Submitted:
13 March 2024
Posted:
14 March 2024
You are already at the latest version
Abstract
Vertical and horizontal bone augmentation is one of the most challenging techniques in bone engineering. The use of barrier membranes and scaffolds in guided bone regeneration (GBR) procedures is a common approach for the treatment of lost bone around teeth and dental implants. The aim of this study was to estimate the barrier effects of a synthetic poly (lactic acid/caprolactone) [P(PA/CL)] bilayer membrane for GBR, compared to a porcine collagen bilayer membrane, in the vertical augmentation model on 10–12-months old rat skull without periosteum. The HAp block (diameter: 4 mm, height: 3 mm, porosity:75%, average pore size:150 μm) was placed on the rat skull without a periosteum. The P(LA/CL) membrane (solid layer: 25 μm, porous layer: 175 μm) or the collagen membrane (solid layer, porous layer) was applied onto the HAp block. At 3, 6, and 12 weeks after the surgery, the incised tissues were fixed, decalcified, and stained with hematoxylin and eosin for histological evaluation. The P(LA/CL) membrane remained until 12 weeks and could achieve barrier effects to inhibit cellular invasion from the repositioned soft tissues. Local bone formation occurred in the interconnected pores of HAp at 6 weeks. On the other hand, the collagen membrane did not inhibit cellular invasion for its expansion until 3 weeks, and was absorbed until 6 weeks. The results indicated that the P(LA/CL) membrane might be effective in GBR as occlusive absorbable membrane.
Keywords:
guided bone regeneration (GBR)
; bone augmentation
; absorbable
; membrane
; collagen
; hydroxyapatite
; poly (lactic acid /caprolactone)
; biomimetics
1. Introduction
Regenerative medicine has been mainly based on biomaterials science. The first clinical case of guided tissue regeneration (GTR) using a barrier membrane was reported in 1982 [1]. The barrier membrane alone for GTR resulted in the membrane compression into the bone defect space by overlying soft tissues. By developing biomaterials science, guided bone regeneration (GBR) technique using the cell-barrier membrane with scaffolds have become a main therapy for bone defects around tooth and/or implant fixture. GBR therapy (barrier membranes with bone graft materials) was shown to produce greater clinical improvements than GTR (barrier membrane alone). Bone tissue regenerates at a rate slower than soft tissues. The main problems in GBR procedure are to control absorption rate of the barrier membrane and block contaminant into the defect space of the graft materials. To overcome the problems, barrier membranes have been developed to control the absorption rate, stabilize bone graft materials, and to serve as a separating barrier between osteogenic space and soft tissues with epithelium in GBR therapy. The first successful use of absorbable membranes for GBR was reported in the early 1990s, and both natural and synthetic polymers have been used extensively with collagen and aliphatic polyesters being the mostly investigated [2]. These membranes are usually used in combination with autogenous bone or synthetic graft materials, with or without screws and pins, because they mostly are incapable of maintaining defect space due to their lack of rigidity. It is required for the barrier membranes to be biocompatible and not evoke any immune reactions or cytotoxicity in host. Ideally, the biodegradation rate of the membranes should match the rate of new tissue formation without residual materials. Also, the mechanical properties of these membranes should be sufficiently high to withstand their placement and use in vivo [2].
Membranes are a key factor to the GBR procedure, being able to function as a barrier against fibroblasts for osteogenic environments. The cell-barrier membranes are divided into absorbable and non-absorbable [2,3,4,5,6]. The non-absorbable membranes require a second surgical procedure for the removal. Therefore, absorbable membranes are recently needed in the field of local bone regeneration for one-staged surgery and avoiding additional morbidity such as a second surgery increasing patient’s pain and costs. Among the absorbable membranes, collagen-based materials have been used widely [7,8,9]. Although animal-derived collagen materials are biocompatible medical devices, it is difficult to control the elasticity and the absorption rate of the collagen-based materials. The enzymatic activity such as matrix metalloproteinases (MMPs) causes the collagen membrane to rapidly digest and decreases the cell-barrier function. Therefore, a novel polymer membrane composed of poly (lactic acid) (PLA) and poly (caprolactone) (PCL) has been developed to act as a cell-barrier membrane during bone formation for GBR (not GTR) in Japan [10], and the bio-absorbable GBR membrane is a poly (lactic acid /caprolactone) [P(LA/CL)] bilayer membrane without animal products [10,11]. The degradation rate of the P(LA/CL) bilayer membrane was 40% and 55% in weight at 12 and 26 weeks, respectively [10].
Already, safety and feasibility of the P(LA/CL) membrane with carbonate apatite granules and autogenous bone was clinically assessed for GBR in bone defects surrounding dental implants in human pilot study [12,13]. In brief, 5 patients for GBR were included in the first-in-human study. The P(LA/CL) membrane was applied simultaneously with dental implant placement to achieve horizontal bone augmentation by GBR procedure. The results of the pilot study demonstrated that the use of the P(LA/CL) membrane for GBR did not cause any irreversible adverse events and showed sufficient performance to regenerate bone as a GBR membrane, although the subjects were limited to only 5 patients [12]. Next, a total of 25 sites from 20 patients were included in the clinical GBR study. The patients required GBR procedure simultaneously or before dental implant placement in edentulous regions. The clinical results indicated that the P(LA/CL) membrane with carbonate apatite granules achieved reasonable bone regeneration for implant placements [13]. However, the fate and behavior of the P(LA/CL) membrane in the applied sites were not mentioned in the clinical papers [12,13].
GBR is the popular technique for horizontal and/or vertical bone augmentation in implant dentistry [14,15]. The vertical augmentation is especially one of the most challenging techniques in bone engineering. Although there have been many animal studies related with GBR, almost all studies have used the GTR membranes in bone defect (inlay) models with periosteum in young-adult rats [16,17]. Briefly, the model was bone defect (diameter: 8 mm) in skull of 15 weeks old rats [16], and the other was same bone defect model of 12 weeks old rats [17]. In addition, the elevated periosteum was repositioned on the GBR membranes in both rat models. In fact, alveolar bone loss in human is accompanied with the periosteal disappearance. Moreover, almost patients related with bone loss by periodontal disease or implant rehabilitation are in the adult-senior stage, not young. In the present study, therefore, aged rats in the adult-senior stage were used, and we focused on the barrier effects of the P(LA/CL) membrane against non-osteogenic soft tissues without periosteum as clinically biomimetic model.
The aim of this study was to estimate the barrier effects of a novel P(LA/CL) bilayer membrane for GBR, compared to a porcine collagen bilayer membrane, histologically in the vertical (onlay) model on skull without a periosteum of 10-12 months old rats.
2. Materials and Methods
2.1. Biomaterials
Absorbable bilayer membranes and non-absorbable synthetic hydroxyapatite (HAp) block were used in this study. The HAp block (diameter: 4 mm, height: 3 mm, porosity: 75%, average pore size: 150 μm) (NEOBONE®, CoorsTek GK, Japan) was placed on the rat skull without a periosteum. As an experimental group, a poly (lactic acid /caprolactone: P(LA/CL)) bilayer membrane (Cytrans®Elashield, GC Corp, Tokyo, Japan) (Figure 1) was applied onto the HAp block for GBR. The synthetic P(LA/CL) membrane consists of a bilayer structure (totally 200 μm in thickness) with solid (25 μm) and porous (175 μm) layers, and has elasticity [9,10]. As a control group, a collagen bilayer membrane (Bio-Guide®, Gaistrich Pharma, Wolhusen, Switzerland) was used onto the HAp block. The non-cross-linked collagen membrane derived from porcine dermis exhibited a dense structure in the upper layer and a porous structure in the lower layer, while the thickness of the membrane was not published [17,18]. Both membranes were cut into a round shape (diameter: 8 mm) by a sterilized biopsy punch (diameter: 8 mm, Kai medical, Japan) before use.
2.2. Animal Experiment
Twenty-seven Wistar rats (10-12 months old, female, weight range: 280-320 g) were used to evaluate in vivo effects of each barrier membrane onto the HAp block. Normal histological structure of head in the retired Wistar rat was shown in Figure 2. The animal experiment was examined by the Institutional Animal Care and Use Committee of the Health Sciences University of Hokkaido (approval number: 21-047).
2.3. Surgical Procedures
The rats were divided randomly into two groups, as follows: the control group, the collagen membrane onto the HAp block on the exposed parietal bone without periosteum (n=15); the experimental group, the p(LA/CL) membrane onto the HAp block (n=12). Wistar rats were subjected to intraperitoneal anesthesia with pentobarbital sodium (4 mg/100 g body weight). Surgical operations were performed under the general anesthesia, the head hairs were shaved and an incision allowing reflection of a full-thickness flap was made in the scalp in the sagittal plane (Figure 3a). The head skin was elevated with galea, and the periosteum was removed from the outer cortical plate of parietal bone (Figure 3b). The HAp block was implanted on the exposed skull without a periosteum (Figure 3c). Each membrane was placed onto the HAp block (Figure 3d,e) without fixation of the membrane by tack pins. The skull skin was sutured with 4/0 polyglactin absorbable sutures. Chloromycetin ointment were used after the sutures (Figure 3f). All surgical procedures were performed by the same surgeon. All rats were fed with a standard diet during the experimental period.
2.4. Histological Examination
At 3, 6, and 12 weeks after the surgery, the rats were sacrificed (4 rats as the control group and 5 rats as the experiment group at each time point) by cervical dislocation under an anesthetic overdose (ketamine at a dose 2–3-fold higher than the anesthetic dosage). After the incision of head skin, a surgical drill attached to an electrical hand motor piece was used to harvest the skull bone with both the implanted materials and the head skin.
The incised tissues were immersed in 20% neutral phosphate-buffered formalin solution, additional immersion by microwave treatment, and then fixed in 20% neutral phosphate-buffered formalin solution for 1 week. The fixed tissues were decalcified in 10% formic acid for 4 weeks, and rinsed overnight with running water. All the samples were dehydrated using ethanol (50%–100%) and processed for paraffin embedding (Vacuum Rotary, VRX-23, Mitsubishi, Tokyo, Japan). Later, histological sections (5 µm thickness) were prepared by a microtome (Yamato Rom 380, Tokyo, Japan) and stained with hematoxylin and eosin (HE) (Wako, Osaka, Japan). The HE-stained sections were examined by using an optical microscopy (Nikon Eclipse 80i, Nikon, Tokyo, Japan) for histological evaluation.
3. Results
3.1. Histological Findings in P(LA/CL) /HAp on Skull without Periosteum
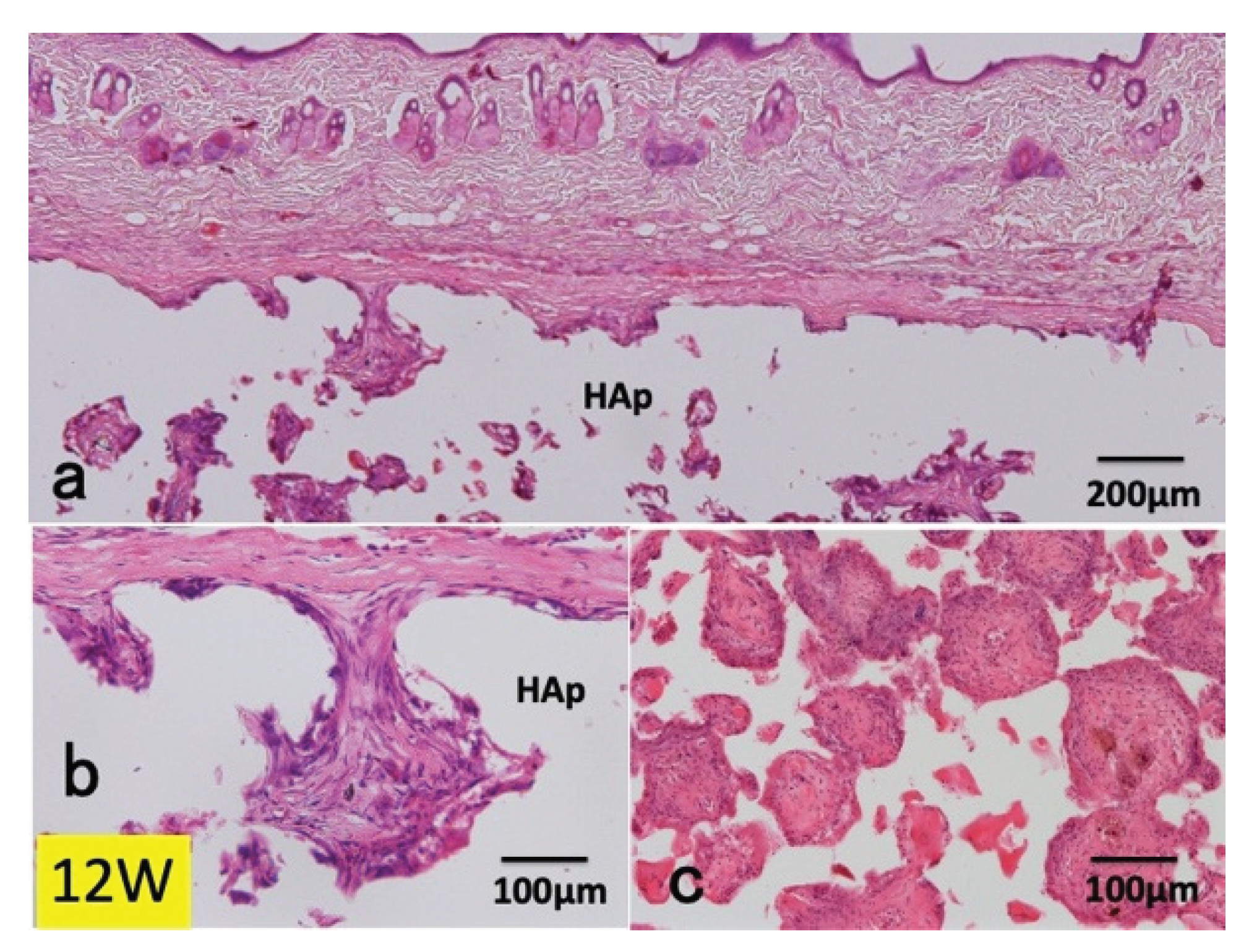
At 3 weeks after the surgery, loose fibrous connective tissues were seen on the P(LA/CL) membrane, which was recognized as a white bundle of clear space in HE. Capillaries including red blood cells and body fluid were observed in the upper pores of HAp (Figure 4). At 6 weeks, P(LA/CL) was clearly seen as a white bundle of clear space, and new bone formation was found locally in the pores nearby the outer cortical bone (Figure 5, 6c). The P(LA/CL)/HAp was totally encapsulated by fibrous connective tissues (Figure 5). Undifferentiated mesenchymal cells and blood cells in immature tissues were observed in the pores (Figure 6a, 6b). In the middle area of HAp, apart from the surface of skull, new bone and immature tissues with undifferentiated mesenchymal cells and red blood cells were found in the pores (Figure 6c, 6d). At 12 weeks, the P(LA/CL)/HAp was encapsulated by fibrous connective tissues (Figure 7: left). P(LA/CL) was clearly seen as a clear space and fibrous connective tissues were formed on P(LA/CL) (Figure 7a). Bone formation occurred in the interconnected pores (Figure 7b). Bony bridge was found between original bone and new bone in the lower pores. Undifferentiated mesenchymal cells, red blood cells and tissue fluid were observed in the middle pores of HAp (Figure 7c). Immature tissues including mesenchymal cells, red blood cells and tissue fluid were found in the middle pores (Figure 7c, 7d). Wound rupture did not occur during 12 weeks.
3.2. Histological Findings in Collagen /HAp on Skull without Periosteum
At 3 weeks after the surgery, the collagen membrane was remarkably expanded except the upper corners of the HAp block (Figure 8a). The fibers of the collagen membrane were stained strongly by eosin, and the collagen membrane on the corners of HAp was extremely thin in thickness (Figure 8a). Strongly eosin-stained collagen fibers were distinguished from pinkish fibers of the original connective tissues. Hematoxyline-stained white blood cells infiltrated into the upper layer of the expanded membrane (Figure 8b). Wavy collagen fibers of the membrane were seen in the top pores of HAp (Figure 8c). At 6 weeks, the collagen membrane disappeared, and fibrous connective tissues were formed in the upper pores (Figure 9). Strongly eosin-stained collagen fibers were not found. At 12 weeks, residues of the collagen membrane were not seen (Figure 10a). Fibrous connective tissues occupied in the upper pores of the HAp block (Figure 10b). Bone formation did not occur, while dense connective tissues were observed in the pores of the middle area of HAp (Figure 10). Wound rupture did not occur during 12 weeks.
4. Discussion
The synthetic P(LA/CL) bilayer membrane, an absorbable and polymeric material, had a better performance in the barrier effects against soft tissues than the porcine skin-derived collagen bilayer membrane. The P(LA/CL) membrane remained until 12 weeks later, while the collagen membrane was totally expanded at 3 weeks and almost absorbed until 6 weeks in this onlay model. The in vivo appearance of the P(LA/CL) membrane at 12 weeks was compatible to the in vitro results indicating 40% degradation rate of the membrane in the dissolution test for 12 weeks in phosphate-buffered saline [10].
4.1. Animal Model
Generally, adult-senior stage patients lose teeth and periosteum with alveolar bone, mainly due to periodontal diseases, and require vertical and/or horizontal bone augmentation for oral rehabilitation. Until now, almost all in vivo studies were done in bone defect (inlay) models with periosteum in young-adult rats [16,17]. Vertical or horizontal augmentation model is not dynamic more than bone defect (inlay) model consisting of 3-4 bony walls. The supply of mesenchymal stem cells and blood was much better in bone defect models than in augmentation models on cortical bone. In this study, therefore, the application of the barrier membranes was used as vertical bone augmentation (onlay) model without periosteum of 10–12-months old rats (adult-senior stage) for GBR. We believe that the present model is biologically similar and biomimetic to real adult-senior staged patients requiring bone augmentation for dental implant placements.
Almost 80% of the experimental animals are rodents that include mice, rats, guinea pigs and others. Among the rodents, rats are the mostly used animals for experimental purposes, followed by mouse, rabbit, dog, pig and primate, especially for in vivo studies. The average weaning age for laboratory rats is 3 weeks, while that for humans is approximately 6 months [18]. Skeletal growth in male and female rats tapers off at approximately 7-8 months of age. From the correlation of rat body weight with different phases of postnatal days, postnatal day 56 (8 weeks) and day 70 (10 weeks) are adolescence stage and young adult stage, relatively [18]. Laboratory rats live about 2-3.5 years (average 3 years), while the worldwide life expectancy of humans is 80 years, with variations in countries in accordance with their socioeconomic conditions.
4.2. Barrier Membranes
Native collagen-based materials have been commonly applied as absorbable barrier membranes for GBR [2,7,8,9,19,20]. Collagen is a main component in human body, and the collagen-based materials have an outstanding biocompatibility [21,22,23,24]. However, it is difficult to control the absorbability and strength of animal-derived collagen materials. It was reported that the collagen membrane (Bio-Guide®) consisting of type I and III collagen was not cross-linked, digested by collagenase, and disappeared generally during 4-8 weeks [2,19,20,25]. Interestingly, as a dry collagen material has a characteristic of high potential of water retention (wettability), the wet expansion of the collagen membrane occurred spontaneously in scalp tissues in the present study. The first biological interaction that occurs is the adsorption of plasma proteins at the membrane–tissue interface. Proteins, although demonstrate an inclination towards aqueous environments but when a protein solution comes into contact with another phase, the proteins have more affinity to accumulate at the interface and surface wettability affects the protein adsorption ability on barrier membranes [2]. Wettability also affects platelet adhesion/activation, blood coagulation, cell and bacterial adhesion [2]. On the other hand, the P(LA/CL) membrane was developed as a prolonged barrier membrane against connective tissues for GBR, composed of both the solid layer inhibiting cellular and bacterial infiltration and the multi-porous layer, and degraded by hydrolysis in about 20 weeks [10,11]. Hydrolysis of PCL occurs by end-chain scission because of its highly crystalline chain structure. Hence, hydrolysis of PLA occurs at random points [10]. In addition to the slower degradation, another advantage of blending PCL is that it produces a less acidic environment during its degradation [9]. The slow degradation prevents the accumulation of by-products in the tissue microenvironment, thereby avoiding an overly acidic pH [26]. The P(LA/CL) membrane remained almost intact as a barrier until 12 weeks later, while the collagen membrane was expanded by body fluid such as blood and tissue liquid until 3 weeks. Moreover, neutrophils infiltrated into the upper layer of expanded collagen fibers at 3 weeks. The residues of the collagen membrane were not observed at 6 and 12 weeks. Until 6 weeks, fibroblasts proliferated in the swelled collagen fibers and should produce MMPs, especially collagenase, in the deformed collagen membrane. The enzymatic activity of fibroblasts, neutrophils and macrophages causes the collagen membrane to rapidly digest, and the collagenous material was replaced by newly formed collagen. The changes in the barrier morphology should correlate strongly with the migration and invasion of fibroblasts, necessary for fibrous tissue formation, from gum and mucosa. In contrast, the P(LA/CL) membrane remained clearly until 12 weeks in this augmentation model. It was reported that the weight of the P(LA/CL) membrane decreased in 45% after 26 weeks in the dissolution test using phosphate-buffered saline at 37℃ [10]. The lower degradation rate of the P(LA/CL) membrane was a better performance in a barrier function than the collagen membrane. In addition, conventional tensile tests showed that the P(LA/CL) membrane had a significantly smaller tensile strength compared with poly (lactic-glycolic acid: PLGA) membrane (GC membrane, GC Corp, Tokyo, Japan) [10]. In contrast, the breaking strain of the P(LA/CL) membrane was more than twenty times greater than that of the PLGA membrane, indicating that the P(LA/CL) membrane underwent a greater deformation prior to the rupture.
Unfortunately, very prolonged residual P(LA/CL) membrane might cause to wound rupture and chronic inflammation. In near future, the absorption of improved barrier membranes will be harmonized with bone-forming process in bone augmentation/regeneration.
4.3. Bone Managements for Bone Formation in Porous Scaffolds
The GBR procedure needs both an adequate scaffold that provides cell-anchorage and sufficient mechanical support and a barrier membrane that inhibits cellular invasion for vertical and/or horizontal augmentation in bone volume loss. It is well known that highly porous scaffolds promote bone formation better than the dense type [25,26,27]. A non-porous solid biomaterial acts like a material’s wall that inhibits both cellular and capillary invasion. In the P(LA/CL)/HAp, bone was locally formed in the middle and lower areas of the HAp block at 6 weeks. The immature tissues were observed in the upper pores of HAp at 12 weeks. Bone formation was not found in the upper pores of HAp even at 12 weeks, although the HAp block was 75% porosity. It was suspected that the main cause was insufficient supplies of mesenchymal stem cells and growth factors from highly calcified cortical bone of aged rats. We believe, therefore, cortical perforations into bone marrows or ultrasonic-scratching technique into the outer cortical plate of skull will contribute to an accelerated bone formation in GBR. The bone managements should contribute to the supply of bone marrow cells and the release of bone matrix- and blood-derived growth factors from the original bone [28,29,30]. The marrow-derived stem cells will proliferate and differentiate into osteoblasts in the interconnected pores of HAp block and in the porous layer of the P(LA/CL) membrane by reacting with several growth factors from bone and blood. Especially, bone morphogenetic proteins (BMPs) in bone matrix are key growth factors for accelerated bone formation in GBP procedure. BMPs has a strong bone-inducing capability, and vertical bone augmentation was achieved at 3 weeks by onlay implant using the composite of recombinant human BMP-2 (10 μg) and atelocollagen material (10 mg) on adult-senior staged rat skull model without periosteum [13]. We propose the application of the P(LA/CL) membrane including recombinant human BMP-2 in the porous layer and the highly porous HAp block combined with recombinant human BMP-2 onto the perforated outer cortical bone in this onlay model for an ideal GBR therapy.
4.4. Limitation
As for the limitation in this study, it was not able to measure the ratio of each tissue (bone, fibrous connective tissue, immature tissue), because of the cylindrical-shape HAp. A maximum split face of the specimen in this study using the cylindrical HAp was only one central area in one tissue block. Therefore, square-shape HAp blocks were better in this model than cylindrical-shape HAp blocks for the morphometrical measurement of bone, fibrous tissues and immature tissue.
5. Conclusions
The barrier effects of the P(LA/CL) membrane and the collagen membrane were evaluated histologically in the vertical augmentation model on 10–12-months old rat skull without periosteum. The P(LA/CL) membrane could achieve barrier effects under the repositioned soft tissues until 12 weeks and local bone formation occurred in the interconnected pores of HAp at 6 weeks. On the other hand, the collagen membrane did not inhibit cellular invasion for its expansion at 3 weeks and was absorbed until 6 weeks. The results indicated that the P(LA/CL) membrane might be effective in GBR procedure. Further investigation will be needed for the improvement of absorption rate and structure of the P(LA/CL) bilayer membrane.
Author Contributions
Conceptualization, K.K. and M.M; methodology, M.M. and A.K.; investigation, K.Y., M.S., and A.K.; data curation, M.S., A.K., and K.Y.; writing-original draft preparation, K.K. and M.M.; writing-review and editing, M.M. and K.K.; supervision, M.M. All authors have read and agreed to the published version of the manuscript.
Funding
This study was kindly supported by the GC Corporation (Tokyo, Japan) and all materials used in this study were provided by the GC Corporation.
Institutional Review Board Statement
The study design was approved from the Institutional Animal Care and Use Committee of the Health Sciences University of Hokkaido (No.21-047) with the principles of the Declaration of Helsinki.
Data Availability Statement
Not applicable.
Conflicts of Interest
Authors declare no conflict of interest.
References
- Scantlebury T.V. 1982-1992: A decade of technology development for guided tissue regeneration. J Periodontol. 1993; Nov;64 Suppl 11S:1129-1137. [CrossRef]
- Sheikh Z., Qureshi J., Alshahrani A.M., Nassar H., Ikeda Y., Glogauer M., Ganss B. Collagen based barrier membranes for periodontal guided bone regeneration applications. Odontology. 2017; Jan;105(1):1-12. [CrossRef]
- Lee S.W., Kim S.G. Membranes for the guided bone regeneration. Maxillofac. Plast. Reconstr. Surg. 2014; 36:239–246. [CrossRef]
- Selvig K.A., Kersten B.G., Chamberlain A.D., Wikesjö U.M., Nilvéus R.E. Regenerative surgery of intrabony periodontal defects using ePTFE barrier membranes: Scanning electron microscopic evaluation of retrieved membranes versus clinical healing. J. Periodontol. 1992; 63:974–978. [CrossRef]
- Zellin G., Gritli-Linde A., Linde A. Healing of mandibular defects with different biodegradable and non-biodegradable membranes: An experimental study in rats. Biomaterials. 1995; 16:601–609. [CrossRef]
- McGinnis M., Larsen P., Miloro M., Beck M. Comparison of resorbable and nonresorbable guided bone regeneration materials: A preliminary study. Int. J. Oral. Maxillofac. Implant. 1998; 13:30–35.
- Bornstein M.M., Bosshardt D., Buser D. Effect of two different bioabsorbable collagen membranes on guided bone regeneration: A comparative histomorphometric study in the dog mandible. J. Periodontol. 2007; 78:1943–1953. [CrossRef]
- Ren Y., Fan L., Alkildani S., Liu L., Emmert S., Najman S., Rimashevskiy D., Schnettler R., Jung O., Xiong X., Barbeck M. Barrier membranes for guided bone regeneration (GBR): A focus on recent advances in collagen membranes. Int. J. Mol. Sci. 2022; Nov 29;23(23):14987. [CrossRef]
- Allan B., Ruan R., Landao-Bassonga E., Gillman N., Wang T., Gao J., Ruan Y., Xu Y., Lee C., Goonewardene M., Zheng M. Collagen membrane for guided bone regeneration in dental and orthopedic applications. Tissue Eng. Part A. 2021; Mar;27(5-6):372-381.
- Abe G.L., Sasaki J., Katata C., Hohno T., Tsuboi R., Kitagawa H., Imazato S. Fabricarion of novel poly (l-lactic acid/ε-caprolactone) bilayer membrane for GBR. Dent. Mater. 2020; 36:626–634.
- Abe G.L., Tsuboi R., Kitagawa H., Sasaki J., Li A., Kohno T., Imazato S. Poly (lactic acid/caprolactone) bilayer membrane blocks bacterial penetration. J. Periodont. Res. 2022; 57:510–518. [CrossRef]
- Ogata K., Ohba S., Sumita Y., Asahina I. Safety and feasibility assessment of biodegradable poly (l-lactic acid/ε-caprolactone) membrane for guided bone regeneration: A case series of first-in-human pilot study. J. Dent. Sci. 2022; 17:368–376. [CrossRef]
- Shido R., Ohba S., Tominaga R., Sumita Y., Asahina I. A prospective study of the assessment of the efficacy of a biodegradable poly (l-lactic acid/ε-caprolactone) membrane for guided bone regeneration. J. Clin. Med. 2023; 15;12(18):5994. [CrossRef]
- Murata M., Maki F., Sato D., Shibata T., Arisue M. Bone augmentation by onlay implant using recombinant human BMP-2 and collagen on adult rat skull without periosteum. Clin. Oral Implants Res. 2000; 11(4):289-95. [CrossRef]
- Okubo N., Ishikawa M., Shakya M., Hosono H., Maehara O., Ohkawara T., Ohnishi S., Akazawa T., Murata M. Autograft of demineralized dentin matrix prepared immediately after extraction for horizontal bone augmentation of the anterior atrophic maxilla: A first case of non-vital tooth-derived dentin. J. Hard Tissue Biol., 2022; 31(1) 47-54. [CrossRef]
- Baek Y.J., Kim J.H., Song J.M., Yoon S.Y., Kim H.S., Shin S.H. Chitin-fibroin-hydroxyapatite membrane for guided bone regeneration: micro-computed tomography evaluation in a rat model. Maxillofac. Plast. Reconstr. Surg. 2016; Mar 22;38(1):14. [CrossRef]
- Ikumi R., Miyahara T., Akino N., Tachikawa N., Kasugai S. Guided bone regeneration using a hydrophilic membrane made of unsintered hydroxyapatite and poly (L-lactic acid) in a rat bone-defect model. Dent. Mater. J. 2018; Nov 30;37(6):912-918. [CrossRef]
- Sengupta P. The laboratory rat: Relating its age with human's. Int. J. Prev. Med. 2013; Jun;4(6):624-30.
- Schlegel A.K., Möhler H., Busch F., Mehl A. Preclinical and clinical studies of a collagen membrane (Bio-Gide). Biomaterials. 1997; Apr;18(7):535-8. [CrossRef]
- Tal H., Kozlovsky A., Artzi Z., Nemcovsky C.E., Moses O. Cross-linked and non-cross-linked collagen barrier membranes disintegrate following surgical exposure to the oral environment: a histological study in the cat. Clin. Oral Implants Res. 2008; Aug;19(8):760-6. [CrossRef]
- Murata M. Collagen biology for bone regenerative surgery. J. Korean Assoc. Oral Maxillofac. Surg. 2013; 38(32), 1-5. [CrossRef]
- Chattopadhyay S., Raines R.T. Review collagen-based biomaterials for wound healing. Biopolymers. 2014; 101:821–833. [CrossRef]
- Kabir M.A., Murata M., Shakya M., Yamada K., Akazawa T. Bio-absorption of human dentin-derived biomaterial in sheep critical-size iliac defects. Materials (Basel). 2021; Jan 5;14(1):223. [CrossRef]
- Murata M., Nezu T., Takebe H., Hirose Y., Okubo N., Saito T., Akazawa T. Human dentin materials for minimally invasive bone regeneration: Animal studies and clinical cases. J. Oral Biosci. 2023; Mar;65(1):13-18. [CrossRef]
- Tal H., Kozlovsky A., Artzi Z., Nemcovsky C.E., Moses O. Long-term bio-degradation of cross-linked and non-cross-linked collagen barriers in human guided bone regeneration. Clin. Oral Implants Res. 2008; Mar;19(3):295-302. [CrossRef]
- Wang W., Nie W., Liu D., Du H., Zhou X., Chen L., Wang H., Mo X., Li L., He C. Macroporous nanofibrous vascular scaffold with improved biodegradability and smooth muscle cells infiltration prepared by dual phase separation technique. Int. J. Nanomedicine. 2018; Nov 1;13:7003-7018. [CrossRef]
- Ripamonti U., Ma S., Reddi A.H. The critical role of geometry of porous hydroxyapatite delivery system in induction of bone by osteogenin, a bone morphogenetic protein. Matrix. 1992; Jun;12(3):202-12.. [CrossRef]
- Kuboki Y., Takita H., Kobayashi D., Tsuruga E., Inoue M., Murata M., Nagai N., Dohi Y., Ohgushi H. BMP-induced osteogenesis on the surface of hydroxyapatite with geometrically feasible and nonfeasible structures: topology of osteogenesis. J. Biomed. Mater. Res. 1998; Feb;39(2):190-9.
- Toosi S., Javid-Naderi M.J., Tamayol A., Ebrahimzadeh M.H., Yaghoubian S., Mousavi Shaegh S.A. Additively manufactured porous scaffolds by design for treatment of bone defects. Front Bioeng. Biotechnol. 2024; Jan 19; 11:1252636. [CrossRef]
- Alvira-González J., De Stavola L. The role of cortical perforations in bone regeneration: a systematic review. Int. J. Oral Maxillofac. Surg. 2020; Jul;49(7):945-951. [CrossRef]
- Shakya, M.; Murata, M.; Yokozeki, K.; Akazawa, T.; Nagayasu, H.; Adhikari, B. R.; Upadhyaya, C. Accelerated bone induction of adult rat compact bone plate scratched by ultrasonic scaler using acidic electrolyzed water. Materials (Basel). 2021; 14(12), 3347. [CrossRef]
- Zhu B., Yokozeki K., Kabir M.A., Todoh M., Akazawa T, Murata M. Chemical properties of human dentin blocks and vertical augmentation by ultrasonically demineralized dentin matrix blocks on scratched skull without periosteum of adult-aged rats. Materials (Basel). 2021; Dec 24;15(1):105. [CrossRef]
Figure 1.
Image of scanning electron microscopy of P(LA/CL) bilayer membrane. Upper layer: solid structure (25 μm). Lower layer: multi-porous (175 μm). Note: upper solid layer contact with repositioned soft tissues.
Figure 1.
Image of scanning electron microscopy of P(LA/CL) bilayer membrane. Upper layer: solid structure (25 μm). Lower layer: multi-porous (175 μm). Note: upper solid layer contact with repositioned soft tissues.
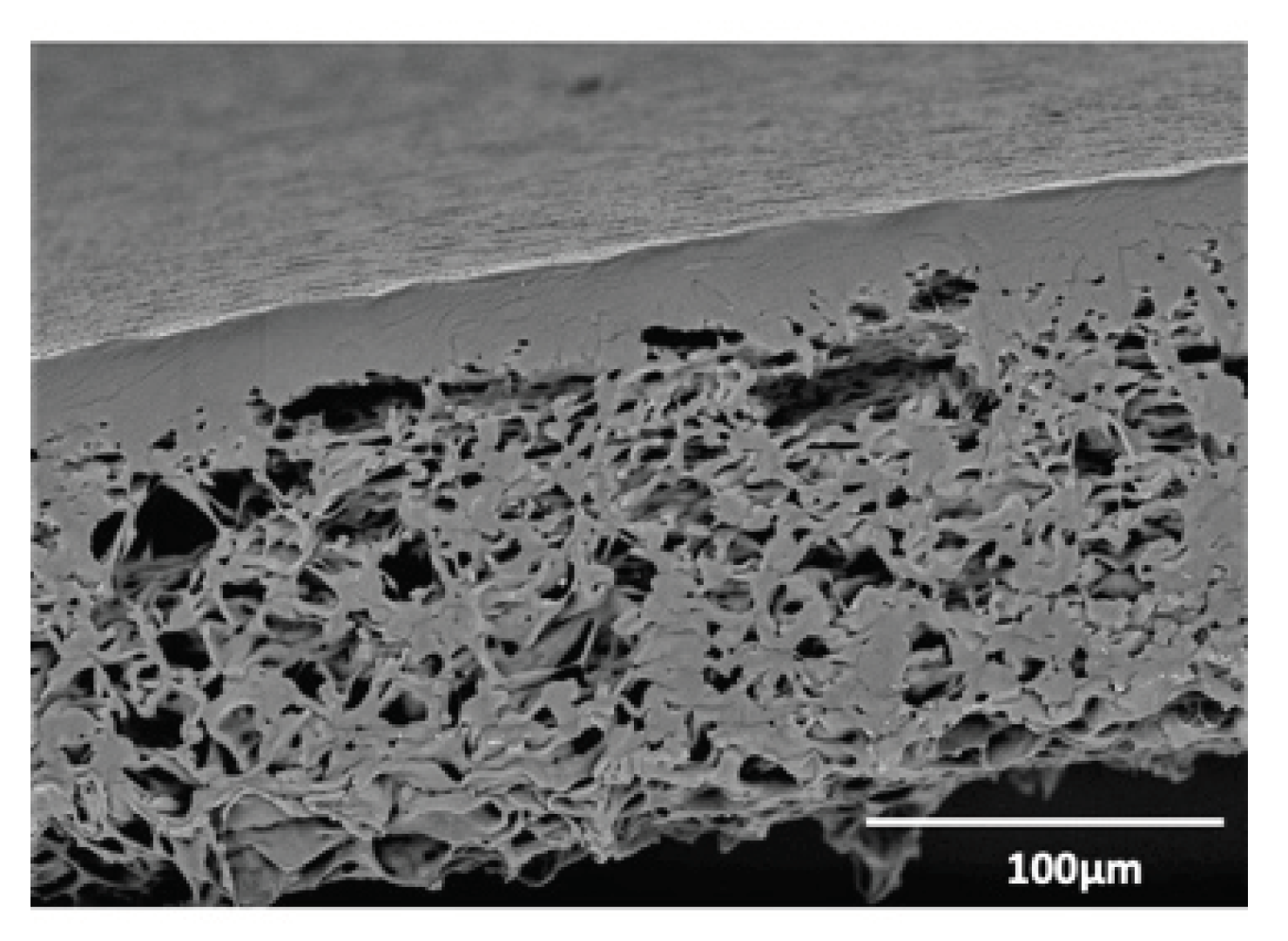
Figure 2.
Histological images of normal skull of 10-12 months old rat. Double arrow indicating periosteum with thick, fat cell-layer on outer cortical plate.
Figure 2.
Histological images of normal skull of 10-12 months old rat. Double arrow indicating periosteum with thick, fat cell-layer on outer cortical plate.
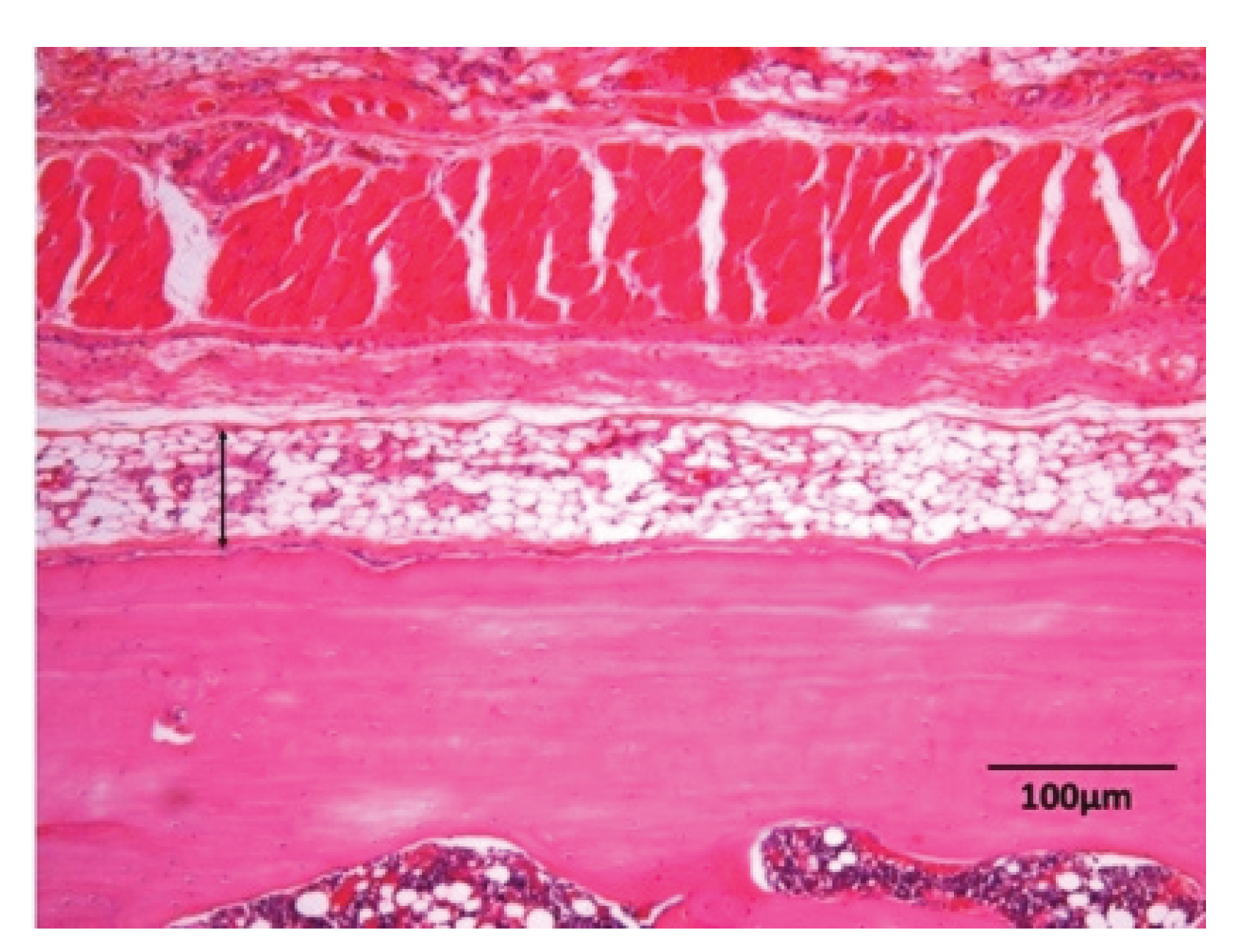
Figure 3.
Photography of surgical procedures on adult-senior staged rat skull in GBR model. (a) Incision and exposure of periosteum, (b) Removal of periosteum from parietal bone after elevation of scalp, (c) Cylindrical HAp block (diameter: 4 mm, height: 3 mm) on exposed parietal bone without periosteum, (d) Barrier membrane insertion (diameter: 8 mm), (e) Membrane between HAp and soft tissues without periosteum. Note: solid (dense) layer of membrane contacted with soft tissues, (f) Antibiotics paste on skin sutured with 5/0 nylon.
Figure 3.
Photography of surgical procedures on adult-senior staged rat skull in GBR model. (a) Incision and exposure of periosteum, (b) Removal of periosteum from parietal bone after elevation of scalp, (c) Cylindrical HAp block (diameter: 4 mm, height: 3 mm) on exposed parietal bone without periosteum, (d) Barrier membrane insertion (diameter: 8 mm), (e) Membrane between HAp and soft tissues without periosteum. Note: solid (dense) layer of membrane contacted with soft tissues, (f) Antibiotics paste on skin sutured with 5/0 nylon.
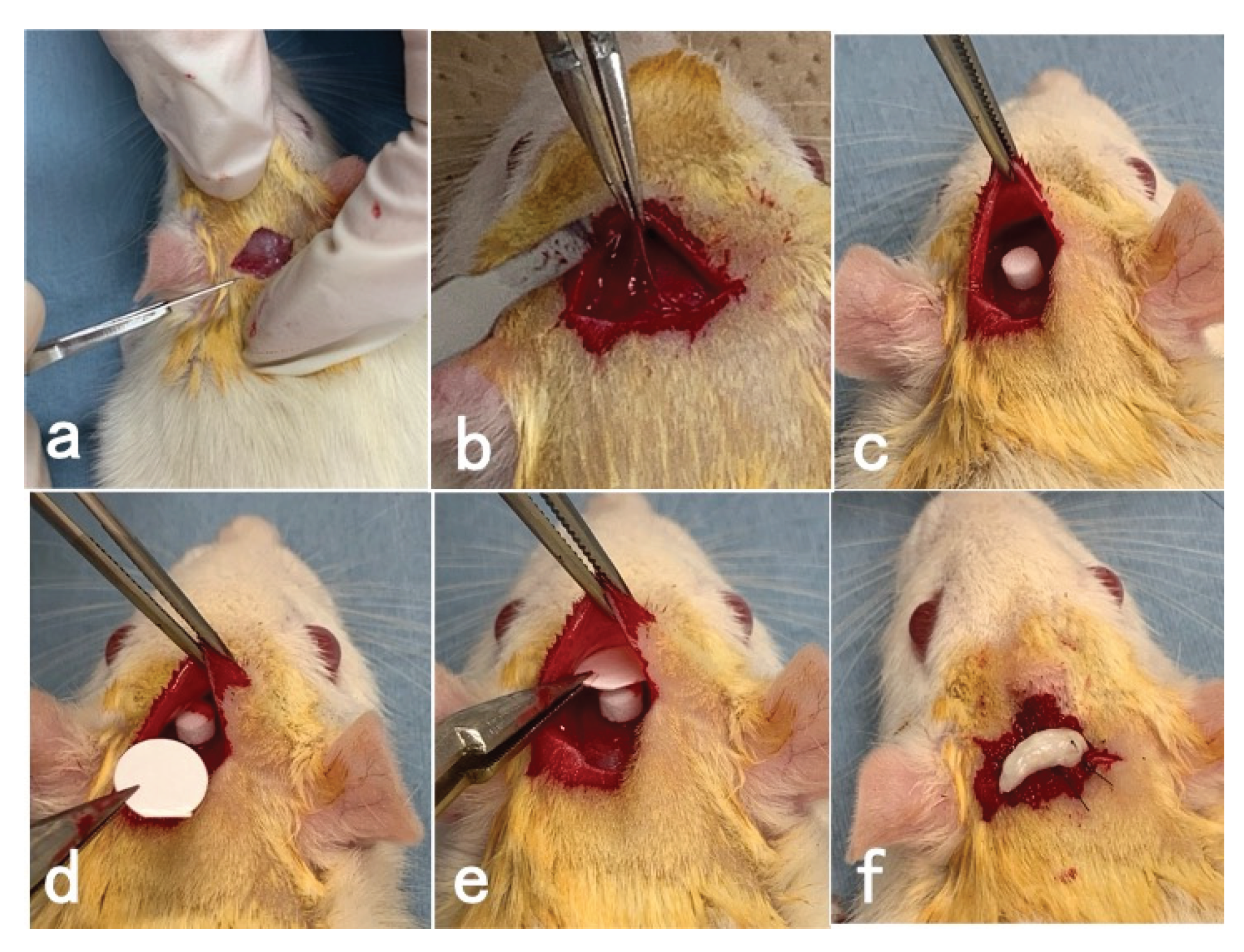
Figure 4.
Histological images of P(LA/CL) /HAp on skull without periosteum at 3 weeks. Fibrous connective tissues on P(LA/CL) membrane. Red blood cells and body fluid in pores of HAp. Note: P(LA/CL) and HAp bulk showing clear spaces after completely demineralization in HE.
Figure 4.
Histological images of P(LA/CL) /HAp on skull without periosteum at 3 weeks. Fibrous connective tissues on P(LA/CL) membrane. Red blood cells and body fluid in pores of HAp. Note: P(LA/CL) and HAp bulk showing clear spaces after completely demineralization in HE.
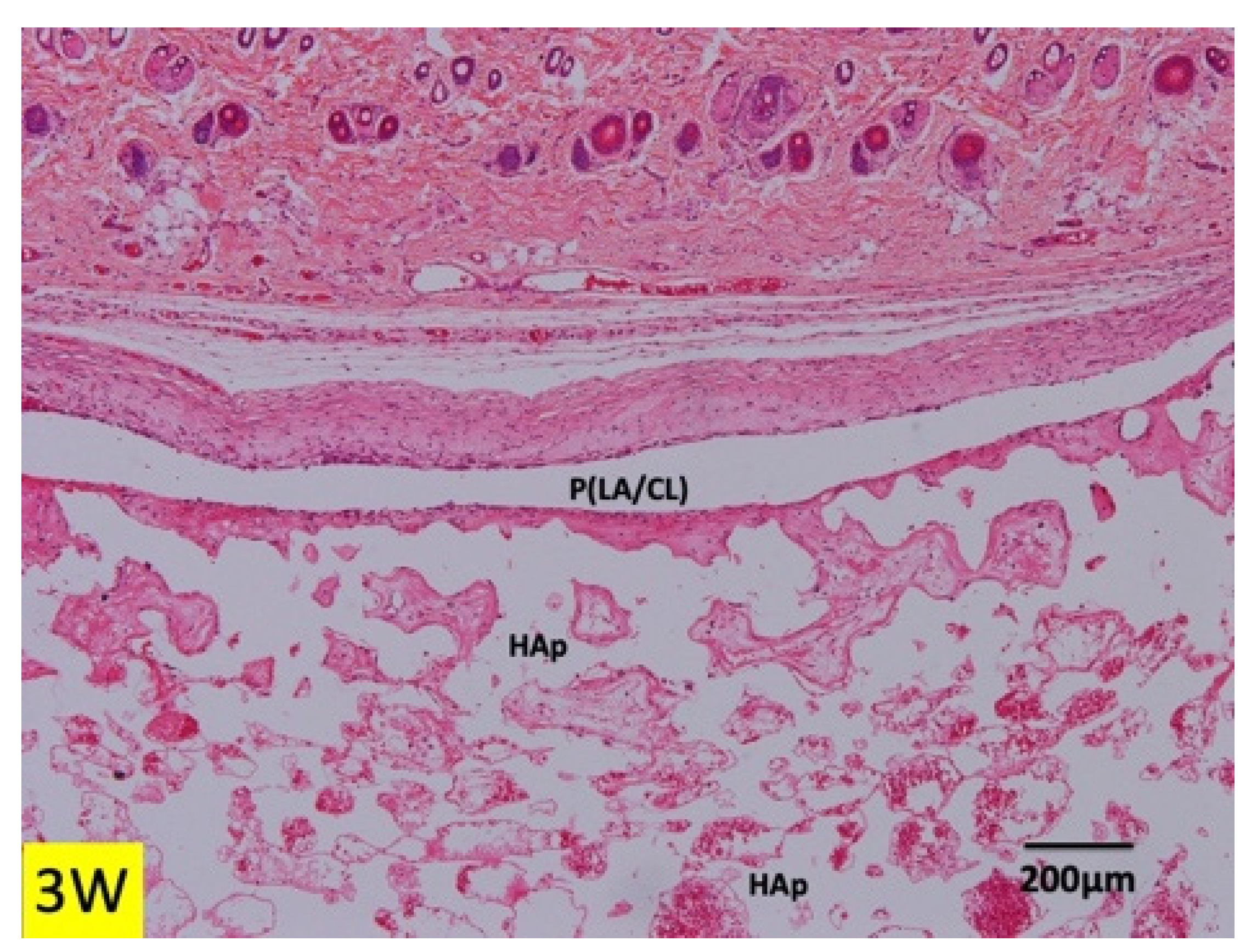
Figure 5.
Histological images of P(LA/CL) / HAp on skull without periosteum at 6 weeks. Left: Total view at 6 weeks. Hair and fibrous connective tissues on P(LA/CL). Right: Higher magnification of white frame in Figure 5 (left). Fibrous connective tissues on P(LA/CL). Undifferentiated mesenchymal cells, red blood cells and body fluid in pores of HAp. Note: P(LA/CL) and HAp bulk showing clear spaces after demineralization (HE).
Figure 5.
Histological images of P(LA/CL) / HAp on skull without periosteum at 6 weeks. Left: Total view at 6 weeks. Hair and fibrous connective tissues on P(LA/CL). Right: Higher magnification of white frame in Figure 5 (left). Fibrous connective tissues on P(LA/CL). Undifferentiated mesenchymal cells, red blood cells and body fluid in pores of HAp. Note: P(LA/CL) and HAp bulk showing clear spaces after demineralization (HE).
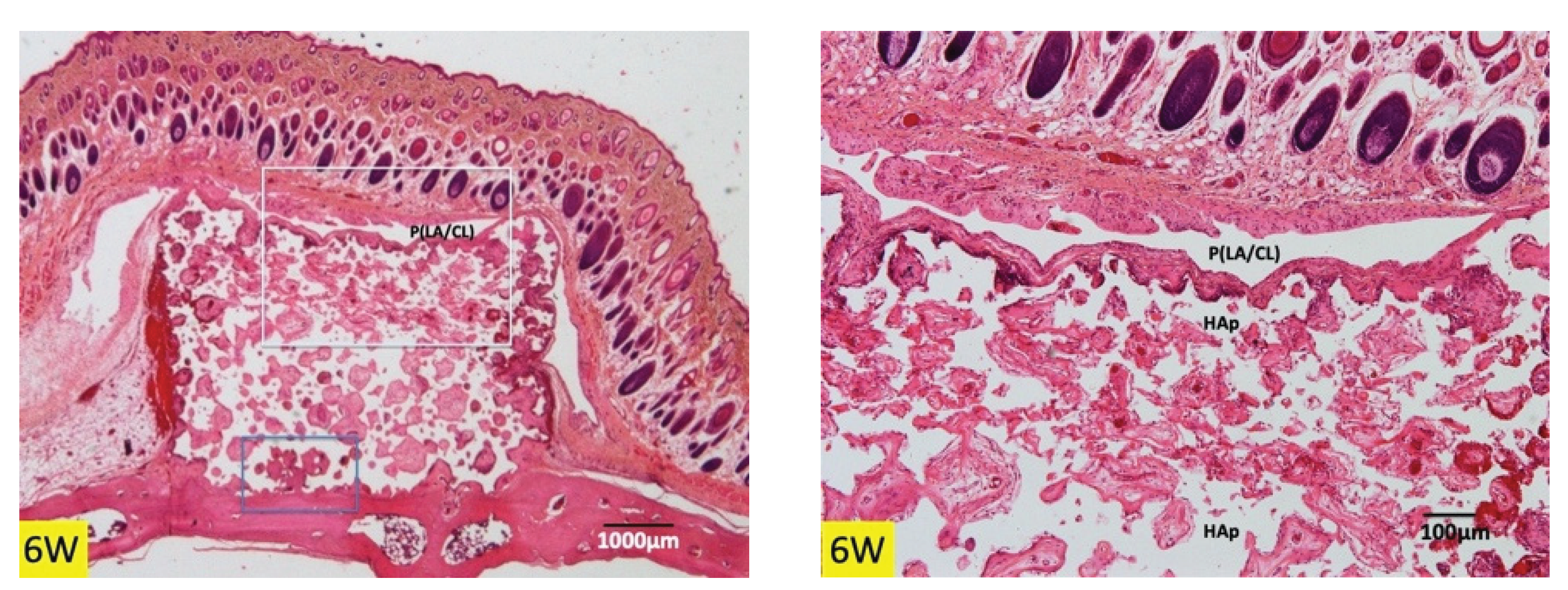
Figure 6.
Histological images of P(LA/CL) / HAp on skull without periosteum at 6 weeks. (a) Residues of bleeding between P(LA/CL) and HAp, (b) Undifferentiated mesenchymal cells and blood cells in immature tissues in pore, (c) Higher magnification of blue frame in Figure 5. Bone formation in pores near skull, (d) Higher magnification of yellow frame in Figure 6c. New bone and immature tissues with undifferentiated mesenchymal cells and red blood cells in pores. B: bone.
Figure 6.
Histological images of P(LA/CL) / HAp on skull without periosteum at 6 weeks. (a) Residues of bleeding between P(LA/CL) and HAp, (b) Undifferentiated mesenchymal cells and blood cells in immature tissues in pore, (c) Higher magnification of blue frame in Figure 5. Bone formation in pores near skull, (d) Higher magnification of yellow frame in Figure 6c. New bone and immature tissues with undifferentiated mesenchymal cells and red blood cells in pores. B: bone.
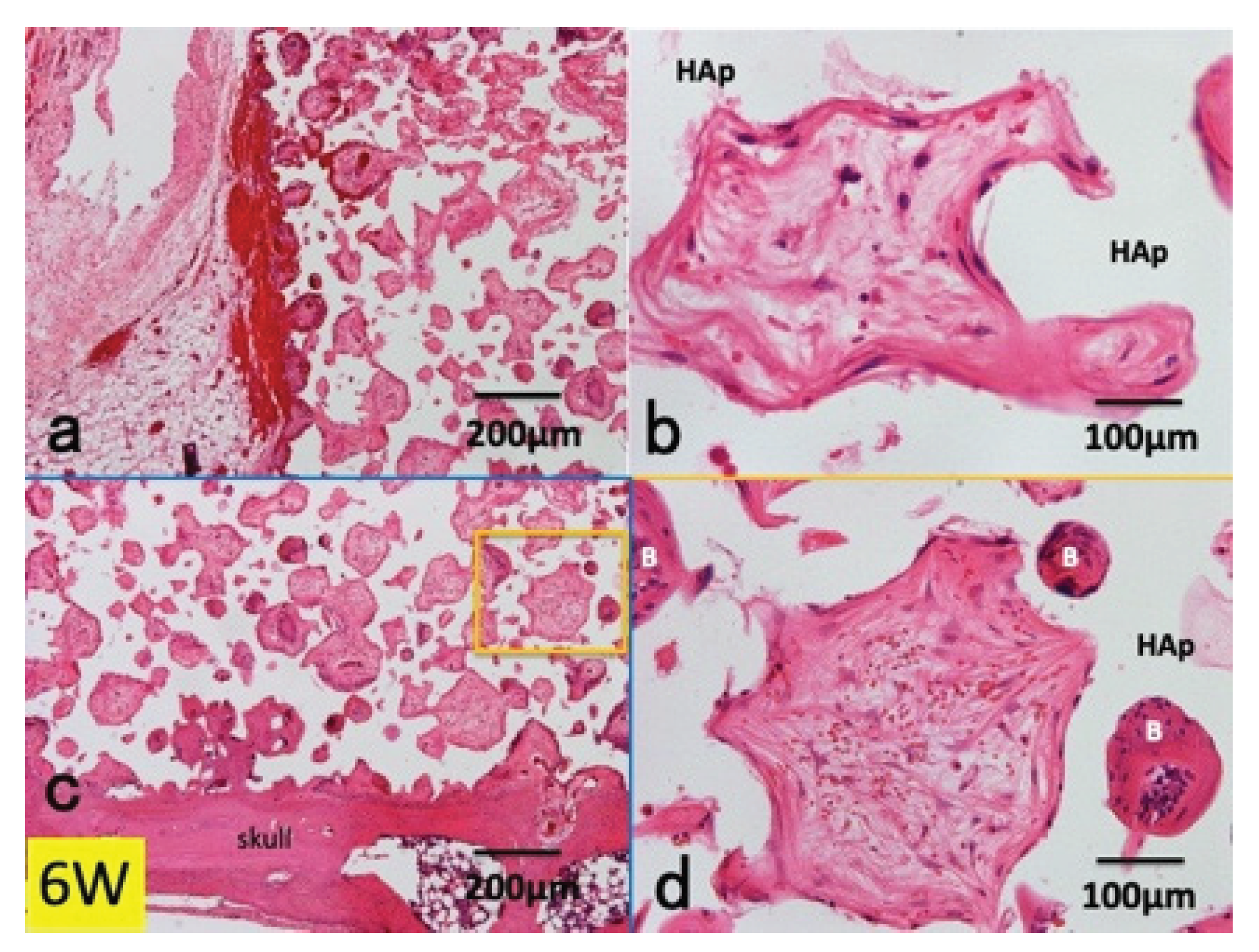
Figure 7.
Histological images of P(LA/CL) / HAp on skull without periosteum at 12 weeks. Left: Total view. Fibrous connective tissues around P(LA/CL) showing clear spaces after demineralization (HE). Immature tissues in middle area of HAp block. Right: (a) Fibrous connective tissues on P(LA/CL), (b) Bone in interconnected pores, (c) Bony bridge between original bone and new bone in lower pores. Undifferentiated mesenchymal cells, red blood cells and body fluid in middle pores of HAp, (d) Bony bridge between original bone and new bone in lower pores. Immature tissues in middle pores.
Figure 7.
Histological images of P(LA/CL) / HAp on skull without periosteum at 12 weeks. Left: Total view. Fibrous connective tissues around P(LA/CL) showing clear spaces after demineralization (HE). Immature tissues in middle area of HAp block. Right: (a) Fibrous connective tissues on P(LA/CL), (b) Bone in interconnected pores, (c) Bony bridge between original bone and new bone in lower pores. Undifferentiated mesenchymal cells, red blood cells and body fluid in middle pores of HAp, (d) Bony bridge between original bone and new bone in lower pores. Immature tissues in middle pores.
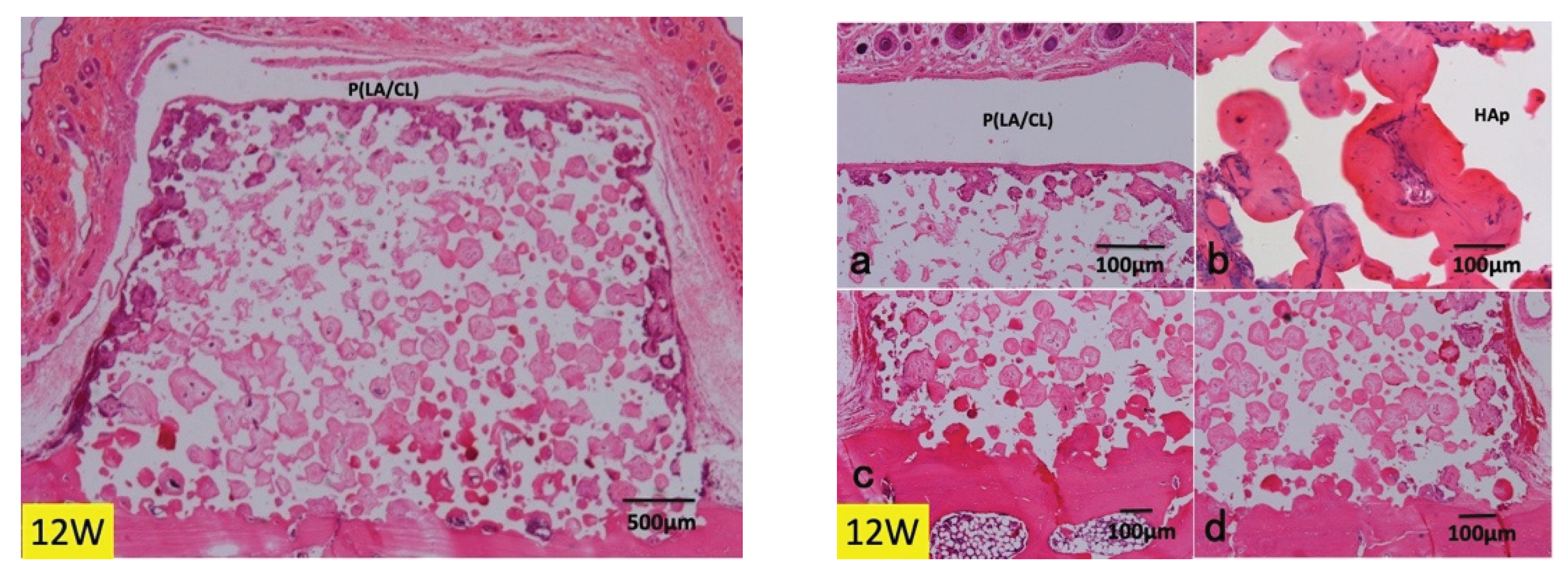
Figure 8.
Histological images of collagen / HAp on skull without periosteum at 3 weeks. (a) Expansion of collagen membrane (*). Eosin-stained collagen fibers of membrane. Note: Thin thickness of collagen membrane on corners of HAp block, (b) Strongly eosin-stained collagen fibers (*), compared to original connective tissues. Haematoxyline-stained white blood cells in upper layer of membrane, (c) Wavy collagen fibers of membrane in top pore of HAp. *: collagen membrane.
Figure 8.
Histological images of collagen / HAp on skull without periosteum at 3 weeks. (a) Expansion of collagen membrane (*). Eosin-stained collagen fibers of membrane. Note: Thin thickness of collagen membrane on corners of HAp block, (b) Strongly eosin-stained collagen fibers (*), compared to original connective tissues. Haematoxyline-stained white blood cells in upper layer of membrane, (c) Wavy collagen fibers of membrane in top pore of HAp. *: collagen membrane.
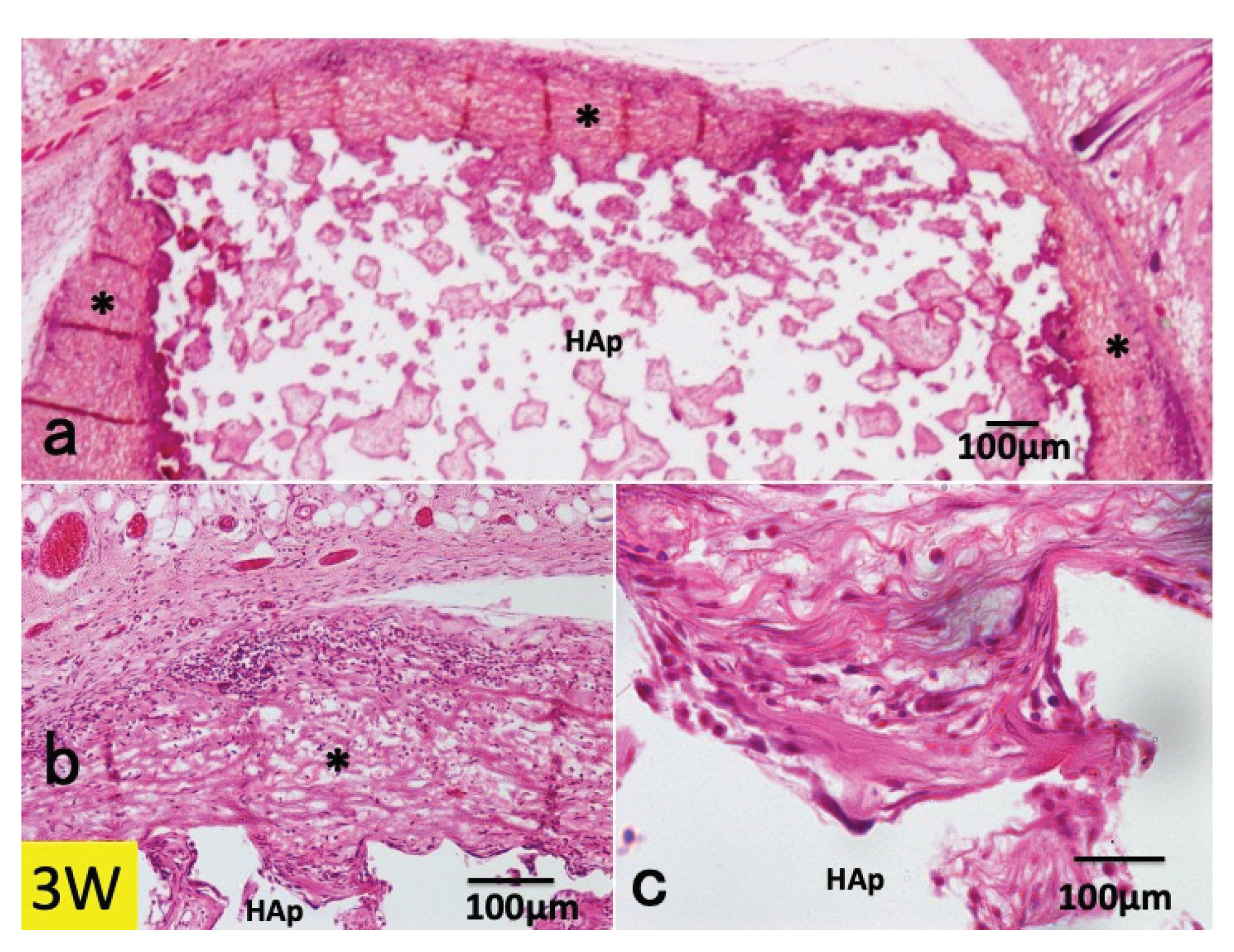
Figure 9.
Histological images of collagen / HAp on skull without periosteum at 6 weeks. Disappearance of collagen membrane. Fibrous connective tissue formation in upper pores.
Figure 9.
Histological images of collagen / HAp on skull without periosteum at 6 weeks. Disappearance of collagen membrane. Fibrous connective tissue formation in upper pores.
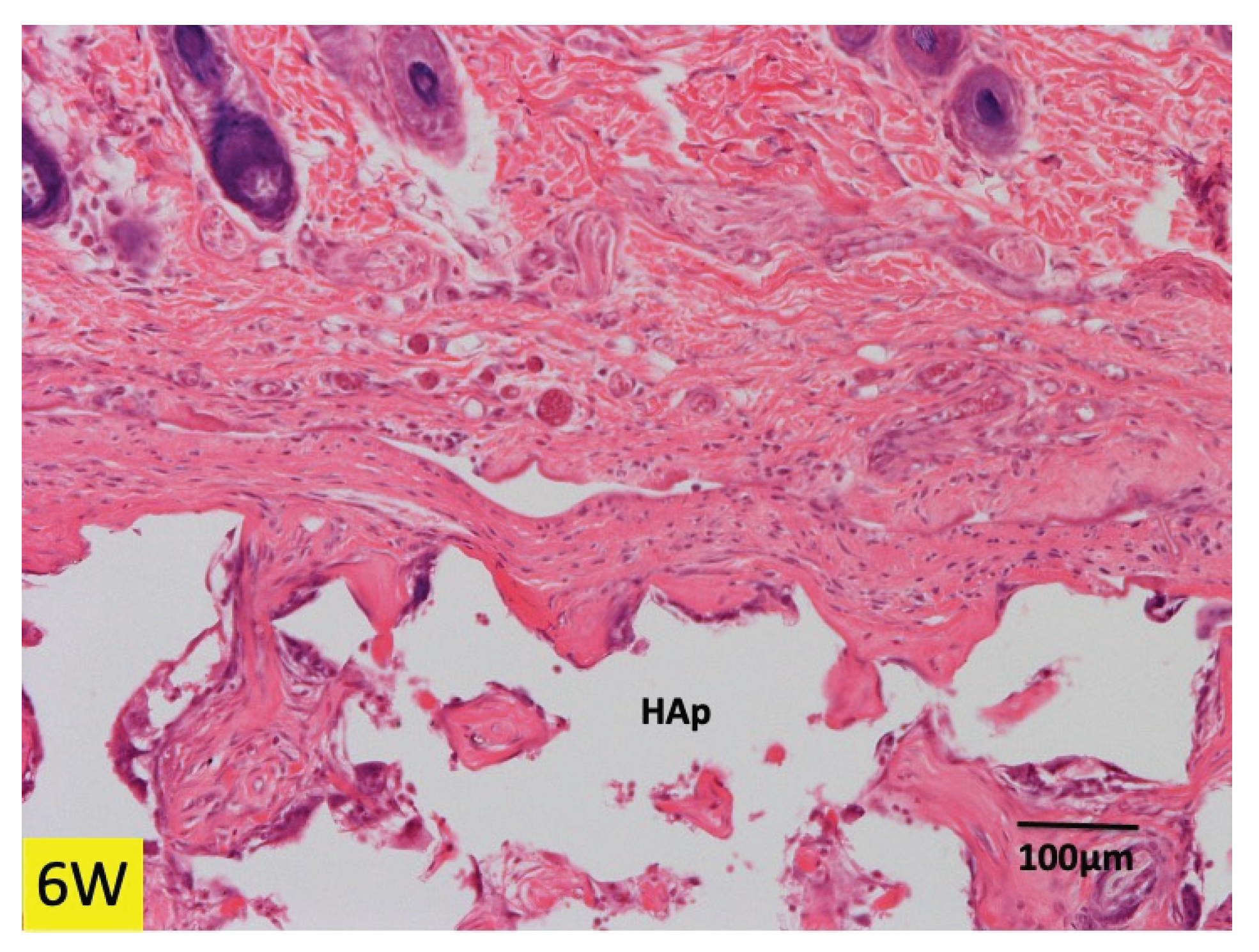
Figure 10.
Histological images of collagen / HAp on skull without periosteum at 12 weeks. (a) Disappearance of collagen membrane. HAp covered with fibrous connective tissues, (b) Fibrous connective tissue in upper pores. (c) Dense connective tissues in pores of middle area of HAp block.
Figure 10.
Histological images of collagen / HAp on skull without periosteum at 12 weeks. (a) Disappearance of collagen membrane. HAp covered with fibrous connective tissues, (b) Fibrous connective tissue in upper pores. (c) Dense connective tissues in pores of middle area of HAp block.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



