
Submitted:
25 November 2023
Posted:
30 November 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
For over two years, the global COVID-19 pandemic has persisted, and its continuation is anticipated. The emergence and rapid spread of numerous new virus variations across continents have been observed. These variants, differing from previously known strains, manifest a spectrum of behaviors and clinical presentations, ranging from asymptomatic cases to severe illnesses and fatalities. Despite substantial research efforts in recent years, significant uncertainties persist in understanding the disease, encompassing variations in clinical outcomes, comorbidities, and challenges faced by individuals infected with COVID-19. Beyond the acute phase of infection, the prevalence of post-COVID-19 symptoms, often denoted as "long COVID," is notable, particularly in individuals recovering from the disease. Nevertheless, a research gap persists concerning the pathophysiological mechanisms underlying newly emerging viral variant infections, post-COVID-19 conditions, and the corresponding therapeutic strategies. This review is presented to analyze recent advancements in comprehending the pathophysiology and therapy of COVID-19.
Keywords:
COVID 19
; recent advances
; pathophysiology
; therapy
1. Introduction
The onset of the COVID-19 pandemic in December 2019, marked by the diagnosis of patients in Wuhan, China with an atypical pneumonia, is on the brink of entering its fourth year. This event signifies the third major coronavirus outbreak, with the prior Middle East respiratory disease (MERS) and severe acute respiratory syndrome (SARS) viruses being contained before causing global pandemics. The ongoing evolution of SARS-CoV-2 has historically detrimentally impacted both global public health and the economy. By July 2023, the global tally of confirmed COVID-19 cases reached almost 767 million, resulting in nearly 6.95 million fatalities. Beyond acute illness and mortality, the pandemic has adversely affected psychological well-being, economic stability, and access to healthcare for other conditions, contributing to increased fatalities from additional medical complications. Moreover, the virus's rapid mutation and distribution have led to the emergence of various strains, including Alpha, Beta, Gamma, Delta, and Omicron, with heightened infectivity observed in several variants. Despite substantial research efforts, numerous unresolved issues persist regarding the disease, encompassing variations in clinical outcomes, comorbidities, and challenges faced by those infected. Notably, the prevalence of post-COVID-19 symptoms, known as "long COVID," remains a global concern. Yet, a notable research gap exists concerning the pathophysiological mechanisms of emerging viral variants, post-COVID-19 conditions, and corresponding therapeutic strategies. Consequently, this review is presented to analyze recent developments in comprehending the pathophysiology and therapy of COVID-19.
2. Pathophysiology and Pathogenesis
2.1. Interactions and entry of the SARS-CoV-2 into the cell
The main source of new infections is asymptomatic carriers and confirmed COVID-19 patients (16). It has been hypothesised that infection can occur via the fecal-oral pathway in addition to respiratory droplets and interaction with surfaces that are contaminated.[33–35] The viral spike (S) protein, which interacts to the angiotensin-converting enzyme 2 (ACE2) receptor when SARS-CoV-2 first infects humans, facilitates the virus's entrance into host cells like pneumocytes, bronchial epithelial cells, and nasal cells. The S protein of SARS-CoV-2 exhibits a binding affinity with ACE2 that is 10-20 times greater than that of SARS-CoV, which could account for the rapid spread of the pandemic. [36–38]
Figure 1.
Schematic representation of SARS-CoV-2 virus showing the Spike (S) protein which is heavily glycosylated (O-glycosylation and N-glycosylation) with numerous fucose, mannose and sialyl residues. These sugar moieties have the potential to bind to C-lectin type receptors (CLR), mannose receptor (MR), dendritic cell-specific intracellular adhesion molecule-3-grabbing non-integrin (DC-SIGN), homologue dendritic cell-specific intercellular adhesion molecule-3-grabbing nonintegrin related (L-SIGN), macrophage galactose-type lectin (MGL), toll-like receptors (TLR), and glucose regulated protein 78 (GRP78).
Figure 1.
Schematic representation of SARS-CoV-2 virus showing the Spike (S) protein which is heavily glycosylated (O-glycosylation and N-glycosylation) with numerous fucose, mannose and sialyl residues. These sugar moieties have the potential to bind to C-lectin type receptors (CLR), mannose receptor (MR), dendritic cell-specific intracellular adhesion molecule-3-grabbing non-integrin (DC-SIGN), homologue dendritic cell-specific intercellular adhesion molecule-3-grabbing nonintegrin related (L-SIGN), macrophage galactose-type lectin (MGL), toll-like receptors (TLR), and glucose regulated protein 78 (GRP78).
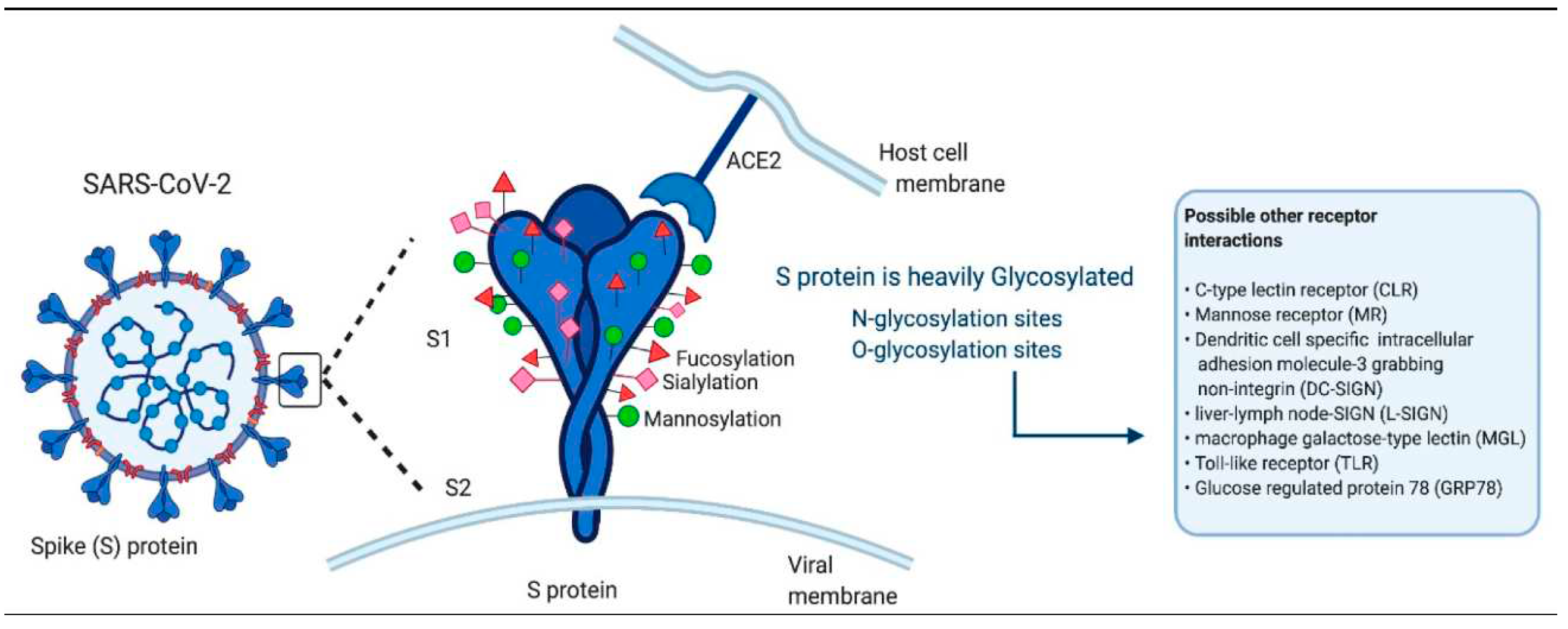
Figure 2.
Interaction between SARS-CoV-2 and host cell. The SARS-CoV-2 virion is composed of 4 structural proteins, spike protein (S), membrane protein (M), envelope protein (E), and nucleocapsid protein (N), associated with single-stranded RNA (ssRNA) of the virion. S protein interacts with the host cell ACE2 protein and is activated by TMPRSS2 as part of the infection mechanism.
Figure 2.
Interaction between SARS-CoV-2 and host cell. The SARS-CoV-2 virion is composed of 4 structural proteins, spike protein (S), membrane protein (M), envelope protein (E), and nucleocapsid protein (N), associated with single-stranded RNA (ssRNA) of the virion. S protein interacts with the host cell ACE2 protein and is activated by TMPRSS2 as part of the infection mechanism.

2.2. Long COVID
Even while extended COVID-19 is quite prevalent, little is known about the fundamental pathophysiology's mechanisms. A number of theories have been put forth to explain the pathophysiology of long-term COVID-19.[65,66] These include the following: dysfunctional neurological signalling, imbalance in microbiome in the gastrointestinal tract, reinstatement of secondary infectious agents (e.g., EBV, HHV-6, HCMV, VZV, etc.), immune system disruption, long-term exposure of SARS-CoV-2 in tissues, endothelial irregularities in microvascular clotting of the blood, autoimmunity along with immune priming from molecular mimicry, among others.[67,68] More research has revealed that two thirds of people with long-term COVID are linked to a number of possible risk factors and diseases, such as type 2 diabetes, female sex, underpinning viral reactivation, the existence of particular autoantibodies, along with disorders of connective tissue. There have been reports of a higher incidence of long COVID-19 in several ethnic groups, such as those who identify as Latino or Hispanic. Long COVID-19, which is associated to diminished income and lack of adequate rest in preliminary weeks following SARS-CoV-2 infection, characterised by neurological symptoms, gastrointestinal symptoms, cognitive impairment, brain fog, incomplete sleep, fatigue, pain, postural orthostatic tachycardia syndrome post-exertional and malaise and other symptoms. (69,70)
3. Recent Advances in Pathophysiology of COVID -19
3.1. Role of Soluble PD-L1 in the Course of Severe and Non-Severe COVID-19
After discovering that high levels of sPD-L1 corresponded with low lymphocyte counts and high CRP levels, as well as longer hospital length of stay (LOS) and death, Sabbatino, F.'s study suggested sPD-L1 as a useful prognostic biomarker for COVID-19. Moreover, SARS-CoV-2-infected epithelial cells showed an increase of sPD-L1 [20]. sPD-L1 overexpression was observed in COVID-19 patients who needed invasive mechanical breathing, according to another observational investigation [21]. It was determined that although sPD-L1 stimulates an immune escape during the early stages of COVID-19, it may also function to reduce an overabundance of an immune response later on, demonstrating its significance in COVID-19 prognosis.34-45
3.2. Molecular Dynamics Simulations Suggest SARS-CoV-2 3CLpro Mutations in Beta and Omicron Variants Do Not Alter Binding Affinities for Cleavage Sites of Non-Structural Proteins
De Freitas Amorim et al. found that Gly143 and Glu166 are important residues in substrate recognition based on hydrogen bonding investigations, indicating that these residues may be included as pharmacophoric centres for Beta and Omicron variations in drug design. Based on our findings, Gly143 and Glu166 may be broad-spectrum pharmacophoric centres of SARS-CoV-2 3CLpro since they are necessary residues to interact with Gln6 of the various substrates.41-46
3.3. Growth Arrest of Alveolar Cells in Response to Cytokines from Spike S1-Activated Macrophages: Role of IFN-γ
The symptoms of acute respiratory distress syndrome (ARDS) include high-permeability pulmonary edoema and severe hypoxemia.Along with these changes, there is an increase in the amount of amino acids inside the cell, which is probably related to the activation of protein degradation, as well as a blockade of protein synthesis and the activation of autophagy. Owing to an increased secretion of IFN-γ in the conditioned medium by S1-activated macrophages, these alterations are correlated with the induction of IFN-regulatory factor 1 (IRF-1). When baricitinib is added, the effects that are seen are avoided. Finally, our results imply that the alveolar epithelial damage seen in COVID-19-related ARDS may be related to the IFN-γ-IRF-1 signalling pathway.47-51
3.4. Molecular Dynamics Simulations Suggest SARS-CoV-2 3CLpro Mutations in Beta and Omicron Variants Do Not Alter Binding Affinities for Cleavage Sites of Non-Structural Proteins
The 3CL or nsp5 protease, the most significant viral protease needed for the maturation of viral proteins during host infection, is essential to the course of the SARS-CoV-2 infection. Here, 3CLproWT, 3CLproH41A, 3CLproBeta, and 3CLproOmicron were simulated for 500 ns in complex with the substrates nsp 4|5 and nsp 5|6 by de Freitas Amorim et al. De Freitas Amorim et al. demonstrate that neither conformational changes nor alterations in substrate binding affinities were significantly caused by mutations in the 3CLpro found in the SARS-CoV-2 variants of concern (VOCs). Nonetheless, 3CLproBeta and 3CLproOmicron showed noticeably high cleavage rates at the nsp4–nsp5 boundary, which may be crucial for viral fitness gain and replication.. Based on our findings, Gly143 and Glu166 may be broad-spectrum pharmacophoric centres of SARS since they are necessary residues to interact with Gln6 of the various substrates.-CoV-2 3CLpro.52-56
3.5. S-Peptide RBD 484–508 Induces IFN-γ T-Cell Response in Naïve-to-Infection and Unvaccinated Subjects with Close Contact with SARS-CoV-2-Positive Patients
Even though various anti-SARS-CoV-2 vaccines are available on the market, it is still unclear if these can promote long-lasting protection. Developing vaccines and pandemic control strategies require a thorough understanding of the adaptive immune response to SARS-CoV-2. IFN-γ is one of the key cytokines that lymphocytes release in response to viral infection, and it is essential for both innate and adaptive immunity. Murdoca M et al. report on 28 subjects who were unvaccinated and naïve to SARS-Cov-2 infection, and who had reported close and extended contact with COVID-19-positive patients. Based on the findings, T-cells infected with SARS-CoV-2 pseudovirus exhibit similar levels of IFN-γ gene expression and protein production when exposed to one of these peptides, RBD 484–508.57-62
Figure 3.
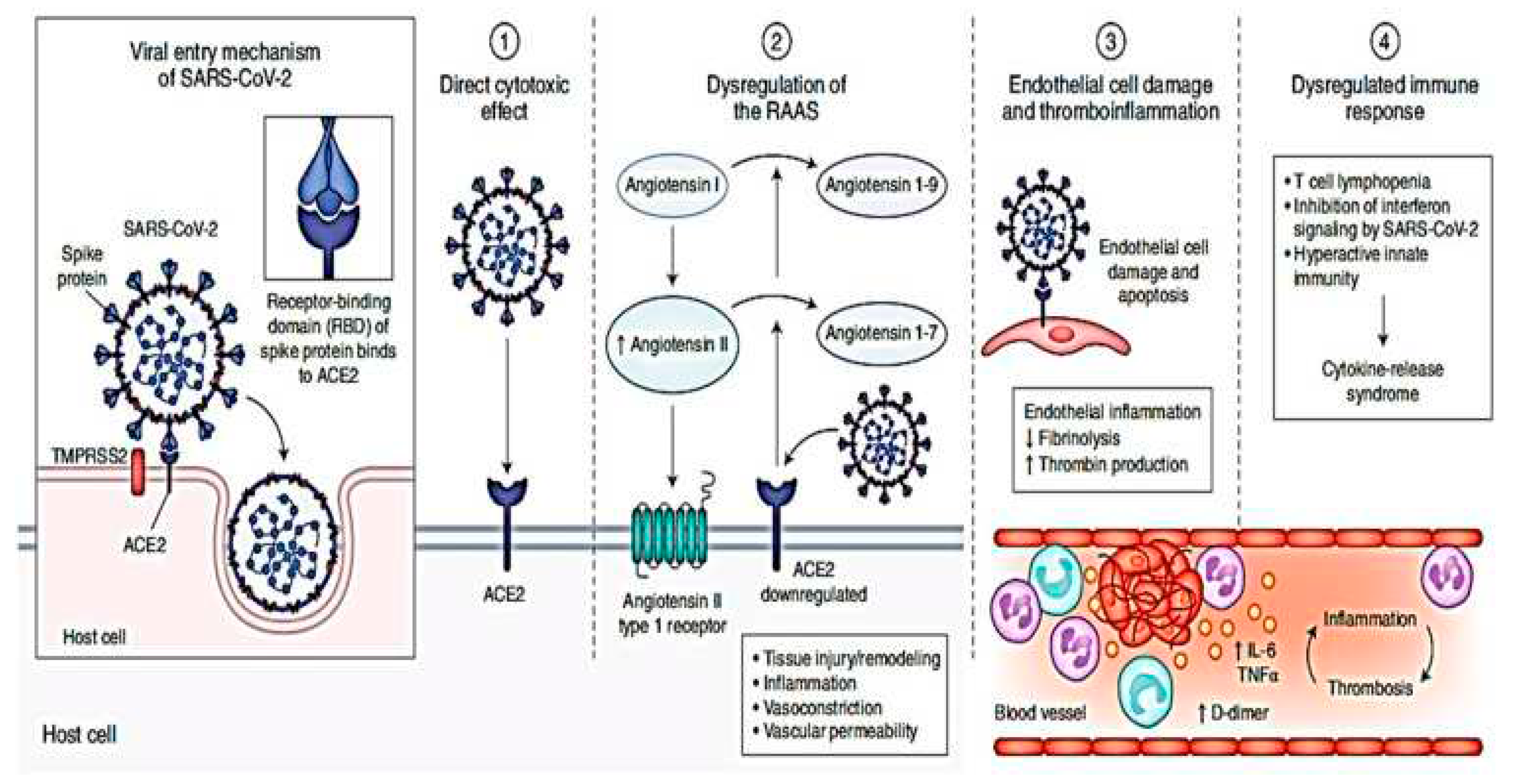
Pathophysiology of COVID-19 indicate virus entering the host cells through interaction of its spike protein with the entry receptor ACE2 in the presence of TMPRSS2. Notes: Reproduced by permission from: Gupta A, Madhavan MV, Sehgal K, et al. Extrapulmonary manifestations of COVID-19. Nature Medicine. 2020;26(7):1017–1032. doi:10.1038/s41591-020-0968-3.75 © Springer Nature America, Inc. 2020. This image is exlcuded from the Creative Commons license: Figure 1 is copyright protected and excluded from the open access license.
Figure 3.
Pathophysiology of COVID-19 indicate virus entering the host cells through interaction of its spike protein with the entry receptor ACE2 in the presence of TMPRSS2. Notes: Reproduced by permission from: Gupta A, Madhavan MV, Sehgal K, et al. Extrapulmonary manifestations of COVID-19. Nature Medicine. 2020;26(7):1017–1032. doi:10.1038/s41591-020-0968-3.75 © Springer Nature America, Inc. 2020. This image is exlcuded from the Creative Commons license: Figure 1 is copyright protected and excluded from the open access license.
3.6. New COVID Variants and their Implications
Genetic variations of SARS-CoV-2 continue to be surfacing and spreading over the globe since the start of this outbreak. Towards the end of 2020, however, a number of new variants that were linked to a catastrophic form of the condition and had enhanced transmission capability and infectiousness were found.3. These variations could be distinguished from other strains in circulation thanks to one or more mutations or spike protein substitutions. These variants were categorised into three types for convenience of understanding: variant of high consequence, variant of interest, and variant of concern (VOC) (Table 1).[75,76]. Depending on how a novel variant affects disease severity, diagnosis, treatment, vaccination, and transmission, it may or may not be included to one of these classifications. As a result, based on the most recent scientific information, a variant's status may increase or decrease.
3.7. Variants of Interest (VOI)
| WHO label | Lineage + additional mutations | Country first detected (community) | Spike mutations of interest | Year and month first detected | Impact on transmissibility | Impact on immunity | Impact on severity | Transmission in EU/EEA |
| Omicron | BA.2.75 (x) | India | (y) | May 2022 | Unclear (1) | Similar to Baseline (2-4) | No evidence | Community |
| Omicron | XBB.1.5-like (a) | United States | N460K, S486P, F490S | n/a | Similar to Baseline (5, 6) | Reduced (v) (5, 7) | Similar to Baseline (8) | Community |
| Omicron | XBB.1.5-like + F456L (b) (e.g. EG.5, FL.1.5.1, XBB.1.16.6, and FE.1) |
n/a | F456L, N460K, S486P, F490S | n/a | Baseline | Baseline (9) | Baseline | Dominant |
| Omicron | BA.2.86 | n/a | I332V, D339H, R403K, V445H, G446S, N450D, L452W, N481K, 483del, E484K, F486P | n/a | Unclear (10) | Unclear (10-12) | No evidence | Community |
3.8. Variants under monitoring.
| WHO label | Lineage + additional mutations | Country first detected (community) | Spike mutations of interest | Year and month first detected | Impact on transmissibility | Impact on immunity | Impact on severity | Transmission in EU/EEA |
| Omicron | XBB.1.16 | n/a | E180V, T478R, F486P | n/a | No evidence | No evidence | No evidence | Detected (a) |
| Omicron | DV.7.1 | n/a | K444T, L452R, L455F | n/a | No evidence | No evidence | No evidence | Detected (a) |
| Omicron | XBB.1.5-like + L455F + F456L (b) | n/a | L455F, F456L, N460K, S486P, F490S | n/a | No evidence | No evidence | No evidence | Detected (a |
3.9. Pathology and Postmortem Changes.
|
Lung |
Severe squamous metaplasia with atypia, interstitial and intra-alveolar oedema, type 2 pneumocyte hyperplasia, capillary congestion, hyaline membranes, pneumocytic necrosis, and exudative and proliferative widespread alveolar damage |
|
Liver |
Pathological lesions, such as cardiac hypertrophy, atherosclerosis, general interstitial fibrosis, mild myocardial edoema, and atypical, minor, localised, and perivascular interstitial fibrosis, were seen in the livers of COVID-19-related deaths. |
|
Brain |
Microthrombi and acute infarcts, hypoxic alterations without any specific disease, and perivascular lymphocytic infiltration in the brainstem |
|
Coagulation Abnormality |
Disseminated intravascular coagulopathy (DIC), PE, deep vein thrombosis (DVT), arterial thrombosis, hypercoagulable coagulopathy, and intra-catheter thrombosis, among other thrombotic and/or thromboembolic complications. |
|
Kidneys |
Diffuse proximal tubule damage with brush boundary loss, non-isometric vacuolar degeneration, and frank necrosis were observed in the kidneys of COVID-19 patients. |
3.10. Diagnosis
Microbiological testing is required for COVID-19 diagnosis. Individuals who experienced fever, respiratory symptoms, or a lower respiratory tract (LRT) infection are among those who should be tested. Those with a history of travel or those who have come into contact with suspected or confirmed COVID-19 cases are more likely to get the virus. The CDC and the Infectious Diseases Society of America (IDSA) had, however, highlighted the patient priorities for COVID-19 testing, including symptomatic critically ill persons, front-liners, and individuals with risk indicators, because to limits in testing capacity. [90–97]

Table 1.
: Diagnostic approaches for COVID-19.
| Types of diagnostic tests | Mechanism of detection | Source of samples | Result Interpretation |
|---|---|---|---|
| Nucleic acid amplification | Real Time PCR and NGS sequencing by using gene specific primer such as N,S,E and RdRP genes two independent sequences need to be detected | Nasal Swab, throat Swab, Bronchoalveolar lavage, blood faces and endotracheal aspirate | SARS-CoV2 Infection |
| Antibody based immunoassay | SARS-CoV2 IgM and IgG antibodies detection by ELISA | Serum | Immunity/Overall infection |
| Antigen based immunoassay | SARS-CoV2 detection protein | Nasal Swab, throat Swab, Bronchoalveolar lavage, blood faces and endotracheal aspirate | Confirm current SARS-CoV2 |
| CT- Imaging | Clinical symptoms (Fever/Cough, epidemiological history imaging CT) | Radiological features | Trade to identify for further target |
3.11. Clustered Regularly Interspaced Short Palindromic Repeats (CRISPR)
CRISPR is an expedient method specifically designed to identify SARS-CoV-2. Early in 2020, the USA-FDA approved the technique as a substitute test for COVID-19 identification.The assay's sample pool is comparable to that of RT-PCR. SARS-CoV-2 DETECTR is an assay that uses loop-mediated amplification (LMA) to perform isothermal amplification and simultaneous recombinase polymerase amplification (RPA) from the extracted RNA, followed by Cas12 detection.[57–67] The SARS-CoV-2 DETECTR test has several advantages over RT-PCR for COVID-19 detection. It requires fewer bulky apparatus, has an increased limit of detection, a quicker assay reaction time, and requires less assay sample. [68–87]
4. Recent Therapy in Management of COVID -19
4.1. High-Affinity Neutralizing DNA Aptamers against SARS-CoV-2 Spike Protein Variants
The ongoing emergence of novel SARS-CoV-2 variants that warrant concern has posed a challenge to current therapeutic approaches. In order to solve this, Ayass, M.A. et al. created a number of single-stranded DNA aptamers that both bind to the SARS-CoV-2 trimer S protein specifically and prevent it from interacting with ACE2 receptors. Short, single-stranded RNA or DNA molecules with a strong affinity for particular target molecules are known as aptamers. Since aptamers and their targets interact similarly to antigen-antibody interactions, they are frequently referred to as chemical antibodies. Aptamers, on the other hand, have a number of benefits over antibodies, including reduced size, decreased immunogenicity, long stability and shelf life, less variation from batch to batch, ease of modification, affordability, and speed of production.
More versatility in the selection of aptamers for diverse targets, including peptides, proteins, small organic compounds, toxins, cells, viruses, bacteria, etc., is made possible by the aptamers' flexible three-dimensional structures, which enable them to fold around the intricate surfaces of their target molecules. A number of groups have recently discovered DNA aptamers that are capable of recognising the S protein of SARS-CoV-2. Most of them were devoted to creating aptamers that attach to the S protein's RBD or S1 domain.56-71
Inhibition of PERK Kinase, an Orchestrator of the Unfolded Protein Response (UPR), Significantly Reduces Apoptosis and Inflammation of Lung Epithelial Cells Triggered by SARS-CoV-2 ORF3a Protein
It was discovered that the SARS-CoV-2 ORF3a accessory protein was pro-apoptotic, involved in immunomodulation, and released the virus. To investigate a possible mechanism of ORF3a-induced apoptotic and inflammatory death, ORF3a mRNA synthesised in vitro was transfected into lung epithelial cells (A549). It has been amply demonstrated that the protein plays a dynamic role as a "stress factor" for the endoplasmic reticulum, activating PERK kinase and other UPR-involved proteins and subsequently leading to the upregulation of their signalling pathway executers (ATF6, XBP-1s, PERK, phospho eIF2a, ATF4, CHOP, GADD34). In light of the aforementioned, we note that PERK kinase is a "master tactician" and that the emergence of ORF3a's apoptotic and inflammatory nature is primarily caused by its activation. As such, it may be a viable target for the development of novel therapeutic strategies.72-76
4.2. BREATHOX® Device Inhalation on Acute Symptoms Associated with COVID-19
According to Tanni, S. et al.'s hypothesis, patients with mild COVID-19 symptoms would have fewer respiratory symptoms when they used BREATHOX® to inhale NaCl particles. Thus, the main objective of this research was to compare the duration of COVID-19-induced acute symptoms to the standard of care (SOC) and assess the impact of oral and nasal inhalation of hypertonic NaCl particles (BREATHOX®). Secondly, we examined the incidence of unfavourable incidents associated with the use of the device.It was determined that BREATHOX® inhalation is safe and might help shorten the amount of time that COVID-19-induced coughing lasts.34-47
4.3. Role of Selective Digestive Decontamination in the Prevention of Ventilator-Associated Pneumonia in COVID-19 Patients
It has been reported that bacterial pneumonia, primarily ventilator-associated pneumonia (VAP), is a common complication in critically ill COVID-19 patients. The incidence of VAP ranges from 40 to 60%, and is approximately three times higher than in non-COVID-19 patients. assess whether the use of SDD in a systematic protocol for the prevention of ventilator-associated pneumonia (VAP) was successful in lowering the incidence of VAP in COVID-19 patients while maintaining the microbiological pattern of antibiotic resistance. Our pre-post observational study in COVID-19 patients, in light of other experiences, concludes that there is a correlation between the use of SDD in a structured protocol for VAP prevention and a decrease in the incidence of VAP, particularly late VAP, without an increase in the incidence of VAP caused by multidrug-resistant bacteria.67-78
4.4. Tocilizumab
A humanised monoclonal antibody directed against the IL-6 receptor is called tocilizumab. Early observational data indicated that tocilizumab treatment improved survival in hospitalised COVID-19 patients, especially if the medication was given early in the course of the illness. These results are in opposition to the results of the early RCTs, which were underpowered to rule out a sizable therapeutic effect but were mainly negative. Two sizable pragmatic RCTs afterwards showed an advantage in terms of mortality.[67–78]
4.5. Baricitinib
An oral inhibitor of Janus kinase 1 (JAK1) and JAK2 that has anti-inflammatory qualities is called baricitinib. A randomised controlled trial (RCT) involving 1,033 adult inpatients discovered that the combination of baricitinib (4 mg/day, for up to 14 days) and the antiviral medication remdesivir reduced recovery time more effectively than remdesivir alone.
Table 2.
: SARS-CoV-2 candidate drug treatments in Phase III-IV trials.
| Drug candidate | Description | Existing disease approval |
|---|---|---|
| Ritonavir | Anti-HIV Drug | Investigational combination |
| Lopinavir | Anti-viral | Investigational combination |
| Favipiravir | Antiviral agent against influenza | Influenza |
| Remdesivir | Viral RNA-dependent RNA polymerase | Broad spectrum anti-viral drug |
| Prezcobix | HIV-1 protease inhibitor | HIV infection |
| Galidesivir | Viral replication inhibitor | Antiviral against RNA viruses |
| Danoprevir | Inhibitors of NS3/4A | HCV Protease inhibitor |
| Umifenovir | Replication inhibitors | Anti-viral used for Influenza |
| Baloxavir marboxil (BXM) | Polymerase acidic endonuclease inhibitor | Anti-viral used for Influenza |
| Levovir | polymerase inhibitor | Anti-viral used for hepatitis B Virus |
| Dexamethasone | Anti-inflammatory | Rheumatoid arthritis |
| Oseltamivir | Neuraminidase inhibitor | Prevent Influenza A and B |
4.6. Antiviral therapies
Antiviral drugs were not authorised for use in treating COVID-19 at the onset of the pandemic. As a result, a number of repurposed treatments that demonstrated antiviral effectiveness in vitro were examined in clinical trials before being used in clinical settings. More potent antivirals are now available, although many commonly used medications, including hydroxychloroquine, lopinavir or ritonavir, and ivermectin, were demonstrated to be ineffective COVID-19 treatments when examined in well powered RCTs. [26–28]
4.7. Remdesivir
Remdesivir is an analogue of a prodrug nucleoside that displays antiviral action against several RNA viruses in vitro, including SARS-CoV-2. Its active metabolite inhibits RNA-dependent RNA polymerase, reducing genome replication [29,30]. Remdesivir has been investigated in both inpatient and outpatient COVID-19 patient situations.
4.8. Molnupiravir
An oral prodrug called molnupiravir is derived from β-D-N4-hydroxycytidine (NHC), an analogue of cytidine with broad-spectrum antiviral action against SARS-CoV-2 in vitro. As new RNA strands of the SARS-CoV-2 genome are synthesised, NHC is integrated into them, leading to a build-up of harmful mutations known as fatal mutagenesis. Molnupiravir decreased 29-day hospitalisation or mortality in the MOVe-OUT study, which included 1,433 adult outpatients with mild-to-moderate COVID-19. This was an impact that was not as significant as that seen with other antivirals. [99–105]
4.9. Antithrombotic therapies
Hospitalised COVID-19 patients had comparatively high rates of thrombotic and hemorrhagic sequelae, including venous thromboembolism (VTE), which can be fatal [48,49]. Known as "COVID-19-associated coagulopathy," these problems arise from a state of malfunction in the thrombo-inflammatory coagulation system[50]. This coagulopathy's pathophysiology is unclear and appears to be complex. Acute-phase reactant coagulation factors (especially fibrinogen and factor VIII) at elevated levels can cause endothelial injury, which can be attributed to the virus or the anti-viral immune response. Other pro-inflammatory mechanisms, such as the creation of neutrophil extracellular traps, can also play a role [49–52].
4.10. Neutralizing antibody therapies
Antibodies are essential for the adaptive immune response and for defending the body against infections. In order to neutralise a target virus by targeting it for elimination and preventing its entry into host cells, pathogen-specific polyclonal or monoclonal antibodies (mAbs) have been passively administered to control viral infections. This has led to the elimination of the infection-associated disease. Pathogen-specific neutralising antibodies can be produced as recombinant neutralising mAbs using proven molecular engineering techniques, or they can be transplanted from patients who have recovered from a viral infection (known as convalescent plasma).[134–137]
4.11. Therapies targeting the RAAS
Therapies that inhibit the production of angiotensin II (ACE inhibitors), inhibit the binding of angiotensin II to the angiotensin type I receptor (ARBs), speed up the conversion of angiotensin II to angiotensin (recombinant ACE2), or activate the angiotensin signalling (investigational drugs, including TRV–027 and TXA–127) are among those being assessed in randomised controlled trials. Recombinant ACE2 may also have the benefit of acting as a ruse for SARS-CoV-2, which could prevent viral spread.[132,133]
4.12. Development of SARS-CoV-2 Immunoglobulin based treatments option.
| Leading candidate | Description |
| Convalescent plasma | Passively transfer antibodies (Immunoglobulin) |
| STI-5656 (Abivertinib) | Tyrosine kinase inhibitor |
| PRO 140 (Leronlimab) | Monoclonal antibody targeted against CCR5 receptor |
| PTC299 | Dihydroorotate dehydrogenase inhibitors |
| CD24Fc | Immunomodulator (New drug) |
| Lenzilumab | Chronic Myelomonocytic leukemia |
| Tocilizumab | Immunosuppression |
| Sarilumab | Rheumatoid arthritis |
| Ravulizumab | Compliment inhibitors |
| Losmapimod | MAPK as potent suppressors of DUX4 expression |
| Pepcid H2 blocker | Mitigare (Colcrys) Anti-inflammatory agent |
4.13. Therapies for acute respiratory failure
Although there are other possible ways that COVID-19 can induce severe disease, acute hypoxemic respiratory failure is still the main culprit. In treating COVID-19-induced respiratory failure, particular attention must be paid to the timing of intubation, the mode of oxygen delivery, the use of prone positioning, and the use of adjuvant therapies for refractory hypoxaemia, in addition to decisions about the use of antivirals, immunomodulators, and anticoagulants, which may be beneficial to patients across the spectrum of illness.[130]
4.14. Oxygen delivery
For patients who need more oxygen than what a standard nasal cannula can provide, there are three noninvasive methods available: high-flow nasal cannula (HFNC), which provides warmed and humidified oxygen through large-bore nasal cannulas at flow rates higher than the patient's peak inspiratory flow rate; or noninvasive ventilation (NIV), which uses a tight-fitting mask connected to a noninvasive ventilation machine to provide continuous positive airway pressure or bilevel positive airway pressure.[131,132]
4.15. Prone positioning
Among those intubated for non-COVID-19 ARDS, prone positioning is one of the few therapies that has been demonstrated to lower mortality. Proning has not, however, been widely used in patients with COVID-19 ARDS due to persistent worries about its efficacy, resource usage, and potential to dislodge assist devices; data indicate significant inter-hospital variation in proning. Although proning in COVID-19 intubated patients has not been studied in randomised controlled trials, observational studies indicate that proning these patients early on may lower their mortality.
4.16. Adjunctive therapy for hypoxemia
The application of neuromuscular blockade in ARDS has been the subject of intense discussion in the years preceding the COVID-19 pandemic. According to the 2019 Reevaluation of Systemic Early Neuromuscular Blockade (ROSE) trial, neuromuscular blockade for 48 hours did not reduce 90-day mortality in patients with a partial pressure of arterial oxygen (PaO2) to fraction of inspired oxygen (FiO2) ratio less than 150 mmHg.
4.17. ECMO
ECMO may be a life-saving treatment for patients whose hypoxaemia is unresponsive to maximal ventilatory support, proning, neuromuscular inhibition, and inhaled pulmonary vasodilators. In patients with non-COVID-19 ARDS who had severe hypoxaemia, the ECMO to Rescue Lung Injury in Severe ARDS (EOLIA) trial, which was reported in 2018, revealed a mortality advantage. During the COVID-19 pandemic, ECMO use surged significantly.
4.18. Vaccines
In the case of the COVID-19 pandemic, vaccinations are an essential and affordable means of preventing the illness and reducing its severity. A potent vaccine is essential for stopping the virus's transmission and reducing the severity of the illness. There are several vaccinations on the market right now, including subunit, mRNA, inactivated, and viral vector vaccines. According to preliminary statistics, adenoviral vector vaccinations were 73% along with messenger RNA (mRNA) vaccines were 85 percent successful among individuals who were 18 years of age or older. After receiving the first and second doses of the vaccine, people produce neutralising antibodies against the targeted area. Vaccine recipients can mount robust immune responses against SARS-CoV-2 RBDs using adenovirus, mRNAs, and inactivated vaccines. [75–79]
Table 4.
:Tabular representation of ongoing clinical studies of vaccines for SARS-CoV-2.
| Vaccine candidate | Details |
|---|---|
| mRNA-1273 | mRNA-1273, a vaccine candidate based on previous study of SARS and MERS |
| Ad5-nCoV | Recombinant novel corona virus vaccine with adenovirus type 5 vector (Ad5) |
| ChAdOx1 | SARS-CoV-2, adenovirus vaccine vector MERS vaccine. |
| INO-4800 | DNA vaccine for SARS-CoV-2 |
| BNT162 | Modified mRNA-based, SARS-CoV-2 vaccine |
| NVX-CoV2373 | Recombinant nanoparticle vaccine candidates for SARS-CoV-2 |
| CureVac | mRNA-based SARS-CoV-2 vaccine |
| Vaxart | Oral recombinant SARS-CoV-2 vaccine; gene-based vaccine |
| DNA vaccine candidates | DNA-based vaccine for SARS-CoV-2 |
| mRNA vaccine | Repurposed SARS vaccine and mRNA vaccine candidate |
| DNA plasmid vaccine candidate | Modified vaccinia ankara virus like particles (MVA-VLP) vaccine candidate for SARS-CoV-2 |
| Adenovirus-based vector vaccine for SARS-CoV-2 | Adenovirus-based vector vaccine for SARS-CoV-2 |
| Modified avian coronavirus vaccine | Genetically similar avian coronavirus Infectious Bronchitis Virus |
| Gene-encoded antibody vaccine candidate | Next-generation, gene-encoded antibody vaccine for SARS-CoV-2 |
| DPX- SARS-CoV-2 | T-cell activating immunotherapy antigen vaccine |
| Intranasal DNA-based vaccine candidate | Stimulating an immune response in the nasal cavity |
| Single-dose patch delivery vaccine | Vaccine candidate for SARS-CoV-2 delivered through a single-dose patch |
Nonetheless, these vaccines' effectiveness is assessed in the first six months following inoculation. Over time, the immune system progressively weakened, making breakthrough infections more frequent. Furthermore, SARS-CoV-2 mutations have the ability to undermine protection and infect vaccinated individuals. It is effective to reduce the severity and mortality of disease by increasing host immunity with extra vaccination doses, particularly in elderly patients. Given the young participants' low hospitalisation and fatality rates, as well as the possibility of a significant immune response to the initial doses of the vaccine, it is challenging to determine whether boosters have any positive effects. Nonetheless, individuals with carcinomas and other immunosuppressive conditions have shown that current immunisations can elicit a sufficient immune response. Furthermore, variant-specific vaccinations have recently been created and licenced, but it is still unclear if they are exactly superior in real-world situations.[74–79]
4.19. Impact of new COVID 19 variants on vaccine
Variants of SARS-CoV-2, particularly VOCs, are a hazard to the ongoing COVID-19 pandemic containment efforts. Certain variations may even have a higher capacity for transmission, different aetiology and illness severity, and a connection to the sharp rise in COVID-19 cases and related hospitalisations. By changing the neutralising activity of monoclonal and vaccine-elicited antibodies, the VOCs directly affect the COVID-19 vaccines and immunotherapeutics that are now on the market, causing a modest to significant loss of efficacy. As of right now, no SARS-CoV-2 variant has the capacity to become severe enough to be categorised as a "variant of high consequence." It is impossible to completely rule out the prospect of such a variety emerging in the future, though. As a result, monitoring systems that can track the global appearance of new SARS-CoV-2 variants must be established. By putting prevention and control mechanisms in place early on, it will be possible to stop the spread of novel variations with significant consequences even if they do arise. [70–76]
5. FUTURE TRENDS
5.1. Intranasal gene therapy to prevent infection by SARS-CoV-2 variants
Since SARS-CoV-2 variants are more pathogenic and transmissible and can evade immunity, first-generation vaccines and monoclonal antibodies may no longer be as effective. A strategy to stop clinical consequences and the spread of SARS-CoV-2 variants was presented by Sims JJ et al. First, an angiotensin-converting enzyme 2 (ACE2) decoy protein was affinity matured by Sims JJ et al., leading to 1000-fold improvements in binding across a variety of SARS-CoV-2 variants and distantly related ACE2-dependent coronaviruses. They then showed how this ruse could be expressed in the proximal airway when an AAV vector was administered intranasally. When administered intraperitoneally, this intervention successfully achieved therapeutic levels of decoy expression at the surface of proximal airways, thereby significantly reducing the clinical and pathologic consequences of the SARS-CoV-2 challenge in a mouse model.56-65
5.2. Single-dose skin patch-delivered SARS-CoV-2 spike vaccine
Although there are several vaccines against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the world still faces numerous obstacles in the implementation of these treatments. SARS-CoV-2 has sickened over 160 million people and killed over 3.3 million. A study uses the high-density microarray patch (HD-MAP) to apply a skin-based vaccine against the spike subunit of SARS-CoV-2. They demonstrate how the vaccine is thermostable on the patches and how the administration of the patch boosts the immune system's cellular and antibody responses. Strong neutralisation of clinically significant isolates, such as the Alpha and Beta varieties, is achieved by evoked antibodies. Finally, in an ACE2-transgenic mouse model, a single dose of HD-MAP-delivered spike offered total protection against a fatal virus challenge. Taken together, these findings demonstrate that HD-MAP administration of a SARS-CoV-2 vaccine outperformed conventional needle-and-syringe vaccination and could be a valuable contribution to the ongoing COVID-19 (coronavirus disease 2019) pandemic.66-71
5.3. Oral vaccination
An investigational COVID vaccination that can be given orally has been found to protect the host while also reducing the virus's airborne transmission to unprotected people. Still more research is required and being conducted.
5.4. Ethical considerations
The COVID-19 pandemic presents complex ethical challenges across diverse domains, encompassing resource allocation, physical distancing, public health surveillance, and healthcare workers' rights. These issues are compounded by variations in health systems, cultural contexts, and socioeconomic environments globally. Recognizing the imperative for ethical guidance, the World Health Organization (WHO) established the Working Group on Ethics and COVID-19. This international group offers guidance on ethical considerations in clinical care, research, and public health policymaking. Noteworthy activities include providing advice on COVID-19 study ethics, contributing to WHO guidelines, and formulating emergency protocols for human research committees. Additionally, WHO collaborates with the Access to COVID-19 Tools (ACT) Accelerator, addressing diagnostics, therapeutics, and vaccine distribution ethically. The Global Health Ethics team at WHO coordinates international efforts, involving the Global Network of WHO Collaborating Centres for Bioethics and National Ethics Committees. The Public Health Emergency Preparedness and Response Ethics Network (PHEPREN) supports ethical decision-making during global health emergencies, focusing on the COVID-19 pandemic.
6. Conclusion
Over the past four years, there has been a considerable improvement in our understanding of COVID-19 pathophysiology, clinical care, and therapies. The ongoing appearance of variations, however, seriously jeopardises the efficacy of treatment and prevention strategies. The failure to administer early antiviral agents, high rates of false-negative diagnoses, conflicting information regarding the effectiveness of specific therapeutic drugs, and the quick progression of these infections to severe conditions like ARDS, pulmonary embolism, disseminated intravascular coagulation, sepsis, and cytokine storm pose challenges to the clinical management of these infections. The international effort to combat COVID-19 is probably going to take a while until we find antiviral medications or vaccines that are 100% successful at preventing the disease from spreading. Furthermore, as the pandemic fades, particular attention should be paid to the long-term effects like extended COVID-19, which could pose a significant healthcare problem in the years to come.
Author Contributions
Imran Rangraze1 – Concept, methodology, original draft, data analysis, writing and editing; Malay Jhancy2, - Data collection, editing,data analysis and proof reading; Shehla Shafi Khan3 – Data collection, editing, data analysis, proof reading
Funding
No funding was required during the preparation of this article
Informed Consent Statement
NA
Data Availability Statement
: from the PUBMED and related sources
Acknowledgements
We would like to thank our University President, Prof. Ismail Matalka, VP- Academics, prof. Ali Hajeer, VP-Research, Prof. Tanani and our Dean, Prof Bairy for their unconditional support.
Conflicts of Interest
The authors declare no conflict of interest
References
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet 2020, 395, 1054–62. [Google Scholar] [CrossRef] [PubMed]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; et al. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med 2020, 382, 727–33. [Google Scholar] [CrossRef] [PubMed]
- Malik, Y.A. Properties of coronavirus and SARS-coV-2. Malays J Pathol 2020, 42, 3–11 PubMed Abstract | Google Scholar. [Google Scholar] [PubMed]
- Thakur, V.; Ratho, R.K. OMICRON (B.1.1.529): A new SARS-CoV-2 variant of concern mounting worldwide fear. J Med Virol 2022, 94, 1821–24. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://covid19.who.int/?mapFilter=cases.
- Dang, A.; Thakker, R.; Li, S.; Hommel, E.; Mehta, H.B.; Goodwin, J.S. Hospitalizations and mortality from non-SARS-coV-2 causes among medicare beneficiaries at US hospitals during the SARS-coV-2 pandemic. JAMA Netw Open 2022, 5, :e221754. [Google Scholar] [CrossRef] [PubMed]
- Sher, L. The impact of the COVID-19 pandemic on suicide rates. QJM 2020, 113, 707–12. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the chinese center for disease control and prevention. JAMA 2020, 323, 1239–42. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Z.; Peng, F.; Xu, B.; Zhao, J.; Liu, H.; Peng, J.; et al. Risk factors of critical & mortal COVID-19 cases: A systematic literature review and meta-analysis. J Infect 2020, 81, e16–25. [Google Scholar] [CrossRef] [PubMed]
- Al-Aly, Z.; Xie, Y.; Bowe, B. High-dimensional characterization of post-acute sequelae of COVID-19. Nature 2021, 594, 259–64. [Google Scholar] [CrossRef]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; et al. Post-acute COVID-19 syndrome. Nat Med 2021, 27, 601–15. [Google Scholar] [CrossRef]
- Ceban, F.; Ling, S.; Lui, L.M.W.; Lee, Y.; Gill, H.; Teopiz, K.M.; et al. Fatigue and cognitive impairment in Post-COVID-19 Syndrome: A systematic review and meta-analysis. Brain Behav Immun 2022, 101, 93–135. [Google Scholar] [CrossRef]
- Davis, H.E.; McCorkell, L.; Vogel, J.M.; Topol, E.J. Author Correction: Long COVID: major findings, mechanisms and recommendations. Nat Rev Microbiol 2023, 21, 408. [Google Scholar] [CrossRef] [PubMed]
- Kedor, C.; Freitag, H.; Meyer-Arndt, L.; Wittke, K.; Hanitsch, L.G.; Zoller, T.; et al. A prospective observational study of post-COVID-19 chronic fatigue syndrome following the first pandemic wave in Germany and biomarkers associated with symptom severity. Nat Commun 2022, 13, 5104. [Google Scholar] [CrossRef]
- Klein, J.; Wood, J.; Jaycox, J.; Lu, P.; Dhodapkar, R.M.; Gehlhausen, J.R.; et al. Distinguishing features of Long COVID identified through immune profiling. medRxiv ( 2022. [CrossRef] [PubMed]
- Hoehl, S.; Rabenau, H.; Berger, A.; Kortenbusch, M.; Cinatl, J.; Bojkova, D.; et al. Evidence of SARS-coV-2 infection in returning travelers from wuhan, China. N Engl J Med 2020, 382, 1278–80. [Google Scholar] [CrossRef]
- National Health Commission Of The People's Republic Of China. Protocol for prevention and control of COVID-19 (Trial edition 6); Available online: http://wwwnhcgovcn/yzygj/s7653p/202203/b74ade1ba4494583805a3d2e40093d88shtml.
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Kruger, N.; Herrler, T.; Erichsen, S.; et al. SARS-coV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell 2020, 181, 271–80 e8. [Google Scholar] [CrossRef] [PubMed]
- Wrapp, D.; Wang, N.; Corbett, K.S.; Goldsmith, J.A.; Hsieh, C.L.; Abiona, O.; et al. Cryo-EM structure of the 2019-nCoV spike in the prefusion conformation. bioRxiv ( 2020. [CrossRef]
- Sungnak, W.; Huang, N.; Becavin, C.; Berg, M.; Queen, R.; Litvinukova, M.; et al. SARS-CoV-2 entry factors are highly expressed in nasal epithelial cells together with innate immune genes. Nat Med 2020, 26, 681–87. [Google Scholar] [CrossRef]
- Zou, X.; Chen, K.; Zou, J.; Han, P.; Hao, J.; Han, Z. Single-cell RNA-seq data analysis on the receptor ACE2 expression reveals the potential risk of different human organs vulnerable to 2019-nCoV infection. Front Med 2020, 14, 185–92. [Google Scholar] [CrossRef]
- Chen, R.; Fu, J.; Hu, J.; Li, C.; Zhao, Y.; Qu, H.; et al. Identification of the immunodominant neutralizing regions in the spike glycoprotein of porcine deltacoronavirus. Virus Res 2020, 276, 197834. [Google Scholar] [CrossRef]
- Zhao, Y.; Zhao, Z.; Wang, Y.; Zhou, Y.; Ma, Y.; Zuo, W. Single-cell RNA expression profiling of ACE2, the receptor of SARS-coV-2. Am J Respir Crit Care Med 2020, 202, 756–59. [Google Scholar] [CrossRef] [PubMed]
- Sefik, E.; Qu, R.; Junqueira, C.; Kaffe, E.; Mirza, H.; Zhao, J.; et al. Inflammasome activation in infected macrophages drives COVID-19 pathology. Nature 2022, 606, 585–93. [Google Scholar] [CrossRef] [PubMed]
- He, X.; Lau, E.H.Y.; Wu, P.; Deng, X.; Wang, J.; Hao, X.; et al. Temporal dynamics in viral shedding and transmissibility of COVID-19. Nat Med 2020, 26, 672–75. [Google Scholar] [CrossRef] [PubMed]
- Parasher, A. COVID-19: Current understanding of its Pathophysiology, Clinical presentation and Treatment. Postgrad Med J 2021, 97, 312–20. [Google Scholar] [CrossRef] [PubMed]
- Wan, Y.; Shang, J.; Graham, R.; Baric, R.S.; Li, F. Receptor recognition by the novel coronavirus from wuhan: an analysis based on decade-long structural studies of SARS coronavirus. J Virol 2020, 94. [Google Scholar] [CrossRef] [PubMed]
- Bai, Y.; Yao, L.; Wei, T.; Tian, F.; Jin, D.Y.; Chen, L.; et al. Presumed asymptomatic carrier transmission of COVID-19. JAMA 2020, 323, 1406–07. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Tian, S.; Lou, J.; Chen, Y. Familial cluster of COVID-19 infection from an asymptomatic. Crit Care 2020, 24, 119. [Google Scholar] [CrossRef] [PubMed]
- Ganyani, T.; Kremer, C.; Chen, D.; Torneri, A.; Faes, C.; Wallinga, J. Estimating the generation interval for coronavirus disease (COVID-19) based on symptom onset data, March 2020. Euro Surveill 2020, 25. [Google Scholar] [CrossRef]
- Anka, A.U.; Tahir, M.I.; Abubakar, S.D.; Alsabbagh, M.; Zian, Z.; Hamedifar, H.; et al. Coronavirus disease 2019 (COVID-19): An overview of the immunopathology, serological diagnosis and management. Scand J Immunol 2021, 93, e12998. [Google Scholar] [CrossRef]
- Yoshida, M.; Worlock, K.B.; Huang, N.; Huang, N.; Lindeboom, R.G.H.; Butler, C.R.; Kumasaka, N.; et al. Local and systemic responses to SARS-CoV-2 infection in children and adults. Nature 2022, 602, 321–27. [Google Scholar] [CrossRef]
- Hadjadj, J.; Yatim, N.; Barnabei, L.; Corneau, A.; Boussier, J.; Smith, N.; et al. Impaired type I interferon activity and inflammatory responses in severe COVID-19 patients. Science 2020, 369, 718–24. [Google Scholar] [CrossRef] [PubMed]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, transmission, diagnosis, and treatment of coronavirus disease 2019 (COVID-19): A review. JAMA 2020, 324, 782–93. [Google Scholar] [CrossRef] [PubMed]
- Leisman, D.E.; Deutschman, C.S.; Legrand, M. Facing COVID-19 in the ICU: vascular dysfunction, thrombosis, and dysregulated inflammation. Intensive Care Med 2020, 46, 1105–08. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; Shi, L.; Wang, Y.; Zhang, J.; Huang, L.; Zhang, C.; et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir Med 2020, 8, 420–22. [Google Scholar] [CrossRef] [PubMed]
- van de Veerdonk, F.L.; Netea, M.G.; van Deuren, M.; van der Meer, J.W.; de Mast, Q.; Bruggemann, R.J.; et al. Kallikrein-kinin blockade in patients with COVID-19 to prevent acute respiratory distress syndrome. Elife 2020, 9. [Google Scholar] [CrossRef]
- Singh, S.P.; Pritam, M.; Pandey, B.; Yadav, T.P. Microstructure, pathophysiology, and potential therapeutics of COVID-19: A comprehensive review. J Med Virol 2021, 93, 275–99. [Google Scholar] [CrossRef] [PubMed]
- Fu, Y.; Cheng, Y.; Wu, Y. Understanding SARS-coV-2-mediated inflammatory responses: from mechanisms to potential therapeutic tools. Virol Sin 2020, 35, 266–71. [Google Scholar] [CrossRef]
- Feldmann, M.; Maini, R.N.; Woody, J.N.; Holgate, S.T.; Winter, G.; Rowland, M.; et al. Trials of anti-tumour necrosis factor therapy for COVID-19 are urgently needed. Lancet 2020, 395, 1407–09. [Google Scholar] [CrossRef]
- Garbers, C.; Rose-John, S. Genetic IL-6R variants and therapeutic inhibition of IL-6 receptor signalling in COVID-19. Lancet Rheumatol 2021, 3, e96–7. [Google Scholar] [CrossRef]
- Li, H.; Liu, L.; Zhang, D.; Xu, J.; Dai, H.; Tang, N.; et al. SARS-CoV-2 and viral sepsis: observations and hypotheses. Lancet 2020, 395, 1517–20. [Google Scholar] [CrossRef]
- Lin, L.; Lu, L.; Cao, W.; Li, T. Hypothesis for potential pathogenesis of SARS-CoV-2 infection-a review of immune changes in patients with viral pneumonia. Emerg Microbes Infect 2020, 9, 727–32. [Google Scholar] [CrossRef]
- Ochani, R.; Asad, A.; Yasmin, F.; Shaikh, S.; Khalid, H.; Batra, S.; et al. COVID-19 pandemic: from origins to outcomes. A comprehensive review of viral pathogenesis, clinical manifestations, diagnostic evaluation, and management. Infez Med 2021, 29, 20–36. [Google Scholar] [PubMed]
- Cascella, M.; Rajnik, M.; Aleem, A.; Dulebohn, S.C.; Di Napoli, R. Features, evaluation, and treatment of coronavirus (COVID-19); StatPearls: Treasure Island, FL.
- Helms, J.; Tacquard, C.; Severac, F.; Leonard-Lorant, I.; Ohana, M.; Delabranche, X.; et al. High risk of thrombosis in patients with severe SARS-CoV-2 infection: a multicenter prospective cohort study. Intensive Care Med 2020, 46, 1089–98. [Google Scholar] [CrossRef] [PubMed]
- Wichmann, D.; Sperhake, J.P.; Lutgehetmann, M.; Steurer, S.; Edler, C.; Heinemann, A.; et al. Autopsy findings and venous thromboembolism in patients with COVID-19: A prospective cohort study. Ann Intern Med 2020, 173, 268–77. [Google Scholar] [CrossRef]
- McGonagle, D.; Bridgewood, C.; Ramanan, A.V.; Meaney, J.F.M.; Watad, A. COVID-19 vasculitis and novel vasculitis mimics. Lancet Rheumatol 2021, 3, e224–e33. [Google Scholar] [CrossRef] [PubMed]
- Nishiga, M.; Wang, D.W.; Han, Y.; Lewis, D.B.; Wu, J.C. COVID-19 and cardiovascular disease: from basic mechanisms to clinical perspectives. Nat Rev Cardiol 2020, 17, 543–58. [Google Scholar] [CrossRef]
- Bonaventura, A.; Vecchie, A.; Dagna, L.; Martinod, K.; Dixon, D.L.; Van Tassell, B.W.; et al. Endothelial dysfunction and immunothrombosis as key pathogenic mechanisms in COVID-19. Nat Rev Immunol 2021, 21, 319–29. [Google Scholar] [CrossRef]
- Blanco-Melo, D.; Nilsson-Payant, B.E.; Liu, W.C.; Uhl, S.; Hoagland, D.; Moller, R.; et al. Imbalanced host response to SARS-coV-2 drives development of COVID-19. Cell 2020, 181, 1036–45 e9. [Google Scholar] [CrossRef]
- Sariol, A.; Perlman, S. Lessons for COVID-19 immunity from other coronavirus infections. Immunity 2020, 53, 248–63. [Google Scholar] [CrossRef]
- Cui, L.; Wang, H.; Ji, Y.; Yang, J.; Xu, S.; Huang, X.; et al. The nucleocapsid protein of coronaviruses acts as a viral suppressor of RNA silencing in mamMalian cells. J Virol 2015, 89, 9029–43. [Google Scholar] [CrossRef]
- Hurst, K.R.; Koetzner, C.A.; Masters, P.S. Characterization of a critical interaction between the coronavirus nucleocapsid protein and nonstructural protein 3 of the viral replicase-transcriptase complex. J Virol 2013, 87, 9159–72. [Google Scholar] [CrossRef] [PubMed]
- Walz, L.; Cohen, A.J.; Rebaza, A.P.; Vanchieri, J.; Slade, M.D.; Dela Cruz, C.S.; et al. JAK-inhibitor and type I interferon ability to produce favorable clinical outcomes in COVID-19 patients: a systematic review and meta-analysis. BMC Infect Dis 2021, 21, 47. [Google Scholar] [CrossRef] [PubMed]
- Cicco, S.; Cicco, G.; Racanelli, V.; Vacca, A. Neutrophil extracellular traps (NETs) and damage-associated molecular patterns (DAMPs): two potential targets for COVID-19 treatment. Mediators Inflammation 2020, 2020, 7527953. [Google Scholar] [CrossRef]
- Day, J.D.; Park, S.; Ranard, B.L.; Singh, H.; Chow, C.C.; Vodovotz, Y. Divergent COVID-19 disease trajectories predicted by a DAMP-centered immune network model. Front Immunol 2021, 12, 754127. [Google Scholar] [CrossRef] [PubMed]
- Canaday, D.H.; Oyebanji, O.A.; White, E.; Keresztesy, D.; Payne, M.; Wilk, D.; et al. Significantly elevated antibody levels and neutralization titers in nursing home residents after SARS-CoV-2 BNT162b2 mRNA booster vaccination. medRxiv ( 2021. [CrossRef]
- Lucas, C.; Klein, J.; Sundaram, M.E.; Liu, F.; Wong, P.; Silva, J.; et al. Delayed production of neutralizing antibodies correlates with fatal COVID-19. Nat Med 2021, 27, 1178–86. [Google Scholar] [CrossRef] [PubMed]
- Ren, L.; Zhang, L.; Chang, D.; Wang, J.; Hu, Y.; Chen, H.; et al. The kinetics of humoral response and its relationship with the disease severity in COVID-19. Commun Biol 2020, 3, 780. [Google Scholar] [CrossRef]
- Xie, C.; Li, Q.; Li, L.; Peng, X.; Ling, Z.; Xiao, B.; et al. Association of early inflammation with age and asymptomatic disease in COVID-19. J Inflammation Res 2021, 14, 1207–16. [Google Scholar] [CrossRef] [PubMed]
- Therapeutics and COVID-19: living guideline, 22 april 2022; WHO/2019-nCoV/therapeutics/20223; World Health Organization: Geneva, 2022.
- Pretorius, E.; Venter, C.; Laubscher, G.J.; Kotze, M.J.; Oladejo, S.O.; Watson, L.R.; et al. Prevalence of symptoms, comorbidities, fibrin amyloid microclots and platelet pathology in individuals with Long COVID/Post-Acute Sequelae of COVID-19 (PASC). Cardiovasc Diabetol 2022, 21, 148. [Google Scholar] [CrossRef]
- Proal, A.D.; VanElzakker, M.B. Long COVID or post-acute sequelae of COVID-19 (PASC): an overview of biological factors that may contribute to persistent symptoms. Front Microbiol 2021, 12, 698169. [Google Scholar] [CrossRef]
- Spudich, S.; Nath, A. Nervous system consequences of COVID-19. Science 2022, 375, 267–69. [Google Scholar] [CrossRef] [PubMed]
- Zubchenko, S.; Kril, I.; Nadizhko, O.; Matsyura, O.; Chopyak, V. Herpesvirus infections and post-COVID-19 manifestations: a pilot observational study. Rheumatol Int 2022, 42, 1523–30. [Google Scholar] [CrossRef] [PubMed]
- Merzon, E.; Weiss, M.; Krone, B.; Cohen, S.; Ilani, G.; Vinker, S.; et al. Clinical and socio-demographic variables associated with the diagnosis of long COVID syndrome in youth: A population-based study. Int J Environ Res Public Health. [CrossRef]
- Renz-Polster, H.; Tremblay, M.E.; Bienzle, D.; Fischer, J.E. The pathobiology of myalgic encephalomyelitis/chronic fatigue syndrome: the case for neuroglial failure. Front Cell Neurosci 2022, 16, 888232. [Google Scholar] [CrossRef] [PubMed]
- Su, Y.; Yuan, D.; Chen, D.G.; Ng, R.H.; Wang, K.; Choi, J.; et al. Multiple early factors anticipate post-acute COVID-19 sequelae. Cell 2022, 185, 881–95 e20. [Google Scholar] [CrossRef]
- Choutka, J.; Jansari, V.; Hornig, M.; Iwasaki, A. Unexplained post-acute infection syndromes. Nat Med 2022, 28, 911–23. [Google Scholar] [CrossRef] [PubMed]
- Williamson, A.E.; Tydeman, F.; Miners, A.; Pyper, K.; Martineau, A.R. Short-term and long-term impacts of COVID-19 on economic vulnerability: a population-based longitudinal study (COVIDENCE UK). BMJ Open 2022, 12, e065083. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Zai, J.; Zhao, Q.; Nie, Q.; Li, Y.; Foley, B.T.; et al. Evolutionary history, potential intermediate animal host, and cross-species analyses of SARS-CoV-2. J Med Virol 2020, 92, 602–11. [Google Scholar] [CrossRef]
- van Doremalen, N.; Bushmaker, T.; Morris, D.H.; Holbrook, M.G.; Gamble, A.; Williamson, B.N.; et al. Aerosol and surface stability of SARS-coV-2 as compared with SARS-coV-1. N Engl J Med 2020, 382, 1564–67. [Google Scholar] [CrossRef] [PubMed]
- Sharif, N.; Alzahrani, K.J.; Ahmed, S.N.; Opu, R.R.; Ahmed, N.; Talukder, A.; et al. Protective measures are associated with the reduction of transmission of COVID-19 in Bangladesh: A nationwide cross-sectional study. PloS One 2021, 16, e0260287. [Google Scholar] [CrossRef]
- Ahmed, S.F.; Quadeer, A.A.; McKay, M.R. Preliminary identification of potential vaccine targets for the COVID-19 coronavirus (SARS-coV-2) based on SARS-coV immunological studies. Viruses ( 2020. [CrossRef]
- Sharif, N.; Alzahrani, K.J.; Ahmed, S.N.; Dey, S.K. Efficacy, immunogenicity and safety of COVID-19 vaccines: A systematic review and meta-analysis. Front Immunol 2021, 12, 714170. [Google Scholar] [CrossRef] [PubMed]
- McDonald, I.; Murray, S.M.; Reynolds, C.J.; Altmann, D.M.; Boyton, R.J. Comparative systematic review and meta-analysis of reactogenicity, immunogenicity and efficacy of vaccines against SARS-CoV-2. NPJ Vaccines 2021, 6, 74. [Google Scholar] [CrossRef] [PubMed]
- Seyahi, E.; Bakhdiyarli, G.; Oztas, M.; Kuskucu, M.A.; Tok, Y.; Sut, N.; et al. Antibody response to inactivated COVID-19 vaccine (CoronaVac) in immune-mediated diseases: a controlled study among hospital workers and elderly. Rheumatol Int 2021, 41, 1429–40. [Google Scholar] [CrossRef] [PubMed]
- Sonani, B.; Aslam, F.; Goyal, A.; Patel, J.; Bansal, P. COVID-19 vaccination in immunocompromised patients. Clin Rheumatol 2021, 40, 797–98. [Google Scholar] [CrossRef] [PubMed]
- Dai, W.C.; Zhang, H.W.; Yu, J.; Xu, H.J.; Chen, H.; Luo, S.P.; et al. CT imaging and differential diagnosis of COVID-19. Can Assoc Radiol J 2020, 71, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Fistera, D.; Hartl, A.; Pabst, D.; Manegold, R.; Holzner, C.; Taube, C.; et al. What about the others: differential diagnosis of COVID-19 in a German emergency department. BMC Infect Dis 2021, 21, 969. [Google Scholar] [CrossRef] [PubMed]
- Rai, P.; Kumar, B.K.; Deekshit, V.K.; Karunasagar, I.; Karunasagar, I. Detection technologies and recent developments in the diagnosis of COVID-19 infection. Appl Microbiol Biotechnol 2021, 105, 441–55. [Google Scholar] [CrossRef] [PubMed]
- Spinner, C.D.; Gottlieb, R.L.; Criner, G.J.; Arribas Lopez, J.R.; Cattelan, A.M.; Soriano Viladomiu, A.; et al. Effect of Remdesivir vs Standard Care on Clinical Status at 11 Days in Patients With Moderate COVID-19: A Randomized Clinical Trial. JAMA 2020, 324, 1048–57. [Google Scholar] [CrossRef]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; et al. Remdesivir for the treatment of covid-19 - final report. N Engl J Med 2020, 383, 1813–26. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, D.; Du, G.; Du, R.; Zhao, J.; Jin, Y.; et al. Remdesivir in adults with severe COVID-19: a randomised, double-blind, placebo-controlled, multicentre trial. Lancet 2020, 395, 1569–78. [Google Scholar] [CrossRef]
- Jayk Bernal, A.; Gomes da Silva, M.M.; Musungaie, D.B.; Kovalchuk, E.; Gonzalez, A.; Delos Reyes, V.; et al. Molnupiravir for oral treatment of covid-19 in nonhospitalized patients. N Engl J Med 2022, 386, 509–20. [Google Scholar] [CrossRef] [PubMed]
- Hammond, J.; Leister-Tebbe, H.; Gardner, A.; Abreu, P.; Bao, W.; Wisemandle, W.; et al. Oral nirmatrelvir for high-risk, nonhospitalized adults with covid-19. N Engl J Med 2022, 386, 1397–408. [Google Scholar] [CrossRef] [PubMed]
- Dougan, M.; Nirula, A.; Azizad, M.; Mocherla, B.; Gottlieb, R.L.; Chen, P.; et al. Bamlanivimab plus etesevimab in mild or moderate covid-19. N Engl J Med 2021, 385, 1382–92. [Google Scholar] [CrossRef] [PubMed]
- Weinreich, D.M.; Sivapalasingam, S.; Norton, T.; Ali, S.; Gao, H.; Bhore, R.; et al. REGN-COV2, a neutralizing antibody cocktail, in outpatients with covid-19. N Engl J Med 2021, 384, 238–51. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.; Nirula, A.; Heller, B.; Gottlieb, R.L.; Boscia, J.; Morris, J.; et al. SARS-coV-2 neutralizing antibody LY-coV555 in outpatients with covid-19. N Engl J Med 2021, 384, 229–37. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.S.; Nirula, A.; Mulligan, M.J.; Novak, R.M.; Marovich, M.; Yen, C.; et al. Effect of bamlanivimab vs placebo on incidence of COVID-19 among residents and staff of skilled nursing and assisted living facilities: A randomized clinical trial. JAMA 2021, 326, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Guimaraes, P.O.; Quirk, D.; Furtado, R.H.; Maia, L.N.; Saraiva, J.F.; Antunes, M.O.; et al. Tofacitinib in patients hospitalized with covid-19 pneumonia. N Engl J Med 2021, 385, 406–15. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Wei, J.; Zou, L.; Jiang, T.; Wang, G.; Chen, L.; et al. Ruxolitinib in treatment of severe coronavirus disease 2019 (COVID-19): A multicenter, single-blind, randomized controlled trial. J Allergy Clin Immunol 2020, 146, 137–46 e3. [Google Scholar] [CrossRef]
- Shen, C.; Wang, Z.; Zhao, F.; Yang, Y.; Li, J.; Yuan, J.; et al. Treatment of 5 critically ill patients with COVID-19 with convalescent plasma. JAMA 2020, 323, 1582–89. [Google Scholar] [CrossRef]
- Simonovich, V.A.; Burgos Pratx, L.D.; Scibona, P.; Beruto, M.V.; Vallone, M.G.; Vazquez, C.; et al. A randomized trial of convalescent plasma in covid-19 severe pneumonia. N Engl J Med 2021, 384, 619–29. [Google Scholar] [CrossRef]
- A living WHO guideline on drugs for covid-19. BMJ 2022, 377, o1045. [CrossRef]
- Gordon, C.J.; Tchesnokov, E.P.; Woolner, E.; Perry, J.K.; Feng, J.Y.; Porter, D.P.; et al. Remdesivir is a direct-acting antiviral that inhibits RNA-dependent RNA polymerase from severe acute respiratory syndrome coronavirus 2 with high potency. J Biol Chem 2020, 295, 6785–97. [Google Scholar] [CrossRef] [PubMed]
- Gavriatopoulou, M.; Ntanasis-Stathopoulos, I.; Korompoki, E.; Fotiou, D.; Migkou, M.; Tzanninis, I.G.; et al. Emerging treatment strategies for COVID-19 infection. Clin Exp Med 2021, 21, 167–79. [Google Scholar] [CrossRef] [PubMed]
- Menendez-Arias, L. Decoding molnupiravir-induced mutagenesis in SARS-CoV-2. J Biol Chem 2021, 297, 100867. [Google Scholar] [CrossRef] [PubMed]
- Gordon, C.J.; Tchesnokov, E.P.; SChinazi, R.F.; Gotte, M. Molnupiravir promotes SARS-CoV-2 mutagenesis via the RNA template. J Biol Chem 2021, 297, 100770. [Google Scholar] [CrossRef] [PubMed]
- Kabinger, F.; Stiller, C.; Schmitzova, J.; Dienemann, C.; Kokic, G.; Hillen, H.S.; et al. Mechanism of molnupiravir-induced SARS-CoV-2 mutagenesis. Nat Struct Mol Biol 2021, 28, 740–46. [Google Scholar] [CrossRef] [PubMed]
- Abdelnabi, R.; Foo, C.S.; De Jonghe, S.; Maes, P.; Weynand, B.; Neyts, J. Molnupiravir inhibits replication of the emerging SARS-coV-2 variants of concern in a hamster infection model. J Infect Dis 2021, 224, 749–53. [Google Scholar] [CrossRef]
- Vangeel, L.; Chiu, W.; De Jonghe, S.; Maes, P.; Slechten, B.; Raymenants, J.; et al. Remdesivir, Molnupiravir and Nirmatrelvir remain active against SARS-CoV-2 Omicron and other variants of concern. Antiviral Res 2022, 198, 105252. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Lu, T.L.; Lin, L. Real-world clinical outcomes of molnupiravir for the treatment of mild to moderate COVID-19 in adult patients during the dominance of the omicron variant: A meta-analysis. Antibiotics (Basel). [CrossRef]
- Owen, D.R.; Allerton, C.M.N.; Anderson, A.S.; Aschenbrenner, L.; Avery, M.; Berritt, S.; et al. An oral SARS-CoV-2 M(pro) inhibitor clinical candidate for the treatment of COVID-19. Science 2021, 374, 1586–93. [Google Scholar] [CrossRef]
- Sevrioukova, I.F.; Poulos, T.L. Structure and mechanism of the complex between cytochrome P4503A4 and ritonavir. Proc Natl Acad Sci U.S.A. 2010, 107, 18422–7. [Google Scholar] [CrossRef]
- Ju, B.; Zhang, Q.; Ge, J.; Wang, R.; Sun, J.; Ge, X.; et al. Human neutralizing antibodies elicited by SARS-CoV-2 infection. Nature 2020, 584, 115–19. [Google Scholar] [CrossRef] [PubMed]
- Klank, D.; Hoffmann, M.; Claus, B.; Zinke, F.; Bergner, R.; Paschka, P. Monoclonal antibodies for the prevention and treatment of COVID-19 disease in patients with hematological Malignancies: two case reports and a literature review. Hemasphere 2021, 5, e651. [Google Scholar] [CrossRef] [PubMed]
- O'Brien, M.P.; Forleo-Neto, E.; Musser, B.J.; Isa, F.; Chan, K.C.; Sarkar, N.; et al. Subcutaneous REGEN-COV antibody combination to prevent covid-19. N Engl J Med 2021, 385, 1184–95. [Google Scholar] [CrossRef] [PubMed]
- Bavaro, D.F.; Diella, L.; Solimando, A.G.; Mocherla, B.; Gottlieb, R.L.; Chen, P.; et al. Bamlanivimab and Etesevimab administered in an outpatient setting for SARS-CoV-2 infection. Pathog Glob Health 2022, 116, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Jenks, J.D.; Aslam, S.; Horton, L.E.; Law, N.; Bharti, A.; Logan, C.; et al. Early monoclonal antibody administration can reduce both hospitalizations and mortality in high-risk outpatients with coronavirus disease 2019 (COVID-19). Clin Infect Dis 2022, 74, 752–53. [Google Scholar] [CrossRef] [PubMed]
- WHO Rapid Evidence Appraisal for COVID-19 Therapies (REACT) Working Group. Anti-interleukin-6 therapies for hospitalized patients with COVID-19: a protocol for a prospective meta-analysis of randomized trials. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-PMA_protocols-anti-IL-6-2021.1 (accessed on 10 June 2021).
- Group WHOREAfC-TW, Shankar-Hari M, Vale CL, Godolphin PJ, Fisher D, Higgins JPT, et al. Association between administration of IL-6 antagonists and mortality among patients hospitalized for COVID-19: A meta-analysis. JAMA 2021, 326, 499–518. [Google Scholar] [CrossRef] [PubMed]
- Study to assess the efficacy and safety of ruxolitinib in patients with COVID-19 associated cytokine storm (RUXCOVID); ClinicalTrials.gov National Library of Medicine: Bethesda, MD, USA; Available online: https://clinicaltrials.gov/ct2/show/results/NCT04362137 (accessed on 04 January 2022).
- Fragoulis, G.E.; McInnes, I.B.; Siebert, S. JAK-inhibitors. New players in the field of immune-mediated diseases, beyond rheumatoid arthritis. Rheumatol (Oxford) (2019) 58(Suppl 1):i43–54. [CrossRef]
- Schwartz, D.M.; Kanno, Y.; Villarino, A.; Ward, M.; Gadina, M.; O'Shea, J.J. JAK inhibition as a therapeutic strategy for immune and inflammatory diseases. Nat Rev Drug Discovery 2017, 16, 843–62. [Google Scholar] [CrossRef] [PubMed]
- Alhazzani, W.; Moller, M.H.; Arabi, Y.M.; Loeb, M.; Gong, M.N.; Fan, E.; et al. Surviving Sepsis Campaign: guidelines on the management of critically ill adults with Coronavirus Disease 2019 (COVID-19). Intensive Care Med 2020, 46, 854–87. [Google Scholar] [CrossRef] [PubMed]
- Bai, C.; Chotirmall, S.H.; Rello, J.; Alba, G.A.; Ginns, L.C.; Krishnan, J.A.; et al. Updated guidance on the management of COVID-19: from an American Thoracic Society/European Respiratory Society coordinated International Task Force (29 July 2020). Eur Respir Rev 2020, 29. [Google Scholar] [CrossRef]
- Calzetta, L.; Aiello, M.; Frizzelli, A.; Rogliani, P.; Chetta, A. Dexamethasone in patients hospitalized with COVID-19: whether, when and to whom. J Clin Med 2021, 10. [Google Scholar] [CrossRef]
- Jamaati, H.; Hashemian, S.M.; Farzanegan, B.; Malekmohammad, M.; Tabarsi, P.; Marjani, M.; et al. No clinical benefit of high dose corticosteroid administration in patients with COVID-19: A preliminary report of a randomized clinical trial. Eur J Pharmacol 2021, 897, 173947. [Google Scholar] [CrossRef]
- Roback, J.D.; Guarner, J. Convalescent plasma to treat COVID-19: possibilities and challenges. JAMA 2020, 323, 1561–62. [Google Scholar] [CrossRef] [PubMed]
- Ankcorn, M.; Gallacher, J.; Ijaz, S.; Taha, Y.; Harvala, H.; Maclennan, S.; et al. Convalescent plasma therapy for persistent hepatitis E virus infection. J Hepatol 2019, 71, 434–38. [Google Scholar] [CrossRef]
- van Griensven, J.; Edwards, T.; de Lamballerie, X.; Semple, M.G.; Gallian, P.; Baize, S.; et al. Evaluation of convalescent plasma for ebola virus disease in Guinea. N Engl J Med 2016, 374, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Zhou, B.; Zhong, N.; Guan, Y. Treatment with convalescent plasma for influenza A (H5N1) infection. N Engl J Med 2007, 357, 1450–1. [Google Scholar] [CrossRef] [PubMed]
- Lamikanra, A.; Nguyen, D.; Simmonds, P.; Williams, S.; Bentley, E.M.; Rowe, C.; et al. Comparability of six different immunoassays measuring SARS-CoV-2 antibodies with neutralizing antibody levels in convalescent plasma: From utility to prediction. Transfusion 2021, 61, 2837–43. [Google Scholar] [CrossRef]
- O'Donnell, M.R.; Grinsztejn, B.; Cummings, M.J.; Justman, J.E.; Lamb, M.R.; Eckhardt, C.M.; et al. A randomized double-blind controlled trial of convalescent plasma in adults with severe COVID-19. J Clin Invest 2021, 131. [Google Scholar] [CrossRef]
- Haagmans, B.L.; Noack, D.; Okba, N.M.A.; Li, W.; Wang, C.; Bestebroer, T.; et al. SARS-coV-2 neutralizing human antibodies protect against lower respiratory tract disease in a hamster model. J Infect Dis 2021, 223, 2020–28. [Google Scholar] [CrossRef]
- Sharma, R.; Sharma, S. Physiology, blood volume; StatPearls: Treasure Island, FL, 2022. [Google Scholar]
- Siemieniuk, R.A.; Bartoszko, J.J.; Diaz Martinez, J.P.; Kum, E.; Qasim, A.; Zeraatkar, D.; et al. Antibody and cellular therapies for treatment of covid-19: a living systematic review and network meta-analysis. BMJ 2021, 374, n2231. [Google Scholar] [CrossRef]
- Cheung, J.C.; Ho, L.T.; Cheng, J.V.; Cham, E.Y.K.; Lam, K.N. Staff safety during emergency airway management for COVID-19 in Hong Kong. Lancet Respir Med 2020, 8, e19. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



