
Submitted:
02 April 2024
Posted:
02 April 2024
You are already at the latest version
Abstract
Objectives: To assess the short-term impact of a single global stretching session on plantar pressures and lumbar range of motion (RoM) over one week in sedentary university students. Design: A randomised controlled trial with two parallel groups. Participants: Sixty-four university students were randomly assigned to a stretching group or control group. The stretching group received a single session of global stretching and the control group remained seated for the same length of time as the stretching session. Main outcome measures: Lumbar RoM and plantar pressures were assessed before, immediately after, 48 hours after, and 7 days after intervention. Results: Group-by-time interaction was significant for lumbar lateral flexion (p = 0.044), right maximal pressure (p = 0.003), left maximal pressure (p = 0.008), right mean pressure (p = 0.025), left mean pressure (p = 0.002), and maximal pressure minus mean pressure in right foot (p = 0.007). The model with plantar pressures showed a significant difference for group-by-time interaction (p = 0.010).Conclusion: Global stretching seems to counteract the ill-effects of prolonged sitting up to seven days with respect to plantar pressure in standing without improving lumbar ROM
Keywords:
stretching
; manual therapy
; posture
; range of motion
; plantar pressures
1. Introduction
University students remain seated for many hours in class and currently also spend many hours in front of the computer. Trunk muscles are adversely affected by maintaining a sitting posture for long periods of time [1], and after only one hour of sitting, the onset of the flexion relaxation phenomenon in the lumbar paraspinal muscles occurs at a larger angle of flexion. The flexed posture of the lumbar spine adopted during seated deskwork may induce a residual deformation in the spine’s viscoelastic passive tissues [2] and reduce spinal height and lumbar range of motion (RoM) [3]. Also, prolonged lumbar flexion could be a risk factor for low back disorders [4] and a significant proportion of university students report experiencing musculoskeletal discomfort associated with laptop computer use [5]. Postural performance in standing task is worse than sitting, and more neuromuscular activity would be required to maintain balance compared to sitting position. In the standing position, the time for which balance can be maintained using passive joint stiffness and reflex modulation is briefer than sitting [6]. Likewise, non-specific low back pain is closely related to changes in postural stability [7].
In addition, the spinal musculature and the plantar musculature appear to act synergistically while standing [8]. To maintain the upright position, the destabilising force of gravity must be corrected by the forces of the feet on the supporting surface [9]. The foot can be considered as a postural proprioceptive system because it allows segmental adjustment of the leg with respect to itself. Considering the feet as fixed points while standing, it is possible to reduce postural disorders caused by prolonged sitting by manipulating the neuromuscular state of the feet [10]. Also, when vertical and torsional muscular effects are present, the feet alterations are more significant in standing [11] and the measurement of plantar pressures can be used to quantify possible changes of the musculoskeletal activity after a manual therapy treatment [10,12,13].
Likewise, anatomical muscle continuity has been observed between the plantar muscles and the muscles of the lower limbs and trunk in the so-called myofascial chains [14]. Krause et al. [15] proposed to investigate the practical relevance of these intermuscular myofascial connections for exercise, prevention, and rehabilitation. In contrast to segmental stretching [16,17,18], global postural re-education (GPR) is a global stretching technique that suggests slower and longer stretching of every tonic myofascial chain with a specific manual therapy to correct postural compensations or musculoskeletal disorders [16,19]. This technique is achieved by holding different postural positions during a physiotherapy session under the guidance of a therapist. The postures must also be actively maintained by the patient in order to better integrate the stretching [20,21]. Because prolonged sitting positions in university students can cause lumbar disorders and changes on standing postural control, we hypothesise that performing a global stretching single session can produce changes in lumbar active RoM and plantar pressures in a week [2,3,4,5].
Therefore, the aim of this study was to assess the short-term impact of a single global stretching session on plantar pressures and lumbar range of motion (RoM) over one week in sedentary university students.
2. Methods
2.1. Study Design and Sample
A randomised controlled trial with two parallel groups (experimental and control) was designed. Written informed consent was obtained from the subjects before data collection. The study was approved by the Ethical Committee in Clinical Research of the Miguel Hernández University (UMH), and the protocol was performed following the Ethical Principles for Medical Research in Humans of the Declaration of Helsinki. The study was registered in clinicaltrials.gov (NCT02175667).
The study compromised university students from UMH and the study was conducted in a physiotherapy research centre. The inclusion criteria to participate was to remain seated or in front of data visualisation screens (tablets, computers, smartphones) for at least 4 hours a day, a moderate physical activity level (no more than 3 days/week), and between 18 to 35 years old. Exclusion criteria were subjects who had been diagnosed with a severe comorbid disorder or who had undergone surgery in the 6 months prior to recruitment. Subjects with some type of musculoskeletal injury or disability or those who were scheduled for physiotherapy treatment or training during the study period were also excluded.
2.2. Group Allocation and Procedures
Using a uniform distribution (0, 1) with the Microsoft Excel 2013 program, the random allocation sequence and the enrolment of the participants were generated by a different researcher who did not participate in interventions. All subjects underwent baseline baropodometric and lumbar RoM measurements. Once these had been taken, the subjects of the experimental group were treated with GPR by an experienced therapist to correct compensations in muscles chains. The control group remained seated for the same length of time as the stretching session and the participants only completed questionnaires for this time.
2.3. Blinding
The participants and therapist could not be blinded for the allocated group after randomisation. However, to avoid any influence in the results, no participants knew any results of the different measurements during the study.
2.4. Intervention and Follow-Up
For the subjects allocated to the stretching group, global stretching was based on the GPR technique. The procedure (45 minutes) consisted of four treatment phases and three stretching postures (Figure 1; supplemental video). In the first phase (5–6 min), the therapist started with specific work of muscles involved in breathing. In the second phase (25 min), in order to stretch the anterior muscle master chain, the subjects were positioned by the therapist in an “open hip angle with upper limbs in adduction” posture. With an initial traction of the sacrum performed by the therapist, the pelvis of the subjects is kept in retroversion, while the lumbar spine remains stabilised. In the third phase (10–15 min), the therapist stretched the posterior muscle master chain in the posture “closed hip angle with upper limbs in abduction”. In the final phase (3–5 min), the therapist worked postural integration with the subjects in the posture “standing in the centre”. The complete description of the global stretching session was described in a previous study [22].
After the stretching session, subjects had 5 min rest in a sitting position and the measurements were repeated. The subjects from the control group underwent the exact same measures, but instead of receiving the stretching session, they remained seated for the same length of time while they completed questionnaires as a task similar to studying.
Baseline measurements of plantar pressures and lumbar RoM were taken for both groups before intervention and were repeated immediately after, 2 days later, and 7 days later.
2.5. Outcomes Measures
All measurements (plantar pressures and lumbar RoM and) were performed by a single examiner and the measurement conditions were exactly reproduced for each trial and each group.
2.5.1. Plantar Pressures
The following data were collected from each subject and foot in static and standing position: maximum pressure (Pmax) and mean pressure (Pmean). The values were collected on the entire sole of each foot, without distinction of zones. To show the behaviour differences between Pmax and Pmean, a variable with pressure differences for each foot (right and left Pmax-Pmean) was calculated. To demonstrate if load percentage asymmetry between feet increase or decrease, a variable with these differences of load percentage (Dif.%Load) was calculated. For these measurements the Freemed™ (Roma, Italia) pressure platform with the FreeStep® software v.1.0.3 (Roma, Italia) were used. All measurements were conducted over 90 s and the procedure of the subjects on the platform was described in a previous study [22].
2.5.2. Lumbar RoM
The following data of lumbar RoM was collected from each subject: flexion, extension, right and left rotation, and right and left lateral flexion. The lumbar RoM measurements were taken with a Back Range of Motion instrument (BRoM). The BRoM contains two separate gravity goniometers for flexion and extension movements, another instrument with one gravity goniometer for lateral flexions, and with one compass goniometer for rotations (included a magnetic yoke for iliac control).
For lumbar RoM measurements, S1 was located by palpation following the iliac crest medially, and two levels inferiorly. T12 vertebra was also located by palpation, following the twelfth rib medially and superiorly. The examiner marked the anatomical references related to the instrument with a marker pen on the subjects. Lumbar RoM was assessed with the subjects in erect standing position for flexion, extension, and lateral flexion [23]. For flexion and extension, two measurements were registered for each movement: with the inclinometer on T12 and with the inclinometer on S1. The difference of these two measurements was the result for each movement. During lateral flexion measurements, the instrument was on T12, and the subjects were instructed to slide their hand down the side of their thigh while maintaining their weight over the other leg. For rotations, the subjects were in a sitting position to block pelvic movements (completely seated and erected) and always with the same leg position and arms crossed over the chest. The magnetic booster was placed around the subjects’ pelvis at the level of the iliac crest and the compass goniometer on T12. Then, the subjects were instructed to twist their trunk to one side and repeat to the other.
The reliability of the measurements of lumbar RoM and plantar pressures was calculated using the results at baseline and one hour later from the control group only (32 subjects). (Supplemental Table 1).
2.6. Statistical Analyses
2.6.1. Sample Size Calculation
To compare the results between the experimental group and control group at a period (three time points), repeated measures analysis of variance (ANOVA) with between–within interactions was used. For the sample size, we considered a medium effect size (f = 0.25), a type I error of 5% and 90% power, as well as minimum correlation of 0.5 between measures. The levels of between factors are 2, the levels of repeated measures factors are 3, and the nonsphericity correction considered is 0.5. At least a total sample size of 60 individuals would be necessary (30 per group). The GPower 3.1 statistical package was used for this calculation. We estimated possible losses of subjects of 25% (inclusion criteria, follow up losses) [24] and, therefore, finally selected 82 individuals.
2.6.2. Data Analysis
Intraclass correlation coefficients obtained by ANOVA were calculated to evaluate the reliability of plantar pressures and lumbar RoM measurements. Descriptive statistics are presented using mean and standard deviation (SD) for continuous variables (counts and percentages for qualitative variables). A Kolmogorov-Smirnov test was used to adjust the normal distribution of quantitative variables. Differences between groups are expressed as mean differences with 95% confidence intervals (95% CI). For measured differences in baseline, a Student’s t-test for independent samples was used in continuous variables. Chi squared test was used for gender. In each group separately (control and intervention), we used paired t-test for compared pre-treatment values and values immediately after, 2 days after, and 7 days after.
A general linear model for repeated measures was used to assess the effect of experimental group as inter-subject factor, and time as intra-subject factor (ANOVA). We performed a MANOVA of repeated measures with the variables that presented ANOVA significant differences and a significant association between all the variables (Pearson correlation coefficient).
Data was analysed using the Statistical Package for Social Sciences for Windows (version 24; SPSS, Inc., Chicago, IL).
3. Results
3.1. Flow of Subjects
A total of 82 subjects were recruited at the university campus (Figure 2), of which 67 were randomised and 64 completed the final analysis process: 39 women and 25 men; mean age 22.0 years (SD 3.7, range 19 to 35 years); mean height 169.2 cm (SD 10.0, range 151 to 193 cm); mean weight 66.0 kg (SD 14.1, range 42 to 111 kg); body mass index (BMI) mean 22.9 (SD 3.2, range 17 to 32.8). Baseline characteristics of participants are shown in Table 1.
3.2. Effect of the Intervention
Within-group comparison of pre-treatment values and values immediately after, 2 days after, and 7 days after are shown in Table 2. Statistical significance (p < 0.05) in different variables are observed in the stretching group in the three moments after intervention. Changes in both right lateral flexion and right rotation are observed after one week.
The results of the model for repeated measurements for plantar pressures and lumbar RoM are shown in Table 3, considering the interaction of time-by-group. Statistically significant differences were found for variables lumbar left lateral flexion (p = 0.044), right Pmax (p = 0.003), left Pmax (p = 0.008), right Pmean (p = 0.025), left Pmean (p = 0.002), and right Pmax-Pmean (p = 0.007).
The Pearson correlation coefficient between all the variables did not show a correlation between any variable of plantar pressures and any variable of lumbar RoM (Supplemental Table 2). All the variables of plantar pressures were significantly correlated and only Dif.%Load did not have any significant correlation. On lumbar RoM variables, lumbar flexion was correlated with the rotation movements, and lumbar extension was correlated only with right rotation. Both rotations were correlated between them and both lateral flexions were correlated.
The MANOVA with significant plantar pressures variables (right and left Pmax, right and left Pmean, and right Pmax-mean) showed a significant difference for the interaction time-by-group (p = 0.010).
4. Discussion and Conclusions
In our study, after a single global stretching session in university students who spent a long time sitting, we can observe different musculoskeletal effects over one week. These results could give us an idea of how to plan session intervals to include scheduled stretching and prevent musculoskeletal disorders.
About the effects of GPR technique, our previous study showed changes on postural sway after a global stretching session [22]. Estepa-Gallego et al. [25] also found changes in postural sway and dynamic balance after 8 weeks with weekly sessions of GPR. With the same follow up, GPR sessions show better results in flexibility than an analytic stretching program [26] and an important reduction of pain. Several other clinical trials have evaluated the effects of GPR treatments measuring low back pain, neck pain, quality of life, or evaluating disability questionnaires, with strong evidence of GPR as an effective method for treating spinal disorders [27,28].
We have not found any other clinical trials that assess global stretching techniques effect for postural correction using specific lumbar RoM instruments. In the present study, although the single session of global stretching was conducted in neutral lumbar positions, the findings on lumbar RoM movements appeared mainly in lumbar lateral flexions, as well as in right rotation, but the increment in Lumbar RoM appeared not only in the intervention group. A slight increase was observed in the control group that could be explained by a learning effect acquired throughout the measurements or due to the repeated movements of the measurements (three times each movement evaluated) that could have an elasticity effect on the tissues.
Hamstring stretching is a common practice in physical therapy to change lumbar motion. Static stretching of the hamstring muscles performed over 20 s for three times demonstrated an association with immediate changes in the sagittal spinal curvatures allowing greater lumbar flexion [18], but the authors did not assess rotation measures and these changes were not followed for more days in comparison with our study. Li et al. [17] observed an increase on motion during forward bending after a program of stretching, but they did not observe a relationship between hamstrings muscle length and lumbopelvic posture. Borman et al. [16] observed an effect on hamstring muscle length after a 4-week stretching program (static stretches for 30 s with two repetitions and 4 days per week), but they found no changes in lumbar flexion RoM.
In comparison with different techniques of lumbar ROM measurements, an analytic manual therapy, such as Mulligan’s mobilisation, did not demonstrate significant differences in flexion lumbar RoM compared with a placebo group [29]. Stamos-Papastamos et al. [30] also found no significant effect on flexion or extension lumbar RoM. Both studies measured RoM with different instruments, but they did not measure rotation movements nor did a follow-up of the subjects. In Shankar Ganesh et al., an ipsilateral lumbar spine zygopophyseal joint mobilisation showed an improvement in passive straight leg raise and the results were consistent after 24 hours but no more follow-ups were conducted.
Regarding plantar pressures in the standing position, we wanted to see the global changes in pressures without analysing whether the weight is better or worse in one zone or another, only if there were general changes in the distribution between both feet and changes in the maximum pressure peaks. In this sense, we observe a significantly different behaviour in the variables right and left Pmax and Pmean between the experimental group and the control group. In the experimental group, the Pmax of both feet increases immediately after the intervention, decreases significantly at 48 hours (under baseline measurement), and tend to return at 7 days. In contrast, in the control group there appears a small decrease initially and then (2 days and 7 days follow-up) returns close to baseline. On the other hand, in the experimental group, the variable Pmean in both feet shows an increase immediately after and returns to baseline at 48 h. In the control group, the variables of both feet show values near baseline at immediately after, 2 days after, and 7 days after measurements. We hypothesise the cause of Pmax and Pmean initial increase in subjects treated with GPR could be the possible instability immediately after a stretching exercise. Lima et al. [32] found an increased postural sway and activity of lower limb muscles after a static stretching of the plantar muscles in healthy subjects. Moreover, Romero-Franco et al. [33] showed induced short-term negative effects on the stabilometry with a proprioceptive exercise session using unstable platforms, and these results could support our findings. Despite a high degree of linear dependence among the Pmax and Pmean [34], the difference of these variables in both feet (Pmax-Pmean) produced a decrease clinically interesting in our study: the subjects treated with GPR had more homogeneous distribution of plantar pressures in comparison with controls, especially after 2 days. Furthermore, the global differences between the stretching group and control group over one week were also observed in the complete analysis model of plantar pressures. Regarding load distribution, the results found in the experimental group show that the differences of load percentage between feet decreased close to 0% after a single session of global stretching. After intervention, the treated subjects showed a better (more equal) load distribution between feet than before the stretching session and better than the control subjects. In reference to the use of pressure platforms to control postural changes after a global stretching session, the previous study showed changes on postural sway mainly at 48 hours and the values then tended to return to baseline after one week [22]. Takahashi et al. [35] found that GPR technique is effective for improving symmetry in body weight load between feet and plantar surface in patients with unilateral hindfoot valgus. Teodori et al. [36] evaluated the modifications in plantar pressures distribution and centre of pressure location in a subject with an ankle sprain history. The results of this case report showed evident symmetry recovery maintained for 7 days and authors concluded that a single session of GPR was enough to balance contact pressure distribution and that positively interfered in the centre of pressure. Other studies have examined the effects of other manual therapy techniques on baropodometry. Grassi et al. [37] analysed the effects of a sacroiliac joint manipulation because they believed that this manipulation could influence asymmetric tension throughout the pelvic complex and result in a more equal force distribution to the lower extremities. They obtained a positive influence on weight distribution among the feet of an asymptomatic population immediately and one week after a high-velocity, low-amplitude sacroiliac joint thrust. They did not study the changes in maximum and mean plantar pressures, but their findings in load redistribution after one week reinforce our results. In another study, Mendez-Sanchez et al. [13] found some immediate changes in load distribution on plantar support in the standing position after a bilateral manipulation of sacroiliac join applied in asymptomatic subjects, but they did not follow-up on these effects and they did not observe Pmax and Pmean. Lopez-Rodriguez et al. [10], in another controlled trial with placebo group, in athletic patients with grade II ankle sprain, observed the load supports at foot level and maximum and mean plantar pressures. They did not follow-up on subjects in the successive days but they found that the application of a caudal talocrural joint manipulation redistributed the load immediately after. Therefore, the authors considered that the baropodometric recordings could be used as a suitable method to evaluate the changes after peripheral or spinal manipulative procedures. A more recent study [38] has found changes in myofascial induction in plantar fascia increase surface in the fore foot and increase maximum pressure in the fore foot, but no changes were found in postural sway and there was no follow-up for a few days. Despite that, we did not find any correlation between Lumbar RoM and plantar pressures. Hawrylak et al. [39] studied spinal RoM and plantar pressures in sport climbers with similar measurements to our study. They found an increase of spinal RoM and differences in plantar pressure distribution versus the control group, but no intervention was performed.
Although our study analyses the short-term effect of a global stretching session over one-week, future studies should evaluate the effects on lumbar RoM and/or plantar pressures after more sessions of GPR with a medium- and long-term follow-up. Also, our study was not blinded, and the intervention group was not compared with other techniques or a placebo group.
Finally, the aim of this study was to investigate in university sedentary students the short-term effect of a single session of global stretching on plantar pressures in standing position and lumbar ROM. Our findings suggest that although a single session of global stretching produced a general increase of lumbar RoM in university students who spent a long time sitting, mainly in lateral flexions and right rotation, and mainly after one week, the differences with the control group were not significant except on right lateral flexion.
In plantar pressure measurements and compared with the control group, after a single session of global stretching the results showed an initial increase (worsening) of maximal and mean plantar pressures but then, after two days and seven days, they tended to decrease under baseline (improvement).
Despite limitations of the results, global stretching sessions might be considered in clinical practise to prevent musculoskeletal imbalances related with postural habits and the one-week interval could be considered to plan clinical sessions.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
References
- Watanabe, M., Kaneoka, K., Wada, Y., Matsui, Y., & Miyakawa, S. (2014). Trunk muscle activity with different sitting postures and pelvic inclination. Journal of Back and Musculoskeletal Rehabilitation, 27(4), 531-536. [CrossRef]
- Howarth, S.J., Glisic, D., Lee, J.G., & Beach, T.A. (2013). Does prolonged seated deskwork alter the lumbar flexion relaxation phenomenon? Journal of Electromyography and Kinesiology : Official Journal of the International Society of Electrophysiological Kinesiology, 23, 587–593. [CrossRef]
- Phimphasak, C., Swangnetr, M., Puntumetakul, R., Chatchawan, U., & Boucaut, R. (2016). Effects of seated lumbar extension postures on spinal height and lumbar range of motion during prolonged sitting. Ergonomics, 59(1), 112-120. [CrossRef]
- Shin, G., & Mirka, G.A. (2007). An in vivo assessment of the low back response to prolonged flexion: Interplay between active and passive tissues. Clinical Biomechanics (Bristol, Avon), 22(9), 965-971. [CrossRef]
- Bubric, K., & Hedge, A. (2016). Differential patterns of laptop use and associated musculoskeletal discomfort in male and female college students. Work (Reading, Mass.), 55(3), 663–671. [CrossRef]
- Serra-Ano, P., Lopez-Bueno, L., Garcia-Masso, X., Pellicer-Chenoll, M.T., & Gonzalez, L. M. (2015). Postural control mechanisms in healthy adults in sitting and standing positions. Perceptual and Motor Skills, 121(1), 119-134. [CrossRef]
- Ruhe, A., Fejer, R., & Walker, B. (2012). Pain relief is associated with decreasing postural sway in patients with non-specific low back pain. BMC Musculoskeletal Disorders, 13, 39-2474-13-39. [CrossRef]
- Gerasimenko, Y., Gad, P., Sayenko, D., McKinney, Z., Gorodnichev, R., Puhov, A., …, & Edgerton, V.R. (2016). Integration of sensory, spinal, and volitional descending inputs in regulation of human locomotion. J Neurophysiol, 116(1), 98-105. [CrossRef]
- Peterka, R.J. (2002). Sensorimotor integration in human postural control. Journal of Neurophysiology, 88(3), 1097-1118.
- Lopez-Rodriguez, S., Fernandez de-Las-Penas, C., Alburquerque-Sendin, F., Rodriguez-Blanco, C., & Palomeque-del-Cerro, L. (2007). Immediate effects of manipulation of the talocrural joint on stabilometry and baropodometry in patients with ankle sprain. Journal of Manipulative and Physiological Therapeutics, 30(3), 186-192. [CrossRef]
- Rosario, J.L. (2014). A review of the utilization of baropodometry in postural assessment. Journal of Bodywork and Movement Therapies, 18(2), 215-219. [CrossRef]
- Ferreira, G.E., Viero, C.C., Silveira, M.N., Robinson, C.C., & Silva, M.F. (2013). Immediate effects of hip mobilization on pain and baropodometric variables--a case report. Manual Therapy, 18(6), 628-631. [CrossRef]
- Mendez-Sanchez, R., Gonzalez-Iglesias, J., Sanchez-Sanchez, J.L., & Puente-Gonzalez, A.S. (2014). Immediate effects of bilateral sacroiliac joint manipulation on plantar pressure distribution in asymptomatic participants. Journal of Alternative and Complementary Medicine (New York, N.Y.), 20(4), 251-257. [CrossRef]
- Bordoni, B., & Myers, T. (2020). A Review of the Theoretical Fascial Models: Biotensegrity, Fascintegrity, and Myofascial Chains. Cureus, 12(2):e7092. [CrossRef]
- Krause, F., Wilke, J., Vogt, L., & Banzer, W. (2016). Intermuscular force transmission along myofascial chains: a systematic review. J Anat, 228(6):910-8. [CrossRef]
- Borman, N.P., Trudelle-Jackson, E., & Smith, S.S. (2011). Effect of stretch positions on hamstring muscle length, lumbar flexion range of motion, and lumbar curvature in healthy adults. Physiotherapy Theory and Practice, 27(2), 146-154. [CrossRef]
- Li, Y., McClure, P.W., & Pratt, N. (1996). The effect of hamstring muscle stretching on standing posture and on lumbar and hip motions during forward bending. Physical Therapy, 76(8), 836-45; discussion 845-9.
- Lopez-Minarro, P.A., Muyor, J.M., Belmonte, F., & Alacid, F. (2012). Acute effects of hamstring stretching on sagittal spinal curvatures and pelvic tilt. Journal of Human Kinetics, 31, 69-78. [CrossRef]
- Ferreira, G.E., Barreto, R.G., Robinson, C.C., Plentz, R.D., & Silva, M.F. (2016). Global postural reeducation for patients with musculoskeletal conditions: A systematic review of randomized controlled trials. Brazilian Journal of Physical Therapy, 20(3), 194-205. [CrossRef]
- Castagnoli, C., Cecchi, F., Del Canto, A., Paperini, A., Boni, R., Pasquini, G., Vannetti, F., & Macchi, C. (2015). Effects in Short and Long Term of Global Postural Reeducation (GPR) on Chronic Low Back Pain: A Controlled Study with One-Year Follow-Up. TheScientificWorldJournal, 2015, 271436. [CrossRef]
- Lawand, P., Lombardi Júnior, I., Jones, A., Sardim, C., Ribeiro, L. H., & Natour, J. (2015). Effect of a muscle stretching program using the global postural reeducation method for patients with chronic low back pain: A randomized controlled trial. Joint bone spine, 82(4), 272–277. [CrossRef]
- Lozano-Quijada, C., Poveda-Pagan, E.J., Segura-Heras, J.V., Hernandez-Sanchez, S., & Prieto-Castello, M.J. (2017). Changes in postural sway after a single global postural reeducation session in university students: A randomized controlled trial. Journal of Manipulative and Physiological Therapeutics, 40(7), 467-476. [CrossRef]
- Atya, A.M. (2013). The validity of spinal mobility for prediction of functional disability in male patients with low back pain. Journal of Advanced Research, 4(1), 43-49. [CrossRef]
- Cunha, A.C., Burke, T.N., Franca, F.J., & Marques, A.P. (2008). Effect of global posture reeducation and of static stretching on pain, range of motion, and quality of life in women with chronic neck pain: A randomized clinical trial. Clinics (Sao Paulo, Brazil), 63(6), 763-770. [CrossRef]
- Estepa-Gallego, A., Ibañez-Vera, A.J., Estudillo-Martínez, M.D., Castellote-Caballero, Y., Bergamin, M., Gobbo, S., …, & Cruz-Díaz, D. (2022). Effects of global postural reeducation on postural control, dynamic balance, and ankle range of motion in patients with hallux abducto valgus. A randomized controlled trial. J Orthop Res, 40(6):1436-1445. [CrossRef]
- Matos, F.P., Dantas, E.H.M., de Oliveira, F.B., de Castro, J.B.P., Conceição, M.C.S.C., Nunes, R.A.M, & Vale, R.G.S. (2020) Analysis of pain symptoms, flexibility and hydroxyproline concentration in individuals with low back pain submitted to Global Postural Re- education and stretching. Pain Manag, 10(3):167-177. [CrossRef]
- Gonzalez-Medina, G., Perez-Cabezas, V., Ruiz-Molinero, C., Chamorro-Moriana, G., Jimenez-Rejano, J.J., & Galán-Mercant, A. (2021). Effectiveness of Global Postural Re-Education in Chronic Non-Specific Low Back Pain: Systematic Review and Meta-Analysis. J Clin Med,10(22):5327. [CrossRef]
- Lomas-Vega, R., Garrido-Jaut, M.V., Rus, A., & Del-Pino-Casado, R. (2017). Effectiveness of Global Postural Re-education for Treatment of Spinal Disorders: A Meta-analysis. Am J Phys Med Rehabil, 96(2):124-130. [CrossRef]
- Moutzouri, M., Billis, E., Strimpakos, N., Kottika, P., & Oldham, J.A. (2008). The effects of the mulligan sustained natural apophyseal glide (SNAG) mobilisation in the lumbar flexion range of asymptomatic subjects as measured by the zebris CMS20 3-D motion analysis system. BMC Musculoskeletal Disorders, 9, 131-2474-9-131. [CrossRef]
- Stamos-Papastamos, N., Petty, N.J., & Williams, J.M. (2011). Changes in bending stiffness and lumbar spine range of movement following lumbar mobilization and manipulation. Journal of Manipulative and Physiological Therapeutics, 34(1), 46-53. [CrossRef]
- Shankar Ganesh, G., Mohanty, P., & Smita Pattnaik, S. (2015). The immediate and 24-hour follow-up effect of unilateral lumbar Z-joint mobilisation on posterior chain neurodynamics. Journal of Bodywork and Movement Therapies, 19(2), 226-231. [CrossRef]
- Lima, B.N., Lucareli, P.R., Gomes, W.A., Silva, J.J., Bley, A.S., Hartigan, E.H., & Marchetti, P.H. (2014). The acute effects of unilateral ankle plantar flexors static- stretching on postural sway and gastrocnemius muscle activity during single-leg balance tasks. Journal of Sports Science & Medicine, 13(3), 564-570.
- Romero-Franco, N., Martinez-Lopez, E.J., Lomas-Vega, R., Hita-Contreras, F., Osuna-Perez, M.C., & Martinez-Amat, A. (2013). Short-term effects of proprioceptive training with unstable platform on athletes' stabilometry. Journal of Strength and Conditioning Research / National Strength & Conditioning Association, 27(8), 2189-2197. [CrossRef]
- Keijsers, N.L., Stolwijk, N.M., & Pataky, T.C. (2010). Linear dependence of peak, mean, and pressure-time integral values in plantar pressure images. Gait & Posture, 31(1), 140-142. [CrossRef]
- Takahashi, H.A., & Quevedo, A.A.F. (2021). Quantitative study of PIMT technique aiming its validation as physical therapy procedure. Foot (Edinb), 47:101800. [CrossRef]
- Teodori, M.S., Guirro, E.C.O., & Santos, R.M. (2005). Plantar pressure distribution and center force location after postural global reeducation: A case relate. Physical Therapy in Movement, 18(1), 27-35.
- Grassi Dde, O., de Souza, M.Z., Ferrareto, S.B., Montebelo, M.I., & Guirro, E.C. (2011). Immediate and lasting improvements in weight distribution seen in baropodometry following a high-velocity, low-amplitude thrust manipulation of the sacroiliac joint. Manual Therapy, 16(5), 495-500. [CrossRef]
- Martínez-Jiménez, E.M., Becerro-de-Bengoa-Vallejo, R., Losa-Iglesias, M.E., Rodríguez-Sanz, D., Díaz-Velázquez, J. I., Casado-Hernández, I., …, & López-López, D. (2020). Acute effects of myofascial induction technique in plantar fascia complex in patients with myofascial pain syndrome on postural sway and plantar pressures: A quasi-experimental study. Physical Therapy in Sport: Official Journal of the Association of Chartered Physiotherapists in Sports Medicine, 43, 70-76. [CrossRef]
- Hawrylak, A., Chromik, K., Ratajczak, B., Barczyk-Pawelec, K., & Demczuk-Włodarczyk, E. (2017). Spinal range of motion and plantar pressure in sport climbers. Acta of Bioengineering and Biomechanics, 19(2), 169-173.
Figure 1.
Phases of the global stretching session. A: Soft cervical traction and work of anterior muscles involved in breathing. B: Traction of the sacrum in an “open hip angle with upper limbs in adduction” posture. C: Specific work of lower limbs with pelvic corrections: the therapist extended the lower limbs of the subject as much as possible while stretching iliopsoas, adductors of hip, and rectus femoris, tibialis anterior and dorsiflexors of the feet. D: “Closed hip angle with upper limbs in abduction” posture with cervical traction to stretch erector spinae, gluteus maximus, hamstrings, triceps surae, and foot intrinsic muscles. E: Specific stretching of plantar muscles. F: Corrections of the feet in the “standing in the centre” posture. G: Final lumbar corrections and integration of the whole stretching.
Figure 1.
Phases of the global stretching session. A: Soft cervical traction and work of anterior muscles involved in breathing. B: Traction of the sacrum in an “open hip angle with upper limbs in adduction” posture. C: Specific work of lower limbs with pelvic corrections: the therapist extended the lower limbs of the subject as much as possible while stretching iliopsoas, adductors of hip, and rectus femoris, tibialis anterior and dorsiflexors of the feet. D: “Closed hip angle with upper limbs in abduction” posture with cervical traction to stretch erector spinae, gluteus maximus, hamstrings, triceps surae, and foot intrinsic muscles. E: Specific stretching of plantar muscles. F: Corrections of the feet in the “standing in the centre” posture. G: Final lumbar corrections and integration of the whole stretching.
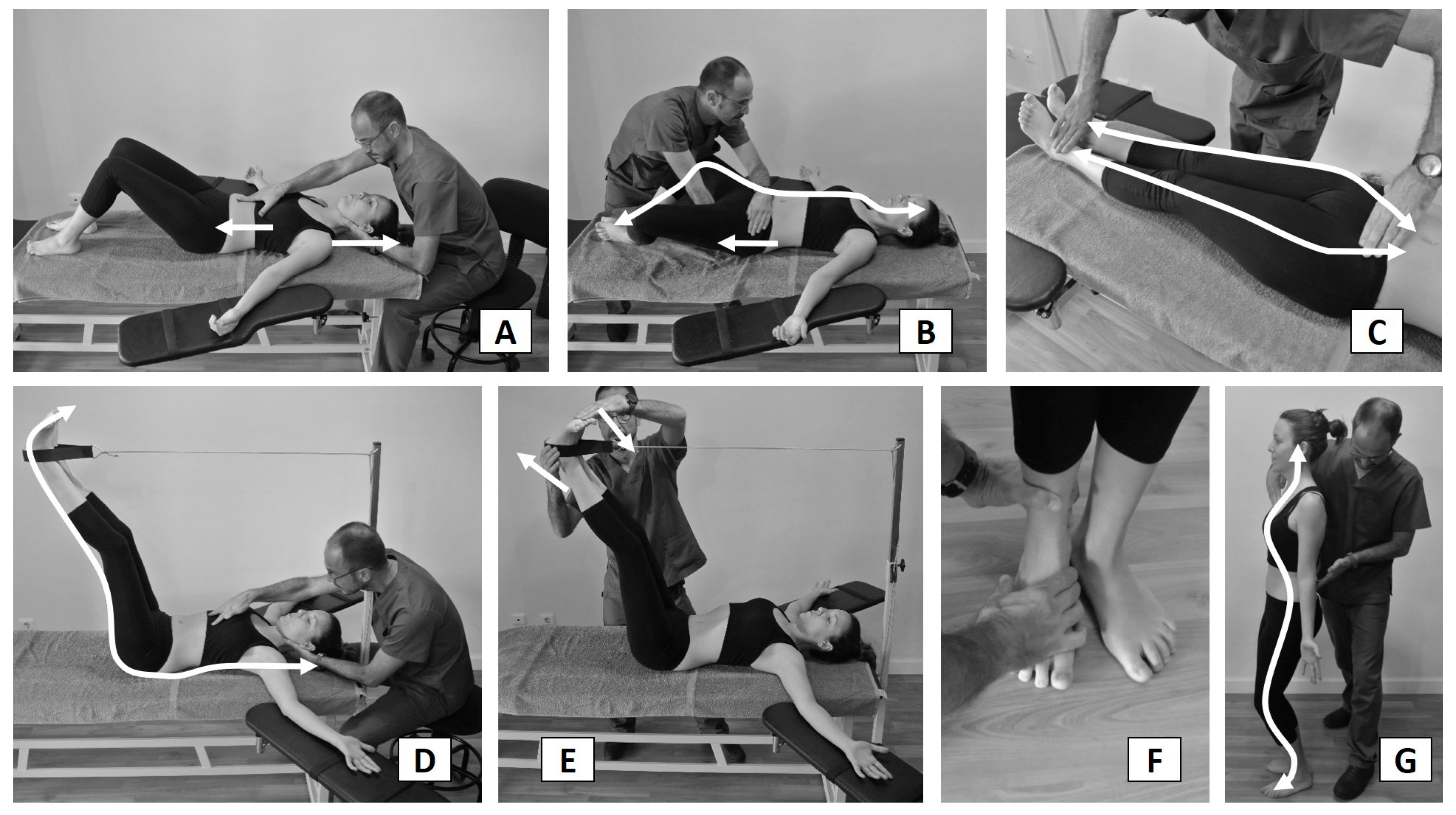
Figure 2.
CONSORT 2010 flow diagram.


Table 1.
Baseline characteristics of participants.
| Control (n=32) Mean (SD) |
Global Stretching (n=32) Mean (SD) |
p-value (Effect size) |
||||
| Age (year) | 22.66 (4.08) | 21.38 (3.10) | .162 (.083) | |||
| Weight (kg) | 70.14 (15.97) | 61.88 (10.89) | .019 (.183) | |||
| Height (m) | 170.81 (10.64) | 167.58 (9.32) | .201 (.027) | |||
| BMI (kg/m2) | 23.78 (3.24) | 21.94 (2.86) | .019 (.117) | |||
| Lumbar ROM | Flexion | 50.42 (7.12) | 48.34 (6.62) | .233 (.060) | ||
| Extension | 17.21 (8.16) | 19.83 (10.58) | .271 (.173) | |||
| Right Rotation | 10.81 (16.31) | 13.42 (14.11) | .497 (.175) | |||
| Left Rotation | 8.96 (13.41) | 12.42 (13.65) | .310 (.380) | |||
| Right Lateral Flexion | 27.65 (4.48) | 27.35 (5.02) | .807 (.015) | |||
| Left Lateral Flexion | 26.06 (5.01) | 25.54 (5.1) | .681 (.028) | |||
| Plantar Pressures | Right Pmax | 613.63 (114.21) | 654.72 (125.82) | .176 (.087) | ||
| Left Pmax | 607.31 (119.5) | 647.03 (126.71) | .202 (.085) | |||
| Right Pmean | 294.63 (58.36) | 308.09 (56.87) | .353 (.061) | |||
| Left Pmean | 291.09 (59.27) | 308.03 (60.56) | .263 (.076) | |||
| Right Pmax-mean | 319 (59.48) | 346.63 (76.02) | .111 (.109) | |||
| Left Pmax-mean | 316.22 (66.6) | 339 (72.21) | .194 (.093) | |||
| Dif.Load% | 0.5 (5.97) | -0.5 (7.22) | .548 (.236) | |||
| Gender | n (%) | n (%) | ||||
| Male | 13 (40.6) | 12 (37.5) | .798 | |||
| Female | 19 (59.4) | 20 (62.5) | ||||
Pmax=maximal pressure; Pmean= mean pressure; Pmax-mean= maximal pressure minus mean pressure; Dif.%Load= Difference of percentage of load left foot minus right foot.
Table 2.
Within-Group comparison of pretreatment values and values immediately after, 2 days after and 7 days after.
Table 2.
Within-Group comparison of pretreatment values and values immediately after, 2 days after and 7 days after.
| Within-Group change scores immediately after session |
Within-Group change scores 2 days after session |
Within-Group change scores 7 days after session |
|||||||||
| Mean diff. | CI 95% | p-value (Effect size) |
Mean diff. | CI 95% | p-value (Effect size) |
Mean diff. | CI 95% | p-value (Effect size) |
|||
| LUMBAR ROM | Flexion | ||||||||||
| Control | -1.46 | (-3.52,0.6) | .159 (.203) | 1,0 | (-0.97,2.97) | .309 (.138) | 6.19 | (-6.8,19.18) | .339 (.263) | ||
| Stretching | -0.53 | (-3.2,2.14) | .688 (.074) | 1.24 | (-0.69,3.17) | .199 (.180) | 0.64 | (-1.69,2.96) | .581 (.092) | ||
| Extension | |||||||||||
| Control | 1.31 | (-0.67,3.29) | .186 (.165) | -0.31 | (-2.38,1.76) | .760 (.037) | 0.13 | (-2.05,2.3) | .908 (.016) | ||
| Stretching | -1.54 | (-3.69,0.61) | .154 (.151) | -1.44 | (-3.83,0.96) | .230 (.138) | -1.15 | (-3.78,1.48) | .381 (.116) | ||
| Right Rotation | |||||||||||
| Control | -0.21 | (-1.41,1) | .727 (.013) | -1.38 | (-3.52,0.77) | .201 (.082) | -1.25 | (-3.59,1.09) | .284 (.078) | ||
| Stretching | 2.44 | (0.92,3.96) | .003 (.144) | 2.04 | (-0.17,4.26) | .070 (.137) | 2.56 | (0.17,4.96) | .037 (.172) | ||
| Left Rotation | |||||||||||
| Control | -0.42 | (-1.6,0.77) | .479 (.031) | -0.27 | (-1.25,0.71) | .578 (.020) | -0.67 | (-2.18,0.85) | .377 (.050) | ||
| Stretching | 0.5 | (-1.49,2.49) | .612 (.037) | 1.5 | (-0.55,3.55) | .145 (.107) | 1.08 | (-1,3.17) | .297 (.080) | ||
| Right Lateral | |||||||||||
| Control | -0.9 | (-1.93,0.14) | .087 (.186) | 0.65 | (-0.36,1.65) | .201 (.143) | -0.56 | (-1.69,0.57) | .318 (.124) | ||
| Stretching | 1.21 | (-0.14,2.55) | .077 (.253) | 1.46 | (0.01,2.91) | .049 (.317) | 1.58 | (0.14,3.03) | .033 (.323) | ||
| Left Lateral | |||||||||||
| Control | -1.04 | (-1.8,-0.29) | .008 (.208) | 0.63 | (-0.24,1.49) | .150 (.127) | -0.63 | (-1.73,0.48) | .256 (.132) | ||
| Stretching | 0.58 | (-0.56,1.73) | .308 (.111) | 0.63 | (-0.75,2) | .360 (.124) | 1.21 | (0.02,2.4) | .047 (.253) | ||
| PLANTAR PRESSURES | Right Pmax | ||||||||||
| Control | -2.53 | (-23.71,18.65) | .809 (.023) | 9,0 | (-7.08,25.08) | .262 (.080) | -0.13 | (-21.74,21.49) | .991 (.001) | ||
| Stretching | 14.84 | (-9.24,38.93) | .218 (.106) | -21.03 | (-49.25,7.19) | .139 (.161) | -15.44 | (-41.83,10.96) | .242 (.121) | ||
| Left Pmax | |||||||||||
| Control | -11.56 | (-34.39,11.27) | .310 (.101) | 3.09 | (-12.72,18.91) | .693 (.026) | -2.28 | (-24.86,20.29) | .838 (.019) | ||
| Stretching | 6.41 | (-15.15,27.97) | .549 (.046) | -28.09 | (-61.83,5.64) | .099 (.211) | -17.59 | (-43.33,8.14) | .173 (.139) | ||
| Right Pmean | |||||||||||
| Control | 1.72 | (-8.22,11.66) | .727 (.030) | 3.19 | (-5.5,11.88) | .460 (.056) | -0.06 | (-10.09,9.96) | .990 (.001) | ||
| Stretching | 15.22 | (5.54,24.9) | .003 (.231) | -2.16 | (-13.56,9.25) | .702 (.037) | 0.06 | (-11.62,11.74) | .991 (.001) | ||
| Left Pmean | |||||||||||
| Control | -5.81 | (-16.39,4.76) | .271 (.101) | -0.72 | (-9.66,8.22) | .871 (.012) | -0.75 | (-13.36,11.86) | .904 (.013) | ||
| Stretching | 14.69 | (4.64,24.73) | .006 (.207) | -2.03 | (-14.36,10.3) | .739 (.032) | -2.47 | (-14.36,9.42) | .675 (.041) | ||
| Right Pmax-mean | |||||||||||
| Control | -4.25 | (-18.39,9.89) | .544 (.720) | 5.81 | (-5.4,17.03) | .299 (.093) | -0.06 | (-14.07,13.94) | .993 (.001) | ||
| Stretching | -0.38 | (-17.49,16.74) | .965 (.005) | -18.88 | (-38.23,0.48) | .056 (.242) | -15.5 | (-32.58,1.58) | .074 (.209) | ||
| Left Pmax-mean | |||||||||||
| Control | -5.75 | (-19.93,8.43) | .415 (.091) | 3.81 | (-6.31,13.93) | .448 (.058) | -1.53 | (-14.8,11.74) | .815 (.024) | ||
| Stretching | -8.28 | (-23.33,6.76) | .270 (.111) | -26.06 | (-49.91,-2.22) | .033 (.334) | -15.13 | (-31.31,1.06) | .066 (.211) | ||
| Dif.Load% | |||||||||||
| Control | -3.31 | (-5.61,-1.01) | .006 (.536) | -2.13 | (-4.03,-0.22) | .030 (.364) | -1.31 | (-3.11,0.49) | .147 (.229) | ||
| Stretching | -0.13 | (-1.91,1.66) | .887 (.019) | 0.19 | (-1.45,1.83) | .817 (.027) | 0.25 | (-2.23,2.73) | .838 (.038) | ||
Pmax=maximal pressure; Pmean= mean pressure; Pmax-mean= maximal pressure minus mean pressure; Dif.%Load= Difference of percentage of load left foot minus right foot.
Table 3.
ANOVA for Lumbar ROM and Plantar Pressures.
| Preintervention | 0 h Postintervention |
2 days Postintervention |
7 days Postintervention |
Group x Time P-value |
Effect Size | |||
| Lumbar ROM | Flexion | .362 | .014 | |||||
| Control | 50.4 (7.1) | 49 (7.3) | 51.4 (7.3) | 56.6 (34.1) | ||||
| Stretching | 48.3 (6.6) | 47.8 (7.6) | 49.6 (7.1) | 49 (7.1) | ||||
| Extension | .380 | .015 | ||||||
| Control | 17.2 (8.2) | 18.5 (7.6) | 16.9 (8.7) | 17.3 (7.1) | ||||
| Stretching | 19.8 (10.6) | 18.3 (9.5) | 18.4 (10.2) | 18.7 (8.6) | ||||
| Right Rotation | .610 | .007 | ||||||
| Control | 10.8 (16.3) | 10.6 (15.6) | 9.4 (13.6) | 9.6 (14.2) | ||||
| Stretching | 13.4 (14.1) | 15.9 (16.1) | 15.5 (15.2) | 16 (15.3) | ||||
| Left Rotation | .569 | .009 | ||||||
| Control | 9 (13.4) | 8.5 (12.9) | 8.7 (12.9) | 8.3 (12.2) | ||||
| Stretching | 12.4 (13.6) | 12.9 (13.1) | 13.9 (14.2) | 13.5 (13.5) | ||||
| Right Lateral | .195 | .026 | ||||||
| Control | 27.6 (4.5) | 26.8 (5) | 28.3 (4.5) | 27.1 (4.6) | ||||
| Stretching | 27.4 (5) | 28.6 (4.4) | 28.8 (3.9) | 28.9 (4.8) | ||||
| Left Lateral | .044 | .051 | ||||||
| Control | 26.1 (5) | 25 (5) | 26.7 (4.8) | 25.4 (3.9) | ||||
| Stretching | 25.5 (5.1) | 26.1 (5.4) | 26.2 (5) | 26.8 (3.8) | ||||
| Plantar Pressures | Right Pmax | .003 | .088 | |||||
| Control | 613.6 (114.2) | 611.1 (103.5) | 622.6 (111.9) | 613.5 (117.3) | ||||
| Stretching | 654.7 (125.8) | 669.6 (143.9) | 633.7 (133.8) | 639.3 (128.8) | ||||
| Left Pmax | .008 | .074 | ||||||
| Control | 607.3 (119.5) | 595.8 (103.7) | 610.4 (113.4) | 605 (115.3) | ||||
| Stretching | 647 (126.7) | 653.4 (141.5) | 618.9 (137.6) | 629.4 (125.9) | ||||
| Right Pmean | .025 | .057 | ||||||
| Control | 294.6 (58.4) | 296.3 (53.1) | 297.8 (55) | 294.6 (60) | ||||
| Stretching | 308.1 (56.9) | 323.3 (66.6) | 305.9 (59.6) | 308.2 (60.2) | ||||
| Left Pmean | .002 | .097 | ||||||
| Control | 291.1 (59.3) | 285.3 (55.4) | 290.4 (62.1) | 290.3 (59.7) | ||||
| Stretching | 308 (60.6) | 322.7 (71.1) | 306 (66.1) | 305.6 (60.6) | ||||
| Right Pmax-Mean | .007 | .077 | ||||||
| Control | 319 (59.5) | 314.8 (58.6) | 324.8 (64) | 318.9 (63.3) | ||||
| Stretching | 346.6 (76) | 346.3 (82.4) | 327.8 (79.5) | 331.1 (71.7) | ||||
| Left Pmax-Mean | .065 | .045 | ||||||
| Control | 316.2 (66.6) | 310.5 (54.5) | 320 (57.6) | 314.7 (59.4) | ||||
| Stretching | 339 (72.2) | 330.7 (76) | 312.9 (82.3) | 323.9 (70.9) | ||||
| Dif.Load% | .463 | .012 | ||||||
| Control | 0.5 (6) | -2.8 (6.4) | -1.6 (5.7) | -0.8 (5.4) | ||||
| Stretching | -0.5 (7.2) | -0.6 (5.2) | -0.3 (6.1) | -0.3 (5.7) | ||||
Pmax=maximal pressure; Pmean= mean pressure; Pmax-mean= maximal pressure minus mean pressure; Dif.%Load= Difference of percentage of load left foot minus right foot.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



