Submitted:
13 June 2024
Posted:
14 June 2024
You are already at the latest version
Abstract
This study documented the experiences of health system personnel in the implementation of mass distribution campaigns for the control of Lymphatic Filariasis in rural Guinea. This was an exploratory qualitative study using data collected from implementing actors of mass distribution campaigns in the Boké health district.
Results showed four main facilitators of mass distribution campaigns rollout in Boké health district: i) support to the district teams in the organization of the campaigns; ii) involvement of community-based associations in social mobilization; iii) strong adherence of the communities to the different mass distribution campaigns, facilitated through the involvement of community relays, who are members of these communities, in the distribution of drugs; and iv) transparency in the allocation of incentives to drug dispensers and supervisors.
However, the frequent shortages of medicines, the difficulties of access to rural areas and the lack of logistical means for the su-pervision of activities were the main obstacles to the success of the various mass distribution campaigns in Boké.
The provision of buffer stocks for special areas such as Boké by national program actors and partners, joint planning of campaign activities with local managers of health systems and services, and improvement of existing mechanisms for motivating health workers, including community health workers, during future campaigns should help to achieve national objectives in the fight against NTDs in Guinea.
Keywords:
experience
; mass distribution
; lymphatic filariasis
; Guinea
1. Introduction
Lymphatic filariasis is a parasitic disease transmitted to humans through the bite of an insect, the mosquito. The disease affects the lymphatic system, often resulting in abnormal enlargement of certain parts of the body such as the feet and scrotum. This is a severe disability and often causes social stigma [1]. According to recent estimates by the World Health Organization (WHO), about 17% of the world's population, mainly in Africa and Southeast Asia, is at risk of lymphatic filariasis [2].
In recent years, enormous progress has been made in the control of filariasis worldwide, thanks in particular to repeated chemoprevention in countries endemic for the disease [1]. In 2018 alone, 51 million new filariasis infections were reported worldwide; a 74% decline in the incidence of cases since the global elimination programme began in 2000 [1].
The experience of lymphatic filariasis elimination is well documented in several Asian and North African countries [3,4,5]. Abdoul et al. reported that the success of lymphatic filariasis elimination in Yemen was linked to good collaboration between national and international actors as well as the integration of efforts to control all other neglected tropical diseases (3–5). Other authors have also indicated that decentralization of the disease control activities to the community level, capacity building of local health facilities in the management of complicated forms (lymphedema, hydrocele, adenolymphangitis, etc.) including training and the provision of equipment, and supervision of health personnel have been important facilitators in the elimination of lymphatic filariasis in Yemen [4,5].
In Guinea, 24 out of 38 health districts in the country were endemic to lymphatic filariasis in 2013 [6]. Among these health districts, five were considered hyper endemic, namely Boké (13%), Forécariah (11%), Kérouané (12%), and Beyla (14%) [6]. However, efforts deployed by the government have resulted in reduction of disease prevalence in most endemic health districts, especially in Boké[7,8]. In fact, the disease prevalence has dropped from 13% in 2013 to 0.3% in Boké health district according to the results of the preliminary assessment survey of Lymphatic Filariasis Transmission conducted in 2021 [7]. Similarly, another assessment survey conducted in 2022 found no cases of lymphatic filariasis among nearly 1,600 children sampled and tested in the Boké health district [8].
Despite this success, little is known about the determinants of the success of lymphatic filariasis control in Boké health district. This study was therefore initiated to document the experience of health system personnel in Boké in implementing mass distribution campaigns for lymphatic filariasis control. Specifically, this study aimed to explore health system personnel’s perceptions of the rollout of facilitators in mass distribution campaigns and describe best practices and obstacles that health system personnel faced in implementing these mass distribution campaigns. The findings of this study could provide the national programme for neglected tropical disease (NTD) control with relevant information for the control and elimination of lymphatic filariasis control in the country as well as other NTDs in Guinea and other similarly affected countries.
2. Materials and Methods
2.1. Type and Period of Study
This was an exploratory qualitative study to document the experience of implementing health system personnel in mass distribution campaigns against lymphatic filariasis in Boké health district, Guinea, in 2022.
2.2. Study Settings
2.2.1. General Parameters
The Republic of Guinea is located in West Africa and has 38 health districts. Its population was estimated at 13 million in 2022 [9,10]. The majority of the population live in rural areas (65%) and beneath the poverty line (55%). The health system is tiered to a primary level (413 health centres and 726 health posts), a secondary level (26 prefectural hospitals, 7 regional hospitals and 8 medical centres) and a tertiary level (3 national reference hospitals) of health facilities. [11].
2.2.2. Specific Parameters
The study was conducted in the health district of Boké. This rural health district is located at a distance of nearly 250 kilometres from the capital city, Conakry. It had an estimated population of 568 thousand inhabitants in 2022 [9]. Agriculture, fishing, and animal breeding are the main activities carried out by the population of Boké health district.
The local health system includes a health district management team, a district hospital, 13 health centres (10 of which are located in rural areas), and 53 health posts (See Figure 1 - map of Boké and the study sites).
Lymphatic Filariasis Control in Guinea
The strategy for lymphatic filariasis control in Guinea is in line with WHO recommendations and consists of preventive (chemotherapy) and curative (management of cases) services. Significant efforts have been made in recent years to control lymphatic filariasis in Guinea. Among these efforts is the mass administration, on an annual basis, of Ivermectin and Albendazole to people aged 5 years and older in all endemic districts. During the five years of mass treatment against lymphatic filariasis, the health district of Boké has recorded very good epidemiological coverage of 65% or more [6].
With respect to the management of complications of lymphatic filariasis (lymphedema and hydroceles), training of community health workers was provided in 24 health districts for the detection of complications and the reporting of information to the district and regional levels. This was accompanied by training of surgeons and surgical staff in all regions endemic for the disease. The management of complications of lymphatic filariasis is individual at the level of the surgical services and it is the responsibility of patients since 2021 to present themselves for treatment.
2.3. Study Participants and Recruitment
According to the levels of the health pyramid in Guinea, three [3] groups of participants were interviewed in this study: managers of the national programme for the control of NTDs at national, regional and district levels; health service managers and healthcare providers; and social mobilizers involved in the distribution campaigns in Boké.
2.4. Data Collection Technique and Tool
Data were collected through in-depth individual interviews with the implementing actors (health personnel involved in the distribution of the drugs, Ivermectin and Albendazole).
The key informant interviews allowed us to better understand the best practices, facilitators and challenges of implementing mass distribution campaigns for lymphatic filariasis control in Boké health district. These key informants were selected based on their involvement in the implementation process of the lymphatic filariasis mass distribution campaigns in Boké.
Interview guides were developed for the different stakeholder groups targeted in the study. The guides were developed based on the research questions of the study, including best practices adopted in the implementation of the campaigns, facilitators and obstacles to the implementation of filariasis control campaigns in Boké. The interviews were recorded using a smartphone, after obtaining permission from the participants.
2.6. Data Analysis
The interviews were literally transcribed and this was followed by thematic analysis. A list of terms was generated using a deductive approach. All the transcripts were coded manually using an Excel spreadsheet. The diversity of data sources contributed to the internal validity of the study through triangulation [12].
2.7. Ethical Considerations
The research protocol for this study was approved by the National Health Research Ethics Committee of Guinea (number: N-114-CNERS-22) before data collection began.
3. Results
3.1. Profile of Health System Personnel Interviewed in the Study
A total of 18 participants were interviewed for this study, including health system personnel from the regional and district management teams, skilled healthcare providers and community health workers. Of the 18 participants who were interviewed, 14 (78%) were men and 4 were women (22%). Their characteristics are shown in Table 1.
3.2. Health System Personnel Perceptions of Facilitators for the Implementation of Mass Distribution Campaigns for Lymphatic Filariasis Control
Analysis of interviews with the study participants revealed four [4] main facilitators of the implementation of mass distribution campaigns for lymphatic filariasis control in Boké health district.
The first reported facilitator was the support given to the district teams in organizing the campaigns. This support consisted of the mobilization of material, financial and human resources necessary to conduct these campaigns. The availability of material, human and financial resources during the mass distribution campaigns in Boké health district enabled the teams to comply with the national directives required for the implementation of these campaigns, in particular the organization of cascade training involving, from the top to the bottom level, the national supervisors, the regional and district level trainers, the managers of the primary health care facilities (health centres), the proximity supervisors, and the community distributors. Another aspect of this support, according to respondents, was the provision and distribution of work tools such as registers, height measurement tools and medicines to community distributors.
The second facilitator of the successful implementation of mass distribution campaigns was the involvement of community-based associations-such as women and youth groups as well as community leaders in social mobilization, as illustrated by the respondent below.
" .... Sometimes, we involve women leaders and religious leaders in community mobilization... Each of these actors plays a role in removing community reluctance towards the campaigns... For example, if community health workers fail to remove the reluctance, they call on the sector chief, and so on up to the district supervisor..." EIA 03, Community Health Worker, Male.
The third reported facilitator was the strong support of the communities for the various mass distribution campaigns. According to the respondents, medication adherence was facilitated by the involvement of the community health workers (who are members of these communities) in drug distribution. Respondents also mentioned that providing CHWs with picture boards facilitated their work of informing communities about the risks of lymphatic filariasis and their consequences.
"In 2019, in Fria and Coyah health districts people who received Praziquantel during the distribution campaign developed reactions [side effects] ... If it had not been for the involvement of the communities [community health workers] in our various distribution campaigns, we would not have been able to overcome the reluctance [and get the communities to adhere]”. EIA 01, Regional health system manager, Male.
Finally, the fourth reported facilitator was the transparency involved in the allocation of field bonuses for drug distribution agents and supervisors. According to the respondents, this transparency in the allocation of field bonuses was key in motivating local health system actors to carry out the activities planned for the achievement of the campaign coverage objectives.
3.3. Best Practices Undertaken by Health System Personnel in Implementing Mass Distribution Campaigns against Lymphatic Filariasis
Several best practices emerged from the interviews with respondents. First, it was emphasized that simulation sessions were organized for the distribution agents in Boké health district. These simulation sessions included filling out the register for counting and distributing medicines, the attitude to adopt towards communities, including what clothing to wear, and the key messages to convey during community awareness-raising.
"... During the training, we break up the groups to do the simulation... We make sure that the distribution agents understand how to proceed in the field, through simulation sessions..." EIA 03, community health worker, Male
"In carrying out the practice, [we have] charts on which the agents are trained on reporting the quantities of tablets used, how to proceed with tracing the registers and measure the height... We also do demonstrations on how to take the height, how to administer the tablets..." EIA 13, Health Centre Manager, Female.
Second, another best practice identified was the adaptation of national planning and strategies to the local realities. For example, it was noted that health system personnel in the Boké health district recruited additional community supervisors to cover all endemic localities, including those omitted in the initial planning by the central level actors. In such circumstances, the initial planned field bonuses were distributed to all supervisors, including those mobilized at the last moment.
"... Sometimes also, some remote areas are omitted from the national [NTD] program planning, due to lack of resources.... In such circumstances, we rework the composition of the teams and redeploy supervisors and distribution agents... We also ensure the provision of vehicles and fuel to these teams to cover the omitted areas... If two supervisors were originally planned, but we have a need for five supervisors, we deploy the five supervisors and redistribute the field bonuses of the two supervisors to the five who actually participated in the work" EIA 01, Regional health system Manager, Male.
It was also reported that some health centre managers used their facility's revenues to support the deployment and motivation of distribution agents in hard-to-reach locations. For example, participants mentioned that due to the limited number of inhabitants in some villages, central or district team planning would rarely take these locations into account. In these contexts, health centre managers would deploy additional teams of distribution agents from their revenue to cover these locations and allow for coverage of their entire health area.
"When a health centre chief reports such a situation to us, we tell him to draw on their revenue but to justify it.... There are also islands, you know, islands where you have to rent boats [canoe], which requires resources because they are often mobilized for entire days... We can rent a canoe for 2,000,000 GNF per day...". EIA 01, Regional health system manager, male.
A third best practice was advocacy with local authorities for the mobilization of additional material and logistical resources. It was explicitly reported that local authorities were involved in mobilizing means of transportation (motorcycles, canoes) to facilitate the access of distribution agents to remote locations.
"For example, if we say that a team must reach 50 people, you will find that there is a village 20-25 km away and there are only 5 people there, so you need a special motivation... The islands too, there are islands. Perhaps the programme says that we take only 5 islands whereas there are 15 islands in Boké. It is necessary then to sensitize those who have the canoes to help us.... Or we can go to the local authorities to request support to reach these populations...". EIA 01, Regional health system manager, male.
3.4. Obstacles Faced by Health System Personnel in Mass Distribution Campaigns for the Control of Lymphatic Filariasis
From the interviews with the participants, it emerged that five main obstacles undermined the implementation of the mass distribution campaigns for the control of lymphatic filariasis in Boké health district.
The first obstacle was the centralized planning of the distribution campaigns, which could result in shortcomings or omissions in the estimation of resources needed for the campaign. However, health district and services managers undertook initiatives to reduce the effect of these omissions or shortcomings on the effective implementation of the campaigns. Among these adaptation measures were the reorganization of the supervision teams, the deployment of additional distribution agents and the mobilization of additional resources (financial, human, and logistics) to support the campaigns.
"In the case of the islands, we find the means to send a boat to the islands or to rent a boat… To send a team more than 50 km away, we must send a motorcycle, if the service has a motorcycle. But if the service does not have a motorcycle, we have to rent it and pay for the fuel, and the person who goes there has to be given a bonus to encourage him”. EIA 01, Regional health system manager, Male.
The second obstacle was the frequent stock outs of medicines in certain localities during the distribution campaigns. These drug stock outs were said to be maintained by uncontrolled movements of populations in the mining areas of Boké health district. Faced with such a situation, participants stressed that coordination and communication between teams of supervisors were often used to solve these problems of drug shortages.
"It is that there are movements of our population, often underestimated in mining areas, which leads to shortages of medicines, especially deworming medicines, and the quantity that comes is insufficient for the needs”. EIA 04, health centre chief, male.
The third obstacle was the reluctance of some communities to participate in the campaigns. This reluctance was reportedly due to the adverse events experienced by some children in Fria and Coyah following the administration of drugs (Praziquantel). Other participants also mentioned that this reluctance was related to false rumours about the effects of mass drugs and medical products administered during campaigns on the fertility of communities.
"People say that the medicine we give them affects women's fertility..." EIA 11, Community Health Worker, male.
The fourth obstacle was the difficulty of accessing certain areas of the Boké health district, particularly the remote areas and the islands. Regarding the difficulty of access to certain localities, we provide the following quote from a community health worker.
"The sectors are too far apart. However, if it is not for the community, we cannot accept that. If you have to go to a locality where you are going to pay 40,000 GNF for transport to and from the location, if you are given 50,000fg what are you going to do with that? So, we have to look at the transportation of the people who travel according to the distances they cover". EIA 15, community health worker, female.
Finally, it emerged that the implementation of mass distribution campaigns for the control of lymphatic filariasis often coincided with periods of intense agricultural activities by the population.
"If it is at the time of the rainy season, at the time of cultivation when we go to certain villages, it is difficult to find people" EIA 03, community health worker, male.
The facilitators, best practices and obstacles are summarised in Figure 2.
4. Discussion
This study explored the facilitators, best practices and barriers to the implementation of mass distribution campaigns for the control of lymphatic filariasis in the health district of Boké, Guinea. Our results show that the involvement of community members in drug administration and the adaptation of national guidelines to local realities were respectively key facilitators and best practices for the success of the distribution campaigns in Boké. However, drug shortages during the campaigns were noted as one of the main obstacles to the effective implementation of the distribution campaigns in Boké.
This study has one main limitation that should be noted. It is possible that our data are associated with (recall) bias since some of the distributors surveyed had not been involved in drug distribution for 2 years.
The involvement of community members, particularly community health workers, was an important facilitator of successful mass distribution campaigns for the control of lymphatic filariasis in Boké. In the Guinean context, community outreach workers are recruited by the communities themselves under the supervision of local health service managers (head of health centres). Their selection follows rigorous criteria such as being able to read and write, having a good reputation within their community, being motivated and able to serve their community, and being able to speak the local language. The use of community members in the administration of drugs in their communities contributed to the fight against community reluctance to participate and adhere to medication and false rumours. The use of community members in drug distribution has already been documented in Kenya as an effective means of communication and community adherence to lymphatic filariasis control campaigns [2]. Silumbwe et al. in their systematic review also highlighted that raising awareness through innovative community participation programmes and building partnerships and collaborations with community members in organizing campaigns were facilitators in the implementation of mass distribution campaigns against filariasis in sub-Saharan Africa [2]. The findings of our study emphasise the need for decision-makers in the national programme for NTDs control to safeguard the involvement of community members in the mass distribution campaigns. National policies and health system actions should also work to improve the motivation of community health workers to achieve the national objectives of the fight against NTDs. The motivation needed could include provision of equipment (torch, bag, telephone, etc.) and means of transportation (bicycle, motorcycle, etc.). This recommendation is all the more obvious as findings from this study show how difficult working conditions may be – for example, long distances from the villages and blocks to be covered, poor road networks, insufficient incentives, etc.
Our study also showed that the adaptation of national guidelines for mass distribution campaigns to local realities was an essential best practice for the effective implementation of lymphatic filariasis distribution campaigns in Boké. The adaptation of national guidelines included the redefinition of the areas to be covered, the composition of supervisory teams and the local mobilization of additional resources (logistical, human, financial, etc.) to achieve campaign coverage objectives. The findings reflect the experience, positive aptitude and motivation of the managers of the health system and services in Boké for the implementation of mass distribution campaigns.
The findings also call on the key personnel of the national programme for NTDs control and their partners to work towards decentralizing the planning and implementation of distribution campaign activities. Indeed, the readjustments of directives to overcome the shortcomings in the central planning of campaign activities played an important part in the overall success of the activity. For example, faced with insufficient human and financial resources to cover all areas of the Boké health district, an area endemic for filariasis, the implementing health system personnel resorted to using revenues from the health centres. In the short and medium term (1-3 years), joint planning of campaign activities with local health system personnel should be considered by national officers for the control of NTDs. In the long term, decentralization of the planning and execution of campaign activities to the district level should be considered by the national NTD programme. In such an organizational arrangement, the national NTD control programme would have the role of mobilizing resources, supervising campaigns, and evaluating the impact of these campaigns, among other things. All of this would contribute to anticipating potential undesired effects (e.g., weak financial and organizational autonomy of health centres) on local health structures and to sustaining the achievements of the national programme for the control of NTDs in order to reach national control objectives. These recommendations on the progressive decentralization of NTD control activities are relevant to consider as mass distribution campaigns are increasingly seen as non-essential to interrupting lymphatic filariasis transmission in West Africa due to low levels of the disease transmission in the region [5].
Frequent drug shortages during distribution campaigns were noted as a major obstacle to the effective implementation of mass distribution campaigns in Boké. This obstacle has already been documented by other authors in Africa and elsewhere [13]. In our study, this result was related to uncontrolled population movements in the mining areas of Boké, leading to miscalculations in the population estimates. This finding of frequent drug shortages suggests the need for the national NTD programme to provide buffer stocks for Boké district, and other similar areas in Guinea, during mass distribution campaigns.
5. Conclusions
The results of this study showed that there are several factors that determine the success of mass distribution campaigns for the control of lymphatic filariasis in Boké health district. These factors include, among others, the involvement of communities in the distribution of drugs, the significant mobilization of human, financial and logistic resources, and the existence of experienced and motivated local teams for the execution of campaign activities. However, the frequent shortages of medicines, the difficulties of access to rural areas, and the lack of logistical means for the supervision of activities are the main obstacles to the success of the various mass distribution campaigns in Boké. The provision of buffer stocks for special areas such as Boké by national program officers and partners, joint planning of campaign activities with local managers of health systems and services, and improvement of existing mechanisms for motivating health workers, including community health workers, during future campaigns should help to achieve national objectives in the fight against NTDs in Guinea.
Author Contributions
Delphin kolie, study design, research methods, data interpretation, critical revision of the article , Lamine lamah, interpretation of data, critical revision of the article. Nouhou konkoure Diallo and Aissatou Tounkara research methods, data analysis. Pr. Mamadou camara, research methods, interpretation of data, critical revision of the article. Pr. Alexandre Delamou and Hawa Manet study design, research methods, data interpretation, final approval of the version to be published.
Funding
This SORT IT course on NTDs in Guinea was funded by TDR, the Special Programme for Research and Training in Tropical Diseases at the World Health Organization (WHO) and implementing partners. TDR is able to conduct its work thanks to the commitment and support from a variety of funders. A full list of TDR donors is available at https://tdr.who.int/about-us/our-donors.
Acknowledgments
This research was conducted through the Structured Operational Research and Training Initiative SORT IT) a global partnership coordinated by the Special Programme for Research and Training in Tropical Diseases (TDR) at the World Health Organization (WHO). The specific SORT IT on Neglected Tropical Diseases (NTDs) that led to these publications included a partnership of TDR with the National Directorate of Epidemiology and Diseases Control of the Ministry of Health of Guinea, the Africa Center of Excellence for Prevention and Control of Communicable Diseases (CEA-PCMT) of the University Gamal Abdel Nasser of Conakry, the National Program for Control of Neglected Tropical Diseases of Guinea, the Reseau National pour la Recherche Opérationnelle en Guinée (RENAROG), and the WHO country in Guinea.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
References
- Filariose lymphatique [Internet]. [cité 27 mai 2022]. Disponible sur: https://www.who.int/fr/news-room/fact-sheets/detail/lymphatic-filariasis.
- Silumbwe, A.; Zulu, J.M.; Halwindi, H.; Jacobs, C.; Zgambo, J.; Dambe, R.; Chola, M.; Chongwe, G.; Michelo, C. A systematic review of factors that shape implementation of mass drug administration for lymphatic filariasis in sub-Saharan Africa. BMC Public Heal. 2017, 17, 484. [Google Scholar] [CrossRef] [PubMed]
- Al-Kubati, A.S.; Al-Samie, A.R.; Al-Kubati, S.; Ramzy, R.M. The story of Lymphatic Filariasis elimination as a public health problem from Yemen. Acta Trop. 2020, 212, 105676. [Google Scholar] [CrossRef]
- Yajima, A.; Ichimori, K. Progress in the elimination of lymphatic filariasis in the Western Pacific Region: successes and challenges. Int. Heal. 2020, 13, S10–S16. [Google Scholar] [CrossRef] [PubMed]
- Ramzy, R.M.; Kamal, H.A.; Hassan, M.A.; Haggag, A.A. Elimination of lymphatic filariasis as a public health problem from the Arab Republic of Egypt. Acta Trop. 2019, 199, 105121. [Google Scholar] [CrossRef] [PubMed]
- Programme national de lutte contre les maladies tropicales négligées en Guinée. Plan directeur de la lutte contre les maladies tropicales négligées en Guinée. Conakry ( Guinée): Ministère de la santé; 2018 déc p. 80.
- Guinea_Rapport_Enquête pre-TAS_Boké-Guéckédou_2021.docx.
- Programme national de lutte contre les maladies tropicales négligées. Rapport d’enquête d’évaluation de la transmission de la filariose dans le district sanitaire de Boke (tas 1). 2022 mai p. 11.
- Institut national de la statistique. Troisieme recensement général de la population et de l’habitation (rgph3). 2017 déc.
- Ministère de sante. Plan nation de développement sanitaire ( pnds) 2015 -2024 [Internet]. 2015 mars. Disponible sur: https://www.prb.org/wp-content/uploads/2018/05/Plan-National-de-De%CC%81veloppement-Sanitaire-2015-2024.-Guine%CC%81e.pdf.
- Loubna B, Delphin K, Hawa M, Salim CB, Harouna M, Etienne G, et al. Protocole de recherche : « étude socio anthropologique sur l’organisation de la prise en charge du VIH en Guinée ». :12.
- Levac, D.; Colquhoun, H.; O'Brien, K.K. Scoping studies: advancing the methodology. Implement. Sci. 2010, 5, 69–69. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, E.; Kelly-Hanku, A.; Krentel, A.; Romani, L.; Robinson, L.J.; Nery, S.V.; Kaldor, J.; Steer, A.C.; Bell, S. Community perceptions and acceptability of mass drug administration for the control of neglected tropical diseases in Asia-Pacific countries: A systematic scoping review of qualitative research. PLOS Neglected Trop. Dis. 2022, 16, e0010215. [Google Scholar] [CrossRef]
Figure 1.
Study sites.
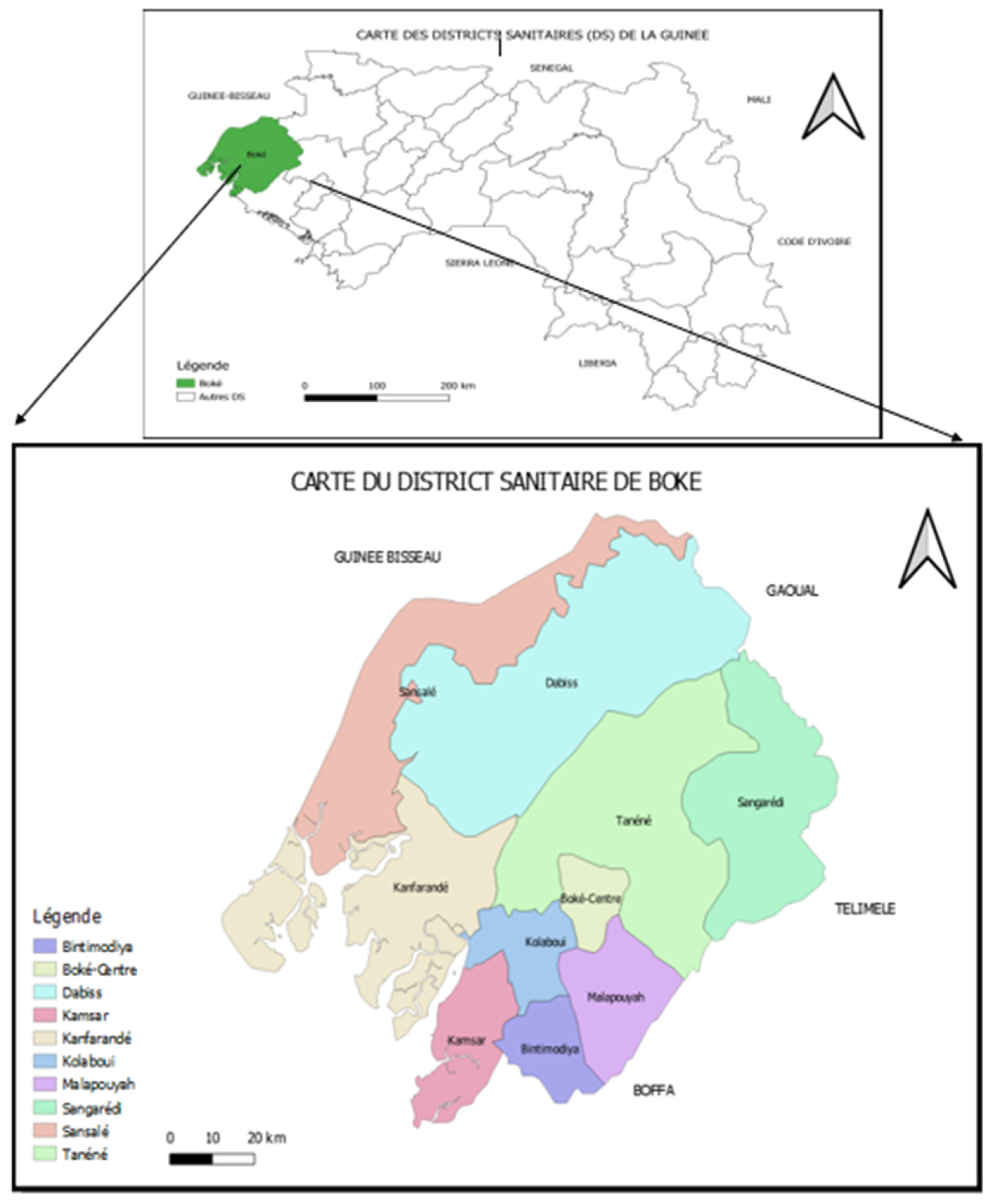
Figure 2.
Summary of facilitators, best practices, and barriers to implementing mass distribution campaigns for lymphatic filariasis control in the health district of Boké, Guinea, 2022.
Figure 2.
Summary of facilitators, best practices, and barriers to implementing mass distribution campaigns for lymphatic filariasis control in the health district of Boké, Guinea, 2022.
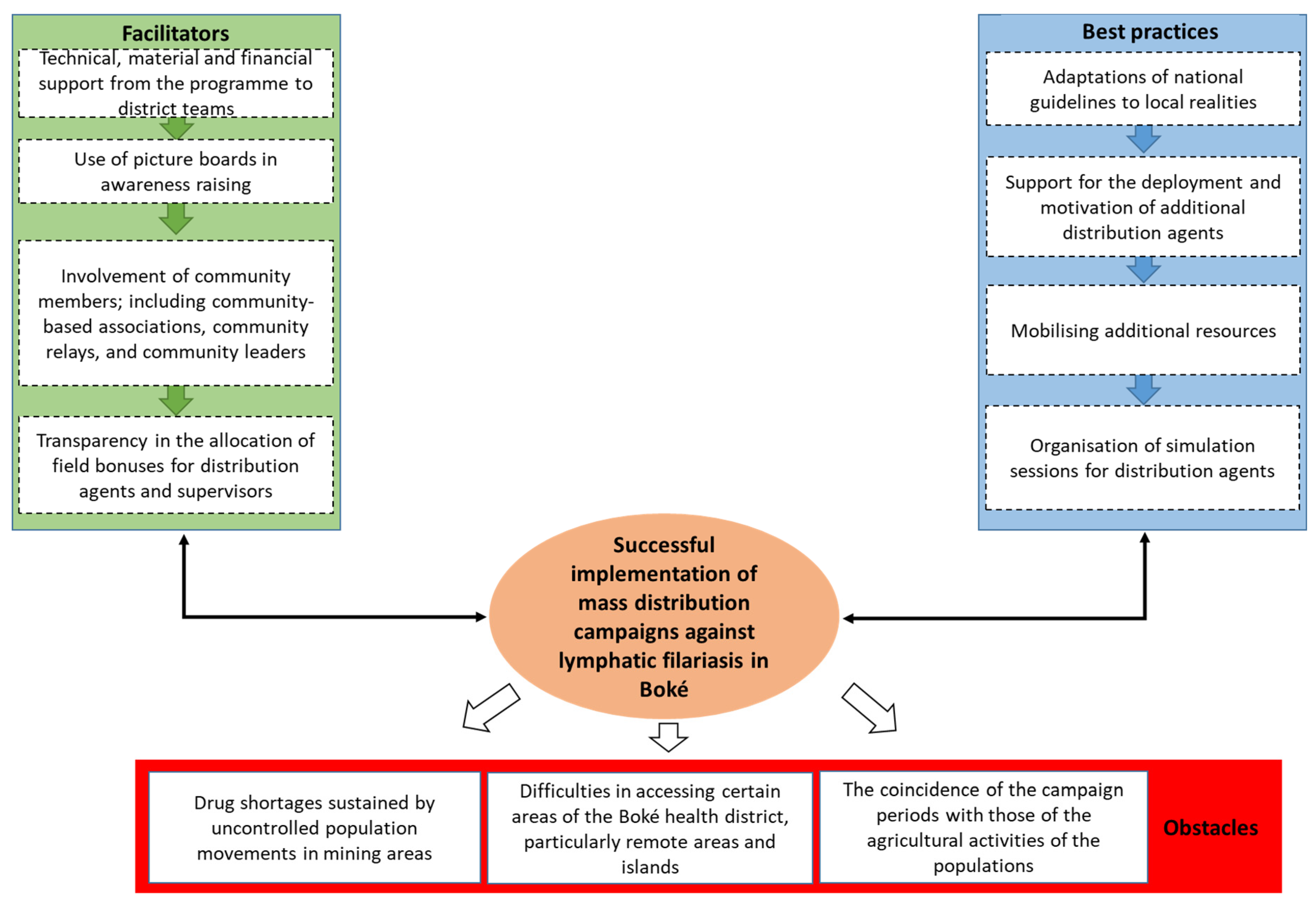

Table 1.
Profile of health system personnel participating in the study, Boké Health District, N=18.
| Profile | Number (%) |
|---|---|
| Health system and services managers | 03 (17) |
| Skilled healthcare providers | 10 (55) |
| Communities (Community Leaders, community health workers ) | 05 (28) |
| Sex | |
| Men | 14 |
| Women | 4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



