Submitted:
18 December 2023
Posted:
20 December 2023
You are already at the latest version
Abstract
Dengue is one of the most important arboviruses worldwide, with currently approximately 2.5 billion people at risk of becoming infected, mainly in tropical countries. The present study evaluated the influence of climatic variables on the incidence of dengue fever in an endemic urban area. A time series study of cases was carried out with all confirmed cases of dengue fever in the municipality of Belo Horizonte from 2001 to 2021. The climatic explanatory variables were obtained from the National Institute of Meteorology. The analysis was performed using a generalized linear regression model with three scenarios: a no-lag model, 1-month lag model (1 month earlier) and 2-month lag model (2 months earlier). In the no-lag model, the maximum temperature was associated with an increase in the monthly incidence of dengue (IRR: 1.5). In the 1- and 2-month lag models, the monthly average temperature was associated with an increase in incidence (IRR: 1.9 in both). Our results suggest that temperature contributed to the increase in the incidence of dengue, and an increase of 1 °C could increase the incidence of the disease by approximately 90%. Thus, temperature monitoring can direct efforts towards prevention and control of the disease.
Keywords:
dengue fever
; climate
; incidence
; temperature
; epidemiology
; Brazil
1. Introduction
In the year 2023, the Americas had more than three million cases of dengue fever officially registered, this being the second highest annual incidence of the disease since records began by the Pan American Health Organization in 1980 [1]. According to the Brazilian Ministry of Health, from 2000 to 2022, almost 16 million suspected cases of dengue were reported with approximately 9200 deaths [2,3]. Despite dengue’s low mortality rate, it contributes to the loss of healthy years of life in Brazil, as it affects a large number of people, of all age groups, and can cause disability during infection and lead to death, mainly in children [4]. Another issue to consider is the burden on health services. Dengue control is a costly activity in health surveillance and dengue epidemics generate high hospitalization and care costs. In the Americas, from 2000 to 2007, an average cost of $2.1 billion per year was estimated to be spent to control the disease, approximately 41% of this resource used by Brazil [5].
The Brazilian National Dengue Control Program (PNCD) has as its main strategy the reduction in infestation by Aedes aegypti, the main vector of the disease. Aedes aegypti is well adapted to the domestic and peridomestic environments, being able to reproduce using different types of containers with stagnant water, which favored its dispersion, also causing outbreaks of arboviruses such as yellow fever, dengue, Zika and chikungunya worldwide [6]. The Brazilian program emphasizes the need for residents to keep their yards clean and eliminate water-accumulating containers that can serve as habitat for larvae. Several factors contribute to the population success of Ae. aegypti, such as the resistance of eggs to desiccation, the rapid development and proliferation, neat adaptation to live close to humans, feeding preferentially on human blood, and, more recently, resistance to insecticides [7].
The expansion of dengue is generally associated with disorderly urbanization, without adequate sanitation infrastructure, which contributes to the proliferation of the vector [8]. However, In Brazil, since 2017, a total of 481 new municipalities detected community transmission of dengue for the first time, with a large expansion observed in the southern region of the country, which is associated with climate change, an obvious driver of disease expansion, along with urbanization and mobility [9]. Likewise, since 2012 dengue has been recorded as an new endemic disease in high altitude cities of Southeastern Brazil [10]. Among factors influencing the territorial expansion of the disease, those related to a warmer and more unpredictable planet, as higher temperatures, precipitation, and humidity, may favor the development and proliferation of both mature and immature forms of the vector insect. Furthermore, anthropogenic factors such as deforestation and poor sanitarian conditions also favors the population dynamics of this arbovirus. Aedes aegypti is uncapable to invade native forests, and in cities it adapted to lay eggs and develop in any small pots, taking advantage of garbage and urban untreated trashes [11,12,13]. For instance, Cunha et al. [12] identified that preserved native forests close to neighborhoods under great socio-economic vulnerability in a large Brazilian city, functioned as a barrier against the occurrence of dengue. The protection of natural green areas has proven efficiency in reducing thermal gains and works as barriers against mosquitoes that transmit diseases to humans and animal.
According to the Intergovernmental Panel on Climate Change (IPCC), the Earth’s surface temperature has increased by approximately 1.1 °C since the Industrial Age and is likely to rise further [14]. These climate changes directly affect the biology of insect vectors, favoring the transmission, outbreaks, and dissemination of dengue to regions previously inhospitable to Ae. Aegypti [10,15]. Follows that approximately half of the world’s population will live in regions that will be suitable for arbovirus transmission by the year 2050 [16]. Because of global warming, local climatic conditions tend to extreme events, which might be important factors for epidemic years. For dengue, an epidemy is the co-occurrence of several outbreaks triggered for similar causes along a large geographic area, even intercontinental areas, and result in spreading of previously rare serotypes [17]. However, the intensity of each outbreak and its actual threat to populations can be strongly influenced by climatic conditions at each local.
Belo Horizonte, a city located in southeastern Brazil. With 2.3 million people, is the sixth most populous municipality in Brazil and has undergone a rapid and intense growth and unplanned urbanization process. The municipality had its first case of dengue fever reported in 1996, and since then, five major outbreaks have been recorded [18]. From 2007 to 2020 a total of 463,566 dengue cases and 125 deaths were reported in the city, with an increase in severe cases and deaths [2,3]. Campos et al. [19] demonstrated that increases in annual temperature and relative humidity were correlated with increased numbers of cases in this city. Similar positive effects of warmer and rainier years, above the average, on dengue cases were observed for an Amazonian city [20], as well as heatwaves to cases in Hanoi, Vietnam [21]. However, no detailed analysis on a long term dengue/climate time series have been investigated with a proper autocorrelation approach for Southeastern Brazil.
The present study aims to evaluate the impact of climatic variables on the incidence of dengue over a long time period, in Belo Horizonte, a dengue hyperendemic urban area, in Southeastern Brazil. Our hypothetical prediction is that climate alone might explain epidemic years, due to warmer temperatures driving Ae. aegypti population growth, and regardless the disease epidemiological history in the previous years. The analysis of climate variables in long time series can contribute to predicting possible epidemic periods.
2. Materials and Methods
2.1. Study Area and Sampling Design
Belo Horizonte is located in the state of Minas Gerais, southeastern Brazil, at an average altitude of 859.19 meters above sea level, with a land area of 331,354 km². The estimated population for 2022, according to the Brazilian Institute of Geography and Statistics (IBGE), was 2,315,560 inhabitants, with a population density of 6988.18 inhabitants/km2 [22]. Belo Horizonte is divided into nine administrative regions. This separation aims to meet the needs of each location and define specific programs and actions in different areas, such as health, sport, leisure and education [23]. The city has a high literacy rate of 97.6% for ages 6 to 14. Per capita gross domestic product was R$38,670.40 in 2020 and 96.2% of the municipality has adequate sanitation. The climate is tropical and seasonal, with rainy summers and dry winters [22].
2.2. Data Source and Variables
We used a time series of all confirmed cases of dengue fever in Belo Horizonte, by month, from 2001 to 2021. Throughout the entire historical series, we analyzed all climatic factors likely to affect fluctuation in the number of monthly cases. Information on dengue fever cases was obtained from the Brazilian Notifiable Disease Information System (SINAN database). The present study included cases that met the clinical epidemiological or laboratory criteria according to the manual of diagnosis and clinical management of dengue in adult and child. This database has the year and month of notification, in which we evaluated the years from 2001 to 2021. To calculate the incidence, population data were obtained each year from the IBGE. The monthly climate variables were obtained from the National Institute of Meteorology (INMET) at weather station 83587, namely: total precipitation, maximum temperature, minimum temperature, mean temperature and relative humidity.
2.3. Data Analysis
The analysis of a continuous response variable using the usual multiple linear regression model assumes that the errors are independent and identically distributed according to a normal distribution with mean 0. Discrete data, such as the monthly number of dengue cases in Belo Horizonte, often are not suitable for the use of normal distribution. Therefore, other more robust models must be adopted, especially when discrete data are highly skewed.
The negative binomial regression model is a method of predicting the discrete variable from a set of explanatory variables. This model is a generalization of the Poisson regression model that accounts for overdispersion by including a disturbance or error term [24]. The usual functional form for the negative binomial regression model is given by
where
- is the expected value of the response variable yi for subject i;
- is the model intercept and are the k independent explanatory variables with corresponding regression coefficients
- σεi is the disturbance term.
In this study, the response variable represents the total number of confirmed cases of dengue fever in Belo Horizonte each month from 2001 to 2021. As explanatory variables, the 5 climatic variables (total precipitation, maximum temperature, minimum temperature, mean temperature and relative humidity) were evaluated together with the month of the year. The annual population of Belo Horizonte was used as an offset variable to adjust for differential exposure time. Then, we are no longer modeling count data and the analysis is directed to incidence modeling.
When fitting the model, three scenarios were considered: a no-lag model, 1-month lag model (1 month earlier) and 2-month lag model (2 months earlier). This is an interesting perspective since characteristics such as incubation time, transmissibility and notification are considered. In each scenario, the climatic variables were considered according to the respective lag, and those that presented a p value less than 0.05 were maintained. To choose the best model in each scenario, the Akaike Information Criterion AIC was used, which is based on the Kullback-Leibler Divergence. This, in turn, is a measure of the “distance” between the fitted model and a theoretical “real model”. How the real model is unknown, the creator developed a way to measure the distance using the data used in modeling, through the likelihood function of the model in terms of the number of parameters that must be estimated. The parameters of the model in each scenario were estimated by the maximum likelihood method using the function glm.nb from package MASS of R-Studio [25].
For Negative Binomial regression, by taking the exponent of the coefficient, we obtain the rate ratio Incidence Rate Ratio (IRR). This is interpreted in similar way to the odds ratio for logistic regression, which is approximately the relative risk given a predictor. If the explanatory variable is quantitative, the IRR evaluates the impact on the incidence rate when increasing this variable by one unit. If the variable is qualitative, the IRR evaluates the impact of moving to one of the variable’s categories considering one of them as a reference.
3. Results
3.1. Annual and Monthly Incidence of Dengue Fever
A total of 488,756 dengue fever cases were recorded from 2001 to 2021. The occurrence of four outbreaks of the disease was observed in the study period, namely, 2010, 2013, 2016 and 2019, with an incidence of 2056, 3920, 6258 and 4620 per 100,000 inhabitants respectively (Figure 1A). The highest peak occurred in 2016, totaling 155,320 cases. The highest monthly average incidence of dengue fever occurred between January and June, with April having the highest incidence rate (304.64 per 100,000 inhabitants), while in the period from July to December the average incidence was 2.64 per 100,000 inhabitants (Figure 1B).
3.2. Monthly Climate Variables (2001–2021)
Maximum, mean and minimum temperatures followed the same distribution pattern throughout the year. The highest temperatures were recorded in the months of October to April, the hottest being February (maximum: 29.1 °C; mean: 24.0 °C and minimum: 20.2 °C) and October (maximum: 29.1 °C; mean: 23.2 °C and minimum: 18.9 °C) (Figure 2A).
The months with the highest precipitation occurred between October and March, with January (318.0 mm) and December (346.8 mm) being the months with the greatest rainfall volume (Figure 2B). The period with relative humidity above 60% was from November to June, with the months with the highest humidity being January (67.1%) and December (69.7%) (Figure 2C).
3.3. Dengue Incidence Rates in Epidemic Years in Response to Climatic Variables
There was a preceding substantial increase in the temperatures defining the occurrence of dengue outbreaks. When maximum temperatures were around 30 °C in February, an outbreak occurred in March, April and May. In the non-epidemic year, the maximum temperature in February was 28.9 °C (Figure 3). As predicted in climate change models, above average temperatures normally are followed by stormy rains. In our case, we observed a substantial pluviosity in the months of the rainy seasons, also preceding outbreaks. For one particular non-epidemic year (2005) and all epidemic years of 2010, 2013, 2016 and 2019, there were rainfall greater than 200mm in the months of November to January preceding in one to two months a peak of dengue incidence, an effect confounding with temperature, thus, not statistically significant, but still a likely signaling event for predictive analysis. Concerning humidity, we observed a variation from 50% to 75% throughout the year, with the rainiest months being November to June, regardless of whether the year was epidemic or not.
3.4. Effect of Climatic Variables on the Incidence of Dengue Fever
Only maximum temperature and average temperature explained significantly the incidence of dengue. In the no-lag model, each 1 °C increase in the maximum temperature was associated with a 51% increase in the monthly incidence of dengue (incidence rate ratio [IRR]: 1.51; 95% confidence interval [CI]: 1.27–1.78) adjusted by month (Table 1).
In the 1-month lag model, each 1 °C increase in the monthly average temperature was associated with an 89% increase in the incidence of the disease in the following month (IRR: 1.89; 95% CI: 1.55-2.35) adjusted by month. The 2-month lag model showed that each 1 °C increase in the monthly average temperature was associated with a 92% increase in the incidence of the disease after 2 months (IRR: 1.92; 95% CI: 1.57-2.35) adjusted by month (Table 1).
4. Discussion
In this study, outbreaks were observed every 3 years from the second decade of the 21st century, with cases concentrated from January to June, with April having the highest incidences. Temperatures of approximately 30°C in February preceded outbreaks, and an association between the incidence of dengue and temperature was clearly demonstrated, with an increase of one degree resulting in an increase of approximately 90% in the dengue incidence, regardless previous years dynamics of the disease.
Similar patterns and the importance of heatwaves in dengue outbreaks was already demonstrated to Hanoi, Vietnam [21]. On the contrary, in urban centers, the presence of water throughout the year is assured by a number of abandoned lands with likely places for stagnated water, and many other human microhabitats prone to water accumulation. Hence, although the presence of water is necessary for immature forms of the vector to develop [26], the urban great number of water savings could be a reason why pluviosity was not a significant explanatory factor, even though we detected a likely positive effect of storms, in a confound association to high temperatures in the last months of summer. Rose et al. [27] described the evolutionary process of domestication of Ae. aegypti, showing that preference for human than other animal odors evolved in response to dry season intensity and human population density.
Powell & Tabachnick [28] and Brown et al. [29] reviewed the most likely evolutionary specialization paths for the prevalent Ae. aegypti subspecies dominant worldwide, tracking it back exactly to a greater predictability of water sources in urban reservoirs, created in northeast Africa civilizations by the time of an increasing drought severity. Hence, the very existence of this species in our cities is evolutionarily adjusted to an urban resource, stored water, that made this a rainfall independent species. Along with Ae. aegypti, dengue also evolved and adjusted to become an anthropophilic rather than a sylvatic arbovirus [30]. Saeed & Asif [31] showed how the epidemic dynamics of all serotypes shifted to a more severe form, resulting in frequent outbreaks, due to ecological disturbances after the World War II. Hence, environmental unpredictability, habitat and lifestyle deterioration are deeply entangled with dengue disease, and may be more influential to DENV variation along time and outbreaks, than the DENV re-emergence per se.
Epidemiologists have consider so far that the emergence and circulation of new serotypes of the disease might favor the occurrence of dengue epidemics [17,19]. However, our results showed clearly that temperature is a main primary driver of outbreaks, independently of serotypes incidence. Hence, our results support a different explanation, which may better accommodate the current understanding of the relation between virulence/dissemination. Well established knowledge since pioneering work of May & Andersen [32], and widely demonstrated along the COVID-19 pandemic, transmissibility is not related, or even is inversely related, to virulence. Contrasting 2003 SARS epidemic to the most recent SARS-CoV-2 pandemic, it is clear that a virulent variant/genotype will decrease its incidence in the host population, while those genotypes which are less virulent may evolve towards forms which are more transmissible, thus, becoming highly incident, even though more difficult to detect due to low hospitalization [33,34,35,36,37]
Even though virulence of dengue is expected to be preserved along time due to the insect vector phase, especially considering vertical transmission [38], a newly arriving serotype must cause more severe disease but not further dissemination. On the contrary, the fast hospitalization removes a host to the transmission cycle. As a consequence, it is going to be much more frequent for the public health service to record the virulent form disproportionally and unlikely to be related to the actual cause of an outbreak, or to the relative prevalence of other serotypes. Therefore, despite the fact that a new serotype will spread fast among a naïve population, it might not be the cause of outbreaks, but been easier discovered due to an outbreak which is, primarily, produced by a boost in the mosquito population in hot years. Hence, we propose that a serotype must have to emerge in a community before an outbreak, and will have an increasing detection in the epidemic year, due to fast and intense infection when there is a large Ae. aegypti population. Indeed, the public data on serotype variations in time for Belo Horizonte suggested that this is the case.
In the initial years of dengue occurrence in Belo Horizonte (1996 and 1997), the circulation of DENV1 was detected. In 1998, in addition to DENV1, DENV2 was detected, even in the winter period, when, generally, the abundance of vectors is lower [17]. Until 2001, serotypes DENV1 and DENV2 had been isolated; between 2002 and 2005, DENV1, DENV2 and DENV3 were circulating; and from 2005 to 2007, only DENV3 was identified. Between 2009 and 2014, DENV1 was identified again in approximately 60.4% of cases, followed by DENV4 (22.1%), DENV2 (9.8%) and DENV3 (7.7%). In 2010 and 2013, the years of disease outbreaks, the circulation of three (DENV1, DENV2 and DENV3) and two serotypes (DENV1 and DENV4), respectively, were recorded [19]. Em 2016 DENV1 e 2019 DENV1 and DENV 2. Finally, 2023 ongoing outbreak is dominated by DENV1, with few records for DENV2. As already said, in an epidemic year, a long-absent serotype might have more records, but mostly important, the Belo Horizonte’s data shows that a serotype which break out in the year ‘i’ happened at some low rates in the year ‘i-1′. That was the case for DENV3 from 2006 to 2008, DENV1 from 2009 to 2010, DENV4 from 2012 to 2013, and DENV2 from 2018 to 2019 [39]. Hence, the circulation of a new serotype per se was not seem enough to produce an outbreak, but its previous occurrence to a hot year, must contribute to its wide detection in an epidemic event caused by a large number of mosquitos.
In this study, the maximum temperature (no-lag model), and the average temperature (1- and 2-month lag models) were associated with an increase in the monthly incidence of dengue fever. The lag models between climate variation and incidence can be explained according to the time necessary to the environment to reach suitable conditions for the development of Ae. aegypti, until the actual occurrence of diagnoses of the disease [20].
High temperatures with warmer winters and summers have begun to occur more frequently [40]. Pedrosa et al. [10] showed that the increase in the maximum temperature of the dry seasons (winter) and its persistence over the years favored the invasion of Ae. aegypti in a high altitude town in southeastern Brazil. In addition, they observed that the intensity of yearly high temperatures has risen steadily in montane regions since 2007 [10]. A study carried out in Hanoi, Vietnam, reported that after the occurrence of sustained periods (days to weeks) of high temperatures, so-called heatwaves, there were higher occurrence of dengue cases [21]. Unusually warm weather in Cairns Queensland Australia, with daily mean temperatures exceeding 30 °C, would have shortened up the extrinsic incubation period of the virus, which was as low as 9–11 days. This was supported by a laboratory vector competence study which showed transmission by Ae. aegypti within only five days after exposure at 28 °C [41].
High temperatures reduce the extrinsic incubation period (EIP) of dengue inside Ae. aegypti, leading to sudden increasing in dengue transmission rate, and subsequent dissemination [42,43]. While the EIP of dengue viruses is typically reported to range from 8–12 days, a recent study suggests greater variability, with extreme low range varying between 2 to 5 days [44]. Considering a nominal daily survival of 0.90 Ae. aegypti female, a conservative reduction in the EIP from 8 to 5 days would result in an increasing of 37% in infected mosquitoes (Ritchie, Pyke et al. 2013). A reduced EIP has important epidemiological implications, as demonstrated in Cairns, Austrália [41].
At lower temperatures, mosquitoes may not survive, and the population should collapse, taking longer to recover and re-establish [7]. In addition, there is an effect of temperature on the intrinsic activities of Ae. aegypti, such as the speed of flight, the distance and height flown, the number of wing beats, and the number of bites performed on the host [41,45]. The temperature range for Ae. aegypti larval development are from 16 °C to 34 °C and 8 °C for survival, from which the larvae become immobile and eventually die. The temperature between 15 °C and 32 °C is considered the range within which female mosquitoes are able to maintain a sustainable flight, while in extreme temperatures such as 10 °C and 35 °C, flight is possible, but only for short periods of time [45].
In recent years, a rise in global temperature has been observed, mainly caused by the increase in the emission of gases that produce the greenhouse effect, along with an rampant deforestation in different ecosystems [46,47]. In Belo Horizonte, natural and preserved green areas protect socio-economically vulnerable communities against the occurrence of dengue fever [13].
In 2023, the twenty-eighth United Nations Conference on Climate Change (COP28) was held in Dubai, in the United Arab Emirates. Representatives from almost 200 countries approved the final document that makes a commitment to reduce the use of fossil fuels, so that nations can reach the zero-carbon target by 2050, thus limiting the increase in temperature on the planet [48]. This measure, if implemented, could enable humanity to avoid, among other damages, the expansion of arboviruses.
5. Conclusions
The resurgence and emergence of new serotypes, although important in defining epidemic years, cannot be considered the only determinant of epidemic years, requiring a combination of climatic conditions that provide an increase in the population of insect vectors and transmission of the virus. Temperature contributed considerably to the increase in the number of dengue cases, and an increase of 1 °C could increase the incidence of the disease by approximately 90%. Thus, temperature monitoring through epidemiological surveillance, especially in the months from November to April, can direct efforts towards prevention, control and actions to address cases of the disease in the warmer periods to come.
Author Contributions
Conceptualization, W.C.-V., S.P.R., A.B.R., M.H.F.-M., M.C. and T.C.C.; methodology and formal analysis, T.C.C., S.P.R., R.V.D., J.C.L.M. and G.A.V.; data curation, T.C.C., R.V.D., J.C.L.M., G.A.V. and M.H.F.-M.; writing—original draft preparation, T.C.C., S.P.R., R.V.D., J.C.L.M., G.A.V., M.C., S.P.R., A.B.R. and W.C.-V.; supervision, S.P.R. and W.C.-V.; funding acquisition, W.C.-V. All authors have read and agreed to the published version of the manuscript. T.C.C. and S.P.R. have equal contribution as first authors.
Funding
This research was funded by CNPq/BR, grant number 407195/2021-1 and grant number 305168/2022-3.
Institutional Review Board Statement
This work was approved by the Research Ethics Committee of the Federal University of Ouro Preto (n° 3.291.628) in april 29 of 2019 and by the Ethics Committee of the Municipality of Belo Horizonte (n° 3.343.825) in may 29 of 2019.
Informed Consent Statement
Not applicable.
Data Availability Statement
The raw data supporting the conclusions of this article are available at the: https://datasus.saude.gov.br/informacoes-de-saude-tabnet/ and https://bdmep.inmet.gov.br/#.
Acknowledgments
JCLM, SPR, MC, ABR and WCV are grateful to the CNPq for fellowships.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Lenharo, M. Dengue is breaking records in the Americas—what’s behind the surge? Nature 2023. [Google Scholar] [CrossRef] [PubMed]
- BRASIL. Ministério da Saúde. Série histórica—Casos prováveis de dengue (2000-2023). Avaiable at:https://www.gov.br/saude/pt-br/assuntos/saude-de-a-a-z/d/dengue/situacao-epidemiologica/serie-historica-casos-provaveis-de-dengue-2000-2023/view.
- 2023 .
- BRASIL. Ministério da Saúde. Série histórica—Casos de óbitos dengue (2000-2023). Avaiable at: https://www.gov.br/saude/pt-br/assuntos/saude-de-a-a-z/d/dengue/situacao-epidemiologica/serie-historica-casos-de-obitos-dengue-2000-2023/view. 2023.
- Araujo, V.E.M.; Bezerra, J.M.T.; Amancio, F.F.; Passos, V.M.A.; Carneiro, M. Increase in the burden of dengue in Brazil and federated units, 2000 and 2015: analysis of the Global Burden of Disease Study 2015. Rev Bras Epidemiol 2017, 20 (Suppl. 1), 205–216. [Google Scholar] [CrossRef] [PubMed]
- Shepard, D.S.; Coudeville, L.; Halasa, Y.A.; Zambrano, B.; Dayan, G.H. Economic impact of dengue illness in the Americas. Am J Trop Med Hyg 2011, 84, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Iwamura, T.; Guzman-Holst, A.; Murray, K.A. Accelerating invasion potential of disease vector Aedes aegypti under climate change. Nat Commun 2020, 11, 2130. [Google Scholar] [CrossRef] [PubMed]
- Brady, O.J.; Hay, S.I. The Global Expansion of Dengue: How Aedes aegypti Mosquitoes Enabled the First Pandemic Arbovirus. Annu Rev Entomol 2020, 65, 191–208. [Google Scholar] [CrossRef] [PubMed]
- Goncalves Neto, V.S.; Rebelo, J.M. [Epidemiological characteristics of dengue in the Municipality of Sao Luis, Maranhao, Brazil, 1997-2002]. Cad Saude Publica 2004, 20, 1424–1431. [Google Scholar] [CrossRef] [PubMed]
- Codeco, C.T.; Oliveira, S.S.; Ferreira, D.A.C.; Riback, T.I.S.; Bastos, L.S.; Lana, R.M.; Almeida, I.F.; Godinho, V.B.; Cruz, O.G.; Coelho, F.C. Fast expansion of dengue in Brazil. Lancet Reg Health Am 2022, 12, 100274. [Google Scholar] [CrossRef]
- Pedrosa, M.C.; Borges, M.A.Z.; Eiras, A.E.; Caldas, S.; Cecilio, A.B.; Brito, M.F.; Ribeiro, S.P. Invasion of Tropical Montane Cities by Aedes aegypti and Aedes albopictus (Diptera: Culicidae) Depends on Continuous Warm Winters and Suitable Urban Biotopes. J Med Entomol 2021, 58, 333–342. [Google Scholar] [CrossRef]
- de Sousa, S.C.; Carneiro, M.; Eiras, A.E.; Bezerra, J.M.T.; Barbosa, D.S. Factors associated with the occurrence of dengue epidemics in Brazil: a systematic review. Rev Panam Salud Publica 2021, 45, e84. [Google Scholar] [CrossRef]
- Cunha, M.; Ju, Y.; Morais, M.H.F.; Dronova, I.; Ribeiro, S.P.; Bruhn, F.R.P.; Lima, L.L.; Sales, D.M.; Schultes, O.L.; Rodriguez, D.A.; et al. Disentangling associations between vegetation greenness and dengue in a Latin American city: Findings and challenges. Landsc Urban Plan 2021, 216, None. [Google Scholar] [CrossRef]
- Assis, W.L.; Abreu, M.L. [The urban climate of Belo Horizonte: temporal-spatial analysis of the thermal and water field]. Revista de C. Humanas 2010, 10, 47–63. [Google Scholar]
- Masson-Delmotte, V., P. ; Zhai, A.; Pirani, S.L.; Connors, C.; Péan, S.; Berger, N.; Caud, Y.; Chen, L.; Goldfarb, M.I.; Gomis, M.; et al. Climate Change 2021: The Physical Science Basis. Contribution of Working Group I to the Sixth Assessment Report of the Intergovernmental Panel on Climate Change, Cambridge University Press.; 2021.
- Fouque, F.; Reeder, J.C. Impact of past and on-going changes on climate and weather on vector-borne diseases transmission: a look at the evidence. Infect Dis Poverty 2019, 8, 51. [Google Scholar] [CrossRef] [PubMed]
- Kraemer, M.U.G.; Reiner, R.C., Jr.; Brady, O.J.; Messina, J.P.; Gilbert, M.; Pigott, D.M.; Yi, D.; Johnson, K.; Earl, L.; Marczak, L.B.; et al. Past and future spread of the arbovirus vectors Aedes aegypti and Aedes albopictus. Nat Microbiol 2019, 4, 854–863. [Google Scholar] [CrossRef] [PubMed]
- Cunha, M.d.C.M.; Caiaffa, W.T.; Oliveira, C.d.L.; Kroon, E.G.; Pessanha, J.E.M.; Lima, J.A.; Proietti, F.A. Fatores associados à infecção pelo vírus do dengue no Município de Belo Horizonte, Estado de Minas Gerais, Brasil: características individuais e diferenças intra-urbanas. Epidemiologia e serviços de saúde 2008, 17, 217–230. [Google Scholar] [CrossRef]
- PBH. Prefeitura de Belo Horizonte. Dengue. 2023. Availabe online: https//prefeitura.pbh.gov.br/saude/informacoes/vigilancia/vigilancia-epidemiologica/doencas-transmissiveis/dengue (accessed on 21 April 2023).
- Campos, N.B.D.; Morais, M.H.F.; Ceolin, A.P.R.; Cunha, M.; Nicolino, R.R.; Schultes, O.L.; Friche, A.A.L.; Caiaffa, W.T. Twenty-Two years of dengue fever (1996-2017): an epidemiological study in a Brazilian city. Int J Environ Health Res 2021, 31, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Duarte, J.L.; Diaz-Quijano, F.A.; Batista, A.C.; Giatti, L.L. Climatic variables associated with dengue incidence in a city of the Western Brazilian Amazon region. Rev Soc Bras Med Trop 2019, 52, e20180429. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.; Bambrick, H.; Yakob, L.; Devine, G.; Frentiu, F.D.; Toan, D.T.T.; Thai, P.Q.; Xu, Z.; Hu, W. Heatwaves and dengue outbreaks in Hanoi, Vietnam: New evidence on early warning. PLoS Negl Trop Dis 2020, 14, e0007997. [Google Scholar] [CrossRef] [PubMed]
- IBGE. Panorama Belo Horizonte. Rio de Janeiro: IBGE, 2023. Avaiable at: https://cidades.ibge.gov.br/brasil/mg/belo-horizonte/panorama. 2023.
- PBH. Prefeitura Municipal de Belo Horizonte. Prodabel detalha tamanho e número de bairros das regionais. Belo Horizonte: Prefeitura de Belo Horizonte, 2021. Avaiable at: https://prefeitura.pbh.gov.br/noticias/prodabel-detalha-tamanho-e-numero-de-bairros-das-regionais. 2021.
- Agresti, A. Categorical data analysis; John Wiley & Sons: 2012; Vol. 792.
- Allaire, J. RStudio: integrated development environment for R. Boston, MA 2012, 770, 165–171. [Google Scholar]
- Gabriel, A.F.B.; Abe, K.C.; Guimarães, M.d.P.; Miraglia, S.G.E.K. Health impact assessment of the incidence of dengue associated with precipitation in the city of Ribeirão Preto, São Paulo. Cadernos Saúde Coletiva 2018, 26, 446–452. [Google Scholar] [CrossRef]
- Rose, N.H.; Sylla, M.; Badolo, A.; Lutomiah, J.; Ayala, D.; Aribodor, O.B.; Ibe, N.; Akorli, J.; Otoo, S.; Mutebi, J.P.; et al. Climate and Urbanization Drive Mosquito Preference for Humans. Curr Biol 2020, 30, 3570–3579.e6. [Google Scholar] [CrossRef]
- Powell, J.R.; Tabachnick, W.J. History of domestication and spread of Aedes aegypti--a review. Mem Inst Oswaldo Cruz 2013, 108 (Suppl. 1), 11–17. [Google Scholar] [CrossRef]
- Brown, J.E.; Evans, B.R.; Zheng, W.; Obas, V.; Barrera-Martinez, L.; Egizi, A.; Zhao, H.; Caccone, A.; Powell, J.R. Human impacts have shaped historical and recent evolution in Aedes aegypti, the dengue and yellow fever mosquito. Evolution 2014, 68, 514–525. [Google Scholar] [CrossRef] [PubMed]
- Weaver, S.C.; Vasilakis, N. Molecular evolution of dengue viruses: contributions of phylogenetics to understanding the history and epidemiology of the preeminent arboviral disease. Infect Genet Evol 2009, 9, 523–540. [Google Scholar] [CrossRef] [PubMed]
- Saeed, O.; Asif, A. Chapter 2—Dengue virus disease; the origins. Academic Press, Dengue Virus Disease From Origin to Outbreak 2020, 10.1016/B978-0-12-818270-3.00002-3, 9-16. [CrossRef]
- May, R.M.; Anderson, R.M. Epidemiology and genetics in the coevolution of parasites and hosts. Proc R Soc Lond B Biol Sci 1983, 219, 281–313. [Google Scholar] [CrossRef] [PubMed]
- Barh, D.; Tiwari, S.; Rodrigues Gomes, L.G.; Ramalho Pinto, C.H.; Andrade, B.S.; Ahmad, S.; Aljabali, A.A.A.; Alzahrani, K.J.; Banjer, H.J.; Hassan, S.S.; et al. SARS-CoV-2 Variants Show a Gradual Declining Pathogenicity and Pro-Inflammatory Cytokine Stimulation, an Increasing Antigenic and Anti-Inflammatory Cytokine Induction, and Rising Structural Protein Instability: A Minimal Number Genome-Based Approach. Inflammation 2023, 46, 297–312. [Google Scholar] [CrossRef] [PubMed]
- Koelle, K.; Martin, M.A.; Antia, R.; Lopman, B.; Dean, N.E. The changing epidemiology of SARS-CoV-2. Science 2022, 375, 1116–1121. [Google Scholar] [CrossRef]
- Sayeed, M.A.; Ferdous, J.; Saha, O.; Islam, S.; Choudhury, S.D.; Abedin, J.; Hassan, M.M.; Islam, A. Transmission Dynamics and Genomic Epidemiology of Emerging Variants of SARS-CoV-2 in Bangladesh. Trop Med Infect Dis 2022, 7. [Google Scholar] [CrossRef] [PubMed]
- Castro, E.S.A.; Bernardes, A.T.; Barbosa, E.A.G.; Chagas, I.; Dattilo, W.; Reis, A.B.; Ribeiro, S.P. Successive Pandemic Waves with Different Virulent Strains and the Effects of Vaccination for SARS-CoV-2. Vaccines (Basel) 2022, 10. [Google Scholar] [CrossRef]
- Hung, L.S. The SARS epidemic in Hong Kong: what lessons have we learned? J R Soc Med 2003, 96, 374–378. [Google Scholar] [CrossRef]
- Ferreira-de-Lima, V.H.; Lima-Camara, T.N. Natural vertical transmission of dengue virus in Aedes aegypti and Aedes albopictus: a systematic review. Parasit Vectors 2018, 11, 77. [Google Scholar] [CrossRef]
- Cunha, M.d.C.M. Dengue em Belo Horizonte, 2002 a 2016: Distribuição espaço-temporal e intervenções de requalificação urbana. Universidade Federal de Minas Gerais, 2021.
- Robert, M.A.; Stewart-Ibarra, A.M.; Estallo, E.L. Climate change and viral emergence: evidence from Aedes-borne arboviruses. Curr Opin Virol 2020, 40, 41–47. [Google Scholar] [CrossRef]
- Ritchie, S.A.; Pyke, A.T.; Hall-Mendelin, S.; Day, A.; Mores, C.N.; Christofferson, R.C.; Gubler, D.J.; Bennett, S.N.; van den Hurk, A.F. An explosive epidemic of DENV-3 in Cairns, Australia. PLoS One 2013, 8, e68137. [Google Scholar] [CrossRef]
- Watts, D.M.; Burke, D.S.; Harrison, B.A.; Whitmire, R.E.; Nisalak, A. Effect of temperature on the vector efficiency of Aedes aegypti for dengue 2 virus. Am J Trop Med Hyg 1987, 36, 143–152. [Google Scholar] [CrossRef]
- Focks, D.A.; Daniels, E.; Haile, D.G.; Keesling, J.E. A simulation model of the epidemiology of urban dengue fever: literature analysis, model development, preliminary validation, and samples of simulation results. Am J Trop Med Hyg 1995, 53, 489–506. [Google Scholar] [CrossRef]
- Chan, M.; Johansson, M.A. The incubation periods of Dengue viruses. PLoS One 2012, 7, e50972. [Google Scholar] [CrossRef] [PubMed]
- Reinhold, J.M.; Lazzari, C.R.; Lahondere, C. Effects of the Environmental Temperature on Aedes aegypti and Aedes albopictus Mosquitoes: A Review. Insects 2018, 9. [Google Scholar] [CrossRef] [PubMed]
- Alves de Oliveira, B.F.; Bottino, M.J.; Nobre, P.; Nobre, C.A. Deforestation and climate change are projected to increase heat stress risk in the Brazilian Amazon. Communications Earth & Environment 2021, 2, 207. [Google Scholar] [CrossRef]
- Graça, M.; Cruz, S.; Monteiro, A.; Neset, T.-S. Designing urban green spaces for climate adaptation: A critical review of research outputs. Urban Climate 2022, 42, 101126. [Google Scholar] [CrossRef]
- COP28. Conference of the Parties serving as the meeting of the Parties to the Paris Agreement, Fifth session, United Arab Emirates, 30 November to 12 December 2023, Agenda item 4, First global stocktake. Acessed in 14 December 2023 in https://www.cop28.com/en/. 2023.
Figure 1.
Incidence of dengue fever per year (A) and average incidence per month (B), Belo Horizonte, Brazil.
Figure 1.
Incidence of dengue fever per year (A) and average incidence per month (B), Belo Horizonte, Brazil.
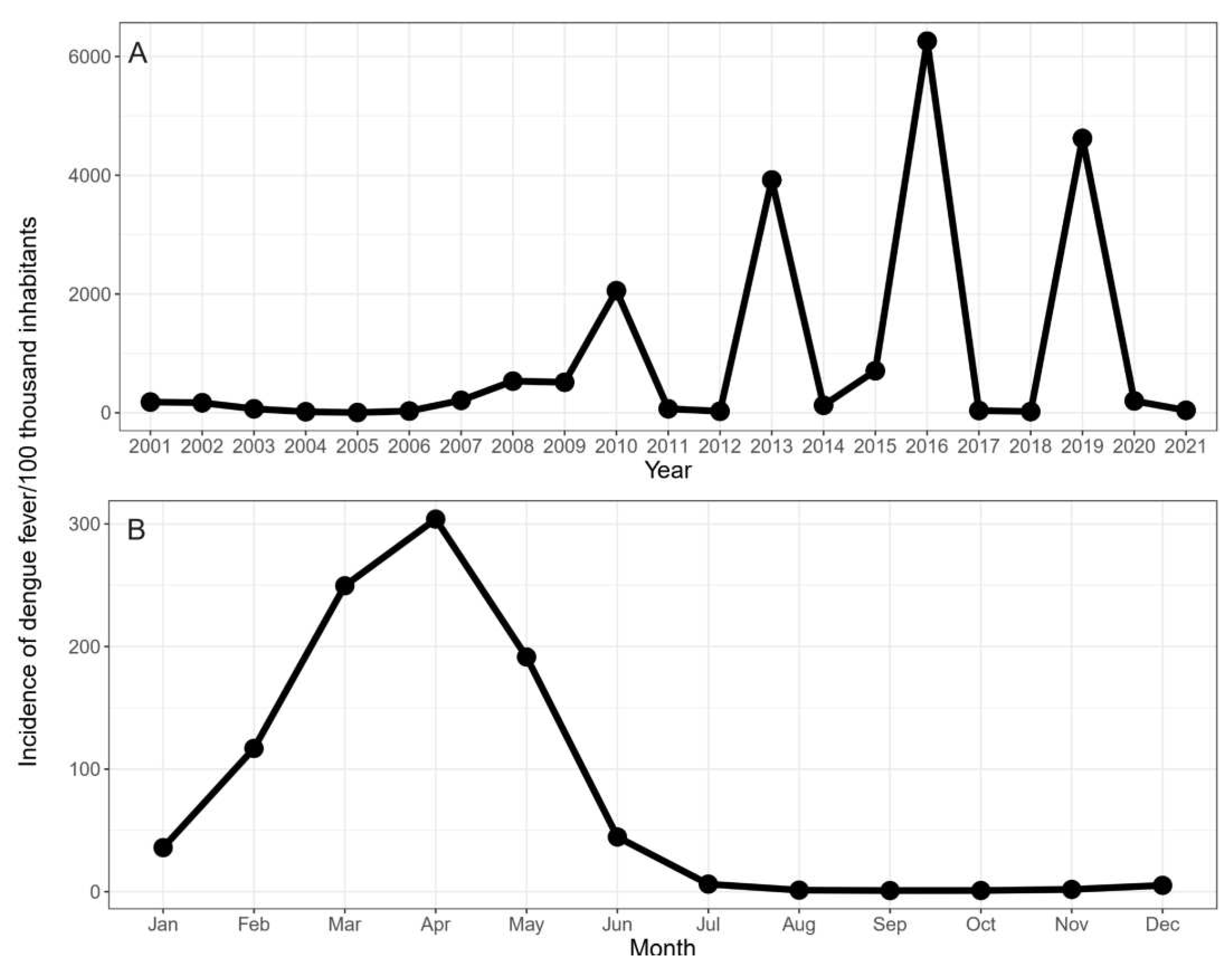
Figure 2.
(A) Monthly average maximum, mean and minimum temperature, (B) average monthly precipitation and (C) average monthly relative humidity.
Figure 2.
(A) Monthly average maximum, mean and minimum temperature, (B) average monthly precipitation and (C) average monthly relative humidity.
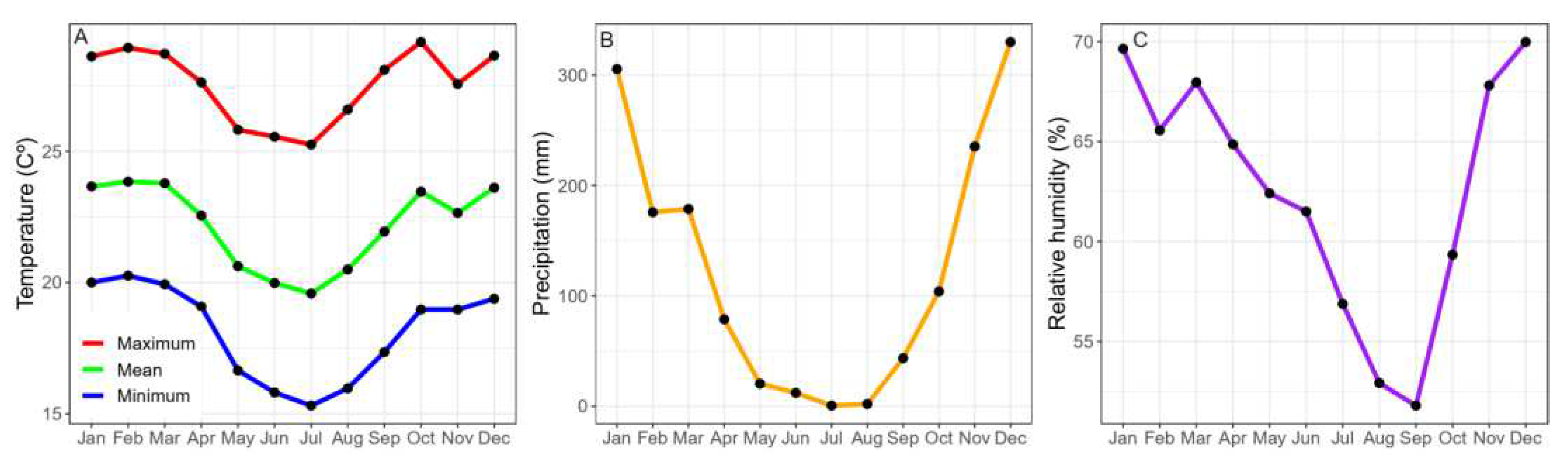
Figure 3.
Dengue incidence rates in epidemic years or not in response to monthly average maximum, mean and minimum temperature, average monthly precipitation and average monthly relative humidity.
Figure 3.
Dengue incidence rates in epidemic years or not in response to monthly average maximum, mean and minimum temperature, average monthly precipitation and average monthly relative humidity.
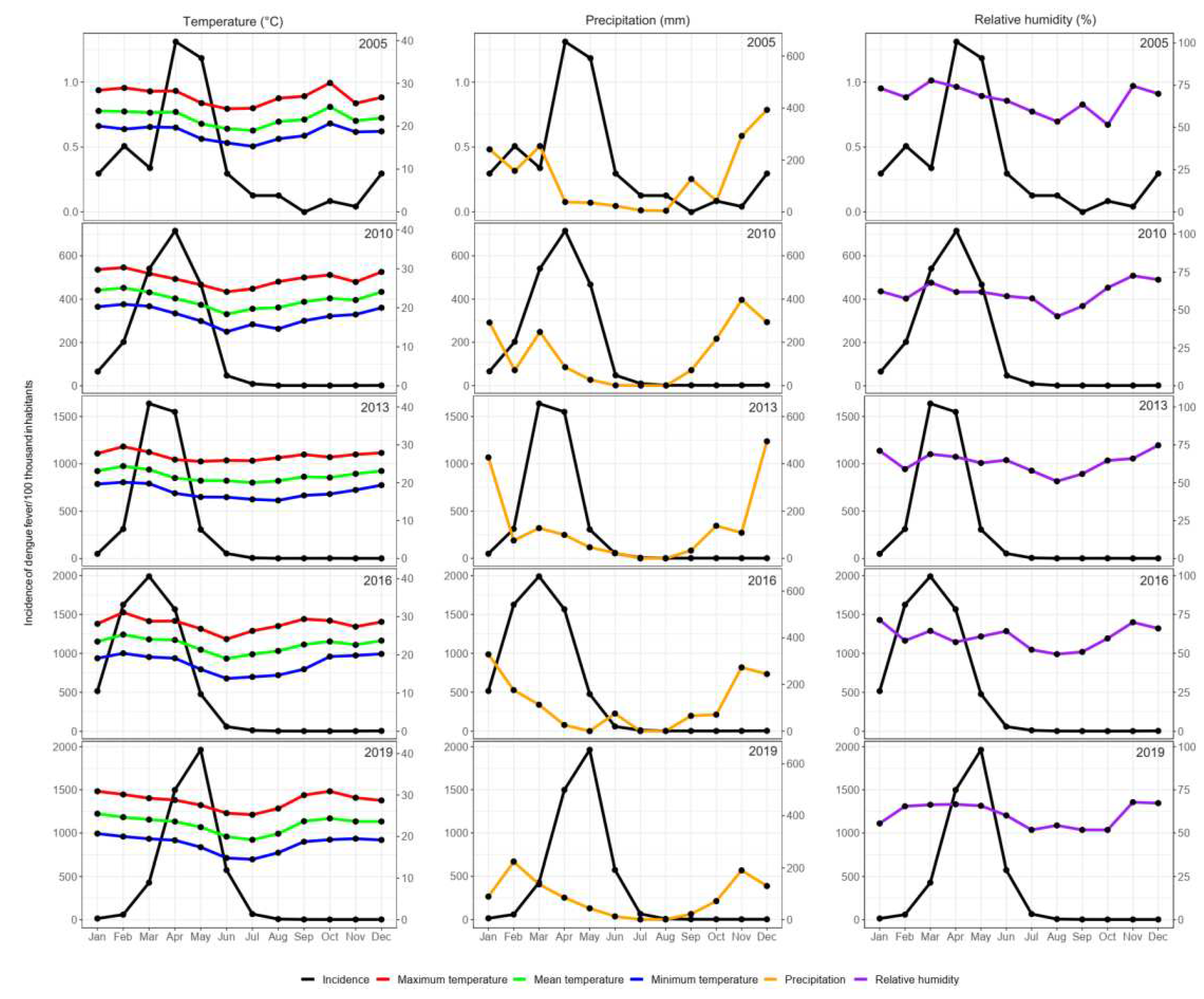

Table 1.
Climatic and temporal variables associated with the incidence of dengue fever, 2001-2021, Belo Horizonte, Brazil.
Table 1.
Climatic and temporal variables associated with the incidence of dengue fever, 2001-2021, Belo Horizonte, Brazil.
| Variables | No-Lag Model | 1-Month Lag Model | 2-Month Lag Model | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| IRR | 95% CI | p Value | IRR | 95% CI | p Value | IRR | 95% CI | p Value | ||||
| Maximum temperature | 1.501 | 1.267 | 1.781 | < 0.001 | ||||||||
| Mean temperature |
1.89 | 1.555 | 2.35 | < 0.001 | 1.918 | 1.573 | 2.349 | < 0.001 | ||||
| April | Reference | Reference | Reference | |||||||||
| January | 0.086 | 0.035 | 0.216 | < 0.001 | 0.177 | 0.073 | 0.432 | < 0.001 | 0.068 | 0.028 | 0.166 | < 0.001 |
| February | 0.115 | 0.041 | 0.316 | < 0.001 | 0.429 | 0.179 | 1.021 | 0.055 | 0.401 | 0.168 | 0.953 | 0.036 |
| March | 0.523 | 0.209 | 1.300 | 0.153 | 0.443 | 0.180 | 1.082 | 0.066 | 0.595 | 0.247 | 1.424 | 0.250 |
| May | 0.909 | 0.367 | 2.238 | 0.840 | 0.553 | 0.230 | 1.323 | 0.177 | 0.238 | 0.095 | 0.598 | 0.002 |
| June | 0.353 | 0.135 | 0.914 | 0.035 | 0.639 | 0.237 | 1.715 | 0.393 | 0.082 | 0.034 | 0.200 | < 0.001 |
| July | 0.049 | 0.019 | 0.128 | < 0.001 | 0.279 | 0.085 | 0.909 | 0.0289 | 0.064 | 0.025 | 0.162 | < 0.001 |
| August | 0.006 | 0.002 | 0.015 | < 0.001 | 0.067 | 0.020 | 0.226 | < 0.001 | 0.036 | 0.012 | 0.106 | < 0.001 |
| September | 0.002 | 0.001 | 0.005 | < 0.001 | 0.026 | 0.009 | 0.077 | < 0.001 | 0.033 | 0.011 | 0.103 | < 0.001 |
| October | 0.002 | 0.001 | 0.005 | < 0.001 | 0.009 | 0.003 | 0.022 | < 0.001 | 0.017 | 0.006 | 0.044 | < 0.001 |
| November | 0.005 | 0.002 | 0.012 | < 0.001 | 0.009 | 0.004 | 0.021 | < 0.001 | 0.008 | 0.003 | 0.020 | < 0.001 |
| December | 0.009 | 0.004 | 0.023 | < 0.001 | 0.016 | 0.007 | 0.039 | < 0.001 | 0.009 | 0.004 | 0.022 | < 0.001 |
| AIC | 3325.805 | 3310.732 | 3307.799 | |||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



