Submitted:
16 January 2024
Posted:
17 January 2024
You are already at the latest version
Abstract
Abstract: (1) Background: No consensus has been reached on indicators and protocols for monitoring drug concentrations in organ transplant recipients for the immunosuppressant mycophenolic acid (MPA) in clinical therapy.In this study, we propose to establish a Ultra Performance Liquid Chromatography–Tandem Mass Spectrometry (UPLC-MS/MS) for quantitative determination of MPA and its metabolites ( mycophenolic acid carboxybutoxyether, MPAG and mycophenolic acid carboxyglucuronide, AcMPAG) concentrations in peripheral blood mononuclear cells (PBMCs) and to assess the clinical application of PBMCs concentration detection of MPA and its metabolites in infection prediction in Chinese kidney transplant recipients(KTRs); (2) Methods: PBMCs were isolated with Ficoll-Paque solution, and cells were counted. Acetonitrile precipitated proteins to extract the target compounds.Waters ACQUITY UPLC BEH C18 column of 1.7μm (2.1 mm*50 mm) and an ACQUITY-Xevo TQ-S UPLC-MS/MS system were used for the detection with mobile phases: water and methanol (containing 2 mmol/L NH4Ac + 0.1% formic acid); flow rate: 0.3 mL/min. After gradient elution, the samples were positively ionized by an electrospray positive ion source (ESI) and then quantitatively analyzed by a triple quadrupole tandem mass spectrometer in multiple reaction monitoring (MRM) mode. The performance of the established method was evaluated through a series of validation experiments according to the requirements of the relevant guidelines. We enrolled 7 KTRs with stable conditions and 8 KTRs with infection from August to November 2022, who were treated at the West China Hospital of Sichuan University.Their peripheral blood samples were collected and detected MPA, MPAG, and AcMPAG concentrations in PBMCs using the methods mentioned above and evaluated for their clinical application in the prediction and monitoring of infections in KTRs; (3) Results: After validation of the methodology, the UPLC-MS/MS method established in this study for the determination of MPA, MPAG, and AcMPAG concentrations in PBMCs showed good linearity in the quantitative ranges of 0.0625-50 ng/ml, 0.5-50 ng/ml and 0.1-20 ng/ml, and the selectivity, specificity, matrix effect, carry-over contamination, reproducibility, precision and accuracy all satisfied the requirements.AcMPAG in PBMCs was poorly stabilized and showed significant degradation after -80°C storage for 24 h or 3 cycles of freeze-thaw.There was a large variability in MPA and MPAG concentrations in PBMCs of KTRs and it correlated poorly with plasma MPA concentrations (rs=0.206,p=0.117).Subgroup analysis showed that the correlation between MPA in plasma and PBMCs was still poor in the infected group(rs=0.201,p=0.116), but significant correlation in the stable group (rs=0.643,p=0.001). A significantly higher level of MPA in PBMCs was observed in the infected group than those in the stable group at 2h and 4h after drug dosing (p<0.05).AcMPAG concentrations in PBMCs of KTRs were extremely low and virtually undetectable.ROC curve analysis (area under the curve, AUC) was performed for infection after renal transplantation with indicators of significant difference showed that the area AUC for PBMCs-MPA-C4 was 0.928 ,for PBMCs-MPA-C2 was 0.875,and for Plasma-MPA-C4 was 0.803; (4) Conclusions: In this study, a method based on UPLC-MS/MS was developed and validated for the simultaneous determination of MPA, MPAG, and AcMPAG concentrations in PBMCs.With easy operability and good stability, this method provides a reliable analytical method for the clinical implementation of the detection of MPA, MPAG, and AcMPAG concentrations in PBMCs.The concentrations of MPA and MPAG in PBMCs from KTRs were highly variable and were closely associated with the development of infections after renal transplantation.Monitoring MPA and MPAG in PBMCs may be useful indicators for mycophenolic acid therapeutic drug concentration monitoring (TDM) in KTRs.
Keywords:
UPLC-MS/MS
; MPA
; MPAG
; AcMPAG
; PBMC
; Infection
1. Introduction
MPA is widely used in the treatment of solid organ transplant patients as an immunosuppressant, usually in combination with tacrolimus (TAC) or cyclosporine (CsA) and corticosteroids to prevent graft rejection.MPA is metabolized by several uridine diphosphate glucoronosyltransferases into its inactive metabolite mycophenolic acid carboxybutoxyether(MPAG) and the pharmacologically active netabolite mycophenolic acid carboxyglucuronide (AcMPAG)[1].Precursors of MPA include mycophenolate mofetil (MMF) and mycophenolate sodium (MPS). MPA-associated adverse effects such as infection, leukopenia, anemia, and gastrointestinal problems occur frequently. The pre-dose MPA plasma/serum concentration (MPA trough concentration, MPA-C0) is currently the most commonly used cinical MPA therapeutic drug monitoring(TDM) indicator and the area under the complete MPA concentration-time curve (MPA-AUC0-12) is the gold standard for evaluating MPA exposure levels in vivo.However, the correlation between these two commonly used monitoring indicators and drug-related adverse reactions was poor in most studies [5].
It is reorted that some of MPA-related side effects were associated with its metabolites. MPAG has no inhibitory effect on IMPDH activity, but several studies had reported a correlation between MPAG exposure and adverse effects[6].MPAG competes with MPA for the binding of plasma proteins, resulting in an increase of free MPA (fMPA) which is pharmacologically active [7].Some studies have found that the pharmacokinetic parameters of MPAG (AUC0-4h,C0,Cmax) correlate with hemoglobin and hematocrit in KTRs, and MPAG levels may be a predictor of MPA-associated anemia[8].Several studies have found significantly higher plasma concentrations of MPAG among transplant recipients with deteriorating renal function [9-13]. AcMPAG exhibits certain pharmacodynamic activities.AcMPAG has been shown in vitro to inhibit IMPDH and monocyte proliferation, which would increase the risk of opportunistic infections in transplant recipients [14,15].It has been found that higher AcMPAG AUC0-24 was found in hematopoietic stem cell transplant(HSCT) recipients with acute graft wart disease in the gastrointestinal tract [16]. AcMPAG induces mRNA and protein expression of pro-inflammatory cytokines TNF-α and IL-6, which may lead to leukocyte activation and/or direct damage to the gastrointestinal mucosa in some HSCT patients causing inflammatory gastrointestinal symptoms[17].It was also found in a cohort study that AcMPAG levels were positively correlated with bacterial infections in liver transplant recipients[18]. These reports indicates monitoring of MPAG and AcMPAG concentration may be beneficial to the rational clinical usage of MPA.
Lymphocyte is the main target cell of immunosuppressive agents[19].Therefore, the intra-lymphocyte drug concentration is believed to have a more direct relationship with the immunosuppressive efficacy. The detection of drug concentration in peripheral blood mononuclear cells (PBMCs) is a new technique for drug concentration analysis that has been explored by a few foreign scholars in recent years.Existing studies have mainly focused on PBMC-Tacrolimus (TAC) concentration and PBMC-cyclosporine (CsA) concentration. In recent years, PBMC-MPA concentration detection has gradually been reported.
The detection of intralcellular drug concentration is much more difficult than plasma or whole blood drug concentration and could not be achieved using routine clinical analitical method (e.g immunological technology). Only a few laboratories have established validated detection method based on ultra-performance liquid chromatography-tandem mass spectrometry (UPLC-MS/MS) technology for the concentration detection of PBMC-TAC, PBMC-CsA, and PBMC-MPA[20,21].To our knownledge, there have been no report available on the simultaneous quantitative detection of MPA and its metabolites in PMBCs.
In this study, we developed and analytically validated a UPLC-MS/MS based method for the determination of MPA and its metabolites concentrations in PBMCs (PBMC-MPA, PBMC-MPAG, MPA-AcMPAG).Blood samples from Chinese KTRs were analysed using this method and the clinical application value of those indicators in the prediction of infection after transplantation were assessed and compared with routine plasma MPA concentration.
2. Materials and Methods
2.1. Sample collection
Blank PBMCs were extracted from 30 heparin-anticoagulated whole blood from healthy volunteers.PBMC’s isolation was obtained by adapting the Leucosep® tubes manufacturer’s protocol.Briefly, the tubes containing the blood were centrifuged (2000 rpm, 5 min), followed by aspirating the middle white-membrane layers, combining all the layers, with equal amounts of PBS, and transferring them to 15 ml separator tubes( CORNING CentriStar, TM).Carefully pour the mixture into several 15 mL test tubes containing 4 mL of FicollPaque Plus solution without mixing.After centrifugation (500g, 30 minutes), the PBMC layers from the tubes were collected.The cells in each tube were washed with 10 mL of PBS (300 g, 10 min), centrifuged and the supernatant discarded, and then lysed with 10 ml of erythrocyte lysate for 20 min, then centrifuged and discarded after washing again with PBS and discarding the supernatant, finally resuspended with an appropriate amount of PBS. Thereafter, 50 uL of the suspension was used for cell counting on a Sysmex® XE- 2100 instrument (Sysmex Corporation, Kobe, Japan).And the remaining fractions were pooled, divided into several aliquots, and packed into EP tubes, each containing approximately 10*106 cells.After centrifugation (300 g, 10 min), these aliquots(50ul each)were stored at −80 °C until analysis for the use of the standards and QC samples blank matrix.
2.2. Reagents and Materials
HPLC-grade methanol, acetonitrile, and formic acid were obtained from Thermo Fisher (St. Louis, MO, USA).Ammonium acetate was obtained from Sigma-Aldrich (St. Louis, MO, USA).The standards of MPA and metabolites were Mycophenolic Acid (MPA) Mycophenolic acid carboxybutoxyether(MPAG)and acyl glucuronide of mycophenolic acid(AcMPAG)were purchased from TRC (Toronto, ON, Canada). We used a stable isotope-labeled internal standard in which MPA-d3 was purchased from TRC (Toronto, ON, Canada). Deionized water was prepared by a Milli-Q integral ultrapure water machine (Merck Millipore, Germany).
2.3. Equipments and Conditions
We used a triple quadrupole LC-MS/MS consisting of an ACQUITY UPLC system in combination with a Xevo TQ-S triple quadrupole mass spectrometer, from Waters (Milford, CT, USA). Method optimization was performed using an Acquity UPLC BEH C18 1.70 um 2.10 mm x 50 mm analytical column. The autosampler temperature was set at 8 ℃ and the column oven temperature was set to 60 ℃. Mobile phases A and B consisted of 2 mM ammonium acetate and 0.10% formic acid, the former in deionized water and the latter in methanol at a flow rate of 0.30 mL/min. The gradient elution program was set to 20% B for 1 min, then the percentage of B was increased to 90% B in 3.8 min, then adjusted to 20% B in 4.3 min, and held 20% B for 4.30 min until 5.0 min.The total injector run time was 5 min and the injection volume for a single analysis was 5 ul.
The mass spectrometer generates positive ions in electrospray ionization (ESI) mode and the analysis was performed in multiple reaction monitoring (MRM) mode. The m/z detected for MPA, MPAG, AcMPAG, and MPA-d3 were 321.27/207.15, 514.27/321.2, 514.26/321.2, and 324.26/210.15, respectively,which were shown in Table 1.
2.4. Calibration Standards and Quality Control Samples
MPA standard was weighed to prepare 1.00 mg/mL stock solutions with methanol. MPAG and AcMPAG standards were weighed to prepare 0.10 mg/mL stock solutions with methanol. The isotope internal standard MPA-d3 wasweighed to make a 0.04 mg/mL stock solution with methanol.The stock solutions were dispensed into 1.50 mL centrifuge tubes and stored at -_80℃. Working solutions of MPA, MPAG, and AcMPAG standards were prepared in methanol/water (50/50).The internal standard was prepared in acetonitrile.
The concentration range of the calibrators were 0.0625, 0.125, 0.25, 0.5, 1.00, 2.00, 5.00, 10.00, 25.00, 50.00ng/ml for MPA;0.5, 1.00, 2.00, 5.00, 10.00, 25.00, 50.00ng/ml for MPAG;and 0.10, 0.20, 0.40, 0.80, 2.00, 4.00, 10.00, 20.00ng/ml for AcMPAG. For MPA, 0.050 ng/mL was set as the lower limit of quantitation (LLOQ),0.150 ng/mL was set as the low concentration quality control (LQC), 10.00 ng/mL was set as the medium concentration quality control (MQC), and 40.00 ng/mL was set as the high concentration quality control (HQC). For MPAG and AcMPAG, 0.500 ng/mL and 0.100ng/ml wereset as LLOQ,1.500 ng/mL and 0.3 ng/mL as LQC, 10.00 ng/mL and 4.00 ng/mL as MQC, and 40.00 ng/mL and 16.00 ng/mL as HQC.Healthy volunteers mixing PBMCs were used as a blank control.Calibration standards and quality control samples were prepared in healthy volunteers mixing PBMCs. Fresh calibration standards and QC samples were prepared for each analysis and discarded after the analysis was complete.
2.5. Sample pre-processing methods
Acetonitrile precipitation was used to remove the proteins from PBMCs to extract the substances to be tested.Accurately aspirate 50µL of prepared standard curve or room temperature re-solubilized patient PBMCs into a 1.5mL EP tube. Then,100uL of acetonitrile and IS (1ng/mL d3-MPA) were added. After vigorous vortexing (10 min) and centrifugation (5 min, 12,000g, 4°C), 50ul of supernatant and 50ul mobile phase A were taken, and the mixture was transferred to the injection vial for LC-MS/MS analysis.
2.6. Bioanalytical Validation
Development and validation were carried out following the Food and Drug Admin- istration and European Medicines Agency guidelines for the validation of bioanalytical methods [22,23]. Accuracy was expressed by deviation %,calculated from [(measured concentration _ theoretical concentration) x 100]/theoretical concentration, precision was the coefficient of variation, the formula was CV (%) = (standard deviation/mean) x 100. N represented the number of sample preparations.
2.6.1. Standard Curve and Lower Limit of Quantitation
Prepared blank samples, zero concentration samples, and the concentration point samples.The standards used to build the standard curve.A sequence of injections was taken from the low-level standard to the high-level standard.The standard curve fitted linearly Y =aX + b with 1/X as a weighting factor, where X was the amount of MPA, MPAG, AcMPAG, and Y the ratio of the chromatographic peak areas (MPA/ISTD, MPAG/ISTD, AcMPAG/ISTD).If both the correlation coefficient (r2) was >0.99 and SD from the nominal concentrations was< 15%, except for the lower limit of quantification (LLOQ) (<20%), the curves were considered linear.The limit of detection (LOD) was calculated as the smallest detectable peak above baseline noise (signal/noise>3:1).Three samples with concentrations close to LOQ were selected, and each sample was repeated six times for three consecutive batches when the accuracy was 80%~120%, the precision (coefficient of variation CV) ≤ 20%, it was considered acceptable as the lower limit of quantification (LLOQ).
2.6.2. Selectivity and Carryover Effect
Six blank PBMCs from healthy volunteers were selected for selectivity evaluation. A blank sample was injected after the upper limit of the quantification sample to assess carryover effect and the experiment of carrying contamination rate was carried out by cross-injecting low and high concentration samples.
2.6.3. Matrix Effect and Extraction Recovery
Blank matrix samples were prepared from mixed PBMCs from healthy volunteers, 4 different level concentration analytes(LLOQ,LQC, MQC, and HQC)and internal standards were added after extraction, and pure solutions containing the same concentrations of analytes and internal standards were prepared to study the matrix effect. At the same time, corresponding LLOQ,LQC, MQC, and HQC were prepared to calculate extraction recovery.
2.6.4. Accuracy and precision
Four concentration levels, including LLOQ,LQC,MQC, and HQC, were prepared, five samples at one concentration level, three batches of analysis were completed within three days, and intra- and interassay analysis was performed to assess accuracy and precision.
2.6.5. Stability
The stability of MPA, MPAG, and AcMPAG in PBMCs was investigated under different conditions of time and temperature.Short-term room temperature stability was assessed by storing the QCs at room temperature for 3 hours and 8 hours before sample processing;Short-term refrigerated storage stability was assessed by storing the QCs in the 4°C refrigerator for 24 hours before sample processing;freeze/thaw stability was determined by freezing samples at -80℃ and thawing at room temperature in 3 cycles; post-extracted sample stability was evaluated by storing QCs in the autosampler for 24 hours after sample treatment;long-term stability was assessed by storing QCs at-80C for 24h, 48h, 72h, 7d, 14d.
Through the above experiments, the stability of MPA, MPAG, and AcMPAG under different storage conditions can be determined so that appropriate storage conditions can be selected to ensure the accuracy and reliability of the data in routine analysis.
2.7. Clinical Validation
2.7.1. Patients
The study cohort included patients who received kidney transplantation at the Kidney Transplant Center of West China Hospital.The KTRs who occurred infections with long-term primidone administration were considered as the infected group (n=8). The KTRs with regular long-term follow-ups who had healthy hepatic and renal function and hematology were treated as the stable group (n=7).The exclusion criteria included: renal allograft insuffificiency (eGFR <60 mL/min), hepatic insuffificiency, unstable serum creatinine level or allograft rejection past 1 year; any dose adjustment of immunosuppressants during the past one month; history of malignancy; gastrointestinal disease, and patients with poor compliance.All patients received a triple immunosuppressive regimen including MPA, CNIs, and glucocorticosteroids.4mL blood was collected in heparin anticoagulation tubes from MPA at 0h before, 0.5h after, 2h after, and 4h after dosing. The PBMCs were extracted within 8 hours after the detection of the plasma concentration.
2.7.2. Sample and data collection
Sample collection: PBMCs were collected from infected KTRs and stable KTRs at 0h before, 0.5h after, 2h after, and 4h after the dose of Snapdragon for evaluation of clinical applicability.PBMCs from patients were extracted in the same way as those from healthy volunteers.Other relevant clinical data collection:(Ⅰ)Age, sex, graft duration, dosage of immunosuppressants, history of malignancy, and gastrointestinal disease in the two groups;(Ⅱ)Drug levels in MPA plasma were assayed using Siemens V-TWIN autoanalyzer and accompanying reagents. Pre-dose (MPA-C0), 0.5h post-dose (MPA-C0.5), 2h post-dose (MPA-C2), 4h post-dose (MPA-C4), and simplified area under the curve (MPA-AUC0-4) were collected in plasma of both groups.(Ⅲ)Collected information related to pathogenic microbial results, molecular diagnostic results, imaging data, and clinical diagnosis at the time of hospital admission in the infected group. (Ⅳ)Collected laboratory test results of blood routine, urine routine, liver function, and kidney function of the two groups.
2.8. Statistical Analyses
Performance validation data were analyzed and calculated using SPSS Statistics software (2015, IBM, USA). GraphPad Prism 9.0 was used to analyze the clinical validation data, compare and correlate the two data sets, and finally graphing. The methodology established in this study has detailed experimental procedures, that is., visualizations were created through BioRender.com for better and intuitive understanding. We have obtained publication and license for the data from this website.The specific experimental Flow chart was shown in Figure 1.
3. Results
3.1. Bioanalytical Validation
3.1.1. Standard Curve and Lower Limit of Quantitation
The calibration curves for MPA, MPAG, and AcMPAG were linearly correlated with R2 all exceeding 0.99.The maximum deviation of intra- and interassay LLOQ in MPA was 8.40%, 10.56% forMPAG, and 11.66% for AcMPAG, and CVs were shown to be 3.90%, 6.39%, and 7.37%, all less than 20%.Figure 1 shows the calibration curves and LLOQ chromatograms for all analytes.
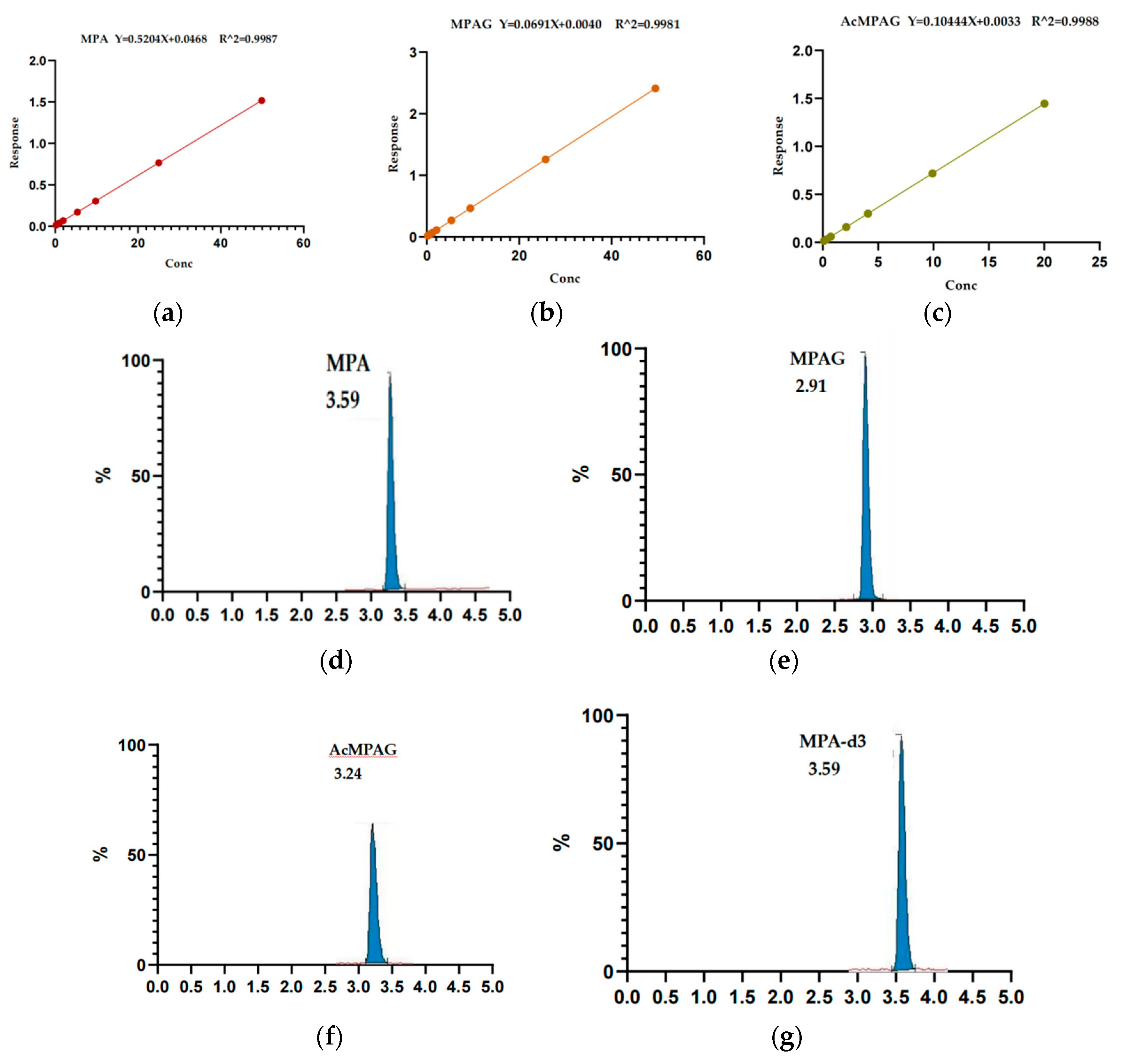
Figure 2.
Standard curves and LLOQion chromatogram peaks for the three analytes. (a) The standard curve range of MPA is 0.0625~50.00 ng/mL; (b) The standard curve range of MPAG is 0.500~50.00 ng/mL; (c) The standard curve range of AcMPAG is 0.100~20 ng/mL; (e) The internal standard channel and analyte channel of MPA LLOQ (0.050 ng/mL) of channel; (f) The internal standard channel and analyte channel of MPAG LLOQ (0.50 ng/mL); (g) The internal standard channel and analyte channel of AcMPAG LLOQ (0.1 ng/ml).
Figure 2.
Standard curves and LLOQion chromatogram peaks for the three analytes. (a) The standard curve range of MPA is 0.0625~50.00 ng/mL; (b) The standard curve range of MPAG is 0.500~50.00 ng/mL; (c) The standard curve range of AcMPAG is 0.100~20 ng/mL; (e) The internal standard channel and analyte channel of MPA LLOQ (0.050 ng/mL) of channel; (f) The internal standard channel and analyte channel of MPAG LLOQ (0.50 ng/mL); (g) The internal standard channel and analyte channel of AcMPAG LLOQ (0.1 ng/ml).
3.1.2. Selective and Carryover Effect
Interference values < 20% LLOQ and <5% IS were observed for the channels of analytes and internal standards in blank matrix from different sources. After injection of LLOQ, no obvious residue was found in the blank sample, and the carrying contamination rates of MPA, MPAG, and AcMPAG were 1.37%, 1.50%,and 2.11%, respectively.
3.1.3. Matrix effect and recoveries
The matrix effects of MPA, MPAG, and AcMPAG in PBMCs were shown in Table 2.All three target analytes were within 100±15% of the matrix effect for each concentration, suggesting that the matrix effect would not limit the accurate quantification for MPA, MPAG, and AcMPAG.The spiked recovery assays for MPA, MPAG, and AcMPAG showed an average recovery of 90.67%-112.89%, 88.00%-112.97%, and 83.33%-103.4%, respectively, with the relative recoveries all in the 80-120% range.
3.1.4. Accuracy and Precision
All obtained assay results met the acceptance criteria (Table 3). The overall deviation range for the three-day accuracy of MPA was shown to be _0.92~10.25%, _1.27~_7.56% for MPAG, and _1.88~9.39% for AcMPAG. The intra- and interassay coefficients of variation were both <15%.
For MPA, the concentrations of LLOQ, LQC, MQC and H QCwere 0.10, 0.15, 10.00 and 40.00 ng/mL respectively. For MPAG, the concentrations of LLOQ, LQC, MQC and HQC were 0.50, 1.50, 10.00 and 40.00 ng/mL respectively.For AcMPAG, the concentrations of LLOQ, LQC, MQC and HQC were 0.10, 0.30, 4.00 and 16.00 ng/mL respectively.
3.1.5. Stability
The CV% of the QCs for MPA and its two metabolites was <15% when placed at room temperature for 8 h and stored at 4°C for 24 h. After 3 freeze-thaw cycles, the CV% deviation of the MPA and MPAG was <15%, but the deviation of the MQC of AcMPAG was >15%.The CV% of MPA, MPAG, and AcMPAG assay results were <15% when retained in the autosampler for 24 hours (Table 4). After 24h, 48h, 72h, 1w, and 2w of frozen storage at -80°C, the QCs of AcMPAG underwent significant degradation, whereas MPA and MPAG were relatively stable (Table 5).
3.2. Clinical application assessment
KTRs in the infected group: the mean MPA levels in PBMCs pre-dose (0h), 0.5h, 2h, and 4h post-dose were 0.781 (0.200-1.358) ng/ml, 1.085 (0.230-2.257) ng/ml,1.860 (0.762-2.981) ng/ml, and 1.631 ( 0.545-4.888) ng/ml (Figure 3a).The mean MPAG levels in PBMCs were 8.616 (1.692-28.146) ng/ml, 9.994 (1.604-28.052) ng/ml,15.346 (1.543-45.347) ng/ml, and 11.16 (2.644-30.297) ng/ml, respectively, at various time points (Figure 3b). And the majority of recipients had the highest levels of MPA and MPAG in their PBMCs at 2 h post-dose.
KTRSs in the stable group: the mean MPA levels in PBMCs were 0.415 (0.137-0.704) ng/ml, 0.962 (0.266-1.509) ng/ml,0.620 (0.189-1.176) ng/ml and 0.369 (0.135-0.659) ng/ml, respectively, at various time points(Figure 3c).The mean MPAG levels in PBMCs were 3.526 (0.318-8.175) ng/ml, 4.232 (0.821-6.498) ng/ml,5.432 (0.501-10.039) ng/ml, and 4.574 (1.061-9.808) ng/ml(Figure 3d).
MPA and MPAG concentrations in PBMCs were different between the infected and stabilized groups.KTRs in the infected group had higher concentrations of MPA and MPAG in PBMCs than the stable group at pre-dose (0h), 0.5h, 2h, and 4h post-dose, with significantly higher MPA in PBMCs for 2h and 4h than in the stable group (p < 0.05) (Figure 4a,b).The plasma concentration of MPA in the infected group was close to the stable group at pre-dose (0h) and 2h post-dose, significantly lower than the stable group at 0.5h post-dose (p<0.05), and significantly higher than the stable group at 4h post-dose (Figure 4c).
PBMCs-MPA-C2, PBMCs-MPA-C4, and Plasma-MPA-C4 of KTRs in the infected group were significantly higher than those in the stable group.ROC curve analysis (area under the curve, AUC) was performed for infection after renal transplantation with indicators of significant difference showed that the area AUC for PBMCs-MPA-C4 was 0.928 (95% CI: 0.798-1.000, p=0.005); for PBMCs-MPA-C2 was 0.875 (95% CI: 0.696-1.000, p=0.015);and for Plasma-MPA-C4 was 0.803 (95% CI: 0.556-1.000, p=0.049) (Figure 5).
In the correlation analysis between MPA in plasma and MPA in PBMCs, we found that although both MPA concentrations in plasma and PBMCs showed similar time-concentration variability regularities in all groups, MPA in plasma correlated poorly with MPA in PBMCs at all time points in all patients (rs=0.281,p = 0.119) (Figure 6a, 6b, 6c).Subgroup analysis showed that the correlation between MPA in plasma and PBMCs was still poor in the infected group(rs=0.201,p=0.116), but significant correlation in the stable group (rs=0.643,p=0.001) (Figure 6d, 6e).
4. Discussion
Numerous methods and related studies have been reported on the detection of MPAG and AcMPAG levels in biological matrices such as plasma, saliva, and urine [24].In recent years, the concentration of MPA in PBMCs has been gradually focused on, whereas no studies related to the detection of MPAG and AcMPAG concentrations in PBMCs have been reported.After the literature search review, to the best of our knowledge, the present study is the first method established based on UPLC-MSMS technology for the simultaneous quantitative determination in PBMCs for MPA and its two main metabolites, MPAG and AcMPAG concentrations.
In this study, a method for the simultaneous determination of MPA and its metabolites MPAG and AcMPAG concentrations in PBMCs using UPLC-MS/MS was developed and systematically and comprehensively validated for method performance with reference to guideline requirements.Our established quantitative analytical method showed good linearity in the ranges of MPA 0.0625-50 ng/ml, MPAG 0.5-50 ng/ml, and AcMPAG 0.1-20 ng/ml, and the selectivity, specificity, matrix effect, carry-over contamination, reproducibility, precision, and accuracy all met the requirements.Using acetonitrile precipitation of proteins effectively lysed the cells and released the drugs and metabolites to be tested, which simplified the sample pre-treatment process and shortened the pre-treatment time, and the chromatographic run time (5 min) was shorter, thus improving the clinical detection capability of the method, and making it suitable for the detection of the concentrations of MPA, MPAG, and AcMPAG in the samples of PBMCs from clinical patients.Few laboratories have reported LC-MSMS assays for PBMC-MPA concentrations.Bing Chen et al. reported a linear range of 0.098-39.2 ng/ml for the quantitative detection of PBMC-MPA by their method[25]. The linear range of our method was 0.0625-50 ng/ml, with lower LLOQ, higher sensitivity, and a wider concentration range.At the same time, this method could accomplish the simultaneous detection of MPA and its metabolites MPAG and AcMPAG in PBMCs through one pre-processing and one sample run, which provided effective methodological support for a more efficient and comprehensive assessment of the drug metabolism status of MPA in renal transplant recipients.
It has been suggested that sufficient cell lysis to enable the full release of immunosuppressants was required to accurately determine the drug concentration in PBMCs.By reviewing the literature, we chose to use precipitated proteins for sample preprocessing.We observed the cell rupture under the microscope and compared the results of the drug concentration of the same sample under different sample pretreatment conditions, including different precipitants (methanol or acetonitrile), different mixing times (5min, 10min, 15min), and different centrifugation times (12000rpm *5min, *10min).It was found that the optimal extraction of MPA, MPAG, and AcMPAG from PBMCs could be achieved most efficiently using acetonitrile, vortexing for 10 minutes, and centrifugation at 12,000 rpm for 5 minutes.Compared with the other reports, our pre-treatment processing method was simpler and less time-consuming.
In the stability experiments, we found that MPA, MPAG, and AcMPAG in PBMCs could maintain their stability well when placed at room temperature for 8 hours or stored refrigerated at 4°C for 24 hours.The stability of MPA and MPAG in PBMCs was relatively stable under -80°C, but AcMPAG measured MQC and HQC levels lower than 34.94-36.23% of the basal levels after 24h of freezing and reconversion.Furthermore, the LQC of AcMPAG were detected at lower values as the freezing time progressed, degrading to 54.03%-56.83% of the basal value at each concentration level towards day 14.The three freeze-thaw cycles had no significant effect on the MPA and MPAG levels in PBMCs, whereas AcMPAG showed a significant decrease in concentration after the third freeze-thaw cycle.It has been reported in the literature that AcMPAG has similarly been found to exhibit limited stability, with AcMPAG in whole blood and non-acidified plasma decreasing significantly after 2-5 hours at room temperature[17].Thus, samples required to detect the AcMPAG levels in PBMCs should be separated as soon as possible after collection and stored in refrigeration for no more than 24 h. Samples that cannot be detected in time should be frozen and thawed no more than 3 times after freezing at -80°C and stored for no more than 24h.It has been reported that acidification of plasma samples could avoid degradation of AcMPAG deglucuronidation, and we will continue to examine whether sample acidification can improve AcMPAG stability in PBMCs in subsequent studies.
Our center used the limited time-point sampling method to detect plasma MPA concentration as the clinical implementation of MPA therapeutic drug concentration monitoring (MPA-TDM) in renal transplant recipients, which was also a more recommended approach for MPA-TDM.In patients using mycophenolate mofetil (Snapdragon®), venous blood was taken before (0h), 0.5 hours (0.5h), 2 hours (2h), and 4 hours (4h) after drug dosing for MPA measurement.We used a sample collection method synchronized with the clinically available blood collection protocol to observe the pharmacokinetic distribution characteristics of MPA, MPAG, and AcMPAG in the PBMCs of KTRs and to evaluate their clinical value in infections.
There were significant individual differences in theconcentrations of MPA and its major metabolite MPAG in PBMCs in KTRs.With the time-lapse after drug administration, MPA and MPAG levels in PBMCs showed a substantially simultaneous trend of concentration changes.The concentration of MPAG in PBMCs from renal transplant recipients was approximately 6.85-11.04 times higher than that of MPA.It has been reported that the concentration of MPAG in plasma was about 20-100 times higher than that of MPA[27].Combined with the results of our study, we suggested that there were differences in the distribution characteristics of MPAG and MPA in plasma and PBMCs, and the differences between MPAG and MPA concentrations in PBMCs were smaller than those in plasma.AcMPAG was virtually undetectable at extremely low levels in PBMCs of KTRs, except in a few recipients.And reports have shown that the concentration of plasma AcMPAG was significantly lower than that of MPA and MPAG, at approximately 10-20% of the MPA concentration [18].Since samples in our study were stored at -80°C for approximately 1 month, we could not eliminate the possibility of AcMPAG being undetectable due to the degradation.We therefore randomly collected samples from six KTRs, isolated PBMCs within 2 hours of sample collection, and immediately preprocessed the samples and assayed them, and the results similarly showed that AcMPAG was virtually undetectable.Our study suggested that a more sensitive method needs to be established to achieve reliable detection of the extremely low level of AcMPAG in PBMCs to provide clinical application.
Immunosuppressive therapy is an important part of the anti-rejection process after renal transplantation. Optimal immunosuppressive management is the foundation for successful kidney transplantation[28,29].Current studies on PBMC-MPA concentration have primarily focused on its association with graft rejection. It has been found that renal transplant recipients who developed rejection had significantly lower PBMC-MPA-C0 than patients without rejection (P=0.029), and there was a concentration-effect relationship between PBMC-MPA-C0 and the rejection severity[30]. However, studies on PBMC-MPA concentrations and infection in renal transplant recipients have hardly been reported.In this study, we found that the PBMCs of KTRs who developed infections had higher concentrations of MAP than the stable group, with significant mean PBMC-MPA concentrations at 2h post-dose and 4h post-dose.It has been confirmed in our previous study that the plasma MPA concentration at 4h post-dose in KTRs with infection was also significantly higher than that in the stable group. In the ROC curve analysis for the diagnosis of infection in KTRs, it was found that the diagnostic efficacy of PBMCs-MPA-C4 for infection was higher than that of PBMCs-MPA-C2 and higher than Plasma-MPA-C4. These results suggested that the level of MPA drug exposure in KTRs at 4 h post-dose may indeed be closely associated with infection, that MPA overexposure may be an important risk factor for the development of infection, and that the detection of MPA concentration in plasma or PBMC at 4 h post-dose may be a useful predictor of infection in KTRs.However, its exact clinical application value deserves further in-depth research by expanding the sampling volume.We also found that the concentration of MPAG in PBMCs at all time points was also higher in the infected group than the stable group of KTRs, but the difference was not statistically significant.
The plasma MPA concentration assay is currently the most commonly used marker for clinical MPA-TDM, which is convenient and automated.Although the PBMC-MPA concentration test is theoretically more responsive to the exposure level of the drug target and thus has a closer relationship with efficacy, it requires a more complex sample pretreatment process and more complicated assay techniques.We compared plasma MPA concentrations and PBMC-MPA concentrations in KTRs and found that while both presented similar drug concentration-time trends, the correlation was poor with each other.When correlation analyses were performed in subgroups, it was found that MPA concentrations in plasma correlated well with PBMCs in the stable group but poorly in the infected group, suggesting that PBMC-MPA but not Plasma-MPA monitoring may be necessary in infected KTRs. When comparing the infected and stable groups we also found that the mean concentration of PBMC-MPA was higher in the infected group than in the stable group at all four-time points, while plasma MPA concentration was higher in the infected group than in the stable group at four hours post-dose at only one-time point.With the overdose of immunosuppressants, there is an excessive suppression of the body’s immune defenses, leading to a decrease in the capacity of the immune system to resist the invasion of pathogens and infection may occur.Therefore, the results of this study indicated that PBMC-MPA concentration could more accurately reflect the immunosuppressive effect of MPA with a narrower range of fluctuation, and might be a more effective new marker for MPA-TDM.
However, there are some limitations in this study.Firstly, the assay was not sensitive enough to detect AcMPAG, leading to the fact that AcMPAG had not been accurately detected in most of the PBMCs. In the future, we will continue to optimize and improve the method for the detect sensitivity.Inadequate inclusion of clinical samples and insufficient time points for the assays may lead to bias in the assessment of PK parameters and clinical applications of MPA, MPAG, and AcMPAG in PBMCs.Follow-up studies remain necessary to expand the sample volume and increase the time points of blood collection for more intensive and detailed research.Finally, this study only focused on the relationship between MPA concentrations in plasma and PBMCs, and subsequent studies will add research on the relationship between MPAG and AcMPAG concentrations in plasma and PBMCs.
5. Conclusions
In this study, We developed an UPLC-MS/MS method for the simultaneous determination of MPA, MPAG, and AcMPAG in PBMCs concerning the Food and Drug Admin- istration and European Medicines Agency guidelines for the validation of bioanalytical methods.Preliminary studies showed that MPA concentrations in PBMCs of KTRs at 2 and 4 hours post-dose were significantly higher in the infected group than the stable group, suggesting that the detection of MPA concentrations in PBMCs may be a useful new laboratory marker for the prediction of infection in KTRs, and its clinical application value needs to be investigated in more intensive studies.
Author Contributions
Data curation, Xiaomei Chen, Shenling Liao and Shaohui Ma; Formal analysis, Xiaomei Chen and Chunxia Chen; Methodology, Xiaomei Chen, Xinhua Dai, Xueqiao Wang and Yangjuan Bai; Resources, Yangjuan Bai; Software, Xiaomei Chen and Xinhua Dai; Validation, Xiaomei Chen, Xinhua Dai and Huan Xu; Writing – original draft, Xiaomei Chen; Writing – review & editing, Yi Li and Yangjuan Bai.
Funding
This work was supported by the 1·3·5 Project for Incubation, West China Hospital, Sichuan University (no. 19HXFH023).
Data Availability Statement
Data are contained within the article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Picard, N.; Ratanasavanh, D.; Prémaud, A.; Le Meur, Y.; Marquet, P. Identification of UDP glucuronosyltransferase isoforms involved in mycophenolic acid phase II metabolism. Drug Metab Dispos 2005, 33, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Kazuaki Yoshimura et al. Pharmacokinetic and Pharmacodynamic Markers of Mycophenolic Acid Associated with Effective Prophylaxis for Acute Graft-Versus-Host Disease and Neutrophil Engraftment in Cord Blood Transplant Patients .Biology of Blood and Marrow Transplantation.2018;S1083-8791. [CrossRef]
- Sobiak J et al.Effffect of mycophenolate mofetil on hematological side effffects incidence in renal transplant recipients.Clin Transplant 2013;E407–E414. [CrossRef]
- Grinyo JM, Ekberg H, Mamelok RD et al: The pharmacokinetics of mycophenolate mofetil in renal transplant recipients receiving standard-dose or low-dose cyclosporine, low-dose tacrolimus or low-dose sirolimus: the Symphony pharmacokinetic substudy. Nephrol Dial Transplant, 2009; 24: 2269–76. 2: Nephrol Dial Transplant, 2009; 24. [CrossRef]
- MASATOMO M, TAKENORI N, SHOUTARO K, et al. Monitoring of mycophenolic acid predose concentrations in the maintenance phase more than one year after renal transplantation.[J]. Therapeutic drug monitoring, 2011,33(3). [CrossRef]
- Zegarska J, Hryniewiecka E, Żochowska D, et al. Mycophenolic acid metabolites acyl-glucuronide and glucoside affect the occurrence of infectious complications and bone marrow dysfunction in liver transplant recipients. Ann Transplant. 2015;20:483-492. [CrossRef]
- Joseph Berthier et al.MRP4 is responsible for the efflux transport of mycophenolic acid β-D glucuronide(MPAG) from hepatocytes to blood .Xenobiotica 2020.1813352. [CrossRef]
- Sobiak J et al.Effffect of mycophenolate mofetil on hematological side effffects incidence in renal transplant recipients.Clin Transplant 2013;E407–E414. [CrossRef]
- Kaplan B.Decreased protein binding of mycophenolic acid associated with leukopenia in a pancreas transplant recipient with renal failure.Transplantation.1998 Apr 27;65(8):1127-9.
- David W Mudge.Severe toxicity associated with a markedly elevated mycophenolic acid free fraction in a renal transplant recipient.Ther Drug Monit. 2004 Aug;26(4):453-5.
- Kamińska, J. Pharmacokinetics of mycophenolic acid and its phenyl glucuronide metabolite in kidney transplant recipients with renal impairment Arch Med Sci. 2012 Feb 29;8(1):88-96.
- Sobiak, J. Effect of mycophenolate mofetil on hematological side effects incidence in renal transplant recipients.Clin Transplant. 2013 Jul-Aug;27(4):E407-14.
- Colom H.Pharmacokinetic modeling of enterohepatic circulation of mycophenolic acid in renal transplant recipients.Kidney Int. 2014 Jun;85(6):1434-43. [CrossRef]
- Olivier Gensburger.Effect of Mycophenolate Acyl-Glucuronide on Human Recombinant Type 2 Inosine Monophosphate Dehydrogenase.Clinical Chemistry. [CrossRef]
- M. Shipkova The Acyl Glucuronide Metabolite of Mycophenolic Acid Inhibits the Proliferation of Human Mononuclear Leukocytes. Elsevier Science Inc 2001.PII S0041-1345.
- Jolanta Zegarska Mycophenolic Acid Metabolites Acyl-Glucuronide and Glucoside Affect the Occurrence of Infectious Complications and Bone Marrow Dysfunction in Liver Transplant Recipients.© Ann Transplant, 2015; 20. [CrossRef]
- Wieland, E. Induction of Cytokine Release by the Acyl Glucuronide of Mycophenolic Acid: A Link to Side Effects? Clinical Biochemistry 2000, 33, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Zegarska J, Hryniewiecka E, Żochowska D, et al. Mycophenolic acid metabolites acyl-glucuronide and glucoside affect the occurrence of infectious complications and bone marrow dysfunction in liver transplant recipients. Ann Transplant. 2015;20:483-492. [CrossRef]
- Staatz CE, Tett SE. Clinical pharmacokinetics and pharmacodynamics of mycophenolate in solid organ transplant recipients. Clin Pharmacokinet 2007; 46: 14–58. [CrossRef]
- Nguyen Thi MT, Capron A, Mourad M, Wallemacq P. Mycophenolic acid quantification in human peripheral blood mononuclear cells using liquid chromatography-tandem mass spectrometry. Clin Biochem. 2013 Dec;46(18):1909-11. [CrossRef]
- Bénech H, Hascoët S, Furlan V, Pruvost A, Durrbach A. Development and validation of an LC/MS/MS assay for mycophenolic acid in human peripheral blood mononuclear cells. J Chromatogr B Analyt Technol Biomed Life Sci. 2007 Jun 15;853(1-2):168-74. [CrossRef]
- Bioanalytical Method Validation Guidance for Industry. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/bioanalytical-method-validation-guidance-industry (accessed on 10 September 2022).
- Bioanalytical Method Validation. Available online: https://www.ema.europa.eu/en/bioanalytical-method-validation (accessed on 10 September 2022).
- Muzeeb Syed,and Nuggehally R. Srinivasb .A comprehensive review of the published assays for the quantitation of the immunosuppressant drug mycophenolic acid and its glucuronidated metabolites in biological fluids.Biomed. Chromatogr. 2016; 30: 721–748.
- Bing Chen, PhD, Jia-Qian Lu, MSc,Pei-Jun Zhou, MD, PhD et al.Establishment of a Liquid Chromatography-Tandem Mass Spectrometry Method for the Determination of Immunosuppressant Levels in the Peripheral Blood Mononuclear Cells of Chinese Renal Transplant Recipients.Ther Drug Monit 2020;42:686–694. [CrossRef]
- Henriette de Loor elt al.Stability of mycophenolic acid and glucuronide metabolites in human plasma and the impact of deproteinization methodology.Clinica Chimica Acta.2008;389 :87–92. [CrossRef]
- Elbarbry FA, Shoker AS.Therapeutic drug measurement of mycophenolic acid derivatives in transplant patients .Clin Biochem. 2007 Jul;40(11):752-64. [CrossRef]
- Halloran PF. Immunosuppressive drugs for kidney transplantation. N Engl J Med 2004; 351:2715–29. [CrossRef]
- Ferrara, J.L.; Levine, J.E.; Reddy, P.; Holler, E. Graft-versus-host disease. Lancet 2009, 373, 1550–1561. [Google Scholar] [CrossRef] [PubMed]
- DOM Z I M, COLLER J K, CARROLL R P, et al. Mycophenolic acid concentrations in peripheral blood mononuclear cells are associated with the incidence of rejection in renal transplant recipients[J]. British Journal of Clinical Pharmacology, 2018,84(10). [CrossRef]
Figure 1.
The work of this study was presented in visual form. The details can be divided into 10 sections as shown in Figure 1. In this study, we developed and established a reliable method to monitor the concentration of MPA and metabolites MPAG and AcMPAG in PBMCs PBMCs and applied it to the analysis of clinical samples from the infected KTRs.
Figure 1.
The work of this study was presented in visual form. The details can be divided into 10 sections as shown in Figure 1. In this study, we developed and established a reliable method to monitor the concentration of MPA and metabolites MPAG and AcMPAG in PBMCs PBMCs and applied it to the analysis of clinical samples from the infected KTRs.
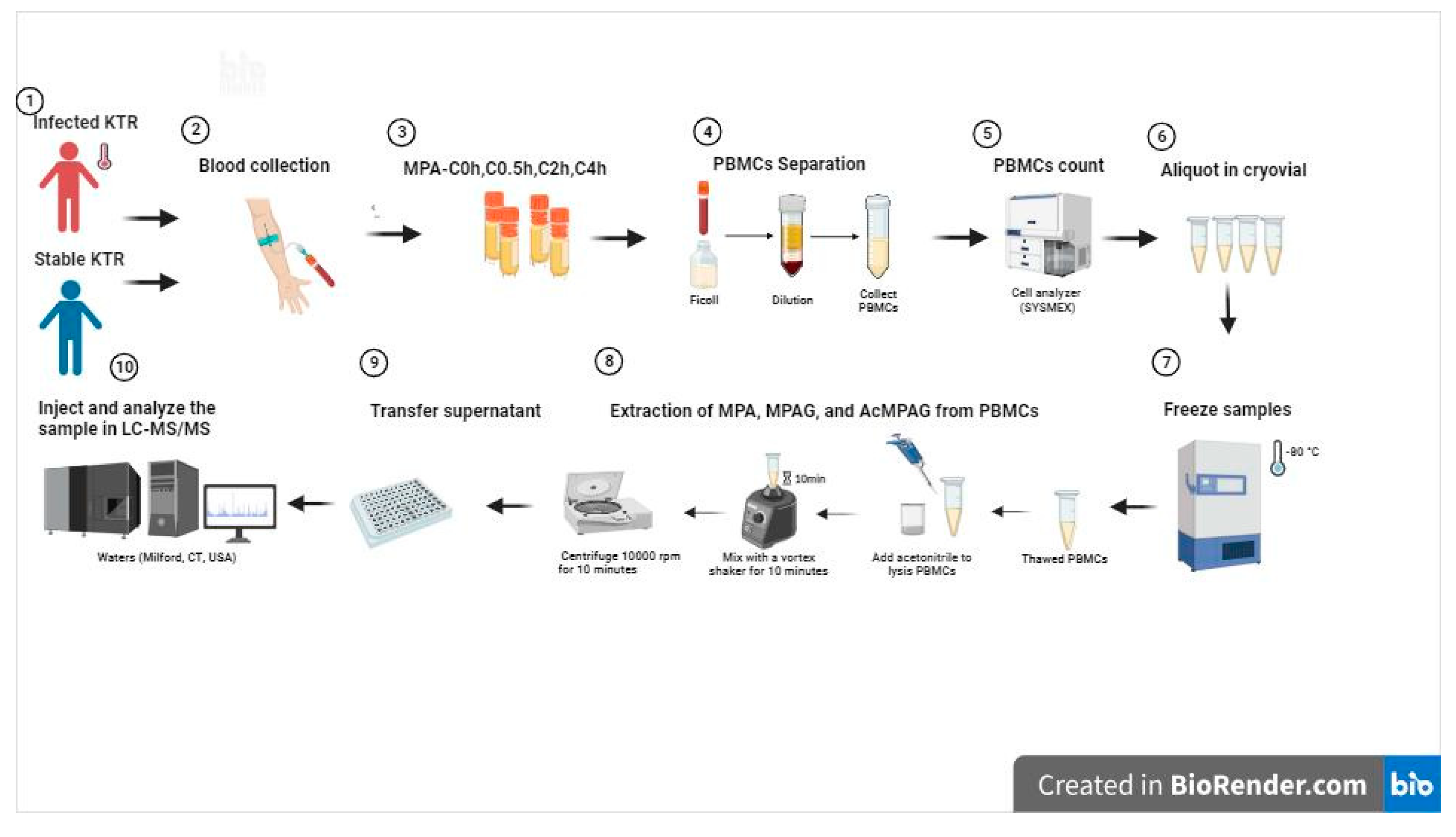
Figure 3.
Characteristics of the distribution of MPA and MPAG concentrations in PBMCs from KTRs in the infected and stable groups.(a)Distribution of concentration of MPA in PBMCs at various time points in the infected group(n=8);(b) Distribution of concentration of MPAG in PBMCs at various time points in the infected group(n=8); (c)Distribution of concentration of MPA in PBMCs at various time points in the stable group(n=7);(d)Distribution of concentration of MPAG in PBMCs at various time points in the stable group(n=7).
Figure 3.
Characteristics of the distribution of MPA and MPAG concentrations in PBMCs from KTRs in the infected and stable groups.(a)Distribution of concentration of MPA in PBMCs at various time points in the infected group(n=8);(b) Distribution of concentration of MPAG in PBMCs at various time points in the infected group(n=8); (c)Distribution of concentration of MPA in PBMCs at various time points in the stable group(n=7);(d)Distribution of concentration of MPAG in PBMCs at various time points in the stable group(n=7).
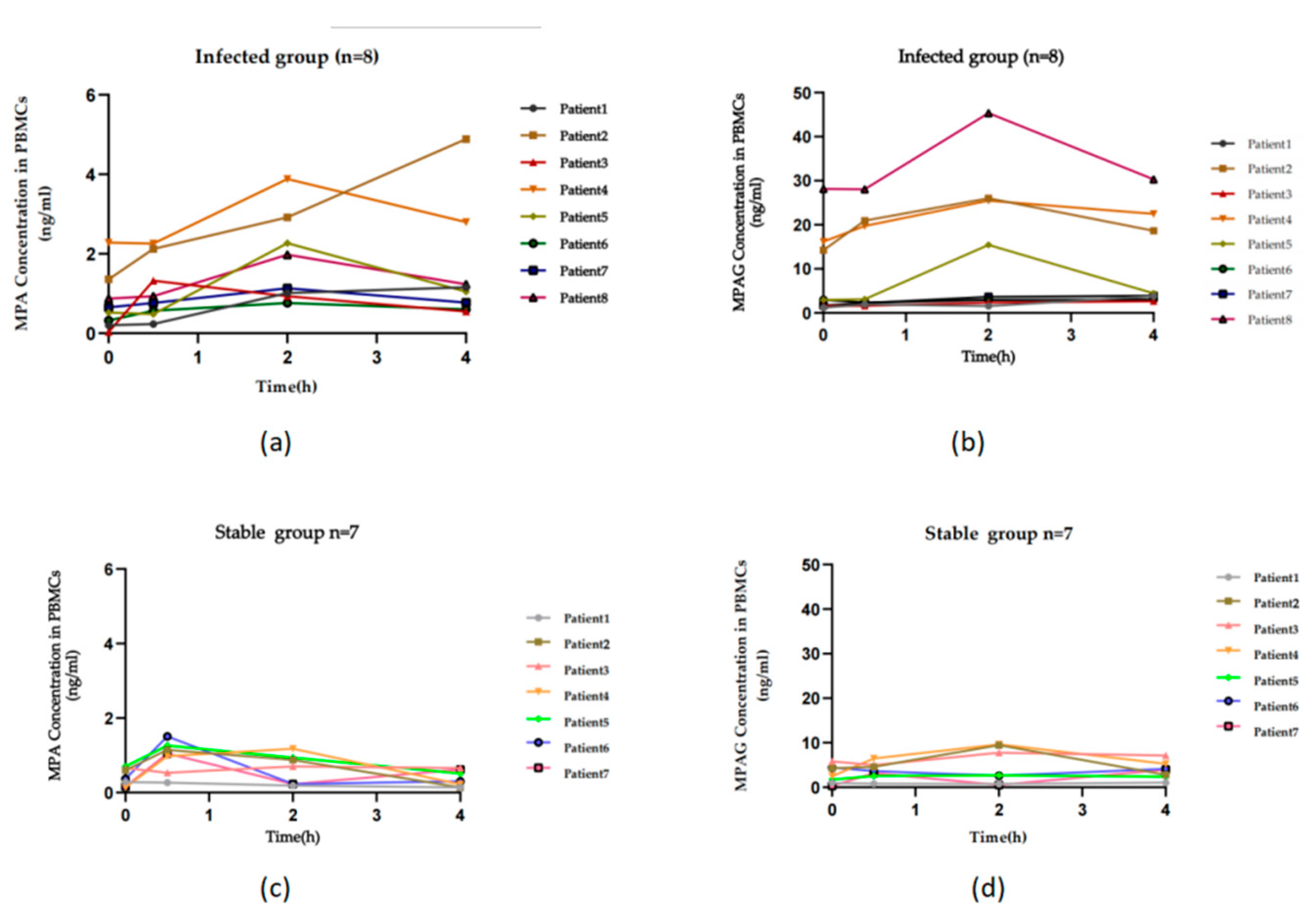
Figure 4.
Differences in concentrations of MPA and MPAG at different time points in PBMCs from infected and stable groups and concentrations of MPA in plasma at different time points.(a)Differences in MPA concentrations in PBMCs between infected and stable groups at various time points;(b)Differences in MPAG concentrations in PBMCs between infected and stable groups at various time points.;(c)Differences in MPA concentrations in Plasma between infected and stable groups at various time points.
Figure 4.
Differences in concentrations of MPA and MPAG at different time points in PBMCs from infected and stable groups and concentrations of MPA in plasma at different time points.(a)Differences in MPA concentrations in PBMCs between infected and stable groups at various time points;(b)Differences in MPAG concentrations in PBMCs between infected and stable groups at various time points.;(c)Differences in MPA concentrations in Plasma between infected and stable groups at various time points.
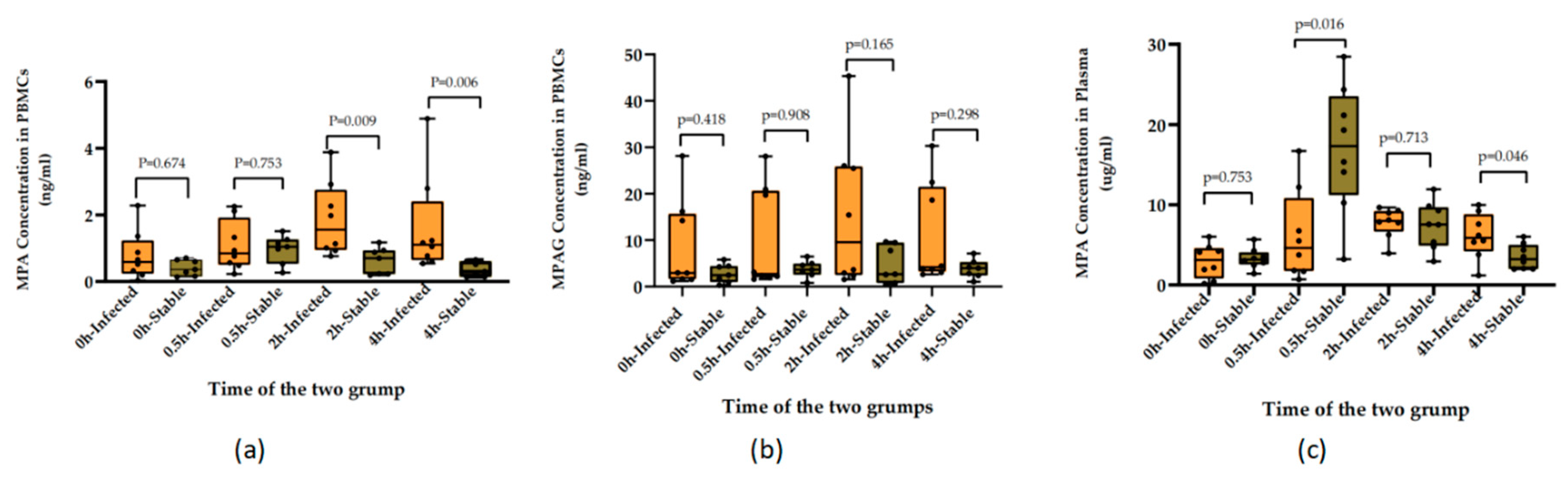
Figure 5.
Analysis of the ROC curve (area under curve,AUC) for infections after renal transplantation.(a)ROC curve analysis of infections after renal transplantation using PBMCs-MPA-C4.(b)ROC curve analysis of infections after renal transplantation using PBMCs-MPA-C2.(c)ROC curve analysis of infections after renal transplantation using Plasma-MPA-C4.
Figure 5.
Analysis of the ROC curve (area under curve,AUC) for infections after renal transplantation.(a)ROC curve analysis of infections after renal transplantation using PBMCs-MPA-C4.(b)ROC curve analysis of infections after renal transplantation using PBMCs-MPA-C2.(c)ROC curve analysis of infections after renal transplantation using Plasma-MPA-C4.
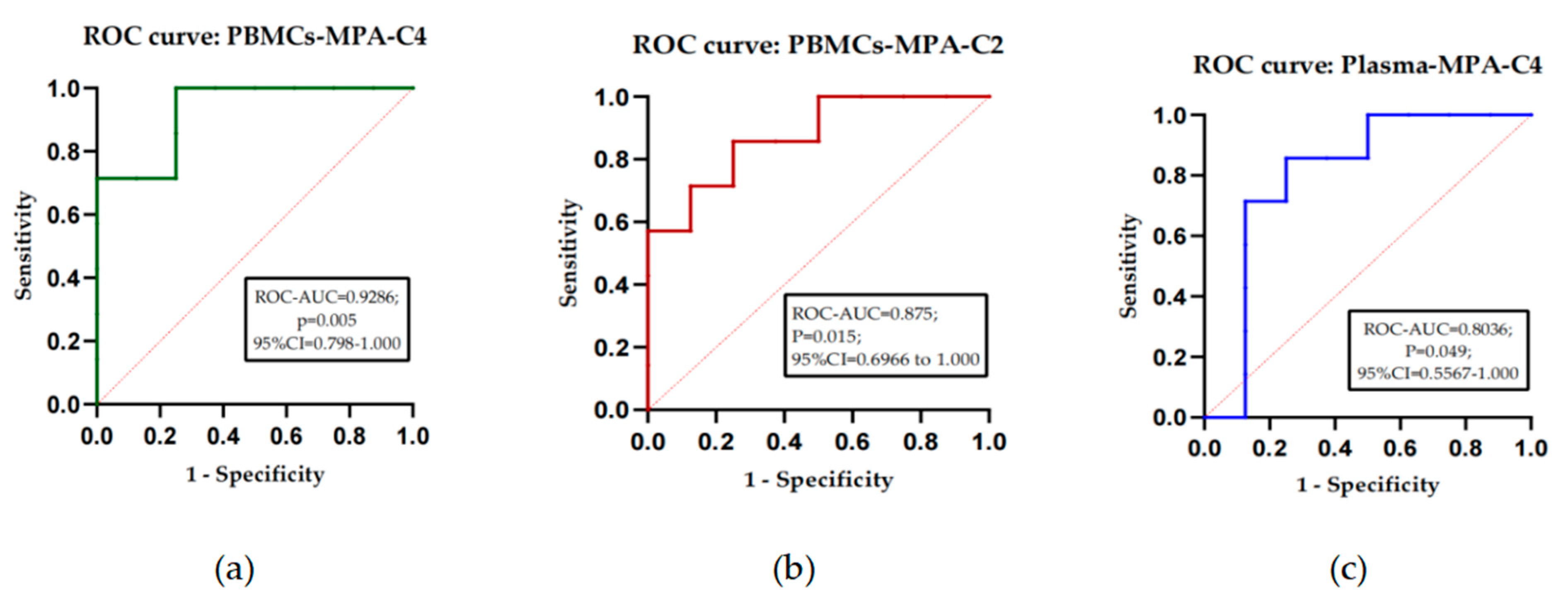
Figure 6.
Correlation analysis of MPA concentrations in PBMCs and plasma.(a)Distribution of MPA in plasma at various time points in the infected group;(b)Distribution of MPA in plasma at various time points in the stable group;(c)Correlation analysis of plasma (X-axis) and concentration of MPA in PBMCs (Y-axis) at various time points in both groups;(d)Correlation analysis of the concentration of MPA in plasma and PBMCs at various time points in the infected group;(e)Correlation analysis of the concentration of MPA in plasma and PBMCs at various time points in the stable group.
Figure 6.
Correlation analysis of MPA concentrations in PBMCs and plasma.(a)Distribution of MPA in plasma at various time points in the infected group;(b)Distribution of MPA in plasma at various time points in the stable group;(c)Correlation analysis of plasma (X-axis) and concentration of MPA in PBMCs (Y-axis) at various time points in both groups;(d)Correlation analysis of the concentration of MPA in plasma and PBMCs at various time points in the infected group;(e)Correlation analysis of the concentration of MPA in plasma and PBMCs at various time points in the stable group.
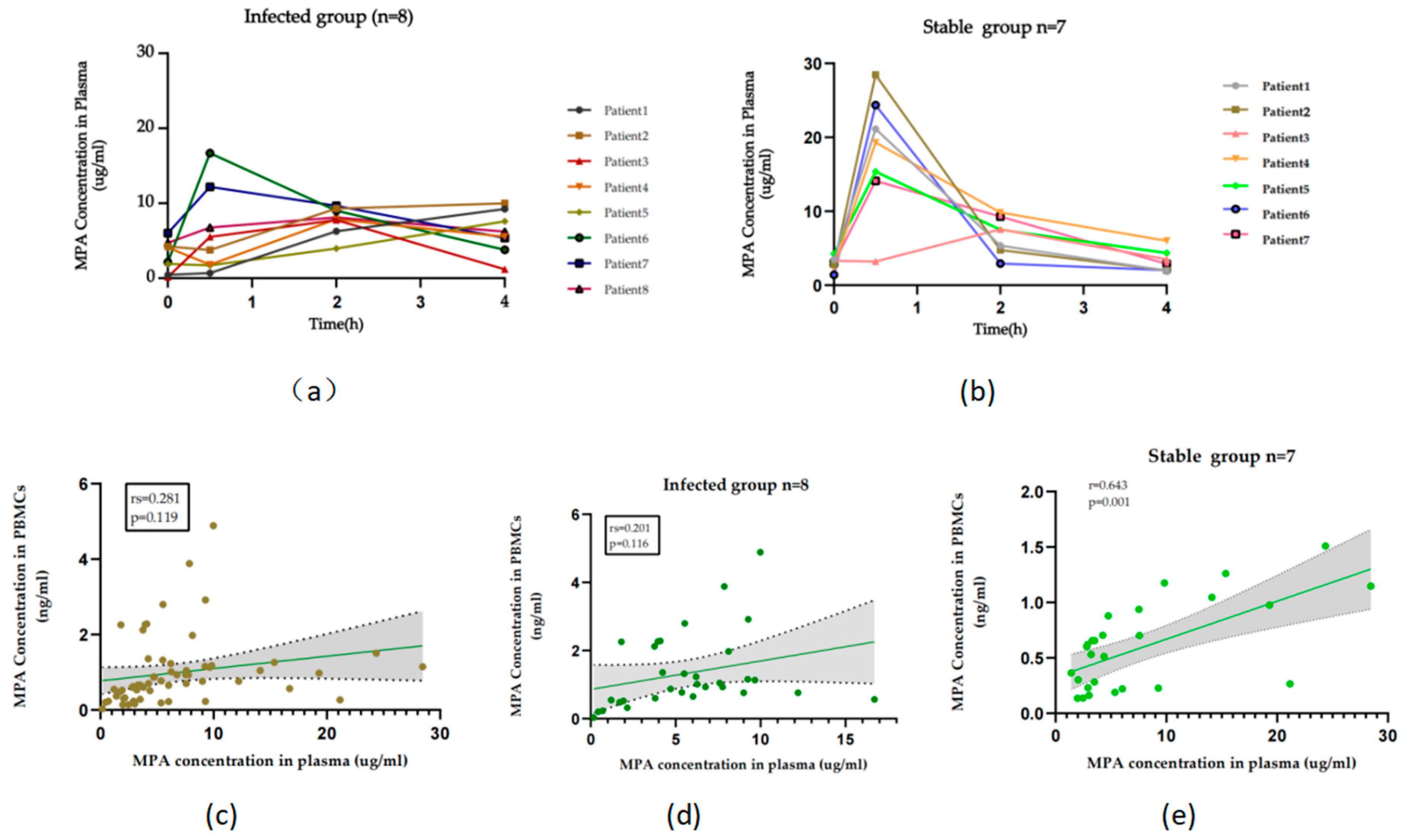

Table 1.
Multiple reaction monitoring (MRM) optimization settings for each analyte.
| Analyte | ESI mode | Parent ion (m/z) |
Product ion (m/z) |
Cone voltage (V) |
Collision energy (eV) |
|---|---|---|---|---|---|
| MPA | + | 321.27 | 207.15 | 80.00 | 22.00 |
| MPAG | + | 514.27 | 321.20 | 8.00 | 10.00 |
| AcMPAG | + | 514.26 | 321.20 | 40.00 | 10.00 |
| MPA-d3 | + | 324.26 | 210.15 | 8.00 | 22.00 |
Table 2.
Matrix and recovery of MPA, MPAG and AcMPAG.
| QCs | Peak area in PBMCs | Peak area in Methanol | Matrix effect(%) | Recovery(%) | |
|---|---|---|---|---|---|
| MPA | LLOQ | 559.13 | 562.82 | -3.65 | 104.4 |
| LQC | 1129.28 | 1115.94 | 0.59 | 103.56 | |
| MQC | 44215.02 | 51203.82 | -9.22 | 100.24 | |
| HQC | 176298.91 | 184589.71 | -2.01 | 96.2 | |
| MPAG | LLOQ | 457.17 | 485.81 | -6.74 | 91.39 |
| LQC | 1015.68 | 942.62 | 10.45 | 96.71 | |
| MQC | 6703.8 | 6250.53 | 6.63 | 109.98 | |
| HQC | 25811.82 | 24554.00 | 7.21 | 107.13 | |
| AcMPAG | LLOQ | 82.43 | 92.06 | -7.49 | 86.6 |
| LQC | 235.01 | 261.15 | -11.42 | 91.62 | |
| MQC | 2962.55 | 3040.46 | -6.45 | 98.58 | |
| HQC | 11953.42 | 12424.06 | -3.66 | 94.95 | |
Table 3.
Intra/inter-batch precision and accuracy of MPA, MPAG and AcMPAG at LLOQ, LQC, MQC and HQC concentrations.
Table 3.
Intra/inter-batch precision and accuracy of MPA, MPAG and AcMPAG at LLOQ, LQC, MQC and HQC concentrations.
| Concentration (ng/mL) |
Intra-batch | Inter-batch | |||||
|---|---|---|---|---|---|---|---|
| Found (ng/mL) |
Imprecision CV (%) |
Accuracy (%) |
Found (ng/mL) |
Imprecision CV (%) |
Accuracy (%) |
||
| MPA * | LLOQ(0.05) | 0.04 | 6.15 | 93.86 | 0.04 | 0.92 | 99.08 |
| LQC(0.15) | 0.14 | 3.52 | 96.48 | 0.15 | 3.40 | 97.60 | |
| MQC(10.00) | 9.41 | 5.95 | 94.05 | 9.49 | 5.36 | 94.64 | |
| HQC(40.00) | 37.61 | 5.98 | 94.02 | 36.28 | 10.25 | 89.75 | |
| MPAG* | LLOQ(0.50) | 0.47 | 5.72 | 94.20 | 0.48 | 4.78 | 95.22 |
| LQC(1.50) | 1.47 | 2.14 | 97.87 | 1.48 | 1.27 | 99.63 | |
| MQC(10.00) | 9.74 | 2.56 | 97.44 | 10.82 | 7.56 | 92.44 | |
| HQC(40.00) | 38.31 | 4.23 | 95.77 | 40.92 | 2.24 | 97.76 | |
| LLOQ(0.10) | 0.09 | 3.76 | 96.00 | 0.09 | 9.39 | 91.61 | |
| AcMPAG | LQC(0.30) MQC(4.00) HQC(16.00) |
0.28 | 6.69 | 93.33 | 0.28 | 7.17 | 92.83 |
| 3.84 | 4.10 | 95.90 | 4.16 | 3.93 | 96.07 | ||
| 15.54 | 2.88 | 97.12 | 15.70 | 1.88 | 98.12 | ||
Table 4.
Stability evaluation of MPA, MPAG and AcMPAG.
| QCs | Room temperature | Frozen(4℃) | Freeze-Thaw(Round1-3) | Autosampler | ||||
|---|---|---|---|---|---|---|---|---|
| 2h-RSD(%) | 8h-RSD (%) |
24h-RSD (%) |
R1-RSD(%) | R2-RSD(%) | R3-RSD(%) | 24h-RSD(%) | ||
| MPA | LLOQ | 8.40 | 6.33 | 3.31 | 0.90 | 2.33 | 6.66 | 2.33 |
| LQC | 10.67 | 10.67 | 5.45 | 10.67 | 10.68 | 10.66 | 10.67 | |
| MQC | 1.09 | 2.29 | 3.53 | 13.65 | 11.58 | 7.73 | 2.28 | |
| HQC | 7.85 | 2.15 | 9.38 | 10.63 | 12.12 | 12.43 | 7.85 | |
| MPAG | LLOQ | 10.56 | 14.4 | 5.51 | 5.20 | 3.50 | 5.13 | 5.19 |
| LQC | 1.55 | 6.06 | 1.14 | 4.61 | 0.13 | 3.31 | 1.15 | |
| MQC | 10.30 | 5.64 | 0.67 | 10.87 | 8.00 | 5.96 | 5.64 | |
| HQC | 1.88 | 9.92 | 9.76 | 7.58 | 8.48 | 7.04 | 8.47 | |
| AcMPAG | LLOQ | 11.66 | 4.10 | 6.95 | 3.50 | 2.15 | 36.50 | 6.95 |
| LQC | 5.16 | 6.80 | 2.46 | 1.44 | 2.05 | 8.05 | 1.43 | |
| MQC | 3.48 | 14.11 | 5.05 | 11.77 | 13.1 | 19.67 | 14.09 | |
| HQC | 4.32 | 8.44 | 4.58 | 1.75 | 0.76 | 2.42 | 0.76 | |
Table 5.
Stability of MPA, MPAG, and AcMPAG of PBMCs at -80°C in frozen.
| QCs | 24h-RSD (%) |
48h-RSD (%) |
72h-RSD (%) |
7d-RSD (%) |
14d-RSD (%) |
||
|---|---|---|---|---|---|---|---|
| MPA | LLOQ | 4.00 | 2.00 | 2.00 | 12.00 | 2.00 | |
| LQC | 5.33 | 0.67 | 4.00 | 10.66 | 11.33 | ||
| MQC | 2.01 | 1.08 | 0.02 | 10.04 | 11.09 | ||
| HQC | 0.31 | 0.80 | 0.39 | 5.52 | 5.02 | ||
| MPAG | LLOQ | 2.60 | 0.20 | 13.60 | 4.20 | 4.60 | |
| LQC | 2.13 | 8.80 | 0.86 | 4.46 | 0.13 | ||
| MQC | 9.80 | 2.11 | 0.01 | 10.87 | 4.33 | ||
| HQC | 0.54 | 1.05 | 0.30 | 2.75 | 2.61 | ||
| AcMPAG | LLOQ | 6.00 | 12.16 | 19.33 | 49.83 | 56.83 | |
| LQC | 13.50 | 30.16 | 48.61 | 53.61 | 53.05 | ||
| MQC | 36.26 | 40.04 | 43.25 | 51.50 | 56.38 | ||
| HQC | 34.92 | 36.25 | 36.16 | 41.97 | 54.03 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



