
Submitted:
25 December 2023
Posted:
26 December 2023
You are already at the latest version
Abstract
BackgroundHeart failure is a life-threatening disease affecting millions worldwide. Tolvaptan is the first FDA-approved orally active nonpeptide vasopressin 2 receptor antagonist to be used in hypervolemic hyponatremia, heart failure, cirrhosis, etc. In clinical trials, tolvaptan impacts short-term in increasing water excretion, and restoring Na+ and dyspnoea. Aims & ObjectivesThe objective is to analyze the outcomes of tolvaptan in existing cases of heart failure. MethodologyWe conducted a database search of the MEDLINE, Embase, and Cochrane Central Register of Controlled Trials and RCTs till 1st September 2019 were included following PRISMA guidelines after being matched with inclusion and exclusion criteria. 21 RCTs were included with 7,357 patients receiving tolvaptan and 7,273 patients being the control group. We used the MESH strings such as 'tolvaptan', 'vasopressin V2 receptor blocker', 'acute heart failure', and 'acute decompensated heart failure'. ResultsMeta-analysis showed that Tolvaptan was associated with a significant reduction in edema (RR = 1.05, 95% CI = 1.019-1.081, p=0.001) and significant body weight reduction (Control-SMD = -0.489, 95% CI =-0.637 to -0.342, p<0.001)&(Placebo-SMD = -0.425, 95% CI = -0.425 to -0.382, p<0.001) It shows significant decrease in serum sodium levels (SMD = 0.678, 95% CI = 0.609 to 0.748, p<0.001). There was no significant decrease in all-cause mortality (Control-RR = 0.855, 95% CI 0.470 to 1.555, p=0.607)(Placebo-RR= 0.972, 95% CI = 0.879-1.074, p=0.575). Results for Worsening renal function in heart failure (Placebo-RR = 0.798 95% CI 0.619 to 1.028, p=0.081)(Control-RR = 1.349, 95% CI=0.927-1.964, p=0.118). ConclusionAlthough tolvaptan may significantly reduce edema, congestive symptoms and decreased body weight, it has no impact on all-cause mortality and worsening renal function in heart failure.
Keywords:
Tolvaptan
; ADHF
; PRISMA
; VRA
Introduction
Heart failure is a serious threat to life affecting millions of people worldwide. Congestive heart failure (CHF) is a clinical condition characterized by reduced cardiac output causing tissue hypo-perfusion, leading to morbidity and mortality. Patients with CHF typically present with shortness of breath, fatigue, leg edema, and exercise intolerance, thereby resulting in poor quality of life, frequent admissions, and a shorter life expectancy. Epidemiologic studies indicate that a total in 2016, there were an estimated 62.5 million premature deaths due to CHF many patients are diagnosed annually, and its incidence and prevalence increase with age.
Treatment of CHF, which aims at an adequate decongestion from the volume overload state, is made up of diuretics, beta-blockers, angiotensin-converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARBs) or angiotensin receptor–neprilysin inhibitor (ARNI), digoxin, and aldosterone antagonists. Adverse effects with pharmacotherapy are common and are abnormal water homeostasis, worsening kidney function, electrolyte disturbances, and drug-drug interactions. The prevalent resistance to diuretics and the associated morbidities have made us invent and have led to the development of effective and safe treatment strategies, which maximize decongestion but minimize the adverse impact on kidney function.
Tolvaptan is the first FDA-approved orally active nonpeptide vasopressin 2 receptor antagonist to be used in hypervolemic hyponatremia, heart failure, cirrhosis, etc. In clinical trials, Tolvaptan impacts short-term improvement in increasing water excretion, and restoring Na+ and dyspnoea. The study's objective is to analyze the effects of Tolvaptan in existing cases of heart failure. However, there is a paucity of evidence guiding its use and a lack of evidence of its long-term efficacy [1]. Arginine vasopressin (AVP) is secreted from the posterior pituitary in response to elevation in plasma osmolality and decreases in arterial pressure in patients with HF and left ventricular systolic dysfunction [2]. Elevated AVP plasma concentrations physiologically activate the V2 receptor which is expressed on the basolateral membranes of renal collecting duct principal cells. It leads to an increase in the expression of AQP channels and causes fluid overload and hyponatremia [3].
Fluid overload has a detrimental effect on patients with HF. As Congestion increases, the presence of hyponatremia is associated with an increased amount of poor outcomes. Patients with heart failure (HF) who experience volume overload may develop congestive signs and symptoms, including peripheral edoema, pulmonary congestion, a lower quality of life, and a higher chance of hospitalisation [4,5].
Presently, only thiazides and loop diuretics are recommended to reduce fluid overload for HF patients [6]. 90% of WHF in the TACTICS-HF trial received extra loop diuretic treatment, which has been linked to a nearly twofold increase in post-discharge incident rates. Consequently, the use of TLV in AHF may help us lower event rates in the post-discharge phase and prevent the need for additional loop diuretics. Conventional diuretics, however, may not always be enough to fully reduce patients' fluid retention. Furthermore, it may result in a number of negative consequences, such as imbalances in neurohormones, renal failure, and electrolyte abnormalities [5].
Our objectives here are to perform a systematic review of different studies to examine the effects of TLV in patients with heart failure; and perform a quantitative meta-analysis comparing the primary and secondary outcomes between TLV and placebo. Impairment of the efficiency of the heart as a pump can lead to a complex clinical syndrome of symptoms and signs, caused by structural or functional abnormalities of the heart. Some patients have heart failure due to left ventricular systolic dysfunction or heart failure with reduced left ventricular ejection fraction (HFREF). Others have heart failure with a preserved ejection fraction (HFPEF). Patients with congestive heart failure (CHF) have higher levels of circulating arginine vasopressin (AVP). The posterior pituitary gland releases the peptide hormone known as AVP in response to decreased cardiopulmonary blood volume, decreased systolic blood pressure, or elevated plasma osmolality. AVP acts via three receptors: V1A, V1B (or V3) and V2.V2 receptors are located in the renal collecting duct, where AVP binding leads to a rise in intracellular cyclic adenosine monophosphate (cAMP) which promotes renal water re-absorption via increased transcription of aquaporin-2.Blocking the renal effects of AVP with a selective V2-receptor antagonist, such as Tolvaptan, should produce a diuresis and maintain renal function by antagonizing elevated endogenous [1].
Materials and Methods
We conducted a database search of the MEDLINE, Embase, and Cochrane Central Register of Controlled Trials, and RCTs till 1st September 2019 were included following PRISMA guidelines after being matched with inclusion and exclusion criteria. 21 RCTs were included with 7,357 patients receiving Tolvaptan and 7,273 patients being the control group. We used the MESH strings such as 'Tolvaptan', 'vasopressin V2 receptor blocker', 'acute heart failure', and 'acute decompensated heart failure'. Articles done with human participants and published in english were only taken into consideration [5,7].
Study selection
The studies were initially filtered based on their titles or abstracts. At this point, irrelevant papers were eliminated after two writers independently reviewed the titles and abstracts of every article that was retrieved. We assessed the remaining articles' eligibility for dispute or ambiguity. Arguments were settled by conversation[5]. we included studies that were randomized to receive treatment with Tolvaptan, in one arm and treatment with placebo in another arm [1].
Inclusion criteria
The inclusion criteria used for the studies were as given below: it should [1] be a randomized, controlled trial [RCT]; [2]should include participants who are adult patients with AHF, defined as patients had dyspnoea at rest requiring urgent hospital admission for evaluation and treatment;[3] compare TLV with controls or other diuretic agents; and [4] include any relevant outcomes: all-cause mortality, clinical events, sodium level, dyspnoea improvement, body weight reduction, and fluid loss [5,7].
Exclusion criteria
Data extraction
Data extraction by both authors. Any disagreements were settled by discussion.
Assessment of risk of bias
The risk of bias for included studies was independently assessed by two reviewers. Disagreements were resolved by discussion.
Statistical analysis
Sensitivity analysis with Relative risk and Standard Mean Difference was performed to identify the stability of statistical data, and publication bias was evaluated by funnel plots. P < 0.05 was considered statistically significant. REVMAN and Excel were used for analysis.
Results
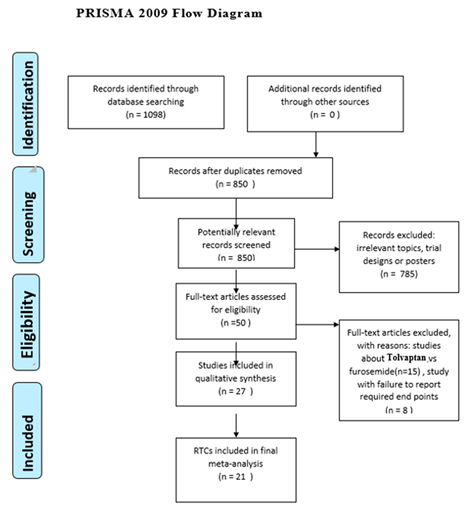
Prisma Flow Chart.
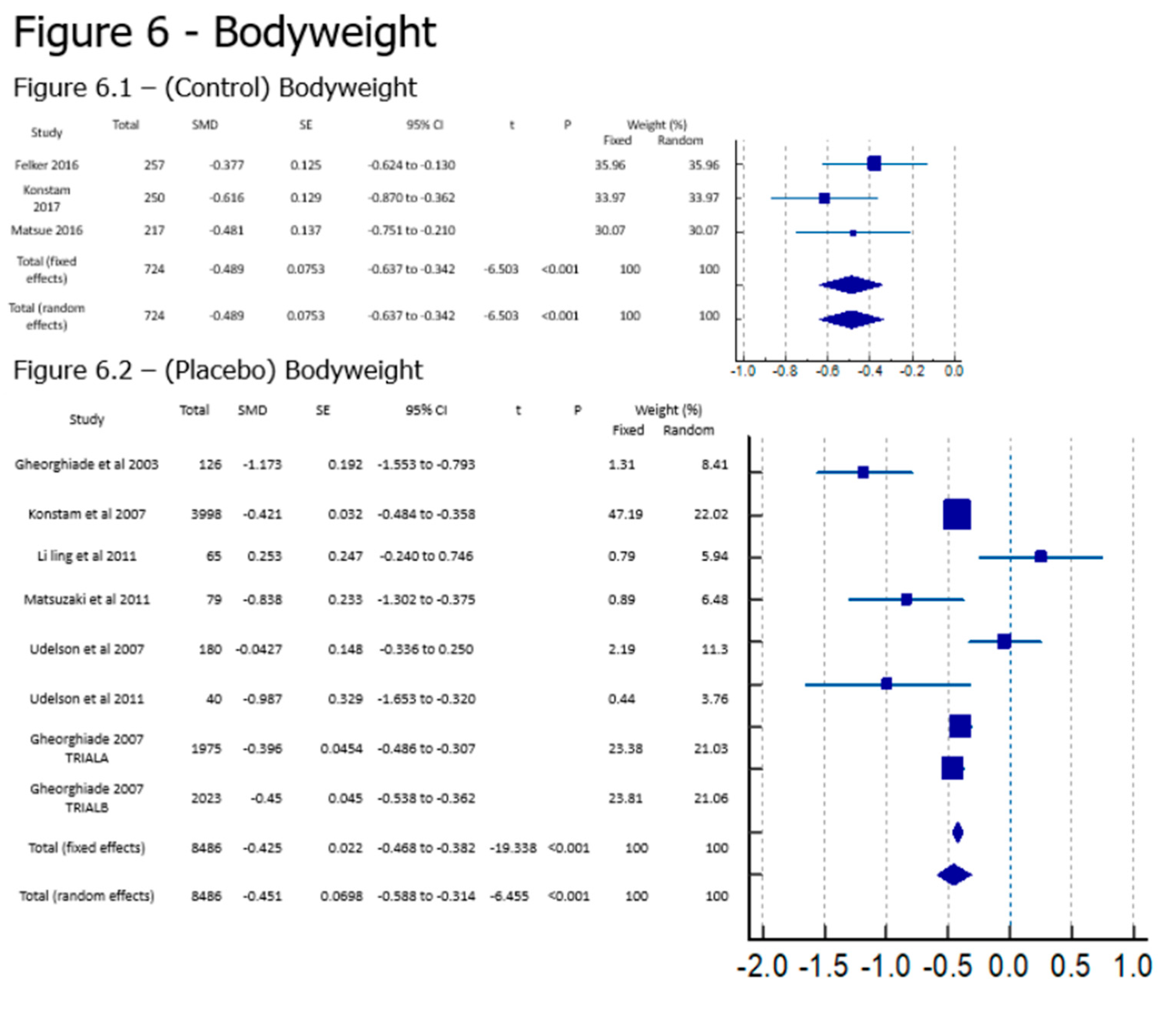
Meta-analysis showed that Tolvaptan was associated with a significant reduction in edema (RR = 1.05, 95% CI = 1.019-1.081, p=0.001) similar to Konstam 2007 [8] when compared against Placebo; Tolvaptan is also causing significant body weight reduction (SMD = -0.489, 95% CI =-0.637 to -0.342, p<0.001) compared against controls and (SMD = -0.425, 95% CI = -0.425 to -0.382, p<0.001) as is can be seen in various studies [9,10,11], but some studies contradict this result [12].
It was also associated with a significant decrease in serum sodium levels (SMD = 0.678, 95% CI = 0.609 to 0.748, p<0.001) when compared to a placebo and is supported by many papers like [13].
On the other hand, however, there was no significant decrease in all-cause mortality (RR = 0.855, 95% CI 0.470 to 1.555, p=0.607) compared to control and (RR= 0.972, 95% CI = 0.879-1.074, p=0.575) against placebo; and worsening renal function in heart failure (RR = 0.798 95% CI 0.619 to 1.028, p=0.081) compared against placebo and (RR = 1.349, 95% CI=0.927-1.964, p=0.118) against Control show widely divided results. Although papers like [14,15] have a relative risk of less than 0.4 when it comes to all-cause mortality and studies like [14,16] have a relative risk of less than 0.3 for Worsening renal Function, some papers show higher than 1 relative risk for All-cause mortality [17] [18] and Worsening renal function [17,19,20].
Discussion
The primary conclusions of this meta-analysis suggest that TLV may lower sodium levels and body weight. TLV did not, however, improve or worsen the incidence of clinical events (WHF), length of hospital stay, or all-cause mortality in patients with AHF [5].
Our study shows that there is a significant decrease in serum sodium levels as in the other trials there is a marked increase in sodium concentration. The study by Shanmugam et al. [17] revealed that TLV given at a dose of 15 mg/day is useful in reversing hyponatremia if it is used over five days, indicating that TLV was more suitable for AHF with hyponatremia. [4,5] and study by Felker 2016 [19], Serum sodium increased by an average of 3 mmol/l in the Tolvaptan group during randomised therapy, as expected based on the drug's mechanism of action, while it remained unchanged in the placebo group. Udelson et all 2011also showed an increase in serum sodium within the normal range was also observed in TLV-treated patients. But Matsuzaki's 2011 [11] phase two trial of Tolvaptan elicited a dose-dependent increase in urine volume and a decrease in urine osmolality, but did not affect urinary sodium or potassium excretion.
According to our analysis, TLV had no impact on WHF or WRF, the clinical events. The term "deterioration of heart failure symptoms" (WHF) refers to a need for more frequent heart failure treatments. These results were in line with those of the biggest EVEREST study [5]. According to Jujo 2016 [14], in our analysis, although TLV did not affect WRF overall, in the subgroup of furosemide, TLV decreased the rate of WRF. The results demonstrate that the use of TLV in AHF might help reduce WRF in comparison to the administration of loop diuretics. By Konstam 2007 [8] secondary observations included both short-term and long-term benefits on serum sodium and pedal edema, with maintenance of renal function. Also, Konstam 2017 [20] showed that in terms of kidney functions over time, there were no significant differences in GFR or serum creatinine. In a study by Felker 2016 [19] Randomization of Tolvaptan was associated with significantly higher weight and fluid loss through the 48-hour treatment period. When worsening renal function was taken as a dichotomous endpoint (defined as a change in serum creatinine of ≥0.3 mg/dl within 72 h), this endpoint was more frequent in patients randomized to Tolvaptan compared to placebo [5].
A post hoc analysis of the Acute and Chronic Therapeutic Impact of a Vasopressin Antagonist (ACTIV) trial suggests that tolvaptan may also lower the mortality rate for heart failure patients who have severe systemic congestion or renal failure. It is important to note, though, that the two studies with positive long-term effects had relatively small sample sizes; as a result, the evidence from them is weaker and could just be the product of chance. The results of our meta-analysis show that tolvaptan did not, at least in the case of HF patients, worsen their prognosis [5]. According to the Jujo 2016 [14] study, Six studies in total reported all-cause mortality of AHF following TLV therapy; two of these reports were short-term (≤30 days), and three of these reports were long-term (>30 days) [5]. In patients with AHF, TLV had no effect on either short-term or long-term all-cause mortality when compared to the control. Similar results can be seen in a study by Konstam 2007 [8], showing Long-term Tolvaptan treatment had no effect, either favorable or unfavorable, on all-cause mortality or the combined endpoint of cardiovascular mortality or subsequent hospitalization for worsening HF. Also, according to Konstam 2017 [20] For clinical outcomes during the 30-day follow-up, there were no differences in changes in the Mini-Mental Status Score, days alive out of hospital, HF re-hospitalization, or death. Ono et al. 2018 [21] also found no significant effect of Tolvaptan on reducing risk or mortality By Felker 2016 [19] also there were no significant differences in WHF between those randomized to Tolvaptan, but the greater volume and weight loss seen with randomization to Tolvaptan was achieved and was associated with a greater incidence of worsening renal function (increased in serum Creatinine >0.3 mg/dl) within 72 h compared with placebo.
This meta-analysis revealed that Tolvaptan significantly reduced body weight and improved the volume overload condition in patients with heart failure without having a serious negative impact [5]. Konstam 2007 [8] showed In patients with baseline pedal edema, edema scores significantly improved at day 7 or discharge in patients receiving Tolvaptan compared with placebo. Matsuzaki phase 3 trial [11] Compared with placebo, Tolvaptan administered for 7 days significantly reduced body weight and improved symptoms associated with volume overload. Gheorghaide 2007 trial A and B [22] Edema at day 7 or discharge improved significantly with Tolvaptan in trial B but did not reach significance in trial A. Nevertheless, two days after starting Tolvaptan treatment, a prior study revealed that the body weight loss of HF patients was gradually restored, and there was no discernible difference between the Tolvaptan and placebo groups [5,7]. A study by Felker 2016 [19] Similar to what was seen in the randomized DOSE trial, as mentioned, the greater volume and weight loss was seen with randomization to Tolvaptan but it was associated with a greater incidence of worsening renal function compared with placebo. By matsuzaki 2011 phase two trial [11] The decrease in body weight from baseline was significantly greater compared with that in the placebo group. Matsuzaki 2011 phase 3 trial [11] Compared with placebo, Tolvaptan administered for 7 days significantly reduced body weight and improved symptoms associated with volume overload to Konstam 2017 [20] the Tolvaptan group had greater weight loss than the placebo group. Gheorghaide 2003 [10] study In patients with CHF, Tolvaptan was well tolerated; it was shown to be reducing body weight, and also in Udelson 2011 [9] study A decrease in body weight with Tolvaptan. At the same point, the placebo group showed a body weight increase. Gheorghaide 2007 [22] study Mean (SD) body weight reduction was greater with Tolvaptan
Serious ADR was also taken note of but wasn’t included in our analysis. However, it is worth noting that Konstam study 2017 [20] showed that compared with the placebo group, patients randomized to Tolvaptan had numerically fewer cardiac failure and hypotension events, numerically higher events of hypernatremia but similar frequency when it comes to renal events.
Konstam 2007 [8] showed findings of sustained reduction in body weight, without worsening of renal function and with sustained normalization of serum sodium levels in patients with baseline hyponatremia, which suggested longer-term or intermittent Tolvaptan treatment at least for the patients in whom abnormalities in fluid and electrolyte balance and/or renal function are difficult to manage by any other means. A role for long-term therapy was also suggested by the favorable findings. Events that occurred more commonly in the Tolvaptan group were dry mouth and thirst. In addition, hypernatremia occurred in 1.7% of Tolvaptan patients which compared to the Placebo group was 0.5%. The incidences of renal failure and hypotension were comparable in the 2 groups in the research paper. Compared with baseline measurements, heart rate and blood pressure both trended downward, slightly and similarly, in the 2 groups.

Table 1.
Description of papers.
| No | Study | Quality | Type of Study | Year of publishing | Place of research | Sample Size | Time Period of Data Collection | Intervention | Follow Up |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Felker 2016 [19] | Good | RCT | 2017 | USA | 257 | at 0,24,48 hours of giving medication | Tolvaptan/Control | 48 hours after administration |
| 2 | Gheorghiade 2007 TRIALA [22] | Good | RCT | 2007 | USA and Europe | 2048 | from Oct 7 2003 to Feb3 2006 | Tolvaptan/Placebo | 7 days |
| 3 | Gheorghiade 2007 TRIALB [22] | Good | RCT | 2007 | USA and Europe | 2058 | from Oct 7 2003 to Feb3 2006 | Tolvaptan/Placebo | 7 days |
| 4 | Gheorghiade et al 2003 [10] | Good | RCT | 2003 | USA | 254 | Tolvaptan/Placebo | 25 days | |
| 5 | Gheorghiade et al 2004 [15] | Good | RCT | 2004 | USA and Argentina | 319 | 60 days | Tolvaptan/Placebo | 60 days |
| 6 | Haught et al 2008 [23] | Good | RCT | 2008 | USA | 181 | Tolvaptan/Placebo | ||
| 7 | Hauptamn 2013 [24] | Good | RCT | 2013 | USA | Tolvaptan/Placebo | |||
| 8 | Jujo et al 2016 [14] | Good | RCT | 2016 | Japan | 60 | Tolvaptan/Control | 5days | |
| 9 | Konstam et al 2007 [8] | Good | RCT | 2007 | USA | 4133 | from Oct 7 2003 to Feb3 2006 | Tolvaptan/Placebo | long term |
| 10 | Konstam et al 2008 [23] | Good | Tolvaptan/Placebo | ||||||
| 11 | Konstam et al 2017 [20] | Good | RCT | 2017 | USA | 250 | Tolvaptan/Placebo | 3 days | |
| 12 | Li ling et al 2011 [12] | Good | RCT | 2011 | China | 65 | 0,4,7 days | Tolvaptan/13Placeb14o | 7 days |
| 13 | Matsue et al 2016 [25] | Good | RCT | 2016 | Japan | 217 | Tolvaptan/Control | 2 days | |
| 14 | Matsue et al 2013 [26] | Good | Observational study | 2013 | Japan | 114 | 0,24,48 hrs | Tolvaptan/Control | 2 days |
| 15 | Matsuzaki et al 2011 [11] | Good | RCT | 2011 | Japan | 117 | 7 days | Tolvaptan/Placebo | 7 days |
| 16 | Ono et al 2018 [21] | Good | Observational study | 2018 | Japan | 58 | Tolvaptan/Control | 6 months | |
| 17 | Shanmugam et al 2016 [17] | Good | RCT | 2016 | India | 51 | Tolvaptan/Placebo | 4 days | |
| 18 | Suzuki 2013 [27] | Good | RCT | 2013 | Japan | 109 | Tolvaptan/Control | ||
| 19 | Tamaki et al 2017 [16] | Good | RCT | 2017 | Japan | 50 | Tolvaptan/Control | 2 days | |
| 20 | Udelson et al 2007 [13] | Good | RCT | 2008 | USA | 181 | Tolvaptan/Placebo | 1 day | |
| 21 | Udelson et al 2011 [9] | Good | RCT | 2011 | USA | 83 | Tolvaptan/Placebo | 2 days | |
| 22 | Vadugnathan 2012 [18] | Good | RCT | 2012 | USA | 759 | Tolvaptan/Placebo | 7 days |
Conclusion
Although Tolvaptan may significantly reduce edema, and congestive symptoms and decrease body weight, it has no impact on all-cause mortality and worsening renal function in heart failure. It is and should be widely used hence in the early stages of diseases along with drugs that can modify all-cause mortality and worsening renal function to manage disease progression.
Funding
None of the authors have a financial interest in any of the products, devices, or drugs mentioned in this manuscript.
Institutional Review Board Statement
Being a meta analysis, there were no ethical issues and IRB permission is not required.
Conflicts of Interest
The authors declare no conflict of interest.
References
- E Alskaf AT, A Al-Mohammad,. Tolvaptan for Heart Failure, Systematic Review and Meta-Analysis of Trials 2016 [Available from: https://pubmed.ncbi.nlm.nih.gov/27159621/.
- Izumi Y MK, Iwao H,. Therapeutic Potential of Vasopressin-Receptor Antagonists in Heart Failure 2014 [Available from: https://pubmed.ncbi.nlm.nih.gov/24401675/.
- Steven R Goldsmith MG. Vasopressin antagonism in heart failure 2005 [Available from: https://pubmed.ncbi.nlm.nih.gov/16286160/. 1628.
- Takanori Yamazaki YI, Yasuhiro Nakamura, Naoto Yamashita, Hiroyuki Fujiki, Mayuko Osada-Oka, et al. Tolvaptan improves left ventricular dysfunction after myocardial infarction in rats 2012 [Available from: https://pubmed.ncbi.nlm.nih.gov/22984091/.
- Chunbin Wang BX, Lin Cai. Effects of Tolvaptan in patients with acute heart failure: a systematic review and meta-analysis 2017 [Available from: https://link.springer.com/article/10.1186/s12872-017-0598-y. [CrossRef]
- Punniyakoti T Veeraveedu SSP, Ken'ichi Yamaguchi, Yutaka Komai, Rajarajan A Thandavarayan, Vijayakumar Sukumaran, et al. Arginine vasopressin receptor antagonists (vaptans): pharmacological tools and potential therapeutic agents 2010 [Available from: https://pubmed.ncbi.nlm.nih.gov/20708094/.
- Xiong B HY, Tan J, Yao Y, Wang C, Qian J, et al. The short-term and long-term effects of tolvaptan in patients with heart failure: a meta-analysis of randomized controlled trials 2015 [Available from: https://pubmed.ncbi.nlm.nih.gov/26334632/#affiliation-1.
- Marvin A Konstam MG, John C Burnett Jr, Liliana Grinfeld, Aldo P Maggioni, Karl Swedberg, et al. Effects of oral tolvaptan in patients hospitalized for worsening heart failure: the EVEREST Outcome Trial 2007 [Available from: https://pubmed.ncbi.nlm.nih.gov/17384437/.
- James E Udelson MB, Paul J Hauptman, Rafael Sequeira, Ignatius Thomas, Terrence O'Brien, et al. A multicenter, randomized, double-blind, placebo-controlled study of tolvaptan monotherapy compared to furosemide and the combination of tolvaptan and furosemide in patients with heart failure and systolic dysfunction 2011 [Available from: https://pubmed.ncbi.nlm.nih.gov/22123358/.
- Mihai Gheorghiade IN, John Ouyang, Frank Czerwiec, Jun-ichi Kambayashi, Manuela Zampino, et al. Vasopressin V2-receptor blockade with tolvaptan in patients with chronic heart failure: results from a double-blind, randomized trial 2003 [Available from: https://pubmed.ncbi.nlm.nih.gov/12742979/.
- Masunori Matsuzaki MH, Tohru Izumi, Masatake Fukunami,. Efficacy and safety of tolvaptan in heart failure patients with volume overload despite the standard treatment with conventional diuretics: a phase III, randomized, double-blind, placebo-controlled study (QUEST study) 2011 [Available from: https://pubmed.ncbi.nlm.nih.gov/22120092/. [CrossRef]
- Li Ling ZW, Bai Hua,. The efficacy and safety of tolvaptan on treating congestive heart failure patients with hyponatremia 2011 [Available from: https://heart.bmj.com/content/97/Suppl_3/A127.1.
- James E Udelson FAM, Enrique Flores, Hassan Ibrahim, Stewart Katz, Gregory Koshkarian, et al. Multicenter, randomized, double-blind, placebo-controlled study on the effect of oral tolvaptan on left ventricular dilation and function in patients with heart failure and systolic dysfunction 2007 [Available from: https://pubmed.ncbi.nlm.nih.gov/17543634/.
- Kentaro Jujo KS, Issei Ishida, Yuho Furuki, Ahsung Kim, Yuki Suzuki, et al. Randomized pilot trial comparing tolvaptan with furosemide on renal and neurohumoral effects in acute heart failure 2016 [Available from: https://pubmed.ncbi.nlm.nih.gov/27818782/.
- Mihai Gheorghiade WAG, Christopher M O'Connor, Kirkwood F Adams Jr, Uri Elkayam, Alejandro Barbagelata, et al. Effects of tolvaptan, a vasopressin antagonist, in patients hospitalized with worsening heart failure: a randomized controlled trial 2004 [Available from: https://pubmed.ncbi.nlm.nih.gov/15113814/.
- Shunsuke Tamaki YS, Takahisa Yamada,Takashi Morita,Yoshio Furukawa,Yusuke Iwasaki, et al. Tolvaptan Reduces the Risk of Worsening Renal Function in Patients With Acute Decompensated Heart Failure and Preserved Left Ventricular Ejection Fraction - Prospective Randomized Controlled Study 2017 [Available from: https://pubmed.ncbi.nlm.nih.gov/28202885/.
- Elangovan Shanmugam CRMPD, Melvin George, Amrita Jena, Muthukumar Rajaram, Balaji Ramaraj, et al. Effect of tolvaptan on acute heart failure with hyponatremia – A randomized, double blind, controlled clinical trial 2016 [Available from: https://www.sciencedirect.com/science/article/pii/S0019483215002394.
- Muthiah Vaduganathan MG, Peter S Pang, Marvin A Konstam, Faiez Zannad, Karl Swedberg, et al. Efficacy of oral tolvaptan in acute heart failure patients with hypotension and renal impairment 2012 [Available from: https://pubmed.ncbi.nlm.nih.gov/22673023/.
- G Michael Felker RJM, Robert T Cole, Kirkwood F Adams, Gregory F Egnaczyk, Mona Fiuzat, et al. Efficacy and Safety of Tolvaptan in Patients Hospitalized With Acute Heart Failure 2017 [Available from: https://pubmed.ncbi.nlm.nih.gov/27654854/.
- Marvin A Konstam MK, Arthur Chandler, Ravi Dhingra, Freny Vaghaiwalla Mody, Howard Eisen, et al. Short-Term Effects of Tolvaptan in Patients With Acute Heart Failure and Volume Overload 2017 [Available from: https://pubmed.ncbi.nlm.nih.gov/28302292/.
- Yohei Ono HT, Masahiro Inoue, Yukio Mabuchi, Tetsuya Ueda, Tadashi Suzuki, et al. Clinical effect of long-term administration of tolvaptan in patients with heart failure and chronic kidney disease 2018 [Available from: https://pubmed.ncbi.nlm.nih.gov/29998996/.
- Mihai Gheorghiade MAK, John C Burnett Jr, Liliana Grinfeld, Aldo P Maggioni, Karl Swedberg, et al. Short-term clinical effects of tolvaptan, an oral vasopressin antagonist, in patients hospitalized for heart failure: the EVEREST Clinical Status Trials 2007 [Available from: https://pubmed.ncbi.nlm.nih.gov/17384438/. [CrossRef]
- James E Udelson CO, John Ouyang, Holly Krasa, Christopher A Zimmer, Geir Frivold, et al. Acute hemodynamic effects of tolvaptan, a vasopressin V2 receptor blocker, in patients with symptomatic heart failure and systolic dysfunction: an international, multicenter, randomized, placebo-controlled trial 2008 [Available from: https://pubmed.ncbi.nlm.nih.gov/19007589/.
- Paul J Hauptman JB, Mihai Gheorghiade, Liliana Grinfeld, Marvin A Konstam, Dusan Kostic, et al. Clinical course of patients with hyponatremia and decompensated systolic heart failure and the effect of vasopressin receptor antagonism with tolvaptan 2013 [Available from: https://pubmed.ncbi.nlm.nih.gov/23743487/.
- Yuya Matsue MS, Sho Torii,Satoshi Yamaguchi,Seiji Fukamizu,Yuichi Ono, et al. Clinical Effectiveness of Tolvaptan in Patients With Acute Heart Failure and Renal Dysfunction 2016 [Available from: https://pubmed.ncbi.nlm.nih.gov/26915749/.
- Yuya Matsue MS, Mie Seya, Ryota Iwatsuka, Akira Mizukami, Wataru Nagahori, et al. Tolvaptan reduces the risk of worsening renal function in patients with acute decompensated heart failure in high-risk population 2013 [Available from: https://pubmed.ncbi.nlm.nih.gov/23159210/.
- Satoshi Suzuki AY, Takayoshi Yamaki, Koichi Sugimoto, Hiroyuki Kunii, Kazuhiko Nakazato, et al. Acute heart failure volume control multicenter randomized (AVCMA) trial: comparison of tolvaptan and carperitide 2013 [Available from: https://pubmed.ncbi.nlm.nih.gov/24142853/.
Figure 1.
All Cause Mortality; Figure 1.1: (Controls) All-Cause Mortality; Figure 1.2: (Placebo) All-Cause Mortality.
Figure 1.
All Cause Mortality; Figure 1.1: (Controls) All-Cause Mortality; Figure 1.2: (Placebo) All-Cause Mortality.
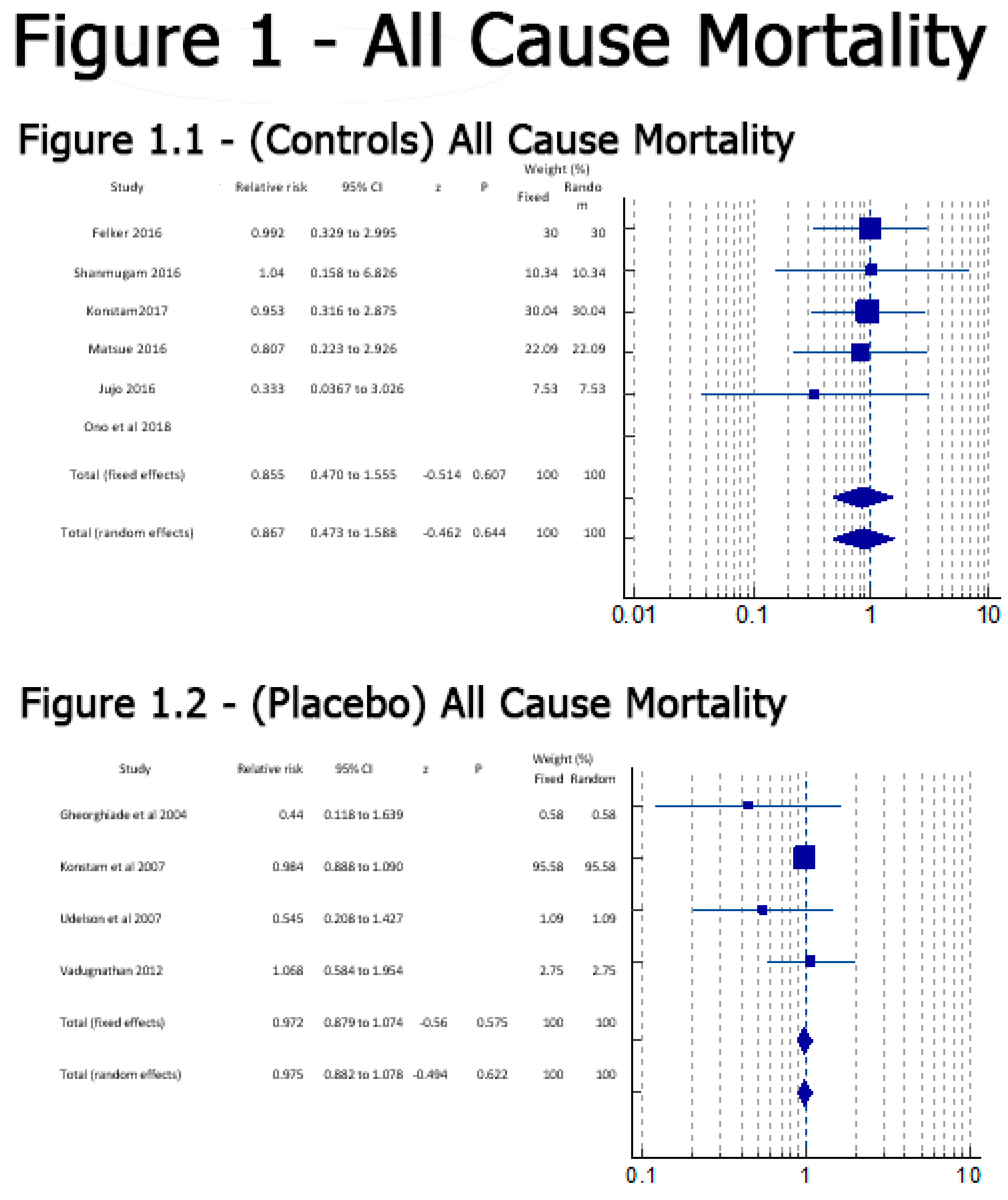
Figure 2.
(Placebo) Serious ADR.
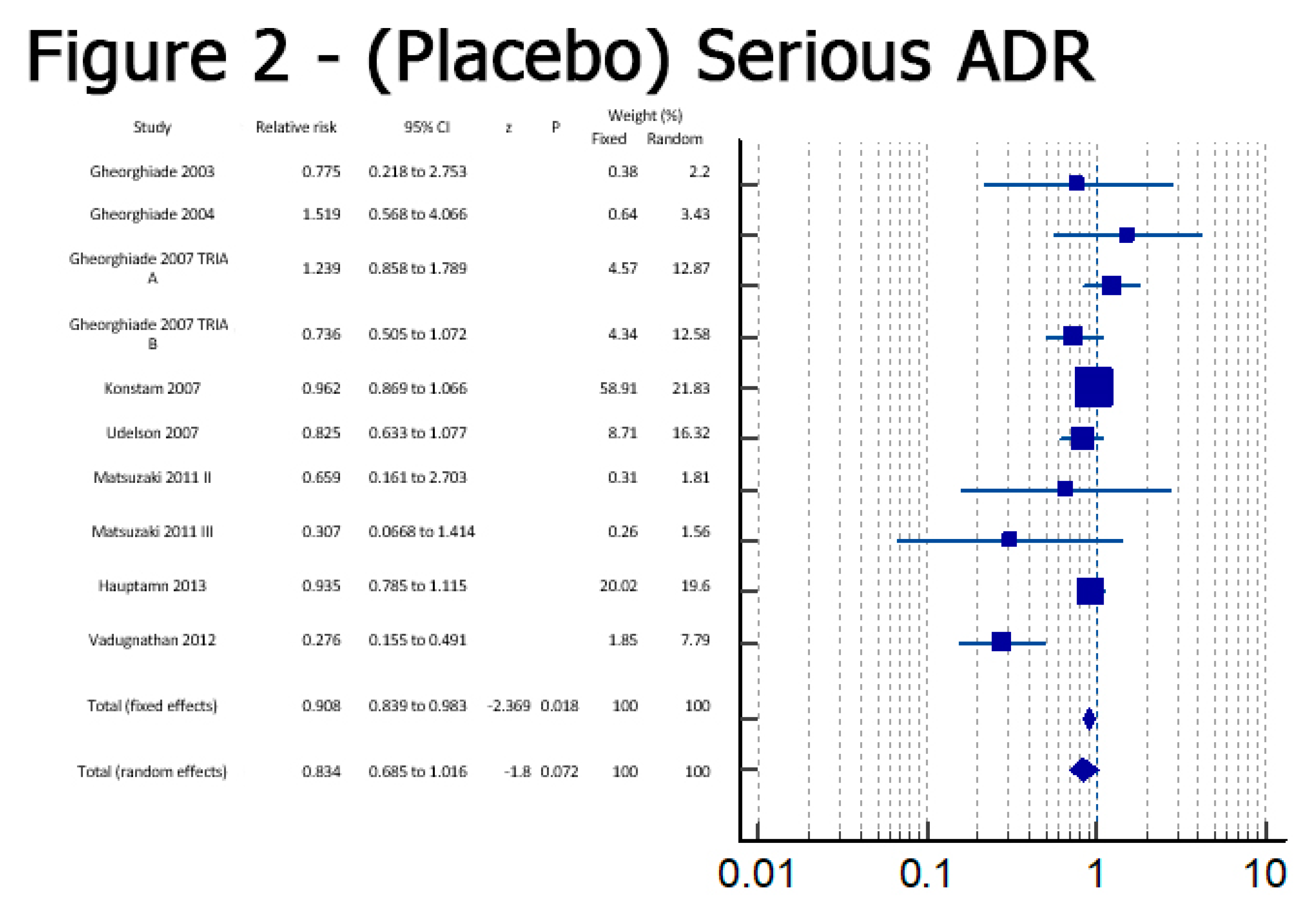
Figure 3.
Worsening RF; Figure 3.1: (Placebo) Worsening RF; Figure 3.2: (Control) Worsening RF.
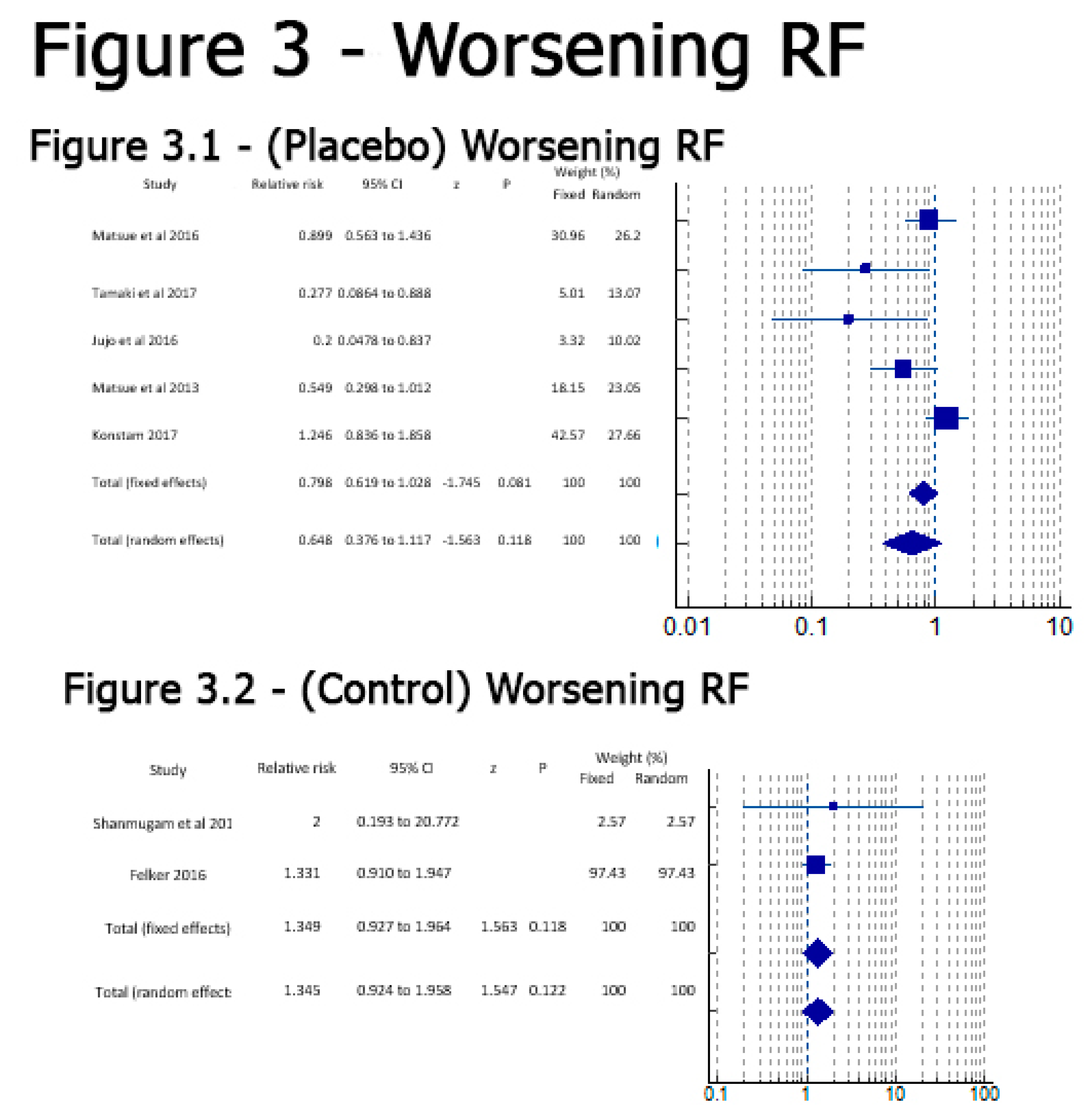
Figure 4.
(Placebo) Edema.
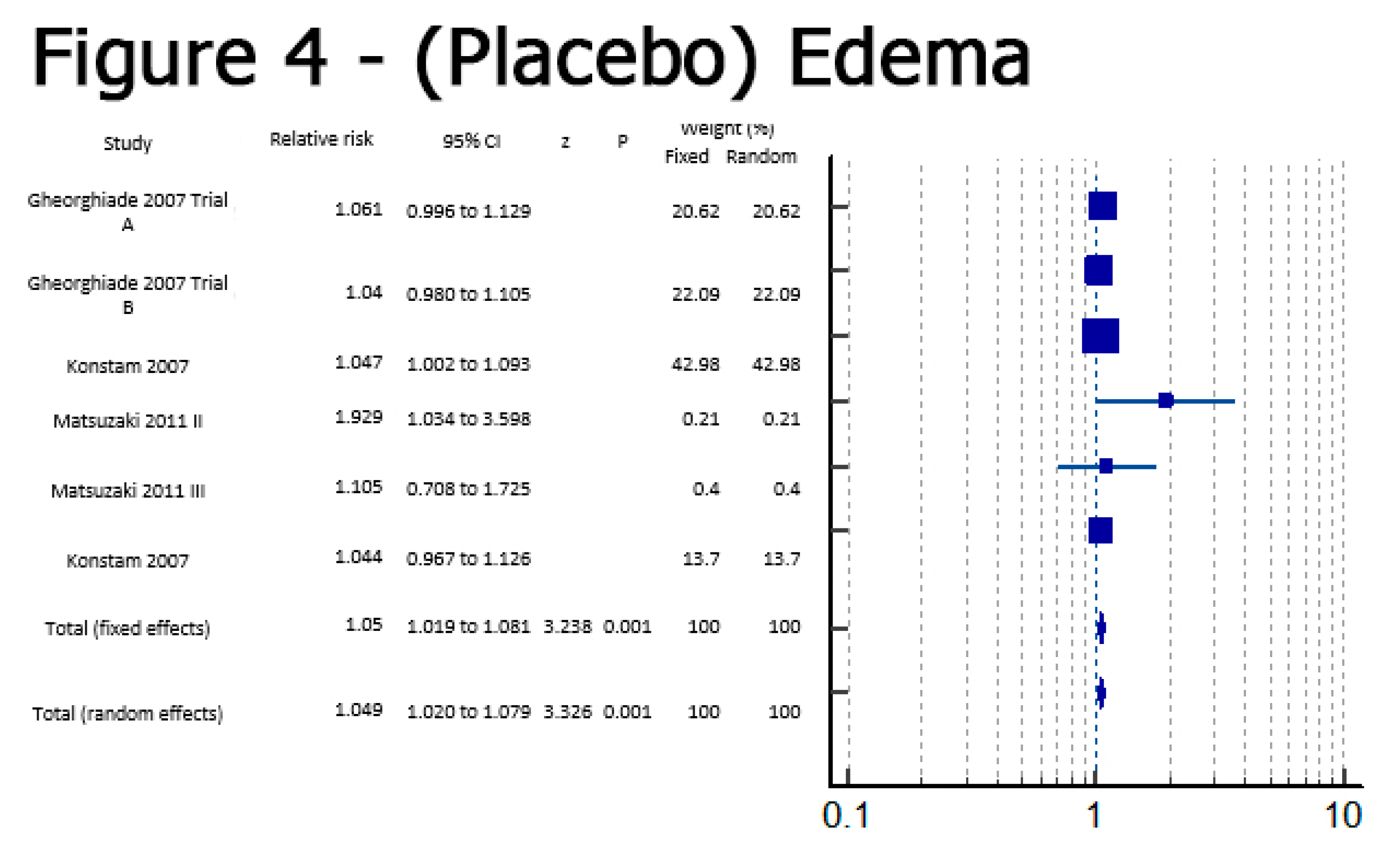
Figure 5.
(Placebo) Na Levels.
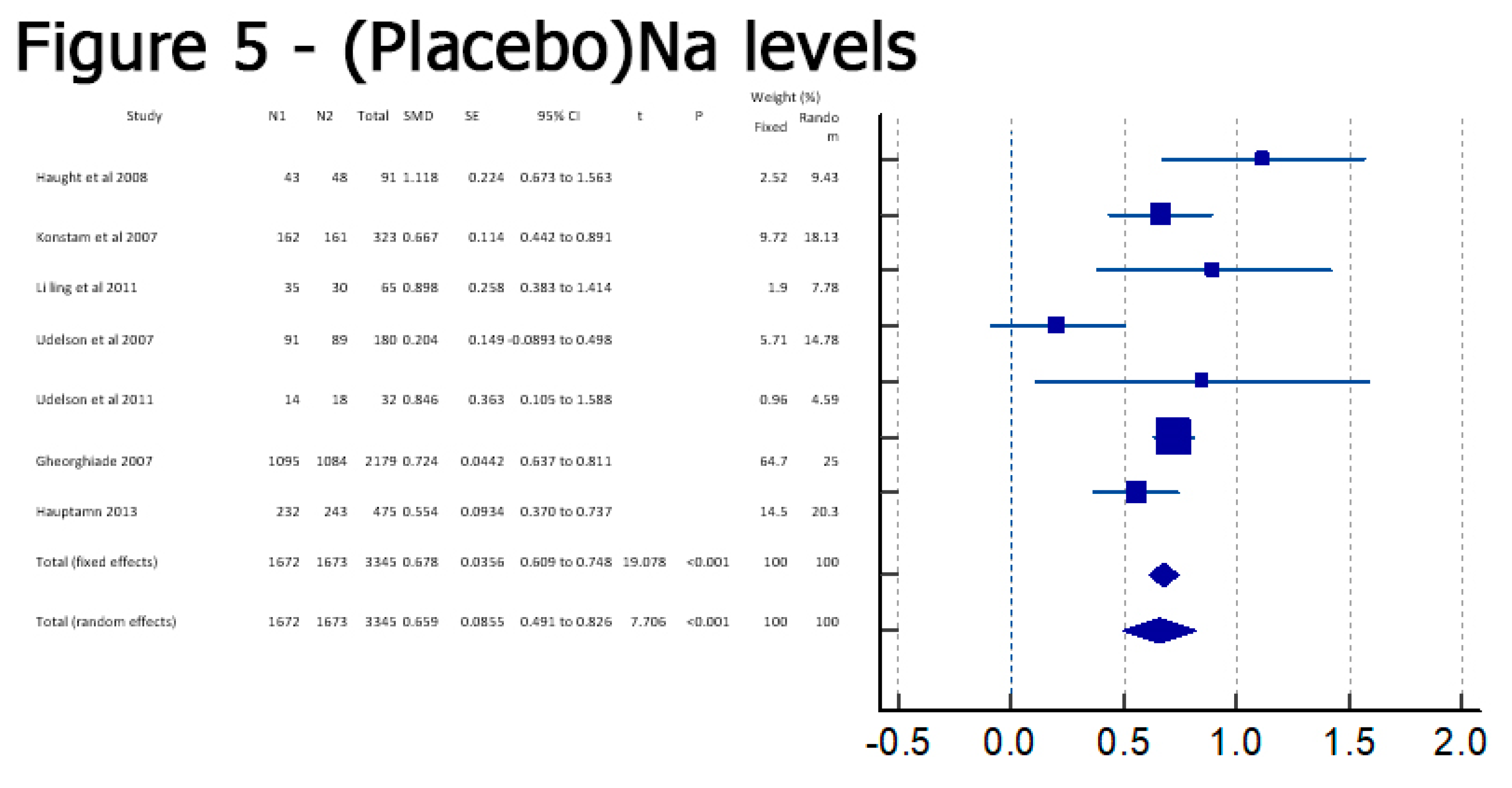
Figure 6.
Bodyweight; Figure 6.1: (Controls) Body Weight; Figure 6.2: (Placebo)Bodyweight.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



