
Submitted:
19 January 2024
Posted:
23 January 2024
You are already at the latest version
Abstract
The changes in body composition during androgen deprivation therapy (ADT) in patients suffer from prostate cancer (PCa) are recognized by professionals more often as key for effective treatment. The aim of this study was to investigate the impact of ADT on the sarcopenia development in PCa. The following databases were used: PubMed, Embase, Web of Science and Scopus databases. Out of 2183 studies, 7 were included in this review. The fixed-effect model was used in the meta-analysis. Significant increase in SATI: 0.32 (95%CI: 0.13-0.51) p= 0.001, de-crease in SMI: -0.38 (95% CI: -0.57 to -0.19) p < 0.0001 and SMD: -0.46 (95% CI: -0.69 to -0.24) p < 0.0001 was observed. No statistical association was visible between ADT and changes in BMI: 0.05 (95%CI: -0.18-0.28), p= 0.686 and VATI: 0.17 (95% CI: -0.02 to 0.37), p=0.074. In conclusion, the ADT significantly contributes to the body composition changes and sarcopenia development.
Keywords:
androgen deprivation therapy
; ADT
; sarcopenia
; prostate cancer
; prostatic neoplasm
; systematic review
1. Introduction
Body composition in prostate cancer (PCa) patients is of high importance as low muscle mass is associated with approximately 50% increased risk of mortality, where the total fat mass (FM) was not found to be a prognostic factor. Specifically, higher subcutaneous fat and lower visceral-to-subcutaneous fat ratio are related to better patient’s survival [1,2]. It is also important to support the implementation of personalized physical activity (PA) in patient’s daily life as there is evidence suggesting that PA has beneficial effect on physical performance [3], lean body mass (LBM) and fat mass during androgen deprivation therapy (ADT) [4].
Low muscle mass is a relevant element of sarcopenia definition. Among the factors that driving force the sarcopenia development are listed the following: aging, comorbidities, cancer, low physical activity and malnutrition [5]. Sarcopenia is recognized as a disease since the 10th revision of the International Classification of Diseases (ICD-10) [6], which is supported by the newest ICD-11 [7]. According to the guidelines of the European Working Group on Sarcopenia in Older People (EWGSOP2), sarcopenia is considered probable when muscle strength is decreased. The observed decline in muscle strength is a leading diagnostic feature. The diagnosis might be confirmed by low muscle quantity or quality [5]. Sarcopenia was also defined by the Asian Working Group for Sarcopenia (AWGS), which focused on age-related muscle and physical performance decline and created a similar algorithm for diagnosis [8]. However, still it is challenging to diagnose sarcopenia in clinical setting as improvement in nutritional status does not play the major role in the treatment of PCa patients.
It should be highlighted that ADT might also influence on muscle health. An association between ADT and a decreased in physical performance [9,10,11,12], muscle strength [10,11,12,13,14] and mass [14,15,16] was confirmed. These results might be indicative of possible sarcopenia development during treatment. The mechanism of ADT influence on muscle health is yet to be determined. In an international survey, physicians reported that 38% of patients with non-metastatic prostate cancer received ADT [21]. Therefore, a wide range of indications for treatment with ADT and its use in clinical settings require thorough examination of the muscle-related side effects [17].
From the clinical perspective it is crucial to establish the direct link between ADT and the development of sarcopenia in men suffer from PCa. These findings might be relevant for the prevention of sarcopenia and indicate the choice of treatment options in future patients’ guidance. Therefore, aim of this study was to assess the influence of ADT on sarcopenia development in PCa patients.
2. Materials and Methods
2.1. Search Strategies
The search was conducted through four databases: PubMed, Embase, Web of Science and Scopus. For the following search strategy Mesh terms, Emtree terms and specific keywords were applied and adapted for each database. No filters were used.
- #1 sarcopenia OR Sarcopenias OR composition, body OR body composition OR Body Compositions OR Compositions, Body OR muscle mass OR muscle volume OR muscle quality OR skeletal muscle loss OR muscle loss
- #2 Ca prostate OR cancer in the prostate OR cancer of the prostate OR cancer, prostate OR carcinogenesis of the prostate OR malignancies of the prostate OR malignancy of the prostate OR malignant neoplasm of the prostate OR malignant prostate tumor OR malignant prostate tumour OR malignant prostatic tumor OR malignant prostatic tumour OR malignant tumor of the prostate OR prostate cancerogenesis OR prostate carcinogenesis OR prostate gland cancer OR prostate malignancies OR prostate malignancy OR prostate malignant neoplasm OR prostate malignant tumor OR prostate malignant tumour OR prostatic cancer OR prostatic cancerogenesis OR prostatic carcinogenesis OR prostatic malignancies OR prostatic malignancy OR prostate cancer OR Prostatic Neoplasms OR Prostate Neoplasms OR Neoplasms, Prostate OR Neoplasm, Prostate OR Prostate Neoplasm OR Neoplasms, Prostatic OR Neoplasm, Prostatic OR Prostatic Neoplasm OR Cancers, Prostate OR Prostate Cancers OR Cancer, Prostatic OR Cancers, Prostatic OR Prostatic Cancers OR Cancer of Prostate
- #3 Antagonists, Androgen OR Antiandrogens OR Androgen Antagonist OR Antagonist, Androgen OR Antiandrogen OR Anti-Androgen Effect OR Anti Androgen Effect OR Effect, Anti-Androgen OR Antiandrogen Effect OR Effect, Antiandrogen OR Antiandrogen Effects OR Effects, Antiandrogen OR Anti-Androgen Effects OR Anti Androgen Effects OR Effects, Anti-Androgen OR Androgen Antagonists OR ADT OR androgen deprivation therapy OR androgen suppresion therapy OR anti androgen OR antiandrogen agent OR antiandrogenic agent OR antiandrogenic drug OR nonsteroidal anti androgen OR nonsteroidal anti androgens OR nonsteroidal anti-androgen OR nonsteroidal anti-androgens OR nonsteroidal antiandrogen OR nonsteroidal antiandrogens OR gonadotropin-releasing hormone antagonist OR gonadotropin-releasing hormone antagonists OR gonadotropin-releasing hormone agonist OR gonadotropin-releasing hormone agonists OR LHRH agonist OR LHRH antagonist OR MAB OR maximum androgen blockade OR CAB OR complete androgen blockade OR gonadorelin antagonist OR antigonadorelin OR gonadorelin, anti OR gonadorelin antagonist OR gonadorelin agonist OR gonadorelin agonist OR gnrh antagonist OR gonadotropin releasing factor antagonist OR gonadotropin releasing hormone antagonist OR gonadotropin releasing hormone antagonists OR lh rh antagonist OR lrf antagonist OR luliberin antagonist OR luteinising hormone releasing hormone antagonist OR luteinizing hormone releasing hormone antagonist OR gnrh agonist OR gonadotropin releasing hormone agonist OR luteinising hormone releasing hormone agonist OR luteinizing hormone releasing hormone agonist OR orchectomy OR orcheotomy OR testectomy OR testis removal OR orchiectomy OR Orchidectomy OR Orchiectomies OR Orchidectomies OR Castration, Male OR Castrations, Male OR Male Castration OR Male Castrations
- #1 AND #2 AND #3
3.2. Study Selection
The results of conducted search are presented as a flow diagram according to the PRISMA statement (Figure 1).
Each database was searched and results were analyzed with help of Zotero software. First, all duplicates were removed. Than the results were screened by two researchers. Titles were assessed and abstracts’ of articles possibly related with the topic were analyzed. Results in English or German were considered. Case reports, case series and conference abstracts were excluded during this phase. Occurring doubts were an indication for full-text assessment. After full-text review chosen studies were assessed for eligibility. For inclusion required were sarcopenia definition, description of assessment method and data about ADT. Authors of reviewed articles were contacted by e-mail when necessary.
3.3. Data Extraction and Analysis
Studies included in the analysis were screened for the description of cancer and its treatment with focus on ADT, clinical characteristics of patients, body composition, physical performance and details of sarcopenia measurement and prevalence. All retrieved details were double checked for mistakes and presented as tables. Collected data was assessed and eligibility for meta-analysis was discussed among researchers.
Meta-analysis was performed with the use of R Project for Statistical Computing [18]. Data in studies considered for meta-analysis was collected at baseline before ADT and at the follow up and presented in different format. Median and quartiles were recalculated to mean and standard deviation using package “estmeansd: Estimating the Sample Mean and Standard Deviation from Commonly Reported Quantiles in Meta-Analysis” [19]. The Method for Unknown Non-Normal Distributions (MLN) was chosen for recalculation. In case of change in investigated parameters calculated mean was added to mean of control and variance of follow up was calculated as a sum of control variance and the change of parameter variance. The meta-analysis was conducted with “dmetar” package [20]. Parameters considered for assessment were BMI, SMD, SMI, SATI and VATI. The fixed-effect or random-effect model was chosen. Korczak et al. [21] and Sheean et al. [22] presented data for two different populations independently (patients with hormone sensitive prostate cancer (HSPC) or castration resistant prostate cancer (CRPC) and black or non-black patients respectively). Therefore, each of the population was considered separately in the meta-analysis. The results of the meta-analysis were presented as a forest plot illustrating the results of the individual studies and the summary effect. Regarding details on the meta-analysis inverse variance method, restricted maximum-likelihood estimator for tau 2 and Q-Profile method for confidence interval of tau 2 and tau were applied.
The heterogeneity of the studies measured with I2 was tested for significance [23]. Since I2 was found to be 0,0% for all analyzed parameters, random-effect model was rejected and not evaluated. Egger’s Regression Test was used for detection of potential publication bias. Importantly, small number of publications (less than 10) makes it very week. Therefore, results indicating no bias should be treated roughly.
3.4. Risk of Bias
The quality of the studies was assessed independently with the use of Newcastle–Ottawa Quality Assessment Scale. A full score using this scale is 10 points. A study with ≥6 points was regarded as a good-quality study and each od included studies fullfieled this criteria.
4. Results
The description of included studies was presented in Table 1. Observational studies were conducted in ethnically diverse groups of PCa patients, where the sarcopenia was assessed either twice (at the baseline and in the follow up) [21,22,24,25,26] or only once during the ADT treatment [27,28]. The largest group of PCa patient’s was found in Chiang et al. [24] and therefore this study will have the greatest impact on the meta-analysis performed. Only one qualified paper [27] had a control group of healthy individuals.
The study patients were elderly men with number of comorbidities characterized by overweight according to Body Mass Index (BMI), with exception of the Kimura et al [28] study. No significant association betweenn BMI (95%CI: -0.18-0.28), p= 0.686) and sarcopenia was observed (Figure 2). The hemoglobin and albumin concentrations were assessed with the normal range and the PSA level exceeded the recommended level for age. In most of the PCa patients the median Gleason score was 8 indicating high grade cancer (Table 2). Patients were on different treatment regimens using ADT, where the ADT du-ration was reported in 4 studies [25,26,27,28] and the dietary counselling was incorporated in the treatment in only 1 study [21] (Table 3). Taking into account selected body composition parameters an increase in SATI and VATI, where the decrease in SMI and SMD over the course of ADT was observed (Table 4). The following parameters shown an association with sarcopenia development in PCa patients: SATI 0.32 (95%CI: 0.13-0.51) p= 0.001; SMD -0.46 (95% CI: -0.69 to -0.24) p< 0.0001; SMI -0.38 (95% CI: -0.57 to -0.19) p < 0.0001 (Figure 3, Figure 4 and Figure 5). No significant association was found between sarcopenia development and VATI 0.17 (95% CI: -0.02 to 0.37), p=0.074 (Figure 6). However, the sarcopenia assessment methodology and time to follow up used in single studies were differentiated which could influence on obtained results. Nevertheless, no association with progression free survival or overall survival was indicted [21,22,24]) (Table 5).

Table 1.
Description of included studies.
| Study | Year | Country | Study design | Study population | Control population | Baseline | Follow up | ADT implementation: prior/post baseline |
|---|---|---|---|---|---|---|---|---|
| SARCOPENIA ASSESSED AT BASELINE AND FOLLOW-UP | ||||||||
| Chiang et al [24] | 2021 | Italy | Retrospective observational study, single-center | 125 | No | Before initiation of ADT+radiotherapy | Within one year after treatment initiation | Post |
| Korczak et al [21] | 2023 | Poland | Prospective observational study, single-centre | HSPC 34 CRPC 30 |
No | HSCPC: before initiation of ADT+docetaxel±radiotherapy CRPC: during ADT+abiraterone or enzalutamide±radiotherapy±prostatectomy |
At the moment of biochemical progression | HSPC post CRPC prior+post; no information about prior treatment |
| Sheean et al [22] | 2022 | USA | Retrospective observational study | 74 Subgroup at baseline: 54 Subgroup at follow-up: 19 |
No | Before initiation of ADT±docetaxel | At the moment of death or last contact | Post |
| Couderc et al [25] | 2020 | France | Prospective observational study, single-centre | 31 Subgroup at follow-up: 6 |
No | Before initiation of ADT+radiotherapy | At the end of the treatment | Post |
| Sheikhbahaei et al [26] | 2020 | USA | Retrospective observational study, single-center | 22 | No | Before initiation of neoadjuvant therapy: ADT+docetaxel | I: 1 month after the completion of neoadjuvant therapy II: approximately 1 year after initiation of neoadjuvant therapy. |
Post |
| SARCOPENIA ASSESSED AS A SINGLE MEASURMENT DURING ADT | ||||||||
| Owen et al [27] | 2019 | Australia | Cross-sectional study | 70 | Non-ADT prostate cancer: 52 Healthy: 70 |
During ADT treatment ± chemotherapy | Prior | |
| Kimura et al [28] | 2019 | Japan | Cross-sectional study | 89 | No | During ADT | Prior | |
ADT androgen deprivation therapy; HSPC hormone sensitive prostate cancer; CRPC castration resistant prostate cancer.
5. Discussion
The use of ADT in prostate cancer patients influenced significantly on nutritional status and therefore was leading to sarcopenia development. The ADT had a strong impact on the reduction in SMD (95% CI: -0.69 to -0.24) and moderate effect on reduction in SMI (95% CI: -0.57 to -0.19) over the time period, where in the changes of SATI (95%CI: 0.13-0.51) significantly increase was noticed during the treatment.
In PCa patients, during aging, we observed in the clinical setting decrease in the physical fitness and testosterone level [29]. The muscle strength and muscle size decrease leading to sarcopenia development, sometimes to sarcopenic obesity being associated with a significant change in body composition. ADT may accelerate unfavorable changes occurring in the patient’s body [30]. The major role plays testosterone secretion that controls muscle volume an strength in men and being significantly decreased during the ADT treatment [31]. The development of sarcopenia, understood as a decreasing amount of muscle mass or a decline in muscle quality [21], is a particular problem affecting people with chronic diseases. This applies not only to the group of men suffer from PCa and treated with ADT, but also to patients suffer from i.e. Chronic obstructive pulmonary disease - COPD or Chronic Liver Disease-CLD [32,33]. The occurrence of sarcopenia is one of the prognostic factors for patients with PC and therefore highlight the importance of proper diet (rich in protein and proper energy value) during the treatment to improve an effectiveness of clinical treatment. It has been proven that cancer progression-free survival for patients with PCa and sarcopenia is shorter [37]. Current results are consistent with those obtained by other researchers [16,21,25,27]. Smith et al. [16,34] determined that taking ADT causes changes in body composition, as the muscle mass decreased with a simultaneous increase in percentage of fat tissue. Finally, changes that occur during the treatment may cause bone fracture because bone mass density (BMD) decreases, which influences strongly on patient’s range of motion. As was highlighted by Shahinian et al [35] patient’s sarcopenia contributes directly to decrease in Quality of life (QoL), in which the physical performance is one of the main aspects that are considered.
The BMI changes were analyzed in 2 papers with no significant changes [24,25] Nevertheless, it should be underlined that the BMI does not reflect real changes in patient’s body composition, therefore an association was not expected. Another analyzed parameter was SATI. In the current study changes in muscle size loss were visible on statistical significance level. The observed effect size was at the 0.32 (statistically moderate). Current results were confirmed by Storer et al. [36] indicating that ADT causes a decrease in muscle mass and an increase in fat mass. Additionally, the SMD parameter indicated structural changes in muscle tissue. It can be probably either an increase in the water content in muscle tissue or an increase in the amount of fat in its place. Both of mentioned has lower HU (Hounsfield unit) than muscle tissue (less or equal 1000) In study by Overkamp et al. [14] patients with PCa during the ADT showed a reduction in the size of type I and II muscle fibers and their capillarization, which resulted in a reduction in SMD. In analyzed results SMI showed statistically significant decrease with the effect size of 0.38 (between moderate and large). Pablos-Rodríguez et al.[37] highlighted that this parameter is crucial in terms of survival prognosis. The decrease of SMI straightly affect survival ratio [38]. As was indicated by McGovern et al [39] this type of relation is observed not only in PCa patients but in other suffer from i.e. colorectal cancer or breast cancer [39]. The VATI parameter is recognized as an indicator for an early cardiometabolic risk [40] Study done by Di Bella et al. [41] confirmed that high VATI being observed in abdominal obesity has a negative effect on the progression in PCa patients [41]. In the current study, the effect size for VATI parameter was small moderate, but not significant. Nevertheless, in is also important to assess patients body composition in relation to dietary habits and changes in body mass over the time period. Even the use of validated questionnaires i.e. NRS, SGA may help to plan personalized nutrition.
Taking into account the importance of body composition in cancer patients it seems to be justified that patient with sarcopenia should be under the care of an interdisciplinary team, including: a dietitian, a physiotherapist, psychologist and oncologist. Such comprehensive approach may increase the chance to minimize the side effects of therapy for example: reduction in muscle mass, worsening functioning in daily life and finally prognosis. There is no doubt that careful observation of the patient regarding correct eating habits and meeting energy needs is extremely important for proper treatment.
Our results showed the importance and complex of sarcopenia as a part of ADT treatment. PC patient should be provided with medical, dietary, and physiotherapeutic care. Only such comprehensive approach is able to minimize the side effects of ADT therapy strongly influencing on patients QoL and treatment response.
6. Conclusions
Androgen deprivation therapy significantly influences on patient’s body composition therefore leading to sarcopenia development. The is a need for further studies with the currently recommended methodology of sarcopenia diagnosis and further personalized dietary intervention and proper physical activity that will influence positively on muscle mass. It seems that ADT with combination of proper lifestyle intervention supplied to prostate cancer patients during the treatment may be good strategy that gives the best results.
Author Contributions
Conceptualization, A.G. and M.S-M.; methodology, A.G., M.S-M., M.M.; validation, M.S-M., W.W., M.M., J.K. and M.L.; formal analysis, W.W. and M.M.; investigation, A.G. and M.S-M.; data curation, M.S-M., A. G., E.W.; writing—original draft preparation, A.G. and M.S-M.; writing—review and editing, M.M., E.W., J.K. and M.L.; visualization, A.G.; supervision, M.S-M.; project administration, M.S-M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Lopez, P.; Newton, R.U.; Taaffe, D.R.; Singh, F.; Buffart, L.M.; Spry, N.; Tang, C.; Saad, F.; Galvão, D.A. Associations of Fat and Muscle Mass with Overall Survival in Men with Prostate Cancer: A Systematic Review with Meta-Analysis. Prostate Cancer Prostatic Dis. 2022, 25, 615–626. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA: A Cancer Journal for Clinicians 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Ussing, A.; Mikkelsen, M.; Villumsen, B.; Wejlgaard, J.; Bistrup, P.; Birkefoss, K.; Bandholm, T. Supervised Exercise Therapy Compared with No Exercise Therapy to Reverse Debilitating Effects of Androgen Deprivation Therapy in Patients with Prostate Cancer: A Systematic Review and Meta-Analysis. PROSTATE CANCER AND PROSTATIC DISEASES 2022, 25, 491–506. [Google Scholar] [CrossRef]
- Shao, W.; Zhang, H.; Qi, H.; Zhang, Y. The Effects of Exercise on Body Composition of Prostate Cancer Patients Receiving Androgen Deprivation Therapy: An Update Systematic Review and Meta-Analysis. PLoS One 2022, 17, e0263918. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European Consensus on Definition and Diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]
- ICD-10 Version:2019. Available online: https://icd.who.int/browse10/2019/en#/M62.5 (accessed on 18 May 2023).
- ICD-11 Coding Tool Mortality and Morbidity Statistics (MMS). Available online: https://icd.who.int/ct11/icd11_mms/en/release (accessed on 18 May 2023).
- Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. Journal of the American Medical Directors Association 2020, 21, 300–307.e2. [CrossRef]
- Clay, C.A.; Perera, S.; Wagner, J.M.; Miller, M.E.; Nelson, J.B.; Greenspan, S.L. Physical Function in Men with Prostate Cancer on Androgen Deprivation Therapy. Phys Ther 2007, 87, 1325–1333. [Google Scholar] [CrossRef]
- Galvão, D.A.; Taaffe, D.R.; Spry, N.; Joseph, D.; Turner, D.; Newton, R.U. Reduced Muscle Strength and Functional Performance in Men with Prostate Cancer Undergoing Androgen Suppression: A Comprehensive Cross-Sectional Investigation. Prostate Cancer Prostatic Dis 2009, 12, 198–203. [Google Scholar] [CrossRef]
- Alibhai, S.M.H.; Breunis, H.; Timilshina, N.; Johnston, C.; Tomlinson, G.; Tannock, I.; Krahn, M.; Fleshner, N.E.; Warde, P.; Canning, S.D.; et al. Impact of Androgen-Deprivation Therapy on Physical Function and Quality of Life in Men with Nonmetastatic Prostate Cancer. J Clin Oncol 2010, 28, 5038–5045. [Google Scholar] [CrossRef]
- Alibhai, S.M.H.; Breunis, H.; Timilshina, N.; Naglie, G.; Tannock, I.; Krahn, M.; Warde, P.; Fleshner, N.E.; Canning, S.D.; Tomlinson, G. Long-Term Impact of Androgen-Deprivation Therapy on Physical Function and Quality of Life. Cancer 2015, 121, 2350–2357. [Google Scholar] [CrossRef] [PubMed]
- Basaria, S.; Lieb, J. 2nd; Tang, A.M.; DeWeese, T.; Carducci, M.; Eisenberger, M.; Dobs, A.S. Long-Term Effects of Androgen Deprivation Therapy in Prostate Cancer Patients. Clin Endocrinol (Oxf) 2002, 56, 779–786. [Google Scholar] [CrossRef] [PubMed]
- Overkamp, M.; Houben, L.H.P.; van der Meer, S.; van Roermund, J.G.H.; Bos, R.; Kokshoorn, A.P.J.; Larsen, M.S.; van Loon, L.J.C.; Beelen, M.; Beijer, S. Onset of Androgen Deprivation Therapy Leads to Rapid Deterioration of Body Composition, Physical Performance, Cardiometabolic Health and Quality-of-Life in Prostate Cancer Patients. Scand J Urol 2023, 57, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Chang, D.; Joseph, D.J.; Ebert, M.A.; Galvão, D.A.; Taaffe, D.R.; Denham, J.W.; Newton, R.U.; Spry, N.A. Effect of Androgen Deprivation Therapy on Muscle Attenuation in Men with Prostate Cancer. J Med Imaging Radiat Oncol 2014, 58, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.R.; Saad, F.; Egerdie, B.; Sieber, P.R.; Tammela, T.L.J.; Ke, C.; Leder, B.Z.; Goessl, C. Sarcopenia during Androgen-Deprivation Therapy for Prostate Cancer. J Clin Oncol 2012, 30, 3271–3276. [Google Scholar] [CrossRef]
- Parker, C.; Castro, E.; Fizazi, K.; Heidenreich, A.; Ost, P.; Procopio, G.; Tombal, B.; Gillessen, S. Prostate Cancer: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up†. Annals of Oncology 2020, 31, 1119–1134. [Google Scholar] [CrossRef] [PubMed]
- R: The R Project for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 20 July 2023).
- McGrath, S.; Zhao, X.; Steele, R.; Benedetti, A. Estmeansd: Estimating the Sample Mean and Standard Deviation from Commonly Reported Quantiles in Meta-Analysis 2022.
- Companion R Package for the Guide Doing Meta-Analysis in R. Available online: https://dmetar.protectlab.org/ (accessed on 20 July 2023).
- Korczak, J.; Mardas, M.; Litwiniuk, M.; Bogdański, P.; Stelmach-Mardas, M. Androgen Deprivation Therapy for Prostate Cancer Influences Body Composition Increasing Risk of Sarcopenia. Nutrients 2023, 15. [Google Scholar] [CrossRef] [PubMed]
- Sheean, P.M.; O’Connor, P.; Joyce, C.; Vasilopoulos, V.; Badami, A.; Stolley, M. Clinical Features and Body Composition in Men with Hormone-Sensitive Metastatic Prostate Cancer: A Pilot Study Examining Differences by Race. Prostate Cancer 2022, 2022. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G. Quantifying Heterogeneity in a Meta-Analysis. Stat Med 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Chiang, P.-K.; Tsai, W.-K.; Chiu, A.W.-H.; Lin, J.-B.; Yang, F.-Y.; Lee, J. Muscle Loss During Androgen Deprivation Therapy Is Associated With Higher Risk of Non-Cancer Mortality in High-Risk Prostate Cancer. Front Oncol 2021, 11, 722652. [Google Scholar] [CrossRef]
- Couderc, A.L.; Muracciole, X.; Nouguerede, E.; Rey, D.; Schneider, S.; Champsaur, P.; Lechevallier, E.; Lalys, L.; Villani, P. HoSAGE: Sarcopenia in Older Patients before and after Treatment with Androgen Deprivation Therapy and Radiotherapy for Prostate Cancer. J Nutr Health Aging 2020, 24, 205–209. [Google Scholar] [CrossRef]
- Sheikhbahaei, S.; Reyes, D.K.; Rowe, S.P.; Pienta, K.J. CT-Based Assessment of Body Composition Following Neoadjuvant Chemohormonal Therapy in Patients with Castration-Naïve Oligometastatic Prostate Cancer. Prostate 2021, 81, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Owen, P.J.; Daly, R.M.; Dalla Via, J.; Mundell, N.L.; Livingston, P.M.; Rantalainen, T.; Fraser, S.F. Does Use of Androgen Deprivation Therapy (ADT) in Men with Prostate Cancer Increase the Risk of Sarcopenia? Calcif Tissue Int 2019, 105, 403–411. [Google Scholar] [CrossRef] [PubMed]
- Kimura, Y.; Yamada, M.; Ohji, S.; Ishiyama, D.; Nishio, N.; Otobe, Y.; Koyama, S.; Suzuki, M.; Ichikawa, T.; Ito, D.; et al. Presence of Sarcopenic Obesity and Evaluation of the Associated Muscle Quality in Japanese Older Men with Prostate Cancer Undergoing Androgen Deprivation Therapy. J Geriatr Oncol 2019, 10, 835–838. [Google Scholar] [CrossRef] [PubMed]
- Narici MV.; Maffulli N. Sarcopenia: characteristics, mechanisms and functional significance. Br Med Bull 2010, 95, 139-59. [CrossRef]
- Nam YS.; Lee G, Yun JM.; Cho B. Testosterone Replacement, Muscle Strength, and Physical Function. World J Mens Health 2018, May 36(2), 110-122. [CrossRef]
- Griggs RC.; Kingston W.; Jozefowicz RF.; Herr BE.; Forbes G.; Halliday D. Effect of testosterone on muscle mass and muscle protein synthesis. J Appl Physiol (1985) 1989, Jan 66(1), 498-503. [CrossRef]
- Kaluźniak-Szymanowska A.; Krzymińska-Siemaszko R.; Deskur-Śmielecka E.; Lewandowicz M.; Kaczmarek B.; Wieczorowska-Tobis K.; Malnutrition, Sarcopenia, and Malnutrition-Sarcopenia Syndrome in Older Adults with COPD. Nutrients 2021, Dec 23, 14(1):44. [CrossRef]
- Son SW.; Song DS.; Chang UI.; Yang JM.; Definition of Sarcopenia in Chronic Liver Disease. Life (Basel) 2021, Apr 16, 11(4):349. [CrossRef]
- Smith MR.; Changes in fat and lean body mass during androgen-deprivation therapy for prostate cancer. Urology 2004, 63(4); 742-5. [CrossRef]
- Shahinian VB.; Kuo YF.; Freeman JL.; Goodwin JS. Risk of fracture after androgen deprivation for prostate cancer. N Engl J Med 2005,;352(2); 154-64. [CrossRef]
- Storer TW.; Miciek R.; Travison TG.; Muscle function, physical performance and body composition changes in men with prostate cancer undergoing androgen deprivation therapy. Asian J Androl. 2012 ; 2; 204-21. doi: 10.1038/aja.2011.104. Epub 2012 Feb 27. [CrossRef]
- de Pablos-Rodríguez P, Del Pino-Sedeño T, Infante-Ventura D, de Armas-Castellano A, Ramírez Backhaus M, Ferrer JFL, de Pablos-Velasco P, Rueda-Domínguez A, Trujillo-Martín MM. Prognostic Impact of Sarcopenia in Patients with Advanced Prostate Carcinoma: A Systematic Review. J Clin Med. 2022 Dec 21;12(1):57. doi: 10.3390/jcm12010057. PMID: 36614862; PMCID: PMC982150138. [CrossRef] [PubMed] [PubMed Central]
- Chiang PK.; Tsai WK.; Chiu AW.; Lin JB.; Yang FY.; Lee J. Muscle Loss During Androgen Deprivation Therapy Is Associated With Higher Risk of Non-Cancer Mortality in High-Risk Prostate Cancer. Front Oncol. 2021; Sep 17; 11:722652. [CrossRef]
- McGovern J.; Dolan RD.; Horgan PG.; Laird BJ.; McMillan DC. Computed tomography-defined low skeletal muscle index and density in cancer patients: observations from a systematic review. J Cachexia Sarcopenia Muscle. 2021 Dec;12(6):1408-1417. doi: 10.1002/jcsm.12831. Epub 2021 Oct 18. PMID: 34664431; PMCID: PMC8718024. [CrossRef] [PubMed] [PubMed Central]
- Amato MC, Giordano C, Galia M, Criscimanna A, Vitabile S, Midiri M, Galluzzo A; AlkaMeSy Study Group. Visceral Adiposity Index: a reliable indicator of visceral fat function associated with cardiometabolic risk. Diabetes Care. 2010; ;33(4); 920-2. [CrossRef]
- Di Bella CM.; Howard LE.; Oyekunle T.; De Hoedt AM.; Salama JK.; Song H.; Freedland SJ.; Allott EH. Abdominal and pelvic adipose tissue distribution and risk of prostate cancer recurrence after radiation therapy. Prostate 2020; 80(14); 1244-1252. [CrossRef]
Figure 1.
Flow diagram describing study selection.
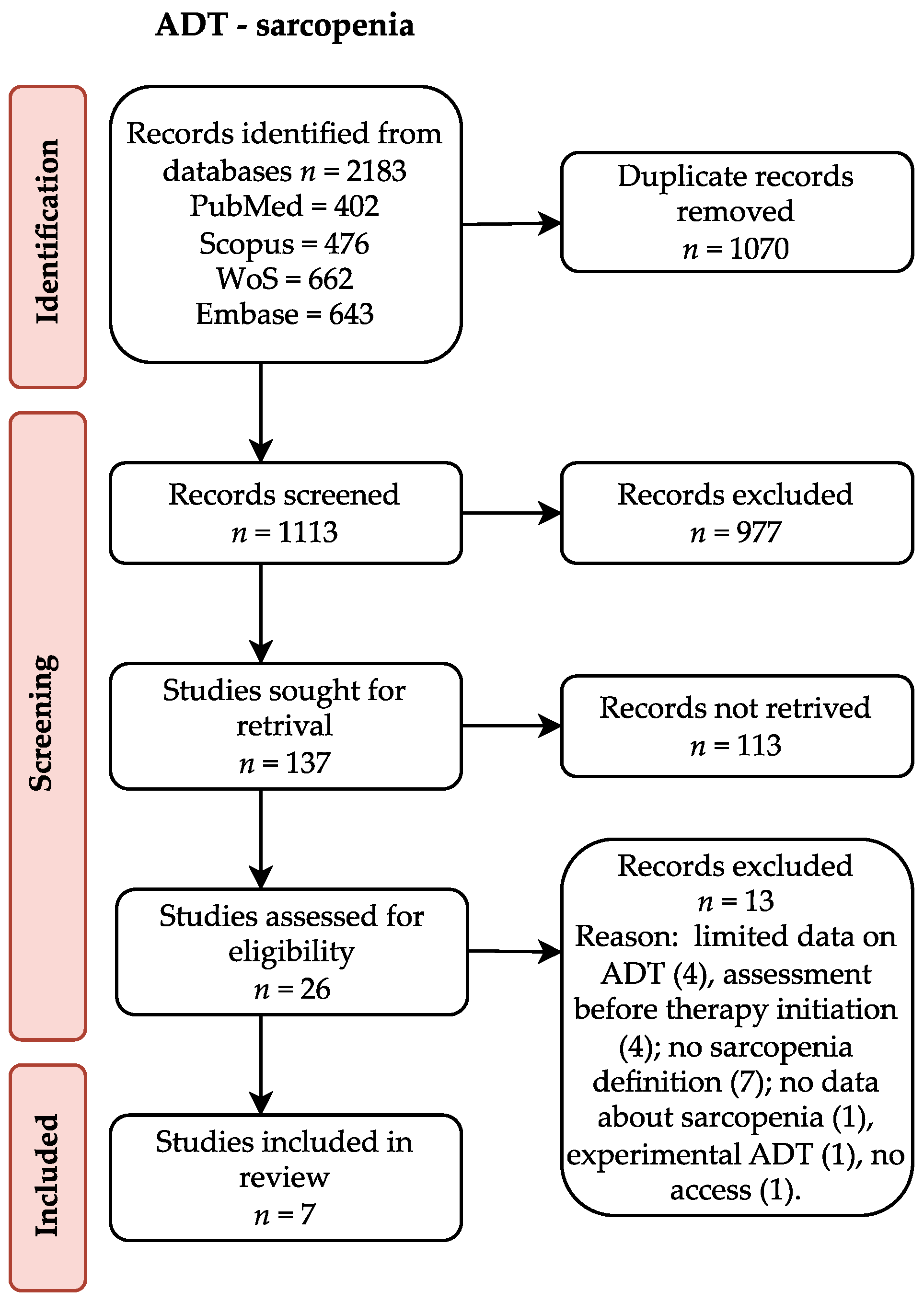
Figure 2.
Forest plot (left) and funnel plot (right) meta-analysis of BMI.
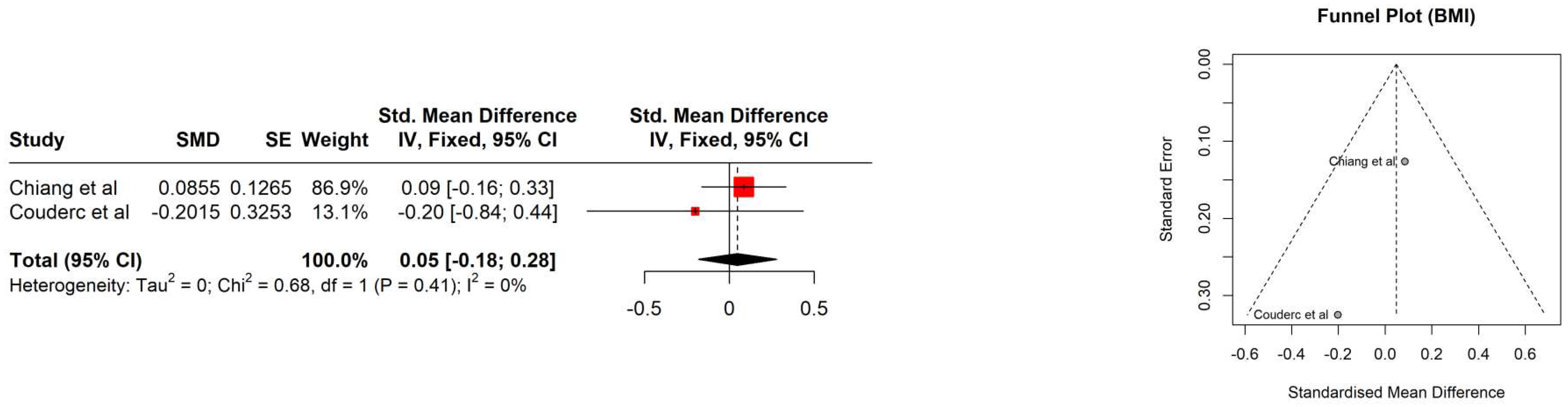
Figure 3.
Forest plot (left) and funnel plot (right) meta-analysis of SATI.
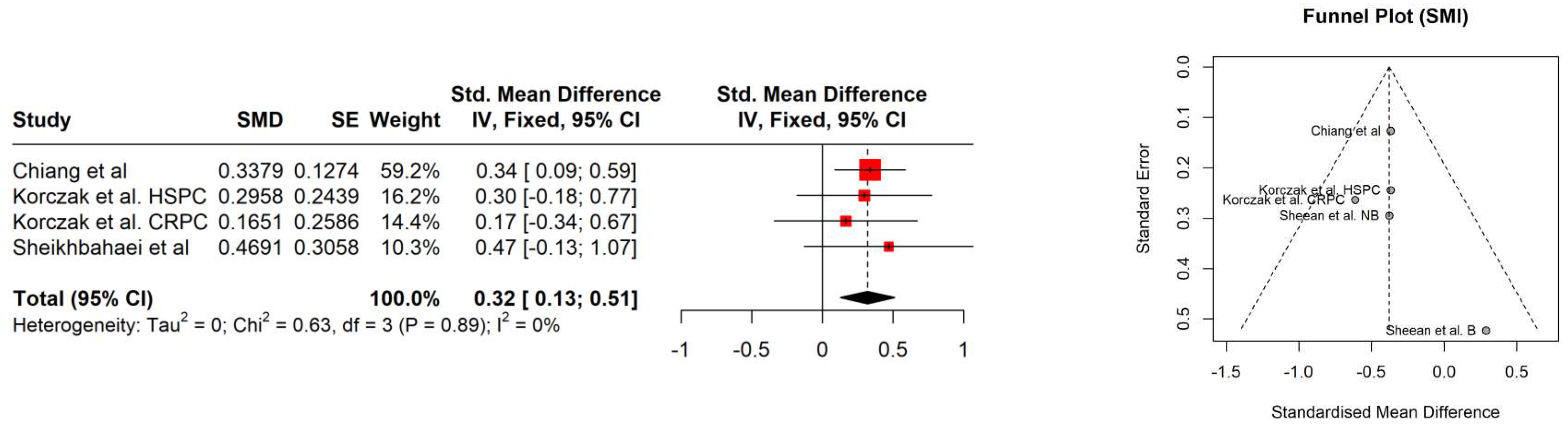
Figure 4.
Forest plot (left) funnel plot (right) meta-analysis of SMD.
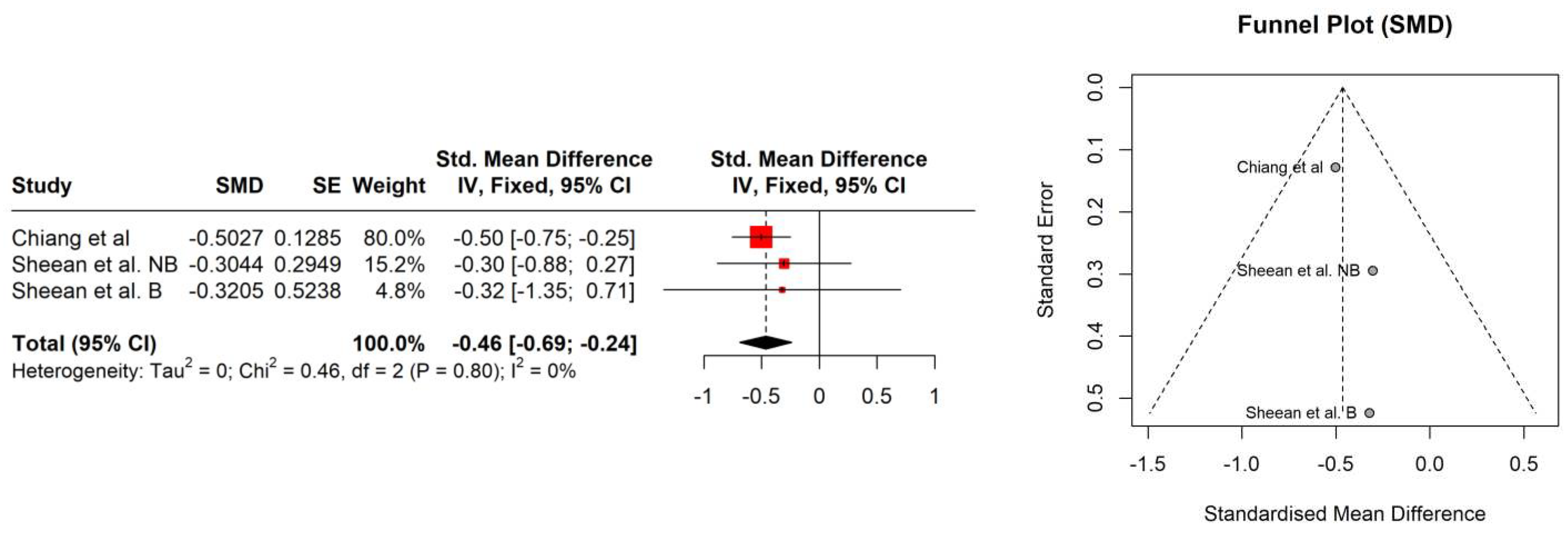
Figure 5.
Forest plot (left) funnel plot (right) meta-analysis of SMI.
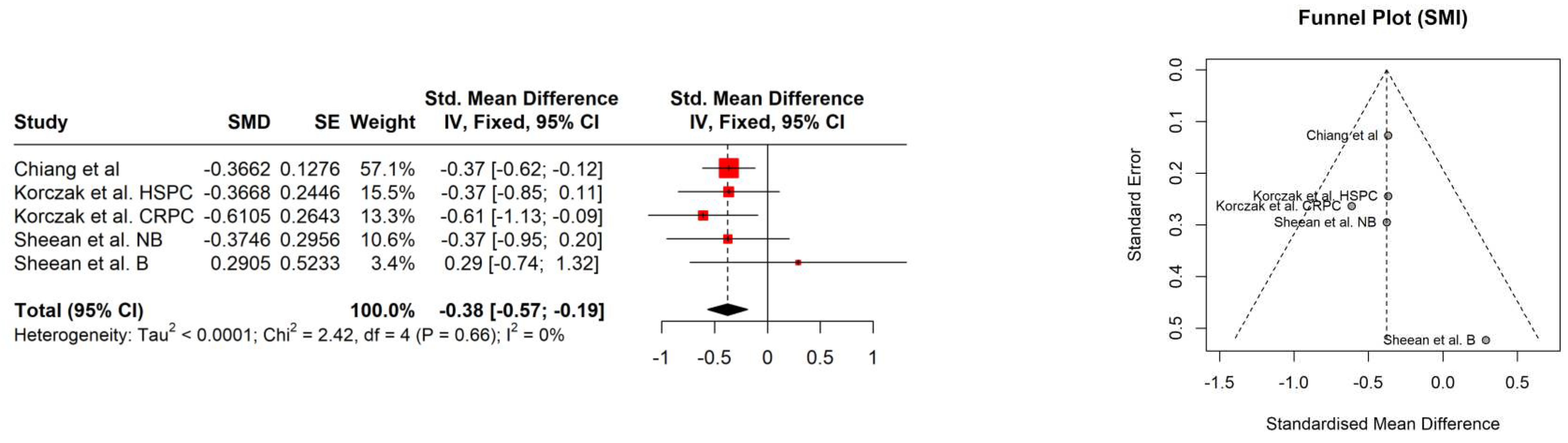
Figure 6.
Forest plot (left) funnel plot (right) meta-analysis of VATI.
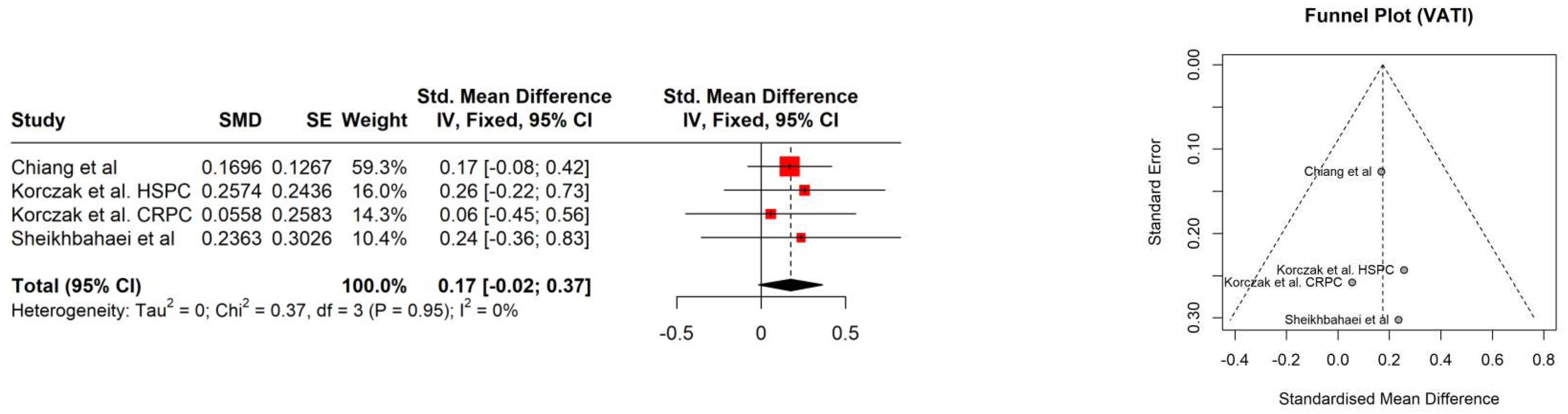
Table 2.
Patients characteristics (baseline) n=802.
| Study | Age [years] | PSA [ng/ml] | Gleason score | Albumin [g/L] | Hb [mmol/l] | Performance status | Comorbidities | BMI [kg/m2] | BMI category |
|---|---|---|---|---|---|---|---|---|---|
| SARCOPENIA ASSESSED AT BASELINE AND FOLLOW-UP | |||||||||
| Chiang et al [24] | 73 median, 67–78 IQR | 27.8 median, 21.2-60.5 IQR | N/A | N/A | N/A | N/A | Age-adjusted CCI: 4 median, 3-5 IQR | 24.2±3.5 | N/A |
| Korczak et al [21] | HSPC: 68.6±7.1 CRPC: 72.0±7.5 |
HSPC: 206.3±547.6 CRPC: 82±155.5 |
HSPC: 8 median, 5-9 range CRPC: 7 median, 4-9 range |
N/A | HSPC: 8.176±0,.8370 CRPC: 8.778±1.406 |
WHO HSPC: 0, 6%; 1, 70%; 2, 24% CRPC: 0, 100% |
Diabetes HSPC: 26.5; CRPC: 16.6 Hypertension HSPC: 61.8; CRPC: 66.7 Ischemic heart disease HSPC: 14.7; CRPC: 46.76 Other HSPC: 44.1; CRPC: 40.0 |
HSPC: 28.5±4.9 CRPC: 29.3±4.4 |
HSPC: underweight 3%; normal: 20%; overweight: 35%; obesity: 42% CRPC: underweight 0%; normal: 19%; overweight: 37%; obesity: 44% |
| Sheean et al [22] | 71 median, 63–79 IQR | N=511 110 median, IQR 35–677 |
7, 36% 8-10, 64% |
N=701 36 median, 34.0–41.0 IQR g/dL |
N=711 7.76 median, 6.83–8.5 IQR |
ECOG 0, 80% ≥1, 20% |
2 median, 1-3 IQR 28% diabetes |
N=711 27.6 median, 24.8–31.1 IQR |
N=551 Normal 22%, overweight 46%, obesity 32% |
| Couderc et al [25] | 80.5±4.3 , 70-88 range | N/A | N/A | 41.8±2.5, 37.6-47.9 range | N/A | N/A | Number of comorbidities 3.4±1.6, 0-7 range ≥5 drugs 58.1% |
26.6±3.6, 21-42 range | N/A |
| Sheikhbahaei et al [26] | 58 median, 54.3–64.3 IQR, 48–75 range | 14 median, 7.2–44 IQR | 8 median, 8–9 IQR, 7–10 range | N/A | N/A | N/A | N/A | 29.3 median, 25.1–33.4 IQR | Normal 22.7%; overweight 27.3%; obese 50% |
| SARCOPENIA ASSESSED AS A SINGLE MEASURMENT DURING ADT | |||||||||
| Owen et al [27] | 71±6 | N/A | N/A | N/A | N/A | N/A | Yes 88.6% If yes, mean 3±1 |
28.8±5.0 | N/A |
| Kimura et al [28] | 79.8±6.4 | 0.67±1.69 | ≤6 16.8% ≤7 27.0% ≥8 56.2% |
N/A | N/A | N/A | ≥3, 16.9% | 23.1±3.0 | N/A |
PSA prostate specific antigen; Hb hemoglobin; IQR interquartile range; ECOG Eastern Cooperative Oncology Group; CCI Charlson Comorbidity Index; HSPC hormone sensitive prostate cancer; CRPC castration resistant prostate cancer. 1 Data collected for limited population.
Table 3.
Cancer and treatment description.
| Study | Cancer | Metastasis sites | Current therapy | ADT drug | ADT duration | Other drugs or intervention |
|---|---|---|---|---|---|---|
| SARCOPENIA ASSESSED AT BASELINE AND FOLLOW-UP | ||||||
| Chiang et al [24] |
NCCN: high-risk 72.0%; very high-risk 28.0% | N/A | ADT+EBRT; 72-76Gy Followed by 2-3 years of adjuvant ADT |
N/A | N/A | N/A |
| Korczak et al [21] |
Metastatic HSPC and CRPC | Bones HSPC: 94%; CRPC: 70% Lymph nodes HSPC: 74%; CRPC: 53% Parenchymal organs HSPC: 3%; CRPC: 0 |
HSPC: ADT+docetaxel 75 mg/m2 79.5%/docetaxel 50mg/m2 20.5%, with radiotherapy 11.8%, prostatectomy 0 CRPC: ADT+abiraterone +predniosne 70%/enzalutamide 30% with radiotherapy 63.3%, prostatectomy 13.3% |
N/A | N/A | Dietary consultation HSPC: 20%; CRPC: 38%; ONS2 for approx. 50% of them if NRS ≥3 |
| Sheean et al [22] |
Metastatic HSPC | Total distant metastases 1 median, 1-2 IQR Bone metastases 76% |
ADT±docetaxel 34% | Androgen receptor inhibitors; gonadotropin-releasing hormone analogues; gonadotropin-releasing hormone antagonists | N/A | N/A |
| Couderc et al [25] |
High-risk 45.2%; intermediate 45.2% |
N/A | N=191 ADT+radiotherapy mean 75.6 Gy |
N/A | N=191 6 months 42.11% 15 months 52.63% 18 months 5.26% |
N/A |
| Sheikhbahaei et al [26] |
Castration naïve oligometastatic cancer | N/A | Neoadjuvant ADT+docetaxel 75/55/35 mg/m2+dexamethasone 2/day, beginning the day before chemotherapy, for 3 days. 45,45%: concurrent abiraterone+prednisone for 1-16 weeks. N=211 radical prostatectomy+radiation therapy to the prostatic/pelvic bed+consolidative stereotactic radiation to metastases |
Luteinizing hormone-releasing hormone agonists | Neoadjuvant therapy 9 weeks median, 9–11 IQR From neoadjuvant therapy to prostatectomy 9 weeks median, 7–10 IQR N=211 ADT for 12 months after prostatectomy |
N/A |
| SARCOPENIA ASSESSED AS A SINGLE MEASURMENT DURING ADT | ||||||
| Owen et al [27] |
Localised/removed 64.3%; advanced 7.1%; unknown 28.6% |
N/A | ADT±prior therapy | Goserelin 57.1% Leuprorelin 20% Goserelin+bicalutamide 7.1% Leuprorelin+bicalutamide 4.3% Triptorelin 4.3% Degarelix 2.9% Abiraterone 1.4% Degarelix+bicalutamide 1.4% Enzalutamide 1.4% |
Min 12 weeks; 25±36 months | Previous prostatectomy 48.6% Previous radiotherapy 68.6% Previous chemotherapy 15.7% |
| Kimura et al [28] |
T1 10.1%; T2 39.3%; T3/T4 50.6% | N/A | ADT±prior therapy | N/A | 83.6±57.6 months | Prostatectomy 6.7% Radiation 21.3% |
BMI body mass index; NCCN National Comprehensive Cancer Network; HSPC hormone sensitive prostate cancer; CRPC castration resistant prostate cancer; ADT androgen deprivation therapy; EBRT external beam radiation therapy; ONS oral nutritional support; NRS nutritional risk score. 1 Data collected for limited population. 2125 mL including 18 g of protein and 300 kcal.
Table 4.
Body composition: BMI and body composition parameters.
| Study | BMI [kg/m2] baseline | BMI [kg/m2] follow up | Appendicular mass [kg/m2] | PMI [cm2 /m2] baseline | PMI [cm2 /m2] follow up | SMI [cm2/m2] baseline | SMI [cm2/m2] follow up | SMD [HU] baseline | SMD [HU] follow up | SATI [cm2/m2] baseline | SATI [cm2/m2] follow up | VATI [cm2/m2] baseline | VATI [cm2/m2] follow up | TATI [cm2/m2] baseline | TATI [cm2/m2] follow up |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SARCOPENIA ASSESSED AT BASELINE AND FOLLOW-UP | |||||||||||||||
| Chiang et al [24] | 24.2±3.5 | 24.5±3.5 | N/A | N/A | N/A | 47.2±7.4 | 44.5±7.3 | 37.8±5.6 | 34.9±5.9 | 39.9±13.6 | 44.7±14.7 | 55.2±28.0 | 60.1±29.6 | 95.1±37.7 | 104.6±40.4 |
| Korczak et al [21] | HSPC: 28.5 ± 4.9 CRPC: 29.3 ±4.4 |
N/A | N/A | N/A | N/A | HSPC: 54.01± 9.85 CRPC: 52.0±8.311 |
HSPC: 50.4 ±9.61 CRPC: 47.4±6.46 |
N/A | N/A | HSPC: 66.47±33.36 CRPC: 86.1±29.7 |
HSPC: 78.2±39.2 CRPC: 92.01±40.2 |
HSPC: 90.40± 44.2 CRPC: 110.2±37.9 |
HSPC: 101.7±42.6 CRPC: 112.4±39.89 |
N/A | N/A |
| Sheean et al [22] | N = 711 27.6 median, 24.8–31.1 IQR |
N/A | N/A | N/A | N/A | N=551 49.8 median, 40.2–56.2 IQR |
Non-black N=141: −3.7 median, (−8.5)–(−0.4) IQR (7% loss) Black N=51: −1.2 median, (−1.8)–12.5) IQR (2% gain) |
N=551 33.8, median 26.3–41.8 IQR | Non-black N=141: −5.7 median, (−9.6)−(3.2) IQR (14%) Black N=51: −5.3 median, (−7.2)−(−1.4) IQR (12%) |
N=551 51.9 median, 33.3–69.4 IQR |
Subcutaneous adipose tissue change [cm2] Non-black N=141: 23.2 median, (−6.5)−51.5 IQR (5% gain) Black N=51: 95.2 median, (89.4–172.3) IQR (8% gain) |
N=551 61.6 median, 33.6–98.9 IQR |
Visceral adipose tissue change [cm2] Non-black N=141: −16.0 median, (−32.2)−3.5 IQR (1% gain) Black N=51: median 40.1, 29.4–41.0 IQR (2% gain) |
N/A | N/A |
| Couderc et al [25] | N=191 26.1±2.6, 21-32 range |
N=191 25.5±3.2, 18-31.9 range |
ASSM/height2 <7.0 for 2 patients | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A |
| Sheikhbahaei et al [26] | 29.3 median, 25.1–33.4 IQR | N/A | N/A | 8.7 median, 8.11–11.3 IQR Psoas muscle mass 27.5 median, 24.6–36.7 IQR |
Psoas muscle area I: −13.9% (−7.6, −16.5) II: −13.2(−6, −11.2)) |
N/A | N/A | N/A | N/A | 72.4 median, 51.0–107.1 IQR Subcutaneous adiposity [cm2]: 217 median, 159.8–340.9 IQR |
Subcutaneous fat [cm2] I: +8.9(+5.1, +21.5) II: +18.9(+6.1, +33.8) |
81.6 median, 46.4–102.9 IQR Visceral adiposity [cm2]: 261.3 median, 142.4–326.9 IQR |
Visceral fat [cm2] I: −1.6(−9.9, +18,7) II: +8.4(−1.7, +23.8) |
Total adiposity [cm2] 476.8 median, 389.8–685 IQR |
Total adiposity[cm2] I: +5.7(+0.8, +15.2) II: +10.3(+2.7, +28.5) |
| SARCOPENIA ASSESSED AS A SINGLE MEASURMENT DURING ADT | |||||||||||||||
| Owen et al [27] | 28.8 ±5.0 | ALMI 8.07±0.95 ALMBMI 0.875±0.117 |
N/A | N/A | N/A | N/A | N/A | N/A | |||||||
| Kimura et al [28] | 23.1±3.0 | N/A | N/A | 7.23±1.10 [kg/m2] | 0.20±0.04 | N/A | N/A | N/A | |||||||
BMI body mass index; HSPC hormone sensitive prostate cancer; CRPC castration resistant prostate cancer; HU Hounsfield units; PMI psoas muscle index; ALMBMI appendicular lean mass adjusted for body mass index; ALMI appendicular lean mass index; ASMM Appendicular Skeletal Muscle Mass; SMD skeletal muscle radiodensity; SMI skeletal muscle index; SATI subcutaneous adipose tissue index; TATI total adipose tissue index; VATI visceral adipose tissue index; FFMI fat-free mass index. 1 Data collected for limited population.
Table 5.
Sarcopenia characteristics.
| Study | Sarcopenia definition | Assessment | Assessment methodology | Sarcopenia at baseline | Sarcopenia at follow up | Time to follow up | Significance of outcomes | Correlation between survival and sarcopenia |
|---|---|---|---|---|---|---|---|---|
| SARCOPENIA ASSESSED AT BASELINE AND FOLLOW-UP | ||||||||
| Chiang et al [24] |
SMI: <43.2cm2/m2 | CT: L3 level | One blinded researcher. | 33.6% | 48.0% | 180 days median, 146-223 IQR | p=0.001 | Sarcopenia at baseline was not associated with 3-year non-cancer-specific survival and 3-year prostate cancer-specific survival. |
| Korczak et al [21] |
SMI: 1. 53cm2/m2 2. 43cm2/m2for BMI <25 kg/m2 3. Sarcopenic obesity: <53cm2/m2 for BMI >30kg/m2 |
CT: L3 level | Software CoreSlicer.com. Manual correction. | HSPC: 47.06% CRPC: 46.67% |
HSPC: 58% CRPC: 79.3% |
12.33 months median, 5.4-26 range | HSPC: NS CRPC: p=0.015 |
Sarcopenia was not correlated with progression-free survival. |
| Sheean et al [22] |
SMI: 1. 53cm2/m2 2. 43cm2/m2for BMI <25kg/m2 3. Sarcopenic obesity: <53cm2/m2for BMI >30kg/m2 |
CT: L3 level | Automated tissue demarcation. Manual correction. 10 images were assessed for quality assurance. | N=55 49% (15% of N=55 had sarcopenic obesity) |
N=8 0% |
12.5 months median |
N/A | Sarcopenia was not correlated with overall survival. |
| Couderc et al [25] |
EWGSOP2 guidelines Hand-grip <27kg DXA ASSM/height² <7.0kg/m2 |
Baseline: hand-grip strength Follow-up: DXA |
Hand-grip strength test was performed according to ASHT recommendations. | N=311 Probable sarcopenia 25% |
N=61 1 patient |
N/A | N/A | N/A |
| Sheikhbahaei et al [26] |
PMI <5.7cm2/m2 Sarcopenic obesity: PMI <5.7cm2/m2 for BMI >30kg/m2 |
CT: L3-L4 level | Manual analysis of anonymized images twice at different time points. Third reviewer assessed differences. | Sarcopenic obesity 9.1% | No change at both follow up CTs | First: 3 months median, 2–3 IQR Second: 12 months median, 10.5–17.5 IQR |
N/A | N/A |
| SARCOPENIA ASSESSED AS A SINGLE MEASURMENT | ||||||||
| Owen et al [27] |
ALMHFM ≤−1.816 and weak handgrip strength and/ or slow gait speed based on EWGSOP1, EWGSOP2, FNIH and IWGS |
Handgrip dynamometer 4 m walk test DXA |
Six tests, three for each hand, were performed for dynamometry (the highest). Dynamometer Jamar Plus Digital. Three test for gait speed were performed (the fastest). For DXA researchers were blinded. Software 12.30.008 (Lunar iDXA, GE Lunar Corp., Madison, USA). |
ADT group: FNIH 1.0% EWGSOP1 1.0% EGSOP2 or IWGS 0 No-ADT group: EWGSOP1 1.92% Healthy group EWGSOP1 1.43% |
N/A | N/A | N/A | |
| Kimura et al [28] |
Walking speed <0.8m/s and/or handgrip strength <26kg+ SMI <7.0kg/m2 Sarcopenic obesity: sarcopenic criteria+body fat ≥25% |
Handgrip dynamometer 5m walking BIA |
Two tests were performed for dynamometry (the highest) and walking test (average). Dynamometer TKK 5401. BMI system MC-780A. | Sarcopenia non-obese 15.7% Sarcopenic obesity 13.5% |
N/A | N/A | N/A | |
CT computed tomography; BIA bioelectrical impedance analyzers; SMI skeletal muscle index; PMI psoas muscle index; HSPC hormone sensitive prostate cancer; CRPC castration resistant prostate cancer; EWGSOP1 European Working Group on Sarcopenia in Older People 2010; EWGSOP2 European Working Group on Sarcopenia in Older People 2018; FNIH Foundation for the National Institutes of Health; IWGS International Working Group on Sarcopenia; ASHT American Society of Hand Therapists. 1 Data collected for limited population.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



