
Submitted:
19 June 2024
Posted:
19 June 2024
You are already at the latest version
Abstract
Diarrhea is a common occurrence following vascular organ transplantation, including kidney transplants. It can be induced by non-infectious factors, adverse effects of immunosuppressive drugs, or infectious agents such as viruses, bacteria, fungi, or parasites. Intestinal protozoan parasites, include Cryptosporidium spp., are causes of infectious diarrhea particularly in immunocompromised patients. This review aims to summarize reports on epidemiology, pathogenesis, clinical presentation, diagnosis, and treatment of Cryptosporidium spp. infection in adult patients, particularly following kidney transplantation.
Keywords:
Cryptosporidium spp.
; kidney transplantation
1. Introduction
In recent years, there has been significant improvement in the survival of kidney transplant recipients due to the prevention of acute rejection through immunosuppressive therapy. However, immunosuppressive treatment can lead to immune impairment, potentially resulting in opportunistic infections, including bacterial, viral, fungal, and parasitic infections. Protozoan pathogens, such as Entamoeba histolytica, Giardia duodenalis, Cyclospora spp., Cystoisospora spp., microsporidia such as Enterocytozoon bieneusi, and Cryptosporidium spp., are well-known causes of diarrhea and pose a major public health concern in developing countries [1]. Cryptosporidium spp. infection is identified as the second leading cause of diarrhea worldwide after rotavirus infection [2]. Deltombe et al. [3] found that the mean onset delay of Cryptosporidium spp. infection was 40.5 months post-transplantation.
Diarrhea is common after kidney transplantion, occurring in 10%-50% of patients [4]. It has been observed that diarrhea associated with immunosuppressive therapy is more prevalent in the early post-transplant period due to the administration of multiple drugs, often in higher doses. Conversely, infectious diarrhea tends to manifest several years after transplantation [5]. This review describes the epidemiology, pathogenesis, clinical presentation, diagnosis, and treatment of Cryptosporidium spp. infection in adult patients, particularly following kidney transplantation. The review is based on scientific articles sourced from validated databases such as PubMed and the National Centre for Biotechnology Information (NCBI), using keywords ‘Cryptosporidium’ AND ‘cryptosporidiosis’ AND ‘kidney’ AND ‘transplant’. Inclusion criteria encompassed human studies, in vitro animal studies, case reports, peer-reviewed journal publications, review articles, and research articles in English. Exclusion criteria included studies not in the English language, gray literature (e.g., conference proceedings and abstracts), and data related to pediatric patients.
2. Epidemiology of Cryptosporidium spp.
The coccidian protozoan Cryptosporidium spp. is an opportunistic intestinal parasite in vertebrate animals. Cryptosporidium infection has been documented in amphibians, reptiles, poultry, and mammals, including humans [6]. More than 40 Cryptosporidium species with over 60 valid genotypes have been identified [7]. Cryptosporidium spp. is recognized as an emerging protozoan parasite by the Centers for Disease Control and Prevention (CDC) [8]. Most human infections are caused by Cryptosporidium parvum, which infects both humans and ruminants, and C. hominis, infects humans and pigs [9]. Cases of cryptosporidiosis caused by other species and genotypes have also been reported. These include C. meleagridis, C. felis, C. canis, C. cuniculus, C. ubiquitum, C. viatorum, C. muris, C. suis, C. fayeri, C. andersoni, C. bovis, C. scrofarum, C. tyzzeri, C. erinacei, and Cryptosporidium horse, skunk, and chipmunk I genotypes [10]. Cryptosporidiosis has been documented in over 40 countries across six continents, affecting both immunocompetent and immunocompromised patients [11]. Cryptosporidium spp. infection is frequently observed in the immunosuppressed patients, including patients with HIV/AIDS, undergoing chemotherapy, or solid organ transplantation (SOT). Based on scientific data, the global prevalence of cryptosporidiosis is 7.6% [10]. The frequency of Cryptosporidium spp. infection depending on study design, area study, population group, sensitivity and and specificity of laboratory methods [12]. The prevalence of Cryptosporidium spp. in Europe and North America is 1%-3% and 5%-10% in Asia and Africa [13]. Several waterborne outbraks of cryptosporidiosis have been documented, with the largest reported in Milwaukee, Wisconsin (USA) in 1993, caused by Cryptosporidium oocysts that passed through the filtration system of one of two water treatment plants [14]. Over 400,000 people were affected by waterborne outbreak of cryptosporidiosis, including 100 immunocompromised patients.
3. Cryptosporidiosis
Cryptosporidium infection may be asymptomatic and self-limiting, which may contribute to its low detectability. In cases of asymptomatic infection, Cryptosporidium spp. has been found in the distal parts of the small intestine and proximal parts of the colon [15]. Cryptosporidium infection of the gastrointestinal tract is most common, respiratory cryptosporidiosis occurring much less frequently. The severity of the disease in immunosuppressed patients, including kidney transplant recipients, can be influenced by host factors such as age and nutritional status, as well as the species and subtype of Cryptosporidium spp. [16]. It has been observed that a CD4+ T-cell count of <200/mm3 increases the risk of prolonged infection, while counts of <100/mm3 may lead to severe, life-threatening diarrhea [17]. Symptoms of cryptosporidiosis commonly appear 1-14 days (average 7 days) post infection (dpi) and persist up to 6-9 dpi [18]. However, some patients may experience symptoms for up to 100-120 days [19]. Cryptosporidium spp. infected patients excrete oocysts in feces for an average of 7 days (1-15 days) after discontinuation of symptoms, exceptionally, up to 2 months [20]. The most common symptom of cryptosporidiosis is severe watery diarrhea (up to 10 times a day), sometimes with mucus. Immunocompetent patients usually experience a self-limiting illness, while immunosuppressed patients, especially those with T-cell deficiency, often develop chronic and severe cryptosporidiosis with a risk of extra-intestinal disease development [21]. The pathophysiology of diarrhea in Cryptosporidium spp. infection remains unclear. It is suggested to be a combination of malabsorption and secretory diarrhea secondary to mucosal attachment, distortion of villous architecture, epicellular infection, inflammatory response, and cellular apoptosis [22]. In renal transplant patients, post-transplant cryptosporidiosis with diarrhea is a common complication [23]. Some researchers argue that in renal transplant recipients, cryptosporidiosis does not appear to be unusually severe or involve extraintestinal sites [24,25]. In the study by Deltombe et al. [3], cryptosporidiosis in renal transplant patients occurred at a mean time of 33.9 months, suggesting that patients were likely infected but asymptomatic prior to transplantation. Patients may also experience nausea, fever, vomiting, abdominal pain, anorexia, dehydration, weight loss (3.6±2.4 kg), and acute transplant dysfunction [3,26]. Immunocompromised patients may experience muscle pain, weakness, fatigue, malaise, headache, or anorexia [27]. Respiratory tract infection by Cryptosporidium spp. has been described for immunodeficient patients. The upper respiratory cryptosporidiosis may cause inflammation of the the nasal mucosa, sinuses, larynx, and trachea, accompanied by nasal discharge and voice changes, while lower respiratory cryptosporidiosis manifests as productive cough, dyspnea, fever, and hypoxemia [28]. Radiological changes visible in the lungs in the form of ground-glass opacities have also been observed. In most patients oocysts have been detected in both saliva and feces [29,30]. However, there is a lack of scientific literature on respiratory cryptosporidiosis in kidney transplant recipients. In immunodeficient patients Cryptosporidium infection may present multiple organ involvement. Generalized cryptosporidiosis has been described, among others, in an HIV-infected patient after kidney transplantation. The development of this form is facilitated by a high number of oocysts in the host’s body [31]. In autopsy, material collected from immunodifiencet patient with generalized cryptosporidiosis caused by C. baileyi oocysts have been found in the esophagus, entire intestine, trachea, larynx, lungs, and gall and urinary bladders [32]. Recurrence of cryptosporidiosis symptoms in immunocompromised patients may occur even after treatment due to inadequate eradication (incorrect medication or dosage). This is caused by incomplete pathogen eradication, especially from the bile ducts, and maintenance of infection in the latent stage. Unrecognized cryptosporidiosis in immunocompromised patients can lead to debilitating diarrhea, epithelial infection of the bile ducts, gastritis, pancreatitis, primary sclerosing cholangitis, bile duct inflammation or cancer, and cirrhosis [12]. Cryptosporidiosis-associated biliary tract inflammation is a particularly serious clinical complication in AIDS patients. Symptoms include abdominal pain, fever, and jaundice. Patients exhibit increased alkaline phosphatase activity in serum and significant anatomical damage to the biliary system [15]. de Souza et al. [33] descrived a cryptosporidiosis of the biliary tract clinically mimicking a pancreatic cancer in an AIDS patient. In addition, Cryptosporidium spp. can cause malignant cancers in the gastrointestinal tract [34]. The type of immunosuppressants used in kidney transplant patients may influence the course of cryptosporidiosis (Table 1). It has been shown that patients using a tacrolimus-based regimen are at greater risk of Cryptosporidium spp. infection compared with a cyclosporine-based regimen [35]. In patients receiving tacrolimus with confirmed Cryptosporidium spp. infection, renal graft dysfunction is more common, possibly due to dehydration and increased tacrolimus concentration [36,37]. In patients receiving tacrolimus with diarrhea, blood levels of this drug should be assessed. Diarrhea, regardless of etiology, increases exposure to tacrolimus, which has a narrow therapeutic index. Elevated drug levels, combined with dehydration, can lead to graft dysfunction [38].
Cryptosporidiosis in Immunocompromised Patients
The National Reference Center in France between 2017 and 2019 reported that 40% of cases notified with cryptosporidiosis with documented immune status occurred in immunodeficient patients, including 53% in solid organ transplant recipients [39]. The majority of data regarding the prevalence of cryptosporidiosis in organ transplant recipients pertains to renal transplant patients. The prevalence of the Cryptosporidium spp. infections in adult kidney transplant recipients was 1.7%-53% (Table 1).
Cryptosporidium spp. infection is restricted to the epithelial cells of the small intestine, with the parasite primarily confined to the apical brush border. The infection, particularly in immunosuppressed patients, can also affect the pharynx, esophagus, stomach, appendix, colon and rectum, gallbladder and pancreatic ducts [45,48]. Cryptosporidium spp. have been reported in respiratory system mucosa, particularly patients infected by HIV or following bone marrow transplantation, as a complication of gastrointestinal infection [12,28,49,50]. The monoxenous life cycle of Cryptosporidium spp. consisting completing their entire life cycle within a single host. Both asexual and sexual stages develop in the intestinal epithelium, leading to the release of two forms of oocysts. Thin-walled oocysts are responsible for autoinfection, whereas thick-walled oocysts are released with the feces to hosts [51]. Oocysts containing sporozoites are excreted in the feces of hosts. The infectious dose was estimated to be 10-30 oocysts [52], although some researchers suggest that even a single oocyst carries a probability of infection, particularly in immunocompromised host [53]. Cryptosporidium oocysts can transmit through direct or indirect human-to-human or animal-to-human and through contaminated water and food. Transmission may occur by ingestion of animal contact, consumption of contaminated water or recreational water, travel to disease-endemic regions, poor hygiene, or foodborne transmission [53]. Airborne transmission and mechanical transport of Cryptosporidium spp. oocysts by flies and other insects have also been postulated [20,54,55]. The dissemination of Cryptosporidium spp. oocysts in the environment is facilitated by the shedding of a large number of oocysts by the host. Oocysts are resistant to environmental factors and disinfection [56]. Oocysts excyst in the small bowel, releasing sporozoites that invade enterocytes. Recipients of transplanted organs may become infected with Cryptosporidium spp. in three different ways: (i) transfer through transplantation, (ii) de novo infection, or (iii) reactivation of latent infection due to immunosuppression [57]. Zoonotic transmission of Cryptosporidium spp. infection cannot be excluded in transplant recipients due to exposure to socio-economic conditions. It is postulated that the transmission of oocysts may also occur through inhalation or accidental entry of oocysts into the respiratory tract during vomiting [28,58]. Cryptosporidium spp. may spread hematogenously from the gastrointestinal tract. The parasite has been detected in the colonic vascular system during histopathological examination [59]. The excretion of oocysts by infected individuals can exceed <109 oocysts in stool per day, with the excretion process lasting up to 50 days after the resolution of diarrhea symptoms.
Host immune Response to Cryptosporidium Infection
Both cellular and humoral immunity play a role in Cryptosporidium spp. infection [60]. Both components of the immune response play a significant role in combating infection and acquiring immunity. The nature of the immune response in Cryptosporidium spp. infection is poorly understood. Much of the data is based on studies conducted using laboratory animals. However, a good experimental model has not yet been developed, and research is ongoing to establish such a model, including studies on various inbred strains of mice, including those with immunosuppression. Most commonly used for research are adult SCID mice and nu/nu mice of all strains, as they develop an initial level of immunity to Cryptosporidium spp. infection within 3 to 5 weeks post-infection [61]. Cell lines are also used for research purposes; however, to date, it has not been confirmed that the same parasite-host interactions occur in the intestinal mucosa in vitro and in vivo. Nevertheless, the occurrence of severe Cryptosporidium spp. infection in patients with reduced immunity and lymphocyte or gammaglobulin deficiencies may suggest the involvement of both cellular and humoral immune responses [62]. In innate immune defense, an initial mechanical and functional barrier involves the mucus layer of the small intestine and intestinal epithelial cells (IECs). Infection with Cryptosporidium spp. activates an intracellular signaling cascade. IECs, similar to biliary epithelial cells, express Toll-like receptors (TLRs), including TLR 2, 4, 5, and 9, which modulate the host immune response and subsequent parasite clearance [39,63,64,65,66]. Recognition and binding of Cryptosporidium spp. ligands by TLRs lead to the activation of a signaling cascade involving the myeloid differentiation primary response gene 88 (MyD88) adaptor protein and the activation of nuclear factor kappa B (NF-κB). Activation of NF-κB results in the expression of genes responsible for the production of chemokines, pro-inflammatory enzymes, cytokines, including tumor necrosis factor α (TNFα), interleukins (IL-1, IL-4, IL-8, and IL-15), C-C motif chemokine ligand 2 (CCL2), and C-X-C motif chemokine ligand 10 (CXCL10), which are responsible for recruiting inflammatory cells and activating acquired immune cells [67,68]. It has been observed that Cryptosporidium spp. infection initially reduces the production of human beta defensins 1 (HBD-1), which may facilitate parasite survival [69]. On the other hand, infection also induces the expression and secretion of HBD-2, which acts against the parasite in vitro and may play a role in recruiting T cells and dendritic cells in vivo, facilitating pathogen eradication [64]. IECs also secrete prostaglandins, which increase the secretion of intestinal fluids and antimicrobial peptides (AMPs), including α- and β-defensins and cathelicidins capable of directly killing sporozoites in vitro [69,70,71]. NF-κB activation leads to the production and release of chemokines and enhances the regulation of anti-apoptotic signals, such as Bcl-2 [72]. Although prostaglandins may contribute to diarrhea pathogenesis by altering chloride ion uptake and fluid secretion, they may also increase mucin secretion from epithelial cells, protecting against Cryptosporidium spp. infection by disrupting parasite adhesion. Additionally, prostaglandins may stimulate the production of certain HBDs and reduce the expression of pro-inflammatory cytokines. It is postulated that the predominant role in the immune response is played by the cellular response, particularly involving interferon γ (IFN-γ) participating in parasite clearance from the gastrointestinal tract and CD4+ T cells [73]. It has been noted that the risk of Cryptosporidium spp. infection development is mainly associated with a decrease in CD4+ T-cell count below 200 cells/μL [74]. In AIDS patients infected with Cryptosporidium spp., granulocytes are not the main component of the inflammatory response [75]. In AIDS patients, depletion of effector T lymphocytes may lead to increased parasite numbers, causing excessive production of CXCL-10. Effective antiretroviral therapy has been observed to be associated with reduced CXCL-10 production by enterocytes [76]. Reduced CXCL-10 levels may also decrease inflammatory reactions in the intestinal mucosa and lead to alleviation of chronic diarrhea. Potentially CXCR-3-positive cells are located in the epithelial layer; however, these cells apparently cannot eliminate the parasite. Effective antiretroviral therapy has been observed to restore the number of CD4+ T lymphocytes in intestinal tissues. Humoral immunity also plays a significant role, as patients with primary immunodeficiency, including X-linked hyper-IgM syndrome and IgA deficiencies, are more susceptible to Cryptosporidium spp. [77]. In immunocompetent individuals after Cryptosporidium spp. infection, a humoral response of IgG, IgM, and IgA dependent on the number of CD4 cells develops [62]. However, the role of antibody responses in protection is still unclear. Based on serological studies in volunteer groups, individuals with antibodies against Cryptosporidium spp. were observed to have less severe symptoms of cryptosporidiosis upon subsequent pathogen exposure [78]. However, it is unknown whether antibodies provide protection against infection or are merely markers of the immune response [73].
Laboratory Diagnosis of Cryptosporidium spp. Infection
Cryptosporidiosis should be considered in cases of diarrhea of unknown epidemiology, especially in patients with lowered immunity levels. The material for examination is stool, and samples from the respiratory tract, including saliva, bronchoalveolar lavage (BAL), sputum, bronchial aspirate, and respiratory epithelial biopsy. Occasionally, colonic biopsies are used, which play an important role in the diagnosis and management of GI disease in renal transplant patients [79,80]. In some patients, mucosal biopsies from the intestine, as well as bile and other body fluids depending on symptoms, are utilized [81,82]. For the diagnosis of Cryptosporidium spp., fresh, frozen, and formalin-fixed stool samples are used. Stool samples fixed with polyvinyl alcohol (PVA) cannot be used in some staining techniques and formally for molecular diagnosis. Most laboratories routinely use microscopic methods in the diagnosis of cryptosporidiosis. Microscopic diagnosis is based on detecting the presence of Cryptosporidium spp. oocysts in samples of the examined material using light microscopy or phase-contrast microscopy. However, methods based on the evaluation of unstained preparations are associated with significant limitations due to the small size of oocysts (3-8 μm) and their similarity to other structures, including debris, yeast forms, and other protozoa. Additionally, a minimum threshold of 50,000 oocysts/ml in a stool sample is required for detection. Therefore, staining methods such as Kinyoun Modified Acid Fast, modified Ziehl-Neelsen method (Figure 1), and alternatively aniline-carbol-methyl violet (ACMV) staining are most commonly used. It has been observed that to increase sensitivity, multiple samples should be examined (Table 2).
The sensitivity of this method is enhanced by concentrating oocysts in stool through centrifugation (1,200 x g), Sheather’s sugar flotation method, saturated salt flotation, and Allen and Ridley’s formalin-ether method [83]. However, even with the use of concentration methods, the sensitivity of the method largely depends on the skills of the person evaluating the preparation. Moreover, these procedures often may be insufficient to detect the presence of Cryptosporidium spp. oocysts in asymptomatic infections.
Immunofluorescence antibody staining (IFA) techniques using monoclonal antibodies against oocyst wall antigen are also used. They are characterized by high sensitivity and are cheaper compared to other traditional staining methods [93]. Serological methods, which rely on the detection of Cryptosporidium antigens or antibodies directed against this pathogen, are characterized by higher sensitivity and specificity than microscopic techniques [94]. Antigen detection can be performed using fluorescently or enzymatically labeled antibodies. Serological methods are considered the best tools for screening a large number of samples, especially in epidemiological studies. Coproantigen detection kits for Cryptosporidium spp. or in combination with Giardia intestinalis and/or Entamoeba histolytica are commonly used [95]. Detection of antibodies against Cryptosporidium spp. specific antigens in serum, saliva, or stool samples is an indirect diagnostic method. The detection of specific antibodies is beneficial only in cases of seroconversion, showing an increase in titer or a change in antibody isotype. Molecular methods are more sensitive, with a detection range from 1 to 106 oocysts. Polymerase chain reaction (PCR), quantitative Real-Time PCR (qRT-PCR), restriction fragment length polymorphism (PCR-RFLP), multiplex allele-specific-PCR (MAS-PCR), and quantitative real-time PCR are used. Genes such as 18S rRNA, TRAP C1, COWP, Hsp 70, and DHFR, subtype glycoprotein (GP) 60 gene, minisatellite, and microsatellite markers are used for species identification, as well as analysis of extrachromosomal double-stranded RNA elements [83]. Due to the structure of the oocyst wall, the DNA isolation procedure requires additional steps of initial homogenization, mechanical homogenization using glass beads, enzymatic lysis, alternate freezing and thawing of biological material, or incubation at temperatures above 70°C [93]. For species determination, the analysis of the rRNA small subunit locus by PCR RFLP is commonly used. Subtypes can be identified using PCR RFLP or sequencing of polymorphic loci, with the Cpgp40/15 locus being the most commonly used (also known as GP60) [68]. Fluorescent in situ hybridization (FISH), where oligonucleotide probes are used to detect the presence of 18S rRNA sequences, can also be applied for Cryptosporidium spp. detection. However, this method is time-consuming and less sensitive than molecular methods. Histological examination of intestinal mucosal biopsies is rarely used for routine diagnosis due to uneven parasite distribution in the biopsy, which can lead to false-negative results, and it is an expensive and time-consuming technique [83].
Treatment for Cryptosporidium Infection
Treatment for cryptosporidiosis, including in transplant recipients, are limited, which may be due to the absence of many organelles in Cryptosporidium spp., including the apicoplast, the target of many pharmacological therapies [96]. Various drugs are used in the treatment of cryptosporidiosis, including nitazoxanide (NTZ), paromomycin, trimethoprim/sulfamethoxazole, rifampin, and fluoroquinolones, either alone or in combination, with variable response durations [97] (Figure 2).
Nitazoxanide has been approved by the Food and Drug Administration (FDA) as the only drug for the treatment of diarrhea caused by Cryptosporidium spp. [98]. It inhibits the action of pyruvate ferredoxin oxidoreductase, an enzyme responsible for electron transport in anaerobic energy metabolism. This is probably not the only mechanism of its action. Based on randomized studies, it has been found that NTZ leads to faster resolution of symptoms and oocyst excretion [99,100]. The drug is available in 500 mg tablets or as a 100 mg/5 ml suspension; taking it with food increases its bioavailability. However, the effectiveness of NTZ in the treatment of cryptosporidiosis in immunosuppressed patients has not been established, which is likely due to the low number of CD4+ lymphocytes [101]. In adult HIV-infected patients, NTZ has not been shown to affect the duration of diarrhea and oocyst excretion [44]. Therefore, it has not been approved by the FDA for the treatment of Cryptosporidium spp.-induced diarrhea in HIV patients. For solid organ transplant (SOT) recipients, the American Society of Transplantation Infectious Diseases Community of Practice recommends the use of NTZ in the treatment of cryptosporidiosis. Data on the use of NTZ in transplant recipients are limited and mainly come from case reports. However, some researchers have noted that long-term NTZ therapy is often effective [102,103]. In immunocompetent patients, the duration of NTZ treatment is three days, while in patients with decreased immunity, including kidney transplant recipients, it can be longer, up to 14 days [104]. Tomczak et al. [44] noted that in SOT patients, resolution of diarrhea was achieved by combining high-dose NTZ with rifaximin and azithromycin (AZCQ), along with reducing tacrolimus levels. Additionally, some studies have shown that macrolides, including AZCQ and spiramycin, have activity against Cryptosporidium and have shown promising results in transplant recipients [105]. Adjusting immunosuppression and monitoring immunosuppressant levels is crucial in both the management and prevention of cryptosporidiosis. Tie et al. [105] observed in a patient after liver transplantation that NTZ therapy, combined with controlled CD4+ T cells at 100-300/mm3, was highly effective against Cryptosporidium without inducing immunorejection. The American Society of Transplantation Infectious Diseases Community of Practice recommends both reducing immunosuppression and using NTZ as initial treatment for SOT recipients with cryptosporidiosis. It has been noted that the severity of the disease probably depends on the degree of immunosuppression and the number of CD4+ T cells, so it is very important in SOT patients to attempt to restore immune function by adjusting or changing immunosuppressive therapy [97]. A higher frequency of Cryptosporidium spp. infection has been demonstrated in individuals taking tacrolimus compared to cyclosporine. It has also been found that diarrhea caused by Cryptosporidium spp. may lead to increased tacrolimus levels, which may in turn worsen kidney function and prolong immunosuppression [35,36,104].It has been found that mycophenolate mofetil (MMF) may have activity against Cryptosporidium spp. by inhibiting folate metabolism [102]. In treatment, conversion to a less potent immunosuppressive drug (cyclosporine) or reduction, if necessary, of previously administered immunosuppressive drug doses should be considered [35]. Infection of the biliary tract in immunocompromised patients may constitute an extraintestinal reservoir, leading to a lack of response to certain drugs (paromomycin) and may lead to relapses. In these patients, drugs excreted in bile, including NTZ, should be administered [106]. Oral bovine immunoglobulin (hyperimmune colostrum) appears to be a viable alternative treatment for cryptosporidiosis [107]. Additionally, a great promise is shown by calcium-dependent protein kinases, microtubule formation inhibitors, hexokinase, lactate dehydrogenase, inosine-5-monophosphate dehydrogenase, and fatty acyl-coenzyme A binding inhibitors, as well as anti-parasite vaccines [96,108]. Love et al. [96] observed that clofazimine also exhibited efficacy against Cryptosporidium, making it a potentially new cryptosporidiosis treatment and a novel chemical tool for understanding Cryptosporidium biology. Kabir et al. [109] suggested that the compounds atropine sulfate and bufotalin could be useful in the development of new anti-Cryptosporidium medications. Symptomatic treatment should also be considered, including correction of fluid and electrolyte deficits, and appropriate nutrition. Garlic (Allium sativum) has an anti-parasitic effect against many parasites [110]. The effect of zinc oxide nanoparticles (ZnO-NPs) as carriers for garlic and NTZ has been investigated in animal models. In well-documented studies, ZnO-NPs have been used as an effective alternative therapy in the treatment of experimental cryptosporidiosis, especially in combination with other treatment methods that enhance their antioxidant activity [111,112]. Research is being conducted on the use of nanoparticles with specific anti-protozoal medications to treat cryptosporidiosis [113].
Prevention
Firstly, to eliminate the possibility of nosocomial infection in patients who will often be in contact during consultations in the nephrology department; secondly, to determine the source of contamination (notably animal) and eliminate it to prevent any subsequent recontamination. To minimize the risk of infection, handwashing is recommended, as well as avoiding contact with young pets and farm animals (calves), infected individuals, and swimming pools. It is also recommended to protect against waterborne Cryptosporidium spp. infections, including boiling drinking water and filtering water through filters that trap particles around 1 µm in size. Pasteurization of milk for approximately 15 seconds at a temperature of around 70°C is also recommended, as it destroys oocysts.
Conclusions
Cryptosporidium spp. infection should be considered in kidney transplant patients with diarrhea. Diagnostic methods should include direct methods and, if possible, molecular methods. Treatment of cryptosporidiosis is combination therapy using nitazoxanide, azithromycin, and rifaximin.
Author Contributions
DKB: literature search and review, manuscript draft preparation, writing the manuscript, and preparation of manuscript revision. N.Ł.A., K.K, J.K.K and P.Z.: participation in writing the manuscript. M.M.M: writing the manuscript, preparation of manuscript revision, and final acceptance of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Fletcher, S.M.; Stark, D.; Harkness, J.; Ellis, J. Enteric protozoa in the developed world: a public health perspective. Clin. Microbiol. Rev. 2012, 25, 420–449. [Google Scholar] [CrossRef] [PubMed]
- Kotloff, K.L. The burden and etiology of diarrheal illness in developing countries. Pediatr. Clin. North Am. 2017, 64, 799–814. [Google Scholar] [CrossRef] [PubMed]
- Deltombe, C.; Lefebvre, M.; Morio, F.; Boutoille, D.; Imbert, B.M.; Le Pape, P.; Raffi, F.; Hourmant, M. Cryptosporidiosis and microsporidiosis as causes of diarrhea in kidney and/or pancreas transplant recipients. Med. Mal. Infect. 2020, 50, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Sonambekar, A.; Mehta, V.; Desai, D.; Abraham, P.; Almeida, A.; Joshi, A.; Gupta, T.; Sirsat, R.; Kothari, J. Diarrhea in kidney transplant recipients: etiology and outcome. Indian. J. Gastroenterol. 2020, 39, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Calmet, F.H.; Yarur, A.J.; Pukazhendhi, G.; Ahmad, J.; Bhamidimarri, K.R. Endoscopic and histological features of mycophenolate mofetil colitis in patients after solid organ transplantation. Ann. Gastroenterol. 2015, 28, 366–373. [Google Scholar] [PubMed]
- Plutzer J, Karanis P. Genetic polymorphism in Cryptosporidium species: an update. Vet Parasitol. 2009;165:187–199.
- Helmy, Y.A.; Hafez, H.M. Cryptosporidiosis: from prevention to treatment, a narrative review. Microorganisms. 2022, 10, 2456. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, A.; Lim, Y.A.; Mahdy, M.A.; Dixon, B.R.; Surin, J. Epidemiology of cryptosporidiosis in HIV-infected individuals: a global perspective. Open Access Sci. Rep. 2012, 1, 431. [Google Scholar]
- Bouzid, M.; Hunter, P.R.; Chalmers, R.M.; Tyler, K.M. Cryptosporidium pathogenicity and virulence. Clin. Microbiol. Rev. 2013, 26, 115–134. [Google Scholar] [CrossRef] [PubMed]
- Hatalova, E.; Guman, T.; Bednarova, V.; Simova, V.T.; Logoida, M.; Halanova, M. Occurrence of Cryptosporidium parvum IIaA17G1R1 in hospitalized hemato-oncological patients in Slovakia. Parasitol. Res. 2022, 121, 471–476. [Google Scholar] [CrossRef]
- Cengiz, Z.T.; Yilmaz, H.; Sahin, I.H.; Kapmaz, M.; Ekici, P. The frequency of Cryptosporidium spp. in immunocompromised patients by modified acid-fast staining, cassette Kit and ELISA methods: comparison of the diagnostic techniques. Jundishapur J. Microbiol 2017, 10, e36479. [Google Scholar] [CrossRef]
- Hunter, P.R.; Nichols, G. Epidemiology and clinical features of Cryptosporidium infection in immunocompromised patients. Clin. Microbiol. Rev. 2002, 15, 145–154. [Google Scholar] [CrossRef] [PubMed]
- Pumipuntu, N.; Piratae, S. Cryptosporidiosis: a zoonotic disease concern. Vet. World. 2018, 11, 681. [Google Scholar] [CrossRef] [PubMed]
- Mac Kenzie, W.R.; Hoxie, N.J.; Proctor, M.E.; Gradus, M.S.; Blair, K.A.; Peterson, D.E.; Kazmierczak, J.J.; Addiss, D.G.; Fox, K.R.; Rose, J.B.; et al. A massive outbreak in Milwaukee of cryptosporidium infection transmitted through the public water supply. N. Engl. J. Med. 1994, 331, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Farthing, M.J. Clinical aspects of human cryptosporidiosis. Contrib. Microbiol. 2000, 6, 50–74. [Google Scholar] [PubMed]
- Shirley, D.A.; Moonah, S.N.; Kotloff, K.L. Burden of disease from cryptosporidiosis. Curr. Opin. Infect. Dis. 2012, 25, 555–563. [Google Scholar] [CrossRef] [PubMed]
- Leitch, G.J.; He, Q. Cryptosporidiosis-an overview. J. Biomed. Res. 2012, 25, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Hunter, P.R.; Hadfield, S.J.; Wilkinson, D.; Lake, I.R.; Harrison, F.C.; Chalmers, R.M. Correlation between subtypes of Cryptosporidium parvum in humans and risk. Emerg. Infect. Dis. 2007, 13, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Robertson, B.; Sinclair, M.I.; Forbes, A.B.; Veitch, M.; Kirk, M.; Cunliffe, D.; Willis, J.; Fairley, C.K. Case-control studies of sporadic cryptosporidiosis in Melbourne and Adelaide, Australia. Epidemiol. Infect. 2002, 128, 419–431. [Google Scholar] [CrossRef]
- Chalmers, R.M.; Davies, A.P. Minireview: clinical cryptosporidiosis. Exp. Parasitol. 2010, 124, 138–146. [Google Scholar] [CrossRef]
- Shrateh, O.N.; Jobran, A.; Zaid, M.A.; Saleh, M. Successful management of life-threatening post-COVID-19 cryptosporidiosis in a renal transplant patient: a case report. Pan Afr. Med. J. 2023, 45, 10. [Google Scholar]
- Bahdi, F.; Jain, S.; Agarwal, S.K. Cryptosporidiosis in an immunosuppressed patient with persistent diarrhea. Cleve Clin. J. Med. 2021, 88, 24–26. [Google Scholar] [CrossRef] [PubMed]
- Aulagnon, F.; Scemla, A.; DeWolf, S.; Legendre, C.; Zuber, J. Diarrhea after kidney transplantation: a new look at a frequent symptom. Transplantation. 2014, 98, 806–816. [Google Scholar] [CrossRef] [PubMed]
- Clifford, C.P.; Crook, D.W.; Conlon, C.P.; Fraise, A.P.; Day, D.G.; Peto, T.E. Impact of waterborne outbreak of cryptosporidiosis on AIDS and renal transplant patients. Lancet. 1990, 335, 1455–1456. [Google Scholar] [CrossRef] [PubMed]
- Roncoroni, A.J.; Gomez, M.A.; Mera, J.; Cagnoni, P.; Michel, M.D. Cryptosporidium infection in renal transplant patients. J. Infect. Dis. 1989, 160, 559. [Google Scholar] [CrossRef] [PubMed]
- Golan Shaposhnik, E.; Abozaid, S.; Grossman, T.; Marva, E.; On, A.; Azrad, M.; Peretz, A. The prevalence of Cryptosporidium among children hospitalized because of gastrointestinal symptoms and the efficiency of diagnostic methods for Cryptosporidium. Am. J. Trop. Med. Hyg. 2019, 101, 160–163. [Google Scholar] [CrossRef] [PubMed]
- Current, W.L.; Garcia, L.S. Cryptosporidiosis. Clin. Microbiol. Rev. 1991, 4, 325–358. [Google Scholar] [CrossRef]
- Sponseller, J.K.; Griffiths, J.K.; Tzipori, S. The evolution of respiratory cryptosporidiosis: evidence for transmission by inhalation. Clin. Microbiol. Rev. 2014, 27, 575–586. [Google Scholar] [CrossRef] [PubMed]
- Clavel, A.; Arnal, A.C.; Sánchez, E.C.; Cuesta, J.; Letona, S.; Amiguet, J.A.; Castillo, F.J.; Varea, M.; Gómez-Lus, R. Respiratory cryptosporidiosis: case series and review of the literature. Infection. 1996, 24, 341–346. [Google Scholar] [CrossRef]
- Pellicelli, A.M.; Palmieri, F.; Spinazzola, F.; D’Ambrosio, C.; Causo, T.; De Mori, P.; Bordi, E.; D’Amato, C. Pulmonary cryptosporidiosis in patients with acquired immunodeficiency syndrome. Minerva Med. 1998, 89, 173–175. [Google Scholar]
- Greenberg, P.D.; Koch, J.; Cello, J.P. Diagnosis of Cryptosporidium parvum in patients with severe diarrhea and AIDS. Dig. Dis. Sci. 1996, 41, 2286–2290. [Google Scholar] [CrossRef]
- Ditrich, O.; Palkovic, L.; Stĕrba, J.; Prokopic, J.; Loudová, J.; Giboda. , M. The first finding of Cryptosporidium baileyi in man. Parasitol. Res. 1991, 77, 44–47. [Google Scholar] [CrossRef] [PubMed]
- de Souza Ldo, R.; Rodrigues, M.A.; Morceli, J.; Kemp, R.; Mendes, R/P. Cryptosporidiosis of the biliary tract mimicking pancreatic cancer in an AIDS patient. Rev. Soc. Bras. Med. Trop. 2004, 37, 182–185. [Google Scholar] [PubMed]
- Kalantari, N.; Gorgani-Firouzjaee, T.; Ghaffari, S.; Bayani, M.; Ghaffari, T.; Chehrazi, M. Association between Cryptosporidium infection and cancer: a systematic review and meta-analysis. Parasitol. Int. 2020, 74, 101979. [Google Scholar] [CrossRef] [PubMed]
- Bhadauria, D.; Goel, A.; Kaul, A.; Sharma, R.K.; Gupta, A.; Ruhela, V.; Gupta, A.; Vardhan, H.; Prasad, N. Cryptosporidium infection after renal transplantation in an endemic area. Transpl. Infect. Dis. 2015, 17, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Bonatti, H.; Barroso, L.F. 2nd; Sawyer, R.G.; Kotton, C.N.; Sifri, C.D. Cryptosporidium enteritis in solid organ transplant recipients: multicenter retrospective evaluation of 10 cases reveals an association with elevated tacrolimus concentrations. Transpl. Infect. Dis. 2012, 14, 635–648. [Google Scholar] [CrossRef] [PubMed]
- Rosser, J.I.; Blackburn, B.G. Pathogenic intestinal parasites in transplant recipients emerging transplant infections. In: Emerging Transplant Infections, Springer 2020, pp. 1397–1450.
- Cheng, F.; Li, Q.; Cui, Z.; Wang, Z.; Zeng, F.; Zhang, Y. Tacrolimus concentration is effectively predicted using combined clinical and genetic factors in the perioperative period of kidney transplantation and associated with acute rejection. J. Immunol. Res. 2022, 2022, 3129389. [Google Scholar] [CrossRef] [PubMed]
- Costa, D.; Razakandrainibe, R.; Valot, S.; Vannier, M.; Sautour, M.; Basmaciyan, L.; Gargala, G.; Viller, V.; Lemeteil, D.; Ballet, J.J.; French National Network on Surveillance of Human Cryptosporidiosis; Dalle, F. ; Favennec, L. Epidemiology of cryptosporidiosis in France from 2017 to 2019. Microorganisms. 2020, 8, 1358. [Google Scholar] [CrossRef]
- Brunet, J.; Lemoine, J.P.; Pesson, B.; Valot, S.; Sautour, M.; Dalle, F.; Muller, C.; Borni-Duval, C.; Caillard, S.; Moulin, B.; Pfaff, A.W.; Razakandrainibe, R.; Abou-Bacar, A.; Favennec, L.; Candolfi, E. Ruling out nosocomial transmission of Cryptosporidium in a renal transplantation unit: case report. BMC Infect. Dis. 2016, 16. [Google Scholar] [CrossRef]
- Ok, U.Z.; Cirit, M.; Uner, A.; Ok, E.; Akcicek, F.; Basci, A.; Ozcel, M.A. Cryptosporidiosis and blastocystosis in renal transplant recipients. Nephron. 1997, 75, 171–174. [Google Scholar] [CrossRef]
- Zheng, S.; Ko, K.K.; Chan, K.S.; Venkatachalam, I. Case report: diagnosis of cryptosporidiosis in renal transplantation in a low-prevalence setting. Am. J. Trop. Med. Hyg. 2019, 100, 78–80. [Google Scholar] [CrossRef]
- Burdese, M.; Veglio, V.; Consiglio, V.; Soragna, G.; Mezza, E.; Bergamo, D.; Tattoli, F.; Rossetti, M.; Jeantet, A.; Segoloni, G.P.; Piccoli, G.B. A dance teacher with kidney-pancreas transplant and diarrhoea: what is the cause? Nephrol. Dial. Transplant. 2005, 20, 1759–1761. [Google Scholar] [CrossRef] [PubMed]
- Tomczak, E.; McDougal, A.N.; White, A.C. Jr. resolution of cryptosporidiosis in transplant recipients: review of the literature and presentation of a renal transplant patient treated with nitazoxanide, azithromycin, and rifaximin. Open Forum Infect. Dis. 2021, 9, ofab610. [Google Scholar] [CrossRef] [PubMed]
- Abdo, A.; Klassen, J.; Urbanski, S.; Raber, E.; Swain, M. G. Reversible sclerosing cholangitis secondary to cryptosporidiosis in a renal transplant patient. J. Hepatol. 2003, 38, 688–691. [Google Scholar] [CrossRef] [PubMed]
- Franco, A.; Rocamora, N.; Merino, E.; Paya, A. Cryptosporidiosis. A rare infection in renal transplantation. Nefrologia. 2006, 26, 753–754. [Google Scholar] [PubMed]
- Tran, M.Q.; Gohh, R.Y.; Morrissey, P.E.; Dworkin, L.D.; Gautam, A.; Monaco, A.P.; Yango, A.F. Jr. Cryptosporidium infection in renal transplant patients. Clin. Nephrol. 2005, 63, 305–309. [Google Scholar] [CrossRef] [PubMed]
- Fayer, R.; Ungar, B.L. Cryptosporidium spp. and cryptosporidiosis. Microbiol. Rev. 1986, 50, 458–483. [Google Scholar] [CrossRef] [PubMed]
- Conlon, C.P.; Simone, M.C. Cryptosporidium and cryptosporidiosis. In: Oxford Textbook of Medicine, Firth J, Conlon C, Cox T (eds). Oxford, 2020.
- Mercado, R.; Buck, G.A.; Manque, P.A.; Ozaki, L.S. Cryptosporidium hominis infection of the human respiratory tract. Emerg. Infect. Dis. 2007, 13, 462–464. [Google Scholar] [CrossRef] [PubMed]
- Lendner, M.; Daugschies, A. Cryptosporidium infections: molecular advances. Parasitology. 2014, 141, 1511–1532. [Google Scholar] [CrossRef] [PubMed]
- Hlavsa, M.C.; Watson, J.C.; Beach, M.J. Cryptosporidiosis surveillance--United States 1999-2002. MMWR Surveill Summ. 2005, 54, 1–8. [Google Scholar]
- Ryan, U.; Fayer, R.; Xiao, L. Cryptosporidium species in humans and animals: current understanding and research needs. Parasitology. 2014, 141, 1667–185. [Google Scholar] [CrossRef]
- Bruce, B.B.; Blass, M.A.; Blumberg, H.M.; Lennox, J.L.; del Rio, C.; Horsburgh, C.R. Jr. Risk of Cryptosporidium parvum transmission between hospital roommates. Clin. Infect. Dis. 2000, 31, 947–950. [Google Scholar] [CrossRef] [PubMed]
- Graczyk, T.K.; Fayer, R.; Knight, R.; Mhangami-Ruwende, B.; Trout, J.M.; Da Silva, A.J.; Pieniazek, N.J. Mechanical transport and transmission of Cryptosporidium parvum oocysts by wild filth flies. Am. J. Trop. Med. Hyg. 2000, 63, 178–183. [Google Scholar] [CrossRef] [PubMed]
- Korich, D.G.; Mead, J.R.; Madore, M.S.; Sinclair, N.A.; Sterling, C.R. Effects of ozone, chlorine dioxide, chlorine, and monochloramine on Cryptosporidium parvum oocyst viability. Appl. Environ Microbiol. 1990, 56, 1423–1428. [Google Scholar] [CrossRef] [PubMed]
- Yadav, P.; Khalil, S.; Mirdha, B. Molecular appraisal of intestinal parasitic infection in transplant recipients. Indian J. Med. Res. 2016, 144, 258–263. [Google Scholar] [PubMed]
- Reina, F.T.; Ribeiro, C.A.; Araujo, R.S.; Matte, M.H.; Castanho, R.E.; Tanaka, I.I.; Viggiani, A.M.; Martins, L.P. Intestinal and pulmonary infection by Cryptosporidium parvum in two patients with HIV/AIDS. Rev. Inst. Med. Trop. Sao Paulo. 2016, 58, 21. [Google Scholar] [CrossRef]
- Gentile, G.; Baldassarri, L.; Caprioli, A.; Donelli, G.; Venditti, M.; Avvisati, G.; Martino, P. Colonic vascular invasion as a possible route of extraintestinal cryptosporidiosis. Am. J. Med. 1987, 82, 574–575. [Google Scholar] [CrossRef] [PubMed]
- Petry, F.; Jakobi, V.; Tessema, T.S. Host immune response to Cryptosporidium parvum infection. Exp. Parasitol. 2010, 126, 304–309. [Google Scholar] [CrossRef]
- Siński, E. Resistance to intestinal opportunistic infections using Cryptosporidium sp. as an example]. Wiad Parazytol. 2000;46:29-40.
- Kaushik, K.; Khurana, S.; Wanchu, A.; Malla, N. Serum immunoglobulin G, M and A response to Cryptosporidium parvum in Cryptosporidium-HIV co-infected patients. BMC Infect. Dis. 2009, 9, 179. [Google Scholar] [CrossRef] [PubMed]
- Barrier, M.; Lacroix-Lamandé, S.; Mancassola, R.; Auray, G.; Bernardet, N.; Chaussé, A.M.; Uematsu, S.; Akira, S.; Laurent, F. Oral and intraperitoneal administration of phosphorothioate oligodeoxynucleotides leads to control of Cryptosporidium parvum infection in neonatal mice. J. Infect. Dis. 2006, 193, 1400–1407. [Google Scholar] [CrossRef]
- Chen, X.M.; O’Hara, S.P.; Nelson, J.B.; Splinter, P.L.; Small, A.J.; Tietz, P.S.; Limper, A.H.; LaRusso, N.F. Multiple TLRs are expressed in human cholangiocytes and mediate host epithelial defense responses to Cryptosporidium parvum via activation of NF-κB. J. Immunol. 2005, 175, 7447–7456. [Google Scholar] [CrossRef]
- Lantier, L.; Drouet, F.; Guesdon, W.; Mancassola, R.; Metton, C.; Lo-Man, R.; Werts, C.; Laurent, F.; Lacroix-Lamandé, S. Poly(I:C)-induced protection of neonatal mice against intestinal Cryptosporidium parvum infection requires an additional TLR5 signal provided by the gut flora. J. Infect. Dis. 2014, 209, 457–467. [Google Scholar] [CrossRef] [PubMed]
- O’Hara, S.P.; Bogert, P.S.; Trussoni, C.E.; Chen, X.; LaRusso, N.F. TLR4 promotes Cryptosporidium parvum clearance in a mouse model of biliary cryptosporidiosis. J. Parasitol. 2011, 97, 813–821. [Google Scholar] [CrossRef]
- Ryan, U.; Zahedi, A.; Paparini, A. Cryptosporidium in humans and animals-a one health approach to prophylaxis. Parasite Immunol. 2016, 38, 535–547. [Google Scholar] [CrossRef]
- Xiao, L. Molecular epidemiology of cryptosporidiosis: an update. Exp. Parasitol. 2010, 124, 80–89. [Google Scholar] [CrossRef] [PubMed]
- Zaalouk, T.K.; Bajaj-Elliott, M.; George, J.T.; McDonald, V. Differential regulation of beta-defensin gene expression during Cryptosporidium parvum infection. Infect. Immun. 2004, 72, 2772–2779. [Google Scholar] [CrossRef] [PubMed]
- Elwin, K.; Hadfield, S.J.; Robinson, G.; Chalmers, R.M. The epidemiology of sporadic human infections with unusual cryptosporidia detected during routine typing in England and Wales, 2000–2008. Epidemiol. Infect. 2012, 140, 673–683. [Google Scholar] [CrossRef]
- Ludington, J.G.; Ward, H.D. Systemic and mucosal immune responses to Cryptosporidium-vaccine development. Curr. Trop. Med. Rep. 2015, 2, 171–180. [Google Scholar] [CrossRef]
- Jobin, C.; Sartor, R.B. The IκB/NF-κB system: a key determinant of mucosal inflammation and protection. Am. J. Physiol. Cell Physiol. 2000, 278, C451–C462. [Google Scholar] [CrossRef]
- Riggs, M.W. Recent advances in cryptosporidiosis: the immune response. Microbes Infect. 2002, 4, 1067–1080. [Google Scholar] [CrossRef]
- Ghafari, R.; Rafiei, A.; Tavalla, M.; Moradi Choghakabodi, P.; Nashibi, R.; Rafiei, R. Prevalence of Cryptosporidium species isolated from HIV/AIDS patients in southwest of Iran. Comp. Immunol. Microbiol. Infect. Dis. 2018, 56, 39–44. [Google Scholar] [CrossRef]
- Borowski, H.; Clode, P.L.; Thompson, R.C. Active invasion and/or encapsulation? A reappraisal of host-cell parasitism by Cryptosporidium. Trends Parasitol. 2008, 24, 509–516. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.C.; Dann, S.M.; Okhuysen, P.C.; Lewis, D.E.; Chappell, C.L.; Adler, D.G.; White, A.C. Jr. High levels of CXCL10 are produced by intestinal epithelial cells in AIDS patients with active cryptosporidiosis but not after reconstitution of immunity. Infect. Immun. 2007, 75, 481–487. [Google Scholar] [CrossRef] [PubMed]
- Mead, J.R. Early immune and host cell responses to Cryptosporidium infection. Front Parasitol. 2023, 2, 1113950. [Google Scholar] [CrossRef] [PubMed]
- Borad, A.; Ward, H. Human immune responses in cryptosporidiosis. Future Microbiol. 2010, 5, 507–519. [Google Scholar] [CrossRef] [PubMed]
- Ishaque, M.; Rashid, R.; Mubarak, M. Gastrointestinal complications in renal transplant recipients detected by endoscopic biopsies in a developing country. Indian J. Gastroenterol. 2015, 34, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Orenstein, J.M.; Dieterich, D.T. The histopathology of consecutive colonoscopy biopsies from 82 symptomatic patients with acquired immunode¢ciency syndrome. Arch. Pathol. Lab. Med. 2001, 125, 1042–1046. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Chadwick, V.; Tie, A.; Harp, J. Cryptosporidium parvum in intestinal mucosal biopsies from patients with inflammatory bowel disease. Am. J. Gastroenterol. 2001, 96, 3463–3464. [Google Scholar] [CrossRef]
- Delis, S.G.; Tector, J.; Kato, T.; Mittal, N.; Weppler, D.; Levi, D.; Ruiz, P.; Nishida, S.; Nery, J.R.; Tzakis, A.G. Diagnosis and treatment of Cryptosporidium infection in intestinal transplant recipients. Transplant. Proc. 2002, 34, 951–952. [Google Scholar] [CrossRef]
- Khurana, S.; Chaudhary, P. Laboratory diagnosis of cryptosporidiosis. Trop. Parasitol. 2018, 8, 2–7. [Google Scholar] [CrossRef]
- Chieffi, P.P.; Sens, Y.A.; Paschoalotti, M.A.; Miorin, L.A.; Silva, H.G.; Jabur, P. Infection by Cryptosporidium parvum in renal patients submitted to renal transplant or hemodialysis. Rev. Soc. Bras. Med. Trop. 1998, 31, 333–337. [Google Scholar] [CrossRef]
- Minz, M.; Udgiri, N.K.; Heer, M.K.; Kashyap, R.; Malla, N. Cryptosporidiasis in live related renal transplant recipients: a single center experience. Transplantation. 2004, 77, 1916–1917. [Google Scholar] [CrossRef] [PubMed]
- Udgiri, N.; Minz, M.; Kashyap, R.; Heer, M.; Gupta, C.S.; Mohandas, K.; Minz, R.W.; Malla, N. Intestinal cryptosporidiasis in living related renal transplant recipients. Transplant Proc. 2004, 36, 2128–2129. [Google Scholar] [CrossRef] [PubMed]
- Hazrati Tappeh, K.H.; Gharavi, M.J.; Makhdoumi, K.; Rahbar, M.; Taghizadeh, A. Prevalence of Cryptosporidium spp. infection in renal transplant and hemodialysis patients. Iran J. Public Health. 2006, 35, 54–57. [Google Scholar]
- Arslan, H.; Inci, E.K.; Azap, O.K.; Karakayali, H.; Torgay, A.; Haberal, M. Etiologic agents of diarrhea in solid organ recipients. Transpl. Infect. Dis. 2007, 9, 270–275. [Google Scholar] [CrossRef] [PubMed]
- Raja, K.; Abbas, Z.; Hassan, S.M.; Luck, N.H.; Aziz, T.; Mubarak, M. Prevalence of cryptosporidiosis in renal transplant recipients presenting with acute diarrhea at a single center in Pakistan. J. Nephropathol. 2014, 3, 127–131. [Google Scholar] [PubMed]
- Mohamed, N.S.; Siddig, E.E.; Mohamed, M.A.; Alzein, B.A.; Osman, H.H.S.; Tanyous, E.E.; Elamin, B.K.; Edris, A.M.M. Enteroparasitosis infections among renal transplant recipients in Khartoum state, Sudan 2012-2013. BMC Res. Notes. 2018, 11, 621. [Google Scholar] [CrossRef] [PubMed]
- Ghoshal, U.; Ranjan, P.; Dey, A.; Ghoshal, U.C. Intestinal cryptosporidiosis in renal transplant recipients: prevalence, species detection and comparative evaluation of SSU rRNA and Cryptosporidium oocyst wall protein genes. Indian J. Med. Microbiol. 2018, 36, 247–250. [Google Scholar] [CrossRef] [PubMed]
- Lanternier, F.; Amazzough, K.; Favennec, L.; Mamzer-Bruneel, M.F.; Abdoul, H.; Tourret, J.; Decramer, S.; Zuber, J.; Scemla, A.; Legendre, C.; Lortholary, O.; Bougnoux, M.E. ; ANOFEL Cryptosporidium National Network and Transplant Cryptosporidium Study Group. Cryptosporidium spp. infection in solid organ transplantation: The Nationwide “TRANSCRYPTO” Study. Transplantation. 2017, 101, 826–830. [Google Scholar] [PubMed]
- Caccio, S.M.; Widmer, G. Cryptosporidium: parasite and disease; Springer: Berlin/Heidelberg, Germany, 2014. [Google Scholar]
- O’Leary, J.K.; Sleator, R.D.; Lucey, B. Cryptosporidium spp. diagnosis and research in the 21st century. Food Waterborne Parasitol. 2021, 24, e00131. [Google Scholar] [CrossRef]
- Van den Bossche, D.; Cnops, L.; Verschueren, J.; Van Esbroeck, M. Comparison of four rapid diagnostic tests, ELISA, microscopy and PCR for the detection of Giardia lamblia, Cryptosporidium spp. and Entamoeba histolytica in feces. J. Microbiol. Methods. 2015, 110, 78–84. [Google Scholar] [CrossRef]
- Love, M.S.; Choy, R.K.M. Emerging treatment options for cryptosporidiosis. Curr. Opin. Infect. Dis. 2021, 34, 455–462. [Google Scholar] [CrossRef]
- Florescu, D.F.; Sandkovsky, U. Cryptosporidium infection in solid organ transplantation. World J. Transplant. 2016, 6, 460–471. [Google Scholar] [CrossRef] [PubMed]
- Miyamoto, Y.; Eckmann, L. Drug development against the major diarrhea-causing parasites of the small intestine, Cryptosporidium and Giardia. Front Microbiol. 2015, 6, 1208. [Google Scholar] [CrossRef] [PubMed]
- Rossignol, J.F.; Ayoub, A.; Ayers, M.S. Treatment of diarrhea caused by Cryptosporidium parvum: a prospective randomized, double-blind, placebo-controlled study of nitazoxanide. J. Infect. Dis. 2001, 184, 103–106. [Google Scholar] [CrossRef] [PubMed]
- Rossignol, J.F.; Kabil, S.M.; el-Gohary, Y.; Younis, A.M. Effect of nitazoxanide in diarrhea and enteritis caused by Cryptosporidium species. Clin. Gastroenterol. Hepatol. 2006, 4, 320–324. [Google Scholar] [CrossRef] [PubMed]
- Faraci, M.; Cappelli, B.; Morreale, G.; Lanino, E.; Moroni, C.; Bandettini, R.; Terranova, M.P.; Di Martino, D.; Coccia, C.; Castagnola, E. Nitazoxanide or CD3+/CD4+ lymphocytes for recovery from severe Cryptosporidium infection after allogeneic bone marrow transplant? Pediatr. Transplant. 2007, 11, 113–116. [Google Scholar] [CrossRef] [PubMed]
- Krause, I.; Amir, J.; Cleper, R.; Dagan, A.; Behor, J.; Samra, Z.; Davidovits, M. Cryptosporidiosis in children following solid organ transplantation. Pediatr. Infect. Dis. J. 2012, 31, 1135–1138. [Google Scholar] [CrossRef] [PubMed]
- Legrand, F.; Grenouillet, F.; Larosa, F.; Dalle, F.; Saas, P.; Millon, L.; Deconinck, E.; Rohrlich, P.S. Diagnosis and treatment of digestive cryptosporidiosis in allogeneic haematopoietic stem cell transplant recipients: a prospective single centre study. Bone Marrow Transplant. 2011, 46, 858–862. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, B.S.; Mawhorter, S.D. Parasitic infections in solid organ transplantation. Am. J. Transplant. 2013, 13, 280–303. [Google Scholar] [CrossRef]
- Tie, X.; Zhang, Z.; Zhou, R.; Li, Y.; Xu, J.; Yin, W. A case of septic shock due to delayed diagnosis of Cryptosporidium infection after liver transplantation. BMC Infect. Dis. 2023, 23, 260. [Google Scholar] [CrossRef]
- Baishanbo, A.; Gargala, G.; Duclos, C.; François, A.; Rossignol, J.F.; Ballet, J.J.; Favennec, L. Efficacy of nitazoxanide and paromomycin in biliary tract cryptosporidiosis in an immunosuppressed gerbil model. J. Antimicrob. Chemother. 2006, 57, 353–355. [Google Scholar] [CrossRef] [PubMed]
- Okhuysen, P.C.; Chappell, C.L.; Crabb, J.; Valdez, L.M.; Douglass, E.T.; DuPont. H.L. Prophylactic effect of bovine anti-Cryptosporidium hyperimmune colostrum immunoglobulin in healthy volunteers challenged with Cryptosporidium parvum. Clin. Infect. Dis. 1998, 26, 1324–1329. [Google Scholar] [CrossRef] [PubMed]
- Dupuy, F.; Valot, S.; Dalle, F.; Sterin, A.; L’Ollivier, C. Disseminated Cryptosporidium infection in an infant with CD40L deficiency. IDCases. 2021, 24, e01115. [Google Scholar] [CrossRef] [PubMed]
- Kabir, M.H.B.; Recuenco, F.C.; Mohd Zin, N.K.; Watanabe, N.; Fukuda, Y.; Bando, H.; Watanabe, K.; Bochimoto, H.; Xuan, X.; Kato, K. Identification of potent anti-Cryptosporidium new drug leads by screening traditional Chinese medicines. PLoS Negl. Trop. Dis. 2022, 16, e0010947. [Google Scholar] [CrossRef] [PubMed]
- Yavuzcan Yildiz, H.; Phan Van, Q.; Parisi, G.; Dam Sao, M. Anti-parasitic activity of garlic (Allium sativum) and onion (Allium cepa) juice against crustacean parasite, Lernantropus kroyeri, found on European sea bass (Dicentrarchus labrax). Ital. J. Anim. Sci. 2019, 18, 833–837. [Google Scholar] [CrossRef]
- Farid, A.; Yousry, M.; Safwat, G. Garlic (Allium sativum Linnaeus) improved inflammation and reduced cryptosporidiosis burden in immunocompromised mice. J. Ethnopharmacol. 2022, 292, 115174. [Google Scholar] [CrossRef] [PubMed]
- Elbahaie, E.S.; El Gamal, R.L.; Fathy, G.M.; Al-Ghandour, A.M.F.; El-Akabawy, N.; Abd El Hameed, B.H.; Yahia, S.H. The controverted therapeutic efficacy of Allium sativum and Artemisia herba-alba extracts on Cryptosporidium-infected mice. J. Infect. Dev. Ctries. 2023, 17, 732–743. [Google Scholar] [CrossRef]
- Hamdy, D.A.; Ismail, M.A.M.; El-Askary, H.M.; Abdel-Tawab, H.; Ahmed, M.M.; Fouad, F.M.; Mohamed, F. Newly fabricated zinc oxide nanoparticles loaded materials for therapeutic nano delivery in experimental cryptosporidiosis. Sci. Rep. 2023, 13, 19650. [Google Scholar] [CrossRef]
Figure 1.
Oocysts of Cryptosporidium spp. in a direct smear (modified Ziehl–Neelsen staining, ×1000).
Figure 1.
Oocysts of Cryptosporidium spp. in a direct smear (modified Ziehl–Neelsen staining, ×1000).
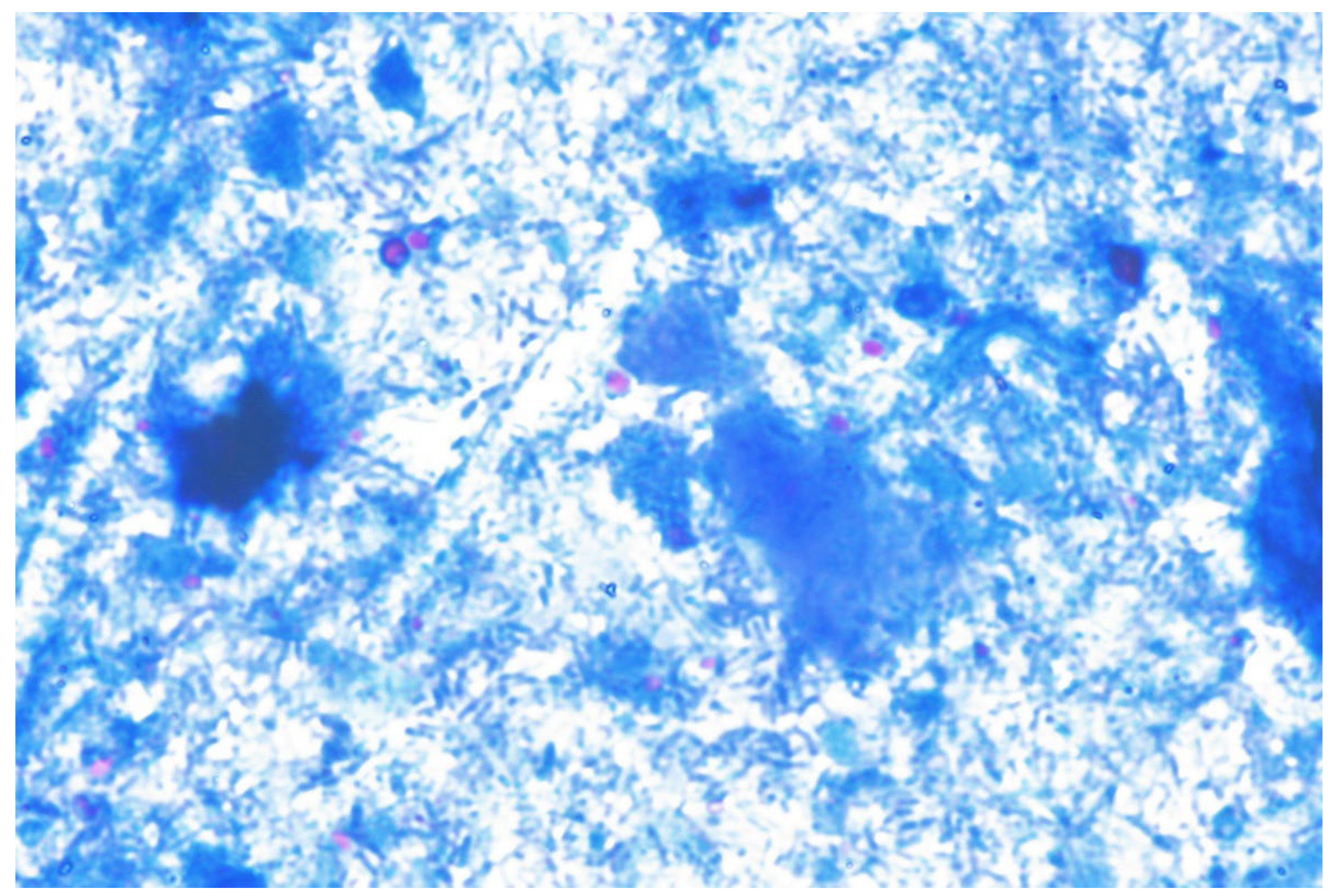
Figure 2.
Treatment algorithm for Cryptosporidium sp. infection in patients after solid organ transplantation, SOT.
Figure 2.
Treatment algorithm for Cryptosporidium sp. infection in patients after solid organ transplantation, SOT.
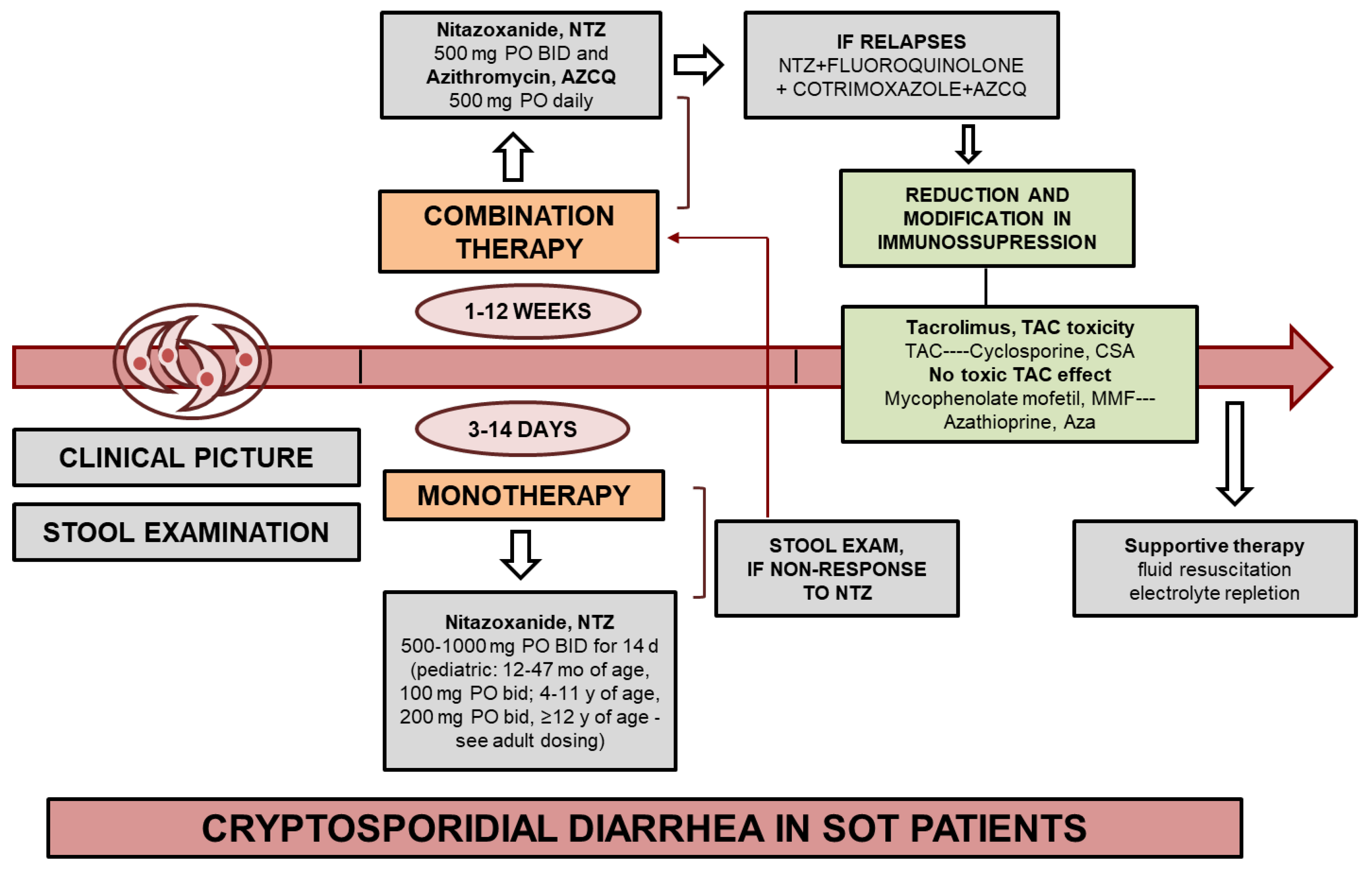

Table 1.
Cases of cryptosporidiosis in a in adult kidney transplant patients based on scientific literature (TAC, tacrolimus; MMF, mycophenolate mofetil; PRED, prednisone; IL-2R, IL-2 receptor ; CNI, calcineurin inhibitor ; NTZ, nitazoxanide; AZM, azithromycin).
Table 1.
Cases of cryptosporidiosis in a in adult kidney transplant patients based on scientific literature (TAC, tacrolimus; MMF, mycophenolate mofetil; PRED, prednisone; IL-2R, IL-2 receptor ; CNI, calcineurin inhibitor ; NTZ, nitazoxanide; AZM, azithromycin).
| Patient age/gender | kidney transplantation | Cryptosporidium infection | Treatment of vryptosporidiosis | Reference | ||||
| Time after | Immunosuppressive treatment | Symptoms | Environmental risk factor | Species (intensity) | Drugs | Treatment result | ||
| 60 | 8 years /1st graft |
TAC (4 mg/day) + MMF) (1 g x 2/day) + PRED(7.5 mg/day) | watery diarrhea, nausea, vomiting, weight loss (6 kg) | admitted to own a dog |
C. felis (5–10 oocysts/slide) |
NTZ (500 mg x 2/day for 14 days) | negative 2 weeks after treatment, with no recurrence of diarrhea observed 4 months | [40] |
| 64 | 2 years /1st graft | TAC (7 mg x 2/day), MMF (750 mg x 2/day), and PRED (10 mg/day) | watery diarrhea, abdominal pain, weight loss (13 Kg) | had travelled to Mali | C. hominis (>100 oocysts/slide) | 1. reduction of TAC | diarrhea regressed after 8 days, 3 months after therapy stools still tested positive | |
| 2. NTZ (500 mg x 2/day for 14 days) | One month stools were tested negative | |||||||
| 34 | 8 years /2st graft |
TAC (6 mg x 2/day), MMF (750 mg x 2/day), and PRED (25 mg/day). | watery diarrhea, abdominal pain weight loss (10 Kg) | had travelled to Kosovo | C. parvum (1–5 oocysts/slide) | 1. reduction of TAC | diarrhea was regressing 1 month after treatment | |
| 2. NTZ (500 mg x 2/day for 14 days) | months after the second treatment course, his stools were tested negative | |||||||
| 38 | 2 years /1st graft | ND | diarrhea | ND | ND | Spiramycin 2 g daily for 10 days | Symptoms resolved second days therapy and reduction oocyst | [41] |
| 42 | 1 year /1st graft |
ND | Abdominal pain, distention | ND | ND | Spiramycin 2 g daily for 10 days | After treatment no symptoms and oocysts | |
| 41/M | 1 year /1st graft |
ND | Weakness, fever of 39°C, yellowish diarrhea occurring 4-5 times daily without blood | ND | ND | NTZ 500 mg twice daily for 3 days. | successful recovery of Cryptosporidium spp. infection | [21] |
| 37 | 1st graft | ND | acute diarrhea, up to 10 times daily, abdominal discomfort, coryzal symptoms | ND | ND | paromomycin 1 g twice daily + AZM 500 mg daily | 1 week after treatment was still positive, after 4 weeks clinical and parasitological resolution |
[42] |
| 42/W | 1 year | TAC (present levels 8–10 ng/ml), MMF (1250 mg/day) and steroids (PRED, 5 mg/day) | abdominal pain, diarrhoea (5 days) | travelled to Cuba | ND | rifaximin (600 mg thrice daily), reduced MMF to 1 g/day | patient’s symptoms resolved within 1 week | [43] |
| 24/M | 1 month/ 2st graft |
TAC + MMF | chronic watery diarrhea, nausea | ND | ND | NTZ monotherapy | ineffective | [44] |
| NTZ (1 g twice daily) + AZM (600 mg daily) + rifaximin (550 mg twice daily) + intravenous fluids + diphenoxylate-atropine; AZM was stopped; TAC was 17 ng/mL, and it was discontinued and later restarted at a lower dose | diarrhea within 10 days without recurrence | |||||||
| 78/W | 9 years /1st graft |
Steroids 3 months post-transplant, TAC + MMF | watery diarrhoea without any pathological substance that had a 7 day evolution, without fever, vomiting or abdominal pain /sclerosing cholangitis | paromomycin + AZM of 14 days, subsequently NTZ for 6 days, doses of TAC and MMF were reduced | diarrhoea disappeared, kidney function recovered to basaline levels, 17 months later the patient was still asymptomatic | [45] | ||
| 60 | 3 months | MMF/CsA/Cs, MMF switched to AZA | Severe diarrhoea | Spiramycin 10 days | Resolved | [46] | ||
| 59 | 1 month | Sir/FK/Cs | Severe diarrhoea | Paromomycin 4 weeks | Resolved | [47] | ||
| 68/M | 56 months /1st graft |
Anti-IL2r CNI + MMF | Diarrhea, vomiting, dehydration, weight loss (8 kg), acute kidney injury, acidosis | Contact with animals and children | C. parvum | Reduced MMF or stopped until diarrhea resolved, 500 mg of NTZ twice a day for four weeks | for the three patients gastrointestinal disorders resolved in the first two weeks; MMF was newly initiated as soon as diarrhea resolved; no relapse was observed | [3] |
| 42/F | 25 months /1st graft |
Anti-IL2r CNI + MMF | Fever, abdominal pain, diarrhea, vomiting, dehydration, weight loss (4 kg) | Previous antibiotic therapy with amoxicillinclavulanic acid | Cryptosporidium spp. | |||
| 77/M | 14 days /1st graft |
Anti-IL2r CNI + MMF | Severe diarrhea, dehydration, weight loss (3 kg), acute kidney injury | Contact with untreated water | C. parvum | |||
| 53/M | 2 days /1st graft |
Anti-IL2r CNI + MMF | Diarrhea, vomiting, dehydration, weight los (4 kg) | Contact with cat | C. felis | |||
| 64/F | 65 months /1st graft |
Depleting therapy CNI + MMF | Fever, abdominal pain, diarrhea, vomiting, dehydration, weight loss (2 kg) | None | C. parvum | |||
| 37/F | 57 months /3st graft |
Desensitization, depleting therapy CNI + MMF | Fever, abdominal pain, diarrhea, vomiting, dehydration, weight loss (3 kg) | Work as a nurse, contact with recreative water, treated with phenoxymethylpenicillin | C. parvum | |||
Table 2.
Cryptosporidium spp. infections in adult kidney transplant recipients (M-FECT, modified formalin-ether concentration technique; MAF, modified acid-fast method; ZN, Ziehl-Neelsen; MZN, modified Ziehl-Neelsen; NR – not reported).
Table 2.
Cryptosporidium spp. infections in adult kidney transplant recipients (M-FECT, modified formalin-ether concentration technique; MAF, modified acid-fast method; ZN, Ziehl-Neelsen; MZN, modified Ziehl-Neelsen; NR – not reported).
| Country | Number of participation | diagnostic method | patients with diarrhea | citation | |
|---|---|---|---|---|---|
| all (n) | infected (n/%) | ||||
| Argentina | 26 | 11/42.3% | MAF after M-FECT | 0 | [25] |
| Türkiye | 69 | 13/18.8% | MAF | 8 | [41] |
| Brazil | 23 | 8/34.8% | ZN after FECT | - | [84] |
| India | 60 | 12/20% | MAF | 2 | [85] |
| India | 60 | 12/20% | MAF | 16.6% | [86] |
| Iran | 87 | 10/11.5% | MAF | - | [87] |
| Türkiye | 43 transplant (40 renal and 3 liver) | 7/21.2% | ZN | 40 | [88] |
| Pakistan | 644 | 343/53% | MZN | 343 | [89] |
| Sudan | 300 | 5/1.7% | NZN, MAF | ND | [90] |
| India | 358 | 13/8.4% | MAF after FECT | - | [91] |
| 307 | 30/9,8% | PCR | 26 | ||
| France | 88 | 41/46.6% | - | [92] | |
| 73 | 6/8.2% | MZN | 6 | [3] | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



