Submitted:
11 December 2023
Posted:
12 December 2023
You are already at the latest version
Abstract
In implantology, among the key choices, to obtain predictable results, it’s essential to establish, using CBCT, the bone site where to insert the implants; these sites must be identified on the mucosa and secondarily, during the surgical phase, on the cortical bone. Surgical templates are a valid aid especially in complex cases which require sev-eral implants.
In cases of single implant, on the other hand, surgical guides are rarely used and the implant is inserted freehand and the identification of the implant site on the oral mucosa is more difficult; for this reason the clinician uses the teeth in the arch as a ref-erence. This experimental study is based on the use of a thermo-printed mask, con-taining radiopaque references which, worn by edentulous patients during the execu-tion of the CBCT, helps to evaluate the identification of the implant sites on the patient when surgical guides are not used and the free hand technique is adopted.
This method is certainly reserved for experienced operators capable of identifying the correct angle of the implants with the freehand technique. The level of experience remains fundamental in the clinician's decision whether or not to use surgical guides; in fact, doctors with little experience should use surgical guides even in the simplest cases to reduce the risk of error.
Keywords:
Implantology
; implant site identification
; freehand technique
INTRODUCTION
In implantology it’s a priority to establish where to insert the implants and which angle to give them. CBCT has allowed, through computerized image processing, a simplified and precise organization of surgical procedures [1,2]; in fact, CBCT permits the clinician to accurately evaluate the maxillary or mandibular bone to decide the best sites for the fixtures.
The three-dimensional CBCT images can be imported into implant planning software, through which they are analyzed in order to determine the bone density and the number, position and correct inclination of the implants.
DICOM data from computed tomography also allow, through their software processing, to produce, using 3D printers, three-dimensional objects such as surgical guides [3,4,5] which simplify the clinical localization of the implant site, guaranteeing predictable results [6,7,8,9,10].
The surgical guides are made with through holes, inside which there are metal bushings that correspond to the position and insertion angle of the implants in order to guide the surgical drills necessary for the creation of the artificial socket.
The surgical guides would guarantee the patient a more comfortable, less invasive and risky surgical procedure (sometimes flapless) and short recovery times.
Nowadays computer-assisted implant planning also permits additional services such as the digital workflow, which allows the dental practice or laboratory to digitalize the entire process, using intraoral and plaster scanners, CAD/CAM system and 3D printers.
On the other hand, the creation of such guides, in some cases, could be an excessively complex and onerous solution when compared to the size of the edentulous site and the number of implants to be inserted [11,12,13]. In some clinical conditions where few implants are foreseen, expert operators prefer, even in totally edentulous arches, to insert the implants freehand. When surgical guides are not used, during the surgical procedures, to identify with certainty where to insert the fixtures becomes a difficult task.
During freehand procedures it’s essential to consider anatomical references, such as the teeth in the arch, which help, first of all, to identify the chosen site on the patient’s mucosa and on the bone.
In the case of mono edentulism, the risk of error in identifying the implant site is minimal thanks to the presence of mesial and/or distal teeth close to the implant area. The error can become greater when the width of the edentulous area increases; the distance between the natural teeth, used as a reference, and the presumed area where the implant will be inserted, can influence the surgeon’s ability to identify the site on the mucosa [14,15,16,17].
If the arch is totally edentulous, identifying the implant sites chosen on the CBCT on the mucosa and secondarily on the bone cortex could be very difficult or even impossible without the help of a surgical guide.
This study proposes a much simpler alternative (although reserved for expert operators) to complex surgical guides when a free hand technique is performed in totally edentulous arches.
In fact, it’s possible to build a thermo printed mask with radiopaque references to be worn by patients during the CBCT procedure.
These simple devices could improve the ability to identify the selected implant sites on CBCT, initially on the mucosa and secondarily on the bone cortex.
MATERIALS AND METHODS
This study is part of a bigger research on how to organize the entire implant protocol optimizing any single step based on the clinical needs of the patient and the implant surgeon.
This clinical research was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of the Paolo Giaccone University of Palermo (Protocol Code: #4-19-04-23).
All patients taking part in the study read and signed a declaration of consent to participate in the research and to publish the data.
From a sample of 54 edentulous patients, 22 patients with total edentulism were selected for whom prosthetic rehabilitations with multiple implants were planned.
In total 128 implants were programmed on 32 totally edentully arches.
Preliminary panoramic radiograph were taken on all patients as well as alginate impressions in order to obtain plaster models.
By interfacing the clinical and radiographic data (panoramic x-ray), an expert implantologist has previously identified the sites where the implants could possibly be positioned, identifying a higher number than the actual number to be inserted. The chosen points were then marked on the plaster models with a marker.
For each patient, steel spheres with a diameter of 3 millimeters were glued onto the diagnostic plaster models exactly in the points marked by the felt-tip pen. Thermo-printed templates (thickness 0.5 mm - soft consistency) were made on the plaster models thus modified.
These templates, during the hot thermoforming, detached and incorporated the tiny spheres previously positioned on the plaster; in this way each template has a radiopaque sphere in correspondence with the presumed implant site.
Figure 1.
Plaster model.
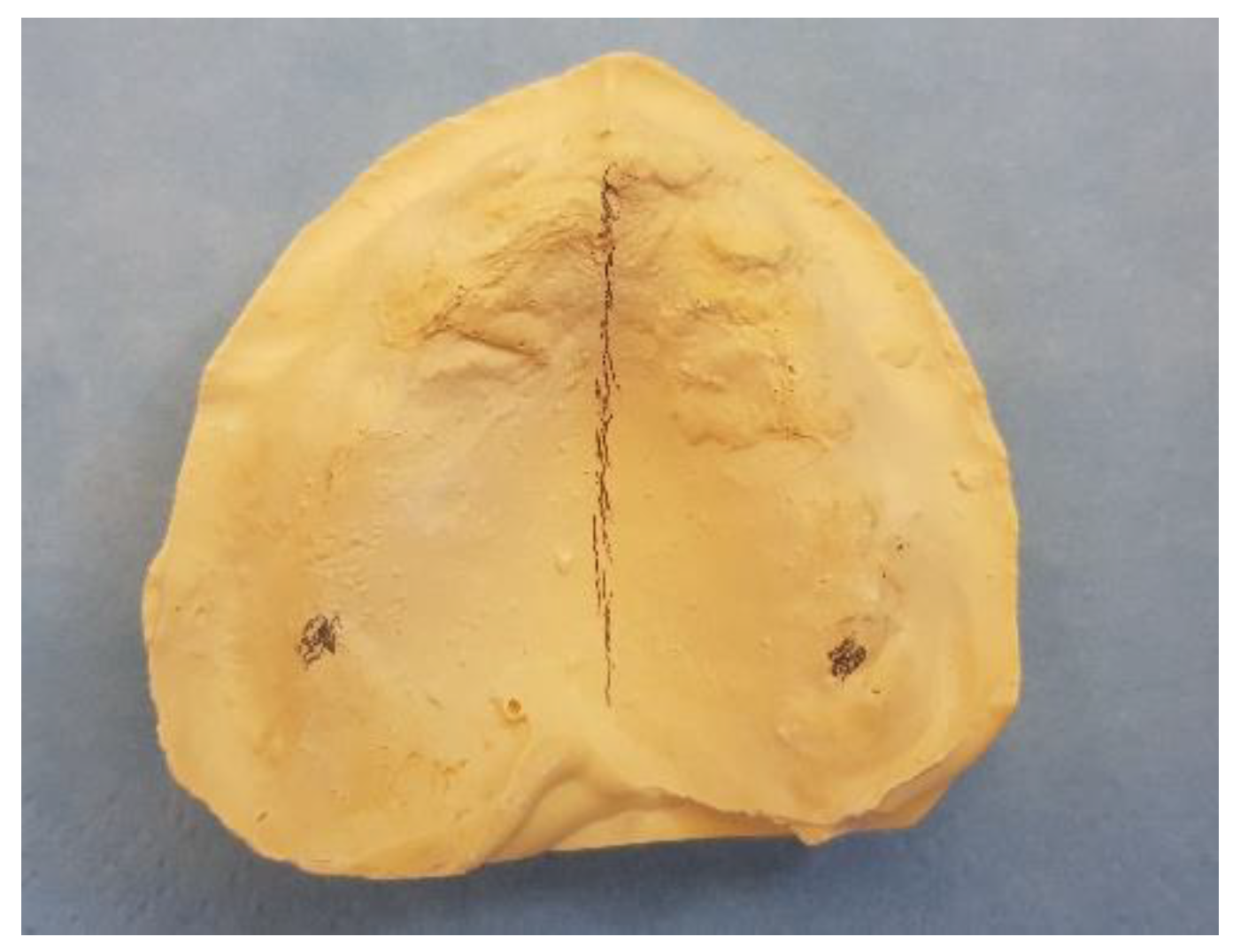
Figure 2.
Experimental template with radiopaque sphere.

A total of 32 masks were thermoformed for each edentulous arch and CBCT was performed for all patients during which the masks with radiopaque references were worn.
Each individual CBCTs was analyzed by an expert implantologist in order to find the best sites where to place the implants.
For a total of 26 implant sites chosen in the panoramic radiograph, the preliminary site selection was confirmed; for the remaining 102 implants a different site was chosen on the CBCT.
During the free hand surgical phase, planned and performed by an expert operator with more than 20 years of experience, in order to best identify the implant sites chosen on the CBCT on the mucosa, the patients wore masks with radiopaque references.
A mark was made on the mucosa in correspondence with the radiographic landmark with an indelible felt-pen.
In this way, these signs, simulating certain and visible anatomical landmarks in the CBCT, have enormously facilitated the identification of the implant site on the cortex which is a very critical phase in the free hand technique (See Table 1).
By interfacing the information coming from the plaster models, from the panoramic radiography, from the CBCT, from the clinical examination of the patient’s mucosa with the mask worn, the risk of error has been minimised.

Table 1.
Flow chart.
| 1 | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|
| Patient selection | Pre-identification of implant sites on panoramic radiograph | Identification of implant sites on plaster cast | Template construction | CBCT with thermoformed tamplate | Final identification implant site on CBCT | Identification implant site on arch by template |
Figure 3.
Panoramic view on CBCT.
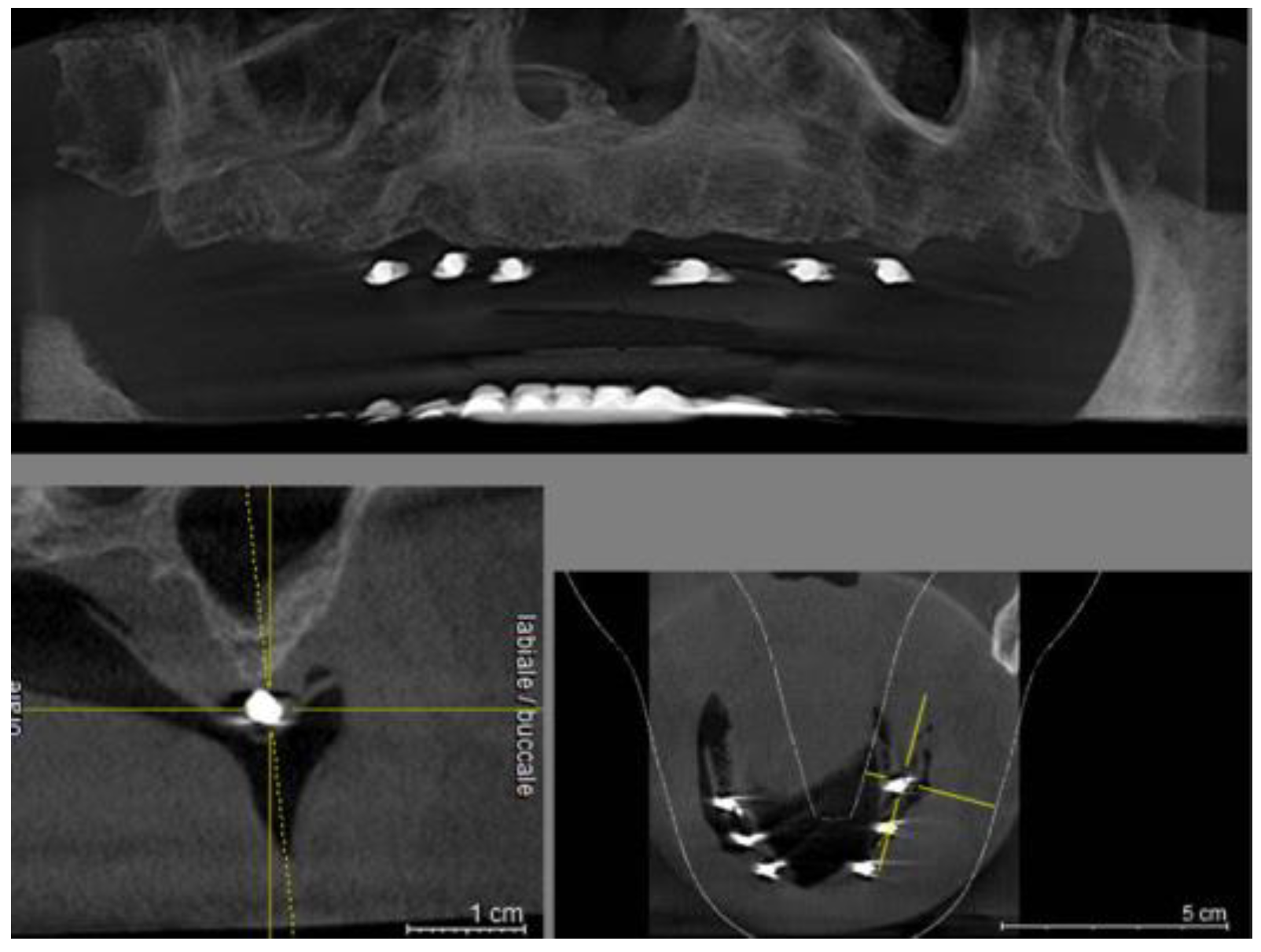
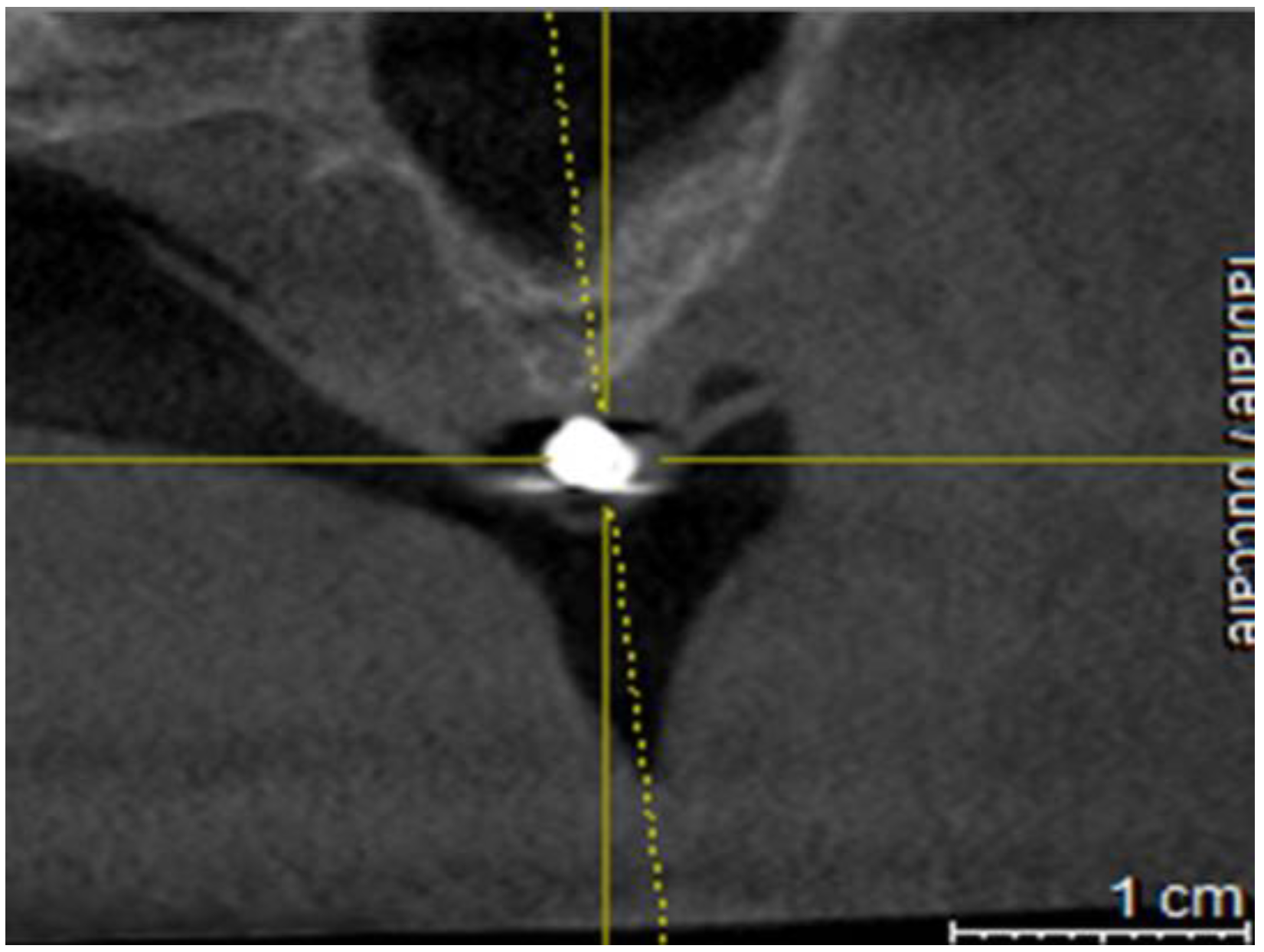
Figure 4.
Cross section on CBCT.
DISCUSSION
Nowadays the use of computers and information technology in dental practices and dental laboratories is widespread and a large part of patient information follows a digital flow which makes clinical procedures faster. All clinical information from the doctor to the dental technician moves digitally and quickly with advantages for the patient. The construction of surgical guides represents an example of how the digital flow of information can help the implantologist especially in complex cases with multiple implants.
In certain clinical conditions, such as monodentulism, it’s easy to identify the spot on the mucosa where to place the implant. In these cases, the presence of contiguous teeth (mesial and/or distal) adjacent to the edentulous site offers the implantologist certain points of reference. When the presumed implant site is far from a natural tooth and when the latter are only mesial or distal (Kennedy class I or II), precisely identifying the exact point of the mucosa where to insert the implant is more difficult.
This imprecision, due to the reduced ability of the human eye to evaluate distances as the reference anatomical finding moves away, often pushes the implantologist to use surgical templates which also give important indications on the angle to be given to the axis of the fixture [18].
In totally edentulous patients, lacking natural teeth that are used as landmarks, it is even more difficult to locate the sites chosen on the CBCT on the mucosa.
This is the reason why surgical guides, in these clinical conditions, are widely used, also providing valuable information on the insertion axis of the implants [19,20].
This preliminary study was conducted by expert implantologists and this could represent a limitation in the experimentation which will be extended to clinicians with different levels of experience in order to obtain more detailed results.
Naturally, the type of information provided by these thermo-printed guides is reduced to the mere identification of the point on the mucosa and bone where to insert the fixture without the aid of additional information on the angle.
Regarding the angulation of the implants, the clinician must refer to the data acquired through a CBCT as normally occurs in the execution of freehand techniques [21,22,23].
In more complex cases, however, the use of more expensive and complex surgical guides appears more appropriate [24,25].
In any case, guided system still remains a more acceptable and stable option for beginners [26].
CONCLUSIONS
This research is part of a study that examines a whole series of preliminary evaluations that the implantologist carries out during the setting of the intervention. The design of such a delicate treatment, which has a high biological cost for the patient, requires attention and is aimed at obtaining predictable results. This study is based on thermo-printed templates that, in particular clinical conditions, could be a valid and chip alternative to the classical surgical dime.
It is important to clarify that dentists should inform patients that computer guided surgery implies additional costs; however the cost-effectiveness involving some positives, like the reduction of surgery time, post-operative discomfort and better soft tissue healing, may render it worthwhile. While implant software is a great help in making clinical decisions, it is important to realize that responsibility for the outcome and patient safety during guided surgery remains with the surgeon.
The level of experience is fundamental in the clinician’s decision whether or not to use surgical guides; in fact doctors with little experience should use surgical guides even in the simplest cases to reduce the risk of error.
This new method, proposed as an alternative to the complex creation of classic surgical guides, can certainly be improved and is the subject of study, in fact further research on what can help the surgeon in the phase planning phase is currently underway.
References
- Orentlicher G, Horowitz A, Abboud M. Computer-guided implant surgery: Indications and guidelines for use. Compend Contin Educ Dent. 2012;33: 720–732; quiz 33.
- D’Haese, J.; Ackhurst, J.; Wismeijer, D.; De Bruyn, H.; Tahmaseb, A. Current state of the art of computer-guided implant surgery. Periodontology 2017, 73, 121–133. [Google Scholar] [CrossRef]
- Graham R N J, Perriss R W, Scarsbrook A F. DICOM demystified: a review of digital file formats and their use in radiological practice Clin. Radiol., 60 (2005), pp. 1133-1140.
- Kalra M, Aparna IN, Dhanasekar B. Evolution of surgical guidance in implant dentistry. Dent Update. 2013;40:577– 578, 581–582.
- Kola MZ, Shah AH, Khalil HS, et al. Surgical templates for dental implant positioning; current knowledge and clinical perspectives. Niger J Surg. 2015; 21:1–5.
- Scherer U, Stoetzer M, Ruecker M, Gellrich N C. See Template-guided vs. non-guided drilling in site preparation of dental implants Clin. Oral Investig., 19 (2015), pp. 1339-1346.
- Schnutenhaus S, Edelmann C, Rudolph H, Dreyhaupt J, Luthardt R G. 3D accuracy of implant positions in template-guided implant placement as a function of the remaining teeth and the surgical procedure. A retrospective study Clin. Oral Investig., 22 (2018), pp. 2363-2372.
- Younes F, Cosyn J, De Bruyckere T, Cleymaet R, Bouckaert E, Eghbali A. A randomized controlled study on the accuracy of free-handed, pilot-drill guided and fully guided implant surgery in partially edentulous patients J. Clin. Periodontol., 45 (2018), pp. 721-732.
- Otaghsara SS, Joda T, Thieringer FM. Accuracy of dental implant placement using static versus dynamic computer-assisted implant surgery: An in vitro study. Journal of Dentistry. 2023 May 1;132:104487.
- Alqutaibi AY. CAD-CAM surgically-guided oral implant site expansion and implant placement in severely atrophic maxilla. Journal of Taibah University Medical Sciences. 2020 Apr 1;15(2):153-9.
- Behneke, M. Burwinkel, N. Behneke Factors influencing transfer accuracy of cone beam CT-derived template-based implant placement Clin. Oral Implants Res., 23 (2012), pp. 416-423.
- Gargallo-Albiol, J., Barootchi, S., Salomó-Coll, O., Wang, H.-L., 2019. Advantages anddisadvantages of implant navigation surgery. A systematic review. Ann. Anat.225, 1–10.
- Sancho-Puchades, M.; Alfaro, F.H.; Naenni, N.; Jung, R.; Hammerle, C.; Schneider, D. A Randomized Controlled Clinical Trial Comparing Conventional and Computer-Assisted Implant Planning and Placement in Partially Edentulous Patients. Part 2: Patient Related Outcome Measures. Int. J. Periodontics Restor. Dent. 2019, 39, e99–e110. [Google Scholar] [CrossRef]
- Choi W, Nguyen B-C, Doan A, Girod S, Gaudilliere B, Gaudilliere D. Freehand versus guided surgery. Factors influencing accuracy of dental implant placement Implant Dent., 26 (2017), pp. 500-509.
- Kramer FJ, Baethge C, Swennen G, et al. Navigated vs. conventional implant insertion for maxillary single tooth replacement. Clin Oral Implants Res. 2005;16:60–68.
- Chen, S.; Ou, Q.; Lin, X.; Wang, Y. Comparison Between a Computer-Aided Surgical Template and the Free-Hand Method: A Systematic Review and Meta-Analysis. Implant Dent. 2019, 28, 578–589. [Google Scholar] [CrossRef] [PubMed]
- Schnitman, P.A.; Hayashi, C.; Han, R.K. Why guided when freehand is easier, quicker, and less costly? J. Oral Implantol. 2014, 40, 670–678. [Google Scholar] [CrossRef]
- Dimitrijevic T, Kahler B, Evans G, Collins M, Moule A. Depth and distance perception of dentists and dental students Oper. Dent., 36 (2011), pp. 467-477.
- S. Hillerup Iatrogenic injury to oral branches of the trigeminal nerve: records of 449 cases Clin. Oral Investig., 11 (2007), pp. 133-142.
- Payer M, Kirmeier R, Jakse N, et al. Surgical factors influencing mesiodistal implant angulation. Clin Oral Implants Res. 2008;19:265–270.
- Nickenig H J, Wichmann M, Hamel J, Schlegel K A, Eitner S. Evaluation of the difference in accuracy between implant placement by virtual planning data and surgical guide templates versus the conventional free-hand method - a combined in vivo – in vitro technique using cone-beam CT (Part II) J. Cranio Maxillofac. Surg., 38 (2010), pp. 488-493.
- Schulz M C, Rittmann L, Range U, Lauer G, Haim D. The use of orientation templates and free-hand implant insertion in artificial mandibles-an experimental laboratory examination in fifth-year dental students Dent. J., 6 (2018).
- Vermeulen, J. The accuracy of implant placement by experienced surgeons. Guided vs freehand approach in a simulated plastic model Int. J. Oral Maxillofac. Implants, 32 (2017), pp. 617-624.
- Schulz, M.C., Hofmann, F., Range, U., Lauer, G., Haim, D., 2019. Pilot-drill guided vs.full-guided implant insertion in artificial mandibles-a prospective laboratorystudy in fifth-year dental students. Int. J. Implant Dent. 5, 23.
- Park, J.Y.; Song, Y.W.; Park, S.H.; Kim, J.H.; Park, J.M.; Lee, J.S. Clinical factors influencing implant positioning by guided surgery using a nonmetal sleeve template in the partially edentulous ridge: Multiple regression analysis of a prospective cohort. Clin. Oral Implants Res. 2020, 31, 1187–1198. [Google Scholar] [CrossRef]
- Shetty SR, Murray CA, Al Kawas S, Jaser S, Al-Rawi N, Talaat W, Narasimhan S, Shetty S, Adtani P, Hegde S. Impact of fully guided implant planning software training on the knowledge acquisition and satisfaction of dental undergraduate students. Medical Education Online. 2023 Dec 31;28(1):2239453.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



