
Submitted:
28 March 2024
Posted:
28 March 2024
You are already at the latest version
Abstract
Cancer being a multi-factorial disease, a multi-target approach is needed to treat it with minimal side-effects. Therefore, combined use of a proven herbal formula with chemo-therapy could be the better therapeutic. It may maintain homeostasis by synergistically targeting multiple signaling pathways involved in tumorigenesis, thus circumventing recurrence, resistance, and immunosuppression. Here we aim to determine the effectiveness and safety of an FDA-approved herbal formula, SR033 in combination with 5-fluorouracil (5FU) and paclitaxel (PTX). We report chemo-sensitization and chemo-synergy in HeLa and MCF-7 cell lines, immunomodulation of COX-2, PD-L1, VEGF and TGFβ and overall survival in-vitro and in-vivo via oral and topical delivery of SR033. In-vitro, SR033/5FU significantly reverses 5FU and PTX-resistance, lower COX-2, and PD-L1, resulting in TGFβ/ VEGF axis modulation. Furthermore, the study suggests that due to anti-oxidative potential of SR033, oral administration exerts chemo-preventive activity and restores cellular compartment in solid tumor and ascites-bearing mice models. Furthermore, the topical application, SR033L with low-dose 5FU increases survival rate, reduces tumor growth, and completely restores local and peripheral neutrophil-lymphocyte ratio in solid tumor mice model. The study indicates that SR033 could be a strong candidate in combination with low-dose 5FU and PTX for a holistic approach to cancer management.
Keywords:
cancer
; 5-fluorouracil
; paclitaxel
; chemo-preventive
; chemo-sensitization
; homeostasis
1. Introduction
Cancer is one of the most common non-communicable diseases and a leading cause of death worldwide. Many cancers arise from sustained chronic inflammation resulting in oxidative stress, critical for tumor progression in every stage [1,2]. However, effective treatments such as chemotherapy also generate free radicals, thereby, increasing inflammation, chemo-resistance, and immunosuppression, affecting overall survival and long-term prognosis of the disease [3].
Vital regulators involved in inflammation include COX-2 which is regulated by oncogenes, pro-inflammatory cytokines such as TGFβ and growth factors such as VEGF [4]. COX-2 has a promoter that displays an NFκB and a cytokine-dependent response element, which is also involved in PD-L1 expression on tumor cells [5]. PD-L1 is a critical modulator in T cell sweating, as it defends tumor cells against triggered T cells and generates immune destruction [6]. Despite the clinical success, immunotherapy costs, and associated complications do not meet patients’ compliance [7,8]. Furthermore, the use of corticosteroids can address inflammation; however, the optimal dose and efficacy of integrative chemotherapy or immunotherapy, have to be further evaluated.
5-fluorouracil (5FU) and paclitaxel (PTX) has been used as a first line therapy for treating few solid tumors, however, had limited clinical application due to side-effects of high drug doses, low drug efficiency and drug-resistance [9,10,11]. Therefore, low-dose metronomic chemotherapy has been used as an alternative for treating some tumors [12] which confers high efficiency, low toxicity and reduced drug-resistance in the clinical settings [13,14]. 5FU and PTX in integration with anti-inflammatory molecules increase drug response [11,15].
Therefore, a change in the paradigm for cancer management by incorporating non-toxic, validated and efficacious anti-inflammatory modalities can be adopted to achieve a better prognosis and a robust treatment plan. According to World Health Organization (WHO) (2019), 88% of Member States have acknowledged their use of Traditional Complementary & Alternative Medicines (T&CAMs) as an essential inclusion in the treatment protocol for a better prognosis of the disease [16]. Herbal formulations are traditionally employed as adjuncts, CAMs, or integrative medicines to combat the adverse effects of chemotherapy. Evidence-based CAMs could illuminate the holistic approach in the clinical setting by decreasing oxidative stress and counteracting drug resistance, thereby achieving a therapeutic index to treat cancer without compromising the quality of life, and maintaining homeostasis [17,18,19,20].
However, this field is mired with constant assertions that natural products are safe and can be prescribed without serious consideration of the extent of the disease as they are not expected to play a pivotal role in the treatment [21]. Further, it has been exploited by several commercial entities to proclaim baseless claims.
Therefore, modern clinical practitioners might find it hard to rationalize its efficacy and fail to incorporate this approach in their treatment protocols. In this study, we aim to overcome the side-effects of chemo-drugs by integrating a herbal formulation, SR033 as an attempt to bridge the gap between traditional and modern approaches. In our study, we hypothesized SR033 as a chemo-protective, chemo-sensitizer, and an integrative adjunct with chemotherapy against cancer.
2. Results
2.1. Quality Assessment and Safety of SR033
NMR is considered one of the gold standard methods for the fingerprinting of novel compounds. NMR chromatogram of the water decoction of SR033 was obtained from its two different batches and found similar (Figure 1.A), which suggested no batch-to-batch variation. Therefore, these profiles could be considered as a quality control parameter of the herbal extract. Additionally, to determine the presence of two major active components of SR033 decoction, curcumin, and EGCG, HPLC was performed. Furthermore, to compare the peaks, we prepared standard curves using different concentrations of curcumin and EGCG standards at 420 and 280 nm, respectively. We found that the HPLC profile of SR033 showed a peak at 11.326 min and 3.109 min corresponding to curcumin and EGCG, respectively at their respective wavelengths (Figure S1a). We also estimated their concentrations and interestingly, we confirmed the presence of 15 ng/mL curcumin and 76 µg/mL EGCG in the plasma of mice treated with SR033 decoction (Figure S1b).
To take it forward, it was important to assess the safety of SR033, thereby identifying its maximum tolerable dose. Thus, we performed the acute toxicity test according to the OECD guideline 425 (OECD., 2001), wherein healthy mice were administered with graded single doses of SR033 decoction for 14 days. We did not observe any lethality or mortality during and after 14 days of administration, up to the maximum dose of 5000 mg SR033/Kg. Therefore, 1/10th, high dose of SR033 (HDS) and 1/20th, low dose of SR033 (LDS) of the maximum tolerable dose were considered as optimal doses for in-vivo studies (Table S2). Additionally, we analyzed H&E-stained liver sections of healthy mice treated with HDS. Liver histology showed normal central vein, predominant cords, and a regular sinusoidal region similar to untreated healthy mice liver (Figure 1B). Therefore, the data suggest high dose of SR033 is safe in terms of mortality and liver toxicity.
2.2. SR033 Prevents and Reduces Tumor Formation, and Improves Life Span in 5FU Treated EAC Tumor Mice Models by Maintaining Homeostasis
Herbal formulae are known to be used in disease risk reduction and as an immune modulator. Since SR033 is non-toxic and consists of well-established anti-oxidative components, we were interested in determining its role in reducing the incidence, recurrence, and severity of cancer. To determine the chemo-preventive facet of SR033, we studied Ehrlich Ascites Carcinoma (EAC) implanted at breast site (solid tumor) and peritoneum region (ascites). In prophylactic models, LDS and HDS (200µL/ day/ mice) were administered orally to respective mice for 15 days before tumor induction. After 30 days of tumor induction, we confirmed that SR033 inhibits tumor growth at both sites (Table 1; Figure S2).
The limit in solid tumor size by HDS was comparable to the therapeutic high dose of 5FU (HDF), moreover, arrest in ascites growth was not significant. Paradoxically, reduction in solid tumor growth was prominent by both P&T effects of HDS, unlikely to the effects observed on ascites volume, where therapeutic HDS effect was more effective than the prophylactic and was correlative to therapeutic HDF. However, no such difference was notable in packed cell volume of both the ascites models as well in 5FU group. Consistent with the role, HDS treatment of solid tumor showed a similar mean survival time as assessed in its prophylactic model, moreover, was higher than that in HDF group.
Cancer is often associated with leucocytosis which may be a marker of an underlying process such as inflammation and aggressive malignancy which is prominent in advanced stages and anemia is also associated with cancer progression. Therefore, we performed total blood count using the whole blood of the surviving mice in each group. We observed a dose-dependent decrease in WBC level, furthermore, following earlier trend, HDS effects on both the solid tumor and ascites models were more competent than 5FU treatment (Table 1; Figure S2). Similarly, we observed that treatment with HDS increases RBCs in both tumor models. Interestingly, opposite to the dose dependent trend in solid and ascites tumors, there was no notable difference in WBC and RBC levels of P&T effects on tumor models. Therefore, the data suggest that SR033 acts in a dose-dependent manner, and due to the severity of ascites and the degree of its progression, SR033 was comparatively effective in solid tumor growth prevention. SR033 also preserved the hematological system in a dose-dependent manner (Table 1; Figure S2), irrespective of the tumor site, indicating SR033 reaches bloodstream and has potential to modulate at molecular level. After the termination of the study, we performed liver histology using H&E stain and observed mild inflammatory infiltration (IF), irregular perisinusoidal cells and hepatocytes, and shrunken sinusoids (S) in the untreated tumor group (T). Furthermore, we confirmed that SR033 restores hepatocytes and sinusoidal regions, however, mild inflammation was also present (Figure S3). These results suggest SR033 is a promising T&CM candidate as it decreases tumor size and improves survival in cancer models while preserving homeostasis.
2.3. Integrative Approach: SR033 with Chemo-Drugs Prevents Chemo-Induced Inflammation, Acts Synergistically, Improves Survival, and Overcomes Drug Resistance
As 5FU modulated blood cell counts and decreased survival, it led us to determine the effect of 5FU on the generation of free radicals and whether anti-oxidative SR033 decoction counteracts it. We investigated percent free radicals by performing SOD assay of the plasma isolated from various treated and untreated groups of therapeutic solid tumor mice model (Figure 2A). We noted that though HDF significantly increases free radical generation, SR033 significantly helped in balancing percent free radicals along with high and low doses of 5FU (HDF and LDF). Interestingly, untreated tumor group generated negligible amount of free radicals. Moreover, the percent free radical with SR033/LDF treatment was similar to the healthy groups. To investigate the downstream effects of 5FU-generated free radicals, we also evaluated the effect of 5FU on inflammatory molecular markers viz. COX-2 transcript, and VEGF and TGFβ protein levels in MCF-7. We noticed a strong correlation between these markers, moreover, 5FU significantly induces COX-2 transcript (Figure 2B) and VEGF and TGFβ protein expression in a time-dependent manner (Figure 2C-D). 5FU induced 77% higher COX-2 at 48 h than at 24 h which was comparable to the effect of PMA (positive control). Additionally, as expected, SR033 prominently decreased the respective molecular markers in a time-dependent manner.
Since the collaborative effect of SR033 and 5FU represent synergy, we investigated this combination for three main impacting factors on cancer treatment: tumor size, survival and hematological parameters in EAC implanted solid tumor at hind region of mice. The tumor was grown for 10 days and then treated with SR033L (400µL/ day/ mice) with and without LDF and HDF. After 30 days of treatment, as expected, SR033L failed to reduce tumor size, however, SR033L/LDF and HDF indicated a noteworthy decrease in tumor size when compared to SR033L alone (Figure 2E). Comparatively, both the 5FU doses showed uniformity in tumor reduction with SR033L, which suggests the use of low-dose chemo-drugs with SR033 as efficacious as LD50, with no toxicity. Similarly, both the combinations showed the best survival outcomes with a significant 13.3% increase, irrespective of 5FU dose (Figure 2F). Similar to oral SR033, SR033L/LDF also restored hematopoietic system by decreasing total WBCs (Figure 2G) and increasing RBCs (Figure 2H). However, there was no evident effect of LDF on hematological parameters, likely due to its limited efficacy and toxicity. Furthermore, we assessed the effect of SR033L on inflammation and necrotic and mitotic cells in the tumor microenvironment. The eosin-stained tumor sections showed recovery with the presence of mixed lymphocytic cells. They showed fewer mitotic cells (Table 2), unlike the tumor sections obtained from untreated EAC control (T). Group T_SR033L showed necrotic replacement of the tumor mass in all animals, although 3/5 (1 animal eliminated from the group due to mortality during the experimental period) showed complete replacement of tumor mass with necrotic lesions. Inflammation was observed around viable portions of the tumor mass (Figure 3A).
In the line, we also noticed that longer exposure to chemo-drugs such as 5FU and PTX led to resistance with the DRI of 2.5×103 and 2.27 on HeLa-R and 2.76 and 8.82 on MCF-7-R cells, respectively (Figure S4). We found that respective EC50 of SR033 achieves 2.5×103- and 79-fold DRR of HeLa-R and 6.93- and 17.3-fold DRR of MCF-7-R to 5FU and PTX, respectively. In addition, when EC50 of SR033 with various lower concentrations of 5FU or PTX was added to resistant cells, the inhibitory effect enhanced when compared with the drug counterparts alone. These findings indicate that SR033 synergizes with even the modest concentrations of 5FU and PTX to enhance the inhibitory effect by 80% and 88% in HeLa-R (Figure 3B and 3C) and 60% and 57% in MCF-7-R cells (Figure 3D and 3E), respectively and also prevents chronic inflammation, chemo-resistance, vascularization, and tumor progression.
2.4. SR033 Restores Immune Status during Chemotherapy
Given that SR033 alone and in combination with chemo-drug preserves hematological parameters, improves survival, and also acts synergistically, we sought to determine whether it preserves neutrophil-to-lymphocyte ratio (NLR) in tumor mice models. Mice with the solid tumor at hind region were treated with different doses of 5FU with and without SR033L. When treated with SR033L/LDF and SR033L alone, NLR was strikingly reduced by 96.6 % (Figure 4A) which was comparative to healthy group, supporting earlier survival response and the trend obtained for hematological parameters. Moreover, SR033L/HDF failed to decrease NLR in tumor-bearing mice models.
As SR033 is acting on lymphocytes, there is a high chance of it acting on markers associated with T cells in tumor progression. An immune marker, PD-L1 expression on tumor cells inhibits T cell response, therefore, we were interested to investigate the effect of SR033 on PD-L1 expression by tumor cells. We noticed that upon IFNγ stimulation, PD-L1 induces in PC3 cells (C) and SR033 represses up to 76.9% of the up-regulated PD-L1 (Figure 4B), supporting the notion that the combination of SR033 with or without low dose chemo-drug, immuno-modulates to maintain homeostasis.
3. Discussion
Inflammation acts as a double-edged sword, which plays an essential role in tumorigenesis, building a pro-tumorigenic micro-environment and in tumor therapy [36,37]. 5FU and PTX are effective and commonly used chemo-drugs, however, their side effects limit their dose and the concern of chemo-resistance restricts the use of several classes of drugs simultaneously which hampers the entire clinical outcome [4,38]. There is mounting evidence that chemotherapy induces inflammation via NFkB pathways leading to COX-2 induction [4,38]. These issues should be alongside addressed by T&CM, which could further improve the chemotherapeutic regimen.
Our study established 5FU-resistant HeLa-R and MCF-7-R cell lines which showed cross-resistance to PTX with a higher DRI than previously reported [39,40,41,42]. Higher DRI is impactful to test the effectiveness of chemo-sensitizing compounds and DRR. Our study observed that SR033 along with 5FU and PTX achieve remarkable 80% inhibition of chemo-resistant cells by sensitizing them to 5FU and PTX and acting synergistically which allowed achieving IC50 at a very minimal concentration of 5FU and PTX (Figure 3B-E). Taken together, we found that even a modest concentration of 5FU and PTX can synergize with SR033 to accelerate resistant cell inhibition and DRR, which is significantly higher than that reported earlier [30]. The DRR property of SR033 could be attributed to its anti-oxidant property, indicating that SR033 synergizes with 5FU and PTX to preserve homeostasis of the body while improving the efficacy of the drug for cancer treatment. The outcomes also correspond with in-vivo data supporting the integrative approach using LDF with SR033.
We undertook in-vivo experiments to further investigate the safety (Table S2), chemo-preventive, anti-tumoral, and immunomodulatory properties of SR033.
We also explored the integrative approach to treat solid tumor using topical SR033L/LDF and compared it with SR033L/HDF (Figure 2E-H). To the best of our knowledge, this is among a few in-vivo studies, integrating topical herbal formulation for treating a superficial tumor. Although effective, chemotherapy produces free radicals, imbalances homeostasis thus decline survival in cancer patients [3,36,43], therefore, mitigating free radical production and suppressing the downstream pathways is of prime importance. We found that SR033 overcome the free radicals generated by HDF and LDF (Figure 2A). SR033L act synergistically to improve the efficacy of 5FU, survival, and the hallmarks of homeostasis. Although the tumor area was reduced significantly by HDF; nevertheless, it was reduced by 35% with SR033L/LDF. Overall, the results indicate that LDF which is an ineffective non-toxic dose; with SR033, proved efficient and competent. Therefore, a validated herbal formula in combination with chemo-drugs could be highly potent holistic medicine and might provide a new approach to cancer management and treatment.
A better way to overcome the limitation of oral route delivery (as discussed above) is to maintain a constant plasma level by regular consumption of these herbal compounds. However, as suggested by the HPLC profiles, it was intriguing to know that the regular intake of SR033 builds plasma levels of curcumin and EGCG up to their effective concentrations in mice. Besides, cytoprotective and anti-oxidant properties, oral SR033 can render protection as a neutraceutical, as documented in our in-vivo studies where we demonstrated the first scientific evidence that a herbal formula consists of curcumin and EGCG holds disease risk reduction. SR033 studies demonstrated a significant increase in MST, moreover, prevented, and decreased tumor growth in mice models (Table 1, Figure S2). Prophylactic LDS and HDS significantly increased MST by 20.85 % and 31.65 %, respectively in solid tumor. Our finding of exploring SR033 was not limited to solid tumor, but ascites also. Paradoxically, the P&T effects of SR033 were more prominent on the solid tumor size than the ascites volume, which could be due to the differences in their histology and also the limited duration of the experiment. Furthermore, this is supported by no notable difference in the actual viable tumor cells, represented by the packed cell volume of the two ascites models. WBC and RBC levels were similar in both the models and tumor sites. However, topical SR033L significantly reduced WBCs and increased RBCs with respect to its oral administration. SR033 treatment also restored the hepatocytes and sinusoidal regions, as liver toxicity is a major concern in the chemotherapy regimen (Figure S3). Taken together, the data suggest that SR033 could be used as a health booster to prevent cancer as it interacts with cellular compartments, reflecting on considering herbal formula as chemo-preventive and also to prevent cancer recurrence while maintaining homeostasis.
5FU and PTX increase inflammation, cell proliferation, and metastasis by secreting inflammatory cytokines, including COX-2 (Figure 5) [43]. Combination drug regimen incorporating COX-2 inhibitors like niflumic acid and NS-398 effectively decreases its level in cell lines [44,45]. Our study found that alike PMA, 5FU also induces COX-2 expression in a time-dependent manner which was significantly decreased by SR033 (1.7 and 2.27 folds, respectively) in MCF-7 (Figure 2B), suggesting SR033 as a COX-2 inhibitor.
COX-2 is correlated with poor cancer prognosis and induces VEGF by a positive feedback loop [4,46,47]. VEGF is an angiogenic factor required for neo-vascularization in tissues. Co-treatment of SR033 with 5FU resulted in 22% decrease in VEGF levels by 48 h as opposed to 72.5% by 24 h in MCF-7 (Figure 2C). This trend was remarked in COX-2 mRNA levels also (68% and 36.2% decrease at 24 h and 48 h, respectively). Lesser reduction of 5FU induced COX-2 and VEGF mRNA at 48h could be due to increased stabilization by HuR protein which is required for their mRNA stability, therefore, helps sustain their expression for a longer period [48]. The other reason is the low half-life of SR033, as reflected in our preliminary stability experiments (not shown), where the activity (EC50 value) of SR033 decreases by 48 h. To address the half-life issue of SR033, we exposed MCF-7 to 5FU for 48 h and SR033 for last 24 h and observed that SR033 decreases VEGF and COX-2 gene expression levels significantly as compared to their respective controls.
Furthermore, a pleiotropic cytokine, TGFβ induces and synergistically enhances COX-2 expression through COX-2 mRNA stability mechanisms [4,49]. There is evidence of high TGFβ and VEGF secretion by tumor cells, and there are few reports on Chinese traditional medicines to show VEGF/TGFβ axis reduction [50,51]. In the present study, TGFβ levels in MCF-7 follow the same trend as VEGF and COX-2 (Figure 2B-D). Our study showed no significant increase in TGFβ levels by 5FU at 48 h, although a slight decrease is observed at 24 h, which could be due to intrinsic factors and saturation of TGFβ levels. However, treatment with SR033 showed a significant decrease in inflammatory and angiogenic markers, indicating a strong correlation with TGFβ/VEGF axis. Thus, considering it as a suitable candidate for CAM and would be among a very few validated herbal formulations used as CAM in Indian Medicinal System for cancer management (Figure 5).
COX-2 is also involved in modulating PD-L1 on tumor cells, which is a potential marker of immune response and is associated with immune evasion [49]. Only 20-40% patients respond to PD-L1 inhibitors due to resistance and a decrease in targetability and hence the efficacy of the drug further reduces in clinical conditions [52,53]. Earlier studies have shown downregulation of IFNγ induced PD-L1 by active herbal components in cancer cell lines [54,55]. We observed a significant reduction in PD-L1 mRNA expression by SR033 in PC3 (Figure 4B). This is very promising and prospective to be used as an adjunct with immunotherapy also, although it necessitates in vivo studies to calculate its therapeutic window, with special emphasis on its bioavailability. This CAM approach could advance combination treatment protocols with standard chemotherapy or checkpoint inhibitors (Figure 5).
Neutrophils are also involved in tumor progression, which may re-route inflammation in a tumor-promoting direction by contributing to angiogenesis and promoting the circulation of the tumor cells [56]. In contrast, the presence of lymphocytes in the circulation is associated with better chemotherapeutic response. Therefore, we estimated NLR using SR033L to relate the immune status and homeostasis in tumor mice model (Figure 4A). For the first time, a herbal formulation restored NLR by 96 % and in the line, SR033L with LDF considerably decreased the number of viable tumor cells in tumor biopsy (Figure 3A, Table 2).
4. Materials and Methods
2.1. Herbal Formulation
SR033 is a novel herbal formula composed of five well-established anti-tumor and anti-inflammatory compounds, such as Curcuma, Syzygium aromaticum, Elettaria cardamomum, Camellia sinensis and Cinnamomum verum [22,23,24,25]. It is developed by Sri Raghavendra Biotechnologies Pvt Ltd., Bangalore which has an FSSAI license and has been registered for patent. For in-vitro studies, hot water decoction of SR033 powder was freshly prepared at the concentration of 0.2 g/mL and filtered using 0.22 μm sterile filter. For the oral route of delivery (in-vivo), SR033 decoction was similarly prepared at the concentrations obtained from the acute toxicity test. For the topical route of delivery (in-vivo), SR033 was extracted in water, followed by ethanol, and mixed with glycerol, camphor, and vegetable starch to form a suitable paste, SR033L (0.12 g SR033 powder/mL of paste).
2.2.1. H-NMR and HPLC
SR033 decoction from two different batches was prepared, lyophilized, and performed 1H-NMR to obtain the spectra/ fingerprint using a Bruker AV400 (BrukerBiospin, Rheinstetten, Germany) spectrometer with a cryoprobe at 298 K, relaxation delay and acquisition time of 3s and 4s, respectively [26].
Levels of curcumin and epigallocatechin gallate (EGCG) in hot water decoction of SR033 were measured using High-Performance Liquid Chromatography (HPLC) with slight modifications [27]. The conditions included a C18 column with 250×4.6 mm dimension and 5 µm pore size; and a mobile phase constituting 1% orthophosphoric acid: methanol (50:50). The injection volume of 20 µL was run for 15 min at 425 nm and for 5 min at 280 nm to determine curcumin and EGCG, respectively. Chromatographic peaks in SR033 were identified by corresponding to the retention time of curcumin and EGCG standards. Furthermore, to detect the components in mice plasma, the mobile phase for EGCG was changed to water: acetonitrile: methanol: ethyl acetate: glacial acetic acid (89:6:1:3:1) and run for 15 min at 280 nm.
2.3. Cell Lines
Human cancer cell lines, including cervical (HeLa), breast (MCF-7), and prostate (PC3), were obtained from NCCS, Pune. Cells were maintained in DMEM/F-12 supplemented with 10 % FBS (Gibco) and 1 % penicillin/ streptomycin (HiMedia) in a humidified incubator at 37˚C with 5% CO2. Passage numbers ranging from 5-7 were used for performing at least three independent in-vitro experiments.
2.3.1. Development of Resistant Cell Lines
Stably resistant cells to 5-Fluorouracil (5FU) were developed as described earlier [28,29] with slight modifications. HeLa and MCF-7 were gradually exposed to increasing concentrations of 5FU and maintained at their 50% inhibitory concentration (IC50), i.e., 2 µg/mL and 9.4 µg/mL to select surviving resistant cells, named HeLa-R and MCF-7-R, respectively.
2.3.2. In-Vitro Groups
PC3 cell line (prostate cancer) is one of the cell lines to determine the expression of CD274, referred as PD-L1. To achieve this, 4×105 PC3 cells were rested for 24 h and were treated under two conditions: 10 ng/mL IFNγ alone and co-treatment of 10 ng/mL IFNγ and ½ EC50 of SR033 (0.6 mg/mL). After 24 h, the cells were used for RNA isolation and PD-L1 gene expression was recorded.
MCF-7 cell line expresses COX-2 gene and VEGF and TGF β proteins under specific conditions. We noticed that COX-2, VEGF, and TGF β was induced with 2 µg/mL (IC50) of 5FU for 24 h and 48 h in MCF-7 cell line. To evaluate their modulation by SR033, 24 h resting culture of 4×105 cells was treated with different conditions. Cells treated with 5FU were co-treated with ½ EC50 of SR033 (0.6 mg/mL) in a time-dependent manner for 24 h and 48 h. In the group, 5FU (48 h)+SR033 (24 h), cells were treated with 2 µg /mL of 5FU for 48 h and 0.6 mg/mL SR033 treatment in the last 24 h. The 10 ng/mL PMA (phorbol myristate acetate) (Thermo Fisher Scientific) was considered a positive control. Finally, RNA was isolated from the cells treated with various conditions and COX-2 gene expression was recorded. To determine the VEGF and TGF β levels, the supernatant from each culture condition was collected and ELISA was performed.
2.3.3. RNA Semi-Quantitative RT-PCR
The cells were trypsinized, total RNA was extracted using RNA isolation kit (Quaigen) and cDNA was obtained using MuLV cDNA synthesis kit (Invitrogen). Semi-qualitative RT-PCR was performed for COX-2 and PD-L1 genes (Table S1). PCR products were analyzed using ImageJ software, and the data was normalized to the housekeeping gene, GAPDH, and relative to the respective control. The fold change of the normalized target gene mRNA levels was measured.
2.3.4. ELISA
The culture medium from each group of the transcriptional study for COX-2 was collected and stored at -80˚C until use. Supernatants were thawed, and VEGF and TGFβ protein release was estimated using respective ELISA (Ray Biotech) and normalized to the respective protein concentration which was estimated by bicinchoninic acid assay (BCA) (Thermo Fisher Scientific).
2.3.5. Survival Assay
Drug resistance reversal (DRR) was determined by analyzing cell viability using MTT assay [28] with slight modification. Briefly, a single-cell suspension of HeLa-R and MCF-7-R was prepared in DMEM/F-12 and allowed to adhere in 96 wells plate (100 µL/well at 2×104 cells/mL). HeLa-R and MCF-7-R were treated with EC50 of SR033 (100 µL/ well), i.e., 600 µg/mL and 1250 µg/mL, respectively. Concentrations of 5FU used on HeLa-R and MCF-R were (4, 2, 1, 0.5, 0.25, 0.12, 0.06, 0.03, 0.01) µg/mL and (50, 25, 12.5, 6.25, 3.1, 1.5, 0.78, 0.39) µg/mL, respectively. Concentrations of paclitaxel (PTX) used on HeLa-R and MCF-R were (5.6, 2.8, 1.41, 0.7, 0.35, 0.17, 0.08, 0.04) × 10-3 µg/mL and (500, 250, 125, 62.5, 31.25, 12.6, 7.8) × 10-3 µg/mL , respectively.
Fresh medium with MTT reagent (5 µg/mL, 100 µL for each well) (Sigma) was added to each well and incubated for 4 h. DMSO was added to dissolve Formazan crystals, and values were measured at OD545. The DRR was calculated according to the following formula: EC50 in blank control group/ EC50 in the reversed group [30]. Similarly, both the cell lines were also treated with SR033 and different concentrations of PTX.
2.4. Animals
The 8-week-old Swiss albino male mice, weighing 20-25 g were obtained from Karnataka College of Pharmacy, Bangalore. The proposed experiments were approved by the Institutional Animal Ethics Committee (1564/PO/Re/S/11/CPCSEA) and confirmed to CPCSEA and ARRIVE guidelines. Six males were randomly assigned to each group and were housed using standard procedures in temperature and a humidity-controlled animal facility equipped with ventilated cages with a 12 h light / dark cycle. They were provided conventional mouse food and tap water ad libitum. Euthanasia was performed by using 40 mg/Kg Pentobarbital sodium (i.p.).
2.4.1. Acute Toxicity
The acute toxicity after a single oral dose of SR033 was evaluated according to the OECD guideline 425 [31]. A graded dose of SR033 (0, 250, 500, 2000, and 5000 mg/kg) extracted in warm drinking water was administered orally to mice (200 μL per mouse) (N=30), respectively and mortality was recorded for fifteen days. The results obtained determine the concentrations of SR033 used for oral studies.
2.4.2. Tumor Implantation
The 2×106 Ehrlich Ascites Carcinoma cells (EAC) within a volume of 200 µL were implanted in all animals, and the tumor (T) was grown for 10-days at the breast region (solid tumor) and peritoneum (ascites) to study SR033 (oral) (Figure 6A), and at hind region (solid tumor) to study SR033L (topical) (Figure 6B).
2.4.3. Oral Administration
SR033 oral administration was studied in two ways; Prophylactic and Therapeutic (P&T) (N=108). Following groups were formed: Group I (Healthy) was on a regular diet, and water (vehicle) by oral gavages daily for the entire study duration. Group II (T) EAC bearing mice without treatment, served as carcinogen control. Group III (T_HDF) EAC bearing mice received 20 mg/mL 5FU (i.p.) bi-weekly after tumor induction. Group IV (T_LDS) EAC bearing mice received a low oral daily dose of 250 mg/Kg SR033. Group V (T_HDS) EAC bearing mice received a high oral daily dose of 500 mg/Kg SR033 after tumor induction. Similar groups were formed for both breast site and peritoneum region tumor. Unlike therapeutic, in prophylactic model, SR033 was administered with low dose of SR033 (LDS) and high dose of SR033 (HDS) orally for 15 days before tumor induction (Figure 6A). On 30th day of the experiment, tumor size and volume were measured, blood and liver were collected to study hematological and histological examination, respectively before euthanizing the animals. Mean survival time (MST) was estimated as (day of 1st death + day of last death)/ 2 [32].
2.4.4. Topical Application
Before topical application of SR033L, fur was depilated before tumor induction using a hair removal cream (N=48). The area was cleaned using cotton dipped in warm water and SR033L (400 µL/ mouse, equivalent to 0.048 g SR033) was applied with a syringe and spatula.
Animals were divided under following scheme: Group I (C) served as a control. Group II (T) EAC bearing animals without treatment, served as carcinogen control. Group III (T_SR033L) EAC bearing animals received daily SR033L application after tumor induction. Group IV (T_LDF+SR033L) and Group V (T_HDF+SR033L) included EAC bearing animals treated bi-weekly with low dose (0.2 mg/Kg) and high dose (20 mg/Kg) of 5FU i.p., respectively, bi-weekly along with daily SR033L topical application. Group VI (T_HDF) EAC bearing animals received standard 5FU (20 mg/Kg), i.p. bi-weekly. For all the groups, treatment was started from day 11 of tumor induction for 30 days. On last day of the experiment, tumor area, survival proportion, hematological parameters, and differential blood count were performed before mice were euthanized and tumor tissue was isolated for analysis (Figure 6B).
2.4.5. Superoxide Dismutase (SOD) Assay
2.4.6. Histopathology
Liver and tumor tissues were washed with buffered saline, and transferred to 10% neutral formalin fixative for 48 h, dissected, and stained using hematoxylin and eosin (H&E) stain as described earlier [35].
2.5. Statistical Analysis
GraphPad Prism 8.0 was used to statistically analyze the data using two-tailed t-test for two groups and one-way ANOVA followed by Tukey's test for more than three groups. ImageJ software was used to analyze the gel images. The Kaplan-Meier curve was used for survival analysis. In-vitro experiments were replicated in triplicate. Statistical significance was considered when p<0.05. The data were represented as mean±SD for in-vitro and as mean±SEM for in-vivo studies.
5. Conclusions
Combination groups of SR033L/ LDF were remarkable in terms of reduction in tumor burden and maintaining hallmarks of homeostasis, reiterating the promise of the CAM approach, and paving the way to treat superficial tumor. Further studies in clinical trials will hold answers to these prospects. Overall, SR033 with LDF, as an integrative approach, could also be examined to prevent and treat tumor metastasis and recurrence. Moreover, the integrative studies of SR033 with other chemo-drugs are also essential to assess. This study limit to validate the integrative approach in-vivo xenotransplantation models.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Figure S1: Chromatographic profiles of SR033 in HPLC; Figure S2: SR033 prevented and suppressed tumor growth in a dose-dependent manner in-vivo. Figure S3: SR033 restored hepatocytes and sinusoidal regions which were compromised in EAC control and LDF treated group. Figure S4: Inhibition of growth of HeLa and MCF-7 and their respective resistant counterparts by 5FU and PTX using MTT assay; Table S1: Primer sequences with their annealing temperatures used for semi-quantitative RT-PCR; Table S2: Data interpretation of acute toxicity test for SR033 (N=6 in each group).
Author Contributions
Jyothsna A. Rao and S.G.A. Rao conceptualized, designed the study and supervised; Ankita Umrao, Pooja Kasture and Madhavi Naik investigated the study, curated data and analyzed data; Debjani Dasgupta and Gururaj A. Rao supervised the study, validate the results and helped in data visualization; Ankita Umrao prepared the manuscript; Jyothsna A. Rao revised the manuscript.
Funding
This work was funded by Sri Raghavendra Biotechnologies Pvt Ltd, Bangalore, which is developing the oral and topical herbal formulations.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Animal Ethics Committee of Karnataka College of Pharmacy, Bangalore on (protocol no. KCP-IAEC/2/17-18/3/15-04-17, approved on 15th April, 2017).
Informed Consent Statement
Not applicable.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Acknowledgments
I am grateful to Dr. Raju Koneri from Karnataka College of Pharmacy, Bangalore for providing the animal house facility and Mr. Deepak Kumar Jha for helping with animal handling. I am thankful to Dr. Arvind Kumar and Dr. Varun Jaiswal for helping in shaping and reviewing the manuscript. SR033 and SR033L were generously provided by Sri Raghavendra Biotechnologies Pvt Ltd., Bangalore for the experiments.
Conflicts of Interest
The authors declare no conflicts of interest. Sri Raghavendra Biotechnologies Pvt. Ltd. helped in publishing the data. The funders had no role in the collection, analyses, or interpretation of data; or in the writing of the manuscript.
References
- Bieniek, J.; Childress, C.; Swatski, M.D.; Yang, W. COX-2 inhibitors arrest prostate cancer cell cycle progression by down-regulation of kinetochore/centromere proteins. The Prostate 2014, 74, 999-1011. [CrossRef]
- Dutta, J.; Fan, Y.; Gupta, N.; Fan, G.; Gelinas, C. Current insights into the regulation of programmed cell death by NF-κ B. Oncogene 2006, 25, 6800-6816. [CrossRef]
- Nedeljković, M.; Damjanović, A. Mechanisms of chemotherapy resistance in triple-negative breast cancer—how we can rise to the challenge. Cells 2019, 8, 957. [CrossRef]
- Abdel-Aziz, A.M.; El-Tahawy, N.F.G.; Mohammed, M.M.; Ali, A.I.; Ibrahim, Y.F. Amelioration of testosterone-induced benign prostatic hyperplasia using febuxostat in rats: The role of VEGF/TGFβ and iNOS/COX-2. Eur. J. Pharmacol. 2020, 889, 173631. [CrossRef]
- Terzuoli, E.; Bellan, C.; Aversa, S.; Ciccone, V.; Morbidelli, L.; Giachetti, A.; Donnini, S.; Ziche, M. ALDH3A1 overexpression in melanoma and lung tumors drives cancer stem cell expansion, impairing immune surveillance through enhanced PD-L1 output. Cancers 2019, 11, 1963. [CrossRef]
- Fan, X.; Jin, J.; Yan, L.; Liu, L.; Li, Q.; Xu, Y. The impaired anti-tumoral effect of immune surveillance cells in the immune microenvironment of gastric cancer. Clin. Immunol. 2020, 108551. [CrossRef]
- Calabrese, L.H.; Calabrese, C.; Cappelli, L.C. Rheumatic immune-related adverse events from cancer immunotherapy. Nature Reviews Rheumatology 2018, 14, 569-579. [CrossRef]
- Dhodapkar, K.M. Autoimmune complications of cancer immunotherapy. Curr. Opin. Immunol. 2019, 61, 54-59. [CrossRef]
- Banerji, A.; Lax, T.; Guyer, A.; Hurwitz, S.; Camargo Jr, C.A.; Long, A.A. Management of hypersensitivity reactions to carboplatin and paclitaxel in an outpatient oncology infusion center: a 5-year review. The Journal of Allergy and Clinical Immunology: In Practice 2014, 2, 428-433.
- Duggett, N.A.; Griffiths, L.A.; McKenna, O.E.; De Santis, V.; Yongsanguanchai, N.; Mokori, E.B.; Flatters, S.J. Oxidative stress in the development, maintenance and resolution of paclitaxel-induced painful neuropathy. Neuroscience 2016, 333, 13-26. [CrossRef]
- Marin, J.J.; Macias, R.I.; Monte, M.J.; Herraez, E.; Peleteiro-Vigil, A.; Blas, B.S.d.; Sanchon-Sanchez, P.; Temprano, A.G.; Espinosa-Escudero, R.A.; Lozano, E. Cellular mechanisms accounting for the refractoriness of colorectal carcinoma to pharmacological treatment. Cancers 2020, 12, 2605. [CrossRef]
- Lien, K.; Georgsdottir, S.; Sivanathan, L.; Chan, K.; Emmenegger, U. Low-dose metronomic chemotherapy: a systematic literature analysis. European Journal of Cancer 2013, 49, 3387-3395. [CrossRef]
- Loven, D.; Hasnis, E.; Bertolini, F.; Shaked, Y. Low-dose metronomic chemotherapy: from past experience to new paradigms in the treatment of cancer. Drug discovery today 2013, 18, 193-201. [CrossRef]
- Gong, L.-H.; Chen, X.-X.; Wang, H.; Jiang, Q.-W.; Pan, S.-S.; Qiu, J.-G.; Mei, X.-L.; Xue, Y.-Q.; Qin, W.-M.; Zheng, F.-Y. Piperlongumine induces apoptosis and synergizes with cisplatin or paclitaxel in human ovarian cancer cells. Oxidative medicine and cellular longevity 2014, 2014. [CrossRef]
- Tinoush, B.; Shirdel, I.; Wink, M. Phytochemicals: potential lead molecules for MDR reversal. Frontiers in Pharmacology 2020, 11, 832. [CrossRef]
- Organization, W.H. WHO global report on traditional and complementary medicine 2019; World Health Organization: 2019.
- Rajagopal, C.; Lankadasari, M.B.; Aranjani, J.M.; Harikumar, K. Targeting oncogenic transcription factors by polyphenols: A novel approach for cancer therapy. Pharmacol. Res. 2018, 130, 273-291. [CrossRef]
- Zangui, M.; Atkin, S.L.; Majeed, M.; Sahebkar, A. Current evidence and future perspectives for curcumin and its analogues as promising adjuncts to oxaliplatin: state-of-the-art. Pharmacol. Res. 2019, 141, 343-356. [CrossRef]
- Zhu, F.; Xu, Y.; Pan, J.; Li, M.; Chen, F.; Xie, G. Epigallocatechin Gallate Protects against MNNG-Induced Precancerous Lesions of Gastric Carcinoma in Rats via PI3K/Akt/mTOR Pathway. Evidence-Based Complementary and Alternative Medicine 2021, 2021. [CrossRef]
- Lopez, G.; McQuade, J.; Cohen, L.; Williams, J.T.; Spelman, A.R.; Fellman, B.; Li, Y.; Bruera, E.; Lee, R.T. Integrative oncology physician consultations at a comprehensive cancer center: analysis of demographic, clinical and patient reported outcomes. Journal of Cancer 2017, 8, 395. [CrossRef]
- Jadhav, N.V.; Prasad, A.I.; Kumar, A.; Mishra, R.; Dhara, S.; Babu, K.; Prajapat, C.; Misra, N.; Ningthoujam, R.; Pandey, B. Synthesis of oleic acid functionalized Fe3O4 magnetic nanoparticles and studying their interaction with tumor cells for potential hyperthermia applications. Colloids Surf. B. Biointerfaces 2013, 108, 158-168. [CrossRef]
- Farhood, B.; Mortezaee, K.; Goradel, N.H.; Khanlarkhani, N.; Salehi, E.; Nashtaei, M.S.; Najafi, M.; Sahebkar, A. Curcumin as an anti-inflammatory agent: Implications to radiotherapy and chemotherapy. J. Cell. Physiol. 2019, 234, 5728-5740. [CrossRef]
- Hayakawa, S.; Ohishi, T.; Miyoshi, N.; Oishi, Y.; Nakamura, Y.; Isemura, M. Anti-cancer effects of green tea epigallocatchin-3-gallate and coffee chlorogenic acid. Molecules 2020, 25, 4553. [CrossRef]
- Kamel, K.M.; Khalil, I.A.; Rateb, M.E.; Elgendy, H.; Elhawary, S. Chitosan-coated cinnamon/oregano-loaded solid lipid nanoparticles to augment 5-fluorouracil cytotoxicity for colorectal cancer: extract standardization, nanoparticle optimization, and cytotoxicity evaluation. J. Agric. Food Chem. 2017, 65, 7966-7981. [CrossRef]
- Chimbetete, N.; Verghese, M.; Sunkara, R.; Walker, L.T. Phytochemical content, radical scavenging ability & enzyme inhibiting activities of selected spices (cinnamon, cardamom and cloves). Food and Nutrition Sciences 2019, 10, 266-275. [CrossRef]
- Han, B.; Huang, H.; Li, Z.; Gong, M.; Shi, W.; Zhu, C.; Gu, Z.; Zou, Z. Therapeutic effects of chinese medicine herb pair, huzhang and guizhi, on monosodium urate crystal-induced gouty arthritis in rats revealed by anti-inflammatory assessments and NMR-based metabonomics. Evidence-Based Complementary and Alternative Medicine 2016, 2016. [CrossRef]
- Baghel, U.; Nagar, A.; Pannu, M.; Singh, D.; Yadav, R. HPLC and HPTLC methods for simultaneous estimation of quercetin and curcumin in polyherbal formulation. Indian Journal of Pharmaceutical Sciences 2017, 79, 197-203. [CrossRef]
- Dallas, N.A.; Xia, L.; Fan, F.; Gray, M.J.; Gaur, P.; Van Buren, G.; Samuel, S.; Kim, M.P.; Lim, S.J.; Ellis, L.M. Chemoresistant colorectal cancer cells, the cancer stem cell phenotype, and increased sensitivity to insulin-like growth factor-I receptor inhibition. Cancer Res. 2009, 69, 1951-1957. [CrossRef]
- McDermott, M.; Eustace, A.; Busschots, S.; Breen, L.; Clynes, M.; O'Donovan, N.; Stordal, B. In vitro development of chemotherapy and targeted therapy drug-resistant cancer cell lines: a practical guide with case studies. Frontiers in oncology 2014, 4, 40. [CrossRef]
- Fan, Y.; Abulimiti, P.; Zhang, H.; Zhou, Y.; Zhu, L. Mechanism of reversal of multidrug resistance by curcumin in human colorectal cancer cell line HCT-8/5-FU. Gen. Mol. Res. 2017, 16.
- Toxicity–Up, A.O. OECD GUIDELINE FOR TESTING OF CHEMICALS. 2001.
- Nicol, B.; Prasad, S. The effects of cyclophosphamide alone and in combination with ascorbic acid against murine ascites Dalton's lymphoma. Indian J Pharmacol 2006, 38, 260. [CrossRef]
- Kleniewska, P.; Hoffmann, A.; Pniewska, E.; Pawliczak, R. The influence of probiotic Lactobacillus casei in combination with prebiotic inulin on the antioxidant capacity of human plasma. Oxidative medicine and cellular longevity 2016, 2016.
- Wen, J.J.; Garg, N.J. Manganese superoxide dismutase deficiency exacerbates the mitochondrial ROS production and oxidative damage in Chagas disease. PLoS neglected tropical diseases 2018, 12, e0006687. [CrossRef]
- Banchroft, J.; Stevens, A.; Turner, D. Theory and practice of histological techniques. 1996.
- Toyokuni, S.; Okamoto, K.; Yodoi, J.; Hiai, H. Persistent oxidative stress in cancer. FEBS Lett. 1995, 358, 1-3. [CrossRef]
- Zhong, J.-H.; Huang, D.-H.; Chen, Z.-Y. Prognostic role of systemic immune-inflammation index in solid tumors: a systematic review and meta-analysis. Oncotarget 2017, 8, 75381. [CrossRef]
- Frattaruolo, L.; Carullo, G.; Brindisi, M.; Mazzotta, S.; Bellissimo, L.; Rago, V.; Curcio, R.; Dolce, V.; Aiello, F.; Cappello, A.R. Antioxidant and anti-inflammatory activities of flavanones from Glycyrrhiza glabra L.(licorice) leaf phytocomplexes: Identification of licoflavanone as a modulator of NF-kB/MAPK pathway. Antioxidants 2019, 8, 186.
- Kamran, S.; Sinniah, A.; Alshawsh, M.A. Synergistic effects of 5-fluorouracil in combination with diosmetin in colorectal cancer cells. In Proceedings of the Presented at the 1st International Electronic Conference on Biomedicine, 2021; p. 26.
- Mawalizadeh, F.; Mohammadzadeh, G. Quercetin Potentiates the Chemosensitivity of Human Breast Cancer Cells to 5-Fluorouracil. 2021.
- Chen, S.; Zhang, Z.; Zhang, J. Emodin enhances antitumor effect of paclitaxel on human non-small-cell lung cancer cells in vitro and in vivo. Drug design, development and therapy 2019, 13, 1145. [CrossRef]
- Ko, G.; Kim, T.; Ko, E.; Park, D.; Lee, Y. Synergistic enhancement of paclitaxel-induced inhibition of cell growth by metformin in melanoma cells. Development & reproduction 2019, 23, 119. [CrossRef]
- Tang, H.; Zeng, L.; Wang, J.; Zhang, X.; Ruan, Q.; Wang, J.; Cui, S.; Yang, D. Reversal of 5-fluorouracil resistance by EGCG is mediate by inactivation of TFAP2A/VEGF signaling pathway and down-regulation of MDR-1 and P-gp expression in gastric cancer. Oncotarget 2017, 8, 82842. [CrossRef]
- Larkins, T.L.; Nowell, M.; Singh, S.; Sanford, G.L. Inhibition of cyclooxygenase-2 decreases breast cancer cell motility, invasion and matrix metalloproteinase expression. BMC Cancer 2006, 6, 1-12. [CrossRef]
- Lau, T.Y.; Leung, L.K. Soya isoflavones suppress phorbol 12-myristate 13-acetate-induced COX-2 expression in MCF-7 cells. Br. J. Nutr. 2006, 96, 169-176. [CrossRef]
- Huang, C.-Y.; Lee, C.-H.; Tu, C.-C.; Wu, C.-H.; Huang, M.-T.; Wei, P.-L.; Chang, Y.-J. Glucose-regulated protein 94 mediates progression and metastasis of esophageal squamous cell carcinoma via mitochondrial function and the NF-kB/COX-2/VEGF axis. Oncotarget 2018, 9, 9425.
- Tong, D.; Liu, Q.; Wang, L.-a.; Xie, Q.; Pang, J.; Huang, Y.; Wang, L.; Liu, G.; Zhang, D.; Lan, W. The roles of the COX2/PGE2/EP axis in therapeutic resistance. Cancer Metastasis Rev. 2018, 37, 355-368.
- Pauzas, H.; Gyvyte, U.; Latkauskas, T.; Kairevice, L.; Lizdenis, P.; Svagzdys, S.; Birgiolaite, E.; Kuliaviene, I.; Kupcinskas, J.; Tamelis, A. The Role of VEGFA, COX2, HUR and CUGBP2 in predicting the response to neoadjuvant therapy in rectal cancer patients. Medicina (Mex). 2020, 56, 192.
- Shimizu, K.; Okita, R.; Saisho, S.; Maeda, A.; Nojima, Y.; Nakata, M. Impact of COX2 inhibitor for regulation of PD-L1 expression in non-small cell lung cancer. Anticancer Res. 2018, 38, 4637-4644. [CrossRef]
- Qi, F.; Zhou, S.; Li, L.; Wei, L.; Shen, A.; Liu, L.; Wang, Y.; Peng, J. Pien Tze Huang inhibits the growth of hepatocellular carcinoma cells by upregulating miR-16 expression. Oncology letters 2017, 14, 8132-8137. [CrossRef]
- Peng, W.; Zhang, S.; Zhang, Z.; Xu, P.; Mao, D.; Huang, S.; Chen, B.; Zhang, C.; Zhang, S. Jianpi Jiedu decoction, a traditional Chinese medicine formula, inhibits tumorigenesis, metastasis, and angiogenesis through the mTOR/HIF-1α/VEGF pathway. J. Ethnopharmacol. 2018, 224, 140-148.
- Spranger, S.; Sivan, A.; Corrales, L.; Gajewski, T.F. Tumor and host factors controlling antitumor immunity and efficacy of cancer immunotherapy. Adv. Immunol. 2016, 130, 75-93.
- Wolchok, J.D.; Chiarion-Sileni, V.; Gonzalez, R.; Rutkowski, P.; Grob, J.-J.; Cowey, C.L.; Lao, C.D.; Wagstaff, J.; Schadendorf, D.; Ferrucci, P.F. Overall survival with combined nivolumab and ipilimumab in advanced melanoma. New Engl. J. Med. 2017, 377, 1345-1356. [CrossRef]
- Xu, L.; Zhang, Y.; Tian, K.; Chen, X.; Zhang, R.; Mu, X.; Wu, Y.; Wang, D.; Wang, S.; Liu, F. Apigenin suppresses PD-L1 expression in melanoma and host dendritic cells to elicit synergistic therapeutic effects. J. Exp. Clin. Cancer Res. 2018, 37, 1-15. [CrossRef]
- Rawangkan, A.; Iida, K.; Sakai, R.; Fujiki, H.; Suganuma, M. Green tea catechin, EGCG, enhances antitumor immunity by down-regulation of PD-L1 expression in non-small human lung cancer cell lines. 2017. [CrossRef]
- Duan, J.; Pan, L.; Yang, M. Preoperative elevated neutrophil-to-lymphocyte ratio (NLR) and derived NLR are associated with poor prognosis in patients with breast cancer: a meta-analysis. Medicine (Baltimore). 2018, 97.
Figure 1.
Quality and safety of SR033. A. NMR profiles of SR033 decoction were obtained from two different batches (Batch I and II) in powder form. B. Representational image of liver sections (N=6) of healthy control and SR033 treated group stained with Hematoxylin and Eosin (20X). NMR: nuclear magnetic resonance, SR033: oral herbal extract, CV: central vein, PV: portal vein, HP: hepatic portal.
Figure 1.
Quality and safety of SR033. A. NMR profiles of SR033 decoction were obtained from two different batches (Batch I and II) in powder form. B. Representational image of liver sections (N=6) of healthy control and SR033 treated group stained with Hematoxylin and Eosin (20X). NMR: nuclear magnetic resonance, SR033: oral herbal extract, CV: central vein, PV: portal vein, HP: hepatic portal.
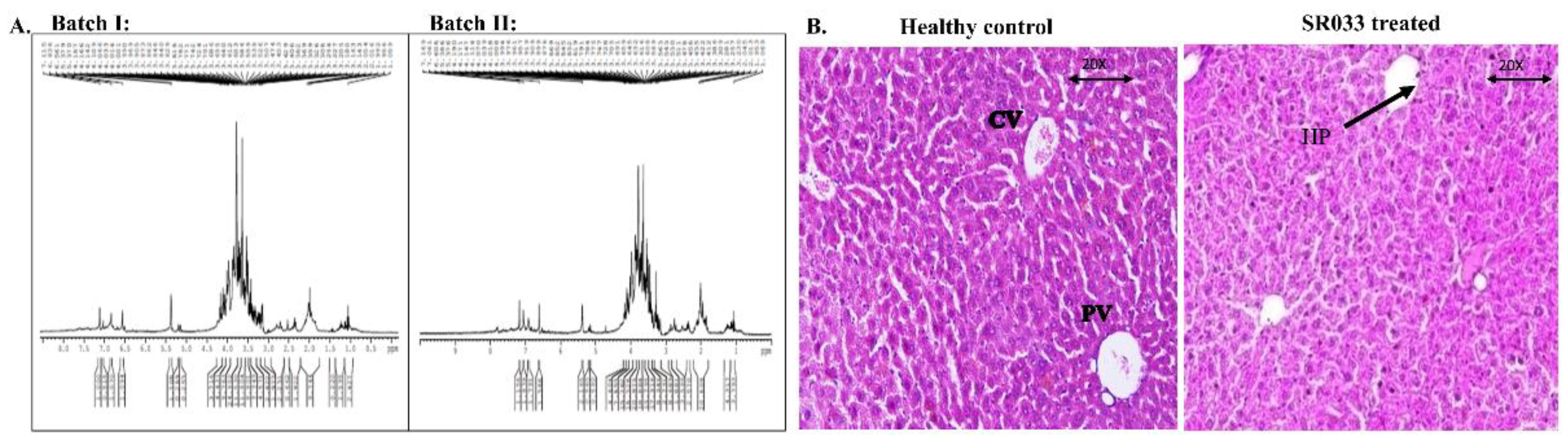
Figure 2.
Integrative and synergistic approach for cancer treatment using SR033, SR033L, and 5FU. A. Effect of SR033 with 5FU on percent free radicals, B, C, D. Representative graph and gel image showed 5FU induced COX-2, TGFβ, and VEGF at transcription level in MCF-7 and was inhibited by SR033 in a time-dependent manner. Mean±SD (N=3) was shown and *p<0.05 was considered significant. In-vivo studies showed E. SR033L in combination with LDF decreases tumor size (cm2) of survived mice similarly as with HDF, F. Kaplan-Meier curve suggested an improvement in survival percentage with SR033L, irrespective of the 5FU dose, G. WBC (103 /cumm) H. and RBC (mil /cumm) levels were also restored with SR033L/ LDF. Mean±SEM (N=6), ***P<0.001 in the groups treated with SR033L when compared with 5FU treated groups. SR033: an oral herbal formulation, SR033L: a topical herbal formulation, 5FU: 5-fluorouracil, COX-2: cyclo-oxygenase-2 mRNA, TGFβ: transforming growth factor β, VEGF: vascular endothelial growth factor, LDF: low dose of 5-fluorouracil, HDF: high dose of 5-fluorouracil, WBC: white blood cells, RBC: red blood cells.
Figure 2.
Integrative and synergistic approach for cancer treatment using SR033, SR033L, and 5FU. A. Effect of SR033 with 5FU on percent free radicals, B, C, D. Representative graph and gel image showed 5FU induced COX-2, TGFβ, and VEGF at transcription level in MCF-7 and was inhibited by SR033 in a time-dependent manner. Mean±SD (N=3) was shown and *p<0.05 was considered significant. In-vivo studies showed E. SR033L in combination with LDF decreases tumor size (cm2) of survived mice similarly as with HDF, F. Kaplan-Meier curve suggested an improvement in survival percentage with SR033L, irrespective of the 5FU dose, G. WBC (103 /cumm) H. and RBC (mil /cumm) levels were also restored with SR033L/ LDF. Mean±SEM (N=6), ***P<0.001 in the groups treated with SR033L when compared with 5FU treated groups. SR033: an oral herbal formulation, SR033L: a topical herbal formulation, 5FU: 5-fluorouracil, COX-2: cyclo-oxygenase-2 mRNA, TGFβ: transforming growth factor β, VEGF: vascular endothelial growth factor, LDF: low dose of 5-fluorouracil, HDF: high dose of 5-fluorouracil, WBC: white blood cells, RBC: red blood cells.
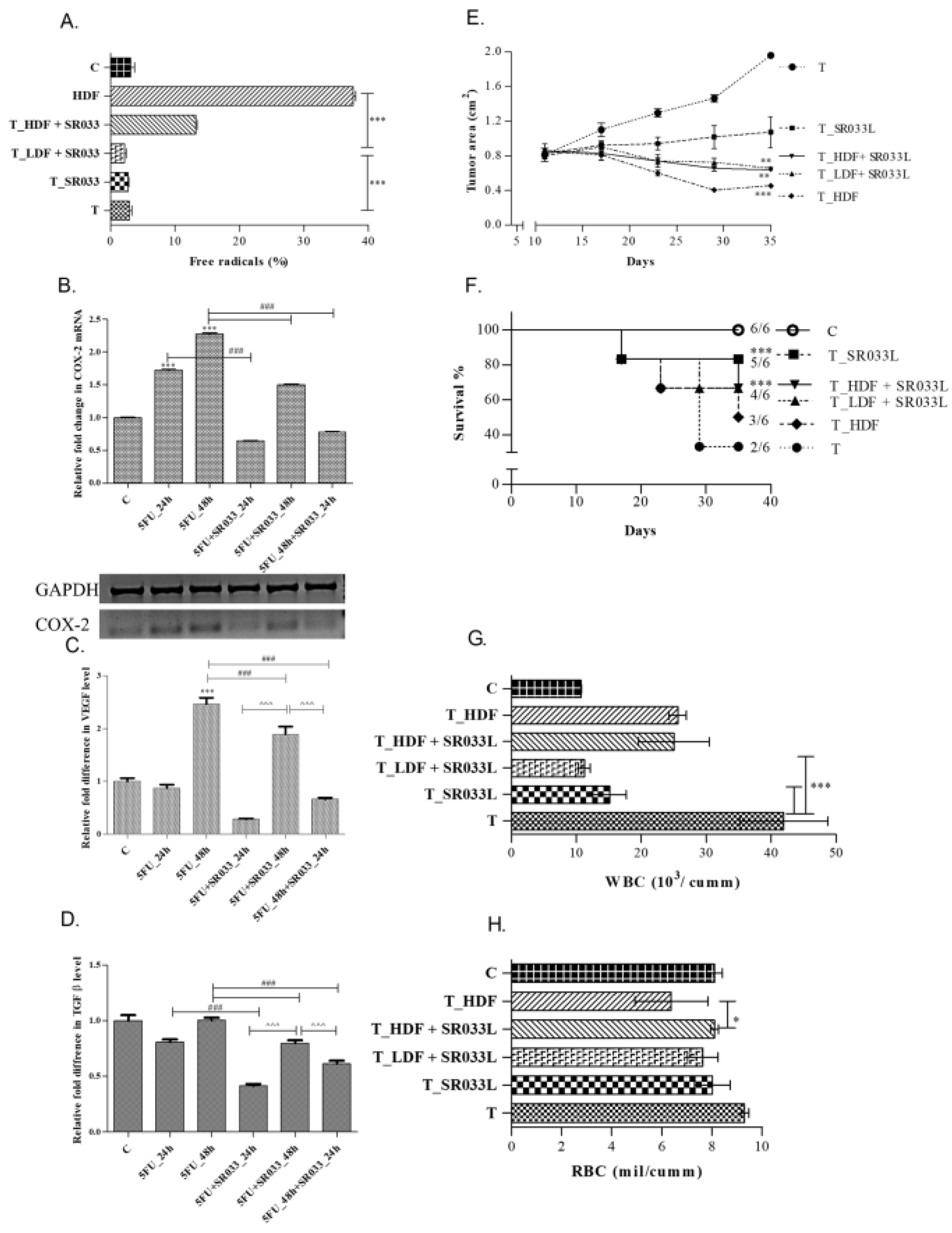
Figure 3.
Synergy of SR033/5FU and SR033/PTX. Left panel: A. Hematoxylin and Eosin-stained tumor biopsy of T (untreated) and SR033L treated tumor-bearing mice (N=6/ group), where dark stained dot-like structures are viable tumor cells (as shown by the yellow arrow at left) and the accumulation of mixed lymphocytic cells in the SR033 treated group (as indicated by white arrows at right) (20X). Right panel: 5FU-resistant HeLa-R and MCF-7-R showed cross-resistance to PTX, which were chemo-sensitized by SR033 with a synergistic effect. MTT assay was performed on HeLa-R using SR033 at its EC50 from HeLa in combination with lower concentrations of B. 5FU and C. PTX and similarly performed on MCF-7-R integrating various low concentrations of D. 5FU and E. PTX. The data represents mean±SD (N=3) and ***p<0.001. 5FU: 5-fluorouracil, PTX: paclitaxel, T: untreated tumor, SR033L: topical application of herbal formulation, SR033: an oral herbal formulation, HeLa-R and MCF-R: 5-fluorouracil resistant HeLa and MCF-7 cells.
Figure 3.
Synergy of SR033/5FU and SR033/PTX. Left panel: A. Hematoxylin and Eosin-stained tumor biopsy of T (untreated) and SR033L treated tumor-bearing mice (N=6/ group), where dark stained dot-like structures are viable tumor cells (as shown by the yellow arrow at left) and the accumulation of mixed lymphocytic cells in the SR033 treated group (as indicated by white arrows at right) (20X). Right panel: 5FU-resistant HeLa-R and MCF-7-R showed cross-resistance to PTX, which were chemo-sensitized by SR033 with a synergistic effect. MTT assay was performed on HeLa-R using SR033 at its EC50 from HeLa in combination with lower concentrations of B. 5FU and C. PTX and similarly performed on MCF-7-R integrating various low concentrations of D. 5FU and E. PTX. The data represents mean±SD (N=3) and ***p<0.001. 5FU: 5-fluorouracil, PTX: paclitaxel, T: untreated tumor, SR033L: topical application of herbal formulation, SR033: an oral herbal formulation, HeLa-R and MCF-R: 5-fluorouracil resistant HeLa and MCF-7 cells.
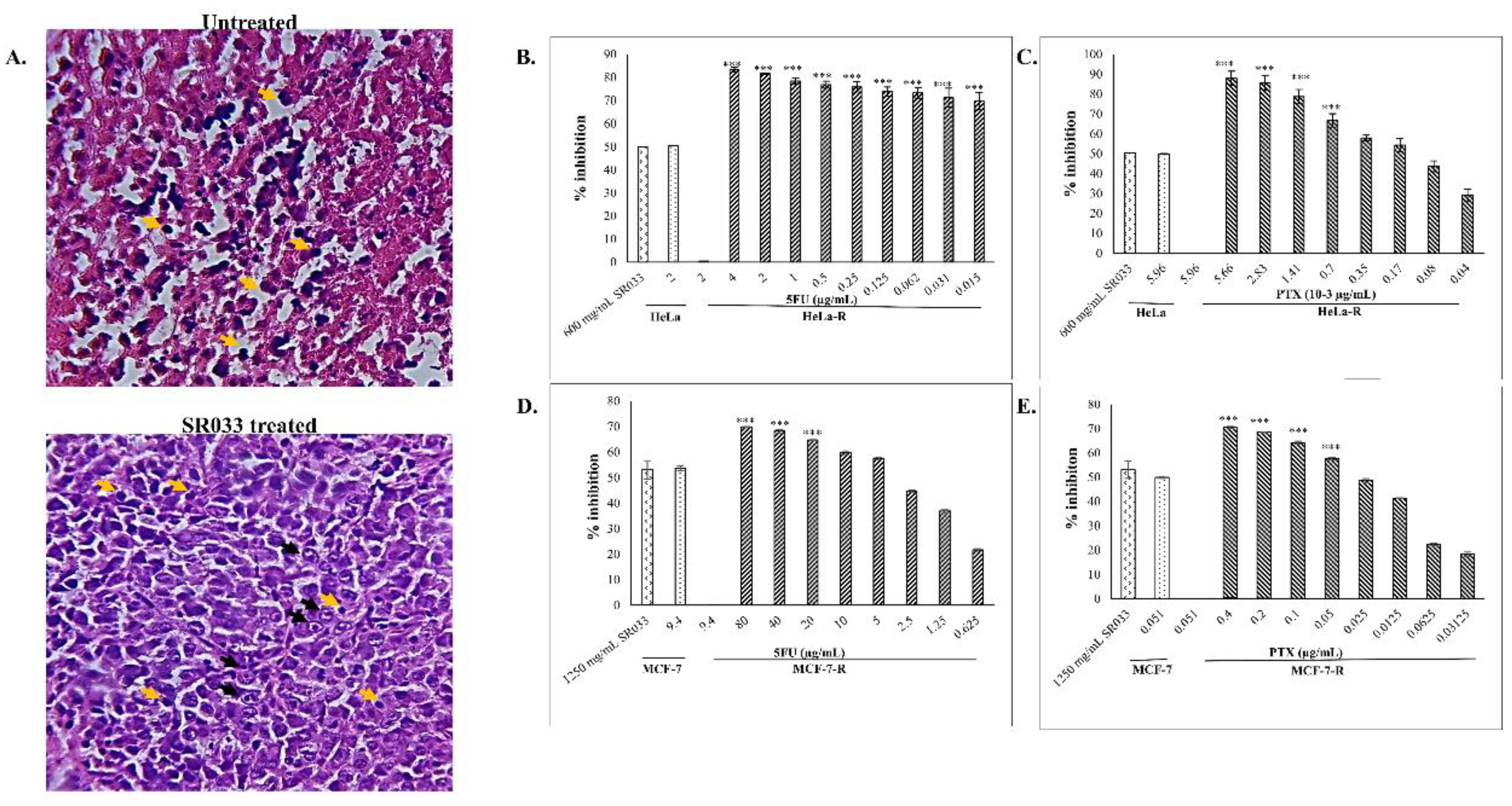
Figure 4.
Restoration of immune status by SR033. A. Neutrophil and Lymphocyte ratio (NLR) in EAC-bearing mice were restored by SR033L alone and with LDF (N=6; mean±SEM). B. Representation of graph and gel showing inhibition of IFNγ induced PD-L1 transcription by SR033 in MCF-7 (N=3; mean±SD). The data represents significance (P<0.001) was depicted as ‘###’ and ‘***’. IFN γ: interferon γ, SR033L: a topical herbal formulation, LDF: low dose of 5-fluorouracil, PD-L1: programmed death-ligand 1 mRNA, SR033: an oral herbal formulation.
Figure 4.
Restoration of immune status by SR033. A. Neutrophil and Lymphocyte ratio (NLR) in EAC-bearing mice were restored by SR033L alone and with LDF (N=6; mean±SEM). B. Representation of graph and gel showing inhibition of IFNγ induced PD-L1 transcription by SR033 in MCF-7 (N=3; mean±SD). The data represents significance (P<0.001) was depicted as ‘###’ and ‘***’. IFN γ: interferon γ, SR033L: a topical herbal formulation, LDF: low dose of 5-fluorouracil, PD-L1: programmed death-ligand 1 mRNA, SR033: an oral herbal formulation.
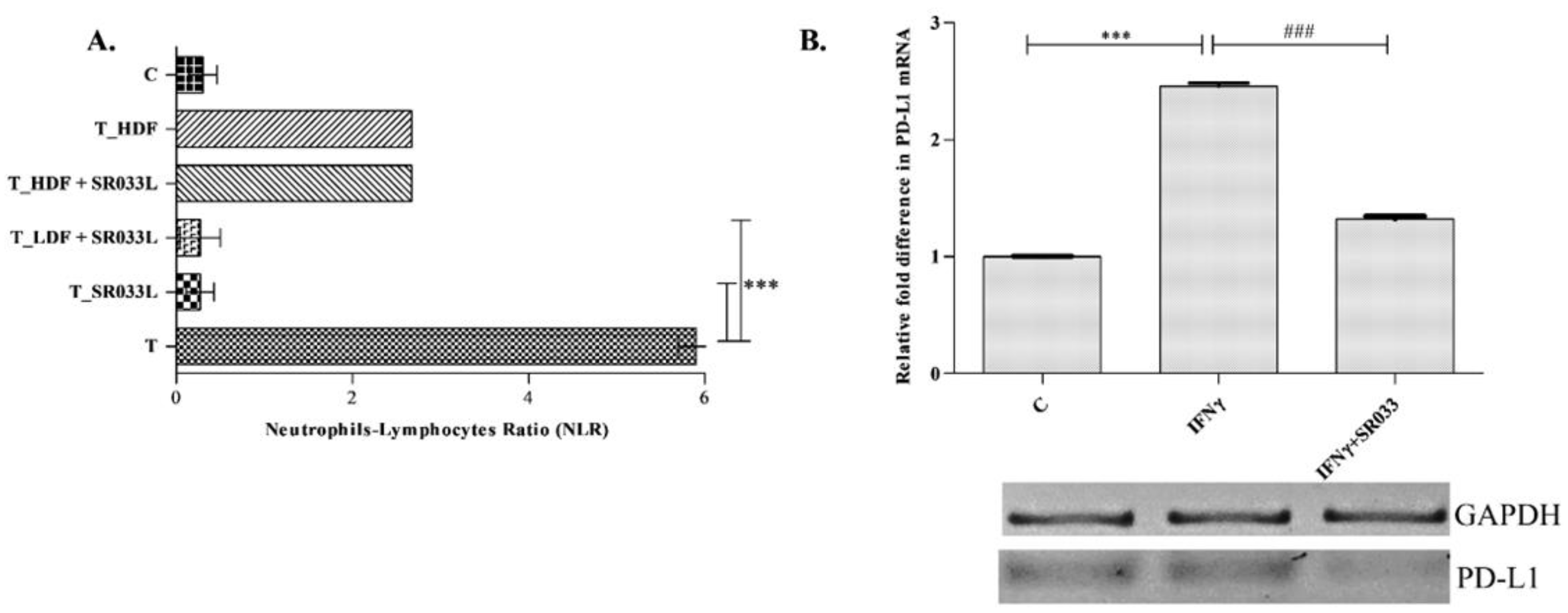
Figure 5.
Illustration of mechanistic action of SR033. Reactive oxygen species (ROS) induces inflammation which furthermore activates nuclear factor-kappa β (NFĸβ). Cyclo-oxygenase-2 (COX-2) is produced as a result of a feedback loop formed by prostaglandin (PGE2) production from arachidonic acid (AA) via the NFĸβ pathway. PGE2 also activates β-catenin pathway which further produces COX-2, vascular endothelial growth factor (VEGF), and is responsible for drug resistance in cancer. NFĸβ pathway also activates transforming growth factor β (TGFβ) gene which in turn induces β-catenin pathway, COX-2, and VEGF. T cells produce interferon γ (IFNγ) which induces programmed death ligand-1 (PD-L1) gene via JAK-STAT pathway in cancer cells, which leads to T cell exhaustion and tumor bypass from immune surveillance due to the expression of programmed death 1 receptor (PD-1R) on T cells. These molecules are highly responsible for epithelial to mesenchymal transition (EMT) of tumor cells and its invasion in other areas through angiogenesis. SR033 proved to inhibit (red arrows) ROS-induced inflammation, thereby inhibiting COX-2 mRNA, VEGF, and TGFβ accumulation and reversing drug resistance. Inhibition of PD-L1 mRNA by SR033 could restore immune status. SR033: novel herbal formula, DNA: deoxyribonucleic acid.
Figure 5.
Illustration of mechanistic action of SR033. Reactive oxygen species (ROS) induces inflammation which furthermore activates nuclear factor-kappa β (NFĸβ). Cyclo-oxygenase-2 (COX-2) is produced as a result of a feedback loop formed by prostaglandin (PGE2) production from arachidonic acid (AA) via the NFĸβ pathway. PGE2 also activates β-catenin pathway which further produces COX-2, vascular endothelial growth factor (VEGF), and is responsible for drug resistance in cancer. NFĸβ pathway also activates transforming growth factor β (TGFβ) gene which in turn induces β-catenin pathway, COX-2, and VEGF. T cells produce interferon γ (IFNγ) which induces programmed death ligand-1 (PD-L1) gene via JAK-STAT pathway in cancer cells, which leads to T cell exhaustion and tumor bypass from immune surveillance due to the expression of programmed death 1 receptor (PD-1R) on T cells. These molecules are highly responsible for epithelial to mesenchymal transition (EMT) of tumor cells and its invasion in other areas through angiogenesis. SR033 proved to inhibit (red arrows) ROS-induced inflammation, thereby inhibiting COX-2 mRNA, VEGF, and TGFβ accumulation and reversing drug resistance. Inhibition of PD-L1 mRNA by SR033 could restore immune status. SR033: novel herbal formula, DNA: deoxyribonucleic acid.
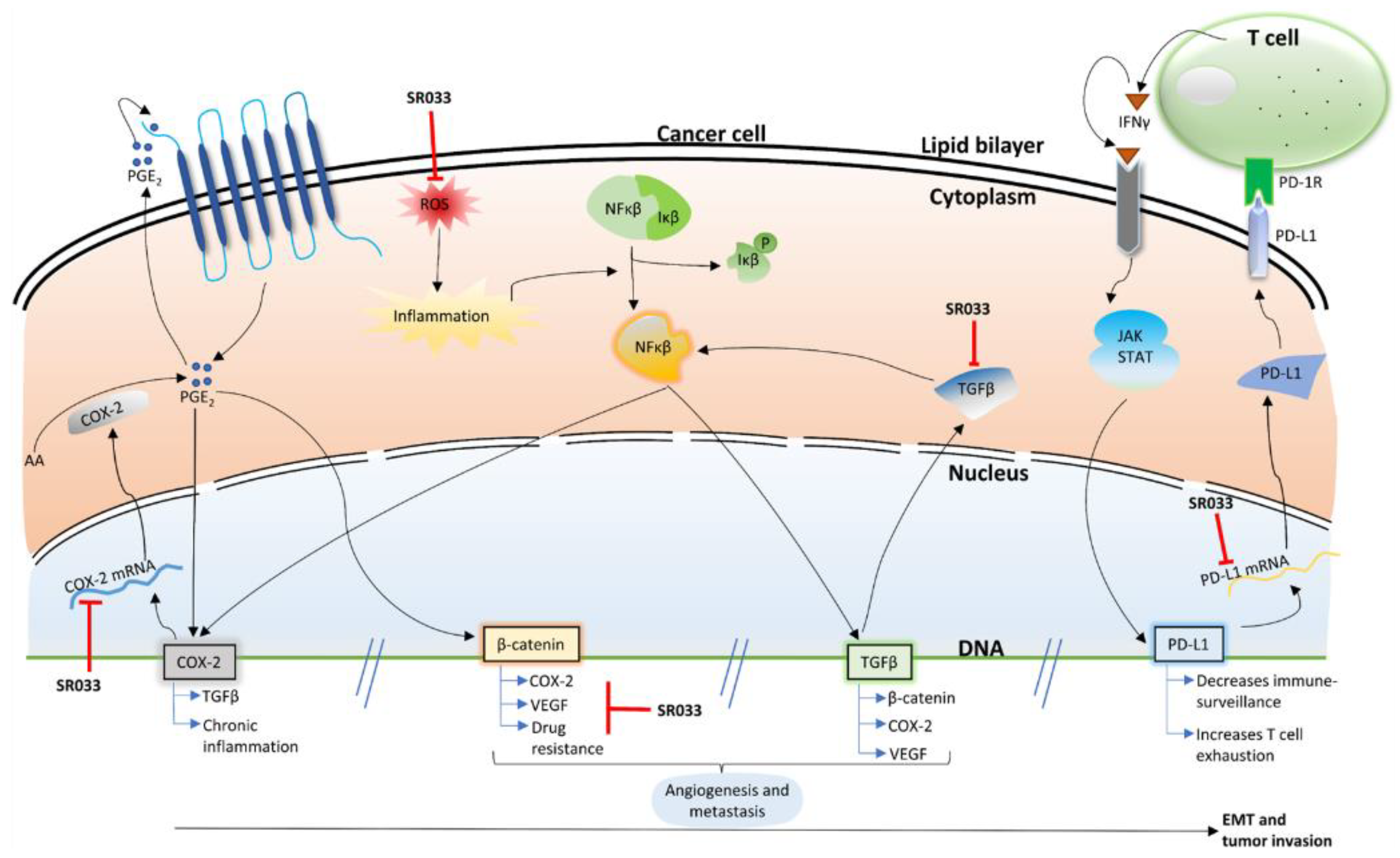
Figure 6.
Schematic representation of the work plan in-vivo experiments. Ehlich Ascites cells were injected in tumor models to determine the effect of A. oral administration of SR033 decoction (prophylactic and therapeutic) and B. topical application of SR033L.
Figure 6.
Schematic representation of the work plan in-vivo experiments. Ehlich Ascites cells were injected in tumor models to determine the effect of A. oral administration of SR033 decoction (prophylactic and therapeutic) and B. topical application of SR033L.
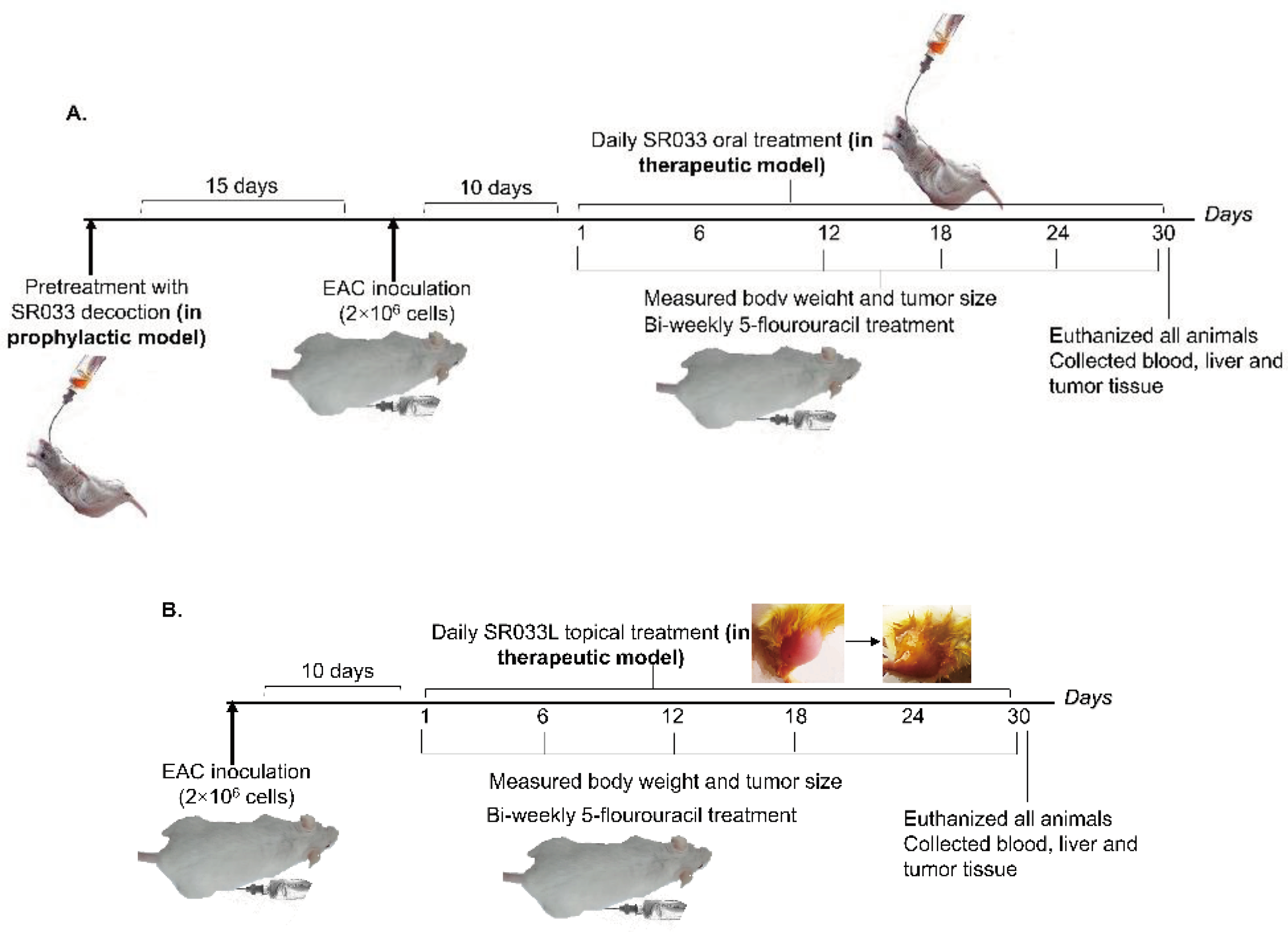

Table 1.
The table depicts tumor size (cm)/ tumor volume (mL), mean survival time, WBC, and RBC in tumor-bearing mice models at breast (solid tumor) and peritoneum (non-solid tumor) sites. The tumor was prevented (prophylactic) and treated (therapeutic) with SR033. Values are expressed as mean ± SEM, N=6, *** signifies p<0.001 w.r.t. T group and ### signifies p<0.001 w.r.t. healthy group.
Table 1.
The table depicts tumor size (cm)/ tumor volume (mL), mean survival time, WBC, and RBC in tumor-bearing mice models at breast (solid tumor) and peritoneum (non-solid tumor) sites. The tumor was prevented (prophylactic) and treated (therapeutic) with SR033. Values are expressed as mean ± SEM, N=6, *** signifies p<0.001 w.r.t. T group and ### signifies p<0.001 w.r.t. healthy group.
| Groups | Breast site | Peritoneum site (Ascites) | |||
|---|---|---|---|---|---|
| Prophylactic | Therapeutic | Prophylactic | Therapeutic | ||
| Tumor size (cm)/ volume (mL) | T1 | 1.69 ± 0.03### | 2.42 ± 0.09### | 18.12 ± 0.09### | 17.50 ± 0.11### |
| T_LDS2 | 1.21 ± 0.02*** | 1.75 ± 0.05*** | 16.18 ± 0.22*** | 13.96 ± 0.34*** | |
| T_HDS3 | 0.75 ± 0.01*** | 1.02 ± 0.05*** | 11.68 ± 0.07*** | 09.89 ± 0.09*** | |
| T_HDF4 | - | 0.78 ± 0.03*** | - | 7.71 ± 0.20*** | |
| Packed cell volume (mL) | T | - | - | 11.95 ± 0.12### | 11.46 ± 0.26### |
| T_LDS | - | - | 07.98 ± 0.09*** | 08.03 ± 0.14*** | |
| T_HDS | - | - | 05.22 ± 0.33*** | 05.06 ± 0.19*** | |
| T_HDF | - | - | - | 04.65 ± 0.11*** | |
| Mean survival time | T | 15.83±0.30### | 17.66±0.21### | ||
| T_LDS | 20 ±0.44*** | 22.83 ±0.30*** | |||
| T_HDS | 23.16±0.30*** | 26.16±0.30*** | |||
| T_HDF | - | 20.66±0.21*** | |||
| WBC (103 cells/mL) | Healthy | 9.69 ± 0.13 | 9.32 ± 0.06 | 9.59 ± 0.18 | 9.32 ± 0.06 |
| T | 19.56 ± 0.26### | 21.21 ± 0.24### | 20.41± 0.41### | 21.34 ± 0.47### | |
| T_LDS | 17.75 ± 0.11*** | 16.61 ± 0.24*** | 18.87 ± 0.21*** | 19.07 ± 0.14*** | |
| T_HDS | 15.44 ± 0.12*** | 14.34 ± 0.18*** | 16.27 ± 0.21*** | 15.97 ± 0.15*** | |
| T_HDF | - | 18.26 ± 0.27*** | - | 18.20 ± 0.16*** | |
| RBC (106 cells/mL) | Healthy | 10.67 ± 0.11 | 10.51 ± 0.20 | 10.46 ± 0.22 | 10.51 ± 0.20 |
| T | 4.11 ± 0.16### | 3.94 ± 0.21### | 4.01 ± 0.12### | 3.84 ± 0.06### | |
| T_LDS | 5.23 ± 0.11*** | 5.44 ± 0.16*** | 4.40 ± 0.18*** | 5.32 ± 0.08*** | |
| T_HDS | 6.34 ± 0.20*** | 6.95 ± 0.08*** | 5.98 ± 0.09*** | 7.08 ± 0.31*** | |
| T_HDF | - | 5.83 ± 0.08*** | - | 5.45 ± 0.12*** | |
1Tumor-bearing mice; 2Tumor-bearing mice treated with low dose SR033; 3Tumor-bearing mice treated with high dose SR033; 4Tumor-bearing mice treated with high dose 5-Fluorouracil.
Table 2.
Report of number of survivors, percentage of viable tumor, necrotic, apoptotic, and immune cells in the tumor biopsy of EAC induced tumor model in response to SR033L with and without 5-FU as compared with tumor.
Table 2.
Report of number of survivors, percentage of viable tumor, necrotic, apoptotic, and immune cells in the tumor biopsy of EAC induced tumor model in response to SR033L with and without 5-FU as compared with tumor.
| Groups | No. of living animals (out of 6) | Viable tumor cells (%) | Necrotic cells (%) | Apoptotic cells (%) | Remarks |
|---|---|---|---|---|---|
| T1 | 2 | 20-25% | 75-80% | 25-30% | Mild TILS2 |
| T_SR033L3 | 5 | 0-30% | 70-100% | - | No TILS, presence of Foamy cells. The tumor was replaced by mixed inflammation on the surface |
| T_SR033L + LDF4 | 4 | 20-30% | 30-50% | 10-30% | Presence of mixed inflammation around the tumor |
| T_SR033L + HDF5 | 4 | 10-25% | 80-90% | 20-35% | No TILS, presence of Foamy cells at margin, one lobe was replaced by inflammation |
| T_HDF6 | 3 | 10-20% | 90-100% | 20-30% | No inflammation or Foamy cells present |
1Tumor bearing mice; 2Tumor infiltrating lymphocytes; 3Tumor-bearing mice treated with SR033L; 4Tumor-bearing mice treated with SR033L and low dose of 5-Fluorouracil; 5Tumor-bearing mice treated with SR033L and high dose of 5-Fluorouracil; 6Tumor-bearing mice treated with high dose of 5-Fluorouracil.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



