
Submitted:
30 March 2024
Posted:
02 April 2024
You are already at the latest version
Abstract
The number of long-term cancer survivors increases continually. Understanding their needs is crucial to ensure an adequate follow-up. The aim of our study was to summarize the current literature concerning needs and what in-fluences these needs. A Scoping review of systematic reviews was conducted according to the recommendations of the Joanna Briggs Institute (JBI). Four electronic databases were searched. Of 414 retrieved papers, 11 met the eligi-bility criteria. Needs were aggregated into six domains (health-related information, health system, mental, practical, relationship and physical) and 15 categories. The lack of adequate information and the lack of access and/or conti-nuity of supportive care were the most prominent needs. Female gender, younger age, a low level of family and/or social support, and higher educational level were identified as risk factors. Employment and relationship status can affect the needs both in a positive or negative way. The weeks or months after the end of the treatments are partic-ularly critical and needs can be emphasized during this period. Cancer survivors could also leave positive changes. The variety of needs affects the quality of life of cancer survivors. The current Swiss healthcare system is not de-signed to support these people. Needs assessments should be systematically provided to ensure a better awareness on the part of health professionals and to allow an individual, holistic, and integrated follow-up.
Keywords:
cancer survivors
; needs
; follow-up
; supportive care
; information
; health system
; assessment
1. Introduction
1.1. Rationale
In 2022 about 20 million people worldwide received a new cancer diagnosis [1]. With the growth of the population, increased life expectancy and the persistence of risk factors (exposures), the trend is estimated to increase up to 32.6 million in 2045 [1]. Cancer is the second cause of death worldwide, just behind cardiovascular diseases [2]. However, thanks to the progress in cancer screening and medical treatments, the mortality rate regularly decreases, and more patients can benefit from a better long-term survival. As a result, an increasing number of people are living with or after cancer. By the end of 2022, approximately 53.5 million people worldwide were estimated to be cancer survivors [3]. In Switzerland, an estimated 450,000 people would be cancer survivors by the end of 2023 [4].
Mullan with his “Seasons of survival” [5] and Miller [6], with a subsequent adaptation, have played a major role defining the several phases of the cancer journey. Among them, the transition to survivorship is not trivial and particularly important. Effectively, end of acute care represents a “Turning point”, accompanied by some important changes and multidimensional distress, but could also lead to “a profound personal growth and transformation” [7]. For Derbez and Rollin, cancer survivors should manage the consequences of the illness in “all spheres of their existence” [8]. In the long term, the social and / or professional activities, as well as the quality of life could be affected. A meta-analysis [9] found a significant impact on quality of life up to 26 years after cancer diagnosis.
1.2. Objectives
The needs of cancer survivors can be diverse and vary in duration, therefore supportive care should be personal and proposed at bio-psycho-social levels. The American Institute of Medicine and National Research Council published 10 recommendations to optimize the provision of supportive care. Two of them emphasize the need to base care on peoples' needs, values and preferences, and the need to anticipate these factors [10]. To support practitioners who accompany cancer survivors in Switzerland, we aim to develop a holistic sensibilization and screening tool to identify survivors' needs. Firstly, a scoping review was conducted to identify the needs of cancer survivors by addressing the following research questions:
- What are the needs in long-term follow-up of cancer survivors?
- Are there socio-demographic differences in the needs (e.g. age, gender, marital status, income, location, etc.)?
- Are the needs greater in the transition phase (directly after acute treatments)?
2. Materials and Methods
This Scoping review was conducted according to the principles of the approach (recommendations) developed by the Joanna Briggs Institute (JBI) [11] for scoping studies. A protocol was written but not published. It is available on request. The PRISMA extension for Scoping reviews checklist (PRISMA-ScR) was used for reporting items [12].
2.1. Eligibility Criteria
This study used the PCC (population, context, concept) framework recommended by the JBI [11]. The “population” was defined as adult cancer survivors. We decided to exclude people who had received a paediatric or adolescent (< 18 years) cancer diagnosis. Due to different stages of physical, psychological, and social development, this section of the population has its own needs. For example, the needs for sexual health, can be very different from those of adults [13] . There is no consensus on the definition of "Cancer Survivor", and self-identification with this group is very personal and depends on many factors [14]. We used the definition of the European Organisation for Research and Treatment of Cancer (EORTC): “a cancer survivor is an individual who was diagnosed with cancer, finished primary cancer treatment and has no evidence of active disease” [15]. The reason was that we wanted to focus on the "post-cancer" period and deal with the chronic aspect of the disease. To ensure we have the right population, we excluded survivors where the time since diagnosis was less than two years. The “concept” was to consider the follow-up needs, domains, and categories (e.g. information, work issues and emotional factors) and not the specific supportive care needs (e.g. physiotherapy or psycho-oncology). Finally, the “context” was high-income countries. We excluded studies focusing on the indigenous population of countries, as this was not relevant for Switzerland.
Inclusion criteria were:
- Study design: Systematic reviews
- Published in peer-review journals
- Languages: English, French and German
-
Focusing on cancer survivors
- o
- all kinds of cancer
- o
- male or female
- o
- curative intent
- Studies from high-income countries
Exclusion criteria were:
- Other study designs, conference proceedings (in the absence of a full-text paper)
- Publications older than 2011
- Focusing on cancer survivors < 18 years old (at diagnosis)
- Time since diagnosis < 2 years
- Studies focusing on specific supportive care needs (e.g. physiotherapy)
- Studies from low- and middle-income countries (LMIC)
- Focusing on the indigenous population of high-income countries (HIC)
2.2. Search Strategies
Four electronic databases were searched with the help of a professional librarian information specialist: PubMed, Embase, Cochrane Library and Epistemonikos. The search was concluded on the 3rd of January 2023.
The search was based on three key concepts: unmet needs, follow-up, and cancer survivors. To increase the sensitivity of the search, controlled terms were associated with free terms (see Appendix A). The search strategy for PubMed is described in Appendix B. The other search strategies are available on request.
2.3. Selection of Sources of Evidence
The elimination of duplicate references was done in the reference management software MENDELEY. The selection of studies that meet the inclusion / exclusion criteria was done using RAYYAN in three distinct steps:
a) Selection based on titles: the first author (NSp) selected based on the titles of the articles. A second author (DK) reviewed the titles of excluded articles, and any differences of opinion were discussed between them;
b) Selection based on abstracts by two independent reviewers (NSp, DK). The results were compared and any differences in the selection of the reviewers were discussed on a case-by-case basis. Reasons for excluding studies were reported;
c) Selection based on the full texts by the first author (NSp). If there were any doubts, the lead author discussed them with the other authors of the review. Reasons for excluding studies were reported. The reference lists of the selected studies were searched for further studies.
2.4. Data Charting Process
The first author (NSp) extracted data from the selected studies using a form with specified categories and sub-categories. A co-author (DK) controlled the extraction of the data and completed any missing items if necessary.
2.5. Data Items
The following variables were reported:
- Source: title, author(s), year, journal, DOI / ISBN
- Characteristics of the study: number of included articles, objectives, database consulted, inclusion / exclusion criteria, bias, results of the quality appraisal
- Population: age, gender, cancer type, number of participants
- Concept: domains of needs
- Context: country, period (of the studies), setting
- Results: needs, unmet needs, conclusion, recommendation for screening tool, influence of the comorbidities, influence of socio-demographical factors, information about the transitional phase
2.6. Critical Appraisal of Individual Sources of Evidence
Analog to Ava Lorenc and his colleagues [16], quality of the individual systematic reviews was assessed with the AMSTAR (Assessing the Methodological Quality of Systematic Reviews) checklist [17]. We judged the validation of 13 of the 16 criteria. The three last criteria are only used for meta-analysis. We awarded two points for each criterion that was met and one for partially met. Studies are considered to be of sufficient quality if they achieve a score of 10 out of 26. Below this level, they are not included in the results. Above 15 points, studies are considered to be of good quality.
2.7. Synthesis of the Results
Due to the heterogeneity of the studies, a narrative analysis was used to identify the domains and categories of needs for each study. If any of the studies included in the selected systematic reviews did not meet the PCC criteria, they were excluded from the synthesis of results.
A map with the identified needs was created. Needs were later aggregated by domains and categories. But due to the heterogeneity of the studies (population, measuring instruments used), it was not possible to find a consensual basis. For this reason, six new global domains and 15 sub-categories of needs were created. These domains were ranked by counting the number of studies reporting the individual needs.
3. Results
3.1. Selection of Sources of Evidence
The search returned 414 results (Figure 1). After de-duplication, 373 were screened by title and abstract. 356 of them were removed, mainly because of the wrong outcome. 17 articles were read full text and 10 were included. In the reference lists of these, one new paper fulfilling all criteria was found. In total, eleven articles were included in this scoping review.
3.2. Characteristics of Sources of Evidence
All reviews were published between 2013 and 2021 (Table 1). These reviews included publications ranging from 1990 to 2021. The main countries analyzed in the reviews are USA (n=8), Canada (n=7), UK (n=6), Australia (n=6) and Netherland (n=4). The rest of the countries are spread all over the world but mostly in Europa and Asia. Some studies focus only on one cancer type: colorectal cancer (n=3), gynaecological (n=2) and thyroid (n=1). The others (n=5) examined three or more cancer types. Five studies mentioned their source of funding [13,18,19,20,21] and none of them disclaimed a conflict of interest.
1.2. Critical Appraisal within Sources of Evidence
According to our quality appraisal, four of the included studies [18,19,23,26] were considered as good quality with a score of 15 or more, six studies [13,20,21,24,25,27] were considered as sufficient quality with a score between 10 and 14. The quality of the last one [22]was not sufficient (6 out of 26) and was not included in the results.
1.3. Results of Individual Sources of Evidence
Some of the included studies did not fully meet the PCC criteria. But for all of them, the results are found in other studies meeting the PCC criteria or it is possible to differentiate the studies within a systematic review and thus exclude the results related to non-PCC studies. This last point is not possible by the study of Lehmann et al. [13]. But as this study is the only one to explore sexual health-related needs of cancer survivors, we decided to keep it. The results of each included study for the three research questions are presented in Table 2.
1.4. Synthesis of Results
As previously mentioned, needs were aggregated and compiled into 15 categories within six domains: health-related information, health system, mental, practical, relationship and physical (Table 3).
3.1. Health-Related Information
This need was reported in all the included studies. To meet certain objectives, cancer survivors should receive and process adequate information on all types of subjects. Timely [24,26], repeatedly-throughout-follow- up [24], and tailored information [18,19], especially about the short- and long-term effects of cancer and / or treatment was particularly needed [13,18,19,20,23,27]. Information on aftercare, support or rehabilitation services was also requested [18,19,20,23,25,27]. Nevertheless, it should be emphasized that the need for information is not only for the survivorship phase but is also perceptible from the very first screening tests and diagnosis, particularly in relation to the disease and the treatment[18,19,20,23,26,27]. Cancer survivors needed help to process the information when their cognitive skills were not sufficient. Pape et al. [26]recommended first assessing the person's level of understanding. Moreover, it was recommended to provide written information in addition to oral information delivered in the consultations[24,26]. To optimize the delivery of information, Maguire et al. advised to systematically assess the impact of the information received [19]. For their part, Kotronoulas and al. encouraged health professionals for better patient education [18].
3.2. Health System
As far as the health system is concerned, one of the most prevalent reported needs was related to the access and / or continuity of care and supportive care [19,21,24,25,26,27], which can intensely influence the experience of people with cancer, particularly at the time of diagnosis [19]. The need for better coordination and communication among healthcare professionals, especially between primary and secondary care was underlined [18,27]. Care navigation [27] and overall post-treatment follow-up (mainly by specialist nurses) was also lacking [18]. Health and social professionals have a role to play in optimizing care for cancer survivors. They should treat the person as an individual and not as a case [18]. They should be good listeners, trustworthy and sensitive (empathy) to the emotions of patients and those around them [13,18,19]. Cancer survivors wished that GPs make pro-active contact and wanted to discuss with them how to manage and adjust to life after treatment [23].
3.3. Mental
Cancer can cause some mental disruptions in the fields of existential, emotional, interpersonal / intimacy, and psychic health that can impact a person's behavior or reasoning. The most prominent concern in this domain was the fear of cancer recurrence and progression [18,19,21,24,25,27]. This persistent need [19,24] has a negative impact on quality of life and emotional well-being [19]. To avoid or limit the stress of cancer survivors, the feeling of being abandoned [18,26,27] should be addressed. This is also true for the “need for reassurance about being treated, especially when the safety net of the treatment ends” [21]. Managing anxiety was a need that was regularly highlighted in the psychic field. It was strongly correlated with a high level of unmet needs, irrespective of the domain [21,25].
3.4. Practical
Cancer can affect the daily life of survivors and their relatives. To improve this situation, support was needed for transportation [18] or travel [27], for commitment to maintaining or adopting healthy behavior [18,24], and for daily activities [21,24,25] like mowing the lawn, washing the car, cleaning the house, or cooking. Out-of-pocket costs for cancer treatment, costs for care and symptom management, as well as indirect costs (travel, loss of earning, etc.) could be a financial burden for cancer survivors [18,19,21,23,24,25,27]. For this reason, keeping a job or returning to work was a key issue. It could be deteriorated among other by the fatigue or some barriers at the office [24]. Cancer survivors needed help with this [18,19,24].
3.5. Relationship
The illness and / or treatments can disrupt interactions with the family and the social environment. The shame or embarrassment felt in certain social situations [19,24] could lead to isolation [19,27]. Support from the family, friends or peers ensured that survivors do not feel abandoned [24,26,27]. Access to support groups was another good strategy [18,27]. Survivors were also concerned about the well-being of their family and loved ones and the impact of their illness on them [19,25,27] In this way, support for the family with regard to their own worries for the survivors [18] could be necessary.
3.6. Physical
Disease and treatments can lead to body and cognitive consequences. The most notable need was the help to cope with lack of energy or cancer-related fatigue [18,19,21,24,25,26]. Other frequently cited needs were dealing with pain [18,19,21,24], urinary inconsistence [19] and bowel dysfunction [19,24]. Cancer survivors also needed help to manage side effects that can affect their sexual lives [13]. Cognitive dysfunctions like memory loss or difficulties to concentrate are less visible but still required support [19]. Although physical problems were not the most frequently mentioned in the selected studies, they were particularly important and needed to be managed because they could influence other areas [24]. For example, they were the cause of major functional limitations that could impact the smooth running of daily life. Changes in physical capacity could also affect the psychological / emotional domain, leading to increased stress, psychological problems, frustration, and uncertainty about the future. Moreover, these disorders were frequently associated with the recurrence or progression of cancer [24].
3.7. Socio-Demographic Factors
Five [13,18,21,25,27] of the studies selected investigated the influence of socio-demographic factors on needs. Female gender [13,18], younger age [13,18,21,25,27], less family or social support [18,21,25] and higher education level [18,21,25,27] were considered as risk factors. Cancer survivors with a higher level of education were also found to be more depressed or have an abnormal fatigue score [27]. Needs were influenced in a different way according to employment status and relationship status. Unemployed people had needs mostly in the domains of health care and information for financial support [21], while employed people needed emotional support, for example [18]. For sexual health-related care needs, single people expressed different needs compared to those with partners [13]. Single persons have more needs for support in dating new partners, while persons who are in partnership need support to discuss frankly about sex [13]. For geographical location, Van der Kruk et al. [27] found that people living in rural areas had certain specific needs. These were related to access to services or the lack of available services. The more isolated their place of residence, or the further away they were from major urban centers, the more these needs were exacerbated [21,27]. Moreover, people living in rural areas were more likely to experience problems related to finance, transport, and separation with family than people living near or in urban centers. They also reported worse social and emotional outcomes than urban survivors [27]. It should be noted that most of the studies included in this systematic review were conducted in large countries (USA, Canada, and Australia), where, due to the distances, the rurality context is different from other countries.
3.8. Transition Phase
The weeks or months following the end of acute treatment are particularly sensitive for cancer survivors. As they receive less support than during the treatment period and begin to feel the first side effects of treatment or disease, they must get on with their lives. In addition to frequent feelings of abandonment [18,24,25], many survivors were anxious to leave the hospital system [25] or should be reassured to continue to be treated [21]. Seven studies [13,18,19,21,23,24,25] found greater needs during this period. Coordination among healthcare professionals [18], proactive approach of general practitioners [23], communication with the treatment team [19], help with specific symptoms [25], long-term support [24] or transmission of information on late effects and supportive care [18,21] were the main needs. The fear of cancer recurrence was not influenced by the period and was just as important throughout the patient's journey [19,24].
4. Discussion
4.1. Summary of Evidence
Cancer survivors are a very heterogeneous group, with a large number and variety of support needs. Our review identifies the main needs experienced by cancer survivors. As these needs are described differently from one study to another, we decided to aggregate them into 15 categories, divided into 6 dimensions. Apart from the health system domain, which is more on a meta-level, our results match those identified by Margaret Fitch almost 20 years ago [28]. In her paper, she said: “Cancer and its treatment have an impact on individuals that is felt in a number of ways”. She proposed a supportive care framework for cancer care, presenting examples of needs for cancer survivors and categorizing them in seven domains: physical, psychological, spiritual, emotional, practical, social, and informational. This review shows that although these needs have been known about for a long time and have changed little over time, they remain problematic and are not yet adequately addressed.
One of the most important needs identified in our review is associated with processing health-related information.
According to Sørensen et al. [29], processing information requires four types of skills: i) be able to access the information; ii) understand; iii) assess its quality in terms of reliability, level of evidence and potential commercial conflicts and iv) be able to apply the information to health-related decisions. This allows the person to take an active role in the management of the illness, leading to a better quality of life. Two of these points are highlighted in our review. First, survivors must have access to good quality and adequate information. When information is not provided, survivors feel “disempowered and unimportant” [30]. More specifically, this information must be clear, accurate and reliable. It must also be provided in good time, in appropriate quantities and in a sensitive manner. This last point depends mainly on the healthcare professional's communication behavior [13]. Secondly, survivors should have certain cognitive abilities to understand this information. In Switzerland, around one out of five (18.48%) cancer survivors has sometimes, and one out of twenty (5.5%) has often or always difficulties understanding health-related written information [31]. Health professionals should therefore assess the understanding and the impact of the received information and provide support if necessary.
Cancer can lead to a variety of specific personal needs. These overlap and are interconnected, and for this reason need to be considered as a whole. Mental health needs are one of the most important. The first six to twelve months after treatment is a critical period for depression and anxiety [32]. In addition, during this period, the quality of life could be affected by the lack of “accessible professional counselling within the hospital framework” [32]. Survivors also need help to deal with uncertainty about the future and difficulty managing adversity, lifestyle changes or the fear of dying. In the emotional sphere, needs mainly concern self-image and the difficulty of managing the associated changes. At the interpersonal / Intimacy level, survivors must deal with changes in sexuality, whether due to dysfunction or loss of desire. Relationships with partners can also be difficult if their desires prove to be problematic for the person affected by mental disorders. Many other reasons can affect relationships and lead to avoiding social contact. For example, embarrassment due to the presence of a stoma and the associated smell [26], difficulties in dealing with tensions or difficulties in managing the social role change. Interactions with family or communication with children could also be a source of preoccupation for the cancer survivor as well as the inability to ask for help or find support for the family’s own worries. Accessing support groups is one of the identified solutions in our review. According to the Macmillan website [33], one of the benefits of the peer support groups is to share experiences and find coping strategies with people who have a similar background. This could be done face to face, online or by telephone. However, it is important to understand that such groups are not for everyone due to some barriers, such as embarrassment about sharing experiences, or the sensitivity of some peers to death [34]. Daily life is also impacted by cancer. Cancer survivors have needs regarding transportation and access to care, and face challenges with daily tasks such as housework, childcare, and gardening. They also have a greater risk of facing financial difficulties than the general population [35]. Cancer survivors need support for dealing with the financial burden and distress (financial toxicity) [35,36] of the disease and / or the treatment, to improve their financial well-being. A way of limiting the financial burden is to ensure that the person can keep an income. In France, the VICAN5 study shows that 20% of people aged between 18 and 54 who were working at the time of diagnosis are no longer working five years later. This loss of employment primarily affects the most vulnerable people in the labour market. Most people stopped working 3 to 5 years after diagnosis, indicating a medium-term effect of the disease [37]. A progressive return to work is recommended and some adaptations (e.g. position, working hours, workload, etc.) are often required. Sometimes a change of activity is the only solution. Among people employed at time of diagnosis, 54.5 % have kept the same job and 17.4% have changed [38]. The role of the employer is important to optimize the work environment [39], particularly in managing the reactions of colleagues and encouraging the integration of the person concerned. Daily health behaviours are also impacted. 53% of French cancer survivors declare having reduced or stopped physical activities compared to 34.3 % which do not change anything, and 12.7 % which train more [40]. Less than one person out of two (39.8%) stopped smoking within five years after diagnosis [41]. Physical inactivity and smoking are negatively associated with the health-related quality of life of cancer survivors [42]. Health promotion must be integrated into the follow-up of cancer survivors [9,43,44,45], and special attention is needed to provide them support to maintain or integrate healthy behaviours in their daily life. Finally, cancer survivors may experience cognitive problems such as memory loss, concentration difficulties or attention problems. They may also experience physical problems that affect all parts of the body and are often linked to the type of cancer. Cancer-related fatigue (CRF) or lack of energy are common symptoms among survivors, which affect the daily activities and well-being of the person. In their systematic review, Ma et al. [46] identify an overall pooled prevalence of CRF of 52%. CRF varies with time and is more significant close to the end of treatment and can affect cancer survivors up to 15 years after diagnosis [47].
The variety and ever-changing difficulties affecting cancer survivors emphasize the need for cancer survivors to have access to personalized, holistic, and integrated follow-up care [48]. Cancer navigation could be an interesting way of meeting all these goals and optimizing care and support throughout the cancer continuum [49]. Knowing the needs of cancer survivors appears to be the starting point for such follow-up care. This underscores the importance of conducting systematic assessments of supportive care needs, as part of the care routine [13,19,20,22,25,27,50] as soon as acute treatment ends. The World Health Organization [51] and the National Comprehensive Cancer Network [52] support these kinds of assessments, as an essential step for managing the late effects of cancer and / or treatments. Recently, more guidelines have been developed which recommend assessments, but there are not enough yet according to Hahn et al. [43]. Health professionals also have a role to play in sustaining survivors in their follow-up journey. According to William et al. [30] “effective communication could involve women being encouraged to ask questions, feeling listened to and not feeling rushed” and “poor communication left them feeling trivialized and uncared for”. This is emphasized by the study from Chamber et al. [34], where advanced prostate cancer survivors described their inability to raise their concerns and to get clear answers to questions due to insufficient and selective communication from clinicians. Consequently, they must find solutions by themselves.
Female gender, young age, lack of family or social support and a high level of education are considered as risk factors, while employment status, relationship status or geographical location can have a positive or negative influence on needs. For all these socio-demographic factors, the level of evidence varies between the authors, but these findings are confirmed by other studies, notably the qualitative systematic review of Bellas et al. [50]. These authors also consider other factors like type of cancer, treatments received, culture, language, and the presence of comorbidities.
Although the concept of moving into survivorship is not clearly defined [7], it is certain that this transition phase is critical for people and their families [10]. At this point, they receive less support than during the treatment period [53], while suffering the side-effects of the treatment or illness. They have a higher prevalence of unmet needs [21] and they often feel abandoned [18,24] and perceive a lack of access to care. This would therefore seem to be a good starting point for a systematic needs' assessment, although it is also advisable to do this beforehand [51]. A survivorship care plan should be developed from the data collected from this needs' assessment to provide "practical guidance" [10].
Lastly, it is important to point out that the experience of cancer can also lead to positive changes [24]. As described by Tedeschi & Calhoun [54], “post-traumatic growth refers to positive psychological change experienced as a result of the struggle with highly challenging life circumstances”. Many cancer survivors, 50% to more than 80%, report some benefits such as “strengthened interpersonal relationships, commitment to life priorities, life appreciation, personal regard, spirituality, and attention to health behaviours” [55]. One hypothesis for these changes is that the proximity of illness and death is an opportunity to take stock and redefine one's priorities in life, leading to changes that are seen as positive. However, these benefits appear to diminish over time [55].
4.2. Review Strengths and Limitations
The principles of the approach (recommendations) developed by the Joanna Briggs Institute [11] for scoping studies were followed for this review, minimizing methodological failures. Only peer-reviewed systematic reviews were included, which optimizes the quality of findings. Using the AMSTAR checklist for quality appraisal [17] ensured that we would avoid the worst quality studies. This review focuses on all types of cancer in developed countries. Although the contexts are different for each study, these findings can be generalized, which is useful for healthcare professionals to understand the overall needs of survivors and offer them appropriate care.
However, some limitations of our review must be acknowledged. Only four databases were used for the research. Moreover, grey literature was not searched. Some articles and information may therefore be missing. Although we cannot rule out the possibility that studies have been published since January 2023, the risk that new knowledge may have emerged between the date of the last electronic search and the publication of this article is low. Finally, due to the heterogeneity of the selected studies, it was impossible to assess the prevalence of needs. This would have helped the prioritization of needs.
5. Conclusions
People with a history of cancer often experience various side effects of the illness or treatments, which can also lead to positive outcomes. This review identifies a wide range of needs in the long-term follow-up of adult cancer survivors and provides a new classification. Although the evidence is not conclusive, there are some indications that these needs are particularly pronounced directly after the completion of the initial treatments and that the needs vary depending on the socio-demographic factors. Cancer survivors, their relatives and health professionals face a multifactorial problem and often have difficulties to identify and prioritize needs, which are highly individual and evolving. To provide an individual, holistic, and integrated follow-up, which is emphasized by the results of this scoping review, needs should be systematically and regularly assessed. This approach will enable the patient and the professional to identify what is really important and what needs to be addressed to help the person affected making this transition to survivorship, boost their self-esteem, enable them to reintegrate more effectively into society and the workplace, avoid precariousness and, ultimately, improve their quality of life.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Appendix A. List of search terms. Appendix B. Search strategy – Pubmed.
Author Contributions
All authors contributed to the study. Literature search and data analysis was performed by NSp. The first draft of the manuscript was written by NSp and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The author confirms that all data analyzed during this study are included in this published article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- WHO Cancer Tomorrow. Available online: https://gco.iarc.fr/tomorrow/en/dataviz/isotype (accessed on 26 February 2024).
- WHO Number of Deaths Caused by Selected Chronic Diseases Worldwide as of 2019 (in 1,000) [Graph]. Available online: https://www.statista.com/statistics/265089/deaths-caused-by-chronic-diseases-worldwide/ (accessed on 30 September 2023).
- WHO World Factsheet. In: International Agency for Research on Cancer. Available online: https://gco.iarc.who.int/media/globocan/factsheets/cancers/39-all-cancers-fact-sheet.pdf (accessed on 26 February 2024).
- Ligue suisse contre le cancer Ligue Suisse Contre Le Cancer. Le Cancer En Suisse : Les Chiffres. Available online: https://www.liguecancer.ch/a-propos-du-cancer/les-chiffres-du-cancer/-dl-/fileadmin/downloads/sheets/chiffres-le-cancer-en-suisse.pdf (accessed on 26 February 2024).
- Mullan, F. Seasons of Survival: Reflections of a Physician with Cancer. New England Journal of Medicine 1985, 313, 270–273. [Google Scholar] [CrossRef]
- Miller, K.; Merry, B.; Miller, J. Seasons of Survivorship Revisited. The Cancer Journal 2008, 14, 369–374. [Google Scholar] [CrossRef]
- Wood, S.K. Transition to Cancer Survivorship: A Concept Analysis. Advances in Nursing Science 2018, 41, 145–160. [Google Scholar] [CrossRef]
- Derbez, B.; Rollin, Z. Sociologie Du Cancer. Edition, La.; Collection Repères: Paris, 2016; ISBN 978-2-7071-8286-9. [Google Scholar]
- Firkins, J.; Hansen, L.; Driessnack, M.; Dieckmann, N. Quality of Life in “Chronic” Cancer Survivors: A Meta-Analysis. Journal of Cancer Survivorship 2020, 14, 504–517. [Google Scholar] [CrossRef]
- Institute of Medicine and National Research Council Delivering Cancer Survivorship Care. From Cancer Patient to Cancer Survivor: Lost in Transition; National Academies Press: Washington, D.C, 2006; ISBN 978-0-309-09595-2. [Google Scholar]
- Peters, M.D.; Godfrey, C.; McInerney, P.; Munn, Z.; Tricco, A.C.; Khalil, H. Chapter 11: Scoping Reviews. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI, 2020.
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, V.; Laan, E.T.M.; den Oudsten, B.L. Sexual Health-Related Care Needs among Young Adult Cancer Patients and Survivors: A Systematic Literature Review. Journal of Cancer Survivorship 2021. [Google Scholar] [CrossRef]
- Cheung, S.Y.; Delfabbro, P. Are You a Cancer Survivor? A Review on Cancer Identity. Journal of Cancer Survivorship 2016, 10, 759–771. [Google Scholar] [CrossRef]
- Fitch, M.I. Take Care When You Use the Word Survivor. Canadian Oncology Nursing Journal 2019, 29, 2019. [Google Scholar]
- Lorenc, A.; Feder, G.; MacPherson, H.; Little, P.; Mercer, S.W.; Sharp, D. Scoping Review of Systematic Reviews of Complementary Medicine for Musculoskeletal and Mental Health Conditions. BMJ Open 2018, 8, e020222. [Google Scholar] [CrossRef] [PubMed]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A Critical Appraisal Tool for Systematic Reviews That Include Randomised or Non-Randomised Studies of Healthcare Interventions, or Both. BMJ 2017, 358, 4008. [Google Scholar] [CrossRef]
- Kotronoulas, G.; Papadopoulou, C.; Burns-Cunningham, K.; Simpson, M.; Maguire, R. A Systematic Review of the Supportive Care Needs of People Living with and beyond Cancer of the Colon and/or Rectum. European Journal of Oncology Nursing 2017, 29, 60–70. [Google Scholar] [CrossRef] [PubMed]
- Maguire, R.; Kotronoulas, G.; Simpson, M.; Paterson, C. A Systematic Review of the Supportive Care Needs of Women Living with and beyond Cervical Cancer. Gynecol Oncol 2015, 136, 478–490. [Google Scholar] [CrossRef] [PubMed]
- Hyun, Y.G.; Alhashemi, A.; Fazelzad, R.; Goldberg, A.S.; Goldstein, D.P.; Sawka, A.M. A Systematic Review of Unmet Information and Psychosocial Support Needs of Adults Diagnosed with Thyroid Cancer. Thyroid 2016, 26, 1239–1250. [Google Scholar] [CrossRef]
- Miroševič, Š.; Prins, J.B.; Selič, P.; Zaletel Kragelj, L.; Klemenc Ketiš, Z. Prevalence and Factors Associated with Unmet Needs in Post-treatment Cancer Survivors: A Systematic Review. Eur J Cancer Care (Engl) 2019, 28, e13060. [Google Scholar] [CrossRef] [PubMed]
- Dahl, L.; Wittrup, I.; Væggemose, U.; Petersen, L.K.; Blaakaer, J. Life After Gynecologic Cancer—A Review of Patients Quality of Life, Needs, and Preferences in Regard to Follow-Up. International Journal of Gynecological Cancer 2013, 23, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Hoekstra, R.A.; Heins, M.J.; Korevaar, J.C. Health Care Needs of Cancer Survivors in General Practice: A Systematic Review. BMC Fam Pract 2014, 15, 94. [Google Scholar] [CrossRef]
- Lim, C.Y.S.; Laidsaar-Powell, R.C.; Young, J.M.; Kao, S.C.; Zhang, Y.; Butow, P. Colorectal Cancer Survivorship: A Systematic Review and Thematic Synthesis of Qualitative Research. Eur J Cancer Care (Engl) 2021, 30, 1–18. [Google Scholar] [CrossRef]
- Lisy, K.; Langdon, L.; Piper, A.; Jefford, M. Identifying the Most Prevalent Unmet Needs of Cancer Survivors in Australia: A Systematic Review. Asia Pac J Clin Oncol 2019, 15, e68–e78. [Google Scholar] [CrossRef]
- Pape, E.; Vlerick, I.; Van Nieuwenhove, Y.; Pattyn, P.; Van de Putte, D.; van Ramshorst, G.H.; Geboes, K.; Van Hecke, A. Experiences and Needs of Patients with Rectal Cancer Confronted with Bowel Problems after Stoma Reversal: A Systematic Review and Thematic-Synthesis. European Journal of Oncology Nursing 2021, 54, 102018. [Google Scholar] [CrossRef]
- van der Kruk, S.R.; Butow, P.; Mesters, I.; Boyle, T.; Olver, I.; White, K.; Sabesan, S.; Zielinski, R.; Chan, B.A.; Spronk, K.; et al. Psychosocial Well-Being and Supportive Care Needs of Cancer Patients and Survivors Living in Rural or Regional Areas: A Systematic Review from 2010 to 2021. Supportive Care in Cancer 2021, 1–44. [Google Scholar] [CrossRef]
- Fitch, M.I. Supportive Care Framework. Canadian Oncology Nursing Journal 2008, 18, 6–14. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, K.; Van den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H. Health Literacy and Public Health: A Systematic Review and Integration of Definitions and Models. BMC Public Health 2012, 12, 80. [Google Scholar] [CrossRef]
- Williams, N.; Griffin, G.; Farrell, V.; Hauck, Y.L. Gaining Insight into the Supportive Care Needs of Women Experiencing Gynaecological Cancer: A Qualitative Study. J Clin Nurs 2020, 29, 1684–1694. [Google Scholar] [CrossRef]
- Arditi, C.; Peytremann Bridevaux, I.; Eicher, M. The Swiss Cancer Patient Experiences-2 (SCAPE-2) Study: A Multicenter Cross-Sectional Survey of Patient Experiences with Cancer Care in the French- and German-Speaking Regions of Switzerland 2023.
- Moore, K.A.; Ford, P.J.; Farah, C.S. “I Have Quality of Life...but...”: Exploring Support Needs Important to Quality of Life in Head and Neck Cancer. European Journal of Oncology Nursing 2014, 18, 192–200. [Google Scholar] [CrossRef]
- Macmillan Cancer Support Cancer Self-Help and Support Groups. Available online: https://www.macmillan.org.uk/cancer-information-and-support/get-help/emotional-help/local-support-groups (accessed on 8 October 2023).
- Chambers, S.K.; Hyde, M.K.; Laurie, K.; Legg, M.; Frydenberg, M.; Davis, I.D.; Lowe, A.; Dunn, J. Experiences of Australian Men Diagnosed with Advanced Prostate Cancer: A Qualitative Study. BMJ Open 2018, 8. [Google Scholar] [CrossRef]
- Lewis, S.E.; Doroudi, M.; Yabroff, K.R. Financial Hardship. In Handbook of Cancer Survivorship; Feuerstein, M., Nekhlyudov, L., Eds.; Springer Cham: Cham, 2018; ISBN 978-3-319-77430-5. [Google Scholar]
- Abrams, H.R.; Durbin, S.; Huang, C.X.; Johnson, S.F.; Nayak, R.K.; Zahner, G.J.; Peppercorn, J. Financial Toxicity in Cancer Care: Origins, Impact, and Solutions. Transl Behav Med 2021, 11, 2043–2054. [Google Scholar] [CrossRef]
- Alleaume, C.; Bousquet, P.-J.; Joutard, X.; Paraponaris, A.; Peretti-Watel, P.; Seror, V.; Vernay, P. Situation Professionnelle Cinq Ans Après Un Diagnostic de Cancer. In La vie cinq ands après diagnostic de cancer; Institut National du Cancer (INCa), Ed.; 2018; pp. 174–201.
- Alleaume, C.; Bousquet, P.-J.; Joutard, X.; Paraponaris, A.; Peretti-Watel, P.; Seror, V. Trajectoire Professionnelle Après Un Diagnostic de Cancer. In La vie cinq ans après un diagnostic de cancer ; Institut National du Cancer (INCa), Ed.; 2018; pp. 202–221.
- Von Ah, D.; Duijts, S.; van Muijen, P.; de Boer, A.; Munir, F. Work. In Handbook of Cancer Survivorship; Feuerstein, M., Nekhlyudov, L., Eds.; Springer Cham: Cham, 2018; ISBN 978-3-319-77430-5. [Google Scholar]
- Ancellin, R.; Ben Diane, M.-K.; Bouhnik, A.-D.; Mancini, J.; Menard, E.; Monet, A.; Peretti-Watel, P.; Sarradon-Eck, A. Alimentation et Activité Physique. In La vie cinq ans après un diagnostic de cancer; Institut National du Cancer (INCa), Ed.; 2018; pp. 278–297.
- Deutsch, A.; Monet, A.; Peretti-Watel, P. Consommation de Tabac et d’alcool. In La vie cinq ans après un diagnostic de cancer; Institut National du Cancer (INCa), 2018; pp. 298–311.
- Han, X.; Robinson, L.A.; Jensen, R.E.; Smith, T.G.; Yabroff, K.R. Factors Associated With Health-Related Quality of Life Among Cancer Survivors in the United States. JNCI Cancer Spectr 2021, 5. [Google Scholar] [CrossRef]
- Hahn, E.E.; Jones, J.; Syrjala, K.L. Comprehensive Healthcare. In Handbook of Cancer Survivorship; Feuerstein, M., Nekhlyudov, L., Eds.; Springer Cham: Cham, 2018; ISBN 978-3-319-77430-5. [Google Scholar]
- Ostroff, J.S.; Riley, K.E.; Dhingra, L.K. Smoking. In Handbook of Cancer Survivorship; Feuerstein, M., Nekhlyudov, L., Eds.; Springer Cham: Cham, 2018; ISBN 978-3-319-77430-5. [Google Scholar]
- Nekhlyudov, L.; Mollica, M.A.; Jacobsen, P.B.; Mayer, D.K.; Shulman, L.N.; Geiger, A.M. Developing a Quality of Cancer Survivorship Care Framework: Implications for Clinical Care, Research and Policy. J Natl Cancer Inst 2019. [Google Scholar] [CrossRef]
- Ma, Y.; He, B.; Jiang, M.; Yang, Y.; Wang, C.; Huang, C.; Han, L. Prevalence and Risk Factors of Cancer-Related Fatigue: A Systematic Review and Meta-Analysis. Int J Nurs Stud 2020, 111. [Google Scholar] [CrossRef] [PubMed]
- Thong, M.S.Y.; van Noorden, C.J.F.; Steindorf, K.; Arndt, V. Cancer-Related Fatigue: Causes and Current Treatment Options. Curr Treat Options Oncol 2020, 21, 17. [Google Scholar] [CrossRef] [PubMed]
- Sperisen, N.; Cardinaux-Fuchs, R.; Schneider-Mörsch, B.; Stoll, S.; Haslbeck, J. Onkologiepflege. Kleinandelfingen 21, pp. 12–14. 20 March.
- Riley, S.; Riley, C. The Role of Patient Navigation in Improving the Value of Oncology Care | Journal of Clinical Pathways. Journal of Clinical Pathways 2016, 1, 41–47. [Google Scholar]
- Bellas, O.; Kemp, E.; Edney, L.; Oster, C.; Roseleur, J. The Impacts of Unmet Supportive Care Needs of Cancer Survivors in Australia: A Qualitative Systematic Review. Eur J Cancer Care (Engl) 2022, 31, e13726. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Supportive, Survivorship and Palliative Care. WHO REPORT ON CANCER: setting priorities, investing wisely and providing care for all; World Health Organization: Geneva, 2020; pp. 94–97. ISBN 978-92-4-000129-9. [Google Scholar]
- National comprehensive cancer network Survivorship Care for Cancer-Related Late and Long-Term Effects 2020.
- Jefford, M.; Karahalios, E.; Pollard, A.; Baravelli, C.; Carey, M.; Franklin, J.; Aranda, S.; Schofield, P. Survivorship Issues Following Treatment Completion-Results from Focus Groups with Australian Cancer Survivors and Health Professionals. Journal of Cancer Survivorship 2008, 2, 20–32. [Google Scholar] [CrossRef] [PubMed]
- Tedeschi, R.G.; Calhoun, L.G. TARGET ARTICLE: “Posttraumatic Growth: Conceptual Foundations and Empirical Evidence. ” Psychol Inq 2004, 15, 1–18. [Google Scholar] [CrossRef]
- Stanton, A.L.; Rowland, J.H.; Ganz, P.A. Life after Diagnosis and Treatment of Cancer in Adulthood: Contributions from Psychosocial Oncology Research. American Psychologist 2015, 70, 159–174. [Google Scholar] [CrossRef]
Figure 1.
PRISMA flow chart.
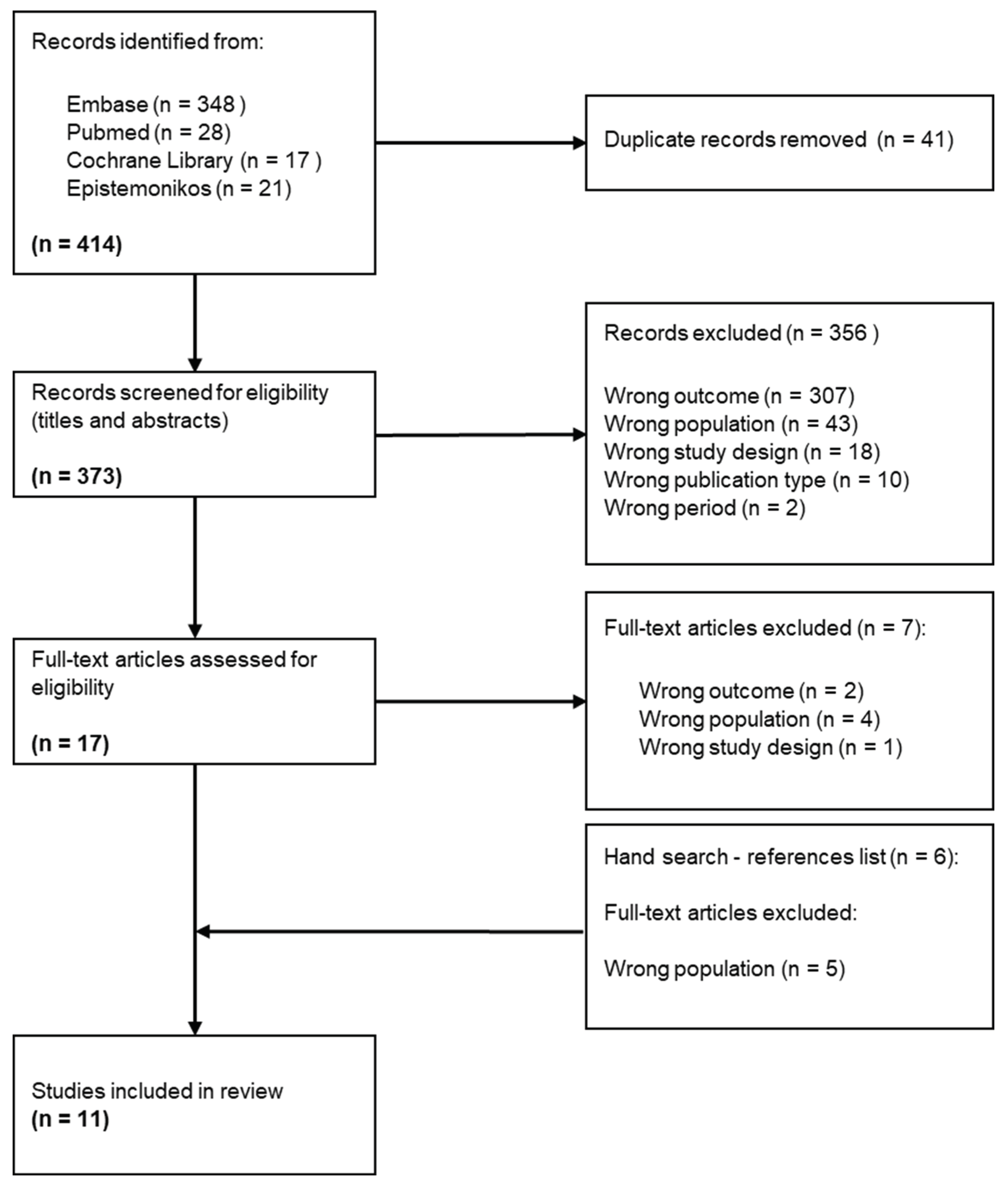

Table 1.
Characteristics of the included studies Critical appraisal within sources of evidence.
| Characteristics of the studies | Context | Population | Limitations | |||||
|---|---|---|---|---|---|---|---|---|
| Aim of the studies | Number of included articles | Period of analysis (of the studies) | Countries | Number of participants (range) | Gender | Cancer type | ||
| Dahl et al. (2013) [22] | To investigate knowledge on the quality of life after cancer, which factors could be predictors, and knowledge on gynecological cancer patients' needs and preferences regarding follow-up | 57 | 1995-2012 | Not reported | Not reported | Not reported | Gynecological | ▪No limitations are reported ▪Little or no information about the target group and setting ▪Prisma flow chart is not available ▪Only capture English research |
| Hoekstra et al. (2014) [23] | To report how adult cancer survivors describe their care needs in the general practice environment | 15 | 1990-2012 | UK, USA, Canada, Denmark, Italy | 970 (6 - 431) | Men, women | Bladder, prostate, breast, colorectal, head and neck, lung, melanoma, testis, gynecological, bowel, hematological, non-Hodgkin's lymphoma, Hodgkin's, gastrointestinal, unknown / other | ▪Use of only 3 databases for the search ▪Delay between the search and the publication ▪Possibly under representation of all existing needs |
| Hyun et al. (2016) [20] | To examine the unmet information needs and the unmet psychosocial support needs of adult thyroid cancer survivors | 7 | 2008-2016 | USA, Canada, Netherlands, South Korea, | 6,215 | Majority of women | Thyroid | ▪Level of agreement between reviewers was limited ▪No stratification of needs according to important variables (clinic-histopathologic sub-group, life stage, or disease status in response to treatment) ▪Only capture English research |
| Kotronoulas et al. (2017) [18] | To synthesize evidence in relation to the supportive care needs of people living with and beyond cancer of the colon and / or rectum | 45 | 1996-2016 | UK, Australia, other (not specified) | 10,057 (5 - 3011) | "Men (64.5%) Women (35.5%)" | Colon and / or rectum | ▪Mixed patient samples ▪No grey literature researches ▪Limitations due to the tool used for appraising the methodological quality ▪Only capture English research |
| Lehmann et al. (2021) [13] | To identify the prevalence of sexual health-related care needs and the types of needs that should be addressed by providers | 35 | 2004-2019 | Denmark, USA, Germany, Canada, Australia, Netherlands | 5,938 (8-879) | Majority of women | Breast, testicular, gynecological, | ▪ Focus on need addressed by professionals ▪ Risk of biased assessment of all the included studies. ▪Only capture English research |
| Lim et al. (2021) [24] | To synthesize the current body of qualitative research on colorectal cancer survivorship as early as the immediate post-operative period, and to compare the experiences of early-stage and advanced colorectal cancer survivors | 81 | 2006-2019 | USA, Europe, UK, Australia, Asia, Canada, New Zealand, Middle East | Not reported | Not reported | Colon and / or rectum | ▪ Search was not exhaustive ▪ Subjective inclusion of articles due to differing definition of "survivorship" and lacked clarity on participants "survivorship status" ▪ Deviation from the original PROSPERO protocol ▪Only capture English research |
| Lisy et al. (2019) [25] | To identify the most prevalent unmet needs of cancer survivors in Australia and to identify demographic, disease, or treatment-related predictors of unmet needs | 17 | 2007-2018 | Australia | Not reported | Not reported | Gynecological, breast, brain, hematological, endometrial, prostate, testicular, various | ▪ Data are limited by the measure used to assess unmet needs ▪ Review does not include a proportionate distribution of cancer types in Australia ▪ Study selection and quality appraisal were conducted primarily by one reviewer ▪ Studies included in this narrative review were equally weighted regardless of sample size |
| Maguire et al. (2015) [19] | To synthesize evidence with regard to the supportive care needs of women living with and beyond cervical cancer | 14 | 1990-2013 | USA, Canada, UK, Indonesia, South Korea, Nigeria, Thailand | 1,414 (10 - 968) | Women | Cervical | ▪ Search was limited to the most common databases ▪ No grey literature research ▪Only capture English research |
| Miroševič et al. (2019) [21] | To determine the prevalence and identify the factors that contribute to higher levels of the unmet needs. To identify the most commonly unmet needs and those factors that contribute to higher levels of unmet needs in each domain separately | 26 | 2007-2015 | Australia, UK, USA, China, Singapore, Canada, Ireland, Netherlands, Iran, South Korea | 10,533 (63 - 1668) | Men, women | Breast, gynecological, hematological, head and neck, colorectal, endometrial, various | ▪Most of the included studies were cross-sectional ▪Included studies lacked information (prevalence, factors associated with specific domains, stage of cancer at diagnosis) ▪Homogenous sample in several studies ▪Only capture English research |
| Pape et al. (2021) [26] | To describe the experiences and needs of patients with rectal cancer confronted with bowel problems after stoma reversal. | 10 | 2006-2021 | UK, USA, China, Taiwan, Sweden, Netherlands | 156 (5 - 36) | "Men (approx. 58%) Women (approx. 42%)" | Rectal with Stoma reversal | ▪ Some studies do not reach data saturation ▪ Small sample for some studies ▪ Some studies were performed as single centre studies ▪ Most of the studies did not report on the severity of participants' bowel problems |
| Van der Kruk et al. (2021) [27] | To review levels of psychosocial morbidity and the experiences and needs of people with cancer and their informal caregivers, living in rural or regional areas | 65 | 2010-2021 | Australia, USA, Canada, Europe | Not reported | Not reported | Breast, hematological, colorectal, lung, head & neck, gynecological, prostate, myeloma, various | ▪ Included studies have different definition of "rurality" ▪ Different methodological approach and data sources of the studies ▪ No meta-analysis was conducted due to the heterogeneity of the studies ▪ Findings are conceptual rather than statistical ▪ Only capture English research |
Table 2.
Results according to research questions.
| Authors (year) | Identified needs (domains) | Socio-demographic factors associated with needs | Greater needs in the transition phase |
|---|---|---|---|
| Hoekstra et al. (2014) [23] | • Medical • Psychosocial • Information • Proactive contact • Other |
- | • Proactive approach of the general practitioner |
| Hyun et al. (2016) [20] | Information on: • Thyroid cancer • Thyroid cancer treatment • Diagnostic tests • Aftercare • Psychosocial issues • Coordination of care • Complementary and alternative medicine |
- | - |
| Kotronoulas et al. (2017) [18] | • Physical / cognitive • Psychosocial / emotional • Family-related • Social / societal • Interpersonal / intimacy • Practical / daily living • Information / education • Health system / patient-clinician communication needs |
• Gender • Age • Education level • Employment status • Family support |
• Better coordination among healthcare professionals • Psychological support for feeling of abandonment |
| Lehmann et al. (2021) [13] | Sexual health-related care / Sex-related: ▪ Information ▪ Practical / emotional support ▪ Communication |
• Age • Gender • Relationship status |
- |
| Lim et al. (2021) [24] | ▪ Physical symptoms ▪ Functional limitations ▪ Psychosocial impacts ▪ Financial impacts ▪ Interaction with healthcare system ▪ Coping ▪ Positive outcome |
- | • Long-term support • Support for feeling of abandonment by the healthcare team |
| Lisy et al. (2019) [25] | • Psychosocial • Supportive care • Physical |
• Age • Education level • Employment status • Social support |
• Support for anxiety about leaving the hospital system |
| Maguire et al. (2015) [19] | • Physical • Psychological / emotional • Social • Interpersonal / intimacy concerns • Health system / information • Patient-clinician communication • Spiritual / existential |
- | • Support about intimate relationships • More information regarding prognosis • Better communication with the clinical team |
| Miroševič et al. (2019) [21] | • Psychological • Physical and daily living, • Relationship • Patient care • Information |
• Age • Employment statusa • Education levela • Social supporta a weak evidence |
• Support for fear of cancer recurrence • Better information • Reassurance about being treated |
| Pape et al. (2021) [26] | Before surgery (stoma reversal): • Information before surgery • Sources of information After surgery: • Management and coping • Support from peers and the environment • Support of the healthcare professionals |
- | - |
| Van der Kruk et al. (2021) [27] | • Financial and travel issues • Accessibility to care • Psychological • Information |
• Location (urban vs rural) • Education level • Age • Income |
- |
Table 3.
Details of domains and categories of needs.
| Domains of needs | Definition | Categories of needs | Examples of challenges | Number of studies reporting these needs |
|---|---|---|---|---|
| Health-related information | Need to receive and process adequate information on all types of subjects to meet certain objectives | Access | Lack of information (all kinds of information), quality and delivery of information | 10 |
| Education | Difficulties to process information, comprehension, and quality assessment | |||
| Health system | Need to access a personalized, comprehensive, and integrated care and support pathway to reduce or treat the consequences of the disease and / or treatments. | Healthcare professionals | Lack of knowledge of the unique needs of rural survivors by medical staff located in metropolitan treatment centers, on-going patient-clinician contact, post-operative follow-up (hospital doctor) or post-treatment follow-up (specialist nurse), helping with common (late) treatment effect, initialization of discussions about sexual health by providers, empathic and sensitive discussion on sexual health, overcome taboos, enough time to discuss sensitive matters | 10 |
| Health and supportive care | Coordination of health care services (primary and secondary), access to counselling / support groups, access to complementary / alternative medicine, gap in supportive care, medical help / treatment for non-cancer related problems, general preventative healthcare, access and continuity of care, comprehensive care, regular monitoring of needs, navigation in health system | |||
| Mental | Supportive care needs to reduce emotional, existential, interpersonal and / or psychic health conditions, due to illness and / or treatment, that disrupt a person's behavior or reasoning | Emotional | Deal with altered body image, appearance (attractiveness, self-image, desirability, femininity), emotional health | 9 |
| Existential | Fear of cancer recurrence, uncertainty, adversity, lifestyle changes, worries about the future | |||
| Interpersonal / intimacy | Changes in sexuality, coping with sexual dysfunction, lack of sexual desire, anxiety about sexual intercourse, feeling to be forced to fulfill the partner's sexual desires (cultural pressure and expectation) | |||
| Psychic | Stress, feeling of abandonment after treatment, anxiety, distress, depression | |||
| Practical | Need for support to limit the impact of the disease and / or treatment on daily life | Daily activities | Not being able to do usual things, transportation, identification, and integration of health behaviors | 7 |
| Financial impact | Financial well-being, worry about earning money, fighting financial toxicity | |||
| Work | Return to work, adapting work to new capacities (position, schedule, workload, etc.), change of professional activity, reactions of colleagues / leaders | |||
| Relationship | Need for support to reduce or deal with the consequences of the illness and / or treatments that disrupt interactions with the family and the social environment | Family | Support of family for its own worries, family's future, worry about partners and family | 6 |
| Social | Embarrassment in social situation, relationship with others, lack of practical and emotional support from peers and the environment, difficulties and tensions in relationships, isolation, social role change, social desirability | |||
| Physical | Supportive care needs to alleviate or treat the physical and cognitive consequences of the disease and / or treatments | Body | Fatigue / lack of energy, pain, physical problems, dysfunction, sleep loss, urinary incontinence, bowel dysfunction, difficulty breathing, infertility, hormone changes, loss of strength, nausea-vomiting, neuropathy, sexual dysfunction, skin irritation, weight changes, infected or bleeding wound, mouth- or eye-related, physical examination, managing side-effects (physical symptoms) | 6 |
| Cognitive | Memory loss, difficulty concentrating or cognitive dysfunction |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



