Submitted:
01 December 2023
Posted:
04 December 2023
You are already at the latest version
Abstract
The lack of accurate and feasible diagnostic tests poses a significant challenge to visceral leish-maniasis (VL) healthcare services in endemic areas. To date, various VL diagnostic tests have been or are being developed, and their diagnostic performance needs to be assessed.. In the present study, the diagnostic performance of rk39RDT, Direct Agglutination Test (DAT), Microscopy, Loop Mediated Isothermal Amplification (LAMP), and miniature direct-on-blood polymerase chain reaction - nucleic acid lateral flow immunoassay (mini-dbPCR-NALFIA) was assessed using quantitative polymerase chain reaction (qPCR) as reference test in an endemic region of Ethiopia. In this study, 235 patients VL suspected patients and 104 non-endemic healthy controls (NEHC) were recruited. Among the VL-suspected patients, 144(61.28%) tested positive with qPCR. Sensi-tivities for rk39 RDT, DAT, Microscopy, LAMP assay, and mini-dbPCR-NALFIA were 88.11%, 96.50%, 76.58%, 94.33%, and 95.80%, respectively. Specificities were 83.33%, 97.96%, 100%, 97.38%, and 98.92% for rk39 RDT, DAT, Microscopy, LAMP assay, and mini-dbPCR-NALFIA, respectively. In conclusion, Rk39 RDT and microscopy exhibited lower sensitivity, while DAT demonstrated excellent performance. LAMP and mini-dbPCR-NALFIA showed excellent perfor-mance with feasibility to implement in remote endemic areas, although the latter requires further evaluation in such regions.
Keywords:
rk39 Rapid Diagnostic Test
; Direct Agglutination Test
; Microscopy
; loop-mediated isothermal am-plification
; miniature direct-on-blood polymerase chain reaction - nucleic acid lateral flow immu-noassay
1. Introduction
Millions of individuals across the globe have the risk of acquiring visceral leishmaniasis (VL), a deadly neglected (sub-)tropical infectious disease caused by parasites of the Leishmania donovani complex and transmitted through the bite of an infected female sand-fly [1] belonging to the genus Phlebotomus in the old world or Lutzomyia in the new-world [2,3]. Worldwide, approximately 50,000 annual deaths are recorded, and East Africa and Southeast Asia share the highest burden of the disease [4]. Over 90% of the world’s VL incidences are attributed to five less developed countries namely Ethiopia, Bangladesh, India, Brazil, Sudan, and South Sudan [5,6]. VL, which is characterized by protracted fever, fatigue, splenomegaly, anemia, and loss of weight, is lethal if accurate therapy is not timely given [7,8]. Post-Kala-Azar Dermal Leishmaniasis (PKDL), a macular, maculopapular, or nodular rash on the face, torso, or other parts of the body, is one of the complications of the VL in immunocompromised individuals, which may occur some months after treatment [9,10]. Since the clinical presentations of VL mimics other febrile diseases and often share the same geographic areas, the clinical features alone are insufficient to make a differential diagnosis and prescribe anti-VL drugs. In addition, anti-VL drugs are not always safe and effective, and therefore empirical treatment is not recommended [11]. Consequently, timely and accurate diagnostic tests are critical to install the best possible treatment options.
In most VL-endemic resource-limited countries, the diagnosis of VL relies on a combination of the patient's clinical presentation and rapid serological tests and/or microscopy of Giemsa-stained tissue aspirate/s [12,13,14]. Despite its poor performance and risky specimen collection procedures, microscopy is still often used as the reference standard for VL diagnosis in many endemic countries. Serologic tests, primarily the rk39-based rapid diagnostic test (RDT), although highly variable and with reported moderate diagnostic performance, is frequently used as a first-line screening test [15,16,17]. The direct agglutination test (DAT), which has a better sensitivity and specificity than rk39 RDT, but requires an overnight incubation and some more laboratory infrastructure, is used as an alternative sero-diagnostic test[18,19]. The main drawback of any of the available serological tests is their inability to differentiate active VL patients from past or asymptomatic infections, especially in the endemic areas [19].
Molecular tests, like end-point Polymerase Chain Reaction (PCR) and qualitative PCR (qPCR),are highly sensitive and specific tests [20,21]. However, due to time-consuming procedures, costly equipment, and reagent and infrastructural requirements, the implementation of molecular tests is hindered in resource-limited countries [22]. In response to this, nowadays efforts are made to innovate and develop sensitive, specific, and rapid tests that are feasible to implement in remote VL endemic areas of resource-constrained countries [23,24,25]. Therefore, the discoveries of cost-effective and user-friendly tests are crucial to enhance the diagnosis and monitoring of VL, particularly in laboratories with limited resources [26]. The loop-mediated isothermal amplification (LAMP) [27,28,29] assay and miniature direct-on-blood polymerase chain reaction combined with nucleic acid lateral flow immunoassay (mini-dbPCR-NALFIA)[30] are two most effective diagnostic techniques that can be used in resource-limited countries.
The LAMP is a rapid, sensitive, and specific molecular diagnostic assay that can amplify DNA at a constant temperature without the need for an expensive thermocycler [31,32]. The LAMP assay is based on auto-cycling and a highly efficient DNA denaturing process mediated by Bst DNA polymerase [33]. The amplification processes of the LAMP assay takes place in two repeated steps; steam loop structure formation and auto-elongation at the 3’ end of the template gene and consecutive annealing and growing of primers using the loop region as template at isothermal temperature [27]. It has been successfully used for detecting Leishmania parasites and the assay has a proven potential for the diagnosis of VL in resource-constrained areas [34].
Similarly, the mini-dbPCR-NALFIA is a low-cost and simplified molecular test that combines the target DNA amplification directly from blood samples using a very simplified and portable mini-PCR machine and a nucleic acid lateral flow immunoassay detection system [35]. The assay utilizes a portable thermocycler that can be operated using portable power supply and solar panels, making it useful in areas where electricity is not available or reliable [30]. Additionally, the mini-dbPCR-NALFIA test was developed to circumvent DNA extraction, reducing the risk of contamination during that process [30]. Moreover, the mini-dbPCR-NALFIA uses a smartphone application to monitor the lysis and amplification process [30]. The resulting readout from the NALFIA strip is easy to interpret, similar to rapid dipstick serological tests, and doesn't necessitate any specialized skills or equipment. The result readout methods in LAMP and min-dbPCR-NALFIA tests are by visual inspection.
The research presented in this paper was designed to compare the diagnostic performance of four different diagnostics, i.e. rk39 RDT, DAT, LAMP assay, and mini-dbPCR-NALFIA, using qPCR as a reference standard to diagnose VL in the Tigray region, north Ethiopia. We have also included data from microscopic examination of Giemsa-stained splenic or bone marrow tissue aspirates, as a confirmatory test. However, this set of data is not complete as in several cases the patient was ineligible to do the sample collection procedure. These criteria include hemoglobin level, platelet count, age, and other underlying medical conditions. The Tigray region is highly endemic for VL and there is a pressing need to implement novel diagnostic tests in (remote) health centers in this region. The study included HIV positive as well as HIV negative cases. This is of particular interest as HIV positive cases tend to have a lower immune response and might be false negative in serological assays[36].
2. Materials and Methods
2.1. Ethical considerations
Ethical clearance was obtained from Mekelle University, College of Health Sciences and Ayder Comprehensive Specialized Referral Hospital, Health Research Ethics Review Committee (ERC number: 1102/2017), Mekelle, Tigray, north Ethiopia. Informed consent or assent was also obtained from the study participants or their guardian. In addition, a permission letter was obtained from the local authorities to each study sites.
2.2. Study Site and Participants
A prospective cohort study was conducted between July 2019 and October 2020 at Ayder Comprehensive Specialized Referral Hospital, Mekelle University, College of Health Sciences, Mekelle, Tigray, north Ethiopia. The objective of this study was to compare the diagnostic performance of 5 different VL diagnostic tests; rk39 RDT, DAT, Microscopy, LAMP, and mini-dbPCR-NALFIA with qPCR as reference standard. Cases clinically suspected of being VL patients were prospectively enrolled and clinical data and blood samples for diagnostic procedures were collected. The HIV-status all suspected VL cases was known prior to enrollment. Patients who had a VL treatment history within the past three months from the enrollment time and/or unable to understand and/or those who refused to give informed consent/assent were excluded from study. All enrolled patients were first tested using the rK39 RDT and/or microscopic examination of Giemsa-stained splenic or bone marrow aspirates to detect L. donovani amastigotes.
Non-endemic healthy controls (NEHCs) were also included in this study. The NEHC participants were recruited from areas that have no history of previous reported VL cases, and who had no travel history to a VL endemic area.
2.3. Laboratory analysis of blood samples
The rk39 RDT: When VL suspected patients visited the outpatient department VL clinics of the study areas, they were screened using rk39 RDT (IT LEISH, Bio-Rad Laboratories. Inc, The Netherlands) according to the manufacturer’s instructions. The rk39 RDT cassette is coated with rk39 antigen at the bottom and with anti-rk39 antigen antibodies at the top of the strips[37]. When the strip was dipped into a well containing a mixture of one drop of buffer (50µl) and 10-12µl of whole blood, the mixture started to move up by capillary action. If the blood contained anti-leishmania antibodies, a visible band or line was developed at test and control areas, and reported positive and if no band or line is appeared in test areas after 10 minutes of incubation, reported as negative[38]. A test result is considered invalid test if a visible line is not developed in the control areas.
The DAT: The DAT was performed at the Academic Medical Centre of the University of Amsterdam, Department of Microbiology and Infection Prevention, Experimental Parasitology Laboratory (AMC), using the Freeze-dried antigen (FD-Ag) produced by AMC. Dried blood spots (5mm) of EDTA blood of study cases on Whatman filter paper were punched out and placed into the first column of the V-shaped micro-titer plate and immersed in 125µL of normal saline[39]. The plates were incubated at ambient temperature (4-20℃) for 18-24 hours to eluate antibodies[40]. A serial dilution was made by adding 50 dilution serum (0.1M BME in 100 mL saline) into the next all columns and transferring 50µl from the first column to the next and continuing until the 11th column[41]. The 12th column was used as negative control and contained only the dilution fluid[1]. The DAT was considered positive if agglutination was observed at a titer of ≥ 1:3200[39].
Microscopy: Microscopic examination was done for clinical purpose. For this research; data were collected from the patients’ medical charts. Microscopic examination was done to detect the amastigote stage of L. donovani in Giemsa-stained splenic or bone marrow tissue aspirate at Pathology laboratory, Ayder Specialized referral Hospital, College of Health Sciences, Mekelle University and Kahsay Abera Hospital, Tigray Ethiopia. Results were reported on a graded scale ranging from negative (grade 0) when no amastigotes were seen, to grade 5+ if 10–100 parasites per field under the 100× oil-immersion lens was observed. Moreover, grading were also used for reporting different parasite densities: grade 4+ for 1–10 parasites per 10 fields, grade 3+ for 1–10 parasites per 100 fields, grade 2+ for 1–10 parasites per 100 fields, and grade 1+ for 1–10 parasites per 1000 fields, all observed through the 100× oil-immersion lens.[42].
LAMP assay: As described by Mukhtar M et al, 2018, the boil-and-spin method was used to extract DNA from the patient's whole blood [43]. In short, 95 µl of the patient’s blood was mixed with 5ml of 10% sodium dodecyl sulfate and mixed by inverting the mixture 10 times in 1.8ml Eppendorf tube. The mixture is then incubated for 10 minutes at room temperature and subsequently mixed to obtain a homogeneous solution. The mixture was next incubated at 95℃ in a heat block after addition of 400 µl of DNA-free water and spin-down at 13000 rpm for 3 minutes. The supernatant was collected for further analysis.
The LAMP assay was performed using LoopAmp Leishmania kit (Eiken Chemical Co., Tokyo, Japan) [44]. The kit employed 6 primers that target conserved Leishmania gene segment[13]: kDNA and 18S rRNA. LAMP assay utilized Bst polymerase, which has auto-DNA denaturing and amplification properties [33]. The LoopAmp kit included both positive and negative controls. For amplification, 3µl of DNA extract was mixed with 27 µl of MQ-water and the total run time was 40 minutes at 65℃ in the LF-160 incubator (HumaLoop M incubator, HUMAN, Wiesbaden, Germany). Results were visually inspected, positive samples turned to green color when exposed to UV light, while negative samples did not show any color change.
The mini-dbPCR-NALFIA: The mini-dbPCR-NALFIA technique for diagnosis VL detects of two distinct gene sets. The first set comprises the minicircle kinetoplast Leishmania DNA (kDNA) gene, which is highly conserved and present across all Leishmania species. The second gene is human glyceraldehyde 3-phosphate dehydrogenase (GAPDH), which serves as an internal amplification control. A mixture of 12.5 µl of Mytaq Blood PCR buffer (Meridian Bio-Sciences, Ohio, USA), 8µl of sterile water, and 0.625 µl each of forward and reverse primers labeled with Dig.-DH and Bio.DH (Eurogentec, Belgium) respectively were used for the kDNA amplification; and 0.375µl each of forward and reverse primers labeled with FAM-DH and Bio-DH (Eurogentec, Belgium) for GAPDH amplification. The mini-dbPCR-NALFIA amplification involved lysing of 2.5µl of EDTA blood at 98℃ for 10 minutes using a mini16 PCR machine. The PCR tube strip was placed into the machine and connected to a smartphone app via Bluetooth to monitor the process. The mini16 PCR amplification process was programmed as: initial denaturation at 95℃ for 3 sec 1x, denaturation at 95℃ for 15 sec 30x, annealing at 58℃ for 30 sec 30x, extension at 72℃ for 45 sec 30 cycles and final extension 72℃ for 120sec for 1x. The amplification process was also monitored by the mini16 mobile app via Bluetooth.
After completion of the PCR cycle and brief spin down, 10µl of the amplification product was added into a 1.5ml tube containing 140 µl of the PCRD flex buffer (Abingdon Health, York, UK).The mixture was gently vortexed and the NALFIA strip was dipped in the solution. The incubation time of the strip in the mixture was 10 minutes, and the presence of 3 black lines (for kDNA, GAPDH and flow control lines) was assessed by putting the strip on the white tissue paper.
The qPCR: qualitative Polymerase Chain Reaction (qPCR) was used as a reference standard to evaluate the different VL diagnostic tests. DNA was extracted using an automated easyMAG DNA extraction machine. In brief, 1.25µl of the extracted DNA template was added to 11.25µL of qPCR master mix which comprised; 6.25µL of iTaq Universal Probes Master Mix, 0.325µl of kDNA Forward primer and kDNA Reversed primer each, 0.125µl of kDNA probe, 0.125µl of Forward and Reverse GAPDH primer each, 0.125µl of GAPDH probe and 3.85µl of DNase-free water. The qPCR run was performed on BioRad CFX96 Real-Time PCR Machine (BioRad Laboratories, USA) which is programed as follows: UNG activation at 50℃ for 10 minutes, initial denaturation at 95°C for 5 minutes, denaturation at 95℃ for 15 seconds and Annealing/elongation + plate read at 59℃ for 15 seconds. With each qPCR run, a 10 folds serially diluted standard curve of DNA extracted from cultured L. donovani promastigotes was used. Analysis of the qPCR results was done using Bio-Rad Maestro data analysis Software.
2.4. Statistical analysis
Median with interquartile ranges (IQR) was used to describe continuous variables, whereas the categorical variables were expressed using proportions. Because of the interest in the performance of the different diagnostic tests in HIV positive individuals, we have used the McNemar chi-square (χ2) test to assess if the diagnostic performance the tests under evaluation significantly differed between HIV- positive and –negative cases. The sensitivity, specificity, positive and negative predictive values of the tests was determined using STATA Ver. 15.0, Stata Corp, College Station, TX using the results of qPCR as reference standard. The agreement between each test with the reference standard and between each other was determined using Cohen's kappa coefficient (kappa value). A p-value of less than 0.05% was considered statistically significant and the Standards for Reporting of Diagnostic Accuracy Studies (STARD) guidelines were followed for reporting the results. Using Stata V.15. The receivers’ operator characteristic curve (ROC curve) analysis was also used for further assessment of the performance of the tests.
Results
3.1. Study Participants
In total, 235 VL-suspected cases were recruited in this study. The median age of the VL-suspected participants was 24.0 ± 13.2 (SD) years. Approximately a quarter of the study participants were pediatric patients (<18 years old). The majority, 220 (93.2%) of the study participants were male and 204 (86.8%) of them were from the Tigray region. The most common clinical presentations of the study participants were fever 226 (96.2%), splenomegaly 179 (76.2%), weight loss 218 (92.8%), and fatigue 199 (84.6%), Table 1. One hundred seventy five (66.8%) of the study participants had abnormally high levels of aspartate aminotransferase (AST) and 101 (42.98%) had elevated alanine aminotransferase (ALT) enzyme levels. In total, 212 (90.2%) of the participants were anemic. Additionally, hepatomegaly was observed in only 73 (31.1%) participants and elevated creatinine levels, is a kidney function test, was detected in 23 (9.9%) participants.
3.2. Performance of the tests
A total of 339 participants, 235 VL-suspected and 104 NEHC participants were enrolled in the study and their blood samples were tested using 5 different VL diagnostics: rk39 RDT, DAT, LAMP assay, mini-dbPCR-NALFIA and qPCR.
Due to the potential risk of splenic bleeding and very painful bone marrow tissue collection procedure, microscopic examination was done for clinical purpose only. Therefore, microscopic examination was done only in 142 (60.4%) of the VL-suspected patients. The sensitivity, specificity and predictive values for positive and negative of the results of the 5 different VL diagnostic tests were computed against the reference standard (qPCR), Table 2. Using qPCR, 144 (61.28%) VL suspected patients were tested positive. For the purpose of comparison with the other five tests, these cases were classified as confirmed VL patients, given the fact that qPCR is the most sensitive test. Only one of the NEHC cases tested positive by qPCR.
The rk39 RDT: one hundred fifty-eight (67.23%) of the VL-suspected participants were tested positive with rk39 RDT. Furthermore, only one of the 104 NEHC, was found positive with rk39 RDT (this was the same case that tested also positive by qPCR). The overall rk39 RDT sensitivity and specificity were 88.11% (95%CI: 84.68 - 91.55%) and 83.33% (95%CI: 79.38 - 87.29%) respectively. Among the HIV-positive and negative VL-suspected patients, sensitivity and specificity of rk39 was also determined. Twenty-three (9.79%) of the VL-suspected patients co-infected patients. The sensitivity of rk39 RDT in HIV-positive patients was lower compared to HIV-negative patients (86.9% Vs 95.2%). Similarly, the proportion rk39 RDT positivity among HIV-positive patients was found significantly lower than HIV-negatives patients (McNemar's χ2 test, P=0.024).
The DAT: DAT was done on samples from 339 participants. Hundred thirty eight of 143 qPCR positive patients were positive for DAT (titer ≥1:3200), giving a sensitivity and specificity of 96.50% (95%CI: 94.55 - 98.46%) and 97.96% (95%CI: 96.45-99.46%) respectively. On the other hand, 9 patients had borderline DAT result (≥1:800 and <1:3200), among these patients, 3 were tested positive and 6 were negative by qPCR. However, when the borderline results were considered as negative, the specificity of DAT was increased to 99.47% (95%CI: 96.32 – 99.78%). Of the 182 DAT negative (titer: <1:800) patients, 2 were found positive by qPCR tests. Similarly, among the patients who tested positive by qPCR, 3 had borderline results and 2 had negative results by the DAT.
Microscopic Examination: Microscopic examination of Giemsa-stained tissue aspirates was conducted on 135 patients VL suspected patients, primarily for clinical purposes, and the data for this research purpose was collected from the patient’s medical chart. Of the total who had microscopic examination, 85(62.96%) of them were positive; and out of these 32(28.83%) and 42(39.64%) of them were with grade 2, and grade 3 and above, respectively.
Notably, 27 (24.1%) specimens deemed negative by microscopic examination were tested positive by qPCR. Importantly, none of the qPCR-negative samples were positive by microscopic examination.. Comparative analysis of the average Cycle Threshold (Ct) values revealed that lower Ct values were found in microscopy-negative/qPCR-positive samples than in microscopy-positive/qPCR-positive samples. The overall sensitivity and specificity of the microscopic examination were 76.58% (95% CI: 69.43-83.72%) and 100%, respectively. Microscopy positivity was significantly higher in HIV-positive patients compared to HIV-negative patients (McNemar χ2 test p=0.001).
Additionally, there was an association between parasite density (grades) and DAT titer. Specifically, 55 (71.43%) of patients with DAT titer ≥1:3200 exhibited grade 2 and above in microscopic examinations. All patients with negative microscopic results were also negative for DAT. However, 12 (24.49%) and 13 (26.53%) of microscopy-negative patients had DAT results at the borderline and DAT positive, respectively.
The LAMP assay: Using qPCR as reference tests, sensitivity and specificity of the employed LAMP assay were 94.33% (95%CI: 91.84 - 96.81%) and 97.38% (95%CI: 95.66 - 99.10%), respectively. All of the HIV-VL co-infected patients were positive by the LAMP assay, giving sensitivity 100%, however, the sensitivity was reduced to 89.2% (95%CI: 84.9 – 93.5%) in HIV-negative patients. On the other hand, the specificity of LAMP assay among HIV-positive and negative patients was remained almost the same (97.88% Vs 97.5%) respectively.
Mini-dbPCR NALFIA test: The mini-dbPCR-NALFIA's sensitivity and specificity to diagnose VL was 95.80 % (95%CI: 93.10 - 98.50%) and 98.92% (97.54 - 100.31%) respectively when using qPCR as a reference test. Only 1 sample that was positive by mini-dbPCR-NALFIA was negative by qPCR and 5 samples which were positive by qPCR were negative by mini-dbPCR-NALFIA. Like the LAMP assay, the sensitivity of the mini-dbPCR-NALFIA among the HIV-positive patients was higher (100%) than HIV-negative patients (91.7%, 95%CI: 73.25–98.12%). However, the specificity of mini-dbPCR-NALFIA between HIV-positive and negative patients was remained almost the same (99.5 vs. 100).
Receivers Operator Characteristics Curve (ROC curve) analysis was done for the various tests to assess their effectiveness in differentiating between VL and non-VL cases. Based on the area under ROC curve analysis, the mini-dbPCR-NALFIA, LAMP assay and DAT showed outstanding performance, AUC=0.991, 0.978 and 0.987 respectively. Moreover, the microscopic examination of Giemsa-stained tissue aspirates had an excellent performance, AUC= 0.88, whereas the rk39 RDT showed a lower value, AUC=0.69, Figure 1.
The agreement of each diagnostic test with the reference standard was evaluated using Cohon's kappa statistics. There was a strong agreement between qPCR and mini-dbPCR-NALFIA (k=0.98, 95%CI: 0.82-1.00), as well as between qPCR and the LAMP assay (k=0.96, 95%CI: 0.79-1.00). Similarly, the agreement between the DAT and qPCR also exhibited an excellent level of agreement (0.97, 95%CI: 0.84-1.01). However, the agreement between the rk39 RDT and qPCR was found to be lower (k=0.85, 95%CI: 0.78-0.98) than that of the mini-dbPCR-NALFIA, LAMP assay and DAT, but still excellent. In contrast, microscopic examination of Giemsa-stained tissue aspirates and the reference test qPCR showed only a substantial level of agreement (K=0.80, 95%CI: 0.39-0.69). Additionally, the agreement between respectively: LAMP assay and mini-dbPCR-NALFIA(0.96, 95%CI: 0.86-1.00), LAMP assay and Microscopy(0.79, 95%CI: 0.65-0.95), LAMP assay and DAT(0.95, 95%CI: 0.76-0.99), LAMP and rk39RDT(0.85, 95%CI: 0.74-0.94), mini-dbPCR-NALFIA and DAT(0.97, 95%CI: 0.85-1.01), mini-dbPCR and rk39 RDT(0.85, 95%CI: 0.75-0.97), mini-dbPCR-NALFIA and microscopy(0.81, 95%CI: 0.71-0.91) DAT and rk39 RDT(85, 95%CI: 0.69-0.98), and DAT and microscopy (0.82, 95%CI: 0.72-0.93) was assessed. All, except the agreement between LAMP assay and microscopy, and rk39 RDT and microscopy, showed an excellent level of agreement.
4. Discussion
Accurate and timely diagnosis of VL is essential to timely start appropriate treatment and to ensure proper case management [45]. However, in many VL endemic countries, due to restrains in resources, the implementation of accurate, affordable and robust diagnostic tests remains a major challenge[46]. Currently, several diagnostic tests are employed to diagnose VL, each with varying degrees of diagnostic accuracy[47]. The present study was designed to evaluate the performance of 5 different VL diagnostic tests that require (relative) little infrastructure against qPCR as references standard with the ultimate aim to implement an appropriate test in endemic remote areas.
The reference test, qPCR, identified 144 out of the suspected patients (61.28%) as cases of VL and only one patient tested positive in the healthy control group. Thus, 91(38.72%) cases among the clinically suspected cases were ruled out by the highly sensitive reference test, qPCR. This underscored that relying solely on the clinical case definition is insufficient for distinguishing VL cases from other diseases with similar symptoms. It also emphasized the need for the implementation of rapid, robust, and straightforward laboratory tests in close proximity to communities in need. For the remaining five diagnostic tests - rk39 RDT, DAT, microscopy, LAMP assay, and mini-dbPCR-NALFIA - patients who tested positive in qPCR were considered confirmed VL cases. The sensitivity of these tests varied, with the lowest sensitivity observed in the microscopic examination of Giemsa-stained tissue aspirate (75.89%) and rK39 RDT (88.11%), to the highest value for DAT (96.50%) and the two simple molecular tests, LAMP (94.33%) and mini-dbPCR-NALFIA (95.80%).
The overall sensitivity of rk39 RDT was 88.11% in the present study, which was consistent with our previous meta-analysis study done in Ethiopia [48]. In addition, similar results were reported from different studies conducted in Ethiopia[49]. Nevertheless, the sensitivity was a slightly lower from the global reports and higher from the east African studies[18]. Parasite heterogeneity particularly in kinesin gene[50], variation in study population[51], variation in reference standard used, and commercial brand difference were the main reasons for the performance variation[52,53,54,55]. The study also revealed that the sensitivity of rk39 RDT in HIV-positive VL patients was lower (86.9%) than in HIV-negative cases (95.2%), which is consistent with a number study done in different parts of the world [1,18,48]. The differences could be explained by the impact of both the virus and Leishmania parasite which compromises the immune response (antibody production), which the main analyte of the rk39 RDT [1,48].
The DAT test was performed with positive cut-of titer ≥1:3200, negative ≤1:800 and borderline with ≥1:800 and <1:3200. The overall sensitivity of DAT was 96.5%, which is significantly higher than observed in some studies conducted in Ethiopia[1], and slightly higher than found in previous studies conducted in Africa [18,51,56,57]. However, these studies used microscopy as a reference standard, which is less sensitivity than DAT. Like the rk39 RDT, the sensitivity of DAT was lower in HIV-positive cases compared with HIV-negative cases, which is in agreement with previous reports in Ethiopia [1,48,58]. Nevertheless, there was less variability observed in the specificity of DAT across the various reports.
Microscopic examination of Giemsa-stained tissue aspirates is commonly considered as the gold standard test, despite its inherent risk and discomfort. Notably, previous research has consistently indicated that this method exhibits a notably low and variable sensitivity. Our findings were in agreement with the previous reports[49,59], revealing that the sensitivity of microscopic examination of Giemsa-stained tissue aspirates is lower than any of the five tests.
Moreover, opposing to the serological tests, microscopy exhibits higher sensitivity in individuals who were HIV-positive in comparison to those who were HIV-negative. This phenomenon could be attributed to compromised immune systems in HIV-positive patients, resulting in elevated parasite loads in the tissue aspirate and subsequently a higher likelihood of a positive microscopic examination[60]. Furthermore, we observed a significant association between parasite density and DAT titer, which in agreement with a study done in Sudan[61] As the density of parasites in the microscopic examination increases, there was a corresponding increase in antibody titer and probability of testing positive for DAT[61]. This indicates the interplay between the density of parasites and the test outcomes, reinforcing the importance of parasite load in diagnostic accuracy.
The LAMP assay and mini-dbPCR-NALFIA are recently developed PoC tests for the diagnosis of VL and they are primarily designed to be implemented as molecular diagnostic tests in remote and/or resource limited endemic areas. The sensitivity and specificity of LAMP assay was 94.33% and 97.88% respectively. Based on the test performance classification by Kristin R. Ferrell, a test with a sensitivity and specificity exceeding 90% is deemed to be excellent[62] and based on Ferrell’s classification, LAMP assay falls in the excellent level. In addition, the boil-and-spin DNA extraction method is another advantage of LAMP because it is very easy to perform with single chemical and its performance is comparable with the Qiagen DNA extraction method[44]. In the present study, LAMP assay showed slightly lower sensitivity(94.33% Vs 95.9%) when evaluating using qPCR as a reference test than using rk39 RDT and/or microscopy of Giemsa-stained tissue aspirates(Chapter 4). This is explained by the impact of imperfect reference standard, as LAMP assay has higher sensitivity than rk39 RDT and/or microscopy[63].
The mini-dbPCR-NALFIA is another simple, robust and rapid test which combines the molecular and immunological techniques. In the current study, the mini-dbPCR-NALFIA exhibited comparable performance to the LAMP assay and DAT, but it demonstrated significantly superior performance when compared to microscopy and rk39 RDT. Besides its robust performance, the mini-dbPCR-NALFIA has been adequately simplified to a feasible extent, making it suitable for implementation in remote endemic areas[62]. It also meets the WHO-recommended ASSURED criteria for Point-of-Care (PoC) tests. Due to its novelty, there have been, apart from our team's earlier laboratory development and evaluation, so far no other studies have done to further confirm the diagnostic performance of mini-dbPCR-NALFIA. In medical tests evaluation, the AUCROC explains how appropriate the test under investigation precisely categorizes the patient into disease and non-disease. The highest the AUCROC (closest to 1.00) value, the best is the performance of the test[64]. In the present study, the AUCROC value ranges from the lowest in rk39 RDT (AUCROC=0.67) to the highest mini-dbPCR-NALFIA (AUCROC=0.98). Both the DAT and LAMP assay demonstrated a very high AUCROC, with a value of 0.97 for each. Therefore, the AUCROC analysis consistently aligned with the sensitivity and specificity outcomes of mini-dbPCR-NALFIA, LAMP assay, and DAT. However, there were conflicting results between AUCROC and the sensitivity/specificity measures for rk39 RDT and microscopy. Based on the AUCROC values, tests which have AUCROC>0.9 and between >0.70 and <0 .9 are considered as excellent and acceptable test respectively. Therefore, LAMP assay, mini-dbPCR-NALFIA and DAT were excellent tests whereas rk39 RDT, whereas microscopy were considered as acceptable tests[65].
Moreover, the agreement of each test with the reference test and within each other was computed using the Cohen’s kappa statistics. Based on our analysis, the agreement between the mini-dbPCR-NALFIA (k=0.98), LAMP assay (k=0.96) and DAT (K=0.97) and qPCR was agreement. The agreement between rk39 RDT and qPCR (k=0.85) was also excellent. However, the agreement between microscopy and the qPCR was substantial (k=0.8). The possible explanation why microscopic examination showed a substantial level of agreement could potentially be the lower sensitivity, as evidenced by 27 of the qPCR-positive patients who were classified as negative in the microscopic examination of Giemsa-stained tissue aspirate.
5. Conclusions
To conclude, based on the findings, the rk39 RDT and microscopic examination of Giemsa-stained tissue aspirates exhibited lower sensitivity when compared to the DAT, LAMP assay, and mini-dbPCR-NALFIA. Compared to microscopy, the rk39 RDT demonstrated superior sensitivity but lower specificity. However, on top of the low sensitivity, it is crucial to acknowledge the drawbacks, including a high risk of internal bleeding (splenic aspiration) and significant pain (bone marrow aspiration), which makes microscopy an inconvenient method. The DAT demonstrated a remarkably high performance, which is comparable to LAMP assay and mini-dbPCR-NALFIA. Nevertheless, 18-24 hours incubation hampers its implementation as point of care test.
The LAMP assay and mini-dbPCR-NALFIA demonstrated an excellent performance, are rapid, simple, and feasible for deployment in endemic areas. Therefore, we recommend the continued use of rk39 and DAT in areas where needed, the substitution of microscopy with the rapid, robust, and feasible molecular test, the LAMP assay, and suggest further on-site investigations into the mini-dbPCR-NALFIA.
Author Contributions
Conceptualization: DGH, YK, MA, HS and DW, Investigation: DGH, YK, MA, HS and DW, Data curation: DGH, YK, MA, HS and DW, Writing—original draft preparation: DGH, YK, MA, HS and DW, Writing—review and Editing: DGH, HS and DW, Supervision: HS and DW. All authors have read and agreed to the published version of the manuscript.
Funding
The research was financially support by European and Developing Countries Clinical Trial Partnership (EDCTP, The Hague, The Netherlands) through a senior fellowship awarded to DW (grant: TMA2016SF-1437; Evaluation of the LAMP & db-PCR-NALFIA for the Diagnosis and/or as Test-of-Cure in Patients with Visceral Leishmaniasis in Ethiopia), and internal funding of the University of Amsterdam, Academic Medical Centre and Mekelle University, College of Health Sciences.
Institutional Review Board Statement
The study was approved by Health Research Ethics Review Committee (ERC number: 1102/2017), College of Health Sciences and Ayder Comprehensive Specialized Referral Hospital Mekelle University.
Informed Consent Statement
Informed consent and/or assent were obtained from the study participants or their guardian. In addition, a permission letter was obtained from the local authorities to each study sites.
Data Availability Statement
The data presented in this study can be obtained by contacting the corresponding author/s upon a reasonable request.
Acknowledgments
We express our gratitude to EDCTP, University of Amsterdam, and Mekelle University for their financial support and facilitating this research. Additionally, we extend our thanks to all study participants, as well as the management and staff of Ayder Specialized Referral Hospital, Mekelle University, College of Health Sciences, for their cooperation, support, and permission to conduct this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Kassa, M.; Abdellati, S.; Cnops, L.; Bremer Hinckel, B.C.; Yeshanew, A.; Hailemichael, W.; Vogt, F.; Adriaensen, W.; Mertens, P.; Diro, E. Diagnostic accuracy of direct agglutination test, rK39 ELISA and six rapid diagnostic tests among visceral leishmaniasis patients with and without HIV coinfection in Ethiopia. PLoS Negl. Trop. Dis. 2020, 14, e0008963. [Google Scholar] [CrossRef] [PubMed]
- Oryan, A.; Akbari, M. Worldwide risk factors in leishmaniasis. Asian Pac. J. Trop. Med. 2016, 9, 925–932. [Google Scholar] [CrossRef] [PubMed]
- Challa¹, P. (2018). Amphotericin B and Fluconazole Susceptibility Profiles of Old World and New World Strains of Leishmania.
- Bi, K.; Chen, Y.; Kuang, S.Z.Y.; Wu, C.-H.J. Current visceral leishmaniasis research: a research review to inspire future study. BioMed research international. 2018. [Google Scholar] [CrossRef] [PubMed]
- De Ruiter, C.; Van Der Veer, C.; Leeflang, M.; Deborggraeve, S.; Lucas, C.; Adams, E. Molecular tools for diagnosis of visceral leishmaniasis: systematic review and meta-analysis of diagnostic test accuracy. J. Clin. Microbiol. 2014, 52, 3147–3155. [Google Scholar] [CrossRef] [PubMed]
- Diro, E.; Lynen, L.; Ritmeijer, K.; Boelaert, M.; Hailu, A.; van Griensven, J. Visceral leishmaniasis and HIV coinfection in East Africa. PLoS Negl. Trop. Dis. 2014, 8, e2869. [Google Scholar] [CrossRef] [PubMed]
- Ghodrati, M.; Spotin, A.; Hazratian, T.; Mahami-Oskouei, M.; Bordbar, A.; Ebrahimi, S.; Fallahi, S.; Parvizi, P. Diagnostic Accuracy of Loop-mediated Isothermal Amplification Assay as a Field Molecular Tool for Rapid Mass Screening of Old World Leishmania Infections in Sand Flies and In Vitro Culture. Iran J Parasitol. 2017, 12, 506–515. [Google Scholar] [PubMed]
- Lopes, E.; Sevá, A.d.P.; Ferreira, F.; Nunes, C.M.; Keid, L.B.; Hiramoto, R.; Ferreira, H.L.; Oliveira, T.M.F.d.S.; Bigotto, M.; Galvis-Ovallos, F. Serological and molecular diagnostic tests for canine visceral leishmaniasis in Brazilian endemic area: one out of five seronegative dogs are infected. Epidemiol. Infect. 2017, 145, 2436–2444. [Google Scholar] [CrossRef] [PubMed]
- Zijlstra, E.; Ali, M.S.; El-Hassan, A.; El-Toum, I.A.; Satti, M.; Ghalib, H.; Sondorp, E.; Winkler, A. Kala-azar in displaced people from southern Sudan: epidemiological, clinical and therapeutic findings. Trans. R. Soc. Trop. Med. Hyg. 1991, 85, 365–369. [Google Scholar] [CrossRef] [PubMed]
- Cloots, K.; Marino, P.; Burza, S.; Gill, N.; Boelaert, M.; Hasker, E. Visceral Leishmaniasis-HIV coinfection as a predictor of increased Leishmania transmission at the village level in Bihar, India. Frontiers in Cellular and Infection Microbiology. 2021, 11, 604117. [Google Scholar] [CrossRef]
- Rijal, S.; Ostyn, B.; Uranw, S.; Rai, K.; Bhattarai, N.R.; Dorlo, T.P.; Beijnen, J.H.; Vanaerschot, M.; Decuypere, S.; Dhakal, S.S. Increasing failure of miltefosine in the treatment of Kala-azar in Nepal and the potential role of parasite drug resistance, reinfection, or noncompliance. Clin. Infect. Dis. 2013, 56, 1530–1538. [Google Scholar] [CrossRef]
- Ortalli, M.; Lorrai, D.; Gaibani, P.; Rossini, G.; Vocale, C.; Re, M.C.; Varani, S. Serodiagnosis of Visceral leishmaniasis in Northeastern Italy: Evaluation of seven serological tests. Microorganisms. 2020, 8, 1847. [Google Scholar] [CrossRef]
- Hagos, D.G.; Kiros, Y.K.; Abdulkader, M.; Arefaine, Z.G.; Nigus, E.; Schallig, H.H.; Wolday, D. Utility of the Loop-Mediated Isothermal Amplification Assay for the Diagnosis of Visceral Leishmaniasis from Blood Samples in Ethiopia. The American Journal of Tropical Medicine and Hygiene. 2021, 105, 1050. [Google Scholar] [CrossRef] [PubMed]
- Hagos, D.G.; Kebede, Y.; Abdulkader, M.; Nigus, E.; Gessesse Arefaine, Z.; Nega, G.; Schallig, H.D.; Wolday, D. Effect of rK39 testing in guiding treatment initiation and outcome in patients with visceral leishmaniasis in Ethiopia: A prospective cohort study. PLoS One. 2021, 16, e0253303. [Google Scholar] [CrossRef] [PubMed]
- da Silva, M.R.B.; Stewart, J.M.; Costa, C.H.N. Sensitivity of bone marrow aspirates in the diagnosis of visceral leishmaniasis. The American journal of tropical medicine and hygiene. 2005, 72, 811–814. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, P.; Dayama, A.; Mehrotra, S.; Sundar, S. Diagnosis of visceral leishmaniasis. Trans. R. Soc. Trop. Med. Hyg. 2011, 105, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Osman, O.F.; Oskam, L.; Zijlstra, E.E.; Kroon, N.; Schoone, G.J.; Khalil, E.; El-Hassan, A.M.; Kager, P.A. Evaluation of PCR for diagnosis of visceral leishmaniasis. J. Clin. Microbiol. 1997, 35, 2454–2457. [Google Scholar] [CrossRef] [PubMed]
- ter Horst, R.; Tefera, T.; Assefa, G.; Ebrahim, A.Z.; Davidson, R.N.; Ritmeijer, K. Field evaluation of rK39 test and direct agglutination test for diagnosis of visceral leishmaniasis in a population with high prevalence of human immunodeficiency virus in Ethiopia. The American journal of tropical medicine and hygiene. 2009, 80, 929–934. [Google Scholar] [CrossRef] [PubMed]
- El-Moamly, A.; El-Sweify, M.; Hafeez, M. Performance of rK39 immunochromatography and freeze-dried direct agglutination tests in the diagnosis of imported visceral leishmaniasis. Parasitol. Res. 2012, 110, 349–354. [Google Scholar] [CrossRef]
- de Paiva Cavalcanti, M.; de Brito, M.E.F.; de Souza, W.V.; de Miranda Gomes, Y.; Abath, F.G. The development of a real-time PCR assay for the quantification of Leishmania infantum DNA in canine blood. The Veterinary Journal. 2009, 182, 356–358. [Google Scholar] [CrossRef]
- Opota, O.; Balmpouzis, Z.; Berutto, C.; Kaiser-Guignard, J.; Greub, G.; Aubert, J.D.; Prod'hom, G.; Manuel, O.; Jaton, K. Visceral leishmaniasis in a lung transplant recipient: usefulness of highly sensitive real-time polymerase chain reaction for preemptive diagnosis. Transpl. Infect. Dis. 2016, 18, 801–804. [Google Scholar] [CrossRef]
- Gedda, M.R.; Madhukar, P.; Shukla, A.; Mudavath, S.L.; Srivastava, O.N.; Singh, O.P.; Sundar, S. Nanodiagnostics in leishmaniasis: A new frontiers for early elimination. Wiley Interdisciplinary Reviews: Nanomedicine and Nanobiotechnology, 2021; 13, e1675. [Google Scholar]
- Mugasa, C.M.; Laurent, T.; Schoone, G.J.; Basiye, F.L.; Saad, A.A.; El Safi, S.; Kager, P.A.; Schallig, H.D. Simplified molecular detection of Leishmania parasites in various clinical samples from patients with leishmaniasis. Parasit Vectors. 2010, 3, 13. [Google Scholar] [CrossRef] [PubMed]
- Mens, P.; De Bes, H.; Sondo, P.; Laochan, N.; Keereecharoen, L.; Van Amerongen, A.; Flint, J.; Sak, J.; Proux, S.; Tinto, H. Direct blood PCR in combination with nucleic acid lateral flow immunoassay for detection of Plasmodium species in settings where malaria is endemic. J. Clin. Microbiol. 2012, 50, 3520–3525. [Google Scholar] [CrossRef] [PubMed]
- Mikita, K.; Maeda, T.; Yoshikawa, S.; Ono, T.; Miyahira, Y.; Kawana, A. The Direct Boil-LAMP method: a simple and rapid diagnostic method for cutaneous leishmaniasis. Parasitol. Int. 2014, 63, 785–789. [Google Scholar] [CrossRef] [PubMed]
- Gao, C.H.; Ding, D.; Wang, J.Y.; Steverding, D.; Wang, X.; Yang, Y.T.; Shi, F. Development of a LAMP assay for detection of Leishmania infantum infection in dogs using conjunctival swab samples. Parasit Vectors. 2015, 8, 370. [Google Scholar] [CrossRef]
- Notomi T; Mori Y; Tomita N; Kanda H. Loop-mediated isothermal amplification (LAMP): principle, features, and future prospects. J. Microbiol. 2015, 53, 1–5. [CrossRef] [PubMed]
- Sriworarat, C.; Phumee, A.; Mungthin, M.; Leelayoova, S.; Siriyasatien, P. Development of loop-mediated isothermal amplification (LAMP) for simple detection of Leishmania infection. Parasit Vectors. 2015, 8, 591. [Google Scholar] [CrossRef]
- Nzelu, C.O.; Caceres, A.G.; Guerrero-Quincho, S.; Tineo-Villafuerte, E.; Rodriquez-Delfin, L.; Mimori, T.; Uezato, H.; Katakura, K.; Gomez, E.A.; Guevara, A.G.; et al. A rapid molecular diagnosis of cutaneous leishmaniasis by colorimetric malachite green-loop-mediated isothermal amplification (LAMP) combined with an FTA card as a direct sampling tool. Acta Trop. 2016, 153, 116–119. [Google Scholar] [CrossRef] [PubMed]
- van Dijk, N.J.; Menting, S.; Wentink-Bonnema, E.M.; Broekhuizen-van Haaften, P.E.; Withycombe, E.; Schallig, H.D.; Mens, P.F. Laboratory evaluation of the miniature direct-on-blood PCR nucleic acid lateral flow immunoassay (mini-dbPCR-NALFIA), a simplified molecular diagnostic test for Plasmodium. Malar. J. 2023, 22, 98. [Google Scholar] [CrossRef] [PubMed]
- Erber, A.C.; Sandler, P.J.; de Avelar, D.M.; Swoboda, I.; Cota, G.; Walochnik, J. Diagnosis of visceral and cutaneous leishmaniasis using loop-mediated isothermal amplification (LAMP) protocols: a systematic review and meta-analysis. Parasites & vectors, 2022; 15, 1–16. [Google Scholar]
- Ruang-Areerate, T.; Sukphattanaudomchoke, C.; Thita, T.; Leelayoova, S.; Piyaraj, P.; Mungthin, M.; Suwannin, P.; Polpanich, D.; Tangchaikeeree, T.; Jangpatarapongsa, K. Development of loop-mediated isothermal amplification (LAMP) assay using SYBR safe and gold-nanoparticle probe for detection of Leishmania in HIV patients. Sci. Rep. 2021, 11, 1–11. [Google Scholar] [CrossRef]
- Sukphattanaudomchoke, C.; Siripattanapipong, S.; Thita, T.; Leelayoova, S.; Piyaraj, P.; Mungthin, M.; Ruang-Areerate, T. Simplified closed tube loop mediated isothermal amplification (LAMP) assay for visual diagnosis of Leishmania infection. Acta Trop. 2020, 212, 105651. [Google Scholar] [CrossRef]
- Nzelu, C.O.; Kato, H.; Peters, N.C. Loop-mediated isothermal amplification (LAMP): An advanced molecular point-of-care technique for the detection of Leishmania infection. PLoS Negl. Trop. Dis. 2019, 13, e0007698. [Google Scholar] [CrossRef]
- Pecchia, S.; Da Lio, D. Development of a rapid PCR-Nucleic Acid Lateral Flow Immunoassay (PCR-NALFIA) based on rDNA IGS sequence analysis for the detection of Macrophomina phaseolina in soil. J. Microbiol. Methods. 2018, 151, 118–128. [Google Scholar] [CrossRef]
- Harizanov, R.N.; Kaftandjiev Iskren, T. Interactions between parasite and host in human visceral leishmaniasis. J Cytol Tissue Biol. 2014, 1. [Google Scholar]
- Vaish, M.; Singh, O.P.; Chakravarty, J.; Sundar, S. rK39 antigen for the diagnosis of visceral leishmaniasis by using human saliva. The American journal of tropical medicine and hygiene. 2012, 86, 598. [Google Scholar] [CrossRef] [PubMed]
- Kaushal, H.; Bhattacharya, S.K.; Verma, S.; Salotra, P. Serological and molecular analysis of Leishmania infection in healthy individuals from two districts of West Bengal, India, endemic for visceral leishmaniasis. The American Journal of Tropical Medicine and Hygiene. 2017, 96, 1448. [Google Scholar] [CrossRef]
- Adams, E.R.; Jacquet, D.; Schoone, G.; Gidwani, K.; Boelaert, M.; Cunningham, J. Leishmaniasis direct agglutination test: using pictorials as training materials to reduce inter-reader variability and improve accuracy. PLoS Negl. Trop. Dis. 2012, 6, e1946. [Google Scholar] [CrossRef]
- Ayelign, B.; Jemal, M.; Negash, M.; Genetu, M.; Wondmagegn, T.; Zeleke, A.J.; Worku, L.; Bayih, A.G.; Shumie, G.; Behaksra, S.W. Validation of in-house liquid direct agglutination test antigen: the potential diagnostic test in visceral Leishimaniasis endemic areas of Northwest Ethiopia. BMC Microbiol. 2020, 20, 1–7. [Google Scholar] [CrossRef]
- Roberts, T.; Keddie, S.H.; Rattanavong, S.; Gomez, S.R.; Bradley, J.; Keogh, R.H.; Bärenbold, O.; Falconer, J.; Mens, P.F.; Hopkins, H. Accuracy of the direct agglutination test for diagnosis of visceral leishmaniasis: a systematic review and meta-analysis. BMC Infect. Dis. 2023, 23, 782. [Google Scholar] [CrossRef] [PubMed]
- Federal Ministry of Health of Ethiopia (FMOH). Guideline for Diagnosis, Treatment and Prevention of Leishmaniasis in Ethiopia. 2013, 2nd edition, Addis Ababa, Ethiopia.
- Mukhtar, M.; Ali, S.S.; Boshara, S.A.; Albertini, A.; Monnerat, S.; Bessell, P.; Mori, Y.; Kubota, Y.; Ndung’u, J.M.; Cruz, I. Sensitive and less invasive confirmatory diagnosis of visceral leishmaniasis in Sudan using loop-mediated isothermal amplification (LAMP). PLoS Negl. Trop. Dis. 2018, 12, e0006264. [Google Scholar] [CrossRef]
- Hossain, F.; Picado, A.; Owen, S.I.; Ghosh, P.; Chowdhury, R.; Maruf, S.; Khan, M.A.A.; Rashid, M.U.; Nath, R.; Baker, J. Evaluation of Loopamp™ Leishmania Detection Kit and Leishmania Antigen ELISA for Post-Elimination Detection and Management of Visceral Leishmaniasis in Bangladesh. Frontiers in Cellular and Infection Microbiology. 2021, 11, 670759. [Google Scholar] [CrossRef]
- Georgiadou, S.P.; Stefos, A.; Spanakos, G.; Skrimpas, S.; Makaritsis, K.; Sipsas, N.V.; Dalekos, G.N. Current clinical, laboratory, and treatment outcome characteristics of visceral leishmaniasis: results from a seven-year retrospective study in Greece. Int. J. Infect. Dis. 2015, 34, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Sundar, S.; Rai, M. Laboratory diagnosis of visceral leishmaniasis. Clin. Vaccine Immunol. 2002, 9, 951–958. [Google Scholar] [CrossRef] [PubMed]
- Boelaert, M.; Rijal, S.; Regmi, S.; Singh, R.; Karki, B.; Jacquet, D.; Chappuis, F.; Campino, L.; Desjeux, P.; Le Ray, D. A comparative study of the effectiveness of diagnostic tests for visceral leishmaniasis. Am. J. Trop. Med. Hyg. 2004, 70, 72. [Google Scholar] [CrossRef] [PubMed]
- Hagos, D.G.; Schallig, H.D.; Kiros, Y.K.; Abdulkadir, M.; Wolday, D. Performance of rapid rk39 tests for the diagnosis of visceral leishmaniasis in Ethiopia: a systematic review and meta-analysis. BMC Infect. Dis. 2021, 21, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Kiros, Y.K.; Regassa, B.F. The role of rk39 serologic test in the diagnosis of visceral leishmaniasis in a Tertiary Hospital, Northern Ethiopia. BMC Res. Notes. 2017, 10, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharyya, T.; Boelaert, M.; Miles, M.A. Comparison of visceral leishmaniasis diagnostic antigens in African and Asian Leishmania donovani reveals extensive diversity and region-specific polymorphisms. PLoS Negl. Trop. Dis. 2013, 7, e2057. [Google Scholar] [CrossRef] [PubMed]
- Bezuneh, A.; Mukhtar, M.; Abdoun, A.; Teferi, T.; Takele, Y.; Diro, E.; Jemaneh, A.; Shiferaw, W.; Wondimu, H.; Bhatia, A. Comparison of point-of-care tests for the rapid diagnosis of visceral leishmaniasis in East African patients. The American journal of tropical medicine and hygiene. 2014, 91, 1109. [Google Scholar] [CrossRef] [PubMed]
- Boelaert, M.; El-Safi, S.; Hailu, A.; Mukhtar, M.; Rijal, S.; Sundar, S.; Wasunna, M.; Aseffa, A.; Mbui, J.; Menten, J. Diagnostic tests for kala-azar: a multi-centre study of the freeze-dried DAT, rK39 strip test and KAtex in East Africa and the Indian subcontinent. Trans. R. Soc. Trop. Med. Hyg. 2008, 102, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Coulborn, R.M.; Gebrehiwot, T.G.; Schneider, M.; Gerstl, S.; Adera, C.; Herrero, M.; Porten, K.; den Boer, M.; Ritmeijer, K.; Alvar, J. Barriers to access to visceral leishmaniasis diagnosis and care among seasonal mobile workers in Western Tigray, Northern Ethiopia: A qualitative study. PLoS Negl. Trop. Dis. 2018, 12, e0006778. [Google Scholar] [CrossRef]
- Ready, P. Leishmaniasis emergence in Europe. Eurosurveillance. 2010, 15, 19505. [Google Scholar] [CrossRef]
- Chappuis, F.; Sundar, S.; Hailu, A.; Ghalib, H.; Rijal, S.; Peeling, R.W.; Alvar, J.; Boelaert, M. Visceral leishmaniasis: what are the needs for diagnosis, treatment and control? Nature reviews microbiology. 2007, 5, 873–882. [Google Scholar] [CrossRef] [PubMed]
- Cota, G.F.; De Sousa, M.R.; Demarqui, F.N.; Rabello, A. The diagnostic accuracy of serologic and molecular methods for detecting visceral leishmaniasis in HIV infected patients: meta-analysis. PLoS Negl. Trop. Dis. 2012, 6, e1665. [Google Scholar] [CrossRef] [PubMed]
- Mukhtar, M.; Ali, S.S.; Boshara, S.A.; Albertini, A.; Monnerat, S.; Bessell, P.; Mori, Y.; Kubota, Y.; Ndung'u, J.M.; Cruz, I. Sensitive and less invasive confirmatory diagnosis of visceral leishmaniasis in Sudan using loop-mediated isothermal amplification (LAMP). PLoS Negl. Trop. Dis. 2018, 12, e0006264. [Google Scholar] [CrossRef] [PubMed]
- Cota, G.F.; de Sousa, M.R.; de Freitas Nogueira, B.M.; Gomes, L.I.; Oliveira, E.; Assis, T.S.M.; de Mendonça, A.L.P.; Pinto, B.F.; Saliba, J.W.; Rabello, A. Comparison of parasitological, serological, and molecular tests for visceral leishmaniasis in HIV-infected patients: a cross-sectional delayed-type study. The American journal of tropical medicine and hygiene. 2013, 89, 570. [Google Scholar] [CrossRef] [PubMed]
- Melkamu, R.; Berhane, N.; Jacobs, B.K.; Mohammed, R.; Kassa, M.; Yeshanew, A.; Fikre, H.; Atnafu, S.; van Henten, S.; van Griensven, J. PCR for detection of Leishmania donovani from microscopically negative tissue smears of suspected patients in Gondar, Ethiopia. PLoS Negl. Trop. Dis. 2023, 17, e0011128. [Google Scholar] [CrossRef] [PubMed]
- Takele, Y.; Mulaw, T.; Adem, E.; Womersley, R.; Kaforou, M.; Franssen, S.U.; Taylor, G.P.; Müller, I.; Cotton, J.A.; Kropf, P. Recurrent visceral leishmaniasis relapses in HIV co-infected patients are characterised by less efficient immune responses and higher parasite load. iScience. 2022, 105867. [Google Scholar]
- Babiker, Z.O.; Davidson, R.; Mazinda, C.; Kipngetich, S.; Ritmeijer, K. Utility of lymph node aspiration in the diagnosis of visceral leishmaniasis in Sudan. The American journal of tropical medicine and hygiene. 2007, 76, 689–693. [Google Scholar] [CrossRef] [PubMed]
- Ferrell, K.R. How to Interpret Sensitivity and Specificity. Western Psychological Services. 2022, 2022. [Google Scholar]
- Waikar, S.S.; Betensky, R.A.; Emerson, S.C.; Bonventre, J.V. Imperfect gold standards for biomarker evaluation. Clinical Trials. 2013, 10, 696–700. [Google Scholar] [CrossRef]
- Narkhede, S. Understanding auc-roc curve. Towards Data Science. 2018, 26, 220–227. [Google Scholar]
- Mandrekar, J.N. Receiver operating characteristic curve in diagnostic test assessment. J. Thorac. Oncol. 2010, 5, 1315–1316. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Comparison of 5 different tests for VL diagnosis using Area under Receiver Operating Characteristic (ROC) curve (AUC). Q-PCR was used as a reference test .
Figure 1.
Comparison of 5 different tests for VL diagnosis using Area under Receiver Operating Characteristic (ROC) curve (AUC). Q-PCR was used as a reference test .
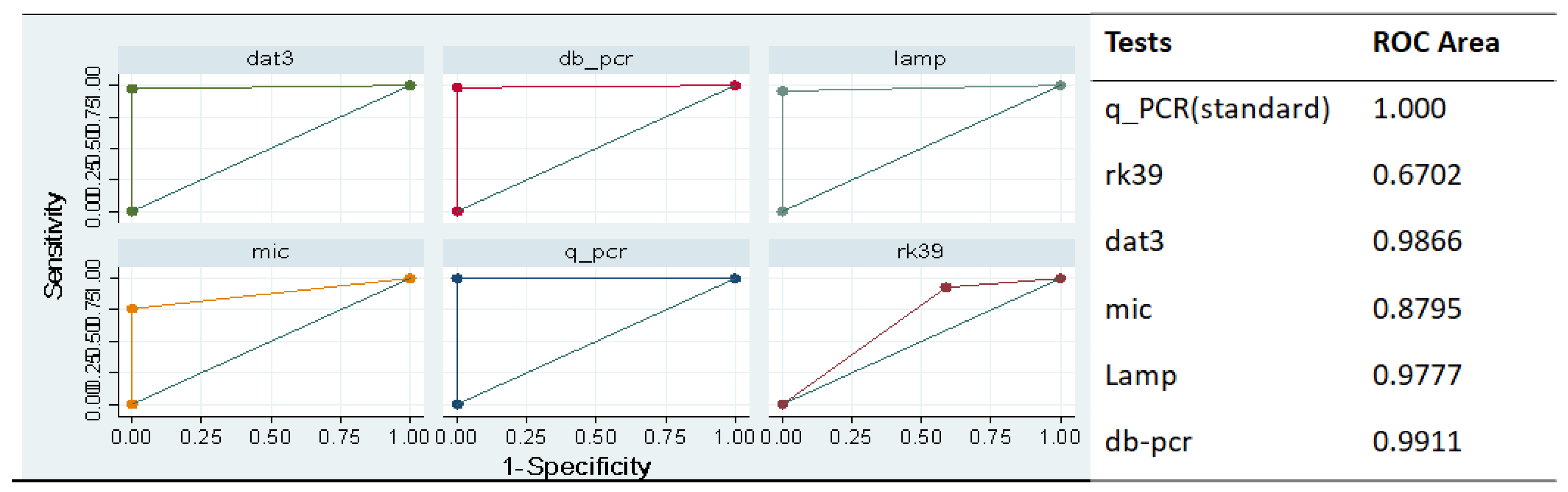

Table 1.
Clinical and socio-demographic characteristic of the VL-suspected study participants.
| Characteristic | All VL cases (N=235) |
Q-PCR+ (n=144/235) |
rk39 RDT+ (n=158/235) |
DAT+ (n=141/235) |
Microscopic+ (n=85/135) |
LAMP+ (n=135/226) |
dbPCR-NALFIA+ (n=138/235) |
| Sex | |||||||
| Male | 220(93.6%) | 142(60.4%) | 155(66.0%) | 139(59.1%) | 84(62.2%) | 131(95.0%) | 13(58.3%) |
| Female | 15(6.450 | 2(0.85%) | 3(1.80%) | 2(0.85%) | 1(0.74%) | 4(1.77%) | 19).43%) |
| Signs & symptoms | |||||||
| Fever(>2wks) | 226 (96.2%), | 139(96.5)% | 148(93.7%) | 133(95.7%) | 83(98.8%) | 128(94.8%) | 132(95.7%) |
| Wt. Lost | 218 (92.8%) | 137(95.1%) | 139(87.9%) | 134(95.0%) | 79(92.9%) | 126(93.3%) | 130(94.2%) |
| Fatigue | 199 (84.6%). | 123985.4%) | 132(83.5) | 126(89.4%) | 82(96.5%) | 128(94.8%) | 131(94.9%) |
| Abdominal swelling | 112(77.8%) | 101(65.2%) | 108(76.6%) | 72(84.7%) | 103(76.3%) | 109(78.9%) | |
| Splenomegaly | 179 (76.2%), | 134(93.1%) | 118(74.7%) | 125(88.7%) | 77(90.6%) | 129(95.6%) | 111(80.4%) |
| Hepatomegaly | 73 (31.1%) | 64(44.4%) | 41(25.9%) | 48(34.0%) | 33(38.8%) | 42(31.1%) | 51(37.0%) |
| Laboratory findings | |||||||
| WBC(x109/L | 1.9(1.5-2.3) | 1.7(1.1-2.6) | 1.8(1.3-2.1) | 2.0(1.6-2.3) | 1.7(1.1-1.9) | 1.6(1.2-2.2) | 1.65(1.2-2.1) |
| Hemoglobin (mg/dL) | 7.6(6.3-11.3) | 7.8(6.3-12.0) | 7.9(6.6-10.1) | 8.1(6.8-12.0) | 7.2(6.1-9.4) | 7.8(6.5-10.2) | 7.4(5.9-9.9) |
| Platelet count (3109/L) | 172(71-352) | 167(165-345) | 177(154-243) | 171(129-271) | 169(116-237) | 174(124-299) | 169(153-253) |
| AST(U/L) | 175(66.8%) | 68(43-168) | 71(39-173) | 66(45-171) | 70(44-143) | 65(39-169) | 66(40-155) |
| ALT(U/L) | 41(23-65) | 42(21-63) | 41(27-67) | 39(28-65) | 38(26-59) | 42(27-61) | 39(24-67) |
| Alkaline phosphate (U/L) | 166(81-342) | 163(78-298) | 171(77-355) | 162(69-343) | 159(89-236) | 164(81-309) | 163(79-321) |
| Creatinine (mg/dL) | 0.7(0.48-0.9) | 0.69(0.46-0.87) | 0.7(0.5-0.97) | 0.69(0.5-0.87) | 0.68(0.5-0.87) | 0.73(0.5-1.01) | 0.68(0.47-0.96) |
Q-PCR-Quantitative polymerase chain reaction, rk39 RDT-rk39 rapid diagnostic tests, DAT-Direct agglutination test, LAMP-Loop mediated Isothermal amplification, dbPCR-NALFIA-direct blood-polymerase chain reaction-nucleic acid lateral flow immunoassay, Wt.lost- weight loss of the cases, AST-aspartate aminotransferase), ALT-Alanine transaminase, and WBC- White blood cells.
Table 2.
The sensitivity, specificity, and negative and positive predictive values of rk39 RDT, DAT, Microscopy, LAMP assay, and min-dbPCR-NALFIA to diagnose VL in north Ethiopia compared to qPCR as reference standard.
Table 2.
The sensitivity, specificity, and negative and positive predictive values of rk39 RDT, DAT, Microscopy, LAMP assay, and min-dbPCR-NALFIA to diagnose VL in north Ethiopia compared to qPCR as reference standard.
| Tests | Sensitivity (95%CI) | Specificity (95%CI) | PPV (95%CI) | NPV (95%CI) |
| Rk39 RDT | 88.11% (84.68 - 91.55%) |
83.33% 79.38-87.29% |
79.25% (74.94-83.55%) | 90.66% 87.57-93.75% |
| DAT | 96.50% (94.55-98.46%) |
97.96% (96.45-99.46%) |
97.18% (95.42-98.94%) | 97.46% (95.79-99.14%) |
| Microscopy |
75.89% (68.68 - 83.11%) |
100.00% (100.0-100.0%) |
100.00% (100.0-100.0%) | 46.00% (37.59 - 54.41% |
| LAMP assay | 94.33% (91.84 - 96.81%) |
97.88% (96.34-99.43%) |
96.38% (94.37 - 98.39% | 95.88% (93.74 - 98.02%) |
| Mini-dbPCR-NALFIA | 95.80% (93.68 - 97.93%) |
98.99% (97.93 - 100.05%) |
98.56% (97.30 - 99.83%) |
97.03% (95.23 - 98.83%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



