Submitted:
23 February 2024
Posted:
29 February 2024
You are already at the latest version
Abstract
The association between normal-range triglycerides and diabetes mortality remains unclear. This cohort study aimed to elucidate this relationship by examining 19,010 US adult participants with fasting serum triglycerides below 150 mg/dL. Cox proportional hazards models were employed to estimate mortality hazard ratios (HRs) and 95% confidence intervals (CIs). Participants were followed up for a mean of 15.3 years, during which 342 diabetes deaths were recorded. A 1-natural-log-unit increase in triglycerides was associated with a 57% higher risk of diabetes mortality (adjusted HR, 1.57; 95% CI, 1.04–2.38). Comparable results were obtained when triglycerides were analyzed in quartiles. Receiver operating characteristic curve analysis identified an optimal triglyceride cutoff of 94.5 mg/dL for diabetes mortality; individuals with triglyceride levels above this threshold faced a greater risk of diabetes mortality (adjusted HR, 1.43; 95% CI, 1.12–1.83). Further investigation revealed a positive association between normal triglyceride levels and all-cause mortality, though no association was observed between normal triglycerides and mortality from hypertension or cardiovascular disease. In conclusion, elevated triglycerides within the normal range were associated with an increased risk of diabetes mortality. Individuals with triglyceride levels of 95 mg/dL or higher may require vigilant monitoring for diabetes and its associated complications.
Keywords:
triglyceride
; diabetes
; hypertension
; cardiovascular disease
; survival
1. Introduction
Diabetes poses a significant global public health concern [1,2], contributing to over one million deaths annually [3]. Consequently, there exists a pressing medical need to identify modifiable risk factors for diabetes development and mortality.
Hypertriglyceridemia, defined as fasting triglycerides ≥ 150 mg/dL [4], frequently coexists with diabetes [5,6]. Individuals with hypertriglyceridemia have an increased risk of diabetes diagnosis [7,8], incidence [9,10,11,12,13], and mortality [8]. As such, the association between diabetes and hypertriglyceridemia is well established. However, the correlation between diabetes and triglycerides within the normal range remains understudied.
To date, only two studies have examined the relationship between triglycerides and diabetes in individuals with normal triglyceride levels [14,15]. Beshara et al [14] discovered that, among 3,722 Israeli individuals with normal triglycerides who were followed up for 7.6 years, elevated triglycerides (ranging from 100 to 149 mg/dL) correlated with a higher risk of new-onset type 2 diabetes compared to those with triglycerides below 100 mg/dL. In a separate study, Wang et al [15] observed a positive association between normal triglyceride levels and the prevalence of type 2 diabetes in 16,706 Chinese adults.
This has prompted a debate regarding whether the hypertriglyceridemia threshold of 150 mg/dL should be lowered for individuals at a higher risk of diabetes. To further this discourse, additional research is warranted, particularly investigating whether triglycerides in the upper normal range are associated with diabetes mortality.
The present study aimed to bridge this knowledge gap by examining the association between triglycerides and diabetes mortality among 19,010 US adult participants with triglyceride levels within the normal range.
Furthermore, hypertriglyceridemia is associated with hypertension [16] and cardiovascular disease (CVD) [17], as well as CVD mortality [18,19,20] and all-cause mortality [21,22]. Consequently, this study also explored whether triglycerides within the normal range were associated with hypertension mortality, CVD mortality, and all-cause mortality.
2. Materials and Methods
2.1. Participants
Participants in this cohort study were from the third National Health and Nutrition Examination Survey (NHANES III, 1988-1994) and the subsequent eight cycles of NHANES from 1999 to 2014 [17]. A total of 19,072 adults aged ≥ 20 years attended the examination who had their fasting serum triglyceride levels within the normal range (<150 mg/dL). The participants with missing fasting plasma glucose (n = 43) and those without a follow-up time or with a follow-up time of 0 month (n = 19) were excluded. Therefore, the remaining 19,010 participants were included in the final analysis.
2.2. Exposure Variable
The exposure variable of this study was the baseline fasting triglyceride level. To measure serum triglycerides, enzymatic methods were employed. These methods involved a sequence of coupled reactions: initially, triglycerides underwent hydrolysis to yield glycerol. Subsequently, glycerol underwent oxidation via glycerol oxidase, resulting in the production of dihydroxyacetone phosphate and H2O2. The generated H2O2 was then transformed by peroxidase into a phenazone compound, which was quantified by assessing absorbance at 500 nm [23].
2.3. Outcome Variables
The outcome variables of this study were various types of mortality. Data pertaining to mortality from diabetes, hypertension, CVD, and all causes were directly retrieved from NHANES-linked mortality files [17]. To evaluate mortality status and the cause of death, the National Center for Health Statistics conducted probabilistic matching to link the NHANES data with death certificate records from the National Death Index (NDI) records [24]. All deaths were classified according to the International Classification of Diseases, 9th Revision (ICD-9) or the International Classification of Diseases, 10th Revision (ICD–10), and subsequently recoded using the Underlying Cause of Death 113 (UCOD_113) system [17]. Follow-up time was the duration from the time when the participant was examined at the Mobile Examination Center until the conclusion of follow-up (December 31, 2019), or until death, whichever occurred first.
2.4. Covariables
Covariables were described previously [25,26] and they included age (continuous), sex (male or female), ethnicity (Hispanic, non-Hispanic white, non-Hispanic black, or other), body mass index (continuous), education (< high school, high school, > high school, or unknown), poverty-income ratio (< 130%, 130%–349%, ≥ 350%, or unknown), survey periods (1988–1991, 1991–1994, 1999–2000, 2001–2002, 2003–2004, 2005–2006, 2007–2008, 2009–2010, 2011–2012, or 2013–2014), physical activity (inactive, insufficiently active, or active), alcohol consumption (never, < 1 drink per week, 1–6 drinks per week, ≥ 7 drinks per week, or unknown), smoking status (current smoker, past smoker, or other), systolic blood pressure (continuous), total cholesterol (continuous), high-density lipoprotein (HDL) cholesterol (continuous), and family history of diabetes (yes, no, or unknown).
2.5. Statistical Analyses
Data were presented as number and percentage for categorical variables, mean and standard deviation for normally distributed continuous variables, or median and interquartile range for not normally distributed continuous variables to describe the baseline characteristics of the participants [27]. Differences in continuous variables were analyzed using one-way ANOVA (normally distributed) or Kruskal Wallis one-way ANOVA (not normally distributed) [28], and differences among categorical variables were analyzed using Pearson's chi-square test [29].
Cox proportional hazards models were used to calculate hazard ratios (HRs) and 95% confidence intervals (CIs) of triglycerides for mortality from hypertension, diabetes, CVD and all causes [30]. Triglycerides were treated as a continuous variable (natural log-transformed) or categorical variable (in observed quartiles: ≤ 67, 68–89, 90–113, or ≥ 114 mg/dL).
Out of 19,010 participants, 604 (3.2%) had missing data including body mass index (n = 196), systolic blood pressure (n = 438), total cholesterol (n = 1), and HDL cholesterol (n = 10). The missing data were imputed via multiple imputation by chained equations [31], with 20 imputed data sets being created [32]. In all the regression analyses, triglycerides, body mass index, systolic blood pressure, total cholesterol, and HDL cholesterol were natural log transformed to improve data distribution [33].
Sensitivity analyses were conducted when the imputed data were not used, i.e., by excluding those 604 participants with missing data from the analysis, or when those with a follow-up time of < 2 years (n = 360) were excluded.
Receiver operating characteristic curves were constructed and the area under the curve (AUC) was calculated to assess the association of triglycerides with diabetes mortality [34] and the optimal cutoff of triglycerides for diabetes mortality was determined by the Youden Index [35]. Kaplan–Meier curves were constructed to estimate the survival rates of participants across triglyceride categories, which were compared using the log-rank test [36].
The null hypothesis was rejected for two-sided values of p <0.05. All analyses were performed using SPSS version 27.0 (IBM SPSS Statistics for Windows, Armonk, NY, IBM Corporation) [37].
3. Results
3.1. General Characteristics
This cohort included 19,010 US adult participants with fasting serum triglycerides within the normal range (< 150 mg/dL). The participants had a mean (standard deviation) age of 47 (19) years. Those with higher triglycerides had higher fasting plasma glucose, higher body mass index, higher systolic blood pressure, higher total cholesterol, and lower HDL cholesterol. In addition, they were older and less physically active and received less education (Table 1).
3.2. Association of Triglycerides within the Normal Range with Diabetes Mortality
This cohort was followed up for 291,286 person-years with a mean follow-up of 15.3 years. During the follow-up, 342 diabetes deaths were recorded.
A 1-natural-log-unit increase in triglycerides was associated with a 57% higher risk of diabetes mortality (HR, 1.57; 95% CI, 1.04–2.38; p = 0.03; Table 2) after adjustment for all the tested confounding factors. When triglycerides were treated as a categorical variable (i.e., observed quartiles), those with triglycerides in the higher quartiles showed a worse survival as analyzed by the Kaplan-Meier survival curve analysis (p <0.001, Figure 1). Cox proportional hazards models confirmed these results: participants with triglycerides in the top two quartiles had a higher risk of diabetes mortality compared with those with triglycerides in the bottom quartile after adjustment for all the tested confounding factors (Table 3).
Sensitivity analyses showed that the positive association between triglycerides within the normal range and diabetes mortality remained after excluding those with a follow-up time of less than 2 years (Table 4) or when the imputed data were not used by excluding those 604 participants with missing data from the analysis (Table 5).
3.3. The Optimal Cutoff of Triglycerides for Diabetes Mortality
Receiver operating characteristic curve analysis showed that the optimal cutoff of triglycerides to classify diabetes mortality was 94.5 mg/dL (Figure 2A). Kaplan-Meier survival curves confirmed this classification, and those with triglycerides above the cutoff (i.e., triglycerides ranging between 95 and 149 mg/dL) had significantly worse survival compared with those with triglycerides below the cutoff (p < 0.001, Figure 2B). Consistently, after adjusting for all the tested confounders, those with normal triglycerides above the cutoff had a 43% higher risk of diabetes mortality (HR, 1.43; 95% CI, 1.12–1.83; p = 0.005; Figure 2C) compared with those with triglycerides below the cutoff.
3.4. Association of Triglycerides with Hypertension Mortality, CVD Mortality, and All-Cause Mortality
During the 291,286 person-years of follow-up, 619 hypertension deaths, 1535 CVD deaths, and 4447 all-cause deaths were recorded.
4. Discussion
Using a large general cohort of US adults (n = 19,010), this study, for the first time, demonstrated that fasting triglycerides in the upper normal range were associated with diabetes mortality. Receiver operating characteristic curve analysis revealed that the optimal cutoff of triglycerides for diabetes mortality was 94.5 mg/dL; individuals surpassing this threshold exhibited a 43% higher multivariable-adjusted risk of diabetes mortality compared to those below it.
Although the association between hypertriglyceridemia and diabetes is well recognized [9,10,11,12,13,38], the underlying mechanisms remain poorly understood. Several mechanisms have been proposed: elevated triglyceride levels may impede glucose transport [39], inhibit glucose oxidation [40], and decrease glycogen synthesis rates [41].
So far, only two studies have explored the association between normal triglycerides and diabetes [14,15], and they have found that triglycerides in the upper normal range are positively associated with the prevalence [15] and new-onset of diabetes [14]. The current study expanded our knowledge and found that triglycerides in the upper normal range were also associated with diabetes mortality. However, the underlying mechanism is unknown. The applicability of proposed mechanisms connecting hypertriglyceridemia and diabetes to triglycerides within the normal range warrants future investigation.
The current study indicated that the optimal cutoff of triglycerides for diabetes mortality was 94.5 mg/dL. This cutoff is supported by the diabetes mortality data: individuals with triglycerides above the cutoff (i.e., 95–149 mg/dL) had a 43% higher risk of diabetes mortality compared with those below the cutoff (i.e., ≤ 94 mg/dL). Moreover, the proximity of this cutoff to the triglyceride cutoff of 96.5 mg/dL for type 2 diabetes prevalence in 16,706 Chinese adults [15] adds weight to its significance. While Beshara et al's study [14] did not pinpoint the optimal cutoff of triglycerides for new-onset type 2 diabetes, their findings among 3,722 Israeli individuals with normal triglycerides indicate that higher normal triglyceride levels (ranging from 100 to 149 mg/dL) were associated with an increased risk of new-onset type 2 diabetes compared to levels below 100 mg/dL, supporting a lower threshold of triglycerides for hypertriglyceridemia. Consequently, the results of this study contribute to the debate surrounding the necessity to lower the current threshold of hypertriglyceridemia (i.e., 150 mg/dL) for individuals at an increased risk of diabetes.
The association between hypertriglyceridemia and all-cause mortality has been intensively investigated [42]. It has been shown that hypertriglyceridemia is associated with an increased risk of all-cause mortality across various populations worldwide, including those in the US [21], Australia [20], and the Czech Republic [22]. The positive association persists among general hospitalized patients [43] and individuals with specific conditions such as coronary heart disease [44] and diabetes [45]. Moreover, a genetic study has demonstrated that reduced plasma triglyceride concentrations genetically correlate with a decreased risk of all-cause mortality [46]. Additionally, reducing triglycerides through fenofibrate as an adjunct to statin treatment has been linked to decreased all-cause mortality risk [47].
The results of the current study showed that triglycerides in the upper normal range were also associated with an increased risk of all-cause mortality, suggesting a potential necessity to lower the hypertriglyceridemia threshold of 150 mg/dL. While previous investigations have not specifically delved into the association between normal-range triglycerides and all-cause mortality as extensively as the current study, a few reports examining the full spectrum of triglyceride levels have observed such a correlation. For instance, Fang et al demonstrated that among 7,476 US adults, individuals with triglyceride levels ranging from 100 to 149 mg/dL faced an elevated risk of all-cause mortality (HR: 1.12; 95% CI 1.01-1.12) compared to those below 100 mg/dL [48]. Similarly, Klempfner et al noted that, in patients with established coronary heart disease, triglyceride levels between 100 and 149 mg/dL were associated with increased all-cause mortality risk (HR: 1.06; 95% CI 1.01-1.12) compared to levels below 100 mg/dL [44].
Many studies across various countries, including Japan [49], Spain [50], China [51], and the US [52], have consistently shown that hypertriglyceridemia increases the risk of new-onset hypertension in the general population. Several proposed mechanisms may underline this association, such as triglycerides contributing to endothelial dysfunction and increased sympathetic nerve activity [53]. Notably, even within the normal range, triglyceride levels have been positively linked to incident hypertension [52,54].
However, in a novel revelation, the current study indicates that triglycerides within the normal range were not associated with hypertension mortality over a mean follow-up of 15.3 years. This implies that while upper normal range triglycerides may elevate the risk of new-onset hypertension, they may not exacerbate hypertension to a fatal extent.
In epidemiological studies, hypertriglyceridemia often correlates with increased CVD mortality risk in the general population [18,19,20] and in sub-populations including patients with coronary artery disease [55], cerebrovascular disease [56], or diabetes [17,57,58]. Yet, conflicting reports exist, with some studies failing to establish such a positive correlation [21,59,60,61]. Nonetheless, a meta-analysis of 19 studies involving 91,285 diabetic patients revealed that triglyceride-lowering therapy was associated with reduced CVD events and mortality [62]. Consequently, hypertriglyceridemia has been recognized as a "risk-enhancing factor" by the American Heart Association and American College of Cardiology [63].
Interestingly, the current study did not find an association between triglycerides within the normal range and CVD mortality. While this suggests that upper normal range triglycerides may not significantly worsen CVD to the point of mortality, it does not rule out their potential contribution to CVD development. Indeed, research has shown that higher normal triglyceride levels (97–141 mg/dL versus < 97 mg/dL) were linked with an increased risk of new-onset ischemic heart disease [64]. Additionally, another study identified 89 mg/dL as the prognostic cutoff value for triglycerides to predict cardiovascular events in a cohort of 14,189 Italian adults [65].
Strengths and limitations One notable strength of this study is its analysis of triglycerides within the normal range in a large representative cohort of US adults (n = 19,010) over a lengthy follow-up period of 15.3 years. Furthermore, the study's adjustment for various confounders, including body mass index, systolic blood pressure, total cholesterol, and HDL cholesterol, enhances the robustness of its findings. This study also has several limitations. First, mortality outcomes were ascertained by linkage to the National Death Index (NDI) records with a probabilistic match, which could result in misclassification [8]. However, this matching method has been shown to be highly accurate with an accuracy rate of 98.5% [66]. Second, triglycerides were only measured once, which may result in bias. However, in epidemiological studies, this bias tends to lead to an underestimate rather than an overestimate of risk due to regression dilution [67]. Therefore, the association of triglycerides within the normal range with diabetes mortality might be much stronger if triglyceride levels were measured repeatedly.
5. Conclusions
This study found that fasting triglycerides in the upper normal range were associated with an increased risk of diabetes mortality. The optimal cutoff of triglycerides to classify diabetes mortality was 94.5 mg/dL, below the current threshold of 150 mg/dL. Individuals with triglyceride levels above the newly determined cutoff (i.e., 94.5 mg/dL) faced a 43% higher risk of diabetes mortality compared to those below the cutoff, underscoring the importance of close monitoring for diabetes and associated complications in such individuals.
Author Contributions
Y.W. solely contributed to all aspects of this study.
Funding
Y.W. was supported by a grant from the National Health and Medical Research Council of Australia (1062671).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the NHANES Institutional Review Board. Approval Code: NHANES Protocol #98-12, #2005-06, and #2011-17.
Informed Consent Statement
All participants provided written informed consent. The participants’ records were anonymized before being accessed by the author.
Data Availability Statement
All data in the current analysis are publicly available on the NHANES website (https://www.cdc.gov/nchs/nhanes/index.htm).
Acknowledgments
None.
Conflicts of Interest
The author declares no conflicts of interest.
References
- Lin, X.; Xu, Y.; Pan, X.; Xu, J.; Ding, Y.; Sun, X.; Song, X.; Ren, Y.; Shan, P.-F. Global, regional, and national burden and trend of diabetes in 195 countries and territories: an analysis from 1990 to 2025. Sci. Rep. 2020, 10, 14790. [Google Scholar] [CrossRef]
- Xie, J.; Wang, M.; Long, Z.; Ning, H.; Li, J.; Cao, Y.; Liao, Y.; Liu, G.; Wang, F.; Pan, A. Global burden of type 2 diabetes in adolescents and young adults, 1990-2019: systematic analysis of the Global Burden of Disease Study 2019. BMJ 2022, 379, e072385. [Google Scholar] [CrossRef]
- Khan, M.A.B.; Hashim, M.J.; King, J.K.; Govender, R.D.; Mustafa, H.; Al Kaabi, J. Epidemiology of Type 2 Diabetes - Global Burden of Disease and Forecasted Trends. J Epidemiol Glob Health 2020, 10, 107–111. [Google Scholar] [CrossRef]
- Simha, V. Management of hypertriglyceridemia. BMJ 2020, 371, m3109. [Google Scholar] [CrossRef]
- Al-Mawali, A.; Al-Harrasi, A.; Jayapal, S.K.; Morsi, M.; Pinto, A.D.; Al-Shekaili, W.; Al-Kharusi, H.; Al-Balushi, Z.; Idikula, J. Prevalence and risk factors of diabetes in a large community-based study in the Sultanate of Oman: STEPS survey 2017. BMC Endocr. Disord. 2021, 21, 42. [Google Scholar] [CrossRef]
- Urrutia, I.; Martín-Nieto, A.; Martínez, R.; Casanovas-Marsal, J.O.; Aguayo, A.; Del Olmo, J.; Arana, E.; Fernandez-Rubio, E.; Castaño, L.; Gaztambide, S. Incidence of diabetes mellitus and associated risk factors in the adult population of the Basque country, Spain. Sci. Rep. 2021, 11, 3016. [Google Scholar] [CrossRef]
- Dai, C.Y.; Huang, J.F.; Hsieh, M.Y.; Lee, L.P.; Hou, N.J.; Yu, M.L.; Chuang, W.L. Links between triglyceride levels, hepatitis C virus infection and diabetes. Gut 2007, 56, 1167–1168. [Google Scholar] [CrossRef]
- Wang, Y. Higher fasting triglyceride predicts higher risks of diabetes mortality in US adults. Lipids Health Dis. 2021, 20, 181. [Google Scholar] [CrossRef] [PubMed]
- D'Agostino, R.B., Jr.; Hamman, R.F.; Karter, A.J.; Mykkanen, L.; Wagenknecht, L.E.; Haffner, S.M. Cardiovascular disease risk factors predict the development of type 2 diabetes: the insulin resistance atherosclerosis study. Diabetes Care 2004, 27, 2234–2240. [Google Scholar] [CrossRef] [PubMed]
- Wilson, P.W.; Meigs, J.B.; Sullivan, L.; Fox, C.S.; Nathan, D.M.; D'Agostino, R.B., Sr. Prediction of incident diabetes mellitus in middle-aged adults: the Framingham Offspring Study. Arch. Intern. Med. 2007, 167, 1068–1074. [Google Scholar] [CrossRef] [PubMed]
- Fujihara, K.; Sugawara, A.; Heianza, Y.; Sairenchi, T.; Irie, F.; Iso, H.; Doi, M.; Shimano, H.; Watanabe, H.; Sone, H.; et al. Utility of the triglyceride level for predicting incident diabetes mellitus according to the fasting status and body mass index category: the Ibaraki Prefectural Health Study. J Atheroscler Thromb 2014, 21, 1152–1169. [Google Scholar] [CrossRef]
- Klimentidis, Y.C.; Chougule, A.; Arora, A.; Frazier-Wood, A.C.; Hsu, C.H. Triglyceride-Increasing Alleles Associated with Protection against Type-2 Diabetes. PLoS Genet. 2015, 11, e1005204. [Google Scholar] [CrossRef]
- Tirosh, A.; Shai, I.; Bitzur, R.; Kochba, I.; Tekes-Manova, D.; Israeli, E.; Shochat, T.; Rudich, A. Changes in triglyceride levels over time and risk of type 2 diabetes in young men. Diabetes Care 2008, 31, 2032–2037. [Google Scholar] [CrossRef]
- Beshara, A.; Cohen, E.; Goldberg, E.; Lilos, P.; Garty, M.; Krause, I. Triglyceride levels and risk of type 2 diabetes mellitus: a longitudinal large study. J. Investig. Med. 2016, 64, 383–387. [Google Scholar] [CrossRef]
- Wang, Y.; Liu, H.; Ma, S.; Qian, T.; Sun, H.; Xu, Q.; Hou, X.; Hu, W.; Zhang, G.; Jelinic, M.; et al. Normal Triglycerides Are Positively Associated with Plasma Glucose and Risk for Type 2 Diabetes in Chinese Adults. Preprints 2024, 2024011501. [Google Scholar] [CrossRef]
- Zhu, B.; Wang, J.; Chen, K.; Yan, W.; Wang, A.; Wang, W.; Gao, Z.; Tang, X.; Yan, L.; Wan, Q.; et al. A high triglyceride glucose index is more closely associated with hypertension than lipid or glycemic parameters in elderly individuals: a cross-sectional survey from the Reaction Study. Cardiovasc. Diabetol. 2020, 19, 112. [Google Scholar] [CrossRef]
- Wang, Y.; Fang, Y.; Magliano, D.J.; Charchar, F.J.; Sobey, C.G.; Drummond, G.R.; Golledge, J. Fasting triglycerides are positively associated with cardiovascular mortality risk in people with diabetes. Cardiovasc. Res. 2023, 119, 826–834. [Google Scholar] [CrossRef]
- Wadström, B.N.; Pedersen, K.M.; Wulff, A.B.; Nordestgaard, B.G. Elevated remnant cholesterol, plasma triglycerides, and cardiovascular and non-cardiovascular mortality. Eur. Heart J. 2023, 44, 1432–1445. [Google Scholar] [CrossRef] [PubMed]
- Lindman, A.S.; Veierød, M.B.; Tverdal, A.; Pedersen, J.I.; Selmer, R. Nonfasting triglycerides and risk of cardiovascular death in men and women from the Norwegian Counties Study. Eur. J. Epidemiol. 2010, 25, 789–798. [Google Scholar] [CrossRef] [PubMed]
- Shankar, A.; Mitchell, P.; Rochtchina, E.; Wang, J.J. The association between circulating white blood cell count, triglyceride level and cardiovascular and all-cause mortality: population-based cohort study. Atherosclerosis 2007, 192, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.Q.; Liu, X.C.; Lo, K.; Feng, Y.Q.; Zhang, B. A dose-independent association of triglyceride levels with all-cause mortality among adults population. Lipids Health Dis. 2020, 19, 225. [Google Scholar] [CrossRef] [PubMed]
- Pikhart, H.; Hubáček, J.A.; Peasey, A.; Kubínová, R.; Bobák, M. Association between fasting plasma triglycerides, all-cause and cardiovascular mortality in Czech population. Results from the HAPIEE study. Physiol. Res. 2015, 64, S355-361. [Google Scholar] [CrossRef] [PubMed]
- Lipoprotein Analytical Laboratory. Total Cholesterol, HDL-Cholesterol, Triglycerides, and LDL-Cholesterol: Laboratory Procedure Manual. Available online: https://wwwn.cdc.gov/nchs/data/nhanes/1999-2000/labmethods/lab13_met_lipids.pdf (accessed on 5 February 2024).
- Wang, Y.; Fang, Y.; Witting, P.K.; Charchar, F.J.; Sobey, C.G.; Drummond, G.R.; Golledge, J. Dietary fatty acids and mortality risk from heart disease in US adults: an analysis based on NHANES. Sci. Rep. 2023, 13, 1614. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y. Definition, prevalence, and risk factors of low sex hormone-binding globulin in US adults. J Clin Endocrinol Metab 2021, 106, e3946–e3956. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Fang, Y. Late non-fasting plasma glucose predicts cardiovascular mortality independent of hemoglobin A1c. Sci. Rep. 2022, 12, 7778. [Google Scholar] [CrossRef] [PubMed]
- Jungo, K.T.; Meier, R.; Valeri, F.; Schwab, N.; Schneider, C.; Reeve, E.; Spruit, M.; Schwenkglenks, M.; Rodondi, N.; Streit, S. Baseline characteristics and comparability of older multimorbid patients with polypharmacy and general practitioners participating in a randomized controlled primary care trial. BMC Fam. Pract. 2021, 22, 123. [Google Scholar] [CrossRef] [PubMed]
- Qian, T.; Sun, H.; Xu, Q.; Hou, X.; Hu, W.; Zhang, G.; Drummond, G.R.; Sobey, C.G.; Charchar, F.J.; Golledge, J.; et al. Hyperuricemia is independently associated with hypertension in men under 60 years in a general Chinese population. J. Hum. Hypertens. 2021, 35, 1020–1028. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y. Stage 1 hypertension and risk of cardiovascular disease mortality in United States adults with or without diabetes. J. Hypertens. 2022, 40, 794–803. [Google Scholar] [CrossRef]
- Harrell, F.E. Cox Proportional Hazards Regression Model. In Regression Modeling Strategies: With Applications to Linear Models, Logistic Regression, and Survival Analysis; Harrell, F.E., Ed.; Springer New York: New York, NY, 2001; pp. 465–507. [Google Scholar] [CrossRef]
- Azur, M.J.; Stuart, E.A.; Frangakis, C.; Leaf, P.J. Multiple imputation by chained equations: what is it and how does it work? Int. J. Methods Psychiatr. Res. 2011, 20, 40–49. [Google Scholar] [CrossRef]
- Kubo, Y.; Noguchi, T.; Hayashi, T.; Tomiyama, N.; Ochi, A.; Hayashi, H. Eating alone and weight change in community-dwelling older adults during the coronavirus pandemic: A longitudinal study. Nutrition 2022, 102, 111697. [Google Scholar] [CrossRef]
- West, R.M. Best practice in statistics: The use of log transformation. Ann. Clin. Biochem. 2022, 59, 162–165. [Google Scholar] [CrossRef]
- Wang, Y.; Fang, Y. Postabsorptive homeostasis model assessment for insulin resistance is a reliable biomarker for cardiovascular disease mortality and all-cause mortality. Diabetes Epidemiology and Management 2021, 6, 100045. [Google Scholar] [CrossRef]
- Unal, I. Defining an Optimal Cut-Point Value in ROC Analysis: An Alternative Approach. Comput. Math. Methods Med. 2017, 2017, 3762651. [Google Scholar] [CrossRef] [PubMed]
- Goel, M.K.; Khanna, P.; Kishore, J. Understanding survival analysis: Kaplan-Meier estimate. Int J Ayurveda Res 2010, 1, 274–278. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhang, W.; Qian, T.; Sun, H.; Xu, Q.; Hou, X.; Hu, W.; Zhang, G.; Drummond, G.R.; Sobey, C.G.; et al. Reduced renal function may explain the higher prevalence of hyperuricemia in older people. Sci. Rep. 2021, 11, 1302. [Google Scholar] [CrossRef] [PubMed]
- Kametani, T.; Koshida, H.; Nagaoka, T.; Miyakoshi, H. Hypertriglyceridemia is an independent risk factor for development of impaired fasting glucose and diabetes mellitus: a 9-year longitudinal study in Japanese. Intern. Med. 2002, 41, 516–521. [Google Scholar] [CrossRef]
- Shulman, G.I. Cellular mechanisms of insulin resistance. J. Clin. Invest. 2000, 106, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Jensen, C.B.; Storgaard, H.; Holst, J.J.; Dela, F.; Madsbad, S.; Vaag, A.A. Insulin secretion and cellular glucose metabolism after prolonged low-grade intralipid infusion in young men. J Clin Endocrinol Metab 2003, 88, 2775–2783. [Google Scholar] [CrossRef] [PubMed]
- Phielix, E.; Begovatz, P.; Gancheva, S.; Bierwagen, A.; Kornips, E.; Schaart, G.; Hesselink, M.K.C.; Schrauwen, P.; Roden, M. Athletes feature greater rates of muscle glucose transport and glycogen synthesis during lipid infusion. JCI insight 2019, 4, e127928. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Zeng, F.-F.; Liu, Z.-M.; Zhang, C.-X.; Ling, W.-H.; Chen, Y.-M. Effects of blood triglycerides on cardiovascular and all-cause mortality: a systematic review and meta-analysis of 61 prospective studies. Lipids Health Dis. 2013, 12, 159–159. [Google Scholar] [CrossRef]
- Patel, R.S.; Pasea, L.; Soran, H.; Downie, P.; Jones, R.; Hingorani, A.D.; Neely, D.; Denaxas, S.; Hemingway, H. Elevated plasma triglyceride concentration and risk of adverse clinical outcomes in 1.5 million people: a CALIBER linked electronic health record study. Cardiovasc. Diabetol. 2022, 21, 102. [Google Scholar] [CrossRef]
- Klempfner, R.; Erez, A.; Sagit, B.-Z.; Goldenberg, I.; Fisman, E.; Kopel, E.; Shlomo, N.; Israel, A.; Tenenbaum, A. Elevated Triglyceride Level Is Independently Associated With Increased All-Cause Mortality in Patients With Established Coronary Heart Disease. Circ. Cardiovasc. Qual. Outcomes 2016, 9, 100–108. [Google Scholar] [CrossRef]
- Miselli, M.-A.; Nora, E.D.; Passaro, A.; Tomasi, F.; Zuliani, G. Plasma triglycerides predict ten-years all-cause mortality in outpatients with type 2 diabetes mellitus: a longitudinal observational study. Cardiovasc. Diabetol. 2014, 13, 135. [Google Scholar] [CrossRef]
- Thomsen, M.; Varbo, A.; Tybjærg-Hansen, A.; Nordestgaard, B.G. Low Nonfasting Triglycerides and Reduced All-Cause Mortality: A Mendelian Randomization Study. Clin. Chem. 2014, 60, 737–746. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.S.; Hong, S.; Han, K.; Park, C.Y. Fenofibrate add-on to statin treatment is associated with low all-cause death and cardiovascular disease in the general population with high triglyceride levels. Metabolism 2022, 137, 155327. [Google Scholar] [CrossRef] [PubMed]
- Fang, Y.; Wang, Y. Fasting status modifies the association between triglyceride and all-cause mortality: A cohort study. Health Sci Rep 2022, 5, e642. [Google Scholar] [CrossRef]
- Tomita, Y.; Sakata, S.; Arima, H.; Yamato, I.; Ibaraki, A.; Ohtsubo, T.; Matsumura, K.; Fukuhara, M.; Goto, K.; Kitazono, T. Relationship between casual serum triglyceride levels and the development of hypertension in Japanese. J. Hypertens. 2021, 39, 677–682. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Íñigo, L.; Navarro-González, D.; Pastrana-Delgado, J.; Fernández-Montero, A.; Martínez, J.A. Association of triglycerides and new lipid markers with the incidence of hypertension in a Spanish cohort. J. Hypertens. 2016, 34, 1257–1265. [Google Scholar] [CrossRef] [PubMed]
- He, D.; Fan, F.; Jia, J.; Jiang, Y.; Sun, P.; Wu, Z.; Li, J.; Huo, Y.; Zhang, Y. Lipid profiles and the risk of new-onset hypertension in a Chinese community-based cohort. Nutrition, Metabolism and Cardiovascular Diseases 2021, 31, 911–920. [Google Scholar] [CrossRef] [PubMed]
- Paynter, N.P.; Sesso, H.D.; Conen, D.; Otvos, J.D.; Mora, S. Lipoprotein subclass abnormalities and incident hypertension in initially healthy women. Clin. Chem. 2011, 57, 1178–1187. [Google Scholar] [CrossRef] [PubMed]
- Goto, K. Triglyceride, an Independent Risk Factor for New-Onset Hypertension: A Perspective. Endocr. Metab. Immune Disord. Drug Targets 2023, 23, 1483–1490. [Google Scholar] [CrossRef]
- Szili-Torok, T.; Xu, Y.; de Borst, M.H.; Bakker, S.J.L.; Tietge, U.J.F. Normal Fasting Triglyceride Levels and Incident Hypertension in Community-Dwelling Individuals Without Metabolic Syndrome. J. Am. Heart. Assoc. 2023, 12, e028372. [Google Scholar] [CrossRef] [PubMed]
- Kasai, T.; Miyauchi, K.; Yanagisawa, N.; Kajimoto, K.; Kubota, N.; Ogita, M.; Tsuboi, S.; Amano, A.; Daida, H. Mortality risk of triglyceride levels in patients with coronary artery disease. Heart 2013, 99, 22–29. [Google Scholar] [CrossRef] [PubMed]
- van den Berg, M.J.; van der Graaf, Y.; de Borst, G.J.; Kappelle, L.J.; Nathoe, H.M.; Visseren, F.L.J. Low-Density Lipoprotein Cholesterol, Non-High-Density Lipoprotein Cholesterol, Triglycerides, and Apolipoprotein B and Cardiovascular Risk in Patients With Manifest Arterial Disease. Am. J. Cardiol. 2016, 118, 804–810. [Google Scholar] [CrossRef] [PubMed]
- Chan, W.B.; Tong, P.C.; Chow, C.C.; So, W.Y.; Ng, M.C.; Ma, R.C.; Osaki, R.; Cockram, C.S.; Chan, J.C. Triglyceride predicts cardiovascular mortality and its relationship with glycaemia and obesity in Chinese type 2 diabetic patients. Diabetes Metab. Res. Rev. 2005, 21, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Yamagishi, K.; Iso, H.; Sairenchi, T.; Irie, F.; Takizawa, N.; Koba, A.; Tomizawa, T.; Ota, H. Diabetes Mellitus Modifies the Association of Serum Triglycerides with Ischemic Cardiovascular Disease Mortality: The Ibaraki Prefectural Health Study (IPHS). J Atheroscler Thromb 2022, 29, 1319–1327. [Google Scholar] [CrossRef]
- Miao, C.Y.; Ye, X.F.; Zhang, W.; Sheng, C.S.; Huang, Q.F.; Wang, J.G. Serum triglycerides concentration in relation to total and cardiovascular mortality in an elderly Chinese population. J Geriatr Cardiol 2022, 19, 603–609. [Google Scholar] [CrossRef] [PubMed]
- Toth, P.P.; Philip, S.; Hull, M.; Granowitz, C. Association of Elevated Triglycerides With Increased Cardiovascular Risk and Direct Costs in Statin-Treated Patients. Mayo Clin. Proc. 2019, 94, 1670–1680. [Google Scholar] [CrossRef]
- Toth, P.P.; Granowitz, C.; Hull, M.; Liassou, D.; Anderson, A.; Philip, S. High Triglycerides Are Associated With Increased Cardiovascular Events, Medical Costs, and Resource Use: A Real-World Administrative Claims Analysis of Statin-Treated Patients With High Residual Cardiovascular Risk. J. Am. Heart. Assoc. 2018, 7, e008740. [Google Scholar] [CrossRef]
- Yang, X.H.; Tu, Q.M.; Li, L.; Guo, Y.P.; Wang, N.S.; Jin, H.M. Triglyceride-lowering therapy for the prevention of cardiovascular events, stroke, and mortality in patients with diabetes: A meta-analysis of randomized controlled trials. Atherosclerosis 2023, 117187. [Google Scholar] [CrossRef]
- Grundy, S.M.; Stone, N.J.; Bailey, A.L.; Beam, C.; Birtcher, K.K.; Blumenthal, R.S.; Braun, L.T.; Ferranti, S.d.; Faiella-Tommasino, J.; Forman, D.E.; et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 139, e1082–e1143. [Google Scholar] [CrossRef]
- Jeppesen, J.ø.; Hein, H.O.; Suadicani, P.; Gyntelberg, F. Triglyceride Concentration and Ischemic Heart Disease. Circulation 1998, 97, 1029–1036. [Google Scholar] [CrossRef] [PubMed]
- Tikhonoff, V.; Casiglia, E.; Virdis, A.; Grassi, G.; Angeli, F.; Arca, M.; Barbagallo, C.M.; Bombelli, M.; Cappelli, F.; Cianci, R.; et al. Prognostic Value and Relative Cutoffs of Triglycerides Predicting Cardiovascular Outcome in a Large Regional-Based Italian Database. J. Am. Heart. Assoc. 2024, 13, e030319. [Google Scholar] [CrossRef]
- Menke, A.; Muntner, P.; Batuman, V.; Silbergeld, E.K.; Guallar, E. Blood lead below 0.48 micromol/L (10 microg/dL) and mortality among US adults. Circulation 2006, 114, 1388–1394. [Google Scholar] [CrossRef] [PubMed]
- MacMahon, S.; Peto, R.; Cutler, J.; Collins, R.; Sorlie, P.; Neaton, J.; Abbott, R.; Godwin, J.; Dyer, A.; Stamler, J. Blood pressure, stroke, and coronary heart disease. Part 1, Prolonged differences in blood pressure: prospective observational studies corrected for the regression dilution bias. Lancet 1990, 335, 765–774. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Kaplan-Meier survival curves of diabetes mortality. Participants were stratified according to the quartiles of triglyceride levels. Q, quartile; TG, triglyceride.
Figure 1.
Kaplan-Meier survival curves of diabetes mortality. Participants were stratified according to the quartiles of triglyceride levels. Q, quartile; TG, triglyceride.
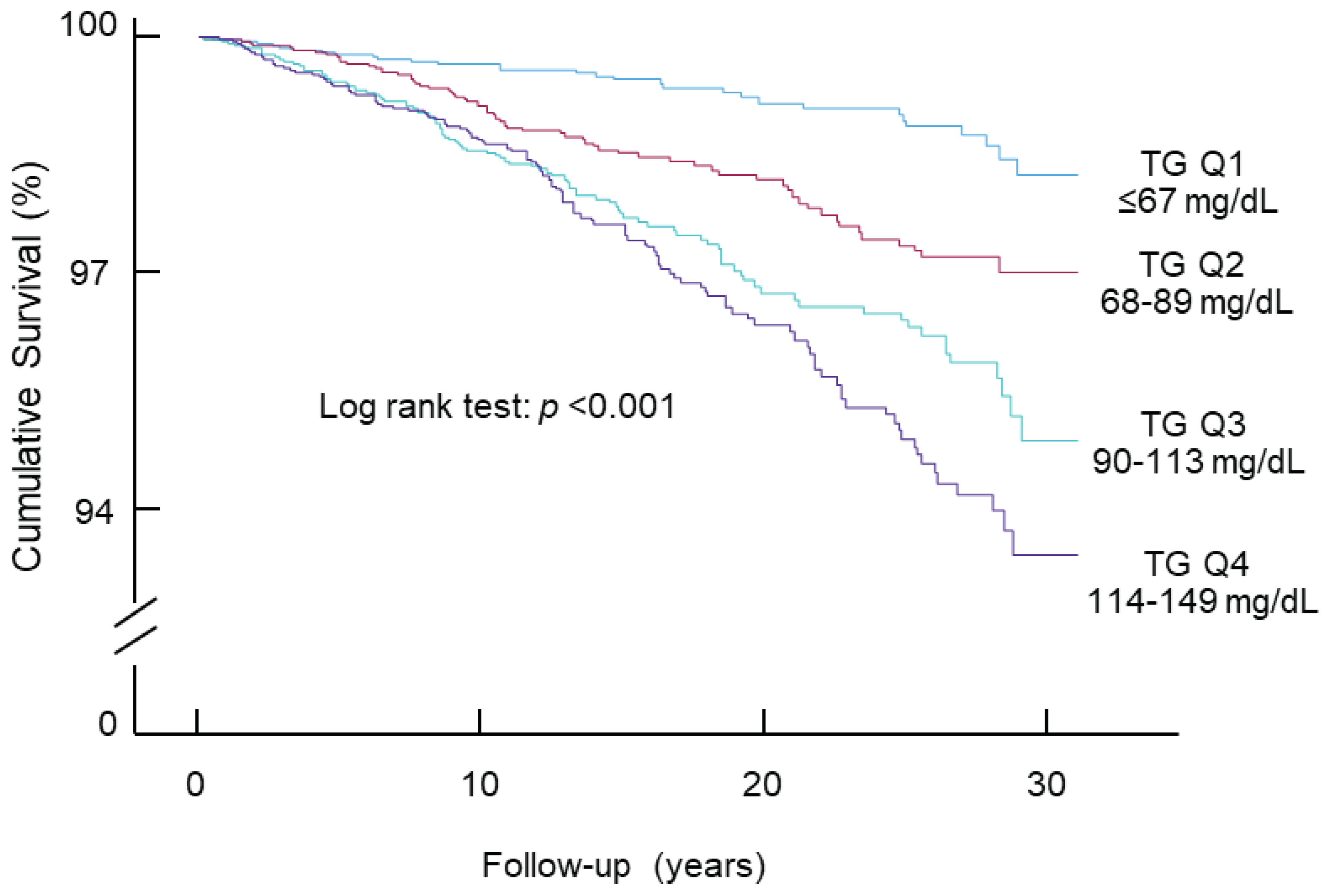
Figure 2.
Determination and validation of cutoff of triglycerides for diabetes mortality. A, ROC curve of triglycerides to classify diabetes mortality. The optimal cutoff was 94.5 mg/dL, with a sensitivity of 65%, specificity of 56%, and an area under the curve (AUC) of 0.623. B, Kaplan-Meier survival curves. C, Diabetes mortality risk associated with triglyceride categories. The analysis was adjusted for age, sex, ethnicity, body mass index, education, poverty-income ratio, survey period, physical activity, alcohol consumption, smoking status, systolic blood pressure, total cholesterol, HDL cholesterol, and family history of diabetes. CI, confidence interval; HR, hazard ratio; No., number; ROC, receiver operating characteristic; TG, triglyceride.
Figure 2.
Determination and validation of cutoff of triglycerides for diabetes mortality. A, ROC curve of triglycerides to classify diabetes mortality. The optimal cutoff was 94.5 mg/dL, with a sensitivity of 65%, specificity of 56%, and an area under the curve (AUC) of 0.623. B, Kaplan-Meier survival curves. C, Diabetes mortality risk associated with triglyceride categories. The analysis was adjusted for age, sex, ethnicity, body mass index, education, poverty-income ratio, survey period, physical activity, alcohol consumption, smoking status, systolic blood pressure, total cholesterol, HDL cholesterol, and family history of diabetes. CI, confidence interval; HR, hazard ratio; No., number; ROC, receiver operating characteristic; TG, triglyceride.
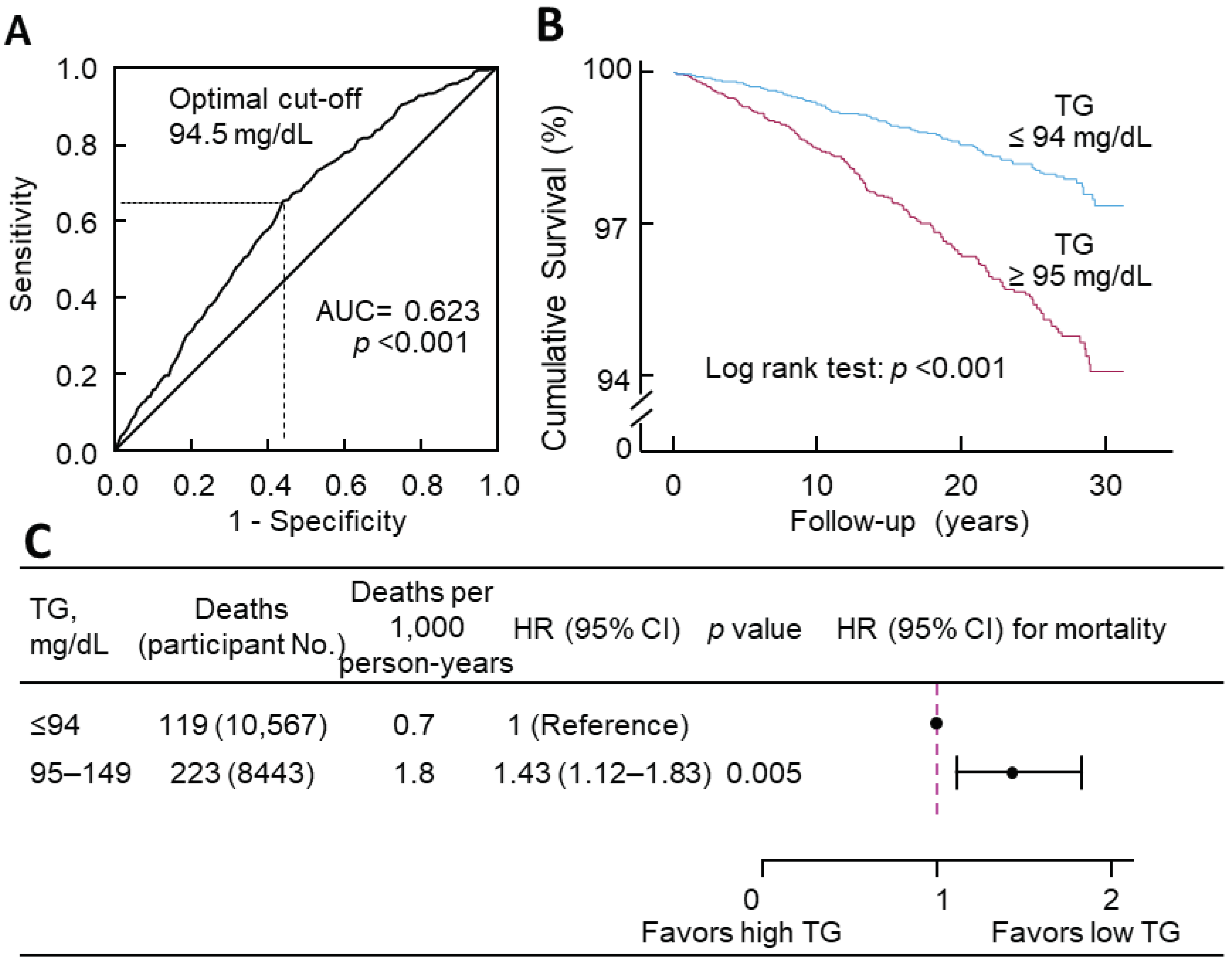

Table 1.
Baseline characteristics of 19,010 US adult participants with triglycerides within the normal range, stratified by observed triglyceride quartiles.
Table 1.
Baseline characteristics of 19,010 US adult participants with triglycerides within the normal range, stratified by observed triglyceride quartiles.
| Quartiles of triglycerides (range, mg/dL) | All | p | ||||
| Q1 (≤ 67) | Q2 (68–89) | Q3 (90–113) | Q4 (114–149) | |||
| Sample size | 4711 | 4798 | 4651 | 4850 | 19,010 | NA |
| Age, y, mean (SD) | 41 (17) | 47 (19) | 49 (19) | 51 (19) | 47 (19) | <0.001 |
| Sex (male), n (%) | 1995 (42) | 2178 (45) | 2225 (48) | 2369 (49) | 8767 (46) | <0.001 |
| Triglycerides, mg/dL, median (IQR) | 56 (47–62) | 79 (73–84) | 101 (95–107) | 129 (121–139) | 89 (68–114) | <0.001 |
| FPG, mg/dL, median (IQR) | 92 (87–99) | 95 (88–102) | 97 (90–105) | 99 (92–108) | 96 (89–104) | <0.001 |
| BMI, kg/m2, median (IQR) | 25 (22–28) | 26 (23–30) | 27 (24–31) | 28 (25–32) | 26 (23–30) | <0.001 |
| SBP, mm Hg, median (IQR) | 115 (106–126) | 118 (109–131) | 120 (111–133) | 123 (112–137) | 119 (109–132) | <0.001 |
| TC, mg/dL, median (IQR) | 173 (152–197) | 186 (164–212) | 194 (170–219) | 201 (177–229) | 188 (164–215) | <0.001 |
| HDL-C, mg/dL, median (IQR) | 59 (50–71) | 55 (46–65) | 52 (44–62) | 48 (41–58) | 54 (45–64) | <0.001 |
| Ethnicity, n (%) | ||||||
| Non-Hispanic white | 1774 (38) | 2027 (42) | 2071 (45) | 2307 (48) | 8179 (43) | <0.001 |
| Non-Hispanic black | 1733 (37) | 1389 (29) | 1053 (23) | 821 (17) | 4996 (26) | |
| Hispanic | 927 (20) | 1132 (24) | 1271 (27) | 1478 (31) | 4808 (25) | |
| Other | 277 (6) | 250 (5) | 256 (6) | 244 (5) | 1027 (5) | |
| Education, n (%) | ||||||
| < High School | 1133 (24) | 1391 (29) | 1497 (32) | 1662 (34) | 5683 (30) | <0.001 |
| High School | 1218 (26) | 1228 (26) | 1177 (25) | 1229 (25) | 4852 (26) | |
| > High School | 2353 (50) | 2153 (45) | 1964 (42) | 1945 (40) | 8415 (44) | |
| Unknown | 7 (0) | 26 (1) | 13 (0) | 14 (0) | 60 (0) | |
| Poverty-income ratio, n (%) | ||||||
| < 130% | 1281 (27) | 1359 (28) | 1314 (28) | 1370 (28) | 5324 (28) | 0.10 |
| 130%–349% | 1726 (37) | 1745 (36) | 1723 (37) | 1872 (39) | 7066 (37) | |
| ≥ 350% | 1315 (28) | 1290 (27) | 1218 (26) | 1248 (26) | 5071 (27) | |
| Unknown | 389 (8) | 404 (8) | 396 (9) | 360 (7) | 1549 (8) | |
| Physical activity, n (%) | ||||||
| Active | 1494 (32) | 1382 (29) | 1220 (26) | 1162 (24) | 5258 (28) | <0.001 |
| Insufficiently active | 1741 (37) | 1758 (37) | 1724 (37) | 1855 (38) | 7078 (37) | |
| Inactive | 1475 (31) | 1657 (35) | 1703 (37) | 1831 (38) | 6666 (35) | |
| Unknown | 1 (0) | 1 (0) | 4 (0) | 2 (0) | 8 (0) | |
| Alcohol consumption, n (%) | ||||||
| 0 drink/week | 722 (15) | 798 (17) | 815 (18) | 905 (19) | 3240 (17) | <0.001 |
| < 1 drink/week | 1092 (23) | 1073 (22) | 1051 (23) | 1100 (23) | 4316 (23) | |
| 1–6 drinks/week | 1135 (24) | 1032 (22) | 954 (21) | 906 (19) | 4027 (21) | |
| ≥ 7 drinks/week | 577 (12) | 617 (13) | 628 (14) | 599 (12) | 2421 (13) | |
| Unknown | 1185 (25) | 1278 (27) | 1203 (26) | 1340 (28) | 5006 (26) | |
| Smoking status, n (%) | ||||||
| Current smoker | 915 (19) | 1121 (23) | 1090 (23) | 1055 (22) | 4181 (22) | <0.001 |
| Past smoker | 904 (19) | 1053 (22) | 1140 (25) | 1307 (27) | 4404 (23) | |
| Non-smoker | 2890 (61) | 2620 (55) | 2417 (52) | 2485 (51) | 10,412 (55) | |
| Unknown | 2 (0) | 4 (0) | 4 (0) | 3 (0) | 13 (0) | |
| Family history of diabetes, n (%) | 0.35 | |||||
| Yes | 1930 (41) | 1964 (41) | 1968 (42) | 2087 (43) | 7949 (42) | |
| No | 2685 (57) | 2744 (57) | 2596 (56) | 2671 (55) | 10,696 (56) | |
| Unknown | 96 (2) | 90 (2) | 87 (2) | 92 (2) | 365 (2) | |
Abbreviations: BMI, body mass index; FPG, fasting plasma glucose; HDL-C, high-density lipoprotein cholesterol; IQR, interquartile range; NA, not applicable; Q, quartile; SBP, systolic blood pressure; SD, standard deviation; TC, total cholesterol.
Table 2.
Association of normal triglycerides (natural log transformed) with diabetes mortality in 19,010 participants.
Table 2.
Association of normal triglycerides (natural log transformed) with diabetes mortality in 19,010 participants.
| Models | HR | 95% CI | p |
| Model 1 | 4.24 | 2.98–6.03 | <0.001 |
| Model 2 | 2.21 | 1.54–3.19 | <0.001 |
| Model 3 | 1.70 | 1.17–2.48 | <0.01 |
| Model 4 | 1.66 | 1.10–2.51 | 0.02 |
| Model 5 | 1.57 | 1.04–2.38 | 0.03 |
CI, confidence interval; HR, hazard ratio. Model 1: not adjusted; Model 2: adjusted for age, sex, and ethnicity; Model 3: adjusted for all the factors in Model 2 plus body mass index, education, poverty-income ratio, and survey period; Model 4: adjusted for all the factors in Model 3 plus physical activity, alcohol consumption, smoking status, systolic blood pressure, total cholesterol, and HDL cholesterol; Model 5: adjusted for all the factors in Model 4 plus family history of diabetes.
Table 3.
Association of normal triglycerides in observed quartiles with diabetes mortality in 19,010 participants.
Table 3.
Association of normal triglycerides in observed quartiles with diabetes mortality in 19,010 participants.
| Models | Q1 | Q2 | Q3 | Q4 | ||||||
| HR | HR | 95% CI | p | HR | 95% CI | p | HR | 95% CI | p | |
| Model 1 | 1 | 2.18 | 1.44–3.29 | <0.001 | 3.44 | 2.33–5.08 | <0.001 | 4.17 | 2.84–6.11 | <0.001 |
| Model 2 | 1 | 1.66 | 1.10–2.52 | 0.02 | 2.12 | 1.43–3.14 | <0.001 | 2.33 | 1.58–3.44 | <0.001 |
| Model 3 | 1 | 1.46 | 0.97–2.22 | 0.07 | 1.81 | 1.22–2.70 | <0.01 | 1.84 | 1.24–2.73 | <0.01 |
| Model 4 | 1 | 1.44 | 0.94–2.20 | 0.09 | 1.81 | 1.20–2.74 | 0.01 | 1.80 | 1.18–2.75 | 0.01 |
| Model 5 | 1 | 1.42 | 0.93–2.16 | 0.11 | 1.77 | 1.17–2.67 | 0.01 | 1.72 | 1.12–2.63 | 0.01 |
CI, confidence interval; HR, hazard ratio; Q, quartile. Model 1: not adjusted; Model 2: adjusted for age, sex, and ethnicity; Model 3: adjusted for all the factors in Model 2 plus body mass index, education, poverty-income ratio, and survey period; Model 4: adjusted for all the factors in Model 3 plus physical activity, alcohol consumption, smoking status, systolic blood pressure, total cholesterol, and HDL cholesterol; Model 5: adjusted for all the factors in Model 4 plus family history of diabetes.
Table 4.
Sensitivity analyses of the association of normal triglycerides with diabetes mortality in 18,650 participants when participants with a follow-up time of less than 2 years (n = 360) were excluded.
Table 4.
Sensitivity analyses of the association of normal triglycerides with diabetes mortality in 18,650 participants when participants with a follow-up time of less than 2 years (n = 360) were excluded.
| Models | HR | 95% CI | p |
| Model 1 | 4.41 | 3.05–6.37 | <0.001 |
| Model 2 | 2.25 | 1.54–3.30 | <0.001 |
| Model 3 | 1.71 | 1.16–2.53 | 0.01 |
| Model 4 | 1.63 | 1.06–2.51 | 0.03 |
| Model 5 | 1.55 | 1.01–2.39 | 0.046 |
CI, confidence interval; HR, hazard ratio. Model 1: not adjusted; Model 2: adjusted for age, sex, and ethnicity; Model 3: adjusted for all the factors in Model 2 plus body mass index, education, poverty-income ratio, and survey period; Model 4: adjusted for all the factors in Model 3 plus physical activity, alcohol consumption, smoking status, systolic blood pressure, total cholesterol, and HDL cholesterol; Model 5: adjusted for all the factors in Model 4 plus family history of diabetes.
Table 5.
Sensitivity analysis of the association of normal triglycerides with diabetes mortality in 18,406 participants when the imputed data (n = 604) were excluded.
Table 5.
Sensitivity analysis of the association of normal triglycerides with diabetes mortality in 18,406 participants when the imputed data (n = 604) were excluded.
| Models | HR | 95% CI | p |
| Model 1 | 4.41 | 3.07–6.35 | <0.001 |
| Model 2 | 2.32 | 1.59–3.39 | <0.001 |
| Model 3 | 1.76 | 1.19–2.60 | <0.01 |
| Model 4 | 1.64 | 1.07–2.52 | 0.02 |
| Model 5 | 1.56 | 1.02–2.40 | 0.04 |
CI, confidence interval; HR, hazard ratio. Model 1: not adjusted; Model 2: adjusted for age, sex, and ethnicity; Model 3: adjusted for all the factors in Model 2 plus body mass index, education, poverty-income ratio, and survey period; Model 4: adjusted for all the factors in Model 3 plus physical activity, alcohol consumption, smoking status, systolic blood pressure, total cholesterol, and HDL cholesterol; Model 5: adjusted for all the factors in Model 4 plus family history of diabetes.
Table 6.
Association of normal triglycerides (natural log transformed) with hypertension mortality, CVD mortality2, and all-cause mortality in 19,010 participants.
Table 6.
Association of normal triglycerides (natural log transformed) with hypertension mortality, CVD mortality2, and all-cause mortality in 19,010 participants.
| Models | Hypertension mortality | CVD mortality | All-cause mortality | ||||||
| HR | 95% CI | p | HR | 95% CI | p | HR | 95% CI | p | |
| Model 1 | 2.54 | 1.99–3.25 | <0.001 | 2.43 | 2.08–2.83 | <0.001 | 2.35 | 2.14–2.57 | <0.001 |
| Model 2 | 1.19 | 0.92–1.54 | 0.19 | 1.08 | 0.92–1.28 | 0.34 | 1.10 | 1.00–1.21 | 0.05 |
| Model 3 | 1.06 | 0.81–1.38 | 0.70 | 1.01 | 0.85–1.19 | 0.93 | 1.10 | 1.00–1.22 | 0.05 |
| Model 4 | 1.07 | 0.79–1.43 | 0.68 | 0.97 | 0.80–1.17 | 0.72 | 1.15 | 1.03–1.28 | 0.01 |
| Model 5 | 1.06 | 0.79–1.43 | 0.70 | 0.96 | 0.79–1.16 | 0.66 | 1.14 | 1.02–1.28 | 0.02 |
CI, confidence interval; CVD, cardiovascular disease; HR, hazard ratio. Model 1: not adjusted; Model 2: adjusted for age, sex, and ethnicity; Model 3: adjusted for all the factors in Model 2 plus body mass index, education, poverty-income ratio, and survey period; Model 4: adjusted for all the factors in Model 3 plus physical activity, alcohol consumption, smoking status, systolic blood pressure, total cholesterol, and HDL cholesterol; Model 5: adjusted for all the factors in Model 4 plus family history of diabetes.
Table 7.
Association of normal triglycerides in observed quartiles with hypertension mortality, CVD mortality, and all-cause mortality in 19,010 participants.
Table 7.
Association of normal triglycerides in observed quartiles with hypertension mortality, CVD mortality, and all-cause mortality in 19,010 participants.
| Models | Q1 | Q2 | Q3 | Q4 | ||||||
| HR | HR | 95% CI | p | HR | 95% CI | p | HR | 95% CI | p | |
| Hypertension mortality | ||||||||||
|
Model 1 |
1 | 1.65 | 1.27–2.13 | <0.001 | 2.02 | 1.57–2.60 | <0.001 | 2.27 | 1.77–2.91 | <0.001 |
|
Model 2 |
1 | 1.18 | 0.91–1.53 | 0.23 | 1.14 | 0.89–1.48 | 0.30 | 1.16 | 0.9–1.49 | 0.25 |
|
Model 3 |
1 | 1.11 | 0.85–1.44 | 0.46 | 1.06 | 0.82–1.37 | 0.68 | 1.04 | 0.81–1.35 | 0.75 |
|
Model 4 |
1 | 1.11 | 0.85–1.45 | 0.46 | 1.05 | 0.80–1.38 | 0.74 | 1.04 | 0.79–1.39 | 0.77 |
|
Model 5 |
1 | 1.11 | 0.85–1.45 | 0.46 | 1.05 | 0.80–1.37 | 0.75 | 1.04 | 0.78–1.38 | 0.79 |
| CVD mortality | ||||||||||
|
Model 1 |
1 | 1.66 | 1.41–1.96 | <0.001 | 2.06 | 1.75–2.42 | <0.001 | 2.25 | 1.92–2.64 | <0.001 |
|
Model 2 |
1 | 1.16 | 0.98–1.37 | 0.08 | 1.13 | 0.96–1.32 | 0.16 | 1.11 | 0.94–1.30 | 0.22 |
|
Model 3 |
1 | 1.14 | 0.96–1.35 | 0.13 | 1.09 | 0.93–1.29 | 0.29 | 1.05 | 0.89–1.24 | 0.55 |
|
Model 4 |
1 | 1.12 | 0.95–1.33 | 0.19 | 1.07 | 0.90–1.27 | 0.45 | 1.01 | 0.85–1.22 | 0.88 |
|
Model 5 |
1 | 1.12 | 0.94–1.33 | 0.20 | 1.07 | 0.90–1.27 | 0.46 | 1.01 | 0.84–1.21 | 0.94 |
| All-cause mortality | ||||||||||
|
Model 1 |
1 | 1.59 | 1.44–1.75 | <0.001 | 1.86 | 1.70–2.05 | <0.001 | 2.16 | 1.98–2.37 | <0.001 |
|
Model 2 |
1 | 1.13 | 1.03–1.25 | 0.01 | 1.06 | 0.97–1.17 | 0.23 | 1.10 | 1.00–1.21 | 0.04 |
|
Model 3 |
1 | 1.14 | 1.04–1.26 | 0.01 | 1.07 | 0.98–1.18 | 0.15 | 1.11 | 1.01–1.22 | 0.03 |
|
Model 4 |
1 | 1.16 | 1.05–1.28 | <0.01 | 1.10 | 1.00–1.22 | 0.06 | 1.15 | 1.03–1.27 | 0.01 |
|
Model 5 |
1 | 1.15 | 1.05–1.27 | <0.01 | 1.10 | 0.99–1.21 | 0.07 | 1.14 | 1.03–1.27 | 0.01 |
CI, confidence interval; CVD, cardiovascular disease; HR, hazard ratio; Q, quartile. Model 1: not adjusted; Model 2: adjusted for age, sex, and ethnicity; Model 3: adjusted for all the factors in Model 2 plus body mass index, education, poverty-income ratio, and survey period; Model 4: adjusted for all the factors in Model 3 plus physical activity, alcohol consumption, smoking status, systolic blood pressure, total cholesterol, and HDL cholesterol; Model 5: adjusted for all the factors in Model 4 plus family history of diabetes.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



