Submitted:
16 November 2023
Posted:
17 November 2023
You are already at the latest version
Abstract
Acute myocardial infarction (AMI), which is characterized by severe and fatal arrhythmias resultant from cardiac ischemia/reperfusion (CIR), is the leading cause of morbidity and mortality in the world. Considering that epiisopiloturin (EPI), an imidazole alkaloid found in the leaves of Pilocarpus microphyllus produded anti-inflammatory and antioxidant effects in an animal model of peritonitis, paw edema and peritonitis in mice, we decided to investigate the potential cardioprotective activity of EPI in animal model of CIR. Then, adult rats submitted to CIR pretreated with EPI 10 mg/kg (EPI10+CIR group) or 15 mg/kg (EPI15+CIR group) were compared to control animals submitted to CIR treated with saline solution 0.9% (CIR group). To evaluate the incidence of ventricular arrhythmias (VA), atrioventricular block (AVB) and lethality (LET) induced by CIR in these rats, the ECG analysis was performed. Serum levels of cardiac damage markers, total creatine kinase (CK) and CK-MB, were measured. The results showed that the AVB incidence was reduced from 80% to 30%, and LET incidence was reduced from 70% to 20%, compared to CIR group. Serum levels of LDH, total CK and, CK-MB was similar in all groups studied. These results indicate that the treatment with EPI (15 mg/kg, IV) before CIR was effective to produce cardioprotective effects. Thus, the use of EPI could be a promisse strategy to reduce the incidence of severe and fatal arrhythmias associated with AMI.
Keywords:
Cardiac Diseases
; Cardiac Ischemia-Reperfusion
; Myocardial Infarction
; Pharmacological Cardioprotection
; Epiisopiloloturine
1. Introduction
Cardiovascular diseases (CVD) will account for more than 26 million annual deaths worldwide by 2023, making them the leading cause of death in both industrialized and underdeveloped countries. Among these illnesses, coronary artery disease (CAD) and acute myocardial infarction (AMI) in particular are the leading causes of morbidity and mortality globally [1,2,3]. One of the potentially fatal coronary-related illnesses closely linked to sudden cardiac death, which affects around three million individuals worldwide each year [4,5], is AMI. The main cause of irreversible myocardial damage in AMI is oxygen deprivation in cardiac cells, which can impair diastolic and systolic function and put the patient at risk for severe and deadly cardiac arrhythmias [4,5,6]. Even though AMI can cause several major issues for cardiac function, there are presently limited pharmacological options available for its therapy.
The fastest possible coronary blood flow restoration following ischemia (reperfusion) is essential for treating AMI [4,5,6,7]. The prognosis improves with earlier treatment (less than 6 hours from the onset of symptoms). Reperfusion of the myocardium submitted to ischemia is the primary form of AMI treatment, but this process can result in severe cardiac dysfunctions, primarily because of abrupt oxygen entry and severe ionic deregulation in cardiac cells caused by cardiac ischemia and reperfusion (CIR) process. These dysfunctions can then cause lethal cardiac arrhythmias that are directly related to deregulation of intracellular Ca2+ homeostasis in cardiac cells [6,7,8,9,10,11,12].
In order to evaluate potential cardioprotective substances, we decided to study one of the most significant genera in Brazilian flora is Pilocarpus, sometimes called "jaborandi," which has native species in the northeast and north of the nation. Because it contains significant amounts of the imidazole alkaloid pilocarpine, which is used to treat glaucoma, stimulate the lachrymal and sweat glands, and manage xerostomia, Pilocarpus microphyllus Stapf (Rutaceae) is the most well-known representative of the jaborandi group economically Pilocarpus microphyllus has been used to identify pilocarpine as well as additional imidazole alkaloids including isopilosine, epiisopilosine, and epiisopiloturine (EPI) [13,14,15,16,17]. Important published studies have demonstrated that EPI has several pharmacological actions, among which we highlight the antiparasitic, anti-inflammatory and antioxidant effects [18,19,10,21,22,23,24]
In fact, nothing is known about the pharmacological activities of the epiisopiloturine on the cardiovascular system, which is why we decided to evaluate the potential cardioprotective and antiarrhythmic activity of EPI, in the present study we used a classical animal model of CIR to evaluate the effects of treatment with EPI on the incidence of arrhythmias (VA and AVB) and lethality (LET), as well as serum concentrations of cardiac injury biomarkers lactate dehydrogenase (LDH), creatine kinase (CK), and CK-MB in rats submitted to CIR.
2. Results
2.1. Incidence of VA, AVB and LET induced by CIR
Before CIR protocol (stabilization periods for 15 min), no cardiac arrhythmias were detected in all animals studied. But, during CIR protocol, VA and AVB incidence in different experimental groups was detected and measured. Figure 1 shows that the VA, AVB and LET incidence in CIR group was 90%, 70%, and 70%, respectively.
2.2. Effects of the EPI on the incidence of VA, AVB and LET induced by CIR
Figure 1 shows that the VA, AVB and LET incidence in EPI10+CIR group was not different of CIR group, indicating that the pretreatment with EPI 10 mg/kg (IV) did not reduce the VA, AVB and LET incidence induced by CIR. However, these incidences were significantly reduced in EPI15+CIR group compared to CIR group, indicating that the pretreatment with EPI 15 mg/kg (IV) was effective to reduce cardiac arrhythmia (VA and AVB) and LET. In EPI15+CIR group, the AVB incidence was reduced from 80% to 30%, and LET incidence was reduced from 70% to 20%, compared to CIR group (See figure 1).
2.3. Effects of the EPI on the biomarker’s levels of cardiac injury total creatine kinase and CK-M in animals submitted to CIR
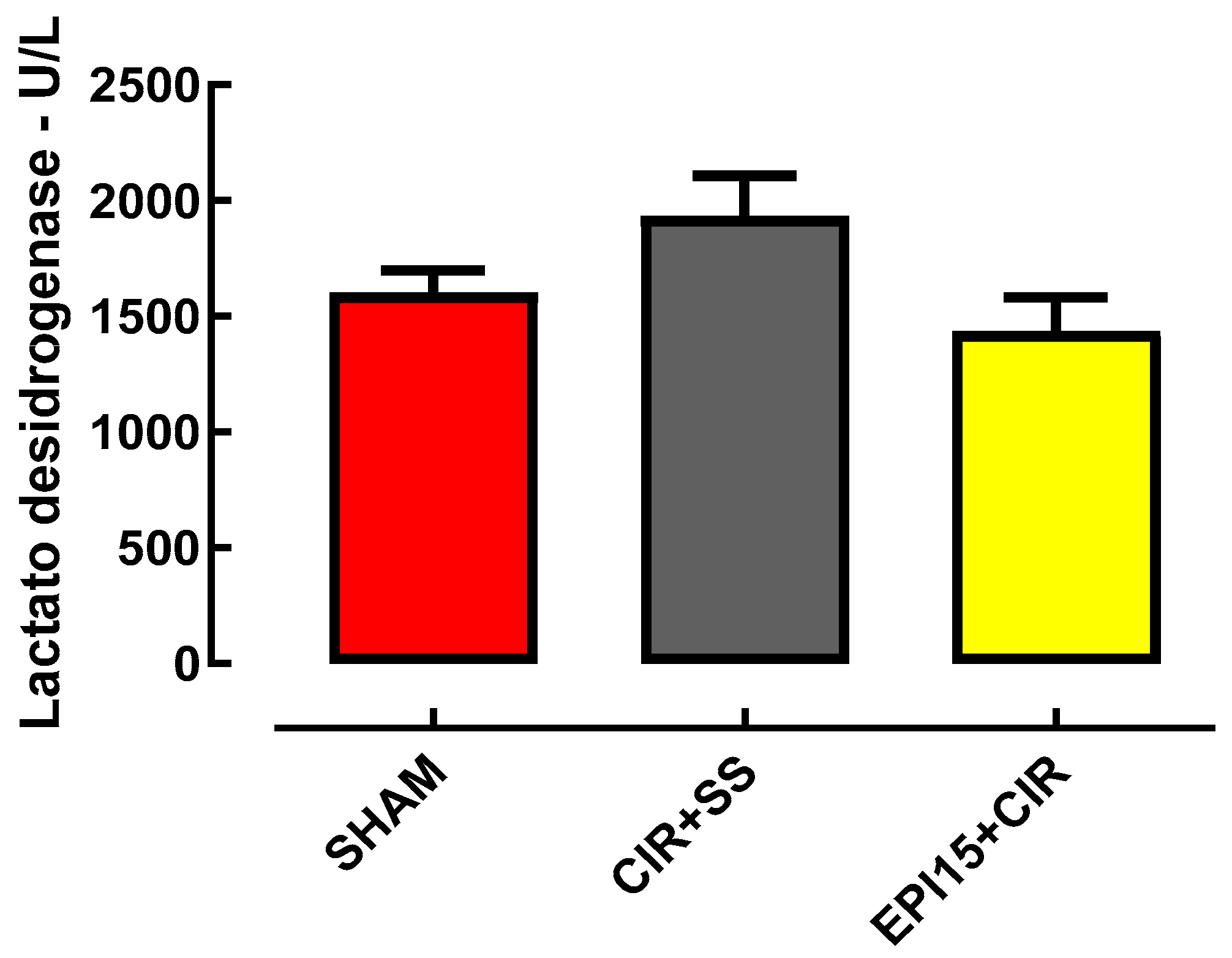
The increase in serum levels of lactate dehydrogenase (LDH) does not exclusively refer to the occurrence of AMI, but has been used as one of the biochemical markers whose increase in serum levels may be related to AMI, in 92-95% of patients, for Therefore, we decided to measure serum LDH concentrations. In NWR animals, in the SHAM group the plasma LDH concentration was (1600 ± 97 U/L), in the CIR+SS group the plasma LDH concentration was (1930 ± 176 U/L) and in the EPI group 15 mg/kg plasma LDH concentration was (1435 ± 146 U/L) (Figure 2).
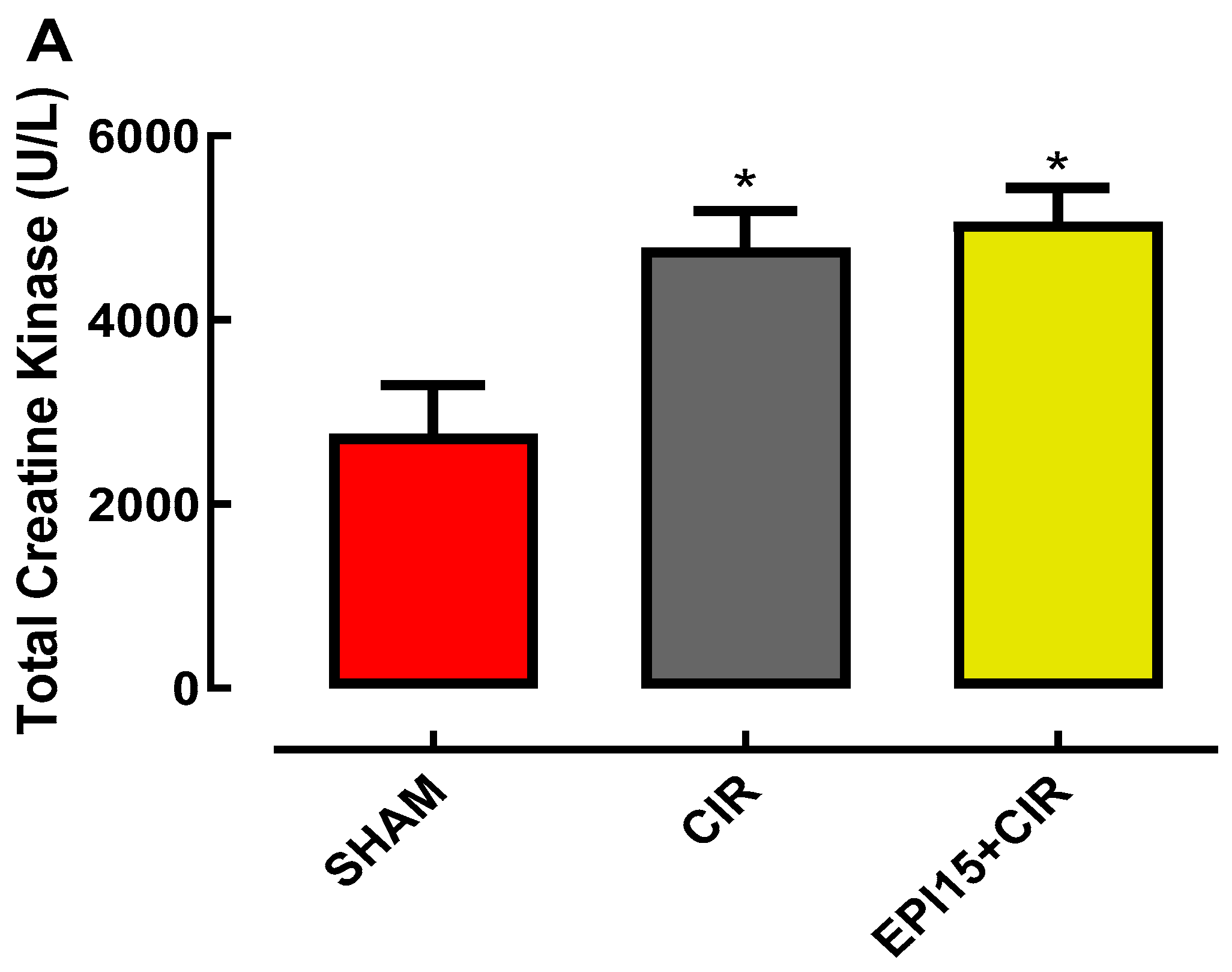
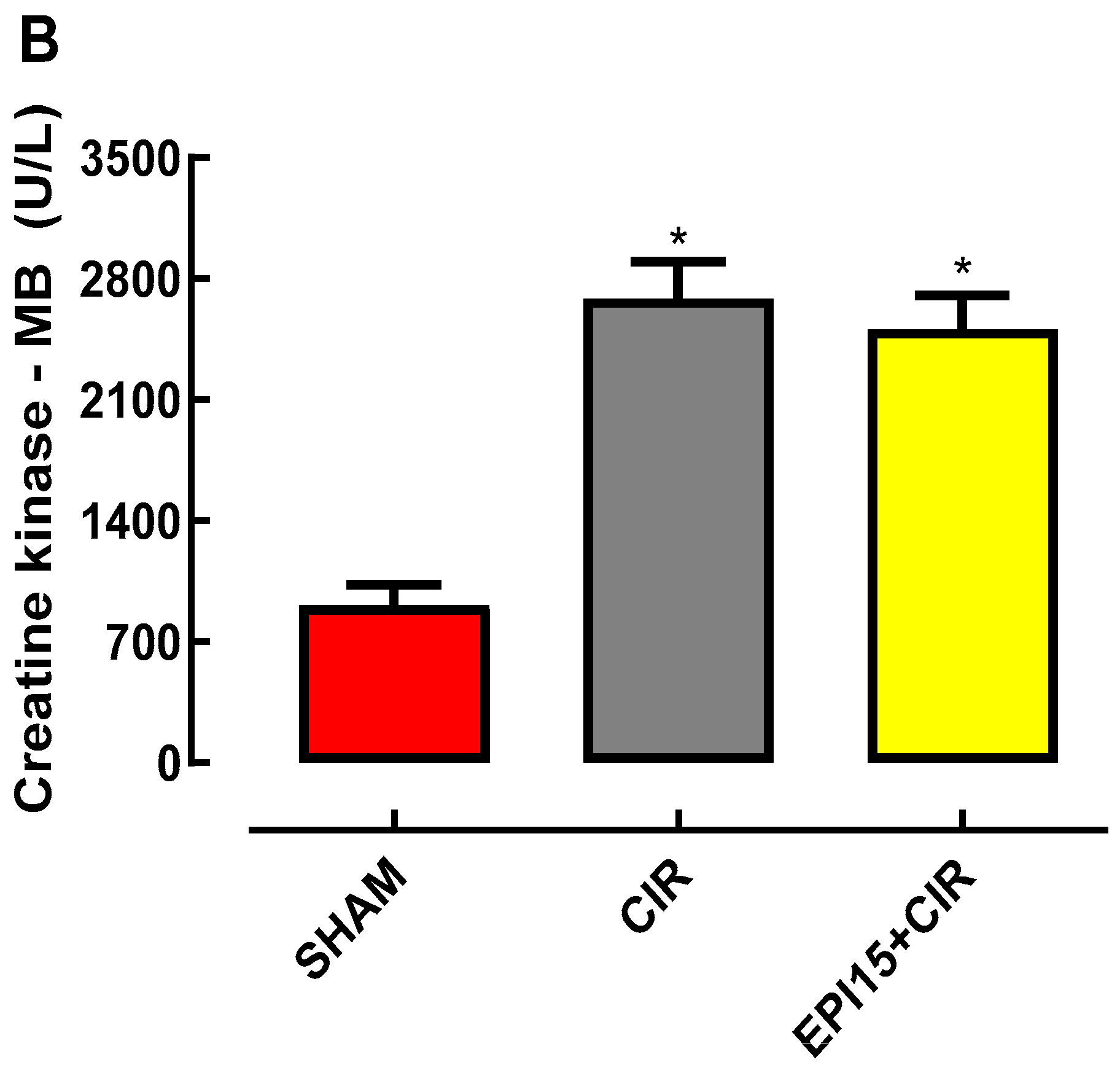
The increase in plasma concentrations of the enzyme total creatine kinase (TCK) has been used as an indicator of cardiac injury, observed in patients with AMI, which is why we decided to evaluate serum levels in NWR animals subjected to our experimental model. In NWR animals, the plasma concentration of CKT in the SHAM group (2,757 ± 532 U/L), in the CIR group (4,815 ± 431 U/L) and in the EPI 15 mg/kg (EPI15+CIR) group (5,063 ± 375 U/L) (Figure 2A). In Figure 2B, we can observe that the serum concentrations of CK-MB in the CIR (2,688 ± 210 U/L, n = 4) and EPI15+CIR (2,511 ± 193 mg/dL, n = 4) groups did not differ statistically from each other, however, the serum CK-MB concentrations of these two groups were statistically higher when compared to the SHAM group (914 ± 118 U/L, n = 4).
Figure 3.
Histograms representing the serum concentrations of Total Creatine Kinase (A) and Creatine Kinase -MB (B) in the SHAM, CIR, and EPI15+CIR groups. The results were expressed as mean ± standard error of the mean and analysis of variance (ANOVA) was applied, followed by Tukey’s post-test (*p<0.05). SHAM= sham-operated group; CIR= group treated with saline and subjected to cardiac ischemia and reperfusion; EPI 15mg/kg = group treated with epiisopiloturine and then subjected to cardiac ischemia and reperfusion. *p < 0.05 statistically different when compared to the SHAM group.
Figure 3.
Histograms representing the serum concentrations of Total Creatine Kinase (A) and Creatine Kinase -MB (B) in the SHAM, CIR, and EPI15+CIR groups. The results were expressed as mean ± standard error of the mean and analysis of variance (ANOVA) was applied, followed by Tukey’s post-test (*p<0.05). SHAM= sham-operated group; CIR= group treated with saline and subjected to cardiac ischemia and reperfusion; EPI 15mg/kg = group treated with epiisopiloturine and then subjected to cardiac ischemia and reperfusion. *p < 0.05 statistically different when compared to the SHAM group.
3. Discussion
In the present work, we showed that pretreatment of animals submitted to CIR with EPI 15 mg/kg (IV) was able to reduce the AVB incidence due to important antiarrhythmic effect, and then reducing the LET incidence (see figure 1). It is worth highlighting that this is the first experimental study that showed consistent evidence on the cardioprotective effects of EPI, an imidazole alkaloid isolated from Pilocarpus microphyllus.
Regarding serum LDH levels measured in the different groups studied, our results demonstrated that there was no statistical difference between the groups studied, that is, SHAM, CIR and EPI15+CIR (Figure 2). Therefore, our results demonstrate that the CIR protocol used in this study caused a statistically significant increase when compared to the plasma concentration of CKT in the SHAM group. The same occurred with EPI+CIR when compared to the SHAM group. Thus, we can observe that the treatment of NWR rats with EPI 15 mg/kg was not able to reverse the increase in serum CKT value observed in the CIR group (Figure 1).
Some studies have suggested that EPI is able to reduce the extracellular Ca2+ influx in neutrophils in a sustained manner, and then significantly reducing the cellular collapse generated by the increment of intracellular Ca2+ concentration ([Ca+2]i. In fact, compounds that have the imidazole ring in their chemical structure, such as antifungal drugs belonging to the azoles class itraconazole, miconazole and ketoconazole, can inhibits the Ca2+ influx through blocking plasma membrane Ca2+ channels, as well as inhibit the displacement of intracellular Ca2+ into the cytosol of mammalian cells [18,19,10,21,22,23,24]. In the cardiovascular system, these cellular actions of EPI could generate cardioprotective effects due to pharmacological modulation of Ca2+/cAMP/ADO signaling in cardiac cells. Our studies [6,7,10] and other relevant studies have demonstrated that the attenuation of cytosolic Ca2+ overload produced by blocking of Ca2+ influx mediated by L-type Ca2+ channel (LTCC) and/or stimulation of cardiac A1-adenosine receptors (A1R) produced by endogenous adenosine (ADO) and others agonists of A1R constitute a common and effective pharmacological strategy used to abolish the cardiac arrhythmias in various clinical situations, and especially in cardiac surgery [8,9,10,25,26,27,28,29]. These EPI actions could prevent contractile dysfunctions of cardiac cells due to attenuation of cytosolic Ca2+ overload and consequent reduction of arrhythmias incidence due to reduction of the probability of excitation-contraction coupling (CECC) mismatch.
In addition to its role in CECC, LTCC-mediated Ca2+ influx in cardiac cells modulates cAMP production by AC isoforms 5 (AC5) and 6 (AC6) [8,9,10], and pharmacological block of Ca2+ via LTCC increases production and efflux of intracellular cAMP [8,9,10,30,31]. Biochemical analyses of membrane preparations in overexpression systems have been used to establish the paradigm for Ca2+-mediated inhibition of AC5 and AC6 in the sub micromolar range [8,9,10,29,30,31]. In the extracellular medium, cAMP is transformed into ADO that can stimulate A1R located in the plasma membrane of cardiac cells to finely regulate cardiac function [8,9,10]. A1R stimulation with ADO is a common and effective strategy used to abolish the cardiac arrhythmias in various clinical situations, and especially in cardiac surgery [8,9,10,29,30,31,32,33,34,35,36,37,38,39,40]. We have proposed that this pharmacological modulation of Ca2+/cAMP/ADO signaling in cardiac cells by means the attenuation of Ca2+ influx via LTCC combined with an increase of activation of A1R by ADO generated by increment of extracellular transport of cAMP may be effective to prevent sudden mortality in individuals with AMI due to severe arrhythmias brought on by cardiac collapse [41,42,43,44].
Furthermore, recent published studies also suggest that EPI is capable of blocking the phosphorylation of the p65 subunit of NF-KB and, therefore, inhibits its translocation to the cell nucleus, where this dimeric protein composed of two subunits (p50 and p65) acts by promoting modulation of gene expression and protein synthesis and, consequently, its action on gene regulation [21]. Without doubt, this inhibitory effect on NF-KB is of great importance considering that it is a fundamental step regarding the role that NF-KB plays in the inflammatory process, as it is from this process that this molecule regulates the genes responsible for the expression of pro-inflammatory cytokines (TNF-a and IL-6), adhesion molecules, chemokines, growth factors, cyclooxygenase-2, inducible nitric oxide synthase [21,22,23,24,25,26]. In addition, the pretreatment with EPI significantly reduced the levels of nitrite produced by cultured microglial cells treated with LPS, which demonstrates the anti-inflammatory effect of EPI, which, at least in part, it is related to the ability of EPI to promote inhibition of intracellular pathways responsible for the pathophysiology of inflammation, such as NF-κB and MAPKs. Furthermore, EPI was also able to inhibit the synthesis of the enzyme inducible nitric oxide synthase (iNOS), significantly reducing the production of inflammatory cytokines such as IL-1 β, IL-6 and TNF-α when compared to the group of microglial cells treated with LPS [21,22,23,24,25,26].
Okada et al. [45] demonstrated through an animal model of intestinal ischemia and reperfusion (IRI) that there is a direct relationship between increases in malondialdehyde (MDA), reactive oxygen species (ROS) and TNF-alpha and cardiac injuries, as the study demonstrated that the MDA content and TNF-alpha quantified from hearts obtained from animals belonging to the Sham group (sham-operated) was statistically lower when compared with hearts from animals in the control group, that is, animals treated with 0.9% saline solution and subjected to IRI. These results corroborate that the antioxidant and anti-inflammatory effects of EPI may be responsible for the decrease in AVB and LET in animals treated with EPI and subsequently subjected to the CIR protocol.
Pre-treatment with EPI was able to significantly reduce the production of IL-1β when compared to the values obtained from the BV-2 cell line not stimulated with LPS. EPI in the production of IL-10, an anti-inflammatory cytokine. Cells exposed to LPS reduced the production of IL-10 by approximately five times when compared to unstimulated BV-2 cells. Without a doubt, such effects probably participated in the antiarrhythmic and cardioprotective effects demonstrated in this study, as all these actions are important and relevant from the point of view of the pathophysiology of CIR.
Thus, we have proposed that pharmacological modulation of Ca2+/cAMP/ADO signaling in cardiac cells could be a promising therapeutic strategy to reduce the incidence of severe and fatal arrhythmias caused by AMI in humans. The present work supports the idea that EPI, an imidazole alkaloid isolated from Pilocarpus microphyllus, could produce cardioprotective effects due its action on the Ca2+/cAMP/ADO signaling in cardiac cells, , just as EPI can also promote cardioprotective effects through both decreasing the production of the pro-inflammatory cytokine IL-1β and increasing the production of the anti-inflammatory cytokine IL-10 and thus being a promising cardioprotective agent in the treatment of AMI.
4. Materials and Methods
4.1. Animals
Male Wistar rats (12- to 16-week-old) weighting between 280 and 320 g, were kept at 21 ± 2°C with 12:12-h light/dark cycle and were given food and water ad libitum. All experimental protocols used in this study were approved by the Ethics Committee of the Escola Paulista de Medicina – Universidade Federal de São Paulo (UNIFESP #9447210317 and #7323080822).
4.2. Cardiac ischemia and reperfusion (CIR) induction
In order to reproduce in laboratory an animal model of AMI, rats were submitted to surgical procedures in accordance with the methodology previously reported by our research group [7,8,9,10,11]. The rats were first given intraperitoneal xylazine (10 mg/kg), ketamine (100 mg/kg), and tramadol (2mg/kg) to induce unconsciousness. Rats were anesthetized, and a Jelco 14G (USA) was used for intubation. An Insight model EFF 312 mechanical ventilator (Insight Equipamentos Cientificos, Brazil) was used for mechanical ventilation [7,8,9,10,11]. After the patient was stabilized for fifteen minutes, a thoracotomy was performed to insert a vascular tourniquet (4/0 braided silk suture coupled to a 10-mm micropoint reverse cutting needle, Ethicon K-890H, USA) around the left anterior descending coronary artery to induce ischemia. After 10 minutes of myocardial ischemia, the tourniquet was removed to enable for 75 minutes of coronary.
4.3. Assessment of cardiac activity during CIR
Using a methodology previously described by our research group [7,8,9,10,11,12], the cardiac activity during CIR was evaluated by electrocardiogram (ECG) analysis. This high-resolution methodology was used in other studies to evaluate the cardioprotective effect of calcium channel blockers and other drugs on the incidence of cardiac arrhythmias (VA and AVB) and lethality (LET) resultant from CIR [7,8,9,10,11]. Initially, the ECG was recorded for 15 minutes prior to the stabilization phase and for 10 minutes during the ischemia and reperfusion protocols, which lasted for 75 minutes each [7,8,9,10,11]. The ECG was recorded using needle electrodes that were subcutaneously placed into the limbs and a biopotential amplifier. The use of ECG alterations (increase in R wave and ST segment) resulting from CIR was employed to verify the effective coronary artery.
The ECG was recorded using a biopotential amplifier and needle electrodes that were subcutaneously implanted into the limbs. The effective blockage of the coronary artery by surgery was verified by the ECG abnormalities (increase in R wave and ST segment) caused by CIR [46,47,48,49]. The body temperature was maintained at 37.5°C using a heated operating table and the appropriate heating lamps, and the temperature was frequently checked with a rectal thermometer [7,8,9,10,11]. ECG data were processed using a computer system composed by AqDados 7.02 hardware (Lynx Tecnologia Ltda, Brazil), and AqDAnalysis 7 software [7,8,9,10,11]. Using this system, we measured heart rates as well as the incidence of VA, AVB, and LET induced by CIR. Ventricular fibrillation, torsades, and atrial fibrillation were all considered VA.
4.4. Biochemical assessment of heart lesions’ biomarkers
To measure the serum levels of markers of cardiac injury biomarkers lactate dehydrogenase (LDH), creatine kinase (CK), and CK-MB, it was determined using the methodology described in our previous studies [12]. Rats that made it through the entire 75-minute CIR treatment provided the blood samples. These samples (4–5 mL) collected from the abdominal aorta and keep in siliconized tubes, were centrifuged at 2,500 rpm for 40 minutes at 5 °C. The supernatant was removed and stored at -20°C for enzymatic analysis of CK and CK-MB at 340 nm using a kinetic UV test kit from Vida Biotecnologia, Belo Horizonte, Brazil.
4.5. Pharmacological Treatments
EPI used to carry out this study was obtained from the residue obtained from the extraction of pilocarpine from the leaves of Pilocarpus microphyllus [17]. The organic phase was subjected to liquid-liquid extraction, alkalinized with ammonium hydroxide solution to precipitate EPI in neutral form and then the solution was filtered under reduced pressure. Then, to remove all impurities, EPI was subjected to the purification process by high-performance liquid chromatography (HPLC), proving to be pure by HPLC (>95%) and showed data consistent with literature values [17]. We used EPI 10 mg/kg and 15 mg/kg, intravenously, on the incidence of VA, AVB and LET caused by CIR, rats were treated with the EPI intravenously (IV) before of CIR. In the present work, the animals used were divided into the following experimental groups:
1) SHAM-operated group (n = 8) - Rats submitted to all CIR procedures, except for both left descending coronary artery tourniquet and myocardial reperfusion and submitted to ECG analysis for determination of the VA, AVB and LET incidence.
2) CIR group (n =30) – Rats submitted to CIR pretreated with saline solution (SS) 0.9% (IV), and submitted to ECG analysis for determination of the VA, AVB and LET incidence;
3) EPI10+CIR group (n = 10) - Rats submitted to CIR pretreated with EPI (10 mg/kg, IV), and submitted to ECG analysis for determination of the VA, AVB and LET incidence;
4) EPI15+CIR group (n = 10) – Rats submitted to CIR pretreated with EPI (15 mg/kg, IV), and submitted to ECG analysis for determination of the VA, AVB and LET incidence.
4.6. Statistical analysis
Using the Prism 8.0 program (GraphPad, USA), data related to VA, AVB, and LET incidences were expressed as percentages and statistically analyzed using Fisher’s exact Test [11]. The values of LDH, total CK and CK-MB were measured in terms of serum concentration (U/L) and expressed as mean ± standard error of mean (SEM). The data were submitted to an Analysis of Variance Test using Prism for statistical analysis. The results were considered statistically significant when p < 0.05 [11].
5. Conclusions
The results obtained in the present study suggest that treatment with EPI decreased both AVB and LET, in a dose-dependent manner, in rats subjected to the CIR protocol and, therefore, appears to be a potential and promising pharmacotherapeutic strategy to reduce the incidence of serious and fatal arrhythmias caused by ischemic heart diseases, such as AMI in humans.
Author Contributions
Conception and design of the study and technical procedures—P.I.D.M.M., F.S.T., R.Y.L, S.A.G.P and E.A.d.A.; interpretation of electrocardiogram and manuscript— P.I.D.M.M. and F.S.T.; analysis and interpretation of data and statistical analysis—R.B.F., C.T.F.O., G.S.O., and A.N.A.; analysis and interpretation of data and manuscript— R.B.G., L.A.D.N., L.M.C.V., and J.V.R.M.; conception and design of the study and interpretation of electrocardiogram—J.G.P.T., M.O.T. and A.I.D.; conception and design of the study and critical revision— C.E.B.F., M.N.M., A.G.W., A.C-N.; conception and design of the study, interpretation of data, and critical revision— A.G.W, A.C.-N. and F.S.M.-R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received external funding from CNPq, CAPES, and FAPESP (#2017/25565-1).
Institutional Review Board Statement
The animal study protocol was approved by the Ethics Committee on the Use of Animals of the Universidade Federal de São Paulo (protocol codes UNIFESP #9447210317 and #7323080822 approved in 2017 and 2022, respectively). Informed Consent Statement: Not applicable.
Data Availability Statement
The data will be available upon justified request and agreement of the authors.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; de Ferranti, S.; Després, J.-P.; Fullerton, H.J.; Howard, V.J.; et al. Heart Disease and Stroke Statistics--2015 Update: A Report from the American Heart Association. Circulation 2015, 131, e29-322.
- Writing Group Members; Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; Das, S.R.; de Ferranti, S.; Després, J.-P.; et al. Heart Disease and Stroke Statistics-2016 Update: A Report From the American Heart Association. Circulation 2016, 133, e38-360.
- Rutledge, T.; Reis, V.A.; Linke, S.E.; Greenberg, B.H.; Mills, P.J. Depression in Heart Failure a Meta-Analytic Review of Prevalence, Intervention Effects, and Associations with Clinical Outcomes. J. Am. Coll. Cardiol. 2006, 48, 1527–1537.
- Frampton, J.; Ortengren, A.R.; Zeitler, E.P. Arrhythmias After Acute Myocardial Infarction. Yale J. Biol. Med. 2023, 96, 83–94.
- Naryzhnaya, N. V; Maslov, L.N.; Derkachev, I.A.; Ma, H.; Zhang, Y.; Prasad, N.R.; Singh, N.; Fu, F.; Pei, J.-M.; Sarybaev, A.; et al. The Effect of an Adaptation to Hypoxia on Cardiac Tolerance to Ischemia/Reperfusion. J. Biomed. Res. 2022, 1–25. [CrossRef]
- Panuccio, G.; Carabetta, N.; Torella, D.; De Rosa, S. Clinical impact of coronary revascularization over medical treatment in chronic coronary syndromes: a systematic review and meta-analysis. Hellenic J Cardiol. 2023, S1109-9666, 00194-X. [CrossRef]
- Menezes-Rodrigues, F.S.; Tavares, J.G.P.; Vasques, E.R.; Errante, P.R.; Araújo, E.A. de; Pires-Oliveira, M.; Scorza, C.A.; Scorza, F.A.; Taha, M.O.; Caricati-Neto, A. Cardioprotective Effects of Pharmacological Blockade of the Mitochondrial Calcium Uniporter on Myocardial Ischemia-Reperfusion Injury. Acta Cir. Bras. 2020, 35, e202000306. [CrossRef]
- Menezes-Rodrigues, F.S.; de Oliveira, M.P.; Araújo, EA.; Ferraz, HB.; Finsterer, J.; Olszewer, E.; Taha, M.O.; Scorza, C.A.; Caricati-Neto, A.; Scorza, F.A. Role of cardiac β1-adrenergic and A1-adenosine receptors in severe arrhythmias related to Parkinson’s disease. Clinics. 2023, 78, 100243.
- Menezes-Rodrigues, F.S.; Errante, P.R.; Tavares, J.G.P.; Ferraz, R.R.N.; Gomes, W.J.; Taha, M.O.; Scorza, C.A.; Scorza, F.A.; Caricati-Neto, A. Pharmacological Modulation of B-Adrenoceptors as a New Cardioprotective Strategy for Therapy of Myocardial Dysfunction Induced by Ischemia and Reperfusion. Acta Cir. Bras. 2019, 34, e201900505. [CrossRef]
- Filho, C.E.B.; Barbosa, A.H.P.; Nicolau, L.A.D.; Medeiros, J.V.R.; Pires-Oliveira, M.; Dos Santos Póvoa, R.M.; Govato, T.C.P.; Júnior, H.J.F.; de Carvalho, R.G.; Luna-Filho, B.; Sabia Tallo, F.; de Araújo, E.A.; Padrão Tavares, J.G.; Arida, R.M.; Caricati-Neto, A.; Menezes-Rodrigues, F.S. Pharmacological Modulation by Low Molecular Weight Heparin of Purinergic Signaling in Cardiac Cells Prevents Arrhythmia and Lethality Induced by Myocardial Infarction. J Cardiovasc Dev Dis 2023, 10, 103. [CrossRef]
- Tallo FS, de Santana PO, Pinto SAG, Lima RY, de Araújo EA, Tavares JGP, Pires-Oliveira M, Nicolau LAD, Medeiros JVR, Taha MO, David AI, Luna-Filho B, Filho CEB, Barbosa AHP, Silva CMC, Wanderley AG, Caixeta A, Caricati-Neto A, Menezes-Rodrigues FS. Pharmacological Modulation of the Ca2+/cAMP/Adenosine Signaling in Cardiac Cells as a New Cardioprotective Strategy to Reduce Severe Arrhythmias in Myocardial Infarction. Pharmaceuticals (Basel). 2023, 16, 1473.
- Gersh, B.J. [The changing prognosis of myocardial infarction in the reperfusion era: implications for evaluation and management of ventricular arrhythmias]. Rev Esp Cardiol 2003, 56, 535-42.
- Santos, A.P.; Moreno, P. R. H. Pilocarpus spp.: A survey of its chemical constituents and biological activities. Brazilian Journal of Pharmaceutical Sciences 2004, 40, 116-137, 2004. [CrossRef]
- Pinheiro, C.U. Jaborandi (Pilocarpus sp., rutaceae): a wild species. Econ. Bot. 1997, 51, 49–58. [CrossRef]
- Andrade-Neto, M.; Mendes, P. H.; Silveira, E. R. An imidazole alkaloid and other constituents from Pilocarpus trachyllophus. Phytochemistry 1996, 42, 885−887. [CrossRef]
- Carvalho, W.A.; Lemônica, L. Molecular and Cellular Mechanisms of Inflammatory Pain. Peripheral Modulation and Therapeutic Advances. Revista Brasileira de Anestesiologia 1998, 48, 137-158.
- Veras,L.M.; Guimaraes, M.A.; Campelo, Y.D.; Vieira, M.M.; Nascimento, C.; Lima, D.F.; Vasconcelos, L.; Nakano, E.; Kuckelhaus, S.S.; Batista, M.C.; Leite, J.R.; Moraes, J.. Activity of epiisopiloturine against Schistosoma mansoni. Curr Med Chem 2012, 19, 2051-8. [CrossRef]
- Silva, V.G.; Silva, R.O.; Damasceno, S.R.B.; Carvalho, N.S.; Prudêncio, RS.; Aragão, KS.; Guimarães, M.A.; Campos, S.A.; Véras, L.M.C.; Godejohann, M.; Leite, J.R.S.A,; Barbosa, A.L.R.; Medeiros, J-V.R. Anti-inflammatory and antinociceptive activity of epiisopiloturine, an imidazole alkaloid isolated from Pilocarpus microphyllus. J Nat Prod 2013, 76, 1071-7. [CrossRef]
- Rocha, T.M.; Machado, N.J.; de Sousa, J.A.C.; Araujo, E.V.O.; Guimaraes, M.A.; Lima, D.F.; de Almeida Leite, J.R.S.; Leal, L.K.A.M. Imidazole alkaloids inhibit the pro-inflammatory mechanisms of human neutrophil and exhibit anti-inflammatory properties in vivo. Journal of Pharmacy and Pharmacology 2019, 71, 849–859.
- Silva, V.G.; Silva, R.O.; Damasceno, S.R.B.; Carvalho, N.S.; Prudêncio, R.S.; Aragão, K.S.; Guimarães, M.A.; Campos, S.A.; Véras, L.M.C.; Godejohann, M.; Leite, J.R.S.; Barbosa, A.L.R.; Medeiros, J-V.R. Anti-inflammatory and antinociceptive activity of epiisopiloturine, an imidazole alkaloid isolated from Pilocarpus microphyllus. J Nat Prod. 2013, 76, 1071-7. [CrossRef]
- de Sousa, J.A.C.; Azul, F.V.C.S.; de Araújo, A.B.; Tomé, R.C.; Silva, F.R.M.; de Vasconcelos, S.M.M.; Rios, F.J.; Leal, L.K.A.M. Epiisopiloturine, an Alkaloid from Pilocarpus microphyllus, Attenuates LPS-Induced Neuroinflammation by Interfering in the TLR4/NF-κB-MAPK Signaling Pathway in Microglial Cells. Oxid Med Cell Longev 2023, 2023, 4752502.
- Sousa, P.S.deA.; Nogueira, S.S.; Ayala, K.N.R.; Silva, P.C.; Santos, E.daS.; Sá, R.E.de.; Lima Neto, F.E.M.de.; LIMA, J.R.daC.; Rodrigues, K.A.da F.; Rocha, J.A.; Véras, L.M.C. Scientific and technological prospection of Pilocarpus microphyllus and the alkaloid epiisopiloturine with emphasis on antileishmanial activity. Research, Society and Development 2021, 10, e59810716984.
- de Carvalho, L.R.; de Brito, T.V.; Júnior , J.S.C.; Júnior, G.J.D.; Magalhãres, D.deA.; Sousa, S.G.; Silva, R.O.; da Silva, F.R.P.; Vasconcelos, D.S.P.; Véras, L.M.C.; Leite, J.R.deS.deA.; Martins, D.S.; Martins, C.daS.; de Oliveira, J.S.; Barbosa, A.L.D.R.. Epiisopiloturine, an imidazole alkaloid, reverses inflammation and lipid peroxidation parameters in the Crohn disease model induced by trinitrobenzenosulfonic acid in Wistar rats. Biomed Pharmacother 2018, 102, 278-285.
- Nicolau, L.A.D.; Carvalho, N.S.; Pacífico, D.M.; Lucetti, L.T.; Aragão, K.S.; Véras, L.M.C.; Souza, M.H.L.P.; Leite, J.R.S.A.; Medeiros, J.V.R. Epiisopiloturine hydrochloride, an imidazole alkaloid isolated from Pilocarpus microphyllus leaves, protects against naproxen-induced gastrointestinal damage in rats. Biomed Pharmacother 2017,87, 188-195. [CrossRef]
- Bers, D.M. Calcium Cycling and Signaling in Cardiac Myocytes. Annu. Rev. Physiol. 2008, 70, 23–49. [CrossRef]
- Wagner, S.; Maier, L.S.; Bers, D.M. Role of Sodium and Calcium Dysregulation in Tachyarrhythmias in Sudden Cardiac Death. Circ. Res. 2015, 116, 1956–1970. [CrossRef]
- Halestrap, A.P.; Clarke, S.J.; Khaliulin, I. The Role of Mitochondria in Protection of the Heart by Preconditioning. Biochim. Biophys. Acta 2007, 1767, 1007–1031. [CrossRef]
- Xie, L.-H.H.; Weiss, J.N. Arrhythmogenic Consequences of Intracellular Calcium Waves. Am. J. Physiol. Heart Circ. Physiol. 2009, 297, H997–H1002. [CrossRef]
- Peart, J.; Flood, A.; Linden, J.; Matherne, G.P.; Headrick, J.P. Adenosine-Mediated Cardioprotection in Ischemic-Reperfused Mouse Heart. J. Cardiovasc. Pharmacol. 2002, 39, 117–129. [CrossRef]
- Lasley, R.D.; Rhee, J.W.; Van Wylen, D.G.; Mentzer, R.M. Adenosine A1 Receptor Mediated Protection of the Globally Ischemic Isolated Rat Heart. J. Mol. Cell. Cardiol. 1990, 22, 39–47.
- Yu, H.J.; Ma, H.; Green, R.D.; Hai Jing Yu; Ma, H.; Green, R.D.; Yu, H.J.; Ma, H.; Green, R.D. Calcium Entry via L-Type Calcium Channels Acts as a Negative Regulator of Adenylyl Cyclase Activity and Cyclic AMP Levels in Cardiac Myocytes. Mol. Pharmacol. 1993, 44, 689–693.
- Sellers, Z.M.; Naren, A.P.; Xiang, Y.; Best, P.M. MRP4 and CFTR in the Regulation of cAMP and β-Adrenergic Contraction in Cardiac Myocytes. Eur. J. Pharmacol. 2012, 681, 80–87. [CrossRef]
- Muthal, A.P.; Kulkarni, R.; Kumar, D.; Bagul, C.; Mukherjee-Kandhare, A.A.; Kandhare, A.D.; Ambavade, S.D.; Wagh, V.; Bodhankar, S.L. Cyclic adenosine monophosphate: Recent and future perspectives on various diseases. Journal of Applied Pharmaceutical Science. 2022, 12, 001-015.
- Halls, M.L.; Cooper, D.M.F. Regulation by Ca2+-Signaling Pathways of Adenylyl Cyclases. Cold Spring Harb Perspect Biol 2011, 3, a004143. [CrossRef]
- Lasley, R.D.; Mentzer, R.M. Dose-Dependent Effects of Adenosine on Interstitial Fluid Adenosine and Postischemic Function in the Isolated Rat Heart. J. Pharmacol. Exp. Ther. 1998, 286, 806–811.
- Lasley, R.D.; Kristo, G.; Keith, B.J.; Mentzer, R.M. The A2a/A2b Receptor Antagonist ZM-241385 Blocks the Cardioprotective Effect of Adenosine Agonist Pretreatment in in Vivo Rat Myocardium. Am. J. Physiol. Heart Circ. Physiol. 2007, 292, H426-31. [CrossRef]
- Dhalla, A.K.; Shryock, J.C.; Shreeniwas, R.; Belardinelli, L. Pharmacology and Therapeutic Applications of A1 Adenosine Receptor Ligands. Curr. Top. Med. Chem. 2003, 3, 369–385. [CrossRef]
- Burnstock, G.; Pelleg, A. Cardiac Purinergic Signalling in Health and Disease. Purinergic Signal. 2015, 11, 1–46. [CrossRef]
- Belardinelli, L.; Lerman, B.B. Adenosine: Cardiac Electrophysiology. Pacing Clin. Electrophysiol. 1991, 14, 1672–1680. [CrossRef]
- Shryock, J.C.; Belardinelli, L. Adenosine and Adenosine Receptors in the Cardiovascular System: Biochemistry, Physiology, and Pharmacology. Am. J. Cardiol. 1997, 79, 2–10. [CrossRef]
- Zhan, E.; McIntosh, V.J.; Lasley, R.D. Adenosine A₂A and A₂B Receptors Are Both Required for Adenosine A₁ Receptor-Mediated Cardioprotection. Am. J. Physiol. Heart Circ. Physiol. 2011, 301, H1183-9.
- Urmaliya, V.B.; Church, J.E.; Coupar, I.M.; Rose’Meyer, R.B.; Pouton, C.W.; White, P.J. Cardioprotection Induced by Adenosine A1 Receptor Agonists in a Cardiac Cell Ischemia Model Involves Cooperative Activation of Adenosine A2A and A2B Receptors by Endogenous Adenosine. J. Cardiovasc. Pharmacol. 2009, 53, 424–433. [CrossRef]
- Safran, N.; Shneyvays, V.; Balas, N.; Jacobson, K.A.; Nawrath, H.; Shainberg, A. Cardioprotective Effects of Adenosine A1 and A3 Receptor Activation during Hypoxia in Isolated Rat Cardiac Myocytes. Mol. Cell. Biochem. 2001, 217, 143–152. [CrossRef]
- Du, L.; Gao, Z.-G.; Nithipatikom, K.; Ijzerman, A.P.; Veldhoven, J.P.D. van; Jacobson, K.A.; Gross, G.J.; Auchampach, J.A. Protection from Myocardial Ischemia/Reperfusion Injury by a Positive Allosteric Modulator of the A₃ Adenosine Receptor. J. Pharmacol. Exp. Ther. 2012, 340, 210–217. [CrossRef]
- Okada, M.; Falcão, L.F.R.; Ferez, D.; Martins, J.L.; Errante, P.R.; Rodrigues, F.S.M.; Caricati-Neto, A.; Marinho, M.; Fenelon, G.; Oliveira-Júnior. I.S.; Effect of atenolol pre-treatment in heart damage in a model of intestinal ischemia-reperfusion. Acta Cir. Bras 2017, 32, 964-972. [CrossRef]
- Di Diego, J.M.; Antzelevitch, C. Cellular Basis for ST-Segment Changes Observed during Ischemia. J. Electrocardiol. 2003, 36 Suppl, 1–5.
- Yan, G.-X.; Lankipalli, R.S.; Burke, J.F.; Musco, S.; Kowey, P.R. Ventricular Repolarization Components on the Electrocardiogram: Cellular Basis and Clinical Significance. J. Am. Coll. Cardiol. 2003, 42, 401–409.
- Walker, M.J.; Curtis, M.J.; Hearse, D.J.; Campbell, R.W.; Janse, M.J.; Yellon, D.M.; Cobbe, S.M.; Coker, S.J.; Harness, J.B.; Harron, D.W. The Lambeth Conventions: Guidelines for the Study of Arrhythmias in Ischaemia Infarction, and Reperfusion. Cardiovasc. Res. 1988, 22, 447–455. [CrossRef]
- Huggins, C.E.; Bell, J.R.; Pepe, S.; Delbridge, L.M.D. Benchmarking Ventricular Arrhythmias in the Mouse--Revisiting the “Lambeth Conventions” 20 Years On. Heart. Lung Circ. 2008, 17, 445–450.
Figure 1.
Histograms representing the (A) Incidence of ventricular arrhythmias (AV), (B) Atrioventricular block (AVB) and (C) Lethality (LET) in the SHAM, CIR, EPI10+CIR (EPI 10 mg/kg), and EPI10+CIR (EPI 15mg/kg) groups. Results were expressed as mean and statistical analysis was performed using Fisher’s exact test (*p < 0.05). The incidence of VA, AVB and LET were significantly reduced in all groups of animals treated with EPI15mg/kg submitted to CIR when compared to the CIR. *p < 0.05 statistically different when compared to the SHAM group. **p < 0.05 statistically different when compared to CIR group.
Figure 1.
Histograms representing the (A) Incidence of ventricular arrhythmias (AV), (B) Atrioventricular block (AVB) and (C) Lethality (LET) in the SHAM, CIR, EPI10+CIR (EPI 10 mg/kg), and EPI10+CIR (EPI 15mg/kg) groups. Results were expressed as mean and statistical analysis was performed using Fisher’s exact test (*p < 0.05). The incidence of VA, AVB and LET were significantly reduced in all groups of animals treated with EPI15mg/kg submitted to CIR when compared to the CIR. *p < 0.05 statistically different when compared to the SHAM group. **p < 0.05 statistically different when compared to CIR group.
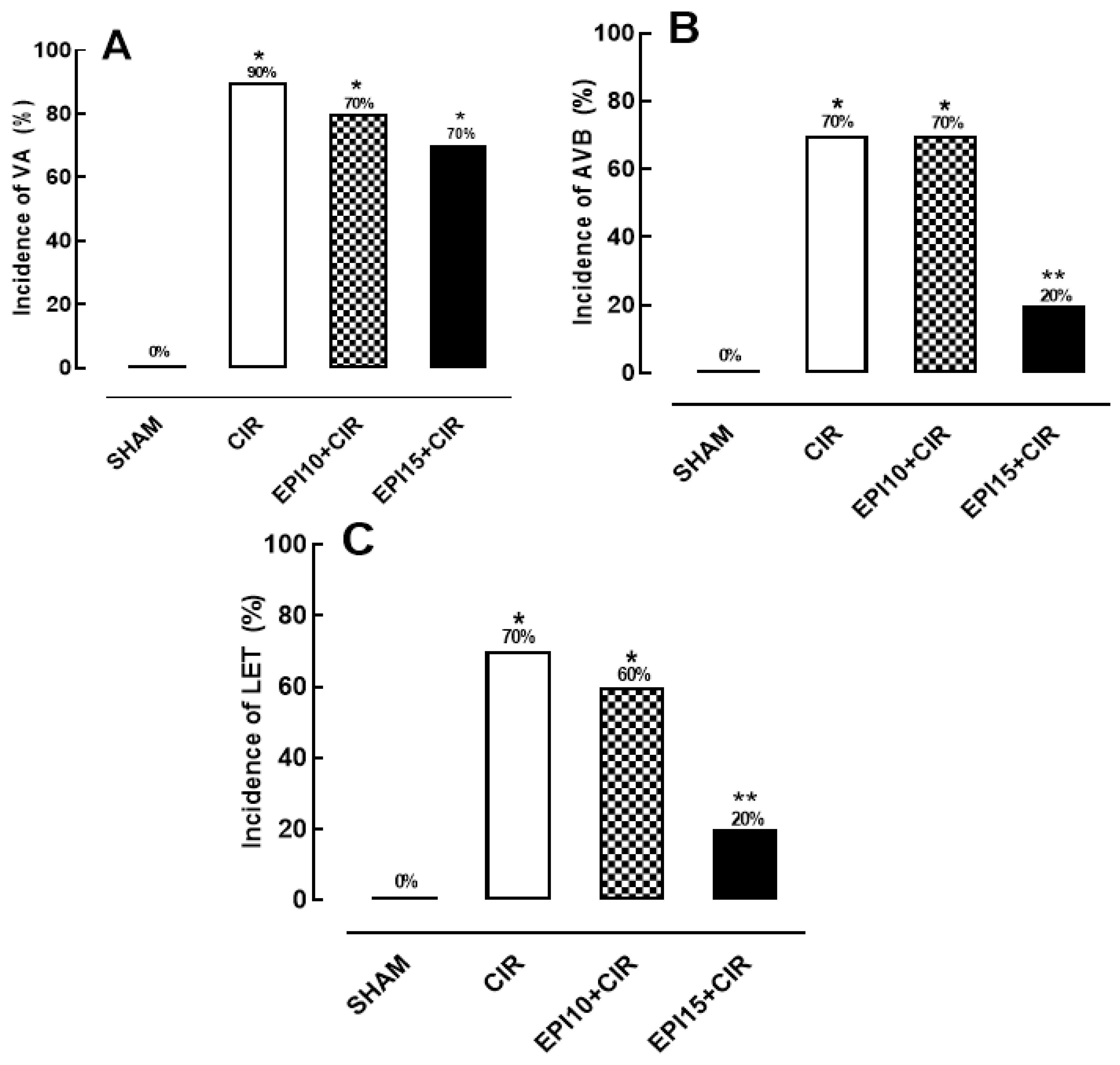
Figure 2.
Serum concentration of Lactate dehydrogenase (LDH) in the SHAM, CIR and EPI 15mg/kg groups. The results were expressed as mean ± standard error of the mean and analysis of variance (ANOVA) was applied, followed by Tukey’s post-test (*p<0.05). SHAM= sham-operated group; CIR= group treated with saline and subjected to cardiac ischemia and reperfusion; EPI 15mg/kg = group treated with epiisopiloturine and then subjected to cardiac ischemia and reperfusion.
Figure 2.
Serum concentration of Lactate dehydrogenase (LDH) in the SHAM, CIR and EPI 15mg/kg groups. The results were expressed as mean ± standard error of the mean and analysis of variance (ANOVA) was applied, followed by Tukey’s post-test (*p<0.05). SHAM= sham-operated group; CIR= group treated with saline and subjected to cardiac ischemia and reperfusion; EPI 15mg/kg = group treated with epiisopiloturine and then subjected to cardiac ischemia and reperfusion.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



