
Submitted:
08 February 2024
Posted:
13 February 2024
You are already at the latest version
Abstract
Diabetes mellitus is one of the most common endocrinopathies, estimated to affect about 5.4% of the world's population around 2025. It is thought that nearly a third of diabetic patients have some type of skin condition. Frequently, the cutaneous effects of this heterogeneous syndrome are ac-curately detected late in the progressive form of the disease. The main objective of the present study was to identify the main cellular characteristics of the cutaneous microenvironment in exper- imentally induced diabetes mellitus. Skin fragments were harvested from adult white Wistar rats of both sexes, with the weight of 200 g, 12 weeks after streptozotocin diabetes was induced. In parallel with histopathological diagnosis by using hematoxylin and eosine staining, samples were processed by transmission electron microscopy technique and examined with a Philips CM100 microscope. In the apparently macroscopically unchanged tegument, photon microscopy revealed both progres ive thinning of the epidermis in the early stages of diabetes and a significant process of fibrosis and collagen hyalinization in the dermis. In addition, in the early stages, the electron microscopic study provided ultrastructural details characteristic of a senescent phenotype with reduced cell proliferation. The morphological changes in the skin may be the first signs of disruption of carbohydrate metabolism and in the case of established diabetes may reflect its progression and the efficacy of therapy.
Keywords:
streptozotocin diabetes
; ultrastructural diagnosis
; insulin resistance
1. Introduction
Worldwide, diabetes is one of the most common endocrinopathies, with significant biological impact on all tissue types. Its incidence is increasing exponentially, which is why it is expected that by 2030 there will be approximately 350 million cases. In addi- tion, poor diagnostic and therapeutic management due to the low volume of specific studies has a negative impact both from a clinico-morphological and developmental perspective. [1,2,3].
In recent decades, the dynamics of the details on skin structure theorisation have shown accelerated kinetics involving the accumulation of notions related to histological aspects in an integrated form. These are corroborated with the results of studies in cutaneous molecular biology, biochemistry, immunology, physiology and skin biophysics [4,5,6]. In this context, the idea that skin is a complex organ, consisting of several cell types and extracellular components, grouped in several layers: epidermis, dermis and hypodermis, is supported [1,2,3,4,5,6,7].
Diabetes mellitus is a heterogeneous syndrome characterised by a complex disorder of the body's energy metabolism, affecting the utilisation of carbohydrates, lipids and pro-teins as well as other metabolisms. These alterations arise from an obligatory insulin se- cretory defect, sometimes associated with a degree of peripheral insulin resistance. Through the biochemical changes that these two disorders bring about, a significant cel-lular dysfunction occurs, followed by irreversible anatomical damage in many tissues and organs. This explains the clinico-pathological heterogeneity of this syndrome [3,6,7,8,9].
Some of the integumentary damage associated with diabetes is a direct result of met-abolic changes such as hyperglycaemia and hyperlipidaemia. The progressive damage to the vascular, neurological and immune systems also contributes significantly to skin le-sions [9].
Compared to type 1 diabetes, which is associated with inflammatory skin lesions common to autoimmune conditions, type 2 is dominated by infection-specific lesions, an important cause of morbidity and mortality. In addition, this association implies the maintenance of a vicious circle in which infection is the result of uncontrollable hypergly-caemia, which aggravates the infectious processes [2,7,10].
Given the intervention of the cutaneous organ in the transduction of complex meta-bolic disorders induced by diabetes mellitus [11], the present study aimed to highlight histologically and ultrastructurally the spectrum of cutaneous changes in experimentally induced diabetes mellitus. A secondary objective was to correlate these changes with the age of diabetes onset and the occurrence of complications.
2. Materials and Methods
2.1. Experimental Model of Streptozotocin Diabetes
To obtain the necessary data we used the experimental model of streptozotocin dia-betes for which we used 48 adult Wistar white rats, aged between 8 months and 10 months, of both sexes, with the weight of 200 g. They were grouped into four groups, namely, 36 diabetic rats (male/female) and 12 control rats (male/female). The experiment lasted 12 weeks.
Diabetes was achieved by administering STZ (2-deoxy-2(3-methyl-nitrozo-ureido)- p-glucopyranose) in a single dose of 60mg/kg body weight, 1% solution in physiological serum, intraperitoneally (i.p.), rapidly after an 18-hour fast.
All experimental procedures on animals used in this study were in strict accordance with international ethical regulations. At the end of the study, the animals were euthanized after i.p. anaesthesia with ketamine 40 mg/kg body and pentobarbital 20 mg/kg body. A rapid, painless death by exsanguination after intracardiac puncture occurred. When vital signs were found to be absent, the animals were dissected for the collection of tegument fragments (Andrews E.J., AVMA Protocol for Euthanasia, 1993).
2.2 Protocol for Routine Staining with Hematoxylin-Eosin
Skin fragments were taken from the experimental animals for paraffin embedding. Skin fragments were harvested from the dorsal leg by scalpel blade biopsy. Subsequent to the sectioning and glass slide display steps, thin sections were deparaffinized with xylol, hydrated with 100%, 90% and 70% alcohol for 30 min each, washed with distilled water, stained with hematoxylin-eosin, mounted with Balsam of Canada and labelled. Examination and photography of the preparations was performed with Olympus BX40 microscope with Olympus E330 camera attached.
2.3 Standard Processing Technique for Transmission Electron Microscopy (TEM)
Tissue fragments were harvested very quickly by microdissection on ice and then processed following the next steps: fixation with 10% buffered glutaraldehyde (Sigma-Aldrich, Germany) and buffered osmium tetraoxide (Sigma-Aldrich, Germany) at 40 C; -washing for 1 h with 0.15M phosphate buffer solution at 40 C; dehydration with 30% ethyl alcohol for 10 min, 50% for 10 min, 70% for 10 min, 90% for 10 min and 2 baths with 100% alcohol for 20 min each; dehydration with 2 acetone baths for 20 min each; embedding in EPON 812 in gelatine capsules at laboratory temperature; fractionation; sectioning with Reichert OmU3 ultramicrotome; staining on metal grids; -contrast with uranyl acetate for 10 min and lead citrate for 3 min; labelling. For the examination of ultrathin sections, we used a Philips CM100 transmission electron microscope (TEM), equipped with a digital video camera with dedicated sensor and photographic system.
3. Results
3.1. Histological Aspects
All rats developed diabetes very quickly after streptozotocin injection. Plasma glucose concentrations three weeks after streptozotocin administration were 3.2 times higher than in control rats. A significant increase in blood glucose was observed from the second day after injection and the increase continued until the third week. After four weeks, transaminase activity (SGOT- serum glutamic-oxaloacetic transaminase and SGPT- serum glutamic-pyruvic transaminase) in diabetic rats was similar to the control group. There was no weight gain during the 3 weeks following streptozotocin adminis-tration.
At the level of the tegument apparently without macroscopic changes, photon mi- croscopy analysis of fine microscopic preparations stained with haematoxylin-eosin re- veals a medium-thickness epidermis, the presence of epithelial ridges and dermal papil lae, as well as hyperkeratosis, acanthosis and dermal fibrosis-like changes (Figure 1).
The stratum corneum showed a different thickness in the animals of the experi-mental batch, although the fragments were harvested from approximately the same re-gion. Thus, in our group there were cases where the epidermis showed a relatively thin, flaking stratum corneum and cases where it had an obvious thickness (Figure 2 a,b).
We have also identified cases with obvious reduction of keratinization, progressive thinning of the epidermis and numerical reduction of papillary ridges and their depth in the dermis. In a few cases, only isolated epithelial ridges were preserved among the papillary dermis structures (Figure 2a).
In the spinous layer there were evident aspects of acanthosis with different histopa-thological forms: in some cases the spinous layer showed moderate thickening and epithelial ridges of varying depths (Figure 3a,b); in other cases the epithelial ridges were deep with relatively thin dermal papillae between them (Figure 3a); in other cases, the process of acanthosis was very pronounced, with epidermal ridges showing significant depths and a germinative layer with areas of bistratification and frequent mitosis (Figure 3b).
In the dermis, especially in the deep dermis, we noticed an important process of fibrosis and collagen hyalinization. At the level of the dermal papillae, we observed the presence of capillaries with much thickened walls and shrunken lumen (Figure 3b).
3.2. Ultrastructural Aspects
Electron microscopic examination revealed changes in both the epidermis, confirm ing the results obtained in photon microscopy, as well as in connective tissue components. Thus, areas where the epidermis showed a relatively thin horny layer alternating with areas of medium and sometimes obvious thickness could be seen (Figure 4a and Table 1). Some cells have two well-represented nuclei, with closely associated heterochromatin, and sometimes hypertrophy of cellular organelles involved in cell synthesis and secretion processes, such as the rough endoplasmic reticulum and the Golgi apparatus (Figure 4b).
Analysis of the cell coupling sites reveals both a slight disorganisation of the desmo-120 somes and a reduction or loss of anchoring fibres at the basement membrane (Figure 5 ab).
The text continues here. As for the vascular endothelium, it is much thickened at the capillary level, with significant secondary narrowing of the lumen (Figure 6ab).
In the case of connective tissue, the frequent presence of enlarged fibroblasts was observed, in the cytoplasm of which a dilated endoplasmic reticulum and numerous vesicular, multilamellar structures were noted; at the level of the mitochondria accumulated especially at the basal pole, a disorganization of the internal structure was observed in many cases - a decrease in the mitochondrial ridges, an amorphous, weakly electron-dense material occupying the entire organelle (Figure 7a).
Another aspect noted is the lack of microtubules in the cytoplasm of these fibroblasts. Analysis of electron microscopy images shows disorganisation of the normal distribution of collagen fibres and the presence of broken elastin fibres separated by dense microfibrillar zones around their ends (Figure 7b).
In patients with experimental diabetes mellitus there are no significant differences between capillary and metarteriolar levels (88.9% vs 72.2%; p=0.137) of vascular endothelium; desmosomes and basement membrane (69.4% vs 63.9%; p=0.802) of junctional complexes and no significant differences between cellular organelles: mitochondrial structure (97.2%), rough endoplasmic reticulum (83.3%) and Golgi apparatus (86.1%) (p=0.201) (Tab. 1).
4. Discussion
Diabetes mellitus has become a problem of major importance for individuals, medicine and society because it is a common, multifactorial endocrinopathy with a chronic course that adversely affects survival and quality of life in the absence of appropriate management. Its impact is therefore multiple: epidemiological, biological, socio-familial, economic and political. For this reason, the healthcare system and society are obliged to develop new strategies and innovative approaches to meet the growing needs in diabetes management [2,9,10,11,12,13].
Over time, the skin of all diabetic patients is affected in one form or another. Early identification of elementary skin lesions is extremely valuable to the clinician. In this con- text, diabetic bullae, diabetic dermopathy, necrobiosis lipoidica diabeticorum and the waxy appearance of the skin in scleroderma-like syndrome can alert and warn the clini- cian to the presence of a diagnosis of diabetes. At the same time, eruptive xanthomas re- flect altered glycaemic status and lipid metabolism [6,7,8,14].
The prevalence of chronic complications and pathologies associated with diabetes is impressive. According to the results of recent research, one third of diabetic patients, re-gardless of the type of diagnosis, suffer from varying degrees of skin damage. Although the lesional polymorphism of the skin mainly accompanies the progressive stage of dia- betic disease, however, there is sufficient data demonstrating its important role in activat-ing destabilizing cellular mechanisms of systemic homeostasis. Therefore, it can be con-sidered that skin lesions may represent the first signs or even precede the manifestations of the primary disease by several years [4,5,6,7,10].
Currently, there are conflicting results on the quantification of cutaneous tissue dam-age specific to diabetic pathology-associated dermatoses. At the same time, several fa-vouring factors that potentiate the severity of skin lesions have been identified and proposed. These include the synergistic action of diabetes-specific metabolic imbalances and the molecular signalling cascade controlling cellular senescence. On the other hand, the relationship: ageing-increased oxidative stress-diabetes-associated neurovascular degen-erative complications is known. The latter have a strong negative impact on skin homeo-stasis [4,5,6,7,10]. Therefore, the present research included both 8-month-old and 10-month-old animals in the study to capture and highlight at morphological and functional levels the age-imbalance of carbohydrate metabolism imbalances. Thus, skin morphological changes can be correlated with the age of diabetes onset and the appearance of complications.
By administration of streptozotocin, a cytotoxic antibiotic synthesized by Streptomyces achromonogenes, insulinopenic diabetes mellitus (DZ) is triggered by selective en-docrino-chemical pancreatectomy, exclusively destroying the beta-Langerhans islet cells of the pancreas. As compared to surgical pancreatectomy the method has the advantage over surgical pancreatectomy of respecting the exocrine pancreas and therefore of not in-fluencing digestive processes. Diabetic permanent hyperglycaemia sets in 24-48 hours after the diabetogenic injection and may be definitive or regress spontaneously within a fewdays. We performed experimental diabetic induction to examine the stratum corneum and epidermis properties of these animals.
Our study is individualized by the identification of morphological lesions and cellu- lar features in the diabetic tegument, which have both functional and etiopathogenic implications for the healing of subsequent lesions [8,14,15,16,17,18].
The cases examined from a histopathological and ultrastructural point of view were represented by tegument samples collected from streptozotocin-induced diabetic rats 3 weeks after diabetes induction, the epidermis of the diabetic group was thicker than that of the control group (Figure 2), aspects which can be clinically translated by the onset of symptoms specific to skin senescence [3,15].
The results of the morphological study indicate alternating progressive thickening and thinning of the epidermis from the early stages of diabetes (Figure 1). Changes in cellular and/or nuclear volume as well as in cell proliferation and differentiation process affecting the functions of the integument are evident (Figure 4). In this context, thickening of the stratum corneum in areas subjected to mechanical stress is a risk factor for ulceration [14,15,16].
It is known that corneocyte surface area increases in senile xerosis, reflecting the rate of epidermal turnover [17]. In the diabetic group analysed in the present research, corne-ocyte surface area tended to increase above the control level, with an increase in the num-ber of keratinocytes in the stratum corneum (Figure 1). These results suggested that the turnover of epidermal cells in experimentally induced diabetic mice has a tendency to slow down (Figure 4) [17,18,19,20].
Some skin disorders associated with diabetes are direct consequences of metabolic changes, such as hyperglycaemia and hyperlipidaemia. Thus, hyperglycaemia leads to nonenzymatic glycosylation of many structural and regulatory proteins, causing acceler- ation of the formation of advanced glycosylation end-products in diabetes [19,20,21,22,23]. At the same time, studies have shown that the level of advanced glycosylation end-products in the skin is strongly correlated with retinopathy, nephropathy and other microvascular complications of diabetes [3,20,24,25].
Over the years, vascular lesions involving the microcirculation as well as the muscu- lar arteries and arterioles, as well as some venous changes have been noted. In the human integument, microcirculation can be classified into: thermoregulatory microcirculation, represented by arteriovenous shunts located at the boundary between the superficial dermis and the deep dermis, and nutritive vascularization, represented by capillary loops located in the dermal papillae [23,24].
The conceptualization of morphological changes specific to diabetic microangiopa- thy reveals two different aspects: the thickening of the basement membrane of capillaries and the presence of proliferative lesions evidenced in the lumen of arteries and arterioles (Figure 3) [3,24,25,26]. Basement membrane thickening is inversely related to the degree of metabolic control, being more important in subjects with poor metabolic control [3,20,24,27].
Contrary to studies in the literature which postulate that the manifestations in the integument occur in relation to the duration of diabetes progression and are associated with the development of microvascular complications, the present study leads to the hy-pothesis that ultrastructural morphological changes (Table 1) are present from the early stages of the onset of diabetic status [4,5,6,21].
Basement membrane thickening has also been reported in the research literature in skeletal muscle capillaries [7,8,28]. In this way, numerous cellular functions are affected, such as vascular permeability, cell adhesiveness, cell proliferation and differentiation, resulting in marked vascular dysfunction. In our study, we observed an evident thickening of the basement membrane in metaarterioles, capillaries (Figure 6), postcapillary venules, which sometimes appeared dilated with a rich haematic content. Endothelial cells and pericytes in capillaries, endothelial cells and smooth muscle fibres in metaarterioles are involved in the mechanism of basement membrane synthesis [7,8,28].
An important role in basement membrane thickening is played by metabolic disturb-ances that occur in these cells. Also, changes in capillary permeability may favour the formation of protein deposits in the basement membrane (Figure 5) [29,30,31,32,33].
These morphological changes affect endothelial synthesis capacity, endothelial per-meability and vasodilation capacity [9,10,34,35,36].
Analysis of the junctional complexes reveals a slight disorganization of the desmo- somes, which is clinically reflected by the appearance of vesicles and bubbles (Figure 5) [30].
The main function of fibroblasts is related to the ground substance, namely the ex-tracellular matrix. Thus, the fibroblast synthesises and degrades the main proteins that form the fibrillar and globular elements of the extracellular matrix in connective tissue. In ddition to collagen, it produces numerous types of matrix proteins such as laminin, fibronectin, vitronectin, thrombospondin [12,13].
Keratinocytes also secrete type IV and VII collagen, various types of laminins, pre-dominantly laminin 5, but also substances such as perlecan, polysaccharides components of proteoglycans. All these molecules actively control the synthesis and secretion of various pro-inflammatory cytokines and epithelial growth factors. In this way, it can explain the importance of the interdependence of cellular signalling evidenced between fibroblasts and keratinocytes, both in normal situations and in case of inflammation or in response to mechanical stimuli [3,23,36].
The morphological patterns revealed in the integument from the earliest stages of the development of diabetes are similar to the elements which are characteristic of senescent organisms. The presence of a degree of hypertrophy of cellular organelles involved in cell synthesis, in particular the rough endoplasmic reticulum, suggests increased protein synthesis while the frequently observed disorganisation of mitochondrial structure indicates deficient cellular energetics (Figure 4). On the other hand, degenerative aspects of collagen fibres are determined by the accumulation of glycation products from the early stages of diabetes onset (Figure 7).
In the case of the tissue harvested from the experimental diabetic mice, the total ab-sence or sporadic presence of microtubule-like cytoskeletal structures indicates disruption of intracellular vesicular trafficking and thus disruption of important cellular physiologi-cal processes such as receptor-mediated endocytosis, delivery of molecules synthesized in the rough endoplasmic reticulum to other cellular structures as well as impairment of proliferation and/or cell differentiation processes.
Glycosylation of collagen leads to an increase in intramolecular linkages, which in-creases stiffness and resistance to collagenase action but reduces resistance to tensile forces. Keratin is another protein subject to glycosylation, which favours hyperkeratosis that occurs in the integument and the risk of development of ulcers. The non-enzymatic glycosylation phenomenon makes a significant contribution to basement membrane thickening and to changes in permeability [4,16,34].
Electronomicroscopic evidence in the cytoplasm of fibroblasts of numerous vesicular bodies indicates a marked turnover of intracellular structures while the absence of microtubules or their sporadic presence could be one of the components of the mechanism responsible for the decreased proliferation rate observed [3,36].
On the other hand, the presence of fibroblasts with increased cell volume, indicating a hypertrophic phenotype, and the decreased proliferation index suggested by the existence of a reduced number of cells in the G2/M phases, are elements that are usually found in senescent organisms. This is in agreement with some literature data according to which diabetes prematurely induces degenerative changes that are usually associated with aging [4,5,6,37].
In some cases, the deep dermis has a pronounced sclerotic appearance. Collagen fi-bres are thick, long and with sinuous tracts, forming a dense, semi-coordinated connective tissue (Figure 7). In the presence of chronic hyperglycaemia, free glucose molecules spon-taneously attach to protein molecules in a process of non-enzymatic glycosylation, which has also been shown in other proteins, which leads to morphological and molecular changes that significantly influence some physical properties, such as flexibility [6,7,8,9,24].Early characterization and quantification of the pathophysiological details of diabetes mellitus and its complications correlates with more effective diagnostic and therapeutic methods, and implicitly with improved survival and quality of life [23,37,38,39,40].
5. Limitations of the Study
Hyperglycaemia is the consequence of the interdependence of two important abnor-malities: insulin resistance and insulin secretion disturbance. In addition, insulin resistance is an early change that precedes altered carbohydrate homeostasis and diabetes. The experimental model analysed is similar to insulinopenic type I diabetes. Therefore, the design of the present study did not allow the evaluation of the cutaneous microenvironment in insulin-resistant diabetes mellitus.
The skin is the mirror of diabetic pathology The integrative functions of the integu-ment, supported by mechanophysical and biochemical properties, are dependent on the topographic features of the tissue architecture. The integrity of the skin barrier depends on maintaining the balance of key determinants such as transepidermal water loss (TEWL), skin pH and stratum corneum lipid composition. At the same time, the acidic pH characteristic of glycated skin in type I diabetes is essential for stratum corneum lipid synthesis, epidermal differentiation and desquamation. To this end, skin fragments were harvested from the dorsal leg. The short time frame allocated to the current research did not make it possible to harvest skin fragments from different anatomical regions to comparatively analyse the morphological changes identified in experimentally induced diabetes.
6. Conclusions
Analysing the data of the present study, it can be stated that the morphological and molecular changes identified in the integument, in the context of the experimental model, represent the support of the etiopathogenic and anatomo-clinical variability characteristic of diabetes mellitus. In addition, they are not always conditioned by the age of diabetes progression.
The correlation of the results of the morphological study with the staging of the diabetic disease supports the idea that cellular changes in the skin epithelium may be the first signs of a disturbance in carbohydrate metabolism and, in the case of established diabetes, may reflect its prognostic and therapeutic evolution.
The characterization of the cellular microenvironment, at the ultrastructural level, draws attention to an altered control of intercellular signalling mechanisms at early stages of the onset of diabetic status. Early diagnosis of these can be a warning signal for the need to modulate therapy and the possibility of predisposition to a particular type of complication.
The observations provided by the current research can contribute to the development of a set of investigations that will allow the early identification and the efficiency of a personalized diagnostic-therapeutic algorithm, which is the desideratum of modern medicine. Techniques that allow sensitive and specific analysis of skin lesions associated with diabetic endocrinopathy need to be further developed.
Author Contributions
Conceptualization, D.T.-O. and E.-C.C.; methodology, M.P.; software, P.O.; validation, L.S., A.-E.B. and V.-B.G.; formal analysis, P.B.; investigation, I.-C.B.; re- sources, M.P.; data curation, P.O.; writing—original draft preparation, D.T.-O.; writing—review and editing, C.-E.C.; visualization, L.S.; supervision, M.P.; project administration, D.T.-O.; funding acquisition, L.S. All authors have read and agreed to the published version of the manuscript
Funding
This research received no external funding.
Institutional Review Board Statement
The animal study protocol was approved by Ethics Co mittee of “Grigore T. Popa” University of Medicine and Pharmacy (protocol code 776 / 2.02.2022).
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Quondamatteo, F. Skin and diabetes mellitus: what do we know? Cell Tissue Res 2014, 355(1), 1–21. [Google Scholar] [CrossRef] [PubMed]
- Kochet, K.; Lytus, I.; Svistunov, I.; Sulaieva, O. Skin pathology in diabetes mellitus: clinical and pathophysiological correlations (Review). Georgian Med News 2017, 273, 41–46. [Google Scholar]
- Horikawa, T.; Hiramoto, K.; Goto, K.; Sekijima, H.; Ooi, K. Differences in the mechanism of type 1 and type 2 diabetes-induced skin dryness by using model mice. Int J Med Sci 2021, 18(2), 474–481. [Google Scholar] [CrossRef] [PubMed]
- Guy, R. Diagnostic devices: Managing diabetes through the skin. Nat Nanotechnol 2016, 11(6), 493–494. [Google Scholar] [CrossRef]
- Condurache Hritcu, O.M.; Botez, A.E.; Olinici, D.T.; Onofrei, P.; Stoica, L.; Grecu, V.B.; Toader, P.M.; Gheucă-Solovăstru, L.; Cotrutz, E.C. Molecular markers associated with potentially malignant oral lesions (Review). Exp Ther Med 2021, 22(2), 834. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, M.S.; Kimhofer, T.; Ahmad, S.; AlAma, M.N.; Mosli, H.H.; Hindawi, S.I.; Mook-Kanamori, D.O.; Šebeková, K.; Damanhouri, Z.A.; Holmes, E. Ethnicity and skin autofluorescence-based risk-engines for cardiovascular disease and diabetes mellitus. PLoS One 2017, 12(9), e0185175. [Google Scholar] [CrossRef]
- Aoki, E.; Hirashima, T.; Kumamoto, Y.; Yamamoto, Y.; Suzuki, N.; Oshima, T.; Saito, D.; Hirano, T. Clinical significance of skin autofluorescence for diabetic macroangiopathy and comparison with conventional markers of atherosclerosis: a cross-sectionaland prospective study. Diabetol Int 2022, 14(2), 145–154. [Google Scholar] [CrossRef] [PubMed]
- Škrha, J.Jr.; Horová, E.; Šoupal, J.; Valeriánová, A.; Malík, J.; Prázný, M. ; Zima T, Kalousová M, Škrha J. Skin autofluorescence corresponds to microvascular reactivity in diabetes mellitus. J Diabetes Complications 2022, 36(7), 108206. [Google Scholar] [PubMed]
- Rajaobelina, K.; Cougnard-Gregoire, A.; Delcourt, C.; Gin, H.; Barberger-Gateau, P.; Rigalleau, V. Autofluorescence of Skin Advanced Glycation End Products: Marker of Metabolic Memory in Elderly Population. J Gerontol A Biol Sci Med Sci 2015, 70(7), 841–846. [Google Scholar] [CrossRef] [PubMed]
- Pichardo-Geisinger, R. Commentary on "Diabetes Mellitus and the Skin: Recognition and Management of Cutaneous Manifestations". South Med J 2016, 109(10), 647. [Google Scholar] [CrossRef]
- Singh, A.V.; Chandrasekar, V.; Paudel, N.; Laux, P.; Luch, A.; Gemmati, D.; Tisato, V.; Prabhu, S.K.; Uddin, S.; Dakua, S.P. Integrative toxicogenomics: Advancing precision medicine and toxicology through artificial intelligence and OMICs technology. Biomedicine & Pharmacotherapy 2023, 163, 114784. [Google Scholar]
- Dremin, V.; Marcinkevics, Z.; Zherebtsov, E.; Popov, A.; Grabovskis, A.; Kronberga, H.; Geldnere, K.; Doronin, A.; Meglinski, I.; Bykov, A. Skin Complications of Diabetes Mellitus Revealed by Polarized Hyperspectral Imaging and Machine Learning. IEEE Trans Med Imaging 2021, 40(4), 1207–1216. [Google Scholar] [CrossRef] [PubMed]
- Ozdogan, C.Y.; Kenar, H.; Davun, K.E.; Yucel, D.; Doger, E.; Alagoz, S. An in vitro 3D diabetic human skin model from diabetic primary cells. Biomed Mater 2020, 16(1), 015027. [Google Scholar] [CrossRef] [PubMed]
- Wei, Y.; Chen, H.; Chi, Q.; He, Y.; Mu, L.; Liu, C.; Lu, Y. Synchronized research on endothelial dysfunction and microcirculation structure in dorsal skin of rats with type 2 diabetes mellitus. Med Biol Eng Comput 2021, 59(5), 1151–1166. [Google Scholar] [CrossRef] [PubMed]
- Yaseen, H.; Khamaisi, M. Skin well-being in diabetes: Role of macrophages. Cell Immunol 2020, 356, 104154. [Google Scholar] [CrossRef]
- Olinici, D.; Gheucă-Solovăstru, L.; Stoica, L.; Bădescu, L.; Onofrei, P.; Botez, E.A.; Cotrutz, C.E. The molecular mosaic of the premaignant cutaneous lesions. Rom J Morphol Embryol 2016, 57(2), 353–359. [Google Scholar]
- Fokkens, B.T.; Smit, A.J. Skin fluorescence as a clinical tool for non-invasive assessment of advanced glycation and long-term complications of diabetes. Glycoconj J 2016, 33(4), 527–35. [Google Scholar] [CrossRef]
- Nejaddehbashi, F.; Rafiee, Z.; Orazizadeh, M.; Bayati, V.; Hemmati, A.; Hashemitabar, M.; Makvandi, P. Antibacterial and antioxidant double-layered nanofibrous mat promotes wound healing in diabetic rats. Sci Rep 2023, 13(1), 1–15. [Google Scholar] [CrossRef]
- Wielicka, M.; Neubauer-Geryk, J.; Brandt-Varma, A.; Myśliwiec, M.; Bieniaszewski, L. Skin microvascular circulation is not af-437 fected by diabetes duration in young patients with non-complicated type 1 diabetes mellitus. Pediatr Endocrinol Diabetes Metab 2019, 25(4), 183–187. [Google Scholar] [CrossRef]
- Dornuf, F.; Martín-Mateos, P.; Duarte, B.; Hils, B.; Bonilla-Manrique, O.E.; Larcher, F.; Acedo, P.; Krozer, V. Classification of skin phenotypes caused by diabetes mellitus using complex scattering parameters in the millimeter-wave frequency range. Sci Rep 2017, 7(1), 5822. [Google Scholar] [CrossRef]
- Wang, X.; Zhao, X.; Lian, T.; Wei, J.; Yue, W.; Zhang, S.; Chen, Q. Skin autofluorescence and the complexity of complications in 443 patients with type 2 diabetes mellitus: a cross-sectional study. BMC Endocr Disord 2021, 21(1), 58. [Google Scholar] [CrossRef]
- Sveen, K.A.; Dahl-Jørgensen, K.; Stensaeth, K.H.; Angel, K.; Seljeflot, I.; Sell, D.R.; Monnier, V.M.; Hanssen, K.F. Glucosepane and oxidative markers in skin collagen correlate with intima media thickness and arterial stiffness in long-term type 1 diabetes. J Diabetes Complications 2015, 29(3), 407–412. [Google Scholar] [CrossRef] [PubMed]
- Wan, L.; Qin, G.; Yan, W.; Sun, T. Skin Autofluorescence Is Associated with Diabetic Peripheral Neuropathy in Chinese Patients with Type 2 Diabetes: A Cross-Sectional Study. Genet Test Mol Biomarkers 2019, 23(6), 387–392. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Jiao, L.; Shao, Y.; Li, M.; Gong, M.; Zhang, Y.; Tan, Z.; Wang, Y.; Yang, X.; Wang, Z.; Zhang, Y. Topical GDF11 accelerates skin 450 wound healing in both type 1 and 2 diabetic mouse models. Biochem Biophys Res Commun 2020, 529(1), 7–14. [Google Scholar] [CrossRef] [PubMed]
- Yoon, H.S.; Baik, S.H.; Oh, C.H. Quantitative measurement of desquamation and skin elasticity in diabetic patients. Skin Res 452 Technol 2020, 8(4), 250–254. [Google Scholar] [CrossRef]
- Paolillo, F.R.; Mattos, V.S.; Borghi-Silva, A.; Bagnato, V.S.; de Castro Neto, J.C. Advanced Glycation Endproducts as Biomarkers for Risk of Diabetes and Cardiovascular Diseases by Skin Autofluorescence: A Noninvasive Optical Screening. Photobiomodul Photomed Laser Surg 2019, 37(3), 168–174. [Google Scholar] [CrossRef]
- Brzezinski, P.; Chiriac, A.E.; Pinteala, T.; Foia, L.; Chiriac, A. Diabetic dermopathy ("shin spots") and diabetic bullae ("bullosis diabeticorum") at the same patient. Pak J Med Sci 2015, 31(5), 1275–6. [Google Scholar] [CrossRef]
- Adamska, A.; Pilacinski, S.; Zozulinska-Ziolkiewicz, D.; Gandecka, A.; Grzelka, A.; Konwerska, A.; Malinska, A.; Nowicki, M.; Araszkiewicz, A. An increased skin microvessel density is associated with neurovascular complications in type 1 diabetes mellitus. Diab Vasc Dis Res 2019, 16(6), 513–522. [Google Scholar] [CrossRef]
- Chehelcheraghi, F.; Chien, S.; Bayat, M. Mesenchymal stem cells improve survival in ischemic diabetic random skin flap via increased angiogenesis and VEGF expression. J Cell Biochem 2019, 120(10), 17491–17499. [Google Scholar] [CrossRef]
- Tellechea, A.; Leal, E.C.; Kafanas, A.; Auster, M.E.; Kuchibhotla, S.; Ostrovsky, Y.; Tecilazich, F.; Baltzis, D.; Zheng, Y.; Carvalho, E.; Zabolotny, J.M.; Weng, Z.; Petra, A.; Patel, A.; Panagiotidou, S.; Pradhan-Nabzdyk, L.; Theoharides, T.C.; Veves, A. Mast Cells Regulate Wound Healing in Diabetes. Diabetes 2016, 65(7), 2006–2019. [Google Scholar] [CrossRef]
- Bönhof, G.J.; Strom, A.; Püttgen, S.; Ringel, B.; Brüggemann, J.; Bódis, K.; Müssig, K.; Szendroedi, J.; Roden, M.; Ziegler, D. Patterns 467 of cutaneous nerve fibre loss and regeneration in type 2 diabetes with painful and painless polyneuropathy. Diabetologia 2017, 60(12), 2495–2503. [Google Scholar] [CrossRef] [PubMed]
- Araszkiewicz, A.; Gandecka, A.; Nowicki, M.; Uruska, A.; Malińska, A.; Kowalska, K.; Wierusz-Wysocka, B.; Zozulińska-Ziółkiewicz, D. Association between small fiber neuropathy and higher skin accumulation of advanced glycation end products in patients with type 1 diabetes. Pol Arch Med Wewn 2016, 126(11), 847–853. [Google Scholar] [CrossRef] [PubMed]
- Hoppenbrouwers, T.; Tuk, B.; Fijneman, E.M.; de Maat, M.P.; van Neck, J.W. Fibrin improves skin wound perfusion in a diabetic rat model. Thromb Res 2017, 151, 36–40. [Google Scholar] [CrossRef] [PubMed]
- Kirsner, R.S.; Yosipovitch, G.; Hu, S.; Andriessen, A.; Hanft, J.R.; Kim, P.J.; Lavery, L.; Meneghini, L.; Ruotsi, L.C. Diabetic SkinChanges Can Benefit from Moisturizer and Cleanser Use: A Review. J Drugs Dermatol 2019, 18(12), 1211–1217. [Google Scholar]
- Virador, G.M.; de Marcos, L.; Virador, V.M. Skin Wound Healing: Refractory Wounds and Novel Solutions. Methods Mol Biol 2019, 1879, 221–241. [Google Scholar] [PubMed]
- Monnier, V.M.; Genuth, S.; Sell, D.R. The pecking order of skin Advanced Glycation Endproducts (AGEs) as long-term markers of glycemic damage and risk factors for micro- and subclinical macrovascular disease progression in Type 1 diabetes. Glycoconj J 2016, 33(4), 569–79. [Google Scholar] [CrossRef] [PubMed]
- Roshandel, D.; Klein, R.; Klein, B.E.; Wolffenbuttel, B.H.; van der Klauw, M.M.; van Vliet-Ostaptchouk, J.V.; Atzmon, G.; Ben-Avraham, D.; Crandall, J.P.; Barzilai, N.; Bull, S.B.; Canty, A.J.; Hosseini, S.M.; Hiraki, L.T.; Maynard, J.; Sell, D.R.; Monnier, V.M.; Cleary, P.A.; Braffett, B.H.; DCCT/EDIC Research Group; Paterson, A.D. D. New Locus for Skin Intrinsic Fluorescence in Type 1Diabetes Also Associated With Blood and Skin Glycated Proteins. Diabetes 2016, 65(7), 2060–2071. [Google Scholar] [CrossRef] [PubMed]
- Andrade, T.A.M.; Masson-Meyers, D.S.; Caetano, G.F.; Terra, V.A.; Ovidio, P.P.; Jordão-Júnior, A.A.; Frade MAC. Skin changes in streptozotocin-induced diabetic rats. Biochem Biophys Res Commun 2017, 490(4), 1154–1161. [Google Scholar] [CrossRef] [PubMed]
- Lykov, A.P.; Bondarenko, N.A.; Poveshchenko, O.V.; Miller, T.V.; Poveshchenko, A.F.; Surovtseva, M.A.; Bgatova, N.P.; Kone kov, VI. Prospect of Using Cell Product for the Therapy of Skin Defects in Diabetes Mellitus. Bull Exp Biol Med 2017, 164(2), 266–268. [Google Scholar] [CrossRef] [PubMed]
- Liao, B.; Ouyang, Q.; Song, H.; Wang, Z.; Ou, J.; Huang, J.; Liu, L. Characteristic analysis of skin keratinocytes in patients with type 2 diabetes based on the single-cell levels. Chin Med J (Engl) 2022, 135(20), 2461–2466. [Google Scholar] [CrossRef]
- Osawa, S.; Katakami, N.; Sato, I.; Ninomiya, H.; Omori, K.; Yamamoto, Y.; Takahara, M.; Miyashita, K.; Sakamoto, F.; Kawamori, D.; Matsuoka, T.; Shimomura, I. Skin autofluorescence is associated with vascular complications in patients with type 2 diabetes. J 493 Diabetes Complications 2018, 32(9), 839–844. [Google Scholar] [CrossRef]
Figure 1.
Tegument. Photon microscopy. HE,100x,- hyperkeratosis, hypergranulosis.

Figure 2.
Tegument. Photon microscopy. HE,100x, (a) hyperkeratosis, hypergranulosis, reduction of interpapillary ridges; (b) uneven thickened epidermis.
Figure 2.
Tegument. Photon microscopy. HE,100x, (a) hyperkeratosis, hypergranulosis, reduction of interpapillary ridges; (b) uneven thickened epidermis.
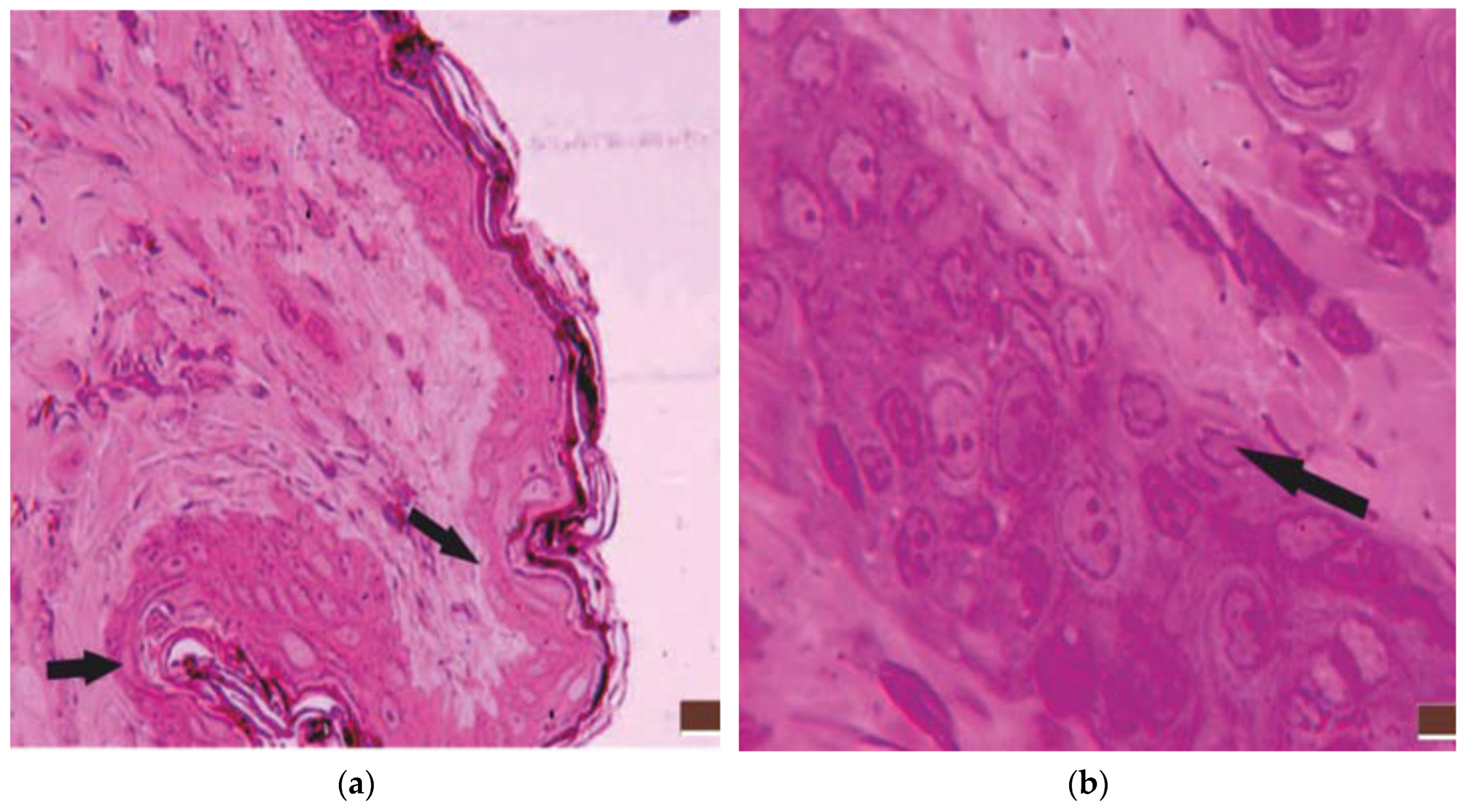
Figure 3.
Tegument. Photon microscopy. HE,100x, (a) different degrees of acanthosis; (b) capillary lumen decrease.
Figure 3.
Tegument. Photon microscopy. HE,100x, (a) different degrees of acanthosis; (b) capillary lumen decrease.
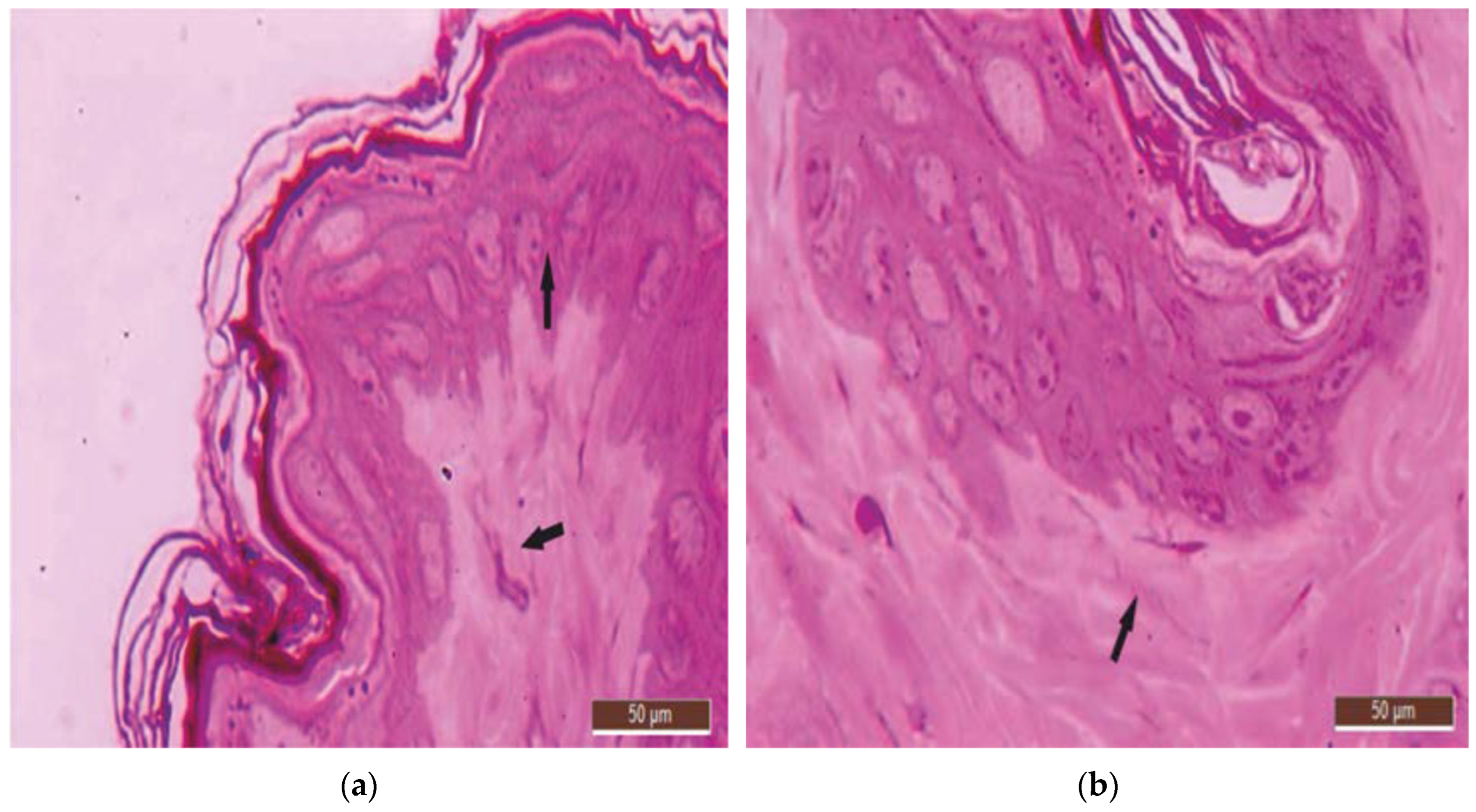
Figure 4.
TEM. Tegument - experimental diabetes mellitus- (a) different degrees of epidermal thickening; (b) presence of vesiculo-vacuolar structures in the cytoplasm; different degrees of epidermal thickening.
Figure 4.
TEM. Tegument - experimental diabetes mellitus- (a) different degrees of epidermal thickening; (b) presence of vesiculo-vacuolar structures in the cytoplasm; different degrees of epidermal thickening.
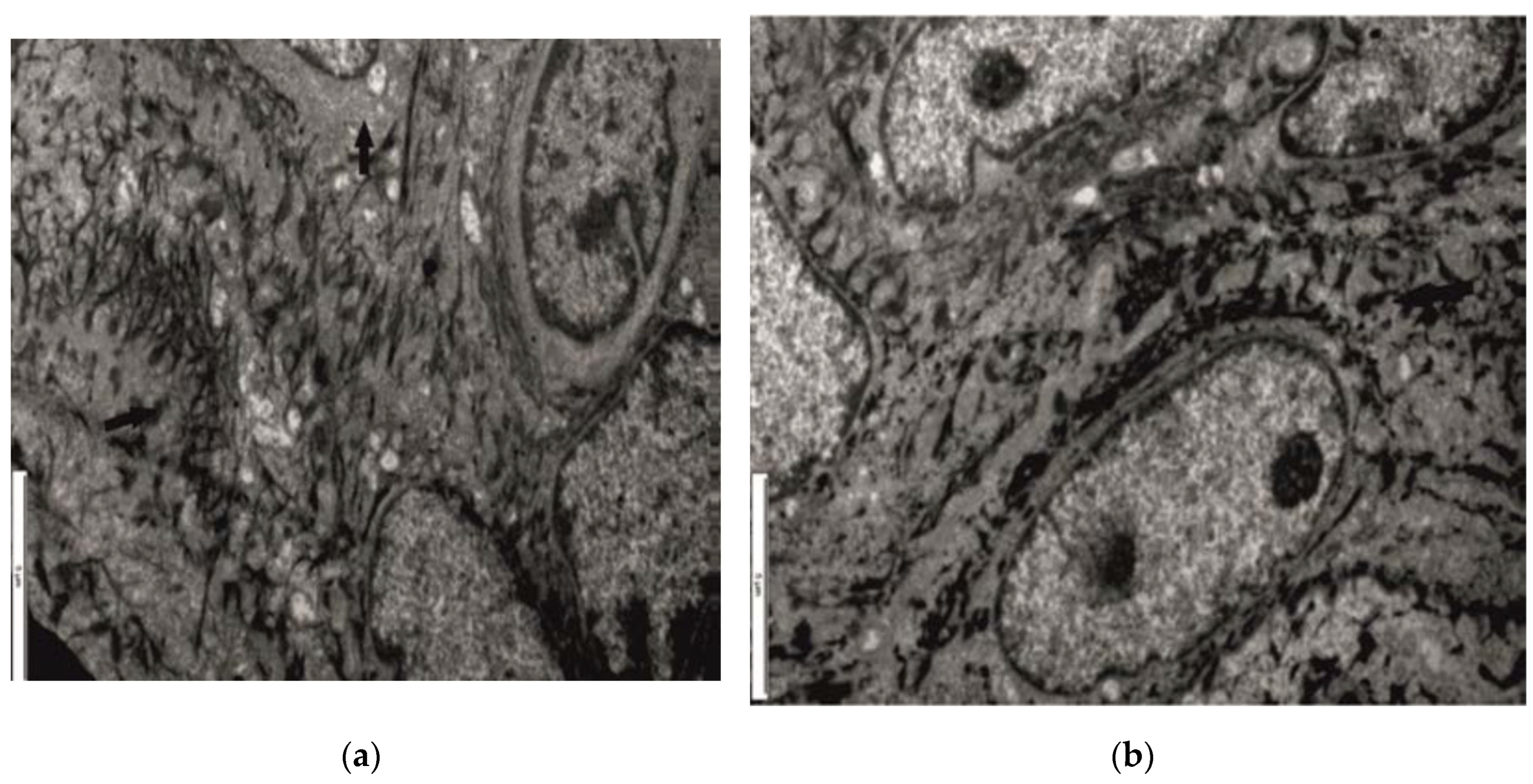
Figure 5.
TEM. Tegument - experimental diabetes mellitus – a) desmosomes; b) basement membrane.
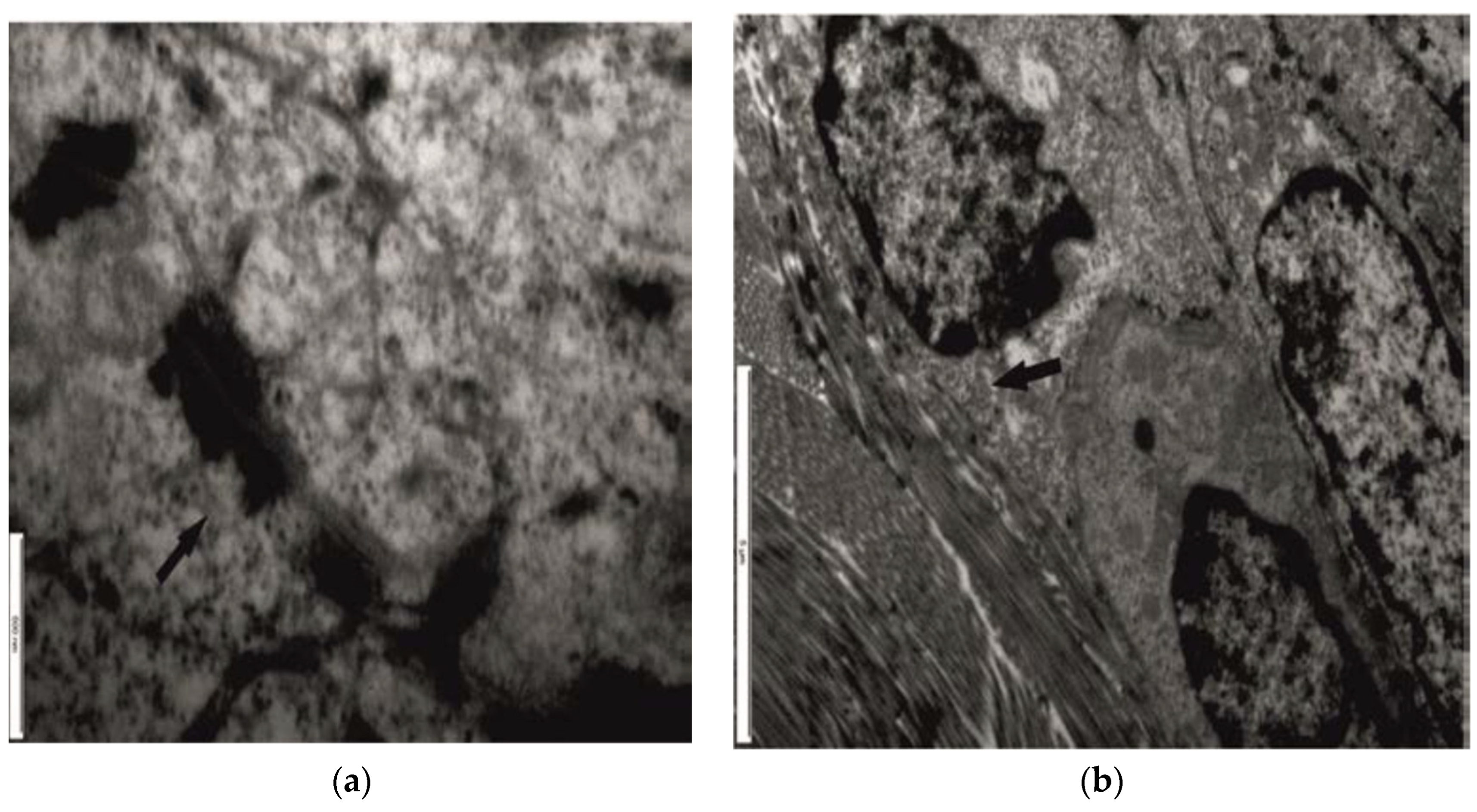
Figure 6.
TEM. Tissue - experimental diabetes mellitus - morphological changes in capillaries.
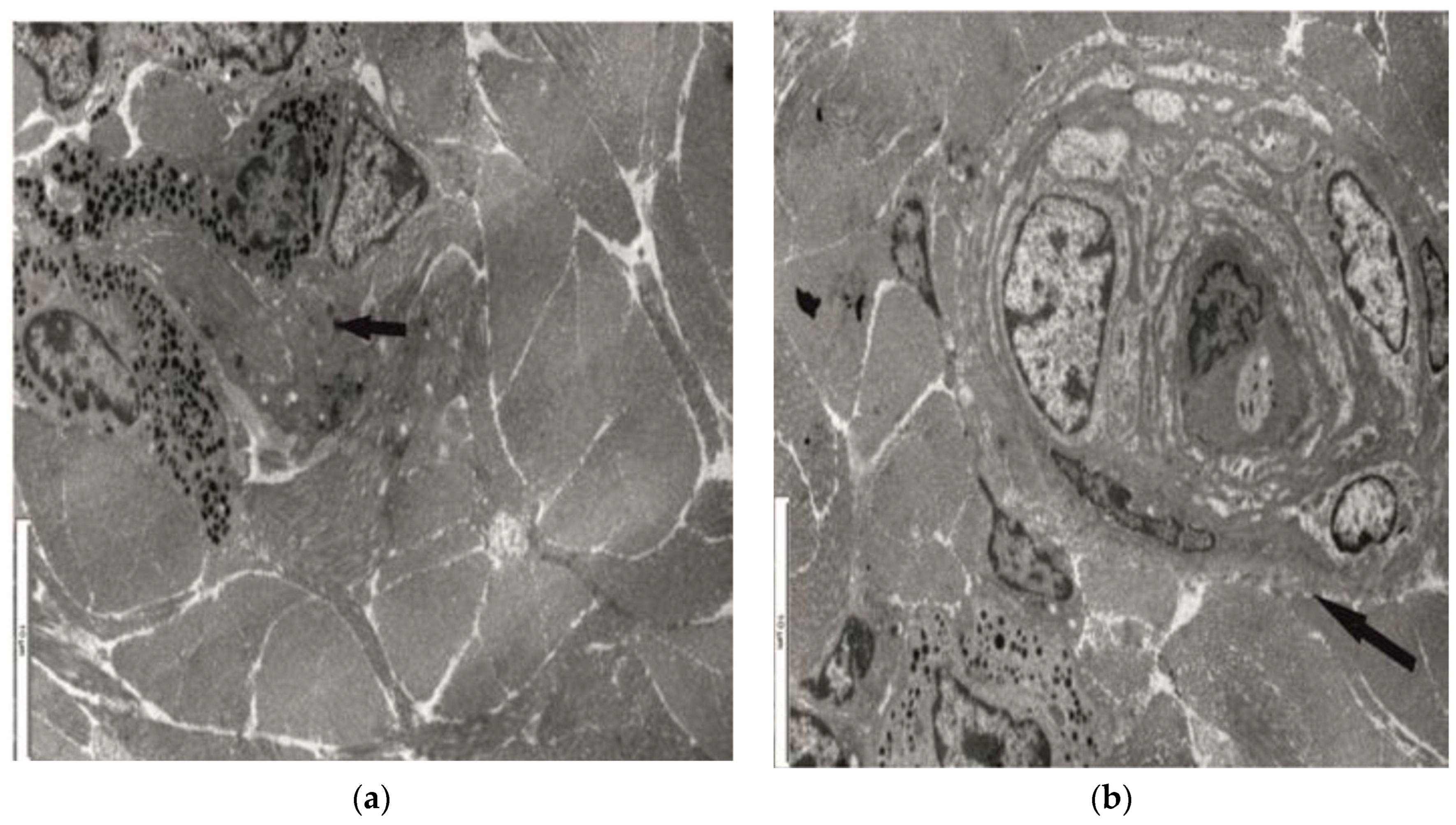
Figure 7.
TEM. Tissue - experimental diabetes -a) vesiculo-vacuolar structures, disorganization of mitochondrial internal structure; b) lack of microtubules.
Figure 7.
TEM. Tissue - experimental diabetes -a) vesiculo-vacuolar structures, disorganization of mitochondrial internal structure; b) lack of microtubules.


Table 1.
Ultrastructural aspects.
| Experimental diabetes mellitus (n = 36) | P1 | |
|---|---|---|
| vascular endothelium (n) |
dcapillary level (32) | 0.137 |
| metarteriolar level (26) | ||
| junctional complexes (n) | desmosomes (25) | 0.802 |
| basement membrane (23) | ||
| cellular organelles (n) | mitochondrial structure (35) | 0.201 |
| rough endoplasmic reticulum (30) | ||
| Golgi apparatus (31) |
1 P values for Chi square test Likelihood Ratio
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



