (MPO), an oxidative stress marker, and matrix metalloproteinase-9 (MMP-9), a plaque destabilizer, both signaling a worse prognosis [121]. In addition to that, OSA severity and smoking are independent predictors of peripheral arterial tonometry (PAT), a marker which quantifies endothelial dysfunction [122]. Nevertheless, a study on upper airway surgery in patients with OSAHS demonstrated that post-operative smoking does not worsen glycemic or lipid profile, which are improved with the surgery [93]. Finally, apart from coronary arteries, smoking and OSAHS seem to also insult the myocardium, since, in patients with systolic heart failure, they predispose to nocturnal ventricular arrythmias, that might be proved fatal [123].
Apart from metabolic and cardiovascular diseases, poor sleep combined with smoking participate in the pathophysiological mechanism of numerous medical conditions. They increase hemoglobulin (Hb) [5], and along with hyperlipidemia are risk factors for proteinuria among high altitude mountain trekkers [124], while they are related with lower levels of iron and magnesium [9]. Furthermore, they are related with increased cortisol levels, which in turn play a role in wake time after sleep onset [108], however, sleep, but not smoking, is related with serum testosterone levels and liver steatosis [125, 126]. Central nervous system also seems to be affected, since dopamine was found significantly increased, while dopamine transporter was found significantly decreased in the cerebrospinal fluid (CSF) of active smokers with poor sleep [33]. Similarly inflammatory markers such as tumor necrosis factor alpha (TNF-a) and interleukin-1b (IL-1b) were also increased [28]. Perhaps, these changes in CSF play a role in smokers with poor sleep quality and masticatory myofascial pain [127], pain related with rheumatic diseases [96], or COVID-19 [95]. In any case the combination of smoking and poor sleep quality is not only a feature in COVID-19 pandemic but also in HIV one [47, 128]. Furthermore, poor sleep quality, along with several other unhealthy habits, have been associated with lower grey matter brain volume and although smoking was not a significant factor in the multivariate analysis [129], it has been associated with several neurological defects such as mild cognitive impairment, memory problems and even sudden deafness [15, 27, 130, 131]. In addition, smoking combined with poor sleep quality have also been associated with mental health problems [55] such as anxiety, depression and bipolar disorder [22, 46, 51, 132]. This has also been demonstrated in a genetic study, in which smoking and sleep quality were independent risk factors for both depression and bipolar disorder [16]. Perhaps, this is associated with the effect of nicotine in the cholinergic system [111]. In any case, poor sleep and smoking have also been related with other substance misuse, such as cannabis [57].
Another link between smoking and sleep with other medical conditions is that with respiratory system problems. In a study of children with asthma it was found that smoking of the caregivers leads to increased reliever medication use, which in turn disrupted the sleep quality of children [133]. However, another study demonstrated that OSAHS is a determinant of asthma control irrespective of smoking [134]. As far as chronic obstructive pulmonary disease (COPD), in patients with OSA and COPD who still smoke, smoking-related airway inflammation, is characterized by higher levels of exhaled CO and H2S and lower levels of NO, which consequently augments the effect of ozone on SpO2 during sleep [14]. Furthermore, patients with OSAHS who smoke have worse forced expiratory volume in 1 second to forced vital capacity (FEV1/FVC) ratio and are presented more frequently with COPD [5, 80], although this was not evident in another study [91].
Finally, a distinct mention is required for the relationship between smoking and sleep problems with gynecological and infant problems. In a genetic study about risk factors for breast cancer, sleep satisfaction was included among them, but smoking was not [135]. Sleep-disordered breathing also seems to be a risk factor for gestational diabetes mellitus, irrespective of smoking status [136], however smoking seems to induce several sleep problems to pregnant women such as difficulty in initiating or maintaining sleep, short sleep duration, insufficient sleep, poor sleep quality, early-morning awakening, excessive daytime sleepiness and tiredness and restless legs syndrome [17, 102]. Even exposure to passive smoking seems to exacerbate such sleep disturbances [137], while post-partum behavioral interventions in sleep of these women helps to prevent them from relapsing in smoking [138]. Maternal smoking also has deleterious effects in the sleep of their infants. These infants sleep less in overall, with a higher proportion of active sleep and a lower proportion of quiet sleep, and have more wakefulness after sleep onset, with more body movements and, as a result, more disturbed sleep [18, 112]. They also tend to have increased risk for GER during REM sleep [113], while they also are at greater risk for admitting to the neonatal intensive care unit [139]. Furthermore, when they grow up, they face an increased risk of adolescent parasomnias including sleep-walking, sleep-talking and nightmares, and an increased likelihood of reporting sleep problems at the 14 years of age [100]. Finally, maternal smoking along with supine sleep position are risk factors for sudden infant death syndrome [107, 140-143].
Smoking Cessation and Sleep
Sleep quality is an important factor in a smoking cessation effort [144]. Sleep duration is positively associated with smoking cessation [145], while insomnia decreases the odds for a successful smoking cessation effort [54]. Heavy smokers often suffer from nocturnal sleep-disturbing nicotine craving [2], while poor sleep quality during a smoking cessation effort leads to increased withdrawal, craving, irritability, anxiety, tension and total smoking urges [4, 104]. Sleep disorders are considered as withdrawal symptoms during cessation. Emotional disturbances such as anxiety and depression are common in those who experience poor sleep quality during smoking cessation and might be a target for cognitive behavioral treatment [70, 132, 146]. Olfactory aversive conditioning during sleep might reduce cigarette-smoking behavior in a sleep stage-dependent manner, persisting for several days [147]. Additionally, targeting sleep quality might improve smoking cessation odds [68, 138], however, this was not the case in two studies that try to implement this theory [97, 148]. Smoking cessation also has not improved other sleep disorders, such as bruxism [103]. In a smoking cessation study, it was demonstrated that varenicline and transdermal nicotine patches might increase sleep disturbance, although they attenuate withdrawal symptoms unrelated to sleep compared to placebo [149]. Nevertheless, in another study, varenicline had a little effect in sleep macro architecture in patients with OSA, although it did slightly increased arousal index and decreased sleep efficiency [105]. Furthermore, the 24-h nicotine patch, compared to the 16-h one, improved sleep quality and decreased smoking urges [106, 110, 150].
4. Conclusions
Smoking has a deleterious effect on sleep quality, while poor sleep quality also seems to increase the likelihood for smoking. It is not clear whether smoking participates in the pathogenesis of OSAHS, however, smokers with OSAHS present a more severe disease as far as their physiological measurements. Furthermore, smoking seems to exacerbates other sleep disorders such as insomnia, parasomnias, arousals, bruxism and restless legs, while it disrupts sleep architecture by promoting a less deep and consequently less restful and refreshing sleep. Alarmingly, poor sleep multiplies the effect of smoking in numerous medical conditions and vice versa, while good quality of sleep might increase the likelihood for a successful smoking cessation effort.
Author Contributions
Conceptualization, I.G. and SC.K; Methodology, I.G. and SC.K; Software, SC.K; Validation, K.P, D.S, and A.T; Formal Analysis, I.G and SC.K; Investigation, I.G, A.M and I.A; Resources, SC.K, C.M and C.M; Data Curation, SC.K, and A.M; Writing – Original Draft Preparation, I.G and SC.K; Writing – Review & Editing, I.G, SC.K, I.P, and A.P; Visualization, I.G; Supervision, A.P
Funding
None
Acknowledgments
None
Conflicts of interest
All authors disclose that they do not have any financial or other relationships, which might lead to a conflict of interest regarding this paper.
References
- Woo, D.H.; Park, M.; Jang, S.-Y.; Park, S.; Jang, S.-I. Association between smoking status and subjective quality of sleep in the South Korean population: a cross-sectional study. Sleep Breath. 2022, 27, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Riemerth, A.; Kunze, U.; Groman, E. Nocturnal sleep-disturbing nicotine craving and accomplishment with a smoking cessation program. Wien. Med. Wochenschr. 2009, 159, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Truong, M.K.; Berger, M.; Haba-Rubio, J.; Siclari, F.; Marques-Vidal, P.; Heinzer, R. Impact of smoking on sleep macro– and microstructure. Sleep Med. 2021, 84, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Purani, H.; Friedrichsen, S.; Allen, A.M. Sleep quality in cigarette smokers: Associations with smoking-related outcomes and exercise. Addict. Behav. 2018, 90, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Yosunkaya, S.; Kutlu, R.; Vatansev, H. Effects of smokıng on patıents wıth obstructıve sleep apnea syndrome. Clin. Respir. J. 2020, 15, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Nuñez, A.; Rhee, J.U.; Haynes, P.; Chakravorty, S.; Patterson, F.; Killgore, W.D.; Gallagher, R.A.; Hale, L.; Branas, C.; Carrazco, N.; et al. Smoke at night and sleep worse? The associations between cigarette smoking with insomnia severity and sleep duration. Sleep Heal. 2020, 7, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Grigoriou, I.; Skalisti, P.; Papagiouvanni, I.; Michailidou, A.; Charalampidis, K.; Kotoulas, S.-C.; Porpodis, K.; Spyratos, D.; Pataka, A. Smoking-Induced Disturbed Sleep. A Distinct Sleep-Related Disorder Pattern? Healthcare 2023, 11, 205. [Google Scholar] [CrossRef] [PubMed]
- Provini, F.; Vetrugno, R.; Montagna, P. Sleep-related smoking syndrome. Sleep Med. 2008, 9, 903–905. [Google Scholar] [CrossRef] [PubMed]
- Frosztega, W.; Wieckiewicz, M.; Nowacki, D.; Michalek-Zrabkowska, M.; Poreba, R.; Wojakowska, A.; Kanclerska, J.; Mazur, G.; Martynowicz, H. Polysomnographic Assessment of Effects of Tobacco Smoking and Alcohol Consumption on Sleep Bruxism Intensity. J. Clin. Med. 2022, 11, 7453. [Google Scholar] [CrossRef]
- Lavigne, G.J.; Lobbezoo, F.; Rompré, P.H.; Nielsen, T.A.; Montplaisir, J. Cigarette Smoking as a Risk Factor or an Exacerbating Factor for Restless Legs Syndrome and Sleep Bruxism. Sleep 1997, 20, 290–293. [Google Scholar] [CrossRef]
- Alsulami, S.; Althagafi, N.; Hazazi, E.; Alsayed, R.; Alghamdi, M.; Almohammadi, T.; Almurashi, S.; Baig, M. Obesity and Its Associations with Gender, Smoking, Consumption of Sugary Drinks, and Hour of Sleep Among King Abdulaziz University Students in Saudi Arabia. Diabetes, Metab. Syndr. Obesity: Targets Ther. 2023, 16, 925–934. [Google Scholar] [CrossRef]
- Zhu, H.; Xu, H.; Chen, R.; Liu, S.; Xia, Y.; Fu, Y.; Li, X.; Qian, Y.; Zou, J.; Yi, H.; et al. Smoking, obstructive sleep apnea syndrome and their combined effects on metabolic parameters: Evidence from a large cross-sectional study. Sci. Rep. 2017, 7, 1–8. [Google Scholar] [CrossRef]
- Ioannidou, D.; Kalamaras, G.; Kotoulas, S.-C.; Pataka, A. Smoking and Obstructive Sleep Apnea: Is There An Association between These Cardiometabolic Risk Factors?—Gender Analysis. Medicina 2021, 57, 1137. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Wang, J.; Chen, B.; Ji, X.; Zhao, C.; Chen, M.; Liao, S.; Jiang, S.; Pan, Z.; Wang, W.; et al. Association of multiple air pollutants with oxygen saturation during sleep in COPD patients: Effect modification by smoking status and airway inflammatory phenotypes. J. Hazard. Mater. 2023, 454, 131550. [Google Scholar] [CrossRef] [PubMed]
- Hu, M.; Yin, H.; Shu, X.; Jia, Y.; Leng, M.; Chen, L. Multi-angles of smoking and mild cognitive impairment: is the association mediated by sleep duration? Neurol. Sci. 2019, 40, 1019–1027. [Google Scholar] [CrossRef] [PubMed]
- He, M.; Zhou, J.; Li, X.; Wang, R. Investigating the causal effects of smoking, sleep, and BMI on major depressive disorder and bipolar disorder: a univariable and multivariable two-sample Mendelian randomization study. Front. Psychiatry 2023, 14, 1206657. [Google Scholar] [CrossRef] [PubMed]
- Merikanto, I.; Paavonen, E.J.; Saarenpää-Heikkilä, O.; Paunio, T.; Partonen, T. Eveningness associates with smoking and sleep problems among pregnant women. Chrono- Int. 2017, 34, 650–658. [Google Scholar] [CrossRef] [PubMed]
- Mennella, J.A.; Yourshaw, L.M.; Morgan, L.K. Breastfeeding and Smoking: Short-term Effects on Infant Feeding and Sleep. Pediatrics 2007, 120, 497–502. [Google Scholar] [CrossRef] [PubMed]
- Soldatos, C.R.; Kales, J.D.; Scharf, M.B.; Bixler, E.O.; Kales, A. Cigarette Smoking Associated with Sleep Difficulty. Science 1980, 207, 551–553. [Google Scholar] [CrossRef]
- Delasnerie-Laupretre, N.; Patois, E.; Valatx, J.; Kauffmann, F.; Alperovitch, A. Sleep, snoring and smoking in high school students. J. Sleep Res. 1993, 2, 138–142. [Google Scholar] [CrossRef]
- Wetter, D.; Young, T. The Relation Between Cigarette Smoking and Sleep Disturbance. Prev. Med. 1994, 23, 328–334. [Google Scholar] [CrossRef]
- A Phillips, B.; Danner, F.J. Cigarette smoking and sleep disturbance. 1995, 155, 734–7. [Google Scholar] [CrossRef] [PubMed]
- Bale, P.; White, M. The effects of smoking on the health and sleep of sportswomen. Br. J. Sports Med. 1982, 16, 149–153. [Google Scholar] [CrossRef]
- Lexcen, F.J.; Hicks, R.A. Does Cigarette Smoking Increase Sleep Problems? 1993, 77, 16–18. [Google Scholar] [CrossRef]
- Patten, C.A.; Choi, W.S.; Gillin, J.C.; Pierce, J.P. Depressive Symptoms and Cigarette Smoking Predict Development and Persistence of Sleep Problems in US Adolescents. 2000, 106, e23–e23. [Google Scholar] [CrossRef]
- Jaehne, A.; Unbehaun, T.; Feige, B.; Lutz, U.C.; Batra, A.; Riemann, D. How smoking affects sleep: A polysomnographical analysis. Sleep Med. 2012, 13, 1286–1292. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.-T.; Lee, I.-H.; Wang, C.-H.; Chen, K.-C.; Lee, C.-I.; Yang, Y.-K. Cigarette smoking might impair memory and sleep quality. J. Formos. Med Assoc. 2013, 112, 287–290. [Google Scholar] [CrossRef]
- Liu, Y.; Li, H.; Li, G.; Kang, Y.; Shi, J.; Kong, T.; Yang, X.; Xu, J.; Li, C.; Su, K.-P.; et al. Active smoking, sleep quality and cerebrospinal fluid biomarkers of neuroinflammation. Brain, Behav. Immun. 2020, 89, 623–627. [Google Scholar] [CrossRef] [PubMed]
- Peters, E.N.; Fucito, L.M.; Novosad, C.; Toll, B.A.; O'Malley, S.S. Effect of night smoking, sleep disturbance, and their co-occurrence on smoking outcomes. Psychol. Addict. Behav. 2011, 25, 312–319. [Google Scholar] [CrossRef]
- Woo, D.H.; Park, M.; Jang, S.-Y.; Park, S.; Jang, S.-I. Association between smoking status and subjective quality of sleep in the South Korean population: a cross-sectional study. Sleep Breath. 2022, 27, 1–8. [Google Scholar] [CrossRef]
- Hwang, J.H.; Park, S.-W. The relationship between poor sleep quality measured by the Pittsburgh Sleep Quality Index and smoking status according to sex and age: an analysis of the 2018 Korean Community Health Survey. Epidemiology Heal. 2022, 44, e2022022. [Google Scholar] [CrossRef] [PubMed]
- Al-Mshari, A.; AlSheikh, M.H.; Latif, R.; Mumtaz, S.; Albaker, W.; Al-Hariri, M. Impact of smoking intensities on sleep quality in young Saudi males: a comparative study. J. Med. Life 2023, 15, 1392–1396. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Liu, Y.; Xing, L.; Yang, X.; Xu, J.; Ren, Q.; Su, K.-P.; Lu, Y.; Wang, F. Association of Cigarette Smoking with Sleep Disturbance and Neurotransmitters in Cerebrospinal Fluid. Nat. Sci. Sleep 2020, 12, 801–808. [Google Scholar] [CrossRef] [PubMed]
- Bellatorre, A.; Choi, K.; Lewin, D.; Haynie, D.; Simons-Morton, B. Relationships Between Smoking and Sleep Problems in Black and White Adolescents. Sleep 2016, 40. [Google Scholar] [CrossRef] [PubMed]
- Sahlin, C.; Franklin, K.A.; Stenlund, H.; Lindberg, E. Sleep in women: Normal values for sleep stages and position and the effect of age, obesity, sleep apnea, smoking, alcohol and hypertension. Sleep Med. 2009, 10, 1025–1030. [Google Scholar] [CrossRef] [PubMed]
- McNamara, J.P.; Wang, J.; Holiday, D.B.; Warren, J.Y.; Paradoa, M.; Balkhi, A.M.; Fernandez-Baca, J.; McCrae, C.S. Sleep disturbances associated with cigarette smoking. Psychol. Heal. Med. 2013, 19, 410–419. [Google Scholar] [CrossRef] [PubMed]
- Mak, K.-K.; Ho, S.-Y.; Thomas, G.N.; Lo, W.-S.; Cheuk, D.K.-L.; Lai, Y.-K.; Lam, T.-H. Smoking and sleep disorders in Chinese adolescents. Sleep Med. 2010, 11, 268–273. [Google Scholar] [CrossRef] [PubMed]
- Mehari, A.; Weir, N.A.; Gillum, R.F. Gender and the Association of Smoking with Sleep Quantity and Quality in American Adults. Women Heal. 2014, 54, 1–14. [Google Scholar] [CrossRef]
- Merianos, A.L.; Mahabee-Gittens, E.M.; Hill, M.J.; Olaniyan, A.C.; Smith, M.L.; Choi, K. Electronic cigarette use and cigarette smoking associated with inadequate sleep duration among U.S. young adults. Prev. Med. 2023, 175, 107712. [Google Scholar] [CrossRef]
- Sujarwoto, S. Sleep Disturbance in Indonesia: How Much Does Smoking Contribute? Behav. Sleep Med. 2019, 18, 760–773. [Google Scholar] [CrossRef]
- AlRyalat, S.A.; Kussad, S.; El Khatib, O.; Hamad, I.; Al-Tanjy, A.; Alshnneikat, M.; AbuMahfouz, B. Assessing the effect of nicotine dose in cigarette smoking on sleep quality. Sleep Breath. 2021, 25, 1319–1324. [Google Scholar] [CrossRef] [PubMed]
- Nasri, O.; Pouragha, H.; Baigi, V.; Shalyari, N.; Yunesian, M. Quality of life and sleep disorders in Tehran Employees Cohort (TEC); Association with secondhand smoking and wealth index. J. Environ. Heal. Sci. Eng. 2021, 19, 1473–1481. [Google Scholar] [CrossRef] [PubMed]
- Al Banna, H.; Brazendale, K.; Hamiduzzaman, M.; Ahinkorah, B.O.; Abid, M.T.; Rifat, M.A.; Sultana, M.S.; Tetteh, J.K.; Kundu, S.; Shekhar, S.R.; et al. Exposure to secondhand smoke is associated with poor sleep quality among non-smoking university students in Bangladesh: a cross-sectional survey. Sci. Rep. 2023, 13, 1–8. [Google Scholar] [CrossRef]
- Nakata, A.; Takahashi, M.; Haratani, T.; Ikeda, T.; Hojou, M.; Fujioka, Y.; Araki, S. Association of active and passive smoking with sleep disturbances and short sleep duration among Japanese working population. Int. J. Behav. Med. 2008, 15, 81–91. [Google Scholar] [CrossRef] [PubMed]
- Sabanayagam, C.; Shankar, A. The association between active smoking, smokeless tobacco, second-hand smoke exposure and insufficient sleep. Sleep Med. 2011, 12, 7–11. [Google Scholar] [CrossRef]
- Bilsky, S.A.; Feldner, M.T.; Knapp, A.A.; Babson, K.A.; Leen-Feldner, E.W. The interaction between anxiety sensitivity and cigarette smoking level in relation to sleep onset latency among adolescent cigarette smokers. J. Adolesc. 2016, 51, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Bar-Zeev, Y.; Shauly-Aharonov, M.; Neumark, Y.; Hirshoren, N. Changes in Smoking Behavior, Stress, and Sleep Duration Among Israeli Hospital Workers During the COVID-19 Pandemic: A Cross-sectional Study. Nicotine Tob. Res. 2022, 25, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Patterson, F.; Malone, S.K.; Lozano, A.; Grandner, M.A.; Hanlon, A.L. Smoking, Screen-Based Sedentary Behavior, and Diet Associated with Habitual Sleep Duration and Chronotype: Data from the UK Biobank. Ann. Behav. Med. 2016, 50, 715–726. [Google Scholar] [CrossRef] [PubMed]
- Parkes, K. Age, smoking, and negative affectivity as predictors of sleep patterns among shiftworkers in two environments. J. Occup. Heal. Psychol. 2002, 7, 156–173. [Google Scholar] [CrossRef]
- Otsuka, Y.; Takeshima, O.; Itani, O.; Matsumoto, Y.; Kaneita, Y. Associations among Alcohol Drinking, Smoking, and Nonrestorative Sleep: A Population-Based Study in Japan. Clocks Sleep 2022, 4, 595–606. [Google Scholar] [CrossRef]
- Hattatoğlu, D.G.; Aydin, .; Yildiz, B.P. Does smoking impair sleep hygiene? Arq. de Neuro-Psiquiatria 2021, 79, 1123–1128. [Google Scholar] [CrossRef]
- Oh, S.; Kim, S.; Sung, E.; Kim, C.-H.; Kang, J.-H.; Shin, H.; Cho, I.Y. The association between cotinine-measured smoking intensity and sleep quality. Tob. Induc. Dis. 2022, 20, 1–11. [Google Scholar] [CrossRef]
- Zhou, B.; Ma, Y.; Wei, F.; Zhang, L.; Chen, X.; Peng, S.; Xiong, F.; Peng, X.; NiZam, B.; Zou, Y.; et al. Association of active/passive smoking and urinary 1-hydroxypyrene with poor sleep quality: A cross-sectional survey among Chinese male enterprise workers. Tob. Induc. Dis. 2018, 16, 23. [Google Scholar] [CrossRef]
- Gibson, M.; Munafò, M.R.; E Taylor, A.; Treur, J.L. Evidence for Genetic Correlations and Bidirectional, Causal Effects Between Smoking and Sleep Behaviors. Nicotine Tob. Res. 2018, 21, 731–738. [Google Scholar] [CrossRef]
- Metse, A.P.; Clinton-McHarg, T.; Skinner, E.; Yogaraj, Y.; Colyvas, K.; Bowman, J. Associations between Suboptimal Sleep and Smoking, Poor Nutrition, Harmful Alcohol Consumption and Inadequate Physical Activity (‘SNAP Risks’): A Comparison of People with and without a Mental Health Condition in an Australian Community Survey. Int. J. Environ. Res. Public Heal. 2021, 18, 5946. [Google Scholar] [CrossRef]
- Riera-Sampol, A.; Rodas, L.; Martínez, S.; Moir, H.J.; Tauler, P. Caffeine Intake among Undergraduate Students: Sex Differences, Sources, Motivations, and Associations with Smoking Status and Self-Reported Sleep Quality. Nutrients 2022, 14, 1661. [Google Scholar] [CrossRef] [PubMed]
- Leger, D.; Andler, R.; Richard, J.; Nguyen-Thanh, V.; Collin, O.; Chennaoui, M.; Metlaine, A. Sleep, substance misuse and addictions: a nationwide observational survey on smoking, alcohol, cannabis and sleep in 12,637 adults. J. Sleep Res. 2022, 31, e13553. [Google Scholar] [CrossRef] [PubMed]
- Hussain, J.; Ling, L.; Alonzo, R.T.; Rodrigues, R.; Nicholson, K.; Stranges, S.; Anderson, K.K. Associations between sleep patterns, smoking, and alcohol use among older adults in Canada: Insights from the Canadian Longitudinal Study on Aging (CLSA). Addict. Behav. 2022, 132, 107345. [Google Scholar] [CrossRef] [PubMed]
- Palmer, C.; Harrison, G.; Hiorns, R. Association between smoking and drinking and sleep duration. Ann. Hum. Biol. 1980, 7, 103–107. [Google Scholar] [CrossRef]
- Bahammam, A.S.; Manzar, M.; Salahuddin, M.; Alamri, M.; Maru, T.T.; Pandi-Perumal, S.R. Poor sleep in concurrent users of alcohol, khat, and tobacco smoking in community-dwelling Ethiopian adults. Ann. Thorac. Med. 2018, 13, 220–225. [Google Scholar] [CrossRef]
- Masood, S.; Cappelli, C.; Li, Y.; Tanenbaum, H.; Chou, C.-P.; Spruijt-Metz, D.; Palmer, P.H.; Johnson, C.A.; Xie, B. Cigarette smoking is associated with unhealthy patterns of food consumption, physical activity, sleep impairment, and alcohol drinking in Chinese male adults. Int. J. Public Heal. 2015, 60, 891–899. [Google Scholar] [CrossRef] [PubMed]
- Chang, L.-Y.; Chang, H.-Y.; Wu, W.-C.; Lin, L.N.; Wu, C.-C.; Yen, L.-L. Dual Trajectories of Sleep Duration and Cigarette Smoking during Adolescence: Relation to Subsequent Internalizing Problems. J. Abnorm. Child Psychol. 2018, 46, 1651–1663. [Google Scholar] [CrossRef] [PubMed]
- Sabatier, T.; Kousignian, I.; Gomajee, R.; Barry, K.; Melchior, M.; Mary-Krause, M. Association between Sleep Disturbances During Childhood and Smoking Trajectories During Adulthood: The Longitudinal TEMPO Cohort Study. Behav. Sleep Med. 2022, 21, 556–569. [Google Scholar] [CrossRef] [PubMed]
- Oshri, A.; Kogan, S.; Liu, S.; Sweet, L.; Mackillop, J. Pathways Linking Adverse Childhood Experiences to Cigarette Smoking Among Young Black Men: a Prospective Analysis of the Role of Sleep Problems and Delayed Reward Discounting. Ann. Behav. Med. 2017, 51, 890–898. [Google Scholar] [CrossRef]
- Patterson, F.; Grandner, M.A.; Lozano, A.; Satti, A.; Ma, G. Transitioning from adequate to inadequate sleep duration associated with higher smoking rate and greater nicotine dependence in a population sample. Addict. Behav. 2018, 77, 47–50. [Google Scholar] [CrossRef] [PubMed]
- Hamidovic, A.; de Wit, H. Sleep deprivation increases cigarette smoking. Pharmacol. Biochem. Behav. 2009, 93, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Kageyama, T.; Kobayashi, T.; Nishikido, N.; Oga, J.; Kawashima, M. Associations of Sleep Problems and Recent Life Events with Smoking Behaviors among Female Staff Nurses in Japanese Hospitals. Ind. Heal. 2005, 43, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Nair, U.S.; Haynes, P.; Collins, B.N. Baseline sleep quality is a significant predictor of quit-day smoking self-efficacy among low-income treatment-seeking smokers. J. Heal. Psychol. 2017, 24, 1484–1493. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Bo, Q.-G.; Jia, C.-X.; Liu, X. Sleep Problems in Relation to Smoking and Alcohol Use in Chinese Adolescents. J. Nerv. Ment. Dis. 2017, 205, 353–360. [Google Scholar] [CrossRef]
- Fillo, J.; Alfano, C.A.; Paulus, D.J.; Smits, J.A.; Davis, M.L.; Rosenfield, D.; Marcus, B.H.; Church, T.S.; Powers, M.B.; Otto, M.W.; et al. Emotion dysregulation explains relations between sleep disturbance and smoking quit-related cognition and behavior. Addict. Behav. 2016, 57, 6–12. [Google Scholar] [CrossRef]
- Kim, K.S.; Kim, J.H.; Park, S.Y.; Won, H.-R.; Lee, H.-J.; Yang, H.S.; Kim, H.J. Smoking Induces Oropharyngeal Narrowing and Increases the Severity of Obstructive Sleep Apnea Syndrome. J. Clin. Sleep Med. 2012, 8, 367–374. [Google Scholar] [CrossRef]
- Dülger, S.; Çapkur, .; Gençay, S.; Özmen, S.; Solmaz, F.; Dikiş, ..; Yıldız, T. The Relationship Between Nasal Mucociliary Clearance Time and the Degree of Smoking Dependence in Smokers with Obstructive Sleep Apnea Syndrome. Adv. Respir. Med. 2021, 89, 353–358. [Google Scholar] [CrossRef]
- Virkkula, P.; Bachour, A.; Hytönen, M.; Malmberg, H.; Salmi, T.; Maasilta, P. Patient- and Bed Partner-Reported Symptoms, Smoking, and Nasal Resistance in Sleep-Disordered Breathing. Chest 2005, 128, 2176–2182. [Google Scholar] [CrossRef]
- Jang, Y.S.; Nerobkova, N.; Hurh, K.; Park, E.-C.; Shin, J. Association between smoking and obstructive sleep apnea based on the STOP-Bang index. Sci. Rep. 2023, 13, 1–10. [Google Scholar] [CrossRef]
- Zhang, Q.; Yang, Z.-W.; He, Q.-Y.; Xing, Z.-L.; Pang, G.-F.; Wu, R.-Q.; Yang, L.-Y.; Sun, L.-X.; Han, F.; Wang, Y.; et al. [Epidemiologic study on the relationship between smoking and sleep apnea/hypopnea syndrome]. . 2007, 28, 841–3. [Google Scholar]
- Wetter, D.W.; Young, T.B.; Bidwell, T.R.; Badr, M.S.; Palta, M. Smoking as a risk factor for sleep-disordered breathing. 1994, 154, 2219–24. [Google Scholar] [CrossRef]
- Kashyap, R.; Hock, L.M.; Bowman, T.J. Higher Prevalence of Smoking in Patients Diagnosed as Having Obstructive Sleep Apnea. Sleep Breath. 2001, 5, 167–172. [Google Scholar] [CrossRef]
- Cohen, O.; Strizich, G.M.; Ramos, A.R.; Zee, P.C.; Reid, K.J.; Mani, V.; Rapoport, D.M.; Redline, S.; Kaplan, R.C.; Shah, N.A. Sex Differences in the Association Between Smoking and Sleep-Disordered Breathing in the Hispanic Community Health Study/Study of Latinos. Chest 2019, 156, 944–953. [Google Scholar] [CrossRef] [PubMed]
- Esen, A.D.; Akpinar, M. Relevance of obstructive sleep apnea and smoking: Obstructive sleep apnea and smoking. Fam. Pr. 2020, 38, 180–185. [Google Scholar] [CrossRef] [PubMed]
- Oțelea, M.R.; Trenchea, M.; Rașcu, A.; Antoniu, S.; Zugravu, C.; Busnatu, .; Simionescu, A.A.; Arghir, O.C. Smoking Obstructive Sleep Apnea: Arguments for a Distinctive Phenotype and a Personalized Intervention. J. Pers. Med. 2022, 12, 293. [Google Scholar] [CrossRef] [PubMed]
- Varol, Y.; Anar, C.; Tuzel, O.E.; Guclu, S.Z.; Ucar, Z.Z. The impact of active and former smoking on the severity of obstructive sleep apnea. Sleep Breath. 2015, 19, 1279–1284. [Google Scholar] [CrossRef] [PubMed]
- Bielicki, P.; Trojnar, A.; Sobieraj, P.; Wąsik, M. Smoking Status in Relation to Obstructive Sleep Apnea Severity (OSA) And Cardiovascular Comorbidity in Patients with Newly Diagnosed OSA. Adv. Respir. Med. 2019, 87, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Boussoffara, L.; Boudawara, N.; Sakka, M.; Knani, J. Tabagisme et sévérité du syndrome d’apnées hypopnées obstructives du sommeil. Rev. des Mal. Respir. 2013, 30, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Porebska, I.; Kosacka, M.; Choła, J.; Gładka, A.; Wnek, P.; Brzecka, A. [Smoking among patients with obstructive sleep apnea syndrome--preliminary report]. . 2014, 37, 265–8. [Google Scholar] [PubMed]
- Shao, C.; Qi, H.; Fang, Q.; Tu, J.; Li, Q.; Wang, L. Smoking history and its relationship with comorbidities in patients with obstructive sleep apnea. Tob. Induc. Dis. 2020, 18, 56. [Google Scholar] [CrossRef] [PubMed]
- Mauries, S.; Bertrand, L.; Frija-Masson, J.; Benzaquen, H.; Kalamarides, S.; Sauvage, K.; Lejoyeux, M.; D’ortho, M.-P.; Geoffroy, P.A. Effects of smoking on sleep architecture and ventilatory parameters including apneas: Results of the Tab-OSA study. Sleep Med. X 2023, 6. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Li, W.; Zhou, J.; Wei, Z.; Li, X.; Xu, J.; Zhang, F.; Wang, W. Smoking and sleep apnea duration mediated the sex difference in daytime sleepiness in OSA patients. Sleep Breath. 2021, 25, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Casasola, G.G.; Tashkin, D.P.; Álvarez-Sala, J.L.; Marques, J.A.; Sánchez-Alarcos, J.M.F.; Espinós, D. Cigarette Smoking Behavior and Respiratory Alterations During Sleep in a Healthy Population. Sleep Breath. 2002, 6, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Conway, S.; Roizenblatt, S.; Palombini, L.; Castro, L.; Bittencourt, L.; Silva, R.; Tufik, S. Effect of smoking habits on sleep. Braz. J. Med Biol. Res. 2008, 41, 722–727. [Google Scholar] [CrossRef]
- Hoflstein, V. Relationship between smoking and sleep apnea in clinic population. Sleep. 2002 Aug 1;25(5):519-24.
- Ben Amar, J.; Ben Mansour, A.; Zaibi, H.; Ben Safta, B.; Dhahri, B.; Aouina, H. Impact of smoking on the severity of Obstructive Sleep Apnea Hypopnea Syndrome. . 2018, 96, 477–482. [Google Scholar]
- Suzgun, M.A.; Kabeloglu, V.; Senel, G.B.; Karadeniz, D. Smoking Disturbs the Beneficial Effects of Continuous Positive Airway Pressure Therapy on Leptin Level in Obstructive Sleep Apnea. J. Obes. Metab. Syndr. 2023, 32, 338–345. [Google Scholar] [CrossRef] [PubMed]
- 华, .; 红, .; 建, .; 建, .; 华, .; 玉, . 吸烟对OSA患者术后糖脂代谢及睡眠结构的影响. 2021, 35, 146–151. [CrossRef]
- Yang, Y.; Wu, J.; Li, S.; Yu, W.; Zhu, H.; Wang, Y.; Li, Y. Smoking, Coffee Consumption, Alcohol Intake, and Obstructive Sleep Apnea: A Mendelian Randomization Study. Curr. Neurovascular Res. 2023, 20, 280–289. [Google Scholar] [CrossRef] [PubMed]
- Ilgin, V.E.; Yayla, A.; Ozlu, Z.K.; Ozlu, I.; Toraman, R.L.; Toraman, M.M. Pain, Sleep Disturbance and Smoking Among Patients with Covid-19 Presenting to the Emergency Department. Florence Nightingale J. Nurs. 2022, 31, 48–55. [Google Scholar] [CrossRef]
- Stipelman, B.A.; Augustson, E.; McNeel, T. The relationship among smoking, sleep, and chronic rheumatic conditions commonly associated with pain in the national health interview survey. J. Behav. Med. 2012, 36, 539–548. [Google Scholar] [CrossRef] [PubMed]
- Fucito, L.M.; Redeker, N.S.; Ball, S.A.; Toll, B.A.; Ikomi, J.T.; Carroll, K.M. Integrating a Behavioural Sleep Intervention into Smoking Cessation Treatment for Smokers with Insomnia: A Randomised Pilot Study. J. Smok. Cessat. 2013, 9, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Riedel, B.W.; Durrence, H.H.; Lichstein, K.L.; Taylor, D.J.; Bush, A.J. The Relation Between Smoking and Sleep: The Influence of Smoking Level, Health, and Psychological Variables. Behav. Sleep Med. 2004, 2, 63–78. [Google Scholar] [CrossRef] [PubMed]
- Kazi, S.E.; Mohammed, J.M.M.; Schenck, C.H. Sleepwalking, sleep-related eating disorder and sleep-related smoking successfully treated with topiramate: a case report. Sleep Sci. 2022, 15, 370–373. [Google Scholar] [CrossRef] [PubMed]
- O’callaghan, F.; O’callaghan, M.; Scott, J.G.; Najman, J.; Al Mamun, A. Effect of maternal smoking in pregnancy and childhood on child and adolescent sleep outcomes to 21 years: a birth cohort study. BMC Pediatr. 2019, 19, 70. [Google Scholar] [CrossRef] [PubMed]
- Yahia, N.; Brown, C.; Potter, S.; Szymanski, H.; Smith, K.; Pringle, L.; Herman, C.; Uribe, M.; Fu, Z.; Chung, M.; et al. Night eating syndrome and its association with weight status, physical activity, eating habits, smoking status, and sleep patterns among college students. Eat. Weight. Disord. - Stud. Anorexia, Bulim. Obes. 2017, 22, 421–433. [Google Scholar] [CrossRef]
- Kaneita, Y.; Ohida, T.; Takemura, S.; Sone, T.; Suzuki, K.; Miyake, T.; Yokoyama, E.; Umeda, T. Relation of smoking and drinking to sleep disturbance among Japanese pregnant women. Prev. Med. 2005, 41, 877–882. [Google Scholar] [CrossRef] [PubMed]
- Ahlberg, J.; Lobbezoo, F.; Hublin, C.; Piirtola, M.; Kaprio, J. Smoking cessation is not associated with a decline in reported sleep bruxism in middle-aged Finnish twins: Data revisited. J. Oral Rehabilitation 2023, 51, 117–118. [Google Scholar] [CrossRef] [PubMed]
- Prosise, G.L.; Bonnet, M.H.; Berry, R.B.; Dickel, M.J. Effects of Abstinence From Smoking on Sleep and Daytime Sleepiness. Chest 1994, 105, 1136–1141. [Google Scholar] [CrossRef] [PubMed]
- Pataka, A.; Frantzidis, C.; Kalamaras, G.; Gkivogkli, P.; Kotoulas, S.; Nday, C.; Chriskos, P.; Karagianni, M.; Styliadis, C.; Paraskevopoulos, E.; et al. Varenicline administration for smoking cessation may reduce apnea hypopnea index in sleep apnea patients. Sleep Med. 2021, 88, 87–89. [Google Scholar] [CrossRef] [PubMed]
- Staner, L.; Luthringer, R.; Dupont, C.; Aubin, H.; Lagrue, G. Sleep effects of a 24-h versus a 16-h nicotine patch: A polysomnographic study during smoking cessation. Sleep Med. 2006, 7, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Sawnani, H.; Jackson, T.; Murphy, T.; Beckerman, R.; Simakajornboon, N. The Effect of Maternal Smoking on Respiratory and Arousal Patterns in Preterm Infants during Sleep. Am. J. Respir. Crit. Care Med. 2004, 169, 733–738. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.; Colodner, R.; Masalha, R.; Haimov, I. The Relationship Between Tobacco Smoking, Cortisol Secretion, and Sleep Continuity. Subst. Use Misuse 2019, 54, 1705–1714. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Samet, J.; Caffo, B.; Punjabi, N.M. Cigarette Smoking and Nocturnal Sleep Architecture. Am. J. Epidemiology 2006, 164, 529–537. [Google Scholar] [CrossRef] [PubMed]
- Aubin, H.; Luthringer, R.; Demazières, A.; Dupont, C.; Lagrue, G. Comparison of the effects of a 24-hour nicotine patch and a 16-hour nicotine patch on smoking urges and sleep. Nicotine Tob. Res. 2006, 8, 193–201. [Google Scholar] [CrossRef]
- Salin-Pascual, R.J. Relationship between mood improvement and sleep changes with acute nicotine administration in non-smoking major depressed patients. . 2002, 54, 36–40. [Google Scholar]
- Stéphan-Blanchard, E.; Telliez, F.; Léké, A.; Djeddi, D.; Bach, V.; Libert, J.-P.; Chardon, K. The Influence of In Utero Exposure to Smoking on Sleep Patterns in Preterm Neonates. Sleep 2008, 31, 1683–1689. [Google Scholar] [CrossRef] [PubMed]
- Djeddi, D.; Stephan-Blanchard, E.; Léké, A.; Ammari, M.; Delanaud, S.; Lemaire-Hurtel, A.-S.; Bach, V.; Telliez, F. Effects of Smoking Exposure in Infants on Gastroesophageal Reflux as a Function of the Sleep–Wakefulness State. J. Pediatr. 2018, 201, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Aldahash, F.D.; Alasmari, S.A.; Alnomsi, S.J.; Alshehri, A.M.; Alharthi, N.F.; Aloufi, A.A.H.; Al Atawi, M.S.; Alotaibi, A.A.; Mirghani, H.O. Relationship of body mass index to sleep duration, and current smoking among medical students in Tabuk City, Saudi Arabia. Electron. Physician 2018, 10, 7273–7278. [Google Scholar] [CrossRef] [PubMed]
- Aksu, K.; Güven, S.F.; Aksu, F.; Ciftci, B.; Ciftci, T.U.; Aksaray, S.; Şipit, T.; Peker, Y. Obstructive Sleep Apnoea, Cigarette Smoking and Plasma Orexin-A in a Sleep Clinic Cohort. J. Int. Med Res. 2009, 37, 331–340. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Gong, S.; Xu, C.; Zhou, J.Y.; Wang, K.-S. Sleep duration and smoking are associated with coronary heart disease among US adults with type 2 diabetes: Gender differences. Diabetes Res. Clin. Pr. 2016, 124, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Donovan, L.M.; Feemster, L.C.; Billings, M.E.; Spece, L.J.; Griffith, M.F.; Rise, P.J.; Parsons, E.C.; Palen, B.N.; O'Hearn, D.J.; Redline, S.; et al. Risk of Cardiovascular Disease Related to Smoking Is Greater Among Women With Sleep-Disordered Breathing. J. Clin. Sleep Med. 2018, 14, 1929–1935. [Google Scholar] [CrossRef] [PubMed]
- Lavie, L.; Lavie, P. Smoking interacts with sleep apnea to increase cardiovascular risk. Sleep Med. 2007, 9, 247–253. [Google Scholar] [CrossRef]
- Costa Filho, A.M.; Mambrini, J.V.M.; Malta, D.C.; Lima-Costa, M.F.; Peixoto, S.V. Contribution of chronic diseases to the prevalence of disability in basic and instrumental activities of daily living in elderly Brazilians: the National Health Survey (2013). Cad. Saúde Pública 2018, 34, e00204016. [Google Scholar] [CrossRef] [PubMed]
- Blazejová, K.; Sonka, K.; Skodová, Z.; Nevsímalová, S. [Prevalence of obesity, hypertension and smoking in patients with the sleep apnea syndrome--comparison with the Czech population]. . 2000, 139, 339–42. [Google Scholar]
- Özkan, E.; Celik, Y.; Yucel-Lindberg, T.; Peker, Y. Current Smoking Determines the Levels of Circulating MPO and MMP-9 in Adults with Coronary Artery Disease and Obstructive Sleep Apnea. J. Clin. Med. 2023, 12, 4053. [Google Scholar] [CrossRef]
- Lui, M.M.S.; Mak, J.C.W.; Lai, A.Y.K.; Hui, C.K.M.; Lam, J.C.M.; Lam, D.C.L.; Ip, M.S.M. The Impact of Obstructive Sleep Apnea and Tobacco Smoking on Endothelial Function. Respiration 2016, 91, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Javaheri, S.; Shukla, R.; Wexler, L. Association of Smoking, Sleep Apnea, and Plasma Alkalosis With Nocturnal Ventricular Arrhythmias in Men With Systolic Heart Failure. Chest 2012, 141, 1449–1456. [Google Scholar] [CrossRef] [PubMed]
- Wada, K.; Mizuguchi, Y.; Wada, Y.; Ohno, Y.; Iino, Y. Hyperlipidaemia, lack of sleep and smoking as risk factors for proteinuria among high altitude mountain trekkers. Nephrology 2006, 11, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Kirbas, G.; Abakay, A.; Topcu, F.; Kaplan, A.; Ünlu, M.; Peker, Y. Obstructive Sleep Apnoea, Cigarette Smoking and Serum Testosterone Levels in a Male Sleep Clinic Cohort. J. Int. Med Res. 2007, 35, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Mikolasevic, I.; Domislovic, V.; Kanizaj, T.F.; Radic-Kristo, D.; Krznaric, Z.; Milovanovic, T.; Juric, T.; Klapan, M.; Skenderevic, N.; Delija, B.; et al. Relationship between coffee consumption, sleep duration and smoking status with elastographic parameters of liver steatosis and fibrosis; controlled attenuation parameter and liver stiffness measurements. Int. J. Clin. Pract. 2020, 75, e13770. [Google Scholar] [CrossRef]
- Custodio, L.; Carlson, C.R.; Upton, B.; Okeson, J.P.; Harrison, A.L.; de Leeuw, R. The Impact of Cigarette Smoking on Sleep Quality of Patients with Masticatory Myofascial Pain. J. Oral Facial Pain Headache 2015, 29, 15–23. [Google Scholar] [CrossRef]
- Patterson, F.; Connick, E.; Brewer, B.; Grandner, M.A. HIV status and sleep disturbance in college students and relationship with smoking. Sleep Heal. 2019, 5, 395–400. [Google Scholar] [CrossRef]
- Kokubun, K.; Pineda, J.C.D.; Yamakawa, Y. Unhealthy lifestyles and brain condition: Examining the relations of BMI, living alone, alcohol intake, short sleep, smoking, and lack of exercise with gray matter volume. PLOS ONE 2021, 16, e0255285. [Google Scholar] [CrossRef]
- Ni Lin, Y.; Na Zhou, L.; Zhang, X.J.; Li, Q.Y.; Wang, Q.; Xu, H.J. Combined effect of obstructive sleep apnea and chronic smoking on cognitive impairment. Sleep Breath. 2015, 20, 51–59. [Google Scholar] [CrossRef]
- Nakamura, M.; Aoki, N.; Nakashima, T.; Hoshino, T.; Yokoyama, T.; Morioka, S.; Kawamura, T.; Tanaka, H.; Hashimoto, T.; Ohno, Y.; et al. Smoking, Alcohol, Sleep and Risk of Idiopathic Sudden Deafness: A Case-Control Study Using Pooled Controls. J. Epidemiology 2001, 11, 81–86. [Google Scholar] [CrossRef]
- Hahad, O.; Beutel, M.; Gilan, D.A.; Michal, M.; Schulz, A.; Pfeiffer, N.; König, J.; Lackner, K.; Wild, P.; Daiber, A.; et al. The association of smoking and smoking cessation with prevalent and incident symptoms of depression, anxiety, and sleep disturbance in the general population. J. Affect. Disord. 2022, 313, 100–109. [Google Scholar] [CrossRef] [PubMed]
- Miadich, S.A.; Everhart, R.S.; Heron, K.E.; Cobb, C.O. Medication use, sleep, and caregiver smoking status among urban children with asthma. J. Asthma 2017, 55, 588–595. [Google Scholar] [CrossRef]
- Mat, D. .; Firat, S.; Aksu, K.; Aksu, F.; Duyar, S.. Obstructive sleep apnea is a determinant of asthma control independent of smoking, reflux, and rhinitis. Allergy Asthma Proc. 2021, 42, e25–e29. [Google Scholar] [CrossRef]
- Yu, L.; Liu, L.; Xiang, Y.; Wang, F.; Zhou, F.; Huang, S.; Zheng, C.; Ye, C.; Zhou, W.; Yin, G.; et al. XRCC5/6 polymorphisms and their interactions with smoking, alcohol consumption, and sleep satisfaction in breast cancer risk: A Chinese multi-center study. Cancer Med. 2021, 10, 2752–2762. [Google Scholar] [CrossRef] [PubMed]
- Teni, M.T.; Loux, T.; Kuhlmann, A.S. Racial disparity in gestational diabetes mellitus and the association with sleep-disordered breathing and smoking cigarettes: a cross-sectional study. J. Matern. Neonatal Med. 2022, 35, 10601–10607. [Google Scholar] [CrossRef] [PubMed]
- Ohida, T.; Kaneita, Y.; Osaki, Y.; Harano, S.; Tanihata, T.; Takemura, S.; Wada, K.; Kanda, H.; Hayashi, K.; Uchiyama, M. Is Passive Smoking Associated With Sleep Disturbance Among Pregnant Women? Sleep 2007, 30, 1155–1161. [Google Scholar] [CrossRef] [PubMed]
- Stone, K.C. Postpartum Behavioral Sleep Intervention for Smoking Relapse Prevention: A Pilot Trial. Matern. Child Heal. J. 2023, 27, 272–285. [Google Scholar] [CrossRef] [PubMed]
- Hannan, K.E.; Smith, R.A.; Barfield, W.D.; Hwang, S.S. Association between Neonatal Intensive Care Unit Admission and Supine Sleep Positioning, Breastfeeding, and Postnatal Smoking among Mothers of Late Preterm Infants. J. Pediatr. 2020, 227, 114–120. [Google Scholar] [CrossRef] [PubMed]
- Horne, R.S.C.; Ferens, D.; Watts, A.-M.; Vitkovic, J.; Lacey, B.; Andrew, S.; Cranage, S.M.; Chau, B.; Greaves, R.; Adamson, T.M. Effects of maternal tobacco smoking, sleeping position, and sleep state on arousal in healthy term infants. Arch. Dis. Child. - Fetal Neonatal Ed. 2002, 87, 100F–105. [Google Scholar] [CrossRef]
- Nelson, E.; Taylor, B. International Child Care Practices Study: infant sleep position and parental smoking. Early Hum. Dev. 2001, 64, 7–20. [Google Scholar] [CrossRef]
- E Anderson, M.; Johnson, D.C.; A Batal, H. Sudden Infant Death Syndrome and prenatal maternal smoking: rising attributed risk in the Back to Sleepera. BMC Med. 2005, 3, 4–4. [Google Scholar] [CrossRef] [PubMed]
- Tirosh, E.; Libon, D.; Bader, D. The effect of maternal smoking during pregnancy on sleep respiratory and arousal patterns in neonates. . 1996, 16, 435–8. [Google Scholar] [PubMed]
- Peltier, M.R.; Lee, J.; Ma, P.; Businelle, M.S.; Kendzor, D.E. The influence of sleep quality on smoking cessation in socioeconomically disadvantaged adults. Addict. Behav. 2017, 66, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Rapp, K.; Buechele, G.; Weiland, S.K. Sleep duration and smoking cessation in student nurses. Addict. Behav. 2007, 32, 1505–1510. [Google Scholar] [CrossRef] [PubMed]
- Farris, S.G.; Matsko, S.V.; Uebelacker, L.A.; Brown, R.A.; Price, L.H.; Abrantes, A.M. Anxiety sensitivity and daily cigarette smoking in relation to sleep disturbances in treatment-seeking smokers. Cogn. Behav. Ther. 2019, 49, 137–148. [Google Scholar] [CrossRef] [PubMed]
- Arzi, A.; Holtzman, Y.; Samnon, P.; Eshel, N.; Harel, E.; Sobel, N. Olfactory Aversive Conditioning during Sleep Reduces Cigarette-Smoking Behavior. J. Neurosci. 2014, 34, 15382–15393. [Google Scholar] [CrossRef]
- Okun, M.L.; Levine, M.D.; Houck, P.; Perkins, K.A.; Marcus, M.D. Subjective sleep disturbance during a smoking cessation program: Associations with relapse. Addict. Behav. 2011, 36, 861–864. [Google Scholar] [CrossRef] [PubMed]
- Ashare, R.L.; Lerman, C.; Tyndale, R.F.; Hawk, L.W.; George, T.P.; Cinciripini, P.; Schnoll, R.A. Sleep Disturbance During Smoking Cessation: Withdrawal or Side Effect of Treatment? J. Smok. Cessat. 2016, 12, 63–70. [Google Scholar] [CrossRef]
- Wolter, T.D.; Hauri, P.J.; Schroeder, D.R.; Wisbey, J.A.; Croghan, I.T.; Offord, K.P.; Dale, L.C.; Hurt, R.D. Effects of 24-hr nicotine replacement on sleep and daytime activity during smoking cessation. Prev. Med. 1996, 25, 601–610. [Google Scholar] [CrossRef]
Figure 1.
Flow diagram of study selection progress.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



