
Submitted:
22 November 2023
Posted:
26 November 2023
You are already at the latest version
Abstract
Energy imbalance gap (EIG) is defined as the average daily difference between energy intake (EI) and energy expenditure (EE). This study aimed to examine the associations between EIG and sociodemographic and anthropometric variables in the adolescent population of eight Latin American countries. A total of 680 adolescents aged 15 to 18 were included in this study. EI was estimated using two non-consecutive 24-hour dietary recalls. EE was predicted from Schofield equations using physical activity levels obtained through the long version of the International Physical Activity Questionnaire. Sociodemographic data and anthropometric measurements were also obtained. A descriptive analysis and multilevel linear regression models were used to examine associations between variables. The mean EI, EE, and EIG were 2091.3 kcal, 2067.8 kcal, and 23.5 kcal, respectively. Argentina and Colombia had the highest EI and EIG, whereas Chile and Costa Rica had the lowest EI and EIG. Males had a higher EI (2262.4 kcal) and EE (2172.2 kcal) than females (1930.1 kcal and 2084.5 kcal), respectively (p<0,05). Overweight subjects had a lower EIG than did underweight and normal-weight subjects (p<0,05). Subjects with high SES had a lower EE (2047.0 kcal) than those with low SES (1963.7 kcal) (p<0,05). Sex and BMI were associated with EIG in adolescents from Latin America.
Keywords:
energy balance
; energy expenditure
; energy intake
; energy imbalance gap
; underweight
; overweight
; Latin America
1. Introduction
Latin America (LA) is a region with several and complex health concern and the double burden of malnutrition is an important one. Globally, there has been interest in adolescents as a group that is relevant for the future health of the population, thus, the World Health Organization (WHO) included among its prioritizing groups adolescents [1]. A previous global report [2] established that overweight in adolescents is increasing in LA, with a prevalence between 15 and 25% in most countries of the region. In contrast, the moderate and severe underweight prevalence was below 10% for both girls and boys in all LA countries [2]. On the other hand, according to a recent report [3], in LA and the Caribbean, almost two thirds of adolescents are insufficiently physically active. More of 40% were sedentary, and more of 20% were physically inactive. These results were more frequent among girls than boys. These constitute low energy expenditure (EE) indicators in adolescents of the region.
For approximately a century, weight control has been assumed to be the consequence of small cumulative imbalance gaps between energy intake (EI) and EE [4]. The energy imbalance gap (EIG) is defined as the average daily difference between EI and EE [5]. Therefore, a positive energy balance occurs when EI exceeds EE. In contrast, a negative energy balance occurs when the EE is larger than the EI [6] by applying the First Law of Thermodynamics (energy conservation principle) [7]. This approach is simple and easy to remember by the general population; therefore, it is commonly used for educational purposes in public health, especially in dietary guidelines [8,9].
Nevertheless, at the individual level, the energy balance model states that the brain is the primary organ responsible for body weight regulation via the integration of neuro-endocrine-gastrointestinal signaling pathways that increase or decrease overall EI [10]. Additionally, EIG is influenced by major environmental, economic, and social trends [11] and must be evaluated equally. Owing to this complex system, an individual's energy balance can vary daily. Therefore, accurate measures of energy balance in humans are controversial. More precise methods are costly and challenging to perform in public health and epidemiological studies. Nevertheless, knowing the trends within a population is key to monitoring well-being and contributing to the prevention of chronic diseases [12].
To date, only a limited number of studies have been conducted to examine EIG in a large population [5,6,13,14], finding that there is heterogeneity in EIG by ethnicity, sex, and body mass index (BMI) in adults. A previous experience of authors in adults of LA [6], found that the overall EIG was positive, meaning that people consumed more energy than they were expending. This was more pronounced in men and people of higher socioeconomic status. Overweight and obese people from Argentina, Costa Rica, Ecuador, Peru, and Venezuela had a significantly lower EIG than underweight people. These findings suggest a high variability in the EIG and its correlates in eight countries of LA. For the age group of adolescents, much uncertainty still exists about the relationship between EIG and socioeconomic status, anthropometrics, and lifestyle.
This context highlights the relevance of studying the characteristics associated with maintaining a good balance between EI and EE in adolescents, as a key component of overall regional prevention policies. Being overweight in adolescents can cause various health and emotional problems, including type 2 diabetes, obstructive sleep apnea, hypertension, dyslipidemia, metabolic syndrome, eating disorders, and depression [15,16]. However, undernutrition can also increase the risk for suffering other chronic health problems such as lower fat oxidation, lower energy expenditure, insulin resistance, a higher risk of diabetes in adulthood, hypertension, dyslipidemia, and a lowered working capacity of manual workers [17].
This study aimed to examine the associations between the EIG and sociodemographic and anthropometric variables in the adolescent population of the eight LA countries evaluated.
2. Materials and Methods
2.1. Study Design and Sample
The Latin American Study of Nutrition and Health (Estudio Lationamericano de Nutrición y Salud; ELANS) is a multicenter cross-sectional nutritional and health surveillance study of a nationally representative sample of urban populations from eight Latin American countries (Argentina, Brazil, Chile, Colombia, Costa Rica, Ecuador, Peru and Venezuela). This study addressed EI, EE, and anthropometric measurements in 10,134 subjects between 15 and 65 years of age, in a lapse between September 2014 and July 2015.
A multistage sampling process was used to select the sample, stratified by geographical location, sex, age, and socioeconomic status (SES), with a random selection of primary and secondary sampling units for the urban population in order to achieve an urban representative sample [18]. Of 9,218 subjects, only 937 were adolescents (15-18 years), and another group of 257 subjects was excluded due to incomplete data. The final sample consisted of 680 adolescents (Figure 1).
2.2. Socioeconomic and anthropometric variables
A sociodemographic questionnaire was developed to evaluate the sociodemographic characteristics of the adolescents, such as country, sex, age, SES, educational level, and ethnicity. Household SES was measured using appropriate scales for each country and classified as high, middle, and low. For educational level, the categories were basis, high school, and undergraduate. Ethnicity was obtained based on self-reported race or ethnicity and divided into five groups: Caucasian, Mestizo, Afro-American, Indigenous and Others.
After administering the questionnaire, adolescents’ body weight and height were measured and recorded following the standard method, wearing light clothing and no shoes. Body weight (kg) was measured using calibrated electronic scales (Seca®, Hamburg, Germany), with an accuracy of 0.1 kg. Body height (cm) was measured using a portable stadiometer (Seca®, Hamburg, Germany) with an accuracy of 0.1 cm. BMI was calculated as the weight in kilograms divided by the square of height in meters. The BMI for age and height for age were assessed according to the reference values of the WHO [20]; and classified as underweight, normal weight or overweight. On the other hand, height was classified as low height, risk of low height, and normal height according to the WHO standard.
2.3. Energy intake
To estimate EI, a dietary assessment using two nonconsecutive 24 h food recalls was applied. The Multiple Pass Method was employed to assess all foods and beverages consumed on the previous day [21]. To estimate portion sizes, photographic albums of common foods from each country and household utensils were used. The selected portions transformed into grams and milliliters by a group of nutritionists trained for this activity.
In another step, macronutrients consumption was transformed into EI using the software Nutrition Data System for Research (NDS-R, Minnesota University, MN, USA. Version 2013). The web-based statistical modelling technique, the Multiple Source Method (MSM), proposed by the European Prospective Investigation into Cancer and Nutrition (EPIC) [22], was used to estimate the usual EI considering within-person variance.
2.4. Energy expenditure
The total EE was calculated using the basal metabolic rate (BMR) according to the FAO/WHO [23] and the activity factors for physical activity (PA) published by Gerrior et al. [24]; using the following formula:
Energy Expenditure Equation: (EE = BMR x PA)
To estimate the BMR, the equations of the “Human Energy Requirements” report were used, which comprised variables such as sex, age and weight.
PA was assessed using the International Physical Activity Questionnaire (IPAQ) in its extended Spanish version, which was validated for LA [25]. The domains of active transportation and leisure-time PA were included because of the greater relevance of these domains for guiding public health policies and programs [25] and the relatively low validity of the IPAQ items on occupational and home-based PA questions in adolescents of LA countries.
Thus, data on PA from the questionnaire were reported as min/day of walking, moderate, and vigorous PA. The metabolic equivalents (METs)— minutes/day and minutes/week (MET–min/day and MET–min/week, respectively)—in each PA were calculated according to the Compendium of Physical Activities [26]. Finally, according to the IPAQ protocol, the participants were divided into the following three groups: high, moderate, and low PA.
2.5. Energy Imbalance Gap
2.6. Statistical analysis
Statistical analyses were performed using IBM SPSS software (SPSS Inc., version 26; IBM Corp., Armonk, New York, NY, USA). The Kolmogorov–Smirnov test was used to verify whether the data were normally distributed. Means, 95% confidence intervals (95% CI), specific percentiles (3rd, 10th, 25th, 50th, 75th, 90th, and 97th), and percentages were computed as needed to describe the variables. Weighting was conducted according to sociodemographic characteristics, sex, SES, and country.
Multilevel linear regression models (β coefficient; 95% confidence intervals [95% CI]) were used (ensuring assumptions of linearity, independence, homoscedasticity, and normality were met) to examine the associations between sociodemographic characteristics (independent variables) with EI, EE, and EIG (dependent variable) for each country and overall. The models included regions and cities as random effects. Moreover, they were adjusted for sex, SES, education level, ethnicity, and BMI as well as reported unstandardized beta coefficients and 95% CI. A significance level of 5% was considered to be statistically significant.
3. Results
The total sample comprised 680 adolescents (mean age 16.5 ± 1.2 years). Descriptive characteristics of the participants are presented in Table 1. Overall, the proportion of males was higher than that of females, except in Venezuela. About half (53.1%) were classified as having a low SES; 82.8% had a basic or lower educational level; and 48.7% were of the Mestizo ethnicity. More than 80% of the adolescents had normal weight and height. The prevalence of low height was higher than the prevalence of overweight in this group of adolescents (7.5% vs. 6.2%, respectively).
Overall, the mean EI, EE and EIG was 2091.3 kcal, 2067.8 kcal and 23.5 kcal, respectively. For EI, Chile had the lowest values (mean 1884.6 kcal; 95% CI: 1777.9; 1991.3) and Argentina had the highest average (mean 2323.1 kcal; 95% CI: 2202.7; 2443.6). The difference between the two countries is 438.5 kcal. For EE, the highest values were in Costa Rica (mean: 2172.2 kcal; 95% CI: 2047.0; 2297.3) and the lowest was in Peru (mean: 1963.7 kcal; 95% CI: 1882.7; 2044.7). The mean difference between these two countries was 208.5 kcal. Regarding the EIG, the mean difference between Argentina (highest energy balance) and Chile (lowest energy balance) was 489.1 kcal (Table 2).
In the EI percentiles (Figure 2A), Argentina consumed the most energy and Chile had the least caloric intake (2262.4 kcal and 1930.1 kcal). By sex, all percentiles for males were higher than those for females. In addition, subjects with a high SES, underweight subjects and people with normal height consumed more energy at the 50th percentile (See online supplementary material, Supplementary Table S1).
EE (Figure 2B), in Chile was the highest, and Peru was the one with the lowest expenditure (2084.5 kcal and 1848.5 kcal, respectively). In addition, in overall countries, males spent more energy than females, as did individuals with a high SES, overweight, and normal height (Supplementary Table S2).
In the EIG (Figure 2C), Ecuador had the highest positive EIG at the 50th percentile and Chile had the highest negative EIG (144.9 kcal and -291.5 kcal, respectively). By sex, males had a negative energy balance at the percentile 50th, and females had a positive balance (-33.4 kcal and 94.0 kcal, respectively). In addition, subjects with high SES had a negative energy balance compared to the rest of the group, as did overweight subjects. In contrast, in terms of height for age, all categories had a positive EIG at the 50th percentile (Supplementary Table S3).
The associations between the correlates and the total EI, EE, and EIG are presented in Table 3. As expected, the results showed that males consume more energy than females and had a higher EE (433.0 kcal and 581.0 kcal, respectively; p<0.05), therefore they had a negative energy balance in relation to the female sex (-148.1kcal; p < 0.05). In the SES, the subjects with high SES spent more energy than those with low SES (110.1 kcal; p < 0.05). Regarding the body mass index for age, it was observed that underweight adolescents and normal-weight subjects spent less energy than overweight subjects (p < 0.05), so these two groups had a positive energy balance (+979.6 kcal and +394.1 kcal, respectively). Finally, in terms of height for age, the risk of low- and low-height subjects consumed and spent less energy than normal height subjects, but they had a positive energy balance; however, these results were not significant (p > 0.05).
4. Discussion
This study examined firstly the gaps between EI and EE and second, the associations between EIG and sociodemographic and nutritional status variables in the urban adolescent population of ELANS countries. The results showed that there was a positive energy balance in general, with EI values (2091 kcal) being higher than EE values (2068 kcal).
Growth and development have a significant impact on energy requirements, during adolescence. Adolescents typically need extra calories to fuel metabolic and physical activities, as well as to increase the amount of important body tissues such as bone, muscle, blood, and body organs [27]. A positive energy balance is necessary for growth; however, it is important for adolescents to maintain a healthy energy balance and avoid weight gain. A negative energy balance can prevent adolescents from growing properly, which is a public health concern [28].
The WHO [29] has strengthen its approach towards adolescence as a period in which rapid changes are manifested, and risks for diseases need to be addressed. According to the same source, adolescents between 10-14 years old are more at risk of experiencing diseases as a result of lack of sanitation; however, the risks associated with those between 15-19 years old are related to behaviors including diet, PA, substance misuse, and unsafe sex.
The positive EIG in most ELANS countries suggests that adolescents consume more energy than they are expending, which could lead to weight gain over time. This is especially concerning in Argentina, Colombia, and Peru, where the EIG is > 100 calories. Previous studies have found that these three countries also have a positive energy balance in their adult populations [6]. Additionally, a study of the anthropometric profiles of ELANS countries found that Argentina had the fourth highest prevalence of obesity [30].
In terms of energy expenditure, Peru had the lowest value in this study, probably because of low level of PA. Wei et al. [31] described a model that suggests that Hispanic adolescents are likely to participate in less PA than others, which gives them a higher risk of obesity. The higher EI and EE in male adolescents than in females were consistent with previous studies. Silva et al. [32] studied 459 adolescents aged 10 to 17 in Portugal and found an energy imbalance gap of -50.7 kcal in males, with both EI and EE significantly higher than in females.
Literature has consistently supported that male adolescents have a higher basal metabolic rate (BMR) and are more active than females [33,34]. Males have a greater BMR per unit of body than females because of body composition differences, including more lean body mass [33]. Additionally, males spend more time on high-intensity activities than females, who spend more time on low-intensity activities [34]. These findings suggest that biological and behavioral factors contribute to higher EI and EE in male adolescents.
The EE reported by adolescents in the present study was higher in subjects with high SES than in those with a low SES. This is likely because adolescents from higher SES families are more likely to live in neighborhoods with parks, playgrounds, and other facilities that are conducive to PA, normally have the financial resources to purchase sports equipment and transportation to sports activities [31,35], and they are more likely to receive encouragement and support from their parents and peers to be physically active [36,37]. However, studies are necessary to confirm this finding in the urban areas of Latin American context.
Regarding BMI, there was a positive EIG in underweight and normal-weight adolescents compared with overweight adolescents. This is likely due to the compensatory strategies. Underweight adolescents have the lowest EE, which is likely due to a compensatory decrease in PA and a lower BMR due to their lower body weight. It is well established that underweight can induce reductions in EE and slow down growth to favor subsequent body weight gain [38]. Lazzer et al. [39] found that obese adolescents have a higher BMR due to their high weight, and higher EE compared to non-obese subjects. They also found that obese subjects spent more time on light physical activities, such as shopping or slow walking during the weekend, but much less time on moderate and sports activities than did the non-obese subjects. This could explain the results on Chile and Costa Rica, which had the lowest EIG values, with a higher EE than EI, and with high prevalence of obesity by BMI [30]. Therefore, despite being in a negative energy balance, they do not present high levels of malnutrition in their population. Thivel et al. [40] established that obese adolescents may spontaneously decrease EI after intensive exercise, an important compensatory theory, especially for this research because overweight adolescents had an EI very similar to that of the normal weight group.
These compensatory strategies may have implications for adolescents’ health. For example, underweight as much as overweight adolescents may be at risk for nutrient deficiencies, and overweight adolescents may also be at risk for chronic diseases, such as heart disease and type 2 diabetes.
This study has some strengths, among which we can mention the 2 non-consecutive 24-hour recalls, the PA recall using the extensively validated IPAQ questionnaire, and the randomized multistage sampling. However, some limitations need to be considered. First, this study was cross-sectional; therefore, it cannot be used to establish causality. The data on EI and EE were self-reported, which may have introduced some bias for the technique used. The study was conducted in a limited number of countries; therefore, the findings may not be generalizable to all LA regions.
On the other hand, the methodology used in this study to evaluate EIG has been controversially discussed as it goes away from the direct and indirect calorimetry using a metabolic chamber and metabolic cart, respectively; and the doubly labelled water technique (41). However, these methods are costly or invasive to be performed in epidemiological studies, thus the results of this study constitute a first step to understand the balance between EI and EE in LA adolescents, and the results may constitute an input to promote public policies aimed at reducing the prevalence of obesity in urban areas of the LA region.
5. Conclusions
In conclusion, the findings of this study suggest that the sex and BMI are associated with EIG in adolescents of ELANS countries. These factors should be taken into account when developing public health policies to prevent weight gain and promote healthy weight in this age group. The findings of this study also suggest that there is a need to implement public health interventions to address the issue of EIG in adolescents in LA. These interventions should focus on promoting healthy eating and PA.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S1: Energy intake percentiles by sociodemographic variables; Table S2: Energy expenditure percentiles by sociodemographic variables; Table S3: Energy imbalance gap percentiles by sociodemographic variables.
Author Contributions
Conceptualization, P.H., M.H.C., M.C.Y.G., and L.Y.C.S.; methodology, M.H.C., M.C.Y.G., L.Y.C.S., and M.V.C.; formal analysis, G.F., and R.Y.A.; investigation and resources, I.K., G.G., R.M.R., A.R., L.Y.C.S., M.C.Y.G., R.P., M.H.C., Y.S., M.L.J., and M.F.; data curation, I.K., G.G., R.M.R., A.R., L.Y.C.S., M.C.Y.G., R.P., M.H.C., and M.F.; writing—original draft preparation, P.H., M.H.C., Y.S., M.L.Y., M.C.Y.G., L.Y.C.S., and M.V.C.; writing—review and editing, G.F., R.Y.A., G.G., R.M.R., R.P., A.R., I.K., and M.F.; visualization, P.H.; supervision, M.H.C., Y.S., M.L.J.; funding acquisition, I.K. and M.F. All authors have read and agreed to the published version of the manuscript.
Funding
The fieldwork and data analysis in ELANS protocol was supported by a scientific grant from the Coca Cola Company (ended in 2016) and by grant and/or support from Instituto Pensi/Hospital Infantil Sabara, International Life Science Institute of Argentina, Universidad de Costa Rica, Pontificia Universidad Catolica de Chile, Pontificia Universidad Javeriana, Universidad Central de Venezuela/Fundación Bengoa, Universidad San Francisco de Quito, and Instituto de Investigación Nutricional from Perú. The founders have no role in the study design, data collection, analysis, decision to publish or preparation of this manuscript.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. Ethical approval was provided by the Western Institutional Review Board (#20140605), and by the ethical review boards of the participating institutions. This study is registered at Clinical Trials #NCT02226627.
Informed Consent Statement
Written informed consent/assent was obtained from all individuals before commencement of the study.
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available due the terms of consent/assent to which the participants agreed but are available from the corresponding author on reasonable request. Please contact the corresponding author to discuss availability of data and materials.
Acknowledgments
The authors would like to thank the staff and participants from each of the participating sites who made substantial contributions to ELANS. The following are members of ELANS Study Group: Chairs: Mauro Fisberg and Irina Kovalskys; Co-chair: Georgina Gómez; Core Group members: Attilio Rigotti, Lilia Yadira Cortés, Georgina Gómez, Martha Cecilia Yépez García, Rossina Gabriela Pareja, and Marianella Herrera-Cuenca; Project Managers: Viviana Guajardo and Ioná Zalcman Zimberg; Dietary Intake Advisor: Agatha Nogueira Previdelli; Physical Activity Advisor: Gerson Ferrari. In addition, the authors would like to thank the external committee, Berthold Koletzko, Luis A. Moreno, and Miichael Pratt.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- UNFPA, WHO. Technical guidance for prioritizing adolescent health. UNFPA: New York City, United States; 2017. Available online: https://www.unfpa.org/sites/default/files/pub-pdf/UNFPA_EWEC_Report_EN_WEB.
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet. 2017; 390(10113): 2627-2642. [CrossRef]
- Bernabe-Ortiz A, Carrillo-Larco RM. Physical activity patterns among adolescents in latin america and the caribbean region. J Phys Act Health. 2022; 19(9): 607-614. [CrossRef]
- Ludwig D.S., Aronne L.J., Astrup A., de Cabo R., Cantley L.C., Friedman M.I., Heymsfield S.B., Johnson J.D., King J.C., Krauss R.M., Lieberman D.E., Taubes G., Volek J.S., Westman E.C., Willett W.C., Yancy W.S., Ebbeling C.B. The carbohydrate-insulin model: a physiological perspective on the obesity pandemic. Am J Clin Nutr. 2021; 114(6):1873-1885. [CrossRef]
- Fallah-Fini S., Vandevijvere S., Rezaei T., Heke I., Swinburn B. Three Decades of New Zealand Adults Obesity Trends: An Estimation of Energy Imbalance Gaps Using System Dynamics Modeling. Obesity (Silver Spring). 2019; 27(7): 1141-1149. [CrossRef]
- Yépez García M.C., Herrera-Cuenca M., Ferrari G., Sanabria L.Y.C., Hernández P., Almeida R.Y., Villar Cáceres M., Gómez G., Pareja R., Rigotti A., Kovalskys I., Fisberg M. Energy Imbalance Gap, Anthropometric Measures, Lifestyle, and Sociodemographic Correlates in Latin American Adults-Results from the ELANS Study. Int J Environ Res Public Health. 2022; 19(3): 1129. [CrossRef]
- Geary N. Energy homeostasis from Lavoisier to control theory. Phil. Trans. R. Soc. B. 2023; 378: 20220201. [CrossRef]
- U.S. Department of Agriculture and U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 2020-2025. 9th Edition. December 2020. Available online: https://DietaryGuidelines.gov.
- Lau D.C., Douketis J.D., Morrison K.M., Hramiak I.M., Sharma A.M., Ur E. Obesity Canada Clinical Practice Guidelines Expert Panel. 2006 Canadian clinical practice guidelines on the management and prevention of obesity in adults and children [summary]. CMAJ. 2007;176(8): S1-13. [CrossRef]
- Hall K.D., Farooqi I.S., Friedman J.M., Klein S., Loos R.J.F., Mangelsdorf D.J., O'Rahilly S., Ravussin E., Redman L.M., Ryan D.H., Speakman J.R., Tobias D.K. The energy balance model of obesity: beyond calories in, calories out. Am J Clin Nutr. 2022; 115(5): 1243-1254. [CrossRef]
- Swinburn B.A., Sacks G., Hall K.D., McPherson K., Finegood D.T., Moodie M.L., Gortmaker S.L. The global obesity pandemic: shaped by global drivers and local environments. Lancet. 2011 Aug 27;378(9793):804-14. [CrossRef]
- Satija A., Yu E., Willett W.C., Hu F.B. Objective measures are complementary to, rather than a replacement for, self-reported methods. Int. J. Obes. 2015; 39: 1179. [CrossRef]
- Fallah-Fini S., Ikeda N., Nishi N. Trends in Energy Imbalance Gap and Body Weight Status in the Japanese Adult Population: A System Dynamics Approach. J Epidemiol. 2021; 31(5): 335-342. [CrossRef]
- Fallah-Fini S., Rezaei T., Ridder K., Vandevijvere S. Trends in adults’ energy imbalance gaps over two decades in Belgium using system dynamics modelling. BMC Nutr. 2023; 9(1): 66. [CrossRef]
- Daniels S.R., Arnett D.K., Eckel R.H., Gidding S.S., Hayman L.L., Kumanyika S., Robinson T.N., Scott B.J., St Jeor S., Williams C.L. Overweight in children and adolescents: pathophysiology, consequences, prevention, and treatment. Circulation. 2005; 111(15): 1999-2012. [CrossRef]
- La Marra M., Messina A., Ilardi C.R., Staiano M., Di Maio G., Messina G., Polito R., Valenzano A., Cibelli G., Monda V., Chieffi S., Iavarone A., Villano I. Factorial Model of Obese Adolescents: The Role of Body Image Concerns and Selective Depersonalization-A Pilot Study. Int J Environ Res Public Health. 2022; 19(18): 11501. [CrossRef]
- Martins V.J., Toledo Florêncio T.M., Grillo L.P., do Carmo P. Franco M, Martins P.A., Clemente A.P., Santos C.D., de Fatima A. Vieira M, Sawaya A.L. Long-lasting effects of undernutrition. Int J Environ Res Public Health. 2011; 8(6): 1817-46. [CrossRef]
- Fisberg M., Kovalskys I., Gómez G., Rigotti A., Cortés L.Y., Herrera-Cuenca M., Yépez M.C., Pareja R.G., Guajardo V., et al. Latin American Study of Nutrition and Health (ELANS): Rationale and study design. BMC Public Health. 2015; 16: 93. [CrossRef]
- Kovalskys I., Fisberg M., Gómez G., Rigotti A., Cortés L.Y., Yépez M.C., Pareja R.G., Herrera-Cuenca M., Zimberg I.Z., Tucker K.L., Koletzko B., Pratt M, ELANS Study Group. Standardization of the Food Composition Database Used in the Latin American Nutrition and Health Study (ELANS). Nutrients. 2015 Sep 16;7(9):7914-24. [CrossRef]
- WHO Multicenter Growth Reference Study, de Onis M. WHO Child Growth Standards based on length/height, weight and age. Acta Pædiatrica. 2006; 95: 76-85.
- Moshfegh A.J., Rhodes D.G., Baer D.J., et al. The US Department of Agriculture Automated Multiple-Pass Method reduces bias in the collection of energy intakes. Am J Clin Nutr. 2008; 88: 324–332. [CrossRef]
- Haubrock J., Nothlings U., Volatier J.L., et al. Estimating usual food intake distributions by using the multiple source method in the EPIC-Potsdam Calibration Study. J Nutr 2011; 141(5): 914-20. [CrossRef]
- FAO. Human Energy Requirements. FAO; Rome: 2001.
- Gerrior S., Juan W., Peter B. An Easy Approach to Calculating Estimated Energy Requirements. Prev. Chronic Dis. 2006;3:A129.
- Hallal P., Gómez L., Parra D., Lobelo F., Mosquera J., Florindo A. Lecciones aprendidas después de 10 Años del uso de IPAQ en Brasil y Colombia. J. Phys. Act. Health. 2010;7:259–264. [CrossRef]
- Ainsworth B.E., Haskell W.L., Whitt M.C., Irwin M.L., Swartz A.M., Strath S.J., O’Brien W.L., Bassett D.R., Jr., Schmitz K.H., Emplaincourt P.O., et al. Compendium of Physical Activities: An update of activity codes and MET intensities. Med. Sci. Sports Exerc. 2000;32:S498–S516. [CrossRef]
- Savarino G., Corsello A., Corsello G. Macronutrient balance and micronutrient amounts through growth and development. Ital J Pediatr. 2021; 47(1): 109. [CrossRef]
- Areta J.L. Physical performance during energy deficiency in humans: An evolutionary perspective. Comp Biochem Physiol A Mol Integr Physiol. 2023; 284:111473. [CrossRef]
- World Health Organization (WHO). Adolescent health. Available online: https://www.who.int/health-topics/adolescent-health.
- Herrera-Cuenca M., Kovalskys I., Gerardi A., Hernandez P., Sifontes Y., Gómez G., Yépez García M.C., Méndez-Pérez B., Landaeta-Jimenez M., Pareja R., Cortés L.Y., Rigotti A., Fisberg M., Zimberg I.Z. Anthropometric Profile of Latin American Population: Results From the ELANS Study. Front Nutr. 2021 Nov 8;8:740361. [CrossRef]
- Wei Y.D., Xiao W., Garcia I. Neighborhood environment, active commute, and healthy BMI in adolescents. Sustainability. 2021; 13(15): 8286. [CrossRef]
- Silva A.L., Teles J., Olivares L.F., Fragoso I. Energy intake and expenditure in children and adolescents, contributions of biological maturity. Am J Hum Biol. 2021; 33(6): e23529. [CrossRef]
- Wu B.N., O'Sullivan A.J. Sex differences in energy metabolism need to be considered with lifestyle modifications in humans. J Nutr Metab. 2011; 2011:391809. [CrossRef]
- Schwarzfischer P., Weber M., Gruszfeld D., Socha P., Luque V., Escribano J., Xhonneux A., Verduci E., Mariani B., Koletzko B., et al. BMI and recommended levels of physical activity in school children. BMC Public Health. 2017; 17:595. [CrossRef]
- Ke Y., Shi L., Peng L., Chen S., Hong J., Liu Y. Associations between socioeconomic status and physical activity: A cross-sectional analysis of Chinese children and adolescents. Front Psychol. 2022; 13: 904506. [CrossRef]
- Qiu N., Gao X., Zhang X., Fu J., Wang Y., Li R. Associations between psychosocial variables, availability of physical Activity resources in neighborhood environment, and out-of-school physical Activity among Chinese adolescents. Int. J. Environ. Res. Public Health. 2021; 18:6643. [CrossRef]
- Stalsberg R., Pedersen A.V. Effects of socioeconomic status on the physical activity in adolescents: a systematic review of the evidence. Scand J Med Sci Sports. 2010; 20(3): 368-83. [CrossRef]
- Lazzer S., O’Malley G., M.V. Frelut M.L., editor. Metabolic And Mechanical Cost Of Sedentary And Physical Activities In Obese Children And Adolescents. The ECOG’s eBook on Child and Adolescent Obesity. 2015. Available online: https://ebook.ecog-obesity.eu.
- Lazzer S., Boirie Y., Bitar A., Montaurier C., Vernet J., Meyer M., Vermorel M. Assessment of energy expenditure associated with physical activities in free-living obese and nonobese adolescents. Am J Clin Nutr. 2003; 78(3): 471-9. [CrossRef]
- Thivel D., Aucouturier J., Doucet É., Saunders T.J., Chaput J.P. Daily energy balance in children and adolescents. Does energy expenditure predict subsequent energy intake? Appetite. 2013; 60(1):58-64. [CrossRef]
- Dhurandhar N.V., Schoeller D., Brown A.W., Heymsfield S.B., Thomas D., Sørensen T.I., Speakman J.R., Jeansonne M., Allison D.B.; Energy Balance Measurement Working Group. Energy balance measurement: when something is not better than nothing. Int J Obes (Lond). 2015; 39(7): 1109-13. [CrossRef]
Figure 1.
Flow chart of selection of adolescent participants.
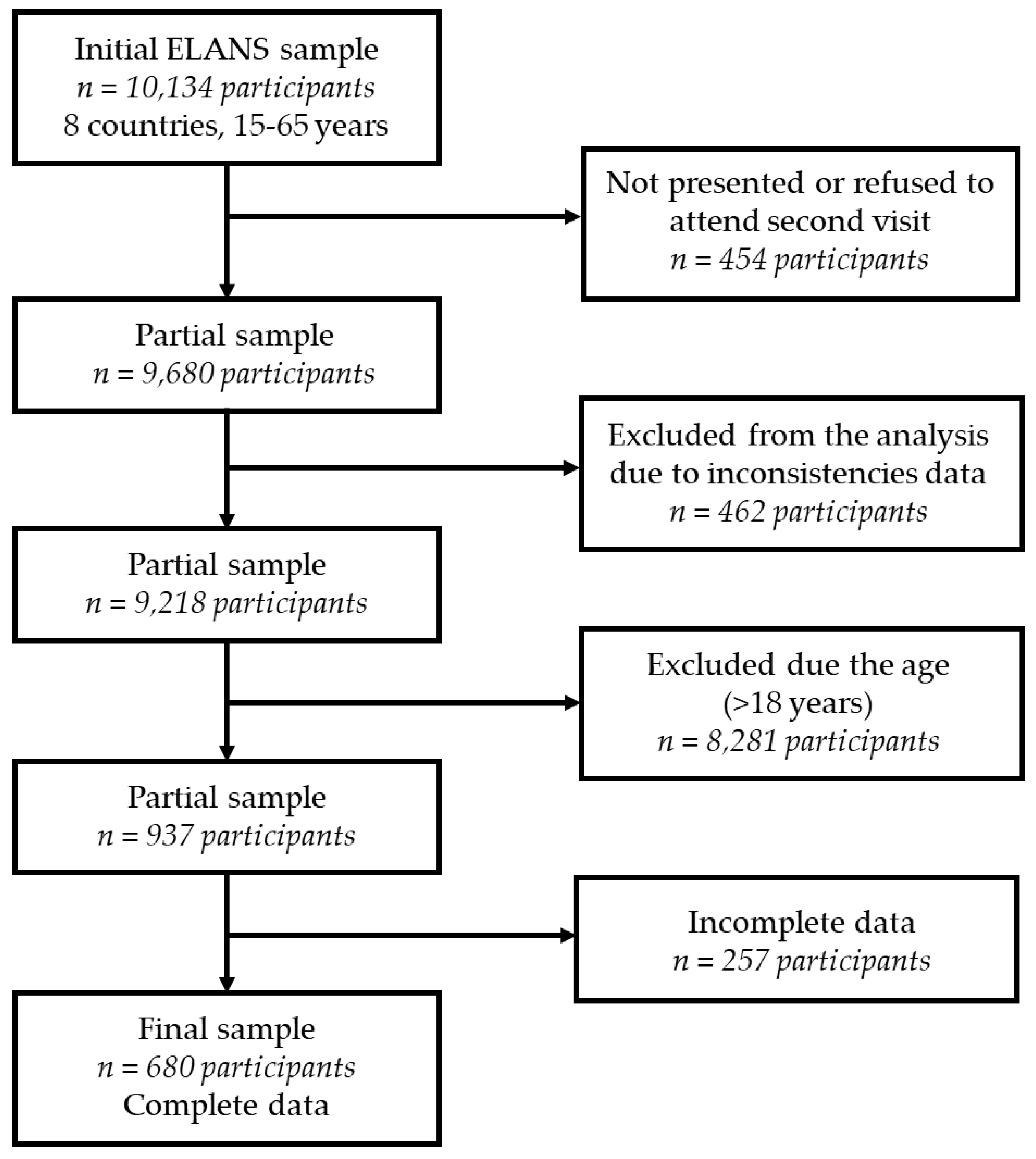
Figure 2.
Bloxplot of energy intake (A), energy expenditure (B), and energy imbalance gap (C) values by country. In the figure, the median is represented by the vertical line between the colors in the box. The part of the box above the median is shown in blue, and the part of the box below the median is shown in green.
Figure 2.
Bloxplot of energy intake (A), energy expenditure (B), and energy imbalance gap (C) values by country. In the figure, the median is represented by the vertical line between the colors in the box. The part of the box above the median is shown in blue, and the part of the box below the median is shown in green.
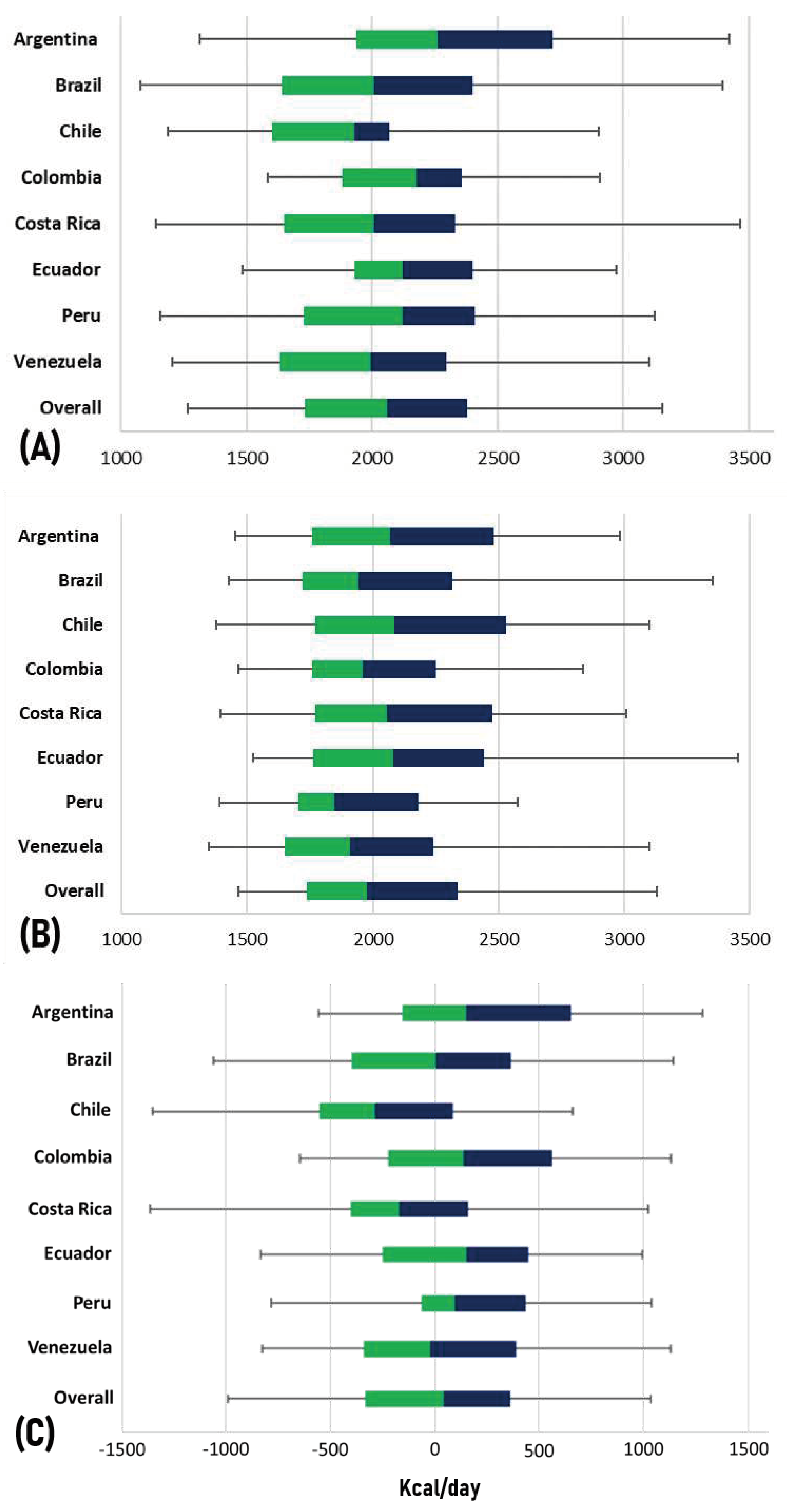

Table 1.
Distribution of adolescents according to sociodemographic variables by country.
| Variables | Argentina | Brazil | Chile | Colombia | Costa Rica | Ecuador | Peru | Venezuela | Overall |
| n (%) | 87 (12.8) | 123 (18.1) | 64 (9.4) | 73 (10.7) | 69 (10.2) | 73 (10.7) | 97 (14.3) | 94 (13.8) | 680 (100.0) |
| Sex | |||||||||
| Male | 57 (65.5) | 76 (61.8) | 35 (54.7) | 43 (58.9) | 42 (60.9) | 41 (56.2) | 51 (52.6) | 45 (47.9) | 390 (57.4) |
| Female | 30 (34.5) | 47 (38.2) | 29 (45.3) | 30 (41.1) | 27 (39.1) | 32 (43.8) | 46 (47.4) | 49 (52.1) | 290 (42.6) |
| Socio-economic status | |||||||||
| Low | 55 (63.2) | 48 (39.0) | 25 (39.1) | 49 (67.1) | 23 (33.3) | 34 (46.6) | 50 (51.5) | 77 (81.9) | 361 (53.1) |
| Middle | 29 (33.3) | 64 (52.0) | 32 (50.0) | 19 (26.0) | 38 (55.1) | 32 (43.8) | 31 (32.0) | 13 (13.8) | 258 (37.9) |
| High | 3 (3.4) | 11 (8.9) | 7 (10.9) | 5 (6.8) | 8 (11.6) | 7 (9.6) | 16 (16.5) | 4 (4.3) | 61 (9.0) |
| Educational level | |||||||||
| Basic | 83 (95.4) | 99 (80.5) | 60 (93.8) | 56 (76.7) | 65 (94.2) | 71 (97.3) | 52 (53.6) | 77 (81.9) | 563 (82.8) |
| High school | 3 (3.4) | 24 (19.5) | 3 (4.7) | 15 (20.5) | 4 (5.8) | 2 (2.7) | 44 (45.4) | 3 (3.2) | 98 (14.4) |
| Undergraduate | 1 (1.1) | 0 (0.0) | 1 (1.6) | 2 (2.7) | 0 (0.0) | 0 (0.0) | 1 (1.0) | 14 (14.9) | 19 (2.8) |
| Ethnicity | |||||||||
| Caucasian | 59 (67.8) | 49 (39.8) | 24 (37.5) | 25 (34.2) | 36 (52.2) | 4 (5.5) | 7 (7.2) | 30 (31.9) | 234 (34.4) |
| Mestizo | 16 (18.4) | 22 (17.9) | 31 (48.4) | 38 (52.1) | 19 (27.5) | 65 (89.0) | 85 (87.6) | 55 (58.5) | 331 (48.7) |
| Afro-American | 1 (1.1) | 23 (18.7) | 0 (0.0) | 2 (2.7) | 0 (0.0) | 3 (4.1) | 1 (1.0) | 2 (2.1) | 32 (4.7) |
| Indigenous | 0 (0.0) | 4 (3.3) | 2 (3.1) | 2 (2.7) | 1 (1.4) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 9 (1.3) |
| Others | 11 (12.6) | 25 (20.3) | 7 (10.9) | 6 (8.2) | 13 (18.8) | 1 (1.4) | 4 (4.1) | 7 (7.4) | 74 (10.9) |
| Body mass index for age | |||||||||
| Underweight | 2 (2.3) | 5 (4.1) | 0 (0.0) | 1 (1.4) | 0 (0.0) | 2 (2.7) | 1 (1.0) | 1 (1.1) | 12 (1.8) |
| Normal weight | 80 (92.0) | 111 (90.2) | 59 (92.2) | 68 (93.2) | 62 (89.9) | 69 (94.5) | 89 (91.8) | 88 (93.6) | 626 (92.1) |
| Overweight | 5 (5.7) | 7 (5.7) | 5 (7.8) | 4 (5.5) | 7 (10.1) | 2 (2.7) | 7 (7.2) | 5 (5.3) | 42 (6.2) |
| Height for age | |||||||||
| Low | 5 (5.7) | 6 (4.9) | 0 (0.0) | 9 (12.3) | 3 (4.3) | 7 (9.6) | 13 (13.4) | 8 (8.5) | 51 (7.5) |
| Risk of low height | 5 (5.7) | 9 (7.3) | 8 (12.5) | 6 (8.2) | 11 (15.9) | 7 (9.6) | 15 (15.5) | 7 (7.4) | 68 (10.0) |
| Normal | 77 (88.5) | 108 (87.8) | 56 (87.5) | 58 (79.5) | 55 (79.7) | 59 (80.8) | 69 (71.1) | 79 (84.0) | 561 (82.5) |
Table 2.
Energy intake, energy expenditure and energy imbalance gap by sociodemographic characteristics.
Table 2.
Energy intake, energy expenditure and energy imbalance gap by sociodemographic characteristics.
| Variables | n (%) | Mean (95% CI) of EI (kcal/day) | Mean (95% CI) of EE (kcal/day) | Mean (95% CI) of EIG (kcal/day) |
|---|---|---|---|---|
| Overall | 680 (100.0) | 2091.3 (2054.0;2128.6) | 2067.8 (2033.6;2102.1) | 23.5 (-16.9;63.8) |
| Country | ||||
| Argentina | 87 (12.8) | 2323.1 (2202.7;2443.6) | 2116.9 (2026.1;2207.8) | 206.2 (91.9;320.5) |
| Brazil | 123 (18.1) | 2046.1 (1944.1;2148.1) | 2070.6 (1982.6;2158.6) | -24.5 (-129.9;80.9) |
| Chile | 64 (9.4) | 1884.6 (1777.9;1991.3) | 2167.5 (2053.6;2281.4) | -282.9 (-408.8;-156.9) |
| Colombia | 73 (10.7) | 2190.9 (2085.9;2296.0) | 2020.5 (1927.2;2113.7) | 170.5 (59.4;281.5) |
| Costa Rica | 69 (10.1) | 2003.8 (1895.3;2112.3) | 2172.2 (2047.0;2297.3) | -168.4 (-299.7;-37.0) |
| Ecuador | 73 (10.7) | 2177.0 (2081.0;2273.0) | 2103.1 (2010.3;2195.9) | 74.0 (-33.4;181.3) |
| Peru | 97 (14.3) | 2087.1 (2002.1;2172.1) | 1963.7 (1882.7;2044.7) | 123.4 (30.3;216.5) |
| Venezuela | 94 (13.8) | 2001.2 (1906.2;2096.1) | 1991.2 (1892.3;2090.1) | 10.0 (-96.3;116.2) |
| Sex | ||||
| Male | 390 (57.4) | 2276.2 (2228.3;2324.0) | 2311.3 (2268.8;2353.7) | -35.1 (-93.7;23.5) |
| Female | 290 (42.6) | 1842.7 (1796.7;1888.6) | 1740.4 (1713.6;1767.3) | 102.2 (50.7;153.7) |
| Socio-economic status | ||||
| Low | 361 (53.1) | 2102.6 (2051.0;2154.1) | 2047.3 (2003.2;2091.5) | 55.2 (0.3;110.1) |
| Middle | 258 (37.9) | 2067.9 (2007.0;2128.8) | 2073.7 (2015.6;2131.8) | -5.8 (-72.1;60.5) |
| High | 61 (9.0) | 2123.5 (2000.4;2246.5) | 2164.2 (2030.5;2297.9) | -40.8 (-180.7;99.2) |
| Education level | ||||
| Basic | 563 (82.8) | 2113.7 (2071.9;2155.5) | 2084.8 (2047.3;2122.3) | 28.9 (-16.2;74.1) |
| High school | 98 (14.4) | 1966.9 (1880.0;2053.7) | 1946.5 (1867.3;2025.6) | 20.4 (-71.1;111.9) |
| Undergraduate | 19 (2.8) | 2069.2 (1855.8;2282.5) | 2191.3 (1867.9;2514.7) | -122.1 (-428.8;184.6) |
| Ethnicity | ||||
| Caucasian | 234 (34.4) | 2092.6 (2028.8;2156.3) | 2127.3 (2060.9;2193.6) | -34.7 (-107.7;38.3) |
| Mestizo | 331 (48.7) | 2085.2 (2033.3;2137.1) | 2018.2 (1975.1;2061.3) | 67.0 (12.6;121.4) |
| Afro-American | 32 (4.7) | 2078.8 (1848.4;2309.1) | 2009.1 (1856.2;2162.0) | 69.7 (-156.4;295.8) |
| Indigenous | 9 (1.3) | 2006.9 (1808.8;2204.9) | 2163.8 (1840.8;2486.7) | -156.9 (-392.5;78.7) |
| Others | 74 (10.9) | 2130.1 (2008.3;2251.9) | 2115.5 (2003.2;2227.9) | 14.6 (-112.4;141.6) |
| Body mass index for age | ||||
| Underweight | 12 (1.8) | 2233.5 (1949.6;2517.5) | 1887.3 (1736.0;2038.6) | 346.2 (70.2;622.2) |
| Normal weight | 626 (92.1) | 2086.7 (2048.2;2125.3) | 2044.2 (2011.6;2076.7) | 42.5 (2.7;82.4) |
| Overweight | 42 (6.2) | 2119.0 (1940.2;2297.8) | 2472.1 (2231.4;2712.9) | -353.1 (-595.5;-110.7) |
| Height for age | ||||
| Low | 51 (7.5) | 2029.0 (1900.0;2157.9) | 1921.8 (1835.2;2008.4) | 107.2 (-10.5;224.8) |
| Risk of low height | 68 (10.0) | 2041.3 (1921.6;2160.9) | 2000.0 (1891.9;2108.1) | 41.3 (-84.7;167.3) |
| Normal | 561 (82.5) | 2103.0 (2061.6;2144.4) | 2089.3 (2050.8;2127.8) | 13.7 (-31.7;59.1) |
95% CI: confidence interval 95%; EI: energy intake; EE: energy expenditure; EIG: energy imbalance gap.
Table 3.
Adjusted analyses (β coefficient (95% CI)) between independent variables and energy intake, energy expenditure and energy imbalance gap.
Table 3.
Adjusted analyses (β coefficient (95% CI)) between independent variables and energy intake, energy expenditure and energy imbalance gap.
| Independent variables | Energy Intake | Energy Expenditure | Energy Imbalance Gap |
|---|---|---|---|
| Sex | |||
| Female¹ | Ref. | Ref. | Ref. |
| Male | 433.0 (364.6; 501.4) | 581.0 (529.8; 632.3) | -148.1 (-227.7; -68.4) |
| Socioeconomic status | |||
| Low² | Ref. | Ref. | Ref. |
| Middle | -31.5 (-104.3; 41.3) | 16.5 (-37.1; 70.2) | -48.0 (-132.2; 36.1) |
| High | 20.1 (-104.0; 144.2) | 110.1 (22.4; 197.8) | -90.0 (-230.3; 50.3) |
| Body mass index for age | |||
| Overweight³ | Ref. | Ref. | Ref. |
| Normal weight | -40.4 (-180.7; 100.0) | -434.5 (-539.6; -329.3) | 394.1 (230.4; 557.8) |
| Underweight | -50.1 (-419.9; 319.7) | -1029.7 (-1319.0; -740.5) | 979.6 (518.6; 1440.6) |
| Height for age | |||
| Normal⁴ | Ref. | Ref. | Ref. |
| Risk of low height | -22.9 (-136.1; 90.3) | -40.9 (-125.6; 43.8) | 18.0 (-115.3; 151.3) |
| Low | -41.1 (-171.1; 88.9) | -95.4 (-192.4; 1.6) | 54.3 (-97.2; 205.7) |
Adjusted for 1 sex, 2 socio-economic status, 3 body mass index, and 4 Height.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



