
Submitted:
07 May 2024
Posted:
10 May 2024
You are already at the latest version
Abstract
There is increasing evidence that myocarditis starts as a patchy process, accordingly, the detection of segmental affection is important for early recognition of the disease and proper initiation of anti-inflammatory treatment. We present our first experience here with using speckle-tracking echocardiography to detect subtle segmental involvement of the left ventricle in two cases with suspected myocarditis. STE consolidated the diagnosis and helped with the early initiation of intravenous immunoglobulins and subsequent control of the disease. STE was also able to show the specific topography of distribution, of each pathogen linked to inflammation.
Keywords:
speckle tracking echocardiography
; myocarditis
Background:
Myocarditis is an inflammatory myocardial disease. It can result from viral infections due to molecular mimicry and autoimmunity or can even be associated with autoimmune and autoinflammatory disorders. [1]
It can range from a patchy disease with mild or no manifestations to a diffuse myocardial involvement with significant hemodynamic compromise.[2,3] There is no definite evidence on the percentage of cases progressing from patch to diffuse involvement, and there is also no definite proof whether fulminant cases started as a focal process or as a diffuse inflammation from scratch.
The diagnosis, of myocarditis is also, to date, a point of significant debate. One of the most adopted criteria has been suggested by Caforio et al and includes the presence of one clinical manifestation among acute chest pain, new onset dyspnea, cardiogenic shock, or unexplained syncope, in addition to one positive laboratory or imaging evidence of myocardial affection such as gadolinium enhancement by cardiac magnetic resonance (CMR), positive endomyocardial biopsy, echocardiographic evidence of global or segmental myocardial dysfunction, elevated cardiac enzymes. [1,4]
CMR and too endomyocardial biopsy are expensive, lengthy, or invasive, to be performed, in a stable patient, and elevated cardiac enzymes and/or ST elevation in ECG are non-specific as they can be induced by pericarditis. Hemodynamically stable patients are also not expected to display evidence of global myocardial dysfunction.
The latter points are major flaws in Caforio’s criteria and raise the need for exploring techniques that can detect segmental dysfunction of the myocardium, which can be justified and specific in stable patients and can also be easily performed in hemodynamically unstable patients.
We present two cases of chest pain, where we used 2D speckle tracking via automated functional imaging to prove segmental myocardial involvement as evidence of early myocarditis.
Case Summaries:
Case 1:
A 15-year-old, previously healthy male, presenting 1 month after recovering from influenza A infection with 2 days history of severe chest pain, diffuse, not radiating. They were associated with Upper respiratory tract symptoms and dizziness while standing. The physical examination was unremarkable. CXR was normal. ECG performed showed sloping ST elevation in anteroseptal leads (Figure 1A). Bedside routine echocardiography showed normal myocardial function. Initial investigations showed Normal CBC, elevated cardiac enzymes troponin 1,441, BNP was 147, and total CK 1,062 IU/L. The patient was initially diagnosed with pericarditis and started on Ibuprofen with a plan for follow-up to repeat labs and initial conventional echocardiography showed preserved left ventricular function. One week later, he came with worsening chest pain and as shown in Figure 1B, Troponin levels jumped from 1441 to 2600, at this stage, we decided to perform speckle-tracking echocardiography that demonstrated segmental affection, mainly involving the basal anterolateral segments of the myocardium (Figure 2), with overall preserved global strain, aligning with the apparent absence of LV dysfunction.
Due to the rising titer of cardiac Troponins, a multidisciplinary team decided the administer of intravenous immunoglobulins, which dramatically improved the clinical manifestations and led to a steep decrease in serum Troponin.
Case 2
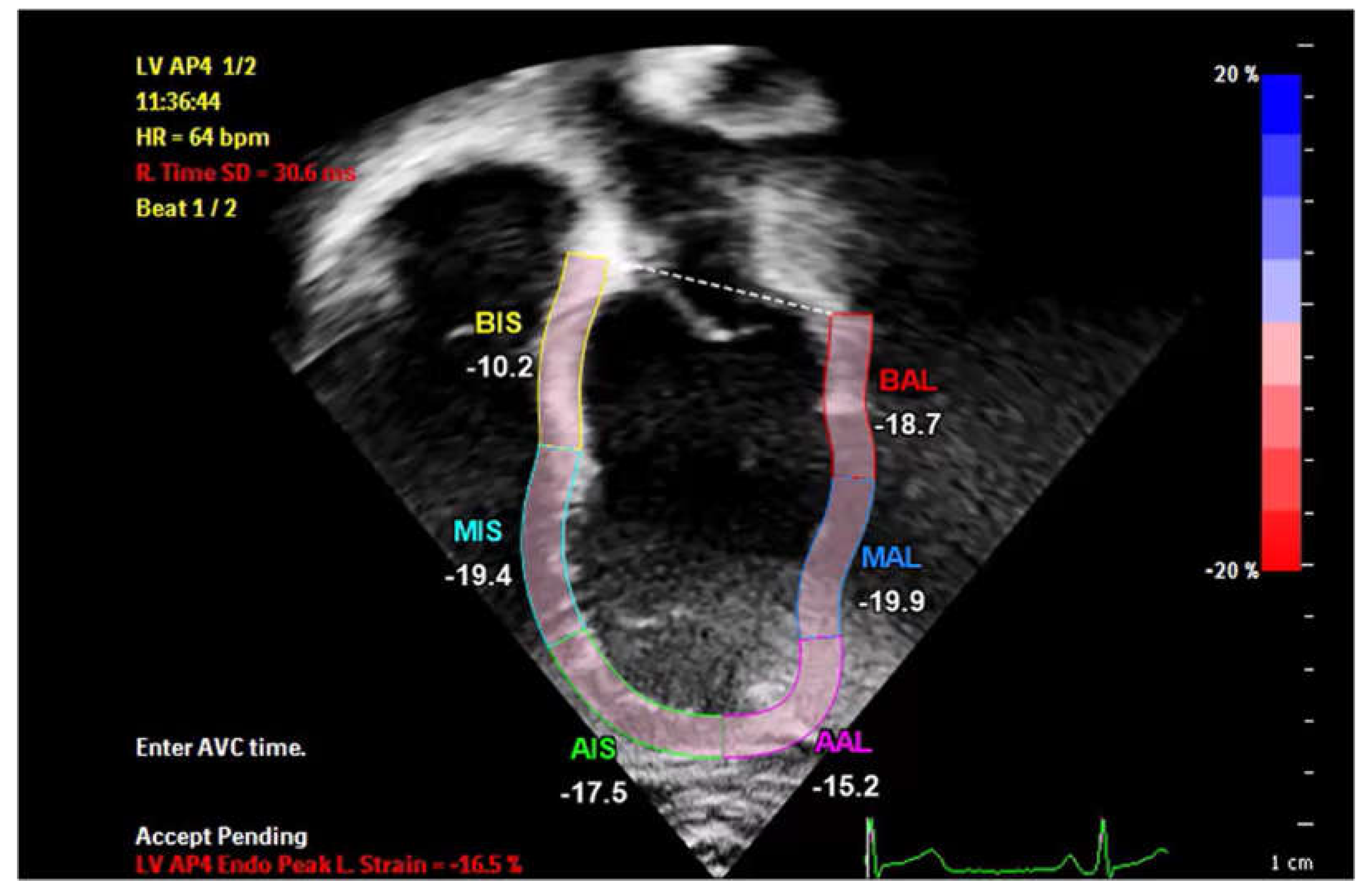
A 16-year-old male patient, presented with chest pain to the ER, alongside symptoms of upper respiratory infection, respiratory panel testing revealed to be adenovirus positive. The patient was hemodynamically compensated with unremarkable cardiac examination. Work-up for cardiac causes of chest pain revealed elevated serum Troponin T and non-specific elevation of the ST segment in the anteroseptal leads (juvenile repolarization pattern-Figure 3A), patient was admitted for observation, and for serial Troponin T testing, which showed persistent elevation at 800 ng/dL (Figure 3B). Following the persistence of manifestations and the lagging Troponin T levels, we performed a speckle-tracking examination of the patient, which, once again displayed a segmental affection of the basal septal part of the LV (Figure 4). At this stage, a dose of intravenous immunoglobulins was administered to the patient, after which there was a progressive decrease in cardiac enzyme levels, normalizing 15 days approximately after the dose. (Figure 3B)
Discussion:
Speckle-tracking echocardiography was initially investigated as a segmental tool that can gradually potentiate the role of echocardiography in coronary syndromes. However, it gradually gained popularity as a global tool, that can diagnose early dysfunction in systemic disease, particularly in cardio-oncology. [5]
Our case series revives the segmental power of STE and shows that it can differentiate pericarditis from myocarditis without resorting to costly and lengthy CMR.
The available studies about the role of 2D or 3D strain in myocarditis mainly focus on global strain in early myocarditis and have been almost exclusively performed in adults, where segmental involvement can be biased by coronary affection. Supel and colleagues benchmarked global 2D strain against CMR in adult patients with myocarditis and found that cases who displayed edema in CMR were more likely to have a significant decrease in GLS by STE. [6]
A case report by Uziębło-Życzkowska, also demonstrated a decreased global strain, despite a preserved LV EF, with an involvement of the basal posterior segments, that aligned with areas of gadolinium enhancement by CMR. [7]
Another interesting study of 3D strain vs. CMR, showed once more that dysfunctional segments by STE corresponded to areas of gadolinium enhancement by CMR. [8,9,10]
In our study, STE was able to demonstrate segmental involvement, before global dysfunction, and was a game-changer in early treatment and significant biochemical improvement of patients.
Another interesting finding of our study was the different distribution of myocardial inflammation in the two cases. Case 1 had a history of influenza, and dysfunction was mainly noted in the basal anterior segments, while case 2, who tested positive for adenovirus, had a basal septal involvement.
An interesting article by Karev et al discusses, how different viruses have divergent tropism to the myocardium, leading to heterogenous affection of cardiomyocytes. For instance, human herpes 6, infects the basal septum, while parvovirus involves the post. There is little or no knowledge of the specific tropism of influenza or adenovirus, before this case series, and two cases are not robust enough to suggest a specific tropism, but might be sight-opening to another advantage of STE, which is the determination of the specific tropism of viruses to certain regions of the cardiac muscle. [11]
Conclusion:
STE was extremely validated in systemic disorders, but its potential role in bedside diagnosis of early focal myocarditis can be a game changer not only in reversing early inflammation but also in recognition of specific viral signatures and tropism to the myocardium.
Author Contributions
Conceptualization, AA, SAD; Methodology, AA, AK, ZC, AM, AG, SAD; software, AA, AK, ZC, AM, AG, SAD; investigation, AA, AK, ZC, AM, AG, SAD; resources, AA, AK, ZC, AM, AG, SAD; data curation, AA, AK, ZC, AM, AG, SAD; writing—original draft preparation, AA, AK, ZC, AM, AG, SAD; writing—review and editing, AA, AK, ZC, AM, AG, SAD; supervision, AA; project administration, AA, SAD; funding acquisition, (none) All authors have read and agreed to Figthe published version of the manuscript.”
Institutional Review Board Statement
IRB approval number is RS-844
Informed Consent Statement
Patient consent has been obtained
Data Availability Statement
All data is made available within the manuscript.
Acknowledgment
As a first author I wanted to dedicate this work to my three children George, Maria and Mark, as they remain my fuel to improve myself
Conflicts of Interest
The authors declare no conflict of interest.
References
- Tschöpe C, Ammirati E, Bozkurt B, Caforio ALP, Cooper LT, Felix SB, Hare JM, Heidecker B, Heymans S, Hübner N, Kelle S, Klingel K, Maatz H, Parwani AS, Spillmann F, Starling RC, Tsutsui H, Seferovic P, Van Linthout S (2021) Myocarditis and inflammatory cardiomyopathy: current evidence and future directions. Nat Rev Cardiol 18:169–193. [CrossRef]
- AbdelMassih AF, Al Ali A, Musleh AS, Ramsi M (2023) Revisiting the role of ischaemia in familial cardiomyopathy: insights from an NRAP gene-related cardiomyopathy. BMJ Case Rep 16:e256111. [CrossRef]
- AbdelMassih A, El-Saiedi S, Hendawy R, Esmail R, AbdelHameed M, Sobeih A, Kharabish A, Diab N, Gaber H, El-Husseiny N, Agha HM (2023) Sphericity index for bedside diagnosis of acute myocarditis. Egypt Pediatr Assoc Gaz 71:68. [CrossRef]
- Caforio ALP, Pankuweit S, Arbustini E, Basso C, Gimeno-Blanes J, Felix SB, Fu M, Heliö T, Heymans S, Jahns R, Klingel K, Linhart A, Maisch B, McKenna W, Mogensen J, Pinto YM, Ristic A, Schultheiss H-P, Seggewiss H, Tavazzi L, Thiene G, Yilmaz A, Charron P, Elliott PM, European Society of Cardiology Working Group on Myocardial and Pericardial Diseases (2013) Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J 34:2636–48, 2648a-2648d. [CrossRef]
- Iskander J, Kelada P, Rashad L, Massoud D, Afdal P, Abdelmassih AF (2022) Advanced Echocardiography Techniques: The Future Stethoscope of Systemic Diseases. Curr Probl Cardiol 47:100847. [CrossRef]
- Sharifkazemi M, Rezaian G, Lotfi M (2023) Evaluation of myocardial performance by serial speckle tracking echocardiography in diagnosis and follow-up of a patient with eosinophilic myocarditis. Echo Res Pract 10:1–12. [CrossRef]
- Uziȩbło-ZYczkowska B, Mielniczuk M, Ryczek R, Krzesiński P (2020) Myocarditis successfully diagnosed and controlled with speckle tracking echocardiography. Cardiovasc Ultrasound 18:1–4. [CrossRef]
- Goody PR, Zimmer S, Öztürk C, Zimmer A, Kreuz J, Becher MU, Isaak A, Luetkens J, Sugiura A, Jansen F, Nickenig G, Hammerstingl C, Tiyerili V (2022) 3D-speckle-tracking echocardiography correlates with cardiovascular magnetic resonance imaging diagnosis of acute myocarditis – An observational study. IJC Hear Vasc 41:. [CrossRef]
- Supeł K, Wieczorkiewicz P, Przybylak K, Zielińska M (2023) 2D Strain Analysis in Myocarditis—Can We Be Any Closer to Diagnose the Acute Phase of the Disease? J Clin Med 12:. [CrossRef]
- Rroku A, Kottwitz J, Heidecker B (2021) Update on myocarditis-what we know so far and where we may be heading. Eur Hear J Acute Cardiovasc Care 10:455–467. [CrossRef]
- Karev V, Starshinova AY, Glushkova A, Kudlay D, Starshinova A (2023) Features of Myocarditis: Morphological Differential Diagnosis in Post-COVID-19 Children. Diagnostics (Basel, Switzerland) 13:. [CrossRef]
Figure 1.
B: Troponin T levels (ng/L) in Case 1.
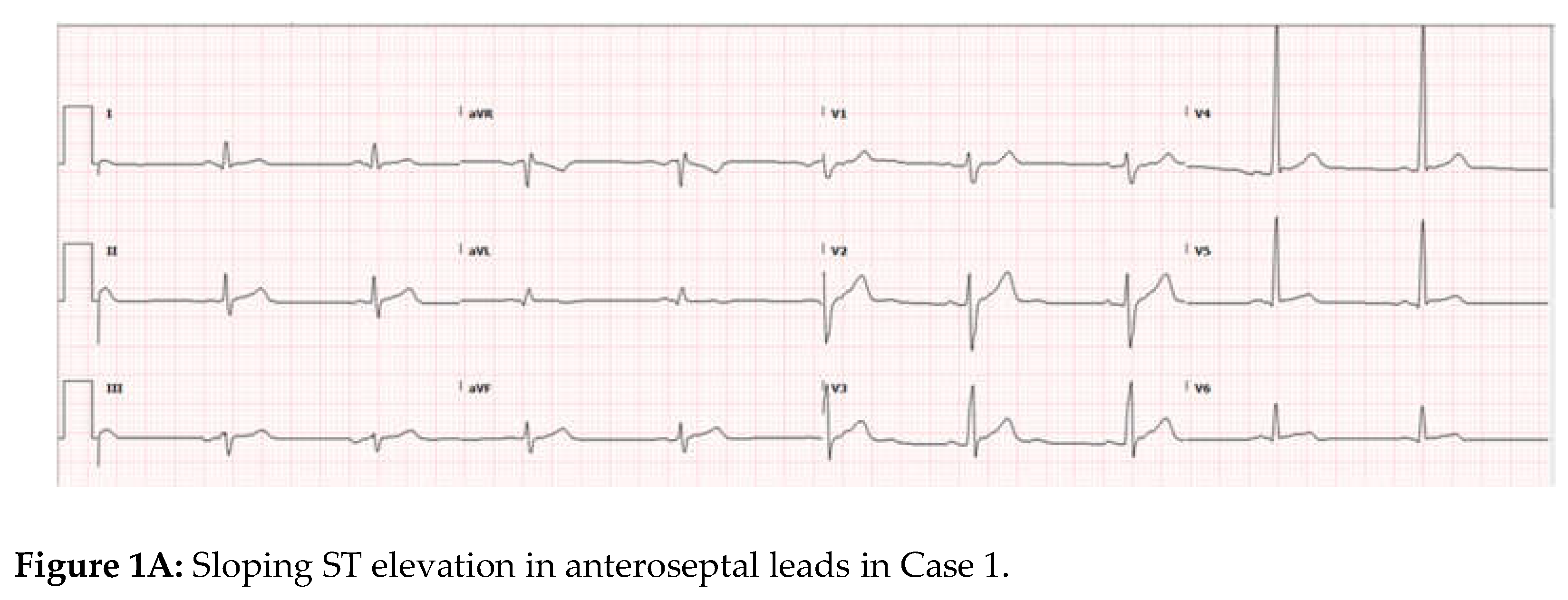
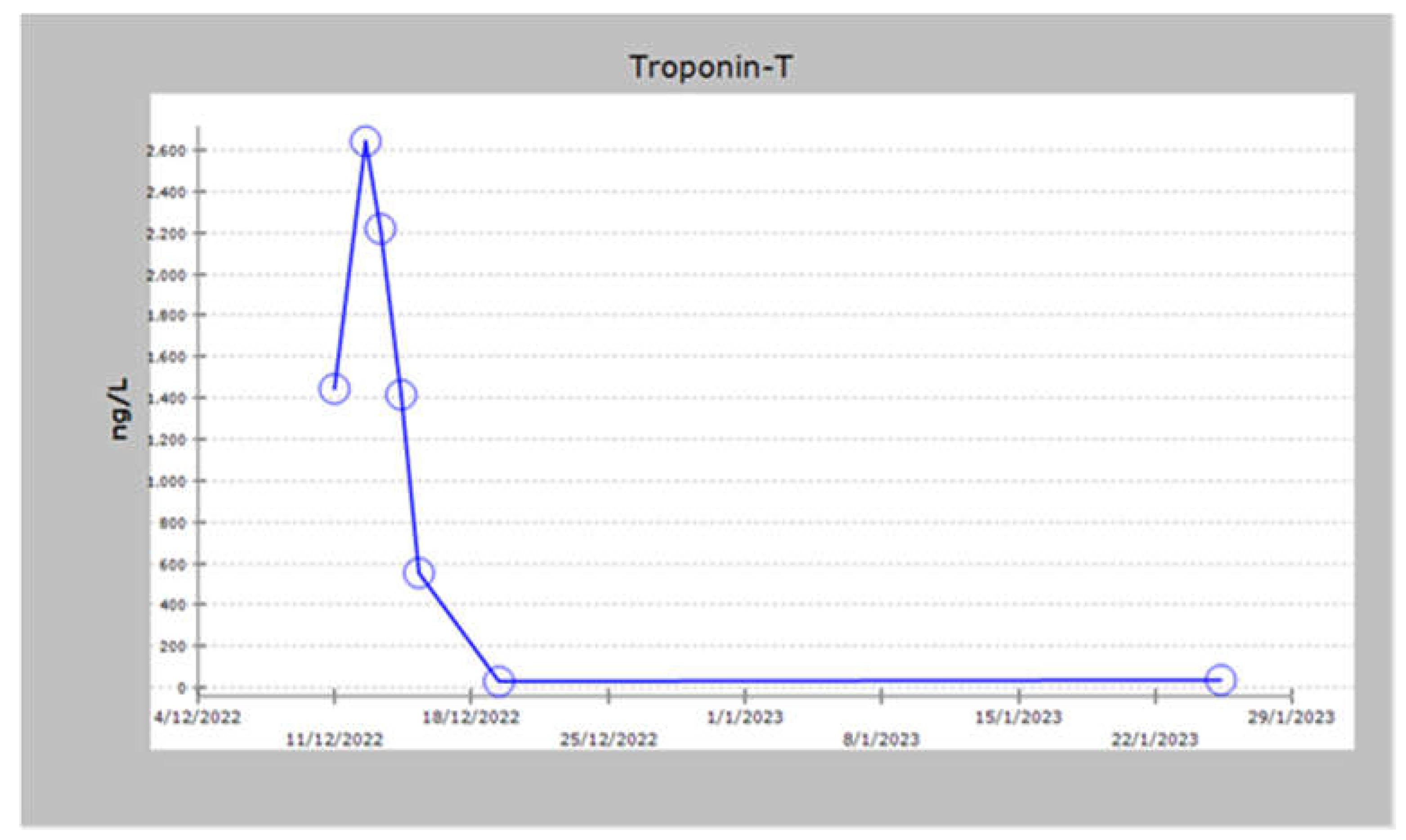
Figure 2.
Bull’s eye showing segmental basal lateral affection of the left ventricle in Case 1.
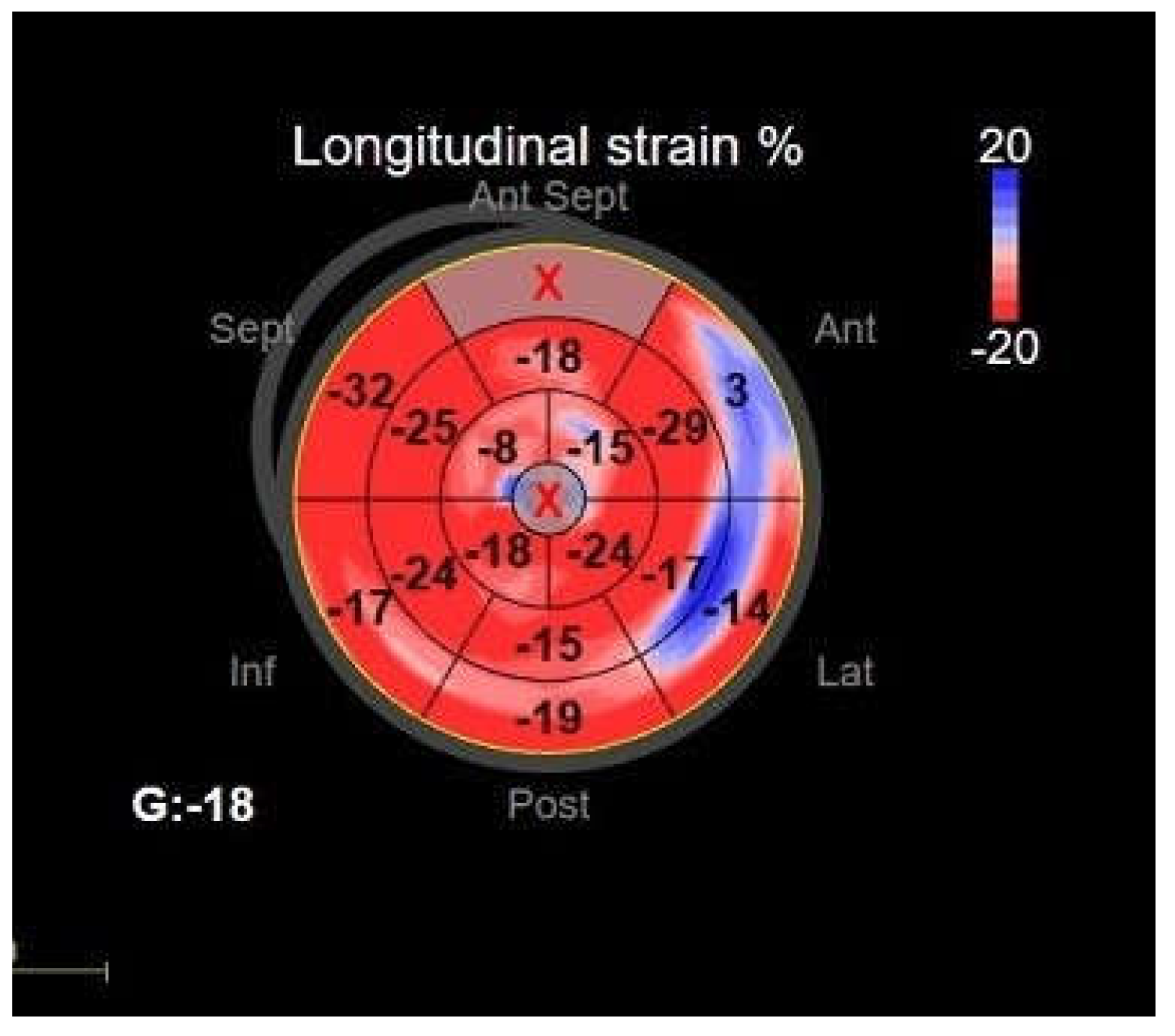
Figure 3.
B: Troponin T levels in Case 2.
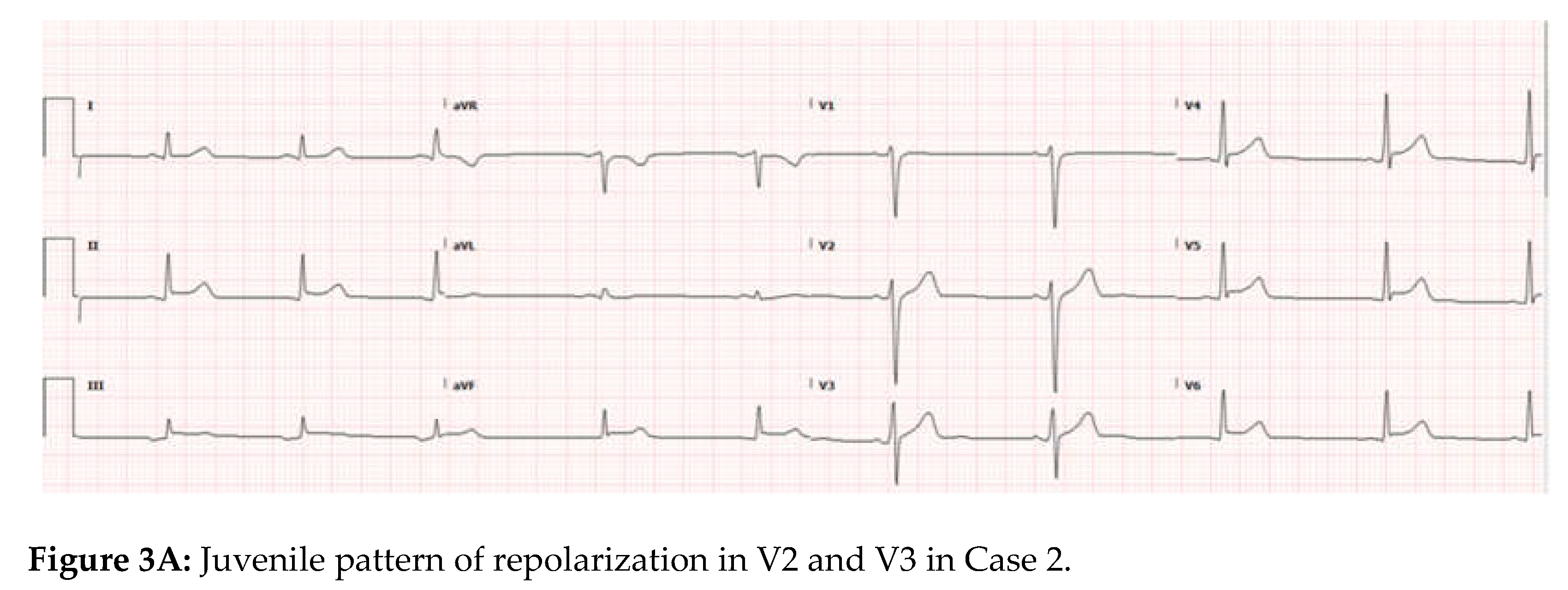
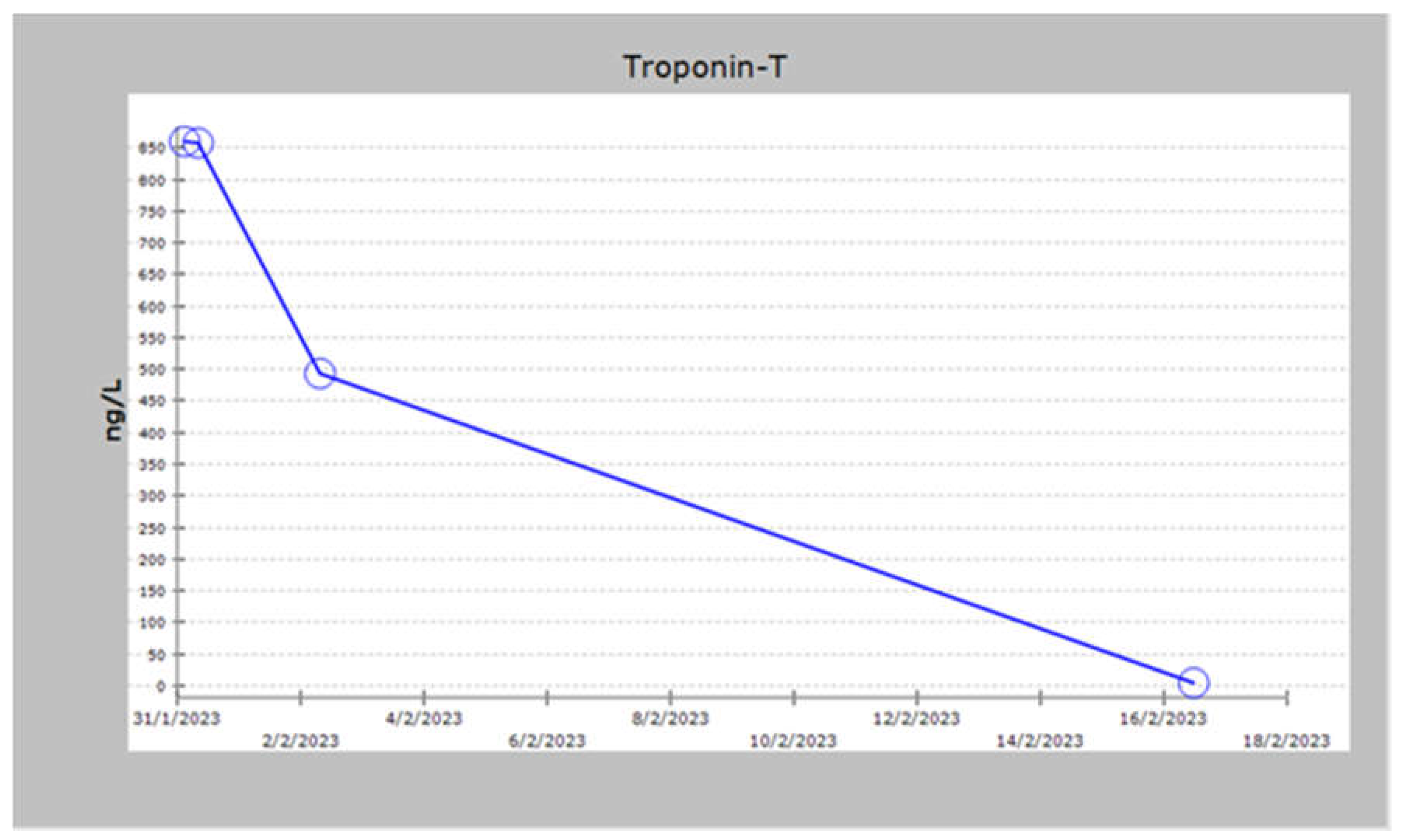
Figure 4.
Basal Septal affection by 2 D speckle tracking in Case 2 .
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



