Submitted:
26 December 2023
Posted:
27 December 2023
You are already at the latest version
Abstract
Arrhythmogenic cardiomyopathy is a primary genetic disease caused by mutations of the desmosome genes. Ever since the introduction of new imaging criteria, like cardiovascular magnetic resonance, the diagnosis of arrhythmogenic cardiomyopathy is more challenging as left ventricular or biventricular variants may cause resemblance with other cardiomyopathies or myocarditis. Not only this, but they may also share an acute phase that might determine even more confusion and misdiagnosis which can influence prognosis and outcome. In this case report we present a 31-year-old patient with multiple clinical pictures: acute chest pain, new onset of heart failure and arrhythmia symptoms which determined a dynamic change in clinical diagnosis and management, ultimately taking into consideration arrhythmogenic cardiomyopathy. Through the article we try to emerge and explain common pathophysiological pathways shared by arrhythmogenic cardiomyopathy and other clinical entities with a special focus on inflammation. The final question remains: “If there is more than one heart disorder that eventually will lead to the same clinical picture, one could not but wonder if arrhythmogenic cardiomyopathy is rather a syndrome than a specific condition?”
Keywords:
inflammation
; myocarditis
; arrhythmogenic cardiomyopathy
; cardiovascular magnetic resonance
Figure 1.
ECG, echocardiography and coronary angiography: notched R and S wave (arrow on ECG), “slow-flow” phenomenon left anterior descendent artery (arrow on angiography). A 31-year-old male patient smoker, presented to the emergency department for anterior chest pain with sudden onset and neck radiation. From his personal and family medical history we haven’t depicted any relevant cardiovascular health issues. His heart rate, blood pressure and vitals at presentation were in the normal range. The electrocardiogram showed a 2 mm ST segment elevation in V2-V3 and QRS fragmentation with notching of R wave in D2 and aVF and of S wave in V1-V2. The lab exam showed a markedly increased high-sensitive troponin (hsTnI = 16.879ng/mL) and normal LDL cholesterol. Echocardiographic imaging revealed mild systolic dysfunction (EF= 45%) with hypokinesia of mid-apical septum. The patient was referred immediately to the catheterization laboratory where coronary angiography showed normal coronary arteries but with a “slow-flow” phenomenon (CSF) on the left anterior descendent artery. Because the patient did not present multiple cardiovascular risk factors and due to the aspect of the “slow-flow” feature seen at invasive coronary angiography, the diagnosis of Myocardial Infarction with non-obstructive coronary arteries (MINOCA) with possible thrombophilia or autoimmune disorders etiology were taken into consideration. The panel tests for autoimmune disorders were normal instead the hereditary profile for thrombophilia revealed a positive mutation for factor V Leiden and a heterozygote genotype mutation of the MTHFR gene at the level of C677T and A1298C locus. The patient was discharged with the following pharmacological treatment: aspirin, apixaban, non-dihydropyridine calcium channel blockers and long-acting nitrates.
Figure 1.
ECG, echocardiography and coronary angiography: notched R and S wave (arrow on ECG), “slow-flow” phenomenon left anterior descendent artery (arrow on angiography). A 31-year-old male patient smoker, presented to the emergency department for anterior chest pain with sudden onset and neck radiation. From his personal and family medical history we haven’t depicted any relevant cardiovascular health issues. His heart rate, blood pressure and vitals at presentation were in the normal range. The electrocardiogram showed a 2 mm ST segment elevation in V2-V3 and QRS fragmentation with notching of R wave in D2 and aVF and of S wave in V1-V2. The lab exam showed a markedly increased high-sensitive troponin (hsTnI = 16.879ng/mL) and normal LDL cholesterol. Echocardiographic imaging revealed mild systolic dysfunction (EF= 45%) with hypokinesia of mid-apical septum. The patient was referred immediately to the catheterization laboratory where coronary angiography showed normal coronary arteries but with a “slow-flow” phenomenon (CSF) on the left anterior descendent artery. Because the patient did not present multiple cardiovascular risk factors and due to the aspect of the “slow-flow” feature seen at invasive coronary angiography, the diagnosis of Myocardial Infarction with non-obstructive coronary arteries (MINOCA) with possible thrombophilia or autoimmune disorders etiology were taken into consideration. The panel tests for autoimmune disorders were normal instead the hereditary profile for thrombophilia revealed a positive mutation for factor V Leiden and a heterozygote genotype mutation of the MTHFR gene at the level of C677T and A1298C locus. The patient was discharged with the following pharmacological treatment: aspirin, apixaban, non-dihydropyridine calcium channel blockers and long-acting nitrates.
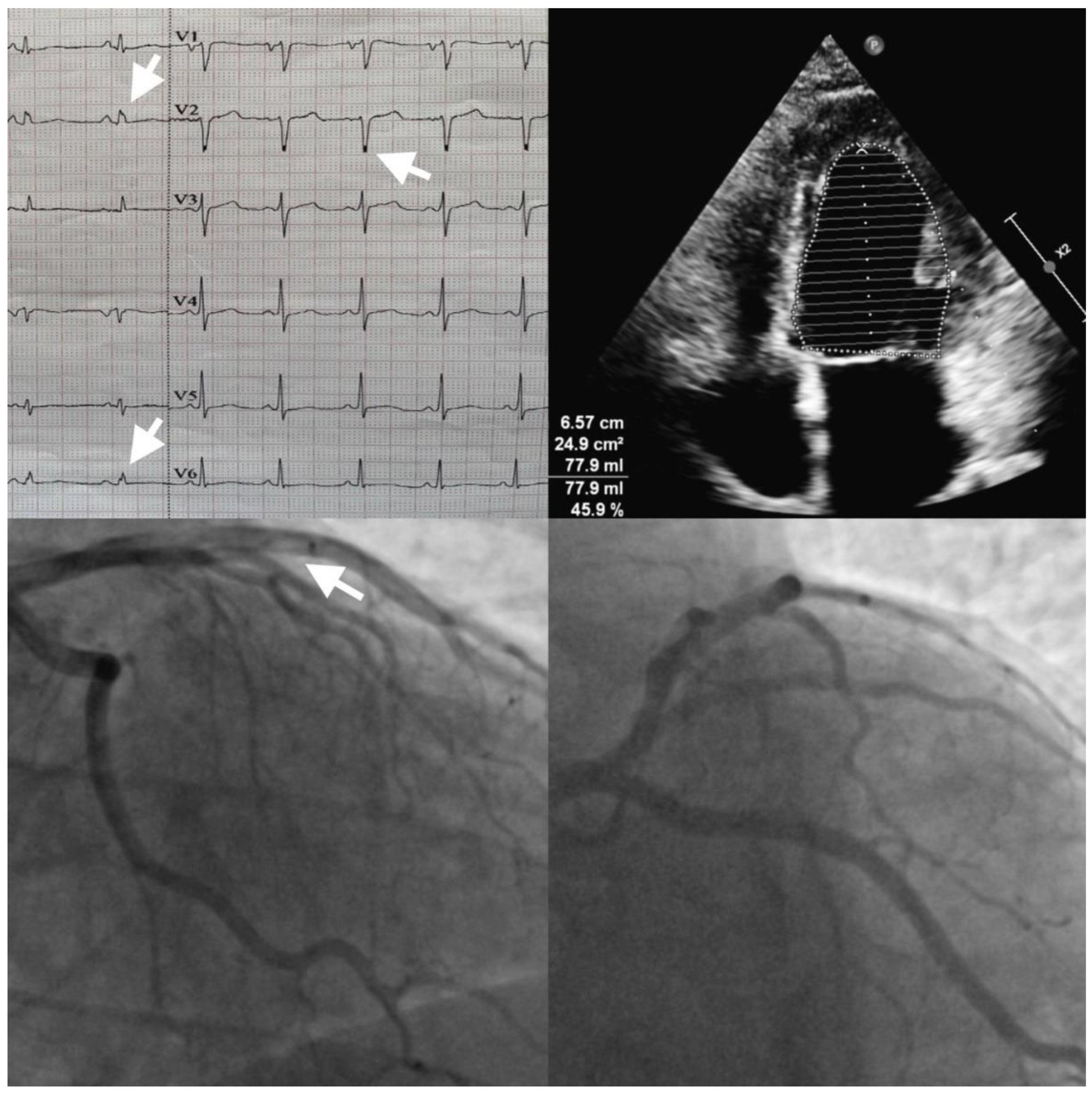
Figure 2.
Cardiovascular magnetic resonance (CMR): steady-state-free-precession images SSFP (A,C,D arrows) show “chemical shift” and micro-aneurisms; T1-weighted image B shows (arrow) fat-infiltration. After two weeks, the patient presents in the ambulatory office with exertional dyspnea and high levels of natriuretic peptides (NT-proBNP = 924 pg/ml). A cardiac MRI was performed which showed dilated left ventricle with moderate systolic dysfunction (EF=35%), mid-apical anterior wall hypokinesia, septum, inferior and lateral wall hypokinesia of the apical segments. At CINE images “chemical shift” was depicted at basal segment of the septum and of the apical segment suggestive of fat metaplasia. Fat infiltration was also observed in T1 weighted and T2 weighted sequences at the level of the basal segment of the septum and lateral wall. The presence of micro-aneurysms were spotted at the level of mid-apical segments of the lateral wall. According to the “Padua Criteria” for diagnosing Arrhythmogenic Cardiomyopathy (ACM), morpho-functional and structural MRI lesions were suggestive for dominant left ventricular arrhythmogenic cardiomyopathy. [1] To our knowledge, this is the first clinical case to highlight AC features in a patient with initial diagnosis of MINOCA.
Figure 2.
Cardiovascular magnetic resonance (CMR): steady-state-free-precession images SSFP (A,C,D arrows) show “chemical shift” and micro-aneurisms; T1-weighted image B shows (arrow) fat-infiltration. After two weeks, the patient presents in the ambulatory office with exertional dyspnea and high levels of natriuretic peptides (NT-proBNP = 924 pg/ml). A cardiac MRI was performed which showed dilated left ventricle with moderate systolic dysfunction (EF=35%), mid-apical anterior wall hypokinesia, septum, inferior and lateral wall hypokinesia of the apical segments. At CINE images “chemical shift” was depicted at basal segment of the septum and of the apical segment suggestive of fat metaplasia. Fat infiltration was also observed in T1 weighted and T2 weighted sequences at the level of the basal segment of the septum and lateral wall. The presence of micro-aneurysms were spotted at the level of mid-apical segments of the lateral wall. According to the “Padua Criteria” for diagnosing Arrhythmogenic Cardiomyopathy (ACM), morpho-functional and structural MRI lesions were suggestive for dominant left ventricular arrhythmogenic cardiomyopathy. [1] To our knowledge, this is the first clinical case to highlight AC features in a patient with initial diagnosis of MINOCA.
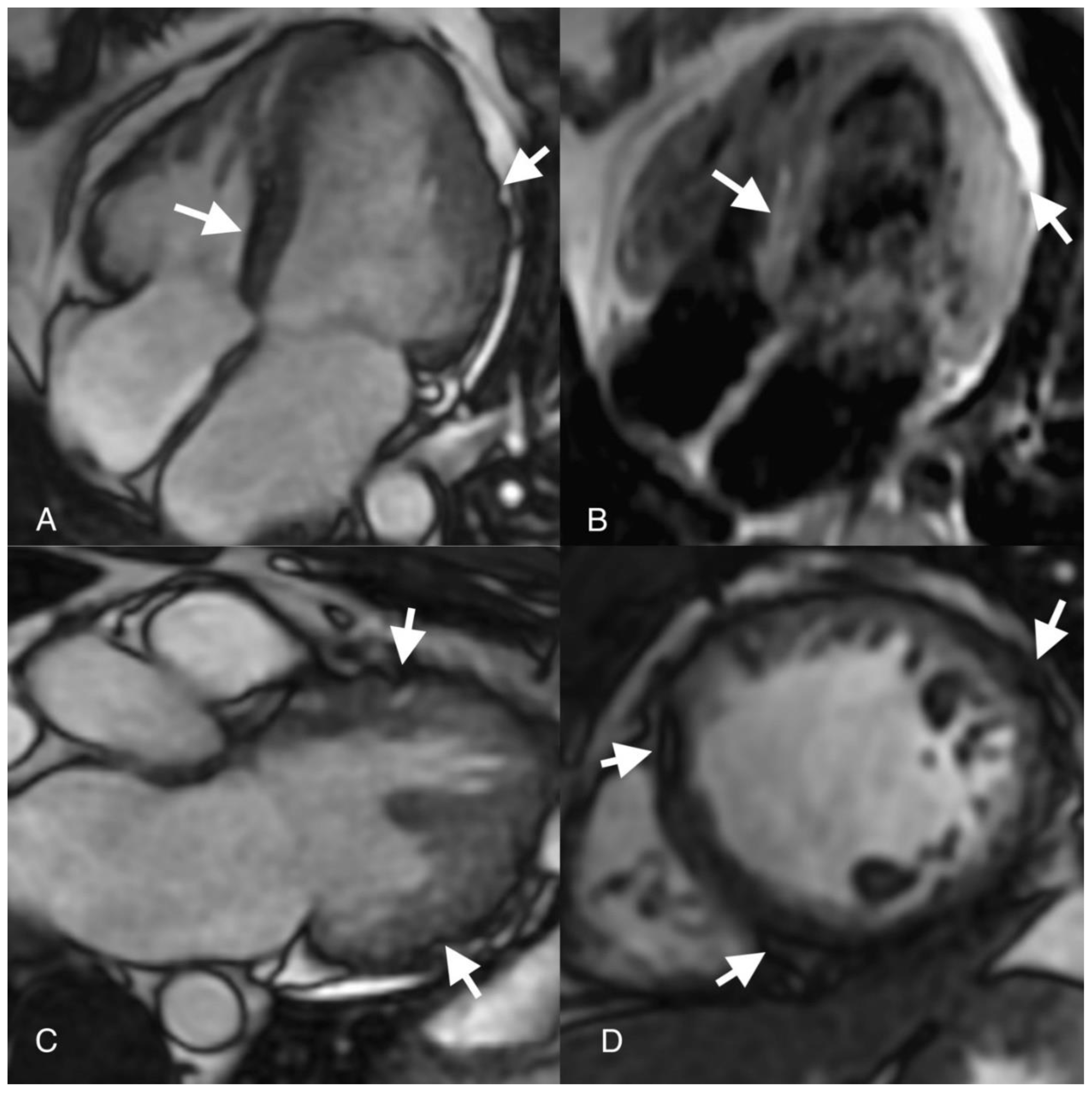
Figure 3.
Cardiovascular Magnetic Resonance (CMR): T2 weighted - Triple Inversion Recovery image (A arrow) show epicardial anterior and lateral wall high-signal-intensity area; Native T1 map image (B arrow) shows high septal T1 (1400ms) on Region of Interest (ROI); Late Gagolinium Enhancement (LGE) images (C, D arrows) show epicardial late enhancement of the antero-septal, antero-lateral and infero-lateral walls basal and mid segments. Epicardial myocardial oedema was seen at the basal segment of the anteroseptal and inferolateral wall on T2 weighted images with a regional SI ratio of myocardium over skeletal muscle over 2. Native T1 mapping showed high T1 values (1400ms) suggestive of myocardial edema. On LGE images epicardial fibrosis was described on the anterior wall mid-apical segments, inferior wall mid-basal segments, septum and lateral wall all segments. Besides the “Padua Criteria”, the patient’s MRI lesions according to “Lake Louise” criteria were also suggestive of acute myocarditis. The pathophysiology of ACM is rather complex and involves multiple signalling pathways perturbations like: plakoglobin redistribution, gap junction remodeling, myocardial apoptosis and high-circulating levels of proinflammatory cytokines. [2] Inflammation secondary to viral infection has been suggested to influence ACM pathophysiology as initial histological reports showed patchy inflammatory infiltrates in patients with ARVC. [3] While this may be, there were also a lot of reports of misdiagnosed ACM as considered to be myocarditis. [4] The highly phenotypical resemblance between these conditions, opened a “Pandora’s box” of discussion whether inflammation triggers ACM or it is just a secondary mechanism of maladaptive immunomodulatory response involving cytokine encoding genes of ACM. Although local interstitial right ventricle (RV) and left ventricle (LV) inflammation infiltrates were demonstrated in several studies on ACM cases, this pattern is not universally found in ACM histology. [2] The presence of inflammation in ACM hearts varied from 30% to 67% involving most often lymphocytes, monocytes, neutrophils and less often mast cells, macrophages and histiocytes in areas of fibro-fatty replacement. [5-6] On the other hand, fibro-fatty replacement is not a characteristic feature for myocarditis pathology. There are frequent reports in literature where ACM patients clinically present with an acute phase of “myocarditis-like” features (dyspnea, chest pain, elevated troponin levels, ECG abnormalities). [7] Martins et al showed on a pediatric population with different variants of ACM, the presence of an “acute-phase” in six patients of the entire cohort, neither of them being identified with an infectious trigger but rather exercise induced. [8] There are also some small studies that demonstrated even the presence of cardiotropic viruses in biopsies of ARVC hearts. [9] Inflammation was imagistically evaluated in 2 small sample studies of patients with ACM by myocardial scintigraphy and 18-FDG PET scan. [10-11] There was a significantly higher myocardial uptake of radiotracers in the ACM group compared to the control group thus indicating the presence of inflammation. [10-11] Two cases with ACM and confirmed desmoplakin (DSP) mutation were described as presenting with an acute phase episode of myocarditis-like phenotype and subepicardial LGE on CMR after sports activity. [12] Interestingly it only involved the LV and no other imagistic criteria for ACM was met. [12] In human heart biopsies there was a trend of inflammatory infiltrates associated to fibro-fatty replacement in the ACM LV dominant form (75%) compared to the RV dominant form (30%). [5] Also, these patients showed similar patterns to patients with myocarditis, meaning sub-epicardial scarring in the inferolateral wall. But inflammation is not always linked to an infectious trigger, as ACM patients were described to experience “myocarditis-like” episodes with inflammation depicted at CMR in the absence of a viral disease. [13] These episodes are now recognised as the “hot phases” of ACM and are considered to be responsible for disease progression. [7].
Figure 3.
Cardiovascular Magnetic Resonance (CMR): T2 weighted - Triple Inversion Recovery image (A arrow) show epicardial anterior and lateral wall high-signal-intensity area; Native T1 map image (B arrow) shows high septal T1 (1400ms) on Region of Interest (ROI); Late Gagolinium Enhancement (LGE) images (C, D arrows) show epicardial late enhancement of the antero-septal, antero-lateral and infero-lateral walls basal and mid segments. Epicardial myocardial oedema was seen at the basal segment of the anteroseptal and inferolateral wall on T2 weighted images with a regional SI ratio of myocardium over skeletal muscle over 2. Native T1 mapping showed high T1 values (1400ms) suggestive of myocardial edema. On LGE images epicardial fibrosis was described on the anterior wall mid-apical segments, inferior wall mid-basal segments, septum and lateral wall all segments. Besides the “Padua Criteria”, the patient’s MRI lesions according to “Lake Louise” criteria were also suggestive of acute myocarditis. The pathophysiology of ACM is rather complex and involves multiple signalling pathways perturbations like: plakoglobin redistribution, gap junction remodeling, myocardial apoptosis and high-circulating levels of proinflammatory cytokines. [2] Inflammation secondary to viral infection has been suggested to influence ACM pathophysiology as initial histological reports showed patchy inflammatory infiltrates in patients with ARVC. [3] While this may be, there were also a lot of reports of misdiagnosed ACM as considered to be myocarditis. [4] The highly phenotypical resemblance between these conditions, opened a “Pandora’s box” of discussion whether inflammation triggers ACM or it is just a secondary mechanism of maladaptive immunomodulatory response involving cytokine encoding genes of ACM. Although local interstitial right ventricle (RV) and left ventricle (LV) inflammation infiltrates were demonstrated in several studies on ACM cases, this pattern is not universally found in ACM histology. [2] The presence of inflammation in ACM hearts varied from 30% to 67% involving most often lymphocytes, monocytes, neutrophils and less often mast cells, macrophages and histiocytes in areas of fibro-fatty replacement. [5-6] On the other hand, fibro-fatty replacement is not a characteristic feature for myocarditis pathology. There are frequent reports in literature where ACM patients clinically present with an acute phase of “myocarditis-like” features (dyspnea, chest pain, elevated troponin levels, ECG abnormalities). [7] Martins et al showed on a pediatric population with different variants of ACM, the presence of an “acute-phase” in six patients of the entire cohort, neither of them being identified with an infectious trigger but rather exercise induced. [8] There are also some small studies that demonstrated even the presence of cardiotropic viruses in biopsies of ARVC hearts. [9] Inflammation was imagistically evaluated in 2 small sample studies of patients with ACM by myocardial scintigraphy and 18-FDG PET scan. [10-11] There was a significantly higher myocardial uptake of radiotracers in the ACM group compared to the control group thus indicating the presence of inflammation. [10-11] Two cases with ACM and confirmed desmoplakin (DSP) mutation were described as presenting with an acute phase episode of myocarditis-like phenotype and subepicardial LGE on CMR after sports activity. [12] Interestingly it only involved the LV and no other imagistic criteria for ACM was met. [12] In human heart biopsies there was a trend of inflammatory infiltrates associated to fibro-fatty replacement in the ACM LV dominant form (75%) compared to the RV dominant form (30%). [5] Also, these patients showed similar patterns to patients with myocarditis, meaning sub-epicardial scarring in the inferolateral wall. But inflammation is not always linked to an infectious trigger, as ACM patients were described to experience “myocarditis-like” episodes with inflammation depicted at CMR in the absence of a viral disease. [13] These episodes are now recognised as the “hot phases” of ACM and are considered to be responsible for disease progression. [7].
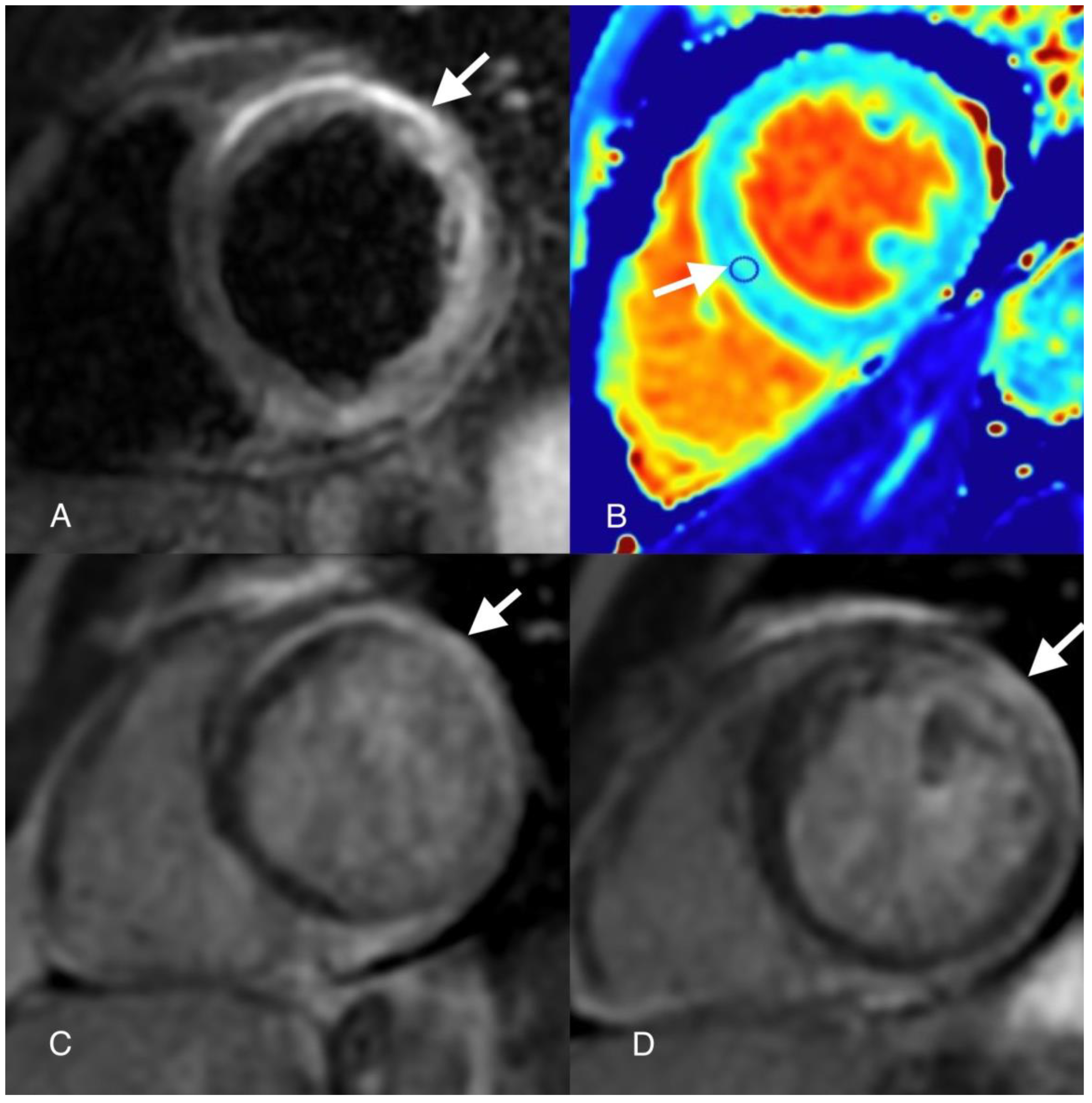
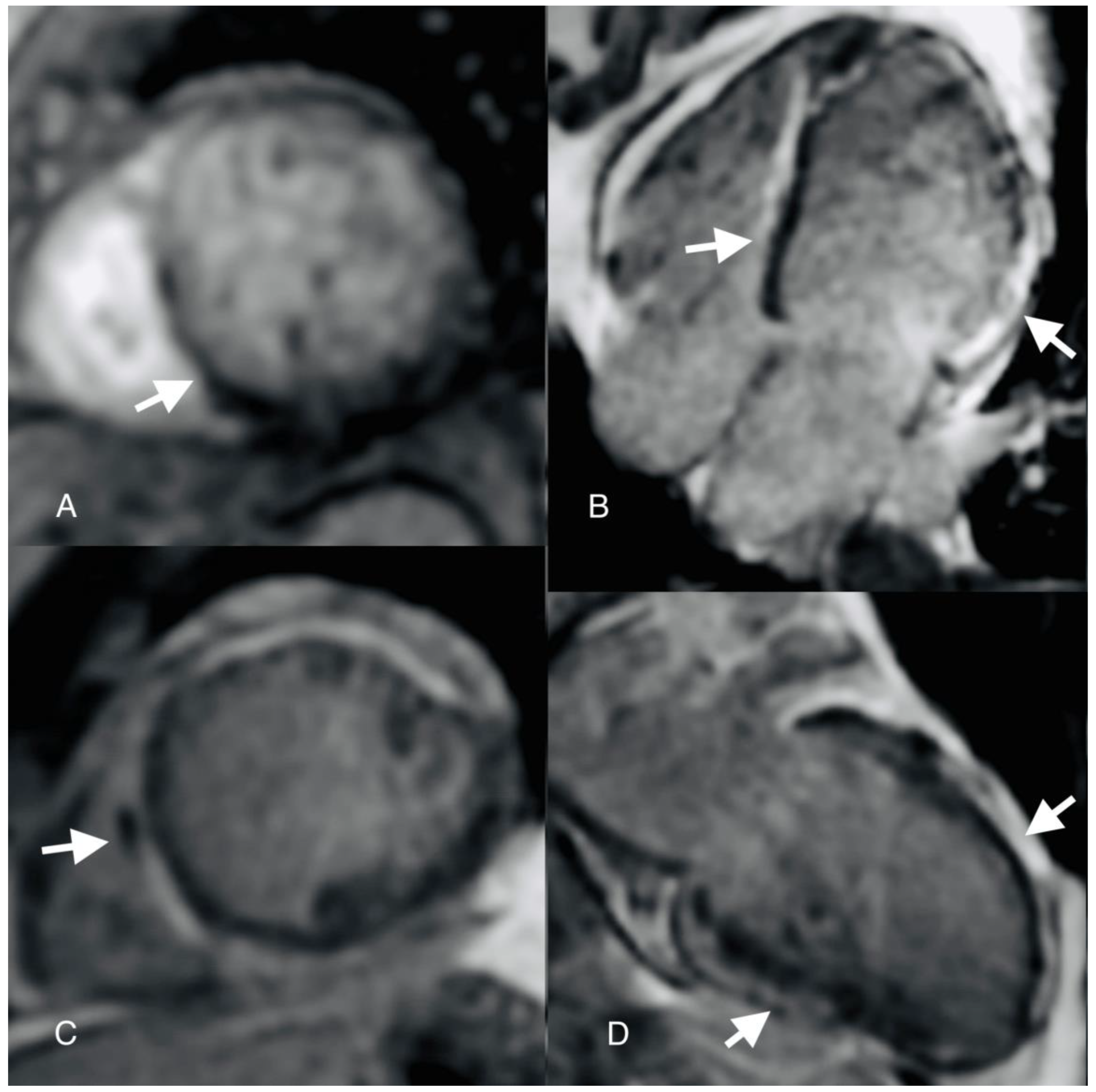
Figure 4.
Cardiovascular Magnetic Resonance (CMR): First pass perfusion image (A arrow) shows inferoseptal perfusion defect; Late gadolinium enhancement image (C arrow) shows a low-signal-intensity area at the level of the septum mid segment; Horizontal (B) and Vertical (D) Long Axis Late Gadolinium Enhancement (LGE) Images show epicardial late enhancement of the anterior, lateral, inferior and septum walls. Also, at the level of the septum mid segment a hypointense signal was depicted on LGE sequences suggestive of microvascular obstruction (MVO). A first pass perfusion was performed which evidenced an inferoseptal perfusion defect in concordance with the “slow-flow phenomenon” described at coronary angiography in the emergency setting. There is however a particular aspect regarding this case, mainly the “slow-flow” phenomenon described at coronary angiography which created some confusion regarding the patients’ management. This term is mainly used at invasive coronary angiography to describe the delayed progression of contrast media through the coronary artery tree during injection. This phenomenon is frequently encountered in acute coronary syndromes and is due to microvascular obstruction. While the patient was positive for thrombophilia, in the context of CSF, coronary thromboembolism was a reasonable mechanism thought to be responsible for the acute presentation. But there are many underlying pathogenic mechanisms responsible for this phenomenon besides obstruction, such as: small vessel disease, endothelial dysfunction or inflammation. [14] It is known that myocarditis may be accompanied by impaired coronary microcirculation. Active pro-inflammation together with damaged endothelium predisposes to thrombus formation and aberrant microvascular vasomotor function that might explain CSF phenomenon. [15] But infectious agents are not solely responsible for changes in the microvasculature, such changes being also observed in non-viral mechanisms. In support to this comes a small study by Paul et al on 10 patients with arrhythmogenic right ventricular cardiomyopathy (ARVC) in which it was shown on PET scan that there is reduced hyperaemic myocardial blood flow and increased coronary vascular resistance. [16] Inflammation and microvascular dysfunction are common mechanisms in true ischemic MINOCA, myocarditis and ACM, that is why work-flow diagnosis in MINOCA should include specific testing for the last two entities, especially in patients with arrhythmic burden thus to avoid possible catastrophic events. The patient was initiated with heart failure-treatment: neprilysine inhibitors, beta-blockers, dapaglifozin and spironolactone. After one month, the patient presented an episode of syncope while at home, reading. A 24-hour Holter ECG was placed which recorded 2 episodes of non-sustained ventricular tachycardia. The patient underwent intracardiac defibrillator implantation. After 3 months of optimal heart failure treatment, the ejection fraction remained 35 % with no obvious improvement while the patient remained in NYHA II class. It is quite clear the clinical overlap between these two entities myocarditis and ACM in certain circumstances, making things in the acute phase indistinguishable. That is why according to the new proposed Padua Criteria there is need for geneting testing to differentiate between these two entities. [1] The main limitations of this case were: lack of performing geneting testing and endomyocardial biopsy with PCR analysis for viral agent. The fact that the patient presented three consecutive and different clinical pictures: “chest-pain” like episode followed by heart failure-like episode and finally an arrhythmia event led us to believe that we are dealing with an acute episode of myocarditis evolving towards auto reactive myocarditis and inflammatory cardiomyopathy. Of course, in this situation things remain unclear whether this was the case of an acute myocarditis or ACM ALVC variant with a “hot phase”. One should bear in mind that with genetic testing according to available literature a specific causative desmosomal gene mutation is only found in 50% of cases. [17] One thing is for certain, inflammation stands in both entities ACM and myocarditis and there are common pathways which produces an overlap and misdiagnosing. Future studies are needed to understand the behavior of inflammatory pathways in these diseases because targeting inflammation might prevent disease progression and impact outcome. Whether inflammation acts as a primary trigger or a secondary cause of event it is not well established, but one cannot help but wonder: if two things look the same and act the same what do you call them?
Figure 4.
Cardiovascular Magnetic Resonance (CMR): First pass perfusion image (A arrow) shows inferoseptal perfusion defect; Late gadolinium enhancement image (C arrow) shows a low-signal-intensity area at the level of the septum mid segment; Horizontal (B) and Vertical (D) Long Axis Late Gadolinium Enhancement (LGE) Images show epicardial late enhancement of the anterior, lateral, inferior and septum walls. Also, at the level of the septum mid segment a hypointense signal was depicted on LGE sequences suggestive of microvascular obstruction (MVO). A first pass perfusion was performed which evidenced an inferoseptal perfusion defect in concordance with the “slow-flow phenomenon” described at coronary angiography in the emergency setting. There is however a particular aspect regarding this case, mainly the “slow-flow” phenomenon described at coronary angiography which created some confusion regarding the patients’ management. This term is mainly used at invasive coronary angiography to describe the delayed progression of contrast media through the coronary artery tree during injection. This phenomenon is frequently encountered in acute coronary syndromes and is due to microvascular obstruction. While the patient was positive for thrombophilia, in the context of CSF, coronary thromboembolism was a reasonable mechanism thought to be responsible for the acute presentation. But there are many underlying pathogenic mechanisms responsible for this phenomenon besides obstruction, such as: small vessel disease, endothelial dysfunction or inflammation. [14] It is known that myocarditis may be accompanied by impaired coronary microcirculation. Active pro-inflammation together with damaged endothelium predisposes to thrombus formation and aberrant microvascular vasomotor function that might explain CSF phenomenon. [15] But infectious agents are not solely responsible for changes in the microvasculature, such changes being also observed in non-viral mechanisms. In support to this comes a small study by Paul et al on 10 patients with arrhythmogenic right ventricular cardiomyopathy (ARVC) in which it was shown on PET scan that there is reduced hyperaemic myocardial blood flow and increased coronary vascular resistance. [16] Inflammation and microvascular dysfunction are common mechanisms in true ischemic MINOCA, myocarditis and ACM, that is why work-flow diagnosis in MINOCA should include specific testing for the last two entities, especially in patients with arrhythmic burden thus to avoid possible catastrophic events. The patient was initiated with heart failure-treatment: neprilysine inhibitors, beta-blockers, dapaglifozin and spironolactone. After one month, the patient presented an episode of syncope while at home, reading. A 24-hour Holter ECG was placed which recorded 2 episodes of non-sustained ventricular tachycardia. The patient underwent intracardiac defibrillator implantation. After 3 months of optimal heart failure treatment, the ejection fraction remained 35 % with no obvious improvement while the patient remained in NYHA II class. It is quite clear the clinical overlap between these two entities myocarditis and ACM in certain circumstances, making things in the acute phase indistinguishable. That is why according to the new proposed Padua Criteria there is need for geneting testing to differentiate between these two entities. [1] The main limitations of this case were: lack of performing geneting testing and endomyocardial biopsy with PCR analysis for viral agent. The fact that the patient presented three consecutive and different clinical pictures: “chest-pain” like episode followed by heart failure-like episode and finally an arrhythmia event led us to believe that we are dealing with an acute episode of myocarditis evolving towards auto reactive myocarditis and inflammatory cardiomyopathy. Of course, in this situation things remain unclear whether this was the case of an acute myocarditis or ACM ALVC variant with a “hot phase”. One should bear in mind that with genetic testing according to available literature a specific causative desmosomal gene mutation is only found in 50% of cases. [17] One thing is for certain, inflammation stands in both entities ACM and myocarditis and there are common pathways which produces an overlap and misdiagnosing. Future studies are needed to understand the behavior of inflammatory pathways in these diseases because targeting inflammation might prevent disease progression and impact outcome. Whether inflammation acts as a primary trigger or a secondary cause of event it is not well established, but one cannot help but wonder: if two things look the same and act the same what do you call them?
Author Contributions
Conceptualization: IRL; Methodology: IRL; Validation: APM.; writing—review and editing: IRL; visualization: APM.; supervision: APM. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Data Availability Statement
Data is unavailable due to privacy and ethical restrictions.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Corrado D, Perazzolo Marra M, Zorzi A, Beffagna G, Cipriani A, Lazzari M, Migliore F, Pilichou K, Rampazzo A, Rigato I, Rizzo S, Thiene G, Anastasakis A, Asimaki A, Bucciarelli-Ducci C, Haugaa KH, Marchlinski FE, Mazzanti A, McKenna WJ, Pantazis A, Pelliccia A, Schmied C, Sharma S, Wichter T, Bauce B, Basso C. Diagnosis of arrhythmogenic cardiomyopathy: The Padua criteria. Int J Cardiol. 2020 Nov 15;319:106-114. [CrossRef]
- Asatryan B, Asimaki A, Landstrom AP, Khanji MY, Odening KE, Cooper LT, Marchlinski FE, Gelzer AR, Semsarian C, Reichlin T, Owens AT, Chahal CAA. Inflammation and Immune Response in Arrhythmogenic Cardiomyopathy: State-of-the-Art Review. Circulation. 2021 Nov 16;144(20):1646-1655. [CrossRef]
- Basso C, Thiene G, Corrado D, Angelini A, Nava A, Valente M. Arrhythmo- genic right ventricular cardiomyopathy. Dysplasia, dystrophy, or myocarditis? Circulation. 1996;94:983–991. [CrossRef]
- Reichl K, Kreykes SE, Martin CM, Shenoy C. Desmoplakin variant-as- sociated arrhythmogenic cardiomyopathy presenting as acute myo- carditis. Circ Genom Precis Med. 2018;11:e002373. [CrossRef]
- Corrado D, Basso C, Thiene G, McKenna WJ, Davies MJ, Fontaliran F, et al. Spectrum of clinicopathologic manifestations of arrhythmogenic right ventricular cardiomyopathy/dysplasia: a multicenter study. J Am Coll Cardiol. (1997) 30:1512–20. [CrossRef]
- Campuzano O, Alcalde M, Iglesias A, Barahona-Dussault C, Sarquella-Brugada G, Benito B, et al. Arrhythmogenic right ventricular cardiomyopathy: severe structural alterations are associated with inflammation. J Clin Pathol. (2012) 65:1077–83. [CrossRef]
- Bariani R, Rigato I, Cipriani A, Bueno Marinas M, Celeghin R, Basso C, Corrado D, Pilichou K, Bauce B. Myocarditis-like Episodes in Patients with Arrhythmogenic Cardiomyopathy: A Systematic Review on the So-Called Hot-Phase of the Disease. Biomolecules. 2022 Sep 19;12(9):1324. [CrossRef]
- Martins D, Ovaert C, Khraiche D, Boddaert N, Bonnet D, Raimondi F. Myocardial inflammation detected by cardiac MRI in Arrhythmogenic right ventricular cardiomyopathy: A paediatric case series. Int J Cardiol. 2018 Nov 15;271:81-86. [CrossRef]
- Bowles NE, Ni J, Marcus F, Towbin JA. The detection of cardiotropic viruses in the myocardium of patients with arrhythmogenic right ventriculardysplasia/cardiomyopathy. J Am Coll Cardiol. (2002) 39:892–5.
- Campian ME, Verberne HJ, Hardziyenka M, de Groot EA, van Moerkerken AF, van Eck-Smit BL, Tan HL. Assessment of inflammation in patients with arrhythmogenic right ventricular cardiomyopathy/dysplasia. Eur J Nucl Med Mol Imaging. 2010;37:2079–2085. [CrossRef]
- Protonotarios A, Wicks E, Ashworth M, Stephenson E, Guttmann O, Savvatis K, Sekhri N, Mohiddin SA, Syrris P, Menezes L, et al. Prevalence of 18F- fluorodeoxyglucose positron emission tomography abnormalities in pa- tients with arrhythmogenic right ventricular cardiomyopathy. Int J Cardiol. 2019;284:99–104. [CrossRef]
- Poller W, Haas J, Klingel K, Kühnisch J, Gast M, Kaya Z, Escher F, Kayvanpour E, Degener F, Opgen-Rhein B, et al. Familial recurrent myocarditis triggered by exercise in patients with a truncating variant of the desmoplakin gene. J Am Heart Assoc. 2020;9:e015289. [CrossRef]
- Mavrogeni S, Protonotarios N, Tsatsopoulou A, Papachristou P, Sfendouraki E, Papadopoulos G. Naxos disease evolution mimicking acute myocarditis: the role of cardiovascular magnetic resonance imaging. Int J Cardiol. (2013) 166:e14–5. [CrossRef]
- Zhu Q, Wang S, Huang X, Zhao C, Wang Y, Li X, Jia D, Ma C. Understanding the pathogenesis of coronary slow flow: Recent advances. Trends Cardiovasc Med. 2022 Dec 11:S1050-1738(22)00142-6. [CrossRef]
- Woudstra L, Juffermans LJM, van Rossum AC, Niessen HWM, Krijnen PAJ. Infectious myocarditis: the role of the cardiac vasculature. Heart Fail Rev. 2018 Jul;23(4):583-595. [CrossRef]
- Paul M, Rahbar K, Gerss J, Kies P, Schober O, Schäfers K, Breithardt G, Schulze-Bahr E, Wichter T, Schäfers M. Microvascular dysfunction in nonfailing arrhythmogenic right ventricular cardiomyopathy. Eur J Nucl Med Mol Imaging. 2012 Mar;39(3):416-20. [CrossRef]
- Gerull, B.; Brodehl, A. Insights Into Genetics and Pathophysiology of Arrhythmogenic Cardiomyopathy. Curr. Heart Fail. Rep. 2021, 18, 378–390. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



