
Submitted:
19 January 2024
Posted:
22 January 2024
You are already at the latest version
Abstract
Purpose: This study aimed to elucidate the various new classifications and the use of LDLT in this context for HCC beyond milan criteria.
Methods: The clinical data of patients with HCC outside milan criteria who underwent LT at Jena University between Januar 2007 and August 2023 were retrospectively analyzed. Eligible patients were classified according to various classification systems. Clinicopathological features, overall- and disease-free survival rates were compared between the two groups (LT vs. LDLT) and in context for bridging therapy.
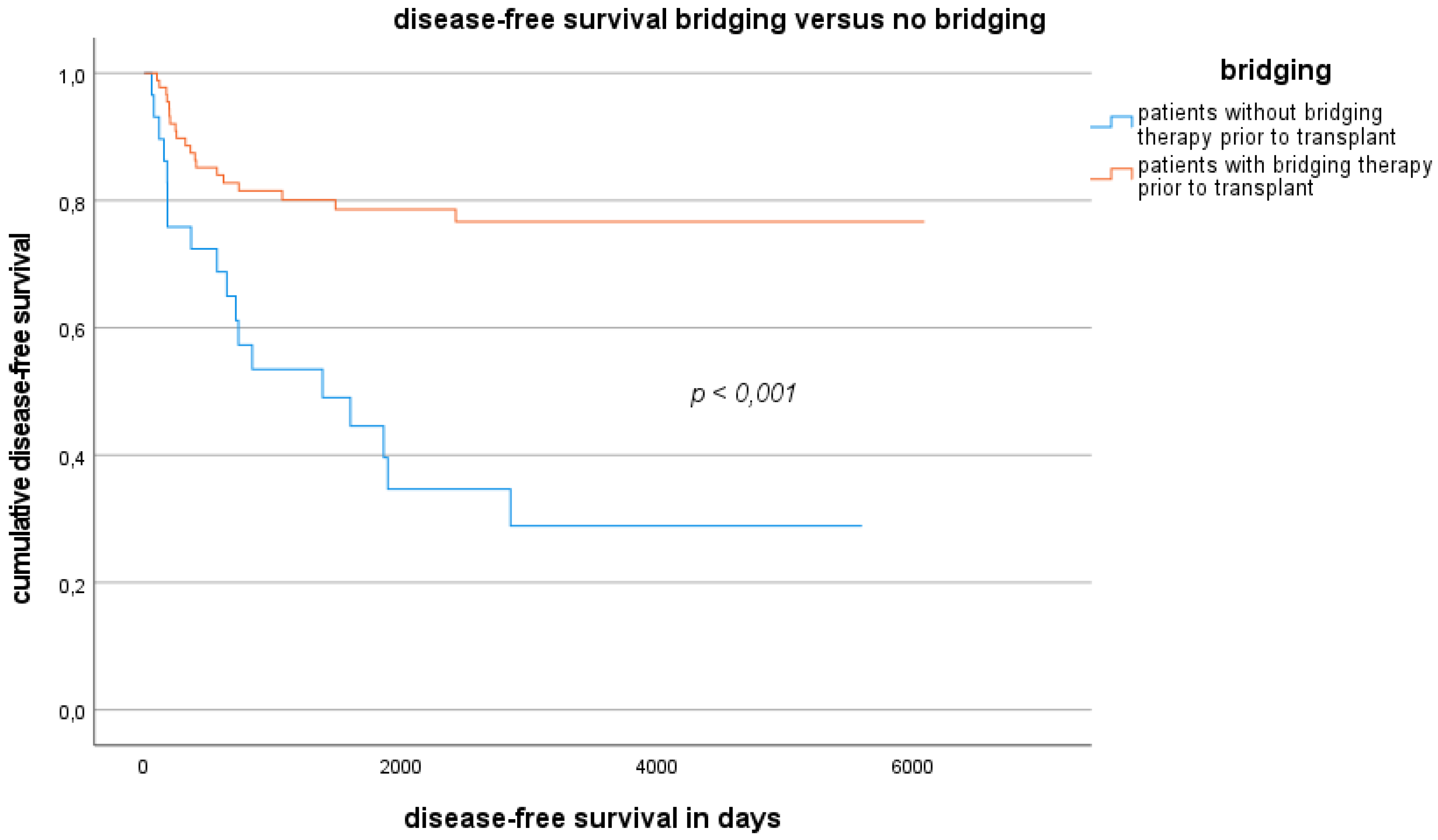
Results: Among the 245 patients analyzed, 120 patients were outside milan criteria and 125 patients were inside milan. There was no significant difference for patients outside milan in overall survival for LT versus LDLT (OS 44,3 months vs. 28,3 months; 5y survival, 56,4% vs. 40%; p = 0.84). G3 tumor differentiation, presence of angioinvasion and lack of bridging were statistically significant risk factors predicting tumor recurrence in univariate and multivariate analysis (HR 6.34; p = 0.0002; HR 8.21; p < 0.0001; HR 7.50; p = 0.0001). Bridging therapy before transplantation provides a significant survival advantage regardless of the transplant procedure (OS: p = 0.008 ; DFS: p < 0.001).
Conclusions: Patients with HCC outside milan criteria who underwent LT or LDLT had comparable outcome to patients inside milan criteria. Nevertheless, these patients remain disadvantaged on the waiting list, which is why LDLT represents a safe alternative to LT and should be considered in bridged HCC patients depending on tumor differentiation, size and tumor marker dynamics.
Keywords:
hepatocellular carcinoma
; Milan criteria
; living-donor liver transplantation
; transplant outcome
Introduction
Liver transplantation (LT) is the only curative option for patients with liver cirrhosis and hepatocellular carcinoma (HCC)1. HCC represents the most common malignant indication for LT2.
The Milan criteria3 (MC) were introduced in 1996 to assess the prognosis after LT for patients with hepatocellular carcinoma and liver cirrhosis and are still used today for organ allocation, with the standard exception of the MELD score, to prioritize patients with HCC inside the MC in the Eurotransplant area. In this region, organ allocation is based on the MELD system, and patients with hepatocellular carcinoma fulfilling the MC can generate exceptional points regardless of their labMELD score on the waiting list.
After more than 25 years of MC use, adjustments to the organ allocation criteria for patients with HCC outside of the Milan population are now being discussed, and even Mazzaferro et al. discussed expanding their own criteria over time4.
Bridging procedures such as transcatheter arterial chemoembolization and selective internal radiotherapy have been able to further improve oncological outcomes in patients with HCC, and new therapeutic approaches such as immunotherapy have been established5,6,7,8,9,10. Even if immune checkpoint inhibition is currently not implemented in the bridging of patients with HCC on the waiting list, it is encouraging that this approach has the potential to further improve bridging therapy in combination with conventional bridging methods8,11,12,13.
The present guidelines for HCC outside the MC are currently being further adapted internationally, for example, in the University of California San Francisco criteria (UCSF)14, the extended Toronto criteria for liver transplantation15, the up-to-seven rule4, the Japanese 5-5-500 rule16, adapted treatment recommendations for patients with hepatocellular carcinoma in Spain (Barcelona Clinic Liver Cancer classification)17 and in the transplant region of Australia and New Zealand18.
The prognostic factors relevant for HCC in the context of LT were tumour morphology, tumour biology, tumour grade, cancer-related symptoms, the dynamics of the tumour biomarker alpha-fetoprotein, the response to bridging therapy19 and the presence of angioinvasion.
Because the organ donation shortage in some transplant regions causes the waiting time and the average MELD score at the time of LT to continually increase, the probability of LT for patients with HCC outside the MC decreases, and thus, the number of HCC-associated deaths on the waiting list increases20,21,22. Therefore, the allocation criteria for these patients should be adjusted to allow them fair access to donor organs. The impportance of the various new classification systems has not been conclusively assessed. These developments have led to the importance of LDLT for HCC patients, and an increasing in LDLT is also being seen in non-Asian transplant centres21.
The aim of the work was to show the results of liver transplants in patients with HCC inside and outside the MC and to compare the different HCC classifications with each other based on the results of the study population. Therefore, we wanted to demonstrate our bridging and transplantation strategies for these patients and the use of living liver donation. The primary endpoints for this study were overall survival (OS) and disease-free survival (DFS). Markers for poor transplant outcome and oncological outcome were identified in our study population through univariate and multivariate analyses.
Materials and Methods
Patient selection
The clinical data of the patients were collected through a retrospective review of medical records. Eligible patients were those who were diagnosed with HCC or who underwent LT for HCC between January 2007 and August Patient data were retrieved from the hospital database. Patients who underwent LT before January 2007 (before the introduction of the MELD score23 system for organ allocation in the Eurotransplant area) were not included.
Details on organ allocation and information about the donor were obtained from the 245 patients via the Eurotransplant database (ENIS-next).
In addition, patients who were delisted from the waiting list were evaluated via the centre list during the period examined.
Outcome measures
All eligible patients who underwent LT or LDLT were stratified into two groups according to the MC. In the outside-Milan group, information about tumour location, bridging therapy, treatment response to bridging therapy, postoperative survival time, postoperative complications, hospital stay, ICU stay, tumour size, number of tumour nodes, histopathological findings, duration of alpha-fetoprotein perioperatively, and the timing of recurrence and treatment of the recurrence were investigated. The patients in the outside-Milan group were then further classified according to the expanded criteria (UCSF, Toronto, 5-5-500-rule, UTSC, BCLC).
Patients with HCC according to the MC were then categorized into two groups to compare the outcomes according to the surgical procedure (LDLT vs. LT).
Comparisons of preoperative factors, surgery-related factors, pathological findings, postoperative course, overall survival (OS) and disease-free survival (DFS) rates were performed between the two groups. The independently associated factors for OS and DFS were investigated.
Statistical analysis
A normality test could not verify the normality of the data. Therefore, median values were calculated, and nonparametric statistical tests were used (the Shapiro‒Wilk test and the Kolmogorov‒Smirnov test). Clinical factors were compared using the Chi-square test, Fisher’s exact test, and Mann–Whitney U test. DFS was calculated from the date of transplantation to the first imaging-proven evidence of recurrence. DFS and OS curves were established using the Kaplan–Meier method and compared using log-rank tests. The Cox proportional hazards model was used to calculate hazard ratios (HRs) with 95% confidence intervals (CIs) for the risk factors for DFS and OS. Factors that were significant in the univariate analysis were included in the multivariate analysis.
All the statistical analyses were performed using IBM® SPSS Statistics 29 (IBM®, Armonk, USA). A p value of <0.05 was considered indicative of statistical significance.
General medical data and parameters related to transplant outcomes were examined for the included patients. The patients were then grouped according to whether bridging was performed, which transplant procedure was used (LT vs. LDLT) or whether they developed a recurrence.
Results
Epidemiology
A total of 245 patients who underwent LT for hepatocellular carcinoma at the Jena University Hospital Transplant Center between January 2007 and August 2023 were enrolled in this study as shown in Figure Of these, 125 (51%) patients met the MC, and 120 (49 %) were outside the MC. The general epidemiological data for patients inside and outside the MC are presented in Figure 2 and LDLT was performed in significantly younger patients with lower MELD scores and larger tumours; these patients were less likely to be able to undergo bridging therapy successfully and were less likely to have decompensated liver cirrhosis. LDLT was always used when the urgency of the transplant in relation to the oncological outcome was not adequately reflected by the MELD system, and the time window for a promising transplant was therefore too short. As shown in Figure 1, many patients with HCC cannot receive transplantation in a timely manner and therefore have to leave the transplant waiting list due to disease progression and associated death.
The median follow-up period for all patients was 114 months.
Overall survival rate inside and outside the MC
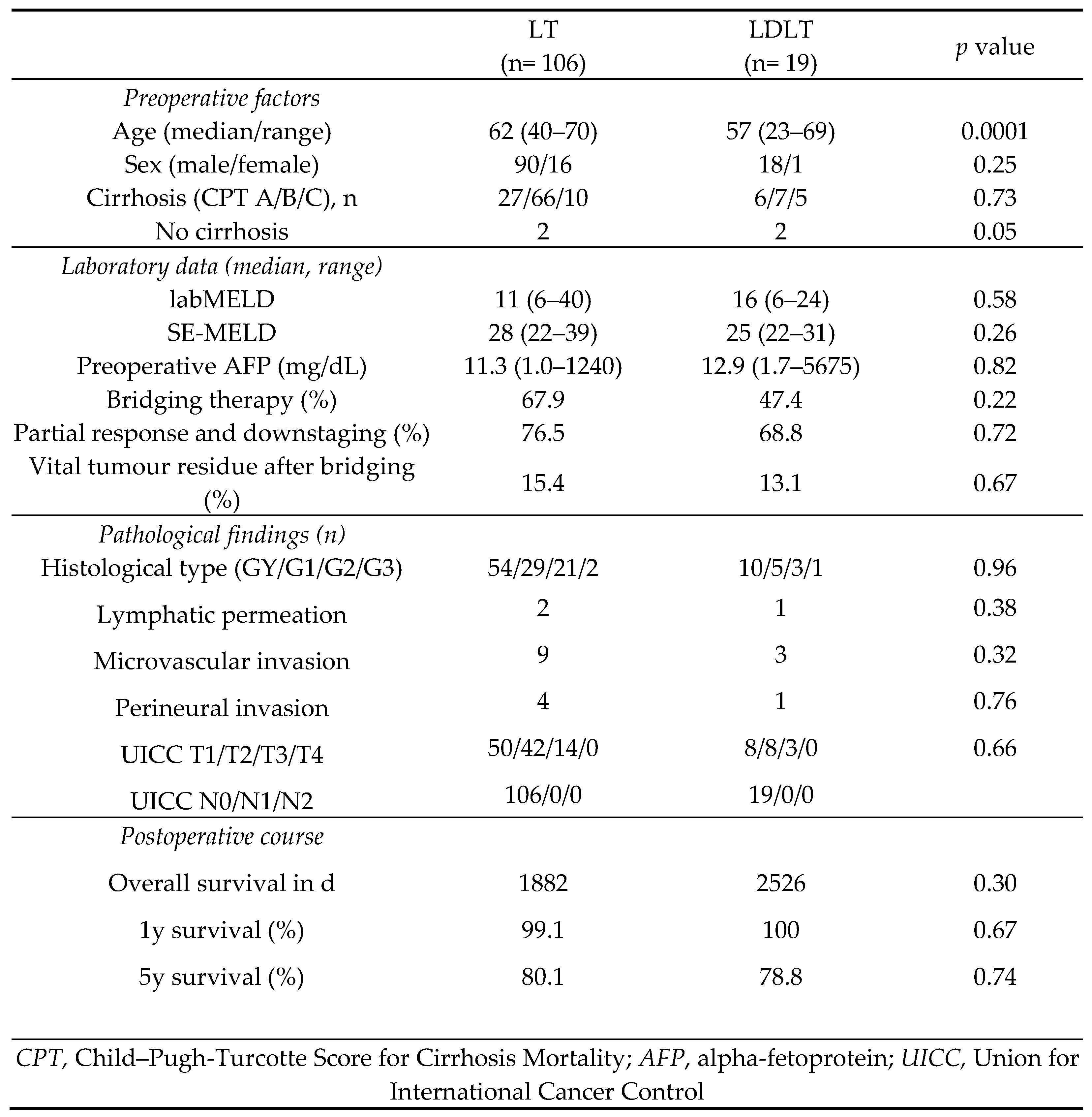
The median OS time in the LDLT inside the MC group was 84.2 months, and the overall 1- and 5-year survival rates were 100% and 78.8%, respectively (Figure 2). The median OS time in the LT group inside the MC was 62.8 months, and the overall 1- and 5-year OS rates were 99.1 % and 80.1 %, respectively. There were no significant differences between the LDLT and LT groups (p = 0.30).
The median OS time in the LDLT outside-MC subgroup was 28.3 months, and the overall 1- and 5-year survival rates were 84.2% and 40%, respectively (Figure 3). The median OS time in the LT outside-MC group was 44.3 months, and the overall 1- and 5-year OS rates were 75.9% and 56.4%, respectively. OS was not significantly shorter in the LDLT group (p = 0.52).
Figure 3.
Characteristics of patients with HCC outside the Milan range stratified by transplantation.
Figure 3.
Characteristics of patients with HCC outside the Milan range stratified by transplantation.
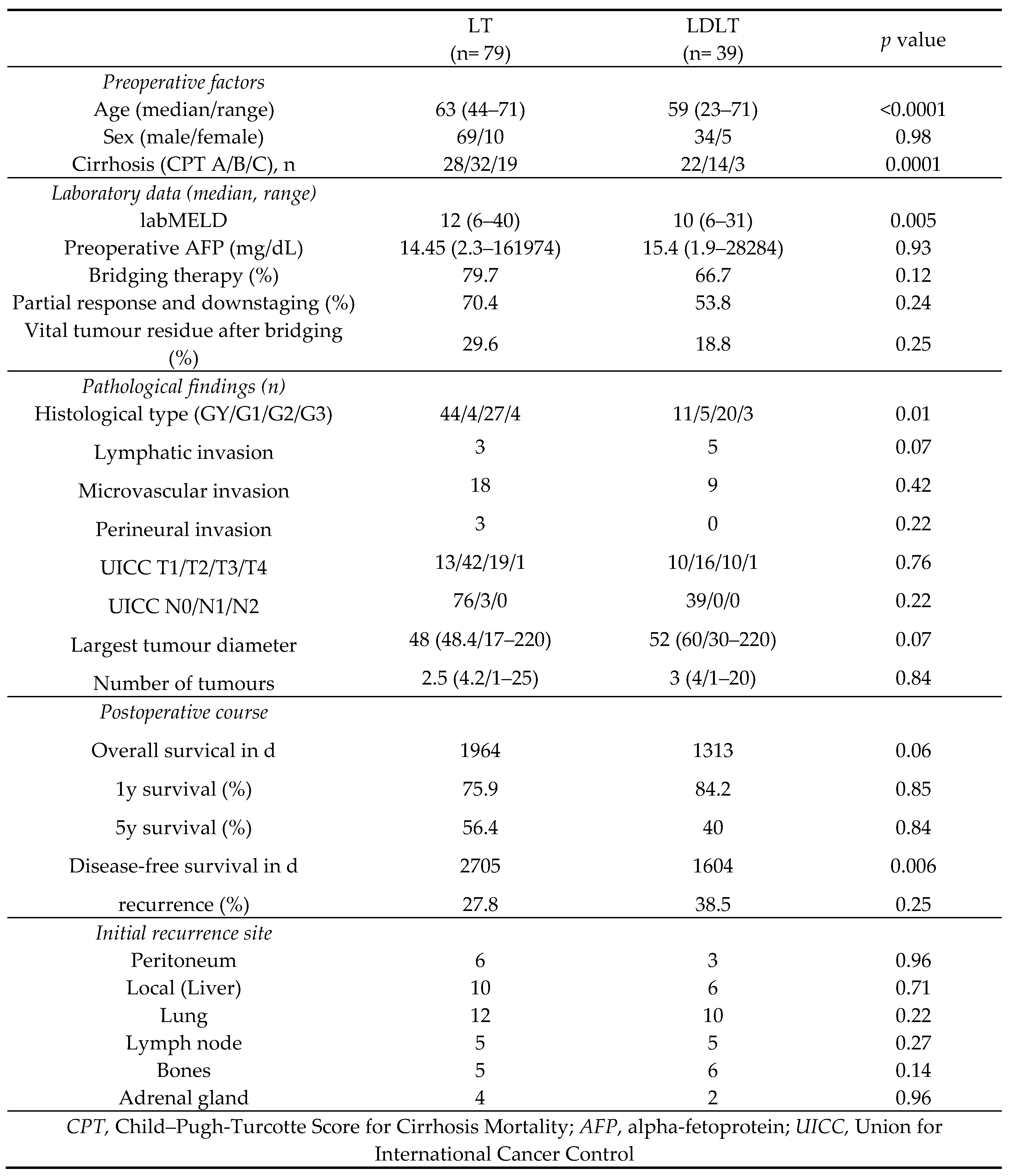
Figure 4.
Cox proportional hazard analysis of risk factors for disease-free survival AFP, alpha-fetoprotein; Complication, Complication Clavien‒Dindo ≥3a.
Figure 4.
Cox proportional hazard analysis of risk factors for disease-free survival AFP, alpha-fetoprotein; Complication, Complication Clavien‒Dindo ≥3a.
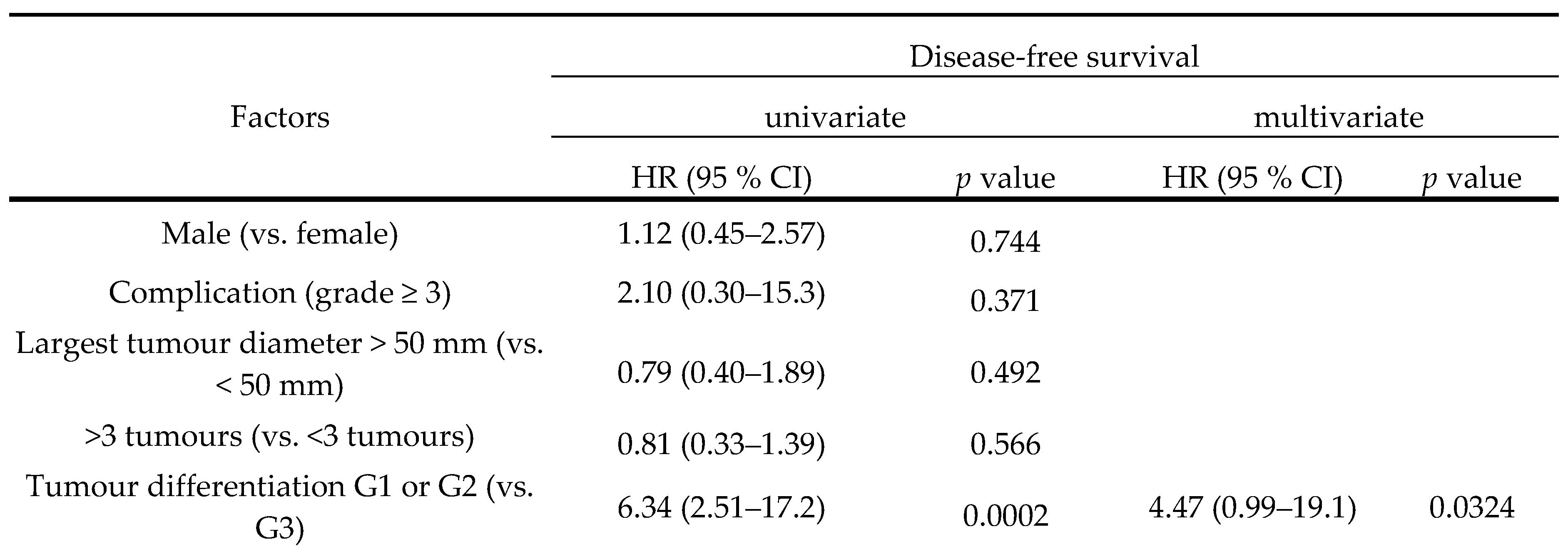
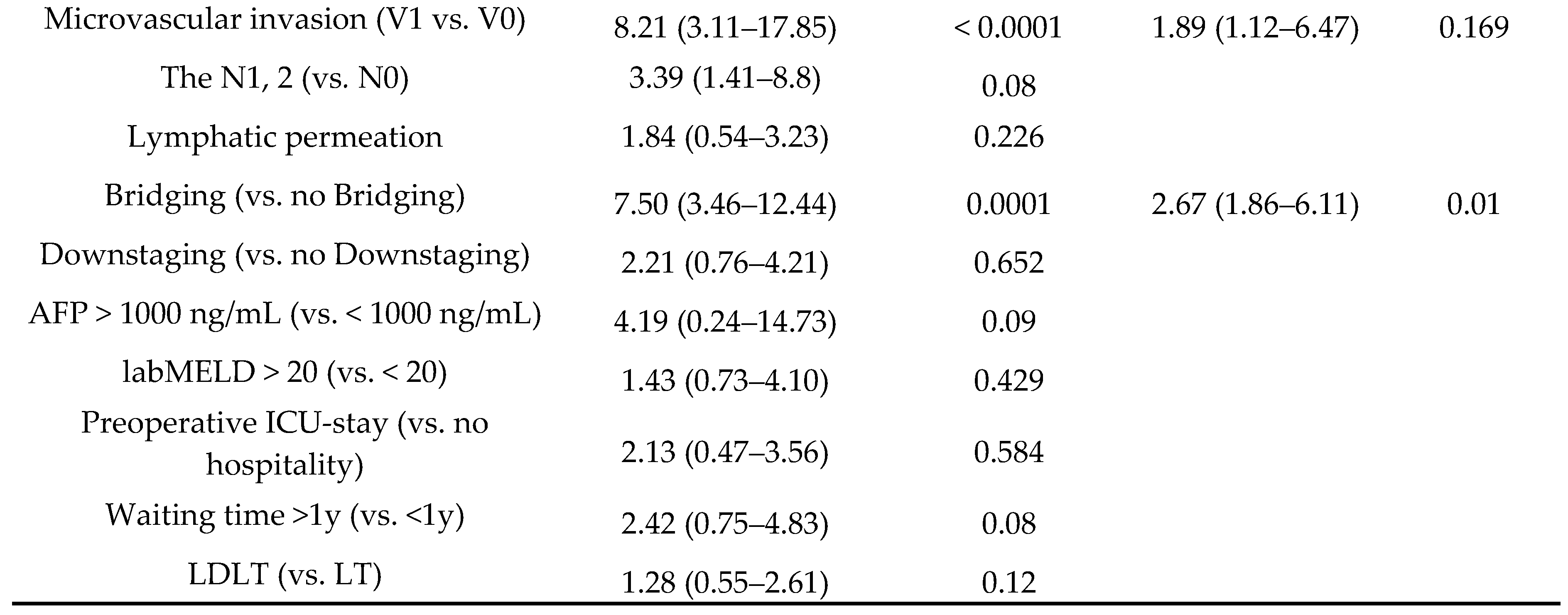
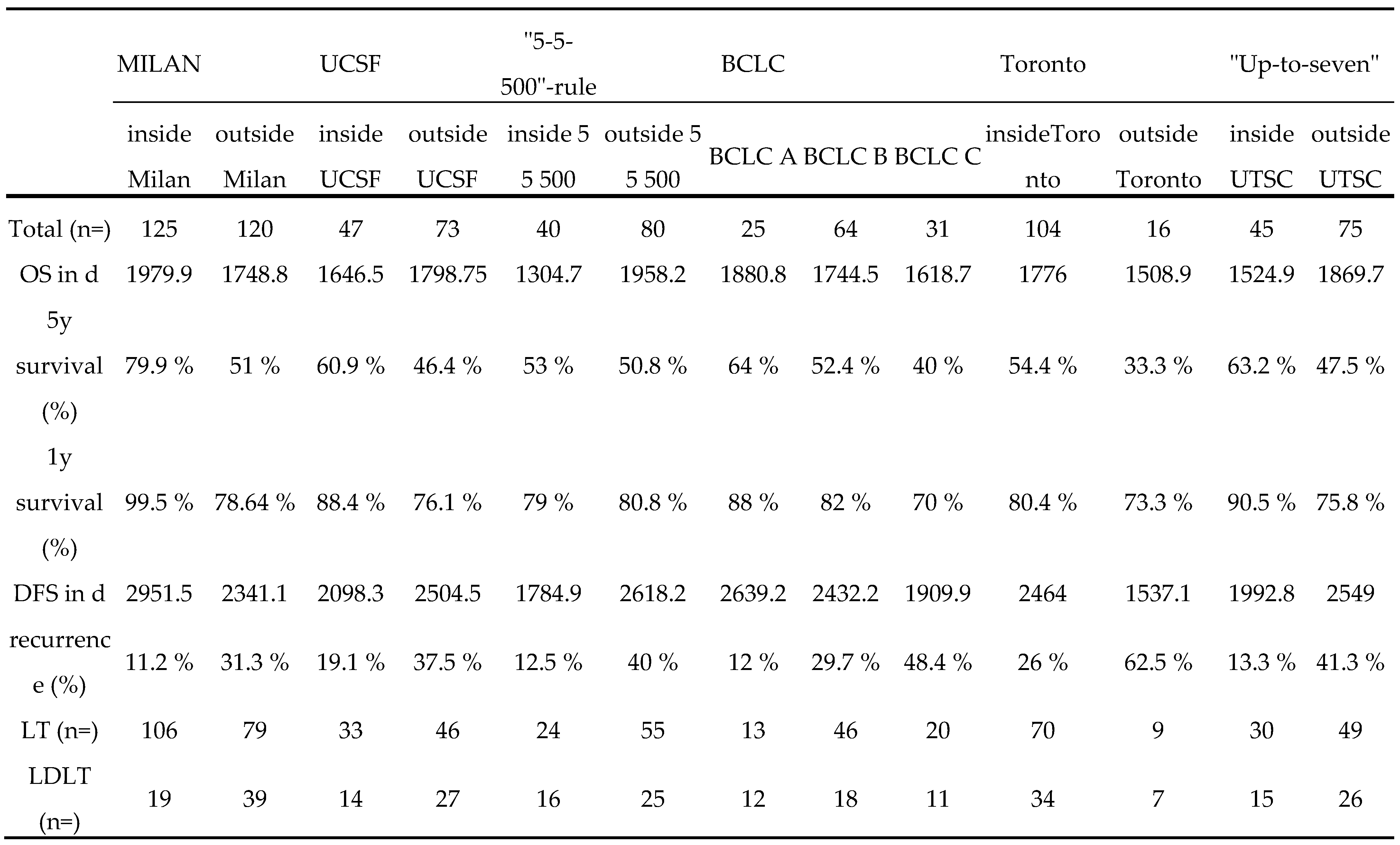
Figure 5.
Comparison of HCC classification systems.
DFS and OS for patients who underwent LDLT or LT outside the MC
The DFS and OS of patients in the LDLT group and LT group are presented as Kaplan‒Meier curves in Figure 6 and Although the OS in the LDLT group was lower, the groups did not significantly differ.
Figure 6.
OS and DFS for LT versus LDLT outside the MC.
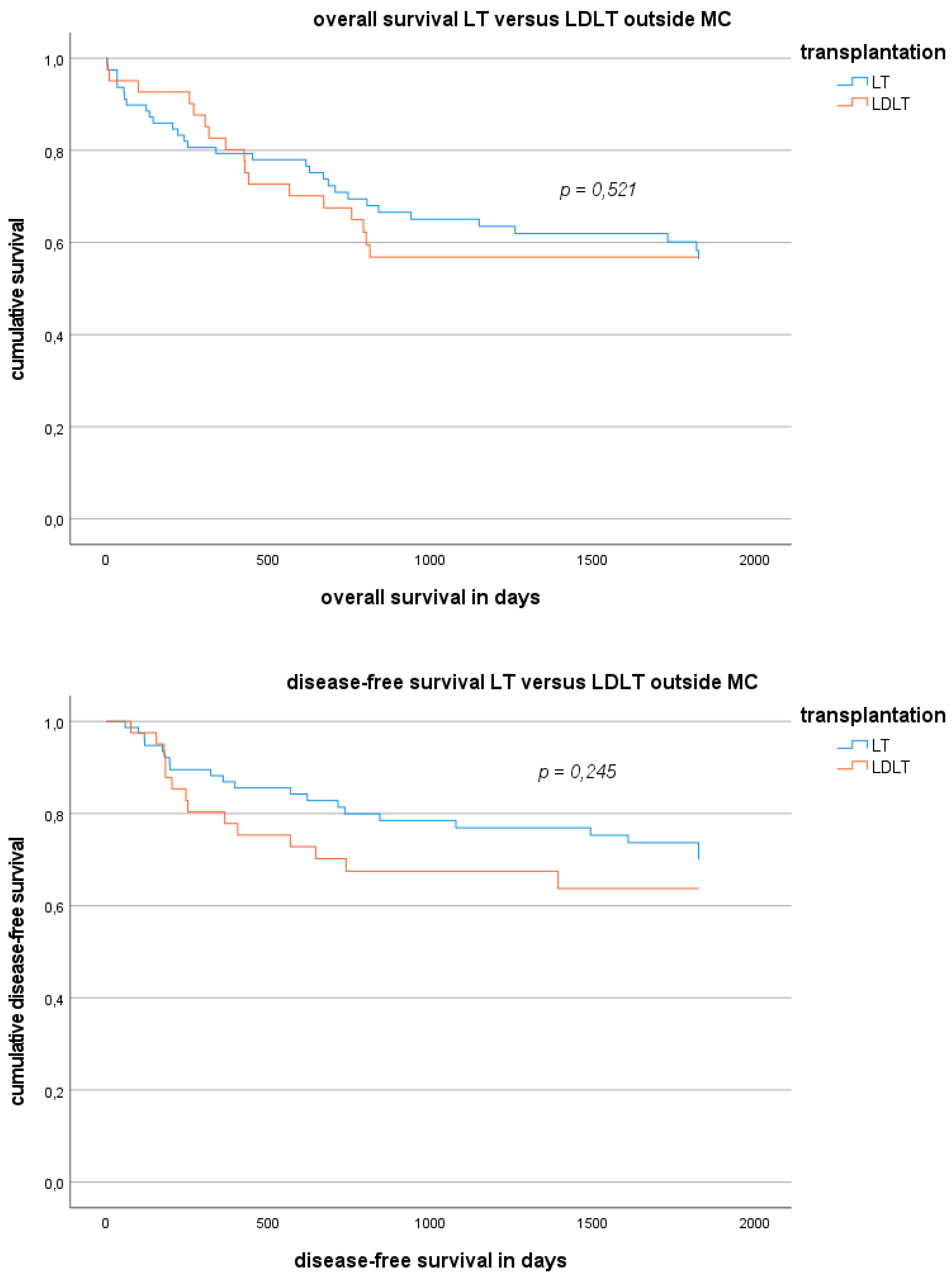
Figure 7.
DFS for LT versus LDLT inside and outside the MC.
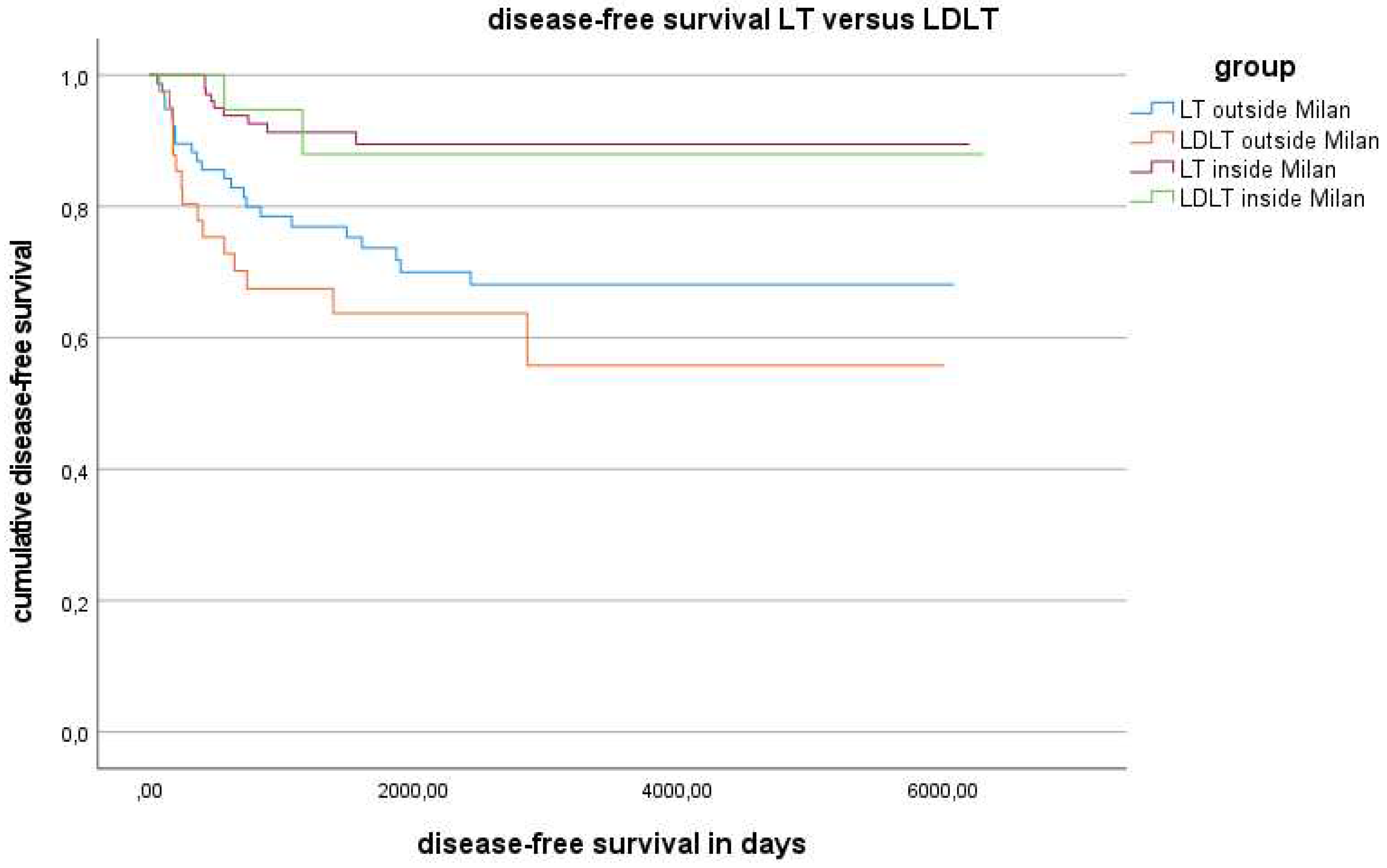
Figure 8.
OS depending on bridging therapy inside and outside the MC.
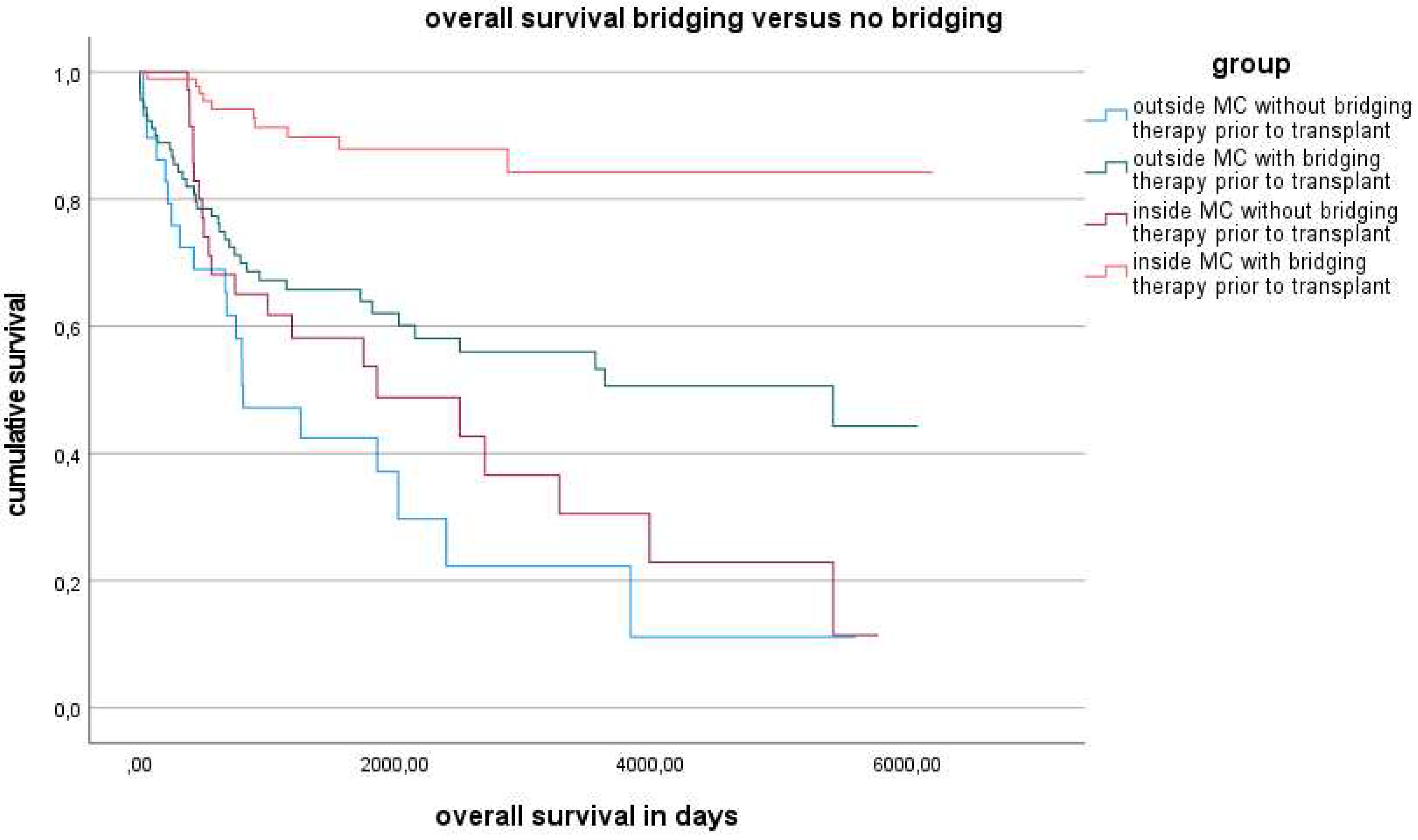
Figure 9.
DFS depending on bridging therapy inside and outside the MC.
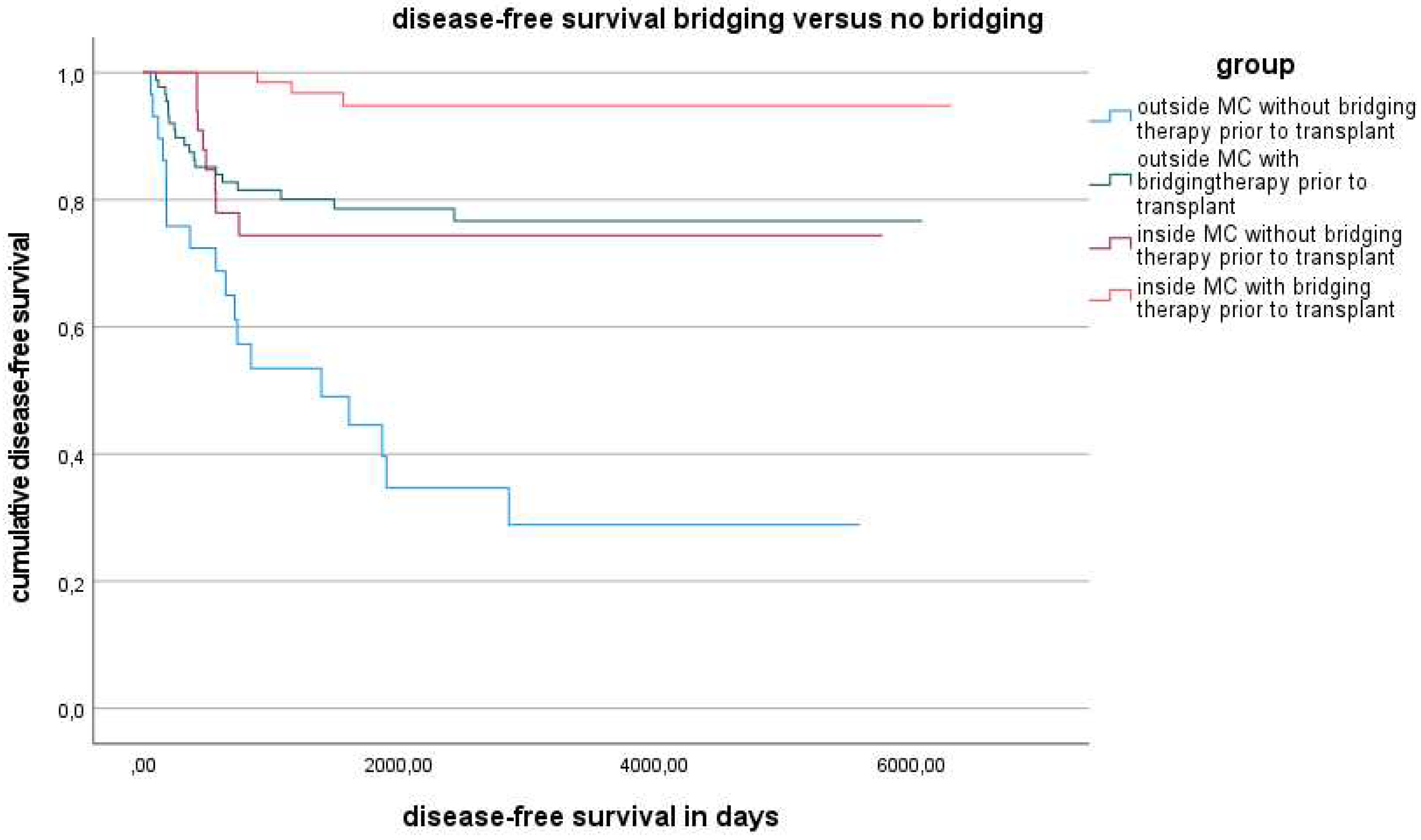
Figure 10.
DFS was also stratified according to bridging therapy.
MELD score, tumour morphology and bridging response outside the MC
The median labMELD score was 10 in the LDLT group (mean 11.8; range 6–31) and 12 in the LT group (mean 16.7; range 6–40). The MELD score was significantly lower in the LDLT group (p = 0.005).
The median tumour size (determined by pathological examination) was 52 mm (mean 60 mm, range 30–220 mm) in the LDLT group and 48 mm (mean 48.4 mm; range 17–120 mm) in the LT group (p = 0.07).
The number of tumour nodes (determined by pathological examination) was 3 (mean 4, range 1–20) in the LDLT group and 2.5 (mean 4.2; range 1–25) in the LT group (p = 0.84).
Downstaging after bridging therapy (regardless of the bridging method and frequency) was achieved for 43.8% of patients in the LDLT group and 50.7% of patients in the LT group (p = 0.52). A partial response after bridging therapy was observed in 59.4% of the LDLT group and 70.4% of the LT group (p = 0.27). Vital tumour residue after bridging was present in 18.8% of the LDLT group and 29.6% of the LT group (p = 0.25).
Results according to different classifications beyond the Milan grade
The classification results of the patients according to the different classifications (Milan, UCSF, 5-5-500, UPTS, Toronto and BCLC) are presented in Figure Our data showed that all the classifications used enabled identification of patients who had a higher risk of developing recurrence after transplantation. However, it appears that the recurrence rate did not correlate with overall survival, disease-free survival, or 1-year or 5-year survival in any subgroup. The only classifications that were separated here were BCLC and Toronto. All (newer) classifications were deemed inferior to the MC according to the criteria above (survival rate and recurrence rate).
HCC waitlist dynamics
In addition to the transplanted patients, we also observed those who were diagnosed with HCC at our transplant centre. A total of 259 patients were removed from the waiting list during the observation period; 82 patients were no longer eligible for transplantation due to disease progression, and 177 died on the waiting list due to disease progression and liver failure.
Discussion
Liver transplantation is a curative procedure for the treatment of HCC inside the MC, but it also yields good results for patients outside the MC and is superior to systemic therapy (OS 58.3 months versus 7.9-19.2 months)26. However, this treatment option is limited for patients due to organ shortages. LDLT can therefore be used for selected patients to enable those patients to undergo a transplant. Patients were selected on the basis of tumour biology markers such as AFP levels27,28,29, tumour differentiation30,31, response to bridging therapy5,9,19 and the presence of cancer-related symptoms15.
LT for patients with HCC outside the MC is still more demanding than for those with HCC inside the MC but may constitute an established procedure with acceptable survival and recurrence rates at selected transplant centres because this procedure has been applied due to improvements in bridging therapy and patient selection far from purely morphological aspects. Nevertheless, doubts remain about the equivalence of patients outside the MC; equivalence with patients inside Milan should be established according to the new extended criteria if bridging or even downstaging is possible.
Patients with hepatocellular carcinoma outside the MC have a significantly worse outcome than patients with HCC inside the MC if bridging therapy is not feasible. However, there are significant differences among the patients in the outside-Milan group, so that they should not be disadvantaged across the board in organ allocation.
LDLT is a good option for transplant patients with HCC who have no chance of receiving a liver transplant via a postmortem organ. We must clarify that the groups of patients who underwent LT or LDLT represented two different populations due to preselection as shown in the epidemiological distribution. Living donation should be considered, especially for young patients with low labMELD scores or poorly bridgeable or nonbridgeable HCC due to large or multifocal tumours.
The LDLT-patient group had a slightly worse outcome than the LT-patient group did, but this can be explained by selection bias since the factors mentioned above played an important role in patient selection in the LDLT group as shown in Figure 3 (due to larger tumours, 52 mm vs. 48 mm, p = 0.07; higher number of tumours, 3 versus 2.5, p = 0.84; poorer bridging, 66.7% versus 79.7%, p = 0.12; poorer bridging response, 53.8% versus 70.4%, p = 0.24; poorer tumour differentiation, p = 0.01).
It is still controversial whether LDLT or LT is more beneficial for patients with HCC. A well-designed, randomized, controlled trial is needed, which is not possible. The existing studies addressing this topic have shown conflicting results30,32,33,34,35,36,37.
Over the years, various additions to the MC have been made to push its boundaries. Starting with UCSF expansion to the MC, the first attempt was to adjust the tumour morphology, particularly the allowable tumour size, via a similar approach to that of Mazzaferro et al.3,4.
Among the classifications considered to be related to morphological aspects beyond Milan, the UCSF classification expands the tumour size range (<80 mm)14 compared to that of the MC. In our centre, we recommend a progressive strategy and perform transplants (via LDLT) regardless of tumour size because we consider other aspects, such as the response to bridging therapy, the dynamics of tumour markers and tumour grading, to be more relevant.
Only the extended Toronto criteria were used for other aspects, in addition to the tumour size and number of tumour nodules, which can predict a poor outcome. These criteria stand out among those included because they have no upper limit on size or number of lesions but exclude patients with cancer-related symptoms (weight loss >10 lbs or worsening performance status over 3 months)15,38. We support the basic idea of these criteria, but obligatory tumour biopsy for assessing microscopic angioinvasion needs to be discussed. There are no observations as to whether it makes sense to take the risk of carrying tumour cells during biopsy to detect the V1 situation. For this reason, we do not currently favour this approach.
The BCLC has been published as a guide for therapeutic decision-making in patients with HCC. Two new aspects, the general conditions and the liver parenchyma changes of the patients, were highlighted and influenced the outcome17. For this purpose, the classification system uses the Eastern Cooperative Oncology Group (ECOG) scale as a simple but effective diagnostic tool39. However, we consider the classification to be too regressive and would like to better demonstrate the role of living liver donation in the decision-making process.
As a further development of its own criteria, Mazzaferro’s working group has also published an adaptation of the MC for patients outside Milan4. In studies, up to seven criteria showed no differences in MC40. We can share this assessment and consider the up-to-seven rule and MC to no longer be up-to-date41.
In recent years, Asian transplant centres have also been working on further developments for prognosis assessments14,16,42,43. Among the various classifications, we have included the "5-5-500" rule here, which has gained increased attention due to its simplicity. Compared to the other classifications, this rule is relatively conservative regarding selection, and although it includes AFP as a tumour marker, it is not very revolutionary regarding morphological aspects. The use of the AFP concentration as a guide for predicting the outcome of HCC after LT has also been examined in various ways19,27,29,31,44,45,46,47,48. Our own experience shows that the preoperative AFP level alone determines oncological outcome in terms of DFS and OS. There is no clear cutoff for the AFP value for assessing the outcome of a transplant. Methodologically, the problem is that there is no clearly defined period during which the AFP level is meaningful, and the dynamics of the AFP level have thus far had no influence on the evaluation. In unbridged or inadequately bridged HCC, rapid AFP dynamics before transplantation can indicate a poor oncological outcome. We also observed that an insufficient or delayed decrease in the AFP value after liver transplantation can indicate early recurrence.
There have been further adjustments to the classification for HCC which have not been discussed further here28,43,49,50. These include, for example, the modification of the TNM criteria for HCC from Pittsburgh51 and the Hangzhou criteria49 for LT at HCC. We have not included the Pittsburgh modified TNM criteria because the disadvantage of these TNM adjustments is the limited accuracy of the pretransplant predictions of pTNM51.
The TNM classification of HCC has already been controversially discussed28,43,51,52. Our data show large discrepancies in tumour sizes and the number of tumour foci according to imaging and pathology. This restriction should ultimately be extended to all classifications with a purely morphological consideration of HCC.
In relation to bridging and recurrence, our data show that bridging should always occur if this approach is technically feasible to improve the OS and DFS of these patients. In the case of living liver donation, bridging should take place before transplantation whenever technically possible, even if the transplant is delayed.
Furthermore, our data showed that the occurrence of tumour recurrence is not necessarily associated with a poorer survival prognosis. On the one hand, this difference may be related to the improvement in relapse therapy efficacy, although not much has changed in terms of medication. In our patient population, a large proportion of patients with HCC recurrence after LT underwent surgery. This subgroup also exhibited improved overall survival compared with patients who were treated only with medication during relapse. We therefore recommend considering surgical therapy, depending on the patient’s condition, even in patients with oligometastasis.
This study has several limitations. Topping the list is the retrospective single-centre nature of the study, involving data from which unexpected bias cannot be completely excluded. The number of patients was small and not comparable to that of Asian high-volume transplant centres; therefore, the importance of the findings is limited to Western centres. A Germany-wide or Eurotransplant-wide evaluation would certainly be useful here. Another point that arises from this is that we would like to submit a plea for adjustments to the organ allocation guidelines in the Eurotransplant region to address the disadvantage of patients with HCC outside Milan compared to patients without HCC on the waiting list. A suggestion for the Eurotransplant region would be to distribute SE-MELD points also for patients with HCC outside the Milan range. However, this distribution should occur in a reduced form. Currently, patients with HCC inside the Milan start with a matchMELD score of 22 points, and 3 additional points are added every 3 months if the MC are still met. The model for patients with HCC outside the Milan could start with a reduced number of SE-MELD points and include a smaller gain to give these patients a realistic chance of a liver transplant.
Conclusion
Liver transplantation is the best treatment option for patients with HCC complicated with cirrhosis. LT for patients with HCC outside the Milan should be considered regardless of the morphological aspects that indicate G1 or G2 differentiation, without microscopic angioinvasion and with favourable AFP dynamics if preoperative bridging therapy can be performed. However, there is not yet enough data for an obligatory preoperative biopsy due to tumour spread, so no final recommendation can be made in this regard. Prompt LDLT after bridging therapy may be a solution in individual cases. Additionally, LDLT should be evaluated, especially if bridging therapy is not feasible, as survival is superior to conservative therapy in this situation.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by the ethics committee of University Hospital Jena (2023-3179-Data).
Informed Consent Statement
Informed consent was obtained from all the subjects involved in the study.
Data Availability Statement
The data can be shared upon request.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
References
- Da, B.L. et al. Pathogenesis to management of hepatocellular carcinoma. Genes Cancer 13, 72–87 (2022). [CrossRef]
- Dopazo, C. et al. Hepatocellular carcinoma. Eur. J. Surg. Oncol. 50, 107313 (2024). [CrossRef]
- Mazzaferro, V. et al. Liver Transplantation for the Treatment of Small Hepatocellular Carcinomas in Patients with Cirrhosis. N. Engl. J. Med. 334, 693–700 (1996). [CrossRef]
- Mazzaferro, V. et al. Predicting survival after liver transplantation in patients with hepatocellular carcinoma beyond the Milan criteria: a retrospective, exploratory analysis. Lancet Oncol. 10, 35–43 (2009). [CrossRef]
- Shehta, A. et al. Bridging and downstaging role of trans-arterial radio-embolization for expected small remnant volume before liver resection for hepatocellular carcinoma. Ann. Hepato-Biliary-Pancreat. Surg. 24, 421–430 (2020). [CrossRef]
- Kim, M., Hui, K.M., Shi, M., Reau, N. & Aloman, C. Differential expression of hepatic cancer stemness and hypoxia markers in residual cancer after locoregional therapies for hepatocellular carcinoma. Hepatol. Commun. 6, 3247–3259 (2022). [CrossRef]
- Ettorre, G.M. & Laurenzi, A. Liver Transplantation and Hepatobiliary Surgery, Interplay of Technical and Theoretical Aspects. 183–191 (2019). [CrossRef]
- Gao, Q., Anwar, I.J., Abraham, N. & Barbas, A.S. Liver Transplantation for Hepatocellular Carcinoma after Downstaging or Bridging Therapy with Immune Checkpoint Inhibitors. Cancers 13, 6307 (2021). [CrossRef]
- Zori, A.G. et al. Locoregional Therapy Protocols With and Without Radioembolization for Hepatocellular Carcinoma as Bridge to Liver Transplantation. Am. J. Clin. Oncol. 43, 325–333 (2020). [CrossRef]
- Makary, M.S., Bozer, J., Miller, E.D., Diaz, D.A. & Rikabi, A. Long-term Clinical Outcomes of Yttrium-90 Transarterial Radioembolization for Hepatocellular Carcinoma: A 5-Year Institutional Experience. Acad. Radiol. (2023). [CrossRef]
- Zhang, J. et al. Immune Checkpoint Inhibitors in HBV-Caused Hepatocellular Carcinoma Therapy. Vaccines 11, 614 (2023). [CrossRef]
- Wassmer, C.-H. et al. Immunotherapy and Liver Transplantation: A Narrative Review of Basic and Clinical Data. Cancers 15, 4574 (2023). [CrossRef]
- Wehrenberg-Klee, E., Goyal, L., Dugan, M., Zhu, A.X. & Ganguli, S. Y-90 Radioembolization Combined with a PD-1 Inhibitor for Advanced Hepatocellular Carcinoma. Cardiovasc. Interv. Radiol. 41, 1799–1802 (2018). [CrossRef]
- Yao, F.Y. et al. Liver Transplantation for Hepatocellular Carcinoma: Validation of the UCSF-Expanded Criteria Based on Preoperative Imaging. Am. J. Transplant. 7, 2587–2596 (2007). [CrossRef]
- Sapisochin, G. et al. The extended Toronto criteria for liver transplantation in patients with hepatocellular carcinoma: A prospective validation study. Hepatology 64, 2077–2088 (2016). [CrossRef]
- TAKISHIMA, T. et al. The Japanese 5-5-500 Rule Predicts Prognosis of Hepatocellular Carcinoma After Hepatic Resection. Anticancer Res. 43, 1623–1629 (2023). [CrossRef]
- Reig, M. et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J. Hepatol. 76, 681–693 (2022). [CrossRef]
- Lubel, J.S., Roberts, S.K., Strasser, S.I. & Shackel, N. Australian recommendations for the management of hepatocellular carcinoma. Méd. J. Aust. 215, 334-334.e1 (2021). [CrossRef]
- Seehofer, D. et al. Patient Selection for Downstaging of Hepatocellular Carcinoma Prior to Liver Transplantation—Adjusting the Odds? Transpl. Int. 35, 10333 (2022). [CrossRef]
- DSO. Jahresbericht der deutschen Stiftung für Organspende https://dso.de/BerichteTransplantationszentren/Grafiken%20D%202021%20Leber.pdf (2021).
- Goldaracena, N. et al. Live donor liver transplantation for patients with hepatocellular carcinoma offers increased survival vs. deceased donation. J. Hepatol. 70, 666–673 (2019). [CrossRef]
- Nadalin, S. et al. Living donor liver transplantation in Europe. Hepatobiliary Surg Nutrition 5, 159–75 (2016). [CrossRef]
- Malinchoc, M. et al. A model to predict poor survival in patients undergoing transjugular intrahepatic portosystemic shunts. Hepatology 31, 864–871 (2000). [CrossRef]
- Lencioni, R. & Llovet, J. Modified RECIST (mRECIST) Assessment for Hepatocellular Carcinoma. Semin Liver Dis 30, 052–060 (2010). [CrossRef]
- Eisenhauer, E.A. et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 45, 228–247 (2009). [CrossRef]
- Vogel, A., Meyer, T., Sapisochin, G., Salem, R. & Saborowski, A. Hepatocellular carcinoma. Lancet 400, 1345–1362 (2022). [CrossRef]
- Hameed, B., Mehta, N., Sapisochin, G., Roberts, J.P. & Yao, F.Y. Alpha-fetoprotein level > 1000 ng/mL as an exclusion criterion for liver transplantation in patients with hepatocellular carcinoma meeting the Milan criteria. Liver Transplant. 20, 945–951 (2014). [CrossRef]
- Feng, L.-H. et al. A Practical Risk Classification of Early Recurrence in Hepatocellular Carcinoma Patients with Microvascular invasion after Hepatectomy: A Decision Tree Analysis. Ann. Surg. Oncol. 30, 363–372 (2023). [CrossRef]
- Toso, C. et al. Total tumor volume and alpha-fetoprotein for selection of transplant candidates with hepatocellular carcinoma: A prospective validation. Hepatology 62, 158–165 (2015). [CrossRef]
- Bhangui, P. et al. Intention-to-treat analysis of liver transplantation for hepatocellular carcinoma: Living versus deceased donor transplantation. Hepatology 53, 1570–1579 (2011). [CrossRef]
- Yao, F.Y. et al. Liver transplantation for hepatocellular carcinoma: Expansion of the tumor size limits does not adversely impact survival. Hepatology 33, 1394–1403 (2001). [CrossRef]
- Sotiropoulos, G.C. et al. Liver Transplantation for Hepatocellular Carcinoma: University Hospital Essen Experience and Metaanalysis of Prognostic Factors. J. Am. Coll. Surg. 205, 661–675 (2007). [CrossRef]
- Vakili, K. et al. Living donor liver transplantation for hepatocellular carcinoma: Increased recurrence but improved survival. Liver Transplant. 15, 1861–1866 (2009). [CrossRef]
- Sandro, S.D. et al. Living Donor Liver Transplantation for Hepatocellular Carcinoma: Long-Term Results Compared With Deceased Donor Liver Transplantation. Transplant. Proc. 41, 1283–1285 (2009). [CrossRef]
- Sandhu, L. et al. Living donor liver transplantation versus deceased donor liver transplantation for hepatocellular carcinoma: Comparable survival and recurrence. Liver Transplant. 18, 315–322 (2012). [CrossRef]
- Park, M.-S. et al. Living-Donor Liver Transplantation Associated With Higher Incidence of Hepatocellular Carcinoma Recurrence Than Deceased-Donor Liver Transplantation. Transplant. J. 97, 71–77 (2014). [CrossRef]
- Hwang, S., Lee, S., Joh, J., Suh, K. & Kim, D. Liver transplantation for adult patients with hepatocellular carcinoma in Korea: Comparison between cadaveric donor and living donor liver transplantations. Liver Transplant. 11, 1265–1272 (2005). [CrossRef]
- Sandri, G.B.L., Rayar, M., Qi, X. & Lucatelli, P. Liver transplant for patients outside Milan criteria. Transl. Gastroenterol. Hepatol. 3, 81–81 (2018). [CrossRef]
- Ramos, F. et al. ECOG Performance Status Shows a Stronger Association with Treatment Tolerability Than Some Multidimensional Scales in Elderly Patients Diagnosed with Hematological Malignancies. Blood 136, 15–16 (2020). [CrossRef]
- Martino, M.D. et al. Comparison of Up-to-seven criteria with Milan Criteria for liver transplantation in patients with HCC. Trends Transplant. 14, (2021). [CrossRef]
- Rauchfuß, F. et al. Searching the ideal hepatocellular carcinoma patient for liver transplantation: are the Toronto criteria a step in the right direction? Hepatobiliary Surg. Nutr. 6, 342–343 (2017). [CrossRef]
- Zheng, S.-S. et al. Liver transplantation for hepatocellular carcinoma: Hangzhou experiences. Transplantation 85, 1726–32 (2008). [CrossRef]
- Yan, P. & Yan, L.-N. Staging of hepatocellular carcinoma. Hepatobiliary Pancreat. Dis. Int.: HBPD INT 2, 491–5 (2003).
- Yap, A.Q. et al. Clinicopathological factors impact the survival outcome following the resection of combined hepatocellular carcinoma and cholangiocarcinoma. Surg Oncol 22, 55–60 (2013). [CrossRef]
- Bhatti, A.B.H. et al. Living donor liver transplantation for advanced hepatocellular carcinoma including macrovascular invasion. J. Cancer Res. Clin. Oncol. 148, 245–253 (2022). [CrossRef]
- Lin, C.-C. & Chen, C.-L. Living donor liver transplantation for hepatocellular carcinoma achieves better outcomes. Hepatobiliary Surg Nutrition 5, 415–421 (2016). [CrossRef]
- Bhatti, A.B.H., Waheed, A. & Khan, N.A. Living Donor Liver Transplantation for Hepatocellular Carcinoma: Appraisal of the United Network for Organ Sharing Modified TNM Staging. Front. Surg. 7, 622170 (2021). [CrossRef]
- Wong, T.C.L. et al. Long-Term Survival Outcome Between Living Donor and Deceased Donor Liver Transplant for Hepatocellular Carcinoma: Intention-to-Treat and Propensity Score Matching Analyses. Ann. Surg. Oncol. 26, 1454–1462 (2019). [CrossRef]
- Lei, J.Y., Wang, W.T. & Yan, L.N. Hangzhou criteria for liver transplantation in hepatocellular carcinoma: a single-center experience. Eur. J. Gastroenterol. Hepatol. 26, 200–204 (2014). [CrossRef]
- Ivanics, T. et al. Living Donor Liver Transplantation (LDLT) for Hepatocellular Carcinoma (HCC) within and Outside Traditional Selection Criteria: A Multicentric North American Experience. Ann. Surg. (2023). [CrossRef]
- Chen, J., Xu, X., Ling, Q., Wu, J. & Zheng, S. Role of Pittsburgh modified TNM criteria in prognosis prediction of liver transplantation for hepatocellular carcinoma. Chin. Méd. J. 120, 2200–3 (2007). [CrossRef]
- PONS, F., VARELA, M. & LLOVET, J.M. Staging systems in hepatocellular carcinoma. HPB 7, 35–41 (2005). [CrossRef]
Figure 1.
Selection progress.
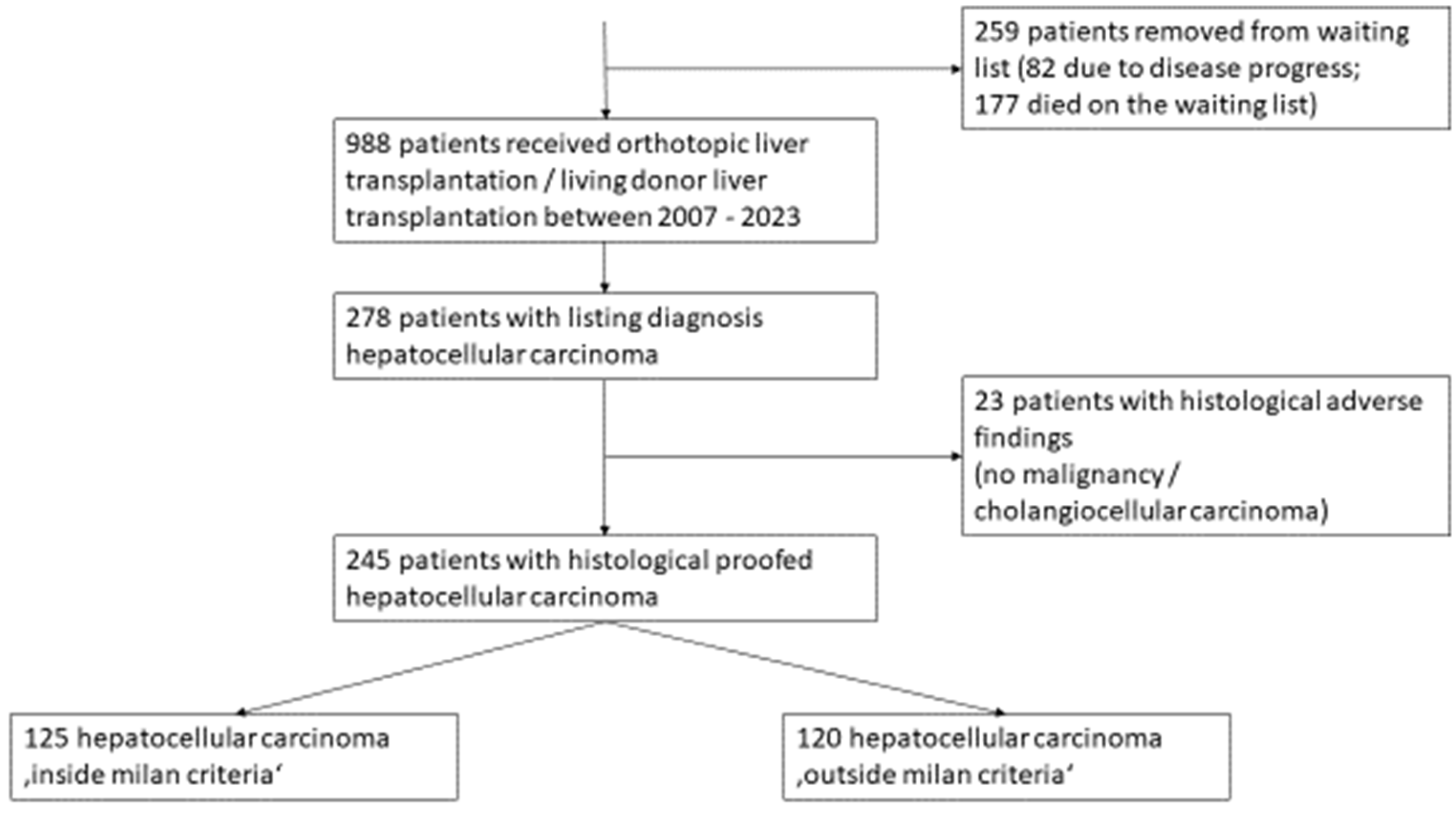
Figure 2.
Characteristics of patients with HCC inside the Milan stratified by transplantation.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



