Submitted:
20 December 2023
Posted:
20 December 2023
You are already at the latest version
Abstract
Background: Phimosis is the inability to completely retract the foreskin and expose the glans. The treatment of phimosis varies depending on the age of the patient and the severity of the disease; a great number of conservative or surgical treatments are currently available.
Aim: To provide the first review summarizing the available options for the treatment of adult phimosis.
Methods: A PubMed, Cochrane and Embase search for peer-reviewed studies, published between January 2001 - December 2022 was performed using the search terms “phimosis AND treatment”.
Results: A total of 288 publications were initially identified through database searching. Thirty manuscripts were ultimately eligible for inclusion in this review.
Conservative treatment is an option and it includes topical steroid application and the new medical silicon tubes (Phimostop™) application for gentle prepuce dilation.
Concerning the surgical approach, the gold-standard treatment is represented by circumcision in which tissue synthesis after prepuce removal can be also obtained with barbed sutures, fibrin glues or staples. Laser circumcision seems providing superior outcomes in terms of operative time and postoperative complication rate when compared to the traditional one.
Several techniques of preputioplasty and use of in-situ devices (which crush the foreskin and simultaneously create haemostasis) have been also described. These in-situ devices seem feasible, safe and effective in treating phimosis while they also reduce the operative time when compared to the traditional circumcision.
Patient satisfaction rates, complications and impact on sexual function of the main surgical treatments are presented.
Conclusion:
Many conservative and surgical treatments are available for the treatment of the adult phimosis. The choice of the right treatment depends on the grade of phimosis, results, complications, and cost-effectiveness.
Keywords:
phimosis
; foreskin
; circumcision
; penis
; lichen sclerosus
1. INTRODUCTION
Phimosis is defined as the inability to completely retract the foreskin and expose the glans. This common condition can be congenital (primary, without signs of scarring) or acquired (secondary and pathological); the latter as a consequence of local inflammation (recurrent balanitis or balanoposthitis) or infections due to poor hygiene [1]. Some diseases like diabetes mellitus and lichen sclerosus (LS) could also cause phimosis [2,3]. It is mostly common in children in the first decade of life with a second peak of incidence occurring after the sixth decade of life [4].
The treatment of phimosis varies depending on the age of the patient and severity of disease. Conservative treatment is an option both in congenital and acquired phimosis, especially if grade 0-2 [5,6].
About surgical approach, circumcision remains the gold-standard. Circumcision is considered a simple surgical procedure; however, an overall complication risk of 3.8% has been reported [7]. Bleeding, pain, urinary retention, recurrent phimosis, redundant skin, wound infection, necrosis, fistulas, iatrogenic hypospadias and epispadias, meatitis, meatal stenosis, concealed penis [8], non-satisfying cosmetic appearance, and impotence are the described complications, most of which may significantly impact on healthcare costs and on patient’s quality of life [9,10,11].
In an effort to maintain the efficacy and reduce the risk of complications, other more conservative surgical techniques (dorsal incision, partial circumcision, preputioplasty) [12,13,14] and use of several in-situ devices which crush the foreskin and simultaneously create haemostasis have been described.
To the best of our knowledge, this narrative review is the first paper providing an overview of all therapies, surgical techniques and devices for the treatment of phimosis in the adult setting.
1. MATERIALS AND METHODS
We performed a PubMed, Cochrane and Embase search for peer-reviewed studies, published between January 2001-December 2022. The following search terms were used used to detect all full-text publications written in English: “phimosis AND treatment”. Two authors (ADA and ER) independently screened the titles and abstracts of each citation. The reference lists of the eligible articles were reviewed, and the “Related citations” PubMed feature was also utilized. Manuscripts have been assessed according to their level of scientific evidence (Oxford Center for Evidence-based Medicine).
Cohort and case control studies as well as randomized trials were included. Case reports, review articles and abstracts not followed by full text were excluded. Finally, studies referring on paediatric (exclusively) or female cohort, as well as studies referring on animal models were excluded.
1. RESULTS
A total of 288 publications were initially identified through database searching. Thirty manuscripts were ultimately eligible for inclusion in this review. Figure 1 provides a diagram on the flow of information through the different phases of this systematic review according to the PRISMA criteria [15].
Fourteen studies (46,7%) were classified as case-series [4], [16,17,18,19,20,21,22,23,24,25,26,27,28] and 6 studies (20,0%) were classified as case-comparative series, in both cases with a retrospective evaluation of the reported data [29,30,31,32,33,34]. Finally, 10 (33,3 %) were prospective case–control studies [6], [35,36,37,38,39,40,41,42,43].
3.1. CONSERVATIVE TREATMENTS
3.1.1. Topical corticosteroids
Non-surgical treatment of adult phimosis (Table 1) is principally based on the application of topical corticosteroids of different potency and concentration for 4–8 weeks [5]. The guidelines for the management of lichen sclerosus, an autoimmune, inflammatory dermatosis, that usually lead to tightening of the foreskin in male adult and children, sometimes causing phimosis, recommend the use of a very potent corticosteroid ointment or cream (e.g. clobetasol propionate 0.05% cream or ointment) [44] (Table 2) with significant improvement in discomfort and skin tightness, reducing the need for circumcision.
Compared to placebo or manual reduction, corticosteroids significantly increase complete or partial clinical resolution of phimosis, but there it not long-term follow-up data on the durability of the results [45,46,47]. However, these drugs could induce skin atrophy (skin thinning, desirable only for the management of LS), telangiectasia (distended blood capillaries giving a spidery red spot) and immunosuppression (increasing the risk of malignancy) [44].
3.2.2. The Platelet-rich plasma (PRP) for lichen sclerosus (LS)
A single retrospective study used the PRP as II line treatment of LS in patients with poor outcome after long-term treatment with ultra-potent steroids (standard treatment) [22].
PRP contains several different growth factors which play a key role in the stimulation and regulation of wound healing. As described, a blood sample of 50 ml was drawn from the patient to obtain approximately 5 ml of PRP. About 2cc (range 1–3 cc) of PRP per treatment was injected in the affected areas followed by application of local antibiotic ointment. In all patients, a significant improvement in clinical conditions was observed with reduction or even disappearance of symptoms; only one patient required a circumcision procedure. Both the Investigator’s Global Assessment and the Dermatology Life Quality Index scores showed a significant difference before and after the treatment. A strict follow-up was recommended by the authors in order to detect the onset of malignant disease although no study has documented that PRP promotes carcinogenesis [22].
3.2.3. PhimoStop™
PhimoStop™ (Phimomed S.r.l., Rome, Italy) is a certified medical device consisting of 22 medical silicone tuboids designed to apply the well-established technique of progressive and gentle skin dilation to the phimotic ring and solve phimosis without circumcision (Figure 2) [6]. The silicone tuboids are of increasing size: once the foreskin has been fully retracted, the tuboid can be applied on the glans with the central hole overlaying the urethral meatus, allowing the patient to urinate without removing the device [6]. The inner foreskin is then pulled back alongside the lateral aspect of the tuboid. Thus, the phimotic ring lies on the cylindrical portion of the tuboid undergoing a slightly forced and progressive dilation. Through the constant application of PhimoStop™, the scar ring is weakened and thinned, allowing the growth of new elastic cells that replace, in a short period of time, the inelastic ones. A single-center prospective study evaluated the effectiveness of the device in both the short and long-term follow-up on 85 patients with acquired phimosis (grade ≤2 according to Kikiros) and indication for circumcision [6]. Primary outcome was to avoid circumcision in 30% of the patients [6]. The study was completed by 71/85 (83%) patients. The median duration of application of the PhimoStop™ device was 60 days. The main objective was largely achieved, since more than half (37/71, 52%) of the patients had no indication for circumcision after treatment. 31/37 (81%) patients who avoided circumcision maintained good outcomes at a median follow-up of 24 months. Finally, side-effects were scarce, and in most cases, they were represented by discomfort with larger tuboid size [6].
1. Surgical treatments
4.1. Circumcision
Male circumcision seems to be one of the oldest surgical procedures, and it has been practiced since ancient times for medical or non-medical reasons (religious in Jewish, Muslim, and traditional African cultures, social, cultural and personal reasons). Importantly, voluntary medical male circumcision (VMMC) is a key World Health Organization (WHO) HIV preventive intervention. It is estimated that 37-39% of men worldwide are circumcised[5].
In United States, the adult circumcision varied significantly across the age ranges and geographic regions; the most common indications for adult are phimosis (52.5%), routine/ritual circumcision (28.7%), phimosis + balanitis/balanoposthitis (6.8%), balanitis (3.8%) and balanoposthitis (2.6%) [15]. Also, dyspareunia may represent a frequent indication for circumcision [19].
4.1.1. Techniques of circumcision
In men and older boys, the best technique seems to be the sleeve circumcision (Figure 3). In clinical practice, the incision line should be extended straight across the base of the frenulum, thought the dartos fascia to the superficial lamina of the Buck fascia. After foreskin reduction, a second incision is marked, following the outline of the coronal margin and the V of the frenulum on the ventral side. The frenulum usually retracts into a V. Frenuloplasty without circumcision is not considered a gold standard treatment, but it can be used in young patients who want to avoid or postpone total circumcision [21].
In a randomized multicentre clinical trial, Jiang ZL et al describe a novel technique of circumcision, which retains more prepuce while sparing the frenulum. The 2 layers (internal and external plates) were cut off separately so that the adhering blood vessels could be stripped off [35]. Compared to the conventional dissection, the new technique provided significantly less wound healing time, scar width and recovery time, while the intraoperative bleeding volume, surgical time, and the rate of satisfaction with appearance of the penis was significantly higher. The cost of surgery to the 2 groups was similar [35].
Pagano C et al proposed a dissection of deep fascia after conventional circumcision to improve length and circumference of the penis in a retrospective study on 36 male patients [20]. A two-step surgical procedure was described: the first step consisted in a conventional circumcision; in the second step the skin of the penis body was retracted to the base showing ventrally the presence of the areolar tissue and Buck’s Fascia and adherent bridles were identified and bluntly dissected. A relaxation of the adherences of the Buck’s fascia of penis and a decompression of the corpora cavernosa were obtained, causing an improvement of penile length and circumference [20].
Beside to the tradition sutures for sleeve circumcision, barbed sutures, biologic glues and staplers have been used to obtain tissue synthesis after surgery. The Quill™ Knotless Tissue- Closure Device (Quill™ Device) is a unique bidirectional barb which can be fixed bidirectionally within the wound [48]. Gu C et al performed 70 consecutive cases of sleeve circumcision by a single surgeon using the Quill™ device (3/0 – 4/0) via subcuticular suture to reduce suture marks on the skin of the penis. The sutures were first placed through the skin of the frenulum and the outer dorsal layer of preputial skin. Complications included one case of minor postoperative hematoma (1.4%), one case of wound infection (1.4%) and one case of pain during intercourse. All three patients (4.3%) were managed conservatively. The ultimate cosmetic results were to the satisfaction of both the patients and the surgeon [27].
The use of fibrin glue in medicine is not new and its effect is to promote the natural clotting pathway without causing foreign body or fibrosis reactions. It has widespread use in emergency departments particularly in children [49]. D’Arcy FT et al report a series of 38 men circumcised using a fibrin glue, DERMABOND (2-octyl cyanoacrylate from ETHICON): after removing the outer and inner prepuce and obtaining hemostasis, the wound is approximated by using 2–5 ml of fibrin glue, handing out the glue with the tip of the applicator. Care should be taken to avoid the external urethral meatus [23]. The glue dries approximately 20 seconds after application [23]. All patients were satisfied with the procedure and outcome except for one patient who developed an allergic reaction, one developed a self-limiting postoperative bleed and other one a focal dehiscence that required no operative intervention[23].
Circumcision staple devices can simultaneously fulfill foreskin cutting and suturing. Disposable circumcision suture devices appeared in China in 2013 and then these have spread worldwide [27].
All devices consist of bell-shaped glans pedestal, suture staple, ring-shaped blade, handle, and shell; different size devices are available. For phimosis patients with a small preputial ostium, the foreskin may be cut with scissors to help the inner rod insertion. The blade cut the foreskin instantly, while simultaneously staples are placed by tightening the knob at the bottom for 3–5 s and then releasing it.
Shen J et al compared circumcisions using two different disposable suture devices: Group A using Langhe circumcision suture devices (Jiangxi Langhe Medical Instrument Co., Ltd.) and group B using Daming circumcision suture devices (Jiangsu Changshu Henry Medical Instrument Co., Ltd)[33]. There are some differences between devices’ suturing technique: Daming device incorporates a pressure by plastic sheet upon the incision wound and the staples fix the wound outside the plastic sheet; Langhe device directly fixes the incision wound with the staples[33]. The intraoperative blood loss of group A was higher than of group B and 2 cases from group A underwent second operation. On the other hand, Group B was characterized by longer staple-shedding time after surgery and these patients also suffered longer postoperative edema, especially on the site of frenulum of prepuce, greater postoperative pain and higher incidence of postoperative infection[33].
Lv BD et al conducted a prospective randomized trial to assess the benefits of a new disposable circumcision suture device (DCSD, Jiangxi Yuansheng Lang He Medical Instrument Co., Ltd. Ji’an, China): 942 patients were equally divided into three groups (conventional circumcision, Shang ring and disposable suture device group) [36]. Operation time and intra-operative blood loss, intra-operative and post-operative pain were significantly lower in the Shang ring and suture device groups compared to the conventional group. Patients in the suture device (80.57%) and Shang ring (73.57%) groups were more satisfied with penile appearances compared with the conventional circumcision group (20.06%, P<0.05) [36]. The authors concluded that their modification of the traditional anesthetic and surgical methods of circumcision reduced the number of incidences of post-operative complications, intra-operative and post-operative pain and improved penile appearance and patient satisfaction [36].
Similar results are shown in a prospective non-randomized controlled study, using the same device (DCSD, Jiangxi Yuansheng Lang He Medical Instrument Co., Ltd. Ji’an, China), on 582 cases of excess foreskin and 62 phimosis patients that underwent circumcision (DCSC n = 295; conventional suture approach n = 287). Nevertheless, a multivariate logistic regression with likelihood ratio test revealed that phimosis was the significant predictor of edema occurrence postoperatively (p = 0.025) [37].
Han H. et al randomized 124 adult male patients to perform novel penile circumcision suturing devices (PCSD, Changshu Henry Medical Instrument Co., Ltd. in Jiangshu China) or SR (Shang Ring) circumcision: there were not significant differences in blood loss (P= 0.054), in VAS score evaluation at the operation time, at 6 or 24 hours after surgery (P>0.05) or in the rates of edema, hematoma and incision dehiscence; in the PCSD group wound healing times was significantly longer (30.2±4.9 vs. 15.7±3.0 days, P<0.01) but the cosmetic results was more satisfying (P<0.01) at three weeks after the operation. The mean costs (US dollars) for the two groups were 259.6±3.8 and 267.6±8.4 (P<0.01) [38].
Wang J et al compared the results obtained in patients treated with sleeve circumcision or device technique using Langhe device: no significant difference in postoperative pain, wound healing, or satisfaction were reported between the 2 groups for any day of follow-up (P>0.05) reducing operative time and blood loss [40].
Su Q et al compared the results of 241 male patients submitted to traditional circumcision (Group A=79), modified circumcision (dorsal slit, Group B=80) and disposable suturing device circumcision (TONCARE, Group C=82). The operation time and volume of blood loss in groups B and C were significantly lower than those in group A (P < 0.05). Groups A and B were superior to group C in terms of the 6-h postoperative visual analog scale score and appearance satisfaction (P < 0.05) but there were no differences in the 7-day postoperative pain score and total healing time (P > 0.05). The costs in groups A and B were lower than that in group C (P < 0.05) [29].
Beside to the conventional and device-based also the laser circumcision has been described. With the goals of complete removal of the foreskin, fine hemostasis, wound healing, cosmetics and patients’ satisfaction, the laser circumcision has been tested to both the pediatric and adult populations. To our knowledge, there is only one prospective randomized study including a pure adult population [43] and one retrospective study [34] including both adults and children.
The prospective randomized controlled clinical study [43] compared the conventional circumcision (150 patients) to the modified CO2 laser circumcision technique (150 patients). There was no statistically significant difference in age distribution and indications between the two groups. Compared with the conventional group, there were shorter operative time [21.1±2.7 vs 10.5±0.9, p<0.05], less blood loss and lower postoperative complication rate (mainly of postoperative pronounced oedema of the prepuce) in the laser group. The CO2 laser technique was associated with much less pain, as quantitated by a 10-point visual analogue scale pain score at both 1 day and 7 days postoperatively. The only disadvantage associated with the use of CO2 laser observed is the possible delay of wound healing compared with the conventional method. Wound dehiscence was observed in one patient in the laser group (vs none in the conventional circumcision), but the patient had had sexual intercourse at 23 days postoperatively, despite having been advised to avoid sexual intercourse for 6 weeks.
Ronchi et al retrospectively evaluated the medical records of 482 patients who had been circumcised under local anesthesia traditionally (168 patients-Group A) or using a CO2 laser (314 patients-Group B) [34]. Pain was evaluated using a verbal numerical rating scale for pain assessment. Postoperative wound swelling, bleeding, infection, and pain were assessed at 4 hours, 24 hours and 7 days after surgery. There were no significant differences between the two groups in terms of bleeding and infections. The operating times was significantly lower in group B (23.1±2.8 vs 12.8±0.9 minutes, p<0.001). Pain scores were low and there was less pain in Group B than in Group A during the first 4 hours (1.8 vs 3.7; p<0.002) as well as at 1 day (p<0.002) and 7 days (p<0.001) postoperatively. The cosmetic results were superior in Group B; a linear surgical scar developed in 94.9% of patients in Group B versus 61.3% in Group A (p<0.001). Finally, significantly lower rates of buried penis were observed in Group B (10.7% vs 2.9%, p <0.002). The authors concluded that the use of a CO2 laser was associated with a shorter operative time, less wound irritation and better cosmetic appearance compared with standard surgical techniques for circumcision.
4.1.2. Circumcision in elderly patients
In this category of patients, surgery is frequently associated to anxiety related to operation time and occurrence of bleeding.
In the Mu J et al study, 132 elderly males underwent circumcision with four different surgical methods: Group A (traditional male circumcision, n = 38), Group B (sleeve circumcision, n = 23), Group C (Shang Ring circumcision, n = 42), and Group D (suturing device circumcision, Jiangxi Yuanshenglang Medical Equipment Technology Co., Ltd., Yongfeng City, Jiangxi Province, China, n = 29) [32]. Group C (SR circumcision) exhibited the shortest operation time and the least blood loss but the longest healing time. Furthermore, some patients experimented incrustation and edema even after the SR was removed, due to the thicker foreskin in elderly males [32]. The findings of this study suggest that SR circumcision should be avoided in cases of prepuce with hyperplasia and hypertrophy and increased veins: in these cases, sleeve circumcision appeared to be the best treatment to avoid complications. Instead, short operation and recovery times, obtained by SR or stapler device reduce pain stimulation which could cause heart burden, myocardial ischemia, severe angina pectoris, and even myocardial infarction in elderly patients [32].
4.1.3. Effect of circumcision on sexual function
The evidence concerning the effect of circumcision on sexual function is lacking and the effect of surgery on the sensitivity of the glans and sexual pleasure are not known. Fink KS et al examined sexual function outcomes in men who have experienced sexual intercourse in the uncircumcised and circumcised conditions: of the responders 47% reported that sex was physically more pleasurable and 47% also said that their sex lives were more satisfying after circumcision; overall, 62% of men were satisfied with having been circumcised [24].
Czajkowski M et al investigated the effect of male circumcision on erectile function and satisfaction with the appearance of the genitals. The study outcomes were obtained using questionnaires such as visual analogue scale (0-10 for itching, burning, penile pain, and penile pain during intercourse), International Index of Erectile Function (IIEF-5) and Male Genital Self Image Scale 7 (MGSIS-7) to assess the changes in patients sexual functioning [50]. Before the circumcision, 59/69 patients (86%) reported some subjective symptoms of phimosis (in order of frequency pain during intercourse, itching and burning, penile pain) [50]. After 3 months from circumcision, subjective symptoms almost completely disappeared, and all patients achieved significant improvement in both obtaining and maintaining an erection (based on IIEF-5 score: 13.3 ± 9.5 vs 15.4 ± 10.2, p < 0.001). Also, satisfaction with genital self-image increased significantly (17 ± 4.3 vs 21.9 ± 4.2, p < 0.001) [50].
4.2. Preputial sparing techniques
4.2.1. Prepuce-sparing plasty and simple running suture
Prepuce-sparing techniques have been recently developed to improve the aesthetic outcomes of radical circumcision through an increased preservation of the penile foreskin.
Monarca C et al describe their 5 years’ experience of prepuce–sparing plasty in 52 patients that were eligible to undergo phimosis surgery [18]. The first incision is made on the external lamina of the prepuce; the second one on the internal lamina in an oblique opposite direction in order to allow the total removal of the phimotic ring and to increase the circumference of the two laminae that are then realigned and sutured with 5/0 Monocryl simple running sutures [18].
Evaluation of results was made through comparative photos and verified by using presence/absence of recurrence, scarring evaluation, and VAS for patient satisfaction: there was no pathological scarring during follow–up and there were no phimosis recurrences. Finally, all patients restarted the normal sexual activity [18].
4.2.2. Y – V Preputioplasty (Figure 4)
A Y-V plasty procedure to relieve phimosis was first described by Ebbehøj’s group in 1984. This procedure is limited to men who can partially retract the foreskin [25].
In this technique, the constricting phimotic band was incised with a single, full-skin thickness dorsal cut. The incision was extended distally in 2 directions to form a “Y” shape. The resulting triangular flap was advanced proximally over the defect and sutured with a 4/0 vicryl. Munro NP et al reported the outcomes of this technique on 89 males: 12 patients (40%) were very satisfied and 10 (33%) were satisfied, whereas 4 (13%) were indifferent and 4 (13%) were dissatisfied. Only two patients have subsequently undergone circumcision [25].
4.2.3. Heineke-Mikulicz Preputioplasty (Figure 5)
Heineke-Mikulicz preputioplasty (HMP) is a foreskin-preserving surgical treatment for phimosis in the adult population. The technique is performed using a 2-3 cm vertical incision over the phimotic band on the dorsal surface to just above Buck's fascia and an additional incision on the ventral surface if phimosis remains persistent after dorsal release. The incision is closed horizontally in 2 layers.
Figure 5.
– Heineke-Mikulicz Preputioplasty.
Xu AJ et al report the data of HMP on 7 patients: 2 patients required both dorsal and ventral incisions; no intraoperative complications were reported, and 1 patient reported bothersome phimosis secondary to scar formation treated successfully with triamcinolone [16].
4.3. In-situ devices
4.3.1. The PrePex device (Figure 6)
The PrePex (Circ MedTech Ltd, Israel) is a device which offers potential advantages in reduction of operative time, requires a lower asepsis and the procedures can be performed by less skilled providers. The time required for placement is 3 minutes [51]. The manufacturer’s cost per PrePex device for this study was USD $20.00 (not including the costs of personnel, other accessories and facilities) [28].
The PrePex device is applied under topical anesthesia because the foreskin remains intact and is compressed by radial elastic pressure leading to distal necrosis. The necrotic skin could be removed at 5–9 days post-placement. The adverse events are rare (~1.7%) mainly due to displacement or self-removal [51]. Pain after Prepex placement was mild and was reported at 30 minutes. Some authors reported an unpleasant smell during the first week after PrePex placement in a great part of patient series. In a series, wound healing was certified as complete in 56.7% (185/326) PrePex and 98.7% (74/75) dorsal slit circumcisions (p<0.0001) [28].
Figure 6.
– PrePex device.
4.3.2. The Shang Ring™ device (Figure 7)
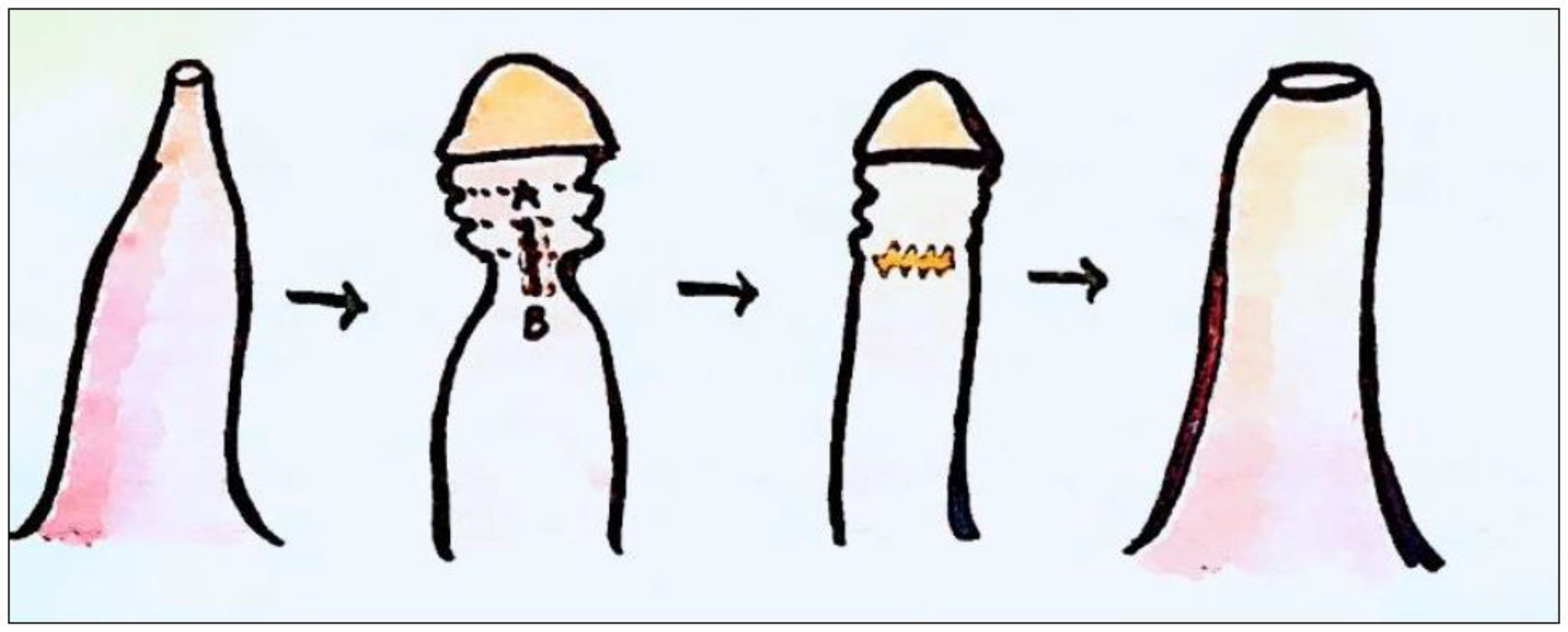
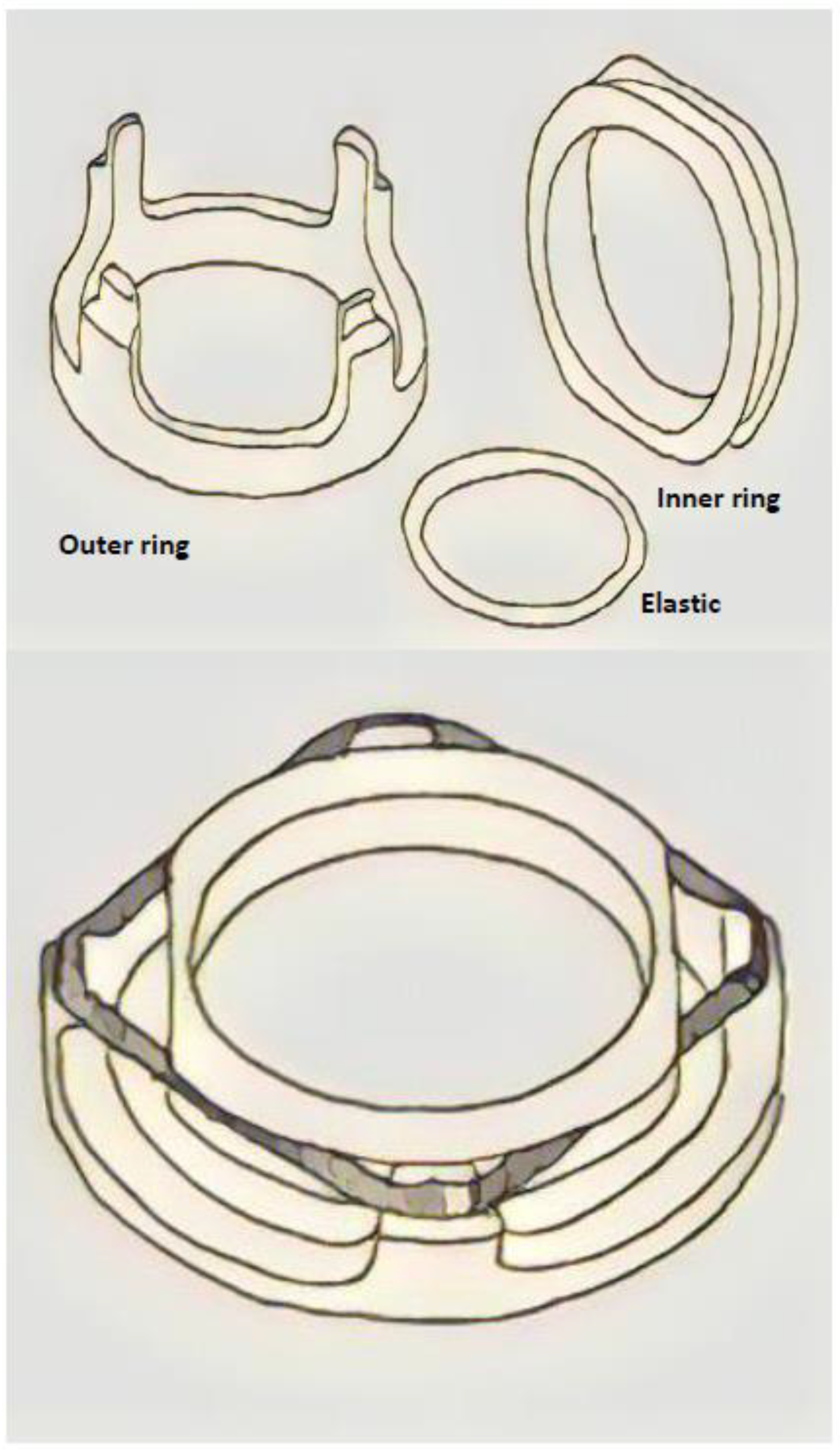
The Shang Ring™ (Wuhu Shengda Medical Treatment Appliance Technology Co.,Ltd. Wuhu City, Anhui Province, China) is a single – use device composed of an inner and outer ring, needed to block blood supply to the distal end of the foreskin, causing necrosis of the skin between. Local anesthesia is required during the procedure. The size of the Shang Ring (SR) needs to be chosen properly to avoid complication as pain, notable edema, or difficult postoperative healing.
Figure 7.
– The Shang Ring™ device.
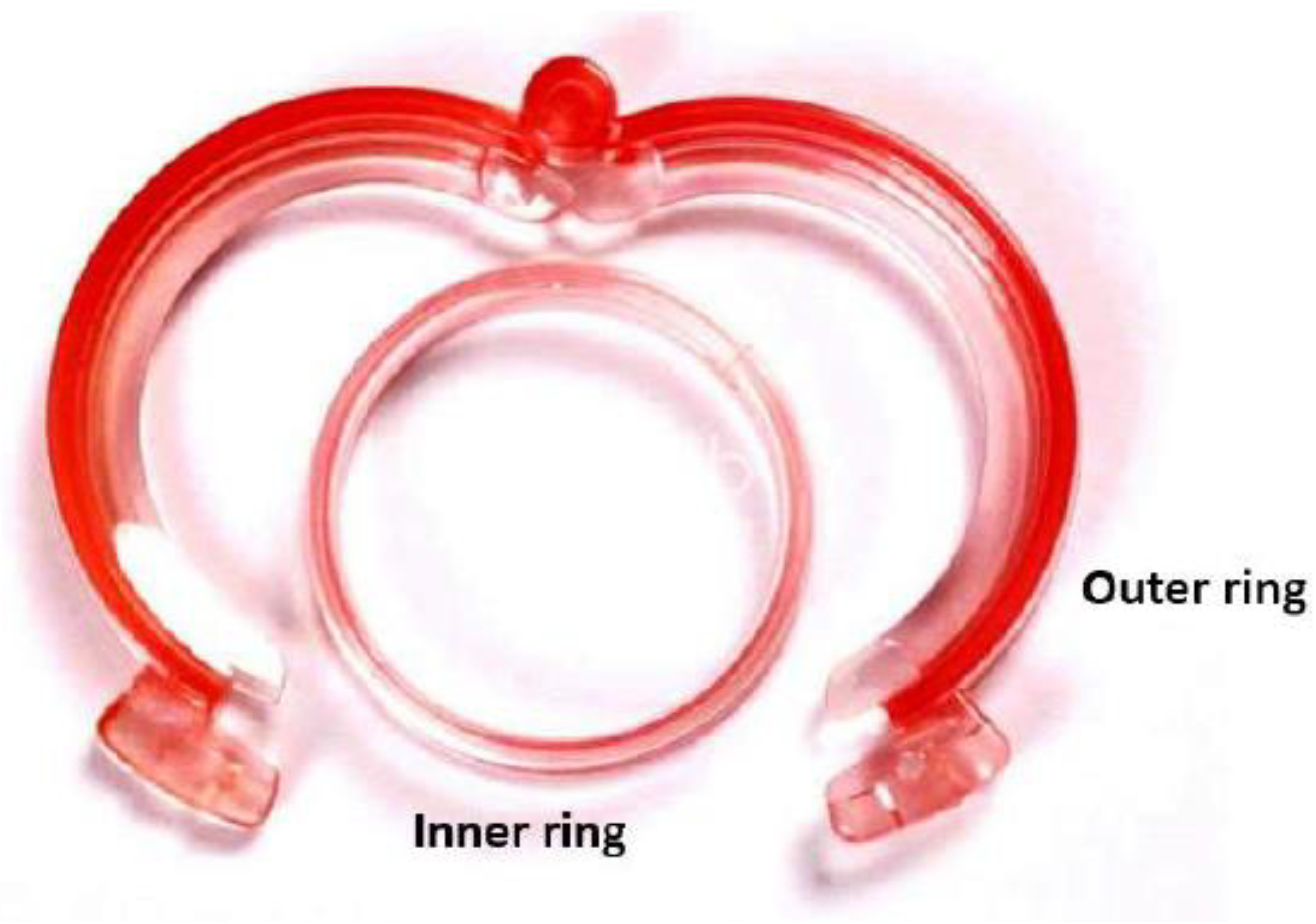
Wu X. et al report a large case-series including 702 adult patients (ages ranged 18-65 years old) treated with the SR [31]. The average operative time of the adult group was 4.26-2.57 minutes, and the timing of ring removal was 11.59-3.28 days (literature time reported is 7-9 after surgery). The most common complications are infections (in 8 patients, 1.14%), postoperative bleeding (in 2 patients, 0.3%) caused by fall of ring or mild pain (48 hours after surgery) in all patients during nocturnal erections. In a percentage of 30.06% of patients, yellow/white tissue exudate/lymph exudate occurred. Mild edema usually disappeared about 2 weeks after surgery, severe edema did not disappear until 2-3 months later. In a few cases, the edema persisted after half a year [31].
Barone MA et al conducted a randomized controlled trial of no-flip SR circumcision with removal 7 days post circumcision versus spontaneous detachment [26]. The main difference from the original technique, is the placement of the inner ring: in the no-flip technique, the inner ring is inserted under the foreskin and then the outer ring is placed over the inner ring eliminating the need to evert the foreskin. With this technique the inner ring is proximal to the wound, and it is necessary to cut off the inner ring as the ring cannot be safely sipped over the wound and off the penis [26].
Overall, 4/115 of adult participants in the spontaneous group and in 7 – days removal group develop adverse events (edema, infections). The median time to detachment was 14.0 (IQR: 7–21, range: 5–35) days. The no-flip technique and spontaneous detachment are safe, effective, and acceptable [26].
Lei HJ et al conducted a single-center prospective study to compare the clinical effectiveness and safety of adult male circumcision using the SR with the no-flip technique versus the Dorsal Slit (DS) surgical method [39]. The no-flip SR method was found to be superior to the DS method for its short operation time (<5 min, p < 0.001), involving less pain (during the procedure and >24h, p < 0,001), bleeding (p = 0.001), infection (p = 0.034), and resulting in a satisfactory appearance (p < 0.001) [39].
1. CONCLUSIONS
Conservative treatment for adult phimosis is an option and it includes the application of topical steroids or the very promising Phimostop™ device. The gold standard surgical treatment is represented by circumcision in which barbed sutures, fibrin glues or staples could be used after prepuce removal for tissue synthesis. Laser circumcision seems providing superior outcomes in terms of operative time and postoperative complication rate when compared to the traditional one. Preputioplasty could be proposed in selective cases for aesthetic reasons, while some in situ-devices have been described.
The choice of the right treatment depends on the grade of phimosis, results, complications and cost-effectiveness.
Author Contributions
Conceptualizzation and design of work: ADA, RM; Acquisition and analysis: ADA, ER; Interpretation of data: ADA, RM, SG; Writing – Original Draft Preparation: ER, ADA; Writing – Review & Editing: ADA, RM, SG.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The datasets used and analyzed for the current review are available from the corresponding author upon reasonable request.
Acknowledgments
All the authors have approved the submitted version (and version substantially edited by journal staff that involves the author’s contribution to the study) and all the authors agree to be personally accountable for the author’s own contributions and for ensuring that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved, and documented in the literature.
Conflicts of Interest
The authors declare no conflict of interest.
References
- L. S. Palmer and et al., Management of abnormalities of the external genitalia in boys. In: CampbellWalsh Urology. , vol. 11th ed. Vol. 4. 2016.
- D. GAIRDNER, “The fate of the foreskin, a study of circumcision.,” Br Med J, vol. 2, no. 4642, pp. 1433–7, illust, Dec. 1949. [CrossRef]
- M. Czajkowski et al., “Lichen Sclerosus and Phimosis - Discrepancies Between Clinical and Pathological Diagnosis and Its Consequences.,” Urology, vol. 148, pp. 274–279, Feb. 2021. [CrossRef]
- F. Korkes, J. L. Silva, and A. C. L. Pompeo, “Circumcisions for medical reasons in the Brazilian public health system: epidemiology and trends.,” Einstein (Sao Paulo), vol. 10, no. 3, pp. 342–6, 2012. [CrossRef]
- C. Radmayr and et al., “EAU Guidelines on Paediatric Urology, 2022,” 2022.
- M. Carilli et al., “Can circumcision be avoided in adult male with phimosis? Results of the PhimoStopTM prospective trial.,” Transl Androl Urol, vol. 10, no. 11, pp. 4152–4160, Nov. 2021. [CrossRef]
- D. M. Shabanzadeh, S. Clausen, K. Maigaard, and M. Fode, “Male Circumcision Complications - A Systematic Review, Meta-Analysis and Meta-Regression.,” Urology, vol. 152, pp. 25–34, Jun. 2021. [CrossRef]
- A. D. Asimakopoulos, B. Iorio, G. Vespasiani, V. Cervelli, and E. Spera, “Autologous split-thickness skin graft for penile coverage in the treatment of buried (trapped) penis after radical circumcision,” BJU Int, vol. 110, no. 4, pp. 602–606, Aug. 2012. [CrossRef]
- A. J. Krill, L. S. Palmer, and J. S. Palmer, “Complications of circumcision.,” ScientificWorldJournal, vol. 11, pp. 2458–68, 2011. [CrossRef]
- A. Abdulwahab-Ahmed and I. A. Mungadi, “Techniques of male circumcision.,” J Surg Tech Case Rep, vol. 5, no. 1, pp. 1–7, Jan. 2013. [CrossRef]
- A. D. Asimakopoulos, B. Iorio, G. Vespasiani, V. Cervelli, and E. Spera, “Autologous split-thickness skin graft for penile coverage in the treatment of buried (trapped) penis after radical circumcision.,” BJU Int, vol. 110, no. 4, pp. 602–6, Aug. 2012. [CrossRef]
- P. Pedersini, F. Parolini, A. L. Bulotta, and D. Alberti, “‘Trident’ preputial plasty for phimosis in childhood.,” J Pediatr Urol, vol. 13, no. 3, pp. 278.e1-278.e4, Jun. 2017. [CrossRef]
- M. Benson and M. K. Hanna, “Prepuce sparing: Use of Z-plasty for treatment of phimosis and scarred foreskin.,” J Pediatr Urol, vol. 14, no. 6, pp. 545.e1-545.e4, Dec. 2018. [CrossRef]
- A.C. Peterson, B. D. Joyner, and R. C. Allen, “Plastibell template circumcision: a new technique.,” Urology, vol. 58, no. 4, pp. 603–4, Oct. 2001. [CrossRef]
- M. J. Page et al., “The PRISMA 2020 statement: an updated guideline for reporting systematic reviews.,” BMJ, vol. 372, p. n71, Mar. 2021. [CrossRef]
- A. J. Xu, K. Mishra, and L. C. Zhao, “Heineke-Mikulicz Preputioplasty: Surgical Technique and Outcomes.,” Urology, vol. 166, pp. 271–276, Aug. 2022. [CrossRef]
- B. Nabavizadeh, K. D. Li, N. Hakam, N. M. Shaw, M. S. Leapman, and B. N. Breyer, “Incidence of circumcision among insured adults in the United States.,” PLoS One, vol. 17, no. 10, p. e0275207, 2022. [CrossRef]
- C. Monarca, M. I. Rizzo, L. Quadrini, G. Sanese, G. Prezzemoli, and N. Scuderi, “Prepuce-sparing plasty and simple running suture for phimosis.,” G Chir, vol. 34, no. 1–2, pp. 38–41, 2013.
- M. Siev, M. Keheila, P. Motamedinia, and A. Smith, “Indications for adult circumcision: a contemporary analysis.,” Can J Urol, vol. 23, no. 2, pp. 8204–8, Apr. 2016.
- P. Carmine et al., “Circumferential dissection of deep fascia as ancillary technique in circumcision: is it possible to correct phimosis increasing penis size?,” BMC Urol, vol. 21, no. 1, p. 15, Feb. 2021. [CrossRef]
- P. Rajan, S. A. McNeill, and K. J. Turner, “Is frenuloplasty worthwhile? A 12-year experience.,” Ann R Coll Surg Engl, vol. 88, no. 6, pp. 583–4, Oct. 2006. [CrossRef]
- F. Casabona, I. Gambelli, F. Casabona, P. Santi, G. Santori, and I. Baldelli, “Autologous platelet-rich plasma (PRP) in chronic penile lichen sclerosus: the impact on tissue repair and patient quality of life.,” Int Urol Nephrol, vol. 49, no. 4, pp. 573–580, Apr. 2017. [CrossRef]
- F. T. D’Arcy and S. Q. Jaffry, “A review of 100 consecutive sutureless child and adult circumcisions.,” Ir J Med Sci, vol. 180, no. 1, pp. 51–3, Mar. 2011. [CrossRef]
- K. S. Fink, C. C. Carson, and R. F. DeVellis, “Adult circumcision outcomes study: effect on erectile function, penile sensitivity, sexual activity and satisfaction.,” J Urol, vol. 167, no. 5, pp. 2113–6, May 2002.
- N. P. Munro, H. Khan, N. A. Shaikh, I. Appleyard, and P. Koenig, “Y-V preputioplasty for adult phimosis: a review of 89 cases.,” Urology, vol. 72, no. 4, pp. 918–20, Oct. 2008. [CrossRef]
- M. A. Barone et al., “Simplifying the ShangRing technique for circumcision in boys and men: use of the no-flip technique with randomization to removal at 7 days versus spontaneous detachment.,” Asian J Androl, vol. 21, no. 4, pp. 324–331, 2019. [CrossRef]
- C. Gu et al., “Introducing the QuillTM device for modified sleeve circumcision with subcutaneous suture: a retrospective study of 70 cases.,” Urol Int, vol. 94, no. 3, pp. 255–61, 2015. [CrossRef]
- G. Kigozi et al., “The safety and acceptance of the PrePex device for non-surgical adult male circumcision in Rakai, Uganda. A non-randomized observational study.,” PLoS One, vol. 9, no. 8, p. e100008, 2014. [CrossRef]
- Q. Su et al., “A Comparative Study on the Clinical Efficacy of Modified Circumcision and Two Other Types of Circumcision.,” Urol J, vol. 18, no. 5, pp. 556–560, Oct. 2020. [CrossRef]
- D. Jasaitiene et al., “Lichen sclerosus et atrophicus in pediatric and adult male patients with congenital and acquired phimosis.,” Medicina (Kaunas), vol. 44, no. 6, pp. 460–6, 2008.
- X. Wu et al., “A report of 918 cases of circumcision with the Shang Ring: comparison between children and adults.,” Urology, vol. 81, no. 5, pp. 1058–63, May 2013. [CrossRef]
- J. Mu, L. Fan, D. Liu, and D. Zhu, “A Comparative Study on the Efficacy of Four Types of Circumcision for Elderly Males with Redundant Prepuce.,” Urol J, vol. 17, no. 3, pp. 301–305, May 2020. [CrossRef]
- J. Shen et al., “A Comparative Study on the Clinical Efficacy of Two Different Disposable Circumcision Suture Devices in Adult Males.,” Urol J, vol. 14, no. 5, pp. 5013–5017, Aug. 2017.
- P. Ronchi, S. Manno, and L. Dell’Atti, “<p>Technology Meets Tradition: CO2 Laser Circumcision versus Conventional Surgical Technique</p>,” Res Rep Urol, vol. Volume 12, pp. 255–260, Jul. 2020. [CrossRef]
- Z.-L. Jiang, C.-W. Sun, J. Sun, G.-F. Shi, and H. Li, “Subcutaneous tissue-sparing dorsal slit with new marking technique: A novel circumcision method.,” Medicine, vol. 98, no. 16, p. e15322, Apr. 2019. [CrossRef]
- B.-D. Lv et al., “Disposable circumcision suture device: clinical effect and patient satisfaction.,” Asian J Androl, vol. 16, no. 3, pp. 453–6, 2014. [CrossRef]
- Z. Zhang et al., “Application of a novel disposable suture device in circumcision: a prospective non-randomized controlled study.,” Int Urol Nephrol, vol. 48, no. 4, pp. 465–73, Apr. 2016. [CrossRef]
- H. Han, D.-W. Xie, X.-G. Zhou, and X.-D. Zhang, “Novel penile circumcision suturing devices versus the shang ring for adult male circumcision: a prospective study.,” Int Braz J Urol, vol. 43, no. 4, pp. 736–745, 2017. [CrossRef]
- J.-H. Lei et al., “Circumcision with ‘no-flip Shang Ring’ and ‘Dorsal Slit’ methods for adult males: a single-centered, prospective, clinical study.,” Asian J Androl, vol. 18, no. 5, pp. 798–802, 2016. [CrossRef]
- J. Wang et al., “Safety and efficacy of a novel disposable circumcision device: a pilot randomized controlled clinical trial at 2 centers.,” Med Sci Monit, vol. 20, pp. 454–62, Mar. 2014. [CrossRef]
- P. Malone and H. Steinbrecher, “Medical aspects of male circumcision.,” BMJ, vol. 335, no. 7631, pp. 1206–90, Dec. 2007. [CrossRef]
- C.-C. Chi, G. Kirtschig, M. Baldo, F. Brackenbury, F. Lewis, and F. Wojnarowska, “Topical interventions for genital lichen sclerosus.,” Cochrane Database Syst Rev, vol. 2011, no. 12, p. CD008240, Dec. 2011. [CrossRef]
- Y. Xu et al., “A Prospective, Randomized Controlled Trial of Circumcision in Adult Males Using the CO 2 Laser: Modified Technique Compared with the Conventional Dorsal-Slit Technique,” Photomed Laser Surg, vol. 31, no. 9, pp. 422–427, Sep. 2013. [CrossRef]
- S. M. Neill, F. M. Lewis, F. M. Tatnall, N. H. Cox, and British Association of Dermatologists, “British Association of Dermatologists’ guidelines for the management of lichen sclerosus 2010.,” Br J Dermatol, vol. 163, no. 4, pp. 672–82, Oct. 2010. [CrossRef]
- G. Moreno, J. Corbalán, B. Peñaloza, and T. Pantoja, “Topical corticosteroids for treating phimosis in boys.,” Cochrane Database Syst Rev, no. 9, p. CD008973, Sep. 2014. [CrossRef]
- J. Liu, J. Yang, Y. Chen, S. Cheng, C. Xia, and T. Deng, “Is steroids therapy effective in treating phimosis? A meta-analysis.,” Int Urol Nephrol, vol. 48, no. 3, pp. 335–42, Mar. 2016. [CrossRef]
- Kikiros CS, Beasley SW, and Woodward AA, “The response of phimosis to local steroid application. ,” Pediatr Surg Int , vol. 8, pp. 329–332, 1993.
- S. Shikanov et al., “Knotless Closure of the Collecting System and Renal Parenchyma with a Novel Barbed Suture During Laparoscopic Porcine Partial Nephrectomy,” J Endourol, vol. 23, no. 7, pp. 1157–1160, Jul. 2009. [CrossRef]
- F. N. Elmasalme, S. A. Matbouli, and M. S. Zuberi, “Use of tissue adhesive in the closure of small incisions and lacerations.,” J Pediatr Surg, vol. 30, no. 6, pp. 837–8, Jun. 1995. [CrossRef]
- M. Czajkowski et al., “Male Circumcision Due to Phimosis as the Procedure That Is Not Only Relieving Clinical Symptoms of Phimosis But Also Improves the Quality of Sexual Life.,” Sex Med, vol. 9, no. 2, p. 100315, Apr. 2021. [CrossRef]
- V. Mutabazi et al., “One-arm, open-label, prospective, cohort field study to assess the safety and efficacy of the PrePex device for scale-up of nonsurgical circumcision when performed by nurses in resource-limited settings for HIV prevention.,” J Acquir Immune Defic Syndr, vol. 63, no. 3, pp. 315–22, Jul. 2013. [CrossRef]
Figure 1.
PRISMA flow chart.
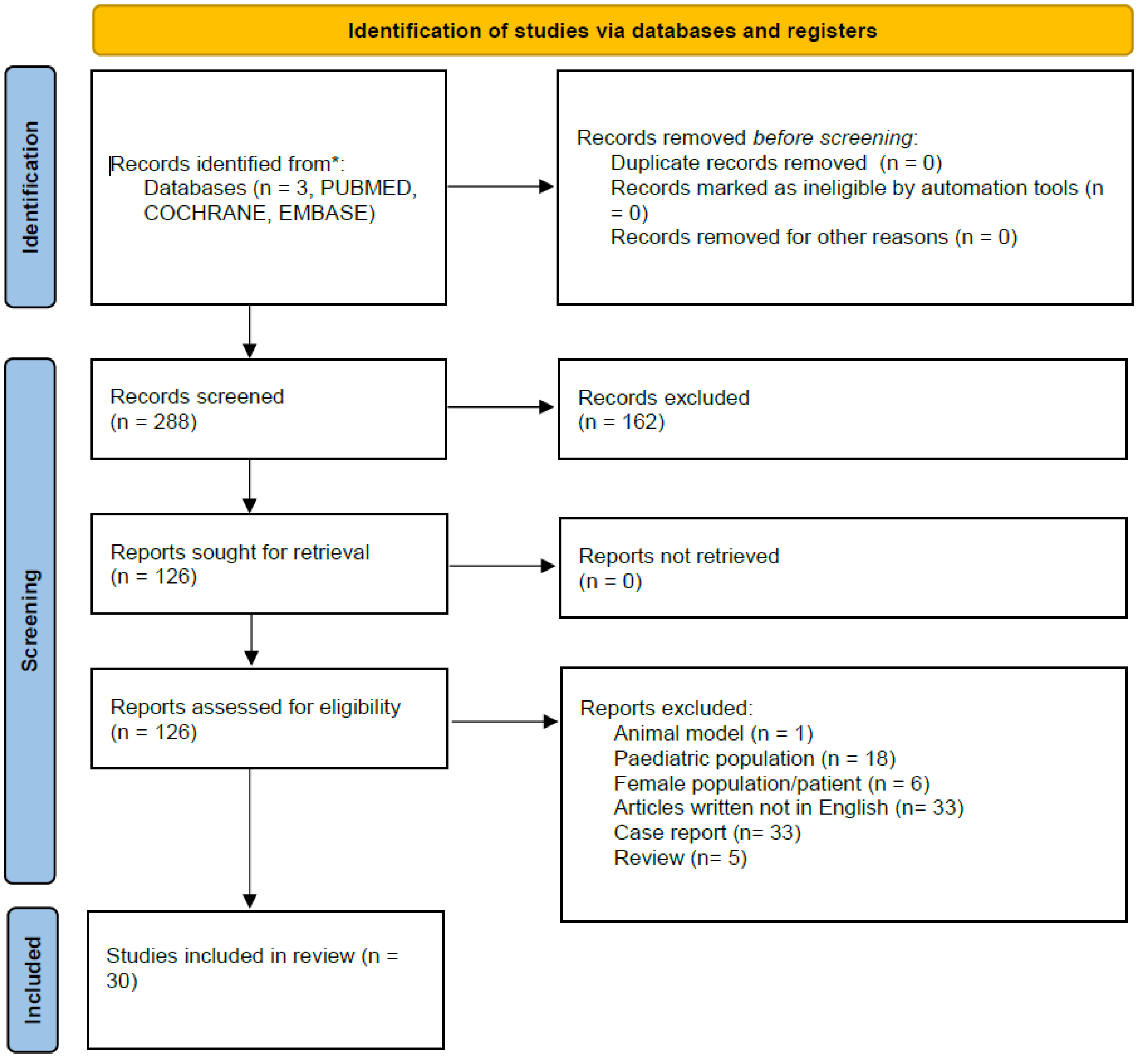
Figure 2.
– PhimoStopTM device. (A) Standard tuboids (top row) and intermediate tuboids (bottom row). The fins of standard tuboids are fixed outside the prepuce with adhesive patches. (B) Insertion of the intermediate tuboid on the standard one, allowing a gradual increase of the tuboid diameter of half a size.
Figure 2.
– PhimoStopTM device. (A) Standard tuboids (top row) and intermediate tuboids (bottom row). The fins of standard tuboids are fixed outside the prepuce with adhesive patches. (B) Insertion of the intermediate tuboid on the standard one, allowing a gradual increase of the tuboid diameter of half a size.

Figure 3.
– Circumcision.
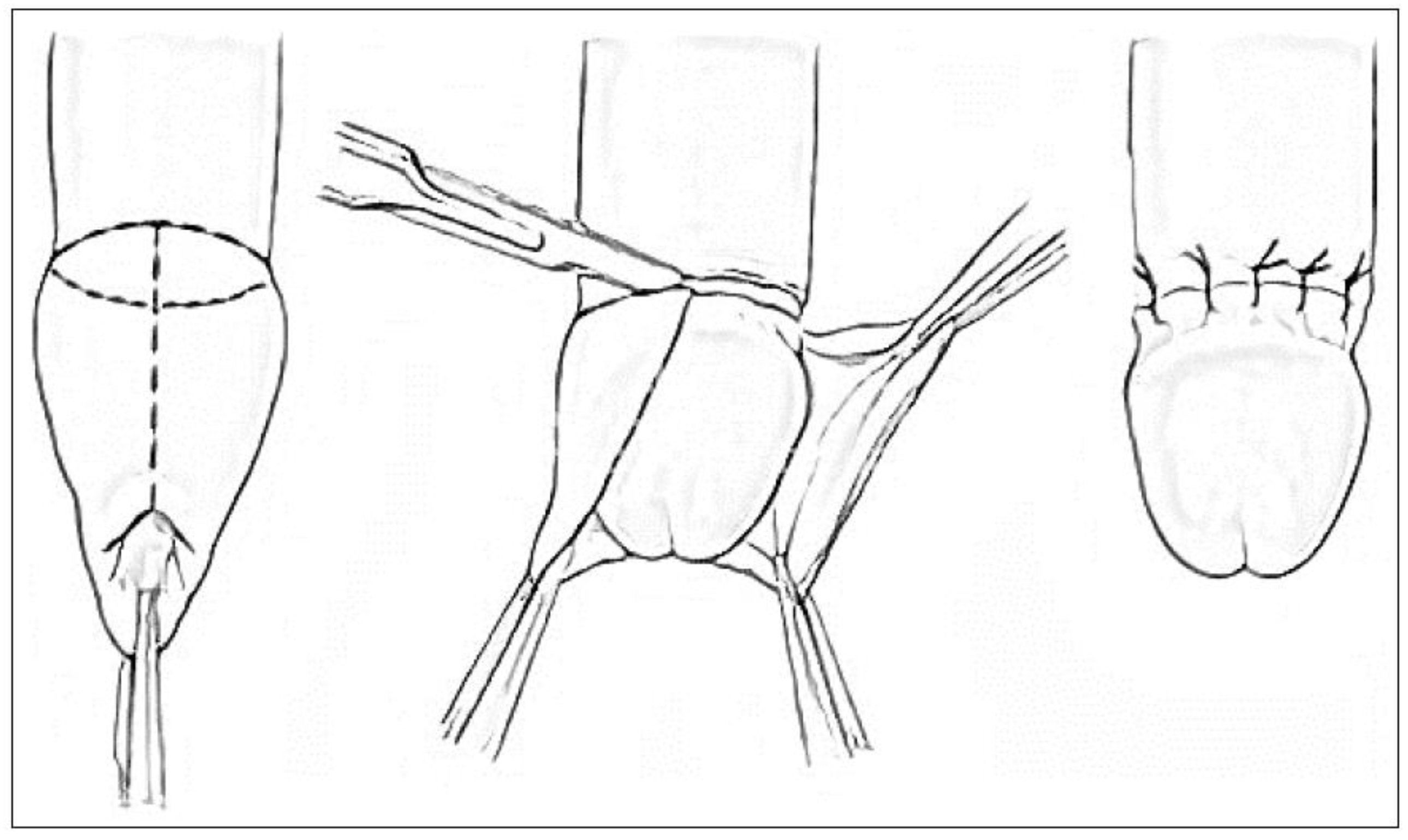
Figure 4.
– Y – V plasty.
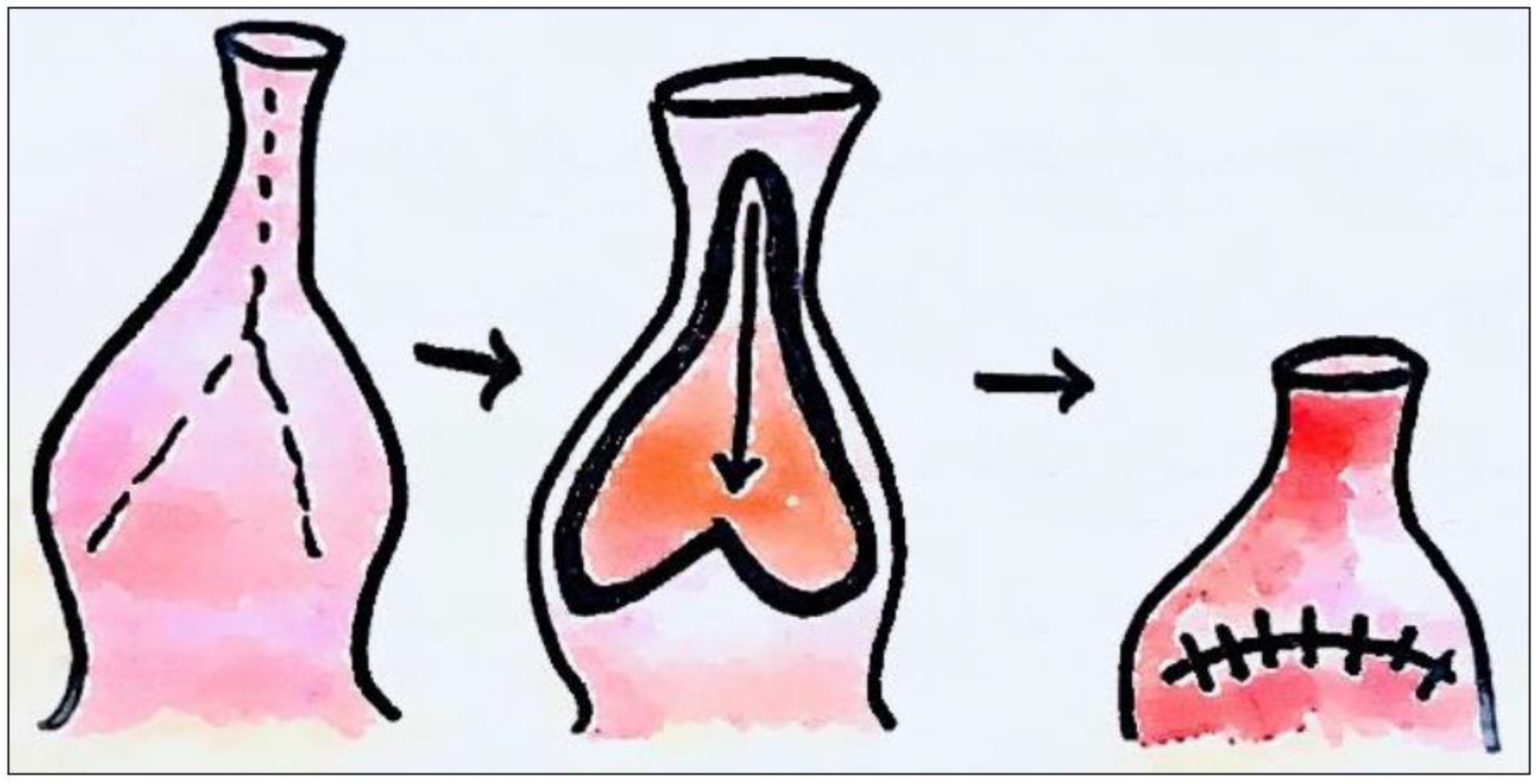

Table 1.
– Summary of conservative treatments for adult phimosis.
| Treatment | Advantage/Disavantage | Side Effects |
|---|---|---|
| Phimostop™[Carilli M et al,5] | Shaped silicone tuboids of increasing size to obtain a non-forced dilation of the prepuce | Scarce: discomfort with larger tuboid size |
| Platelet-rich plasma (PRP) [Casabona F et al, 20] | Reduction/disappearance of symptoms and/or of lichen sclerosus | Risk of malignant disease (actually no study demonstrates that PRP promotes hyperplasia, carcinogenesis, or tumor growth) |
| Topical corticosteroids [Moreno G et al, Liu J et al] | Complete or partial clinical resolution of phimosis (long – term follow – up not available) | These drugs could induce skin atrophy, telangiectasia and immunosuppression (increasing the risk of malignancy) |
Table 2.
– Potency of main topical corticosteroids (British National Formulary).
| Potency | Topical corticosteroids |
|---|---|
| Very potent | Clobetasol propionate 0.05% Diflucortolone valerate 0.3% |
| Potent | Bethametasone dipropionate 0.05% to 0.064% Bethametasone valerate 0.1% to 0.12% Diflucortolone valerato 0.1% Hydrocortisone butyrate 0.1% Mometasone furoate 0.1% Triamcinolone acetonide 0.1% |
| Moderate | Betamethasone valerate 0.025% Clobetasone butyrate 0.05% |
| Mild | Hydrocortisone 0.1% to 2.5% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



