Submitted:
09 January 2024
Posted:
09 January 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background: To describe the effectiveness and safety of COVID-19 vaccine in a series of patients with rheumatoid arthritis (RA). Methods: Retrospective single-center study of RA patients, fulfilling the ACR 1987 or ACR/EULAR 2010 classification criteria, that received first COVID-19 vaccine between December 2020 and October 2021, had post-vaccination serology and subsequent follow-up of at least 6 months in a university hospital. Vaccine effectiveness was evaluated by the serological response and the incidence of post-vaccine COVID-19, and safety by the incidence of adverse events (AE) and RA flares. Adjusted logistic and linear multivariate regression analyses were carried out with Stata® to identify factors associated with vaccine response. Results: We included 118 patients with RA (87.2% women, age 65.4±11.6 years, evolution 12.0±9.6 years). 95.8% received complete vaccination schedule. Most patients (88.1%) developed adequate humoral immunogenicity, and the degree of serological response was significantly related to younger age and previous COVID-19 infection. After vaccination, 18.6% presented mild SARS-CoV-2 infection. Vaccine AE (19.5%) were mostly mild and inversely associated with age (OR 0.95). RA flares were anecdotal (1.7%) and inversely related to age (OR 0.95). Conclusion: Our results suggest that COVID-19 vaccine induces adequate humoral immunogenicity, with an acceptable safety profile in RA patients.
Keywords:
Rheumatoid arthritis
; COVID-19 vaccine
; humoral response
; effectiveness
; safety
1. Introduction
Rheumatoid arthritis (RA) is a chronic systemic inflammatory disease with a prevalence of 0.9% in Spain and 0.2-1.2% worldwide, being more common in women [1,2].
In its etiopathogenesis converge predisposing genetic factors (HLA-DR4 in the white race, shared epitope), which subjected to various environmental stimuli that are not completely elucidated (continuous exposure to tobacco, certain viral infections, etc.) can trigger an immune response that initiates subclinical organic damage that, after a second impact or environmental exposure, gives rise to symptomatic joint and/or extra-articular damage [3].
This underlying immune disorder justifies that the mainstay of treatment is immunomodulatory drugs such as disease-modifying antirheumatic drugs (DMARDs), frequently requiring the addition of glucocorticoids (GC). Conventional synthetic DMARDs (csDMARDs) such as methotrexate (MTX), leflunomide, sulfasalazine or hydroxychloroquine constitute the first therapeutic step, with MTX being its cornerstone. When an adequate response is not achieved, they are replaced or combined with each other or with targeted-directed DMARDs (tdDMARDs) such as JAK inhibitors (JAKinh) or with biological DMARDs (bDMARDs) such as tumor necrosis factor alpha antagonists (aTNF) (infliximab, etarnecept, adalimumab, golimumab or certolizumab), rituximab (RTX), abatacept (ABA) or interleukin-6 receptor inhibitors (tocilizumab or sarilumab), mainly.
The immune system dysfunction generated by the disease itself and by its immunomodulatory treatments increases the predisposition of these patients to suffer infections, as well as their severity. For this reason, the magnitude and severity of the SARS-CoV-2 coronavirus pandemic raised particular initial concern about its potential impact on RA patients. In the early stages of the SARS-CoV-2 pandemic, several studies suggested that the risk of the COronaVIrus Disease 2019 (COVID-19) was 1.3 to 3 times higher in patients with autoimmune diseases, and that the disease itself might constitute a risk factor for infection severity related to high disease activity or some of its treatments, such as RTX or high doses of GC [4-7]. However, later on evidence identified in RA patients the relevance of infection severity risk factors that were common to the general population, such as advanced age and comorbidities, including cardiovascular disease (CVD), chronic obstructive pulmonary disease (COPD) or chronic kidney failure [6].
The lack of a specific treatment for COVID-19 at the beginning of the pandemic made crucial the efforts to develop an effective vaccine that would prevent transmission and/or severe clinical manifestations in patients with RA. However, the clinical trials carried out for the vaccine registration did not allow conclusions to be drawn for patients with RA, as they were excluded [8]. Furthermore, in patients with immune-mediated inflammatory diseases (IMIDs) such as RA, it is especially important to study not only the immunogenic response to the vaccine, as it could potentially be reduced by both the disease itself and the DMARDs used, but also the potential risk of reactivation of the disease after vaccination [9].
Previous research with other commonly used vaccines, such as influenza vaccine and pneumococcal vaccine, have shown that they are safe in RA, but some DMARDs such as MTX, ABA and RTX decrease their immunogenicity, reason why some guidelines and authors have advised temporary therapeutic adjustments to mitigate their impact [10-15]. Focusing on MTX, which is the most widely used drug for the treatment of RA, two randomized studies concluded that the suspension of MTX for 2 weeks after influenza vaccination in patients with RA improved the humoral response by 20%, without associating an increased risk of disease relapse [14,15].
In the case of the SARS-CoV-2 vaccines, it is not only relevant to have data on their efficacy and safety in RA, but also to investigate the factors potentially associated with the immunogenic response to the vaccines and to analyze potential differences related to the type of vaccine administered. In Spain, COVID-19 vaccines initially available were messenger RNA (mRNA) vaccines (BNT162b2 from Pfizer®, mRNA-1273 from Moderna®) and adenovirus vector vaccines (AZD1222 from AstraZeneca®, Ad.26.COV2.S from Johnson & Johnson®), characterized by quite novel mechanisms. The former had been tested in humans against influenza virus and rabies virus, but had not been used on a large scale; and the latter ones had recently been commercialized [16]. As an additional variability factor, each vaccine has a different dosage and administration schedule: a) BNT162b2: two doses of 30 micrograms separated by 3 weeks; b) mRNA-1273: two doses of 100 micrograms separated by 4 weeks; c) AZD1222: two 0.5 milliliter doses separated by 10 to 12 weeks; d) Ad.26.COV2.S: single dose of 0.5 milliliters [16,17].
On the other hand, based on the evidence on influenza vaccine [12,14,15], it is presumable that the humoral immunogenicity of the SARS-CoV-2 vaccine in patients with RA on DMARDs therapy might be decreased and could be improved with short temporary drug withdrawals in the peri-vaccine period. This objective led the American College of Rheumatology (ACR) to publish preliminary recommendations agreed by experts, that have been recently updated, on the possibility of taking rest periods from some DMARDs after vaccination against SARS-CoV-2 in patients with RA, with controlled disease and at the discretion of their attending rheumatologist [8, 18]. However, the lack of scientific evidence and uniform recommendations from different societies on the guidelines to be followed at the beginning of the vaccination campaign, the characteristics of the disease and the comorbidities of each patient, as well as the different physician’s criteria and the patients' opinion, will have probably led to heterogeneous management of DMARDs in the peri-vaccine period, with a potential influence on the humoral immunogenicity of the vaccine. However, and without downplaying the development of antibodies after the COVID-19 vaccine, another crucial aspect is the clinical effectiveness of vaccination in patients with RA in terms of reducing the incidence of infection and/or its severity, as final objectives.
The severity of the SARS-CoV-2 pandemic, as well as the well-founded suspicion of the need for successive administrations of this vaccine to patients with RA in the coming years led us to study the effectiveness and safety of the COVID-19 vaccine in this population.
2. Materials and Methods
2.1. Hypothesis
Based on previous evidence on the efficacy and safety of the COVID-19 vaccine in the general population along with existing data on the behavior of other vaccines such as influenza or pneumococcus in patients with RA, our starting hypothesis was that the COVID-19 vaccine would be capable of inducing an adequate humoral response in the majority of patients, would be safe and would have a beneficial clinical impact, allowing the incidence and/or severity of infection by the SARS-CoV2 virus to be reduced. We also hypothesized that disease activity, age, comorbidity, treatment with DMARDs and/or the type of vaccine administered, among other factors, could have an influence on the efficacy and safety of the COVID-19 vaccine in this population.
2.2. Methods
We designed a retrospective longitudinal study that included patients with RA that had been vaccinated against the SARS-CoV-2 during the first COVID-19 vaccination campaign in 2020-2021, and who had subsequent follow-up under conditions of real-world clinical practice in a tertiary hospital center for at least 6 months.
2.2.1. Objectives of the study
2.2.1.1. Primary objectives
To evaluate the profile of humoral immunogenicity induced by the SARS-CoV-2 vaccine and to investigate its safety in patients with RA.
2.2.1.2. Secondary objectives
To identify the factors associated with the humoral response to the vaccine and its potential adverse events and to analyze the protective effect of this vaccine against the SARS-CoV-2 infection and/or its severity.
2.2.3. Study population
Patients with RA diagnosed according to the 1987 ACR classification criteria [19] and/or the 2010 ACR/EULAR classification criteria [20], treated in the Rheumatology Department of the Hospital Universitario de La Princesa (HUP), who had been administered the COVID-19 vaccine between December 2020 and October 2021, had a post-vaccination control serology and a subsequent follow-up at the outpatients’ clinic for a minimum of 6 months.
As this is a retrospective “non-intervention” study, informed consent (IC) was not required for the use of data in an academic research study. Nonetheless, the study protocol received approval from the Ethics Committee for Research with Medicines of the HUP (number ecl.4790).
2.2.4. Analyzed variables
Reviewing the data available in each patient's electronic medical record, the variables listed in Table A1 (Appendix A), including socio-demographic characteristics, RA and its treatment, vaccination against SARS-CoV-2 and serological response, and both previous and post-vaccination COVID-19, were collected in an anonymized database.
Anti-SARS-CoV-2 IgG antibody titers were obtained with the SARS CoV-2 IgG II QUANT Alinity technique (Abbott®). Humoral response to the vaccine was considered negative if <7.1 BAU/mL and positive if ≥7.1 BAU/mL.
2.2.5. Statistical analysis
A descriptive analysis was performed with measures of central tendency (mean and/or median) and dispersion (standard deviation (SD) and/or interquartile range (IQR)) for the quantitative variables, showing frequencies and proportions for the qualitative variables. For analytical studies aimed at investigating the factors associated with the efficacy and/or safety of SARS-CoV-2 vaccine, univariate analysis of variance (ANOVA), Student's t test and Fisher's exact test were used, depending on the characteristics of the variables under analysis. Subsequently, a multivariate logistic and linear regression analysis was performed, including the variables that were significant in the bivariate analysis. Values were considered statistically significant if p≤0.05. Statistical analysis was performed with Stata v.14® (StataCorp, United States).
3. Results
3.1. Characteristics of the study population
Between December 2021 and April 2022, we analyzed 118 patients with RA who had received at least one dose of the SARS-CoV-2 vaccine. The mean (±SD) age of the study population was 65.47±11.69 years, with 87.29% being women and 92.37% of European ancestry.
It is noteworthy that 35.59% were active smokers or ex-smokers, and 57.63% had comorbidities (Figure 1), the most frequent being dyslipidemia (41.53%) and high blood pressure (31.36%).
Mean age of RA onset was 53.04±13.64 years. The characteristics of RA are shown in Table 1 and the types of extra-articular manifestations in Figure 2.
Regarding previous RA treatment, 30.51% had been treated with GC, 96.61% with MTX, 22.03% with hydroxychloroquine, 38.14% with leflunomide and 49.15% with bDMARDs or JAKinh. Current therapies can be seen in Table 2 and included: 83.89% MTX and 46.61% bDMARDs or JAKinh, RTX being the most frequent biological therapy (16.10%), with an average of 6.88±4.05 treatment cycles. Combined treatment of csDMARDs and bDMARDs or JAKinh was used in 51.7% of patients, with an average number of DMARDs of 1.5±0.6. When assessing the immunogenicity induced by vaccination, it is important to take into account that 17.8% of our population had previously been infected by SARS-CoV-2. The diagnosis was made by polymerase chain reaction (PCR) in 54.55% and by antigen test in 45.45%, at Primary Care (68.18%) or Hospital Care (31.82%) settings. All the cases were symptomatic, and the most frequent manifestations were fever (66.67%) and cough (47.61%). COVID-19 was severe in 6 patients (5.08%) who required hospitalization, lasting 3.95±9.44 days, and high-flow oxygen therapy, but none of them needed to be admitted to the ICU. Pre-vaccination infection was significantly associated with male sex (p=0.016).
3.2. Vaccination against SARS-CoV-2
95.76% of patients received the complete vaccination schedule. Five patients, who had previously suffered COVID-19, received just one dose of the vaccine (1 BNT162b2 and 4 AZD1222), following the initial vaccination recommendations of our Local Health Authorities.
The most frequently administered vaccine was the BNT162b2 mRNA vaccine (67.8%), followed by the AZD1222 adenovirus vector vaccine (16.1%). The types of vaccines administered are shown in Figure 3.
3.3. Vaccine efficacy and safety
3.3.1. Positive serological response and degree of response
104 (88.13%) patients developed humoral immunogenicity after vaccination. The mean post-vaccination serological levels were 939.72±1,657.33 BAU/mL, being the mean time from vaccination to serological determination of 4.4±2.2 months. The achievement and degree of the serological response was not associated either with the type of vaccine or with the number of doses administrated. Regarding peri-vaccine adjustments of DMARDs, the mean time from the last dose of RTX to vaccination was 12±10.5 months (range: 0.5–36.7) and the mean time to administration of further RTX cycles after vaccination was 5.2±1.9 months (range:1.6–8.2). Regarding MTX, at least 37.28% of the patients temporary withdrew it for 1.55±0.55 weeks. No information was available for the rest of DMARDs in the electronic records.
Table 2 shows the bivariate analysis carried out to identify the factors associated with the achievement of serological response to the vaccine. The humoral response induced by the vaccine showed a significant inverse association with the smoking pack-years (p<0.001), extra-articular manifestations (p=0.045) and anti-cyclic citrullinated peptide (aCCP) antibodies titer (p=0.005).
Regarding the degree of serological response, in bivariate analysis it was significantly associated with male sex (p=0.019), CRP (p=0.006), adalimumab treatment (p=0.003), leflunomide dose (p=0.012) and previous COVID-19 infection (p<0.001), and inversely related to ESR (p=0.020). The DMARDs not shown in the table did not present a significant association with either the humoral response or the degree of humoral immunogenicity.
Multivariate logistic and linear regression analysis were adjusted for age, sex, and time elapsed from vaccination to serological determination. The only factors that maintained statistical significance were smoking pack-years (OR 0.96, 95% CI: 0.94–0.99, p=0.034), which showed an inverse association with vaccine immunogenicity, and previous infection by COVID-19 (coefficient 4.496, 95% CI: 3.604–5.388, p<0.001) and age (coefficient -16.11, 95% CI: -31.84 to -0.39, p=0.045), which were directly and inversely associated with the degree of response to the vaccine, respectively.
3.3.2. Post-vaccination SARS-CoV-2 infection
During follow-up, 22 (18.64%) patients suffered post-vaccination COVID-19, 3 of whom had been previously infected. At the time of post-vaccination infection, 10 (45.45%) of them had already received a third booster dose. Of the 3 patients with previous COVID-19, two of them had received just 1 dose of the vaccine and the third one had been administered 2 doses and an additional booster dose. We did not find a significant association between post-vaccination infection and the number of vaccine doses received (p=0.541) or degree of the serological response to the vaccine (p=0.1447). The majority of patients, 17 (77.27%), were symptomatic, being cough (40.90%), nasal congestion (36.36%), expectoration (27.27%), fever (27.27%) and malaise (27.27%) the most frequent symptoms. Most notably, and in contrast to pre-vaccination infection, none of them required hospital admission. Bivariate analysis showed that post-vaccination SARS-CoV-2 infection was significantly associated with the presence of comorbidities such as deep vein thrombosis (p=0.033) and asthma (p=0.039), and as far as treatment is concerned, with the use of ABA (p=0.033), identifying a trend towards association with younger age (p=0.058) and shorter RA evolution (p=0.051). However, only the coexistence of asthma showed statistical significance in multivariate logistic regression analysis (OR 7.6, 95% CI 1.6-36.2, p=0.011).
3.3.3. Vaccine safety
Vaccination was generally well tolerated. AE following vaccination occurred in 19.5% (n=23) of the patients after the first dose and in 18.6% (n=19) after the second dose, but none of them were severe (Figure 4). The most frequent AE were skin rash and arthralgias.
Only 2 (1.7%) patients had mild reactivation of arthritis after vaccination: 1 of them after both vaccine doses, and the other one only after the first dose. These symptoms resolved without any readjustment of their RA treatment.
Younger age (60.6±13.7 versus 66.7±10.9, p=0.02) and receiving RTX treatment (8 (34.8%) versus 11 (11.6%), p=0.007) were associated with the occurrence of AE after the first dose of the vaccine. Only RTX treatment maintained statistical significance in multivariate logistic regression analysis (OR 3.7, 95%CI 1.2-11.0, p=0.020), with a trend towards significance for age (OR 0.96, 95%CI 0.9-1.0, p=0.052). After the second dose of vaccine, in addition to younger age (60.4±11.7 versus 67.3±11.6, p=0.020) and RTX treatment (6 [31.6%] versus 11 [13.1%], p=0.050), mRNA-1273 vaccine (5 [26, 3%] versus 4 [4.8%], p=0.019) and having had AE after the first dose of COVID-19 vaccine (10 [52.6%] versus 10 [11.9%], p<0.001) were also associated with the occurrence of AE. In multivariate logistic regression analysis, only age (OR 0.95, 95%CI 0.91-0.99, p=0.042) and previous AE (OR 6.2, 95%CI 1.8-20.7, p=0.052) showed inverse and direct significant association with the occurrence of AE after the second dose of COVID-19 vaccine, respectively. AE were not related to either the serological response or its degree.
4. Discussion
The uncertainty initially generated about the potential negative effect of the immune dysfunction related to certain IMIDs such as RA, and/or its treatments on the immunogenicity to the SARS-CoV-2 vaccine has aroused enormous interest from the outset, and fortunately, our data on the effectiveness and safety of the COVID-19 vaccine in this population are reassuring and support its use. The seroconversion rate of our RA patients is high (88.14%) and closer to the upper range described by other authors, who report values ranging from 61.8% to 94% [21-25]. There are several possible explanations for these favorable humoral immunogenicity results in our population. Firstly, mRNA vaccines were the most frequently used in our population and this type of vaccines has been identified as the most effective both in the general population and in patients with RA, achieving higher seroconversion percentages and antibody titers, as well as greater persistence of antibody titers throughout follow-up [23,26-29]. Even boosters with heterologous mRNA vaccines in patients who had received initial treatment with adenoviral vector vaccines have been shown to improve seroconversion rates [30]. However, we did not find an association between the type of vaccine and the humoral response in our patients, probably due to the sample size and the lower representation of the rest of the types of vaccines.
Furthermore, the majority of patients (95.8%) had received the complete vaccination regimen with 2 doses of mRNA vaccines or AZD1222 adenoviral vector vaccine. Multiple studies have reported an increase in seroconversion rates, antibody levels and cellular response to COVID-19 vaccines associated with increasing number of doses of the vaccine, allowing the immune response to be sustained and broadened with successive boosters (3rd and 4th doses) [31-36].
Additionally, most of the patients were in remission or low disease activity and were not taking GC (90%), and those who received prednisone were at a low dose (average 5 mg/d), which we think may have played a beneficial role on the humoral response to the vaccine, since some authors have reported a reduction in seroconversion rates in patients receiving associated treatment with prednisone, especially at doses > 7.5 mg/d [21,22,27].
Previous SARS-CoV-2 infection revealed to be one of the main factors associated with increased immunogenicity to COVID-19 vaccine in our population, in line with data reported in literature [23,31,34,37]. A study by Saleem et al. involving 100 patients with RA reported lower seroconversion rates (55.4%) in patients without previous COVID-19 than in those previously infected (100%) [31]. The equivalent rates in our patients were 85.57% and 100%, respectively. Furthermore, age was the second most relevant factor independently and inversely associated with humoral immunogenicity, in agreement with a phase 4 prospective study including 260 patients with RA and 104 healthy controls that observed lower seroconversion rates in older individuals (OR=0.79, p<0.001) [21]. Despite the existing discrepancies in the literature on the impact of age on the humoral response to the vaccine (seroconversion and/or neutralizing antibodies), studies that describe a lower seroconversion in older people [21,23,27,25,38,39] predominate over those that do not find age-related differences [24,34].
The negative association of smoking with the humoral response found in our study is especially interesting given its known role in the pathogenesis of RA and some of its comorbidities such as interstitial lung disease, and also its link with systemic inflammation. We have not found any reference to this factor in literature.
Regarding the role of disease activity measured by DAS28 on humoral immunogenicity, we found no significant association, probably related to the fact that the majority of the patients were in remission or with low disease activity. However, other markers of inflammation, such as ESR, and of disease severity like aCCP antibodies or extra-articular manifestations were associated with a significantly lower humoral response in bivariate analysis. On the contrary, other studies have observed a significant association between the presence of aCCP antibodies and higher levels of specific anti-spike antibodies against SARS-CoV-2 [23,32]. Comorbidities did not seem to have an impact on the humoral response to vaccines as it has been described by other authors [24,40].
Especially reassuring are the high seroconversion rates achieved in our patients who were mostly on treatment with DMARDs, even in combination in 51.7% of them. Among csDMARDs, MTX seemed to have the greatest impact on immunogenicity, while all patients treated with sulfasalazine and hydroxychloroquine had adequate humoral seroconversion, and leflunomide dose was associated with higher degree of antibody titers. These data are in line with previous studies that describe a low impact on the humoral immunogenicity of non-MTX csDMARDS, unless administered as a combination treatment [21,22].
The negative effect of MTX on the humoral response to the COVID-19 vaccine has been described both for seroconversion, antibody titers, neutralizing antibodies or cellular response, even in the administration of booster doses, with a dose-dependent effect [21,22,24,31,41,42]. In order to mitigate these deleterious effects, some authors have investigated temporary MTX rest strategies in the peri-vaccine period [28,43,44]. The randomized study by Araujo et al. demonstrated greater seroconversion rates in RA patients who rested from MTX in the 2 weeks following each vaccine dose, with no significant differences in the appearance of flares at 28 days, although they were slightly higher at 69 days [43]. Along these lines, Haberman et al. described that a week of rest from MTX after the administration of a booster dose of a mRNA vaccine achieves a humoral response in patients with RA similar to that of healthy controls, suggesting that the optimal rest would be 10 days [44]. Recent data from a randomized study by Martínez-Fleta et al. support the usefulness and safety of MTX rest in patients with RA and psoriatic arthritis, with the effect of a 2-week rest being superior to that of one week [28]. It is possible that the favorable data from our patients is partly related to the fact that at least 37.8% of them rested from MTX an average of 1.5 weeks after each COVID-19 vaccine, as shown in their electronic records. It is also relevant that the average number of DMARDs used in combination in our patients was 1.5, since a greater reduction in seroconversion has been described with the greater number of DMARDs used [21,40].
Our seroconversion data in patients treated with TNF antagonists, JAK inhibitors and IL6 receptor inhibitors were also generally favorable, in accordance with those described by other authors, who did not find a relevant effect of these drugs on the humoral response, or it was only mild when used in combination, especially with MTX [21-23,27,31, 33,38,45]. The use of ABA and RTX seemed not to be a big problem in our patients either, differing from what has been published to date since both ABA and especially RTX have been associated with a negative effect on the humoral response [21-23,27,31,33,38]. In fact, RTX has been described as the main predictor of a negative immunogenicity response, with virtual abolition of antibody production [25,38,46]. Our ABA data must be evaluated with caution due to the small number of cases. In relation to RTX, a potential explanation for our results is that the time periods between the administration of RTX and the vaccine were long, being the mean time from the last dose of RTX to vaccination of 12±10.5 months (range: 0.5–36.7) and the mean time between vaccination and the administration of further RTX cycles of 5.2±1.9 months (range: 1.6–8.2), since it has been described that the probability of seroconversion increases with lower cumulative dose of RTX and longer intervals between drug administration and vaccination [47,48].
Despite the importance of the ability of COVID-19 vaccines to generate an adequate protective antibody response in patients with RA, their effectiveness in reducing the occurrence of new SARS-CoV-2 infections or their severity is probably even more relevant. We consider this to be one of the main contributions of our study, since there are few data reported to date. 18.6% of our patients had a SARS-CoV-2 infection during the 6 months of follow-up, despite the fact that 10 (45.45%) of them had received a booster dose. The most notable observations are that the majority were asymptomatic (17/22), the symptomatic ones presented mild manifestations, and none required hospital admission, unlike the pre-vaccine period in which 5% of patients with COVID-19 had suffered a serious infection.
Le Moine et al. found an incidence of COVID-19 of 8.9% six months after vaccination, and like us, without serious cases [33]. Cook et al. found a similar incidence of COVID-19 between mRNA vaccines (8.1% BNT162b2 versus 7.6% mRNA-1273) in patients with systemic autoimmune diseases [49]. Colmegna et al. found an incidence of SARS-CoV-2 infection of 14.5% 12 months after vaccination, self-reported by patients through a questionnaire [25], while Picchianti-Diamanti et al. described that 42% of the RA patients in their study presented with SARS-CoV-2 infection after an average time of 6 months since the last vaccine [50]. Although the majority were pauci-symptomatic, 8.5% required admission, with RTX being the main risk factor associated with admission [50]. In our study, the only factor associated with the incidence of COVID-19 was the presence of asthma.
An increase in the incidence of COVID-19 has been described with the passage of time since vaccination (1.3% after the first cycle to 19.2% after the administration of the 3rd dose), as well as a greater risk of infection and hospitalization than in the general population from 9 months after vaccination, which reinforces the importance of administering boosters and using other prevention strategies [51,52]. In our population, 10 (45.45%) of the patients with post-vaccine infection had received a booster vaccine dose. This could be explained by the emergence of new SARS-CoV-2 strains and the antibody titer decrease over time. In fact, a recent study evaluating the humoral immunity in 104 RA patients at 1, 3 and 6 months after receiving the full vaccination schedule concluded that it decreased significantly (p<0.01) between 1 and 3 months, with an 8.9% incidence rate of post-vaccination infection, all cases being observed between 3 and 6 months after vaccination [33].
Regarding the safety of the vaccine, we found no warning signs. Adverse events of SARS-CoV-2 vaccination in our sample occurred in around 20% of the patients, were mostly mild and showed a profile similar to that described in the general population. Other authors have reported in patients with autoimmune rheumatic diseases similar frequency and severity of AEs than healthy controls and other non-rheumatic autoimmune diseases reinforcing the safety of vaccines in patients with RA [53-55].
The percentage of AEs in our patients was generally lower than that described by other authors, whose values range between 27.7% and 86% [25,51,54,56-58]. Most authors also found that AEs were mostly mild to moderate, although 0.5% to 4.2% serious AEs have been reported [53,58]. We found that AEs were associated with RTX treatment, younger age and, for the second vaccine dose, with the occurrence of AE after the first dose. Other studies have also observed that the AE frequency is higher at younger ages and females [9,54,56,57]. In contrast to our data, that showed a similar percentage of AEs after the 1st and 2nd doses of the vaccine, the Korean College of Rheumatology argues that AEs may be more intense after the second dose [9].
We found no differences in AE between vaccine types, although some authors have reported a higher frequency of AE with mRNA vaccines [26,53], while others have described higher frequency of arthralgia with AZD1222 vaccine [56].
The second most frequent AE in our population were arthralgias, but mild RA flares occurred in only 1.7% of patients. A study comparing AE of vaccination in 1198 RA patients and 1117 hospital workers concluded that arthralgias were more frequent (3.1% vs. 0.8%, p<0.0001) and longer lasting in RA patients, with no significant change in disease activity [59]. The rate of RA flares in our patients was very low, probably because most were in remission or low activity, in agreement with studies that found an association between flares after vaccination and the disease activity [54,60]. Other authors have also found that COVID-19 vaccines were associated with 4.4%-15.7% of RA flares, and although many of them were mild and self-limiting, in other cases they were moderate-severe and required to make changes to the background treatment in 1.5-30% of cases [51,54,58-62]. We also found that RA flares were inversely related to age, in line with the study of Ma et al. [60].
Limitations
The main limitations of our study are those derived from the sample size, its retrospective design and the lack of a control group. The good control of the disease activity of our patients may be related to the favorable response to COVID-19 vaccines in our population, in terms of effectiveness and safety, and may not be extrapolated to other groups of patients with worse disease control. The retrospective design with data obtained from the electronic records of the patients does not allow us to exclude that the perivaccine adjustment rate of DMARDs could have been higher, having a greater weight in achieving an adequate humoral response to the vaccine. The periods for determining the serological response were variable, and in some cases later than a month after completing the vaccination, as it was a real-life clinical practice study, and although the analyzes were adjusted for this factor, it could have influenced the results. In any case, if the determinations had been closer in time to the administration of the vaccine, it is expected that the seroconversion would have been even greater, reinforcing the good results obtained.
5. Conclusions
Humoral immunogenicity induced by SARS-CoV-2 vaccines can be considered reasonably adequate in our RA patient population with adequate disease control, and the factors most strongly associated with a greater humoral response to vaccines were previous SARS-CoV-2 infection and younger age. Despite the incidence of COVID-19 infection after vaccination remained high, a reduction of the severity was found, without the need of hospital admissions, reinforcing the effectiveness of these vaccines, that showed a good safety profile and acceptable tolerability in our population of patients with RA. Further prospective studies with higher sample size are needed to determine the evolution of antibody titers over time and the number and frequency of doses required to achieve better protection against SARS-CoV-2 in patients with RA.
6. Patents
There are no patents resulting from the work reported in this manuscript.
Author Contributions
Conceptualization, EF.V-R., M.T-R. and S.C.; methodology, EF.V-R., M.T-R. and S.C.; software, EF.V-R.; validation, all authors; formal analysis, EF.V-R., M.T-R. and S.C.; investigation, EF.V-R., M.T-R. and S.C.; resources, EF.V-R., M.T-R. and S.C.; data curation, EF.V-R., M.T-R. and S.C.; writing—original draft preparation, EF.V-R., M.T-R. and S.C.; writing—review and editing, all authors; visualization, all authors; supervision, al authors; project administration, EF.V-R., M.T-R. and S.C.; funding acquisition, S.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research has not received financial support from any institutional or private organization. S. Castañeda is granted by Ministerio de Economía y Competitividad (Instituto de Salud Carlos III) (grant number PI21/01474) and co-funded by the European Regional Development Fund (ERDF) “A way to make Europe”.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee for Research with medicines of the Hospital Universitario de La Princesa (protocol code: ecl.4790, and date of approval: 10 March 2022).
Informed Consent Statement
Patient consent was waived due to this research is a retrospective “non-intervention” study, whose data have been used for an academic research study.
Data Availability Statement
Data is unavailable due to privacy and ethical restrictions.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results”.
Appendix A

Table A1.
Description of analyzed variables.
| Groups of variables | Type of variable | Description |
|---|---|---|
| Sociodemographic variables | Age | Years |
| Sex | Male, female | |
| Smoking | Pack-years | |
| Comorbidities | Presence Type: AHT, DM, DL, obesity, ischemic heart disease, thromboembolic disease, cardiovascular disease, stroke, peripheral arterial disease, arrhythmias, heart failure, thromboembolic disease, pulmonary thromboembolism, deep vein thrombosis, renal failure, COPD, asthma |
|
| RA characteristics | Onset date | Date |
| Diagnosis date | Date | |
| Rheumatoid factor | Presence, titer | |
| aCCP antibodies | Presence, titer | |
| Erosive RA | Yes / No | |
| Extra-articular manifestations |
Nodules, interstitial lung disease, atlanto-axial subluxation, others | |
| Disease activity and functionality | ESR, CRP, DAS28, HAQ | |
| RA treatment | Previous therapy | GC, MTX, OHCQ, SSZ, CsA, AZA, MPM, TACRO, TOFA, BARI, ANAK, ABA, RTX, TCZ, SARI, IFX, ETN, ADA, GOLI |
| Current therapy | Starting date and dosage of GC, MTX, OHCQ, SSZ, CsA, AZA, MPM, TACRO, TOFA, BARI, ANAK, ABA, RTX, TCZ, SARI, IFX, ETN, ADA and/or GOLI | |
|
Previous COVID-19 |
Diagnosis | Data, method (PCR / antigen test), place (Primary Care / Hospital Care) |
| Symptoms and complications |
Cough, fever, expectoration, nasal congestion, pneumonia, dyspnoea, desaturation, chest pain, palpitations, tachycardia, back pain, arthralgia, myalgia, arthritis, malaise, anosmia, ageusia, nausea, vomiting, diarrhoea, headache, dizziness, rash, superinfection, thrombosis, arrhythmia, renal failure | |
| Severity | Hospital admission, ICU admission | |
| Sequelae | Free text for description | |
| RA activity at diagnosis of COVID-19 |
Remission, low, moderate, severe | |
| Treatments received | Anti-inflammatory, antiviral, respiratory support, modification of usual RA treatment | |
|
COVID-19 vaccine |
Type of vaccine | AZD1222, Ad.26.COV2.s, mRNA-1237, BNT162b2 |
| Number of vaccine doses | Number of doses administered | |
| First dose | Date, AE (fever, arthralgia, myalgia, arthritis, headache, dizziness, nausea, vomiting, rash, anaphylaxis, thrombosis), severe AE | |
| Second dose | Date, AE (fever, arthralgia, myalgia, arthritis, headache, dizziness, nausea, vomiting, rash, anaphylaxis, thrombosis), severe AE | |
| Humoral response* | Post-vaccine serology (BAU/mL), serology collection date | |
|
Post-vaccine COVID-19 |
Symptoms and signs | Cough, fever, expectoration, nasal congestion, pneumonia, dyspnoea, desaturation, chest pain, palpitations, tachycardia, back pain, arthralgia, myalgia, arthritis, malaise, anosmia, ageusia, nausea, vomiting, diarrhoea, headache, dizziness, rash, superinfection, thrombosis, arrhythmia, renal failure |
| Severity | Hospital admission, ICU admission |
ABA: abatacept; aCCP: anti-cyclic citrullinated peptide antibodies; ADA: adalimumab; AE: adverse events; AHT: arterial hypertension; ANAK: anakinra; AZA: azathioprine; BARI: baricitinib; BAU: Binding Antibody Units; COPD: chronic obstructive pulmonary disease; COVID-19: Coronavirus Disease 2019; CRP: C-reactive protein; CsA: cyclosporine A; CTZ: certolizumab; DAS28: Disease Activity Score of 28 joints; DM: diabetes mellitus; DL: dyslipidemia; ESR: erythrocyte sedimentation rate; ETN: etanercept; GC: glucocorticoids; GOLI: golimumab; HAQ: Health Assessment Questionnaire; ICU: intensive care unit; IFX: infliximab; LF: leflunomide; mL: milliliter; MPM: mycophenolate mofetil; MTX: methotrexate; OHCQ: hydroxychloroquine; PCR: polymerase chain reaction; RA: rheumatoid arthritis; RTX: rituximab; SARI: sarilumab; SSZ: sulfasalazine; TC: tacrolimus; TCZ: tocilizumab; TOFA: tofacitinib. *Anti-SARS-CoV-2 IgG antibody titers (obtained with the SARS CoV-2 IgG II QUANT Alinity technique, Abbott®) were considered negative if <7.1 BAU/mL and positive if ≥7.1 BAU/mL.
References
- Seoane-Mato, D.; Sánchez-Piedra, C.; Díaz-González, F.; et al. Prevalence of rheumatic diseases in adult population in Spain. EPISER 2016 study. Ann Rheum Dis. 2018, 77, 535–536. [Google Scholar] [CrossRef]
- García de Yébenes, M.J.; Loza, E. Rheumatoid arthritis: epidemiology and socio-health impact. Clinical Rheumatology Supplements 2018, 14, 3. [Google Scholar]
- Lozano, J.A. Rheumatoid arthritis (I). Etiopathogenesis, symptomatology, diagnosis and prognosis. OFFARM, 2021; 20, 94–100. [Google Scholar]
- Brito-Zerón, P.; Sisó-Almirall, A.; Flores-Chavez, A.; et al. SARS-CoV-2 infection in patients with systemic autoimmune diseases. Clin Exp Rheumatol. 2021, 39, 676–687. [Google Scholar] [CrossRef] [PubMed]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef]
- Hasseli, R.; Mueller-Ladner, U.; Hoyer, B.F.; et al. Older age, comorbidity, glucocorticoid use and disease activity are risk factors for COVID-19 hospitalisation in patients with inflammatory rheumatic and musculoskeletal diseases. RMD Open 2021, 7, e001464. [Google Scholar] [CrossRef]
- Schulze-Koops, H.; Krueger, K.; Vallbracht, I.; et al. Increased risk for severe COVID-19 in patients with inflammatory rheumatic diseases treated with rituximab. Ann Rheum Dis. 2021, 80, e67. [Google Scholar] [CrossRef]
- Curtis, J.R.; Johnson, S.R.; Anthony, D.D.; et al. American College of Rheumatology Guidance for COVID-19 Vaccination in Patients With Rheumatic and Musculoskeletal Diseases: Version 3. Arthritis Rheumatol. 2021, 73, e60–e75. [Google Scholar] [CrossRef] [PubMed]
- Park, J.K.; Lee, E.B.; Shin, K.; et al. COVID-19 Vaccination in Patients with Autoimmune Inflammatory Rheumatic Diseases: Clinical Guidance of the Korean College of Rheumatology. J Korean Med Sci. 2021, 36, e95. [Google Scholar] [CrossRef] [PubMed]
- Alten, R.; Bingham, C.O.; Cohen, S.B.; et al. Antibody response to pneumococcal and influenza vaccination in patients with rheumatoid arthritis receiving abatacept. BMC Musculoskelet Disord. 2016, 17, 231. [Google Scholar] [CrossRef]
- Crnkic Kapetanovic, M.; Saxne, T.; Jönsson, G.; et al. Rituximab and abatacept but not tocilizumab impair antibody response to pneumococcal conjugate vaccine in patients with rheumatoid arthritis. Arthritis Res Ther. 2013, 15, R171. [Google Scholar] [CrossRef]
- Furer, V.; Rondaan, C.; Heijstek, M.W.; et al. 2019 update of EULAR recommendations for vaccination in adult patients with autoimmune inflammatory rheumatic diseases. Ann Rheum Dis. 2020, 79, 39–52. [Google Scholar] [CrossRef]
- Hua, C.; Barnetche, T.; Combe, B.; Morel, J. Effect of methotrexate, anti-tumor necrosis factor α, and rituximab on the immune response to influenza and pneumococcal vaccines in patients with rheumatoid arthritis: a systematic review and meta-analysis. Arthritis Care Res (Hoboken) 2014, 66, 1016–1026. [Google Scholar] [CrossRef] [PubMed]
- Park, J.K.; Lee, M.A.; Lee, E.Y.; et al. Effect of methotrexate discontinuation on efficacy of seasonal influenza vaccination in patients with rheumatoid arthritis: a randomised clinical trial. Ann Rheum Dis. 2017, 76, 1559–1565. [Google Scholar] [CrossRef]
- Park, J.K.; Lee, Y.J.; Shin, K.; et al. Impact of temporary methotrexate discontinuation for 2 weeks on immunogenicity of seasonal influenza vaccination in patients with rheumatoid arthritis: a randomised clinical trial. Ann Rheum Dis. 2018, 77, 898–904. [Google Scholar] [CrossRef] [PubMed]
- Grupo de Trabajo Técnico de Vacunación COVID-19, de la Ponencia de Programa y Registro de Vacunaciones. Estrategia de vacunación frente a COVID-19 en España. Ministerio de Sanidad. Available online: https://www.sanidad.gob.es/profesionales/saludPublica/prevPromocion/vacunaciones/covid19/Actualizaciones_Estrategia_Vacunacion/docs/COVID-19_EstrategiaVacunacion.pdf (accessed on 28 April 2022).
- Grupo de Trabajo Técnico de Vacunación COVID-19, de la Ponencia de Programa y Registro de Vacunaciones. Estrategia de vacunación frente a COVID-19 en España: actualización 3. Ministerio de Sanidad. Available online: https://www.sanidad.gob.es/profesionales/saludPublica/prevPromocion/vacunaciones/covid19/Actualizaciones_Estrategia_Vacunacion/docs/COVID-19_Actualizacion3_EstrategiaVacunacion.pdf (accessed on 28 April 2022).
- Curtis, J.R.; Johnson, S.R.; Anthony, D.D.; et al. American College of Rheumatology Guidance for COVID-19 Vaccination in Patients With Rheumatic and Musculoskeletal Diseases: Version 5. Arthritis Rheumatol. 2023, 75, e1–e16. [Google Scholar] [CrossRef]
- Arnett, F.C.; Edworthy, S.M.; Bloch, D.A.; et al. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 1988, 31, 315–324. [Google Scholar] [CrossRef]
- Aletaha, D.; Neogi, T.; Silman, A.J.; et al. 2010 Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Ann Rheum Dis. 2010, 69, 1580–1588. [Google Scholar] [CrossRef] [PubMed]
- Medeiros-Ribeiro, A.C.; Bonfiglioli, K.R.; Domiciano, D.S.; et al. Distinct impact of DMARD combination and monotherapy in immunogenicity of an inactivated SARS-CoV-2 vaccine in rheumatoid arthritis. Ann Rheum Dis. 2022, 81, 710–719. [Google Scholar] [CrossRef] [PubMed]
- Jena, A.; Mishra, S.; Deepak, P.; et al. Response to SARS-CoV-2 vaccination in immune mediated inflammatory diseases: Systematic review and meta-analysis. Autoimmun Rev. 2022, 21, 102927. [Google Scholar] [CrossRef]
- Nemeth, D.; Vago, H.; Tothfalusi, L.; et al. Factors influencing the SARS-CoV-2 infection and vaccination induced immune response in rheumatoid arthritis. Front Immunol. 2022, 13, 960001. [Google Scholar] [CrossRef]
- Ammitzbøll, C.; Thomsen, M.K.; Andersen, J.B.; et al. COVID-19 vaccination in patients with rheumatic diseases leads to a high seroconversion rate and reduced self-imposed isolation and shielding behaviour. Mod Rheumatol. 2023, 33, 777–785. [Google Scholar] [CrossRef]
- Colmegna, I.; Valerio, V.; Amiable, N.; et al. COVID-19 Vaccine in Immunosuppressed Adults with Autoimmune rheumatic Diseases (COVIAAD): safety, immunogenicity and antibody persistence at 12 months following Moderna Spikevax primary series. RMD Open 2023, 9, e003400. [Google Scholar] [CrossRef] [PubMed]
- Jiesisibieke, Z. L.; Liu, W. Y.; Yang, Y. P.; et al. Effectiveness and Safety of COVID-19 Vaccinations: An Umbrella Meta-Analysis. Int J Public Health 2023, 68, 1605526. [Google Scholar] [CrossRef] [PubMed]
- Le Moine, C.; Soyfoo, M.S.; Mekkaoui, L.; et al. Impaired Humoral Immunogenicity of SARS-CoV-2 Vaccination in Patients With Rheumatoid Arthritis. J Rheumatol. 2022, 49, 855–858. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Fleta, P.; Vicente-Rabaneda, E.F.; Triguero-Martínez, A.; et al. Beneficial effect of temporary methotrexate interruption on B and T cell responses upon SARS-CoV-2 vaccination in patients with rheumatoid arthritis or psoriatic arthritis. NPJ Vaccines, 2024, in press. [CrossRef] [PubMed]
- Romero-Ibarguengoitia, M.E.; Rivera-Salinas, D.; Sarti, R.; et al. Efficacy of Six Different SARS-CoV-2 Vaccines during a Six-Month Follow-Up and Five COVID-19 Waves in Brazil and Mexico. Vaccines (Basel) 2023, 11, 842. [Google Scholar] [CrossRef] [PubMed]
- Hitchon, C.A.; Mesa, C.; Bernstein, C.N.; et al. Immunogenicity and safety of mixed COVID-19 vaccine regimens in patients with immune-mediated inflammatory diseases: a single-centre prospective cohort study. BMJ Open 2023, 13, e071397. [Google Scholar] [CrossRef] [PubMed]
- Saleem, B.; Ross, R.L.; Bissell, L.A.; et al. Effectiveness of SARS-CoV-2 vaccination in patients with rheumatoid arthritis (RA) on DMARDs: as determined by antibody and T cell responses. RMD Open 2022, 8, e002050. [Google Scholar] [CrossRef] [PubMed]
- Limoges, M. A.; Lortie, A.; Demontier, É.; et al. SARS-CoV-2 mRNA vaccine-induced immune responses in rheumatoid arthritis. J Leuk Biol. 2023, 114, 358–367. [Google Scholar] [CrossRef]
- Le Moine, C.; Soyfoo, M. S.; Mekkaoui, L.; et al. Waning humoral immunity of SARS-CoV-2 vaccination in a rheumatoid arthritis cohort and the benefits of a vaccine booster dose. Clin Exp Rheumatol. 2023, 41, 82–87. [Google Scholar] [CrossRef]
- Benoit, J.M.; Breznik, J.A.; Ang, J.C.; et al. Immunomodulatory drugs have divergent effects on humoral and cellular immune responses to SARS-CoV-2 vaccination in people living with rheumatoid arthritis. Sci Rep. 2023, 13, 22846. [Google Scholar] [CrossRef] [PubMed]
- Ammitzbøll, C.; Thomsen, M.K.; Andersen, J.B.; et al. Revaccination of patients with systemic lupus erythematosus or rheumatoid arthritis without an initial COVID-19 vaccine response elicits seroconversion in half of the patients. Clin Exp Rheumatol. 2023. [CrossRef] [PubMed]
- Cheung, M.W.; Dayam, R.M.; Shapiro, J.R.; et al. Third and Fourth Vaccine Doses Broaden and Prolong Immunity to SARS-CoV-2 in Adult Patients with Immune-Mediated Inflammatory Diseases. J Immunol. 2023, 211, 351–364. [Google Scholar] [CrossRef] [PubMed]
- Zamani, B.; Moradi Hasan-Abad, A.; Piroozmand, A.; et al. Immunogenicity and safety of the BBIBP-CorV vaccine in patients with autoimmune inflammatory rheumatic diseases undergoing mmunosuppressive therapy in a monocentric cohort. Immun Inflamm Dis. 2023, 11, e858. [Google Scholar] [CrossRef] [PubMed]
- Frommert, L.M.; Arumahandi de Silva, A.N.; Zernicke, J.; et al. Type of vaccine and immunosuppressive therapy but not diagnosis critically influence antibody response after COVID-19 vaccination in patients with rheumatic disease. RMD Open 2022, 8, e002650. [Google Scholar] [CrossRef]
- Dudley, H.M.; O'Mara, M.; Auma, A.; et al. Rheumatoid arthritis and older age are associated with lower humoral and cellular immune response to primary series COVID-19 mRNA vaccine. Vaccine 2023, 41, 6112–6119. [Google Scholar] [CrossRef] [PubMed]
- Eerike, M.; Parimi, V.P. ; D M; et al. Clinical and immunological responses to COVID-19 vaccination in rheumatoid arthritis patients on disease modifying antirheumatic drugs: a cross-sectional study. J Rheum Dis. 2024 31, 15-24. [CrossRef]
- Shirata, M.; Ito, I.; Tanaka, M.; et al. Impact of methotrexate on humoral and cellular immune responses to SARS-CoV-2 mRNA vaccine in patients with rheumatoid arthritis. Clin Exp Med. 2023, 23, 4707–4720. [Google Scholar] [CrossRef] [PubMed]
- Tedeschi, S.K.; Solomon, D.H.; Chen, Y.; et al. Humoral and cellular immune responses in persons with rheumatoid arthritis after a third dose of mRNA COVID-19 vaccine. Semin Arthritis Rheum. 2023, 59, 152177. [Google Scholar] [CrossRef]
- Araujo, C.S.R.; Medeiros-Ribeiro, A.C.; Saad, C.G.S.; Bonfiglioli, K.R.; et al. Two-week methotrexate discontinuation in patients with rheumatoid arthritis vaccinated with inactivated SARS-CoV-2 vaccine: a randomised clinical trial. Ann Rheum Dis. 2022, 81, 889–897. [Google Scholar] [CrossRef]
- Habermann, E.; Gieselmann, L.; Tober-Lau, P.; et al. Pausing methotrexate prevents impairment of Omicron BA.1 and BA.2 neutralisation after COVID-19 booster vaccination. RMD Open, 2022; 8, e002639. [Google Scholar] [CrossRef]
- Serra López-Matencio, J.M.; Vicente-Rabaneda, E.F.; Alañón, E.; et al. COVID-19 Vaccination and Immunosuppressive Therapy in Immune-Mediated Inflammatory Diseases. Vaccines (Basel) 2023, 11, 1813. [Google Scholar] [CrossRef]
- Md Yusof, M.Y.; Arnold, J.; Saleem, B.; et al. Breakthrough SARS-CoV-2 infections and prediction of moderate-to-severe outcomes during rituximab therapy in patients with rheumatic and musculoskeletal diseases in the UK: a single-centre cohort study. Lancet Rheumatol. 2023, 5, e88–e98. [Google Scholar] [CrossRef] [PubMed]
- Furer, V.; Eviatar, T.; Zisman, D.; et al. Predictors of Immunogenic Response to the BNT162b2 mRNA COVID-19 Vaccination in Patients with Autoimmune Inflammatory Rheumatic Diseases Treated with Rituximab. Vaccines 2022, 10, 901. [Google Scholar] [CrossRef] [PubMed]
- van der Togt, C.J.T.; Ten Cate, D.F.; den Broeder, N.; et al. Humoral response to coronavirus disease-19 vaccines is dependent on dosage and timing of rituximab in patients with rheumatoid arthritis. Rheumatology (Oxford) 2022, 61, SI175–SI179. [Google Scholar] [CrossRef] [PubMed]
- Cook, C.E.; Patel, N.J.; Fu, X.; et al. Comparative Effectiveness of BNT162b2 and mRNA-1273 Vaccines Against COVID-19 Infection Among Patients With Systemic Autoimmune Rheumatic Diseases on Immunomodulatory Medications. J Rheumatol. 2023, 50, 697–703. [Google Scholar] [CrossRef]
- Picchianti-Diamanti, A.; Navarra, A.; Aiello, A.; et al. Older Age, a High Titre of Neutralising Antibodies and Therapy with Conventional DMARDs Are Associated with Protection from Breakthrough Infection in Rheumatoid Arthritis Patients after the Booster Dose of Anti-SARS-CoV-2 Vaccine. Vaccines (Basel) 2023, 11, 1684. [Google Scholar] [CrossRef] [PubMed]
- Picchianti Diamanti, A.; Navarra, A.; Cuzzi, G.; et al. The Third Dose of BNT162b2 COVID-19 Vaccine Does Not "Boost" Disease Flares and Adverse Events in Patients with Rheumatoid Arthritis. Biomedicines 2023, 11, 687. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Wallace, Z.S.; Sparks, J.A.; et al. Risk of COVID-19 Among Unvaccinated and Vaccinated Patients With Rheumatoid Arthritis: A General Population Study. Arthritis Care Res (Hoboken) 2023, 75, 956–966. [Google Scholar] [CrossRef]
- Naveen, R.; Parodis, I.; Joshi, M.; et al. COVID-19 vaccination in autoimmune diseases (COVAD) study: vaccine safety and tolerance in rheumatoid arthritis. Rheumatology (Oxford) 2023, 62, 2366–2376. [Google Scholar] [CrossRef]
- De Stefano, L.; Balduzzi, S.; Bogliolo, L.; et al. Reactogenicity, safety and disease flares following BNT162b2 mRNA COVID-19 vaccine in patients with chronic immune-inflammatory arthritis treated with biological and targeted synthetic disease-modifying anti-rheumatic drugs. Clin Exp Rheumatol. 2023, 41, 667–675. [Google Scholar] [CrossRef]
- Lee, J.J.Y.; Bernatsky, S.; Kwong, J.C.; et al. Safety and Health Care Use Following COVID-19 Vaccination Among Adults with Rheumatoid Arthritis: A Population-Based Self-Controlled Case Series Analysis. J Rheumatol. 2023, jrheum, 2023–0355. [Google Scholar] [CrossRef]
- Boekel, L.; Kummer, L.Y.; van Dam, K.; et al. Adverse events after first COVID-19 vaccination in patients with autoimmune diseases. Lancet Rheumatol. 2021, 3, e542–e545. [Google Scholar] [CrossRef]
- Oleszczyk, M.; Marciniak, Z.; Nessler, K.; et al. COVID-19 vaccine short-term adverse events in the real-life family practice in Krakow, Poland. Eur J Gen Pract. 2023, 29, 2147500. [Google Scholar] [CrossRef] [PubMed]
- Machado, P.M.; Lawson-Tovey, S.; Strangfeld, A.; et al. Safety of vaccination against SARS-CoV-2 in people with rheumatic and musculoskeletal diseases: results from the EULAR Coronavirus Vaccine (COVAX) physician-reported registry. Ann Rheum Dis. 2022, 81, 695–709. [Google Scholar] [CrossRef] [PubMed]
- Takatani, A.; Iwamoto, N.; Koto, S.; Aramaki, T. , Terada, K., Ueki, Y., Kawakami, A., & Eguchi, K. Impact of SARS-CoV-2 mRNA vaccine on arthritis condition in rheumatoid arthritis. Front Immunol. 2023; 14, 1256655. [Google Scholar] [CrossRef]
- Ma, M.; Santosa, A.; Fong, W.; et al. Post-mRNA vaccine flares in autoimmune inflammatory rheumatic diseases: Results from the COronavirus National Vaccine registry for ImmuNe diseases SINGapore (CONVIN-SING). J Autoimmun. 2023, 134, 102959. [Google Scholar] [CrossRef] [PubMed]
- Rider, L.G.; Parks, C.G.; Wilkerson, J.; et al. Baseline Factors Associated with Self-reported Disease Flares Following COVID-19 Vaccination among Adults with Systemic Rheumatic Disease: Results from the COVID-19 Global Rheumatology Alliance Vaccine Survey. Rheumatology (Oxford) 2022, 61, SI143–SI150. [Google Scholar] [CrossRef]
- Striani, G.; Hoxha, A.; Lorenzin, M.; et al. The impact of SARS-CoV-2 infection and vaccination on inflammatory arthritis: a cohort study. Front Immunol. 2023, 14, 1207015. [Google Scholar] [CrossRef]
Figure 1.
Comorbidities present in our population of patients with rheumatoid arthritis. COPD: chronic obstructive pulmonary disease.
Figure 1.
Comorbidities present in our population of patients with rheumatoid arthritis. COPD: chronic obstructive pulmonary disease.
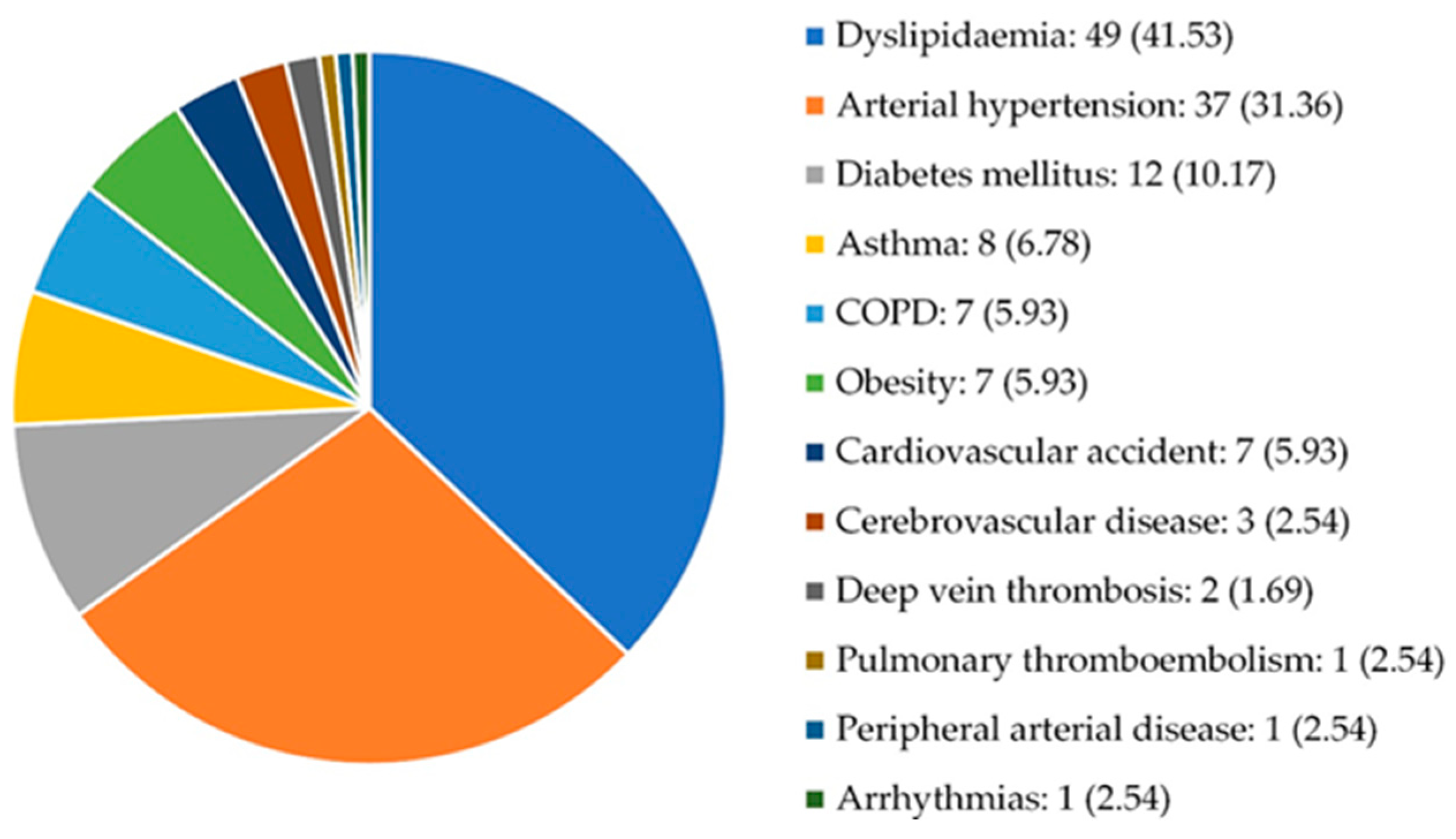
Figure 2.
Types of extra-articular manifestations. Others: Keratoconjunctivitis sicca, secondary amyloidosis and osteoporosis.
Figure 2.
Types of extra-articular manifestations. Others: Keratoconjunctivitis sicca, secondary amyloidosis and osteoporosis.
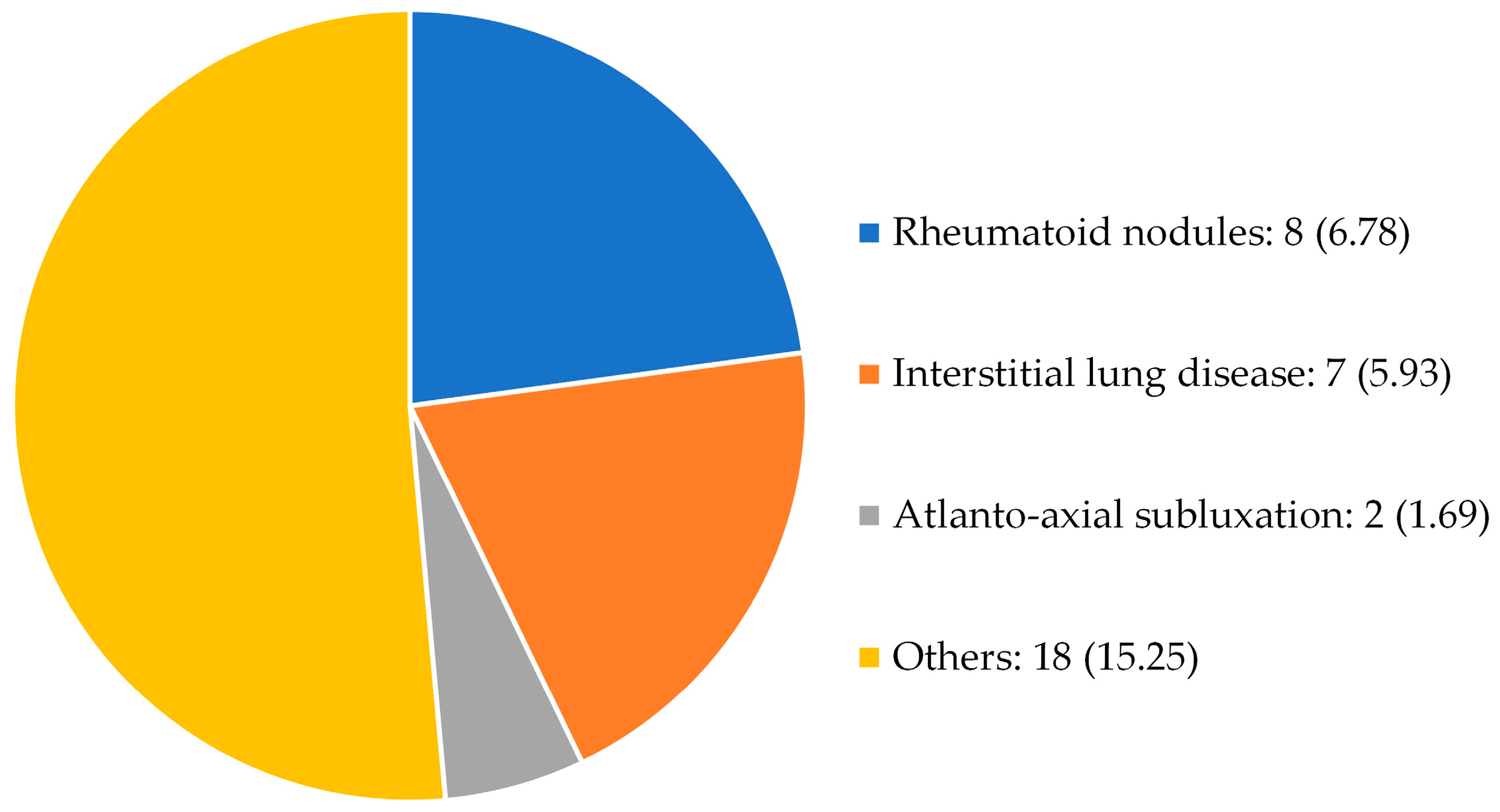
Figure 3.
Types of COVID-19 vaccines administered.
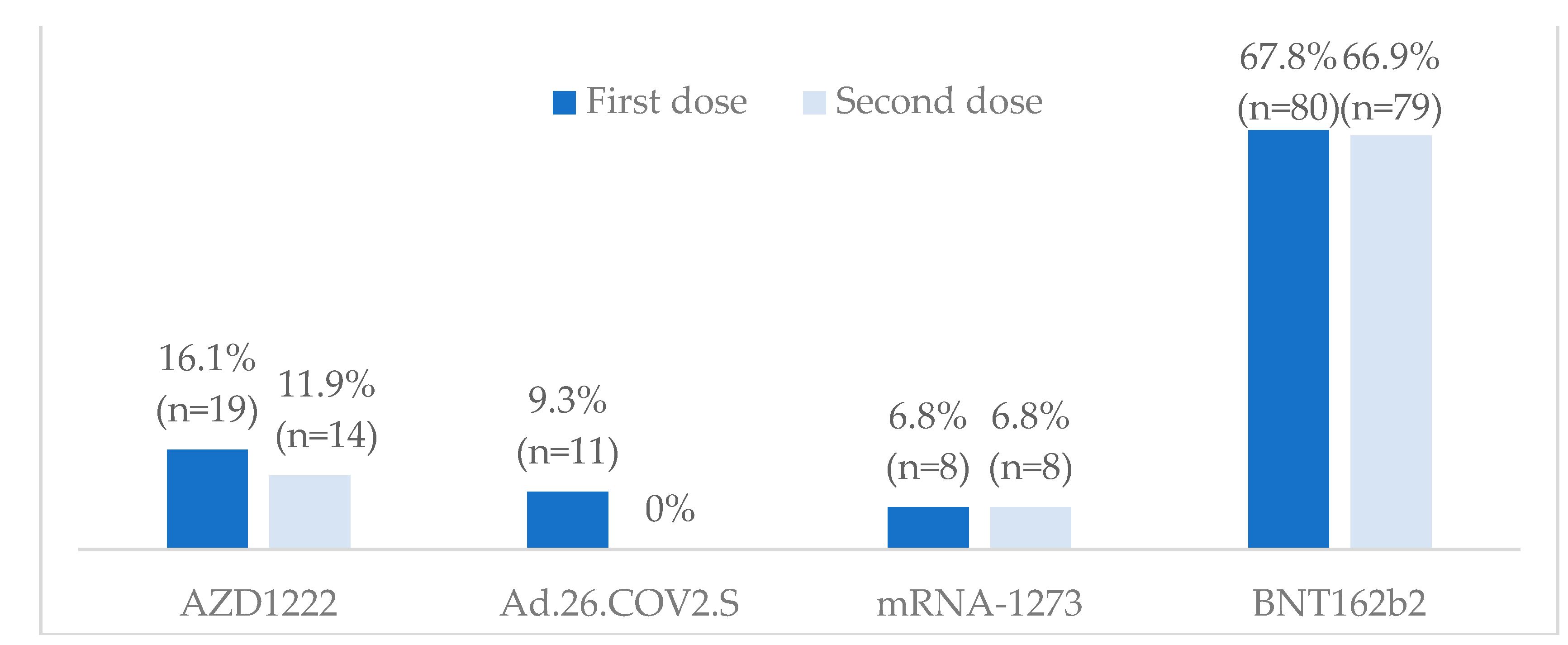
Figure 4.
Adverse events of COVID-19 vaccines in our population.
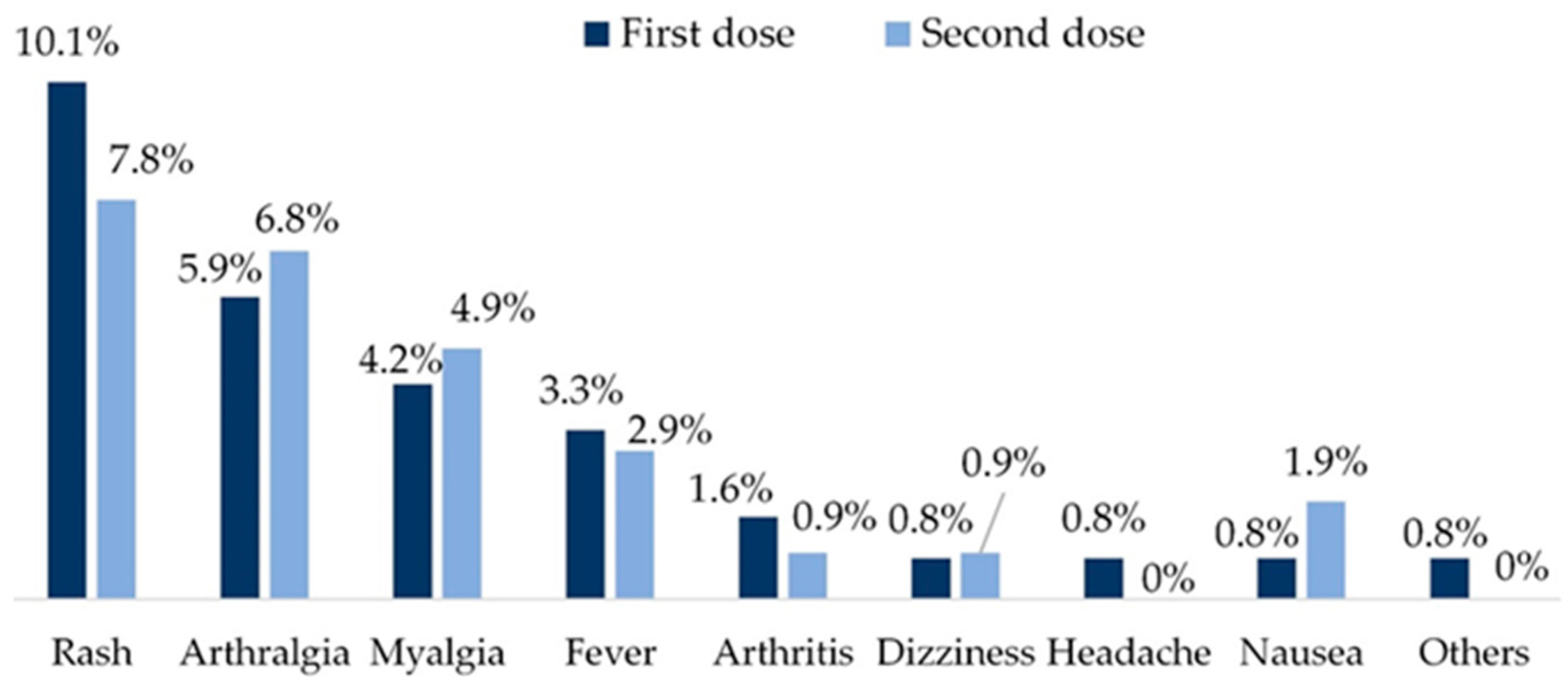
Table 1.
Characteristics and current treatments of the study population.
| Variables | Descriptive analysis | |
|---|---|---|
| Age (years) | 65.47±11.69 | |
| Sex (female) | 103 (87.29) | |
| Smoking (pack-years) | 8.79±18.55 | |
| Comorbidities | 68 (57.63) | |
| RA evolution | 12.08±9.63 | |
| RA onset | 53.04±13.64 | |
| Rheumatoid factor (positive) | 79 (66.95) | |
| - Titer | 111.49±269.16 | |
| aCCP antibodies (positive) | 63 (53.39) | |
| - Titer | 201.53±255.74 | |
| Erosive RA | 32 (27.11) | |
| Extra-articular manifestations | 26 (22.03) | |
| ESR (mm/h) | 19.88±18.64 | |
| CRP (mg/dl) | 0.51±0.78 | |
| HAQ | 0.575±0.660 | |
| DAS28 | 2.39±1.07 | |
| Previous COVID-19 | 21 (17.8) | |
| Severe previous COVID-19* | 6 (5.08) | |
| Glucocorticoids | 11 (9.32) | |
| - Dose (mg/d) | 5.34±2.24 | |
| Methotrexate | 99 (83.89) | |
| - Dose (mg/w) | 13.18±4.55 | |
| Hydroxycloroquine | 6 (5.08) | |
| Sulfasalazine | 3 (2.54) | |
| Leflunomide | 20 (16.94) | |
| - Dose (mg/d) | 15.75±4.94 | |
| Tofacitinib | 2 (1.69) | |
| Baricitinib | 3 (2.54) | |
| Abatacept sc | 2 (1.69) | |
| Rituximab iv | 19 (16.10) | |
| Tocilizumab sc or iv | 2 (1.69) | |
| Sarilumab sc | 3 (2.54) | |
| Infliximab iv | 1 (0.85) | |
| Etarnecept sc | 14 (11.86) | |
| Adalimumab sc | 4 (3.39) | |
| Certolizumab sc | 4 (3.39) | |
| Golimumab sc | 1 (0.85) |
aCCP: anti-cyclic citrullinated peptide antibodies; COVID-19: Coronavirus Disease 2019; CRP: C-reactive protein; DAS28: Disease Activity Score of 28 joints; d: day; dl: deciliter; ESR: erythrocyte sedimentation rate; g: gram; h: hour; HAQ: Health Assessment Questionnaire; iv: intravenous; mg: milligram; RA: rheumatoid arthritis; sc: subcutaneous; w: week. Numerical variables are expressed as mean ± standard deviation and qualitative variables as number (percentage). *Severe previous COVID-19 was considered when hospital admission was required.
Table 2.
Serological response to the COVID-19 vaccine.
| Serological response | |||
|---|---|---|---|
| Variables | YES | NO | p |
| Age (years) | 65.25±11.67 | 67.14±12.10 | 0.233 |
| Sex (female) | 92 (88.46) | 11 (78.57) | 0.385 |
| Smoking (pack-years) | 6.87±15.23 | 23.01±31.83 | <0.001 |
| Comorbidities | 58 (55.77) | 10 (71.43) | 0.389 |
| RA evolution | 11.57±8.59 | 15.93±15.28 | 0.994 |
| RA onset | 53.50±13.06 | 49.61±17.58 | 0.319 |
| Rheumatoid factor (positive) | 72 (69.23) | 7 (50.00) | 0.151 |
| - Titer | 117.61±282.15 | 66.07±136.97 | 0.999 |
| aCCP antibodies (positive) | 52 (82.54) | 52 (94.55) | 0.051 |
| - Titer | 196.34±252.54 | 240.07±285.45 | 0.005 |
| Erosive RA | 26 (25.00) | 6 (42.86) | 0.158 |
| Extra-articular manifestations | 20 (19.23) | 6 (42.86) | 0.045 |
| ESR (mm/h) | 20.00±19.04 | 19.00±15.94 | 0.855 |
| CRP (mg/dl) | 0.47±0.64 | 0.82±1.44 | 0.239 |
| HAQ | 0.59±0.67 | 0.43±0.59 | 0.810 |
| DAS28 | 2.37±1.12 | 2.53±0.60 | 0.110 |
| Previous COVID-19 | 22 (20.19) | 0 (0) | 0.072 |
| Severe previous COVID-19* | 6 (5.77) | 0 (0) | 0.460 |
| Glucocorticoids | 8 (7.69) | 3 (21.43) | 0.124 |
| Methotrexate | 88 (84.62) | 11 (78.57) | 0.444 |
| Hydroxycloroquine | 6 (5.77) | 0 (0) | 0.356 |
| Sulfasalazine | 3 (2.88) | 0 (0) | 1.000 |
| Leflunomide | 17 (16.35) | 3 (21.43) | 0.704 |
| Rituximab | 2 (1.92) | 0 (0) | 0.463 |
| Etarnecept | 3 (2.88) | 0 (0) | 0.215 |
| Adalimumab | 2 (1.92) | 0 (0) | 1.000 |
aCCP: anti-cyclic citrullinated peptide antibodies; COVID-19: Coronavirus Disease 2019; CRP: C-reactive protein; DAS28: Disease Activity Score of 28 joints; d: day; dl: deciliter; ESR: erythrocyte sedimentation rate; g: gram; h: hour; HAQ: Health Assessment Questionnaire; iv: intravenous; mg: milligram; RA: rheumatoid arthritis; sc: subcutaneous; w: week. Numerical variables are expressed as mean ± standard deviation and qualitative variables as number (percentage).*Severe previous COVID-19 was considered when hospital admission was required.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



