
Submitted:
03 January 2024
Posted:
04 January 2024
You are already at the latest version
Abstract
Candidiasis is one of the global public health problems. In fluconazole resistant Candida spp. (FRCS), mutations in ergosterol biosynthesis gene 11 (ERG 11) have been commonly found. This study aimed to determine the profile of FRCS isolates and to detect mutations in part of ERG 11 gene in fluconazole resistant Candida albicans (FRCA) isolates. Study was conducted on 150 isolates of FRCS obtained from patients admitted in a tertiary care hospital, South India from September 2019 to December 2021. Candida spp. was identified by MALDI-TOF MS and fluconazole resistance was detected by VITEK 2 system. Following which a part of the ERG 11 gene of the FRCA isolates were amplified, purified, sequenced and a phylogenetic tree was constructed. Out of the 150 FRCS, the most common FRCS was C. auris followed by C. glabrata, C. krusei, C. parapsilosis, C. albicans, C. tropicalis and C. guilliermondii. Sequencing of amplicons detected a single missense mutation and 44 silent mutations. We opined that fluconazole resistance in FRCA isolates may be due to mecha-nisms other than the studied one in our region. Phylogenetic analysis of amplified sequences of 12 FRCA isolates observed three clusters and all 12 sequences showed relatedness to Malaysian 2019 isolates.
Keywords:
Candida albicans
; ERG 11
; fluconazole resistant
; matrix-assisted laser desorption/ionization-time of flight mass spectrometry
; MALDI TOF
; VITEK 2
1. Introduction
Candida is a yeast like fungi present as normal flora of skin, mucosa and various internal organs. They commonly reside in oral cavity, throat, gut and vagina without causing any clinical problems. But they are responsible for variety of opportunistic infections when the host’s defense mechanism is compromised. Opportunistic candidiasis is ranging from skin and mucosal infection to invasive and allergic manifestations in humans. Currently, candidiasis is one of the globally found common infections that of growing medical concern. According to a large study conducted in 2013 with more than 1800 clinical fungal isolates from 31 countries, it was reported that 82% of which was caused by Candida spp. [1]. Globally invasive candidiasis is one of the commonest opportunistic infection with high rate of morbidity and mortality. It accounts for more than 250,000 cases and a mortality of more than 50,000 people worldwide. According to a multicentre study in five tertiary care teaching hospitals in Italy and Spain during 2008 to 2010, 995 cases have been reported. Here the overall incidence was 1.55 cases in 1000 admissions [2]. In India, the occurrence is 6-18%, among which Candida tropicalis is the predominant causative agent of invasive candidiasis [3]. In most of the regions, incidence rates is either stable or increasing. But in some regions, the disease is controlled by proper patient management, hygienic practices and nutritional improvement among infants [4].
In most of the cases, invasive candidiasis is associated with prolonged ICU stay, granulocytopenia, abdominal surgery, necrotizing pancreatitis, haematological malignancies, tumors, solid organ transplantation, preterm and malnourished infants, haemodialysis, cancer chemotherapy and other prolonged antimicrobial therapy, extremes of age, diabetes, total parenteral nutrition and presence of central vascular catheters [5]. Invasive candidiasis includes both candidemia and deep-seated tissue candidiasis. The most common type is candidemia. Candidemia in humans is caused by more than 15 different Candida species. The most common among them are Candida albicans, Candida tropicalis, Candida parapsilosis, Candida glabrata, Candida krusei and Candida auris. Haematogenous dissemination or direct inoculation of Candida species to a sterile region, such as the peritoneal cavity, causes deep-seated candidiasis [6].
Distribution of C. albicans and other non-albicans Candida (NAC) species varies greatly according to the geographical area, underlying medical conditions of patients, antifungal agents received and other conditions in hospital and patient’s immune status. C. albicans was found to be the most frequently isolated pathogen in Northern and Central Europe and the United States, while NAC species were found to predominate in Asia, Southern Europe, and South America, according to a recent systematic review that evaluated the geographical distribution of Candida species in blood samples from inpatients in various parts of the world [5,7]. Shift of Candida species from commensal flora to pathogenic agent is a result from interplay between host’s immune system and fungal virulence. Clinically invasive candidiasis ranging from asymptomatic to deep-seated candidiasis with more than 70% mortality rate. Deep seated candidiasis includes intra-abdominal abscess, peritonitis, osteomyelitis etc. [8].
Candida species can resist host’s defense mechanism by expressing several virulence factors including adhesins and invasins, hydrolytic enzymes, toxins and pseudohyphal formation. Expression of these virulence factors may vary according to different species, geographical origin, type of infection and susceptibility to the host. The resistant mechanisms are different such as expression of adhesins and invasins, thigmotropism, biofilm formation, secretion of hydrolytic enzymes such as hemolysins, aspartyl protease and serine proteases and phenotypic switching mechanism. In addition to that adaptation to fluctuations in environmental pH and temperature, metabolic flexibility, powerful nutrient acquisition system, and stress response mechanism are also added to their pathogenesis [9].
Even though candidiasis is a global infection, currently the treatment options are limited to only four antifungal drug families, which are azoles, polyenes, echinocandins and pyrimidine analogues [5]. Candidiasis is a curable condition with accurate diagnosis and management of patients. The clinical practice guidelines for management of candidiasis is released by the Infectious Disease Society of America (IDSA) in 2016. Generally, for oral and mucocutaneous candidiasis topical application of azole creams like cotrimoxazole, miconazole, ketoconazole and econazole are recommended. In addition, itraconazole solution for topical application may be used. While for systemic infections, echinocandins or intravenous administration of amphotericin B are used. Some azole drugs like ketoconazole, fluconazole and itraconazole can be given orally [10].
Resistance to various azole drugs to different species of Candida are emerging nowadays. Hence, antifungal susceptibility testing (AFST) is crucial in providing targeted therapy. Antifungal resistance can be either clinical or microbiological. Clinical resistance refers to the persistence of a fungal infection even after the complete course of treatment and microbiological resistance is the in vitro resistance towards some particular drugs compared to the other isolates of the same species. Microbiological resistance can be investigated and can be determined. Furthermore, microbiological resistance may be either intrinsic or acquired. Intrinsic resistance occur naturally without any prior exposure to drugs. In contrast, acquired resistance develops either after repeated exposure to an antimicrobial drug or due to altered gene expressions due to mutation [11]. Among the four groups of anticandidal drugs resistance to azole group of drugs are more common. Resistance to polyene group of drugs like amphotericin B is less commonly reported [12].
Azoles generally inhibit enzymes like lanosterol 14α-demethylase, which is involved in final stage of ergosterol synthesis resulting in accumulation of sterol precursors that leads to cell membrane instability and impaired fungal growth. Azole resistance in Candida species is evolved due to the combination of various mechanisms [13]. It includes decrease in the intracellular concentration of the drug due to expression of ATP-binding cassette (ABC) or major facilitator superfamily (MFS) transporters, mutation in drug target like mutation in ERG 11 gene and increased production of lanosterol 14α-demethylase due to multiple factors like gene duplication, mutation in promoter gene or mutation in gene encoding for the target enzyme [14]. CDR1 and CDR2 are two important transporters responsible for azole resistance in Candida spp. [15]. Deletion of both alleles in CDR1, over expression of either CDR1 or CDR2 or both, fungal homologues of CDR1 and CDR2 such as CgCDR1, CgCDR2, CgSNQ2 in C. glabrata, CdCDR1 and CdCDR2 in C. dubliniensis and ABC1 in C. krusei are some of the mechanisms described for resistance [14]. MFS transporters are involved in the transport of molecules by means of a proton gradient mechanism in the plasma membrane [16]. Ninety-five MFS transporters has been identified in C. albicans among which only the product of multidrug resistance 1 gene (MDR1) is associated with clinical azole resistance [15]. Expression of transcription factor multidrug-resistance regulator 1 (MRR1), inactivation of MRR1 in clinical C. albicans strains blocked MDR1 expression, gain-of-function mutations in MRR1 causing constitutive up-regulation of MDR1 are some of the mechanism involved in MDR1 expression [14].
Increased production of ergosterol by over expression of ERG 11 gene have also found to be one of the mechanism in azole resistance predominantly in C. albicans. ERG 11 overexpression is linked to mainly two mechanisms in C. albicans: (i) an increase in the expression of the transcription factor Upc2, which controls the expression of the majority of genes involved in biosynthesis of ergosterol and (ii) production of an isochromosome with two copies of left arm of chromosome 5, which contains the ERG 11 gene, or the chromosome is duplicated in its entirety [13]. In C. dubliniensis, C. glabrata, C. krusei, C. parapsilosis, and C. tropicalis, there has also been a link between enhanced ERG 11 expression and azole resistance [17].
Changes in target site of enzyme resulted by mutations are the frequently encountered mechanism in azole resistance. Therefore, most of the study were conducted to determine mutation in ERG 11 gene and in C. albicans isolates. Here ergosterol synthesis of the yeasts get impaired due to mutation in ERG 11 gene by changing the structure of lanosterol 14α- demethylase which result in decreased affinity of this molecule to azoles [14,15]. There are more than 140 amino acid substitutions reported in C. albicans. Some of those substitutions resulting only in azole resistance are K143R, S405F, G464S, I471T and R467K [18]. Other than C. albicans, mutation in ERG 11 gene have also been reported in C. dubliniensis, C. tropicalis, C. krusei, C. kefyr and C. parapsilosis isolates [14]. Currently, many clinical isolates with reduced fluconazole susceptibilities carry mutations in ERG 11 gene. In a study conducted by Stephanie A et al, among the 63 isolates that were determined to be resistant to fluconazole, 55 carried a mutation in ERG 11 that led to at least one amino acid substitution [19]. Fluconazole resistant Candida species (FRCS) are responsible for 44,800 infections and 2,200 deaths in the United States, according to a 2019 report by the Centres for Disease Control and Prevention (CDC) [20]. C. albicans was the most common causative agent in the study.
There is a challenge in successful treatment if the infection is caused by the azole resistant isolates. Therefore, determining the local epidemiology of the resistant isolates and understanding the mechanism of resistance will help in better treatment and management of patients. There are limited studies available in India for detection of mutation in ERG 11 gene in fluconazole resistant Candida albicans (FRCA) isolates. Therefore, this study was aimed to determine the profile of FRCS isolates and to detect the mutation in ERG 11 gene in FRCA isolates obtained from patients admitted in a tertiary care hospital, South India.
2. Materials and Methods
2.1. Inclusion criteria
A cross-sectional study was conducted from April to December 2021 in the Mycology section of the Department of Microbiology, Jawaharlal Institute of Postgraduate Medical Education & Research (JIPMER), Puducherry, India. All non-duplicate 150 FRCS isolates which were stocked and available in the Mycology section, which were collected from the patients admitted in JIPMER from September 2019 to December 2021 were included in the study.
2.2. Ethics
The study was conducted after getting approval from Institute Ethics Committee (IEC) - Project no. JIP/IEC/2021/068 with waiver of consent.
2.3. Clinicodemographic details
Clinicodemographic details including age, gender, ward, sample, diabetic status and HIV status of the patient from whom FRCS was isolated, were collected from the laboratory register or hospital information system (HIS) and recorded.
2.4. Identification of Candida species by MALDI-TOF MS
All the 150 FRCS isolates were revived by subculturing onto sabouraud dextrose agar (SDA). Matrix-Assisted Laser Desorption/Ionization Time-of-Flight Mass Spectrometry - MALDI-TOF MS (VITEK ® MS, Biomerieux, France) was used for the identification of FRCS isolates revived on SDA as per the manufacturer’s instruction.
2.5. Detection of fluconazole susceptibility by VITEK 2 system
Fluconazole susceptibility of the all FRCS isolates were confirmed by VITEK 2 (VITEK® 2, BIOMERIEUX, USA) automated system by using YS08 (VITEK® 2 AST- YS08, 2881896403) as per the manufacturer’s instruction.
2.6. DNA Extraction and amplification of the FRCA isolates
DNA extraction of the FRCA isolates were performed by QIAamp DNA Mini kit (Qiagen - 51304, Hilden, Germany). Following which PCR was performed for each FRCA isolates as per the method described by Xu et al [21], and optimized in our laboratory. There are three primer sets which amplify whole length of ERG 11 gene. However, we could optimize amplification from one primer set - ERGSec3A (5’ -AGGTGGTG ATTTGAATGATTTGACTT-3’) and ERGSec3B (5’ -GAACTATA ATCAGGGTCAGGCA CTTT-3’) targeting for an expected PCR product extending from 1067 to 1576 bp of the ERG 11 gene. There was a limited financial support, which restricts us for amplifying PCR products from the other two primer sets. Optimization was done with thirty- three cycles of amplification were done with a total reaction volume of 25 µl. Total duration of PCR was 2 hours and 26 minutes.
2.7. Quality control
A positive clinical FRCA strain was used as positive control and nuclease free water was used as negative control.
2.8. Gel electrophoresis and documentation
Gel electrophoresis was performed using gel electrophoretic equipment -BIO-RAD, PowerPacTM –HV, USA. Amplification products of ERG 11 gene were observed using gel documentation system - BIO-RAD, Gel Doc XR System, USA. Amplicon product sizes were recorded and compared with 100 bp DNA ladder. FRCA isolates which showed 510 bp band in gel electrophoresis were considered successful amplification of the part of ERG 11 gene.
2.9. Detection of mutation in ERG 11 gene
The ERG 11 gene products were purified and subjected for sanger sequencing with an ABI PRISM DNA analyzer (Applied Biosystems) and mutation were detected by using Mega (version 7) software by comparing with the published GenBank sequence AF153844.1 of Candida albicans strain ATCC 28516.
2.10. Phylogenetic tree
Phylogenetic tree was constructed by using published GenBank sequences from five different continents. Forty nucleic acid sequences from Asia including twelve sequences from this study, 10 sequences each from Africa, Australia and Europe, seven sequences from South America and one sequence of Candida albicans ATCC 28516 were used for the phylogenetic tree construction. The evolutionary history was inferred using the Neighbor-Joining method [22]. The bootstrap consensus tree inferred from 1000 replicates were taken to represent the evolutionary history of the taxa analyzed [23]. Branches corresponding to partitions reproduced in less than 50% bootstrap replicates were collapsed.
2.11. Statistics
Categorical variables like gender, ward, sample, diabetic status, Human Immunodeficiency virus (HIV) status, presence of ERG 11 gene, and mutation in ERG 11 gene were expressed in percentage. Continuous variable like age was expressed as mean with standard deviation.
3. Results
3.1. Clinicodemographic details
A total of 150 FRCS isolates were included in the study and were collected from the Mycology section of Department of Microbiology, Jawaharlal Institute of Postgraduate Medical Education and Research, Puducherry, India from September 2019 to December 2021. Among these 150 isolates, 78 (52%) isolates were recovered from male patients and 72 (48%) isolates were recovered from female patients. Samples were collected from new-born babies to adults upto 80 years. Predominant age group of candidiasis patients was 21-30 years with a mean age of 35.5 years and standard deviation of 18.6 years. (Figure 1).
Candidemia was the most common presentation and more than 50% isolates were recovered from blood sample. Distribution of different samples from which the FRCS were isolated, is shown in Figure 2 and the location of patients is illustrated in Figure 3. Most of the patients were from medicine wards. All except six patients were investigated for diabetes and ninety-two patients (61.3%) yielded fluconazole resistant candidiasis were found diabetic. All patients were investigated for HIV status but none were found positive for HIV.
3.2. Identification of FRCS isolates by MALDI-TOF MS
All FRCS isolates were revived on SDA medium and were identified by MALDI-TOF MS. 88.7% cases were identified as non-albicans fluconazole resistant candidiasis and only 11.3% (17/150) isolates were identified as C. albicans. Among the non-albicans candidiasis cases C. auris (40%) was the predominant isolate. Species wise distribution of fluconazole resistant candidiasis is illustrated in Figure 4.
3.3. Amplification of FRCA ERG 11 gene
All the FRCA were subjected to nucleic acid extraction and amplification. There were a total of 17 FRCA - nine isolates were obtained from genital swabs, five from blood and a single isolate each from perianal swab, ear swab and sputum. Twelve (70.6%) out of 17 FRCA isolates yielded 510 bp region in ERG 11 gene. Gel electrophoresis image of PCR products of ERG 11 gene is depicted in Figure 5.
3.4. Clinicodemographic details of 12 patients from whom FRCA ERG 11 gene amplified
Clinicodemographic details of the 12 patients from whom FRCA ERG 11 gene amplified is depicted in Table 1.
3.5. Mutations in ERG 11 gene of FRCA isolates
Sequencing of these products and comparison with GenBank sequence AF153844.1 of Candida albicans strain ATCC 28516, detected mutations and is depicted in Table 2.
All twelve sequences have been deposited in GenBank under the accession numbers OP324744.1 to OP324755.1. It showed a single missense mutation G1309A (V437I) in one FRCA isolate and 44 silent mutations. Most of the FRCA isolates had an average of four silent mutations (observed in six isolates) and a single isolate had six silent mutations. One of the FRCA isolate didn’t have any mutation. Eight different silent mutations were observed among FRCA isolates - T1296C 10 (83.3%), C1203T 8 (66.7%), A1440G 8 (66.7%), C1302T 6 (50%), T1470C 6 (50%), T1140C 3 (25%), T1110C 2 (16.7%), and T1284C 1 (8.3%).
3.6. Phylogenetic tree
A phylogenetic tree was constructed by using 65 published GenBank sequences of ERG 11 gene from five different continents – Asia, Africa, Australia, Europe and South America; and 12 sequences from this study. GenBank sequence accession number AF153844.1 ATCC 28516 C. albicans was considered as reference sequence. Phylogenetic tree is illustrated in Figure 6. Twelve isolates studied here are arranged in three clusters – first cluster of 7 isolates which are closely related to MN537022.1MALAYSIA2019, second cluster of 3 isolates which are closely related to MN537023.1MALAYSIA2019 and third cluster of 2 isolates which are closely related to MN537021.1MALAYSIA2019. One of the 12 isolates OP324751 also showed closeness to one Japan sequence AB071959.1JAPAN2001.
4. Discussion
Candidiasis is a growing medical problem. Candidemia is the most serious clinical presentation among candidiasis. A limited study is available which describes incidence or prevalence of candidemia involving multiple hospitals and especially in India. In South Asia, prevalence of candidemia were observed ranging from 0.16 to 4.53 cases per 1000 hospital discharges and 11.7 cases per 1000 ICU discharges [24]. Invasive candidiasis includes candidemia as well as subcutaneous and deep-seated tissue candidiasis. The important causative agents are Candida albicans, Candida tropicalis, Candida parapsilosis, Candida glabrata, Candida krusei and Candida auris. Fluconazole is the most common antifungal drug used in the treatment of candidiasis. Indiscriminate use of fluconazole results in increase in the FRCS isolates. CDC observed 7% Candida spp. isolates were resistant to fluconazole during 2012 to 2016 and C. albicans was the most common causative agent [20]. Mutation in the ERG 11 gene of C. albicans is considered for the fluconazole resistance and therefore mutation in the ERG 11 gene of C. albicans isolates were studied most. Molecular mechanism were not studied much in India. Therefore, here the study was conducted on FRCS isolates and the mutation in a part of ERG 11 gene of FRCA isolates. A total of 150 FRCS isolates were available in the Mycology section of Department of Microbiology, Jawaharlal Institute of Postgraduate Medical Education and Research, Puducherry, India from September 2019 to December 2021 and were included in the study. Isolates were received from both male and female patients almost in an equal proportion. It indicates that FRCS causes infection equally to both genders. FRCS isolates were recovered from patients from newborn infants to elderly up to 80 years with a predominant age group between 21 years to 30 years. Very few studies were encountered on FRCS. A similar study conducted in Iran by Sardari et al observed 23% FRCA isolates were isolated from the patients with age group of 31 to 40 followed by 20% from 21 to 30 [25]. Both the studies showed that candidiasis caused by fluconazole resistant isolates commonly affect adult and earning population. It needs further evaluation to prevent it.
Candidemia was the predominant form of candidiasis (64.7%) followed by vaginal candidiasis (18%) in this study. Similar finding was observed by Chakrabarti et al in 2014. He reviewed candidemia as the most prevalent clinical condition in hospitalized patients with a higher mortality rate. He also identified abdominal candidiasis as one of the common form of candidiasis in South India whereas we identified only 2% gastro intestinal candidiasis in our study [24]. Earlier study from our Institute observed 27.3 % cases of vulvovaginal candidiasis during 2017 [26]. Vijaya et al identified 17.7% cases of vaginal candidiasis in 2014 [27]. Most of the isolates were recovered from samples received from Medicine department i.e., 48 out of 150 (32%) followed by Obstetrics and Gynaecology, Paediatrics, Surgery, Surgical gastroenterology, Orthopaedics, Nephrology, Pulmonary Medicine, Skin and STD, Clinical Immunology department, Neurology, ENT and Oncology departments. According to a prospective multicentric study conducted in Spain between 2011 and 2016, 204 (55.3%) were from medical wards, while 165 (44.7%) of the 369 cases admitted in a hospital were from surgical wards [28]. The most common presentation of candidiasis is candidemia who are admitted in medical speciality and the same was observed in this study.
Candidiasis is linked to a number of comorbid illnesses, including diabetes, HIV/AIDS, indwelling catheters, and antibiotic overuse. Here, 92 (61.3%) patients were diabetic and was the most common predisposing factor. India has now become a diabetic hub and therefore diabetes is the commonest risk factor for the development of candidal infection. Goswami et al. found a statistically significant difference in the isolation rate of various Candida spp. in diabetic patients (46%) compared to control subjects (23%) [29]. Even though candidiasis is a prevalent opportunistic illness in HIV patients, none of the isolates in our investigation was from HIV patients. Khan et al. did a prospective study on AIDS patients and found that, out of a total 165 HIV-positive individuals, 80 were diagnosed with candidiasis [30]. It may be due to active antiretroviral therapy provided by the government hospitals to HIV infected persons which prevents candidal infection in our region.
All 150 FRCS isolates were identified by MALDI-TOF MS. C. auris was the predominant species isolated in this study. Forty percentage (60/150) isolates were of C. auris followed by 16% (24/150) C. glabrata, 12.7% (19/150) C. krusei, 12% (18/150) C. parapsilosis, 11.3% (17/150) C. albicans, 6.7% (10/150) C. tropicalis and 1.3% (2/150) C. guilliermondii. According to a retrospective study of six years from China, the most common Candida species identified was C. albicans (46.3%), followed by C. parapsilosis (19.5%), C. glabrata (15.9%), and C. tropicalis (14.6%). Few isolates were found resistant to fluconazole and maximum number were observed in C. parapsilosis, followed by C. tropicalis and C. glabrata. None of the C. albicans isolates were resistant to fluconazole [31}. Whereas, there is a shift towards non-albicans candidemia in India and here C. tropicalis is the most common causative agent of candidemia. Tak et al in his study identified C. tropicalis (39%) as the commonest isolate followed by C. parapsilosis (18-20%), C. albicans (12-14%) and C. glabrata (11-12%) [32]. It is found that fluconazole resistance in C. albicans is rare in the United States, affecting just 0.5–2% of cases. Conversely, C. parapsilosis, C. tropicalis, and C. glabrata had greater rates, ranging from 4-9%, 2-6%, and 11-13%, respectively [33,34]. In contrast to these resistance patterns the newly emerging Candida species, C. auris have shown a higher resistance rate of 93% [35]. C. krusei have shown intrinsic resistance to fluconazole [36]. Similarly in another recent USA study describing that the least resistant species to fluconazole is C. tropicalis (2.3%), followed by C. parapsilosis (3.4%), C. albicans (3.5%) and C. glabrata (7.8%) [37]. Rise of antimicrobial resistance is considered a global public health problem. Therefore, Indian Council of Medical Research (ICMR) is monitoring antimicrobial resistance in India through a network of diagnostic laboratories. According to the ICMR annual report 2022 January to 2022 December, antifungal susceptibility profiling showed that 93% isolates of C. albicans and C. tropicalis were fluconazole susceptible, although C. utilis, C. parapsilosis, and C. glabrata showed diminishing susceptibility rates (77%–85%). C. auris had lowest susceptibility percentages to fluconazole [38]. According to a recent study in India during 2020, 67% of candidemia detected from Corona virus disease patients were caused by C. auris. Several other major outbreaks of candidemia also been reported from various parts of world like Columbia, South Africa, United Kingdom and United States [39,40,41]. C. auris is resistant to fluconazole, amphotericin B, and echinocandins and therefore it is unique and are multi-drug resistant [42].
Molecular characterization of FRCA ERG 11 gene were done in this study to detect mutations in the gene. Out of 17 isolates, only 12 (70.6%) isolates of FRCA had amplified a part of ERG 11 gene in this study. It may be postulated that five FRCA isolates may have mutations at the primers site and therefore they may not had amplified. Sequencing of these amplified products detected a single missense mutation G1309A (V437I) in one FRCA isolate and eight different silent mutations were observed. Here most of the FRCA isolates had an average of four silent mutations (observed in six isolates) and a single isolate had six silent mutations. Eight different silent mutations were observed among FRCA isolates - T1296C 10 (83.3%), C1203T 8 (66.7%), A1440G 8 (66.7%), C1302T 6 (50%), T1470C 6 (50%), T1140C 3 (25%), T1110C 2 (16.7%), and T1284C 1 (8.3%) in this study. Fluconazole resistance in C. albicans was said to be due to mutation in ERG 11 gene in other similar studies but limited in number. Sardari et al studied 216 clinical Candida isolates including 100 FRCA isolates and identified sixteen different nucleic acid substitutions. Among which only two showed amino acid substitutions - E266D and V488I [25]. In an another study conducted by Paul et al in Chennai, all the fluconazole resistant Candida isolates showed mutation in ERG 11 gene including two extensive mutations. They found many non-sense mutations and missense mutations like Y18D, D23Y, V28L, G36D, Y41N, F49L, R53P, M63R, E243D etc. and they concluded that these mutations are contributing to fluconazole resistance [43]. Mane et al in India observed 6 amino acid substitutions in FRCA isolates including E116D, F145L, E226D, I437V, P406L and Q474H. But they concluded that azole resistance was primarily due to CDR1 mediated mechanisms [44]. Xiang et al, found 17 aminoacid substitutions in ERG 11 gene including seven novel mutations such as K143Q, Y205E, A255V, E260V, N435V, G472R, and D502. They observed V437I (G1309A) mutation which was also identified in this study. But they observed this mutation in both fluconazole resistant and susceptible isolates, suggesting that there is no association of this mutation with fluconazole resistance [45]. We observed less number of mutations in FRCA isolates. It may be due to less number of FRCA isolates studied and we could only amplify a part of ERG 11 gene - from 1067 to 1576 bp part of the 1587 bp of ERG 11 gene. Mutation may be present in other part of ERG 11 gene and five of FRCA isolates failed to amplify. Even though there were many limitations in this study, but we are having opinion that resistant in FRCA isolates are primarily due to some other mechanism other than mutations in ERG 11 gene as suggested by Mane et al [44].
A phylogenetic tree was constructed combining 12 sequences of this study with a reference sequence of AF153844.1 ATCC 28516 C. albicans and 65 published sequences in GenBank from five different continents - Asia, Africa, Australia, Europe and South America. We observed that our isolates arranged in three clusters (Figure 6). Interestingly, all twelve isolates and the three clusters showed relatedness to Malaysian 2019 isolates. Here all twelve isolates were recovered from 12 different patients, from different sites and at different time frame - from 2019 to 2021. We don’t have travel history of these 12 patients to Malayasia, as this is primarily a retrospective study. But it can be concluded that FRCA isolates circulating in our region might have ancestral source in Malayasia. Further study is required to identify the mode and source of transmission of FRCA isolates. It will help us to implement appropriate preventive measures.
5. Conclusions
C. auris was the most common fluconazole resistant isolate observed, followed by C. glabrata, C. krusei, C. parapsilosis, C. albicans, C. tropicalis and C. guilliermondii. Only 12 out of 17 FRCA isolates amplified a part of ERG 11 gene. There were many silent mutations observed in ERG 11 gene of FRCA isolates and detected only a single missense mutation -V437I. We opined that fluconazole resistance in C. albicans may be due to other mechanisms – other than mutations in ERG 11 gene in our region. All twelve FRCA isolates showed relatedness to Malaysian 2019 isolates indicating that FRCA isolates circulating in our region might have ancestral source in Malayasia.
Author Contributions
Conceptualization, Rakesh Singh (R.S.).; Methodology, R.S. and Sheena M S. (S.MS.); Resources, R.S.; Investigation and data collection, S.MS.; Validation, R.S.; formal analysis, S.MS. and R.S.; Writing—original draft preparation, S.MS.; Writing—review and editing, R.S..; Visualization, S.MS.; Supervision, R.S.; Project administration, R.S.; Funding acquisition, R.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Jawaharlal Institute of Postgraduate Medical Education & Research (JIPMER) intramural research grant. Puducherry, India.
Institutional Review Board Statement
Study was approved by JIPMER Institutional Ethics Committee (IEC) – Project No.: JIP/EC/2021/068 with waiver of consent.
Informed Consent Statement
Patient consent was waived by JIPMER Institutional Ethics Committee (IEC).
Data Availability Statement
The data underlying this article will be shared on request to the corresponding author.
Acknowledgments
The authors would like to thank JIPMER for providing financial support for the study.
Conflicts of Interest
The Authors declare that they have no conflicts of interest regarding the publication of the present study.
References
- Castanheira M, Messer SA, Rhomberg PR, Pfaller MA. Antifungal susceptibility patterns of a global collection of fungal isolates: results of the SENTRY Antifungal Surveillance Program (2013). Diagn Microbiol Infect Dis 2016, 85, 200-204. [CrossRef]
- Bassetti M, Merelli M, Righi E, Diaz-Martin A, Rosello EM, Luzzati R, Parra A, Trecarichi EM, Sanguinetti M, Posteraro B, Garnacho-Montero J. Epidemiology, species distribution, antifungal susceptibility, and outcome of candidemia across five sites in Italy and Spain. J Clin Microbiol 2013, 51, 4167-4172. [CrossRef]
- Kothari A, Sagar V. Epidemiology of Candida bloodstream infections in a tertiary care institute in India. Indian J Med Microbiol 2009, 27, 171–172. [CrossRef]
- Cleveland AA, Harrison LH, Farley MM, Hollick R, Stein B, Chiller TM, et al. Declining Incidence of Candidemia and the Shifting Epidemiology of Candida Resistance in Two US Metropolitan Areas, 2008–2013: Results from Population-Based Surveillance. PLoS ONE 2015, 10, e0120452. [CrossRef]
- Odds FC, Brown AJ, Gow NA. Antifungal agents: mechanisms of action. Trends Microbiol 2003, 11, 272-9. [CrossRef]
- Zeng Z rui, Tian G, Ding Y huan, Yang K, Liu J bo, Deng J. Surveillance study of the prevalence, species distribution, antifungal susceptibility, risk factors and mortality of invasive candidiasis in a tertiary teaching hospital in Southwest China. BMC Infect Dis 2019, 19, 939. [CrossRef]
- Sanguinetti M, Posteraro B, Lass-Flörl C. Antifungal drug resistance among Candida species: mechanisms and clinical impact. Mycoses 2015, 58, 2–13. [CrossRef]
- Pappas PG, Lionakis MS, Arendrup MC, Ostrosky-Zeichner L, Kullberg BJ. Invasive candidiasis. Nat Re Dis Primers 2018, 4, 1-20. [CrossRef]
- Mayer FL, Wilson D, Hube B. Candida albicans pathogenicity mechanisms. Virulence 2013, 4, 119–128. [CrossRef]
- Pappas PG, Kauffman CA, Andes DR, Clancy CJ, Marr KA, Ostrosky-Zeichner L, et al. Clinical Practice Guideline for the Management of Candidiasis. Clin Infect Dis Off Publ Infect Dis Soc Am 2016, 62, 1–50. [CrossRef]
- Kanafani ZA, Perfect JR. Resistance to Antifungal Agents: Mechanisms and Clinical Impact. Clin Infect Dis 2008, 46, 120–128. [CrossRef]
- Tortorano AM, Rigoni AL, Biraghi E, Prigitano A, Viviani MA. The European Confederation of Medical Mycology ECMM) survey of candidaemia in Italy: antifungal susceptibility patterns of 261 non-albicans Candida isolates from blood. J Antimicrob Chemother 2003, 52, 679-682. [CrossRef]
- Cowen LE, Sanglard D, Howard SJ, Rogers PD, Perlin DS. Mechanisms of Antifungal Drug Resistance. Cold Spring Harb Perspect Med 2015, 5, a019752. [CrossRef]
- Gonçalves SS, Souza ACR, Chowdhary A, Meis JF, Colombo AL. Epidemiology and molecular mechanisms of antifungal resistance in Candida and Aspergillus. Mycoses 2016, 59, 198–219. [CrossRef]
- Das I, Nightingale P, Patel M, Jumaa P. Epidemiology, clinical characteristics, and outcome of candidemia: experience in a tertiary referral center in the UK. Int J Infect Dis 2011, 15, 759-763. [CrossRef]
- Sanglard D, Coste A, Ferrari S. Antifungal drug resistance mechanisms in fungal pathogens from the perspective of transcriptional gene regulation. FEMS Yeast Res 2009, 9, 1029-1050. [CrossRef]
- Redding SW, Kirkpatrick WR, Coco BJ, Sadkowski L, Fothergill AW, Rinaldi MG, et al. Candida glabrata Oropharyngeal Candidiasis in Patients Receiving Radiation Treatment for Head and Neck Cancer. J Clin Microbiol 2002, 40, 1879–1881. [CrossRef]
- Morio F, Loge C, Besse B, Hennequin C, Le Pape P. Screening for amino acid substitutions in the Candida albicans ERG 11 protein of azole-susceptible and azole-resistant clinical isolates: new substitutions and a review of the literature. Diag Microbiol Infect Dis 2010, 66, 373-384. [CrossRef]
- Flowers SA, Colón B, Whaley SG, Schuler MA, Rogers PD. Contribution of Clinically Derived Mutations in ERG 11 to Azole Resistance in Candida albicans. Antimicrob Agents Chemother 2015, 59, 450–460. [CrossRef]
- Toda M, Williams SR, Berkow EL, et al. Population-Based Active Surveillance for Culture-Confirmed Candidemia — Four Sites, United States, 2012–2016. MMWR Surveill Summ 2019, 68, 1–15. [CrossRef]
- Xu Y, Chen L, Li C. Susceptibility of clinical isolates of Candida species to fluconazole and detection of Candida albicans ERG 11 mutations. J Antimicrob Chemother 2008, 61, 798–804. [CrossRef]
- Saitou N and Nei M. The Neighbour joining method: A new method for reconstructing phylogenetic trees. Mol Biol and Evol 1987, 4, 406-425. [CrossRef]
- Felsenstein J. Confidence limits on phylogenies: an approach using the bootstrap. Evol 1985, 39, 783-791. [CrossRef]
- Singh R, Chakrabarti A. Invasive candidiasis in the Southeast-Asian region. In Candida albicans. Cell Mol Biol 2017, 25-40. [CrossRef]
- Sardari A, Zarrinfar H, Mohammadi R. Detection of ERG 11 point mutations in Iranian fluconazole-resistant Candida albicans isolates. Curr Med Mycol 2019, 5, 7–14. [CrossRef]
- Kalaiarasan K, Singh R, Chaturvedula L. Fungal Profile of Vulvovaginal Candidiasis in a Tertiary Care Hospital. J Clin Diagn Res JCDR 2017, 11, DC06–9. [CrossRef]
- Vijaya D, Dhanalakshmi TA, Kulkarni S. Changing trends of vulvovaginal candidiasis. J Lab Physicians 2014, 6, 28-30. [CrossRef]
- Knitsch W, Vincent JL, Utzolino S, François B, Dinya T, Dimopoulos G, et al. A Randomized, Placebo-controlled Trial of Preemptive Antifungal Therapy for the Prevention of Invasive Candidiasis Following Gastrointestinal Surgery for Intra-abdominal Infections. Clin Infect Dis 2015, 61, 1671–1678. [CrossRef]
- Willis AM, Coulter WA, Fulton CR, Hayes JR, Bell PM, Lamey PJ. Oral Candida l carriage and infection in insulin-treated diabetic patients. Diabet Med 1999 16 , 675-679. [CrossRef]
- Anwar KP, Malik A, Subhan KH. Profile of candidiasis in HIV infected patients. Iran J Microbiol 2012, 4, 204–209.
- Xiao Z, Wang Q, Zhu F, An Y. Epidemiology, species distribution, antifungal susceptibility and mortality risk factors of candidemia among critically ill patients: a retrospective study from 2011 to 2017 in a teaching hospital in China. Antimicrob Resist Infect Control 2019, 8, 89. [CrossRef]
- Tak V, Mathur P, Varghese P, Gunjiyal J, Xess I, Misra MC. The Epidemiological Profile of Candidemia at an Indian Trauma Care Center. J Lab Physicians 2014, 6, 96–101. [CrossRef]
- Cleveland AA, Farley MM, Harrison LH, Stein B, Hollick R, Lockhart SR, Magill SS, Derado G, Park BJ, Chiller TM. Changes in incidence and antifungal drug resistance in candidemia: results from population-based laboratory surveillance in Atlanta and Baltimore, 2008–2011. Clin infect dis 2012, 55, 1352-1361. [CrossRef]
- Pfaller MA, Rhomberg PR, Messer SA, Jones RN, Castanheira M. Isavuconazole, micafungin, and 8 comparator antifungal agents’ susceptibility profiles for common and uncommon opportunistic fungi collected in 2013: temporal analysis of antifungal drug resistance using CLSI species-specific clinical breakpoints and proposed epidemiological cutoff values. Diagn Microbiol Infect Dis 2015, 82, 303–313. [CrossRef]
- Lockhart SR, Etienne KA, Vallabhaneni S, et al. Simultaneous emergence of multidrug-resistant Candida auris on 3 continents confirmed by whole-genome sequencing and epidemiological analyses. Clin Infect Dis 2017, 64, 134–140. [CrossRef]
- Marichal P, Gorrens J, Coene MC, Le Jeune L, Vanden Bossche H. Origin of differences in susceptibility of Candida krusei to azole antifungal agents. Mycoses 1995, 38, 111–117. [CrossRef]
- Whaley SG, Berkow EL, Rybak JM, Nishimoto AT, Barker KS, Rogers PD. Azole antifungal resistance in Candida albicans and emerging non-albicans Candida species. Front microbiol 2017, 7, 2173. [CrossRef]
- ICMR Annual Report 2022. Annual Report Antimicrobial Resistance Research and Surveillance Network. Available online: https://main.icmr.nic.in/sites/default/files/guidelines/AMRSN_Annual_Report_2022.pdf (Accessed on 27th October 2022).
- Cortegiani A, Misseri G, Fasciana T, Giammanco A, Giarratano A, Chowdhary A. Epidemiology, clinical characteristics, resistance, and treatment of infections by Candida auris. J Intensive Care 2018, 6, 69. [CrossRef]
- Adams E, Quinn M, Tsay S, Poirot E, Chaturvedi S, Southwick K, et al. Candida auris in Healthcare Facilities, New York, USA, 2013–2017. Emerg Infect Dis 2018, 24, 1816–1824. [CrossRef]
- Arensman K, Miller JL, Chiang A, Mai N, Levato J, LaChance E, et al. Clinical Outcomes of Patients Treated for Candida auris Infections in a Multisite Health System, Illinois, USA. Emerg Infect Dis 2020, 26, 876–880. [CrossRef]
- Chowdhary A, Sharma C, Meis JF. Candida auris: A rapidly emerging cause of hospital-acquired multidrug-resistant fungal infections globally. PLOS Pathog 2017, 13, e1006290. [CrossRef]
- Paul S, Kannan I, Mohanram K. Extensive ERG 11 mutations associated with fluconazole-resistant Candida albicans isolated from HIV-infected patients. Curr Med Mycol 2019, 5, 1–6. [CrossRef]
- Mane A, Vidhate P, Kusro C, Waman V, Saxena V, Kulkarni-Kale U, et al. Molecular mechanisms associated with Fluconazole resistance in clinical Candida albicans isolates from India. Mycoses 2016, 59, 93–100. [CrossRef]
- Xiang MJ, Liu JY, Ni PH, Wang S, Shi C, Wei B, et al. ERG 11 mutations associated with azole resistance in clinical isolates of Candida Candida. FEMS Yeast Res 2013, 13, 386–393. [CrossRef]
Figure 1.
Age wise (in years) distribution of patients yielded fluconazole resistant Candida spp. (FRCS).
Figure 1.
Age wise (in years) distribution of patients yielded fluconazole resistant Candida spp. (FRCS).
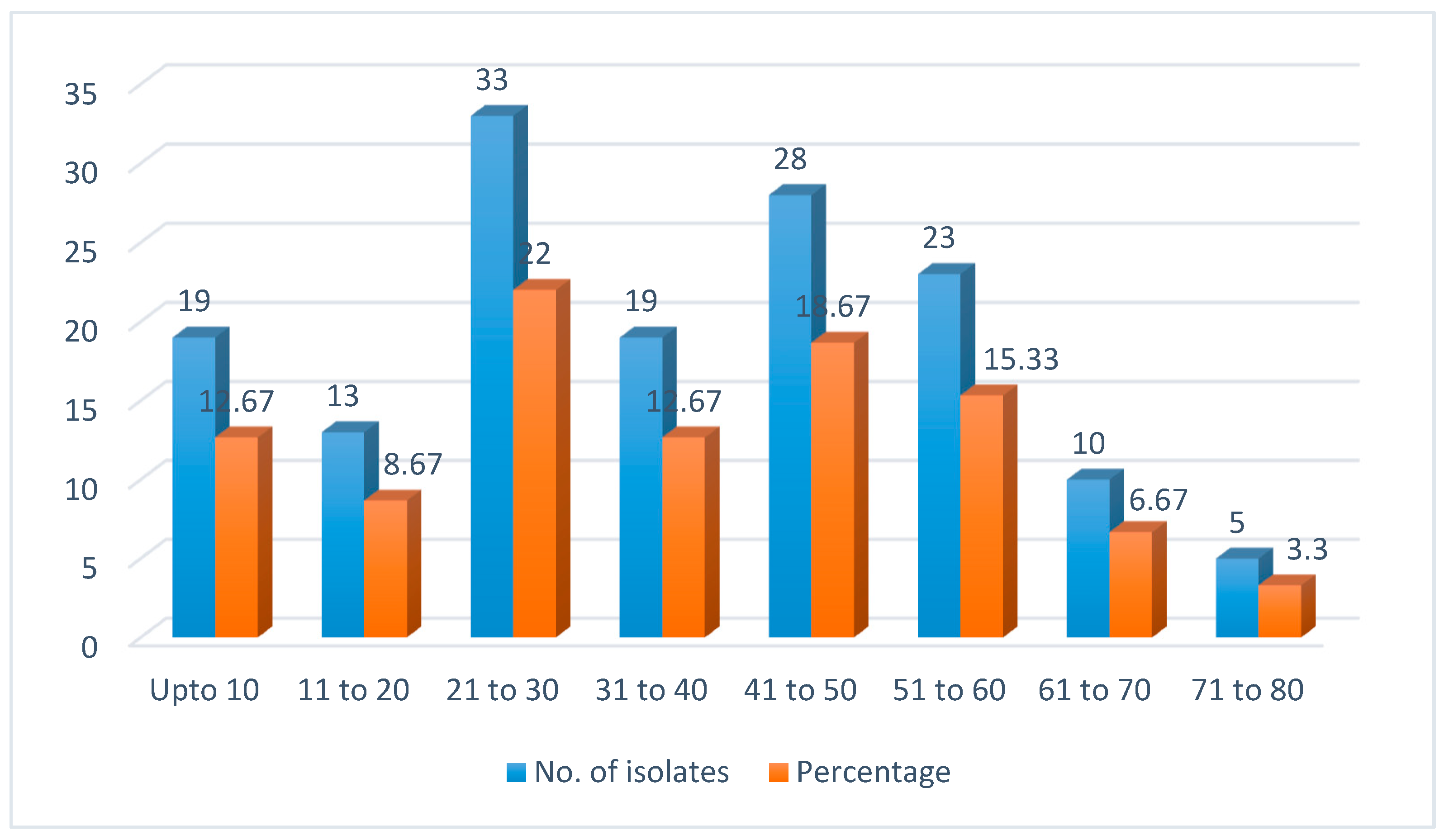
Figure 2.
Specimen wise distribution which yielded fluconazole resistant Candida spp. (FRCS) isolates.
Figure 2.
Specimen wise distribution which yielded fluconazole resistant Candida spp. (FRCS) isolates.
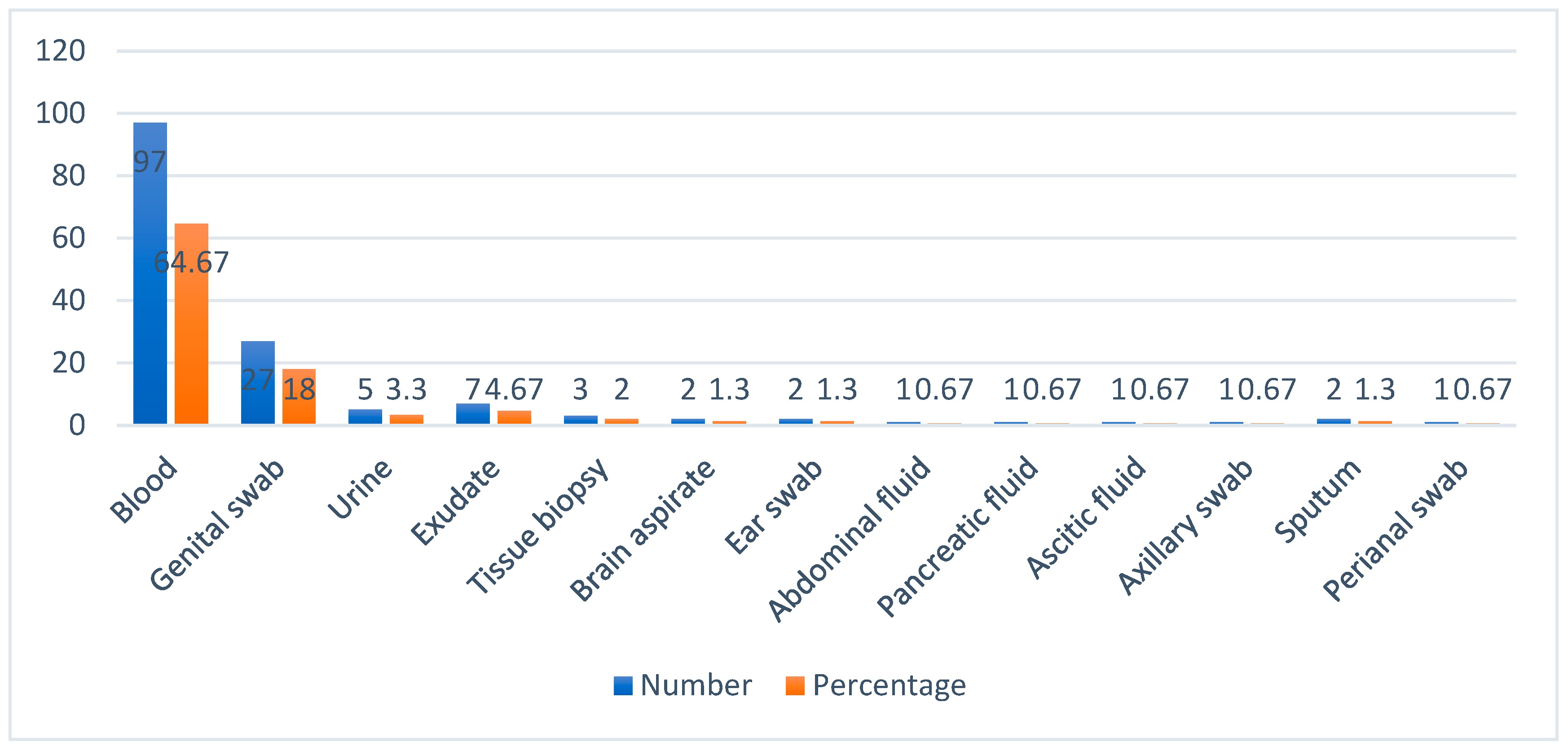
Figure 3.
Service wise distribution of patients yielded fluconazole resistant Candida spp. (FRCS).
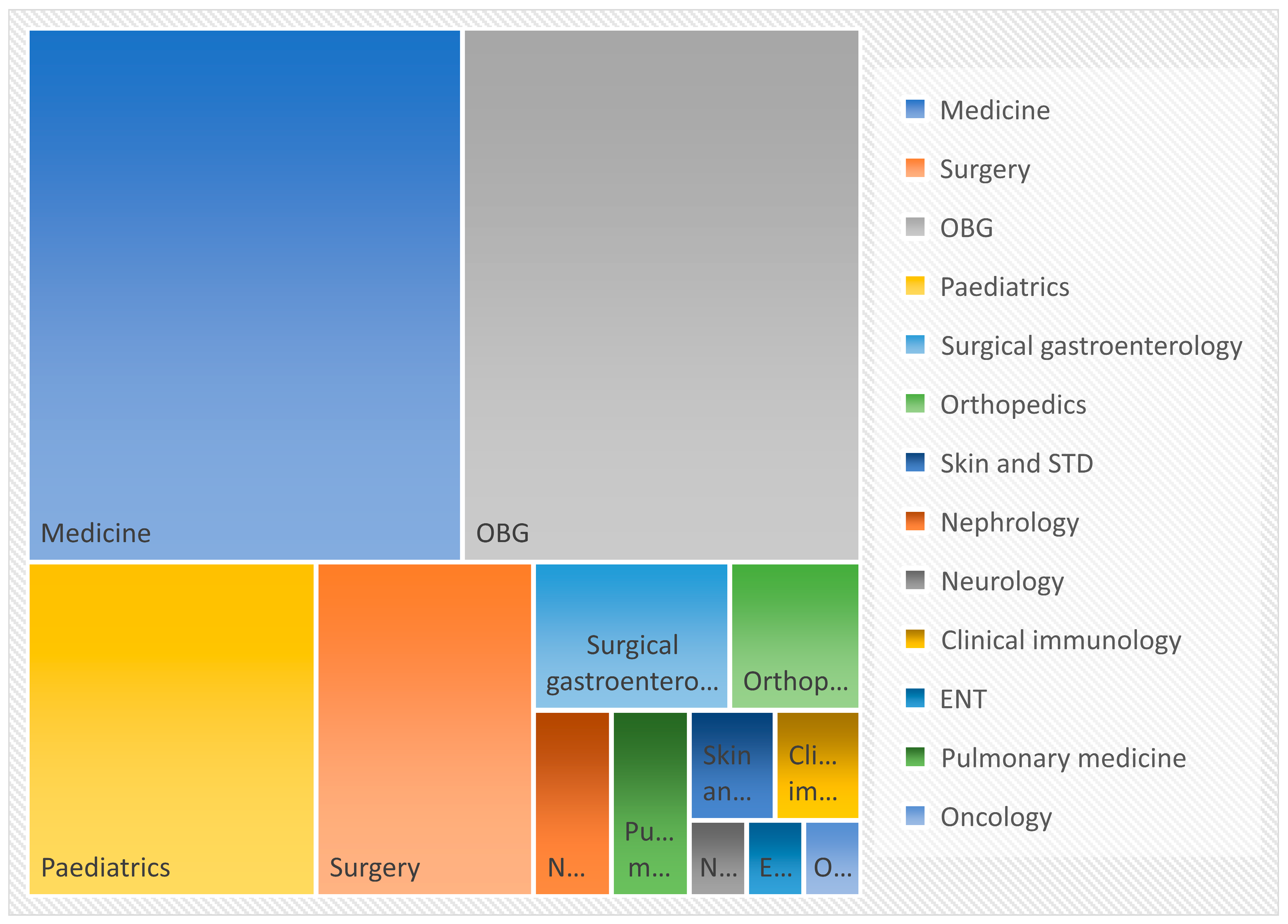
Figure 4.
Species wise distribution of fluconazole resistant Candida spp. (FRCS) isolates.
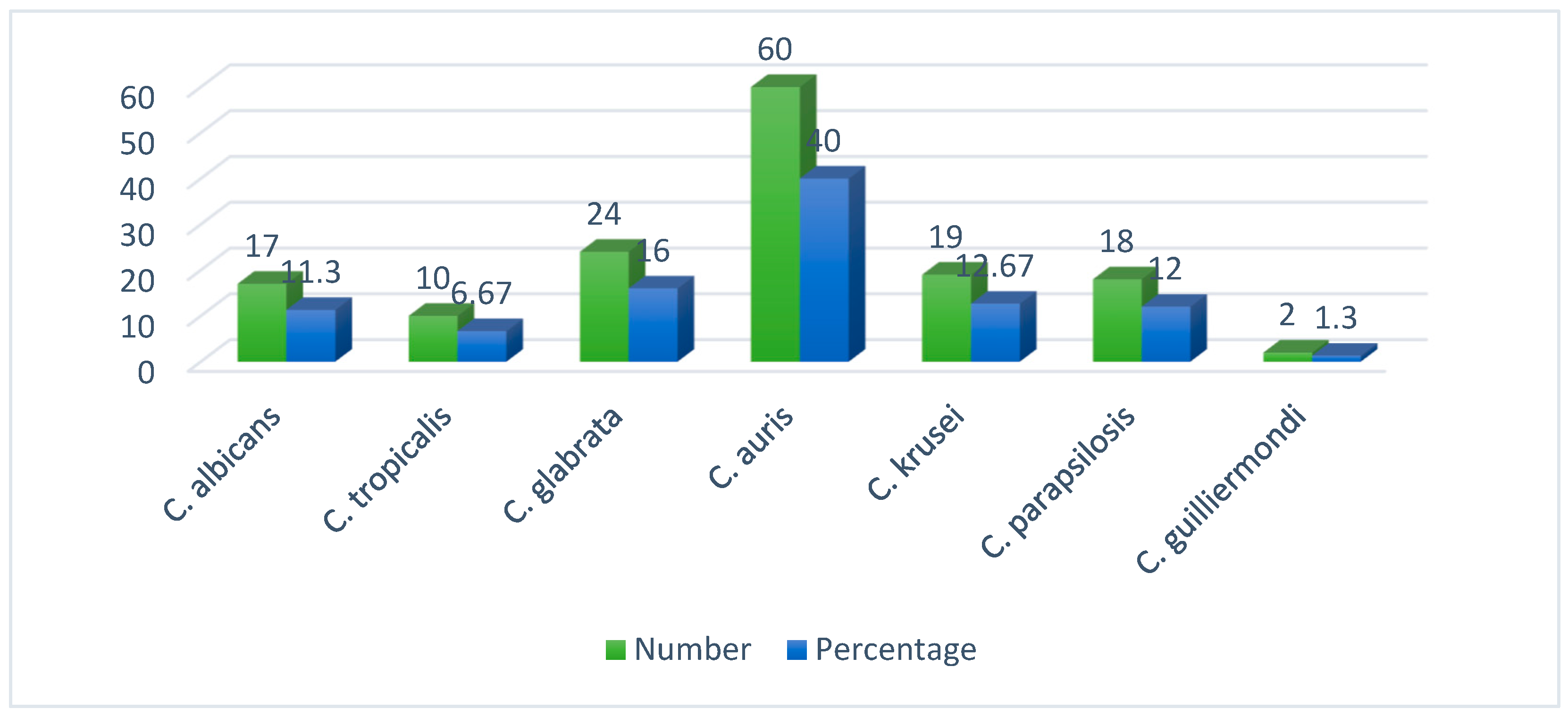
Figure 5.
Gel electrophoresis image of PCR products of ERG 11 gene.
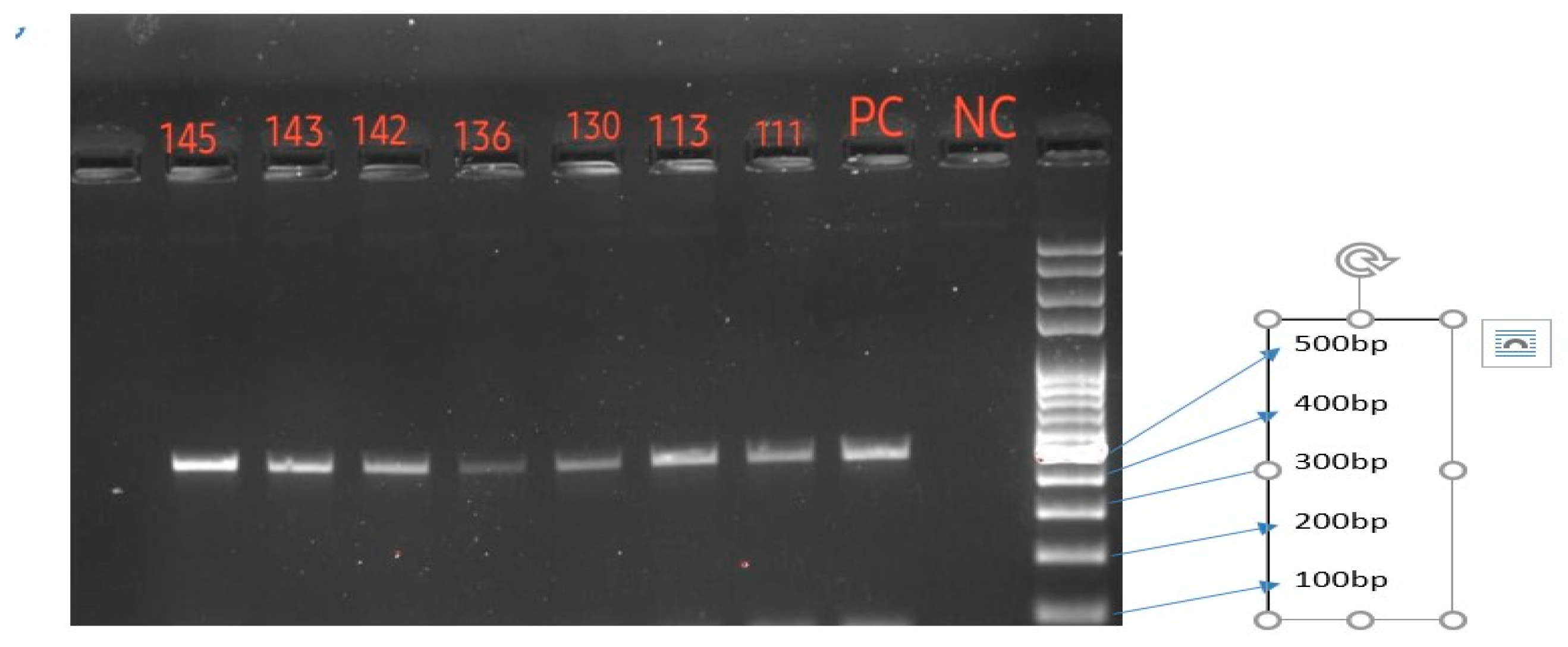
Figure 6.
Phylogenetic tree based on part of ERG 11 gene. Twelve isolates of this study showed three clusters.
Figure 6.
Phylogenetic tree based on part of ERG 11 gene. Twelve isolates of this study showed three clusters.
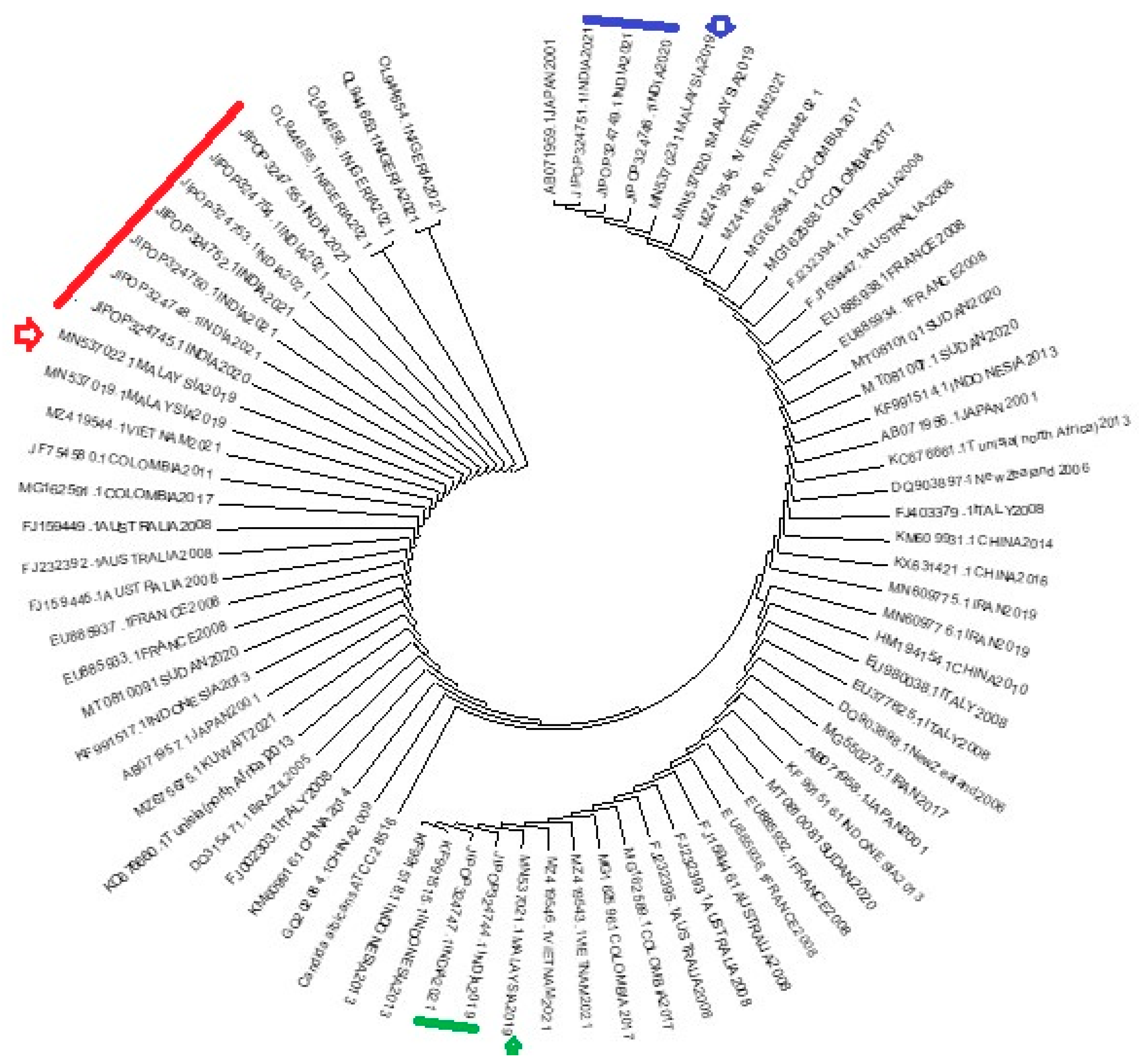

Table 1.
Clinicodemographic details of the patients yielded ERG11 gene.
| Serial Number | Isolate Number | Year of isolation | Age | Gender | Specimen | Service | Diabetic Status | HIV Status |
|---|---|---|---|---|---|---|---|---|
| 1 | 10 | 2019 | 24 | F | Genital swab | OBG | Diabetic | Negative |
| 2 | 21 | 2020 | 48 | F | Ear swab | ENT | Diabetic | Negative |
| 3 | 25 | 2020 | 26 | F | Genital swab | OBG | Diabetic | Negative |
| 4 | 42 | 2021 | 49 | F | Blood | Medicine | Diabetic | Negative |
| 5 | 111 | 2021 | 34 | F | Perianal swab | OBG | Diabetic | Negative |
| 6 | 113 | 2021 | 23 | F | Genital swab | OBG | Nondiabetic | Negative |
| 7 | 130 | 2021 | 20 | F | Genital swab | OBG | Nondiabetic | Negative |
| 8 | 136 | 2021 | 42 | M | Genital swab | Medicine | Diabetic | Negative |
| 9 | 142 | 2021 | 24 | F | Genital swab | OBG | Nondiabetic | Negative |
| 10 | 143 | 2021 | 59 | M | Blood | Pulmonary medicine | Diabetic | Negative |
| 11 | 145 | 2021 | 9 | M | Blood | Paediatrics | Unknown | Negative |
| 12 | 147 | 2021 | 27 | F | Genital swab | OBG | Diabetic | Negative |
Table 2.
Mutation in part of ERG 11 gene of FRCA isolates.
| Serial Number | Isolate Number | Accession ID | T1110C | T1140C | C1203T | T1284C | T1296C | C1302T | G1309A | A1440G | T1470C | Total silent mutations | Total missense mutations |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 10 | OP324744.1 | - | + | - | - | + | + | - | + | - | 4 | - |
| 2 | 21 | OP324745.1 | - | + | - | - | + | + | - | + | + | 5 | - |
| 3 | 25 | OP324746.1 | - | + | + | - | + | + | + | + | + | 6 | 1 |
| 4 | 42 | OP324747.1 | - | - | - | + | + | - | - | + | - | 3 | - |
| 5 | 111 | OP324748.1 | - | - | + | - | + | - | - | + | + | 4 | - |
| 6 | 113 | OP324749.1 | + | - | + | - | + | + | - | - | - | 4 | - |
| 7 | 130 | OP324750.1 | + | - | + | - | + | + | - | - | - | 4 | - |
| 8 | 136 | OP324751.1 | _ | - | + | - | + | + | - | + | + | 5 | - |
| 9 | 142 | OP324752.1 | - | - | + | - | + | - | - | + | + | 4 | - |
| 10 | 143 | OP324753.1 | - | - | - | - | - | - | - | - | - | - | - |
| 11 | 145 | OP324754.1 | - | - | + | - | - | - | - | - | - | 1 | - |
| 12 | 147 | OP324755.1 | - | - | + | - | + | - | - | + | + | 4 | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



